Acute Compartment Syndrome Fasciotomy: Urgent Surgical Guide
Key Takeaway
Here are the crucial details you must know about Acute Compartment Syndrome Fasciotomy: Urgent Surgical Guide. Acute compartment syndrome is a critical orthopedic emergency where increased pressure within an osteofascial compartment compromises blood flow, leading to tissue damage and cell death. Untreated, it can cause myonecrosis, acute renal failure, and limb loss. An **acute compartment syndrome fasciotomy** is a vital surgical procedure to relieve this pressure, restore circulation, and prevent devastating, life-threatening complications.
Comprehensive Introduction and Patho-Epidemiology
Acute compartment syndrome (ACS) remains one of the most devastating and time-critical orthopedic emergencies encountered in clinical practice. The profound clinical sequelae and the severe medicolegal implications associated with a delayed or missed diagnosis make it an entity of paramount importance in the entirety of orthopedic surgery. At its core, compartment syndrome is a condition characterized by an elevation of interstitial pressure within a closed osteofascial compartment to a level that severely compromises the microcirculation of the tissues within that space. When the intracompartmental pressure exceeds the intramuscular arteriolar and capillary perfusion pressures, the resultant cessation of blood flow leads to a precipitous decline in oxygen diffusion, initiating a cascade of cellular ischemia, anoxia, and ultimately, irreversible myonecrosis and nerve death.
The historical recognition of this pathology dates back to 1872 when Richard von Volkmann first documented the catastrophic nerve injury and subsequent irreversible muscle contracture following a supracondylar humerus fracture. Decades later, in 1906, Dr. Hildebrand applied the term "Volkmann ischemic contracture" to define the devastating end-stage result of untreated compartment syndrome. By 1909, Dr. Thomas had systematically reviewed 112 published cases, identifying fractures as the predominant etiology. The conceptualization of surgical decompression was introduced by Dr. Murphy in 1914, who first suggested that fasciotomy could prevent these debilitating contractures. However, the modern understanding of lower extremity compartment syndrome was not fully established until 1967, when Seddon, Kelly, and Whitesides accurately described the existence of four distinct compartments in the lower leg, emphasizing the absolute necessity of decompressing all compartments rather than just the anterior compartment.
Epidemiologically, the incidence of acute compartment syndrome is approximately 7.3 per 100,000 in males and 0.7 per 100,000 in females, reflecting a demographic skew toward young males involved in high-energy trauma. Fractures represent the most common etiology, accounting for up to 69% of all cases, with diaphyseal tibial fractures and tibial plateau fractures being the most frequent culprits. Notably, it is estimated that up to 9.1% of high-energy tibial plateau fractures develop ACS. Blunt soft tissue trauma without fracture is the second most common cause, responsible for approximately 23% of cases. Crucially, as demonstrated by McQueen et al., the incidence of compartment syndrome is nearly equal across both high- and low-energy injuries. Furthermore, the presence of an open fracture does not inherently decompress the compartments; the fascial envelope often remains intact despite the cutaneous violation, meaning open wounds are absolutely not protective against the development of ACS.
The pathogenesis of ACS is driven by a fundamental mismatch between the volume of the compartment contents and the unyielding nature of the surrounding fascial envelope. This can occur either via an increase in the volume of the compartment contents (e.g., hemorrhage from fractures or major vessel injury, capillary leakage from ischemia or burns, and iatrogenic fluid extravasation) or a decrease in the absolute volume of the compartment (e.g., tight circumferential casts, localized external pressure from prolonged immobilization, or burn eschars). As intracompartmental pressure rises, venous outflow is obstructed, leading to venous engorgement and a further increase in capillary hydrostatic pressure. This initiates a vicious cycle of capillary leakage, exacerbating tissue edema. At the cellular level, ischemia leads to a failure of ATP-dependent sodium-potassium pumps, resulting in an influx of intracellular calcium, cellular swelling, and eventual necrosis. If left untreated, the systemic release of myoglobin, potassium, and inflammatory mediators from necrotic muscle can precipitate acute kidney injury, cardiac arrhythmias, multiorgan failure, and death.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the lower extremity osteofascial anatomy is the absolute prerequisite for performing an effective and safe fasciotomy. The lower leg is enveloped by the unyielding crural fascia and is anatomically divided into four distinct compartments: the anterior, lateral, superficial posterior, and deep posterior compartments. The rigid boundaries of these compartments are defined by the tibia, the fibula, the interosseous membrane, and the dense intermuscular septa. Because the crural fascia is essentially inelastic, any accumulation of fluid or hemorrhage within these confined spaces inevitably leads to a rapid exponential rise in interstitial pressure.

