OITE & ABOS Orthopedic Board Prep MCQs: Trauma & Nerve Injuries Part 96

Key Takeaway
This page offers Part 96 of a comprehensive OITE and AAOS Orthopedic Surgery Board Review. It provides 100 verified, high-yield MCQs, specifically designed for orthopedic surgeons and residents preparing for their board certification exams. Utilize our interactive quiz with study and exam modes for effective preparation.
About This Board Review Set
This is Part 96 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 96
This module focuses heavily on: Fracture, Nerve.
Sample Questions from This Set
Sample Question 1: What is the most common long-term complication of the fracture shown in Figure 32?...
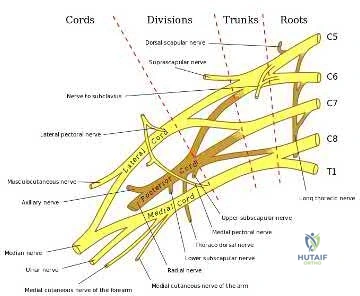
Sample Question 2: In a postganglionic brachial plexus lesion at Erb’s point (point of formation of the upper trunk by the C5 and C6 nerve roots), which of the following nerves will still function normally?...
Sample Question 3: The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?...
Sample Question 4: -A 17-year old boy who sustained a closed clavicle fracture after he was ejected from an all-terrain vehicle was treated with a figure-of-8 brace 1 year ago. He now reports continuous pain at the site of the fracture and is unable to active...
Sample Question 5: A 12-year-old girl has a 4-cm limb-length discrepancy following a fracture of the left distal femur 2 years ago. Examination reveals 18 degrees of genu valgum on the involved side, with 7 degrees of genu valgum on the opposite side. Radiogr...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What is the most common long-term complication of the fracture shown in Figure 32?
Explanation
REFERENCES: Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Higgins TF, Baumgaertner MR: Diagnosis and treatment of fractures of the talus: A comprehensive review of the literature. Foot Ankle Int 1999;20:595-605.
Question 2
In a postganglionic brachial plexus lesion at Erb’s point (point of formation of the upper trunk by the C5 and C6 nerve roots), which of the following nerves will still function normally?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, pp 28-29.
Zimmerman NB, Weiland AJ: Assessment and monitoring of brachial plexus injury in the adult, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA,
JB Lippincott, 1991, vol 2, pp 1273-1283.
Question 3
The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?
Explanation
REFERENCE: Mazzoca AD: Principles of internal fixation, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 308-309.
Question 4
- A 17-year old boy who sustained a closed clavicle fracture after he was ejected from an all-terrain vehicle was treated with a figure-of-8 brace 1 year ago. He now reports continuous pain at the site of the fracture and is unable to actively raise his arm above his head. A radiograph is shown in Figure 1. Management should now include
Explanation
Selection (1) would not provide adequate fixation to promote healing. (2) Electrical stimulation would not be sufficient for the above reasons. (3) Resection of the distal clavicle would not be indicate for this case because it promote further instability of the clavicle and increasing the affected forces to the clavicle.
(5) Kirschner wire fixation with bone graft, the author stated would provide fixation, but they achieved better results with plate fixation and bone graft Question 6 -
A 75-year-old woman sustains a fracture below the level of a total hip prosthesis. Radiographs demonstrate loosening of the prosthetic component. Treatment should consist of
a cast brace
a spica cast
plate fixation
allograft strut fixation
long stem revision
The key to this question lies in the radiographic evidence of loosening of the prosthetic component. The long stem revision is clearly indicated in this case because of various factors, one decreases impingement of the loose stem against the lateral femoral cortex. A non-surgical approach in the elderly patient will only increase the many risk factors such as atelectasis, pneumonia, and thromboembolic disease.[Instructional Course 44 pg. 293-303]
Question 5
A 12-year-old girl has a 4-cm limb-length discrepancy following a fracture of the left distal femur 2 years ago. Examination reveals 18 degrees of genu valgum on the involved side, with 7 degrees of genu valgum on the opposite side. Radiographs show that the left distal femoral growth plate is now closed; however, the tibial growth plate is still open. Her bone age matches her chronologic age. Management should consist of
Explanation
long-term solution.
REFERENCES: Westh RN, Menelaus MB: A simple calculation for the timing of epiphyseal arrest: A further report. J Bone Joint Surg Br 1981;63:117-119.
Sasso RC, Urquhart BA, Cain TE: Closed femoral shortening. J Pediatr Orthop 1993;13:51-56.
Nordsletten L, Holm I, Steen H, Bjerkreim I: Muscle function after femoral shortening osteotomies at the subtrochanteric and mid-diaphyseal level: A follow-up study. Arch Orthop Trauma Surg 1994;114:37-39.
Question 6
Figures 23a through 23h are the radiographs and MR images of a 32-year-old man with worsening left knee pain. A 3-foot hip-to-ankle radiograph shows a 13-degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability symptoms. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to decrease stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but, if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should only be performed at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL reconstruction alone is not indicated for this patient.
Question 7
- What is the treatment of choice for an adult who has an isolated fracture of the ulna at the junction of the distal and middle thirds, with 5 degrees apex dorsal angulation and 25% displacement?
Explanation
Question 8
What is the most common complication after distal biceps tendon repair at the elbow?
Explanation
Cain and associates retrospectively reviewed 198 consecutive surgical repairs of the biceps and noted a 36% overall complication rate, including 26% paresthesia of the lateral antebrachial cutaneous nerve, 6% paresthesia of the sensory branch of the radial nerve, 2% superficial infection, 4% injury to the posterior interosseous nerve, 3% symptomatic heterotopic ossification, and 2% rerupture. Grewal and associates randomized 47 patients to have single-incision repair with two suture anchors and 44 patients to have two-incision transosseous suture repair. They reported that the single-incision technique had a higher rate of transient neurapraxia to the lateral antebrachial cutaneous nerve, affecting 19 of 47 in the suture anchor group and three of 43 in the transosseous group. Also, four reruptures occurred, which appeared to be independent of the repair technique. Recordon and associates found only three complications in their series of 46 patients, 19 having endobutton repair and 27 with transosseous suture repair. They reported two injuries to the lateral antebrachial cutaneous nerve and one case of heterotopic ossification. The review by Banerjee and associates showed one rupture of repair (disengagement of the cortical button), two persistent lesions of the superficial branch of the radial nerve, and one symptomatic heterotopic ossification. Co hen remarked that rerupture of the tendon after repair is uncommon in both one-incision and two-incision techniques. Van den Bogaerde and Shin presented a case of posterior interosseous nerve
incarceration with endobutton repair.
Question 9
Which of the following growth factors binds and activates the lipoprotein receptor-related protein 5/6 (LRP5/6) during bone development? Review Topic
Explanation
Question 10
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
Explanation
REFERENCES: Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Siegal T, Siegal T: Current considerations in the management of neoplastic spinal cord compression. Spine 1989;14:223-228.
Question 11
A 25-year-old man is unresponsive at the scene of a high-speed motor vehicle accident and remains obtunded. Initial evaluation in the emergency department reveals a left-sided femoral shaft fracture and a right-sided humeral shaft fracture. The cervical spine remains immobilized in a semi-rigid cervical collar, and the initial AP and lateral radiographs obtained in the emergency department are unremarkable. What is the most appropriate management at this time? Review Topic
Explanation
Question 12
A 15-year-old boy has had pain in the right shoulder for the past 3 months. He denies any history of trauma and has no constitutional symptoms. Examination reveals a large firm mass in the proximal arm. A radiograph and MRI scan are shown in Figures 27a and 27b. Biopsy specimens are shown in Figures 27c and 27d. Management should consist of
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 232-233.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-196.
Question 13
Figures 177a and 177b are the radiographs of a 7-year-old boy with spastic cerebral palsy. He has quadriparetic involvement and is unable to ambulate. He has very limited abduction, 30 degrees of flexion contractures, and pain on abduction. Bilateral varus osteotomies are scheduled with acetabular procedures to improve stability. Which type of acetabular osteotomy should be performed?
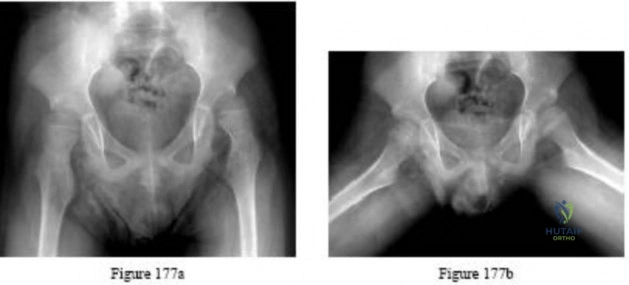
Explanation

Question 14
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study results fits the definition of chronic prosthetic joint infection?
Explanation
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
Question 15
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure 34. What is the next most appropriate step in the orthopaedic management of this patient?
Explanation
REFERENCE: Simon JA, Puopolo SM, Capla EL, et al: Accuracy of the axillary projection to determine fracture angulation of the proximal humerus. Orthopedics 2004;27:205-207.
Question 16
When comparing the addition of a trough at the greater tuberosity to direct repair of cortical bone, simulated rotator cuff repair in animal models has shown what type of change in the strength of the repair?
Explanation
REFERENCE: St Pierre P, Olson EJ, Elliott JJ, et al: Tendon healing to cortical bone compared with healing to a cancellous trough. J Bone Joint Surg Am 1995;77:1858-1866.
Question 17
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
REFERENCES: Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Kapp S, Cummings D: Transtibial amputation: Prosthetic management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 453-478.
Question 18
A 60-year-old man is evaluated in the ICU after a rollover motor vehicle accident 3 days ago. He has multiple upper and lower extremity trauma and was found unresponsive at the accident scene. Surgery is planned for the extremity trauma once the patient is medically stable. He remains intubated and the cervical spine is immobilized in a semi-rigid collar. Examination reveals mild erythema in the posterior occipital cervical region. Initial AP and lateral radiographs of the cervical spine have not revealed any obvious fracture. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Ackland HM, Cooper DJ, Malham GM, et al: Factors predicting cervical collar-related decubitus ulceration in major trauma patients. Spine 2007;32:423-428.
Hewitt S: Skin necrosis caused by semi-rigid cervical collar in a ventilated patient with multiple injuries. Injury 1994;25:323-324.
Question 19
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
Question 20
A 47-year-old woman has a painful bunion of the right foot, and shoe wear modifications have failed to provide relief. Examination reveals a severe hallux valgus with dorsal subluxation of the second toe. Radiographs are shown in Figures 14a and 14b. The most appropriate management should include
Explanation
REFERENCE: Mann RA, Rudicel S, Graves SC: Repair of hallux valgus with a distal soft-tissue procedure and proximal metatarsal osteotomy: A long-term follow-up. J Bone Joint Surg Am 1992;74:124-129.
Question 21
What form of fixation is associated with the highest incidence of osseous union when using segmental allograft reconstruction following tumor resection?
Explanation
REFERENCE: Vander Griend RA: The effect of internal fixation on the healing of large allografts. J Bone Joint Surg Am 1994;76:657-663.
Question 22
A 46-year-old man has acute tenderness along the ulnar aspect of the wrist after falling on his outstretched hand while playing basketball. Examination reveals tenderness and mild swelling along the volar ulnar aspect of the wrist. Radiogaphs are shown in Figures 14a through 14c. Management should consist of
Explanation
REFERENCES: Failla JM, Amadio PC: Recognition and treatment of uncommon carpal fractures. Hand Clin 1988;4:469-476.
Botte MJ, Gelberman RH: Fractures of the carpus, excluding the scaphoid. Hand Clin 1987;3:149-161.
Question 23
Figure 12 shows the radiograph of a 55-year-old man who has severe, painful osteoarthritis of the left hip and is scheduled to undergo a left total hip arthroplasty. History reveals that he underwent a right total hip arthroplasty 5 years ago that remains pain-free. Based on the preoperative radiograph, the patient is at greatest risk for what complication?
Explanation
REFERENCE: Ranawat CS, Rodriguez JA: Functional leg-length inequality following total hip arthroplasty. J Arthroplasty 1997;12:359-364.
Question 24
Deep anterior compartment
Explanation
Question 25
A surgeon desires to use an implant that will be able to absorb as much energy as possible before it fails. The implant should be made of a material that has which of the following properties?
Explanation
Question 26
When evaluating articular cartilage, what extracellular matrix component is most closely associated with the deep calcified cartilage zone?
Explanation
REFERENCES: Buckwalter JA, Mankin HJ: Articular cartilage: Tissue design and chondrocyte matrix interactions. Instr Course Lect 1998;47:477-486.
Poole AR, Kojima J, Yasuda T, Mwale F, Kobayasai M, Laverty S: Composition and structure of articular cartilage: A template for tissue repair. Clin Orthop 2001;391:S26-S33.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 27
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
Explanation
REFERENCES: Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
O’Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
Question 28
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
Explanation
REFERENCES: Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273.
Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Kim WY, Hearn TC, Seleem O, et al: Effect of pin location on stability of pelvic external fixation. Clin Orthop Relat Res 1999;361:237-244.
Question 29
A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root. You suggest a left-sided L5-S1 microdiskectomy and tell her that when comparing tubular diskectomy and open procedures
Explanation
Several comparative studies have reported no difference in functional outcomes between tubular diskectomy and microsurgical lumbar diskectomy. A recent systematic review by Kamper and associates in which conventional microdiskectomy and minimally invasive approaches were compared revealed that there was no difference between the procedures in terms of clinical outcomes, complication risk, or rate of revision surgery.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183.View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 30
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
REFERENCES: Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Hughes LO, Beaty JH: Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 1994;76:283-292.
Question 31
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
REFERENCES: Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393.
Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Kostuik JP, Valdevit A, Chang HG, et al: Biomechanical testing of the lumbosacral spine. Spine 1998;23:1721-1728.
Question 32
A 43-year-old woman has had pain in the left hip for the past 2 months. A radiograph, CT scan, MRI scan, and biopsy specimens are shown in Figures 16a through 16e. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra JM, Gold R, Downs J, Eckardt JJ: A new histologic approach to the differentiation of enchondroma and chondrosarcoma of the bones: A clinicopathologic analysis of 51 cases. Clin Orthop 1985;201:214-237.
Question 33
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mmP3P, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management? Review Topic
Explanation
(SBQ13PE.16) A 4-week-old infant who had been born with a dislocated hip has been treated in a Pavlik Harness since 1 week of age. Parents have been compliant with the prescribed bracing protocol, and no complications or neurologic abnormalities have been noted. The hip remains Ortolani positive. Figure A shows the ultrasound image obtained in the office. What is the next best step in management? Review Topic

