Detailed Patient Presentation and Biomechanical Pathophysiology
The patient is a 21-year-old female with a body mass index (BMI) of 22, presenting with a classic and highly debilitating constellation of symptoms indicative of symptomatic adult developmental dysplasia of the hip (DDH). Her primary complaint consists of insidious-onset, progressive groin and lateral trochanteric pain that is heavily exacerbated by physical activity and persists well after the cessation of weight-bearing loads. This presentation is the hallmark of the "dysplastic cascade," wherein a structurally deficient acetabulum fails to provide adequate osseous coverage for the femoral head, leading to supraphysiologic sheer forces across the articular cartilage and the chondrolabral junction. Over the past twenty-four months, she has undergone exhaustive non-operative management, including targeted physical therapy focusing on core and pelvic stabilizer strengthening, activity modification, and the scheduled use of non-steroidal anti-inflammatory drugs (NSAIDs). Unfortunately, these conservative measures have failed to halt the progression of her symptoms, a common trajectory when the underlying pathology is a fundamental geometric mismatch of the hip joint.
To understand this patient's clinical picture, one must delve into the specific biomechanics of hip dysplasia. In the normal hip, the acetabulum provides a deep, congruent socket that distributes joint reaction forces evenly across a broad surface area of hyaline cartilage. In this patient's dysplastic hip, there is significant lateral uncoverage of the femoral head. This structural deficiency shifts the weight-bearing zone to a drastically reduced surface area on the lateral acetabular rim. Consequently, the joint contact pressures skyrocket in this localized region, leading to edge-loading. The labrum, which normally functions as a suction seal and a secondary stabilizer, is forced to take on a primary load-bearing role for which it is not histologically equipped. This chronic mechanical overload has predictably resulted in a labral tear, which is the primary source of her deep, sharp groin pain.

Furthermore, the patient's lateral trochanteric pain highlights the extra-articular consequences of intra-articular instability. Because the femoral head is subluxated laterally and superiorly, the center of rotation of the hip joint is displaced. This displacement shortens the lever arm of the hip abductor musculature (primarily the gluteus medius and minimus). To maintain a level pelvis during the single-leg stance phase of the gait cycle, these muscles must generate significantly higher contractile forces than they would in a structurally normal hip. Over time, this chronic overexertion leads to abductor fatigue, myofascial pain, and secondary greater trochanteric pain syndrome (GTPS). Her low BMI of 22 is actually a favorable prognostic factor, as it limits the absolute joint reaction forces, but it has not been sufficient to protect her from the geometric realities of her dysplasia.
The failure of twenty-four months of conservative therapy is a critical inflection point in her clinical timeline. Prolonged non-operative management in the setting of symptomatic structural dysplasia and a known labral tear often leads to irreversible chondral damage. The cartilage of the anterosuperior acetabulum is particularly vulnerable to delamination due to the continuous shear forces exerted by the under-covered femoral head. Therefore, recognizing the limits of physical therapy in altering bone morphology is paramount. We are now faced with a young, otherwise healthy patient whose joint is actively deteriorating, necessitating a definitive, joint-preserving structural intervention before the onset of secondary osteoarthritis precludes any option other than total hip arthroplasty.
Comprehensive Clinical Examination Findings
A meticulous clinical examination is the cornerstone of evaluating the young adult dysplastic hip, bridging the gap between patient symptoms and radiographic metrics. Upon observation of the patient's gait, a subtle but distinct abductor lurch (compensated Trendelenburg gait) is noted. During the single-leg stance phase on the affected side, the patient shifts her torso laterally over the symptomatic hip. This compensatory maneuver medializes her center of gravity, thereby reducing the required force output from her exhausted gluteus medius and minimizing the resultant joint reaction force across the dysplastic joint. Static evaluation reveals no clinically significant leg length discrepancy, and her spinal alignment is unremarkable, ruling out a primary spinopelvic driver for her altered gait mechanics.
