Comprehensive Introduction and Patho-Epidemiology
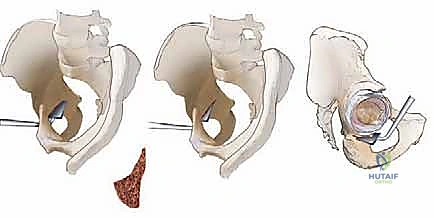
The periacetabular osteotomy (PAO) represents the zenith of reconstructive hip preservation surgery, standing as a technically demanding yet profoundly rewarding procedure for the treatment of symptomatic developmental dysplasia of the hip (DDH) and other complex acetabular malorientations. Originally conceptualized and popularized by Reinhold Ganz and his colleagues in Bern, Switzerland, in the 1980s, the Bernese PAO was a revolutionary departure from the redirectional osteotomies of the past. Unlike the single-cut Salter innominate osteotomy or the triple pelvic osteotomies of Steel and Tönnis, the Bernese PAO achieves complete mobilization of the acetabulum through a series of extra-articular, polygonal cuts while meticulously preserving the posterior column of the hemipelvis. This inherent posterior column stability is the hallmark of the procedure, allowing for profound triplanar correction of the acetabulum without compromising the structural integrity of the pelvic ring.
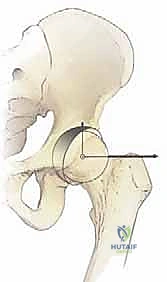
At its biomechanical core, the PAO is designed to completely dislodge the hip socket from its osseous bed, facilitating its reorientation into a biologically and mechanically optimized position. The primary objective in the dysplastic hip is to augment anterior and lateral femoral head coverage, thereby medializing the joint center of rotation and dramatically reducing the superolateral contact stresses that precipitate early-onset osteoarthritis. By normalizing these sheer forces and restoring a congruent articular relationship, the PAO alters the natural history of the dysplastic hip. Furthermore, the procedure is remarkably versatile; it is increasingly utilized to correct acetabular retroversion, a focal over-coverage pathology implicated in pincer-type femoroacetabular impingement (FAI), by anteverting the mobilized fragment.
The epidemiological burden of symptomatic hip dysplasia in the young adult population is substantial, often presenting insidiously in the second or third decade of life. Left untreated, the pathomechanics of a shallow, lateralized acetabulum lead to labral hypertrophy, chondral delamination, and eventual joint space collapse. The PAO intervenes at a critical juncture in this patho-epidemiological cascade, aiming to preserve the native joint and delay or entirely circumvent the need for total hip arthroplasty (THA). Because the procedure exclusively modifies the orientation of the acetabulum without distorting the true pelvic volume, it maintains the normal dimensions of the birth canal, a paramount consideration given that the majority of patients undergoing this procedure are women of childbearing age.
Historically, the evolution of the PAO was preceded by various spherical and rotational osteotomies, such as those described by Eppright, Ninomiya, and Wagner. While innovative, these earlier iterations possessed distinct limitations. The Eppright barrel-shaped cut offered excellent lateral coverage but restricted anterior correction. The Wagner type I osteotomy provided rotatory displacement but was impeded by an intact quadrilateral plate, precluding the essential medialization of the hip center. The Bernese technique circumvented these limitations by utilizing a single-incision approach to execute reproducible, straight cuts that allow for massive, multidirectional corrections. This evolution has solidified the Ganz PAO as the gold standard in contemporary hip preservation, demanding from the modern orthopedic surgeon a flawless grasp of tridimensional pelvic anatomy and meticulous surgical execution.
Detailed Surgical Anatomy and Biomechanics
Mastery of the periacetabular osteotomy is inextricably linked to an intimate, three-dimensional understanding of pelvic osteology, musculotendinous intervals, and the treacherous neurovascular topography surrounding the hip joint. The surgeon must navigate a complex landscape where millimeter-level deviations in osteotome trajectory can result in catastrophic complications, ranging from intra-articular fracture to major neurovascular compromise.
