

Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and this definitive masterclass on the surgical management of Superior Labral Anterior Posterior (SLAP) lesions. Since the landmark description by Snyder et al. in 1990, the diagnosis and treatment of SLAP tears have evolved dramatically. This pathology involves the superior aspect of the glenoid labrum, extending from anterior to posterior, and critically, encompasses the origin of the long head of the biceps tendon (LHBT)—the biceps anchor. Understanding the intricate anatomy, nuanced biomechanics, and precise surgical indications for this region is paramount to achieving durable, successful outcomes and avoiding the significant morbidities associated with over-treatment or technical failure.
The pathophysiology of SLAP tears is generally categorized into two distinct mechanisms: acute traumatic events and chronic repetitive microtrauma. Acute injuries frequently result from a sudden traction force applied to the arm, such as lifting a heavy object, or a compression force, classically seen in falls onto an outstretched hand (FOOSH) where the humeral head is driven superiorly into the labral complex. Conversely, chronic repetitive microtrauma is the hallmark of the overhead athlete, such as baseball pitchers, volleyball players, and tennis players. In these patients, the "peel-back" mechanism, as elegantly described by Burkhart and Morgan, is the primary driver. During the late cocking phase of throwing, the shoulder is in maximum abduction and external rotation. This position causes the vector of the biceps tendon to shift posteriorly, creating a torsional force that literally peels the posterosuperior labrum away from the glenoid rim.
Clinically, patients present with a constellation of vague, deep-seated shoulder pain and persistent mechanical symptoms. They frequently report catching, locking, popping, or a sensation of instability, particularly with overhead activities. The physical examination is notoriously challenging due to the lack of a single pathognomonic clinical test. A high index of suspicion must be maintained. We routinely employ a battery of provocative maneuvers, including the O’Brien (active compression) test, Speed test, Yergason test, dynamic labral shear test, and the crank test. Pain with the O'Brien test that is elicited in pronation and relieved with supination, or painful clicking during the dynamic shear test, significantly increases the pre-test probability of a SLAP lesion. However, these tests must be interpreted within the context of the patient's entire clinical picture, as they frequently cross-react with acromioclavicular joint pathology and biceps tendinopathy.

Snyder’s original classification system remains the foundational framework for guiding our surgical strategy, though it has since been expanded by Maffet and Powell to include more complex tear patterns. Snyder categorized SLAP tears into four primary types. Type I involves degenerative fraying of the superior labrum with an intact biceps anchor, typically treated with simple debridement. Type II, the most commonly encountered operative lesion and the primary focus of this chapter, involves pathological detachment of the superior labrum and biceps anchor from the superior glenoid. Type III is a bucket-handle tear of the superior labrum with an intact biceps anchor, while Type IV is a bucket-handle tear that extends directly into the substance of the biceps tendon. It is critical to recognize that these lesions are rarely isolated. In younger demographics, they frequently co-exist with Bankart lesions and capsular laxity, whereas in patients over the age of 40, they are highly correlated with partial or full-thickness rotator cuff tears.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the superior glenohumeral anatomy is the prerequisite for any arthroscopic intervention. The superior glenoid labrum is a robust, triangular, fibrocartilaginous structure that seamlessly blends with the articular cartilage of the glenoid. Its primary biomechanical function is to deepen the relatively flat glenoid fossa by approximately 50%, thereby significantly enhancing concavity compression and static glenohumeral stability. Furthermore, it serves as the critical attachment site for the long head of the biceps tendon, forming the biceps anchor at the supraglenoid tubercle. This anchor acts as a dynamic stabilizer; contraction of the biceps depresses the humeral head, resisting superior translation during the early phases of elevation, and acts as an adjunct anterior stabilizer when the arm is abducted and externally rotated.

Surgeons must possess a keen awareness of normal anatomical variants to avoid the catastrophic error of "repairing" a normal structure, which inevitably leads to severe postoperative stiffness. Two primary variants demand our attention: the sublabral foramen and the Buford complex. A sublabral foramen is an unattached anterosuperior labrum (typically between the 11 and 3 o'clock positions) that does not extend posterior to the biceps anchor. The Buford complex is characterized by a completely absent anterosuperior labrum combined with a thickened, cord-like middle glenohumeral ligament (MGHL). Attempting to suture a Buford complex to the anterior glenoid rim will severely restrict external rotation and cause profound iatrogenic morbidity.
The vascular supply to the superior labrum is notoriously tenuous, which directly impacts its healing potential following surgical repair. Microvascular studies by Cooper et al. demonstrated that the labrum does not receive significant blood supply from the underlying glenoid bone. Instead, it relies entirely on penetrating branches from the suprascapular, circumflex scapular, and posterior humeral circumflex arteries that travel through the adjacent joint capsule and periosteal tissues. Histological analysis reveals a relative "watershed" or avascular zone in the anterosuperior and superior aspects of the labrum. This physiological limitation mandates meticulous surgical preparation of the bony bed to stimulate a marrow-derived healing response.

