Full Question & Answer Text (for Search Engines)
Question 1:
A 12-year-old Little League pitcher reports lateral elbow pain and “catching.” Examination reveals painful pronation and supination and tenderness over the lateral elbow. Radiographs are shown in Figures 22a and 22b. Initial management should consist of
Options:
- rest and repeat examination and radiographs until complete healing occurs.
- rest and resumption of play when he is asymptomatic and examination shows restoration of painless range of motion.
- arthroscopic in situ drilling.
- arthroscopic drilling and internal fixation.
- arthroscopy with removal of the loose body, followed by lateral column osteotomy.
Correct Answer: rest and resumption of play when he is asymptomatic and examination shows restoration of painless range of motion.
Explanation:
DISCUSSION: Osteochondritis of the capitellum is a common problem in young throwing athletes and gymnasts. The mechanism of injury involves lateral compression and axial loading of the capitellum. Repetitive trauma causes ischemia with resultant osteochondral necrosis and sometimes eventual separation. Initial management includes rest for a minimum of 6 weeks; occasionally bracing is used. At long-term follow-up, there is typically an observed radiographic abnormality indicating incomplete healing even in asymptomatic patients. Arthroscopy with in situ drilling is reserved for symptomatic lesions that have an intact articular surface. Lesions with partial separation often require fixation. Lateral column osteotomy is a new investigational procedure designed to relieve lateral compression forces and may be used in salvage cases.
REFERENCES: Kobayashi K, Burton KJ, Rodner C, et al: Lateral compression injuries in the pediatric elbow: Panner’s disease and osteochondritis dissecans of the capitellum. J Am Acad Orthop Surg 2004;12:246-254.
Yadao MA, Field LD, Savoie FH III: Osteochondritis dissecans of the elbow. Instr Course Lect 2004;53:599-606.
Question 2:
In a patient with a C5-6 herniation, the most likely sensory deficit will be in the
Options:
- lateral shoulder.
- radial forearm, thumb, and index finger.
- dorsal forearm and middle finger.
- ulnar forearm, ring finger, and little finger.
- volar forearm and palm.
Correct Answer: radial forearm, thumb, and index finger.
Explanation:
DISCUSSION: A C5-6 herniation compresses the C6 root, which innervates the radial forearm, thumb, and index finger. The lateral shoulder is innervated by C5. The dorsal forearm and the middle finger typically are innervated by C7. The ulnar forearm, ring finger, and little finger are innervated by C8. There is no specific nerve associated with the volar forearm and palm.
REFERENCE: Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 3:
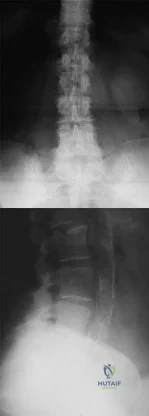
A 78-year-old woman reports a 1-week history of severe low back pain. She denies any trauma or recent falls. She is neurologically intact, and is able to ambulate, although she does require the use of a walker. Radiographs of the lumbar spine show a T11 compression fracture with a 20% loss of anterior column height. What is the most appropriate management at this time? Review Topic
Options:
- Bed rest until symptoms resolve
- Analgesics and progressive rehabilitation
- Anterior thoracic corpectomy and arthrodesis with instrumentation
- Posterior thoracic decompression and fusion
- Vertebral cement augmentation
Correct Answer: Analgesics and progressive rehabilitation
Explanation:
The patient has sustained a thoracic compression fracture, which is very common in elderly patients, and can occur with minimal to no trauma. There is approximately a 20% loss of anterior vertebral body height. The patient is neurologically stable, and is able to ambulate with an assistive device. Initial treatment should consist of progressive mobilization with analgesics as needed. Fractures treated in this manner have a high rate of success, and surgical treatment is often not necessary. In the absence of neurologic impairment or impending structural instability, surgical decompression and fusion is not indicated. Bed rest is contraindicated. Cement augmentation is a reasonable treatment option when a patient fails nonsurgical management, although recent studies have called into question its efficacy when compared with placebo.
Question 4:
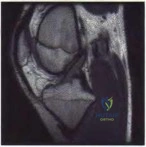
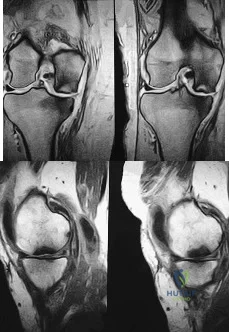
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. The injured structure is composed of an
Options:
- anterolateral bundle that is tight in flexion and a posteromedial bundle that is tight in extension.
- anterolateral bundle that is tight in extension and a posteromedial bundle that is tight in flexion.
- anteromedial bundle that is tight in flexion and a posterolateral bundle that is tight in extension.
- anteromedial bundle that is tight in extension and a posterolateral bundle that is tight in flexion.
Correct Answer: anterolateral bundle that is tight in flexion and a posteromedial bundle that is tight in extension.
Explanation:
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used.
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for
vascular injury.
Question 5:
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Options:
- directly posterior to the posterior cruciate ligament (PCL).
- posteromedial to the PCL.
- posterolateral to the PCL.
- in the posteromedial corner of the knee.
Correct Answer: posterolateral to the PCL.
Explanation:
DISCUSSION:
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 6:
A college basketball player is struck in the eye by a player’s hand while driving to the basket. Fluorescein evaluation reveals the injury shown in Figure 18. Management should consist of
Options:
- administration of ophthalmic corticosteroids and antibiotics with application of an eye patch.
- evaluation of intact visual fields and pupillary responses prior to a return to play.
- consultation with an ophthalmologist prior to emergent repair of the damaged structure.
- measurement of ocular pressure and fundoscopic examination in a properly lit examination room.
- strict bed rest with the head elevated, minimizing head motion during the healing process.
Correct Answer: administration of ophthalmic corticosteroids and antibiotics with application of an eye patch.
Explanation:
DISCUSSION: The athlete has a corneal abrasion. Fluorescein staining identifies the break in the epithelium when examined with ultraviolet light. Topical antibiotics are used as prophylaxis against secondary bacterial infection, and the patch, applied with the lid closed, is used for comfort and to promote epithelial healing. The accompanying symptoms, including pain, tearing, and photophobia, are usually too intense to allow a return to play. Surgery is reserved for a corneal laceration with associated loss of the anterior chamber. While a proper fundoscopic examination may be a consideration, increased intraocular pressure is not typically associated with this injury. Traumatic hemorrhage in the anterior chamber (hyphema) necessitates strict bed rest during the early phases of healing; examination will most likely reveal the red fluid level of blood settling inferiorly in the anterior chamber. It is often associated with increased intraocular pressure.