The anterior compartment is bounded anteriorly by the crural fascia, laterally by the anterior intermuscular septum, medially by the lateral surface of the tibia, and posteriorly by the interosseous membrane. It contains four primary muscles: the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and peroneus tertius. The critical neurovascular bundle of this compartment consists of the deep peroneal nerve and the anterior tibial artery. The deep peroneal nerve provides motor innervation to the compartment's musculature and descends to provide sensory innervation to the first dorsal web space of the foot. The anterior tibial artery courses just anterior to the interosseous membrane and continues distally as the dorsalis pedis artery. Ischemia in this compartment frequently presents as weakness in ankle dorsiflexion and sensory deficits in the first web space.

The lateral compartment is bordered anteriorly by the anterior intermuscular septum, posteriorly by the posterior intermuscular septum, and medially by the lateral surface of the fibula. It contains only two muscles: the peroneus longus and the peroneus brevis, which act as the primary evertors of the foot. The neurovascular supply is dominated by the superficial peroneal nerve, which provides motor function to these muscles before piercing the crural fascia approximately 10 to 12 centimeters proximal to the lateral malleolus to provide sensation to the dorsum of the foot. Notably, the deep peroneal nerve also courses through the proximal aspect of this compartment as it winds around the fibular neck, making it susceptible to injury both from elevated pressures and during surgical approaches. There is no major axial artery within the lateral compartment; the musculature relies on perforating branches from the peroneal and anterior tibial arteries.
The posterior aspect of the leg is divided by the transverse intermuscular septum into superficial and deep compartments. The superficial posterior compartment contains the gastrocnemius, soleus, and plantaris muscles. These powerful plantar flexors are supplied by branches of the tibial nerve, as well as the posterior tibial and peroneal arteries. The sural nerve courses superficially over this compartment, providing sensation to the posterolateral aspect of the leg and foot. The deep posterior compartment is situated beneath the soleus and is bounded anteriorly by the posterior surfaces of the tibia, fibula, and interosseous membrane. It contains the flexor digitorum longus, tibialis posterior, and flexor hallucis longus. The tibialis posterior is often enveloped in its own distinct fascial layer, which must be independently released during decompression. This compartment houses the critical posterior neurovascular bundle, including the tibial nerve, the posterior tibial artery and vein, and the peroneal artery and vein.
Exhaustive Indications and Contraindications
The decision to proceed with an emergent four-compartment fasciotomy is based on a synthesis of meticulous clinical examination and, when necessary, precise invasive pressure monitoring. The classic "six Ps" of compartment syndrome—pain, paresthesias, pallor, paralysis, pulselessness, and poikilothermia—are historically taught but are clinically treacherous if relied upon rigidly. Pulselessness and pallor are extremely late findings; their absence does not rule out compartment syndrome, as capillary perfusion ceases long before arterial pressure is overcome. By the time paralysis or pulselessness is present, irreversible myonecrosis and nerve damage have almost certainly occurred.
The earliest and most sensitive clinical indicator of acute compartment syndrome is pain that is out of proportion to the apparent injury, particularly pain elicited by passive stretch of the ischemic muscles. For example, passive plantar flexion of the toes will exacerbate pain in the anterior compartment (stretching the extensor digitorum longus and extensor hallucis longus). Paresthesias in the distribution of the nerves traversing the compartments (e.g., the deep peroneal nerve in the first dorsal web space) indicate early ischemic neurapraxia, as sensory nerves are highly sensitive to hypoxia and begin to lose function within 2 hours of ischemia. However, clinical examination is often confounded by factors such as polytrauma, traumatic brain injury, intubation, sedation, or the use of regional anesthesia (e.g., epidural or peripheral nerve blocks), which can mask the cardinal symptom of pain.

