Comprehensive Introduction and Patho-Epidemiology
The Salter Innominate Osteotomy (SIO) stands as a monumental cornerstone procedure in pediatric orthopaedic surgery, designed specifically to address the complex pathomorphology of developmental dysplasia of the hip (DDH). Introduced by Dr. Robert B. Salter in 1961, this procedure represented a paradigm shift from palliative salvage operations to true biomechanical redirection of the acetabulum. This is not merely an exercise in cutting bone; it is a profound intervention aimed at understanding and manipulating the biomechanics of the developing pediatric pelvis, restoring articular congruity, and ultimately setting a child on a trajectory for a lifetime of pain-free, native hip function. The SIO is most frequently executed in conjunction with an open reduction for a dislocated hip in DDH, yet it remains an exceptionally powerful tool for addressing residual acetabular dysplasia even in the setting of a concentrically reduced joint. Our definitive surgical goal is unambiguous: to structurally redirect the acetabulum as a single unit, thereby dramatically improving anterior and lateral femoral head coverage and correcting the inherent spatial orientation of the dysplastic socket.
Before we even consider the surgical incision, we must comprehensively grasp the patho-epidemiology and pathomechanics that necessitate our intervention. Acetabular dysplasia is not a static deformity but a dynamic failure of development stemming from several interconnected primary drivers. The most critical factor is the absence of a concentrically reduced, spherical femoral head within the growing acetabulum. The acetabulum fundamentally requires the femoral head to act as a physical and biomechanical template for proper, reciprocal development. When the head is subluxated or dislocated, this crucial templating effect is lost. Furthermore, abnormal interstitial and appositional growth occurs within the acetabular and triradiate cartilage complexes. This altered growth vector leads to a shallow, morphologically deficient, and often excessively anteverted socket that fails to provide adequate structural support for the femoral head during weight-bearing activities.
Compounding these structural deficiencies is the abnormal development of the secondary centers of ossification. The ilium, pubis, and ischium fail to ossify at normal rates or in normal spatial configurations, directly contributing to the dysplastic morphology of the hemipelvis. Soft tissue interposition further complicates the pathology. In a developmentally dislocated hip, the acetabular labrum often flattens, hypertrophies, and inverts, forming what is known as a "neolimbus." This fibrotic ridge, along with a hypertrophied pulvinar, an elongated ligamentum teres, and a contracted transverse acetabular ligament, creates a formidable mechanical obstruction to concentric reduction. The SIO addresses the bony deficiency, but its success is entirely predicated on the concurrent or pre-existing management of these soft tissue obstacles.
The natural history of an untreated or persistently dysplastic hip, particularly in the presence of subluxation, is unequivocally grim. Aberrant joint contact forces lead to accelerated wear of the articular cartilage. Patients inevitably develop insidious pain, functional disability, and progressive secondary osteoarthrosis. In cases of severe subluxation, these degenerative changes can manifest as early as the patient's third decade of life. Even in the absence of frank subluxation, subtle but persistent dysplasia significantly alters the biomechanical loading of the hip joint, frequently culminating in end-stage osteoarthrosis by the fifth or sixth decade. Our surgical intervention with the Salter Innominate Osteotomy is a prophylactic strike, aiming to normalize joint mechanics, maximize the weight-bearing surface area, and definitively prevent this predictable cascade of joint destruction.
Detailed Surgical Anatomy and Biomechanics
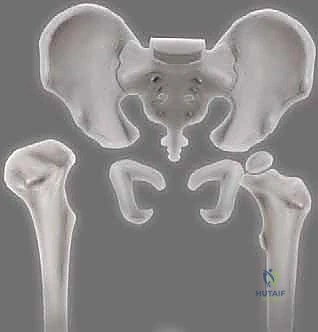
To execute the Salter Innominate Osteotomy safely and effectively, the surgeon must possess an intimate, three-dimensional understanding of pediatric pelvic osteology and the surrounding neurovascular topography. The SIO is biomechanically unique among pelvic osteotomies because it relies on the rotation of the entire distal innominate fragment around a precise, anatomically defined axis. This hinge axis runs obliquely from the posterior cortex of the sciatic notch to the flexible, cartilaginous midpoint of the symphysis pubis. By pivoting the distal fragment around this axis, the osteotomy effectively redirects the entire acetabular complex as a single structural unit. This redirection converts a sloped, dysplastic roof into a horizontal, stable weight-bearing surface, dramatically improving anterior and lateral coverage of the femoral head. During the redirection maneuver, the distal fragment undergoes a complex spatial translation: it moves distally, posteriorly, and medially. This multiplanar shift is what fundamentally corrects the abnormal anteversion and lack of lateral coverage inherent to DDH.