REFERENCES: Brucker AJ, Kozart DM, Nichols CW, et al: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby-Year Book, 1991, pp 650-670.
Zagelbaum BM: Treating corneal abrasions and lacerations. Phys Sports Med 1997;25:38-44.
Question 7:
A child with an idiopathic clubfoot is successfully treated by the Ponseti method. The risk of recurrence of the deformity is most dependent on which of the following factors? Review Topic
Options:
- Maternal age
- Positive family history
- Family's compliance with bracing
- The child's age at walking
- The child's body mass index
Correct Answer: Family's compliance with bracing
Explanation:
The recurrence rate of clubfoot deformity after successful correction by the Ponseti method has been shown to inversely correlate with reported brace compliance. Maternal age, walking age, and body mass index have not been correlated to recurrence. A positive family history increases the risk of a child being born with a clubfoot but does not influence the recurrence rate.
Question 8:
The acceleration of an object under the influence of a force depends directly on the mass of the object. The angular acceleration of an object under the influence of a moment depends directly on the
Options:
- area moment of inertia.
- weight squared.
- length of the lever arm.
- mass moment of inertia.
- initial velocity.
Correct Answer: mass moment of inertia.
Explanation:
DISCUSSION: Similar to the action of a force, a moment tends to angularly accelerate an object in a manner proportional to a quantity related to the mass of the object. The concept of a more massive object requiring a larger force to cause the same straight line acceleration is straightforward. The concept for changing angular velocity is similar but not identical. The proportional constant between the moment and the resulting angular acceleration is the mass moment of inertia, which depends not only on the mass of the object, but also its distribution. The unit of mass moment of inertia is obtained by multiplying the mass of the object by the square of the distance between an equivalent location of the center of rotation of the object and an equivalent location of the center of mass. Orthopaedic surgeons can change both the amount of mass carried by a limb and the way that the mass is distributed. For example, in applying a cast to the leg, the physician can affect the mass of the cast by the choice of casting material and by the size of the cast. As the mass moment of inertia of the limb increases (eg, by applying the cast farther down on the leg or using a heavier casting material), the patient will need to exert larger moments to angularly accelerate the leg during gait.
REFERENCES: Andriacchi T, Natarajan RN, Hurwitz DE: Musculoskeletal dynamics, locomotion, and clinical applications, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 43-47.
Burstein AH, Wright TM: Fundamentals of Orthopaedic Biomechanics. Baltimore, MD, Williams and Wilkins, 1994, pp 3-7.
Question 9:
A 42-year-old patient has had painful inferior subluxation of the glenohumeral joint following a recent cerebrovascular accident (CVA). Figure 34 shows the AP radiograph of the shoulder. Management should consist of
Options:
- closed reduction.
- symptomatic sling support and range-of-motion exercises.
- arthroscopic thermal capsulorrhaphy.
- an open anterior-inferior capsular shift.
- a Laterjet procedure.
Correct Answer: symptomatic sling support and range-of-motion exercises.
Explanation:
DISCUSSION: Following a CVA and with the resumption of upright posture, downward subluxation of the glenohumeral joint may occur. Although usually painless, some patients may report pain secondary to stretching of the brachial plexus. This is the result of flaccid paralysis of the deltoid muscle, and it will persist until some motor tone or spasticity returns to the shoulder girdle musculature. Early sling support and range-of-motion exercises to prevent contracture will provide the best relief. Surgical procedures are not indicated.
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
Question 10:
Figures 21a through 21c show the radiographs of a 70-year-old woman who has persistent pain with activity after undergoing hip revision 6 months ago. Treatment should now consist of
Options:
- shortening of the femoral neck.
- exchange of the acetabular liner.
- revision of the femoral component.
- revision of both components.
- revision of the acetabular component.
Correct Answer: revision of the acetabular component.
Explanation:
DISCUSSION: The radiographs show disruption of the posterior column of the acetabulum with radiolucencies about the component. Because the patient requires a stable construct to allow the bone to heal, the treatment of choice is an antiprotrusio cage and a graft.
REFERENCES: Gill TJ, Sledge JB, Muller ME: The Burch-Schneider anti-protrusio cage in revision total hip arthroplasty: Indications, principles, and long-term results. J Bone Joint Surg Br 1998;80:946-953.
Sharkey PF, Hozack WJ, Callaghan JJ, et al: Acetabular fracture associated with cementless acetabular component insertion: A report of 13 cases. J Arthroplasty 1999;14:426-431.
Question 11:
Surgical treatment for symptomatic disk herniations is associated with which of the following?
Options:
- Substantial rate of nerve root injury
- Early relief of pain sustained out to 2 years
- Recurrent herniation rate of 35%
- Outcomes that are substantially worse than nonsurgical management
- 10% rate of infectious diskitis
Correct Answer: Early relief of pain sustained out to 2 years
Explanation:
DISCUSSION: The recently published SPORT trial verifies that surgical treatment of symptomatic disk herniations is associated with early and sustained pain relief. The trial also verifies that nonsurgical management is associated with improved symptoms as well. Nerve root injury, recurrent herniation, and diskitis are known complications of surgery, but all are less common than described above.
REFERENCE: Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.
Question 12:
Figures 6a through 6d show the radiographs and biopsy specimens of an 8-year-old girl with leg pain. Management of the lesion should consist of
Options:
- wide resection and salvage of the physis.
- resection and hemicondylar osteoarticular allograft.
- cryosurgery.
- radiation therapy.
- curettage and bone grafting.
Correct Answer: curettage and bone grafting.
Explanation:
DISCUSSION: The biopsy specimens show a chondromyxoid fibroma with varying amounts of cartilage, benign fibrous tissue, giant cells, and loose myxoid areas. Chondromyxoid fibroma is a benign active bone lesion that is best treated with aggressive curettage and bone grafting. Although recurrences are common, more aggressive treatment is not warranted initially.
REFERENCES: Wilson AJ, Kyriakos M, Ackerman LV: Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-518.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 167-189.
Question 13:
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of
Options:
- chemotherapy, wide resection, and endoprosthetic reconstruction.
- radiation therapy only.
- chemotherapy only.
- prophylactic internal fixation with a locked intramedullary rod.
- open curettage, bone grafting, dynamic hip screw fixation, and radiation therapy.
