Comprehensive Case Study: Chronic Exertional Compartment Syndrome in a Long-Distance Runner
Key Takeaway
Chronic Exertional Compartment Syndrome (CECS) in runners is diagnosed through a combination of classic exertional leg pain, specific clinical findings post-exertion (weakness, paresthesia), and ruling out other pathologies with imaging. The gold standard for definitive diagnosis involves invasive compartment pressure testing performed during or immediately after symptomatic exercise.
Patient Presentation and History
A 25-year-old male, a competitive long-distance runner with a half-marathon personal best of 1 hour 25 minutes, presented to the clinic with a chief complaint of bilateral lower leg pain, tightness, and paresthesias primarily affecting the anterior and lateral compartments. The symptoms had an insidious onset approximately six months prior to presentation and were directly correlated with running activity. Initially, the discomfort would manifest after approximately 30 minutes of running at a moderate pace. Over the subsequent months, the symptom-free interval progressively shortened, such that by the time of presentation, pain and tightness would consistently develop within 10 to 15 minutes of initiating a run, necessitating cessation of activity.
The patient described the pain as a bursting or cramping sensation, often accompanied by a feeling of profound muscle weakness and foot drop sensation, particularly on the right side. He also reported transient numbness and tingling along the dorsum of both feet, which would resolve completely within 15 to 20 minutes of resting. Symptoms were consistently bilateral, though slightly more pronounced in the right leg. There was no history of acute trauma, sudden increase in training volume, or recent changes in footwear. His past medical history was otherwise unremarkable, with no known chronic illnesses, neurological conditions, or vascular pathologies. He denied smoking, alcohol abuse, or recreational drug use. Family history was non-contributory. His primary athletic goal was to continue competitive running at an elite level, and the current symptoms were severely impeding his training and performance. Conservative measures, including activity modification, stretching, foam rolling, non-steroidal anti-inflammatory drugs, and a course of physiotherapy focusing on gait analysis and strengthening, had provided no significant or lasting relief.
Pathophysiology and Biomechanical Considerations
To fully contextualize this presentation, it is imperative to understand the underlying pathophysiology of Chronic Exertional Compartment Syndrome. Unlike acute compartment syndrome, which is typically driven by trauma or hemorrhage leading to a rapid, irreversible increase in intracompartmental pressure, Chronic Exertional Compartment Syndrome is a reversible, exercise-induced phenomenon. During vigorous exercise, skeletal muscle volume can increase by up to twenty percent due to increased capillary perfusion, extracellular fluid accumulation, and metabolic hyperemia.
In a normal physiological state, the surrounding fascial envelopes possess sufficient compliance to accommodate this transient volumetric expansion. However, in patients with Chronic Exertional Compartment Syndrome, the osseofascial boundaries are pathologically non-compliant. This rigidity prevents adequate expansion, leading to a precipitous rise in interstitial tissue pressure. As the intracompartmental pressure surpasses the capillary venous pressure, venous outflow is obstructed. This creates a localized venous stasis, which further exacerbates the interstitial edema and drives the pressure higher, eventually compromising the arteriovenous gradient.
The resultant microvascular ischemia leads to a shift toward anaerobic metabolism, producing lactic acid and other noxious metabolites that stimulate group IV nociceptive afferent nerve fibers, producing the characteristic bursting pain. Furthermore, the elevated pressure directly compresses traversing peripheral nerves. In the anterior and lateral compartments, the deep peroneal nerve and superficial peroneal nerve are particularly vulnerable. Ischemic neuropraxia of the deep peroneal nerve results in the transient anterior tibialis weakness and foot drop reported by the patient, while compression of the superficial peroneal nerve yields the dorsal paresthesias. Once the exertional stimulus is removed, the metabolic demand decreases, capillary perfusion normalizes, and the accumulated fluid is gradually resorbed, leading to the characteristic resolution of symptoms at rest.
Longitudinal Training History and Microtrauma
Further detailed history taking revealed that the patient maintained a baseline training volume of approximately 60 to 70 miles per week, primarily consisting of road running with variable elevation profiles. While he denied a sudden acute spike in volume, he noted a gradual shift toward more intensive interval training and hill repeats over the preceding eight months.
