Bernese Periacetabular Osteotomy: A Masterclass in Hip Preservation

Key Takeaway
This masterclass details the Bernese Periacetabular Osteotomy (PAO) for hip dysplasia. Fellows will learn comprehensive anatomy, meticulous preoperative planning, and granular intraoperative execution from a surgeon's perspective. We cover neurovascular risks, precise osteotomy techniques, and essential pearls for successful acetabular reorientation, aiming to prevent arthrosis and restore hip function.
Introduction and Epidemiology
The Bernese periacetabular osteotomy is a highly sophisticated and powerful acetabular redirectional procedure designed for the surgical management of symptomatic developmental dysplasia of the hip in skeletally mature patients. Originally described by Reinhold Ganz and his colleagues in Bern, Switzerland, in 1984, the procedure involves a series of meticulously planned, connecting polygonal osteotomies that liberate the acetabulum from the innominate bone while preserving the structural integrity of the posterior column.
This technique allows for profound multiplanar reorientation of the acetabulum to optimize femoral head coverage, normalize joint contact pressures, and restore hip biomechanics. Because the posterior column remains intact, the pelvis maintains inherent mechanical stability, which permits early postoperative mobilization and avoids the need for postoperative spica casting or prolonged strict bed rest.

Developmental dysplasia of the hip encompasses a spectrum of pathoanatomy characterized by a shallow, lateralized, and often anteverted acetabulum. Epidemiologically, residual dysplasia is a leading cause of secondary osteoarthritis of the hip in young adults, responsible for a significant percentage of total hip arthroplasties performed in patients under the age of 50. The Bernese periacetabular osteotomy has become the gold standard and the most commonly performed acetabular redirectional osteotomy for mature hip dysplasia in North America and Europe, superseding older techniques such as the Salter, dial, and spherical osteotomies due to its superior biomechanical advantages and versatility.


The pathomechanics of developmental dysplasia of the hip result in elevated edge-loading and sheer stresses across the articular cartilage, leading to labral hypertrophy, labral tearing, and eventual chondral delamination. By executing a periacetabular osteotomy, the surgeon medializes the hip center of rotation, thereby decreasing the reactive joint forces and increasing the abductor moment arm. This complex interplay of geometric correction and biomechanical optimization is the cornerstone of joint preservation in the dysplastic hip.


Surgical Anatomy and Biomechanics
Osteology and Pelvic Architecture
A profound understanding of pelvic osteology and its associated neurovascular relations is paramount for the safe execution of the Bernese periacetabular osteotomy. The innominate bone consists of the ilium, ischium, and pubis, which fuse at the triradiate cartilage at skeletal maturity. The osteotomies must navigate these regions without violating the articular surface or the posterior column. The intact posterior column, extending from the sciatic notch to the ischial tuberosity, provides the structural foundation that differentiates the Bernese periacetabular osteotomy from triple innominate osteotomies.

The quadrilateral plate forms the medial wall of the acetabulum and serves as a critical landmark during the deep intrapelvic dissection. The ischial spine and the lesser sciatic notch are essential reference points for the retroacetabular osteotomy. Precise spatial awareness of the acetabular dome thickness is required to avoid inadvertent intra-articular extension during the supra-acetabular cut.

Vascular Supply and Anastomotic Networks
The vascular supply to the mobilized acetabular fragment is a critical consideration. The fragment relies heavily on the supra-acetabular and retroacetabular anastomotic networks. The inferior gluteal artery and the medial circumflex femoral artery provide essential perfusion. The surgical approach and osteotomy cuts are specifically designed to preserve the capsular blood supply and the muscular pedicles attached to the fragment.


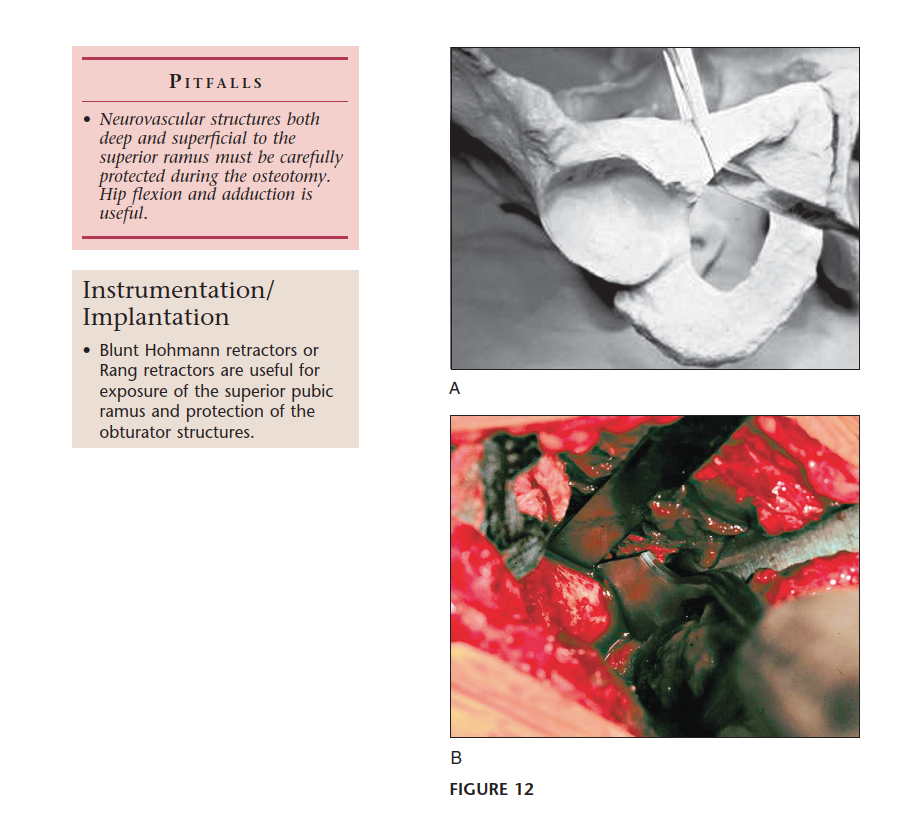
Additionally, the corona mortis—an anastomosis between the external iliac or inferior epigastric and obturator vessels crossing the superior pubic ramus—must be identified and ligated during the pubic osteotomy to prevent catastrophic hemorrhage. The obturator artery and vein course through the obturator canal and are at risk during the pubic osteotomy if the osteotome deviates inferiorly or medially.


