Introduction and Epidemiology
Conservative Head Reduction Osteotomy represents a highly specialized, joint-preserving surgical intervention designed to address severe morphologic deformities of the proximal femur in the adolescent and young adult population. The primary objective of this procedure is to restore congruency to the hip joint, normalize kinematics, and delay the inevitable progression to end-stage osteoarthritis requiring total hip arthroplasty. The procedure is most frequently indicated in the sequelae of Legg-Calvé-Perthes disease, severe slipped capital femoral epiphysis, post-traumatic avascular necrosis, and complex developmental dysplasia of the hip.

The hallmark pathoanatomy addressed by this procedure is coxa magna, characterized by an enlarged, often flattened, and extruded femoral head that results in hinge abduction and severe femoroacetabular impingement. Epidemiologically, the sequelae of childhood hip disorders present a significant burden, with untreated or severe Legg-Calvé-Perthes disease leading to premature osteoarthritis in the third or fourth decade of life. By surgically reducing the volume and reshaping the geometry of the deformed femoral head, orthopedic surgeons can re-establish a functional articulation within the native acetabulum. This conservative, albeit technically demanding, approach relies heavily on the principles of safe surgical dislocation of the hip, allowing for global access to the femoral head without compromising its tenuous vascular supply.
Surgical Anatomy and Biomechanics
A profound understanding of the extra-articular and intra-articular vascular anatomy of the proximal femur is the absolute prerequisite for performing a Conservative Head Reduction Osteotomy. The procedure hinges on the ability to dislocate the hip and perform intra-articular osteotomies without inducing iatrogenic avascular necrosis.
Vascular Supply of the Proximal Femur
The medial femoral circumflex artery provides the predominant blood supply to the mature femoral head. The deep branch of the medial femoral circumflex artery courses posteriorly, traversing the interval between the pectineus and iliopsoas, and runs predictably along the inferior border of the obturator externus. It then crosses posterior to the obturator externus tendon and anterior to the superior gemellus and obturator internus tendons.
As the deep branch reaches the intertrochanteric crest, it gives rise to the retinacular vessels. These critical vessels perforate the capsule near the superior capsular insertion and travel along the posterosuperior aspect of the femoral neck beneath the synovial reflection to supply the epiphysis. Preservation of the obturator externus and the short external rotators during surgical exposure is mandatory to protect this vascular leash. The Ganz surgical dislocation approach utilizes a trochanteric flip osteotomy to maintain the integrity of these posterior structures while providing 360-degree access to the joint.
Hip Joint Biomechanics and Kinematics
In the setting of coxa magna or severe cam deformity, the biomechanics of the hip are profoundly altered. The aspherical femoral head creates an abnormal center of rotation and leads to non-concentric articulation. During abduction, the enlarged lateral portion of the femoral head hinges against the lateral acetabular rim, a phenomenon known as hinge abduction. This hinging levers the medial femoral head out of the acetabulum, exponentially increasing contact pressures on the lateral compartment and leading to rapid articular cartilage degradation.
By performing a reduction osteotomy, the surgeon excises the central or lateral incongruent segment of the femoral head and compresses the remaining viable articular segments. This restores the spherical geometry of the head, allowing it to seat concentrically within the acetabulum. Normalizing the center of rotation improves the mechanical advantage of the abductor musculature and distributes joint reactive forces evenly across the articular cartilage, thereby mitigating the progression of secondary osteoarthritis.
Indications and Contraindications
Patient selection is the most critical determinant of success in Conservative Head Reduction Osteotomy. The procedure is reserved for young, active patients who present with mechanical hip pain, restricted range of motion, and radiographic evidence of severe femoral head deformity, but who retain a functional layer of articular cartilage.
Patient Selection Criteria
The ideal candidate is typically between the ages of 12 and 35, presenting with sequelae of pediatric hip disease. Pain is usually localized to the groin or lateral hip and is exacerbated by activity or specific ranges of motion, particularly flexion and internal rotation.
Radiographic evaluation must demonstrate a clear structural conflict, such as an extruded lateral head segment causing hinge abduction, but without advanced joint space narrowing. The presence of a "hinge" can often be confirmed dynamically under fluoroscopy or via abduction-internal rotation plain radiographs.
Operative Versus Non Operative Management
| Clinical Scenario | Management Strategy | Rationale and Considerations |
|---|---|---|
| Asymptomatic Coxa Magna | Non-Operative | Observation and activity modification. Prophylactic osteotomy is not indicated in the absence of pain or progressive loss of motion. |
| Painful Hinge Abduction with Preserved Joint Space | Operative | Strong indication for Conservative Head Reduction Osteotomy. Restores sphericity, relieves impingement, and improves abductor mechanics. |
| Tonnis Grade 3 Osteoarthritis | Non-Operative | Contraindication for joint preservation. Advanced cartilage loss requires arthroplasty or arthrodesis depending on patient age and functional demands. |
| Active Joint Infection | Non-Operative | Absolute contraindication. Eradication of infection is required prior to any reconstructive intervention. |
| Avascular Necrosis with Complete Head Collapse | Non-Operative | If structural integrity of the subchondral bone is completely lost, a reshaping osteotomy will fail. Arthroplasty is indicated. |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is essential to determine the precise location, geometry, and volume of the osteotomy required to restore congruency. Advanced imaging modalities are indispensable in this phase.
Advanced Imaging and Templating
Standard radiographic series should include an anteroposterior pelvis, cross-table lateral, and false profile views of the affected hip. Functional views, such as maximum abduction and adduction radiographs, help quantify the degree of hinge abduction and the potential for concentric reduction.