Assessment of her hip range of motion (ROM) reveals an arc that is quantitatively normal but qualitatively pathologic. She demonstrates full flexion to 120 degrees, internal rotation of 35 degrees, and external rotation of 45 degrees in a seated position. However, this motion is accompanied by significant pain at the extreme endpoints. The presence of normal to hypermobile ROM is highly characteristic of DDH, where the shallow acetabulum fails to provide a bony block to extreme motion. The pain at the endpoints is multifactored: anteriorly, it represents impingement of the hypertrophied, torn labrum between the femoral neck and the deficient acetabular rim; posteriorly and laterally, it represents capsular strain as the hip attempts to subluxate out of its shallow socket.

Provocative testing is highly localizing in this patient. The anterior impingement test (FADIR: Flexion, Adduction, Internal Rotation) is strongly positive, reproducing her sharp, anterior groin pain. While classically associated with Femoroacetabular Impingement (FAI), a positive FADIR in a dysplastic hip typically indicates a mechanically overloaded and torn anterior labrum. Even more diagnostic is her positive anterior apprehension test. When the hip is brought into extension and external rotation, the patient experiences a profound sense of instability and apprehension, often accompanied by anterior pain. This occurs because the anterior capsuloligamentous structures (primarily the iliofemoral ligament) are chronically attenuated in DDH, and this maneuver forces the femoral head against the deficient anterior acetabular wall, simulating an anterior subluxation event.
Extra-articular palpation confirms the secondary effects of her altered biomechanics. There is marked point tenderness over the posterior and superior facets of the greater trochanter, corroborating the diagnosis of secondary abductor tendinopathy. Furthermore, the iliopsoas tendon is tender to palpation as it crosses the pelvic brim. In the dysplastic hip, the iliopsoas often hypertrophies and becomes a secondary dynamic stabilizer to resist anterior femoral head translation. This "psoas overactivity" leads to tendinitis and anterior snapping. Crucially, a thorough neurovascular examination of the lower extremities is entirely normal, with intact motor function, symmetric reflexes, and palpable distal pulses, ensuring that her symptoms are purely musculoskeletal in origin and not referred from a lumbosacral radiculopathy.
Advanced Imaging and Diagnostics
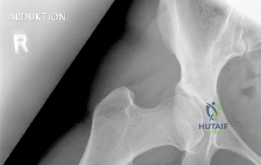
The radiographic evaluation of the dysplastic hip requires a highly standardized and rigorous protocol to accurately quantify the three-dimensional deformity. The initial assessment begins with a standing anteroposterior (AP) radiograph of the pelvis. In this patient, the AP view immediately reveals the hallmark signs of DDH: decreased anterolateral coverage of the femoral head and a broken Shenton line. The broken Shenton line—a step-off between the medial border of the femoral neck and the inferior border of the superior pubic ramus—indicates proximal and lateral migration of the femoral head due to structural instability. Furthermore, we observe an increased Tönnis angle (acetabular inclination) and a significantly reduced Lateral Center Edge Angle (LCEA) of Wiberg, confirming the diagnosis of severe lateral uncoverage.
Beyond the AP pelvis, the False Profile view of Lequesne and de Sèze is mandatory to evaluate anterior coverage, which is frequently deficient in DDH. This view allows for the measurement of the Anterior Center Edge Angle (ACEA). In this patient, the ACEA is markedly reduced, correlating directly with her positive anterior apprehension test and the anterior location of her labral tear. We must also scrutinize the AP radiograph for signs of acetabular retroversion, such as the crossover sign, ischial spine sign, and posterior wall sign. Dysplasia is rarely a simple lack of lateral coverage; it is often a complex, multi-planar deformity where the acetabulum is not only shallow but also maloriented in the sagittal and axial planes.

