Mastering Fasciotomy for Chronic Exertional Compartment Syndrome: An Intraoperative Guide

Key Takeaway
This masterclass provides an exhaustive, real-time guide to fasciotomy for Chronic Exertional Compartment Syndrome (CECS). Fellows will learn critical surgical anatomy, meticulous preoperative planning, and granular, step-by-step intraoperative techniques for single, dual, and perifibular approaches. We'll cover instrument use, precise dissections, neurovascular protection, and crucial pearls to avoid pitfalls. Postoperative rehabilitation and complication management are also detailed for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Chronic Exertional Compartment Syndrome (CECS) represents a fascinating, complex, and often debilitating condition that frequently perplexes both clinicians and patients. Unlike its acute counterpart, which is typically precipitated by high-energy trauma or fractures and demands emergent surgical intervention to prevent irreversible myonecrosis, CECS is a reversible, exercise-induced phenomenon. It predominantly afflicts a specific demographic: highly active individuals, competitive athletes, and military personnel. The hallmark of this syndrome is a predictable, exertion-induced escalation of pain, accompanied by paresthesias, numbness, and subjective weakness, all of which rapidly abate upon cessation of the offending activity. This transient but recurrent elevation in intramuscular pressure compromises local microvascular perfusion, leading to a state of exertional ischemia that severely limits athletic performance and occupational readiness.
The underlying pathophysiologic mechanisms driving CECS, while not entirely elucidated, are widely accepted to be multifactorial, centering on the fundamental principles of fascial compliance and fluid dynamics. During strenuous exercise, skeletal muscle volume can physiologically expand by up to 20% due to increased capillary hydrostatic pressure, hyperemia, and the accumulation of osmotic metabolites within the interstitial space. In a normal physiologic state, the surrounding fascial envelope accommodates this expansion. However, in patients with CECS, it is postulated that the fascial envelope is uniquely non-compliant or pathologically thickened. This rigid anatomical boundary prevents adequate volumetric expansion, leading to an exponential rise in intracompartmental pressure. When this pressure surpasses the capillary perfusion pressure—typically around 20 to 30 mm Hg—microvascular blood flow is critically impeded, initiating a cascade of tissue hypoxia, anaerobic metabolism, and the accumulation of pain-inducing neuropeptides and lactic acid.
Epidemiologically, the incidence of CECS is frequently underestimated, largely due to its transient nature and the overlap of its symptoms with other common exertion-related leg pathologies, such as medial tibial stress syndrome (MTSS) or stress fractures. Contemporary literature suggests a prevalence of up to 14% among individuals presenting to sports medicine clinics with chronic lower leg pain. Interestingly, the condition demonstrates a near-equal predilection for both males and females, though the specific athletic pursuits often differ, with high-impact running, soccer, and military marching being the most common triggers. Furthermore, CECS is remarkably bilateral in its presentation, affecting both lower extremities in up to 70% to 80% of documented cases. While the lower leg is unequivocally the most common anatomical site, rare but well-documented case reports exist detailing CECS in the volar forearm of elite rowers and motorcyclists, the thigh, and even the paraspinal musculature.