When clinical signs are ambiguous or the patient is unexaminable, objective measurement of intracompartmental pressures is mandatory. The Stryker intracompartmental pressure monitor is the most widely utilized device. Current evidence-based guidelines, spearheaded by the landmark work of McQueen and Court-Brown, dictate that the absolute compartment pressure is less relevant than the differential pressure, or "Delta P." The Delta P is calculated by subtracting the measured compartment pressure from the patient's diastolic blood pressure. A Delta P of less than or equal to 30 mm Hg is an absolute indication for emergent fasciotomy. This threshold accounts for systemic hypotension, which lowers the perfusion pressure and makes the limb more susceptible to ischemic injury at lower absolute compartment pressures.
| Indications for Fasciotomy | Contraindications to Fasciotomy |
|---|---|
| Delta P (Diastolic BP - Compartment Pressure) ≤ 30 mm Hg | Missed ACS with ischemia > 24-48 hours (muscle is entirely necrotic; fasciotomy risks fatal infection) |
| Unequivocal clinical signs (pain out of proportion, pain on passive stretch) in an awake, alert patient | Prophylactic fasciotomy in low-risk, asymptomatic patients without objective pressure data |
| Unexaminable patient (intubated, obtunded) with high-risk injury (e.g., high-energy tibial plateau fracture) and rising pressures | Pre-existing severe peripheral vascular disease where amputation is the definitive life-saving procedure |
| Arterial injury with prolonged ischemia time (> 4-6 hours) requiring vascular repair | Exertional compartment syndrome (chronic, non-emergent condition treated electively) |
Relative contraindications exist primarily in the setting of a "missed" compartment syndrome. If the diagnosis is delayed beyond 24 to 48 hours and the limb is entirely insensate and paralyzed, the musculature is likely completely necrotic. In this grim scenario, performing a fasciotomy exposes dead tissue to hospital-acquired pathogens, leading to a massive risk of deep infection, sepsis, and a significantly higher rate of eventual amputation. In such cases, observation with delayed orthotic management of the resulting Volkmann contracture, or primary amputation, may be the more prudent surgical decision.
Pre-Operative Planning, Templating, and Patient Positioning
Once the diagnosis of acute compartment syndrome is established, surgical intervention must proceed with absolute urgency. The universally accepted upper limit of tissue viability is 6 hours of ischemia. Beyond 8 hours, irreversible myonecrosis and permanent nerve damage are virtually guaranteed. Therefore, preoperative preparation must occur simultaneously with operating room mobilization. All constrictive dressings, casts, and splints must be immediately removed down to the skin. Bivalving a cast and cutting the underlying padding can reduce compartment pressures by up to 50-85%, providing a critical, albeit temporary, improvement in microcirculation while awaiting surgical decompression.

Coordination with the anesthesia team is vital. General anesthesia is strongly preferred over regional anesthesia. Regional blocks cause sympathectomy, which can exacerbate local swelling, and more importantly, they mask postoperative pain, eliminating the surgeon's ability to clinically monitor for inadequate decompression or recurrent compartment syndrome. Furthermore, the anesthesia team must be instructed to maintain normotension. Permissive hypotension, often utilized in trauma resuscitation, must be avoided in the setting of ACS, as a drop in systemic diastolic blood pressure directly reduces the perfusion pressure (Delta P), exacerbating tissue ischemia. Aggressive intravenous fluid hydration is also initiated to maintain renal perfusion and mitigate the nephrotoxic effects of circulating myoglobin released from damaged muscle.
Patient positioning is straightforward but requires meticulous attention to detail to ensure unhindered access to both the medial and lateral aspects of the leg. The patient is placed supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the lateral compartment into view, while allowing the leg to easily fall into external rotation for medial access. The entire lower extremity, from the iliac crest to the toes, is prepped and draped free. A sterile tourniquet may be placed on the proximal thigh but should strictly NOT be inflated during the decompression phase, as it exacerbates ischemia and prevents the visual assessment of muscle viability and bleeding upon fascial release.
