Acute Upper Extremity Compartment Syndrome: A Masterclass in Decompressive Fasciotomy

Key Takeaway
This masterclass guides fellows through acute upper extremity compartment syndrome decompression. We cover detailed surgical anatomy, meticulous patient positioning, and step-by-step intraoperative execution for arm, forearm, hand, and digits. Learn critical neurovascular protection, precise fascial release techniques, and essential pearls for managing this limb-threatening condition, ensuring optimal patient outcomes through comprehensive surgical and postoperative strategies.
Comprehensive Introduction and Patho-Epidemiology
Acute compartment syndrome (ACS) of the upper extremity represents one of the most time-sensitive, limb-threatening emergencies encountered in the practice of orthopedic surgery. It is a devastating condition characterized by a critical elevation of interstitial tissue pressure within a closed and unyielding osteofascial envelope. This pathological pressure surge rapidly compromises the microcirculation, leading to a cascade of ischemia, anoxia, and, if left surgically unaddressed, irreversible myoneural necrosis. The ultimate sequela of missed or delayed diagnosis is Volkmann’s ischemic contracture—a catastrophic, fibrotic, and functionally devastating end-stage limb deformity that serves as a grim testament to surgical hesitancy.
The pathophysiological mechanism of acute compartment syndrome is fundamentally a vicious cycle of ischemia and edema. The precipitating insult—whether a high-energy crush injury, a displaced both-bone forearm fracture, circumferential thermal burns, or even an iatrogenic reperfusion injury following vascular repair—initiates local tissue trauma. This trauma induces a localized inflammatory response, drastically increasing capillary permeability. As intravascular fluid third-spaces into the interstitial compartment, the volume within the fixed fascial boundaries expands. Because the fascia possesses negligible compliance, this volume increase translates directly into an exponential rise in intracompartmental pressure (ICP).
When the ICP surpasses the capillary perfusion pressure (typically around 30 mm Hg), the thin-walled venules collapse. This venous outflow obstruction further exacerbates the interstitial edema, propelling the pressure even higher until it overcomes the precapillary arteriolar pressure. At this critical juncture, arterial inflow ceases, plunging the enclosed musculature and neural structures into profound ischemia. Skeletal muscle can tolerate ischemia for approximately four hours before irreversible mitochondrial damage and cellular death commence; peripheral nerves are even more sensitive, with functional impairment manifesting within 30 minutes and permanent axonal death occurring by 12 hours.
Epidemiologically, acute compartment syndrome of the upper extremity is most frequently observed in young adult males, correlating heavily with high-energy trauma mechanisms. Diaphyseal fractures of the radius and ulna, supracondylar humerus fractures in the pediatric population, and severe crush injuries to the forearm and hand are the most common culprits. However, the orthopedic surgeon must maintain a high index of suspicion in non-traumatic etiologies as well, including bleeding diatheses, constrictive casts or dressings, extravasation of intravenous fluids or vesicants, and prolonged limb compression in the obtunded patient. Recognizing the insidious onset of this ischemic cascade and intervening decisively is the hallmark of a master orthopedic surgeon.
Detailed Surgical Anatomy and Biomechanics
A masterful decompressive fasciotomy requires an intimate, three-dimensional understanding of the upper extremity's compartmental anatomy. The surgeon must navigate complex neurovascular planes, ensuring complete release of all involved fascial envelopes while meticulously protecting the critical structures that provide function to the limb. The upper extremity is anatomically partitioned into distinct compartments by robust intermuscular septa and deep investing fascia.
The Arm Compartments
The arm is divided into two primary fascial compartments by the medial and lateral intermuscular septa, which extend from the deep investing fascia to the supracondylar ridges of the humerus.
The anterior compartment contains the primary flexors of the elbow: the biceps brachii, brachialis, and coracobrachialis. Crucially, it also houses the brachial artery, the median nerve, and the musculocutaneous nerve. The posterior compartment contains the triceps brachii muscle.
