Comprehensive Introduction and Patho-Epidemiology
Defining the Triple Innominate Osteotomy
The triple innominate osteotomy (TIO) is a highly sophisticated, joint-preserving surgical procedure designed to comprehensively reorient the acetabulum to achieve optimal coverage of the femoral head. Conceived to address the limitations of single-cut pelvic osteotomies, the TIO involves distinct, complete osteotomies of the ilium, ischium, and pubis. By freeing the acetabulum from its three primary pelvic attachments, the surgeon gains the unprecedented ability to rotate the acetabular fragment in three dimensions around the femoral head. This profound freedom of rotation allows the TIO to be utilized in cases of severe dysplasia and in older, skeletally immature children where a traditional Salter innominate osteotomy would fail to provide sufficient rotation or adequate anterolateral coverage. Crucially, the TIO is an articular-sparing procedure; it maintains the pristine hyaline cartilage contact between the femoral head and the acetabulum. This stands in stark contrast to salvage operations, such as the shelf procedure or the Chiari osteotomy, which rely on the metaplasia of the joint capsule into inferior fibrocartilage to act as a secondary weight-bearing surface.


Pathogenesis of Developmental Dysplasia of the Hip (DDH)
The etiology of developmental dysplasia of the hip is multifactorial, encompassing a complex interplay of genetic, mechanical, and hormonal variables. A strong genetic diathesis is confirmed by the high concordance rates among monozygotic twins and the significantly elevated incidence of DDH in infants with affected parents or siblings. Mechanically, intrauterine "packaging" problems play a critical role. Primigravida status, oligohydramnios, and high birth weight limit the intrauterine space, restricting fetal movement and leading to abnormal mechanical forces across the developing hip joint. This mechanical theory is further supported by the frequent clinical association of DDH with other packaging deformities, including congenital muscular torticollis and metatarsus adductus. Hormonally, the maternal production of relaxin and other ligamentous laxity-inducing hormones disproportionately affects female fetuses, explaining the striking female predominance in DDH. When these factors converge, the femoral head fails to seat concentrically within the acetabulum, leading to a shallow, dysplastic joint.
Pathogenesis of Legg-Calvé-Perthes Disease and Avascular Necrosis
In contrast to the primary structural deficiency seen in DDH, Legg-Calvé-Perthes disease (LCPD) represents an idiopathic avascular necrosis (AVN) of the capital femoral epiphysis in the developing child. While the exact etiology remains elusive, it is characterized by a temporary disruption of the blood supply to the femoral head, leading to infarction, subsequent fragmentation, and eventual reossification. A consistent finding in LCPD is delayed skeletal maturation; many postulate that LCPD may represent a localized form of epiphyseal dysplasia where the delayed maturation of the preossific nucleus fails to adequately protect the vulnerable retinacular vessels ascending the femoral neck. Furthermore, recent hematologic studies have implicated a hypercoagulable state—specifically, deficiencies in protein C and protein S—as a potential trigger for microvascular thrombosis. Environmental insults, notably passive exposure to tobacco smoke, have also been strongly correlated with the onset of LCPD, likely exacerbating these underlying microvascular vulnerabilities.
Natural History and the Imperative for Intervention
The natural history of untreated or undertreated hip dysplasia is the inexorable progression to premature secondary osteoarthritis (OA). A dysplastic hip is characterized by a shallow acetabulum with an upturned sourcil (the radiographic "eyebrow" representing the sclerotic weight-bearing zone). This aberrant geometry drastically reduces the contact area between the femoral head and the acetabulum, exponentially increasing the sheer forces across the articular cartilage. Over time, these pathological shear stresses lead to labral hypertrophy, eventual labral tearing, chondral delamination, and early-onset degenerative joint disease, frequently necessitating total hip arthroplasty in young adulthood. In LCPD, the natural history is heavily dependent on the age of onset and the extent of epiphyseal involvement (Herring lateral pillar classification). Children presenting under the age of 8 with Herring A classification generally experience a benign course. However, older children with Herring B or C classifications are at severe risk for lateral subluxation, hinge abduction, and permanent loss of femoral head sphericity, resulting in a joint that is mechanically doomed without aggressive surgical containment.


Detailed Surgical Anatomy and Biomechanics
Osteology and the Triradiate Cartilage
The immature pelvis is a complex biomechanical structure where the acetabulum is formed by the confluence of three distinct bones: the ilium, the ischium, and the pubis. These three osseous components are united by the triradiate cartilage, a vital, triflanged physeal growth center. The triradiate cartilage is solely responsible for the proportional expansion of the acetabulum, ensuring it grows in tandem with the enlarging femoral head to provide a deep, stable, and congruent joint. The fundamental brilliance of the TIO lies in its precise anatomical routing: the osteotomies are meticulously planned to bypass the triradiate cartilage entirely. Because the procedure does not violate this critical growth center, it can be safely executed in skeletally immature patients without the catastrophic risk of inducing premature physeal arrest. Consequently, the intrinsic volume of the acetabulum remains constant, while the entire complex is redirected to maximize the weight-bearing surface over the femoral head.