Osteology and Articular Configuration
The acetabulum is a hemispherical construct formed by the confluence of the ilium, ischium, and pubis, which fuse at the triradiate cartilage by approximately 15 to 16 years of age. This fusion is a mandatory prerequisite for the standard Bernese PAO, as the osteotomy cuts traverse the fused triradiate complex. The native acetabulum is oriented approximately 45 degrees caudally and 15 degrees anteriorly, providing coverage for roughly 170 degrees of the femoral head. In the dysplastic hip, this orientation is pathologically altered, typically presenting with a steepened sourcil (increased Tönnis angle), deficient anterior and lateral coverage (decreased center-edge angle), and a lateralized center of rotation.
The articular surface itself is horseshoe-shaped, lined with hyaline cartilage, and deficient inferiorly at the acetabular notch, which is bridged by the transverse acetabular ligament. Surrounding the bony rim is the fibrocartilaginous labrum, a critical structure that deepens the socket, provides a suction seal, and enhances fluid-film lubrication. The labrum's blood supply is precarious, derived primarily from the capsular reflection via branches of the obturator, superior gluteal, and inferior gluteal arteries, penetrating only its peripheral third. Understanding this vascular limitation is crucial when performing concomitant arthrotomy or labral repair during a PAO, as aggressive capsular stripping can precipitate labral necrosis.
The posterior column, a massive pillar of bone extending from the sciatic notch to the ischial tuberosity, is the structural foundation of the hemipelvis. The genius of the Bernese PAO lies in the preservation of this column. The retro-acetabular cut must be executed with extreme precision to separate the acetabulum from the posterior column without violating the column's integrity or breaching the articular cartilage. The quadrilateral plate, forming the medial wall of the acetabulum, must also be carefully navigated during the ischial and pubic cuts to ensure complete mobilization of the fragment while avoiding intrapelvic visceral injury.

Musculotendinous Intervals and Dynamic Stabilizers
The surgical approach for a PAO requires precise dissection through the complex muscular layers of the anterior and lateral hip. The primary interval utilized is the modified Smith-Petersen approach, exploiting the internervous plane between the sartorius (femoral nerve) and the tensor fasciae latae (superior gluteal nerve). The anterior superior iliac spine (ASIS) serves as the critical superficial landmark, acting as the origin for the sartorius, while the anterior inferior iliac spine (AIIS) gives rise to the direct head of the rectus femoris.
Deep to this superficial interval, the surgeon encounters the robust iliopsoas muscle complex. The iliopsoas tendon must be mobilized and often fractionally lengthened or tenotomized to relieve anterior impingement and facilitate exposure of the pubic root and medial joint capsule. The rectus femoris is typically detached from the AIIS and reflected distally to expose the supra-acetabular region and the anterior capsule. Preservation of the abductor musculature (gluteus medius and minimus) is paramount. Unlike older approaches that required extensive abductor detachment, the modern PAO meticulously preserves these dynamic stabilizers, peeling them subperiosteally only as far as necessary to execute the iliac osteotomy, thereby minimizing postoperative limp and accelerating rehabilitation.
The capsular ligaments—the iliofemoral (ligament of Bigelow), pubofemoral, and ischiofemoral ligaments—form a robust static stabilizing network. The iliofemoral ligament, with its inverted Y-shape, is the strongest ligament in the body and tightens in extension and external rotation. During the mobilization phase of the PAO, the capsule must be carefully managed. While the osteotomy is extra-articular, the capsule remains attached to the mobilized acetabular fragment. The surgeon must ensure that the soft tissue attachments to the fragment, particularly the inferior capsular reflections, are preserved to maintain the critical blood supply to the reoriented acetabulum.

Critical Neurovascular Topography
The neurovascular anatomy surrounding the acetabulum is unforgiving, and iatrogenic injury is a devastating complication. The arterial supply to the acetabular fragment is the most critical consideration during the osteotomy. The fragment's viability depends heavily on the supra- and infra-acetabular branches of the superior and inferior gluteal arteries, as well as contributions from the obturator artery. The inferior gluteal artery is particularly vital; excessive posterior dissection or errant osteotome placement in the greater sciatic notch can sever this vessel, leading to avascular necrosis of the acetabular fragment.
