Comprehensive Introduction and Patho-Epidemiology
The Pathomechanics of Acetabular Dysplasia
The normal growth and maturation of the pediatric acetabulum represent a highly orchestrated, delicate balance of biomechanical forces and biological potential. It requires all of its primary growth centers—the ilium, ischium, and pubis, which converge at the triradiate cartilage complex—to remain open, highly vascularized, and functioning normally. Critically, the femoral head must remain concentrically reduced and stable within the acetabular vault to provide the necessary spherical template for normal development. The dynamic interplay between the spherical femoral head and the developing acetabulum follows the Hueter-Volkmann principle, where concentric pressure stimulates appropriate cartilaginous growth and ossification.
If these critical growth centers are compromised, either pathologically through congenital malformation, neuromuscular imbalance, or iatrogenically, normal development is invariably arrested. Furthermore, if the femoral head is subluxated or frankly dislocated, the lack of concentric mechanical stimulation leads to a shallow, capacious, and maloriented acetabulum—the hallmark of hip dysplasia. This pathoanatomy is characterized by an elevated acetabular index, deficient anterior and lateral coverage, and hypertrophy of the pulvinar and ligamentum teres. The capsular structures become redundant, and the labrum may become inverted, further blocking concentric reduction and perpetuating the cycle of dysplasia.
The natural history of untreated or inadequately treated developmental dysplasia of the hip (DDH) is predictably grim. It inexorably leads to progressive subluxation, joint incongruity, and altered contact mechanics. The resulting edge-loading phenomenon dramatically increases peak articular contact stresses, culminating in early-onset osteoarthritis, often manifesting in the second or third decade of life. The primary goal of pericapsular osteotomies is to decisively interrupt this natural history. By reshaping the acetabulum and increasing its volume, we provide the much-needed anterior and lateral coverage, restoring joint stability, normalizing contact pressures, and facilitating ongoing normal hip development.




Evolution of Pericapsular Osteotomies
The surgical management of the dysplastic hip has evolved significantly over the past century, transitioning from simple salvage procedures to sophisticated, biomechanically sound reconstructive techniques. Early interventions often relied on extra-articular shelf arthroplasties, which provided static buttressing but failed to restore true articular congruity or harness the remaining growth potential of the pediatric hip. The paradigm shifted dramatically with the introduction of redirectional osteotomies, most notably the Salter innominate osteotomy, which reorients the entire acetabulum by hinging at the pubic symphysis. However, the Salter osteotomy does not alter the shape or volume of the acetabulum, making it less ideal for the capacious, severely dysplastic hip.
Recognizing the limitations of purely redirectional procedures, Paul Pemberton in 1965 and Wiktor Dega in 1969 introduced their respective pericapsular osteotomies. These are fundamentally reshaping procedures, designed to hinge directly through the flexible triradiate cartilage. Unlike complete transiliac cuts, these incomplete osteotomies allow the surgeon to bend the acetabular roof downwards and laterally, effectively decreasing the radius of curvature of the acetabulum and increasing its concavity. This is particularly advantageous in DDH, where the acetabulum is often excessively large relative to the femoral head.
While both the Pemberton and Dega osteotomies share the common goal of reshaping the acetabulum via a triradiate hinge, they differ profoundly in their execution and biomechanical effects. The Pemberton osteotomy is a bicortical cut through the anterior and middle portions of the ilium that curves inferiorly to bisect the posterior column, terminating at the ilioischial limb of the triradiate cartilage. It provides excellent anterior and lateral coverage. Conversely, the classic Dega osteotomy leaves the inner table of the ilium and the posterior column intact, hinging on this intact medial cortex and the triradiate cartilage. This allows for excellent lateral and posterior coverage, making it historically favored in neuromuscular dysplasia, though modern modifications have blurred these distinct boundaries.
Detailed Surgical Anatomy and Biomechanics
Osteology and the Triradiate Cartilage Complex
The acetabulum is a complex hemispherical socket formed by the confluence of the ilium, ischium, and pubis. In the pediatric patient, these three distinct ossification centers are separated by the Y-shaped triradiate cartilage complex. This cartilaginous structure is not merely a growth plate; in the context of pericapsular osteotomies, it serves as the critical, flexible hinge that permits the reshaping of the acetabular roof. A thorough understanding of the three limbs of the triradiate cartilage—the ilioischial, iliopubic, and ischiopubic limbs—is absolutely essential for the safe and effective execution of these procedures.