The surgical armamentarium must be prepared in advance. This includes a sterile intracompartmental pressure monitor to confirm pressures if necessary, long dissecting scissors (Metzenbaum or Mayo) for fascial release, electrocautery for hemostasis of perforating vessels, and materials for temporary wound closure. Given that the wounds will be left open, a negative pressure wound therapy (NPWT) system or vessel loops for a "shoelace" closure technique should be available on the back table.
Step-by-Step Surgical Approach and Fixation Technique
The gold standard for the treatment of lower extremity acute compartment syndrome is the two-incision, four-compartment fasciotomy, as popularized by Mubarak and Owen. While a single-incision perifibular approach (Matsen technique) exists, it is technically demanding, carries a higher risk of iatrogenic injury to the superficial peroneal nerve, and often results in inadequate decompression of the deep posterior compartment. Therefore, the two-incision technique remains the definitive, safest, and most reliable method for achieving complete fascial release.

The Anterolateral Approach
The anterolateral incision is designed to decompress both the anterior and lateral compartments. The incision is centered exactly midway between the tibial crest and the fibular shaft, typically about 2 centimeters lateral to the anterior border of the tibia. The incision must be extensile, spanning from the level of the tibial tubercle down to 5 centimeters proximal to the lateral malleolus. Subcutaneous dissection is performed sharply, taking immense care to preserve the superficial venous plexus and avoid undermining the skin flaps, which can lead to skin necrosis.
Once the crural fascia is exposed, a transverse nick is made in the fascia midway down the leg. This transverse incision allows the surgeon to identify the anterior intermuscular septum, which separates the anterior and lateral compartments. Using long dissecting scissors, the fascia of the anterior compartment is released longitudinally, aiming proximally toward the patella and distally toward the center of the ankle. Next, the lateral compartment is released. The scissors are directed longitudinally, posterior to the intermuscular septum. The surgeon must exercise extreme caution during the distal aspect of the lateral fascial release, as the superficial peroneal nerve exits the fascia approximately 10 to 12 centimeters proximal to the lateral malleolus. The nerve must be identified, protected, and traced to ensure it is not tethered or injured.
The Posteromedial Approach
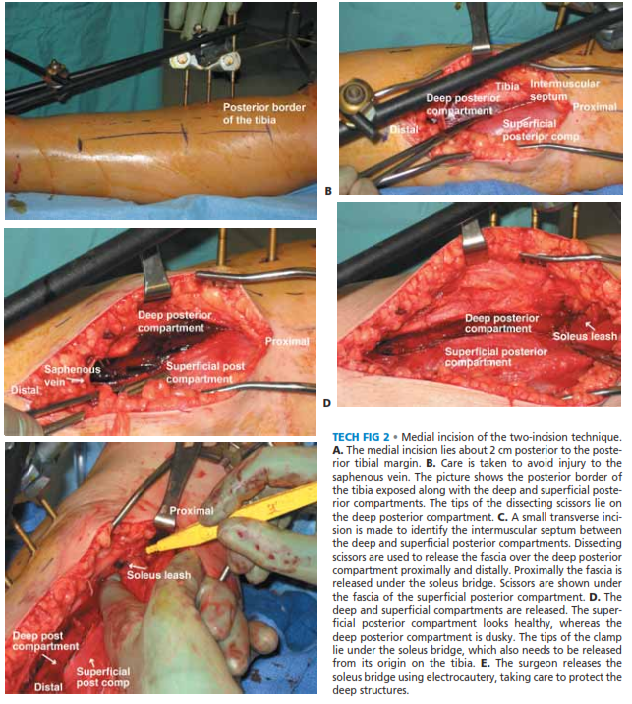
The posteromedial incision decompresses the superficial and deep posterior compartments. The leg is externally rotated, and a longitudinal incision is made 2 centimeters posterior to the posteromedial border of the tibia. This incision also extends from just distal to the tibial plateau down to the level of the medial malleolus. During the superficial dissection, the surgeon must identify and protect the greater saphenous vein and the accompanying saphenous nerve, retracting them anteriorly.

