Medial Epicondyle ORIF: An Intraoperative Masterclass in Open Reduction and Internal Fixation

Key Takeaway
Master the open reduction and internal fixation of medial epicondyle fractures. This intraoperative guide covers comprehensive surgical anatomy, meticulous step-by-step technique, critical pearls and pitfalls, and robust postoperative management. Gain insights into precise instrument use, neurovascular protection, and advanced strategies for optimal patient outcomes. Perfect for orthopaedic fellows.
Introduction and Epidemiology
Medial epicondyle fractures represent a highly specific and clinically significant subset of elbow trauma, predominantly encountered in the skeletally immature population, though occasionally presenting in adults following high-energy trauma or chronic repetitive stress. By definition, this injury is an avulsion fracture of the medial epicondylar apophysis of the distal humerus. In pediatric cohorts, these fractures account for approximately 11% to 20% of all elbow fractures, with a peak incidence occurring between the ages of 9 and 14 years. This age distribution directly correlates with the physiological closure of the apophyseal growth plate, during which the biomechanical integrity of the physis is weaker than the attached ligamentous and musculotendinous structures.
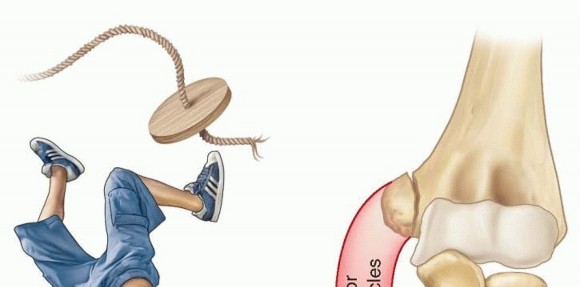
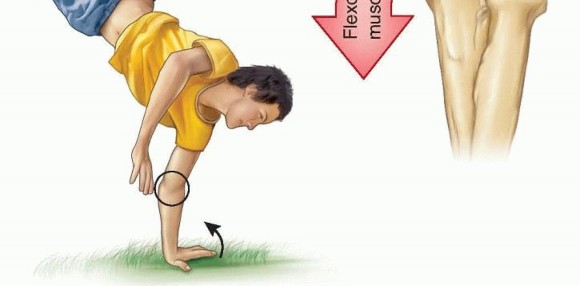
The mechanism of injury is classically bimodal. The most common acute presentation involves a sudden, severe valgus stress applied to an extended elbow, frequently resulting from a fall onto an outstretched hand (FOOSH). This valgus moment is often compounded by a violent, eccentric contraction of the flexor-pronator muscle mass, leading to a tension failure through the apophysis.
In up to 50% of pediatric cases, this fracture is associated with an acute elbow dislocation. During the dislocation and subsequent spontaneous or iatrogenic reduction, the avulsed fragment may become incarcerated within the ulnohumeral joint, a complication that drastically alters the management algorithm.
Epidemiologically, there is a pronounced male predominance, heavily linked to participation in overhead and throwing sports (e.g., baseball pitching). In these athletes, repetitive valgus extension overload can lead to microtrauma, apophysitis ("Little Leaguer's Elbow"), and eventual acute-on-chronic avulsion fractures. In the adult population, where the apophysis is fully fused, isolated medial epicondyle fractures are rare and typically represent a purely ligamentous avulsion equivalent or result from direct, high-energy blunt trauma. The high incidence of concomitant ulnar nerve neuropraxia (reported in 10% to 16% of cases) and the potential for chronic valgus instability mandate a rigorous diagnostic approach and a low threshold for surgical intervention in displaced or unstable patterns.
Surgical Anatomy and Biomechanics
A profound understanding of the medial elbow's osseous and soft-tissue architecture is imperative for executing a successful open reduction and internal fixation (ORIF) and preventing iatrogenic complications.
Osteology and Ossification
The medial epicondyle is an extracapsular, non-articular bony prominence located on the posteromedial aspect of the distal humerus. It serves as the primary anchor for the medial stabilizing structures of the elbow. Developmentally, it is the last ossification center of the distal humerus to fuse. According to the CRITOE mnemonic (Capitellum, Radial head, Internal/medial epicondyle, Trochlea, Olecranon, External/lateral epicondyle), the medial epicondyle ossification center appears radiographically between 5 and 7 years of age and fuses to the humeral shaft between 15 and 20 years of age. Prior to fusion, the cartilaginous physis is highly susceptible to avulsion forces.