The ilium provides the superior dome of the acetabulum and is the primary site of surgical intervention for both Pemberton and Dega osteotomies. The anterior superior iliac spine (ASIS) and the anterior inferior iliac spine (AIIS) serve as critical superficial and deep landmarks, respectively. The AIIS is the origin of the direct head of the rectus femoris and marks the starting point for the osteotomy cuts. Posteriorly, the ilium thickens to form the sciatic buttress and the greater sciatic notch, a region of immense surgical peril due to the proximity of major neurovascular structures.
Biomechanically, the success of a reshaping osteotomy relies entirely on the plasticity of the triradiate cartilage. If the cartilage is prematurely closed or severely traumatized during the procedure, the hinge mechanism is lost, and the osteotomy will either fail to mobilize or will result in an intra-articular fracture. The Pemberton osteotomy, by cutting completely through the posterior column, relies heavily on the flexibility of the iliopubic and ischiopubic limbs to allow the acetabular roof to hinge downward. The Dega osteotomy, by preserving the inner table and posterior column, creates a more constrained hinge that forces the lateral edge of the acetabulum downward, utilizing the intact medial cortex as a fulcrum.




Musculotendinous Intervals and Surgical Windows
Accessing the pediatric pelvis requires precise navigation through complex musculotendinous layers. The standard approach for pericapsular osteotomies is the Smith-Petersen (anterolateral) approach, which utilizes the internervous plane between the femoral nerve (sartorius and rectus femoris) and the superior gluteal nerve (tensor fasciae latae and gluteus medius). Superficially, the dense fascia lata must be incised. To minimize the risk of injury to the lateral femoral cutaneous nerve, this incision is best made slightly lateral to the intermuscular septum, directly over the muscle belly of the tensor fasciae latae.
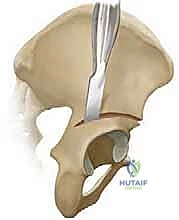
Deep to the superficial fascia, the interval between the tensor fasciae latae laterally and the sartorius medially is developed. This exposes the rectus femoris muscle, which originates via two distinct heads. The direct head originates from the AIIS, while the reflected head originates from the superior rim of the acetabulum and the anterior joint capsule. Release or mobilization of the direct head from the AIIS is almost always required to achieve adequate exposure of the critical starting point for the osteotomy.
The reflected head of the rectus femoris is a vital anatomical landmark. It acts as a reliable guide to the superior border of the hip capsule. Identifying and protecting the capsule is paramount, as inadvertent capsulotomy or intra-articular extension of the osteotomy can lead to devastating complications, including joint stiffness and chondrolysis. Subperiosteal dissection is then meticulously carried out along the inner and outer tables of the iliac wing. This dissection must remain strictly subperiosteal to minimize bleeding and protect the adjacent neurovascular structures, particularly as the dissection proceeds posteriorly toward the sciatic notch.
Neurovascular Topography and At-Risk Structures
The pericapsular region is replete with critical neurovascular structures, making vigilance non-negotiable. The Lateral Femoral Cutaneous Nerve (LFCN) is highly variable in its course and is the most frequently injured structure during the initial exposure. It typically emerges from under the lateral aspect of the inguinal ligament, crosses the iliac crest, and runs either over or through the sartorius or tensor fasciae latae. It is highly susceptible to traction injury during fascial incision and retraction. Gentle, broad retraction and avoiding sharp, focal pressure are essential to preserve its function.
Deep within the pelvis, the sciatic nerve, the largest nerve in the body, lies in extreme peril during the posterior cuts of both osteotomies. It exits the pelvis through the greater sciatic foramen and lies intimately close to the posterior column of the ilium. When performing a Pemberton osteotomy, which requires bisecting the posterior column, the osteotome is directed blindly toward the sciatic notch. Meticulous subperiosteal dissection and the precise placement of broad, curved Chandler retractors or sciatic notch retractors, both medially and laterally, are absolutely critical to create a physical barrier protecting the nerve.
Furthermore, the Superior Gluteal Artery and Nerve exit the pelvis superior to the piriformis muscle, in close proximity to the apex of the greater sciatic notch. These structures are vulnerable during deep posterior dissection and aggressive osteotome advancement. Medially, the Femoral Neurovascular Bundle (femoral nerve, artery, and vein) lies medial to the sartorius and anterior to the iliopsoas. While less directly threatened by the iliac bone cuts, excessive medial retraction or uncontrolled deep dissection anteriorly can jeopardize these structures, leading to catastrophic hemorrhage or profound motor deficits.