The most critical functional radiograph in our preoperative workup is the AP Abduction view (often taken with the hip in 20-30 degrees of abduction and slight internal rotation). This view simulates the mechanical effect of a periacetabular osteotomy by effectively "rotating" the femoral head deeper into the acetabular dome. In this patient's case, the abduction view demonstrates excellent achievable congruency and congruity. The joint space becomes symmetric, and the femoral head centralizes perfectly within the socket. This is the ultimate litmus test for joint preservation: if the abduction view shows persistent incongruency or a "hinging" effect where the joint space narrows medially, a reorientation osteotomy may be contraindicated, as it would simply rotate a misshapen socket over a misshapen head, accelerating arthrosis.

To complete the diagnostic picture, advanced cross-sectional imaging is employed. A high-resolution Magnetic Resonance Imaging (MRI) arthrogram is the gold standard for evaluating the intra-articular soft tissues. In this patient, the MRI confirms a complex tear of the anterosuperior labrum, with associated paralabral cysts indicating chronic failure of the suction seal. Crucially, we utilize delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) or T2 mapping to assess the biochemical integrity of the hyaline cartilage. The patient demonstrates preserved cartilage thickness without deep delamination or full-thickness chondral defects, confirming that she is in the pre-arthritic phase of the dysplastic cascade and is an ideal candidate for a joint-preserving Bernese Periacetabular Osteotomy.
Exhaustive Differential Diagnosis
When evaluating a 21-year-old female with insidious onset groin and lateral hip pain, the differential diagnosis is broad and must be systematically narrowed. The challenge lies in differentiating primary structural pathologies from secondary soft-tissue adaptations, as well as ruling out extra-articular mimics that can present with nearly identical symptomatology. The primary categories of consideration include intra-articular morphologic abnormalities, intra-articular soft tissue derangements, extra-articular tendinopathies, and referred pain syndromes.
The most prominent differential diagnosis in this demographic is Femoroacetabular Impingement (FAI). While DDH represents a state of under-coverage and instability, FAI represents a state of over-coverage and abnormal contact. However, the two can occasionally coexist or mimic one another. For instance, a dysplastic patient may develop a secondary "cam" deformity on the femoral neck as a biologic response to instability, leading to secondary impingement when the hip is flexed. Alternatively, a patient with a primary labral tear without underlying bony dysplasia might present with similar groin pain and a positive FADIR test, but their imaging will lack the characteristic shallow acetabulum and broken Shenton line seen in our patient.
Extra-articular conditions must also be heavily weighed. Athletic pubalgia (core muscle injury) presents with deep groin pain exacerbated by activity, but the pain is typically localized to the pubic symphysis or the insertion of the rectus abdominis, and hip ROM is usually pain-free. Snapping hip syndrome (coxa saltans), particularly internal snapping of the iliopsoas over the iliopectineal eminence, is frequently seen in dysplastic patients as the psoas hypertrophies to provide dynamic stability. While our patient has elements of secondary greater trochanteric pain syndrome, we must ensure this is not her primary pathology. The normal neurovascular exam rules out lumbar radiculopathy or nerve entrapment syndromes (such as meralgia paresthetica).
