This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set 2915AD)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
of 100
Which surgical approach is less useful for children who have reached walking age because it does not allow for capsulorrhaphy?
1
Medial
2
Anterior
3
Lateral
4
Posterior
- Medial_
QUESTION 2 OF 50
A 63-year-old man has long-standing type 2 diabetes. He has had associated ongoing neuropathy for approximately 5 years. He now reports a red, hot, swollen right foot for the past 2 days. You place him supine in your office with the foot elevated for 30 minutes. You return to see that the redness has dissipated. What is the most likely diagnosis?
1
Cellulitis
2
Osteomyelitis
3
Charcot arthropathy
4
Sjogren syndrome
5
Reynaud syndrome
Charcot arthropathy is a progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities. This disorder results in progressive destruction of bone and soft tissues at weight-bearing joints; in its most severe form, it may cause significant disruption of the bony architecture. In patients with diabetes, the incidence of acute Charcot arthropathy of the foot and ankle ranges from 0.15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot’s skin temperature), erythema,joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective
sensation, are often pathognomonic of acute Charcot arthropathy.Cellulitis is an infection of the skin and osteomyelitis is an infection of the bone; examination of the limb would remain unchanged after 30 minutes of elevation. Reynaud and Sjogren syndromes are rheumatologic conditions that do not have these symptoms. CLINICAL SITUATION FOR QUESTIONS 101 THROUGH 103
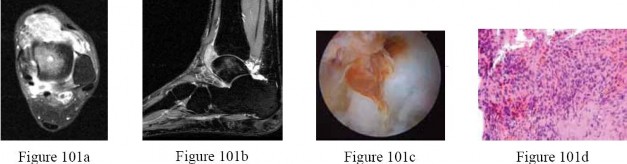
A 27-year-old woman has had pain in her right ankle for 2 years. Examination reveals a slightly warmjoint, without erythema. Ankle range of motion is limited by pain.
Radiographs are unremarkable.Because management consisting of immobilization, nonsteroidal anti-inflammatory drugs, and physiotherapy has failed to provide relief, MRI scans are obtained and shown in Figures 101a and 101b.An intraoperative image and the histology are shown in Figures 101c and 101d.
---
QUESTION 3 OF 50
When do most symptomatic thromboembolic events occur after total joint arthroplasty?
1
On the day of surgery
2
Within the first week after surgery
3
Between 1 week and 6 weeks after surgery
4
More than 3 months after surgery
Most clinical venous thromboembolism events occur between the second and sixth weeks after surgery. It is estimated that 10% of patients are readmitted to the hospital within the first 3 months after total hip or knee arthroplasties. Most pulmonary events on the day of surgery are related to fat embolism or cardiac events.
QUESTION 4 OF 50
When careful evaluation after primary total knee arthroplasty (TKA) is performed, the results of TKA after previous high tibial osteotomy (HTO) have a Knee Society good-to-excellent score what percentage of the time:
1
20%
2
40%
3
60%
4
80%
5
90%
Primary TKA with respect to Knee Society scores and operative complications shows that a primary TKA group scored 88% good to excellent results compared to 63% for the post-HTO group
QUESTION 5 OF 50
of 100
A 10-month-old boy has an untreated developmental hip dislocation.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.
Figure 46a
Figure 46b
Figure 46c
Figure 46d
QUESTION 6 OF 50
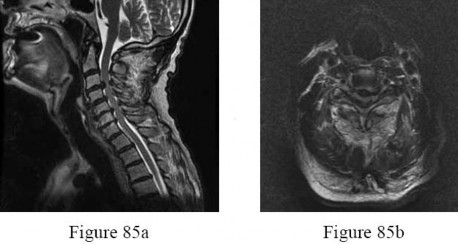
A 69-year-old man has nonpainful weakness in the upper and lower extremities. He also notes progressive instability in his gait and increasing difficulty ambulating, as well as manipulating small objects with his hands. MRI scans of his cervical spine are shown in Figures 85a and 85b. When would be the most appropriate time to proceed with surgical treatment? ---
1
When the patient is medically stable for surgery
2
When the MRI scans show multisegmental high-intensity intramedullary signal changes on T2-weighted sequences
3
When he reaches a Nurick grade of IV for his preoperative neurologic function
4
When he reports neck and/or extremity pain that becomes intolerable or not controlled by medication
5
When he develops bowel or bladder incontinence
The natural history of cervical myelopathy is one of slow deterioration over time, typically in a stepwise fashion with a variable period of stable neurologic function. More recent studies suggest that surgery should be performed as soon as possible when cervical spondylotic myelopathy has been diagnosed. Both anterior and posterior are effective and there is no statistical difference between their outcomes. Surgical outcome is related to the patient’s age, disease course, the presence of osseous spinal stenosis, preoperative comorbidities, the preoperative spinal cord functional score, and the presence of high-signal abnormalities on T2-weighted images. To improve the operative result, all the influencing factors should be considered. Patients with focal high-intensity intramedullary signal changes on T2-weighted images have better clinical outcomes following surgery than do patients with demonstrable multisegmental high-intensity intramedullary signal changes on T2-weighted sequences. The transverse area and shape of the spinal cord at the involved segment may also be predictive of surgical outcome.
With progressive compression, the cross section of the spinal cord changes from a boomerang shape to a teardrop shape to a triangular shape. In patients with a Nurick grade of I, there are signs of cord involvement, but gait remains normal. With a Nurick grade of II, there are mild gait abnormalities,not affecting the patient’s employment status. With a Nurick grade of III, gait abnormalities prevent employment, but the patient remains able to ambulate without assistance. In Nurick grade IV, the patient is only able to ambulate with assistance. In Nurick grade V, the patient is chair-bound or bedridden. Clearly, it is desirable to operate when the patient is functioning with a Nurick grade of I or II. Whereas many patients presenting with cervical spondylotic myelopathy also report axial neck pain and radicular symptoms in the upper extremities, this is not always the case. Surgical intervention will generally be effective in eliminating this pain; however, the pain is not the determining factor for performing surgery.Surgery is performed to preserve and restore function. Changes in bowel and bladder function can occur
in extremely severe cases of myelopathy, but this is quite rare.