No further treatment
Continue Pavlik Harness treatment
Convert to semi-rigid abduction brace
Perform a hip arthrogram with closed vs. open reduction under general anesthesia
Perform a pelvic osteotomy
This is a 4 week old infant with DDH who has failed Pavlik harness treatment for 3 weeks. Figure A is an ultrasound image demonstrating a dislocated hip.
Initial treatment for an infant with a dislocated, but reducible ("Ortolani positive") hip is bracing in a Pavlik Harness. The Pavlik harness is a dynamic brace that requires normal muscle function and tone to help keep the hip in a reduced position. If this treatment fails to hold the hip reduced after three weeks of treatment, the harness should be discontinued to prevent "Pavlik Harness Disease" which involves erosion of the posterior acetabulum as the femoral head is inappropriately being held against it.
After failure of Pavlik harness treatment, if the hip remains subluxated, the next step in treatment is to convert to a semi-rigid orthosis of another 2-3 weeks. If the semi-rigid brace likewise fails to keep the hip reduced, then hip arthrogram with closed vs. open reduction and spica-cast placement can be planned.
Swaroop and Mubarak present a study using a protocol of initial pavlik harness treatment with weekly ultrasound assessment for 3 weeks. If the hip remained unstable but reducible, then semi-rigid abduction bracing with continues weekly ultrasounds were done for an additional 2-3 weeks. This treatment protocol had a 93% success rate, which compared favorably to protocols not including the abduction
brace.
Hedequist et al. presented a review of 15 patients treated similarly with intial pavlik harness treatment for 3-4 weeks, and then abduction bracing if the remained unstable but reducible. They found that abduction bracing produced a stable hip within 1-2 months.
Illustration A shows a baby wearing a semi-rigid orthosis. Illustration B is the hip ultrasound image from Figure A with labels added. Illustration C is an ultrasound of a hip that is not dislocated.
Incorrect answers:
Question 34
A patient sustains a severe lower extremity injury. What can be said about his outcome at 2 years if he chooses reconstruction over amputation?

Explanation
Bosse et al found that at 2 years the SIP score and return to work were not statistically signficantly different between amputation and reconstruction groups. Reconstruction patients had a higher risk of rehospitalization. The psychosocial subscale of SIP did not improve with time. Risk factors for poorer SIP score were: rehospitalization for a major complication, a low educational level, nonwhite race, poverty, lack of private health insurance, poor social-support network, low self-efficacy (the patient's confidence in being able to resume life activities), smoking, and involvement in disability-compensation litigation.
MacKenize et al evaluated factors influential in returning to work (RTW) after severe lower extremity injury. Characteristics that correlated with higher rates of RTW included younger age, higher education, higher income, the presence of strong social support, and employment in a white-collar job that was not physically demanding. Receipt of disability compensation had a strong negative effect on RTW.
Question 35
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. What is the primary cause of a cam deformity?
Explanation
Question 36
In regards to a genetic disorder, which of the following is an example of "anticipation?"
Explanation
Genetic anticipation is an important concept in understanding the development and genetic implications of many heritable disorders. It is a common phenomenon in trinucleotide repeat expansion disorders. These disorders are due to unstable microsatellite trinucleotide repeats that expand beyond the normal threshold. In subsequent generations these expansions become longer and thus express disease characteristics at a younger age of onset, and often with greater severity.
Martorell et al. investigated the development of CTG trinucleotide repeats in patients with myotonic dystrophy type 1 (DM1) and their relatives. They discovered unaffected individuals carry a pre-mutation sequence which can lead to trinucleotide repeat expansion in subsequent generations and thus produce offspring with the disorder.
Kamsteeg et al. compare the characteristics of DM1 and DM2. Both are due to trinucleotide repeat expansions. However, while DM1 can present with earlier onset and increasing severity in each generation, DM2 does not exhibit this genetic anticipation.
Incorrect Answers
Question 37
At which joint do degenerative changes occur first in a patient with chronic, untreated scapholunate dissociation?
Explanation
Stage I of scapholunate advanced collapse (SLAC) is characterized by the presence of radioscaphoid arthritis. A predictable pattern exists of the progression of degenerative changes for SLAC wrist, including stage I (radial styloid involvement at the scaphoid fossa), stage II (scaphoid and entire scaphoid facet involvement), stage III (degeneration between the capitate and lunate), and stage IV (pancarpal involvement). The radiolunate joint is often spared.
Question 38
A 30-year-old right hand-dominant woman is seen in the trauma unit after a high-speed motor vehicle accident. She sustained a right shoulder anterior dislocation that is gently reduced under sedation. A CT scan is shown in Figure 3. If left untreated, the patient is at greatest risk for
Explanation
more common.
REFERENCES: Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment.
J Bone Joint Surg Am 2002;84:1552-1559.
Bigliani LU, Newton PM, Steinmann SP, et al: Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. Am J Sports Med 1998;26:41-45.
Question 39
5cm. Recent radiographs are seen in Figures A and B. What is the most appropriate treatment plan?
Explanation
Subtrochanteric fractures can be treated with cephalomedullary nailing or fixed angle plates. Nailing of these fractures is technically challenging because the fracture must be reduced prior to nail passage. Failure to do so leads to varus and procurvatum malreduction.
Bellabarba et al. reviewed plating of femoral nonunions after intramedullary nailing. Of 23 nonunions, 21 healed at an average of 12 weeks. The remaining 2 cases required repeat plating (at 2 and 8 weeks) for hardware breakage because of noncompliance with weightbearing restrictions. They advocate plating because it allows for correction of malalignment and provides a biomechanically superior tension band construct.
Incorrect Answers:
OrthoCash 2020
A 38-year-old male was struck by a truck and sustained the injury seen in figure A. Treating this injury with an intramedullary nail with a larger radius of curvature can lead to what complication?

Posterior perforation of the distal femur
Varus malreduction
Comminution of the fracture site
Iatrogenic femoral neck fracture
Anterior perforation of the distal femur Corrent answer: 5
According to the study by Egol et al, the average femoral anterior radius of curvature was 120 cm (+/- 36 cm), and currently available femoral nails have a greater radius of curvature (i.e. more straight). This mismatch has been shown to lead to an increased risk of perforation of the anterior distal femur as the nail is impacted into the canal.
The referenced study by Tencer et al noted an increased risk of iatrogenic femoral fracture with anterior starting point >6mm from the anatomic axis.
They recommend starting in line with the femoral axis, or just a few millimeters anterior in order to minimize this risk.
Illustration A depicts anterior femoral cortex penetration secondary to nail/femur radius of curvature mismatch.

OrthoCash 2020
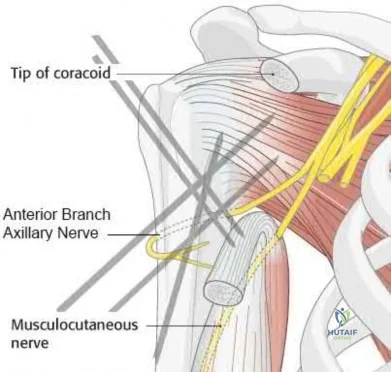
A 60-year-old woman is undergoing closed reduction and percutaneous pinning of a proximal humerus fracture. What structure is at greatest risk for injury from the pin marked by the red arrow in Figure A?
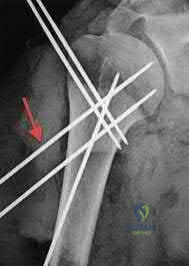
Anterior branch of the axillary nerve
Posterior humeral circumflex artery
Long head of the biceps tendon
Cephalic vein
Musculocutaneous nerve
Certain anatomic structures are at risk with percutaneous pinning of proximal humerus fractures. The red arrow in Figure A marks a proximal lateral pin that would place the anterior branch of the axillary nerve at risk.
Rowles and McGrory performed an anatomic study of the structures at risk with closed reduction and percuatneous pinning of the proximal humerus and found that proximal lateral pins were a mean of 3mm from the anterior branch of the axillary nerve. Pins placed through the anterior cortex and directed into the humeral head fragment were a mean of 2mm from the long head of the biceps tendon and greater tuberosity pins were found to be 8mm from the posterior humeral circumflex and 10mm from the main trunk of the axillary nerve as they penetrated the medial cortex of the humerus.
Jaberg et al retrospectively reviewed the clinical and radiographic results of 48 patients at an average of 3 years after undergoing closed reduction and percutaneous pinning of a proximal humerus fracture. 70% good to excellent results with their described technique, and the authors caution that radiographic malunion did not correlate with patient function.
Incorrect Answers
OrthoCash 2020
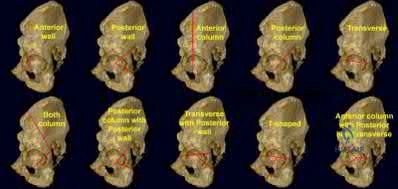
A 42-year-old female sustains the injury seen in the computed tomography images seen in Figures A and B. According to the Letournel classification, what is the injury pattern shown?

Posterior wall
Transverse
Anterior wall
Posterior column
Both column
The axial CT cut and Judet radiographic view shown reveals a transverse fracture pattern according to the Letournel classification system. This can be determined by the fact that the articular surface of the acetabulum is attached to the intact portion of the ilium, which is connected to the axial skeleton posteriorly through the sacroiliac joint. This differs from a both-column fracture, in which the articular surface of the acetabulum has no attachments to the axial skeleton due to fracture line(s). The axial CT scan also shows a vertical fracture line which is typical of a transverse fracture pattern.
Durkee et al review the classification schemes for these injuries, as well as comment on the importance of quality images (Judet views, CT, etc).
Figures A and B show a transverse acetabular fracture with mild displacement.
OrthoCash 2020
Which of the following is true regarding plating of humeral shaft fractures compared to intramedullary nailing?
worse functional results
higher need for subsequent surgeries
higher incidence of radial nerve injury
lower complication rates
decreased nonunion rates Corrent answer: 4
Controversy exists regarding nailing compared with plating of humeral shaft fractures, but the most recent and highest level evidence indicates decreased complication rates with open reduction and internal fixation of these injuries.
Lin et al found less blood loss with intramedullary nailing than plating, but nailing was also associated with increased shoulder surgery, likely due to disruption of the rotator cuff tendon during insertion.
Meekers et al found a higher union rate, better functional results and a lower reoperation rate after plate and screw fixation versus nailing. They concluded that plating was superior in most cases of humeral shaft fracture, however more recent studies have challenged these findings.
Heineman et al. (2012) have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF. The authors found no significant difference between the two treatment modalities for the secondary outcomes (nonunion, infection, nerve palsy, re-operation)
Incorrect Answers:
OrthoCash 2020
A 35-year-old male sustains the fracture seen in Figures A and B. Which of the following substances has been shown to result in the least radiographic subsidence when combined with open reduction and internal fixation?