Exhaustive Indications and Contraindications
Patient Selection Criteria
The ideal candidate for a pericapsular osteotomy is a pediatric patient with documented, progressive acetabular dysplasia who has failed non-operative management or prior closed/open reduction attempts. Age is a critical determinant. The lower age limit is generally considered to be 18 to 24 months, as younger infants may still exhibit spontaneous remodeling potential, and the soft, cartilaginous nature of the infant pelvis makes stable fixation of the osteotomy difficult. The upper age limit is dictated entirely by the status of the triradiate cartilage. Once the triradiate cartilage complex begins to fuse—typically around 10 to 12 years in girls and 12 to 14 years in boys—the essential hinge mechanism is lost, and a reshaping osteotomy is absolutely contraindicated.
Clinical indications include persistent dysplasia characterized by a shallow acetabulum, an elevated acetabular index (typically greater than 25-30 degrees in a toddler), and deficient anterior or lateral coverage of the femoral head. These procedures are particularly useful when a large volume reduction of the acetabular vault is required to match a relatively small or normally sized femoral head. It is frequently performed concomitantly with open reduction of the hip and femoral shortening/derotational osteotomies in older children presenting with neglected or late-diagnosed developmental dysplasia of the hip.
A crucial prerequisite for any pericapsular osteotomy is a concentrically reduced or reducible femoral head. If the hip cannot be concentrically reduced due to intra-articular obstacles (e.g., inverted labrum, hypertrophic pulvinar, tight transverse acetabular ligament) or severe capsular contracture, an open reduction must be performed prior to or simultaneously with the osteotomy. Performing an osteotomy over a subluxated or dislocated femoral head will inevitably lead to increased joint contact pressures, rapid cartilage destruction, and severe osteoarthritis. Furthermore, the absence of significant avascular necrosis (AVN) of the femoral head is preferred, as the increased pressure generated by the osteotomy could theoretically exacerbate existing ischemia.
Comparative Indications: Pemberton versus Dega
While both procedures are reshaping osteotomies, subtle biomechanical differences dictate their optimal application. The Pemberton osteotomy, by cutting through the posterior column, allows for a more dramatic anterior and lateral rotation of the acetabular roof. This makes it exceptionally well-suited for classic Developmental Dysplasia of the Hip (DDH), where the primary deficiency is typically anterolateral. The Pemberton provides excellent correction of the acetabular index and significantly improves anterior coverage, making it the workhorse for DDH in the toddler and young child.
Conversely, the classic Dega osteotomy preserves the posterior column and hinges on the intact medial cortex of the ilium. This configuration forces the lateral and posterior aspects of the acetabulum downward. Consequently, the Dega osteotomy is historically favored in the management of neuromuscular hip dysplasia, particularly in patients with Cerebral Palsy (CP). In neuromuscular dysplasia, the typical pattern of deficiency is posterosuperior, driven by the spasticity of the adductor and flexor musculature. The Dega osteotomy effectively addresses this specific morphological defect.
However, modern pediatric orthopedic practice has seen a convergence of these techniques. Modified Dega osteotomies, which involve more extensive anterior cuts, are frequently used for DDH, while modified Pemberton techniques can be tailored for neuromuscular cases. The choice often relies on the surgeon's training, comfort level, and the specific three-dimensional morphology of the dysplasia as defined by advanced preoperative imaging.
| Parameter | Pemberton Osteotomy | Dega Osteotomy |
|---|---|---|
| Primary Indication | Developmental Dysplasia of the Hip (DDH) | Neuromuscular Dysplasia (e.g., Cerebral Palsy) |
| Primary Deficiency Addressed | Anterolateral deficiency | Posterosuperior and lateral deficiency |
| Posterior Column Status | Bisected (cut entirely through) | Intact (inner table preserved) |
| Hinge Mechanism | Ilioischial and Ischiopubic limbs of TRC | Intact medial cortex and TRC |
| Absolute Contraindication | Closed Triradiate Cartilage | Closed Triradiate Cartilage |
| Relative Contraindication | Severe pre-existing stiffness/AVN | Severe pre-existing stiffness/AVN |
Pre-Operative Planning, Templating, and Patient Positioning
Radiographic Assessment and Advanced Imaging
Meticulous preoperative planning begins with a comprehensive radiographic evaluation. High-quality, properly positioned Anteroposterior (AP) pelvis radiographs are mandatory. The pelvis must be neutral, without excessive tilt or rotation, as these positional errors can artificially alter the perceived acetabular indices. On the AP radiograph, the surgeon must calculate the Acetabular Index (AI), the Lateral Center-Edge Angle (LCEA) of Wiberg, and assess the integrity of Shenton's line. The teardrop should be evaluated for symmetry and shape, as a widened or V-shaped teardrop often indicates lateralization of the femoral head and capsular interposition.