Soft Tissue Attachments
The medial epicondyle serves as the origin for two critical anatomical complexes:
1. The Common Flexor-Pronator Mass: This musculotendinous unit originates from the anterior and inferior aspects of the epicondyle and includes the pronator teres (PT), flexor carpi radialis (FCR), palmaris longus (PL), flexor digitorum superficialis (FDS), and flexor carpi ulnaris (FCU).
2. The Ulnar Collateral Ligament (UCL) Complex: Specifically, the anterior bundle of the UCL, which is the primary restraint to valgus stress at the elbow from 20 to 120 degrees of flexion, originates from the anteroinferior surface of the medial epicondyle and inserts onto the sublime tubercle of the proximal ulna.
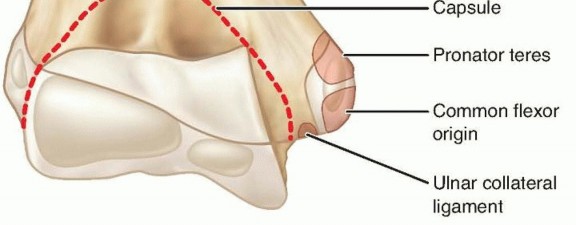
Because the UCL and the flexor-pronator mass remain attached to the avulsed fragment, the typical displacement pattern is distal and anterior. The degree of displacement is a direct reflection of the periosteal tearing and soft tissue disruption.

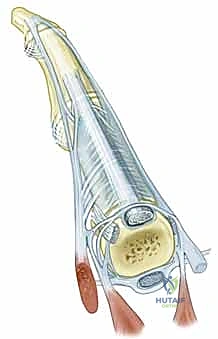
Neurovascular Relationships
The ulnar nerve is the most critical structure at risk during both the initial injury and subsequent surgical intervention. It courses distally through the posterior compartment of the arm, passing behind the medial intermuscular septum, and enters the cubital tunnel directly posterior to the medial epicondyle. The roof of the cubital tunnel is formed by Osborne's fascia (the arcuate ligament bridging the two heads of the FCU). The nerve is highly vulnerable to traction injuries during valgus stress, direct contusion from the bony fragment, or entrapment within the joint if the epicondyle becomes incarcerated.
Indications and Contraindications
The management of medial epicondyle fractures remains a subject of ongoing debate within the orthopedic literature, particularly regarding the exact threshold of displacement that warrants surgical fixation. However, distinct absolute and relative indications have been established to guide surgical decision-making.
Absolute Indications for ORIF
- Intra-articular Incarceration: A fragment trapped within the ulnohumeral joint is an absolute indication for surgery. Failure to extract and fix the fragment will result in a mechanical block to motion, rapid destruction of the articular cartilage, and severe joint arthrosis.
- Open Fractures: Requires immediate surgical debridement, irrigation, and stabilization to mitigate infection risk.
- Associated Ulnar Nerve Palsy (with displacement): While a pure neuropraxia in a minimally displaced fracture may be observed, an acute ulnar nerve palsy in the setting of a displaced fracture or following a reduction maneuver strongly suggests nerve entrapment or severe compression, necessitating exploration and concurrent fracture fixation.
- Symptomatic Nonunion: Chronic pain, weakness, or instability resulting from a failed conservative approach requires surgical intervention.
Relative Indications for ORIF
- Displacement Magnitude: The traditional threshold for surgery in pediatric patients has historically been >5 mm of displacement. However, modern literature increasingly advocates for fixation at >2 mm of displacement, particularly in high-demand overhead athletes, to prevent valgus extension overload and chronic instability. In adults, >2 mm is generally considered an indication for ORIF.
- Valgus Instability: Regardless of the absolute millimeter measurement of displacement on static radiographs, clinical or fluoroscopic evidence of gross valgus instability (often assessed via a "milking maneuver" or moving valgus stress test under anesthesia) is a strong indication for restoring the UCL origin via epicondylar fixation.