Neurologic Considerations
Neurologic structures are at significant risk during the exposure and osteotomy phases. The lateral femoral cutaneous nerve courses anteriorly over the sartorius or through the tensor fasciae latae and is highly susceptible to traction neuropraxia. The femoral nerve lies lateral to the femoral sheath over the iliopsoas muscle and must be protected during the pubic cut, typically with a blunt retractor placed subperiosteally.


The sciatic nerve descends posterior to the posterior column and is at risk during the ischial and retroacetabular osteotomies. Maintaining the osteotome strictly within the osseous confines of the ischium and directing the retroacetabular cut appropriately ensures the sciatic nerve remains undisturbed in the greater sciatic notch.


Indications and Contraindications
The decision to proceed with a Bernese periacetabular osteotomy requires meticulous patient selection. The ideal candidate is a skeletally mature patient (closed triradiate cartilage) under the age of 40 with symptomatic developmental dysplasia of the hip, characterized by mechanical groin pain that correlates with radiographic findings of insufficient femoral head coverage.

Radiographic parameters indicating surgery typically include a lateral center-edge angle of Wiberg less than 20 degrees, an anterior center-edge angle less than 20 degrees, and an acetabular index (Tönnis angle) greater than 10 degrees. Crucially, the hip must demonstrate congruency on functional radiographs (abduction and internal rotation views) and possess preserved articular cartilage (Tönnis grade 0 or 1).


Contraindications include advanced osteoarthritis (Tönnis grade 2 or 3), severe loss of hip range of motion, and inflammatory arthropathies. Relative contraindications encompass patients over the age of 40, high body mass index, and significant proximal femoral deformity that cannot be addressed concurrently.


Operative Versus Non Operative Management
| Parameter | Operative Indication (PAO) | Non-Operative Indication |
|---|---|---|
| Skeletal Maturity | Closed triradiate cartilage | Open triradiate (consider pelvic osteotomies like Salter/Dega) |
| Symptomatology | Refractory mechanical groin pain | Asymptomatic or easily managed with NSAIDs/PT |
| Joint Space | Preserved (>2mm), Tönnis Grade 0-1 | Advanced narrowing, Tönnis Grade 2-3 |
| Functional Congruency | Congruent in abduction/internal rotation | Incongruent joint or fixed subluxation |
| Patient Age | Generally < 40 years | Generally > 45 years with OA (favor THA) |
| Range of Motion | Functional, preserved flexion/abduction | Severe stiffness or contracture |

Pre Operative Planning and Patient Positioning
Advanced Imaging and Templating
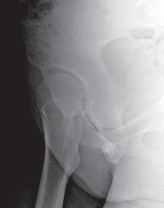
Thorough preoperative planning is non-negotiable. Standard radiographic evaluation includes a weight-bearing anteroposterior pelvis, a false profile view of Lequesne and de Sèze to assess anterior coverage, and a Dunn or cross-table lateral view to evaluate for concurrent cam morphology. The von Rosen view (abduction and internal rotation) is critical to confirm that the femoral head can be concentrically reduced into the dysplastic acetabulum once reoriented.

Computed tomography with three-dimensional surface rendering is heavily utilized to map the precise osseous anatomy, evaluate acetabular version, and plan the osteotomy trajectories. Magnetic resonance imaging or MR arthrography is indicated to evaluate the integrity of the acetabular labrum and articular cartilage. Concomitant labral tears are common and may be addressed via hip arthroscopy either prior to or simultaneously with the periacetabular osteotomy.