Correct Answer: prophylactic internal fixation with a locked intramedullary rod.
Explanation:
DISCUSSION: The underlying diagnosis is multiple myeloma. Because the patient has a large lucent lesion in the peritrochanteric region of the left proximal femur, the risk of pathologic fracture is high. Consideration should be given to prophylactic internal fixation with a locked intramedullary rod. The lesion does not appear to be a sarcoma requiring wide resection and endoprosthetic reconstruction. Neither chemotherapy nor radiation therapy alone is likely to result in long-term stabilization of the proximal femur. Postoperative treatment with bisphosphonates and radiation therapy is indicated to decrease the risk of future pathologic fractures. The patient should also be referred to a medical oncologist for medical management.
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 14:
Figure 2 shows the AP radiograph of an 18-year-old woman with progressive and severe right hip pain. Nonsteroidal anti-inflammatory drugs no longer control her pain. What is the next most appropriate step in management?
Options:
- Total hip arthroplasty
- Single innominate (Salter) osteotomy
- Chiari osteotomy
- Periacetabular osteotomy
- Varus intertrochanteric osteotomy
Correct Answer: Periacetabular osteotomy
Explanation:
DISCUSSION: A concentric hip with acetabular dysplasia in a symptomatic patient is best treated by periacetabular osteotomy. The Salter osteotomy is less optimal because the method has limited correction, is uniaxial, cannot be tailored to the deformity, and lateralizes the entire hip joint, thereby increasing the joint reactive forces. Because the hyaline cartilage of the joint is histologically normal, rotating the hyaline cartilage into an optimal position is preferable to augmenting the acetabulum with a shelf or by Chiari osteotomy. Varus intertrochanteric osteotomy has no significant role in the treatment of acetabular dysplasia. Total hip arthroplasty may be required in the future but should not be the first choice.
REFERENCE: Millis MB, Murphy SB, Poss R: Osteotomies about the hip for the prevention and treatment of osteoarthritis. Instr Course Lect 1996;45:209-226.
Question 15:
..The optimal method to treat a recurrent presentation of pigmented villonodular synovitis (PVNS) with diffuse joint involvement in a 24-year-old woman with pain and symptomatic effusions is
Options:
- 700 cGy of radiation therapy.
- open arthrotomy with synovectomy.
- imatinib therapy.
- observation. DISCUSSION.. Local control of recurrent diffuse PVNS is best accomplished with open arthrotomy and complete synovectomy. Arthroscopic methods in the setting of persistent diffuse PVNS are associated with an unacceptably high rate of recurrence. Radiation therapy (700 cGy) is the typical dose administered for heterotopic ossification prophylaxis, but this dose is not high enough to achieve local control in PVNS. Imatinib, a colony-stimulating factor inhibitor, has been described for recurrent/refractory disease, but is not considered as effective as open surgical treatment.
Correct Answer: open arthrotomy with synovectomy.
Question 16:
A nondisplaced fracture of the proximal medial femoral neck proximal to the lesser trochanter is noted at the time of insertion of a cementless tapered wedge-type femoral component in a total hip arthroplasty. Appropriate perioperative management should include which of the following?
Options:
- Cerclage cable placed proximal to the lesser trochanter with partial weight bearing for 6 weeks postoperatively
- No intraoperative or postoperative modifications are necessary
- Non-weight-bearing for 6 weeks, retention of the femoral component, and no cerclage wire
- Fracture exploration and repair with multiple cerclage cables, strut allograft and revision of the femoral component with a long-stemmed implant
- Revision with a cemented implant
Correct Answer: Cerclage cable placed proximal to the lesser trochanter with partial weight bearing for 6 weeks postoperatively
Explanation:
DISCUSSION: The fracture should be explored in its entirety. If it remains in the intertrochanteric region, a single cerclage cable passed above the lesser trochanter and tightened around the femoral component is appropriate. A more distal or displaced fracture should be repaired with cerclage cables and consideration for revision of the femoral component with a long-stemmed or cemented implant should be given.
REFERENCES: Sharkey PF, Hozack WJ, Booth RE, et al: Intraoperative femoral fractures in cementless total hip arthroplasty. Orthop Rev 1992;21:337-342.
Sharkey PF, Wolf LR, Hume EL, et al: Insertional femoral fracture: A biomechanical study of femoral component stability. Semin Arthroplasty 1990;1:91-94.
Figure 39a Figure 39b Figure 39c
Question 17:
Figures 28a through 28c show the MRI scans of a 30-year-old woman who weighs 290 lb and has low back and left leg pain. She also reports frequent urinary dribbling, which her gynecologist has advised her may be related to obesity. Examination will most likely reveal
Options:
- ipsilateral weakness of the tibialis anterior.
- ipsilateral weakness of the peroneus longus and brevis.
- ipsilateral weakness of the extensor hallucis longus.
- a positive Beevor’s sign.
- a positive ipsilateral Gaenslen’s sign.
Correct Answer: ipsilateral weakness of the tibialis anterior.
Explanation:
DISCUSSION: The patient will most likely exhibit ipsilateral weakness of the tibialis anterior. Gaenslen’s test is designed to detect sacroiliac inflammation as a source of low back pain. Beevor’s sign tests the innervation of the rectus abdominus and paraspinal musculature (L1 innervation). The extensor hallucis longus is predominantly innervated by L5. The peroneals are predominantly innervated by S1.
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Appleton, WI, Century-Crofts, 1976.
Hollinshead WH (ed): Anatomy for Surgeons: The Back and the Limbs, ed 3. Philadelphia, PA, Harper & Rowe, 1982.
Question 18:
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Options:
- immediate split-thickness skin grafting.
- immediate Xenograft application.
- a vacuum-assisted closure device.
- dressing changes with sulfasalazine cream.
- a cross-leg flap.
Correct Answer: a vacuum-assisted closure device.
Explanation:
DISCUSSION: With soft-tissue loss, local or free flap coverage may be necessary to treat exposed tendon and bone. However, a vacuum-assisted closure device is a good temporizing dressing. It prevents external contamination, reduces edema around the wound, increases oxygen tension in the wound, and promotes the formation of granulation tissue. The use of this negative pressure device has been described in both acute traumatic and in chronic wound scenarios. If sufficient granulation tissue forms, closure may be by split graft, avoiding a more complex coverage procedure. Immediate skin grafting over the exposed anterior tibial tendon and tibia would have a low likelihood of success. Dressing changes with sulfasalazine may be beneficial in a burn wound to assist with removal of skin slough; however, in a granulating wound, the material may be toxic to early epithelialization. Xenograft is a foreign body and should not be applied to an acute contaminated open wound. Historically, a cross-leg flap was a treatment alternative for lower extremity soft-tissue loss; however, its current applications are extremely limited.