Cancellous allograft bone chips
Autograft iliac crest
Femoral intramedullary reamings
Calcium phosphate cement
Calcium sulfate cement Corrent answer: 4
Figures A and B show a plateau fracture with a lateral split and depression of the articular surface. In treating tibial plateau fractures, calcium phosphate has been shown to have the least amount of articular subsidence on follow-up examinations due to its high compressive strength.
The study by Lobenhoffer et al noted improved radiographic outcomes and earlier weightbearing with usage of calcium phosphate cement. Welch and Zhang reproduced tibial plateau fractures in goats and compared cancellous autograft to calcium phosphate cement augmentation. At 24 hours, four of five specimens treated with autograft had subsidence of the fragment. Only two specimens from limbs treated with cement showed minimal subsidence; the remaining were congruent.
Yetkinler’s study compared cement to no cement treatment in a model of depressed plateau fractures. Calcium phosphate cement of high compressive
strength provided equivalent or better stability than conventional open reduction
and internal fixation with either auto/allograft bone which had both a lower compressive strength and reduced mechanical stability.
OrthoCash 2020
The modified Judet approach to the posterior scapula exploits the internervous interval between what two muscles?
Supraspinatus and infraspinatus
Supraspinatus and subscapularis
Infraspinatus and teres minor
Teres minor and teres major
Teres major and lattisimus Corrent answer: 3
The posterior or modified Judet approach to the scapula is typically used for internal fixation of scapular fractures. This approach utilizes a transverse incision over the scapular spine with detachment of the posterior deltoid. The interval between the infraspinatus (suprascapular n.) and teres minor (axillary n.) is identified and used to gain access to the posterior aspect of the scapula and glenoid.
The reference by Obremskey et al argues the approach "combines several important goals including: 1) exposure of all bony elements of the scapula which have adequate bone stock for internal fixation; 2) minimal trauma to the rotator cuff musculature; and 3) protection of the major neurologic structures (suprascapular nerve superiorly and axillary nerve laterally)." They believe "the main advantage of the exposure is limiting muscular dissection, which can potentially improve rehabilitation and limit morbidity of the operation."
OrthoCash 2020
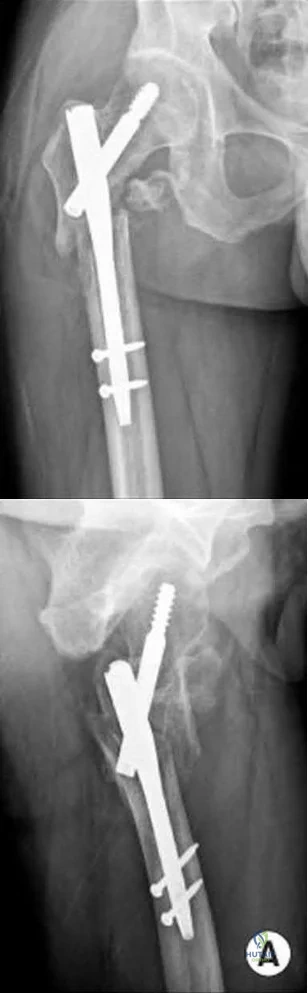
An 82-year-old female sustains an intertrochanteric hip fracture and is treated with a sliding hip screw. What is the most appropriate definitive step in treating the failure seen in figure A?

Non-weight bearing
Valgus proximal femoral osteotomy
Total hip arthroplasty
Revision open reduction and internal fixation
Proximal femoral resection Corrent answer: 3
Figure A shows superior cutout of the lag screw from the sliding hip screw as well as the superior cannulated screw used for an "antirotation" device.
In the referenced review article by Haidukewych and Berry, salvage of failed treatment of hip fractures in the elderly is limited by bone quality and comorbidities. They recommend total hip arthroplasty in this instance to restore function, decrease pain, and limit periods of immobilization. They mention that the major challenges for arthroplasty are: assessing the need for acetabular resurfacing, selecting the femoral implant, and managing the greater trochanter.
OrthoCash 2020
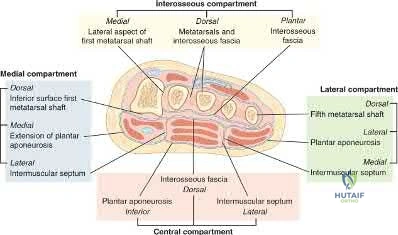
A 13-year-old boy falls out of a tree and sustains the injury seen in Figures A and B. He is taken to the OR for fixation of his fracture.
The next morning, the patient’s blood pressure is 185/105 mm Hg and pulse rate is 130. He complains of pain that is not improved with opiates. On physical exam, the foot is firm. The decision is made to obtain compartment pressures to rule out compartment syndrome of the foot. Which of the following paths in Figure C marks the
appropriate location to measure the central compartment, and what would be considered abnormal values?

Path A, absolute value of 30-45 mmHg or delta p > 30mmHg
Path B, absolute value of 30-45 mmHg or delta p > 30mmHg
Path B, absolute value of 30-45 mmHg or delta p < 30mmHg
Path C, absolute value of 30-45 mmHg or delta p > 30mmHg
Path C, absolute value of 30-45 mmHg or delta p < 30mmHg Corrent answer: 3
The correct approach to measure pressures in the central compartment of the foot is by directing the needle lateral and plantar through the abductor hallicus, just under the base of the first metatarsal. Abnormal values indicating the need for decompression are an absolute value of 30-45 mmHg or a Δp < 30mmHg (the difference between the patient's diastolic blood pressure and compartment pressures).
The most common symptom of compartment syndrome in the extremities is intense pain. However, compartment syndrome can be difficult to diagnose in children and patients who are comatose, nonverbal, and/or mentally compromised because they may not be able to properly express their level of pain. Additionally, in compartment syndrome of the foot, pain on passive extension of the toes may or may not be present, and swelling and absence of the dorsalis pedis pulse may be expected findings with extensive trauma to the foot, making the clinical diagnosis even more difficult. Thus, for patients with equivocal findings on physical exam, foot compartment pressures should be measured in order to confirm the diagnosis. There are 8 compartments in the foot: lateral, medial, central, and 4 interosseous. The lateral compartment
contains the abductor digiti minimi and flexor digiti minimi brevis, and is measured by directing the needle 1cm medial and plantar under the midshaft of the 5th metatarsal. The medial compartment contains the abductor hallicus and flexor hallicus brevis, and is measured by directing the needle lateral and plantar under the base of the first metatarsal. The central compartment contains the oblique head of the adductor hallucis, and is measured through the same approach as the medial compartment after advancing the needle more deeply. The 4 interosseous compartments entail the 2nd, 3rd, and 4th web spaces, and can be measured by directing the needle plantar into each respective dorsal webspace.
Ojika et al. performed a systematic review on foot compartment syndrome. They found that the most common cause of foot compartment syndrome was crush injury to the foot, and that diagnosis was mostly made through a combination of clinical findings and compartment pressure measurements.
Badhe et al. reported 4 cases where competent sensate patients developed compartment syndromes without any significant pain. They found that pain is not a reliable clinical indicator for underlying compartment syndrome, so in a competent sensate patient, the absence of pain does not exclude compartment syndrome. They concluded that a high index of clinical suspicion must prevail in association with either continuous compartment pressure monitoring or frequent repeated documented clinical examination with a low threshold for pressure measurement.
Flynn et al. looked at the diagnosis and outcome of acute traumatic compartment syndrome of the leg in children. They found that a delay in diagnosis may occur because acute traumatic compartment syndrome manifests itself more slowly in children or because the diagnosis is harder to establish in this age group. They state that the results of the present study should raise awareness of late presentation and the importance of vigilance for developing compartment syndrome in the early days after injury.
Figures A and B are lateral and Harris radiographs of the foot demonstrating a calcaneus fracture. Figure C is a cross-sectional image of the foot. Illustration A is an image depicting the compartments of the foot.
Incorrect Answers:
compartment. Additionally, a Δp < 30mmHg (not > 30mmHg) is considered abnormal.
OrthoCash 2020
A 35-year-old female presents to the emergency room after a motor vehicle collision where her leg was pinned under the car for over 30 minutes. A clinical photo and radiographs are shown. Which of the following is the most accurate way to diagnose compartment syndrome?

surgeon's palpation of the leg compartments
paresthesias in her foot
diastolic blood pressure minus intra-compartmental pressure is less than 30 mmHg
diastolic blood pressure minus intra-compartmental pressure is greater than 30 mmHg
intra-compartmental pressure measurement of 25 mmHg Corrent answer: 3
The clinical picture is consistent with compartment syndrome. The most accurate way to make the diagnosis is to measure the difference between the diastolic blood pressure and intracompartmental pressure (delta p).
In a prospective study of 116 patients with tibial diaphyseal fractures, McQueen et al found that the use of a differential pressure of 30 mmHg as a threshold for fasciotomy led to no missed cases of acute compartment syndrome. They recommended that a fasciotomy should be performed if the differential pressure level drops to under 30 mmHg.
The cited study by Kakar et al found the intraoperative DBP is significantly lower than the preoperative DBP in patient undergoing IM nailing for tibia shaft
fractures. Therefore, they emphasize that the surgeon should recognize that intraoperative DeltaP may be lower than DeltaP once the patient is awakened in deciding whether to perform a fasciotomy versus awaken the patient and perform serial examinations and or compartment pressure measurements.
An absolute intra-compartmental value greater than 30 to 45mmHg can also be used to make the diagnosis of compartment syndrome, but is more controversial than the delta p according to Kakar and Amendola.
OrthoCash 2020
What is the most common mode of failure of the lateral ulnar collateral ligament associated with an elbow dislocation?
ligament avulsion off the humeral origin
ligament avulsion off the ulnar insertion
midsubstance rupture
bony avulsion of the humeral origin
combined proximal and distal ligament avulsions Corrent answer: 1
The lateral ulnar collateral ligament (LUCL) is often injured with elbow dislocations, and is most commonly injured at the proximal origin.
McKee noted that in 62 consecutive operative elbow dislocations and fracture/dislocations, the LUCL was ruptured in all of the patients, proximally in 32, bony avulsion proximally in 5, midsubstance rupture in 18, ulnar detachment in 3, ulnar bony avulsion in only 1, and combined patterns in 3.
Pugh et al established a standard protocol to treat elbow fracture dislocations (terrible triad) which includes coronoid repair, radial head repair/replacement, LUCL repair, and MCL and/or external fixation as needed.
OrthoCash 2020
A 24-year-old male sustains the injury seen in Figure A after being thrown from a motorcycle at a high speed. Which of the following fixation methods has been shown to be the most stable fixation construct for this injury?