Magnetic Resonance Imaging or Magnetic Resonance Arthrography is mandatory to assess the integrity of the articular cartilage, the viability of the subchondral bone, and the status of the acetabular labrum. Three-dimensional computed tomography reconstructions are highly recommended to map the exact topography of the deformity. Virtual surgical planning software can be utilized to simulate the osteotomy, calculate the wedge angle, and predict the final head-neck offset and sphericity.
Operating Room Setup
The patient is placed in the lateral decubitus position on a radiolucent operating table. Rigid pelvic fixation using peg boards or a bean bag is required to allow for aggressive manipulation of the operative extremity without altering the pelvic tilt. The entire lower extremity must be prepped and draped free to allow for full, unrestricted range of motion during the dislocation and reduction phases of the procedure. Intraoperative fluoroscopy is positioned to allow for seamless anteroposterior and lateral visualization of the proximal femur and acetabulum.
Detailed Surgical Approach and Technique
The surgical execution of the Conservative Head Reduction Osteotomy relies on the Ganz safe surgical dislocation. This approach provides unparalleled access to the femoral head while safeguarding the medial femoral circumflex artery.
The Surgical Approach
A straight lateral incision is made centered over the greater trochanter. The fascia lata is incised in line with the skin incision. The Gibson interval, located between the gluteus maximus and the gluteus medius, is identified and developed. The gluteus maximus is retracted posteriorly, exposing the posterior border of the gluteus medius and the greater trochanter.

A digastric trochanteric flip osteotomy is then performed. A stepped osteotomy is created from the posterior border of the greater trochanter, exiting anteriorly just proximal to the vastus lateralis ridge. The thickness of the trochanteric fragment should be approximately 1.5 centimeters. The gluteus medius and minimus remain attached to the mobilized fragment, while the vastus lateralis remains attached distally, creating a digastric muscle sleeve. This fragment is retracted anteriorly, exposing the superior and anterior joint capsule.
Capsulotomy and Safe Dislocation
The piriformis tendon is identified, and the interval between the piriformis and the gluteus minimus is developed to expose the superior capsule. The short external rotators, including the obturator externus, are strictly preserved to protect the deep branch of the medial femoral circumflex artery.
A Z-shaped capsulotomy is performed for a right hip (or an inverse Z for a left hip). The longitudinal limb of the capsulotomy is made along the anterosuperior axis of the femoral neck. The proximal transverse limb runs parallel to the acetabular rim, and the distal transverse limb runs parallel to the intertrochanteric line.

Once the capsule is reflected, the hip is dislocated anteriorly by applying a combination of flexion, adduction, and external rotation. The ligamentum teres is sharply excised. The entire femoral head and the acetabular fossa are now fully visualized.
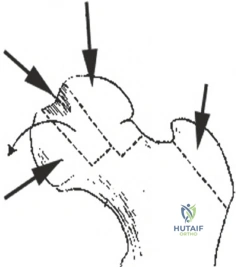
Execution of the Reduction Osteotomy
With the femoral head dislocated, the precise location of the deformity is identified, correlating intraoperative findings with preoperative three-dimensional imaging. The osteotomy is typically designed as a closing wedge, targeting the central necrotic or hypertrophic segment that is causing the asphericity.

Using a fine oscillating saw under constant saline irrigation to prevent thermal necrosis, the planned wedge of bone and overlying cartilage is resected. The depth of the osteotomy must be carefully controlled to avoid compromising the primary retinacular blood supply located posterosuperiorly. In cases of lateral extrusion, a lateral wedge may be resected to allow the medial, more congruent portion of the head to hinge laterally.
Reduction and Internal Fixation
Following the resection of the wedge, the remaining viable segments of the femoral head are approximated. The reduction must restore a spherical contour that matches the native acetabular radius of curvature.