The fascia over the superficial posterior compartment (gastrocnemius and soleus) is incised longitudinally for the entire length of the incision. To access the deep posterior compartment, the soleus muscle must be detached from its origin on the posteromedial tibia. By retracting the soleus and gastrocnemius posteriorly, the fascia covering the deep posterior compartment (flexor digitorum longus, tibialis posterior, and flexor hallucis longus) is exposed. This fascial layer is incised longitudinally. Crucially, the surgeon must ensure that the specific epimysial covering of the tibialis posterior muscle is also released, as it often resides within its own sub-compartment and is a frequent site of isolated missed compartment syndrome.
Following complete decompression of all four compartments, the muscle tissue is meticulously inspected for viability using the "Four Cs": Color, Consistency, Contractility, and Capacity to bleed. Any frankly necrotic muscle must be aggressively debrided to prevent systemic toxicity and infection. The wounds are thoroughly irrigated. Under no circumstances should the skin or fascia be closed primarily. The wounds are typically managed with negative pressure wound therapy (NPWT) set to -125 mm Hg, or a vessel loop "shoelace" technique over a non-adherent dressing, to prevent skin retraction and facilitate delayed closure.
Complications, Incidence Rates, and Salvage Management
The complications associated with acute compartment syndrome are broadly categorized into those arising from the disease process itself (due to delayed treatment) and those occurring as iatrogenic consequences of the surgical intervention. The overarching principle is that prolonged ischemia correlates directly with the severity of both local and systemic complications.
Systemically, the release of intracellular contents from necrotic muscle fibers leads to rhabdomyolysis. The massive influx of myoglobin into the systemic circulation can overwhelm the renal tubules, precipitating acute kidney injury (AKI) in up to 15% of severe cases. This is compounded by metabolic acidosis and hyperkalemia, which can trigger fatal cardiac arrhythmias. Immediate systemic salvage management involves aggressive intravenous hydration, urine alkalinization with sodium bicarbonate, and occasionally, emergent hemodialysis.

Locally, the most feared complication of a missed or delayed fasciotomy is Volkmann ischemic contracture. As necrotic muscle is replaced by dense, inelastic fibrotic scar tissue, the limb is drawn into a rigid, non-functional posture (typically equinovarus in the lower extremity). Sensation is profoundly diminished due to permanent ischemic neuropathy. In severe cases of missed ACS, the incidence of eventual amputation approaches 20-50%.
| Complication | Estimated Incidence | Salvage / Management Strategy |
|---|---|---|
| Acute Kidney Injury (Myoglobinuria) | 10 - 15% in severe cases | Aggressive IV hydration, alkalinization of urine, hemodialysis |
| Superficial Peroneal Nerve Injury | 5 - 10% (Anterolateral approach) | Meticulous intra-op identification; post-op AFO for foot drop |
| Deep Infection / Osteomyelitis | 10 - 20% (Higher with open fractures) | Serial debridement, targeted IV antibiotics, hardware removal if necessary |
| Volkmann Ischemic Contracture | Variable (Depends on delay > 12 hrs) | Tendon transfers, contracture release, orthotic bracing, or amputation |
| Delayed Union / Nonunion of Fracture | 15 - 25% | Bone grafting, optimization of soft tissue envelope, rigid fixation |
Iatrogenic complications during fasciotomy are not uncommon. The superficial peroneal nerve is highly vulnerable during the anterolateral approach, and its transection results in a permanent sensory deficit over the dorsum of the foot. Similarly, the saphenous nerve and vein are at risk during the posteromedial approach. Furthermore, the creation of massive surgical wounds inherently increases the risk of deep infection, particularly when associated with underlying fractures. The loss of the protective soft tissue envelope over a tibial fracture significantly increases the rates of delayed union and nonunion, often necessitating subsequent complex reconstructive procedures, including rotational or free tissue transfer, to achieve bone coverage.
