Arthroscopic Synovectomy: An Intraoperative Masterclass in Knee Joint Preservation

Key Takeaway
Master arthroscopic synovectomy with this expert guide. Learn patient selection, detailed knee anatomy, precise portal placement, and meticulous synovial resection. Understand neurovascular risks, optimize visualization, and manage post-operative care. Essential for fellows tackling chronic knee synovitis, including conditions like rheumatoid arthritis and PVNS, ensuring comprehensive joint preservation.
Comprehensive Introduction and Patho-Epidemiology
Arthroscopic synovectomy represents a cornerstone in the armamentarium of the joint preservation surgeon, offering a minimally invasive yet highly effective intervention for patients afflicted by chronic, debilitating synovial pathology. To master this procedure, one must first possess a profound comprehension of the underlying pathophysiology. The synovial membrane is not merely a passive envelope; it is a highly specialized, vascularized mesenchymal tissue responsible for the production of synovial fluid, which mediates both boundary lubrication and the critical diffusion of nutrients to the avascular articular cartilage. Histologically, the normal synovium consists of an intimal layer populated by macrophage-like type A synoviocytes and fibroblast-like type B synoviocytes, supported by a subintimal layer rich in microvasculature and lymphatics.
In pathological states, this delicate homeostatic balance is catastrophically disrupted. Chronic synovitis is characterized by profound synovial hyperplasia, villous transformation, and intense mononuclear cellular infiltration. This hypertrophic tissue becomes a primary driver of joint destruction. In conditions such as rheumatoid arthritis (RA), the hyperplastic synovium—termed pannus—actively invades and degrades articular cartilage and subchondral bone through the elaboration of matrix metalloproteinases (MMPs), cathepsins, and pro-inflammatory cytokines (e.g., TNF-alpha, IL-1, IL-6). The goal of a synovectomy is therefore not merely mechanical debulking, but the radical extirpation of this biochemically active, destructive tissue to arrest or significantly delay the progression of secondary arthrosis.

The epidemiological landscape of patients requiring arthroscopic synovectomy is diverse, encompassing a spectrum of autoimmune, neoplastic, and hematologic etiologies. While the advent of biologic disease-modifying antirheumatic drugs (bDMARDs) has reduced the incidence of surgical intervention for RA, a significant cohort of patients still presents with recalcitrant monoarticular or oligoarticular disease. Beyond RA, the surgeon must be intimately familiar with pigmented villonodular synovitis (PVNS)—now more accurately termed tenosynovial giant cell tumor (TGCT)—which presents in both localized and diffuse forms, driven by a specific genetic translocation (CSF1R). Other critical etiologies include synovial osteochondromatosis, characterized by metaplastic cartilage formation within the synovium; hemophilic arthropathy, where recurrent hemarthrosis induces a toxic, iron-laden hyperplastic synovitis; and crystalline arthropathies such as severe, tophaceous gout or pseudogout.
Understanding the specific patho-epidemiology of the patient's condition dictates the aggressiveness of the surgical approach. For instance, diffuse PVNS demands an exhaustive, near-total synovectomy encompassing all anterior and posterior compartments to mitigate the notoriously high recurrence rates, which can exceed 30% even in experienced hands. Conversely, a localized nodular PVNS lesion may only require a targeted excision. The operating surgeon must approach the pathological knee not just as a mechanical derangement, but as a complex biological environment where surgical precision directly alters the natural history of the disease.
Detailed Surgical Anatomy and Biomechanics
A masterful arthroscopic synovectomy requires an encyclopedic knowledge of the knee's complex internal topography. The synovial cavity of the knee is the largest and most complex in the human body, characterized by numerous recesses, plicae, and blind pouches that serve as havens for hyperplastic tissue. The suprapatellar pouch, extending superiorly deep to the quadriceps tendon, is often the primary reservoir for massive effusions and exuberant synovial villi. This pouch communicates with the main joint cavity, though occasionally, a complete suprapatellar plica may isolate it, necessitating surgical fenestration for complete access.

Descending into the anterior compartment, the surgeon must navigate the medial and lateral gutters. These recesses extend distally alongside the femoral condyles and are frequently occluded by dense, fibrotic synovium in chronic disease states. The medial gutter is bounded by the medial capsule and the medial patellofemoral ligament, while the lateral gutter is defined by the lateral retinaculum and the popliteus hiatus. The popliteus hiatus itself is a critical anatomical landmark; it represents a synovial extension surrounding the popliteus tendon and is a notorious hiding spot for loose bodies in synovial chondromatosis and residual disease in PVNS. Failure to adequately visualize and debride the popliteus hiatus is a common cause of surgical failure.