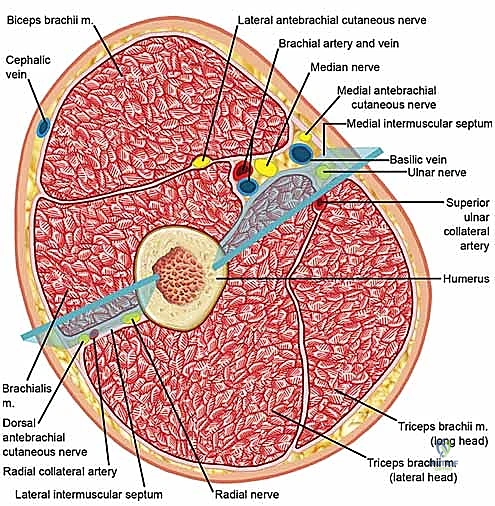
When decompressing the arm, the surgeon must be acutely aware of the radial nerve's trajectory. It courses from the posterior compartment, spirals around the posterior humerus in the radial groove, and pierces the lateral intermuscular septum approximately 10 cm proximal to the lateral epicondyle to enter the anterior compartment. Iatrogenic injury to the radial nerve during lateral septal release is a known and devastating complication.
The Forearm Compartments
The forearm is anatomically dense and biomechanically complex, traditionally divided into three primary compartments, though clinical reality often dictates treating the superficial and deep volar compartments as functionally distinct entities during decompression.
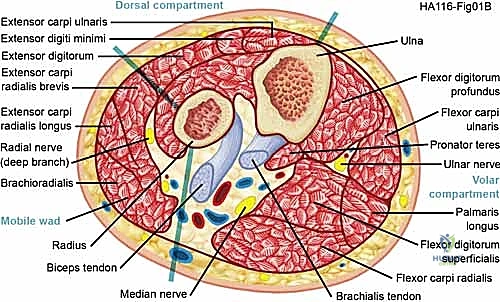
The volar (flexor) compartment is the most frequently involved in ACS. It is subdivided into a superficial layer (pronator teres, flexor carpi radialis, palmaris longus, flexor carpi ulnaris) and a deep layer (flexor digitorum superficialis, flexor digitorum profundus, flexor pollicis longus). The median nerve travels between the FDS and FDP, making it highly vulnerable to ischemic compression. The ulnar nerve and artery course deep to the FCU.
The dorsal (extensor) compartment contains the superficial extensors (extensor digitorum communis, extensor digiti minimi, extensor carpi ulnaris) and the deep extensors (supinator, abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, extensor indicis). The mobile wad of Henry (brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis) is often considered a distinct lateral compartment. Decompression of the dorsal and mobile wad compartments requires vigilance to protect the superficial sensory branch of the radial nerve and the posterior interosseous nerve (PIN) as it dives beneath the arcade of Frohse.
The Hand and Digit Compartments
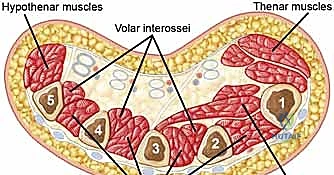
The hand comprises ten distinct, tightly enclosed fascial compartments. These include four dorsal interosseous compartments, three volar interosseous compartments, the thenar compartment, the hypothenar compartment, and the adductor pollicis compartment.

The carpal tunnel, while technically not a muscle compartment, is a critical closed space at the wrist that must be released during volar forearm decompression to prevent median nerve strangulation. In the digits, the fascial anatomy is defined by Cleland’s and Grayson’s ligaments, which compartmentalize the volar and dorsal aspects of the fingers. The limited compliance of the digital skin means that even minor fluid accumulation can lead to digital ischemia, necessitating prompt mid-axial release.
Exhaustive Indications and Contraindications
The diagnosis of acute compartment syndrome is primarily clinical, demanding an astute orthopedic evaluation. The classic "6 Ps" (Pain, Pallor, Paresthesias, Pulselessness, Paralysis, and Poikilothermia) are often taught, but relying on them in totality is a dangerous pitfall. Pallor, pulselessness, and paralysis are late, ominous signs indicating that irreversible ischemic necrosis has likely already occurred. The earliest and most reliable clinical indicator is pain out of proportion to the apparent injury.