Operating Room Setup
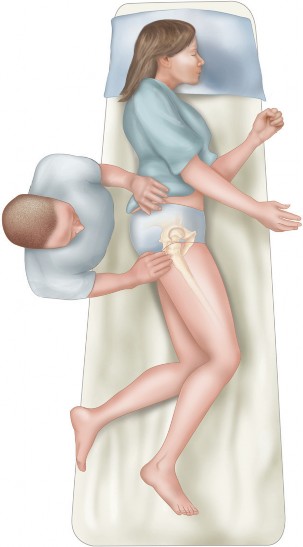
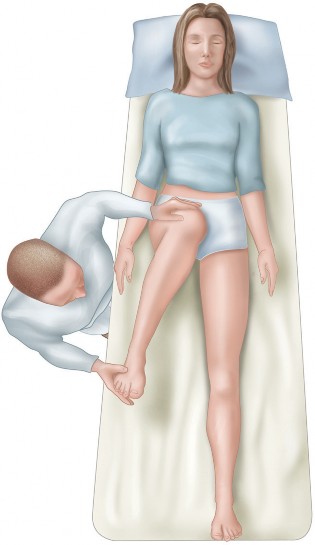
Patient positioning is critical to facilitate fluoroscopic access and intraoperative manipulation. The patient is placed supine on a fully radiolucent operating table. A bump is placed under the ipsilateral hemipelvis to elevate the surgical field, and the ipsilateral lower extremity is draped free to allow for full range of motion during the procedure.


Fluoroscopy must be positioned to obtain true anteroposterior, obturator oblique, and iliac oblique (Judet) views of the pelvis. The ability to seamlessly transition between these views without compromising the sterile field is essential for verifying osteotome placement and confirming final fragment reduction.


Detailed Surgical Approach and Technique
Superficial Dissection and Exposure
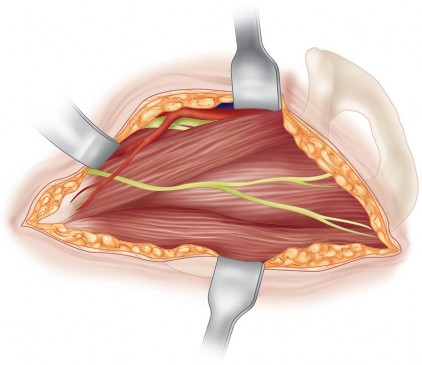
The procedure is most commonly performed through a modified Smith-Petersen approach or an anterior intrapelvic (ilioinguinal) approach. The incision begins along the anterior iliac crest, extending distally towards the anterior superior iliac spine, and curves distally along the interval between the tensor fasciae latae and the sartorius.


Careful identification and mobilization of the lateral femoral cutaneous nerve are imperative. The abdominal obliques and iliacus are elevated subperiosteally from the inner table of the ilium. The rectus femoris origin at the anterior inferior iliac spine may be preserved, tenotomized, or osteotomized depending on surgeon preference and required exposure.


