MCP Joint Synovectomy & Extensor Tendon Centralization in Inflammatory Arthritis: A Masterclass
Key Takeaway
Join us in the OR for a masterclass on metacarpophalangeal (MCP) joint synovectomy and extensor tendon centralization. This immersive guide details patient selection, comprehensive anatomy, meticulous surgical technique, and crucial pearls for managing inflammatory arthritis-induced ulnar deviation. Learn to restore joint mechanics and improve function, ensuring optimal outcomes for your patients.
Introduction and Epidemiology
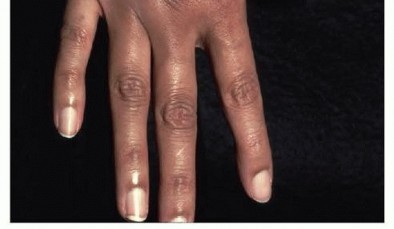
Inflammatory arthritides, most notably rheumatoid arthritis (RA), frequently manifest with debilitating involvement of the small joints of the hand and wrist. The metacarpophalangeal (MCP) joints are characteristically affected early in the disease process, leading to pain, swelling, progressive deformity, and significant functional impairment. The insidious onset of synovial hypertrophy at the MCP joints, particularly of the index and middle fingers, serves as a hallmark of early rheumatoid disease. Left unchecked, this chronic inflammatory state leads to enzymatic degradation of articular cartilage, capsuloligamentous laxity, and pathognomonic deformities such as ulnar deviation of the digits and volar subluxation of the proximal phalanges, accompanied by extensor tendon subluxation.
Historically, surgical intervention—including synovectomy and soft tissue reconstruction—played a prominent role in the earlier stages of the disease. With the advent of biologic disease-modifying antirheumatic drugs (bDMARDs) and optimized conventional synthetic DMARDs (csDMARDs), the natural history of RA has been significantly altered. This pharmacological evolution has delayed or even prevented the need for surgical management in a vast majority of patients. Nevertheless, a distinct subset of patients continues to experience persistent, refractory synovitis, progressive joint destruction, or fixed deformities despite optimal medical therapy. For these individuals, surgical intervention remains a critical component of multidisciplinary care aimed at pain relief, functional restoration, and halting disease progression.
Synovectomy, often combined with extensor tendon centralization and capsular reefing, addresses the inflammatory burden and biomechanical instability before irreversible osseous changes necessitate more extensive salvage procedures, such as arthroplasty or arthrodesis. While RA is the predominant inflammatory arthritis causing these deformities, conditions such as psoriatic arthritis and systemic lupus erythematosus (SLE) can also lead to similar hand manifestations. Notably, radial extensor tendon subluxation is occasionally observed in SLE (Jaccoud's arthropathy), presenting a distinct biomechanical challenge compared to the classic ulnar deviation seen in RA.
Surgical Anatomy and Biomechanics
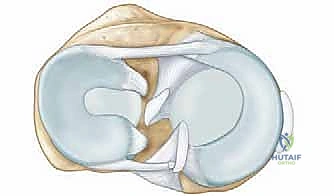
A thorough understanding of the normal and pathological anatomy of the MCP joint is paramount for effective surgical planning and execution. The MCP joint is a diarthrodial condyloid joint, permitting motion in two primary planes: flexion-extension and adduction-abduction, with a minor degree of passive rotation.
Bony Architecture and Joint Stability
The metacarpal head is bicondylar and asymmetric, being broader volarly than dorsally, while the articular base of the proximal phalanx is relatively shallow and concave. This articulation is stabilized by a robust fibrous capsule, a thick volar plate, and a pair of collateral ligaments. The collateral ligaments are composed of two distinct anatomical parts:
1. The Proper Collateral Ligament: Courses obliquely from the dorsal aspect of the metacarpal head to the volar aspect of the proximal phalanx base.