Upon physical examination, the affected compartments will be palpably tense, swollen, and unyielding—often described as having a "wood-like" consistency.

Passive stretch of the muscles within the involved compartment will elicit excruciating pain. For example, passive extension of the digits will cause severe pain in the volar forearm. In patients who are obtunded, intubated, or possess an unreliable clinical exam (e.g., concomitant traumatic brain injury or spinal cord injury), objective intracompartmental pressure (ICP) monitoring is mandatory. The concept of "delta pressure" (Diastolic Blood Pressure minus Intracompartmental Pressure) is the gold standard metric. A delta pressure of less than 30 mm Hg is an absolute indication for immediate decompressive fasciotomy.
| Indication / Contraindication | Clinical Scenario & Rationale |
|---|---|
| Absolute Indication | Delta pressure (Diastolic BP - ICP) < 30 mm Hg in any patient, regardless of clinical exam. |
| Absolute Indication | Tense, "wood-like" compartment with pain out of proportion and severe pain on passive stretch in an awake, alert patient. |
| Absolute Indication | Prophylactic decompression during repair of a major arterial injury with prolonged warm ischemia time (>4-6 hours). |
| Relative Indication | Rising ICP trend in a borderline patient (e.g., Delta pressure 35 mm Hg but trending downward over 2 hours). |
| Absolute Contraindication | Missed compartment syndrome presenting late (>48-72 hours) with established, irreversible myonecrosis and absent motor/sensory function. Fasciotomy here drastically increases the risk of fatal systemic infection and does not restore function; amputation or delayed contracture release is indicated. |
| Relative Contraindication | Uncorrected severe coagulopathy, though this must be weighed against the certainty of limb loss; correction should occur concurrently with surgery. |
Pre-Operative Planning, Templating, and Patient Positioning
Once the decision to proceed with decompressive fasciotomy is made, execution must be rapid and coordinated. Pre-operative planning is minimal but critical. The surgeon must obtain informed consent that explicitly includes the likelihood of large, open wounds, the necessity for multiple subsequent surgeries for wound closure or skin grafting, and the potential for permanent functional deficits despite surgical intervention.
The patient is positioned supine on the operating table with the affected upper extremity extended on a radiolucent hand board. A sterile tourniquet is applied high on the arm. The use of a tourniquet in the setting of compartment syndrome is highly controversial. While it provides a bloodless field for rapid, safe dissection—especially when navigating the median nerve and brachial artery in a traumatized, anatomically distorted forearm—it also exacerbates the ischemic insult to already dying muscle. If utilized, the tourniquet should be inflated only for the most critical portions of the neurovascular dissection and must be deflated prior to assessing muscle viability and performing epimysiotomies. Many purists advocate for a completely tourniquet-less procedure to allow real-time evaluation of tissue perfusion.
Standard prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered. If concomitant fractures are present, the fluoroscopy (C-arm) unit must be positioned appropriately. The surgical plan must account for both the decompression and the subsequent skeletal stabilization, as restoring length and alignment is crucial for reducing secondary compartmental volume restriction.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of an upper extremity fasciotomy must be exhaustive. A "mini-open" or limited incision is a gross violation of surgical principles in this setting; the skin itself acts as a restrictive envelope and must be widely released.
Volar Forearm Decompression
The volar approach is the cornerstone of forearm decompression. A curvilinear incision is utilized to prevent linear scar contracture across the flexion creases. The incision begins just proximal to the medial epicondyle, courses distally and radially across the antecubital fossa, extends longitudinally down the mid-volar forearm, and then curves ulnarly at the wrist to cross the wrist crease obliquely, terminating in the palm along the thenar crease.
The dissection proceeds through the subcutaneous tissues, taking meticulous care to identify and protect the palmar cutaneous branch of the median nerve at the wrist and the medial antebrachial cutaneous nerve proximally. The deep investing fascia of the superficial volar compartment is incised longitudinally.
Crucially, the surgeon must decompress the deep volar compartment. This is achieved by retracting the flexor carpi radialis radially and the flexor digitorum superficialis ulnarly, exposing the deep fascia overlying the flexor digitorum profundus and flexor pollicis longus. This deep fascia is incised entirely.