- High-Demand Athletes: Throwers and gymnasts require absolute anatomical restoration of the medial tension band to return to pre-injury levels of performance.
Contraindications for ORIF
- Minimally Displaced Fractures: Fractures with <2 mm of displacement and no clinical valgus instability are optimally managed non-operatively with brief immobilization followed by early functional rehabilitation.
- Medical Comorbidities: Patients deemed at unacceptably high risk for general anesthesia or surgical intervention.
- Severe Soft Tissue Compromise: Extensive local infection, burns, or severe degloving injuries may preclude immediate internal fixation, necessitating temporizing external fixation or delayed management.
Pre Operative Planning and Patient Positioning
Thorough preoperative preparation is critical for optimizing surgical workflow, anticipating complications, and ensuring anatomical reduction.
Diagnostic Imaging
Standard radiographic evaluation must include true anteroposterior (AP), lateral, and oblique views of the elbow. The lateral radiograph is paramount for identifying intra-articular incarceration; the presence of a bony fragment projecting within the joint space—often referred to as the "teardrop sign"—is pathognomonic for an incarcerated epicondyle.

In complex fracture patterns, severely comminuted cases, or instances where plain radiographs are equivocal regarding incarceration or articular involvement, a Computed Tomography (CT) scan with 3D reconstructions is highly recommended. CT provides precise spatial mapping of the fragment, aiding in implant selection and trajectory planning.

Patient Positioning and Setup
- Anesthesia: General anesthesia is typically employed, often supplemented with a regional block (e.g., supraclavicular or axillary nerve block) for postoperative pain control.
- Positioning: The patient is positioned supine on the operating table. The affected upper extremity is extended onto a radiolucent hand/arm table. The patient's torso is positioned as close to the edge of the main table as safely possible to allow the surgeon unimpeded access to the medial aspect of the elbow.
- Tourniquet: A sterile or non-sterile pneumatic tourniquet is applied high on the proximal arm. Exsanguination with an Esmarch bandage is performed prior to tourniquet inflation to ensure a bloodless surgical field, which is vital for meticulous identification of the ulnar nerve.
- Fluoroscopy: The C-arm is positioned either parallel to the arm table or coming from the head of the bed, ensuring that true AP and lateral orthogonal views can be obtained seamlessly without compromising the sterile field.
Detailed Surgical Approach and Technique
The primary objectives of the surgical procedure are anatomical reduction of the apophysis, rigid internal fixation to allow early range of motion, and meticulous protection of the ulnar nerve.
Surgical Approach
A longitudinal or slightly curvilinear incision is made centered over the medial epicondyle, extending approximately 3 cm proximally along the medial supracondylar ridge and 3 cm distally over the flexor-pronator mass.
During superficial dissection, the surgeon must remain vigilant to identify and protect the anterior and posterior branches of the medial antebrachial cutaneous (MABC) nerve, which cross the operative field transversely.
Ulnar Nerve Management
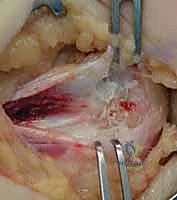
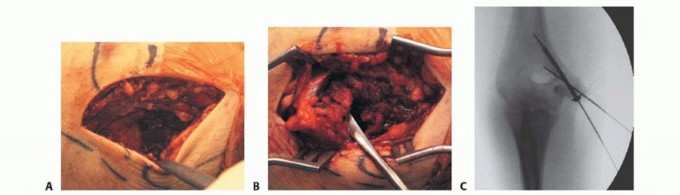
The most critical step prior to fracture manipulation is the identification and protection of the ulnar nerve. The nerve is located posterior to the medial epicondyle within the cubital tunnel. The fascia over the nerve is carefully incised.
* In Situ Decompression vs. Transposition: If the nerve is structurally intact, uninjured, and not under tension upon reduction of the fracture, an in situ decompression is generally sufficient. However, if the nerve is severely contused, incarcerated within the joint, or if the hardware placement threatens to impinge upon the cubital tunnel, a formal anterior subcutaneous or submuscular transposition should be performed. If transposed, the medial intermuscular septum must be excised to prevent kinking of the nerve.