QUESTION 7 OF 50
Which of the following tests is most specific for the diagnosis of Lyme disease:
1
Elevated erythrocyte sedimentation rate (ESR)
2
Elevated C -reactive protein (C RP)
3
Negative antinuclear antibody (ANA)
4
Negative rheumatoid factor
5
Elevated antibody titer to Borrelia burgdorferi
The most specific laboratory finding is an elevated antibody titer to Borrelia burgdorferi. This test is commonly referred to as a
Lyme titer.
All of the mentioned tests are generally seen in Lyme disease, however, elevated erythrocyte sedimentation rate, elevated C - reactive protein, negative antinuclear antibody, and negative rheumatoid factor are all nonspecific.
QUESTION 8 OF 50
A 52-year-old woman with diabetes mellitus has had a plantar foot ulcer under the second metatarsal head for the past week. The patient had a similar ulcer 2 months ago, and total contact casting resulted in healing. Examination reveals no signs of infection. What procedure will best prevent recurrence of the ulcer?
1
Flexor hallucis longus transfer to the Achilles tendon
2
Peripheral vascular bypass
3
Jones procedure (extensor hallucis longus transfer to the first metatarsal with interphalangeal joint fusion)
4
Posterior tibial tendon transfer to the anterior tibialis tendon
5
Achilles tendon lengthening
The contracted Achilles tendon leads to increased forefoot pressure, thus increasing the risk for ulceration in neuropathic patients. Several studies have shown the benefit of Achilles tendon lengthening to heal and prevent forefoot ulceration in these patients. The flexor hallucis longus transfer is used for chronically torn/deficient Achilles tendons, not a contracted Achilles tendon. The Jones procedure works well for the first ray but does not help to alleviate pressure under the second ray. Peripheral bypass surgery is unnecessary because the ulcer healed during the initial treatment, indicating that the patient has adequate circulation. The posterior tibial tendon transfer is used for foot drop or other neuromuscular conditions to correct deformity and increase function. It is not used for forefoot ulcers in patients with diabetes mellitus.
REFERENCES: Armstrong DG, Stacpoole-Shea S, Nguyen H, et al: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Meuller MJ, Sinacore DR, Hastings MK, et al: Effect of Achilles tendon lengthening on neuropathic plantar ulcers: A randomized clinical trial. J Bone Joint Surg Am
2003;85:1436-1445.
QUESTION 9 OF 50
A 58-year-old man has had a 3-year history of recurrent ulcerations of the left ankle and instability despite multiple attempts at custom bracing, contact casting, and surgical debridement. He has an ankle-brachial index of 0.76. A clinical photograph and radiographs are shown in Figures 16a through 16c. Treatment should now consist of
1
transtibial amputation.
2
a double upright brace.
3
dressing changes with platelet-derived growth factor.
4
tibiocalcaneal arthrodesis.
5
total ankle arthroplasty.
Nonsurgical management has failed to provide relief; therefore, the treatment of choice is arthrodesis with an intramedullary nail. Amputation may be indicated if the arthrodesis fails. The patient does have adequate circulation for an attempt at salvage. Total ankle arthroplasty is not indicated in a neuropathic patient.
REFERENCES: Pinzur MS, Kelikian A: Charcot ankle fusion with a retrograde locked intramedullary nail. Foot Ankle Int 1997;18:699-704.
Herbst SA: External fixation of Charcot arthropathy. Foot Ankle Clin 2004;9:595-609.
QUESTION 10 OF 50
A 60-year-old woman has progressive neck pain, upper extremity pain, and paresthesias. A lateral cervical spine radiograph and an MRI scan are shown in Figures 52a and 52b. What is the most likely underlying diagnosis?
1
Osteomyelitis
2
Ankylosing spondylitis
3
Age-related degenerative changes
4
Rheumatoid arthritis
5
Previous cervical decompression
The radiograph and sagittal T2-weighted MRI scan show multilevel degenerative changes and subaxial subluxations with anterolisthesis at C3-C4 and C4-C5 and retrolisthesis at C5-C6. In addition, there is evidence of midcervical kyphosis. Such findings are often seen in patients with rheumatoid arthritis. Patients with osteomyelitis typically show increased signal intensity in the disks and vertebral bodies. Patients with ankylosing spondylitis typically show ankylosis of the disks and vertebral bodies. Age-related degenerative changes typically manifest as degenerative disk disease with occasional single- level spondylolisthesis, but not typically multilevel spondylolisthesis, as seen in this patient. The spinous processes are intact; these changes do not appear to be postoperative.
QUESTION 11 OF 50
A 12-year-old girl is seen after tripping and twisting her ankle earlier in the morning. She had immediate pain and swelling and was unable to bear weight. Radiographs are shown in Figures 80a through 80c.
Appropriate treatment should consist of which of the following?
1
Short leg cast with no weight bearing for the first 3 weeks
2
Short leg cast with immediate weight bearing
3
Long leg cast with no weight bearing for the first 3 weeks
4
Open reduction and internal fixation, avoiding the physeal growth plate and joint
5
CAM walker with immediate weight bearing
DISCUSSION: Salter Harris III and IV fractures of the medial malleolus often contain a large cartilaginous portion, larger than the apparent ossified fragment seen on radiographs. Consequently, articular incongruity is common. As such, open reduction and internal fixation is often required. Growth disturbance and angular deformity are also common complications of Salter Harris III and IV fractures of the distal tibia.
REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.
Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:268-278.
QUESTION 12 OF 50
A 3-year-old girl with spina bifida is able to flex and adduct her hips, but she cannot extend her knees. The hips are both dislocated. The patientâs parents ask how the hips must be treated to optimize function. The recommended treatment is:
1
Observation
2
Bilateral closed reduction
3
Bilateral open reduction
4
Bilateral open reduction and femoral osteotomies
5
Bilateral open reduction with femoral osteotomies and muscle transfers
Nonoperative treatment will allow the patient to retain maximum mobility of the hips.