At the wrist, a formal carpal tunnel release is mandatory. The transverse carpal ligament is divided completely to decompress the median nerve. Proximally, the lacertus fibrosus (bicipital aponeurosis) must be divided to decompress the brachial artery and median nerve in the antecubital fossa. Any muscle bellies that appear pale, dusky, or non-contractile should undergo epimysiotomy (incising the epimysium directly) to further relieve localized pressure.
Dorsal Forearm Decompression
While the volar incision decompresses a significant volume, a dorsal release is frequently required, especially in severe trauma or when dorsal compartment pressures remain elevated. A straight longitudinal incision is made from the lateral epicondyle to the midline of the distal radioulnar joint.

The subcutaneous tissues are divided, protecting the superficial sensory branch of the radial nerve. The extensor retinaculum is preserved if possible to prevent bowstringing of the extensor tendons, but the fascial compartments between the extensor digitorum communis and the mobile wad are widely opened.

Hand and Digit Decompression
Decompression of the hand requires releasing the interosseous, thenar, and hypothenar compartments. Two longitudinal dorsal incisions are typically utilized: one centered over the second metacarpal (to access the first and second dorsal interossei) and one over the fourth metacarpal (to access the third and fourth dorsal interossei).
Blunt dissection is carried down alongside the metacarpal shafts to decompress the volar interossei and the adductor pollicis. The thenar and hypothenar compartments can be decompressed via separate small longitudinal incisions on the radial and ulnar borders of the hand, respectively.
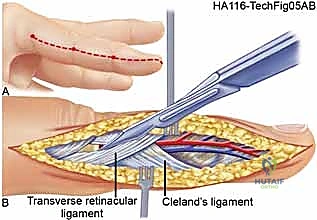
For the digits, mid-axial incisions are placed on the non-contact borders (ulnar border of the index and middle fingers; radial border of the ring and small fingers).

The incision is carried down through the skin and subcutaneous tissue.
The dissection must divide Cleland's and Grayson's ligaments to fully decompress the digital compartments while carefully protecting the neurovascular bundles lying volar to the mid-axial line.

Concomitant Fracture Fixation
If the compartment syndrome is secondary to a fracture (e.g., both-bone forearm fracture), the fracture must be stabilized during the same surgical setting, immediately following the fascial decompression. Rigid internal fixation (plate osteosynthesis) is preferred as it restores the skeletal length, thereby maximizing the volume of the fascial envelope and preventing secondary pressure spikes. External fixation is an alternative in highly contaminated or severely comminuted injuries where internal hardware poses an unacceptable infection risk.
Complications, Incidence Rates, and Salvage Management
Despite aggressive and timely surgical intervention, the morbidity associated with acute compartment syndrome and its treatment remains substantial. The most feared complication is the failure to adequately decompress the limb, leading to Volkmann's ischemic contracture. Iatrogenic injuries during the fasciotomy itself, particularly to the cutaneous nerves (palmar cutaneous branch of the median nerve, superficial radial nerve) or major neurovascular bundles, are also significant risks.
The massive, open wounds created by fasciotomies present their own set of challenges. Desiccation of exposed tendons and neurovascular structures can lead to secondary necrosis. Nosocomial infections are a constant threat, given the compromised local tissue perfusion and large surface area of the open wound.