Fixation is achieved using multiple countersunk headless compression screws or bioabsorbable pins. The trajectory of the screws must be meticulously planned to cross the osteotomy site perpendicularly, maximizing interfragmentary compression while avoiding penetration into the articular surface or the vital posterior retinacular vessels. Fluoroscopy is utilized to confirm anatomic reduction, appropriate screw length, and the absence of intra-articular hardware.
The hip is then reduced back into the acetabulum. The joint is taken through a full range of motion to confirm the resolution of hinge abduction and the restoration of impingement-free kinematics. The capsule is closed loosely to prevent postoperative intra-articular hypertension. The trochanteric flip osteotomy is reduced and fixed using two or three 4.5 millimeter cortical screws.
Complications and Management
While Conservative Head Reduction Osteotomy offers significant joint-preserving benefits, it is a technically demanding procedure associated with a distinct complication profile. Strict adherence to the safe surgical dislocation technique is paramount to minimizing morbidity.
Iatrogenic Avascular Necrosis
The most devastating complication is iatrogenic avascular necrosis of the femoral head, resulting from damage to the medial femoral circumflex artery during the approach or the osteotomy.

Prevention relies on preserving the short external rotators and maintaining the osteotomy planes away from the posterosuperior retinacular vessels. If avascular necrosis occurs and leads to structural collapse, salvage typically requires conversion to a total hip arthroplasty.
Summary of Surgical Complications
| Complication | Estimated Incidence | Prevention and Management Strategies |
|---|---|---|
| Iatrogenic Avascular Necrosis | 2 to 5 Percent | Meticulous preservation of the MFCA and short external rotators. Salvage: Total Hip Arthroplasty. |
| Trochanteric Nonunion | 3 to 8 Percent | Rigid internal fixation with multiple cortical screws; strict postoperative weight-bearing restrictions. Management: Revision open reduction internal fixation with bone grafting. |
| Heterotopic Ossification | 10 to 20 Percent | Careful tissue handling; routine use of prophylactic NSAIDs (e.g., Indomethacin) or single-dose localized radiation. Management: Excision if symptomatic and mature. |
| Chondrolysis | 1 to 3 Percent | Avoidance of thermal necrosis during osteotomy; ensuring no intra-articular hardware penetration. Management: Observation, anti-inflammatories, potential conversion to arthroplasty if progressive. |
| Hardware Failure | 2 to 5 Percent | Use of adequate number of compression screws; adherence to rehab protocols. Management: Hardware removal and revision fixation if nonunion is present. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation following a Conservative Head Reduction Osteotomy is critical for optimizing functional outcomes and ensuring the biological healing of both the intra-articular osteotomy and the greater trochanter. The protocol is phased and requires strict patient compliance.
Initial Protection Phase
During the first six weeks postoperatively, the primary goal is protection of the osteotomy sites. Patients are restricted to toe-touch weight-bearing (approximately 10 to 15 kilograms) using bilateral crutches. Continuous passive motion machines may be utilized immediately postoperatively to prevent intra-articular adhesions and promote cartilage nutrition. Active abduction is strictly prohibited to prevent displacement of the trochanteric osteotomy. Deep vein thrombosis prophylaxis is administered according to institutional protocols, typically for four weeks.
Progressive Mobilization and Strengthening
At six weeks, radiographic evaluation is performed to assess healing of the trochanteric and femoral head osteotomies. If callus formation and interval healing are evident, weight-bearing is gradually advanced by 25 percent of body weight per week until full weight-bearing is achieved. Active-assisted and active range of motion exercises are initiated, focusing on restoring flexion and internal rotation.
Isotonic strengthening of the gluteus medius and minimus begins only after radiographic confirmation of trochanteric union, usually around the 8 to 10-week mark. Return to high-impact activities or sports is generally delayed until 6 to 9 months postoperatively, contingent upon full radiographic consolidation, restoration of symmetric muscle strength, and a pain-free functional assessment.
Summary of Key Literature and Guidelines
The foundational literature supporting Conservative Head Reduction Osteotomy is deeply rooted in the pioneering work of Ganz and colleagues, who developed the safe surgical dislocation approach. This anatomical milestone allowed surgeons to access the femoral head without compromising its perfusion, paving the way for complex intra-articular reshaping procedures.
Subsequent studies by Leunig, Paley, and others have demonstrated the efficacy of head reduction osteotomies in the setting of severe Legg-Calvé-Perthes disease and slipped capital femoral epiphysis. Long-term survivorship data indicates that when performed for the correct indications—specifically, the elimination of hinge abduction in a joint with preserved cartilage—the procedure significantly improves Harris Hip Scores and delays the need for total hip arthroplasty by a decade or more.
Current academic guidelines emphasize that this procedure should be performed in specialized tertiary referral centers by surgeons with extensive experience in hip preservation. The learning curve is steep, and the margin for error regarding the vascular supply is minimal. However, in the carefully selected young adult with a mechanically disadvantageous coxa magna, the Conservative Head Reduction Osteotomy remains a powerful and necessary tool in the orthopedic surgeon's armamentarium.