Operative treatment carries substantial risk of avascular necrosis, stiffness, and redislocation. These risks are not worth taking in view of the patientâs limited muscle strength about the hips. In addition, the motor level alluded to (L2-L3) means that she will not have sensation of pain from the hips.
QUESTION 13 OF 50
During surgical hip dislocation for the management of femoral acetabular impingement, preservation of what structure is paramount to maintaining vascularity to the femoral head? ](http://www.orthobullets.com/anatomy/10123/hip-blood-supply)
1
Metaphyseal vessels
2
Medial epiphyseal artery
3
Superficial branch of the medial femoral circumflex artery
4
Deep branch of the lateral femoral circumflex artery
5
Deep branch of the medial femoral circumflex artery
No detailed explanation provided for this question.
QUESTION 14 OF 50
Which is the most common mechanism for nerve injury after shoulder arthroplasty:
1
Laceration
2
Expanding hematoma
3
Contusion
4
Tearing
5
Temporary neuropraxia due to stretch
The most common reason for a nerve deficit following shoulder arthroplasty is a temporary neuropraxia due to stretch. Correct Answer: Temporary neuropraxia due to stretch
QUESTION 15 OF 50
of 100
A 17-year-old cross country athlete runs 7 miles per day, 6 days per week. She has new-onset right groin pain. Passive flexion of her hip is normal, but internal rotation of the hip, resisted hip flexion, and knee extension reproduce the pain. Hip radiograph findings are normal. What is the best next step?
1
Recommend decreasing training regimen
2
Obtain a bone scan
3
Obtain an MRI scan
4
Obtain a dual-energy x-ray absorptiometry (DEXA) scan
■ A stress fracture of the femoral neck or pelvis should be ruled out in this patient. She should be placed on crutches and not allowed to run. The consequences of missing such a diagnosis can be devastating. Superior cortical femoral neck stress fractures are tension injuries and can progress to a complete fracture and avascular necrosis. Surgical fixation may be indicated. Plain radiographic findings often do not appear until late in the clinical course. MRI is more accurate, more specific, and is superior to radionuclide bone scanning for the diagnosis of stress fracture in young endurance athletes. MRI detects early changes in osseous stress injury and allows precise definition of the anatomy and extent of injury. This patient may have the female athletic triad: disordered eating, amenorrhea, and osteoporosis. However, the workup for this condition (including a possible DEXA scan) may be delayed until after the stress fracture is diagnosed and treated.
QUESTION 16 OF 50
-A tendon repair is thought to be weakest during which phase of tendon healing?
1
Inflammatory
2
Proliferation
3
Maturation
4
Remodeling
No detailed explanation provided for this question.
QUESTION 17 OF 50
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15° of valgus, and forefoot supination can be corrected to 10° from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of
1
medial sliding calcaneal osteotomy with flexor digitorum longus (FDL) transfer.
2
isolated subtalar arthrodesis.
3
isolated talonavicular arthrodesis.
4
triple arthrodesis.
5
subtalar arthroereisis.
The most important determining factor for correction of an adult flatfoot without an arthrodesis is the flexibility of the subtalar and transverse tarsal joints. Rigid deformities cannot be corrected with a medial sliding calcaneal osteotomy with FDL transfer or a subtalar arthroereisis. Isolated subtalar or talonavicular arthrodesis does not correct the deformities entirely. If the patient has forefoot supination that can be corrected to less than 7°, an isolated subtalar fusion is a possible alternative.
REFERENCE: Mann RA: Flatfoot in adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 757-784.
QUESTION 18 OF 50
A 55-year-old patient is seeking a surgical consultation for a painful flatfoot deformity that has failed to respond to nonsteroidal anti-inflammatory drugs, shoe and activity modifications, and orthoses. The patient is of medium build, a nonsmoker, and has no history of diabetes mellitus. Radiographs are shown in Figures 43a through 43c. Based on these findings, treatment should consist of
1
triple arthrodesis.
2
lateral column lengthening with flexor digitorum longus tendon transfer.
subtalar arthroereisis with a Maxwell-Brancheau Arthroereisis titanium implant.
The patient has a degenerative collapse of the midfoot through the tarsometatarsal joints with significant forefoot abduction; therefore, a midfoot arthrodesis is required to address the arthritic joints and deformity at the tarsometatarsal articulation. All of the other procedures correct hindfoot deformities and therefore would not be appropriate treatment.
REFERENCES: Brage M: Degenerative joint disease of the midfoot. Foot Ankle Clin 1999;4:355-367.
Mann RA, Prieskorn D, Sobel M: Mid-tarsal and tarsometatarsal arthrodesis for primary degenerative osteoarthrosis or osteoarthrosis after trauma. J Bone Joint Surg Am
1996;78:1376-1385.
QUESTION 19 OF 50
Which of the following clinical findings is commonly associated with symptomatic partial-thickness rotator cuff tears?
1
Negative impingement signs
2
Abnormal lift-off test
3
External rotation lag sign
4
Painful arc with active range of motion
5
Mismatch in active and passive motion
In symptomatic partial-thickness rotator cuff tears, a painful arc with active range of motion is common, impingement signs are usually positive, and the lift-off test is normal. Active and passive range of motion measurements are often equal, although active range of motion can be painful. External rotation lag signs are often seen with larger full-thickness tears.
REFERENCES: Hertel R, Ballmer FT, Lambert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313.
McConville OR, Iannotti JP: Partial thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43.
Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Fukuda H: Partial-thickness rotator cuff tears: A modern view on Codman’s classic. J Shoulder Elbow Surg 2000;9:163-168.
QUESTION 20 OF 50
A 72-year-old female sustains a displaced intracapsular femoral neck fracture. Which of the following is TRUE regarding the long term differences between possible treatment options for this injury?
1
Patients undergoing total hip arthroplasty are more likely to experience persistent pain than those undergoing internal fixation
2
Patients undergoing total hip arthroplasty are less likely to require reoperation than those undergoing internal fixation
3
There is no difference in functional outcome scores between internal fixation and total hip arthroplasty
4
Patients undergoing internal fixation perform activities of daily living better than those undergoing total hip arthroplasty
5
Mortality rates are higher following total hip arthroplasty than internal fixation
Elderly patients with femoral neck fractures (FNF) undergoing total hip arthroplasty (THA) are less likely to require reoperation than those undergoing internal fixation.