REFERENCES: Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 2002;23:896-901.
Question 19:
Which of the following methods is considered effective in decreasing the dislocation rate following a total hip arthroplasty using a posterior approach to the hip?
Options:
- Use of a shorter neck length
- Use of a smaller diameter head with a skirted neck extension
- Reconstruction of the external rotators and capsular attachments during closure
- Placement of the acetabular component in 60 degrees of abduction as opposed to 45 degrees of abduction
- Placement of the acetabular component in neutral (0 degrees) anteversion as opposed to 15 to 20 degrees of anteversion
Correct Answer: Reconstruction of the external rotators and capsular attachments during closure
Explanation:
DISCUSSION: A total hip arthroplasty using the posterior approach has resulted in hip dislocation under certain circumstances. Reconstruction of the external rotator/capsular complex is recognized as a stability-enhancing mechanism for the posterior approach. During the procedure, the acetabular component should be placed in 15 to 20 degrees of anteversion and approximately 45 degrees of abduction. Relative retroversion is a risk factor for posterior dislocation. High abduction angles result in edge loading of the polyethylene and possible early failure, as well as an increased risk of dislocation. Smaller diameter heads and skirted neck extensions used together decrease the range of motion that is allowed before impingement occurs, and this can result in dislocation. Shorter neck lengths generally result in soft-tissue envelope laxity. If laxity occurs, increased offset, neck length, or both can improve stability.
REFERENCES: Pellicci PM, Bostrom M, Poss R: Posterior approach to total hip replacement using enhanced posterior soft tissue repair. Clin Orthop 1998;355:224-228.
Morrey BF: Difficult complications after hip joint replacement: Dislocation. Clin Orthop 1997;344:179-187.
Question 20:
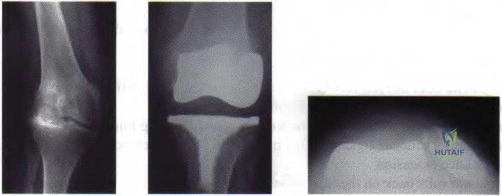
Figure 9 shows the AP radiograph of a 65-year-old man who has knee pain and swelling. What is the most likely diagnosis?
Options:
- Gout
- Chondrocalcinosis (pseudogout)
- Hemochromatosis
- Rheumatoid arthritis
- Ochronosis
Correct Answer: Chondrocalcinosis (pseudogout)
Explanation:
DISCUSSION: Although all the choices are known causes of joint degeneration (secondary osteoarthritis), only chondrocalcinosis shows distinct linear calcification of the cartilage due to deposition of calcium pyrophosphate crystals. Gout is a recurrent acute arthritis resulting from the deposition of monosodium urate from supersaturated hyperuricemic body fluids. Hemochromotosis is characterized by focal or generalized deposition of iron within body tissues. Arthritis may be present but is less common than other manifestations such as liver cirrhosis, skin pigmentation, diabetes mellitus, and cardiac disease. Rheumatoid arthritis is a nonspecific, usually symmetric inflammation of peripheral joints resulting in destruction of articular and periarticular structures. Ochronosis is a hereditary enzyme deficiency (homogentisic acid oxidase) resulting in deposition of homogentisic acid polymers in articular cartilage.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 188.
Berkow R (ed): The Merck Manual, ed 14. Rathway, NJ, Merck, 1984, pp 910, 1176, 1200.
Question 21:
During an anterior retroperitoneal approach to the low lumbar spine, the iliac vessels are mobilized along the lateral side, allowing them to be retracted toward the midline. To gain adequate mobility of the common iliac vein for exposure of L5, it is important to identify which of the following structures?
Options:
- Obturator artery
- Central sacral vessels
- Internal iliac vein
- Ascending lumbar vein
- Iliolumbar vein
Correct Answer: Iliolumbar vein
Explanation:
DISCUSSION: The iliolumbar vein is a large tributary that sits along the lateral surface of the common iliac vein. It can be quite substantial in size and must be identified prior to mobilizing the common iliac vein toward the midline. The other structures are not of surgical significance in performing this exposure.
REFERENCE: Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea & Febiger,
1918, 2000.
Question 22:
Figures 39a and 39b show the current radiographs of an 8-year-old girl who has had pain in the left thigh for the past 3 months. She was recently diagnosed with hypothyroidism and started treatment 1 week ago. Examination reveals a mild abductor deficiency limp on the left side. She lacks 30 degrees internal rotation on the left hip compared with the right hip. Management should consist of
Options:
- abductor muscle strengthening.
- a left 1-½ hip spica cast.
- closed reduction and pinning of the left hip.
- symptomatic treatment with crutch walking and nonsteroidal anti-inflammatory drugs.
- in situ pinning of both hips.
Correct Answer: in situ pinning of both hips.
Explanation:
DISCUSSION: The radiographs confirm a slipped capital femoral epiphysis of the left hip, as well as a widened growth plate on the contralateral hip. This is considered a stable slip because the patient is able to walk. Treatment options for stable slips include in situ pinning, bone graft epiphysiodesis, and in some centers severe slips are treated with primary osteotomy and epiphyseal fixation. Percutaneous in situ fixation is the most popular and widely used method of treatment. This juvenile patient has an endocrine condition and a widened growth plate on the right side; therefore, strong consideration should be given to pinning the contralateral hip
“pre-slip.” Muscle strengthening, hip spica casting, and closed reduction have no place in the primary treatment of a stable slipped capital femoral epiphysis.
REFERENCES: Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Loder R, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Aronson DD, Carlson WE: Slipped capital femoral epiphysis: A prospective study of fixation with a single screw. J Bone Joint Surg Am 1992;74:810-819.
Question 23:
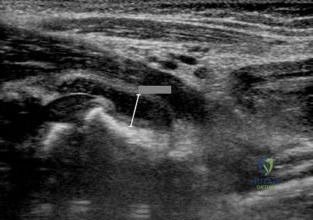
What structure is located at the tip of the arrow in Figure 18? Review Topic
Options:
- Left L3 nerve root
- Right L3 nerve root
- Right L4 segmental artery
- Right L4 nerve root
- Left lateral disk herniation
Correct Answer: Right L3 nerve root
Explanation:
The structure shown is the exiting nerve root at the L3-4 disk, which is the right L3 root.