2. The Accessory Collateral Ligament: Connects the metacarpal head directly to the volar plate.
Due to the cam effect of the metacarpal head, these ligaments are taut in flexion and lax in extension, a crucial feature for MCP joint stability during power grip and pinch. The ulnar collateral ligament is generally more parallel to the long axis of the digit, while the radial collateral ligament is more oblique. This asymmetry contributes to normal biomechanics but also predisposes the joint to pathological supination and ulnar drift in inflammatory states. The volar plate is a thick, fibrocartilaginous structure distally and membranous proximally, limiting hyperextension and providing critical volar stability. It is interconnected to adjacent volar plates by the deep transverse metacarpal ligament, preventing excessive splaying of the metacarpal heads.
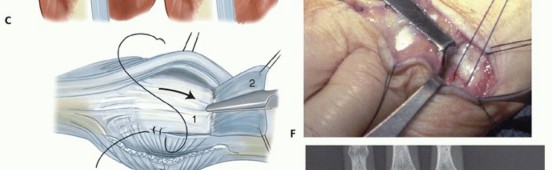
Extensor Mechanism of the Digits
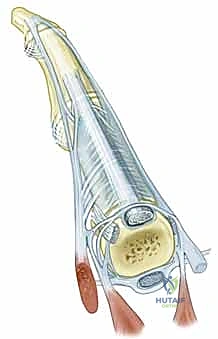
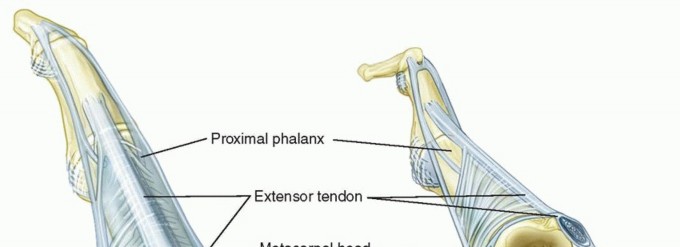
The extensor mechanism over the MCP joint is a highly complex, dynamic arrangement critical for digital extension and interphalangeal coordination. It consists of the extensor digitorum communis (EDC) tendon, the sagittal bands, and the intrinsic musculature (interossei and lumbricals). The EDC tendon travels dorsally, directly over the apex of the metacarpal head.
On either side, the sagittal bands—which form the primary stabilizing sling of the extensor hood—originate from the volar plate and the deep transverse metacarpal ligament. They encircle the metacarpal head and insert into the central EDC tendon. These bands act as a dynamic tether, centering the EDC tendon over the MCP joint and preventing ulnar or radial subluxation during flexion and extension. The intrinsic muscles insert into the lateral bands of the extensor mechanism, contributing to MCP flexion and interphalangeal (IP) extension (the intrinsic-plus position).

Pathomechanics of Ulnar Deviation and Extensor Tendon Subluxation
In inflammatory arthritis, a cascade of localized events leads to the characteristic ulnar drift and extensor tendon subluxation. Chronic synovitis (pannus formation) results in the release of matrix metalloproteinases and other inflammatory cytokines, causing enzymatic degradation and mechanical distension of the joint capsule and ligamentous restraints. This leads to profound laxity, particularly of the radial collateral ligament and the radial sagittal band, which normally stabilize the extensor tendon against ulnar displacement.

As the radial support attenuates, the EDC tendon migrates into the ulnar gutter. This ulnar subluxation of the extensor tendon exacerbates the ulnar deviation of the digit due to several compounding biomechanical factors:
- Mechanical Advantage Alteration: Once subluxated ulnarly, the line of pull of the EDC tendon falls volar to the axis of rotation. It ceases to act as an MCP extensor and instead becomes a deforming force, actively pulling the digit into further ulnar deviation and volar subluxation.
- Intrinsic Muscle Imbalance: The interossei muscles, particularly the ulnar intrinsics (abductor digiti minimi and volar interossei), often undergo contracture or spasticity in inflammatory arthritis, further driving ulnar deviation and MCP flexion contracture.