Neurovascular considerations during SLAP repair are paramount, particularly regarding patient positioning and portal placement. The brachial plexus is the most significant structure at risk, vulnerable to traction neurapraxia if excessive distraction forces are applied in the lateral decubitus position. The suprascapular nerve is also at distinct risk. As it traverses the spinoglenoid notch to innervate the infraspinatus, it lies merely 1 to 2 centimeters medial to the posterosuperior glenoid rim. Errant, overly medial placement of suture anchors, or overly aggressive drilling in the posterior quadrant, can directly injure or entrap the suprascapular nerve. Similarly, the axillary nerve courses inferiorly and is susceptible during the establishment of low anterior portals or during aggressive capsular releases.
Exhaustive Indications and Contraindications
The decision-making paradigm for treating SLAP lesions has undergone a massive paradigm shift over the past decade. We have moved away from the historical approach of universally repairing all Type II tears. The current standard of care demands a highly individualized approach, heavily weighted by the patient's age, activity level, occupation, and concomitant pathology. The literature clearly demonstrates that SLAP repairs in older populations have unacceptably high rates of persistent pain, stiffness, and revision surgery.
Conservative management remains the first-line treatment for almost all suspected SLAP lesions. A rigorous, 3- to 6-month trial of physical therapy is mandatory. This rehabilitation must focus on correcting scapular dyskinesia, restoring periscapular muscle balance, and addressing glenohumeral internal rotation deficit (GIRD) through targeted posterior capsular stretching (e.g., sleeper stretches). Non-steroidal anti-inflammatory drugs (NSAIDs) and judicious use of intra-articular corticosteroid injections can serve as valuable adjuncts to facilitate participation in physical therapy. Only when a patient has unequivocally failed exhaustive conservative measures should surgical intervention be entertained.
Surgical repair is primarily indicated for young, active patients—specifically overhead athletes (pitchers, volleyball players) under the age of 30 to 35—who present with a clear history of injury, mechanical symptoms, and a symptomatic Type II SLAP tear confirmed on MRI and diagnostic arthroscopy. In this specific demographic, restoring the native anatomy is critical for returning to elite levels of overhead function. Conversely, in patients over the age of 40, or those with concurrent rotator cuff pathology, primary biceps tenodesis has emerged as the superior surgical option, providing highly reliable pain relief and functional restoration with a significantly lower complication profile than SLAP repair.
| Clinical Scenario / Factor | Indications for Arthroscopic SLAP Repair | Contraindications for SLAP Repair (Consider Tenodesis/Debridement) |
|---|---|---|
| Patient Age | Generally < 35 years old. | Generally > 40 years old. |
| Activity Level | Elite overhead athletes, heavy manual laborers requiring superior stability. | Low-demand patients, non-overhead athletes. |
| Pathology Type | Symptomatic Type II or Type IV SLAP tears. | Type I or III (Debridement usually sufficient), Sublabral foramen (Normal variant). |
| Concomitant Pathology | Associated Bankart lesion, multidirectional instability. | Concomitant full-thickness rotator cuff tears, advanced glenohumeral osteoarthritis, adhesive capsulitis. |
| Prior Treatment | Failure of 3-6 months of rigorous physical therapy and GIRD correction. | Lack of prior conservative management trial. |
| Tissue Quality | Robust, healthy labral tissue capable of holding suture. | Degenerative, friable labral tissue; chronic retracted tears. |

Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock upon which successful surgical execution is built. The diagnostic gold standard for non-invasive evaluation remains Magnetic Resonance Arthrography (MRA). The intra-articular injection of gadolinium contrast significantly increases the sensitivity and specificity for detecting labral pathology compared to standard MRI. We meticulously scrutinize the axial, coronal, and sagittal sequences for contrast extravasation between the superior labrum and the glenoid. The Abduction and External Rotation (ABER) view is particularly valuable, as it dynamically recreates the peel-back mechanism, often unmasking subtle posterosuperior detachments that might appear intact on standard resting views.
On the day of surgery, the anesthetic plan typically involves a combination of general anesthesia and an interscalene regional nerve block. The regional block provides exceptional postoperative analgesia, minimizing narcotic consumption and facilitating early mobilization. Prior to positioning, a comprehensive Examination Under Anesthesia (EUA) is mandatory. We systematically assess passive range of motion, focusing on external rotation at 90 degrees of abduction, and perform dynamic stability testing (load and shift, sulcus sign) to compare side-to-side laxity. This EUA provides critical baseline data that informs our intraoperative decision-making regarding capsular plication or concomitant stabilization procedures.

