Arthroscopic TFCC Débridement & Ulnar Shortening: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for an immersive masterclass on arthroscopic TFCC débridement and ulnar shortening. We'll meticulously cover patient positioning, portal placement, precise débridement techniques, and controlled ulnar head resection. Learn to navigate critical anatomy, avoid pitfalls, and ensure optimal outcomes for ulnar wrist pain and abutment syndrome.
Introduction and Pathogenesis
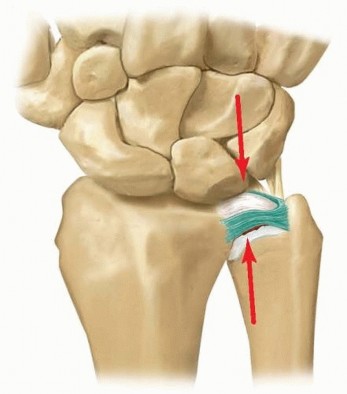
The triangular fibrocartilage complex (TFCC) is a complex, homogenous anatomic structure situated on the ulnar aspect of the wrist. It serves as the primary stabilizer of the distal radioulnar joint (DRUJ) and is responsible for transferring axial loads across the wrist from the ulnar carpus to the distal ulna. Disruption of the TFCC, whether through acute trauma or chronic degeneration, frequently leads to localized synovitis, ulnar-sided wrist pain, grip weakness, and painful mechanical clicking during forearm rotation, significantly impairing upper extremity function.
Pathologically, TFCC lesions are divided into traumatic (Palmer Type I) and degenerative (Palmer Type II) classifications. Acute Palmer Type I injuries typically result from a massive axial load applied to an ulnarly deviated wrist combined with forceful forearm rotation. Biomechanically, the TFCC is compressed and sheared between the ulnar head and the lunate/triquetrum. These injuries are highly prevalent in falls onto a pronated, outstretched hand, or during activities demanding forceful ulnar deviation (e.g., racquet sports, golf). Furthermore, intra-articular fractures of the distal radius demonstrate a concomitant TFCC tear incidence ranging from 50% to 84%; however, many of these remain clinically silent and do not necessitate immediate surgical intervention if the DRUJ remains stable.
Chronic degenerative tears (Palmer Type II) are intimately associated with ulnar positive variance and ulnocarpal impaction syndrome. Ulnar positive variance may be developmental or acquired secondary to distal radius malunion, Essex-Lopresti injuries, or premature radial physeal closure. Ulnocarpal abutment is characterized by chronic compressive overloading of the ulnocarpal joint, leading to progressive attrition of the central articular disc, accompanied by variable chondromalacia of the ulnar head, proximal lunate, and triquetrum.
The natural history of degenerative tears demonstrates a predictable cascade: TFCC wear (IIA), ulnar or lunate chondromalacia (IIB), central TFCC perforation (IIC), lunotriquetral (LT) ligament tearing (IID), and ultimately, ulnocarpal and DRUJ arthrosis (IIE). Arthroscopic TFCC débridement is highly indicated for centrally based, avascular lesions (Palmer IA and IIA-IIC) and is frequently combined with arthroscopic ulnar shortening (the "wafer" procedure) to decompress the ulnocarpal joint in patients with concomitant ulnocarpal abutment.
Surgical Anatomy and Biomechanics
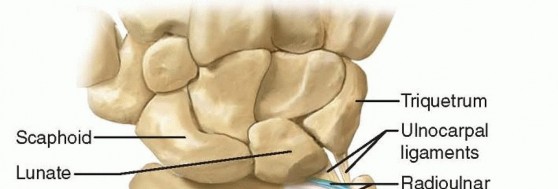
The TFCC is a confluence of ligamentous and cartilaginous structures spanning the DRUJ and ulnocarpal articulations. It originates from the distal margin of the radial sigmoid notch and inserts into the base of the ulnar styloid and the ulnar fovea. The ulnocarpal complex—comprising the ulnolunate ligament, ulnotriquetral ligament, and the extensor carpi ulnaris (ECU) subsheath—provides critical volar and ulnar support.

The radioulnar ligaments (RULs) are the primary stabilizers of the DRUJ. The superficial limbs of the dorsal and palmar RULs insert onto the base of the ulnar styloid, whereas the deep limbs (the ligamentum subcruentum) insert into the fovea. The central articular disc is a thin, avascular fibrocartilaginous structure spanning the distal rim of the sigmoid notch, blending seamlessly with the RULs. Because the central portion is avascular, tears in this region do not heal and are treated with débridement, whereas peripheral tears have a blood supply and are amenable to repair.