Question 24:
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
Options:
- Posterior column/posterior wall acetabular
- Associated both column acetabular
- Transverse plus posterior wall acetabular
- Anterior column posterior hemitransverse acetabular
- Anterior column acetabular
Correct Answer: Anterior column acetabular
Explanation:
DISCUSSION: The radiographs and CT scans reveal an anterior column acetabular fracture. The fracture has quadrilateral plate extension but does not exit out the posterior column. The CT scans confirm an intact posterior column and no wall fracture. A transverse fracture is best seen on the CT scan and runs in the sagittal plane, not the coronal plane.
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 115-140.
Beaule PE, Dorey FJ, Matta JM: Letournel classification of acetabular fractures: Assessment of interobserver and intraobserver reliability. J Bone Joint Surg Am 2003;85:1704-1709.
Question 25:
In regards to a genetic disorder, which of the following is an example of "anticipation?"
Options:
- Gene characteristics more severe and earlier in onset in subsequent generations
- A disorder inherited from a genetic mutation specific to maternal DNA
- Gene characteristics expressed to varying degrees in different individuals
- Variation in the relative frequency of a genotype due to chance
- The presence of an extra copy of a chromosome
Correct Answer: Variation in the relative frequency of a genotype due to chance
Explanation:
Genetic anticipation is a phenomenon in which a genetic disorder becomes progressively more severe and earlier in onset with each generation. Examples of disorders exhibiting anticipation include Huntington's disease and myotonic dystrophy.
Genetic anticipation is an important concept in understanding the development and genetic implications of many heritable disorders. It is a common phenomenon in trinucleotide repeat expansion disorders. These disorders are due to unstable microsatellite trinucleotide repeats that expand beyond the normal threshold. In subsequent generations these expansions become longer and thus express disease characteristics at a younger age of onset, and often with greater severity.
Martorell et al. investigated the development of CTG trinucleotide repeats in patients with myotonic dystrophy type 1 (DM1) and their relatives. They discovered unaffected individuals carry a pre-mutation sequence which can lead to trinucleotide repeat expansion in subsequent generations and thus produce offspring with the disorder.
Kamsteeg et al. compare the characteristics of DM1 and DM2. Both are due to trinucleotide repeat expansions. However, while DM1 can present with earlier onset and increasing severity in each generation, DM2 does not exhibit this genetic anticipation.
Incorrect Answers
Question 26:
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Options:
- Distal portion of the extremity is free during exercise
- More commonly used in upper extremity exercise
- Predictable movement is produced by co-contraction of muscles
- Joint compression is decreased
- Usually involves a single joint
Correct Answer: Predictable movement is produced by co-contraction of muscles
Explanation:
DISCUSSION: Closed-chain exercise requires the distal portion of the extremity to be fixed. It is more commonly used in lower extremity exercise, and movement is produced by co-contraction of muscles. Joint compression is increased, and multiple joints are involved with closed-chain exercise. In open-chain exercise, the distal portion of the extremity is free.
REFERENCES: Braddom RL (ed): Physical Medicine and Rehabilitation, ed 2. Philadelphia, PA, Saunders, 2000, pp 975-976.
Childs DC, Irrang JJ: The language of exercise and rehabilitation, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 329.
Question 27:
Which of the following changes to heart rate, blood pressure, and bulbocavernosus reflex are typical of spinal shock?
Options:
- Tachycardia, hypertension, intact bulbocavernosus reflex
- Tachycardia, hypotension, intact bulbocavernosus reflex
- Tachycardia, hypotension, absent bulbocavernosus reflex
- Bradycardia, hypotension, absent bulbocavernosus reflex
- Bradycardia, hyperthermia, intact bulbocavernosus reflex
Correct Answer: Bradycardia, hypotension, absent bulbocavernosus reflex
Explanation:
DISCUSSION: The term ‘spinal shock’ applies to all phenomena surrounding physiologic or anatomic transection of the spinal cord that results in temporary loss or depression of all or most spinal reflex activity below the level of the injury. Hypotension and bradycardia caused by loss of sympathetic tone is a possible complication, depending on the level of the lesion. The mechanism of injury that causes spinal shock is usually traumatic in origin and occurs immediately, but spinal shock has been described with mechanisms of injury that progress over several hours. Spinal cord reflex arcs immediately above the level of injury also may be depressed severely on the basis of the Schiff-Sherrington phenomenon. The end of the spinal shock phase of spinal cord injury is signaled by the return of elicitable abnormal cutaneospinal or muscle spindle reflex arcs. Autonomic reflex arcs involving relay to secondary ganglionic neurons outside the spinal cord may be affected variably during spinal shock, and their return after spinal shock abates is variable. The returning spinal cord reflex arcs below the level of injury are irrevocably altered and are the substrate on which rehabilitation efforts are based.
REFERENCE: Ditunno JF, Little JW, Tessler A, et al: Spinal shock revisited: A four-phase model. Spinal Cord 2004;42:383-395.
Question 28:
Which of the following is considered the most appropriate shoe modification following transmetatarsal amputation?
Options:
- Foam filling of the forefoot void
- Custom last shoe of a smaller size
- Solid ankle polypropylene ankle-foot orthosis
- Silicone partial foot prosthesis with cosmetic toes
- Cushioned molded insole and toe filler over a carbon fiber footplate
Correct Answer: Cushioned molded insole and toe filler over a carbon fiber footplate
Explanation:
DISCUSSION: Most patients who undergo transmetatarsal amputation do not require custom shoe wear or an orthosis above the ankle. A molded toe filler is used to prevent excessive shear that can lead to ulceration. Use of a soft toe filler without stiffening of the sole results in excessive flexibility from the shortened lever arm, which reduces the efficiency of gait. A firm footplate or carbon fiber base adds rigidity to aid in push-off. A rocker bottom also may be added to the shoe.
REFERENCES: Philbin TM, Leyes M, Sferra JJ, Donley BG: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Marks RM: Mid-foot/mid-tarsus amputations. Foot Ankle Clin 1999;4:1-16.
Question 29:
Torsional moments about the longitudinal axis of a total hip arthroplasty show what change during stair climbing compared with walking?
