Acute Leg Compartment Syndrome Fasciotomy: An Intraoperative Masterclass

Key Takeaway
Acute compartment syndrome is an orthopedic emergency requiring immediate fasciotomy. This masterclass details comprehensive leg anatomy, critical diagnostic criteria, precise dual-incision surgical techniques, intraoperative pearls to prevent complications, and essential postoperative management for optimal patient outcomes. Early intervention is paramount to limb and life salvage, making a thorough understanding of this procedure crucial for every orthopedic surgeon.
Comprehensive Introduction and Patho-Epidemiology
Acute Compartment Syndrome (ACS) of the lower extremity represents one of the most time-sensitive and potentially devastating orthopedic emergencies encountered in clinical practice. The clinical sequelae and medicolegal implications of a missed or delayed diagnosis make it a critical entity that demands absolute mastery from every orthopedic surgeon. This is not merely a soft-tissue procedure; it is a race against the clock to preserve limb viability, optimize functional outcomes, and potentially save the patient's life from the catastrophic systemic effects of massive myonecrosis. In this masterclass, we will meticulously dissect every step of the process, from the foundational pathophysiology to the precise surgical execution of a four-compartment fasciotomy.
Compartment syndrome manifests when the interstitial pressure within a closed, unyielding osteofascial compartment rises to a level that exceeds capillary perfusion pressure. This critical pressure threshold disrupts the microvascular circulation, leading to a profound decrease in oxygen diffusion to the tissues. The ensuing cellular hypoxia triggers a cascade of anaerobic metabolism, lactic acidosis, and ultimately, irreversible cellular anoxia and myonecrosis. The foundational premise of this syndrome relies on either a critical decrease in the space available within the fixed compartment or a pathological increase in the volume of the tissues confined within it. The thick, impermeable fascia of the lower leg prevents fluid extravasation and precludes any compensatory volume expansion that might otherwise mitigate the rising intracompartmental pressure.
Pathological increases in tissue volume are most frequently driven by hemorrhage into the compartment. This is classically associated with high-energy tibial fractures, which remain the most common etiology of ACS. Epidemiological data suggests that up to 9.1% of all tibial plateau fractures and a significant proportion of diaphyseal tibia fractures will develop compartment syndrome. Furthermore, increased capillary permeability secondary to ischemia-reperfusion injury, extensive burns, crush injuries, snake envenomation, or aggressive intravenous fluid resuscitation can precipitate massive third-spacing within the fascial envelopes. Conversely, a decrease in compartment size is typically iatrogenic or environmental, resulting from constrictive circumferential casts, tight dressings, eschar formation in circumferential burns, or prolonged localized external pressure, such as the dependent "well leg" in the lithotomy position during prolonged pelvic or femoral procedures.
The timeline of ischemia is unforgiving. The deleterious effects on neuromuscular function are strictly time-dependent, and prolonged delays correlate directly with catastrophic functional deficits. Peripheral nerves are exquisitely sensitive to ischemia; altered nerve function and paresthesias can manifest after merely two hours of compromised perfusion, with irreversible axonal damage occurring in as little as six hours. Skeletal muscle exhibits slightly more resilience but will suffer irreversible necrosis after eight hours of sustained critical ischemia. Consequently, a six-hour window from the onset of ischemia is universally accepted as the absolute upper limit to guarantee optimal limb salvage and functional recovery. Beyond the localized devastation, the systemic consequences of massive muscle necrosis are profound. The release of myoglobin, intracellular potassium, and acidic metabolites into the systemic circulation precipitates myoglobinuric acute renal failure, life-threatening hyperkalemic cardiac arrhythmias, and severe metabolic acidosis, which can culminate in patient mortality if not aggressively managed.