Biomechanically, the TFCC is a critical load-bearing structure. In an ulnar-neutral wrist, the radius absorbs approximately 82% of the axial load, while the ulnar carpus absorbs 18%. This load distribution is highly sensitive to ulnar variance. An increase in ulnar variance by just 2.5 mm shifts the ulnar axial load to 42%, precipitating ulnocarpal abutment. Conversely, decreasing ulnar variance by 2.5 mm reduces the ulnar load to 4.3%.
Clinical Evaluation and Differential Diagnosis
Patients typically present with insidious or post-traumatic ulnar-sided wrist pain, exacerbated by forearm rotation and ulnar deviation. Mechanical symptoms such as clicking, catching, and a subjective sense of instability are common.
A meticulous physical examination is required to isolate TFCC pathology from other ulnar-sided pain generators:
* Fovea Sign: Direct palpation of the ulnar fovea (between the ulnar styloid and FCU tendon). This test yields a 95.2% sensitivity and 86.5% specificity for TFCC foveal disruptions or ulnotriquetral ligament injuries.
* TFCC Stress Test: Axial loading of the wrist in ulnar deviation combined with passive forearm rotation. Reproduction of a painful click indicates a TFCC tear.
* Ulnocarpal Stress Test: Pronation and supination of the forearm with the wrist held in maximum ulnar deviation to provoke ulnocarpal abutment.
* Pisiform Boost Test: Dorsally directed pressure applied to the palmar aspect of the pisiform while passively ulnarly deviating the wrist. Increased pain indicates ulnocarpal pathology.
* DRUJ Instability (Piano Key / Shuck Test): The distal radius is stabilized while the distal ulna is translated volarly and dorsally in neutral, full pronation, and full supination. Asymmetry compared to the contralateral wrist suggests RUL disruption.
The differential diagnosis for ulnar-sided wrist pain is extensive and includes:
* Ulnocarpal impaction / abutment syndrome
* Ulnocarpal synovitis
* Extrinsic ulnar ligament tears
* Lunotriquetral (LT) joint instability or tears
* DRUJ arthritis or instability
* Ulnar styloid nonunion
* Pisotriquetral arthritis
* Kienböck disease
* Extensor Carpi Ulnaris (ECU) tendinopathy or subluxation
Imaging and Diagnostic Studies
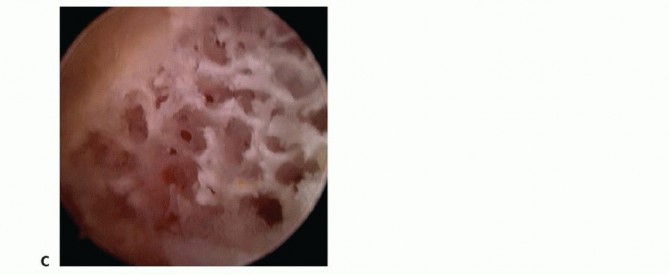
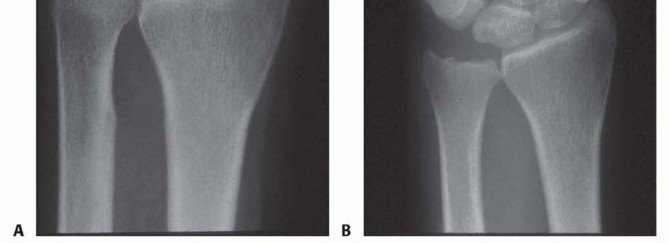
Standard radiographic evaluation must include a posteroanterior (PA) view, a lateral view, a Palmer 90 × 90 neutral rotation view, and a fully pronated grip stress view. The Palmer 90 × 90 view (forearm in neutral rotation, elbow flexed 90 degrees, shoulder abducted 90 degrees) is the gold standard for calculating static ulnar variance.

The fully pronated grip stress view evaluates dynamic ulnar variance. The shoulder is adducted, the forearm fully pronated, and the patient makes a maximal fist. An increase in ulnar variance under these conditions confirms dynamic ulnocarpal impaction. Radiographic hallmarks of chronic ulnar abutment include subchondral sclerosis and cystic changes in the proximal ulnar aspect of the lunate and the radial aspect of the ulnar head.