| Pathology | Primary Pathomechanics | Key Clinical Findings | Radiographic Hallmarks | Treatment Focus |
|---|---|---|---|---|
| Developmental Dysplasia of the Hip (DDH) | Acetabular under-coverage leading to structural instability and edge-loading. | Groin pain, + Apprehension test, hypermobility, abductor fatigue. | LCEA < 20°, broken Shenton line, increased Tönnis angle. | Joint preservation (PAO) to restore bony coverage and mechanics. |
| Femoroacetabular Impingement (FAI) | Abnormal contact between femoral head/neck and acetabular rim (Cam/Pincer). | Groin pain, restricted internal rotation, strongly + FADIR test. | Alpha angle > 55°, crossover sign, coxa profunda. | Arthroscopic osteochondroplasty and labral repair. |
| Primary Labral Tear | Traumatic or degenerative disruption of the chondrolabral junction. | Mechanical symptoms (clicking, catching), + FADIR, no gross instability. | Normal bony morphology, MR arthrogram shows contrast in labrum. | Arthroscopic labral repair or reconstruction. |
| Athletic Pubalgia (Core Muscle Injury) | Shearing forces across the pubic symphysis causing rectus/adductor microtears. | Pain with resisted sit-ups or adduction, pain over pubic tubercle. | Normal hip x-rays. MRI shows edema at pubic symphysis/aponeurosis. | Core rehab, potential surgical pelvic floor repair. |
In synthesizing the clinical and radiographic data, it is unequivocally clear that this patient's primary driver of pathology is structural DDH. The labral tear and the trochanteric pain are secondary victims of the primary geometric mismatch. Treating the labrum in isolation via arthroscopy without addressing the bony dysplasia would be a catastrophic failure of clinical reasoning, as the repaired labrum would rapidly fail again under the uncorrected sheer forces of the dysplastic joint.
Complex Surgical Decision Making and Classifications
The decision to proceed with surgical intervention in the young adult dysplastic hip is governed by a delicate balance of patient symptomatology, radiographic parameters, and the presence or absence of degenerative changes. The primary goal is joint preservation—altering the biomechanical environment to halt the dysplastic cascade and prevent the onset of secondary osteoarthritis. In our 21-year-old patient, the presence of daily, activity-limiting pain that has failed 24 months of conservative management, combined with a Tönnis grade 0 to 1 joint (no to minimal arthritic changes), makes surgical intervention mandatory.

The definitive procedure of choice for symptomatic, pre-arthritic adult DDH is the Bernese Periacetabular Osteotomy (PAO), originally described by Reinhold Ganz in 1988. The genius of the Ganz PAO lies in its specific osteotomy cuts, which free the acetabulum from the hemipelvis while intentionally leaving the posterior column intact. This provides immense intrinsic stability to the pelvis, allowing for early mobilization and avoiding the need for postoperative spica casting, which was a major drawback of older triple pelvic osteotomies. Furthermore, because the osteotomies are extra-articular, the true volume of the pelvis is minimally altered, allowing for normal vaginal delivery in the future—a critical consideration for a 21-year-old female.

Preoperative 3D templating is a critical phase of the surgical decision-making process. The goal of the PAO is not simply to "cover the head," but to optimize the center of rotation and normalize joint reaction forces. By medializing the acetabulum, we decrease the lever arm of body weight and increase the lever arm of the abductors, drastically reducing the force required for single-leg stance. We must carefully calculate the required degrees of anterior and lateral rotation. A major pitfall in PAO surgery is overcorrection, which iatrogenically induces Pincer-type FAI by creating excessive anterior coverage. We utilize specialized planning software to simulate the osteotomy, ensuring that we achieve an LCEA of 25-30 degrees and an ACEA of roughly 30 degrees, while maintaining neutral acetabular version.
The management of the concurrent labral tear represents an area of evolving surgical philosophy. Historically, the labrum was either ignored or addressed via an open arthrotomy at the time of the PAO. However, modern joint preservation surgery often employs a hybrid approach. Depending on the severity of the tear, we may perform a concurrent hip arthroscopy immediately prior to the PAO to repair the labrum and assess the cartilage directly. Alternatively, if the labrum is simply hypertrophied and intrinsically stable, restoring the bony coverage via the PAO may offload the labrum sufficiently to render it asymptomatic. In this specific case, given the confirmed tear on MRI, we will plan for a comprehensive approach: structural reorientation via PAO, with readiness to address the intra-articular pathology to ensure a complete resolution of her groin pain.