The surgical approach demands precise navigation through specific muscular intervals. We utilize a modified anterior Smith-Petersen approach, exploiting the internervous and intermuscular plane between the sartorius muscle (innervated by the femoral nerve) medially and the tensor fasciae latae (innervated by the superior gluteal nerve) laterally. Deep to this superficial interval, the surgeon encounters the rectus femoris muscle. The direct head of the rectus femoris originates from the anterior inferior iliac spine (AIIS), while the reflected head originates from the superior lip of the acetabulum and the anterior hip capsule. Managing the rectus femoris, either by reflection or careful retraction, is critical for exposing the ilium down to the level of the joint capsule. The iliac apophysis, the iliac tubercle, and the AIIS serve as our primary tactile and visual landmarks for both the incision and the subsequent osteotomy. Throughout this exposure, the triradiate cartilage—the vital growth plate of the acetabulum—must be rigorously protected from both direct mechanical injury and thermal necrosis.
Navigating the neurovascular landscape during this procedure is fraught with potential hazards that demand meticulous surgical technique. The Lateral Femoral Cutaneous Nerve (LFCN) is the first structure at risk. This purely sensory nerve pierces the fascia lata and exhibits highly variable branching patterns. It is exceptionally susceptible to iatrogenic injury during the initial skin incision, subcutaneous dissection, and subsequent medial retraction of the sartorius. The femoral nerve, located deeper and medial to the psoas muscle, is at risk during excessive, forceful, or prolonged retraction of the anterior structures, and is particularly vulnerable if an intramuscular psoas lengthening is performed without precise anatomical identification.
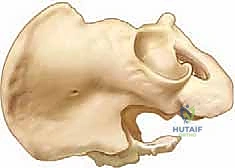
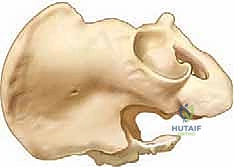
The most critical anatomical danger zone, however, lies within the greater sciatic notch. The superior gluteal artery and nerve exit the pelvis through the greater sciatic foramen, immediately superior to the piriformis muscle. The massive sciatic nerve, along with the inferior gluteal artery and nerve, exit inferior to the piriformis. When passing dissecting instruments, right-angle forceps, and ultimately the Gigli saw through the sciatic notch to initiate the osteotomy, these vital structures are at extreme risk of catastrophic injury. Strict, meticulous subperiosteal dissection along both the inner and outer tables of the ilium, coupled with the careful, visually confirmed placement of protective retractors (such as sciatic notch retractors or cautiously placed malleable retractors), is absolutely essential to shield these neurovascular bundles from the oscillating teeth of the Gigli saw.
Exhaustive Indications and Contraindications
The decision to proceed with a Salter Innominate Osteotomy requires rigorous patient selection based on strict clinical and radiographic criteria. The procedure is highly age-dependent, typically indicated for children between 18 months and 6 years of age. This specific chronological window is critical. Operating before 18 months is generally avoided because the infant pelvis lacks sufficient ossified bone stock to securely hold the fixation pins, and there is still a high potential for spontaneous acetabular remodeling if a concentric closed reduction is maintained. Conversely, operating beyond 6 to 8 years of age becomes progressively more challenging; the symphysis pubis loses its cartilaginous flexibility, making the required rotational redirection of the distal fragment biomechanically difficult or impossible without adding a concomitant pubic osteotomy.
The primary radiographic indication is a persistently elevated Acetabular Index (AI), indicative of a shallow, dysplastic socket. We expect normal AI values to be approximately 35 degrees at birth, decreasing to 25 degrees at 1 year, and settling near 20 degrees by 2 years of age. Any persistent elevation beyond these normative developmental milestones, particularly in the setting of subluxation or after a failed trial of nonoperative management, warrants strong consideration for an SIO. However, the most non-negotiable prerequisite for this procedure is a perfectly concentric hip reduction. The hip must be concentrically reduced, either preoperatively (confirmed via arthrogram) or achieved intraoperatively via a formal open reduction. Performing a Salter osteotomy on a hip that remains subluxated or dislocated is an exercise in futility; it will not stabilize the joint and will rapidly lead to failure, recurrent dislocation, and accelerated joint destruction.
Contraindications must be strictly observed to prevent disastrous outcomes. The SIO is fundamentally designed to correct anterior and lateral acetabular deficiency. Therefore, it is absolutely contraindicated in conditions characterized by posterior hip dysplasia. In neuromuscular conditions such as cerebral palsy or myelomeningocele, the acetabular deficiency is frequently posterosuperior. Because the SIO essentially retroverts the acetabulum to gain anterior coverage, performing this osteotomy in a neuromuscular patient will actively uncover the posterior aspect of the femoral head, directly precipitating a posterior dislocation. Furthermore, significant pre-existing osteoarthrosis or a stiff hip (lacking at least 100 degrees of flexion and 30 degrees of abduction) are strong contraindications, as the osteotomy relies on a mobile joint to function properly and cannot reverse established degenerative cartilage loss.
