Acute Compartment Syndrome: Timely Fasciotomy Explained
Key Takeaway
Learn more about Acute Compartment Syndrome: Timely Fasciotomy Explained and how to manage it. Compartment syndrome is a condition where pressure within an osteofascial compartment rises, exceeding intramuscular arteriolar pressure. This reduces blood flow, causing decreased oxygen diffusion to tissues and, ultimately, cell death. It's an orthopedic emergency where delayed treatment leads to worse outcomes, including life- and limb-threatening sequelae like myonecrosis. Understanding compartment syndrome j is critical.
Comprehensive Introduction and Patho-Epidemiology
Definition and Clinical Significance
Acute compartment syndrome (ACS) remains one of the most devastating and time-critical orthopaedic emergencies, representing a true race against irreversible tissue necrosis. If not recognized and treated with emergent decompressive fasciotomy, the condition progresses rapidly to catastrophic myonecrosis, permanent neurologic deficit, and potentially life-threatening systemic complications. The potential clinical sequelae and the profound medicolegal implications of a missed or delayed diagnosis make ACS one of the most heavily scrutinized entities in all of surgical practice. Compartment syndrome is defined as a critical elevation of interstitial pressure within a closed, non-yielding osteofascial compartment, which rises to a level that exceeds intramuscular arteriolar pressure. This pressure gradient reversal results in the cessation of capillary perfusion, severe localized tissue hypoxia, and ultimately, widespread cellular death.

Unlike many orthopaedic conditions where delayed intervention may only marginally affect the final functional outcome, ACS is the quintessential surgical emergency where evidence unequivocally demonstrates that any delay in treatment directly correlates with exponentially worse outcomes. The clinical sequelae of a missed compartment syndrome extend far beyond the affected limb. Unrelenting myonecrosis leads to massive rhabdomyolysis, releasing toxic intracellular contents into the systemic circulation, which can precipitate acute renal failure, cardiac arrhythmias from hyperkalemia, multiorgan dysfunction syndrome (MODS), and death. Consequently, the orthopaedic surgeon must maintain a high index of suspicion, particularly in high-energy trauma settings, as the window for successful intervention is notoriously narrow.
This chapter explicitly focuses on acute compartment syndrome, which must be strictly differentiated from chronic exertional compartment syndrome (CECS). While CECS is a transient, exercise-induced phenomenon that resolves with rest and rarely threatens limb viability, ACS is a progressive, unrelenting pathological cascade. Any situation that leads to either an increase in the volume of the compartment contents or a decrease in the overall volume capacity of the compartment can precipitate ACS. The thick, unyielding nature of the surrounding deep fascia prevents fluid from extravasating and precludes any compensatory volume expansion, thus trapping the expanding tissues in a rigid container.

Pathophysiology of Tissue Ischemia
The exact pathophysiology of compartment syndrome, while extensively studied, is a complex interplay of microvascular hemodynamics and cellular metabolic failure. The fundamental mechanism is characterized by a vicious cycle of ischemia and edema. As intracompartmental pressure rises, it first surpasses the low-pressure venous outflow system. The collapse of the thin-walled venules leads to venous hypertension and vascular congestion within the compartment. This venous engorgement subsequently increases the hydrostatic pressure at the capillary level, driving more fluid into the interstitial space and further elevating the intracompartmental pressure.
As the interstitial pressure continues to climb, it eventually overcomes the arteriolar perfusion pressure. It is critical to understand that arteriolar collapse occurs long before the intracompartmental pressure reaches the systolic blood pressure; therefore, distal pulses often remain palpable even in the presence of advanced compartment syndrome. The cessation of capillary blood flow deprives the highly metabolically active skeletal muscle and peripheral nerves of oxygen. Without oxygen, cellular metabolism shifts from aerobic to anaerobic glycolysis, producing lactic acid and causing a precipitous drop in local tissue pH.