Options:
- Increase by a factor of 50% during stair climbing
- Increase by a factor of 100% during stair climbing
- Increase only during the first 6 to 8 weeks following implantation, then revert to normal
- Decrease by a factor of 50% during stair descent
- Decrease by a factor of 100% during stair descent
Correct Answer: Increase by a factor of 100% during stair climbing
Explanation:
DISCUSSION: The magnitudes of out-of-plane loads on a total hip replacement during activities of daily living can be substantial. Bergmann and associates studied these forces about two instrumented hip prostheses. They noted that the torsional moment about the hip during stair climbing is twice as high as during slow walking and that similar moments are generated during slow jogging. Higher loads were noted when the patients stumbled without falling. They also noted that the torsional moments observed in vivo were close to or even exceeded the experimentally determined limits of the torsional strength of implant fixations.
REFERENCES: Hurwitz DE, Andriacchi TP: Biomechanics of the hip, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott Raven, 1998, pp 75-85.
Bergmann G, Graichen F, Rohlmann A: Is staircase walking a risk for the fixation of hip implants? J Biomech 1995;28:535-553.
Question 30:
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Options:
- Physical therapy
- Arthroscopic synovectomy
- Tibial insert revision
- Femoral component revision
Correct Answer: Arthroscopic synovectomy
Explanation:
DISCUSSION:
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful total knee arthroplasty.
Question 31:
Figure 61 shows the radiograph of a 28-year-old professional football player who sustained a hyperextension injury to the great toe. He continued to play with pain and loss of push-off strength. What is the most likely diagnosis?
Options:
- Hallux rigidus
- Fracture of the sesamoid
- Disruption of the plantar plate
- Osteonecrosis of the metatarsal head
- Rupture of the flexor hallucis longus
Correct Answer: Disruption of the plantar plate
Explanation:
Upon review of the radiograph give, there is no evidence of fracture or osteonecrosis. Upon review of the article above the most likely diagnosis is “Turf-Toe” or the disruption of the plantar plate. The patient has mechanism of injury, hyperextension and sequelae, decreased push-off strength, which is consistent with this diagnosis. Rupture of the FHL would most likely result in inability to continue playing while hallux rigidus is a potential chronic sequelae with associated dorsal osteophyte formation.
Question 32:
A 55-year-old patient is seeking a surgical consultation for a painful flatfoot deformity that has failed to respond to nonsteroidal anti-inflammatory drugs, shoe and activity modifications, and orthoses. The patient is of medium build, a nonsmoker, and has no history of diabetes mellitus. Radiographs are shown in Figures 43a through 43c. Based on these findings, treatment should consist of
Options:
- triple arthrodesis.
- lateral column lengthening with flexor digitorum longus tendon transfer.
- medial calcaneal displacement osteotomy, flexor digitorum longus transfer, and gastrocnemius recession.
- midfoot arthrodesis.
- subtalar arthroereisis with a Maxwell-Brancheau Arthroereisis titanium implant.
Correct Answer: midfoot arthrodesis.
Explanation:
DISCUSSION: The patient has a degenerative collapse of the midfoot through the tarsometatarsal joints with significant forefoot abduction; therefore, a midfoot arthrodesis is required to address the arthritic joints and deformity at the tarsometatarsal articulation. All of the other procedures correct hindfoot deformities and therefore would not be appropriate treatment.
REFERENCES: Brage M: Degenerative joint disease of the midfoot. Foot Ankle Clin 1999;4:355-367.
Mann RA, Prieskorn D, Sobel M: Mid-tarsal and tarsometatarsal arthrodesis for primary degenerative osteoarthrosis or osteoarthrosis after trauma. J Bone Joint Surg Am
1996;78:1376-1385.
Question 33:
A 7-year-old girl sustains the fracture shown in Figure 29a. Casting results in uneventful healing. Ten months later, the patient has a progressive valgus deformity of the right lower extremity. A radiograph is shown in Figure 29b. Management should now consist of
Options:
- observation.
- proximal tibial osteotomy.
- proximal tibial hemiepiphyseodesis.
- a long leg brace with a varus-producing strap.
- MRI to map the extent of the osseous physeal bridge.
Correct Answer: observation.
Explanation:
DISCUSSION: Although fractures of the proximal tibial metaphysis in young children appear innocuous, development of a progressive valgus deformity is possible despite adequate and appropriate treatment. When treating a child with this injury, it is prudent to warn the parents that a valgus deformity of the tibia may develop. The most likely cause is asymmetric growth of the proximal tibial physis. Because spontaneous angular improvement can be expected in most patients, surgery to correct these deformities should be delayed at least 2 to 3 years and should be limited to patients who have symptoms. There are no studies that document the efficacy of bracing for this deformity.
REFERENCES: Tuten HR, Keeler KA, Gabos PG, et al: Posttraumatic tibia valga in children: A long-term follow-up note. J Bone Joint Surg Am 1999;81:799-810.
McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 34:
A patient sustains a transection of the posterior cord of the brachial plexus from a knife injury. This injury would affect all of the following muscles EXCEPT?
Options:
- Subscapularis
- Latissimus dorsi
- Supraspinatus
- Teres minor
- Brachioradialis
Correct Answer: Subscapularis
Explanation:
DISCUSSION: The posterior cord of the brachial plexus gives rise to the 1) upper subscapular nerve 2) lower subscapular nerve 3) thoracodorsal nerve 4) axillary nerves 5) radial nerve. The upper subscapular nerve innervates the subscapularis. The lower subscapular nerve innervates teres major and also subscapularis. The thoracodorsal nerve innervates latissimus dorsi. The axillary nerves innervates deltoid and teres minor. The radial nerve innervates the triceps, brachioradialis, wrist extensors, and finger extensors. The supraspinatus is innervated by the suprascapular nerve off the upper trunk and therefore would not be affected by an injury to the posterior cord. The anatomy of the brachial plexus is shown in Illustration A.
Question 35:
A 35-year-old man who snowboards sustained the injury shown in Figures 4a through 4c. What is the mechanism of injury?
Options:
- Inversion and external rotation
- Axial loading and internal rotation
- Plantar flexion, axial loading, and inversion
- Dorsiflexion and axial loading
- Dorsiflexion, axial loading, inversion, and external rotation
Correct Answer: Dorsiflexion, axial loading, inversion, and external rotation
Explanation:
DISCUSSION: Fractures of the lateral process of the talus in snowboarders have been thought to result from pure dorsiflexion, inversion, and axial loading. In a cadaveric study, 10 cadavers were placed in fixed dorsiflexion and inversion with an axial load. This was combined with or without external rotation. No fractures occurred after axial loading in the dorsiflexed-inverted position. Fractures of the lateral process of the talus occurred in 75% of the specimens with the addition of external rotation.