Step-by-Step Surgical Technique and Intervention
The patient is positioned supine on a radiolucent operating table. General endotracheal anesthesia is induced, and a Foley catheter is placed to decompress the bladder. A bump is placed under the ipsilateral sacrum to slightly elevate the operative hemipelvis, and the entire lower extremity is prepped and draped free to allow for intraoperative manipulation. We utilize a modified Smith-Petersen (anterior iliofemoral) approach. The skin incision begins just distal to the anterior superior iliac spine (ASIS), extending distally and slightly laterally. We carefully dissect through the subcutaneous tissue to identify the internervous plane between the sartorius (femoral nerve) and the tensor fasciae latae (superior gluteal nerve). The lateral femoral cutaneous nerve is meticulously identified and protected, as neuropraxia of this nerve is the most common complication of this approach.

Once the superficial plane is developed, we detach the direct head of the rectus femoris from the anterior inferior iliac spine (AIIS) to expose the hip capsule. The iliopsoas tendon is identified and mobilized medially to protect the femoral neurovascular bundle. We then proceed with the four highly precise osteotomies that define the Bernese PAO.
1. The Incomplete Ischial Osteotomy: Using an angled osteotome, we create a cut roughly 1-2 cm below the inferior rim of the acetabulum. This cut must be incomplete to avoid violating the posterior column, and the osteotome must be directed carefully to avoid plunging into the sciatic nerve posteriorly or the hip joint superiorly.
2. The Pubic Osteotomy: The superior pubic ramus is exposed subperiosteally. Protecting the obturator neurovascular bundle inferiorly, we perform a complete osteotomy of the pubis just medial to the iliopectineal eminence using a reciprocating saw or osteotomes.
3. The Supra-acetabular Iliac Osteotomy: A saw is used to cut the ilium horizontally, starting from just below the ASIS and extending posteriorly toward the pelvic brim, stopping short of the sacroiliac joint.
4. The Retroacetabular Osteotomy: This is the most technically demanding cut. An osteotome is driven from the posterior end of the iliac cut, angling distally and anteriorly down the quadrilateral surface to connect with the initial ischial cut. This completely frees the acetabular fragment while leaving the posterior column intact.

With the acetabular fragment now mobile, a 5.0mm Schanz pin is placed into the supra-acetabular region to act as a joystick. The fragment is mobilized and rotated laterally and anteriorly to achieve the pre-planned coverage. We also intentionally medialize the fragment to optimize the abductor lever arm. The hip is taken through a full range of motion to ensure there is no iatrogenic anterior impingement. Fluoroscopy is utilized extensively at this stage. We obtain AP, false profile, and obturator oblique views to confirm the correction of the LCEA, ACEA, and Shenton's line, and to ensure the joint space remains perfectly congruent.
Once the optimal position is achieved and verified, provisional fixation is obtained with Kirschner wires. Definitive fixation is then achieved using three or four fully threaded 4.5mm cortical screws directed from the intact ilium down into the acetabular fragment. The screws must be carefully placed to avoid intra-articular penetration. After final fluoroscopic confirmation, the rectus femoris is reattached to the AIIS, and the wound is closed in layers over a deep subfascial drain. The skin is closed with a subcuticular suture to optimize the cosmetic outcome for this young patient.
Strict Post-Operative Protocol and Rehabilitation Stages
The postoperative rehabilitation following a Bernese Periacetabular Osteotomy is a highly structured, multi-phased protocol designed to protect the osteotomy sites while preventing stiffness and muscular atrophy. The immediate inpatient phase (Days 0-3) focuses on pain control, medical stabilization, and early mobilization. Pain is managed via a multimodal approach, often utilizing an epidural or a continuous peripheral nerve block (such as a fascia iliaca block) for the first 48 hours, transitioning to oral narcotics, acetaminophen, and gabapentinoids. Deep vein thrombosis (DVT) prophylaxis is initiated immediately, typically with low-molecular-weight heparin or a direct oral anticoagulant, given the significant pelvic surgery and reduced mobility. Physical therapy begins on postoperative day one, instructing the patient on strict partial weight-bearing (PWB) of 20 kilograms (roughly 45 lbs) on the operative extremity using bilateral crutches.