Intracapsular FNF are common in elderly patients after a fall from standing height. Treatment depends on physiological age and displacement (Garden's classification). For displaced fractures, physiologically young patients are treated with internal fixation while physiologically old patients are treated with
either hemiarthroplasty (debilitated, less active patients) or THA (more active patients, those with acetabular disease or preexisting inflammatory arthritis).
Chammout et al. retrospectively compared the long term (17 years) results of THA (cemented both component) and ORIF (2 cannulated screws) in elderly patients (>65 years). They found no difference in mortality. But hip scores were higher and pain was better in the THA group, while reoperation rates were higher in the ORIF group. Walking speed was initially faster in the THA group, but later did not differ between groups. They recommend THA for elderly patients with displaced FNF.
Rogmark et al. prospectively compared closed reduction and internal fixation (CRIF) with arthroplasty (combining hemiarthroplasty and THA) at 2 years in elderly patients (>70 years). Failure rates were higher, pain was worse, and walking was more impaired after CRIF. They recommend arthroplasty for patients >70 with FNF.
Incorrect Answers:
Answer 1: Patients undergoing THA are more likely to have less pain than internal fixation.
Answer 3: Patients undergoing THA have superior functional outcome scores. Answer 4: Patients undergoing THA perform ADL better in the short term. In the long term, there is no difference in ADL between the groups.
Answer 5: Mortality rates are similar after the two procedures.
QUESTION 21 OF 50
A 56-year-old woman with rheumatoid arthritis who underwent total hip arthroplasty 17 years ago now reports pain and progressive shortening of the extremity over the past year. An AP radiograph of the hip is shown in Figure 72. Laboratory studies show an erythrocyte sedimentation rate (ESR) of 34 mm/h (normal 0 to 28 mm/h) and a C-reactive protein of 10.2 (normal 0.2-8.0). She is presently taking oral antibiotics for a urinary tract infection. What is the next most appropriate step in management?
1
Aspiration of the hip joint and if negative, revision of the acetabular component
2
Aspiration of the hip joint and culture once she has discontinued the antibiotics for 3 weeks
3
Triple phase bone scan
4
Indium-111 leukocyte scan
5
Serial plain radiographs and protected weight bearing
The patient has a loose acetabular component, which explains her pain and progressive shortening. She has a history of inflammatory arthritis, elevated ESR and C-reactive protein, and has recently been treated for an infection. Thus, the suspicion for infection is high and must be ruled out. A triple phase bone scan can assist in the identification of component loosening but cannot differentiate infection from noninfectious causes. Indium-111 scans have been shown to have limited utility, although a negative scan can be helpful in ruling out infection. The selective preoperative use of aspiration of the hip joint has been shown to be effective and is most likely to identify infection; however, the patient must be off of antibiotics for a minimum of 2 weeks prior to her aspiration to avoid a false negative culture.
REFERENCES: Della Valle CJ, Zuckerman JD, Di Cesare PE: Periprosthetic sepsis. Clin Orthop Relat Res 2004;420:26-31.
Lachiewicz PF, Rogers GD, Thomason HC: Aspiration of the hip joint before revision total hip arthroplasty:
Clinical and laboratory factors influencing attainment of a positive culture. J Bone Joint Surg Am 1996;78:749-754. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Figure 73
QUESTION 22 OF 50
-What proteinaceous compound binds to hyaluronic acid to function as an effective boundary molecularlayer in articular cartilage?
1
Lubricin
2
Vitronectin
3
Aggrecan
4
Chondroitin sulfate
No detailed explanation provided for this question.
QUESTION 23 OF 50
Figures 1 through 3 are the radiographs of a 65-year-old man who sustained a fracture from a fall. The patient elects open reduction and internal fixation of the distal radius. After plating the distal radius, the distal radioulnar joint (DRUJ) is examined and found to be unstable in both pronation and supination. What is the best next step? --- --- ---
1
Early range of motion (ROM) program with a removable short-arm splint
2
Long-arm casting in pronation for 4 weeks
3
Pin fixation of the DRUJ
4
Fixation of the ulnar styloid fracture
styloid fracture were found to increase risk for DRUJ instability. An ulnar styloid base fracture involves the insertion of the radioulnar ligaments and can cause DRUJ instability if displaced. If persistent instability is present after fixation of the ulnar styloid, DRUJ pinning is a reasonable option. Early ROM
The initial radiographs show a comminuted displaced distal radius fracture, along with a displaced fracture of the base of the ulnar styloid. The displacement is best seen on the oblique view. After reduction and fixation of the radius, DRUJ stability should be assessed. The majority of scenarios that involve this injury pattern will not be unstable because of the oblique band of the interosseous ligament. When DRUJ instability is present after fixation of the radius, reduction and fixation of the ulnar styloid fracture is the best option to provide stability of the distal radioulnar joint (DRUJ) (Figure below). A study by Lawton and associates revealed that all distal radius fractures complicated by DRUJ instability were accompanied by an ulnar styloid fracture. A fracture at the ulnar styloid’s base and substantial displacement of an ulnar
with splinting would not allow reduction or healing of the ulnar styloid and would result in persistent instability. Short-arm casting also would not allow stability of the DRUJ and would be a less reliable method with which to achieve healing of the ulnar styloid.
---
QUESTION 24 OF 50
A 14-year-old girl is examined because of a pain in her left flank. The radiographs of the lumbar spine show loss of the pedicle with expansion of the lateral wall of the third lumbar vertebral body. Magnetic resonance imaging shows multiple fluid levels in the vertebral body with no additional areas of involvement. She is neurologically normal. The least invasive, effective treatment is which?
1
Observation
2
Radiation therapy
3
Selective arterial embolization
4
Radical en bloc resection
5
C urettage plus radiation therapy
This patient has an aneurysmal bone cyst of the vertebra. Selective arterial embolization is a minimally invasive treatment that often succeeds in arresting the lesions. Many times it is the only treatment needed. Selective arterial embolization can also be used as part of a strategy to be followed by curettage and reconstruction to decrease operative bleeding.