This type of eccentric loading is known to induce microtears in the myofascial interface. It is hypothesized that repetitive microtrauma to the fascia, combined with chronic inflammation, leads to fibrotic thickening and a subsequent reduction in fascial elasticity. This acquired fascial hypertrophy is a critical driver in the pathogenesis of Chronic Exertional Compartment Syndrome in elite endurance athletes, distinguishing it from congenital fascial tightness.
Clinical Examination Findings
Upon initial static inspection, both lower extremities appeared symmetric, with no overt swelling, erythema, muscular atrophy, or obvious deformity. Skin integrity was intact, and there were no signs of chronic venous insufficiency or arterial compromise. Muscle bulk in the gastrocnemius-soleus complex and anterior leg compartments appeared appropriate for an athletic individual, with no obvious hypertrophy.
Palpation at rest revealed mild tenderness over the anterior and lateral compartments of both tibias, more pronounced on the right. There was no focal bony tenderness indicative of stress fracture or periostitis. The compartments felt soft and compliant. Passive and active ranges of motion of the ankle and foot were full and pain-free bilaterally. Muscle strength testing at rest was graded normal across all major muscle groups, with no discernible weakness in ankle dorsiflexion, plantarflexion, inversion, eversion, or toe flexion and extension.
Neurological examination at rest was entirely normal. Sensation to light touch and pinprick was intact in all dermatomal distributions of the lower extremities. Deep tendon reflexes were symmetric bilaterally. Peripheral vascular examination revealed strong and symmetric dorsalis pedis and posterior tibial pulses bilaterally. Capillary refill time was less than two seconds in all digits.
Provocative Testing and Post Exertion Assessment
To confirm the exertional nature of the symptoms and aid in diagnosis, a provocative exercise test was performed. The patient ran on a treadmill at a predefined pace, gradually increasing the intensity until his typical symptoms developed, which occurred at approximately 12 minutes. Immediately post-exertion, re-examination revealed stark contrast to the resting state.
Upon inspection, there was mild, diffuse fullness and increased tension palpable over the anterior and lateral compartments of both lower legs. Muscle herniations, which are frequently observed through fascial defects in the lateral compartment, were not clinically evident in this patient, though their absence does not preclude the diagnosis.
The anterior and lateral compartments felt remarkably tense, described as wood-like upon palpation, demonstrating a significant loss of normal tissue compliance compared to the pre-exercise state. Palpation elicited severe, localized pain over the muscle bellies of the tibialis anterior and the peroneus longus and brevis.
Post Exertional Neurological and Vascular Deficits
A focused neurological examination conducted within three minutes of exercise cessation revealed objective deficits correlating with the patient's subjective complaints. Muscle strength testing demonstrated a discernible weakness in right ankle dorsiflexion and great toe extension, graded at 4-/5, indicating transient paresis of the tibialis anterior and extensor hallucis longus secondary to deep peroneal nerve ischemia.
Sensory examination revealed diminished sharp-dull discrimination over the dorsum of the right foot, corresponding to the cutaneous distribution of the superficial peroneal nerve, and a subtle decrease in sensation in the first dorsal web space, corresponding to the deep peroneal nerve.
Vascular examination remained grossly intact, with palpable dorsalis pedis and posterior tibial pulses. This is a critical clinical finding, as Chronic Exertional Compartment Syndrome primarily affects the microcirculation and capillary beds; major arterial inflow is rarely compromised. The preservation of distal pulses post-exertion helps differentiate this condition from macrovascular pathologies such as Popliteal Artery Entrapment Syndrome or exercise-induced arterial endofibrosis.
Imaging and Diagnostics
The diagnosis of Chronic Exertional Compartment Syndrome is primarily clinical, supported by objective intracompartmental pressure monitoring. However, a comprehensive diagnostic workup is mandatory to exclude other common etiologies of exercise-induced leg pain, collectively referred to as medial tibial stress syndrome or shin splints.