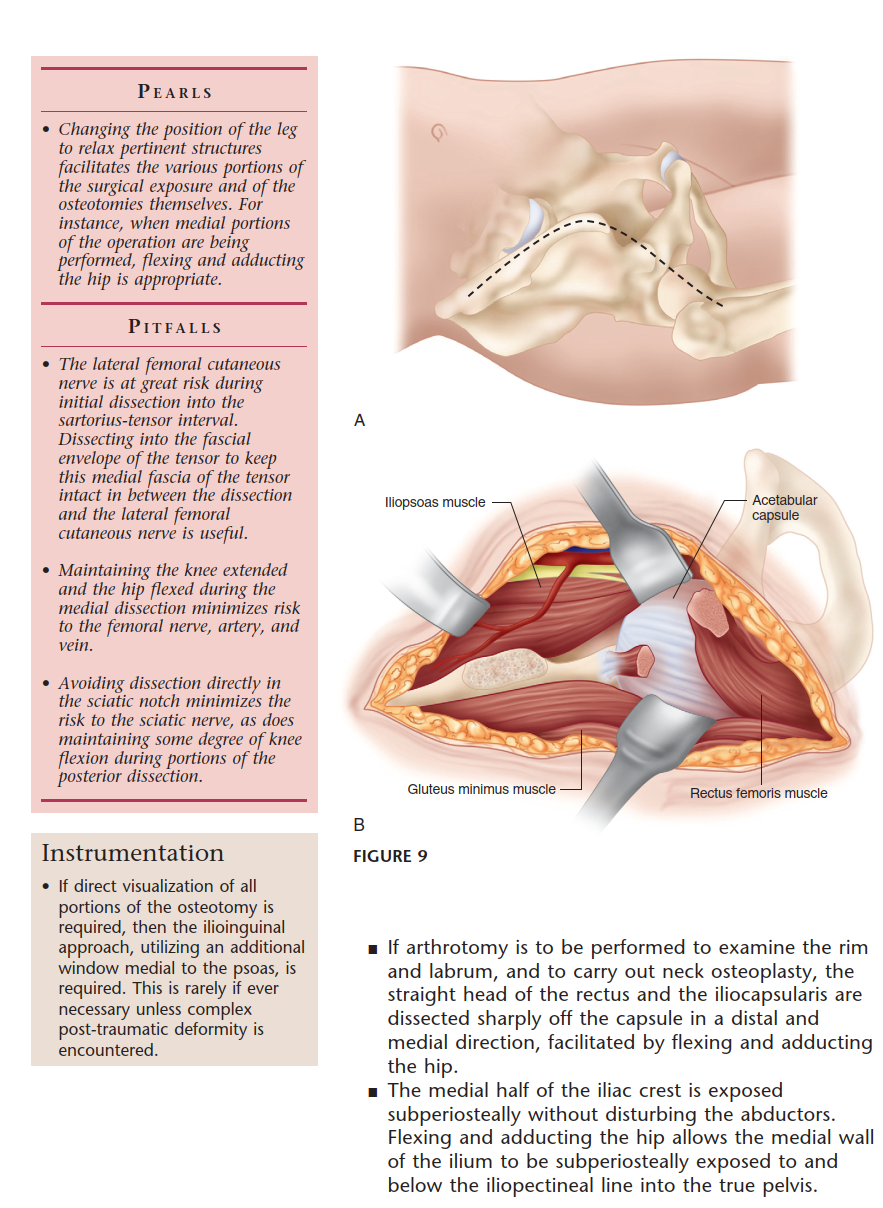
Deep Intrapelvic Dissection
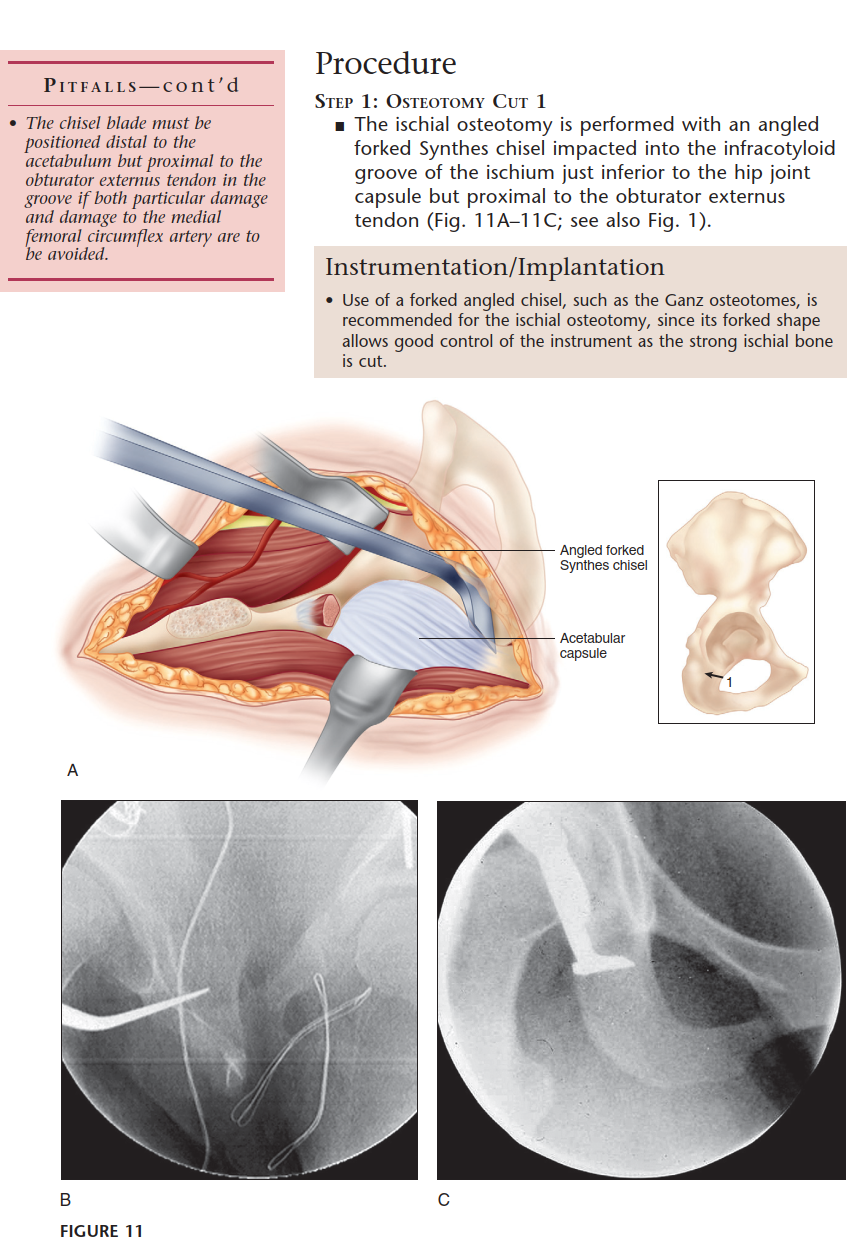
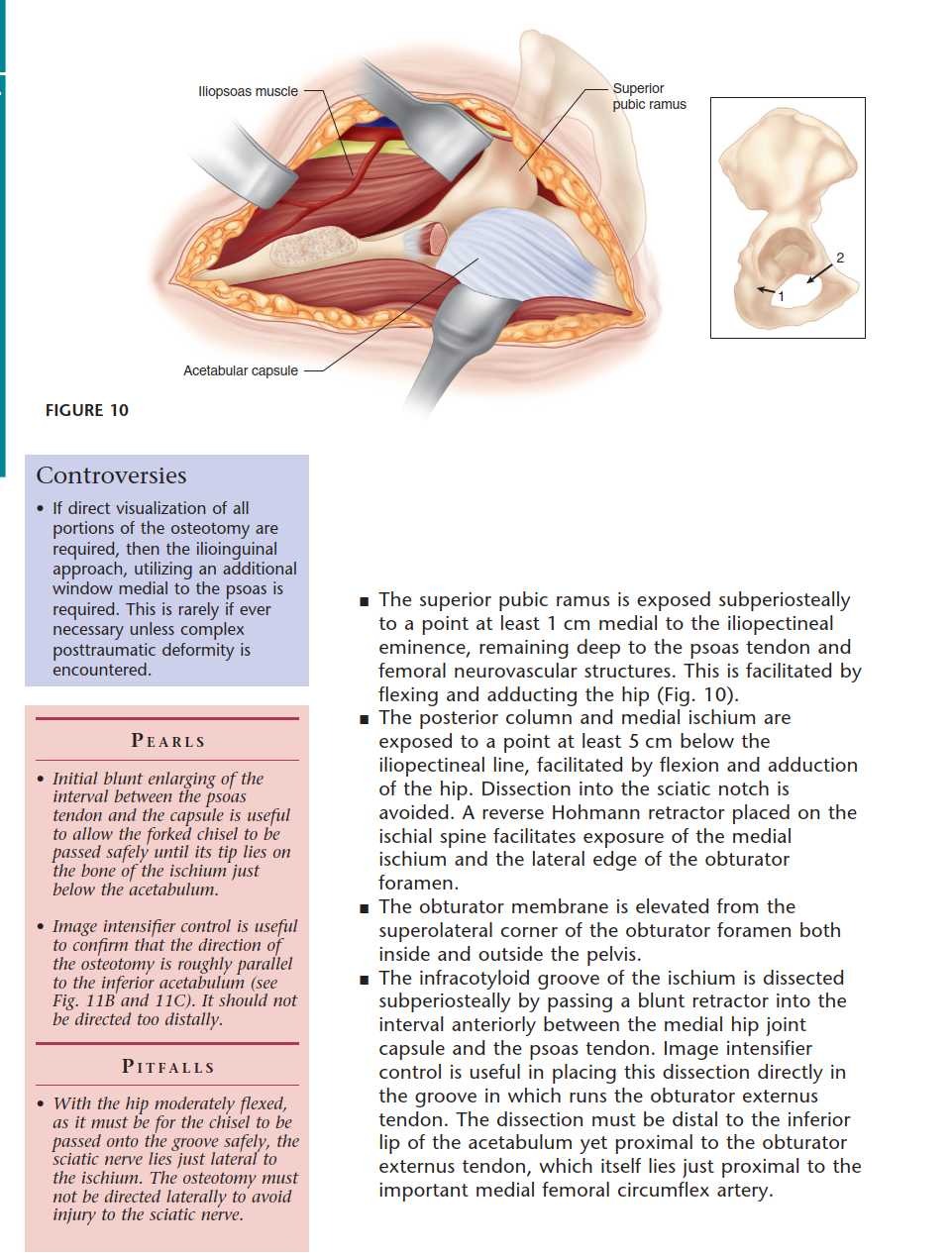
Subperiosteal elevation continues along the quadrilateral plate. The iliopectineal fascia is divided to allow the iliopsoas muscle and femoral neurovascular bundle to be retracted medially. The corona mortis is identified on the superior pubic ramus and meticulously ligated or cauterized. Dissection proceeds inferiorly to identify the ischium, specifically the infracotyloid groove, which serves as the starting point for the first osteotomy.