Posterior bridge plating and anterior ring external fixation
Percutaneous iliosacral screw and anterior ring external fixation
Percutaneous iliosacral screw and anterior ring internal fixation
Transiliac screw
Two percutaneous iliosacral screws Corrent answer: 3
Figure A shows an APC III injury, which is a rotationally and vertically unstable injury, with damage to the anterior ring, pelvic floor, and posterior ligamentous stabilizing structures.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
OrthoCash 2020
A 33-year-old male patient presents with a comminuted open tibia fracture after involvement in a motor vehicle crash. He has a history of smoking but is otherwise healthy. He is given antibiotics, and taken immediately for irrigation and debridement, followed by an un-reamed stainless steel intramedullary nail. Due to bone loss there is a non-circumferential cortical defect measuring 12 mm at the fracture site. All of the following factors in this patient's history and presentation increase his risk for adverse outcome EXCEPT:
High-energy mechanism of injury
Use of un-reamed nail
Implant material
Fracture gap
History of smoking Corrent answer: 2
Of the factors listed only the use of an un-reamed intramedullary nail for an open tibia fracture has not been shown to increase the risk of adverse outcome or need for reoperation.
The treatment of open tibia fractures with intramedullary nailing can be complicated by many factors. High energy mechanism of injury, use of a stainless steel nail, residual fracture gap greater than 1 cm, and a history of smoking have all been shown to increase the risk of adverse outcome. The use of reamed and un-reamed nails for open tibia fractures have been studied, and no significant difference in outcome has been found.
Schemitsch et al. present data from a prospective randomized trial of tibia fractures treated with reamed or unreamed intrameduallry nails. They found no difference in risk of adverse outcome between reamed and un-reamed nails in open tibia fractures. They did, however, find an increased risk of adverse outcomes in high-energy mechanisms, use of stainless steel (versus titanium) rods, and a residual fracture gap of greater than 1 cm. They comment that their data did not show a significant increase in risk due to history of smoking, but cite other studies that have demonstrated such a relationship.
Bhandari et al. present data from a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. For closed fractures they found a lower rate of primary events (most commonly need for dynamization) in the reamed group. However, they found no difference in outcomes for either technique in open fractures.
Incorrect answers:
OrthoCash 2020
Following antegrade intramedullary nailing of a femoral shaft fracture, the complication shown in Figure A occurs. Which of the following errors most likely resulted in this complication?
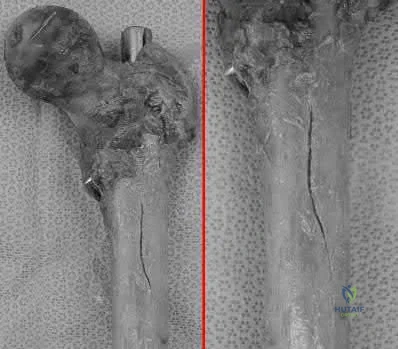
Applying external rotation torque on the proximal femur after placing proximal interlocking screws
Excessive interfragmentary compression of the fracture site prior to placing proximal interlocking screws
Using too anterior a starting point for a piriformis-entry point nail
Inserting a trochanteric-entry point nail through the piriformis fossa
Inserting a right femoral nail into the left femur Corrent answer: 3
Using a piriformis nail, a starting point that is too anterior will result in iatrogenic fracture ("bursting") of the proximal femur.
Antegrade nailing achieves fixation via 3-point fixation. In the sagittal plane, because of anterior sagittal bow, this is achieved at distal anterior cortex, middle posterior cortex (apex of curvature) and proximal anterior cortex. In the coronal plane, because of the lateral bow, this is achieved at the lateral distal femur, middle medial femur (apex of curvature), and proximal lateral femur (greater trochanter). Piriformis nails have a single sagittal bow.
Trochanteric nails are bowed in 2 planes, necessitating a twisting motion during insertion to negotiate both bows.
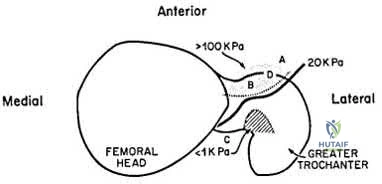
Papadakis et al. performed an experimental study on 18 cadaveric femora. Anterior bursting was found in 56% of nails placed too anteriorly. Bursting was not seen in nails placed through a more posterior entry point. They emphasize the location of the entry point when performing antegrade nailing.
Johnson et al. reviewed the biomechanical factors affecting fracture stability
and femoral bursting. They found that position of the starting hole was most important. Anterior displacement by >6mm led to high hoop stresses and bursting of the anterior cortex. This is important as an eccentrically reamed cortex may be difficult to recover from. They recommend either selecting a smaller diameter nail or overreaming by 1-2mm as a solution.
Figure A shows a fracture split of the proximal femur (left, without magnification; right, close-up). Illustration A shows anterior cortex pressures exceeding 100kPa for too-anterior entry points.
Incorrect Answers:
Wrong-side placement of a trochanteric entry nail would lead to varus malalignment at the fracture site, more so than placing a piriformis nail through the greater trochanter.
OrthoCash 2020
A 30-year-old male sustains a brachial plexus injury as the result of a motor vehicle collision. Palsy of which of the following muscles would not be expected with this injury if the injury was postganglionic in nature?
Rhomboid major
Extensor carpi radialis longus
Biceps brachii
Deltoid
Brachioradialis
A brachial plexus injury would involve all of the upper extremity muscles as well as most of the periscapular muscles. Complete plexus palsies are rare, and are often associated with scapulothoracic dissociation or other high-energy injuries.
Preganglionic injuries often involve the cervical paraspinal musculature as well as a complete plexus injury. EMG evidence of intact signals in the serratus anterior (long thoracic nerve) and rhomboids (dorsal scapular nerve) are suggestive of a postganglionic lesion/injury.
Tubbs et al. reported on the surgical anatomy of the dorsal scapular nerve in a cadaver study. They found that the nerve came off the C5 nerve root in 95%, ran 2.5cm medial to the spinal accessory nerve as it traveled on the anterior border of the trapezius muscle, and was intertwined with the dorsal scapular artery in all specimens.
Balakrishnan et al reported on the comparison of clinical exam and EMG in predicting site of lesions in brachial plexus injuries. The combination of EMG and exam localized the nerve injury in 80%, while the paraspinal EMG was the most sensitive solitary examination method (67%).
Illustration A shows a diagram of the brachial plexus. Incorrect Answers:
5: These muscles are all innervated by nerves that come from the brachial
plexus, and would be affected with a postganglionic injury.
OrthoCash 2020
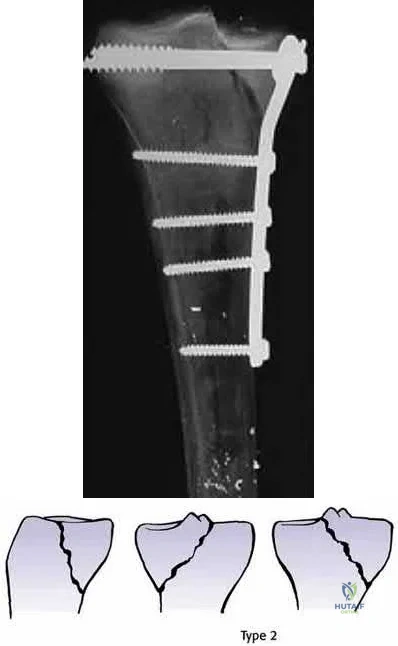
A 40-year-old male sustains a fall from a height. He sustains the isolated injury shown in the radiograph and CT images seen in Figures A through C. Surgery is planned. Which of the following constructs is the most appropriate definitive fixation for this injury?

Lateral locked plating
Medial bridge plating
Medial buttress plate
Medial lag screw with washers
External fixation
This patient has a medial tibial plateau fracture. Medial buttress plating (MBP) is indicated.
Medial tibial plateau fractures (Schatzker IV, Hohl and Moore II) may represent fracture dislocations of the knee. Neurovascular injuries must be excluded. In these instances, the medial fragment represents the stable fragment, and the rest of the tibia is the fractured fragment, with the entire leg acting as the lever arm.
Berkson et al. reviewed high energy tibial plateau fractures. Medial fractures may be treated with a medial plate or external fixation. Open reduction may be necessary because of fracture line obliquity and propensity of the medial plateau to shorten and rotate in the sagittal plane. Meniscal injuries should be repaired and avulsed cruciates fixed early. Collateral ligaments should be reconstructed after obtaining bone healing and range of motion.
Ratcliff et al. compared the stability of lateral locked plates and medial buttress plates in a cadaver model. They found that the medial buttress plate had greater fixation strength/failure force (4136N) compared with the lateral locking plate (2895N), although maximum cyclic displacement and residual displacement results were not different. They concluded that for vertically
orientated medial tibial plateau fractures, medial buttress plates were more stable.
Figure A is a radiograph showing a medial tibial plateau fracture extending across the tibial eminence. This is also classified as a Hohl and Moore Type II fracture. Figures B and C are coronal and axial CT scan images confirming the medial tibial plateau fracture and excluding a bicondylar fracture. Illustration A shows a medial tibial plateau fracture fixed with a medial buttress plate (cadaveric model with fibula removed). Illustration B shows the Hohl and Moore Type II fracture involving the entire condyle.
Incorrect Answers:
OrthoCash 2020
A 39-year-old female presents with the following motor vehicle crash with the injury seen in Figure A (immobilized in a pelvic binder). The iatrogenic neurologic injury most commonly caused by placement of the anterior construct for this injury, as shown in Figure B, would cause which of the following?
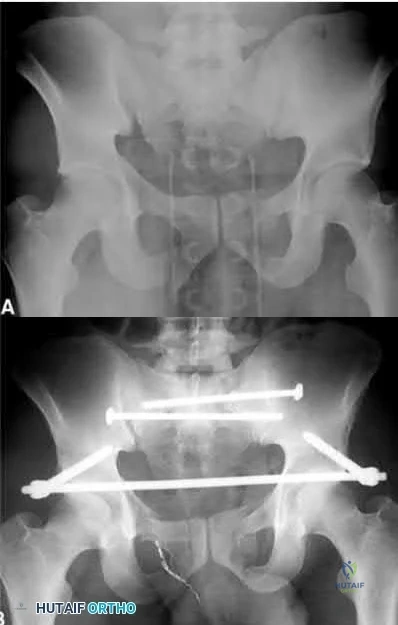
Weakness of hip flexion
Weakness of ankle dorsiflexion
Numbness of the medial thigh
Numbness of the lateral thigh
Numbness of the perineum Corrent answer: 4
This patient was treated with posterior stabilization, and an anterior subcutaneous internal fixator (ASIF). The most common neurologic injury seen following placement of the ASIF construct is irritation of the lateral femoral cutaneous nerve (LFCN), causing numbness and/or pain of the lateral thigh.
Unstable pelvic fractures can be treated in a multitude of ways. The ASIF construct is typically created by placing long pelvic screws or polyaxial pedicle screws in the supraacetabular region, similar to the supraacetabular pins for an
anterior external fixator. Then a curved bar is placed subcutaneously and connected to the supraacetabular screws. They are typically removed after 3-4 months when fracture healing is complete.
Vaidya et al. present a retrospective review of the use of ASIF as definitive treatment of unstable pelvic fractures. All patients in the study tolerated the construct well. LFCN irritation was seen in 30% of patients, and resolved in all but one patient.
Müller et al. present a retrospective review of the use of posterior stabilization and ASIF. They report an acceptably low complication rate, and good to excellent outcomes in 64.5% of patients.
Figure A is a radiograph demonstrating a right APC3 and left APC2 pelvic injury, imaged in a pelvic binder. Figure B is a postoperative radiograph following posterior stabilization and ASIF.
Incorrect answers:
OrthoCash 2020
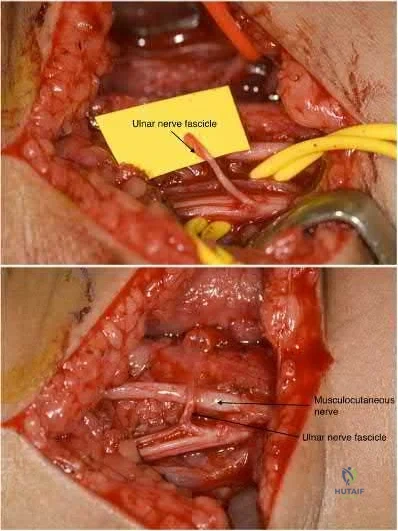
What would be the most appropriate surgical indication for transferring fascicles of the ulnar nerve to the motor nerve of the biceps and fascicles of the median nerve to the motor nerve of the brachialis?
C8 - T1 nerve root avulsion 3 months ago
C5 - C6 nerve root avulsion 2 months ago
Upper brachial plexus palsy 22 months ago
Medial and posterior cord injury from gunshot wound 2 months ago
C6 ASIA A spinal cord injury Corrent answer: 2
Transfer of fascicles from (1) ulnar nerve to the nerve to the biceps and (2) median nerve to the motor nerve of the brachialis would be appropriate in the
treatment of an acute (<3-6 months) upper brachial plexus palsy.
Upper trunk injury (C5, C6) often results from the avulsion of both the C5 and C6 nerve roots. Injuries of this nature usually result from a downward force on the shoulder with lateral bending of the cervical spine in the opposite direction. This results in what is commonly called an Erb-Duchenne palsy. Patients often present with a flail shoulder and loss of elbow flexion. Other common treatments for C5 and C6 root avulsion include neurotization of the musculocutaneous (MSC) nerve by the spinal accessory (SA) or intercostal nerve, and neurotization of the supra-scapular nerve by the SA.
Liverneaux et al. looked at short term results of (1) ulnar nerve fascicle transfer to the nerve to the biceps and (2) fascicle of the median nerve to the motor branch to the brachialis in 15 patients with acute C5 - C6 nerve root avulsion injuries. Grade 4 elbow flexion was restored in each of the 10 patients. There was no secondary deficit in grip strength or sensation.They concluded that this double nerve transfer technique will likely reduce the need for secondary procedures to augment elbow flexion.
Teboul et al. reviewed thirty-two patients with an upper nerve-root brachial plexus injury that underwent ulnar nerve fascicle transfer to the nerve of biceps to restore elbow flexion. After the nerve transfer, twenty-four patients achieved grade 3 elbow flexion strength or better. They note that this procedure will spare the C5 nerve root and other nerves for grafting or transfer elsewhere.
Illustration A shows harvesting of an ulnar nerve fascicle for transfer. Illustration B shows transfer of the fascicle of the ulnar nerve to the motor nerve of the biceps.
Incorrect Answers:
sensory quadriplegia. Nerve transfers using the ulnar nerve (C8-T1) would also be redundant as this nerve would be non-functional in this patient.
OrthoCash 2020
A 31-year-old female presents to the trauma bay following a motorcycle crash. Her blood pressure is 95/70 mmHg, heart rate is 115 bpm. Lactate measured in the trauma bay is 10 mmol/L. She has multiple rib fractures, pulmonary contusions, and a positive FAST exam requiring immediate exploratory laparotomy. After laparotomy her lacate remains unchanged. She has a closed right femur fracture and an open right tibia fracture as seen in Figures A and B. Besides antibiotics and thorough irrigation and debridement, which of the following would be an appropriate step in the immediate management of her fractures?