Radiographic and Advanced Imaging Evaluation
Standard weight-bearing orthogonal radiographs of the tibia and fibula were obtained. These were entirely unremarkable, demonstrating normal bone morphology, adequate cortical thickness, and no evidence of periosteal reaction, cortical hypertrophy, or radiolucent lines that would suggest a tibial or fibular stress fracture.
To further evaluate the osseous and soft tissue structures, Magnetic Resonance Imaging without contrast was ordered. The MRI protocol included axial and sagittal T1-weighted, T2-weighted, and Short Tau Inversion Recovery sequences. The resting MRI demonstrated no bone marrow edema, effectively ruling out early-stage stress fractures and medial tibial stress syndrome. There was no evidence of deep vein thrombosis, popliteal artery entrapment, or focal muscle tears.
While resting MRI is often normal in Chronic Exertional Compartment Syndrome, advanced imaging protocols utilizing post-exercise T2-weighted mapping can be highly suggestive of the condition. In this patient, a post-exercise MRI was not obtained, as the clinical presentation strongly warranted direct pressure measurement, which remains the gold standard. However, it is worth noting that post-exercise T2 hyperintensity within the affected compartments, reflecting increased extracellular fluid and edema, can serve as a valuable non-invasive adjunct in equivocal cases.
Intracompartmental Pressure Monitoring
The definitive diagnostic modality for Chronic Exertional Compartment Syndrome is dynamic intracompartmental pressure monitoring. This was performed using a solid-state transducer intracompartmental catheter system.
The procedure was conducted in the clinic setting. The skin over the anterior, lateral, superficial posterior, and deep posterior compartments was prepped with chlorhexidine and anesthetized with a small wheal of 1% lidocaine, taking care not to inject anesthetic deeply into the muscle belly, which could artificially elevate the pressure readings.
A slit catheter was introduced into the muscle bellies of all four compartments bilaterally at the junction of the proximal and middle thirds of the leg, the zone of maximal muscle girth. Baseline resting pressures were recorded with the patient in a supine position.
The patient was then instructed to run on a treadmill until his typical severe symptoms were reproduced, which occurred at 13 minutes. He immediately returned to the examination table, and post-exercise pressures were recorded at one minute and five minutes post-cessation of activity.
Diagnostic Criteria and Pressure Analysis
The diagnosis of Chronic Exertional Compartment Syndrome is classically established using the Pedowitz criteria. According to these criteria, one or more of the following pressure thresholds must be met to confirm the diagnosis:
1. A pre-exercise resting pressure greater than or equal to 15 mm Hg.
2. A one-minute post-exercise pressure greater than or equal to 30 mm Hg.
3. A five-minute post-exercise pressure greater than or equal to 20 mm Hg.
The patient's pressure readings were as follows:
Right Leg:
* Anterior Compartment: Resting 18 mm Hg, 1-minute post 45 mm Hg, 5-minute post 32 mm Hg.
* Lateral Compartment: Resting 16 mm Hg, 1-minute post 38 mm Hg, 5-minute post 28 mm Hg.
* Deep Posterior Compartment: Resting 10 mm Hg, 1-minute post 18 mm Hg, 5-minute post 12 mm Hg.
* Superficial Posterior Compartment: Resting 8 mm Hg, 1-minute post 15 mm Hg, 5-minute post 10 mm Hg.
Left Leg:
* Anterior Compartment: Resting 16 mm Hg, 1-minute post 40 mm Hg, 5-minute post 28 mm Hg.
* Lateral Compartment: Resting 14 mm Hg, 1-minute post 35 mm Hg, 5-minute post 25 mm Hg.
* Deep Posterior Compartment: Resting 9 mm Hg, 1-minute post 16 mm Hg, 5-minute post 11 mm Hg.
* Superficial Posterior Compartment: Resting 8 mm Hg, 1-minute post 14 mm Hg, 5-minute post 9 mm Hg.
These results unequivocally demonstrated pathologically elevated pressures in the anterior and lateral compartments bilaterally, fulfilling the Pedowitz criteria for Chronic Exertional Compartment Syndrome. The deep and superficial posterior compartments remained well within normal physiological limits, guiding the subsequent surgical planning toward an isolated anterolateral release.