The Ganz Osteotomy Sequence
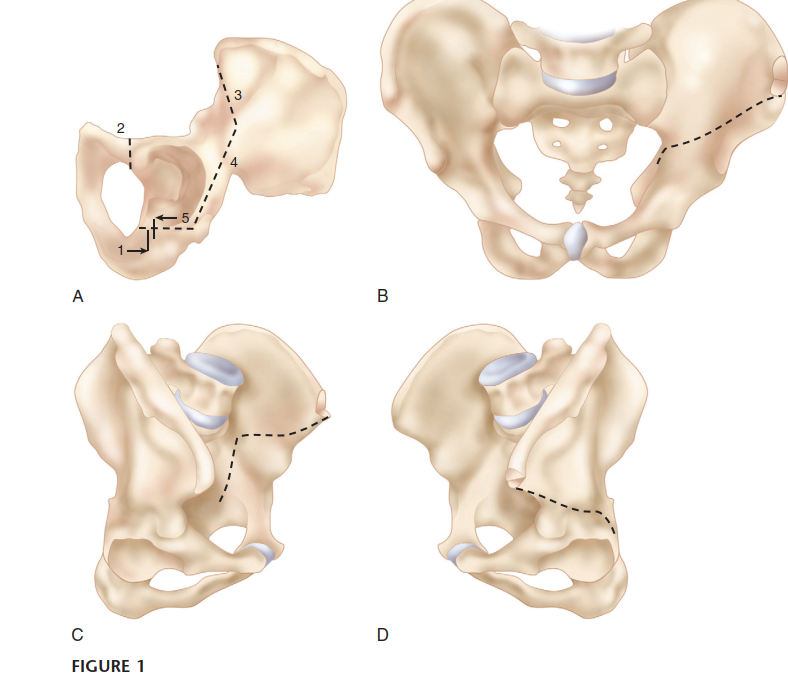
The Bernese periacetabular osteotomy consists of five distinct bone cuts. Execution in the correct sequence is vital for maintaining stability during the procedure.
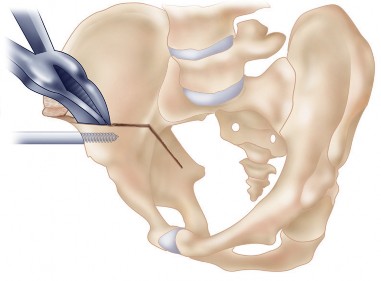
- Incomplete Ischial Osteotomy: An angled osteotome is passed subperiosteally down the quadrilateral plate to the infracotyloid groove. The cut is directed laterally and distally, stopping short of the posterior column.
- Pubic Osteotomy: Performed just medial to the iliopectineal eminence. A blunt retractor protects the obturator nerve and vessels inferiorly, and the femoral bundle superiorly.
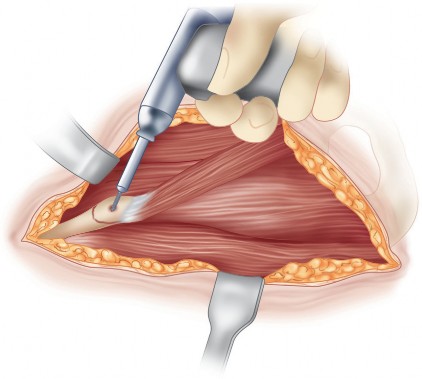