Patient Positioning: The Lateral Decubitus Advantage
For arthroscopic SLAP repair, we strongly advocate for the lateral decubitus position. While the beach-chair position is utilized by many excellent surgeons, the lateral decubitus setup provides unparalleled visualization and access to the superior and posterior labrum. The ability to apply controlled, multi-vector traction allows for optimal distraction of the glenohumeral joint, opening the subacromial and intra-articular spaces simultaneously.
The patient is carefully rolled onto their non-operative side on a standard operating table equipped with a beanbag positioner. A generous, meticulously placed axillary roll is positioned just caudal to the dependent axilla to protect the contralateral brachial plexus and ensure uncompromised venous return. The torso is secured rigidly with the beanbag, and the head is supported in a neutral anatomical alignment to prevent cervical spine hyperextension or lateral bending. All bony prominences, particularly the fibular head and greater trochanter, are heavily padded.

The operative arm is then suspended using a sterile traction sleeve connected to a calibrated boom system. The arm is typically positioned in 45 to 70 degrees of abduction and 15 to 20 degrees of forward flexion. This is a critical safety juncture: Traction weight must be strictly monitored and must never exceed 10 to 15 pounds. Exceeding this threshold, or maintaining traction for prolonged periods (generally > 2 hours), drastically increases the risk of catastrophic brachial plexus traction neurapraxia. The use of an inline tensiometer is highly recommended to ensure objective force measurement throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
With the patient optimally positioned and prepped, we initiate the surgical sequence. The procedure demands precision, respect for the soft tissues, and a deep understanding of arthroscopic spatial orientation.
1. Diagnostic Arthroscopy and Portal Establishment
We begin by establishing the standard posterior viewing portal, located approximately 2 cm inferior and 2 cm medial to the posterolateral corner of the acromion. A #15 blade is used to incise the skin, and a blunt trocar is advanced toward the coracoid process, penetrating the capsule just superior to the posterior band of the rotator cuff. Once intra-articular, the arthroscope is introduced, and the joint is distended with normal saline via an automated pump system maintained at roughly 40-50 mmHg to ensure hemostasis and clear visualization.
A systematic 15-point diagnostic sweep is performed. We meticulously evaluate the biceps tendon, tracing it from its intra-articular origin into the bicipital groove. The superior labrum is probed extensively. It is critical to differentiate a true Type II SLAP tear from a benign sublabral recess. A normal recess will have smooth, well-defined cartilaginous edges, whereas a SLAP tear will exhibit irregular, frayed margins, localized hemorrhage, and most importantly, the detachment will extend posterior to the biceps anchor. We also assess the anterior labrum, the glenohumeral ligaments, the articular cartilage of the humeral head and glenoid, and the undersurface of the rotator cuff.
Once the Type II SLAP lesion is confirmed, we establish our working portals using an outside-in spinal needle localization technique. The anterosuperior (AS) portal is created just off the anterolateral corner of the acromion, entering the joint superior to the biceps tendon. This serves as the primary viewing portal during posterior anchor placement. The anteroinferior (AI) portal is established just superior to the subscapularis tendon, serving as a primary working portal. In many cases, particularly for extensive posterior extensions of the tear, we utilize a trans-rotator cuff portal (often referred to as the Wilmington portal). This portal is localized via a spinal needle passing through the muscular portion of the supraspinatus, allowing for an ideal 45-degree trajectory to the superior glenoid rim for anchor insertion.

2. Glenoid Preparation and Tissue Debridement
Successful biological healing of the labrum to the glenoid requires meticulous preparation of the bony bed. Using an arthroscopic probe, we mobilize the detached labrum to assess the severity of the peel-back. A 4.5-mm motorized shaver is introduced to debride any degenerative, non-viable, or frayed tissue from the labral edge. We must be judicious here—over-resection will leave insufficient tissue for a robust repair.
Next, a motorized burr or a specialized arthroscopic rasp is used to decorticate the superior glenoid neck. The goal is to abrade the cortical bone just medial to the articular cartilage margin until punctate, bleeding cancellous bone is exposed. This bleeding bone provides the necessary marrow-derived stem cells and growth factors to facilitate fibrocartilaginous healing. Surgical Warning: The surgeon must maintain exquisite control of the burr to prevent it from skiving laterally and causing iatrogenic damage to the pristine articular cartilage of the glenoid face.