Detailed Surgical Anatomy and Biomechanics
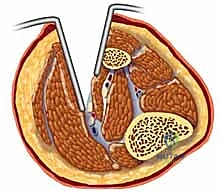
Before a scalpel ever touches the skin, a profound three-dimensional understanding of the lower leg's surgical anatomy is paramount. The lower leg is partitioned into four distinct osteofascial compartments by dense, inelastic fascial septa. A complete and effective fasciotomy mandates the meticulous and complete release of all four compartments. A missed compartment is, by definition, a failed fasciotomy, leading to guaranteed necrosis of the unreleased musculature.
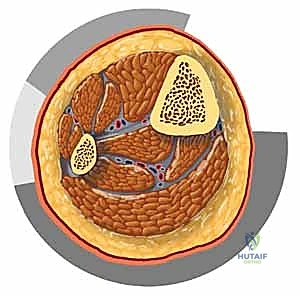
The Anterior Compartment
The anterior compartment is the most frequently involved compartment in lower extremity ACS due to its rigid boundaries and susceptibility to direct trauma. It is bounded anteriorly by the deep crural fascia, laterally by the anterior intermuscular septum, posteriorly by the interosseous membrane, and medially by the lateral surface of the tibia. This compartment houses the primary dorsiflexors of the foot and ankle: the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and peroneus tertius.
The critical neurovascular structures within this space are the deep peroneal nerve and the anterior tibial artery. The deep peroneal nerve courses around the fibular neck, pierces the anterior intermuscular septum, and travels distally, providing motor innervation to the compartment and sensory innervation to the first dorsal web space. The anterior tibial artery runs intimately with the deep peroneal nerve along the anterior aspect of the interosseous membrane. During an anterolateral fasciotomy, these structures are at significant risk if the fascial release is performed blindly or if the scissors plunge excessively deep into the muscle belly.
The Lateral Compartment
The lateral compartment is bordered anteriorly by the anterior intermuscular septum, posteriorly by the posterior intermuscular septum, medially by the lateral surface of the fibula, and laterally by the deep crural fascia. It contains the primary everters of the foot: the peroneus longus and peroneus brevis muscles.
The major neurovascular structure here is the superficial peroneal nerve, which provides motor innervation to the peroneal muscles and sensation to the majority of the dorsum of the foot. Crucially, the superficial peroneal nerve pierces the deep fascia to become subcutaneous in the distal third of the leg, typically 10 to 12 centimeters proximal to the lateral malleolus. This anatomical transition makes the nerve highly vulnerable to iatrogenic transection during the distal extension of the anterolateral fascial incision. The lateral compartment lacks a major longitudinal artery, relying instead on perforating branches from the peroneal artery.
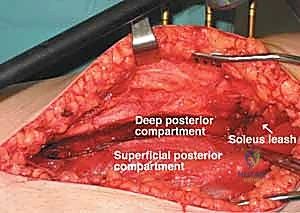
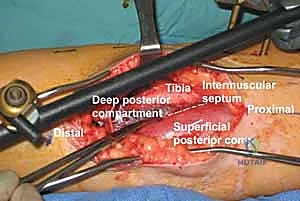
The Deep Posterior Compartment
The deep posterior compartment is the most heavily concealed and technically challenging compartment to adequately decompress. It is bounded anteriorly by the posterior surfaces of the tibia, fibula, and interosseous membrane, and posteriorly by the deep transverse fascial septum, which separates it from the superficial posterior compartment. The musculature includes the flexor digitorum longus, flexor hallucis longus, and the tibialis posterior. It is critical to note that the tibialis posterior muscle often possesses its own distinct fascial envelope, which must be independently identified and released to prevent isolated necrosis.
This compartment houses the master neurovascular bundle of the posterior leg: the tibial nerve and the posterior tibial artery and vein. Furthermore, the peroneal artery and vein travel within this compartment, coursing distally along the medial aspect of the fibula. Incomplete release of the deep posterior compartment, often due to failure to adequately detach the soleal bridge from the posteromedial tibia, is the most common cause of persistent ACS and subsequent deep flexor contractures.