The intercondylar notch houses the cruciate ligaments, which are extrasynovial but intra-articular. They are enveloped by a synovial reflection that extends from the posterior capsule. In severe rheumatoid or hemophilic arthropathy, this synovial envelope becomes massively hypertrophied, encasing the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) and obliterating the notch. Meticulous resection here is paramount, not only to remove the diseased tissue but also to prevent notch impingement and restore terminal extension. The surgeon must exercise extreme caution when using motorized shavers near the cruciate ligaments to avoid iatrogenic structural damage.
Finally, the posterior compartments—posteromedial and posterolateral—represent the most technically demanding anatomical zones for synovectomy. Separated by the thick posterior septum, these compartments require specialized portal placement and a 70-degree arthroscope for adequate visualization. The posteromedial compartment lies behind the medial femoral condyle and the posterior horn of the medial meniscus, extending distally to the semimembranosus bursa. The posterolateral compartment is intimately related to the popliteus tendon and the lateral head of the gastrocnemius. The overarching biomechanical goal of clearing these spaces is to restore normal capsular compliance, thereby normalizing joint kinematics and eliminating the mechanical blocks to flexion often caused by posterior synovial impingement.
Exhaustive Indications and Contraindications
The decision to proceed with an arthroscopic synovectomy is predicated on a rigorous evaluation of the patient's clinical trajectory, recognizing that surgery is typically reserved for cases refractory to exhaustive conservative management. The primary indication is chronic, debilitating synovitis—characterized by persistent pain, recurrent massive effusions, mechanical catching, and loss of motion—that has failed to respond to a minimum of six months of optimal medical therapy. This includes systemic pharmacotherapy (NSAIDs, DMARDs, biologics) managed in conjunction with a rheumatologist, repeated intra-articular corticosteroid or hyaluronic acid injections, and targeted physical therapy aimed at maintaining range of motion (ROM) and muscular strength.

Specific disease states present distinct indications. In Rheumatoid Arthritis, synovectomy is indicated when medical management fails to control local joint inflammation, specifically aiming to halt the progression of cartilaginous erosion. In Pigmented Villonodular Synovitis (PVNS), surgical excision is the definitive treatment; the indication is absolute upon diagnosis, given the aggressive, locally destructive nature of the disease. For Synovial Osteochondromatosis, the presence of symptomatic loose bodies and mechanical locking mandates arthroscopic removal and synovectomy to prevent secondary osteoarthritis. Hemophilic arthropathy presents a unique challenge; synovectomy is indicated to break the vicious cycle of recurrent hemarthrosis and subsequent synovial hypertrophy, though it requires meticulous perioperative factor replacement coordination with hematology.

Contraindications, while relatively few, are absolute in their capacity to predict surgical failure. Advanced degenerative joint disease (Kellgren-Lawrence Grade III or IV) is a primary contraindication; in the presence of bone-on-bone arthrosis, a synovectomy will not alleviate mechanical pain and may paradoxically accelerate the need for total knee arthroplasty (TKA). Significant axial malalignment (severe varus or valgus deformity) or gross ligamentous instability similarly portend poor outcomes, as the underlying biomechanical derangement will continue to drive joint destruction regardless of synovial resection. Furthermore, active intra-articular infection (septic arthritis) requires emergent irrigation and debridement, not a formal synovectomy.
| Category | Indications | Contraindications |
|---|---|---|
| Clinical Status | Chronic synovitis refractory to >6 months of conservative care; Recurrent massive effusions; Mechanical symptoms due to synovial impingement. | Advanced osteoarthritis (Kellgren-Lawrence III/IV); Gross joint instability; Severe axial malalignment. |
| Pathological Etiology | Rheumatoid Arthritis (mono/oligoarticular failure); PVNS (Localized or Diffuse); Synovial Osteochondromatosis; Hemophilic Arthropathy. | Active untreated septic arthritis (requires I&D, not elective synovectomy); Uncorrected coagulopathy. |
| Systemic Factors | Medically optimized patients with localized joint destruction. | Severe cardiopulmonary disease precluding prolonged anesthesia; Active systemic flare of rheumatologic disease. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock upon which a successful, complication-free arthroscopic synovectomy is built. The diagnostic workup must be exhaustive. Joint aspiration is a mandatory first step, serving both therapeutic and diagnostic purposes. Synovial fluid analysis must include cell count with differential, crystal analysis under polarized light microscopy, Gram stain, and aerobic/anaerobic cultures. The macroscopic appearance of the fluid is highly suggestive: frankly bloody or xanthochromic fluid raises high suspicion for PVNS or hemangioma, while turbid, low-viscosity fluid with high leukocyte counts points toward inflammatory arthritides.