This lesion will continue to expand and might cause neurologic compromise or mechanical instability. Radiation therapy poses risks of later malignant degeneration. There are other ways of treating this lesion. Radical en bloc resection may unnecessarily injure neurologic structures.
While curettage is often necessary, there is no reason to introduce the risk of radiation therapy.
QUESTION 25 OF 50
-A previously healthy man who weighs 70 kg (154 lb) sustains an acute blood loss of 2 liters after a motorcycle crash. Which of the following statements about physiologic parameters is unique to this amount of blood loss?
1
Pulse pressure will be widened.
2
Urine output will be at the lower limits of normal.
3
Tachycardia will be present, but with no change in systolic blood pressure.
4
Systolic blood pressure will be decreased with a narrowed pulse pressure.
5
Systolic blood pressure will be maintained with an elevated diastolic blood pressure.
No detailed explanation provided for this question.
QUESTION 26 OF 50
-are the radiographs of a 58-year-old right-hand dominant woman who fell from a standing height directly onto her left shoulder and now reports left shoulder pain and is unable to elevate her arm. She has a normal sensory examination. The patient refuses any type of surgical intervention.What factor will have the greatest impact on her outcome at 1 year?
1
Age
2
Bone quality
3
Hand dominance
4
Initial angulation of fracture
5
Use of a physical therapy program
No detailed explanation provided for this question.
QUESTION 27 OF 50
The term acrosyndactyly describes digits that are:
1
Joined by bone only
2
Joined by soft tissue only
3
Joined proximally but separated distally
4
Joined along the entire length of the web space
5
Joined at the tips but separated proximally
Acrosyndactyly describes digits that are joined distally but remain separated by a proximal cleft. Acrosyndactylized digits initially develop normal web spaces, but are subsequently joined by secondary events, such as the formation of constriction bands. In contrast to syndactylized fingers, which remain joined due to failure of formation of the web space between contiguous digits, acrosyndactyly may form between non-contiguous digits. C omplex syndactyly involves a confluence of distal osseous and nail elements in addition to soft-tissue bridging. Simple syndactyly describes digits that are joined by soft tissue only. Finally, complete syndactyly refers to digits that are joined along their entire lengths, while incomplete syndactyly describes a web that extends more distally than usual, but not all the way to the finger tips.
QUESTION 28 OF 50
What dominant intracellular proteins become directly phosphorylated as a result of bone morphogenetic protein (BMP) binding to its receptors?
1
Myc
2
SMADs
3
Beta-catenin (β-catenin)
4
Adenylate cyclase
No detailed explanation provided for this question.
QUESTION 29 OF 50
An 18-year-old football player lands on a flexed knee and ankle after being tackled. Examination reveals increased external rotation and posterior translation and varus at 30° of flexion, which decreases as the knee is flexed to 90°. What is the most likely diagnosis?
1
Torn posterolateral corner
2
Torn posterior cruciate ligament (PCL) and posterolateral corner
3
Torn PCL
4
Rupture of the quadriceps tendon
5
Rupture of the lateral collateral ligament
The flexed knee and ankle mechanism of injury can result in a PCL and/or posterolateral corner injury. The examination reveals an isolated injury to the posterolateral corner (arcuate, popliteus, posterolateral capsule). This results in increased posterior translation and external rotation, as well as varus that is most notable at 30° of flexion and decreases as the knee is further flexed to 90°. Combined PCL and posterolateral corner injuries are characterized by increasing instability as the knee is flexed to 90° from 30°, while isolated PCL tears show the greatest degree of instability at 90° of flexion. A rupture of the quadriceps tendon would not affect anterior or posterior stability, whereas an isolated rupture of the lateral collateral ligament, which is a rare injury, is characterized by varus instability at 30° of knee flexion without posterior translation.
REFERENCES: Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Veltri DM, Warren RF: Isolated and combined posterior cruciate ligament injuries. J Am Acad Orthop Surg 1993;1:67-75.
QUESTION 30 OF 50
**A prospective outcome study is performed at a single institution to analyze the potential differences in treating intertrochanteric hip fractures with a plate/screw device versus an intramedullary device. No specific randomization is performed because an equal number of surgeons have p
Scientific References
for the use of one of these devices and they are allowed to continue their preferred method. Hip- specific and general health-related outcome measures are used, an excellent follow-up rate of 85% of the patients at 2 years is accomplished, and there appears to be results that favor the intramedullary device but the confidence intervals are wide. This study would be considered to carry what level of evidence?**
1
I
2
II
3
III
4
IV
5
V
#
**
This is a prospective comparative study but is not randomized or blinded and
is therefore a Level II therapeutic study. To qualify as Level I, it would need to be a high- quality randomized trial with narrow confidence intervals regardless of a significant difference or no difference in outcomes. Level III would be
case-control studies or retrospective comparisons. Level IV is case series and Level V is expert opinion.
QUESTION 31 OF 50
A 36-year-old male is brought to the trauma center following a motor vehicle accident. Physical exam shows a deformed left lower extremity with a 1-cm open wound over the anterolateral aspect of his leg. Radiographs are provided in Figures A and
1
Which of the following interventions has been shown in the literature to decrease the occurrence of infection at the fracture site?


1/. Operative debridement within 6 hours of injury
2/. Immediate prophylactic antibiotic administration
3/. Immediate stabilization with internal fixation after debridement
2
Irrigating with a saline solution that is mixed with an antibiotic
3
Irrigating with high pressure pulsatile lavage following surgical debridement
The clinical scenario and radiographs are consistent with a Gustilo and Anderson type 3A open tibia fracture.
