Latissimus Dorsi Transfer for Irreparable Posterosuperior Rotator Cuff Tears: An Intraoperative Masterclass
Key Takeaway
Join us in the OR for a comprehensive masterclass on Latissimus Dorsi Transfer for irreparable posterosuperior rotator cuff tears. We'll meticulously cover patient selection, intricate surgical anatomy, precise intraoperative steps, critical pearls and pitfalls, and robust postoperative rehabilitation protocols. This detailed guide ensures a deep understanding of technique and rationale for optimal patient outcomes.
Alright, fellows, welcome to the operating theater. Today, we're tackling a challenging but incredibly rewarding procedure: the Latissimus Dorsi Transfer for an irreparable posterosuperior rotator cuff tear. This isn't a procedure we undertake lightly; it requires meticulous patient selection, a profound understanding of surgical anatomy, and precise execution. Our goal is to restore active abduction and external rotation, significantly improving the patient's quality of life.
Understanding the Irreparable Tear
First, let's define what we mean by an "irreparable" tear. We're talking about tears involving the supraspinatus and infraspinatus tendons where, even with the arm at the side, we cannot achieve a tension-free repair back to the anatomic footprint of the greater tuberosity. Preoperatively, severe muscle atrophy of the supraspinatus or infraspinatus on MRI or CT scans can strongly indicate irreparability. However, the final determination, as always, is made right here, at the time of surgery, when we assess tissue quality and tendon retraction directly.
Comprehensive Surgical Anatomy: Navigating the Landscape
Before we make a single incision, a thorough understanding of the regional anatomy is paramount. This is where precision prevents peril.
The Latissimus Dorsi Muscle and Tendon:
The latissimus dorsi is a broad, powerful muscle with a vast origin from the aponeurosis of spinous processes T7 through L5, the sacrum, the iliac wing, ribs 9 through 12, and the inferior border of the scapula. Its fibers twist a remarkable 180 degrees from origin to insertion. This anatomical peculiarity allows the muscle, originating posteriorly, to insert immediately anterior to the teres major tendon on the proximal humerus. Its tendon averages 3.1 cm wide and 8.4 cm long at its insertion. Critically, the latissimus dorsi humeral insertion never extends more distal along the humeral shaft than that of the teres major. This distinction is vital during our dissection.
Neurovascular Pedicle:
The lifeblood and innervation of our transfer depend entirely on the thoracodorsal artery and nerve. This neurovascular pedicle, originating from the posterior cord (C6 and C7), enters the anterior, inferior surface of the latissimus dorsi, approximately 13 cm from its humeral insertion site. Anatomic studies confirm this pedicle is typically of adequate length to allow for a tension-free transfer, provided we meticulously release any adhesions and fibrous bands from the anterior surface of the muscle belly.
Relationship with Teres Major:
In most patients, the latissimus dorsi and teres major tendons insert separately onto the proximal humerus. However, be aware that in about 30% of patients, these tendons are conjoined. In such cases, sharp dissection will be required to achieve separation, and we must proceed with extreme caution.
Neurovascular Structures of Concern:
Several critical neurovascular structures lie in close proximity to the latissimus dorsi insertion, and meticulous attention during its release is non-negotiable to avoid devastating injuries.
- Radial Nerve: This nerve passes anterior to the latissimus, averaging 2.4 cm medial to the humeral shaft at the superior border of the tendon. Remember, this distance increases with external rotation and abduction and decreases with internal rotation and adduction. We'll be mindful of arm positioning throughout the case.
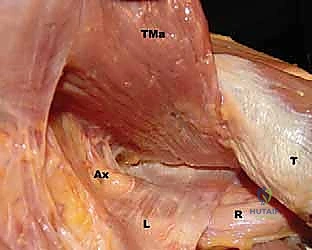
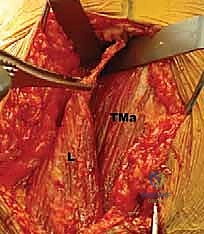
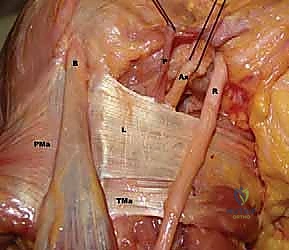
FIG 1 • A. Cadaveric dissection showing the interval between the teres major (TMa) and latissimus dorsi (L) tendons, with the radial nerve (R) deep to the latissimus and the axillary nerve (Ax) superior.