Reamed intramedullary nailing of the tibia and femur
Un-reamed intramedullary nailing of the tibia, and reamed intramedullary nailing of the femur
Reamed intramedullary nail of the tibia, and un-reamed intramedullary nail
of the femur
Posterior slab splint of the tibia, and 10 lbs skeletal traction of the femur
External fixation of the tibia and femur Corrent answer: 5
This patient is suffering from multiple injuries and has evidence of chest injury and incomplete resuscitation. The immediate treatment of her fractures should be external fixation for both the tibia and the femur.
For polytraumatized patients with multiple injuries including extremity fractures, damage control orthopaedics dictates that long bone fractures should be temporarily stabilized. Either inadequate stabilization, or early total care, such as a reamed or unreamed nails, can exacerbate the patient's condition and increase the risk of a second-hit phenomenon. For this patient with pulmonary contusions and continued elevation of lactate indicating end-organ hypoperfusion her extremities should have staged treatment according to damage control principles.
Morshed et al. present a retrospective review of polytraumatized patients with femur fractures and compared outcomes based on the time frame in which their fractures were definitively treated. They found delaying treatment at least 12 hours to allow appropriate resuscitation and treatment of other traumatic injuries led to a decrease in mortality of 50%. Patients with intra-abdominal injuries benefited most from staged treatment of the extremities.
Figure A is a radiograph showing a closed right femur fracture. Figure B is a radiograph of an open right tibia fracture.
Incorrect answers:
OrthoCash 2020
A 68-year-old woman undergoes a hemiarthroplasty for a proximal humerus fracture through a deltopectoral approach. What
range of motion exercise should not be utilized in the immediate postoperative period due to concerns about lesser tuberosity fixation?
Pendulums
Passive internal rotation of the shoulder to the plane of the body
Active forearm supination
Passive external rotation of the shoulder past 30 degrees
Passive forward flexin of the shoulder to 90 degrees Corrent answer: 4
Frankle et al found that passive external rotation of the shoulder placed the most stress on the lesser tuberosity fixation. The subscapularis tendon inserts on the lesser tuberosity and is the deforming force when placed under tension during external rotation. They also found that non-anatomic tuberosity reduction of 4-part proximal humerus fractures treated with hemiarthroplasty increased torque and impaired external rotation kinematics.
OrthoCash 2020
A 72-year-old female sustains a displaced intracapsular femoral neck fracture. Which of the following is TRUE regarding the long term differences between possible treatment options for this injury?
Patients undergoing total hip arthroplasty are more likely to experience persistent pain than those undergoing internal fixation
Patients undergoing total hip arthroplasty are less likely to require reoperation than those undergoing internal fixation
There is no difference in functional outcome scores between internal fixation and total hip arthroplasty
Patients undergoing internal fixation perform activities of daily living better than those undergoing total hip arthroplasty
Mortality rates are higher following total hip arthroplasty than internal fixation
Elderly patients with femoral neck fractures (FNF) undergoing total hip arthroplasty (THA) are less likely to require reoperation than those undergoing internal fixation.
Intracapsular FNF are common in elderly patients after a fall from standing height. Treatment depends on physiological age and displacement (Garden's classification). For displaced fractures, physiologically young patients are treated with internal fixation while physiologically old patients are treated with
either hemiarthroplasty (debilitated, less active patients) or THA (more active patients, those with acetabular disease or preexisting inflammatory arthritis).
Chammout et al. retrospectively compared the long term (17 years) results of THA (cemented both component) and ORIF (2 cannulated screws) in elderly patients (>65 years). They found no difference in mortality. But hip scores were higher and pain was better in the THA group, while reoperation rates were higher in the ORIF group. Walking speed was initially faster in the THA group, but later did not differ between groups. They recommend THA for elderly patients with displaced FNF.
Rogmark et al. prospectively compared closed reduction and internal fixation (CRIF) with arthroplasty (combining hemiarthroplasty and THA) at 2 years in elderly patients (>70 years). Failure rates were higher, pain was worse, and walking was more impaired after CRIF. They recommend arthroplasty for patients >70 with FNF.
Incorrect Answers:
OrthoCash 2020
A polytrauma patient underwent the following procedures: (1) statically locked intramedullary nailing for a right femoral shaft fracture; (2) open reduction with plate-and-screw fixation [ORIF] for a right simple distal fibula fracture; (3) ORIF right middle third radius and ulna fracture; and (4) ORIF left humeral shaft fracture. What is the appropriate weightbearing status for this patient?
Weight bearing as tolerated in all extremities
Early protected weight bearing right lower extremity in walking cast, weight bearing as tolerated left upper extremity, non-weight bearing right forearm
Weight bearing as tolerated in bilateral lower extremities and right upper extremity, non-weight bearing left upper extremity
Non-weight bearing bilateral upper extremities and right lower extremity
Non-weight bearing right upper and lower extremities, weight bearing as tolerated left upper and lower extremities without walking cast
The standard postoperative weightbearing for locked medullary nailing for femoral shaft fractures and humeral shaft fractures is weight bearing as tolerated (WBAT). Simple ORIF ankle fractures may be managed with early protected weight bearing. ORIF right middle third radius and ulna fracture should be managed with a period of non-weight bearing due to risk of secondary displacement of the fracture.
Tingstad et al. examined the effect of immediate weightbearing on plated fractures of the humeral shaft. They reported that immediate weightbearing on humeral shaft fractures, treated with plating and full weightbearing, did not have any negative effect on the union or malunion rates.
Brumback et al. evaluated the feasibility, safety and efficacy of immediate weightbearing after treatment of femoral shaft fractures with statically locked IM nail. Using biomechanical and clinical data, they showed that all fractures united with no loss of fixation or hardware failure.
Starkweather et al. retrospectively assessed the complications and loss of reduction in patients who bore weight in a short leg cast within 15 days after surgical repair of acute unilateral closed ankle fractures. Of the 81 ankle fracture radiographs, 80 (98.8%) showed no displacement in fracture reduction on the final follow-up examination. These results suggest early protected weightbearing may be safe.
Incorrect Answers:
OrthoCash 2020
A 22-year-old female falls off the back of a motorcycle and sustains the injury in Figure A. She is hemodynamically unstable and massive transfusion protocol is activated. What is the correct ratio of transfusion of packed red blood cells, platelets and plasma?

Question 40
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for
Explanation
REFERENCES: Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249.
Linscheid RL, O’Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452.
O’Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Ross G, McDevitt ER, Chronister R, Ove PN: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
Question 41
- Which of the following factors is most likely to predispose a patient to dislocation of the patellar component following total knee arthoplasty?
Explanation
Internally rotating the femoral component produced abnormal laxity seen at 30, 60, and 90 degrees of flexion. There was no gapping noted in the neutral or externally rotated specimens.
The normal pattern for patellar tracking was a gentle curve with maximal deflection at 15 and 60 degrees of flexion. The maximal medial displacement were lowest for the externally rotated specimens.
Although contact areas could not be quantitatively measured accurately, the contact areas were more evenly distributed between the medial and lateral sides of the patella in the externally rotated specimens than they were in either the internally rotated or neutral specimens.
You have to be careful interpreting this data at least in reference to knee stability. In this study a perpendicular tibial cut was made. The normal tibia has a 30 degree varus slope and thus more bone is resected from the lateral surface. External rotation of the femoral component compensates for this.
No tests were done with lateral placement of the femoral component or medial placement of the patellar component.
Question 42
A 10-year-old boy reports heel pain with sporting activities. An examination demonstrates gastrocnemius contracture and tenderness at the calcaneal apophysis. Radiographs are unremarkable. What is the best next step?
Explanation
Sever disease, or calcaneal apophysitis, is best treated with activity modification that includes rest, restriction from sports and running, and Achilles tendon stretching exercises. The diagnosis is clinical (rendering MRI study unnecessary) and the course is usually self-limited, obviating the need for surgery. Occasionally, children with severe symptoms may benefit from a short period of cast or fracture brace immobilization.
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
Question 43
A 32-year-old man sustained an injury to the right thumb metacarpophalangeal (MP) joint ulnar collateral ligament (UCL) and is undergoing surgical repair (Figure 1). What structure in the clinical photograph is blocking reduction of the ulnar collateral ligament?

Explanation
When the thumb MP UCL is torn from the proximal phalanx, the distal stump can be displaced superficial to the adductor aponeurosis, known as a Stener lesion. The adductor aponeurosis effectively blocks reduction of the ligament to the normal attachment site. The EPB and EPL tendons are dorsal to the UCL, and the ulnar sesamoid bone/volar plate are in a volar position in relation to the UCL. The dorsal capsule would also not block reduction of the UCL due to it's anatomic location. The other responses do not block the UCL with this type of injury.
Question 44
In the treatment of rheumatoid arthritis, which medication is an antagonist of tumor necrosis factor-alpha?
Explanation
TNF-alpha is considered to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat rheumatoid arthritis (RA) are manufactured to block TNF-alpha or its receptors. This has been shown to reduce inflammation and stop disease progression. In the USA, Etanercept is approved to treat rheumatoid arthritis, juvenile rheumatoid arthritis and psoriatic arthritis, plaque psoriasis and ankylosing spondylitis. The route of administration is subcutaneous.
Bongartz et al. used a randomized control trial to asses the risk of infection and malignancy rates in RA treated with TNF-alpha antagonist. Overall, patients with RA appear to have an approximately 2-fold increased risk of serious infection compared to the general population and non-RA controls, irrespective of TNF-alpha antagonist use. The pooled odds ratio for malignancy was 3.3 (95% confidence interval [CI], 1.2-
Question 45
Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of
Explanation
REFERENCE: O’Reilly R, Link M, Fletcher B, et al: NCCN pediatric osteosarcoma practice guidelines: The National Comprehensive Cancer Network. Oncology (Huntingt) 1996;10:1799-1806, 1812.
Question 46
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling’s test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis? Review Topic
Explanation
Question 47
Glenohumeral disarticulation often leads to which of the following changes?
Explanation
Question 48
- A 13-year-old quarterback feels a “pop” in his knee while being tackled. Radiographs of the knee and results of a Lachman’s test are normal. Examination reveals tenderness over the distal femoral physis. To help confirm the diagnosis, management should first include
Explanation
Question 49
A 72-year-old man was involved in an automobile accident 4 weeks ago. Initially he noted pain about his nondominant left shoulder, which resolved within a few weeks after the accident. He now describes trouble with gripping and carrying items in his left hand. Radiographs are shown in Figures 20a through 20c. His signs and symptoms are the result of injury to which of the following ligaments?
Explanation
REFERENCES: Berger RA: The ligaments of the wrist: A current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63-82.
Cohen MS, Taleisnik J: Direct ligamentous repair of scapholunate dissociation with capsulodesis augmentation. Tech Hand Up Extrem Surg 1998;2:18-24.
Question 50
Figures 30a and 30b are the radiographs of a 61-year-old man with diabetes who fell from a ladder and sustained an isolated closed fracture. After realignment and splint application, what is the most appropriate next step in management?