Melvin et al review the evidenced-based literature and make recommendations for the initial evaluation and management of open tibial shaft fractures. The time elapsed before antibiotic administration and adequate surgical debridement of all contamination are the only factors definitively shown to reduce infection and improve outcome. Traditional recommendations have suggested surgical debridement of open fractures occur within 6 hours of injury. However, there is no literature to support this time window. Certainly, open fractures should be addressed with urgency, but there is no evidence reporting a definitive time window. There is insufficient data to recommend gram negative coverage with gentamicin for all open fractures although this is a common practice. The addition of antibiotics to the irrigation solution has been shown to decrease bacterial load, but it has also demonstrated host tissue necrosis and delayed wound healing. There is not sufficient data to support its use over a castile soap solution or normal saline. Similarly, high pressure pulsatile lavage decreases bacterial load, but also seeds bacteria deeper within the soft tissues and harms host tissues. There is no evidence to support pulsatile lavage over gravity flow.
QUESTION 32 OF 50
The most accurate way to monitor the motor tracts during spinal surgery is to stimulate which of the following regions:
1
Tibial nerve
2
Peroneal nerve
3
Motor cortex
4
Gastrocnemius
5
Proximal spinal cord
The most accurate way to monitor the motor tracts of the spinal cord is to stimulate the motor cortex. Stimulation at the level of the spinal cord conducts mainly antidromically through sensory pathways. Stimulation of the tibial and peroneal nerve is performed for monitoring sensory pathways only; these are an important indicator of spinal cord integrity but do not monitor the motor pathways per se. Stimulation of the gastrocnemius does not have any value for monitoring.
QUESTION 33 OF 50
A 65-year-old woman landed on her nondominant left shoulder in a fall. An AP radiograph is shown in Figure 39. Management should consist of
1
closed reduction and immobilization.
2
closed reduction and percutaneous pinning.
3
open reduction and internal fixation.
4
humeral hemiarthroplasty with tuberosity repair.
5
total shoulder arthroplasty.
The radiograph reveals a four-part fracture-dislocation of the proximal humerus. Humeral hemiarthroplasty and tuberosity repair is the treatment of choice because the risk of osteonecrosis is high after attempted repair of this injury. Glenoid resurfacing is reserved for acute fractures in which there is significant preexisting glenoid arthrosis, such as in patients with rheumatoid arthritis.
REFERENCES: Neer CS II: Displaced proximal humeral fractures: II. Treatment of three- and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Robinson CM, Page RS, Hill RM, et al: Primary hemiarthroplasty for treatment of proximal humeral fractures. J Bone Joint Surg Am 2003;85:1215-1223.
QUESTION 34 OF 50
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less
than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include
1
closed management of the medial condyle and humeral shaft fractures and open reduction and internal fixation of the both bones forearm fracture.
2
closed management of the humeral shaft fracture and open reduction and internal fixation of the medial condyle and the both bones forearm fractures.
3
open reduction and internal fixation of the humeral shaft, medial condyle, and the both bones forearm fractures.
4
open reduction and internal fixation of the medial condyle and both bones forearm fractures, and external fixation of the humeral shaft fracture.
5
delayed stabilization of all fractures after the open wound has healed.
With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient’s physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach.
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
QUESTION 35 OF 50
In studying a newly recognized disorder using a large population of affected individuals, geneticists discover that although the disorder often affects siblings, it was rarely, if ever, detected in their ancestors. This disorder most closely follows which pattern of inheritance:
1
Autosomal dominant
2
Autosomal recessive
3
Sex-linked
4
Multifactorial
5
Anticipation
Autosomal recessive conditions classically show âhorizontalâ inheritance. Ancestors do not display the gene because they would likely have only one copy of the mutant allele. Only when two carriers reproduce is the phenotype manifest in approximately one- fourth of their offspring.
Autosomal dominant inheritance is characterized by vertical transmission. Many generations manifest the trait because it takes only a single copy of a mutant allele to display the phenotype.
Sex-linked conditions are often traced back in a family. Normally the males are affected and the females are carriers. Multifactorial conditions are thought to result from the combination of different genes. Although the risk of recurrence in kindred is somewhat greater than the population as a whole, it is still quite low (only a few percent). It is rare for siblings to be affected.
Anticipation refers to the phenomenon in which successive generations are likely to display more severe forms of a given disorder. Myotonic dystrophy is a classic example of this phenomenon.
QUESTION 36 OF 50
Posterior cruciate-retaining total knee arthroplasty has been studied by numerous methods including kinematic video fluoroscopy. Which of the following is the best description of typical kinematic behavior?
1
Unpredictable anterior femoral condylar translation from full extension to 90 degrees of flexion
2
Predictable femoral rollback from full extension to 90 degrees of flexion
3
Medial femoral condyle pivot with minimal medial femoral condyle translation and lateral femoral condyle posterior translation in flexion
4
Lateral femoral condyle pivot with minimal medial femoral condyle translation
5
Anterior tibial contact of both the medial and lateral femoral condyles in full extension
DISCUSSION: In vivo fluoroscopic studies have enlightened orthopaedic surgeons as to the actual kinematic performance of the total knee implants. Importantly, many technical factors combine to result in abnormal kinematics after total knee arthroplasty. The typical kinematics of the normal knee are negated by osteoarthritis and the various changes created by the surgeon’s technique. Dennis and associates observed that anterior femoral condylar translation during deep knee flexion was most commonly observed in posterior cruciate-retaining knees.
REFERENCES: Dennis DA, Komistek RD, Mahfouz MR, et al: Multicenter determination of in vivo kinematics after total knee arthroplasty. Clin Orthop Relat Res 2003;416:37-57.
Freeman MA, Pinskerova V: The movement of the normal tibio-femoral joint. J Biomech 2005-38'197- 208.
**42 • American Academy of Orthopaedic Surgeons**
Figure 52
QUESTION 37 OF 50
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What test should be performed to aid in this diagnosis?