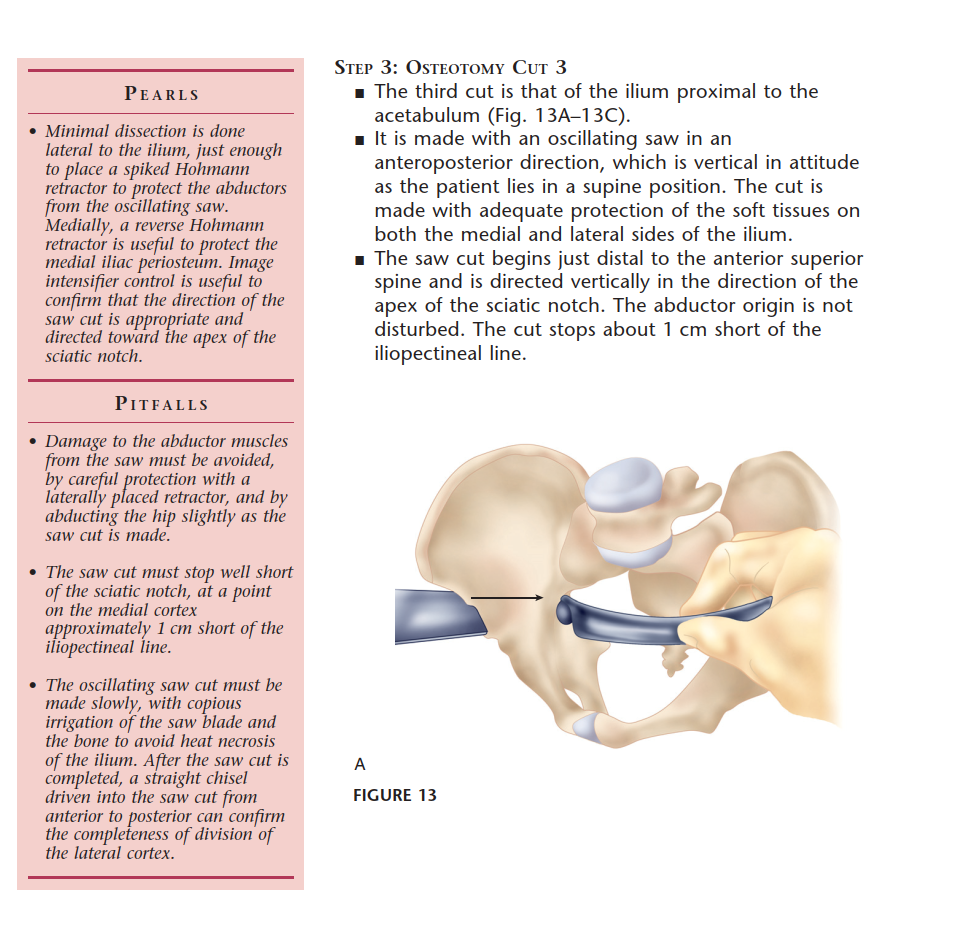
- Supra-acetabular Osteotomy: Initiated on the outer table of the ilium, just proximal to the joint capsule, extending medially towards the pelvic brim.
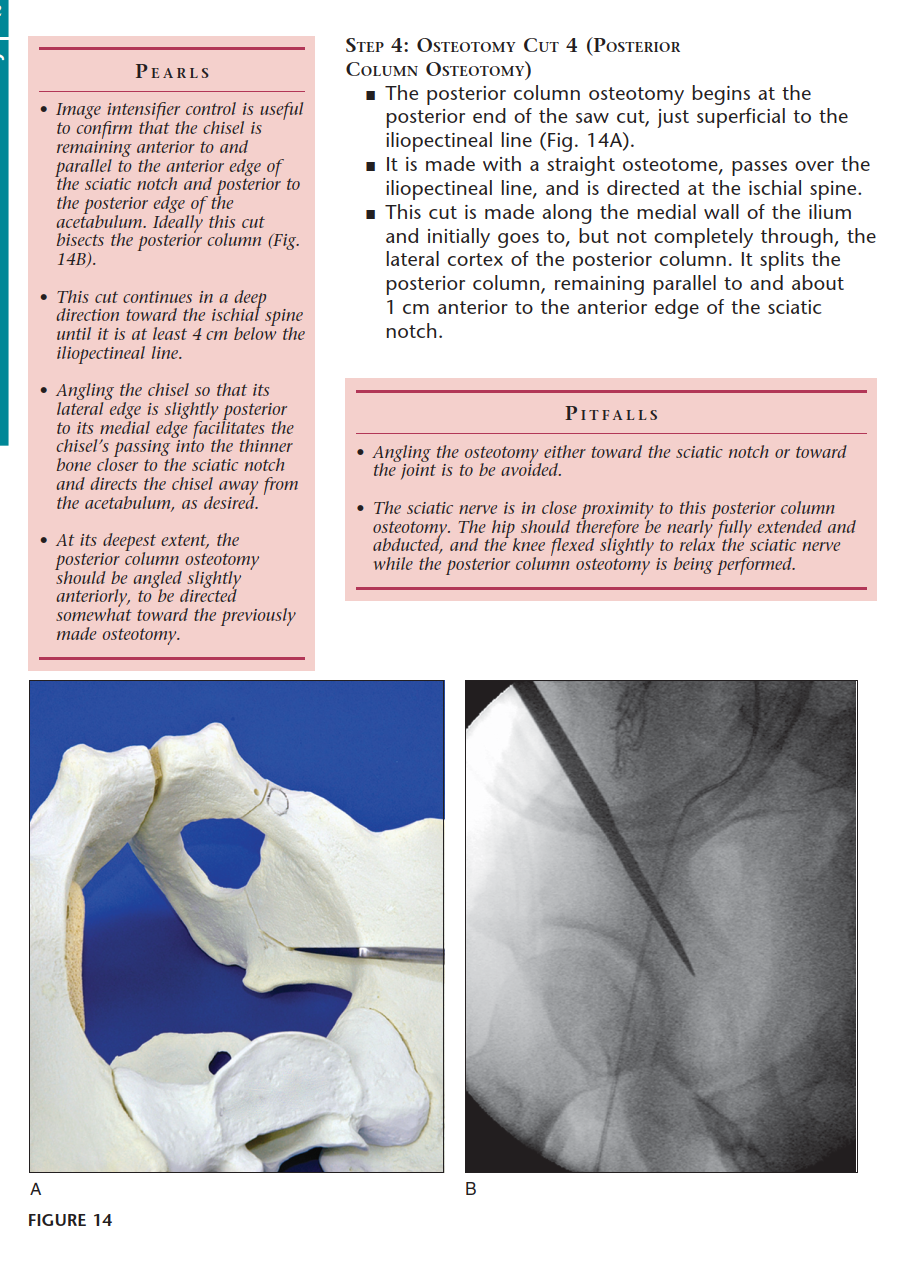
- Retroacetabular Osteotomy: Connects the supra-acetabular cut to the ischial cut. This is the most technically demanding step, requiring precise angulation to avoid violating the joint anteriorly or the posterior column posteriorly.
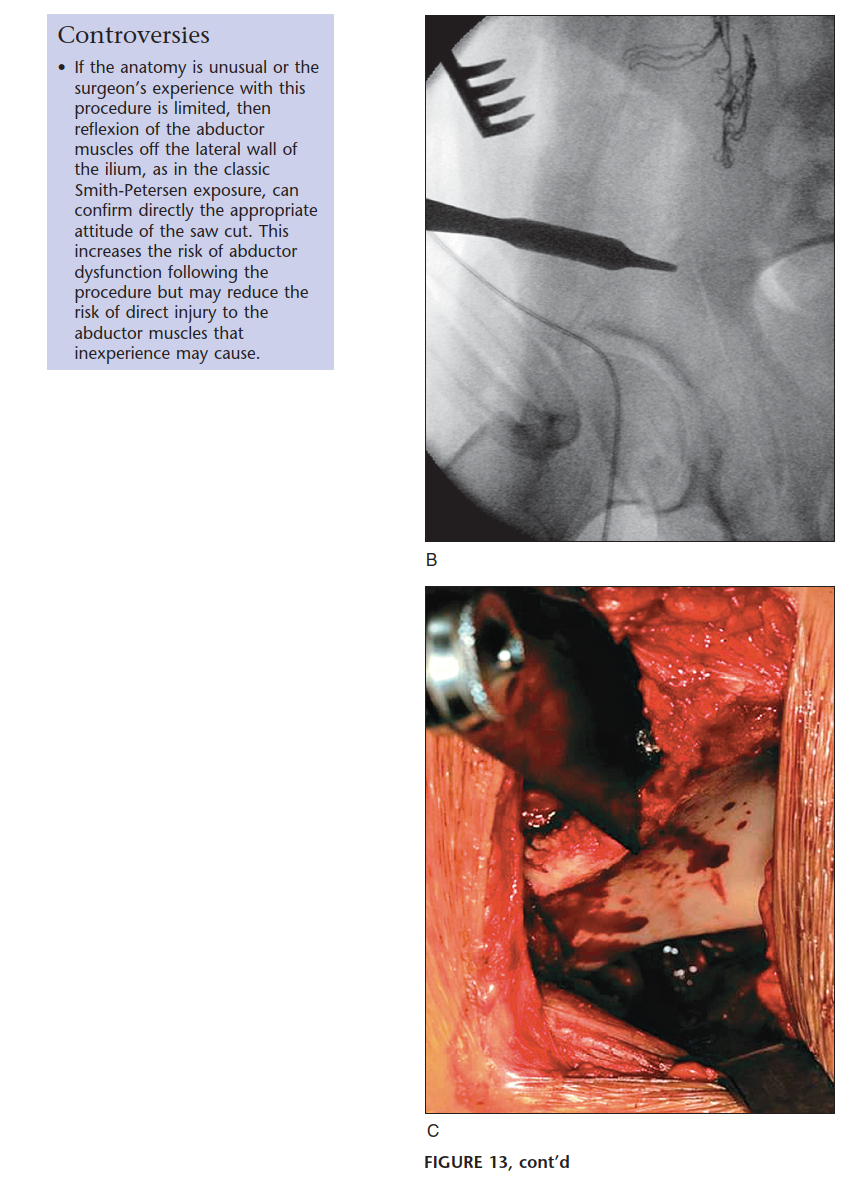
- Final Liberation: The remaining cortical bridges are fractured using controlled leverage with a Schanz pin placed in the supra-acetabular region of the fragment.