| Category | Salter Innominate Osteotomy Parameters |
|---|---|
| Primary Indications | DDH in children aged 18 months to 6 years; Persistent acetabular dysplasia (elevated AI); Concentrically reduced hip (or achievable via concurrent open reduction). |
| Absolute Contraindications | Lack of concentric reduction; Posterior acetabular dysplasia (e.g., Cerebral Palsy, Myelomeningocele); Severe osteoarthritis; Skeletal maturity/inflexible pubic symphysis. |
| Relative Contraindications | Age < 18 months (inadequate bone stock); Age > 8 years (stiff symphysis pubis); Severe joint stiffness (requires >100° flexion, >30° abduction). |
| Prerequisites | Concentric reduction confirmed by arthrogram or direct visualization; Adequate soft tissue releases (psoas, adductors) to prevent excessive joint reaction forces. |
For children under 18 months of age who achieve a successful closed reduction, the standard of care is observation and serial radiographic monitoring of the acetabular index for 12 to 18 months. The developing pelvis has a remarkable capacity for spontaneous remodeling once the femoral head is concentrically seated. If residual dysplasia persists despite this observation period, a delayed SIO is indicated. The decision to perform the osteotomy concurrently with an open reduction versus staging the procedures remains a topic of nuanced clinical debate, highly dependent on the surgeon's experience, the patient's age, and the severity of the dysplasia.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the blueprint for surgical success; it separates a precise, anatomical reconstruction from a chaotic, high-risk exploration. The diagnostic assessment begins with a thorough history, noting risk factors such as breech presentation, positive family history of DDH, and oligohydramnios. The physical examination, particularly in the ambulatory child, provides critical functional data. The surgeon must evaluate for the Galeazzi sign, noting unequal knee heights in the supine, flexed position, which indicates a limb length discrepancy secondary to proximal femoral migration. Limitation of hip abduction is a hallmark sign; normal infant abduction is approximately 80 degrees, and asymmetric or bilaterally restricted abduction strongly suggests pathology. In the walking child, a positive Trendelenburg sign or a compensatory gluteus medius lurch indicates abductor insufficiency due to the altered biomechanics of the dislocated or subluxated hip.
Radiographic evaluation is the cornerstone of preoperative templating. A high-quality standing anteroposterior (AP) pelvis radiograph is mandatory. On this view, we meticulously measure the acetabular index (AI), the angle formed by Hilgenreiner's line (a horizontal line connecting the inferior aspects of the triradiate cartilages) and a line drawn from the inferior margin of the ossified acetabulum to its lateral ossified margin. We also evaluate Shenton's line, a continuous arc formed by the medial cortex of the femoral neck and the superior margin of the obturator foramen. A break or discontinuity in this line is a highly sensitive indicator of proximal femoral migration and subluxation.
In addition to the AP view, a supine frog-leg lateral radiograph provides an orthogonal perspective of femoral head coverage. In older, ambulatory children, the false-profile view of Lequesne and de Sèze is exceptionally valuable for identifying subtle anterior acetabular dysplasia that might be missed on standard AP views. In complex cases, or in older children approaching the upper age limit for the procedure, advanced imaging such as a 3D CT scan or MRI can be invaluable. These modalities allow for precise volumetric assessment of the acetabulum, evaluation of the labrum and cartilage, and detection of complex multiplanar deformities (such as excessive retroversion) that might necessitate alternative osteotomy techniques.
Intraoperative decision-making begins before the skin is incised. A dynamic hip arthrogram is frequently the first step in the operating room. This is crucial for confirming a concentric reduction and assessing the sphericity of the femoral head and the volume of the acetabulum. If the arthrogram reveals an eccentric reduction, an open reduction must be performed first. Furthermore, we use fluoroscopy to estimate femoral anteversion. If anteversion exceeds 45 to 50 degrees, a concurrent proximal femoral derotational osteotomy (VDRO) is strongly considered, as excessive anteversion combined with an SIO can lead to anterior instability and a persistent, compensatory internal rotation gait.
Patient positioning is a critical, often underappreciated aspect of the procedure. The patient is placed supine on a radiolucent operating table. Crucially, a gel roll or a folded blanket is placed longitudinally under the thoracolumbar spine on the operative side. This maneuver elevates the affected hemipelvis into an oblique position, rotating the anterior ilium forward and presenting it much more favorably to the surgeon.