- Axillary Nerve: The axillary nerve runs superior to the latissimus dorsi tendon before exiting the quadrangular space. In neural rotation and adduction, the average distance between the nerve and the superior border of the tendon is 1.9 cm. Like the radial nerve, this distance increases with external rotation and abduction and decreases with internal rotation.

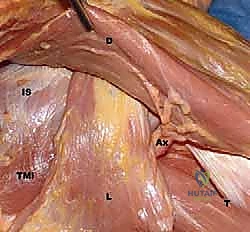
FIG 1 • C. Cadaveric dissection of the superficial muscular anatomy of the posterior shoulder, showing the axillary nerve (Ax) exiting the quadrilateral space.
- Anterior Humeral Circumflex Artery: This vessel runs along the superior border of the latissimus dorsi tendon.
The Rotator Cuff and its Footprint:
The supraspinatus and infraspinatus muscle-tendon units originate from their respective fossae and become confluent, inserting as a common tendon on the greater tuberosity of the humerus, immediately lateral to the humeral head articular margin. Their combined footprint area averages 4.02 cm². The supraspinatus insertion averages 1.27 cm medial to lateral and 1.63 cm anterior to posterior, while the infraspinatus insertion averages 1.34 cm medial to lateral and 1.64 cm anterior to posterior. The deepest fibers of these tendons are intimately interwoven with the joint capsule, forming a functional unit. Consequently, tears here lead to direct communication between the glenohumeral and subacromial spaces.
Preoperative Planning: Setting the Stage for Success
Our success hinges on meticulous planning and patient selection.
Patient History and Physical Findings:
A detailed history is crucial. We need to determine the mechanism and duration of symptoms: was there a specific traumatic event, or is this an acute-on-chronic presentation? The duration of dysfunction is key, as fatty degeneration of the supraspinatus and infraspinatus muscle bellies can begin within weeks, significantly decreasing tissue compliance and increasing tension on any potential repair. A careful neurologic examination, starting with the neck, must be performed to rule out neurologic causes of shoulder symptoms.
A focused examination for the rotator cuff-deficient shoulder includes:
* Active Forward Flexion: Patients with function at or above shoulder level preoperatively are more likely to achieve improved active forward flexion postoperatively.
* Active External Rotation: Decreased external rotation on the affected side indicates partial or complete loss of infraspinatus function.
* External Rotation Lag Sign: An inability to maintain maximal external rotation (≥ 20-degree lag) strongly suggests tear extension well into the infraspinatus.
* Passive Range of Motion: Compare to the contralateral limb. Decreased passive ROM suggests joint contracture, which must be addressed before considering a muscle transfer.
* Modified Belly Press Test: Inability to perform this action indicates a dysfunctional or torn subscapularis tendon, and these patients have a higher rate of clinical failure with latissimus transfer.
* Abduction Strength Testing: Tests deltoid strength. A weak deltoid suggests less postoperative active range of motion.
* External Rotation Strength Testing: Weakness suggests progressive infraspinatus involvement or dysfunction.
* Evaluation for Superior Escape: Superior escape suggests an incompetent coracoacromial arch and a high likelihood of failure to improve with muscle transfer.
Imaging and Diagnostic Studies:
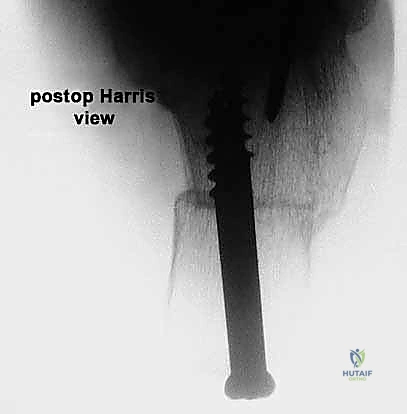
* Radiographs: We obtain true anteroposterior (AP) views of the shoulder in the plane of the scapula and axillary views. These allow us to evaluate glenohumeral arthritis, superior migration of the humeral head, and identify any abnormal bony anatomy.