Phased Post-Operative Rehabilitation Protocols
The postoperative management of a fasciotomy patient is a complex, multi-phased endeavor that requires close collaboration between orthopedic surgeons, plastic surgeons, and physical therapists. The immediate postoperative phase (Days 0 to 3) is focused on systemic stabilization, limb elevation, and continuous monitoring for recurrent compartment syndrome. The limb must be elevated at the level of the heart—not higher, to avoid decreasing arterial perfusion pressure, and not lower, to prevent exacerbation of venous congestion.
Patients are universally returned to the operating room at 48 to 72 hours for a "second look" debridement. During this procedure, the muscle is reassessed for viability, and any delayed necrosis is sharply debrided. If the swelling has subsided sufficiently, delayed primary closure may be attempted, often utilizing vessel loops to gradually approximate the skin edges over several days. However, in the vast majority of cases, the profound tissue edema precludes primary closure. In such instances, a split-thickness skin graft (STSG), typically harvested from the ipsilateral thigh, is applied to the remaining defects once a healthy, granulating wound bed is established, usually between Days 7 and 14.
The subacute rehabilitation phase begins as soon as the soft tissues are stabilized and any associated fractures are rigidly fixed. Early, aggressive physical therapy is absolutely critical to prevent the formation of debilitating contractures. Passive and active range of motion exercises for the ankle and toes are initiated immediately. The most common postural deformity following lower leg fasciotomy is an equinus contracture of the ankle, driven by the relative over-pull of the posterior musculature and the scarring of the anterior compartment. To mitigate this, the ankle must be rigorously splinted in neutral dorsiflexion (90 degrees) at all times when the patient is not actively participating in therapy.
Long-term functional recovery can be protracted. Even with timely intervention, patients frequently experience residual muscle weakness, particularly in dorsiflexion, and chronic sensory deficits. If irreversible damage to the deep peroneal nerve or anterior compartment musculature has occurred, the patient will present with a permanent foot drop. In these cases, early fitting for an Ankle-Foot Orthosis (AFO) is essential to normalize the gait pattern and prevent secondary kinetic chain pathologies. Full return to baseline physical activity can take up to 12 to 18 months, and patients must be extensively counseled regarding these expectations.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of acute compartment syndrome is deeply rooted in several landmark biomechanical and clinical studies that have shaped modern orthopedic guidelines. The foundational understanding of the critical time window for intervention was established by Rorabeck and Macnab in 1975. Through rigorous animal models, they demonstrated that skeletal muscle undergoes irreversible histologic changes after 8 hours of continuous ischemia, while peripheral nerves exhibit irreversible damage after as little as 6 hours. This established the universally accepted 6-hour window for optimal surgical decompression.
The evolution of pressure monitoring thresholds represents another critical milestone in the literature. Early pioneers, including Whitesides et al., initially suggested an absolute compartment pressure of 30 mm Hg as the threshold for fasciotomy. However, subsequent foundational studies by Heckman et al. highlighted the paramount importance of systemic blood pressure in maintaining capillary perfusion. They demonstrated that irreversible ischemic changes occurred when the compartment pressure rose to within 10 to 20 mm Hg of the diastolic pressure.
This concept was definitively codified by McQueen and Court-Brown in 1996. In their landmark prospective study, they introduced the concept of the "Delta P" (diastolic blood pressure minus compartment pressure) and established that a Delta P of less than or equal to 30 mm Hg is the most reliable indicator for fasciotomy. Their cohort demonstrated that utilizing this differential pressure threshold eliminated unnecessary fasciotomies in hypotensive patients while preventing missed compartment syndromes in hypertensive individuals.
Current consensus guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the Orthopaedic Trauma Association (OTA) strongly advocate for continuous intracompartmental pressure monitoring in high-risk patients who are unexaminable due to obtundation, intubation, or polytrauma. Furthermore, the literature unequivocally stresses the medicolegal necessity of meticulous, serial, and thoroughly documented clinical examinations. The standard of care dictates that any high-risk extremity must be evaluated at regular intervals, and any suspicion of ACS must be met with immediate pressure measurement or emergent surgical decompression, as the cost of a missed diagnosis far outweighs the morbidity of a prophylactic fasciotomy.
Clinical & Radiographic Imaging Archive