REFERENCES: Boon AJ, Smith J, Zobitz ME, et al: Snowboarder’s talus fracture: Mechanism of injury. Am J Sports Med 2001;29:333-338.
Kirkpatrick DP, Hunter RE, Janes PC, et al: The snowboarder’s foot and ankle. Am J Sports Med 1998;26:271-277.
Question 36:
What arterial vessel is most prone to injury during posterior iliac crest bone graft harvest?
Options:
- Superior gluteal
- Deep circumflex iliac
- Iliolumbar
- Ascending branch of the lateral femoral circumflex
- Fourth lumbar
Correct Answer: Superior gluteal
Explanation:
DISCUSSION: The superior gluteal artery is most at risk with a posterior iliac crest bone graft harvest. The artery leaves the pelvis through the sciatic notch and can be injured by retractors or other sharp instruments entering the sciatic notch area. The deep circumflex iliac, iliolumbar, and fourth lumbar arteries supply the iliacus and iliopsoas muscles and can be damaged during anterior bone graft harvest. The ascending branch of the lateral femoral circumflex artery is at risk during the anterior approach to the hip.
REFERENCES: Guyer RD, Delmarter RB, Fulp T, Small SD: Complications of cervical spine surgery, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 547.
Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 330-331.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 297, 331-332.
Question 37:
A 62-year-old woman reports diffuse aches and pains of the hip and pelvis. She denies any significant trauma but does have a history of chronic anemia. Figure 17a shows a radiograph of the pelvis, and Figures 17b and 17c show T 2 -weighted MRI scans. What is the most likely diagnosis?
Options:
- Chondrosarcoma
- Diffuse fibrous dysplasia
- Multiple myeloma
- Osteoporosis
- Bone infarcts
Correct Answer: Multiple myeloma
Explanation:
DISCUSSION: The radiograph reveals diffuse osteopenia and areas in the proximal femora that are moth-eaten in appearance. The extent of the marrow-replacing process is evident on the MRI scans, which reveal signal abnormality throughout the entire pelvis and both proximal femora. This represents a marrow-packing process, of which multiple myeloma is the best choice. This diagnosis is also supported by the anemia noted on the patient’s history. Metastatic carcinoma and lymphoma also may have a similar presentation.
REFERENCE: Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA,
WB Saunders, 2002, pp 2189-2216.
Question 38:
A 36-year-old man has a moderate-sized left paracentral L5-S1 disk herniation with compression of the S1 nerve. Examination will most likely reveal sensory changes at what location?
Options:
- Anterior thigh stopping at the knee
- Lateral border of the foot
- Dorsum of the foot and the great toe
- Medial side of the leg
- Perianal region
Correct Answer: Lateral border of the foot
Explanation:
DISCUSSION: Because the left paracentral L5-S1 disk herniation is compressing the left S1 nerve root, the patient will have numbness along the lateral border and plantar surface of the foot. Numbness along the anterior thigh stopping at the knee is consistent with an L3 radiculopathy. Sensory changes at the dorsum of the foot and great toe normally signify an L5 distribution; the medial leg signifies an L4 distribution. Perianal numbness involves the S2-S5 nerve roots.
REFERENCES: Wisneski RJ, Garfin SR, Rothman RH, Lutz GE: Lumbar disk disease, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman and Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, vol 1, pp 629-634.
Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton- Century-Crofts, 1976, pp 249-254.
Question 39:
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Options:
- Weakness of the left extensor hallucis longus and a sensory deficit in the first dorsal web space
- Diminished right Achilles tendon reflex and weakness of the gastrocnemius-soleus complex
- Pain radiating into the anteromedial aspect of the left knee, diminished patellar tendon reflex, and difficulty climbing stairs
- Numbness in the right first dorsal web space and a slap foot gait
- Urinary retention and right quadriceps weakness with diminished patellar tendon reflex
Correct Answer: Pain radiating into the anteromedial aspect of the left knee, diminished patellar tendon reflex, and difficulty climbing stairs
Explanation:
DISCUSSION: The MRI scan shows a far lateral disk herniation. With the L4-5 disk, a far lateral herniation abuts the left L4 nerve root. The findings would be consistent with those of a left L4 radiculopathy and would include pain or a sensory deficit on the anteromedial aspect of the knee, diminished patellar tendon reflex, and quadriceps weakness, perhaps making it difficult to walk up and down stairs.
REFERENCES: Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
O’Hara LJ, Marshall RW: Far lateral lumbar disc herniation: The key to the intertransverse approach. J Bone Joint Surg Br 1997;79:943-947.
Question 40:
The patient is planning on having his contralateral knee replaced as well. He has a mild valgus deformity in his left knee with an overall windswept deformity. Which release is most appropriate in this case if the knee remains tight in extension?
Options:
- Semimembranosis release
- Medial gastrocnemius release
- Medial tibial plateau downsizing osteotomy
- Iliotibial band pie crusting
- Popliteus tendon release
- Cruciate release of the capsule posterior lateral corner
Correct Answer: Iliotibial band pie crusting
Explanation:
DISCUSSION
Balancing a total knee is important for longevity of the device and functional benefit. The surgeon should be systematic in the release of a varus knee. The deep MCL is typically released as part of the approach and osteophytes are then removed. The semimembranosus tendon can then be released from the posterior medial aspect of the tibia. A downsizing osteotomy can be considered for a large deformity if a patient has adequate tibial sizing. If a patient has the smallest implant available prior to the osteotomy, an osteotomy will lead to overhang of the implant and medial impingement on the MCL.
A valgus knee can be treated with pie crusting of the iliotibial band in mild extension deformity. Surgeons should pause prior to taking down the popliteus and lateral collateral
ligament because this can induce posterior rotatory subluxation of a primary knee, especially in the case of a posterior collateral ligament-sacrificing total knee arthroplasty design.
Question 41:
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?
Options:
- 2 cm distal to the articular surface of the radial head
- 1 cm distal to the articular surface of the radial head
- Within a 90-degree arc or safe zone
- Within a 120-degree arc or safe zone
- Within a 180-degree arc or safe zone
Correct Answer: Within a 90-degree arc or safe zone
Explanation:
DISCUSSION: The radial head is covered by cartilage on 360 degrees of its circumference. However, with the normal range of forearm rotation of 160 to 180 degrees, there is a consistent area that is nonarticulating. This area is found by palpation of the radial styloid and Lister’s tubercle. The hardware should be kept within a 90-degree arc on the radial head subtended by these two structures.