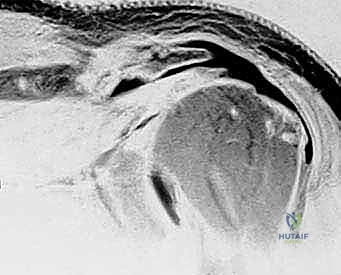
FIG 3 • A. True AP radiographic view showing minimal superior migration and preserved joint space.

FIG 3 • A. Continued: True AP radiographic view.

FIG 3 • B. Axillary lateral view demonstrating joint space preservation and absence of osteophytes.

FIG 3 • C. Radiographic findings of degenerative arthritis with osteophyte formation and superior migration.

FIG 3 • D. Axillary lateral view showing osteoarthritis with early posterior glenoid wear, suggestive of a poor candidate.
- MRI: This is indispensable for evaluating the rotator cuff, biceps tendon, labral, and capsular pathology. We assess the size of the tear, especially subscapularis and infraspinatus involvement, the distance of tendon retraction from the greater tuberosity, and critically, the extent of fatty degeneration in the involved muscle bellies. These changes, often irreversible, lead to decreased tendon excursion and tissue compliance.
- Electromyography (EMG): Necessary if nerve pathology is suspected as a cause of shoulder dysfunction.
Patient Selection: Who is the Ideal Candidate?
This is perhaps the most critical determinant of success. We are looking for a very specific subset of patients.
-
Ideal Candidate Profile:
- Younger patients (though age is relative).
- Good deltoid and subscapularis muscle strength.
- Limited glenohumeral arthritis (no significant superior migration or osteophytes).
- Ability to achieve shoulder-level active forward flexion preoperatively.
- Patients with at least shoulder-level active elevation, with improvement after a positive injection test (10 cc lidocaine into the glenohumeral joint), and without shoulder arthritis.
- Primary indication for surgery is often pain, not just weakness.
- The possibility of needing autograft or allograft tendon to augment the length of the latissimus dorsi transfer should be discussed preoperatively.
-
Less Ideal Candidates (Consider Alternatives):
- Significant glenohumeral arthritis.
- Incompetent subscapularis (positive modified belly press).
- Significant deltoid weakness.
- Superior escape.
- Older patients (e.g., over 65), retired, with low functional demands, whose primary indication is pain, may still be candidates if other criteria are met.
Differential Diagnosis:
Always consider: frozen shoulder, adhesive capsulitis, a massive rotator cuff tear that can be repaired, cervical nerve root compression, suprascapular nerve palsy, and deltoid dysfunction.
Nonoperative Management:
For those not ready or suitable for surgery, nonoperative management focuses on pain management and optimizing current function. This includes physical therapy (maintaining motion, strengthening deltoid and scapular stabilizers, periscapular muscles, internal/external rotators, stretching), cortisone injections (40-80 mg triamcinolone with 5-10 mL 1% Xylocaine in subacromial-glenohumeral space), and activity/expectation modification.
Alternative Surgical Interventions:
For patients who fail nonoperative management but are not good candidates for latissimus transfer, alternatives include:
* Limited-goals arthroscopic débridement: Synovial débridement, bursectomy, abrasion chondroplasty, acromioplasty–greater tuberosity-plasty, and biceps tenotomy or tenodesis to decrease mechanical symptoms.
* Reverse total shoulder arthroplasty: For low-demand patients with significant glenohumeral arthritis and cuff tear arthropathy.
* Shoulder fusion: In young, high-demand manual laborers.
Patient Positioning and Setup
Alright, team, let's get our patient positioned.
- Anesthesia: General anesthesia is standard. We'll also use an interscalene block for postoperative pain control.
- Positioning: We'll position the patient in the beach chair position. This allows for excellent access to both the posterior shoulder for the latissimus harvest and the superior/lateral shoulder for the recipient site.
- Secure the patient firmly to the operating table using a beanbag or vacuum positioner.
- Ensure the head is well-supported and protected, with adequate padding.
- The torso should be slightly elevated, approximately 30-45 degrees, with the back of the table slightly flexed.
- The operative arm needs to be free-draped to allow full range of motion intraoperatively. We'll use an arm holder or assistant to control the arm.
- Fluoroscopy: The C-arm will be positioned to allow for quick and easy AP and axillary views of the glenohumeral joint, which may be needed to confirm hardware placement or assess humeral head position.