The medial femoral circumflex artery (MFCA), the primary blood supply to the femoral head, courses perilously close to the inferior surgical field. It travels between the pectineus and iliopsoas, passing inferior to the obturator externus before ascending posteriorly. While the PAO is an acetabular procedure, deep retractors placed inferior to the transverse acetabular ligament or aggressive dissection around the inferior capsule can compromise the MFCA, risking catastrophic femoral head osteonecrosis. Additionally, the corona mortis—an anastomotic connection between the external iliac/epigastric and obturator vessels crossing the superior pubic ramus—must be routinely identified and ligated during the pubic osteotomy to prevent massive intrapelvic hemorrhage.
Neurologically, the lateral femoral cutaneous nerve (LFCN) is at highest risk during the superficial dissection. Exiting the pelvis medial to the ASIS, it exhibits high anatomic variability and is easily stretched or transected, resulting in meralgia paresthetica. Deep within the pelvis, the obturator nerve runs along the lateral pelvic wall and under the superior pubic ramus; it is vulnerable during the pubic cut if the osteotome plunges medially. Posteriorly, the sciatic nerve lies in close proximity to the posterior column and the ischial spine. The retro-acetabular cut, performed largely by tactile feel and fluoroscopic guidance, must be angled precisely to avoid breaching the posterior cortex of the posterior column and lacerating the sciatic nerve.

Exhaustive Indications and Contraindications
The decision to proceed with a periacetabular osteotomy requires a rigorous evaluation of the patient's clinical presentation, pathoanatomy, and overall joint health. The ideal candidate is a symptomatic, skeletally mature young adult with a mechanically deficient but biologically viable hip joint. Careful patient selection is the single most important predictor of long-term survivorship following a PAO.
Patient Selection Criteria
The primary demographic for a PAO consists of adolescents and young adults, typically between the ages of 14 and 40. Skeletal maturity, defined by the complete closure of the triradiate cartilage, is a strict prerequisite for the standard Bernese technique, as the osteotomy cuts traverse this anatomical junction. Performing a Bernese PAO in a patient with an open triradiate cartilage risks growth arrest and subsequent progressive deformity. In skeletally immature patients, alternative procedures such as the Dega or Salter osteotomies are indicated.
Clinically, the patient must present with symptoms directly attributable to their morphological abnormality. This typically manifests as insidious-onset groin pain exacerbated by weight-bearing activities, prolonged sitting, or specific athletic endeavors. Mechanical symptoms such as catching, clicking, or locking are highly suggestive of concomitant intra-articular pathology, such as a labral tear or chondral flap, which are frequently seen in the dysplastic hip due to chronic shear forces. The physical examination must correlate with the radiographic findings, often revealing pain with flexion, adduction, and internal rotation (anterior impingement) or apprehension and pain with extension and external rotation (anterior instability).
Crucially, the patient must possess a realistic understanding of the extensive nature of the surgery and the prolonged rehabilitation required. Psychological readiness and a commitment to strict postoperative weight-bearing protocols are essential. Furthermore, the surgeon must assess the patient's body mass index (BMI); while obesity is not an absolute contraindication, a significantly elevated BMI complicates the surgical approach, increases the risk of neurovascular injury due to depth of dissection, and places excessive mechanical stress on the fixation construct during the early healing phase.
Pathoanatomic Indications
The classic and most frequent indication for a PAO is symptomatic developmental dysplasia of the hip (DDH). Radiographically, this is characterized by a lateral center-edge angle (LCEA) of Wiberg less than 20 degrees, an anterior center-edge angle (ACEA) of Lequesne less than 20 degrees, and an elevated Tönnis angle (acetabular roof inclination) greater than 10 to 15 degrees. The PAO excels in these cases by providing massive lateral and anterior coverage, thereby normalizing the LCEA and Tönnis angle, and medializing the femoral head to reduce the joint reaction force.
Beyond classic dysplasia, the PAO is increasingly recognized as the definitive treatment for severe acetabular retroversion. In this pathoanatomic variant, the anterior wall of the acetabulum is over-prominent relative to the posterior wall, creating a pincer-type impingement mechanism. Radiographically, this is identified by a positive cross-over sign, an ischial spine sign, and a prominent posterior wall sign on a true anteroposterior (AP) pelvic radiograph. For these patients, the PAO is utilized not to increase coverage, but to antevert the acetabular fragment, thereby relieving anterior impingement while maintaining or slightly improving posterior coverage.