Explanation
internal fixation in the acute phase (6 to 8 hours) or sub-acute phase (2 to 3 days) is difficult.
Question 51
Figure 46 shows the MRI scan of a patient who has a mass in the calf that has been fluctuating in size. Radiographs are negative. Which of the following procedures will most quickly aid in confirming the diagnosis?
Explanation
REFERENCES: Bianchi S, Abdelwahab IF, Kenan S, Zwass A, Ricci G, Palomba G: Intramuscular ganglia arising from the superior tibiofibular joint: CT and MR evaluation. Skeletal Radiol 1995;24:253-256.
Feldman F, Singson RD, Staron RB: Magnetic resonance imaging of para-articular and ectopic ganglia. Skeletal Radiol 1989;18:353-358.
Question 52
preservation of the radioscaphocapitate ligament, the most radial of the palmar extrinsic ligaments, which prevents ulnar subluxation after proximal row carpectomy.
Explanation
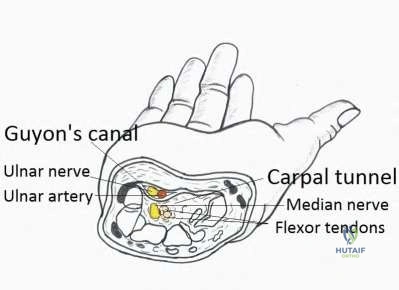
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?
Central space
Hypothenar space
Carpal tunnel
Posterior adductor space
Thenar space CORRECT ANSWER: 5
Flexor tenosynovitis of the thumb flexor tendon sheath can spread proximally and form an abscess within the thenar space of the palm. The flexor pollicis longus tendon does not pass through the central space of the palm or the hypothenar space of the palm. The flexor pollicis longus tendon does pass through the carpal tunnel, but this is not a palmar space. The three palmar spaces include the hypothenar space, the thenar space, and the central space. The posterior adductor space would likely only be involved secondarily after spread from a thenar space infection.
New painful paresthesias near the site of the incision after an ulnar nerve transposition is the result of injury to what nerve?
Medial antebrachial cutaneous
Lateral antebrachial cutaneous
Posterior antebrachial cutaneous
Medial brachial cutaneous
Dorsal antebrachial cutaneous
Branches of the medial antebrachial cutaneous nerve can often be identified during routine ulnar nerve surgery crossing the medial aspect of the elbow. It should be preserved to avoid development of painful paresthesias.
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure
Question 53
A 7-year-old male is struck by a motor vehicle while crossing the street and suffers an open tibia fracture with a crush injury of the ipsilateral foot. After multiple attempts at limb salvage, the family and treating surgeon elect to proceed with a knee disarticulation. What complication of pediatric amputations is avoided with a knee disarticulation as opposed to a transtibial amputation?

Explanation
Krajbich reviews the management of pediatric patients with lower-limb deficiences and amputations. He advocates disarticulation as opposed to transosseous amputation when possible as bone overgrowth has not been observed in bone ends covered by articular cartilage.
O'neal et al retrospectively reviewed their rates of surgical revision for bone overgrowth in pediatric and adolescent amputees. The highest rates of revision were seen with metaphyseal-level amputations (50%) and with traumatic amputations (43%).
Benevenia et al reviewed their rates of overgrowth in skeletally immature transosseous amputees using an autogenous epiphyseal transplant from the amputated limb to cap the medullary canal. They found that only 1 of 10 patients undergoing amputation with this technique had complications due to bone overgrowth, compared with 6 of 7 patients undergoing traditional transosseous amputation.
Illustration A is a clinical photo of bone overgrowth eroding through the soft tissue in a transhumeral amputee. Illustration B demonstrates the radiographic appearance of bone overgrowth in a transtibial amputation.
Incorrect Answers:
Question 54
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management? Review Topic

Explanation
Question 55
A 12-year-old boy has a head-on head collision while playing soccer. He had no loss of consciousness but has persistent headaches for 2 weeks. The patient is now back to school and has no headaches. What is the best next step?
Explanation
Question 56
A 1-year-old infant has the hand deformities shown in Figure 40. What pathologic process is the most likely cause of these deformities?
Explanation
REFERENCE: Foulkes GD, Reinker K: Congenital constriction band syndrome: A seventy-year experience. J Pediatr Orthop 1994;14:242-248.
Question 57
Initial repair of the large U-shaped rotator cuff tear shown in Figure 12 consists of closing the tear side-to-side to take advantage of margin convergence. The most significant biomechanical consequence of this repair step results in
Explanation
REFERENCES: Burkhart SS: A stepwise approach to arthroscopic rotator cuff repair based on biomechanical principles. Arthroscopy 2000;16:82-90.
Burkhart SS, Athanasiou KA, Wirth MA: Margin convergence: A method of reducing strain in massive rotator cuff tears. Arthroscopy 1996;12:335-338.
Question 58
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Explanation
Question 59
An 82-year-old osteoporotic woman undergoes total hip arthroplasty for osteoarthritis. During implant trialing, a crack is heard. Intraoperative fluoroscopy reveals a long, spiral fracture of the distal femur. The fracture is reduced and fixed with an anatomic locking plate. The rest of the total hip arthroplasty proceeds uneventfully. Following surgery the surgeon has a meeting with the family and apologizes and provides full disclosure, accepts responsibility, provides a detailed explanation as to what happened, and gives reassurance that steps will be taken to prevent recurrences. This communication approach will most likely
Explanation
In the event of a medical error or adverse event, effective communication with the patient and family is necessary. Effective communication should comprise: an apology, full disclosure (an explanation of what happened), accepting responsibility, and corrective steps that will be taken to prevent recurrence.While accepting responsibility is integral to the explanation process, it is different from accepting blame.
Mazor et al. found patients would more likely change physicians and seek legal advice in situations with a life-threatening outcome where physicians chose nondisclosure. They recommend full disclosure, acceptance of responsibility, an apology, detailed explanations, and assurances that steps will be taken to prevent recurrences will result in positive outcomes in terms of patient satisfaction, trust, and emotional response.
MacDonald et al. addressed medical errors in an editorial. Besides full disclosure, they feel that an apology is necessary. This includes an acknowledgement of the event and one’s role in the event, and a genuine expression of regret. Apology laws exist to to reduce concerns about legal implications of disclosure and apology.
Incorrect Answers:
Question 60
Acral metastases are most commonly seen in what type of carcinoma?
Explanation
REFERENCES: Hayden RJ, Sullivan LG, Jebson PJ: The hand in metastatic disease and acral manifestations of paraneoplastic syndromes. Hand Clin 2004;20:335-343.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 313.
Question 61
A 25-year-old lineman is referred to your office for a second opinion. 1 year ago, he underwent an arthroscopic procedure for shoulder instability. He complains of persistent sense of instability despite the surgery. Which of the following is a contraindication to revision arthroscopic labral repair for recurrent anterior glenohumeral instability? Review Topic
Explanation
Thermal capsulorrhaphy utilizes heat generated by radiofrequency or laser ablation to cause capsular shrinkage in an effort to treat shoulder instability. However, high recurrence rates have been found, especially around two to three weeks after the index procedure, when the capsular tissue is the weakest. In the setting of recurrence following thermal capsulorrhaphy, open revision is recommended.
Creighton et al. reported on a series of 18 patients undergoing revision arthroscopic stabilization. Of the 18, 3 failed with recurrent instability, all with previous thermal capsulorrhaphy.
Miniaci et al. reviewed the outcomes following thermal capsulorrhaphy noting high rates of recurrent instability, especially in the setting of initial treatment for multidirectional instability.
Park et al. reported on a series of 14 patients undergoing revision following thermal capsulorrhaphy. Ten out of 14 patients had signs of capsular thinning, insufficiency and attenuation.
Wong et al. surveyed 379 shoulder surgeons on the complications following thermal capsulorrhaphy. Capsular insufficiency and thinning were commonly associated with recurrent instability.
Hecht et al. performed thermal capsulorrhaphy and biomechanical analysis of the capsule in a sheep model. The authors found that the capsule was weakest at the 2-3 week post-operative timepoint, leading to the highest rate insufficiency, attenuation and mechanical failure at this time.
Incorrect answers:
Question 62
A 34-year-old man presents to clinic with 4 months of right elbow pain. He began going to the gym and playing squash about 3 months ago. On exam, he is tender over the lateral aspect of the elbow and has pain with resisted wrist extension. Which of the following choices lists the correct compartment of the muscle typically involved in this disease and then lists its antagonist muscle? Review Topic
Explanation
Lateral epicondylitis is an overuse injury, typically secondary to repetitive pronation and supination motion in extension, that leads to inflammation of the ECRB origin at the elbow. Histological analysis typically shows vascular hyperplasia and disorganized collagen. Clinically, patients will have pain over the lateral elbow exacerbated by resisted wrist extension. ECRB, the most commonly involved muscle origin, is innervated by the deep branch of the radial nerve and inserts on the base of the 3rd metacarpal. As it is radial wrist extensor, its antagonist is the ulnar sided wrist flexor.
Brummel et al. reviewed the clinical presentation and management options for lateral epicondylitis. They report acute symptoms in younger patients and chronic symptoms in older patients. NSAIDs, extensor stretching and activity modification are the mainstay of nonsurgical treatment.
Bunata et al. studies 85 cadavar elbows to determine anatomic factors contributing to tennis elbow. They found that the ECRB undersurface rubs against the lateral capitellium in elbow extension leading to tendinosis.
Illustration A is cross-sectional diagram of the forearm with muscle bellies labeled. Notice the location of ECRB in the mobile wad. Illustration B is a coronal T2 MRI showing fluid signal and undersurface tearing near the extensor origin as can be seen in lateral epicondylitis.
Incorrect Answers:
1-4: The ECRB is in the mobile wad and its antagonist is flexor carpi ulnaris. All other answers are incorrect.
Question 63
When treating osteoporosis with alendronate, what is the most common side effect?
Explanation
REFERENCES: Marshall JK, Rainsford KD, James C, et al: A randomized controlled trial to assess alendoronate-associated injury of the upper gastrointestinal tract. Aliment Pharmacol Ther 2000;14:1451-1457.
Lane JM, Sandhu HS: Osteoporosis of the spine, in Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 227-234.
Question 64
Figures 1 through 3 are the radiographs of a 27-year-old man who has had wrist pain since falling 1 day ago. Which treatment offers the best prognosis for prevention of carpal collapse and progressive arthritis?