- Sterile Prep and Drape: A wide sterile prep of the entire shoulder, axilla, and ipsilateral chest wall is crucial, extending down to the iliac crest if a fascial graft is anticipated. The arm will be draped free, as mentioned, to allow full mobility.
Step-by-Step Intraoperative Execution: The Masterclass Unfolds
Now, let's get scrubbed in and begin.
Phase 1: Exposure and Harvest of the Latissimus Dorsi
-
Skin Incision (Posterior Approach):
- We'll start with a curvilinear incision over the posterior aspect of the shoulder and axilla. Begin inferior to the posterior axillary fold, extending superiorly and laterally towards the posterior aspect of the acromion. The length will be approximately 10-12 cm, adjusting as needed for full exposure of the latissimus dorsi muscle belly and its pedicle.
- Surgeon's Directive: "Scalpel, please. Let's make our initial incision, fellows, observing the skin tension lines as much as possible for optimal cosmesis, but prioritizing exposure."
-
Subcutaneous Dissection:
- Carefully incise the subcutaneous tissues and identify the deep fascia. Use electrocautery for hemostasis.
- Surgeon's Directive: "Maintain a clean field, fellows. We're looking for the fascial plane here. Keep your dissection sharp and precise."
-
Identifying the Latissimus Dorsi and Teres Major:
- We'll identify the posterior border of the deltoid and retract it superiorly. Deep to this, we will find the latissimus dorsi and teres major muscles. The latissimus dorsi is typically more superficial and inferior to the teres major at this level.
- Surgeon's Directive: "Now, identify the interval between the deltoid and the underlying structures. We're looking for the characteristic fibers of the latissimus and teres major. Feel the muscle bellies – the latissimus is broad and flat."

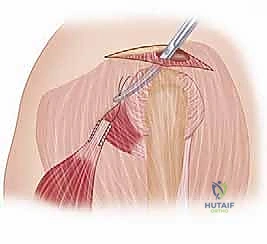
FIG 4 • A. Incision for latissimus dorsi transfer, extending from the posterior axillary fold to the posterior acromion.
-
Dissection of the Latissimus Dorsi Tendon and Humeral Insertion:
- Carefully dissect along the superior border of the latissimus dorsi, separating it from the teres major tendon. This is where we need to be acutely aware of the neurovascular structures.
- Surgeon's Directive: "Let's use our blunt dissection here initially, then sharp dissection as needed. We're working towards the humeral insertion. Remember the 180-degree twist of the latissimus fibers."
- Crucial Step: Identify the conjoined tendon if present (30% of cases). If so, carefully separate the latissimus from the teres major using sharp dissection.
- Surgeon's Directive: "Maintain constant awareness of the radial nerve. It lies anterior to the latissimus. We'll internally rotate and adduct the arm to increase its distance from our working field, but we must protect it throughout this release."
- We will release the latissimus dorsi tendon from its humeral insertion. I prefer to leave a small cuff of tendon on the humerus for later closure if possible, but the priority is a clean release.
- Surgical Warning:
> PITFALL: Radial Nerve Injury. The radial nerve is extremely vulnerable during the release of the latissimus dorsi tendon from the humerus. Keep the arm in abduction and external rotation as much as possible during this phase to maximize the distance between the nerve and the tendon's superior border. Use a blunt instrument (e.g., a small Hohmann retractor) to gently sweep and protect the nerve before cutting the tendon.
-
Mobilization of the Latissimus Dorsi Muscle Belly and Pedicle:
- Once the tendon is released, we need to mobilize the muscle belly extensively. This involves dissecting it off the chest wall and releasing any fibrous bands or adhesions on its anterior surface.
- Surgeon's Directive: "Now we need to free up the muscle belly. This is critical for achieving adequate excursion and a tension-free transfer. We'll sweep our fingers underneath, carefully releasing all adhesions."
- Identifying the Thoracodorsal Pedicle: Trace the thoracodorsal artery and nerve as they enter the anterior, inferior surface of the muscle, about 13 cm from the humeral insertion. We must protect this pedicle at all costs.
- Surgeon's Directive: "Follow the pedicle. Ensure it's completely free from any constricting bands. We need a generous, tension-free pedicle to maintain viability of our transfer."