Another emerging indication is the treatment of complex, multi-planar deformities, such as those seen in syndromic conditions (e.g., Down syndrome, Ehlers-Danlos syndrome) or sequelae of pediatric hip diseases like Legg-Calvé-Perthes disease or slipped capital femoral epiphysis (SCFE). In these scenarios, the PAO may be combined with proximal femoral osteotomies (surgical dislocation and osteochondroplasty) to achieve a congruent and stable articulation. The ability of the PAO to achieve independent, multi-directional correction makes it uniquely suited for these challenging, non-standard morphologies.
Absolute and Relative Contraindications
Despite its versatility, the PAO is contraindicated in several clinical scenarios where the likelihood of failure or accelerated joint degeneration is unacceptably high. The presence of advanced osteoarthritis is the most significant absolute contraindication. Evaluating the joint space is critical; a PAO should not be performed if there is less than 2 millimeters of joint space on weight-bearing radiographs, or if there are extensive subchondral cysts and flattening of the femoral head (Tönnis grade 2 or 3 osteoarthritis). In these patients, a PAO will likely accelerate the arthritic process, and a total hip arthroplasty is the more appropriate intervention.
| Contraindication Category | Specific Condition | Rationale |
|---|---|---|
| Absolute | Advanced Osteoarthritis (Tönnis Grade 2/3) | Insufficient viable cartilage; osteotomy will not halt progression and may accelerate pain. |
| Absolute | Open Triradiate Cartilage | Osteotomy cuts cross the triradiate complex; risks growth arrest and severe secondary deformity. |
| Absolute | Stiff Hip (Lack of Congruency) | Reorientation requires a congruent joint in the new position; a stiff, deformed head will hinge and fail. |
| Relative | Age > 40-45 Years | Decreased biological healing capacity; higher rate of conversion to THA within 5-10 years. |
| Relative | Morbid Obesity (BMI > 35) | Increased surgical morbidity, deep infection risk, and mechanical failure of fixation. |
| Relative | Inflammatory Arthropathy | Systemic cartilage destruction is not addressed by mechanical reorientation. |
A stiff hip with significant loss of motion is another major contraindication. The fundamental premise of a PAO is that the femoral head can find a congruent, stable position within the reoriented acetabulum. If the hip is stiff or the femoral head is severely aspherical (hinge abduction), reorienting the socket will result in point loading, incongruency, and rapid failure. Preoperative functional radiographs, such as abduction-internal rotation views, are essential to confirm that congruency can be achieved in the planned corrected position. Finally, advanced age (typically over 40-45 years) is a relative contraindication, as literature demonstrates a significantly higher rate of conversion to THA in older cohorts, likely due to diminished cartilage resilience and occult degenerative changes.

Pre-Operative Planning, Templating, and Patient Positioning
The execution of a flawless PAO begins weeks before the patient enters the operating theater. The complexity of the triplanar correction demands exhaustive preoperative planning, utilizing a combination of high-quality plain radiography, advanced three-dimensional imaging, and meticulous surgical templating to define the exact magnitude and direction of the required reorientation.
Clinical Evaluation and Radiographic Analysis
The initial radiographic evaluation must include a standardized, high-quality anteroposterior (AP) radiograph of the pelvis. Standardization is critical; the film must be taken with the patient standing, the symphysis pubis centered, and the coccyx pointing directly toward the symphysis with a distance of 1 to 2 centimeters between them to ensure neutral pelvic tilt. On this AP view, the surgeon meticulously measures the lateral center-edge angle (LCEA), the Tönnis angle (acetabular roof angle), and the extrusion index. Furthermore, the surgeon must evaluate the integrity of the Shenton line and scrutinize the radiograph for signs of retroversion, including the cross-over sign, the posterior wall sign, and the ischial spine sign.