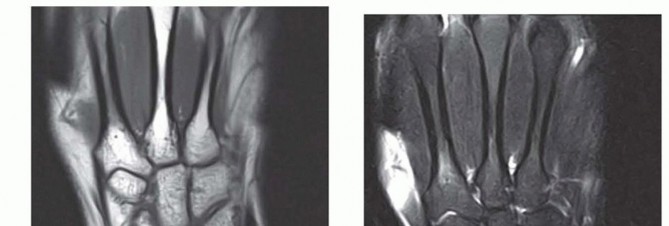
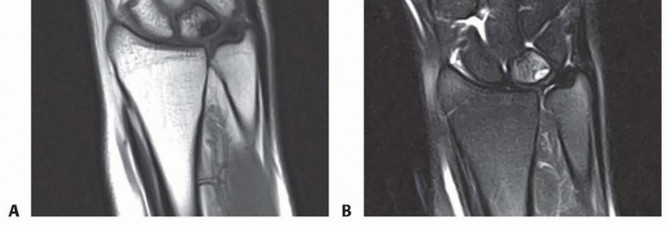
Advanced imaging is critical for surgical planning. Magnetic Resonance Imaging (MRI), particularly MR arthrography, offers high sensitivity for central TFCC tears, though false positives can occur. An intact TFCC demonstrates a homogenous low signal on T2-weighted sequences. In early ulnar impaction syndrome without overt radiographic changes, MRI will reveal bone marrow edema (hyperemia) in the lunate, triquetrum, and ulnar head—characterized by low signal intensity on T1-weighted images and high signal intensity on T2-weighted images. Computed Tomography (CT) arthrography is an excellent alternative with high sensitivity and specificity for central tears when MRI is contraindicated.
Indications and Nonoperative Management
Nonoperative management is the mandatory first-line treatment for TFCC tears in the absence of gross DRUJ instability. The protocol includes:
* Immobilization via a sugar-tong or long-arm Muenster splint for 4 weeks to restrict forearm rotation.
* A scheduled course of nonsteroidal anti-inflammatory drugs (NSAIDs).
* Intra-articular corticosteroid injections (radiocarpal or ulnocarpal), which provide both diagnostic information and therapeutic relief in acute presentations.
* Activity modification to eliminate forceful grip and torque.
* Post-immobilization physical therapy focusing on progressive ROM and isometric strengthening, avoiding torque for 8 weeks.
A 3- to 4-month trial of nonoperative management is standard prior to surgical consideration.
Surgical intervention is indicated for symptomatic patients failing conservative therapy. Arthroscopic débridement is highly successful for Palmer IA tears in ulnar-neutral or ulnar-negative wrists. However, in the setting of ulnar positive variance (Palmer IIA-IIC), débridement alone yields high failure rates; thus, concomitant ulnocarpal decompression (arthroscopic ulnar shortening/wafer procedure or formal ulnar shortening osteotomy) is required. Palmer IID and IIE lesions may require additional lunotriquetral ligament débridement, pinning, or a diaphyseal ulnar shortening osteotomy to tighten the ulnocarpal ligaments.
Preoperative Planning and Patient Positioning
Preoperative radiographic measurement of ulnar variance is paramount. The surgeon must determine if the patient is a candidate for an arthroscopic wafer procedure versus a formal diaphyseal ulnar shortening osteotomy. Arthroscopic shortening is generally limited to a maximum resection of 3 to 4 mm. If the patient has greater than 4 mm of ulnar positive variance, significant lunotriquetral laxity, or peripheral TFCC tears requiring formal repair, an open diaphyseal osteotomy is preferred.
The patient is positioned supine with the operative arm on a hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Following standard prep and drape, the wrist is suspended using a commercially available wrist traction tower, applying 10 to 12 pounds of longitudinal distraction via finger traps on the index and long fingers. The operating room must be equipped with a mini C-arm fluoroscopy unit to confirm the depth of ulnar resection intraoperatively.
Detailed Surgical Technique
Diagnostic Arthroscopy and Portal Placement
Standard radiocarpal portals (3-4, 4-5, 6R) and midcarpal portals are utilized. To minimize the risk of iatrogenic injury to the superficial branch of the radial nerve, dorsal ulnar sensory nerve, or extensor tendons, incisions are made strictly through the skin. A small hemostat is then used to bluntly dissect through the subcutaneous tissues and penetrate the joint capsule.
A comprehensive diagnostic arthroscopy of the radiocarpal, ulnocarpal, and midcarpal joints is performed to evaluate intrinsic/extrinsic ligaments, articular cartilage, and synovium. A thorough synovectomy is initially performed using a shaver in the 4-5 or 6R portal to ensure pristine visualization.