Explanation
Although this patient’s history includes a recent fall, the radiographs show evidence of a scaphoid nonunion with carpal collapse but no arthritis. Obtaining union of the scaphoid is important to prevent progressive carpal collapse and arthritic changes. ORIF with bone graft is most appropriate to obtain union and correct the collapse deformity. Screw fixation with volar wedge graft often is performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal
row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
Question 65
Which of the following factors can contribute to patellar subluxation following routine total knee arthroplasty?
Explanation
REFERENCE: Ayers DC, Dennis DA, Johanson NA, Pelligrini VD: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Question 66
A healthy 25-year-old man sustains a grade IIIB open tibial fracture. Following appropriate debridement, irrigation, and stabilization with an external fixator, the soft-tissue injury is shown in Figure 30. What is the most appropriate definitive soft-tissue coverage procedure?
Explanation
REFERENCES: Mathes SJ, Nahai F: Vascular anatomy of muscle: Classification and applications, in Mathes SJ, Nahai F (eds): Clinical Application for Muscle and Musculocutaneous Flaps. St Louis, MO, CV Mosby, 1982, p 20.
Bos GD, Buehler MJ: Lower-extremity local flaps. J Am Acad Orthop Surg 1994;2:342-351.
Question 67
An 8-year-old girl has had a painless enlarging mass of insidious onset in the left thigh for the past 3 weeks. Her mother denies any history of trauma, fever, or disease. Examination reveals a nontender, mobile mass in the left medial thigh. Her gait is normal. Figures 25a through 25d show the frog-lateral radiograph, the axial and coronal T1-weighted MRI scans, and the axial T2-weighted MRI scan. Biopsy results reveal a nonrhabdomyosarcoma soft-tissue sarcoma. The most appropriate treatment should consist of
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, p 757.
Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 605.
Question 68
-Figures 10a and 10b are the sagittal and coronal MRI scans of a 5-year-old boy who noticed “clicking” in his right knee. His family denied any trauma, but admitted that the child was active and fell frequently.Birth and developmental history were unremarkable, and specifically negative for other musculoskeletal conditions. On physical examination, there was no warmth, tenderness, or erythema, or effusion. The child had an audible and palpable clunk when the knee was taken from a position of extreme flexion to full extension. There was no anterior, posterior, medial, or lateral instability on examination or medial or lateral joint line tenderness. The child had not been systemically ill. Radiographs were unrevealing.What is the most likely diagnosis?
Explanation

Question 69
Following a vertebroplasty of L2, cement is noted to protrude directly anterior to the L2 vertebral body. The cement is closest to which of the following structures?
Explanation
and duodenum are anterior to the aorta. The aorta lies in the midline just in front of the
vertebral body.
REFERENCES: Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3.
Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 331.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, plate 328.
Question 70
What is the most appropriate treatment for a chordoma involving the sacrum?
Explanation
REFERENCES: Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133.
Stener B, Gunterberg B: High amputation of the sacrum for extirpation of tumors: Principles and technique. Spine 1978;3:351-366.
Stener B: Resection of the sacrum for tumors. Chir Organi Mov 1990;75:S108-S110.
Question 71
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Treatment should include

Explanation
Question 72
Based on the appearance of the imaging studies shown in Figures 11a through 11c, what structure has most likely been injured?
Explanation
REFERENCES: Boden BP, Pearsall AW: Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 1997;5:47-57.
Desio SM, Burks RT, Bachus KN: Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 1998;26:59-65.
Question 73
A 6 year-old-boy falls from his bunk bed and suffers the injury seen in Figures A and B. Upon presentation to the emergency room he is noted to have a pink hand with brisk capillary refill, but no palpable pulses. After closed reduction in the operating room and the procedure seen in Figures C and D, he remains well perfused, pulses are still not palpable, but triphasic pulses can be heard on doppler examination. What is the most appropriate course of action? Review Topic

Explanation
Pediatric supracondylar humerus fractures presenting with vascular compromise can present a challenge for clinical decision making. If the hand lacks adequate perfusion on presentation it requires emergent treatment with closed reduction and pinning. If perfusion does not return, then surgical exploration of the antecubital fossa is required. Treatment of the "pink pulseless hand" remains controversial. If the hand is well perfused but lacks palpable pulses then it should be expeditiously reduced and pinned. If the hand remains well perfused with triphasic doppler signals, no additional intervention is required. Recommendations vary if the hand is perfused, and pulses cannot be detected on palpation or doppler.
If there is a normal neurovascular exam on presentation, but abnormal after reduction and pinning, then one must consider that the reduction may have entrapped the brachial artery. If hardware removal and fracture re-displacement does not improve pulses/perfusion of the hand, or if the fracture can not be reduced without diminishing perfusion, then open reduction is indicated to evaluate the brachial artery.
Shah et al. present their preferred algorithm for treatment of a pink pulseless hand. They note that even with good clinical perfusion there may be a vascular injury or entrapment of the brachial artery. Thus they recommend if the hand is pink with no palpable pulse, perform a doppler exam. Triphasic doppler signals allow for observation, while abnormal or non-detectable doppler signals require surgical exploration. If an AIN or median nerve injury is present, exploration is considered. A diagram of their algorithm can be seen in Illustration A.
Weller et al. present a retrospective review of 1297 supracondylar humerus fractures. They had 20 patients (1.5%) with a pink pulseless hand with good doppler signals following closed reduction and fixation. These patients were treated with close observation. One patient developed inadequate perfusion nine hours after reduction and required vascular repair. The remaining 19 patients regained palpable pulses prior to discharge or prior to the first follow-up visit. They recommend observation despite non-palpable pulses as long as other signs of perfusion (capillary refill and doppler signals) suggest the hand is well perfused.
Figures A and B are AP and lateral radiographs of a type III supracondylar humerus fracture. Figures B and C demonstrate this fracture following closed reduction and percutaneous pinning with three lateral pins. Illustration A is a flow chart of a proposed decision making algorithm for a pink pulseless hand as presented by Shah et al.
Incorrect Answers:
reduction and fixation. Answer 2- Changing the pattern of fixation would only be indicated if the current construct did not provide stable fixation of the fracture. Answer 3- Following reduction and fixation of a supracondylar humerus fracture the most appropriate dressing is rigid long arm immobilization in a splint or cast. If there is concern for edema or perfusion then a cast should be bivalved. Answer 5- Surgical exploration of the antecubital fossa would be indicated if the hand had inadequate perfusion, or if the fracture could not be reduced and fixed without causing a notable decrease in pulses or perfusion.
Question 74
A 24-year-old man reports the development of a foot drop following a knee dislocation 1 year ago. The common peroneal nerve was found to be in continuity at the time of surgical reconstruction of the posterolateral corner of the knee joint. He would like to eliminate the need for an ankle-foot orthosis. What is the best option to achieve elimination of the orthosis?
Explanation
REFERENCES: Pinzur MS, Kett N, Trilla M: Combined anteroposterior tibial tendon transfer in post-traumatic peroneal palsy. Foot Ankle 1988;8:27l-275.
Lipscomb P, Sanchez J: Anterior transplantation of the posterior tibial tendon for persistant palsy of the common peroneal nerve. J Bone Joint Surg Am 1961;43:60-66.
Question 75
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel’s sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Styf J: Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165-169.
Sridhara CR, Izzo KL: Terminal sensory branches of the superficial peroneal nerve: An entrapment syndrome. Arch Phys Med Rehabil 1985;66:789-791.
Styf J: Entrapment of the superficial peroneal nerve: Diagnosis and results of decompression.
J Bone Joint Surg Br 1989;71:131-135.
Question 76
What is the most common complication associated with open reduction and internal fixation using a 90/90 plate configuration and olecranon osteotomy for an OTA type C2 distal humerus fracture?
Explanation
Question 77
Figures 17a and 17b show the AP and lateral radiographs of a 75-year-old woman who reports giving way and shifting of the knee, particularly when she is descending stairs or ambulating on level surfaces. History reveals a total knee replacement 5 years ago. Treatment should consist of
Explanation
REFERENCE: Pagnano MW, Cushner FD, Scott WN: Role of the posterior cruciate ligament in total knee arthroplasty. J Am Acad Orthop Surg 1998;6:176-187.
Question 78
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Explanation
REFERENCES: Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 79
A 57-year-old man has had right ankle pain for the past 10 months following an injury that went untreated. Radiographs are shown in Figures 30a through 30c. Management should consist of
Explanation
REFERENCES: Marti RK, Raaymakers EL, Nolte PA: Malunited ankle fractures: The late results of reconstruction. J Bone Joint Surg Br 1990;72:709-713.
Geissler W, Tsao A, Hughes J: Fractures and injuries of the ankle, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2201-2206.
Yablon IG, Leach RE: Reconstruction of malunited fractures of the lateral malleolus. J Bone Joint Surg Am 1989;71:521-527.
Question 80
A 26-year-old man has had a 2-year history of pain and stiffness after sustaining a comminuted olecranon fracture. Treatment at the time of injury consisted of open reduction and internal fixation with tension band wiring. Examination reveals motion of 45 degrees to 110 degrees and pain throughout the arc of motion. Resisted flexion and extension are painful. Forearm rotation is normal. Radiographs are shown in Figure 51. Treatment should consist of
Explanation
REFERENCES: Morrey BF: Distraction arthroplasty: Clinical applications. Clin Orthop 1993;293:46-54.
O’Driscoll SW: Elbow arthritis: Treatment options. J Am Acad Orthop Surg 1993;1:106-116.
Question 81
- Figures 38a & 38b show radiographs of a 40 year old man who underwent a Putti-Platt repair for recurrent dislocations at age 22. He reports increasing pain in the shoulder and limited motion for five years. Examination reveals 130 degrees of elevation and 15 degrees of external rotation. Non-surgical treatment has failed. Treatment should now consist of what?
Explanation
Late onset of pain (average 13 years) was noted following this procedure in a small number of patients. The pain is attributed to excessive G-H compressive forces due to limited external rotation. NSAIDS and PT are first line treatments. If these fail, the authors demonstrated good results with release of the anterior structures. Choices 3 & 4 would probably be reserved for patients older than 50 with more advanced signs of degenerative disease.
Question 82
A 15-year-old right-handed pitcher reports shoulder pain after throwing. His symptoms have been present for 3 months and have been getting progressively worse. Clinical examination shows no atrophy of the shoulder muscles, but he has pain with resisted motion of the shoulder, especially internal rotation. Radiographs are shown in Figures 73a and 73b. What is the next step in the evaluation and treatment of his shoulder pain? Review Topic

Explanation
Question 83
The function of which of the following structures is to resist internal tibial rotation with the knee in full extension? Review Topic
Explanation
The posterior oblique ligament is a structure within the posteromedial corner of the knee, with attachments proximally to the adductor tubercle of the femur and distally to the tibia/posterior knee capsule. The posterior oblique ligament and posteromedial capsule play a significant role in the prevention of additional posterior tibial translation in the knee in the setting of posterior cruciate ligament injury. They also act to resist internal tibial rotation with the knee in full extension.
Griffith et al. reports that the posterior oblique ligament provides significant resistance to valgus and internal rotation forces with knee extension. They used a cadaver model and demonstrated that the superficial MCL resists valgus and external rotation forces more than the posterior oblique ligament, while the posterior oblique ligament is more involved in resisting internal rotation.
Tibor et al. reviews the anatomy of the posteromedial corner of the knee. They report that failing to recognize injury to these structures may cause failure of cruciate ligament reconstruction surgery, and that reconstruction or repair of the posteromedial corner may be indicated in the face of multiple ligament injuries.
Illustration A shows the posteromedial corner of the knee, including the posterior oblique ligament.
Incorrect answers:
1-4: These structures are not primary restraints to internal tibial rotation in full extension.
Question 84
An 80-year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 85
A 66-year-old male undergoes the procedure shown in figures A and B. After 4 years, he develops progressive pain and limitations in his daily function that is refractory to conservative measures. He is indicated for conversion to a total knee replacement with almost complete relief of his symptoms postoperatively. What preoperative factor likely led to the subsequent failure?
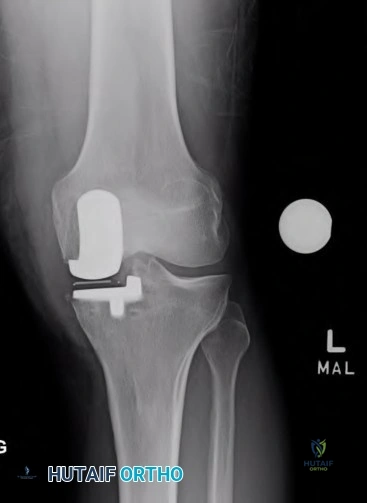
Explanation