The early outpatient phase (Weeks 1-6) is heavily focused on protecting the osseous fixation while restoring basic muscle activation. The patient remains strictly on 20kg PWB. Range of motion exercises are permitted and encouraged within a pain-free arc to prevent capsular adhesions, but active hip flexion is often restricted to avoid excessive strain on the healing rectus femoris repair. Therapy focuses on isometric contractions of the quadriceps, hamstrings, and gluteal musculature. Aquatic therapy can be introduced once the surgical incision is fully healed, utilizing the buoyancy of water to allow for gait mechanics practice without overloading the osteotomy sites. At the 6-week mark, a comprehensive radiographic evaluation is performed to assess for early callus formation and to ensure no loss of fixation or fragment migration has occurred.
The intermediate phase (Weeks 6-12) marks the transition to functional recovery, contingent upon radiographic evidence of bony healing. If the 6-week radiographs are satisfactory, the patient is cleared to initiate a progressive return to full weight-bearing over a 2-to-3-week period, weaning from two crutches to one crutch, and finally to unassisted ambulation. The rehabilitation focus shifts dramatically to closed-kinetic-chain exercises. The gluteus medius, which has been chronically dysfunctional due to the preoperative dysplasia and further traumatized by the surgical approach, requires intensive, targeted strengthening. Exercises such as lateral band walks, single-leg bridges, and dynamic step-ups are introduced. Core stability and pelvic floor integration are also emphasized to ensure a stable base for the lower extremity.
The late phase and return to sport (Months 3-6+) is tailored to the patient's specific functional goals. Once the patient demonstrates a symmetric, pain-free gait and normal abductor strength (a negative Trendelenburg sign), impact loading and plyometric exercises can be gradually introduced. For this 21-year-old patient, the goal is a return to unrestricted physical activity. Sport-specific agility drills, cutting maneuvers, and endurance training are incorporated. It is crucial to counsel the patient that maximum medical improvement and complete resolution of muscular fatigue may take up to 12 to 18 months, as the surrounding soft tissues must adapt to the entirely new biomechanical geometry of her reconstructed hip joint.
High-Yield Clinical Pearls and Pitfalls
Mastering the Bernese Periacetabular Osteotomy requires an intimate understanding of complex pelvic anatomy and a deep respect for the potential complications inherent in major pelvic surgery. One of the most critical clinical pearls in patient selection is the evaluation of the posterior wall. Dysplasia is often accompanied by posterior wall deficiency. If the surgeon aggressively rotates the acetabulum anteriorly to cover the head, they may inadvertently uncover the head posteriorly, leading to iatrogenic posterior instability. Therefore, the "crossover sign" and the "posterior wall sign" must be meticulously evaluated on the preoperative AP radiograph. If the posterior wall is deficient, the surgeon must balance the anterior rotation carefully or consider a concurrent structural bone graft.
Intraoperatively, the precise execution of the osteotomies is fraught with potential pitfalls. The incomplete ischial cut is arguably the most dangerous. The osteotome must be angled precisely 15 degrees distally and 10 degrees medially. If the osteotome is directed too superiorly, it will breach the hip joint, causing catastrophic iatrogenic cartilage damage. If it is driven too far posteriorly and penetrates the posterior cortex of the ischium, it directly endangers the sciatic nerve. A key pearl here is to keep the hip in slight flexion and internal rotation during this cut, which relaxes the sciatic nerve and allows it to fall further away from the posterior bony margin. Similarly, during the pubic osteotomy, a blunt retractor must be placed subperiosteally along the inferior border of the superior pubic ramus to physically shield the obturator nerve and vessels from the saw blade.
A major conceptual pitfall is the failure to recognize and treat concurrent Femoroacetabular Impingement (FAI). As the dysplastic acetabulum is rotated to provide better coverage, any pre-existing cam deformity on the femoral head-neck junction will suddenly be brought into conflict with the newly positioned anterior acet