At the cellular level, this anoxic environment leads to the rapid depletion of adenosine triphosphate (ATP). The failure of ATP-dependent sodium-potassium pumps (Na+/K+-ATPase) on the cell membrane results in a massive influx of extracellular sodium and water, causing severe intracellular cytotoxic edema. Concurrently, intracellular calcium concentrations spike, activating destructive calcium-dependent proteases and phospholipases that dismantle the cellular cytoskeleton and membrane. This "capillary leakage" and cellular swelling add immense volume to the already constrained compartment, exacerbating the pressure and solidifying the destructive feedback loop. Red muscle fibers, which rely heavily on aerobic metabolism, are far more vulnerable to this ischemic cascade than their white muscle fiber counterparts.

Epidemiological Considerations
The epidemiology of acute compartment syndrome provides crucial insights into patient risk stratification. The overall incidence of ACS is estimated at 7.3 per 100,000 in male patients and 0.7 per 100,000 in female patients. This striking 10-to-1 male predominance is largely attributed to the higher baseline muscle mass in young males, which leaves less potential space within the fascial compartments to accommodate post-traumatic swelling. Furthermore, young males are disproportionately involved in high-energy trauma, motor vehicle collisions, and contact sports, which are the primary drivers of the injuries associated with ACS.
Fractures are by far the most common etiology, accounting for up to 75% of all ACS cases. Specifically, diaphyseal fractures of the tibia carry the highest absolute risk, with rates of compartment syndrome ranging from 1% to 11% depending on the energy of the injury and the degree of soft tissue comminution. Proximal third tibial fractures, particularly high-energy tibial plateau fractures (Schatzker IV-VI), carry an even higher risk, estimated between 15% to 28%. Fracture-dislocations of the knee or ankle can push this risk profile as high as 50%. It is a dangerous misconception that open fractures naturally decompress the compartment; the fascial defect is rarely sufficient to relieve global compartment pressure, and studies have shown no significant difference in the incidence of ACS between open and closed tibial fractures.

Blunt soft tissue trauma without fracture is the second most common cause, responsible for approximately 23% of cases. Other etiologies include crush injuries, prolonged limb compression (such as a patient found down after a drug overdose or positioned improperly in the lithotomy position), burns, snake envenomation, and reperfusion injury following acute arterial occlusion repair. The age of the patient is also a highly significant risk factor; patients younger than 35 years are at the greatest risk, again due to the volume of their hypertrophied muscle bellies occupying a larger percentage of the fixed fascial compartment space.
Detailed Surgical Anatomy and Biomechanics
Osteofascial Compartments of the Lower Extremity
A profound understanding of the cross-sectional anatomy of the lower extremity is the absolute prerequisite for performing an effective decompressive fasciotomy. The lower leg is rigidly divided into four distinct osteofascial compartments: the anterior, lateral, superficial posterior, and deep posterior compartments. These compartments are defined by the tibia, the fibula, the interosseous membrane, and a series of robust, unyielding fascial septa. Failure to adequately release any one of these compartments, particularly the deep posterior compartment, is the most common cause of persistent ischemia and surgical failure.
The anterior compartment is bounded anteriorly by the crural fascia, laterally by the anterior intermuscular septum, medially by the lateral surface of the tibia, and posteriorly by the interosseous membrane. It contains four muscles: the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and peroneus tertius. Because the muscles of the anterior compartment are tightly constrained against the rigid tibia and interosseous membrane, this compartment is the most frequently involved in acute compartment syndrome of the lower extremity. The crural fascia here is exceptionally thick, providing virtually no compliance to expanding tissues.