- Gravitational and Functional Forces: Repetitive gripping and pinching activities naturally impose an ulnar and volar deviating force on the digits. In the presence of weakened radial restraints, these daily functional loads accelerate the deformity.
- Supination Deformity: The asymmetric laxity of the collateral ligaments, combined with the ulnar shift of the extensor mechanism, frequently causes supination of the proximal phalanx relative to the metacarpal head during MCP flexion. This supination exacerbates the ulnar deviation in a three-dimensional plane, making the deformity significantly more complex to reconstruct.

These complex biomechanical derangements lead to significant functional compromise, drastically impacting pinch strength, grip strength, and overall hand dexterity. Early surgical intervention aims to correct these deformities while the joints remain flexible and before they become rigidly fixed or progress to severe articular destruction.



Indications and Contraindications
The decision to proceed with synovectomy and extensor tendon centralization at the MCP joint demands a rigorous assessment of disease activity, functional impairment, and radiographic staging. This is typically performed in close collaboration with a rheumatologist. The primary surgical goals are to alleviate pain, improve function, and arrest further capsuloligamentous destruction.
Operative Indications
Operative intervention is primarily indicated for patients with persistent, localized synovitis and early, reducible deformities that are unresponsive to rigorous medical management.
- Refractory Synovitis: Documented intractable synovitis of the MCP joint despite optimal medical therapy (e.g., csDMARDs, bDMARDs) for a minimum of 3-6 months. Clinically, this presents as persistent boggy swelling, pain, and localized warmth.
- Progressive Extensor Tendon Subluxation: Ulnar (or rarely radial) subluxation of the EDC tendon with associated extensor lag or progressive, flexible ulnar drift of the digits.
- Pain and Functional Impairment: Significant pain at the MCP joint that objectively limits activities of daily living (ADLs), grip strength, or key pinch strength.
- Early Radiographic Changes: Radiographic evidence of early marginal erosions or mild joint space narrowing (e.g., Larsen Grades I-II, or early Grade III) without significant architectural destruction that would preclude joint preservation.
- Prophylactic Intervention: In highly selected cases, synovectomy is considered prophylactically to prevent further cartilage destruction and ligamentous attenuation in the face of aggressive, persistent localized inflammation, particularly in younger cohorts.
Non Operative Indications and Contraindications
Non-operative management remains the first line of treatment. Surgical intervention is contraindicated or strictly deferred in several specific clinical scenarios:
- Effective Medical Control: Patients whose symptoms (pain, swelling, deformity) are quiescent or well-controlled by systemic pharmacotherapy.
- Mild Symptoms: Minimal pain or functional impairment that does not significantly restrict the patient's quality of life.
- Early Disease without Deformity: Synovitis without demonstrable extensor tendon subluxation, extensor lag, or significant ulnar drift.
- Advanced Joint Destruction: Severe radiographic changes (Larsen Grades IV-V) characterized by extensive cartilage loss, severe periarticular erosions, and fixed subluxation or dislocation of the joint. In these cases, joint-preserving surgery will fail; arthroplasty (e.g., silicone elastomer or pyrolytic carbon implants) or arthrodesis is the standard of care.
- Active Infection: Any local or systemic infectious process.
- Compromised Soft Tissue Envelope: Poor skin integrity, severe vasculitis, or extreme soft tissue atrophy over the surgical site.
- Complete Tendon Rupture: If the extensor tendon has fully ruptured (e.g., Vaughan-Jackson syndrome), a simple centralization procedure is wholly insufficient; tendon transfer (e.g., EIP to EDC) or grafting is required.