Differential Diagnosis
The differential diagnosis for exertional lower extremity pain in an athlete is broad. A systematic approach is required to differentiate Chronic Exertional Compartment Syndrome from other common pathologies. The primary differentials include Medial Tibial Stress Syndrome, Tibial Stress Fractures, Popliteal Artery Entrapment Syndrome, and exertional peripheral nerve entrapment.
Medial Tibial Stress Syndrome typically presents as diffuse pain along the posteromedial border of the distal third of the tibia. Unlike Chronic Exertional Compartment Syndrome, the pain often occurs at the onset of exercise, may warm up and improve during the activity, and returns post-exercise. Palpation reveals diffuse tenderness along the tibial crest, rather than tense muscle compartments.
Tibial Stress Fractures present with focal, pinpoint bony tenderness. The pain progressively worsens with weight-bearing and is often present even with low-impact activities like walking. Advanced imaging, such as MRI or bone scintigraphy, is diagnostic, showing focal bone marrow edema or cortical disruption.
Popliteal Artery Entrapment Syndrome is a critical vascular differential. It involves the anomalous anatomical relationship between the popliteal artery and the medial head of the gastrocnemius, leading to dynamic arterial occlusion during plantarflexion. Patients present with claudication-like calf pain, cramping, and notably, diminished or absent pedal pulses during active plantarflexion or post-exercise.
Comparative Analysis of Exertional Leg Pain
| Condition | Primary Symptom Presentation | Onset and Offset Characteristics | Key Diagnostic Findings |
|---|---|---|---|
| Chronic Exertional Compartment Syndrome | Bursting pain, tightness, paresthesias in specific muscle compartments. | Insidious onset during exercise at a predictable time/distance. Resolves completely within 30 minutes of rest. | Elevated intracompartmental pressures (Pedowitz criteria). Tense compartments post-exercise. |
| Medial Tibial Stress Syndrome | Diffuse, dull ache along the posteromedial border of the tibia. | Pain early in exercise, may improve during activity, worsens post-exercise. Prolonged ache at rest. | Diffuse tenderness along the distal medial tibial border. Normal compartment pressures. |
| Tibial Stress Fracture | Sharp, focal pain over the tibia. | Pain worsens progressively with any weight-bearing activity. Night pain is common. | Focal bony tenderness. MRI shows bone marrow edema or cortical fracture line. |
| Popliteal Artery Entrapment Syndrome | Cramping, claudication-like pain primarily in the posterior calf. | Predictable onset with exercise, rapid relief with rest. | Diminished distal pulses during active plantarflexion. Abnormal ankle-brachial index post-exercise. |
| Superficial Peroneal Nerve Entrapment | Sharp, shooting pain and numbness over the lateral leg and dorsum of the foot. | Worsens with exercise, particularly activities requiring repetitive ankle inversion/plantarflexion. | Positive Tinel's sign where the nerve exits the deep fascia. EMG/NCS may show conduction delay. |
Surgical Decision Making and Classification
The management of Chronic Exertional Compartment Syndrome follows a distinct algorithm. Conservative management is generally the first-line approach, encompassing activity modification, orthotics, physical therapy, and anti-inflammatory medications. However, in competitive athletes seeking to return to their prior level of performance, conservative measures have a notoriously high failure rate, often exceeding eighty percent.
In this case, the patient had diligently trialed over six months of non-operative modalities without success. Given his desire to return to elite long-distance running, the definitive diagnosis confirmed by intracompartmental pressure monitoring, and the clear failure of conservative treatment, operative intervention was strongly indicated.
Compartment Involvement Classification
Surgical decision-making in Chronic Exertional Compartment Syndrome is heavily dictated by the specific compartments involved. While there is no standardized alphanumeric classification system akin to the AO/OTA fracture classification, the pathology is functionally classified based on anatomical involvement:
1. Isolated Anterior Compartment Syndrome.
2. Combined Anterolateral Compartment Syndrome.
3. Deep Posterior Compartment Syndrome.
4. Four-Compartment Syndrome.
Accurate pre-operative mapping via pressure monitoring is critical. Prophylactic release of uninvolved compartments is not recommended due to the increased risk of iatrogenic morbidity, prolonged recovery, and potential alterations in normal biomechanics. In this patient, the pressure readings clearly localized the pathology to the anterior and lateral compartments bilaterally. Therefore, a bilateral anterolateral fasciotomy was planned.