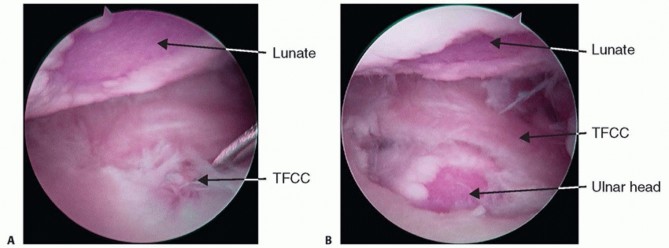
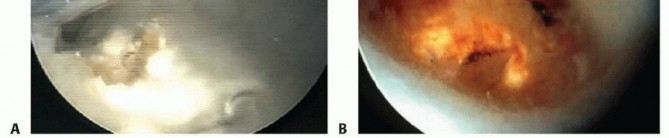
The TFCC is probed to assess the integrity of its peripheral attachments and the "trampoline effect." Articular surfaces of the lunate, triquetrum, and ulnar head are inspected for chondromalacia indicative of ulnocarpal impaction.
Mechanical Triangular Fibrocartilage Complex Débridement
With the arthroscope placed in the 3-4 portal, the 6R portal serves as the primary working portal to débride the radial, palmar, and dorsal aspects of the central TFCC tear. Alternating the arthroscope and working instruments between the 3-4, 4-5, and 6R portals allows comprehensive 360-degree access to the lesion.
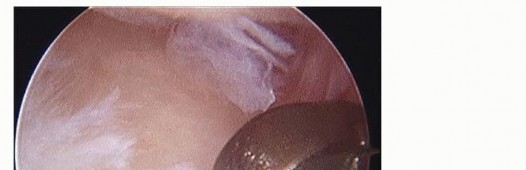

Débridement is achieved using small joint punches (straight and angled), graspers, and a 2.5-mm or 2.9-mm oscillating shaver. A suction punch is particularly effective for excising unstable flaps. Extreme care must be taken to avoid scuffing the underlying ulnar head or the overhanging lunate and triquetrum.
Critical technical points during débridement:
1. Preserve the Periphery: Maintain at least a 2 mm peripheral rim of the TFCC to prevent destabilizing the DRUJ.
2. Protect the Ligaments: Avoid injury to the dorsal and palmar radioulnar ligaments and the foveal insertion.
3. Smooth the Edges: After mechanical excision, the edges of the defect are smoothed using a shaver or a radiofrequency (RF) ablation probe. RF ablation provides the added benefit of thermal tissue shrinkage, which may tighten the remaining peripheral rim.
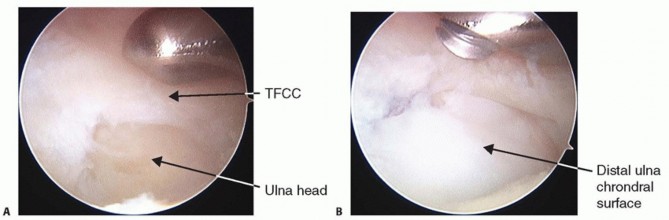
The endpoint of débridement is achieved when a stable, smooth central rim is created (typically a 1 cm defect), and the ulnar head is clearly visible through the defect. Up to 80% of the central avascular substance can be resected without inducing iatrogenic DRUJ instability.
Laser-Assisted Triangular Fibrocartilage Complex Débridement
Laser-assisted débridement offers rapid and precise tissue ablation. The arthroscope is maintained in the 3-4 portal, while a holmium:YAG laser probe is introduced via the 4-5 portal. The laser is typically set to 1.4 to 1.6 Joules at a frequency of 15 pulses per second.
Utilizing a 70-degree side-firing laser tip allows for efficient ablation of the radial, palmar, ulnar, and dorsal components of the tear without needing to switch portals.
During laser application, the surgeon must avoid firing tangentially into the ulnar head. The optimal technique involves passing the probe beneath the TFCC and firing distally. The continuous flow of arthroscopic saline acts as a heat sink, absorbing thermal energy and protecting the lunate and triquetrum from iatrogenic cartilage necrosis.
Arthroscopic Ulnar Shortening
If the patient exhibits ulnar impaction with less than 4 mm of ulnar-plus variance, an arthroscopic ulnar shortening (wafer procedure) is performed immediately following TFCC débridement. The goal is to resect the distal ulnar dome to create a neutral to 2 mm negative ulnar variance, thereby decompressing the ulnocarpal joint while preserving the DRUJ articulation.