In addition to the AP pelvis, a false-profile view of the affected hip is mandatory to assess anterior femoral head coverage. This view, taken with the patient standing and the pelvis rotated 65 degrees relative to the cassette, allows for the measurement of the anterior center-edge angle (ACEA) of Lequesne. A functional view, typically an AP pelvis taken with the hips in abduction and internal rotation, is crucial to assess joint congruency. If the joint space widens or the femoral head hinges laterally on this view, it indicates a severe morphological mismatch that may preclude a successful PAO or necessitate a concomitant proximal femoral osteotomy.
Finally, Dunn views or cross-table lateral radiographs are obtained to evaluate the proximal femur for cam-type morphology, which frequently coexists with acetabular dysplasia or retroversion. If a cam lesion is identified, it must be addressed concurrently during the PAO via an anterior arthrotomy and osteochondroplasty to prevent secondary impingement once the acetabulum is reoriented into a more covering position.
Three-Dimensional Advanced Imaging and Templating
While plain radiographs provide the foundational metrics, advanced imaging with computed tomography (CT) or magnetic resonance imaging (MRI) is now considered standard of care in the preoperative workup for a PAO. A high-resolution, non-contrast CT scan of the pelvis and bilateral knees (to assess femoral version) provides an unparalleled three-dimensional understanding of the osseous morphology. Modern 3D reconstruction software allows the surgeon to virtually rotate the pelvis, assess the exact volume of the anterior and posterior walls, and simulate the osteotomy cuts. This virtual templating is invaluable for determining the exact degrees of lateralization, anterior coverage, and version correction required to achieve optimal biomechanics without creating iatrogenic impingement.
Magnetic resonance arthrography (MRA) or high-resolution non-contrast MRI is essential for evaluating the intra-articular soft tissues. Dysplastic hips are notoriously susceptible to labral hypertrophy, complex labral tears, and perilabral cysts. More importantly, MRI allows for the assessment of the articular cartilage. The presence of full-thickness cartilage delamination, subchondral edema, or paralabral cysts significantly worsens the prognosis and must be factored into the surgical decision-making process. If significant intra-articular pathology is identified, the surgical plan must include an arthrotomy for labral repair, debridement, or cartilage stabilization concurrent with the osteotomy.
Physical templating, utilizing tracing paper over the AP radiograph, remains a valuable exercise for the surgeon. By tracing the acetabular fragment, the femoral head, and the intact pelvis, the surgeon can physically simulate the rotation of the fragment. This allows for the calculation of the expected change in the LCEA and Tönnis angle, and helps determine the optimal point of rotation (usually the center of the femoral head) to ensure that the correction medializes the joint center rather than inadvertently lateralizing it, which would disastrously increase joint reaction forces.

Anesthesia, Patient Positioning, and Fluoroscopic Setup
The PAO is a major surgical undertaking associated with significant blood loss and prolonged operative times. General endotracheal anesthesia is universally employed, often supplemented with a regional technique, such as an epidural or a lumbar plexus block, to provide preemptive analgesia and reduce intraoperative narcotic requirements. Two large-bore intravenous lines, an arterial line for continuous hemodynamic monitoring, and a Foley catheter are mandatory. Given the risk of substantial hemorrhage, particularly from the cancellous bone surfaces of the osteotomies, a cell salvage system should be routinely utilized, and cross-matched blood must be readily available in the operating room.
Patient positioning is critical for both surgical access and accurate fluoroscopic imaging. The patient is placed in the supine position on a radiolucent operating table. A small bump is placed under the ipsilateral sacrum to slightly elevate the operative hip, facilitating access to the posterior column and the greater sciatic notch. The entire ipsilateral lower extremity is prepped and draped free to allow for full range of motion during the procedure. This mobility is essential for relaxing neurovascular structures during specific osteotomy cuts, testing for impingement after fragment reorientation, and utilizing the leg to manipulate the acetabular fragment.
The fluoroscopic setup must be meticulously verified before the incision is made. The C-arm is brought in from the contralateral side of the table. The surgeon must confirm that perfect AP, obturator oblique, and iliac oblique views of the pelvis can be obtained without obstruction from the table pedestal or the patient's contralateral leg. These fluoroscopic views are the surgeon's "eyes" during the deep, extra-articular cuts. The obturator oblique view is particularly crucial for visualizing the posterior column and ensuring the retro-acetabular cut does not violate the joint or completely sever the posterior pelvic ring.