The lateral compartment is bordered anteriorly by the anterior intermuscular septum, posteriorly by the posterior intermuscular septum, medially by the lateral surface of the fibula, and laterally by the crural fascia. It is the smallest of the four compartments and contains only two muscles: the peroneus longus and the peroneus brevis. The superficial posterior compartment is the largest, bounded deeply by the transverse intermuscular septum and superficially by the crural fascia. It houses the gastrocnemius, soleus, and plantaris muscles. Finally, the deep posterior compartment is located between the transverse intermuscular septum posteriorly and the interosseous membrane, tibia, and fibula anteriorly. It contains the flexor digitorum longus, tibialis posterior, and flexor hallucis longus.
Neurovascular Topography
The neurovascular structures within each compartment not only dictate the clinical signs of ischemia but also represent critical hazards during surgical release. In the anterior compartment, the deep peroneal nerve and the anterior tibial artery travel together just anterior to the interosseous membrane. The deep peroneal nerve provides motor innervation to the dorsiflexors and sensory innervation to the first dorsal web space of the foot. Ischemic dysfunction of this nerve manifests early as paresthesia in the first web space and later as a complete foot drop.

The lateral compartment is innervated by the superficial peroneal nerve, which supplies the peroneal musculature before piercing the crural fascia in the distal third of the leg to provide sensation to the dorsum of the foot. Because the superficial peroneal nerve exits the fascia anterior to the fibula, it is at extremely high risk of iatrogenic transection during the anterolateral fasciotomy incision if the surgeon strays too far anteriorly or fails to identify it under the fascia. Both the deep and superficial peroneal nerves originate from the common peroneal nerve, which wraps around the fibular neck, making proximal fibular fractures highly dangerous for both direct nerve injury and compartment syndrome.

The deep posterior compartment is the most anatomically complex and harbors the primary neurovascular bundle of the posterior leg: the tibial nerve, the posterior tibial artery and vein, and the peroneal artery and vein. The tibial nerve supplies motor function to the deep and superficial posterior muscles and sensation to the plantar aspect of the foot. The superficial posterior compartment, notably, does not contain a major named artery; its muscles are supplied by branches piercing the transverse septum. Understanding these pathways is vital, as ischemic pain in the deep posterior compartment is often elicited by passive extension of the toes, and sensory loss on the sole of the foot is a dire warning sign of tibial nerve ischemia.
Biomechanical Implications of Fascial Restraint
The biomechanics of the crural fascia play a central role in the pathogenesis of ACS. The fascia is composed of dense, regularly arranged collagen fibers that provide immense tensile strength but possess a highly non-linear elasticity profile. In a normal physiological state, the fascia allows for minor fluctuations in muscle volume during exercise (hyperemia). However, once the elastic limit of the fascia is reached, its compliance curve flattens dramatically. At this critical juncture, even minuscule additions of fluid volume (as little as 1 to 2 milliliters) result in exponential spikes in intracompartmental pressure.

This biomechanical reality explains why compartment syndrome can develop so rapidly and unpredictably following trauma. The unyielding nature of the fascia also dictates the surgical management: a limited or "mini-open" fasciotomy is biomechanically useless. To effectively alter the volume-pressure curve of the compartment, the fascia must be completely released along the entire length of the muscle belly. If the fascial incision is too short, the unreleased proximal and distal segments will continue to act as a tourniquet, leading to localized muscle necrosis despite a central release.
Furthermore, the epimysium—the connective tissue enveloping individual muscles—can also contribute to the containment of pressure. In severe cases, particularly involving the tibialis posterior muscle in the deep posterior compartment, releasing the overlying crural fascia and transverse septum may not be sufficient. The surgeon must meticulously inspect the individual muscle bellies; if a muscle remains pale and tense after the primary fascial release, an epimysiotomy (longitudinal scoring of the epimysium) is biomechanically required to achieve full decompression of the microvasculature.
Exhaustive Indications and Contraindications
Clinical Diagnosis and Thresholds
The diagnosis of acute compartment syndrome remains fundamentally clinical, heavily reliant on the surgeon’s acumen, serial examinations, and a high index of suspicion. The classic "Ps" of compartment syndrome—Pain out of proportion to the injury, Pain with passive stretch, Paresthesia, Pulselessness, Pallor, and Paralysis—are frequently taught but are not equally reliable. Pain out of proportion to the apparent injury and pain exacerbated by passive stretching of the involved compartment's muscles are the earliest and most sensitive clinical indicators. For example, severe pain upon passive plantarflexion of the ankle and toes strongly implicates the anterior compartment.