Fasciotomy versus Fasciectomy
A critical intra-operative decision involves choosing between a simple fasciotomy, which involves incising the fascia to release tension, and a fasciectomy, which involves excising a strip of the fascia.
While minimally invasive or endoscopic single-incision fasciotomies offer smaller cosmetic scars and theoretically faster initial recovery, they carry a higher risk of incomplete release and subsequent recurrence, particularly in the anterior compartment where the fascia is thick and robust. The recurrence rate for simple fasciotomy in elite athletes can approach fifteen to twenty percent, often due to fascial scarring and re-tethering.
For this high-demand competitive runner, a partial fasciectomy was selected. Excision of a one to two-centimeter strip of the anterior and lateral fascia significantly reduces the risk of fascial re-approximation and recurrent compartmental hypertension. While this approach requires a slightly larger incision and meticulous hemostasis, the long-term functional outcomes and lower recurrence rates make it the preferred technique for elite endurance athletes.
Surgical Technique and Intervention
The patient was taken to the operating room and placed in the supine position on a radiolucent operating table. General anesthesia was induced, and prophylactic intravenous antibiotics were administered prior to tourniquet inflation. Bilateral thigh tourniquets were applied. A bump was placed under the ipsilateral hip to internally rotate the leg, optimizing visualization of the anterolateral aspect of the lower extremity. The bilateral lower extremities were prepped and draped in standard sterile fashion.
The procedure was performed sequentially, beginning with the right leg. The limb was exsanguinated using an Esmarch bandage, and the tourniquet was inflated to 250 mm Hg.
Incision and Superficial Dissection
A single-incision approach was utilized to access both the anterior and lateral compartments. A longitudinal incision, approximately five to seven centimeters in length, was centered over the anterior intermuscular septum at the junction of the middle and distal thirds of the leg, approximately two centimeters lateral to the tibial crest.
Subcutaneous dissection was carried out using electrocautery. Meticulous care was taken to undermine the subcutaneous tissues widely, both anteriorly toward the tibial crest and posteriorly toward the fibula. This wide undermining is critical to allow adequate retraction and visualization for a complete fascial release without placing undue tension on the skin edges, which can lead to postoperative skin necrosis.
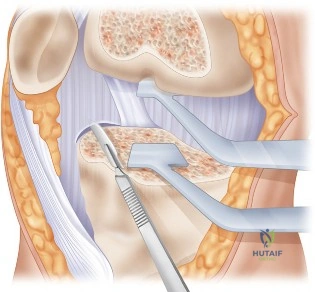
Identification and Protection of the Superficial Peroneal Nerve
The most critical step in this approach is the identification and protection of the superficial peroneal nerve. The nerve typically pierces the deep fascia of the lateral compartment to become subcutaneous approximately ten to twelve centimeters proximal to the lateral malleolus. However, anatomical variations are common. In some patients, the nerve may exit more proximally, or it may have multiple branches exiting through separate fascial defects.
Using blunt dissection with a peanut sponge, the perifascial areolar tissue was swept away. The superficial peroneal nerve was successfully identified exiting the lateral compartment fascia at the distal extent of the incision. The nerve was carefully mobilized and protected with a vessel loop.
Anterolateral Fasciectomy Technique
Once the nerve was secured, the anterior intermuscular septum, which divides the anterior and lateral compartments, was clearly visualized.
Attention was first directed to the anterior compartment. A longitudinal incision was made in the anterior fascia, approximately one centimeter anterior to the septum. Using long Mayo scissors, the fasciotomy was extended proximally all the way to the tibial tubercle. It is imperative to release the fascia completely to the proximal origin of the tibialis anterior muscle. The release was then extended distally down to the level of the superior extensor retinaculum. Following the complete longitudinal release, a parallel incision was made, and a one-centimeter wide strip of anterior fascia was excised along the entire length of the compartment.