Fragment Mobilization and Fixation
Once liberated, the acetabular fragment is highly mobile. A heavy Schanz pin is inserted into the dense bone of the supra-acetabular region to serve as a joystick. The fragment is typically reoriented via a combination of flexion, internal rotation, and medialization.

Fluoroscopy confirms the correction, ensuring a normalized lateral center-edge angle, horizontal Tönnis roof, and appropriate anterior coverage without inducing retroversion (which could cause iatrogenic femoroacetabular impingement). Fixation is achieved using three or four fully threaded 3.5mm or 4.5mm cortical screws directed from the intact ilium into the mobilized fragment.

Complications and Management
Despite its biomechanical elegance, the Bernese periacetabular osteotomy is associated with a steep learning curve and potential for significant complications. Intra-articular fracture extension typically occurs during the retroacetabular cut if the osteotome is directed too anteriorly. Posterior column fracture compromises pelvic stability and necessitates internal fixation.

Neurologic injuries most commonly affect the lateral femoral cutaneous nerve, resulting in anterolateral thigh numbness. Sciatic nerve injury is less common but devastating, usually resulting from over-penetration during the ischial cut. Vascular injuries, particularly to the corona mortis or obturator vessels, require immediate recognition and ligation.


Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| LFCN Neuropraxia | 15% - 30% | Careful superficial dissection; often resolves spontaneously. |
| Intra-articular Fracture | 2% - 5% | Precise fluoroscopic guidance; fix with countersunk screws if displaced. |
| Posterior Column Fracture | 1% - 3% | Avoid overly posterior retroacetabular cut; requires plate/screw fixation. |
| Iatrogenic FAI | 5% - 10% | Avoid excessive anterior coverage/retroversion; treat with subsequent arthroscopy. |
| Vascular Injury (Corona Mortis) | < 1% | Routine identification and ligation during pubic exposure; pack and ligate if bleeding occurs. |
| Nonunion / Delayed Union | 1% - 2% | Rigid internal fixation; bone grafting for persistent nonunion (rare). |


Post Operative Rehabilitation Protocols
The preservation of the posterior column allows for a more aggressive rehabilitation protocol compared to traditional pelvic osteotomies. Postoperative management is divided into distinct phases aimed at protecting the osteotomy sites while restoring joint kinematics and abductor strength.


Phase 1 (0 to 6 weeks) focuses on strict protection. Patients are restricted to toe-touch or flat-foot weight-bearing (approximately 20 pounds) on the operative extremity. Deep vein thrombosis prophylaxis is administered. Continuous passive motion machines and active-assisted range of motion exercises are initiated immediately to prevent capsular adhesions and nourish the articular cartilage.


Phase 2 (6 to 12 weeks) begins upon radiographic confirmation of early callus formation at the osteotomy sites. Weight-bearing is progressively advanced to full over a 4-week period. Emphasis shifts to active range of motion, core stabilization, and isometric abductor strengthening.

Phases 3 and 4 (3 to 6+ months) involve advanced closed-kinetic chain exercises, normalization of gait mechanics, and eventual return to impact activities and sports. Complete osseous integration and maximal functional recovery typically require 6 to 12 months.

Summary of Key Literature and Guidelines
The Bernese periacetabular osteotomy is supported by robust, long-term clinical data, establishing it as the premier joint-preserving operation for adult hip dysplasia. Long-term survivorship studies, particularly those originating from the Bern group (Steppacher et al.), demonstrate hip preservation rates exceeding 70% at 20 years follow-up in properly selected patients.

Level V evidence and expert consensus from high-volume hip preservation centers underscore several critical predictors of
Clinical & Radiographic Imaging

You Might Also Like