It is of paramount importance that this bump is placed under the thorax and spine, not directly under the affected pelvis itself. Placing the bump under the pelvis restricts the mobility of the hemipelvis, making the subsequent redirection maneuver significantly more difficult.

The patient is prepped extensively: proximally to the inferior rib cage, distally to include the entire lower extremity (allowing for full, unencumbered intraoperative range of motion), and from the midline anteriorly to the midline posteriorly. This wide sterile field ensures unimpeded access to the entire ilium for bone graft harvesting and allows the surgeon to freely manipulate the limb to assess reduction and stability. The fluoroscopy C-arm must be positioned to easily obtain both true AP and obturator oblique views of the pelvis, which are essential for guiding pin placement safely away from the joint space and the triradiate cartilage.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the Salter Innominate Osteotomy requires a symphony of precise dissection, calculated bone cuts, and biomechanical manipulation. We begin with a modified anterior Smith-Petersen approach. The skin incision follows the bikini line, starting 1 to 2 cm posterior to the Anterior Superior Iliac Spine (ASIS) and curving gently medially and distally toward the pubic tubercle. This curvilinear trajectory not only provides excellent, expansile exposure but also results in a cosmetically acceptable scar. As we deepen the incision through the subcutaneous tissue and Scarpa's fascia, meticulous hemostasis is maintained. The immediate priority is the identification and protection of the Lateral Femoral Cutaneous Nerve (LFCN). This nerve is notoriously variable; it typically exits medial to the ASIS but can drape across the anterior ilium. Gentle blunt dissection and careful placement of retractors are imperative to prevent traction neuropraxia or complete transection.
We then identify the fascial interval between the sartorius muscle medially and the tensor fasciae latae (TFL) laterally. The fascia is incised longitudinally over the TFL, just lateral to the interval, to avoid the LFCN. Retracting the sartorius medially and the TFL laterally exposes the deep structures. The rectus femoris muscle is identified originating from the Anterior Inferior Iliac Spine (AIIS). Depending on the need for a concurrent open reduction, the direct head of the rectus may be detached from the AIIS and tagged for later repair, or carefully retracted.
Attention is then turned to the iliac crest. The cartilaginous iliac apophysis is sharply incised longitudinally, directly down to the bone. Using a Cobb elevator, a rigorous subperiosteal dissection is performed. We strip the periosteum and the attached iliacus muscle from the inner table of the ilium, sweeping medially toward the sciatic notch. Concurrently, the abductor musculature (gluteus medius and minimus) is elevated subperiosteally from the outer table of the ilium. This subperiosteal plane is critical; straying from it results in massive hemorrhage and significantly increases the risk to neurovascular structures.
The exposure culminates at the greater sciatic notch. This is the most perilous phase of the operation. The subperiosteal dissection on both the inner and outer tables must meet at the notch.
A right-angle forceps (such as a Mixter or a specialized sciatic notch passer) is carefully passed from the inner table to the outer table through the notch. The tip of the instrument must remain in constant, intimate contact with the bone to ensure it passes deep to the periosteum, thereby safely excluding the superior gluteal vessels and the sciatic nerve from the operative field.