| Complication | Estimated Incidence | Prevention & Salvage Management |
|---|---|---|
| Volkmann’s Ischemic Contracture | 1-10% (Highly dependent on time to surgery) | Prevention: Early recognition, continuous ICP monitoring, thorough and complete multiseptal decompression. Salvage: Late management involves complex reconstructive procedures including infarct excision, neurolysis, tendon transfers, and free functional muscle flaps (e.g., gracilis flap). |
| Iatrogenic Nerve Injury | 5-15% | Prevention: Meticulous surgical technique, precise anatomical knowledge, avoiding blind fascial cuts, visual identification of the superficial radial and palmar cutaneous median nerves. Salvage: Primary microscopic neurorrhaphy if recognized intraoperatively; delayed nerve grafting or tendon transfers if recognized late. |
| Deep Tissue Infection / Myonecrosis | 5-20% | Prevention: Aggressive initial debridement of frankly necrotic muscle (the "4 Cs": color, consistency, contractility, capacity to bleed), sterile post-operative dressings (NPWT). Salvage: Serial aggressive surgical debridements, targeted intravenous antibiotics, potential amputation if overwhelming sepsis ensues. |
| Delayed Wound Closure / Need for STSG | 50-80% | Prevention: Vessel loop "shoelace" technique to provide continuous, gentle dynamic traction on the skin margins during the post-operative period. Salvage: Split-thickness skin grafting (STSG) over healthy granulation tissue once edema subsides (typically 7-14 days). |
Phased Post-Operative Rehabilitation Protocols
The immediate post-operative management of the fasciotomy wound is critical to preserving limb function and setting the stage for eventual closure. The wounds are absolutely never closed primarily at the index operation. Instead, they are managed with sterile, non-adherent dressings or, preferably, Negative Pressure Wound Therapy (NPWT / Wound VAC). NPWT at -75 to -125 mm Hg continuous pressure helps manage the copious exudate, reduces interstitial edema, and promotes robust granulation tissue formation.
Alternatively, the vessel loop "shoelace" technique can be employed. Silastic vessel loops are woven through skin staples placed along the wound edges, providing gentle, dynamic, continuous traction. This prevents skin retraction and significantly increases the rate of delayed primary closure.
The patient is returned to the operating room at 48 to 72 hours for a "second look" procedure. At this time, any further necrotic muscle is sharply debrided. If the swelling has subsided sufficiently, delayed primary closure may be attempted. If the wound remains under tension, the NPWT or shoelace technique is reapplied. Most large forearm fasciotomies will ultimately require a split-thickness skin graft (STSG) for definitive closure.
Rehabilitation begins immediately post-operatively. The limb is elevated continuously to facilitate venous and lymphatic drainage. The hand and wrist are splinted in a functional position (wrist in 30 degrees of extension, metacarpophalangeal joints in 70-90 degrees of flexion, interphalangeal joints in full extension) to prevent contractures of the collateral ligaments. As soon as the patient's pain allows, aggressive passive and active range of motion exercises of the digits, wrist, and elbow are initiated under the strict guidance of a certified hand therapist. This early mobilization is paramount to prevent tendon adhesions within the scarred fascial beds.
Summary of Landmark Literature and Clinical Guidelines
The modern understanding and management of acute compartment syndrome are built upon the foundational work of several orthopedic pioneers.
Whitesides et al. revolutionized the diagnostic approach by introducing the concept of the delta pressure. Their landmark studies demonstrated that absolute compartment pressure is less critical than the perfusion pressure gradient. They established that a delta pressure (Diastolic BP - ICP) of less than 30 mm Hg represents the critical threshold at which muscle ischemia occurs, shifting the paradigm away from absolute numbers and accounting for the patient's systemic hemodynamic status.
Mubarak and Hargens contributed extensively to the understanding of the pathophysiology and the development of continuous intracompartmental pressure monitoring techniques. Their work clarified the role of the slit catheter in providing accurate, reproducible pressure readings and standardized the thresholds for intervention, particularly in the pediatric population where clinical diagnosis is notoriously difficult.
McQueen and Court-Brown further validated the importance of continuous pressure monitoring, particularly in high-risk tibial and forearm diaphyseal fractures. Their prospective data reinforced that continuous monitoring significantly reduces the time to fasciotomy and virtually eliminates the incidence of missed compartment syndrome and subsequent severe sequelae.
Current clinical guidelines from major orthopedic bodies (AAOS, OTA) universally mandate a high index of suspicion, emphasize the unreliability of late clinical signs (pallor, pulselessness), and strongly advocate for the use of delta pressure monitoring in any patient with an equivocal clinical exam or an inability to reliably communicate pain. The prevailing dogma remains absolute: when in doubt, decompress. The morbidity of an unnecessary fasciotomy is negligible compared to the catastrophic, lifelong disability of a missed acute compartment syndrome.