- The goal is to achieve enough length and mobility to allow the muscle to reach the greater tuberosity without undue tension on its neurovascular supply.

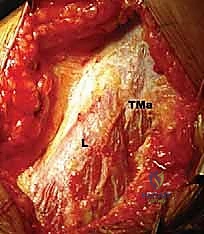
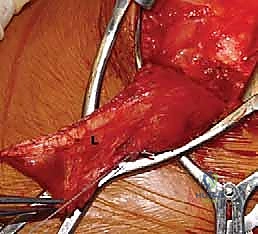
FIG 4 • B. The latissimus dorsi (L) is identified and separated from the teres major (TMa).
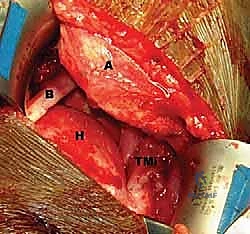
FIG 4 • C. The latissimus dorsi tendon is released from its humeral insertion.
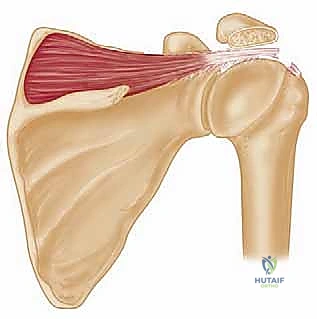
FIG 4 • D. The thoracodorsal neurovascular pedicle (TD) is identified and protected.
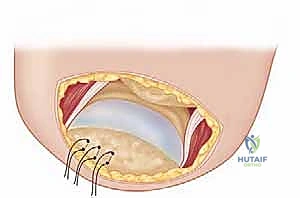
FIG 4 • E. The latissimus dorsi muscle is mobilized.

FIG 4 • F. The muscle is fully mobilized, ready for transfer.
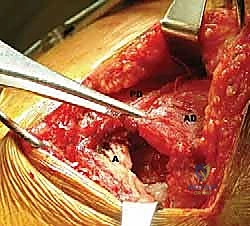
FIG 4 • G. The muscle is prepared for passage.
Phase 2: Preparing the Recipient Site and Tunneling the Tendon
-
Exposure of the Greater Tuberosity:
- Shift our attention to the superior and lateral aspect of the humeral head. We'll use a standard deltoid-splitting approach or extend our posterior incision anteriorly to expose the greater tuberosity.
- Surgeon's Directive: "Let's define our recipient bed now. We need clear visualization of the greater tuberosity."
-
Débridement and Footprint Preparation:
- Débride any residual, irreparable rotator cuff tissue from the greater tuberosity. Our goal is to create a fresh, bleeding bony bed for the transferred tendon. Use a burr or rasp to decorticate the footprint.
- Surgeon's Directive: "We want a good, vascularized bed for healing. Remove all compromised tissue. This is our new footprint."
-
Placement of Suture Anchors:
- Pre-place several suture anchors (typically 3-5, depending on the size of the footprint and tendon) into the prepared greater tuberosity. The number and type of anchors will vary based on surgeon preference. I prefer a double-row technique for robust fixation.
- Surgeon's Directive: "Let's place our anchors now. Aim for strong purchase in good bone. We'll use these to secure our transferred latissimus."
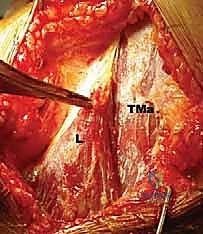
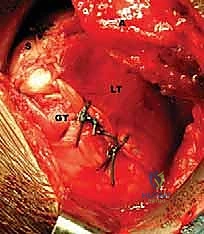
FIG 5 • A. The recipient bed on the greater tuberosity is prepared.

FIG 5 • B. Suture anchors are pre-placed in the greater tuberosity.
- **Tunneling the
Additional Intraoperative Imaging & Surgical Steps






REFERENCES
- External rotation training: A pillow is placed between the arm and chest wall holding the arm abducted 30 degrees. The patient is told to actively externally rotate the arm while adducting the arm against the pillow.
- Aoki M, Okamura K, Fukushima S, et al. Transfer of latissimus dorsi for irreparable rotator-cuff tears. J Bone Joint Surg Br 1996;78B: 761–766.