- Unoptimized Comorbidities: Uncontrolled systemic diseases that elevate perioperative morbidity.
| Category | Operative Indications | Non-Operative Indications/Contraindications |
|---|---|---|
| Disease Activity | Persistent synovitis despite optimal medical therapy | Well-controlled disease with medical therapy |
| Deformity & Instability | Progressive extensor tendon subluxation or flexible ulnar drift | Mild symptoms, no significant dynamic deformity |
| Functional Status | Significant pain and functional impairment limiting ADLs | Minimal functional impairment, acceptable pain levels |
| Radiographic Findings | Early erosions (Larsen I-III) without severe destruction | Advanced joint destruction (Larsen IV-V), fixed dislocation |
| Tendon Integrity | Intact but subluxated extensor tendon | Complete extensor tendon rupture |
| General Health | Medically optimized for elective surgery | Active infection, severe comorbidities, poor skin quality |
Pre Operative Planning and Patient Positioning
Comprehensive pre-operative planning is critical to optimize surgical outcomes and mitigate perioperative complications in the inflammatory arthritis patient.
Clinical and Radiographic Assessment
A meticulous medical history must detail the duration of the arthropathy, the specific sequence of medical treatments (especially the timing of bDMARD administration), previous hand surgeries, and a thorough functional assessment. Concomitant wrist pathology (e.g., radiocarpal subluxation, caput ulnae syndrome) must be evaluated, as proximal instability will rapidly compromise distal MCP joint reconstructions.
Physical examination should focus on:
* Synovial Hypertrophy: Documenting the severity and distribution of the pannus.
* Range of Motion (ROM): Active and passive MCP joint flexion and extension, specifically noting any extension lag or fixed flexion contracture.
* Deformity Reducibility: Quantification of ulnar deviation and volar subluxation, differentiating between a flexible (correctable) versus a fixed deformity.
* Extensor Tendon Tracking: Dynamic assessment for subluxation of the EDC tendon into the ulnar gutter during active flexion.
* Neurologic Status: Evaluation of digital nerve sensation, paying particular attention to the dorsal sensory branches of the radial and ulnar nerves, which are highly vulnerable during dorsal surgical approaches.
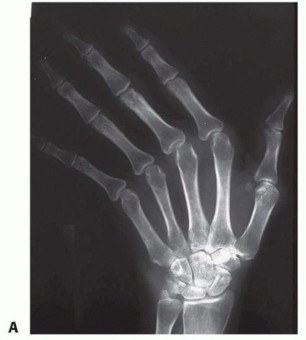
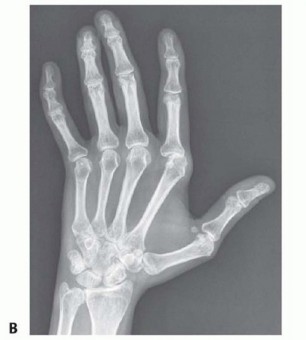
Standard imaging includes:
* Plain Radiographs: True posteroanterior (PA), lateral, and oblique views of the hand and wrist. These are critical for grading joint destruction using the Larsen or Sharp scoring systems, assessing bone stock, and identifying subluxations.
* Advanced Imaging (MRI/Ultrasound): While plain radiographs usually suffice, ultrasound is highly sensitive for detecting active synovitis (Doppler flow) and early tenosynovitis, whereas MRI can delineate early, radiographically occult erosions and precise tendon integrity.
Medical optimization requires close coordination with the treating rheumatologist. Perioperative management of DMARDs and bDMARDs must adhere to current guidelines (e.g., ACR/AAHKS guidelines) to balance the risk of postoperative infection against the risk of an inflammatory flare. Often, bDMARDs are withheld for one dosing cycle prior to surgery and resumed after wound healing (typically 14 days postoperatively). Glucocorticoid stress dosing may be required for patients on chronic steroid therapy.
Medical Optimization and Anesthesia
- Anesthesia: Regional anesthesia (e.g., ultrasound-guided axillary or supraclavicular brachial plexus block) is the gold standard, providing excellent intraoperative conditions, vasodilation, and prolonged postoperative analgesia. General anesthesia is reserved for patient preference or specific contraindications to regional blocks.