1
Thompson test
2
External rotation stress test
3
Anterior drawer test
4
Squeeze test
The anterior drawer test is performed with the ankle in 10° of plantar flexion, which results in the greatest amount of translation. The test investigates the integrity of the anterior talofibular ligament with a key distance of translation being 8 to 10 mm. While the patient is sitting and has her knees flexed over the edge of a table or bench, the physician uses one hand to stabilize the distal leg and with the other hand applies an anterior force to the heel in an attempt to gap the talus anteriorly from under the tibia. The anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
QUESTION 38 OF 50
All of the following muscles are innervated by the median nerve except:
1
The ulnar two lumbricals (lumbricals III and IV)
2
Opponens pollicis
3
Abductor pollicis brevis
4
Flexor pollicis brevis
5
Flexor digitorum profundus to the middle finger
Lumbricals 1 and 2 are innervated by the median nerve, in addition to the opponens pollicis brevis, abductor pollicis brevis, and flexor pollicis brevis.
QUESTION 39 OF 50
of 100
Figures 85a through 85c are the sagittal and axial CT scans and sagittal T2 MR image of a 21-year-old man who was thrown from his motocross bike earlier in the day. He now has significant low-back pain; however, he is neurologically intact and has no trouble voiding urine. A standing plain radiograph obtained the next day is shown in Figure 85d. Treatment should involve A B C D
1
resumption of full activity as soon as tolerated.
2
a brace.
3
anterior stabilization and fusion.
4
posterior stabilization and fusion.
Disruption of the posterior ligamentous complex is an important determinant of the stability of a burst fracture. This patient is neurologically intact and his MR images do not reveal posterior ligamentous complex (PLC) disruption. The standing radiograph confirms that overall alignment is acceptably and relatively preserved. Nonsurgical treatment with or without a brace is acceptable in this scenario; however, the patient should not be cleared to resume full activity until fracture healing, which may be as long as 3 months after the date of injury. Anterior or posterior surgery should be reserved for patients with PLC disruption, neurological injury, or, in some cases, multiple trauma.
RECOMMENDED READINGS
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Zeiller SC, Anderson DG, Bono CM, Stock GH, Brown AK, Kuklo T, Oner FC. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine (Phila Pa 1976). 2005 Oct 15;30(20):2325-33. PubMed PMID: 16227897. ](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16227897)
[Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Lehman RA Jr, Anderson DG, Bono CM, Kuklo T, Oner FC. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005 Jun;18(3):209-15. PubMed PMID: 15905761.](http://www.ncbi.nlm.nih.gov/pubmed/15905761)[View ](http://www.ncbi.nlm.nih.gov/pubmed/15905761)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15905761)
RESPONSES FOR QUESTIONS 86 THROUGH 89
1. Proximal junctional kyphosis (PJK)
2. Adjacent segment degeneration
3. Intraoperative neurological injury
4. Postsurgical wound infection
Please select the complication listed above that most commonly is associated with a clinical scenario described below.
QUESTION 40 OF 50
Figures 18a and 18b are the radiographs of an obese 75-year-old man with a rigid acquired flatfoot deformity. What is the best treatment option?
1
Double calcaneal osteotomy
2
Medial calcaneal osteotomy and tendon transfer
3
Lateral column lengthening and tendon transfer
4
Subtalar arthrodesis
5
Triple arthrodesis
For stage III adult-acquired flatfoot deformity characterized by dysfunction of the posterior tibial tendon, rigid valgus deformity of the hindfoot, and arthritic changes of the hindfoot joints,arthrodesis is the favored procedure. In an overweight patient with degenerative changes affecting the subtalar and Chopart joints, triple arthrodesis is the best treatment option. Subtalar arthrodesis only addresses the talocalcaneal joint and continues to render the patient symptomatic in the talonavicular and calcaneocuboid joints. Advanced stage III disease precludes reconstructive procedures involving calcaneal osteotomy and tendon transfer.
QUESTION 41 OF 50
of 100
Indicates the anterior center edge angle
1
Figure 51a
2
Figure 51b
3
Figure 51c
4
Figure 51d
5
Figure 51e
- Figure 51d_
QUESTION 42 OF 50
The pathology of the lesion shown in Figures 1 and 2 reveal what cellular pattern? --- ---
1
Uniform distribution of stromal cells and giant cells
2
Mixture of mature fat cells and spindle cells
3
Mucin-filled space with occasional spindled fibroblasts
4
Lobular pattern of vascular proliferation with inflammation
No detailed explanation provided for this question.
QUESTION 43 OF 50
of 100
A 4-year-old girl who has midlumbar myelomeningocele and hydrocephalus is being evaluated for her uneven gait. A hip examination reveals a right hip dislocation. Bilateral hips are pain-free with full range of motion and no fixed deformity. What is the most appropriate course of action?
1
Obtain standing AP pelvis to evaluate the hips; plan open reduction of the right hip when the patient starts having hip pain
2
Obtain supine AP pelvis to evaluate the hips; plan open reduction of the right hip as soon as possible
3
Inform the family that the dislocated hip will not limit the ability to ambulate and will not benefit from reduction
4
Inform the family that the patient's ambulatory potential is poor due to the hip dislocation, which cannot be treated successfully
■ A child with midlumbar myelomeningocele, without other lesions, would be expected to have the ability to ambulate, though delayed. She has a high likelihood of hip dislocations because of lack of function of the abductor muscles. The presence or absence of hip dislocation does not affect ambulatory ability; the child is already walking. The best course of action is education of the family and therapist as to the minimal effect that a hip dislocation has in these patients. A shoe lift or brace buildup can address leg length discrepancy; in a hip without contractures, no other treatment is needed.
Radiographs are unnecessary in the management of the hip dislocation in myelomeningocele. Surgery has been shown to convert supple, painless dislocated hips into stiff, painful hips that have a high likelihood of redislocation. Though the dislocation is not recommended for treatment, this does not preclude the ability to safely ambulate and undergo therapy, which is not harmful to the condition.
QUESTION 44 OF 50
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management?