-
Cleeman E, Hazrati Y, Auerbach JD, et al. Latissimus dorsi transfers for massive rotator cuff tears: a cadaveric study. J Shoulder Elbow Surg 2003;12:539–543.
-
Codsi MJ, Hennigan S, Herzog R, et al. Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears: factors affecting outcomes. J Bone Joint Surg Am 2007;89A(Suppl 2):1–9.
-
Cofield RH. Rotator cuff disease of the shoulder. J Bone Joint Surg Am 1985;67A:974–979.
-
Costouros JG, Gerber C, Warner JP. Management of irreparable rotator cuff tears: the role of tendon transfer. In: Iannotti JP, Williams GR, ed. Disorders of the Shoulder: Diagnosis and Management, 2nd ed. Philadelphia: Lippincott-Raven, 1999.
-
Dugas JR, Campbell DA, Warren RF, et al. Anatomy and dimensions of rotator cuff insertions. J Shoulder Elbow Surg 2002;11:498–503.
-
Gerber C. Latissimus dorsi transfer for the treatment of irreparable tears of the rotator cuff. Clin Orthop Relat Res 1992;275:152–160.
-
Gerber C, Vinh TS, Hertel R, et al. Latissimus dorsi transfer for the treatment of massive tears of the rotator cuff: a preliminary report. Clin Orthop Relat Res 1988;232:51–60.
-
Goutallier D, Postel JM, Bernageau J, et al. Fatty muscle degeneration in cuff ruptures: preand postoperative evaluation by CT scan. Clin Orthop Relat Res 1994;304:78–83.
-
Habermeyer P, Magosch P, Rudolph T, et al. Transfer of the tendon of latissimus dorsi for the treatment of massive tears of the rotator cuff: a new single incision technique. J Bone Joint Surg Br 2006;88B:208–212.
-
Iannotti JP, Hennigan S, Herzog R, et al. Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am 2006;88A:342–348.
-
Miniaci A, MacLeod M. Transfer of the latissimus dorsi muscle after failed repair of a massive tear of the rotator cuff: a twoto five-year review. J Bone Joint Surg Am 1999;81A:1120–1127.
-
Pearle AD, Kelly BT, Voos JE, et al. Surgical techniques and anatomic study of latissimus dorsi and teres major transfers. J Bone Joint Surg Am 2006;88A:1524–1531.
-
Schoierer O, Herzberg G, Berthonnaud E, et al. Anatomical basis of latissimus dorsi and teres major transfers on rotator cuff tear surgery with particular reference to the neurovascular pedicles. Surg Radiol Anat 2001;23:75–80.
-
Warner JP. Management of massive irreparable rotator cuff tears: the role of tendon transfers. AAOS Instr Course Lect 2001;50:63–71.
-
Warner PJ, Parsons IM. Latissimus dorsi tendon transfer: a comparative analysis of primary and salvage reconstruction of massive, irreparable rotator cuff tears. J Shoulder Elbow Surg 2001;10:514–521.
Forward elevation training: The patient squeezes a large rubber ball between the palms of the hands while raising both arms forward over the head.
Biofeedback can also be used to show the patient when he or she is actively contracting the latissimus during external rotation and forward elevation.
OUTCOMES
- Significant improvement in pain scores postoperatively is a consistent finding (80% to 100% of patients) across outcome studies, even for patients less satisfied with their final results. 7,11
Sixty-six to 81% of patients report satisfaction postoperatively. Patient satisfaction tends to be associated more with improved active shoulder function than pain relief. 7,11
Patients with better preoperative function tend to have greater postoperative improvements in range of motion and strength compared to patients starting with greater shoulder dysfunction.
Based on our experience and that reported in the literature, postoperative range of motion improves by an average of 35 to 50 degrees in forward flexion and 9 to 40 degrees of external rotation. 1,7,11,16
Patients undergoing latissimus transfer as the first procedure to treat their rotator cuff pathology can expect better outcomes with regard to satisfaction, pain relief, and active range of motion compared to patients undergoing latissimus transfer who have had prior failed surgery for treatment of their rotator cuff. 16
Electromyographic studies show that about 40% to 50% of patients can be retrained to use in-phase latissimus dorsi contraction with active forward flexion or external rotation. 7,11
Female gender and advanced age are associated with worse outcomes.
Subscapularis tendon tears and superior escape of the humeral head are associated with a higher failure rate.