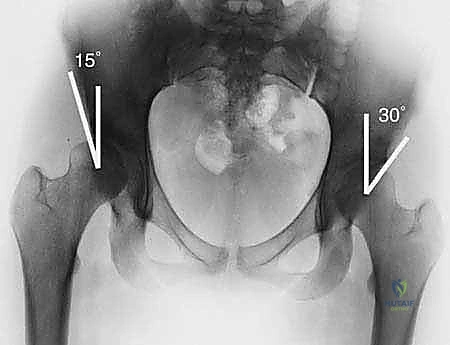
Biomechanics of Acetabular Coverage
In a biomechanically sound hip, the femoral head is concentrically contained by the concave roof of the acetabulum, characterized by a transverse or slightly down-sloping sourcil that gracefully wraps around the femoral head. This geometry ensures that joint reactive forces are distributed evenly across the maximum possible surface area of hyaline cartilage. The center-edge (CE) angle of Wiberg—defined as the angle formed between a vertical line drawn through the center of the femoral head and a line connecting the center of the head to the lateral-most edge of the acetabular roof—is the standard metric for lateral coverage. A normal CE angle should exceed 25 degrees. In the dysplastic hip, the CE angle is severely diminished, the acetabulum is flat, and the sourcil is upturned. This morphological failure results in lateral subluxation of the femoral head, which can be quantified as the percentage of the head remaining uncovered by the acetabular roof. The TIO corrects this by restoring a normal CE angle and converting pathological sheer forces back into physiological compressive forces.


Femoral Head Sphericity and Congruency
The success of any acetabular reorientation procedure is heavily predicated on the sphericity and congruency of the femoral head. The normal hip joint boasts a perfectly spherical femoral head that articulates congruently with the hemispherical acetabulum. Sphericity can be rigorously evaluated using Mose templates, which consist of concentric circles applied to the radiographic image of the femoral head. In conditions like LCPD or post-infectious AVN, the femoral head loses its sphericity, becoming enlarged (coxa magna), flattened (coxa plana), or irregularly shaped. Deformity in Perthes disease is often quantified by the percentage of lateral pillar collapse compared to the contralateral, unaffected side. While TIO is primarily an acetabular procedure, it is frequently utilized to improve the containment of a malformed femoral head, leveraging the biological plasticity of the pediatric hip to encourage remodeling of the head into a more spherical shape during the reossification phase.
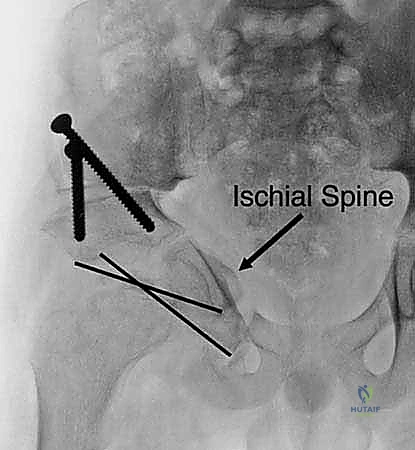
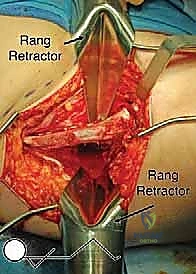
Neurovascular Proximity and Surgical Risk Zones
The surgical anatomy of the TIO is fraught with proximity to critical neurovascular structures, demanding meticulous dissection. The iliac osteotomy, extending from the anterior inferior iliac spine (AIIS) to the greater sciatic notch, places the superior gluteal nerve and artery at risk, particularly if retractors are placed too far posteriorly. The ischial cut, typically performed via an infracotyloid approach, requires careful mobilization of the hamstrings and protection of the sciatic nerve, which courses directly posterior to the ischium. Finally, the pubic osteotomy, executed medial to the iliopectineal eminence, endangers the obturator nerve and vessels lying within the obturator foramen, as well as the femoral neurovascular bundle situated anteriorly. Mastery of these anatomical relationships is non-negotiable for the safe execution of the TIO.