The diagnostic journey for a patient with CECS is often protracted, marked by months or even years of misdiagnoses, failed conservative modalities, and significant psychological frustration. It remains a diagnosis of exclusion, heavily reliant on a meticulous clinical history and the definitive confirmation via dynamic intracompartmental pressure measurements. The economic and career impacts are substantial, particularly within military cohorts where the inability to perform load-bearing marches can result in medical discharge. As orthopedic surgeons, our imperative is to recognize the classic clinical presentation, execute precise diagnostic protocols, and, when non-operative measures inevitably fail, perform a meticulously planned and executed fasciotomy. A thorough understanding of the patho-epidemiology is the foundational first step in mastering the surgical management of this challenging syndrome.
Detailed Surgical Anatomy and Biomechanics
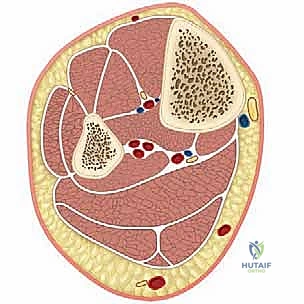
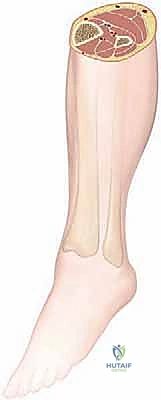
A profound, three-dimensional understanding of the surgical anatomy of the lower extremity is the sine qua non of successful CECS management. The leg is anatomically partitioned into four primary compartments—anterior, lateral, superficial posterior, and deep posterior—each delineated by robust, unyielding fascial septa and osseous boundaries. The biomechanical interplay between these muscular compartments and their investing fascia is critical for normal venous return, acting as a functional musculovenous pump during ambulation. However, in the context of CECS, these rigid boundaries become the primary source of pathology.
The Anterior and Lateral Compartments
The anterior compartment is the most frequently implicated anatomical space in CECS. Its boundaries consist of the lateral surface of the tibia medially, the medial surface of the fibula laterally, the interosseous membrane posteriorly, and the crural fascia anteriorly. It houses the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and peroneus tertius muscles. From a neurovascular standpoint, this compartment is perilous; it contains the deep peroneal nerve and the anterior tibial artery and veins. The deep peroneal nerve courses deep to the extensor digitorum longus and supplies motor innervation to the dorsiflexors before providing critical sensory innervation to the first dorsal web space of the foot. Meticulous care must be taken during anterior fasciotomy to avoid plunging instruments deep into the muscle belly, which could inadvertently lacerate these vital structures.
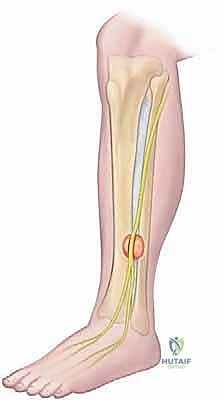
Adjacent to the anterior compartment, separated by the anterior intermuscular septum, lies the lateral compartment. Bound by the fibula medially, the anterior intermuscular septum anteriorly, the posterior intermuscular septum posteriorly, and the deep crural fascia laterally, it contains the peroneus longus and brevis muscles, responsible for foot eversion and plantarflexion stabilization. The critical anatomical feature of this compartment is the superficial peroneal nerve (SPN). The SPN branches from the common peroneal nerve, courses through the substance of the peroneus longus, and descends within the lateral compartment. It typically pierces the deep crural fascia to become subcutaneous in the distal third of the leg, approximately 10 to 12 centimeters proximal to the lateral malleolus.