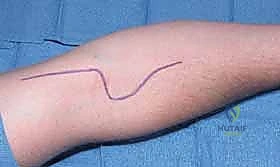
- Patient Positioning: The patient is positioned supine. The operative extremity is abducted onto a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm and typically inflated to 250 mmHg after exsanguination with an Esmarch bandage.
- Instrumentation: A standard hand surgery tray is utilized, featuring fine dissecting scissors (tenotomy, Stevens), delicate retractors (Senn, Ragnell), skin hooks, and a bipolar electrocautery unit for meticulous hemostasis. Kirschner wires (0.045 or 0.062 inches) should be available for temporary joint stabilization if severe instability is encountered.
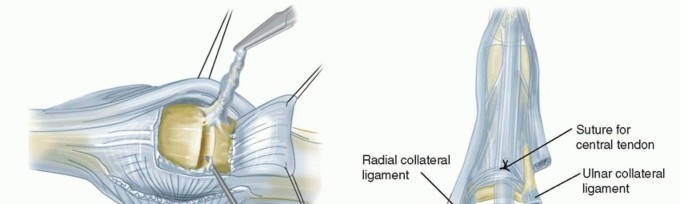
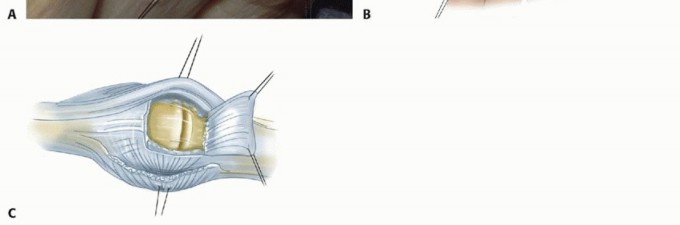
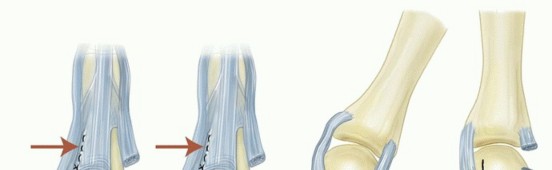
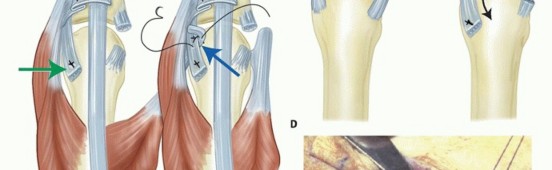
Detailed Surgical Approach and Technique
The fundamental objectives of MCP joint synovectomy and extensor tendon centralization are to radically excise the inflamed synovial pannus, restore the anatomic alignment of the extensor mechanism, and correct flexible deformities while
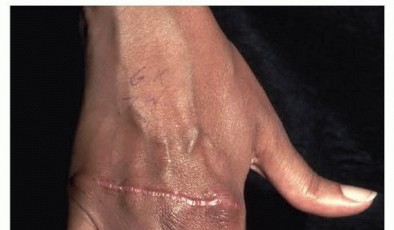
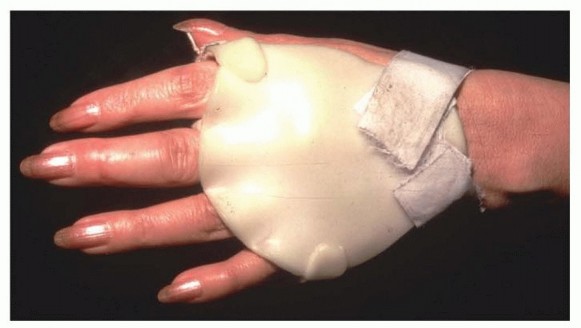
Clinical & Radiographic Imaging

You Might Also Like