Paresthesia is the first objective sign, reflecting the extreme sensitivity of peripheral nerves to ischemia. Decreased two-point discrimination or altered light touch sensation in the specific nerve distribution of the affected compartment (e.g., the first dorsal web space for the anterior compartment) mandates immediate attention. Conversely, pulselessness, pallor, and paralysis are late, ominous signs indicating advanced, often irreversible ischemia. Waiting for the loss of a pulse to diagnose compartment syndrome is a catastrophic error, as tissue necrosis occurs at pressures far below those required to occlude a major artery.
When the clinical picture is equivocal—such as in polytrauma patients, intubated or sedated patients, young children, or patients with regional anesthesia—intracompartmental pressure (ICP) monitoring becomes indispensable. The absolute pressure threshold for fasciotomy has historically been debated (previously considered 30 mm Hg absolute pressure). However, modern orthopaedic consensus relies on the "Delta P" concept (ΔP). The Delta P is calculated by subtracting the compartment pressure from the patient's diastolic blood pressure (ΔP = Diastolic BP - Compartment Pressure). A Delta P of 30 mm Hg or less is a definitive indication for emergent fasciotomy.
Absolute and Relative Indications
The decision to perform a fasciotomy must be made swiftly, balancing the devastating consequences of a missed diagnosis against the morbidity of the procedure itself. Absolute indications for fasciotomy include an unequivocal clinical diagnosis of ACS in an awake, alert patient, regardless of pressure measurements. If a patient with a tibial shaft fracture exhibits escalating pain out of proportion, exquisite pain on passive stretch, and new-onset paresthesias, the patient must be taken to the operating room immediately.

Another absolute indication is an objective Delta P measurement of ≤ 30 mm Hg in an unresponsive, intubated, or uncooperative patient where a reliable clinical examination is impossible. In cases of acute arterial occlusion with prolonged ischemia (typically > 4-6 hours), prophylactic fasciotomy is strongly indicated at the time of vascular repair, as the subsequent reperfusion injury will inevitably lead to massive cellular edema and secondary compartment syndrome.
Relative indications include a rising trend in compartment pressures that are approaching the Delta P threshold, or a patient with a high-risk injury (e.g., high-energy tibial plateau fracture) who requires urgent transport to another facility where serial examinations cannot be reliably performed. In these scenarios, a prophylactic fasciotomy may be the safest course of action to prevent irreversible damage during transport. The threshold for intervention should also be lowered in hypotensive patients, as their decreased diastolic blood pressure severely compromises their Delta P, making them susceptible to muscle necrosis at much lower absolute compartment pressures.
Contraindications and Late Presentations
While the threshold to perform a fasciotomy should generally be low, there is one critical scenario where fasciotomy is absolutely contraindicated: the missed, late-presenting compartment syndrome where the muscle is already dead. Animal models and clinical studies have conclusively demonstrated that irreversible muscle necrosis occurs after 8 to 12 hours of continuous ischemia. If a patient presents with a rigid, painless limb, absent motor function, and absent sensation that has been present for more than 24 to 48 hours, the compartment syndrome has run its course.