Exhaustive Indications and Contraindications
Spectrum of Operative Indications
The indications for TIO are broad but require careful patient selection. TIO is the gold standard for correcting severe primary acetabular dysplasia and residual dysplasia resulting from the incomplete treatment of DDH in children aged 10 years up until the closure of the triradiate cartilage. It is specifically indicated when the degree of dysplasia is too severe for a Salter osteotomy to provide adequate coverage. In the realm of LCPD, TIO is indicated for surgical containment of the capital femoral epiphysis in older children (onset >8 years) or those with severe (Herring B or C) disease, particularly during the biologically active fragmentation and reossification phases. Furthermore, TIO is highly effective for managing hip subluxation secondary to neuromuscular conditions, including cerebral palsy, myelomeningocele, Down syndrome, and Charcot-Marie-Tooth syndrome, where muscle imbalance has driven secondary osseous dysplasia.
Recognizing Contraindications
Contraindications to TIO must be strictly observed to prevent catastrophic joint failure. The absolute contraindication is a skeletally mature patient with a closed triradiate cartilage; in these individuals, a periacetabular osteotomy (PAO, such as the Ganz osteotomy) is strongly preferred because it leaves the posterior column intact, preserving pelvic stability and allowing for immediate postoperative mobilization. Severe joint incongruity or established osteoarthritis (Tonnis grade 2 or 3) is a major contraindication, as reorienting a degenerated joint will only accelerate its demise. Furthermore, the presence of fixed hinge abduction—where the enlarged, deformed femoral head levers against the lateral margin of the acetabulum during abduction, causing the joint to pry open medially—is a contraindication to isolated TIO unless the hinge can be abolished with a concomitant proximal femoral varus osteotomy.
| Category | Indications for TIO | Contraindications for TIO |
|---|---|---|
| Patient Age/Skeletal Maturity | Older children (typically >10 years); Open triradiate cartilage | Skeletally mature (closed triradiate cartilage -> PAO preferred) |
| Primary Diagnosis | Severe DDH; Residual DDH; Neuromuscular dysplasia (CP, Spina Bifida) | Advanced osteoarthritis; Active joint infection |
| LCPD / AVN | Herring B/C in older children; Need for surgical containment | Fixed hinge abduction (unless addressed concomitantly) |
| Joint Mechanics | Spherical or remodeling femoral head; Congruent reduction possible | Severe incongruity; Stiff hip with lack of functional ROM |

Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Symptomatology
A rigorous clinical evaluation forms the foundation of pre-operative planning. Children with hip dysplasia may be entirely asymptomatic in early childhood, but as sheer stresses accumulate, they inevitably develop symptoms. The classic presentation involves insidious onset of deep groin pain, which must be carefully differentiated from lateral trochanteric pain (often bursitis) or posterior pain (often spinal or sacroiliac in origin). Pain exacerbated by internal rotation or prolonged activity strongly suggests labral pathology or early chondral damage. Physical examination frequently reveals a positive Trendelenburg sign, indicative of abductor mechanical disadvantage secondary to lateralization of the hip center. In LCPD, patients may present with referred knee pain, an episodic antalgic gait, and a marked loss of abduction and internal rotation. Crucially, the surgeon must assess for hinge abduction by ranging the hip in full extension; if the pelvis rotates rather than the hip abducting, a hinge is present, signaling a poor prognosis and altering the surgical plan.
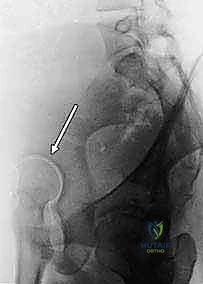
Comprehensive Radiographic Evaluation
Standardized radiographic evaluation is paramount. The protocol must include an anteroposterior (AP) radiograph of the pelvis obtained with the patient supine and the patellae oriented strictly forward to control for femoral version. This view allows calculation of the CE angle of Wiberg, the acetabular index, and the extrusion index. A frog-leg lateral radiograph provides an orthogonal view to assess the sphericity of the femoral head and the extent of anterior/posterior head involvement in LCPD. Because the AP and frog-leg views do not adequately profile the anterior acetabular rim, a false-profile radiograph (Lequesne and de Sèze) is mandatory to evaluate anterior coverage and measure the anterior center-edge angle.

Advanced Imaging and Dynamic Assessment
Plain radiographs provide only a static, two-dimensional representation of a complex three-dimensional deformity. Therefore, three-dimensional computed tomography (3D CT) with multiplanar reconstructions and femoral head subtraction is increasingly utilized to precisely map the acetabular deficiency, evaluate version, and plan the axis of rotation. Magnetic resonance imaging (MRI), preferably with intra-articular gadolinium arthrography, is the modality of choice for evaluating the integrity of the labrum, the articular cartilage, and the vascularity of the femoral head. However, the most critical pre-operative study remains the dynamic arthrogram, performed personally by the operating surgeon under fluoroscopy. The dynamic arthrogram allows direct visualization of the cartilaginous anlage, assesses the congruency of the joint in various positions, and definitively rules in or out the presence of hinge abduction. It dictates the exact position of containment required, guiding the intraoperative rotation of the acetabular fragment.


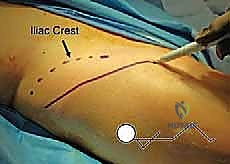
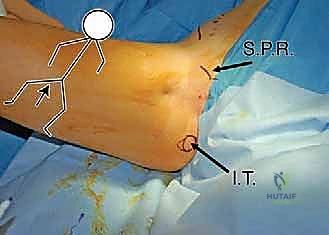
Patient Positioning and Surgical Preparation
Optimal patient positioning is critical to the fluid execution of the TIO. The patient is placed supine on a radiolucent operating table to facilitate unhindered intraoperative fluoroscopy. A small bump is placed under the ipsilateral sacrum to elevate the operative hip slightly, bringing the iliac crest into better relief. The entire hemipelvis, from the umbilicus to the toes, is prepped and draped free in a sterile fashion. This extensive draping is essential, as it allows the surgeon to freely manipulate the lower extremity—flexing
Clinical & Radiographic Imaging Archive