The Superficial Posterior Compartment
The superficial posterior compartment is the largest and most accommodating of the four, bounded anteriorly by the deep transverse fascial septum and posteriorly by the deep investing fascia of the leg. It contains the powerful plantarflexors: the gastrocnemius, soleus, and the vestigial plantaris muscle.
While it lacks a major longitudinal arterial trunk—receiving its blood supply via sural branches from the popliteal artery—it does contain the sural nerve, which travels superficially between the heads of the gastrocnemius. Although generally considered the safest compartment to release, careless medial placement of the posteromedial skin incision can jeopardize the saphenous nerve and the greater saphenous vein.

Exhaustive Indications and Contraindications
The diagnosis of acute compartment syndrome remains primarily clinical. It is an "eyes, hands, and brain" diagnosis that requires a high index of suspicion, continuous serial examinations, and an astute understanding of the patient's injury mechanism. Adjunctive diagnostic modalities, while useful in equivocal cases, must never delay definitive surgical intervention when the clinical picture is clear.
Clinical Diagnostic Criteria
The classic "Six Ps"—Pain, Paresthesias, Pulselessness, Pallor, Paralysis, and Pressure—are heavily taught but notoriously misleading in the acute setting. Relying on the complete presence of these signs guarantees a missed diagnosis and a non-viable limb. Pulselessness and pallor are late, ominous signs indicating complete arterial occlusion, which is rarely the primary driver of early ACS. A patient can suffer from devastating, irreversible compartment syndrome while maintaining perfectly normal, bounding distal pulses. Paralysis is similarly unreliable, as it can be secondary to guarding, primary nerve injury, or the profound pain of the fracture itself.
The most sensitive and earliest clinical indicators are:
1. Pain out of proportion to the apparent injury: This is the hallmark symptom. The patient will exhibit severe, escalating, and unrelenting pain that is refractory to standard opioid analgesia.
2. Pain with passive stretch: Exquisite pain elicited by passive stretching of the muscles within the affected compartment. For the anterior compartment, passive plantarflexion of the toes and ankle will produce agonizing pain.
3. Palpable tenseness: The compartment will feel "wood-like" or rock-hard compared to the contralateral uninjured limb.
4. Paresthesias: Altered sensation in the distribution of the nerves traversing the compartment. Early sensory deficits, such as loss of two-point discrimination in the first dorsal web space (deep peroneal nerve), are critical warning signs.
Objective Pressure Measurement
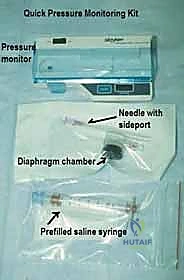
When the clinical examination is equivocal, or when the patient is unable to provide a reliable history (e.g., intubated, comatose, multi-trauma, polytrauma with distracting injuries, or under regional anesthesia), objective intracompartmental pressure (ICP) monitoring is mandatory. The Stryker Intracompartmental Pressure Monitor is the gold standard device.
The absolute pressure reading is less important than the differential pressure, known as the Delta P (ΔP). The Delta P is calculated by subtracting the intracompartmental pressure from the patient's diastolic blood pressure (ΔP = Diastolic BP - ICP). A Delta P of less than 30 mmHg is the universally accepted threshold indicating inadequate capillary perfusion and serves as an absolute indication for emergent fasciotomy.