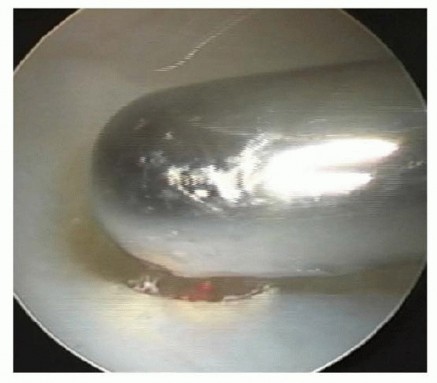
With the arthroscope in the 3-4 portal, a 2.9-mm small joint burr is introduced through the 4-5 portal. The burr is passed through the newly created central TFCC defect to access the ulnar head.


Resection begins centrally and moves peripherally. To ensure a uniform, circumferential resection of the ulnar head, the surgical assistant must fully supinate and pronate the patient's forearm dynamically during the burring process. The burr should be withdrawn intermittently to irrigate bone debris from the joint. Fluoroscopy is utilized frequently to gauge the depth and uniformity of the resection. The surgeon must strictly avoid burring into the ulnar fovea to prevent catastrophic detachment of the deep TFCC fibers.
Alternatively, a holmium:YAG laser can be used to vaporize the hyaline cartilage and subchondral bone of the ulnar seat.

The laser is highly efficient on dense subchondral bone but loses efficacy once the cancellous trabeculae of the distal ulna are exposed. At this juncture, the 2.9-mm burr is reintroduced to finalize the leveling process.
Once resection is complete, the wrist is removed from traction. A dynamic clinical examination is performed (axial load, ulnar deviation, pronation/supination) to ensure no residual crepitus or mechanical impingement exists. Portals are closed with 4-0 non-absorbable sutures, and a bulky, well-padded short-arm volar splint is applied.
Pearls and Pitfalls
TFCC Débridement Pearls:
* Incise skin only and spread with a hemostat to protect the dorsal ulnar sensory nerve (DUSN) and superficial radial nerve (SRN).
* Excise only the unstable central flap; rigorously preserve at least 2 mm of the peripheral rim.
* Utilize a thermal probe to cauterize concurrent synovitis, improving visualization and potentially shrinking redundant capsular tissue.
* Always re-evaluate the wrist off traction post-débridement to ensure the preoperative mechanical click has been eradicated.
TFCC Débridement Pitfalls:
* Iatrogenic injury to the DUSN during 6R or 6U portal placement.
* Over-resection leading to disruption of the dorsal/palmar RULs, causing frank DRUJ instability.
* Failure to recognize a peripheral, vascularized tear that requires formal repair rather than débridement.
* Performing isolated débridement in a patient with unrecognized ulnar positive variance, guaranteeing surgical failure.
Arthroscopic Ulnar Shortening Pearls:
* Obtain true neutral PA and pronated grip radiographs preoperatively to accurately assess dynamic variance.
* Use the 2.9-mm burr head as a visual depth gauge to ensure only 3 to 4 mm of bone is resected.
* Dynamic forearm rotation by an assistant is mandatory during burring to prevent creating an uneven, cam-like ulnar head.
* Routinely perform midcarpal arthroscopy to rule out concurrent lunotriquetral instability.
Arthroscopic Ulnar Shortening Pitfalls:
* Resecting into the ulnar fovea, destabilizing the DRUJ.
* Excessive resection that violates the sigmoid notch articulation, leading to altered DRUJ kinematics and early arthrosis.
* Failure to recognize advanced Palmer IID/IIE lesions, which are better served by an extra-articular ulnar shortening osteotomy to tension the ulnocarpal ligaments.
Complications and Management
- Nerve Injury: The dorsal branch of the ulnar nerve is highly susceptible during 6R/6U portal placement. Strict adherence to blunt dissection techniques is required. Neuromas may require exploration and excision.
- DRUJ Instability: Caused by aggressive débridement violating the RULs or foveal attachments. Management requires open or arthroscopic TFCC repair, or reconstructive stabilization procedures (e.g., Adams-Berger reconstruction).
- Persistent Ulnar-Sided Pain: Frequently due to inadequate or asymmetric ulnar head resection, or failure to address dynamic ulnar impaction. Revision arthroscopic leveling or formal ulnar shortening osteotomy may be necessary.
- Loss of Forearm Rotation: Can result from excessive thermal energy (laser/RF) causing capsular contracture, or from altering the DRUJ mechanics via excessive ulnar head resection. Aggressive postoperative therapy is the first line of management.
Postoperative Rehabilitation and Outcomes
Postoperative protocols
Clinical & Radiographic Imaging

You Might Also Like