OrthoCash 2020
Which of the following is the most common cause of early revision surgery (<20 weeks) following a hip resurfacing arthroplasty?
Periprosthetic fracture
Rupture of abductors
Dislocation
Heterotopic ossification
Post-operative stiffness
Periprosthetic fracture, specifically femoral neck fracture, is the most common cause of early revision less than 20 weeks following surgery.
The rate of femoral neck fractures following hip resurfacing varies, but most literature reports a rate of 1%. A majority of these fractures happen in the early post-operative period and are the most frequent cause of revision surgery within several months following surgery. The cause is usually multifactorial, but placing the femoral implant in varus, osteonecrosis, and notching have been proven risk factors for fracture.
Little el al. report on 377 patients undergoing hip resurfacing. 13 required revision including 8 for fracture of the femoral neck and 3 for loosening of a component. Evidence of osteonecrosis was seen in two of these cases, leading the authors to believe it may contributed to fracture.
Illustration A shows a comparison of a typical total hip replacement and a hip resurfacing arthroplasty. Illustration B shows notching of the femoral neck, a known cause of femoral neck fracture following hip resurfacing. Illustration C shows a femoral neck fracture in a patient with a hip resurfacing.
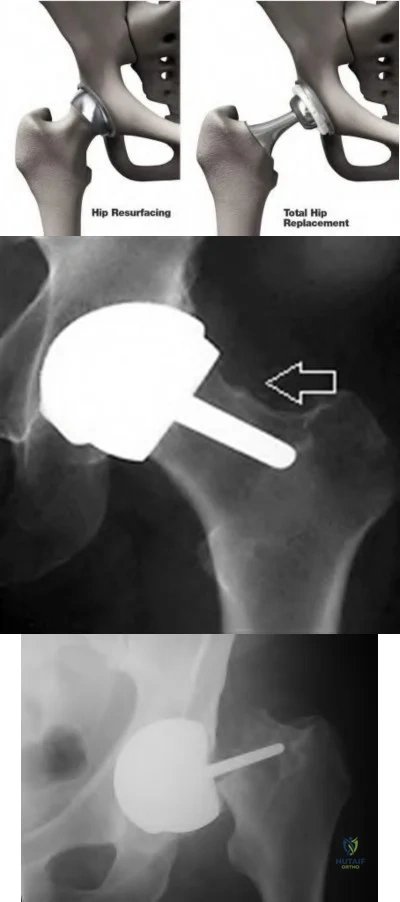
OrthoCash 2020
A 55-year-old male undergoes a revision total knee arthroplasty of an implant that is only 3 years old. At the time of surgery, the tibial polyethylene liner shows catastrophic delamination and cracking. What is the most likely cause of this extensive, accelerated wear of the polyethylene liner?
Sterilization in ethylene oxide
Gamma irradiation of the polyethylene liner in the presence of air
Gamma irradiation of the polyethylene liner with vacuum packaging
Gamma irradiation of the polyethylene liner in nitrogen
Gamma irradiation of the polyethylene liner in argon Corrent answer: 2
Irradiation of polyethylene in air (i.e. oxygen present) has been shown to be a risk factor for catastrophic failure after total knee replacement.
Free radicals are generated when polyethylene is irradiated in the presence of air. Initially, these free radicals result in cross-linking. However, if the polyethylene is exposed to these free radicals for an extended period of time, delamination, cracking, and catastrophic failure may ensue. The industry has completely abandoned this method of sterilization as a result. Currently, the standard of care is irradiation of polyethylene in an inert gas (e.g. argon, nitrogen or vacuum packaging). The amount of oxidative products when polyethylene is sterilized in the absence of oxygen is much less and does not lead to catastrophic failure.
Sterilization without irradiation is another option (ethylene oxide). When this occurs, there is no cross-linking and thus the increased wear properties are lost. However, since there is no oxidization, you do not have the risk of catastrophic failure as seen in those liners irradiated in the presence of oxygen.
The cited reference by McNulty et al. from Orthopedics discusses the influence of sterilization methods on wear performance. They found that gamma irradiation and storage of the polyethylene components in an essentially oxygen-free environment imparted by gamma irradiation in a vacuum foil pouch (GVF) protects the components from oxidization.
Illustration A shows a polyethylene liner that has undergone catastrophic wear as a result of irradiation in the presence of oxygen.
Incorrect Answers:
catastrophic wear, although wear properties are less than gamma irradiation in the absence of air.
OrthoCash 2020
Which of the following interventions reduces osteolysis around distal portion of the femoral stem when performing a total hip arthroplasty?
Use of an extended offset femoral neck component
Use of a proximal circumferentially coated ingrowth stem
Use of a collared stem
Use of a long femoral stem
Ensuring that the stem fills the diaphysis of the femur Corrent answer: 2
Osteolysis of the femur is caused by activation of macrophages by microscopic polyethylene particles within the "effective joint space", defined as any area where joint fluid can come into contact with bone. This can occur above the acetabular cup, through screw holes, and down the femoral shaft around the prosthetic stem. Ideally, with a cementless stem, both the proximal and metaphyseal femur are well filled by the prosthesis. Collared stems are used to augment poor calcar bone quality or bone loss.
Sinha et al showed in a retrospective review of 101 hips with cementless circumferentially coated femoral stems no distal femur osteolysis occurred, but 82% showed “evidence of proximal femur stress shielding”, though only 38% showed proximal femoral osteolysis.
OrthoCash 2020
During a minimally invasive approach to total hip arthroplasty a femoral periprosthetic fracture occurs. Which of the following steps is crucial to properly treat this complication?
Transitioning to an extensile approach to adequately visualize and reduce the fracture
Limiting post-operative weight bearing
Switching to a cemented femoral stem to avoid the stresses created during press-fit fixation
Delaying the arthroplasty until the fracture has healed
Supplementing the fracture with autograft Corrent answer: 1
Proper treatment of an intraoperative femoral fracture during total hip arthroplasty involves adequate exposure, anatomic reduction, and bypassing the fracture site by 2 cortical diameters of the femur with a long stem. This may involve repositioning the patient on the table if the arthroplasty is performed in the supine position. Minimally invasive surgical techniques have been developed to insert the components through smaller exposures and less soft tissue dissection. The purported advantages include faster rehabilitation, less blood loss, shorter hospital stays, and better cosmesis. However, complications an arise if the surgeon sacrifices surgical exposure and visualization.
Fehring et al review 3 cases of total hip arthroplasty performed through minimally invasive techniques with catastrophic outcomes. Intra-operative fracture, chronic instability, and death were all identified.
OrthoCash 2020
A 70-year-old man underwent total hip arthroplasty 4 months ago and has experienced 3 dislocations. Radiographs reveal no failure of the hardware and an acetabular component that has an abduction
angle of 40 degrees and a version of 10 degrees retroverted. What is the most appropriate treatment for the recurrent dislocations?
hip abduction brace
revision of the acetabular liner to a constrained type
revision of the entire acetabular component
revision of the femoral head to a larger size
revision to an extended offset prosthesis Corrent answer: 3
Per Dorr et al: post-operative hip instability can be caused by several factors: soft tissue imbalance, component malposition, or position. Component malposition, as in this case, should be treated with revision of the offending component. In this case the acetabulum was placed in retroversion when it should have been 15-20 degrees anteverted. None of the other options addresses the cause of the instability. According to Morrey, the most signficant risk factors to instability are prior hip surgery, trochanteric nonunion, and posterior surgical approach. He wrote that the most reliable way to correct instability is to reorient a retroverted acetabular cup.
OrthoCash 2020
In patients with sickle cell disease and asymptomatic osteonecrosis of the femoral head identified with magnetic resonance imaging, what percentage will eventually go on to femoral head collapse?
Question 86
- A 15-year-old dancer who has had brief episodes of back pain over the past 2 years now reports a 3 month history of low back pain and a decreased tolerance for dance. Figure 22a-c show flexion and extension x-rays and CT scan. She reports no leg pain, nor any bowel or bladder difficulties. Management should now consist of
Explanation
Question 87
A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
Explanation
Question 88
Up to what time frame are the risks minimized in anterior revision disk replacement surgery?
Explanation
REFERENCE: Tortolani JP, McAfee PC, Saiedy S: Failures of lumbar disc replacement. Sem Spine Surg 2006;18:78-86.
Question 89
Storage of musculoskeletal allografts by cryopreservation is achieved by
Explanation
sulfoxide or glycerol which displaces the cellular water. The controlled rate freezing is then done to prevent ice crystal formation. Fresh allografts are not frozen in order to maintain maximum cellular viability, and this process limits the shelf life of osteochondral allografts. Freeze-drying involves replacement of water in the tissue with alcohol to a moisture level of
5% and then uses a vacuum process to remove the alcohol from the tissue. Preparation of fresh frozen grafts involves freezing the graft twice and packaging the tissue without solution at
minus 80 degrees C.
REFERENCES: American Association of Tissue Banks: Standards for Tissue Banking. MacLean, VA, American Association of Tissue Banks, 1999.
Vangsness CT Jr, Triffon MJ, Joyce MJ, et al: Soft tissue allograft reconstruction of the human knee: A survey of the American Association of Tissue Banks. Am J Sports Med 1996;24:230-234.
Brautigan BE, Johnson DL, Caborn DM, et al: Allograft tissues, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 2003, pp 205-213.
Question 90
Which clinical signs are consistent with the diagnosis of cauda equina syndrome?
Explanation
Cauda equina syndrome is a lower-motor neuron deficit. Hyperreflexia, clonus, and other upper-motor neuron findings would not be seen. Saddle anesthesia, motor weakness, and neurogenic bladder are elements critical to the diagnosis of cauda equina syndrome.
RECOMMENDED READINGS
Kostuik JP, Harrington I, Alexander D, Rand W, Evans D. Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am. 1986 Mar;68(3):386-91. PubMed PMID: 2936744. View Abstract at PubMed
Spector LR, Madigan L, Rhyne A, Darden B 2nd, Kim D. Cauda equina syndrome. J Am Acad Orthop Surg. 2008 Aug;16(8):471-9. Review. PubMed PMID: 18664636. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 78 THROUGH 80
Figures 78a and 78b are the axial and sagittal MR images of an otherwise healthy 24-year-old woman who has had 8 weeks of severe leg pain without weakness.
A B
Question 91
The peroneus tertius is a commonly used landmark for arthroscopic portal placement. What is the function of this tendon?
Explanation
REFERENCES: Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle.
Clin Anat 2006;19:611-614.
Williams PL, Bannister LH, Berry MM, et al (eds): Gray’s Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.
Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 21.
Question 92
..The optimal method to treat a recurrent presentation of pigmented villonodular synovitis (PVNS) with diffuse joint involvement in a 24-year-old woman with pain and symptomatic effusions is
Explanation

Question 93
Histologically, synovial chondromatosis is characterized by
Explanation
REFERENCES: Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;l59:792-801.
Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1962;44:77.
Question 94
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?
Explanation
REFERENCES: Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79.
Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
Davis DA, Cohen PR: Subungual exostosis: Case report and review of the literature. Pediatr Dermatol 1996;13:212-218.
Question 95
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of
Explanation
REFERENCES: Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 961-990.
Question 96
The mechanism for the osseous destruction is attributable to
Explanation
This scenario is a classic example of the development of Charcot foot. A red, swollen, deformed foot without ulceration suggests neuroarthropathy. Normal inflammatory marker findings, no history of fever or chills, and radiographs demonstrating bone loss support the diagnosis. Limb elevation with dramatic reduction in erythema is also characteristic of this disease process and does not occur with infection. Total-contact casting is the cornerstone of treatment for acute Charcot disease. Hemoglobin A1C is an indicator of glucose averaged over a 3-month period, providing the most reliable indication of a patient's ongoing glucose control. The pathophysiology of bone destruction is believed to be hypervascularity of bone. Infection and Charcot disease may develop simultaneously, but the combination is rare.
RECOMMENDED READINGS
Kaynak G, Birsel O, Güven MF, Ogüt T. An overview of the Charcot foot pathophysiology. Diabet Foot Ankle. 2013 Aug 2;4. doi: 10.3402/dfa.v4i0.21117.Print 2013. PubMed PMID: 23919113.View Abstract at PubMed
Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006 May;27(5):324-9. PubMed PMID: 16701052. View Abstract at PubMed
Question 97
Which of the following is an advantage of using blocking screws for tibial nailing?

Explanation
Krettek found that medial and lateral blocking screws can increase the primary stability of distal and proximal metaphyseal fractures after nailing and can be an effective tool for selected cases that exhibit malalignment and/or instability by decreasing mechanically measured deformation.
In a later clinical study, Krettek found that after using blocking screws, tibial healing was evident radiologically at a mean of 5.4 months with a decreased rate of malunions.
Ricci also found that blocking screws are effective to help obtain and maintain alignment of fractures of the proximal third of the tibial shaft treated with intramedullary nails.
Question 98
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?
Explanation
REFERENCES: Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
Wirth MA, Rockwood CA Jr: Complications of total shoulder replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Question 99
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
REFERENCES: Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Warner JJ, Deng XH, Warren RF, Torzilli PA: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Question 100
A 13-year-old boy has a mild deformity of the left sternoclavicular joint after being involved in a rollover accident while riding an all-terrain vehicle. Examination in the emergency department reveals that he is hemodynamically stable, and his neurovascular examination is normal. The CT scan shown in Figure 22 was obtained because radiographs were inconclusive. Management should consist of
Explanation
REFERENCES: Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, p 581.
Wirth MA, Rockwood CA Jr: Acute and chronic traumatic injuries of the sternoclavicular joint. J Am Acad Orthop Surg 1996;4:268-278.