3. Suture Anchor Placement and Trajectory
Anchor placement is arguably the most technically demanding aspect of the procedure. For a standard Type II SLAP repair, we typically utilize one or two small-diameter (1.5 mm to 2.9 mm) biocomposite or all-suture anchors. The first anchor is almost always placed posterior to the biceps anchor to neutralize the peel-back force.
The drill guide is introduced through the optimal portal (often the trans-cuff portal for the posterior anchor). The tip of the guide is positioned on the prepared bone bed, precisely at the articular margin or 1-2 mm medial to it. The trajectory of the drill is critical; it must be inserted at the "deadman's angle"—approximately 45 degrees to the face of the glenoid. This angle maximizes bone purchase and ensures that the tension vector of the sutures pulls the labrum directly down onto the prepared bone bed. Drilling too medially risks penetration of the suprascapular notch and injury to the suprascapular nerve, while drilling too laterally risks violating the articular cartilage.
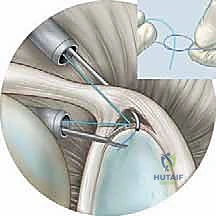
4. Suture Management and Knot Tying
Once the anchor is securely seated, suture passage begins. We employ various suture shuttling devices, such as a penetrating birdbeak or a suture lasso. The device is passed through the labral tissue from inferior to superior, capturing a robust bite of the capsule-labral complex. The suture limb is then retrieved and shuttled through the tissue. We typically utilize a simple suture configuration, passing the suture posterior to the anchor to recreate the anatomical bumper.
Knot tying must be executed flawlessly to avoid creating prominent, abrasive hardware within the joint. We prefer low-profile sliding knots (such as the SMC, Weston, or Duncan loop), backed up by three alternating half-hitches on alternating posts. Crucial Technical Point: The knot must be tied such that the "post" limb is the one exiting the anchor, and the knot is pushed down away from the articular surface, resting securely on the capsular side of the labrum. Knots that migrate medially and abrade the humeral head articular cartilage will cause devastating, rapid-onset chondrolysis. Alternatively, knotless anchor technology can be utilized to completely eliminate the risk of knot impingement, relying on interference fit for tissue tensioning.
After all anchors are placed and tied, we perform a final dynamic assessment. The arm is taken off traction and brought into the provocative abducted and externally rotated position. We confirm visually that the peel-back mechanism has been completely abolished and that the biceps anchor is rigidly stable against the glenoid.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, arthroscopic SLAP repair is fraught with potential complications. The orthopedic surgeon must be acutely aware of these risks, counsel patients appropriately preoperatively, and possess the surgical armamentarium to manage them when they arise.
The most common and frustrating complication following SLAP repair is postoperative stiffness, occurring in up to 15% of patients. This is frequently multifactorial, resulting from over-tensioning of the repair, inadvertent plication of the superior capsule, or delayed initiation of postoperative rehabilitation. Patients present with a profound loss of external rotation and elevation. Initial management consists of aggressive, directed physical therapy. If stiffness persists beyond 6 to 9 months and significantly impairs function, arthroscopic capsular release may be required.
Persistent pain and failure of biological healing represent another significant challenge, particularly in older patients or those involved in workers' compensation claims. Failure rates in patients over 40 years old can exceed 30%. This is often due to unrecognized, concomitant biceps tendinopathy or the inability of the degenerative labral tissue to integrate with the glenoid bone.
Hardware-related complications, while less common with the advent of modern biocomposite and all-suture anchors, still occur. Prominent anchors or bulky suture knots can act as a mechanical abrasive against the humeral head, leading to rapid, catastrophic chondrolysis. Historically, the use of intra-articular pain pumps infusing bupivacaine with epinephrine was definitively linked to massive glenohumeral chondrolysis, a practice that has been universally abandoned.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Postoperative Stiffness | 10% - 15% | Over-tensioning, capsular capture, delayed rehab, older age. | Aggressive PT, intra-articular corticosteroids, Arthroscopic capsular release. |
| Persistent Pain / Non-healing | 5% - 30% (Age dependent) | Poor biology, unrecognized biceps tendinopathy, older age (>40). | Biceps Tenodesis (Gold Standard Salvage), hardware removal. |
| Nerve Injury (Neuropraxia) | < 1% - 2% | Excessive traction (>15 lbs), errant medial drilling (suprascapular nerve). | Observation, EMG at 6 weeks, rarely requires surgical exploration. |
| Hardware Prominence / Chondrolysis | < 1% | Poor anchor trajectory, prominent knots, historical pain pumps. | Immediate arthroscopic hardware removal, chondroplasty, potential arthroplasty if severe. |
| Infection | < 0.5% | Standard surgical risks, inadequate sterilization. | Arthroscopic irrigation and debridement, targeted IV antibiotics. |


Detailed Chapters & Topics
Dive deeper into specialized chapters regarding arthroscopic-treatment-of-superior-labral-slap-tears