In addition to the standard AP view, a false profile view of Lequesne and de Sèze is invaluable for assessing anterior acetabular coverage. This view allows for the measurement of the Anterior Center-Edge Angle (ACEA). For complex deformities, particularly in revision scenarios or severe neuromuscular dysplasia, advanced cross-sectional imaging with a Computed Tomography (CT) scan is highly recommended. Three-dimensional CT reconstructions provide unparalleled visualization of the acetabular morphology, allowing the surgeon to precisely map the areas of maximal deficiency and plan the exact trajectory of the osteotomy cuts.
Dynamic hip ultrasound is generally reserved for infants under 6 months of age and has limited utility in planning pericapsular osteotomies in older children. However, Magnetic Resonance Imaging (MRI) can be particularly useful in assessing the status of the cartilaginous anlage, the presence of an inverted labrum, and the vascularity of the femoral head. Recognizing early signs of avascular necrosis (AVN) is critical, as it may alter the surgical decision-making process, potentially delaying the osteotomy or necessitating a concomitant femoral shortening to decompress the joint.




Templating the Osteotomy Trajectory
Surgical templating is a critical step that bridges preoperative imaging with intraoperative execution. Using digital templating software or traditional acetate overlays on calibrated radiographs, the surgeon must simulate the osteotomy. The starting point at the Anterior Inferior Iliac Spine (AIIS) is identified. For a Pemberton osteotomy, the trajectory is mapped to curve inferiorly and posteriorly, bisecting the posterior column and aiming directly for the ilioischial limb of the triradiate cartilage. The angle of the cut relative to the pelvic brim dictates the degree of lateral versus anterior coverage achieved.
For a Dega osteotomy, the templating focuses on the trajectory through the outer table of the ilium while ensuring the inner table remains inviolate. The cut is planned to start at the AIIS and sweep posteriorly, staying approximately 1.5 to 2 centimeters superior to the acetabular rim. The depth of the cut is critical; it must penetrate the cancellous bone but stop meticulously short of the medial cortex. Templating also helps estimate the size and shape of the required tricortical bone graft, which will be harvested from the ipsilateral anterior iliac crest to maintain the osteotomy in its open, corrected position.
Furthermore, templating must account for any necessary concomitant procedures. If the hip is subluxated, a femoral shortening and derotational osteotomy (VDRO) must be templated to ensure concentric reduction without excessive joint contact pressure. The amount of femoral shortening required is calculated to allow the femoral head to rest comfortably in the true acetabulum without tension on the neurovascular structures or the repaired capsule.
Anesthesia, Positioning, and Fluoroscopic Setup
The procedure is performed under general endotracheal anesthesia, supplemented by a regional block (such as an epidural or a lumbar plexus block) to optimize postoperative pain management and minimize systemic narcotic requirements. Muscle relaxation is essential to facilitate the reduction of the hip and the exposure of the pelvis. Intravenous antibiotics are administered prior to skin incision, and a Foley catheter is placed to decompress the bladder and monitor urine output during the procedure.
Patient positioning is critical for both surgical access and accurate fluoroscopic imaging. The patient is positioned supine on a fully radiolucent operating table. A small bump or sandbag is placed under the ipsilateral flank and hemipelvis to elevate the operative side slightly, typically about 15 to 20 degrees. This allows the abdominal contents to fall away from the iliac fossa, facilitating the medial subperiosteal dissection. The entire lower extremity, from the iliac crest to the toes, is prepped and draped free to allow for dynamic assessment of hip stability and range of motion throughout the procedure.