Performing a fasciotomy in this late stage is not only futile but highly dangerous. Opening a compartment of necrotic muscle exposes the dead tissue to hospital-acquired pathogens, almost guaranteeing a severe, life-threatening infection. This scenario frequently leads to sepsis, necessitating an urgent, higher-level amputation, and carries a significant risk of mortality. In these tragic cases of established myonecrosis, the standard of care is to leave the compartments closed, allow the necrotic muscle to fibrose (which will eventually result in a Volkmann's ischemic contracture), or proceed directly to amputation if systemic toxicity (crush syndrome) dictates.
Relative contraindications include overlying active soft tissue infections (e.g., cellulitis or necrotizing fasciitis), though in the face of true ACS, the mechanical decompression takes precedence, and the infection is managed concomitantly with aggressive debridement and antibiotics. Severe coagulopathy is a challenge but not a strict contraindication; the coagulopathy must be aggressively reversed with blood products while the fasciotomy is performed, as the release of pressure is life-saving.
| Indication Category | Specific Clinical Scenarios | Action / Recommendation |
|---|---|---|
| Absolute Indications | Unequivocal clinical exam (Pain out of proportion, passive stretch pain); Delta P ≤ 30 mmHg in obtunded patient; Reperfusion after >6 hours of ischemia. | Emergent 4-compartment fasciotomy. Do not delay for imaging. |
| Relative Indications | Approaching Delta P threshold with worsening trend; High-risk injury requiring prolonged transport; Hypotensive polytrauma patient. | Prophylactic fasciotomy or continuous invasive ICP monitoring. |
| Absolute Contraindications | Late presentation (>24-48 hours) with established myonecrosis (rigid, insensate, painless limb). | Do NOT open compartments. Manage systemically; consider amputation. |
| Relative Contraindications | Overlying severe infection; Profound, uncorrected coagulopathy. | Proceed with caution. Correct coagulopathy concurrently. |
Pre-Operative Planning, Templating, and Patient Positioning
Diagnostic Modalities and Pressure Monitoring
When the clinical diagnosis is ambiguous, objective measurement of intracompartmental pressures is the gold standard diagnostic modality. The most commonly utilized device is a handheld, solid-state transducer (e.g., the Stryker Intra-Compartmental Pressure Monitor). It is imperative that the surgeon accurately places the needle or slit catheter into the specific compartment of concern. For the lower leg, all four compartments must be measured, ideally within 5 cm of the zone of maximum injury or fracture, as pressures can vary significantly along the length of the compartment.

Continuous pressure monitoring via an indwelling slit catheter is highly recommended for obtunded polytrauma patients or those with severe head injuries. This allows for real-time calculation of the Delta P as the patient's systemic blood pressure fluctuates during resuscitation. The surgeon must coordinate closely with the anesthesia team to ensure an accurate, continuous arterial line blood pressure reading is available. Relying on intermittent, non-invasive blood pressure cuffs can lead to erroneous Delta P calculations, especially in the hemodynamically labile trauma patient.
Advanced imaging modalities, such as MRI or ultrasound, have no role in the acute diagnosis of compartment syndrome. The time required to obtain an MRI is prohibitive and violates the core principle of emergent intervention. While ultrasound can demonstrate fascial bowing or altered muscle echogenicity, it lacks the sensitivity and specificity required to justify surgical intervention. The diagnosis remains tethered to the clinical exam and direct pressure transduction.
Anesthetic Considerations and Resuscitation
The anesthetic management of a patient with suspected or confirmed compartment syndrome requires meticulous coordination. The use of regional anesthesia (e.g., epidural or peripheral nerve blocks) in patients at high risk for ACS is highly controversial. Regional blocks provide excellent analgesia but can completely mask the cardinal symptom of ACS—pain out of proportion. Furthermore, the sympathectomy induced by regional anesthesia causes vasodilation, which can transiently increase blood flow to the limb, exacerbating edema and increasing intracompartmental pressure. Most orthopaedic traumatologists strongly advocate against the use of regional blocks in high-risk lower extremity fractures.