1
Splinting, admission, and frequent neurovascular checks
2
Cylinder cast and discharge
3 _AL_. _-M_ E _ad_ m _en_ e _a_ rg _C_ e _o_ n _p_ t _y_
knee arthroscopy
2010 Pediatric Orthopaedic Examination ook • 43
4. ##### Four-compartment calf fasciotomy
5. ##### Non-weight-bearing, a knee immobilizer, and follow- up in 1 week
PREFERRED RESPONSE: 1
DISCUSSION: The anatomic lesion in this patient is not exactly defined, but she has most likely sustained an injury about the knee. A Salter-Harris type I proximal tibial physeal fracture is likely. The normal radiograph reading can be misleading because these injuries may displace and spontaneously reduce. The child is at risk of compartment syndrome although she is currently not displaying signs of it. Thus, even though this injury may seem trivial by radiographic findings, it should be treated like a knee dislocation with a risk of late developing compartment syndrome. MRI or CT may be necessary to define the injury. She does not require emergent treatment, but merits close observation for possible compartment syndrome. Any of the possible injuries about the knee can be unstable and require internal fixation after reduction.
REFERENCES: McGuigan JA, O’Reilly MJ, Nixon JR: Popliteal arterial thrombosis resulting from disruption of the upper tibial epiphysis. Injury 1984;16:49-50.
Burkhart SS, Peterson HA: Fractures of the proximal tibial epiphysis. J Bone Joint Surg Am
1979;61:996- 1002.
QUESTION 45 OF 50
Haversian bone is composed of vascular channels surrounded circumferentially by lamellar bone. Which of the following terms is used to describe the unit of bone composed of a neurovascular channel surrounded by a cell-permeated layer of bone matrix:
1
Bone remodeling unit
2
Plexiform bone
3
Osteon
4
Volkman unit
5
Canaliculi
The osteon is a unique arrangement of bone cells and matrix surrounding a blood vessel. The osteon is an irregular branching, anastomosing cylinder composed of a centrally placed neurovascular canal surrounded by cell-permeated layers of bone matrix.
The bone remodeling unit refers to the cutting cone of leading osteoclasts and following osteoblasts.
Plexiform bone is a structural type of bone found in large animals where rapid bone growth occurs. There are alternating layers of lamellar and woven bone.
Volkman canals are the channels connecting different osteons or Haversian units.
Canaliculi are small channels through which the cell processes of the osteocytes connect to each other. Correct Answer: Osteon
QUESTION 46 OF 50
The Lisfranc ligament connects the base of the
1
first metatarsal and the medial cuneiform.
2
first metatarsal and the base of the second metatarsal.
3
first metatarsal and the middle cuneiform.
4
second metatarsal and the medial cuneiform.
5
second metatarsal and the middle cuneiform.
The Lisfranc ligament arises from the lateral surface of the first (medial) cuneiform and is directed obliquely outward and slightly downward to insert on the medial surface of the second metatarsal base. It is the strongest of the tarsometatarsal interosseous ligaments.
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Solan MC, Moorman CT III, Miyamoto RG, et al: Ligamentous restraints of the second tarsometatarsal joint: A biomechanical evaluation. Foot Ankle Int 2001;22:637-641.
QUESTION 47 OF 50
A 65-year-old woman has severe pain and numbness in her hand. She notes frequent awakenings at nighttime and difficulty with fine tasks. She also has a history of cervical radiculopathy and notes intermittent pain in her upper arm and periscapular region. An examination reveals a positive Tinel sign over the midforearm and carpal tunnel. Electrodiagnostic testing shows a median nerve sensory distal latency of 3.8 ms (normal latency is 3.5 ms). Which intervention or test would best predict if carpal tunnel release would be successful in relieving this patient's symptoms?
1
Trigger point injections with lidocaine
2
Carpal tunnel corticosteroid injection
3
Ultrasound of the wrist
4
Carpal tunnel view radiograph
This patient demonstrates several upper extremity issues including possible carpal tunnel syndrome, cervical radiculopathy, and pronator syndrome. The electrodiagnostic testing is equivocal, and a corticosteroid carpal tunnel injection should be performed prior to surgical intervention to assess its effectiveness in eliminating the patient's symptoms. Positive response (meaning improvement in symptoms), after corticosteroid injection at the carpal tunnel correlates well with symptom relief following surgery. Trigger-point injections are not indicated for carpal tunnel syndrome. Ultrasound and carpal tunnel view radiograph can provide diagnostic information but would not be helpful in determining _treatment in this specific case._
QUESTION 48 OF 50
The most common location of osteofibrous dysplasia is the:
1
Femur
2
Tibia
3
Fibula
4
Radius
5
Ulna
Osteofibrous dysplasia occurs exclusively in the tibia. This non-neoplastiCcondition may be related to adamantinoma. The lesion is usually located in the anterior cortex and there is often bowing of the tibia.
QUESTION 49 OF 50
A 1-week-old female infant with arthrogryposis multiplex congenital has hips that are stiff in flexion and abduction, and her knees have a range of flexion from 20° to 40°. In addition, her right thigh has become swollen and tender. The most likely cause of this latter problem is:
1
Osteomyelitis of the femur
2
Septic arthritis of the hip
3
Dislocation of the hip
4
Deep vein thrombosis
5
Fracture of the femur
Fracture is common in this condition because of osteopenia and the stress concentration due to joint stiffness.
Osteomyelitis is uncommon in the diaphysis and much less common in this scenario than fracture. Septic arthritis of the hip is uncommon in this disease.
Dislocation of the hip would not cause pain and swelling in this setting. Deep vein thrombosis is uncommon at this age.
QUESTION 50 OF 50
of 100
Figures 1 through 5 are the clinical photographs and radiographs of a 7-year-old boy who has a history of a left elbow supracondylar fracture treated with closed reduction and pinning one year ago. He is referred due to a left arm deformity the family is noticing over the last year. He has no pain. What most accurately describes the nature of this deformity?
1
A cosmetic problem
2
It could lead to tardy posteromedial rotatory instability
3
A varus, extension, and rotational deformity of the distal humerus
4
It has no long-term sequela
■ Cubitus varus deformity may occur after pediatric supracondylar and lateral condyle fractures. The deformity is a combination of varus, extension, and internal rotation. Although pediatric cubitus varus following a pediatric distal humerus fracture or congenital deformity has traditionally been considered a cosmetic problem, adult orthopaedic literature cites the posterolateral rotatory instability, ulnar neuropathy, snapping triceps, progressive varus of the ulna, elbow joint malalignment and tendency to distal humerus lateral condyle fracture as possible long-term sequela.