Fragment Retrieval and Joint Debridement
If the fragment is incarcerated within the joint, blind levering must be strictly avoided to prevent iatrogenic chondral damage. A gentle valgus stress is applied to the elbow while supinating the forearm; a dental pick or fine nerve hook can then be used to carefully tease the fragment out of the joint space. Once the fragment is mobilized, the fracture bed on the distal humerus is thoroughly debrided of hematoma, interposed periosteum, and fibrous debris using a curette to expose bleeding cancellous bone, optimizing the biological environment for union.
Reduction and Provisional Fixation
The avulsed fragment, tethered by the flexor-pronator mass and UCL, is mobilized and anatomically reduced onto its footprint on the distal humerus. Reduction is often facilitated by flexing the elbow and pronating the forearm to relax the flexor-pronator tension. Once reduced, the fragment is provisionally stabilized using one or two smooth Kirschner wires (K-wires), typically 0.045 or 0.062 inches in diameter.

Definitive Internal Fixation
The choice of definitive fixation depends largely on the patient's age, fragment size, and bone quality.
1. Cannulated Screws: For most adolescents and adults with a sufficiently large fragment, fixation with one or two partially threaded cannulated screws (typically 3.5 mm or 4.0 mm) is the gold standard. A guidewire is advanced through the center of the fragment, directed anteriorly and laterally towards the lateral cortex of the distal humerus, carefully avoiding penetration into the olecranon or coronoid fossae. The screw length is measured, and the screw is inserted to achieve interfragmentary compression. In skeletally immature patients, care must be taken not to over-compress and crush the physis.
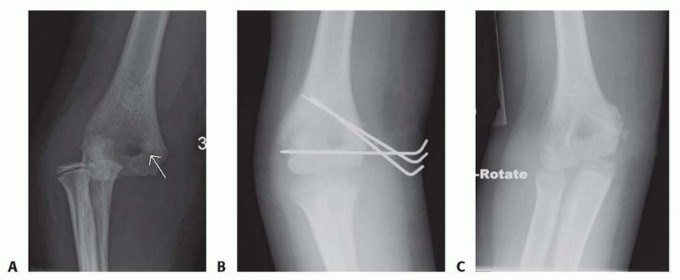
- K-wire Fixation: In very young children with small, predominantly cartilaginous fragments, or in cases of severe comminution, definitive fixation with divergent K-wires may be preferred. The pins are typically bent and cut outside the skin for later removal in the clinic, or buried subcutaneously.
- Suture Anchors: If the bony fragment is too small or comminuted to accept a screw, the UCL and flexor-pronator origin can be repaired directly to the humeral footprint using suture anchors or transosseous sutures.
Intraoperative Confirmation and Closure
Following definitive fixation, orthogonal fluoroscopic imaging is obtained to confirm anatomical reduction, appropriate hardware length, and absence of intra-articular penetration.
The elbow is taken through a full, unrestricted range of motion (flexion, extension, pronation, supination) while directly visualizing the repair to confirm stability and ensure the ulnar nerve is not subluxating or under undue tension. The wound is irrigated, and the fascial layers are closed over a drain (if deemed necessary). The skin is closed with subcuticular sutures, and the arm is placed in a well-padded posterior splint at 90 degrees of flexion with the forearm in neutral rotation.
Complications and Management
Despite meticulous surgical technique, ORIF of the medial epicondyle carries a specific profile of potential complications that surgeons must be prepared to manage.
Ulnar Neuropathy
Ulnar nerve dysfunction is the most frequently reported complication, with an incidence ranging from 10% to 50% depending on the series. It can manifest as transient neuropraxia, delayed tardy ulnar palsy, or severe motor/sensory deficits.
* Etiology: Initial trauma, iatrogenic traction during surgery, entrapment in scar tissue or callus, or direct hardware irritation.
* Management: Transient postoperative paresthesias are typically observed and often resolve within 3 to 6 months. Progressive symptoms, motor weakness, or positive electromyography (EMG) findings warrant prompt surgical re-exploration, neurolysis, and anterior transposition.
Loss of Motion (Elbow Stiffness)
The elbow joint is notoriously prone to post-traumatic stiffness. Loss of terminal extension (typically 10 to 15 degrees) is highly common following medial epicondyle fractures, regardless of operative or non-operative management.