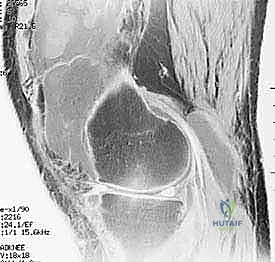
Advanced imaging is non-negotiable. While weight-bearing orthogonal radiographs are essential for assessing joint space narrowing, osteopenia, and periarticular erosions, Magnetic Resonance Imaging (MRI) is the gold standard for preoperative templating in synovectomy. MRI allows the surgeon to map the exact extent of synovial hypertrophy, differentiating localized from diffuse disease. In PVNS, the characteristic hemosiderin deposition appears as a distinct "blooming artifact" with low signal intensity on both T1- and T2-weighted sequences. The surgeon must scrutinize the MRI to identify extracapsular extension or involvement of the posterior compartments, which will dictate the necessity of posteromedial and posterolateral portals.
In the operating theater, anesthesia and patient positioning must be optimized for a prolonged, technically demanding procedure. General anesthesia is preferred, often supplemented by a regional block (e.g., adductor canal block) or an epidural to preemptively manage the significant postoperative pain associated with extensive capsular resection. The patient is positioned supine. Crucially, the operative table is configured to allow the operative leg to hang freely over the edge, with the foot of the bed dropped and the bed slightly flexed. This specific positioning induces slight hip flexion, which significantly decreases tension on the femoral nerve—a vital consideration given the prolonged traction and manipulation required during the case.

A well-padded thigh tourniquet is applied proximally and inflated to 250-300 mmHg only after meticulous exsanguination with an Esmarch bandage. The contralateral leg must be protected with sequential compression devices to mitigate the risk of deep vein thrombosis (DVT). We strictly advocate against the use of a rigid arthroscopic leg holder that locks the knee in flexion. Such devices dangerously restrict the surgeon's ability to manipulate the limb into deep flexion or extension, which is absolutely necessary to access the extreme superior and posterior recesses of the joint. Instead, a simple lateral post positioned at the midthigh serves as a fulcrum for applying valgus stress, allowing dynamic, unrestricted positioning throughout the procedure.

Step-by-Step Surgical Approach and Resection Technique
Portal Placement and Diagnostic Arthroscopy
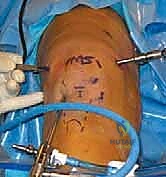
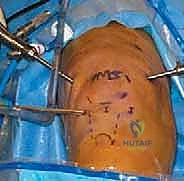
The execution of a comprehensive arthroscopic synovectomy demands a systematic, compartmentalized approach, beginning with strategic portal placement. Standard anterolateral and anteromedial portals are insufficient for a total synovectomy. We routinely employ a minimum of five to six portals. The procedure commences with the establishment of a standard inferolateral viewing portal. Immediately upon entry, a superomedial portal is established to serve as a dedicated, high-flow outflow tract. Continuous, high-volume fluid management is critical; the hyperplastic synovium bleeds profusely, and maintaining visualization requires a robust, dedicated outflow to clear debris and hemorrhage.
With the 30-degree arthroscope in the inferolateral portal, a rigorous diagnostic sweep is performed. The surgeon assesses the integrity of the articular cartilage, the menisci, and the degree of synovial proliferation. Following this, a superolateral working portal is established under direct intra-articular visualization. This portal is the primary conduit for the motorized shaver during the anterior synovectomy. The surgeon must ensure this portal is placed high enough above the patella to allow the shaver to reach the apex of the suprapatellar pouch without levering against the patellofemoral articulation.
Anterior Compartment Synovectomy
The resection begins systematically in the suprapatellar pouch. Utilizing a 4.0mm or 4.5mm aggressive full-radius resector, the surgeon meticulously debulks the hypertrophic tissue. The technique involves a sweeping motion, keeping the cutting window of the shaver facing the capsule and away from the delicate articular cartilage of the trochlea and patella. The surgeon must resect down to the glistening white capsular layer, ensuring no residual islands of pathological tissue remain. A biopsy trap must be connected to the suction line early in this phase to capture representative tissue samples for definitive histopathological and microbiological analysis.

Once the suprapatellar pouch is cleared, attention is turned to the medial and lateral gutters. The arthroscope is swept down the medial gutter, and the shaver follows. Applying a valgus stress against the lateral post opens the medial compartment, facilitating access. The surgeon must be meticulous in clearing the tissue overlying the medial meniscus and the deep medial collateral ligament. The process is repeated in the lateral gutter, applying varus stress. Particular attention must be paid to the popliteus hiatus; the shaver is carefully introduced into the hiatus to clear out synovial reflections and any occult loose bodies, a common site for recurrence in synovial chondromatosis.

The intercondylar notch is addressed next. The hypertrophic synovium here often obscures the ACL and PCL. Using a combination of the motorized shaver and arthroscopic electrocautery (radiofrequency wand), the surgeon carefully skeletonizes the cruciate ligaments. It is imperative to avoid aggressive shaving directly on the ligamentous fibers. The radiofrequency wand is highly effective here for tissue ablation and concurrent hemostasis. Clearing the notch completely is vital for restoring full terminal extension and preventing anterior impingement.