| Indications for Emergent Fasciotomy | Contraindications (Relative and Absolute) |
|---|---|
| Absolute: Clinical diagnosis of ACS (pain out of proportion, pain on passive stretch, tense compartments). | Absolute: Missed ACS with established, irreversible muscle necrosis (>24-48 hours). Fasciotomy here increases infection risk without functional benefit; amputation is often required. |
| Absolute: Delta P (Diastolic BP - ICP) < 30 mmHg in any compartment. | Relative: Overlying severe soft tissue infection or cellulitis (requires careful planning and broad-spectrum antibiotics). |
| Absolute: Absolute ICP > 30-40 mmHg in a normotensive patient (though Delta P is preferred). | Relative: Uncorrected severe coagulopathy (must be corrected concurrently with surgical intervention). |
| Relative: High-risk multi-trauma patient with a tense leg who cannot be serially examined. | Relative: Terminal patient where limb salvage does not align with overall goals of care. |
| Relative: Prophylactic release during revascularization of an ischemic limb (>4-6 hours of ischemia). |

Pre-Operative Planning, Templating, and Patient Positioning
Once the decision to proceed with fasciotomy is made, execution must be swift and highly organized. Delaying the operation for extensive preoperative imaging (such as CT or MRI) is strictly contraindicated. The operating room team must be briefed on the emergent nature of the procedure.
Patient Preparation and Anesthesia
The patient is taken emergently to the operating theater. General anesthesia is typically preferred, as regional anesthesia (spinal or epidural) can cause sympathectomy, dropping the diastolic blood pressure and further compromising the Delta P, exacerbating the ischemic cascade. Furthermore, regional anesthesia masks the immediate postoperative pain, making it difficult to assess for missed compartments or evolving pathology in adjacent limbs.
Broad-spectrum intravenous antibiotics (typically a first-generation cephalosporin, or broader coverage if open fractures or gross contamination are present) must be administered prior to incision. Blood products should be available, as releasing tense compartments can lead to significant acute blood loss.
Positioning and Equipment
The patient is positioned supine on a radiolucent operating table. A bump (rolled blanket or sandbag) is placed under the ipsilateral greater trochanter to internally rotate the leg, bringing the lateral aspect of the tibia into a neutral, easily accessible position. This is crucial for the anterolateral incision. The entire lower extremity, from the toes to the proximal thigh, is prepped and draped in a standard sterile fashion. A sterile tourniquet may be placed on the proximal thigh but should not be inflated unless catastrophic, uncontrollable hemorrhage is encountered. Inflating a tourniquet exacerbates the ischemia and defeats the physiological purpose of the fasciotomy.
Essential equipment includes:
* Standard orthopedic soft tissue tray.
* Long Metzenbaum scissors or a specialized fasciotome.
* Vessel loops (for vessel identification and retraction).
* Negative Pressure Wound Therapy (NPWT / Wound VAC) supplies for immediate postoperative coverage.
* Electrocautery for meticulous hemostasis.
Step-by-Step Surgical Approach and Fixation Technique
The gold standard for comprehensive decompression of the lower leg is the two-incision, four-compartment fasciotomy. While single-incision techniques exist, they carry a significantly higher risk of incomplete release and iatrogenic neurovascular injury, and are generally discouraged in the acute trauma setting.
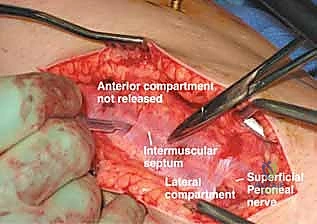
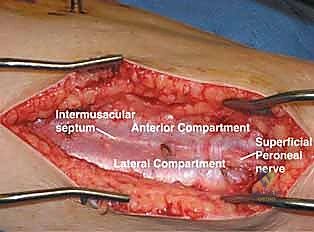
The Anterolateral Approach (Incision 1)
The anterolateral incision is designed to decompress both the anterior and lateral compartments.
- Skin Incision: The incision is centered longitudinally over the anterolateral aspect of the leg. It begins approximately 2 to 3 centimeters lateral to the tibial crest, starting proximally at the level of the tibial tubercle (just distal to Gerdy's tubercle) and extending distally to approximately 5 centimeters proximal to the lateral malleolus. The incision must be generous; inadequate skin incisions can act as a secondary constricting envelope, negating the fascial release.