The Posterior Compartments and Anatomical Variations
The posterior aspect of the leg is divided into the superficial and deep posterior compartments by the transverse intermuscular septum. The superficial posterior compartment, enveloped by the deep fascia of the leg, contains the massive gastrocnemius-soleus complex and the plantaris muscle, which are the primary effectors of ankle plantarflexion. The sural nerve, formed by contributions from the medial and lateral sural cutaneous nerves, descends superficially within this compartment, providing sensation to the posterolateral aspect of the distal leg and lateral foot. While less commonly affected by CECS than the anterior compartment, superficial posterior compartment syndrome can cause severe calf cramping during exertion.
The deep posterior compartment is anatomically complex and technically demanding to access. It is bound anteriorly by the posterior surfaces of the tibia, fibula, and interosseous membrane, and posteriorly by the transverse intermuscular septum. It contains the flexor hallucis longus, flexor digitorum longus, tibialis posterior, and the popliteus muscles. Critically, it houses the posterior tibial artery, peroneal artery, and the tibial nerve. The tibial nerve provides motor innervation to the deep plantarflexors and sensory innervation to the plantar aspect of the foot.

Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for Chronic Exertional Compartment Syndrome must be predicated on a rigorous, evidence-based evaluation. Fasciotomy is not a prophylactic procedure, nor is it a panacea for all forms of exertional leg pain. The primary indication for surgical release is a confirmed diagnosis of CECS in a patient who has failed a comprehensive trial of non-operative management and is unwilling or unable to modify their activity level to mitigate symptoms. Non-operative modalities typically include prolonged rest, non-steroidal anti-inflammatory drugs (NSAIDs), physical therapy focusing on biomechanical gait retraining, orthotic management, and occasionally, botulinum toxin injections, though the efficacy of the latter remains debated.
The diagnostic gold standard, and thus the absolute prerequisite for surgical indication, is dynamic intracompartmental pressure (ICP) testing. We strictly adhere to the modified Pedowitz criteria to establish the diagnosis. A positive test is defined by one or more of the following pressure thresholds: a pre-exercise resting pressure of ≥ 15 mm Hg, a 1-minute post-exercise pressure of ≥ 30 mm Hg, or a 5-minute post-exercise pressure of ≥ 20 mm Hg. It is imperative that the exercise protocol utilized during testing exactly replicates the specific activity that precipitates the patient's symptoms; failure to do so will invariably yield false-negative results.
Conversely, the contraindications to fasciotomy are primarily rooted in misdiagnosis or the presence of alternative pathologies that mimic CECS. Performing a fasciotomy on a patient whose pain is actually derived from medial tibial stress syndrome (MTSS) or a tibial stress fracture will not only fail to relieve their symptoms but will subject them to the unnecessary morbidities of surgery. Furthermore, vascular anomalies such as Popliteal Artery Entrapment Syndrome (PAES) must be meticulously ruled out, particularly in young athletes presenting with exertional calf pain and diminished distal pulses during active plantarflexion.
| Category | Specific Conditions and Parameters |
|---|---|
| Absolute Indications | Confirmed CECS via Pedowitz Criteria (Resting ≥15 mmHg, 1-min post ≥30 mmHg, 5-min post ≥20 mmHg). |
| Absolute Indications | Failure of >3-6 months of conservative management (gait retraining, orthotics, rest). |
| Absolute Indications | Patient inability/unwillingness to permanently cease the precipitating athletic or occupational activity. |
| Relative Indications | Presence of a symptomatic fascial hernia with concomitant, documented elevated compartment pressures. |
| Absolute Contraindications | Equivocal or negative dynamic intracompartmental pressure measurements. |
| Absolute Contraindications | Confirmed alternative diagnosis: Tibial stress fractures, Medial Tibial Stress Syndrome (MTSS). |
| Absolute Contraindications | Popliteal Artery Entrapment Syndrome (PAES) or peripheral arterial claudication. |
| Relative Contraindications | Severe psychological overlay or secondary gain issues (e.g., malingering in military populations). |
| Relative Contraindications | Active local soft tissue infection or severe peripheral neuropathy. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of a successful fasciotomy, mitigating intraoperative complications and drastically reducing the risk of symptom recurrence. The planning phase begins with a comprehensive review of the patient's dynamic ICP testing results to definitively map which compartments require release. It is a well-documented surgical maxim that the most common cause of failed CECS surgery is the incomplete release of an affected compartment, or the complete failure to release a concomitantly involved, but unrecognized, compartment. Therefore, if the anterior compartment tests positive, the lateral compartment must be highly scrutinized, and many surgeons advocate for a prophylactic release of the lateral compartment when addressing the anterior, given their shared fascial boundaries and high rate of dual involvement.
Advanced imaging modalities, while not strictly diagnostic for CECS, play a vital adjunctive role in pre-operative templating. High-resolution Magnetic Resonance Imaging (MRI) is routinely obtained to definitively exclude stress fractures, periostitis, and deep-seated neoplasms. Furthermore, T2-weighted MRI sequences acquired immediately post-exertion can demonstrate diffuse muscle edema and increased signal intensity within the affected compartments, providing supportive anatomical evidence of the syndrome. High-frequency ultrasound is also highly valuable for mapping the precise anatomical course of the superficial peroneal nerve and identifying any fascial defects or muscle herniations that must be addressed during the surgical exposure.

Patient positioning and operating room setup must be standardized to ensure optimal surgical ergonomics and access. For isolated anterior/lateral releases, or comprehensive four-compartment releases, the patient is positioned completely supine on a standard radiolucent operating table. A small, well-padded bump is placed under the ipsilateral greater trochanter to internally rotate the leg slightly, bringing the anterolateral aspect of the tibia into a direct vertical orientation.


Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a fasciotomy for CECS demands precision, anatomical respect, and an unwavering commitment to achieving a complete release. While minimally invasive and endoscopic techniques have been described, the open or semi-open single-incision or dual-incision techniques remain the gold standard, offering superior visualization and a lower risk of iatrogenic nerve injury. We will detail the single-incision lateral approach for combined anterior and lateral compartment release, as it is the most frequently utilized and technically nuanced procedure.
The Single-Incision Anterolateral Approach
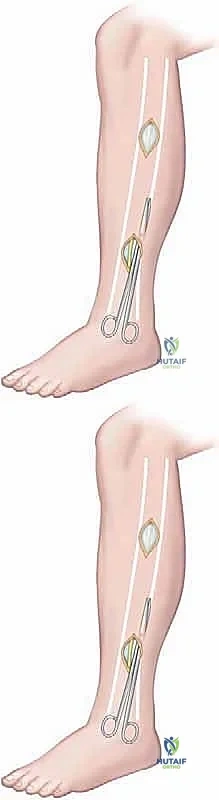
Following exsanguination and tourniquet inflation, the surgical landmarks—the tibial crest, the fibular shaft, and the anticipated course of the superficial peroneal nerve—are meticulously marked. A 5 to 6-centimeter longitudinal incision is centered exactly midway between the tibial crest and the fibular shaft, typically in the middle third of the leg. This placement optimally overlies the anterior intermuscular septum. The skin and subcutaneous tissues are sharply incised down to the glistening crural fascia. Hemostasis is achieved meticulously with bipolar electrocautery to prevent post-operative hematoma.

The critical next step is the identification and protection of the superficial peroneal nerve (SPN). A small, 1-centimeter transverse incision is made through the fascia directly over the anterior intermuscular septum. Using a blunt right-angle clamp or a delicate nerve hook, the surgeon sweeps longitudinally within the lateral compartment, immediately deep to the fascia, to identify the SPN. The nerve is often found intimately associated with the septum and must be gently mobilized and retracted laterally.

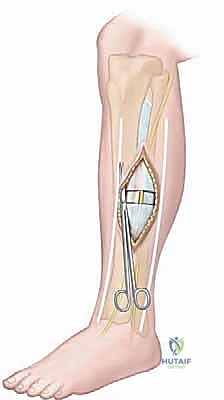
Once the SPN is under direct visualization and protected, the longitudinal fascial releases commence. For the anterior compartment, long, blunt-tipped Metzenbaum scissors or a specialized fasciotome are introduced deep to the fascia but superficial to the epimysium of the tibialis anterior. The scissors are pushed proximally toward the tibial tubercle and distally toward the extensor retinaculum. The release must be complete; a common pitfall is failing to extend the proximal release to the very origin of the muscle.



Attention is then turned to the lateral compartment. The scissors are redirected laterally and posteriorly from the initial fascial window. The lateral fascia is released proximally to the fibular head and distally to the lateral malleolus. Throughout this maneuver, the SPN must be continuously monitored. If a fascial hernia is present, it is incorporated into the longitudinal release, effectively obliterating the defect and preventing future nerve entrapment.





Following complete release, the tourniquet is deflated, and meticulous hemostasis is obtained. The muscle bellies will visibly bulge through the fascial defects, confirming adequate decompression. The deep fascia is left entirely open; no attempt is made to reapproximate it. Only the subcutaneous tissue and skin are closed, typically with interrupted absorbable sutures for the dermis and a running subcuticular closure or nylon sutures for the skin.









Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, fasciotomy for CECS is not without its complications. The most devastating, yet fortunately rare, complication is iatrogenic injury to the superficial peroneal nerve or the saphenous nerve (in medial approaches). Nerve injury can range from transient neurapraxia due to overzealous retraction, to complete transection resulting in permanent sensory deficits and painful neuroma formation. The incidence of SPN injury is reported to be between 2% and 7% in large retrospective cohorts. Prevention relies entirely on direct visualization and the use of blunt-tipped instruments during the blind portions of the fascial release.
Symptom recurrence is perhaps the most frustrating complication for both the surgeon and the patient. Recurrence rates vary widely in the literature, ranging from 5% to 20%, and are significantly higher for deep posterior compartment releases compared to anterior releases. Recurrence is almost universally attributable to one of three factors: an initially incomplete fascial release (failing to extend the incision to the proximal or distal extents of the compartment), the post-operative formation of robust, constricting scar tissue bridging the fascial gap, or an initial misdiagnosis.
When faced with a recurrent case of CECS, a rigorous re-evaluation is mandated. This includes repeat dynamic ICP testing to confirm elevated pressures and an MRI to assess for scar tissue or missed alternative diagnoses. Salvage management typically requires a revision surgery. However, simple repeat fasciotomy is often insufficient due to the altered anatomical planes and dense fibrosis. In these complex revision scenarios, a partial fasciectomy—the actual excision of a 1 to 2-centimeter strip of fascia along the entire length of the compartment—is strongly recommended to definitively prevent re-bridging of the fascial envelope.
| Complication | Estimated Incidence Rate | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Superficial Peroneal Nerve Injury | 2% - 7% | Blind fascial release, aggressive retraction, anatomical variants. | Intra-op: Primary repair. Post-op: Gabapentinoids, neuroma excision and burying in muscle. |
| Symptom Recurrence | 5% - 20% | Incomplete release, robust scar formation, missed secondary compartment. | Repeat ICP testing. Revision surgery with extensive partial fasciectomy. |
| Post-operative Hematoma | 3% - 5% | Inadequate hemostasis, premature return to vigorous activity. | Observation for small hematomas. Evacuation if causing acute compartment pressures or wound compromise. |
| Deep Vein Thrombosis (DVT) | < 1% | Tourniquet time, post-operative immobilization. | Standard anticoagulation protocols. Early mobilization is the best prophylaxis. |
| Wound Dehiscence / Infection | 1% - 3% | Poor skin envelope, excessive edema, premature suture removal. | Local wound care, oral/IV antibiotics. Rarely requires surgical debridement. |
Phased Post-Operative Rehabilitation Protocols
The success of a fasciotomy is intrinsically linked to the quality and adherence to a structured, phased post-operative rehabilitation protocol. The primary goals of rehabilitation are to minimize post-operative edema, prevent the formation of restrictive adhesions across the fasciotomy site, and safely restore the patient to their pre-injury level of athletic or occupational performance. Rehabilitation must be aggressive yet respectful of the healing soft tissues.
Phase 1: Protection and Early Mobility (Weeks 0-2)
Immediately post-operatively, the patient is placed in a bulky, compressive Jones dressing to mitigate hematoma formation and swelling. Weight-bearing is typically allowed as tolerated with the assistance of crutches, though some surgeons prefer a brief period of non-weight-bearing (3-5 days) to minimize bleeding. The critical intervention in this phase is immediate, active range of motion (ROM) of the ankle and toes. Early mobilization is paramount; it acts as an internal massage, utilizing the gliding of the muscle bellies to disrupt early cross-linking of collagen and prevent the fascia from scarring back together. Cryotherapy and strict elevation are enforced to manage edema.
Phase 2: Restoration of Strength and Tissue Gliding (Weeks 2-6)
Sutures are removed at approximately 10 to 14 days, provided the wound is completely epithelialized. Once the incision is secure, aggressive cross-friction scar massage is initiated. This is a vital component of the protocol, aimed at ensuring the skin and subcutaneous tissues glide freely over the underlying muscle, preventing tethering. Patients transition to full weight-bearing without assistive devices. Low-impact cardiovascular activities, such as stationary cycling and deep-water running, are introduced to promote local blood flow and maintain aerobic conditioning without subjecting the compartments to high-impact stress. Isotonic strengthening of the lower extremity musculature begins, focusing on high-repetition, low-resistance exercises.
Phase 3: Plyometrics and Return to Sport (Weeks 6-12+)
The final phase bridges the gap between clinical recovery and functional performance. Patients must demonstrate full, pain-free ROM, symmetrical strength, and an absence of exertional symptoms during low-impact activities before progressing. A graduated return-to-run program is implemented, starting with short intervals of jogging on a soft surface (e.g., a treadmill or rubberized track) and progressively increasing duration and intensity. Plyometric drills, agility training, and sport-specific biomechanical assessments are integrated. For runners, a formal gait analysis is highly recommended to identify and correct any underlying biomechanical flaws—such as over-striding or excessive heel striking—that may have contributed to the initial development of CECS. Full return to unrestricted competitive activity is typically achieved between 8 and 12 weeks post-operatively, though military personnel may require extended conditioning prior to resuming heavy load-bearing marches.
Summary of Landmark Literature and Clinical Guidelines
The contemporary understanding and surgical management of Chronic Exertional Compartment Syndrome are built upon