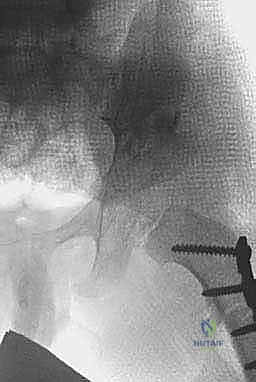
The fluoroscopic C-arm is brought in from the contralateral side of the table. Before the incision is made, orthogonal views (AP and true lateral of the pelvis) must be obtained and verified. The ability to quickly and reliably obtain a clear AP view of the pelvis, visualizing the teardrop, the triradiate cartilage, and the sciatic notch, is non-negotiable. The C-arm monitor must be positioned directly in the surgeon's line of sight. Intraoperative fluoroscopy is not merely a confirmatory tool; it is actively used to guide the osteotome during the posterior, blind portions of the cuts, ensuring the trajectory remains superior to the joint line and safely away from the sciatic notch.
Step-by-Step Surgical Approach and Fixation Technique
The Anterolateral Approach (Smith-Petersen Modification)
The surgical approach begins with a carefully planned incision. While a classic longitudinal Smith-Petersen incision can be used, a "bikini" incision parallel to the iliac crest provides a vastly superior cosmetic result while affording excellent exposure. The incision starts just below the middle of the iliac crest and extends anteriorly and medially toward the anterior superior iliac spine (ASIS), curving slightly downward. Subcutaneous tissues are divided in line with the incision down to the fascia lata.
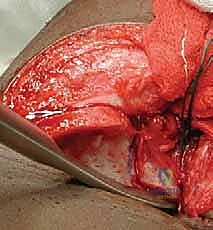
The fascia is incised slightly lateral to the intermuscular interval to protect the lateral femoral cutaneous nerve (LFCN). The interval between the tensor fasciae latae and the sartorius is identified and developed by blunt dissection. The ASIS is identified, and the origin of the sartorius may be partially released if necessary for exposure. The dissection proceeds deeply to expose the rectus femoris. The direct head of the rectus femoris, originating from the anterior inferior iliac spine (AIIS), is identified, tagged with a heavy suture, and tenotomized to expose the inferior aspect of the ilium and the superior hip capsule.
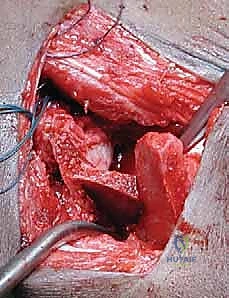
Meticulous subperiosteal dissection is then initiated. The iliac apophysis is split longitudinally along its crest. Using a Cobb elevator, the periosteum and the iliacus muscle are stripped from the inner table of the ilium down to the pelvic brim and posteriorly toward the sciatic notch. Similarly, the gluteal musculature is stripped from the outer table of the ilium down to the superior capsule and posteriorly to the sciatic notch. Broad, curved retractors (such as Chandler or Taylor retractors) are carefully placed subperiosteally into the sciatic notch, both medially and laterally, to protect the sciatic nerve and superior gluteal vessels.




Execution of the Pemberton Osteotomy
With the inner and outer tables exposed and retractors securely in place, the Pemberton osteotomy commences. The starting point is approximately 10 to 15 millimeters superior to the AIIS and the reflected head of the rectus femoris. Using a narrow, curved osteotome (typically 1/4 or 3/8 inch), the cut is initiated on the outer table. The trajectory is directed posteriorly and inferiorly, aiming precisely toward the ilioischial limb of the triradiate cartilage.
The osteotomy is progressively deepened, cutting through both the inner and outer cortices (the anterior and middle columns of the ilium). As the cut proceeds posteriorly, it must bisect the posterior column. This is the most critical and dangerous portion of the procedure. The osteotome is advanced slowly, with frequent fluoroscopic checks to ensure the trajectory is correct and that the instrument does not inadvertently plunge into the sciatic notch or violate the hip joint capsule. The surgeon must rely on tactile feedback, feeling the resistance of the dense cortical bone of the posterior column.
Once the posterior column is completely bisected, a laminar spreader is carefully inserted into the osteotomy site anteriorly. Gentle, progressive opening of the spreader hinges the acetabular roof downward and laterally, pivoting on the flexible iliopubic and ischiopubic limbs of the triradiate cartilage. The surgeon will hear and feel a distinct "crunch" as the greenstick fracture of the posterior hinge occurs. The hip is then reduced, and the adequacy of coverage is assessed both directly and fluoroscopically.