-
Identifying the Septum: Subcutaneous dissection is performed sharply. The deep crural fascia is exposed. The critical landmark here is the anterior intermuscular septum, which separates the anterior and lateral compartments. This can often be identified by a visible fat stripe or by palpating the fascial depression between the tibialis anterior and the peroneal musculature.
-
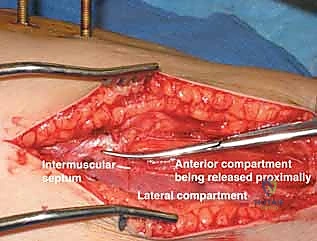
The "H" Cut: To ensure accurate entry into both compartments, a transverse incision is made through the deep fascia across the anterior intermuscular septum, creating an "H" or a cross. This visually confirms the location of the septum and prevents the disastrous error of entering the same compartment twice.
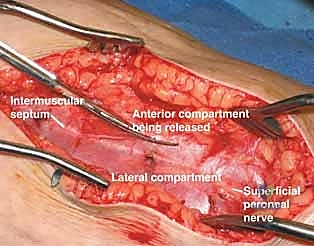
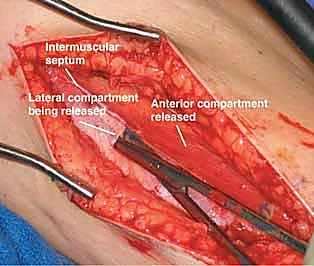
- Releasing the Anterior Compartment: From the transverse cut, long Metzenbaum scissors are introduced into the anterior compartment. The scissors are pushed proximally toward the tibial plateau and distally toward the ankle, keeping the blades slightly open and angled upward against the deep surface of the fascia to avoid plunging into the muscle belly and injuring the deep peroneal nerve or anterior tibial artery. The fascia is incised completely along the entire length of the compartment.
- Releasing the Lateral Compartment: The scissors are then redirected into the lateral compartment from the initial transverse cut. The proximal release is straightforward. During the distal release, extreme caution must be exercised. The superficial peroneal nerve exits the deep fascia to become subcutaneous in the distal third of the leg. The nerve must be visually identified and protected. The fascial release should be directed slightly posterior to the fibula in the distal aspect to safely bypass the nerve.
The Posteromedial Approach (Incision 2)
The posteromedial incision dictates the release of the superficial and, most importantly, the deep posterior compartments.
- Skin Incision: The leg is externally rotated (the hip bump may be removed). The incision begins proximally at the level of the tibial tubercle and extends distally to the level of the medial malleolus. It is placed strictly 2 centimeters posterior to the palpable posteromedial border of the tibia. Placing this incision too anteriorly risks exposing the tibial bone, leading to desiccation and osteomyelitis. Placing it too posteriorly risks injury to the greater saphenous vein and saphenous nerve.
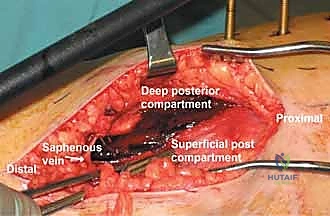
- Protecting Superficial Structures: Careful subcutaneous dissection is performed to identify and retract the greater saphenous vein and saphenous nerve anteriorly.

- Releasing the Superficial Posterior Compartment: The deep fascia enveloping the gastrocnemius and soleus is identified and incised longitudinally. Metzenbaum scissors are used to extend this release proximally and distally along the entire length of the muscle bellies.
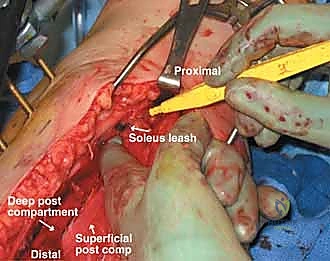
- Releasing the Deep Posterior Compartment: This is the most technically demanding step. The superficial posterior muscles (gastrocnemius and soleus) are retracted posteriorly. The surgeon must identify the fascial bridge connecting the soleus to the posteromedial border of the tibia. This soleal bridge must be sharply taken down or bluntly swept off the tibia to expose the deep transverse fascia covering the flexor digitorum longus and tibialis posterior.