Systemic resuscitation is a critical component of pre-operative planning. Patients with ACS are at extreme risk for rhabdomyolysis and subsequent myoglobinuric renal failure. Aggressive intravenous fluid resuscitation with isotonic crystalloids must be initiated immediately to maintain a high urine output (target > 100 mL/hr). Alkalinization of the urine with sodium bicarbonate may be considered to prevent the precipitation of myoglobin in the renal tubules, though its efficacy compared to aggressive volume expansion alone is debated.
The anesthesia team must also be prepared for the systemic release of potassium and lactic acid that occurs immediately upon fascial release (reperfusion syndrome). This sudden influx of metabolites can precipitate severe cardiac arrhythmias and profound metabolic acidosis. Continuous ECG monitoring and the immediate availability of calcium gluconate, insulin/dextrose, and sodium bicarbonate are essential during the induction and initial surgical release.
Patient Positioning and Surgical Preparation
Proper patient positioning is vital for a swift and comprehensive four-compartment release. The patient is positioned supine on a radiolucent operating table. A bump (sandbag or rolled blankets) is placed under the ipsilateral hip to internally rotate the leg, bringing the posteromedial aspect of the tibia into clear view for the medial incision. The entire lower extremity, from the toes to the proximal thigh, is prepped and draped in a sterile fashion to allow for full mobility of the knee and ankle during the procedure.

The use of a pneumatic tourniquet is a critical decision point. In general, the use of a tourniquet should be strictly avoided if possible, as it induces further global ischemia to an already dying limb. However, in cases of massive trauma with life-threatening hemorrhage, a tourniquet may be applied but should be inflated only for the absolute minimum time required to achieve hemostasis. Once the major vessels are controlled, the tourniquet must be deflated immediately to allow for the assessment of muscle viability and the restoration of perfusion.
Surgical instruments should be prepared in advance, including long Metzenbaum scissors, fasciotomes, and a robust self-retaining retractor system. The surgeon must also anticipate the need for fracture stabilization. If the ACS is secondary to a tibial shaft fracture, the fasciotomy is performed first to restore perfusion, immediately followed by skeletal stabilization, typically with an unreamed intramedullary nail or a spanning external fixator, depending on the patient's physiological status and the degree of soft tissue compromise.
Step-by-Step Surgical Approach and Fixation Technique
Dual-Incision Fasciotomy Technique
The gold standard for the treatment of lower extremity acute compartment syndrome is the dual-incision, four-compartment fasciotomy. This technique provides complete, unhindered access to all compartments and allows for thorough visual inspection of the muscle bellies. The procedure begins with the anterolateral incision to decompress the anterior and lateral compartments. A longitudinal incision, approximately 15 to 20 cm in length, is made centered exactly halfway between the tibial crest and the fibular shaft.

Subcutaneous dissection is carried down to the crural fascia. The surgeon must meticulously identify and protect the superficial peroneal nerve, which typically exits the lateral compartment fascia in the distal third of the leg, though anatomical variations are common. Once the nerve is protected, a transverse nick is made in the fascia to identify the anterior intermuscular septum. The anterior compartment fascia is then released longitudinally utilizing long scissors, extending proximally to the tibial tubercle and distally to the extensor retinaculum. The lateral compartment is subsequently released in a similar fashion, remaining posterior to the septum and extending towards the lateral malleolus.

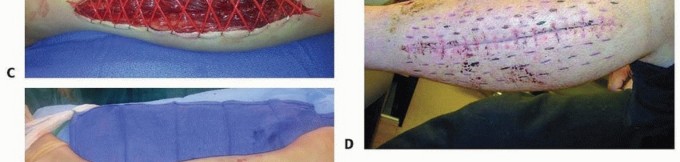
The posteromedial incision is then executed to decompress the superficial and deep posterior compartments. A 15 to 20 cm longitudinal incision is made 2 cm posterior to the posteromedial border of the tibia. This offset is critical to prevent exposing the medial face of the tibia, which would rapidly desiccate and complicate future soft tissue coverage. The
Clinical & Radiographic Imaging Archive