Step-by-Step Surgical Approach and Fixation Technique
The execution of the Bernese PAO is a highly orchestrated sequence of surgical maneuvers, demanding technical precision, spatial awareness, and constant vigilance regarding neurovascular proximity. The procedure can be conceptualized in four distinct phases: the surgical approach, the execution of the four osteotomy cuts, the mobilization and reorientation of the fragment, and the definitive fixation.
The Modified Smith-Petersen Approach and Soft Tissue Dissection
The procedure begins with a modified Smith-Petersen approach, utilizing either a longitudinal incision centered over the ASIS or a transverse "bikini" incision for superior cosmetic outcome. The incision extends distally along the interval between the sartorius and the tensor fasciae latae (TFL). Careful superficial dissection is paramount to identify and protect the lateral femoral cutaneous nerve (LFCN), which typically crosses the surgical field just distal to the ASIS. Once the LFCN is mobilized and protected, the deep fascia is incised, and the internervous plane between the sartorius (femoral nerve) and TFL (superior gluteal nerve) is developed.
The ASIS is identified, and the origin of the sartorius is either released or osteotomized with a small flake of bone to facilitate later repair. Deep to the sartorius, the rectus femoris is identified at its origin on the AIIS. The direct head is detached from the AIIS, and the reflected head is released from the superior joint capsule. The rectus is then tagged and retracted distally, exposing the underlying iliopsoas muscle and the anterior capsule of the hip joint. The iliopsoas tendon is identified as it crosses the pelvic brim; it is mobilized medially, and a fractional lengthening or tenotomy is often performed to relieve anterior tension and improve exposure of the superior pubic ramus.
Subperiosteal dissection is then carried out along the inner and outer tables of the iliac wing. On the medial side, the iliacus muscle is elevated off the false pelvis down to the pelvic brim, exposing the quadrilateral plate. On the lateral side, the gluteus minimus and medius are carefully elevated off the outer table of the ilium, just enough to accommodate the supra-acetabular osteotomy cut. Posteriorly, the dissection extends along the pelvic brim to the greater sciatic notch. A blunt retractor is carefully placed subperiosteally into the sciatic notch to protect the superior gluteal neurovascular bundle and the sciatic nerve during the subsequent posterior column osteotomy.

Executing the Bernese Osteotomy Sequence
The defining characteristic of the Bernese PAO is the sequence of four extra-articular cuts designed to free the acetabulum while preserving the posterior column.
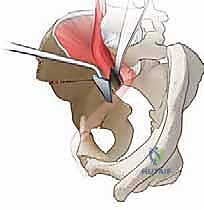
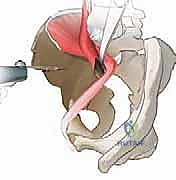
1. The Incomplete Ischial Cut: The first cut targets the ischium. Using a specialized angled osteotome (often a Ganz osteotome), the surgeon approaches the ischium from the medial side of the pelvis, sliding down the quadrilateral surface. The osteotome is positioned just inferior to the acetabulum, aiming toward the ischial spine. This cut is incomplete; it does not transect the entire ischium but rather creates a deep groove in the medial ischial cortex. This incomplete cut serves as a stress riser, allowing the bone to fracture in a controlled manner during final mobilization, thereby preserving the structural integrity of the posterior column. Fluoroscopic guidance (obturator oblique view) is critical to ensure the osteotome does not plunge too deep or violate the inferior joint space.
2. The Pubic Cut: The second cut completely transects the superior pubic ramus. The periosteum over the superior pubic ramus is elevated circumferentially. Blunt retractors (such as Homan retractors) are placed superiorly and inferiorly to protect the femoral neurovascular bundle (laterally) and the obturator neurovascular bundle (medially and inferiorly). The corona mortis, if present, is identified and ligated. An oscillating saw or a sharp osteotome is used to make a vertical cut through the
Clinical & Radiographic Imaging Archive