- Complete Deep Decompression: Once the deep transverse fascia is exposed, it is incised longitudinally. The release must extend distally to the ankle and proximally up to the origin of the soleus. The surgeon must verify that the tibialis posterior muscle is fully decompressed, as it often lies within its own sub-compartment. The neurovascular bundle (tibial nerve, posterior tibial vessels) lies immediately superficial to the tibialis posterior and must be meticulously protected during this deep fascial release.
Muscle Viability Assessment
Following complete decompression, the musculature must be assessed for viability using the "Four Cs":
* Color: Healthy muscle is beefy red; necrotic muscle is pale, grey, or dark purple.
* Consistency: Healthy muscle is firm and resilient; necrotic muscle is mushy and friable.
* Contractility: Healthy muscle twitches when stimulated with electrocautery or forceps.
* Capacity to Bleed: Healthy muscle bleeds briskly when cut.
Frankly necrotic muscle must be aggressively debrided to prevent overwhelming sepsis and myoglobinuric renal failure. However, in the acute setting immediately following decompression, borderline muscle should be left in situ and re-evaluated during a planned second-look operation 48 to 72 hours later, as reperfusion can salvage stunned tissue.

Complications, Incidence Rates, and Salvage Management
Despite flawless surgical technique, the nature of acute compartment syndrome inherently carries a high risk of complications. The most devastating complication is a missed or incomplete fasciotomy, which guarantees irreversible myonecrosis, severe contractures (such as the classic equinovarus deformity from deep posterior necrosis), and frequent progression to amputation.
| Complication | Incidence Rate | Pathophysiology & Salvage Management |
|---|---|---|
| Incomplete Fasciotomy / Missed Compartment | 5 - 15% | Usually involves the deep posterior compartment. Leads to irreversible necrosis. Salvage requires immediate re-operation, radical debridement of dead muscle, and often results in permanent foot drop or equinus contracture requiring late tendon transfers or arthrodesis. |
| Iatrogenic Nerve Injury | 2 - 10% | Superficial peroneal nerve (anterolateral incision) and saphenous nerve (posteromedial incision) are most at risk. Results in painful neuromas and sensory deficits. Management involves careful intraoperative protection; if severed, primary repair or burying the stump into muscle is required. |
| Wound Infection / Osteomyelitis | 10 - 20% | Open fasciotomy wounds are highly susceptible to nosocomial colonization. Exposed tibia (from a poorly placed medial incision) desiccates and becomes infected. Management dictates meticulous local wound care, NPWT, aggressive debridement, and culture-directed intravenous antibiotics. |
| Myoglobinuric Renal Failure | 5 - 30% (in delayed cases) | Massive myonecrosis releases myoglobin, precipitating in renal tubules. Requires aggressive IV fluid hydration, alkalinization of urine (sodium bicarbonate), and potentially emergent hemodialysis. |
| Chronic Venous Insufficiency | 15 - 40% | Destruction of the fascial pump mechanism impairs venous return. Patients suffer from chronic dependent edema and skin changes. Managed conservatively with lifelong compression stockings and elevation. |

If a patient presents with a "missed" compartment syndrome—typically defined as a presentation greater than 24 to 48 hours after the onset of ischemia, with clinically dead, silent compartments and absent motor function—the decision-making paradigm shifts drastically. Performing a fasciotomy in this late stage does not restore muscle function; rather, it introduces hospital-acquired pathogens into a bed of necrotic tissue, almost ensuring a catastrophic, limb-threatening infection. In these tragic scenarios, the standard of care is to allow the limb to declare itself. The patient is monitored closely for systemic toxicity (renal failure, sepsis). If systemic
Clinical & Radiographic Imaging Archive