Attention was then turned to the lateral compartment. A longitudinal incision was made in the lateral fascia, approximately one centimeter posterior to the intermuscular septum, remaining strictly posterior to the course of the superficial peroneal nerve. The lateral fascia was released proximally to the level of the fibular head and distally to the lateral malleolus. A similar one-centimeter strip of lateral fascia was excised.
Hemostasis and Closure
Following completion of the bilateral anterolateral fasciectomies, the tourniquets were deflated. This is a crucial step to ensure meticulous hemostasis. The extensive intramuscular capillary beds, which have been compressed by the elevated compartment pressures, often exhibit reactive hyperemia once released. All muscular bleeding points were carefully coagulated using bipolar electrocautery to prevent postoperative hematoma formation, which is a primary cause of excessive scarring and poor outcomes.
The surgical sites were profusely irrigated with sterile saline. The deep fascial layers were explicitly left open. Closure consisted only of reapproximating the subcutaneous tissue with 2-0 absorbable sutures and closing the skin with a running subcuticular 3-0 monofilament suture. Sterile compressive dressings, consisting of non-adherent gauze, fluffs, and an elastic bandage, were applied from the toes to the tibial tubercle. The identical procedure was then performed on the left leg.
Post Operative Protocol and Rehabilitation
The postoperative rehabilitation protocol is meticulously structured to balance the need for soft tissue healing with the prevention of restrictive scar tissue formation. The rehabilitation is divided into three distinct phases.
Phase 1: Immediate Post-Operative Period (Weeks 0 to 2)
The primary goals of the initial phase are wound healing, edema control, and restoration of basic range of motion. The patient was allowed to weight-bear as tolerated immediately post-operatively, utilizing crutches for support only if necessary due to pain. Early weight-bearing is encouraged to promote the calf muscle pump mechanism, which aids in reducing venous stasis and edema.
The patient was instructed to keep the lower extremities elevated above the level of the heart when resting. Active and passive range of motion exercises for the ankle and toes were initiated on postoperative day one. These exercises, particularly active dorsiflexion and plantarflexion, are critical to prevent the muscles from scarring down to the overlying subcutaneous tissues and skin. The compressive dressings were removed at the first postoperative visit at two weeks, at which point the incisions were evaluated, and the subcuticular sutures were trimmed.
Phase 2: Early Rehabilitation and Strengthening (Weeks 2 to 6)
Once the incisions were fully healed, the patient progressed to phase two. The focus shifted toward restoring full lower extremity flexibility, core stability, and initiating low-impact cardiovascular conditioning.
Manual therapy, including soft tissue mobilization and cross-friction massage over the surgical sites, was initiated to ensure the mobility of the skin and subcutaneous tissues over the underlying muscle bellies. The patient began using a stationary bicycle and an elliptical trainer to maintain cardiovascular fitness without subjecting the lower extremities to the repetitive impact of running. Swimming and deep-water running were also incorporated.
Isometric and progressive isotonic strengthening exercises for the anterior and lateral compartments were introduced. Particular emphasis was placed on eccentric strengthening of the tibialis anterior to prepare the muscle for the demands of the heel strike phase of the running gait cycle.
Phase 3: Advanced Rehabilitation and Return to Sport (Weeks 6 to 12)
At six weeks post-operation, assuming the patient was pain-free with activities of daily living and low-impact exercise, a graduated return to running program was initiated.
This phase utilized an anti-gravity treadmill to allow the patient to begin running at a reduced percentage of his body weight, progressively increasing the load as tolerated. The initial running intervals were short, typically alternating one minute of running with four minutes of walking.
Over the subsequent six weeks, the running intervals and intensity were systematically increased, guided by the patient's symptoms. The physical therapy team also conducted a comprehensive biomechanical running analysis to identify and correct any kinematic flaws, such as over-striding or excessive heel strike, which could predispose the patient to future lower extremity injuries. By twelve weeks post-operation, the patient successfully returned to full, unrestricted training, completely free of his previous exertional symptoms, and was cleared for competitive racing.
Clinical Pearls and Pitfalls
The surgical management of Chronic Exertional Compartment Syndrome, while highly successful when executed correctly, is fraught with technical nuances that can dictate the clinical outcome.
Clinical Pearls