* Management: Prevention is paramount, achieved through rigid internal fixation allowing for early, supervised active-assisted range of motion. If severe arthrofibrosis develops, dynamic splinting or, rarely, surgical arthrolysis may be required.
Nonunion and Malunion
Nonunion occurs in approximately 5% to 15% of cases, often due to inadequate fixation, soft tissue interposition, or premature aggressive rehabilitation.
* Management: Asymptomatic nonunions, particularly in low-demand patients, can often be observed. Symptomatic nonunions presenting with valgus instability or pain require revision ORIF with bone grafting or, in chronic cases with small fragments, excision of the fragment and direct repair of the UCL and flexor-pronator mass to the humerus.
Hardware Prominence and Irritation
Due to the paucity of subcutaneous fat over the medial epicondyle, screw heads or K-wires frequently become palpable and symptomatic once edema subsides.
* Management: Elective hardware removal is routinely performed after radiographic confirmation of solid bony union (typically 6 to 12 months postoperatively).
Post Operative Rehabilitation Protocols
A structured, phased rehabilitation protocol is critical for optimizing functional recovery while protecting the surgical construct.
Phase 1: Tissue Healing and Protection (Weeks 0-2)
- Immobilization: The patient remains in the postoperative posterior splint or is transitioned to a hinged elbow brace locked at 90 degrees of flexion.
- Motion: Active range of motion (AROM) of the shoulder, wrist, and digits is encouraged immediately to prevent distal edema and proximal stiffness.
- Precautions: Strict avoidance of elbow ROM and valgus stress.
Phase 2: Early Motion (Weeks 2-6)
- Bracing: The hinged brace is unlocked to allow a progressive arc of motion, typically starting from 30 to 100 degrees and advancing weekly.
- Motion: Supervised active and active-assisted ROM for elbow flexion and extension. Gentle forearm pronation and supination are initiated.
- Precautions: Passive stretching and valgus stress (e.g., carrying heavy objects) remain strictly contraindicated to protect the healing UCL and apophysis.
Phase 3: Strengthening (Weeks 6-12)
- Motion: Goal is to achieve full, symmetric ROM. Terminal extension stretching may be initiated if stiffness persists.
- Strengthening: Isotonic strengthening of the biceps, triceps, and forearm musculature begins. Eccentric flexor-pronator exercises are gradually introduced.
- Clinical Milestone: Radiographic evidence of bridging callus or obliteration of the fracture line should be evident before advancing to heavy resistance.
Phase 4: Return to Sport (Months 3-6+)
- Progression: Plyometric exercises and sport-specific functional drills are incorporated.
- Overhead Athletes: A formal, structured interval throwing program is mandatory for baseball pitchers and other overhead athletes. Return to competitive play is permitted only when full, painless ROM is achieved, valgus stability is clinically equal to the contralateral side, and isokinetic strength testing demonstrates >90% symmetry.
Summary of Key Literature and Guidelines
The paradigm for treating medial epicondyle fractures has shifted over the last two decades, moving from a predominantly conservative approach to a more aggressive surgical stance, particularly in athletes.
Historically, conservative management was championed by authors like Fowles and Kassabian (1974), who suggested that even significant displacement (up to 15 mm) could yield acceptable functional results in non-athletes. However, contemporary systematic reviews and clinical practice guidelines emphasize the biomechanical importance of the medial tension band.
- Displacement Thresholds: Current consensus, supported by the American Academy of Orthopaedic Surgeons (AAOS) guidelines, strongly leans toward ORIF for any displacement >5 mm in the general pediatric population, and >2 mm in high-demand athletes or adults.
- **Instability
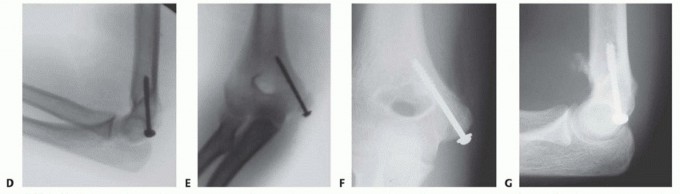
Clinical & Radiographic Imaging
You Might Also Like