Once the forceps is successfully passed, a Gigli saw is grasped and pulled through the notch.

The osteotomy is performed using the Gigli saw, cutting from the sciatic notch straight anteriorly to emerge just superior to the AIIS. The surgeon must maintain a steady, continuous stroke, ensuring the cut is perpendicular to the ilium to prevent creating a sloped osteotomy that could lead to graft displacement.
Simultaneously, a triangular wedge of bone is harvested from the anterior aspect of the proximal iliac crest.

This bone graft is carefully fashioned using a rongeur or a saw to match the anticipated opening of the osteotomy site. The base of the wedge should correspond to the amount of anterior and lateral coverage required.
The redirection maneuver is the biomechanical heart of the procedure. A stout towel clip is placed securely into the anterior aspect of the distal innominate fragment (the AIIS region).

The surgeon applies a firm, sustained pull on the towel clip, directing the force distally, laterally, and anteriorly. This maneuver rotates the entire acetabular complex around the symphysis pubis hinge, effectively opening the osteotomy site anteriorly and laterally while keeping the posterior aspect (at the sciatic notch) closed as a hinge.

Once the desired redirection is achieved, the previously harvested, triangular bone graft is firmly impacted into the open osteotomy gap. The graft acts as a structural strut, maintaining the newly acquired acetabular orientation.
Fixation is achieved using two stout, threaded Steinmann pins or Kirschner wires. The pins are driven from the proximal iliac segment, across the bone graft, and deep into the distal fragment.

The trajectory of these pins is absolutely critical. They must be directed posteriorly and medially to ensure maximum purchase in the thick bone of the posterior column, while strictly avoiding penetration into the hip joint space or the triradiate cartilage.

Fluoroscopic imaging, particularly the obturator oblique view, is mandatory at this stage to definitively confirm intraosseous pin placement and verify that the joint space is free of hardware. The pins are cut short, leaving enough length outside the bone for easy removal later, and the wound is closed in meticulous layers, ensuring the cartilaginous apophysis is tightly reapproximated over the hardware.
Complications, Incidence Rates, and Salvage Management
While the Salter Innominate Osteotomy is a highly successful procedure in experienced hands, it is technically demanding and carries a steep learning curve. Complications, when they occur, can significantly compromise the final outcome and often require complex salvage interventions. The surgeon must be acutely aware of these risks and employ rigorous preventative strategies throughout the operation.
Pin-related complications are among the most frequently encountered issues. Pin migration, either backing out into the subcutaneous tissues or advancing into the hip joint or pelvic viscera, is a known risk, particularly if smooth pins are used or if the pins fail to gain adequate purchase in the dense bone of the posterior column. Threaded pins are strongly preferred to mitigate this risk. Superficial pin tract infections can occur but generally resolve with oral antibiotics and subsequent pin removal. Catastrophic pin breakage is rare but can complicate removal. Intraoperative fluoroscopy is the primary defense against aberrant pin placement; the surgeon must meticulously verify trajectory on multiple orthogonal views before concluding the procedure.
Neurologic injuries represent a severe complication profile. The Lateral Femoral Cutaneous Nerve (LFCN) is at high risk during the initial approach; injury results in painful meralgia paresthetica or numbness over the anterolateral thigh. While often transient, it can be distressing. Far more devastating is injury to the sciatic nerve or the superior gluteal vessels during the passage of instruments or the Gigli saw through the greater sciatic notch. This usually results from a failure to maintain a strict subperiosteal plane. If massive hemorrhage occurs from the notch, the surgeon must immediately pack the area and consider extending the exposure for direct vascular control; blind clamping is strictly prohibited as it virtually guarantees sciatic nerve transection.
Loss of surgical reduction or displacement of the bone graft is typically a consequence of technical error. This can occur if the bone graft is improperly sized, if the osteotomy cut is excessively sloped (allowing the graft to slide out), or if the pin fixation is biomechanically inadequate. Furthermore, if the hip was not concentrically reduced prior to the osteotomy, the persistent eccentric joint forces will inevitably lead to graft collapse and recurrent subluxation. Premature closure of the triradiate cartilage is a late, disastrous complication resulting from direct mechanical trauma