Posterior Compartment Synovectomy and the Trans-Septal Approach
Addressing the posterior compartments is the hallmark of a masterclass synovectomy. For diffuse disease, a trans-septal approach is frequently required. The arthroscope is passed through the intercondylar notch (the Gillquist maneuver) to visualize the posteromedial compartment. Under direct trans-notch visualization, a posteromedial portal is established using a spinal needle for localization, followed by a scalpel and blunt trocar. The surgeon must stay superior to the joint line to avoid the saphenous vein and nerve.

Once the posteromedial portal is established, a 70-degree arthroscope is introduced here to visualize the posterior septum. A posterolateral portal is then created. Using a shaver or radiofrequency wand from the posterolateral portal, the surgeon carefully fenestrates the posterior septum, creating a communication between the posteromedial and posterolateral compartments. Surgical Warning: The middle geniculate artery and the popliteal neurovascular bundle lie immediately posterior to this septum. Extreme caution, meticulous depth control, and maintaining the shaver blade facing anteriorly are absolute requirements to prevent catastrophic vascular injury.

With the trans-septal window created, the surgeon can now pass instruments freely between the posterior portals, performing a radical resection of the posterior capsular synovium. The 70-degree scope provides unparalleled visualization of the posterior femoral condyles and the posterior horn of the menisci. All recesses, including the semimembranosus bursa extension, must be meticulously cleared.

Hemostasis and Final Execution
The final, and arguably most critical, phase of the procedure is achieving absolute hemostasis. An extensive synovectomy leaves a massive, raw, highly vascularized capsular surface. Before concluding, the tourniquet must be deflated while the arthroscope remains in the joint. The joint is thoroughly irrigated, and fluid pressure is temporarily lowered to identify bleeding vessels.

The surgeon systematically sweeps through all compartments with the radiofrequency wand, meticulously coagulating any active bleeders. Failure to achieve meticulous hemostasis will inevitably result in a massive postoperative hemarthrosis, leading to severe pain, delayed rehabilitation, and a high risk of arthrofibrosis. Once hemostasis is verified, a large-bore intra-articular drain (e.g., Hemovac) is routinely placed through one of the superior portals to evacuate postoperative hematoma. The portals are then closed with non-absorbable sutures, and a bulky, compressive Jones dressing is applied before the patient is awakened.


Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, arthroscopic synovectomy carries a distinct complication profile that the orthopedic surgeon must be prepared to manage. The most frequent immediate postoperative complication is hemarthrosis, occurring in 5% to 15% of cases, heavily dependent on the thoroughness of intraoperative hemostasis upon tourniquet deflation. A tense hemarthrosis causes excruciating pain, stretches the joint capsule, and acts as a biological catalyst for profound arthrofibrosis. Management requires immediate aspiration under sterile conditions and, if recurrent, a return to the operating room for arthroscopic washout and electrocoagulation of the bleeding source.

Infection, while rare (incidence < 1%), is a devastating complication, particularly in immunocompromised patients with rheumatoid arthritis on biologic therapies. Superficial portal site infections can typically be managed with oral antibiotics, but deep joint sepsis demands emergent arthroscopic irrigation and debridement (I&D) coupled with targeted intravenous antibiotic therapy. Iatrogenic neurovascular injury is the most feared complication, specifically injury to the popliteal artery or vein during posterior compartment work. Adherence to safe zones—staying anterior to the posterior capsule and directing instruments away from the popliteal fossa—is mandatory. Injury to the infrapatellar branch of the saphenous nerve during anteromedial portal placement can lead to chronic anterior knee pain and numbness.
Disease recurrence is a biological reality rather than a strict surgical complication, particularly in the context of diffuse PVNS, where recurrence rates can approach 30-40% at 5 years. Salvage management for recurrent PVNS may involve a repeat, more aggressive open synovectomy, often combined with adjuvant therapies such as intra-articular radiation synovectomy (e.g., Yttrium-90) or systemic targeted therapies (CSF1R inhibitors like pexidartinib). For patients with inflammatory arthritides who progress to end-stage joint destruction despite synovectomy, Total Knee Arthroplasty (TKA) remains the ultimate salvage procedure, though the surgeon must be aware that prior synovectomy can complicate the surgical exposure due to capsular scarring.

| Complication | Estimated Incidence | Prevention & Salvage Management |
|---|---|---|
| Hemarthrosis | 5% - 15% | Prevention: Meticulous RF ablation after tourniquet let-down; Drain placement. Management: Sterile aspiration; return to OR for washout if tense/recurrent. |
| Arthrofibrosis | 3% - 8% | Prevention: Early, aggressive ROM; CPM machine |
Clinical & Radiographic Imaging Archive