REFERENCES: Smith GR, Hotchkiss RN: Radial head and neck fractures: Anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg 1996;5:113-117.
Caputo AE, Mazzocca AD, Santoro VM: The nonarticulating portion of the radial head: Anatomic and clinical correlations for internal fixation. J Hand Surg Am 1998;23:1082-1090.
Question 42:
A 24-year-old dancer reports posterior ankle pain when in the “en pointe” position. Examination reveals posteromedial tenderness, no pain reproduction with passive forced planter flexion, and pain with motion of the hallux. What is the most likely diagnosis?
Options:
- Painful os trigonum
- Posterior ankle soft-tissue impingement
- Stricture in the knot of Henry
- Flexor digitorum longus tendinitis
- Flexor hallucis longus tendinitis
Correct Answer: Flexor hallucis longus tendinitis
Explanation:
DISCUSSION: Flexor hallucis longus tendinitis is a common cause of posterior ankle pain in dancers. It tends to be more posteromedial and is characterized by a clicking or catching sensation posteromedially with motion of the great toe. A painful os trigonum typically causes more posterolateral ankle pain and may occur after an ankle sprain or plantar flexion injury where there may be a fracture of the os trigonum.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 249-261.
Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
Question 43:
03 Which of the following findings is the best indication for the use of temporary external fixation of a femoral shaft fracture?
Options:
- Type IIIA open fracture
- back to this question next question
- Hemodynamic instability
- Segmental fracture
- Distal one third fracture
- Ipsilateral tibial shaft fracture 33.03
Correct Answer: back to this question next question
Explanation:
These days, femoral shaft fractures at Tulane / Charity are commonly encountered by orthopaedic residents on the night-float team.
Despite the presence of a well-rested 4th year surgeon, definitive orthopaedic fixation is not always the correct answer for each trauma patient.
Tulane defines “Orthopaedic Tunnel Vision” as a condition commonly associated with a young MD at the Bulldog without a proper
wing-man, trying to make advances on the wrong patron due to his relatively easy 80-hour work week schedule and a few too many refined hops.
Skeletal Trauma (p. 1967) describes “Orthopaedic Tunnel Vision” as looking at the orthopaedic injury without considering the
patient’s injury in general. Femoral shaft fractures are typically high energy injuries which often do not occur in isolation. In these fractures, it is particularly important to not have tunnel vision.
Indications for temporary bridging external fixation includes hemodynamic instability
(ans. 2), acidosis, hypothermjia, hypoxemia, coagulopathy, sepsis or severely contaminated soft tissues that cannot be adequately debrided. Definitive fixation is performed after the general surgical and medical issues have resolved.
The other answer choices, including the type IIIA open fracture are not contraindications to definitive fixation in themselves (typically IM nailing—antegrade or retrograde).
Question 44:
Figure 43 shows an arthroscopic view of a right shoulder through a lateral portal in the beach chair position. The arrow is pointing to what structure?
Options:
- Biceps tendon
- Coracohumeral ligament
- Superior glenohumeral ligament
- Middle glenohumeral ligament
- Inferior glenohumeral ligament
Correct Answer: Biceps tendon
Explanation:
DISCUSSION: This view from the lateral portal shows a full-thickness rotator cuff tear. The glenohumeral joint can be visualized through this tear. The glenoid, labrum, and biceps tendon attaching to the superior aspect of the glenoid are easily viewed from this portal, and the arrow is pointing to the biceps tendon. Arthroscopic rotator cuff repair can be performed while visualizing from this portal and using anterior and posterior working portals.
REFERENCES: Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principles of techniques, in McGinty JB (ed): Operative Arthroscopy,
ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Burkhart, SS: Arthroscopic management of rotator cuff tears, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 508-546.
Question 45:
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?
Options:
- Osteopenia
- Excessive anteversion
- Excessive varus
- Excessive bowing
- Stove-pipe femur
Correct Answer: Excessive anteversion
Explanation:
DISCUSSION: Developmental dysplasia of the hip (DDH) leads to early arthritis of the hip as seen in this patient. Although DDH is believed to mostly affect the acetabulum, most patients with DDH also have anatomic aberrations of the femur. Using three-dimensional computer models generated by reconstruction of CT scans, dysplastic femurs were shown to have shorter necks and smaller, straighter canals than the controls. The shape of the canal became more abnormal with increasing subluxation. The studies also have shown that the primary deformity of the dysplastic femur is rotational, with an increase in anteversion of 5 degrees to 16 degrees, depending on the degree of subluxation of the hip. The rotational deformity of the dysplastic femur arises within the diaphysis between the lesser trochanter and the isthmus and is not attributable to a torsional deformity of the metaphysis. Osteopenia is not a concern in a patient with an excellent cortical index (thick cortices and narrow canal). Femoral varus or bowing of the femur is not a typical finding in patients with DDH.
REFERENCES: Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
Sugano N, Noble PC, Kamaric E, et al: The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-719.
Question 46:
Following total knee arthroplasty, a patient is noted to have asymmetrical absent pulses and poor capillary refill. What is the next most appropriate step in management?
Options:
- Observation of the limb for 4 hours to see if the arterial spasm resolves
- Measurement of lower leg compartment pressures
- Magnetic resonance angiogram
- Emergent return to the operating room for wound exploration while the patient anesthesia
- Return to the operating room, obtain a vascular surgery consultation, and intraoperative arteriogram
Correct Answer: Return to the operating room, obtain a vascular surgery consultation, and intraoperative arteriogram
Explanation:
is still under
perform an
DISCUSSION: An assessment of the location of the vascular compromise is necessary prior to surgical exploration. Vascular repair will most likely require a separate surgical exposure. Vascular reperfusion may be accomplished at the time of an arteriogram with the use of a stent in certain situations. Return to the operating room with vascular surgical consultation and intraoperative arteriogram is appropriate.
An immediate postoperative compartment syndrome is unlikely. Magnetic resonance angiogram is not appropriate because of the potential for a delay in diagnosis.
REFERENCE: Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001 ;9;253-257.
Question 47:
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
Options:
- Valgus extension overload
- Varus posteromedial rotatory instability (VPMRI)
- Valgus posterolateral rotatory instability (VPLRI)
- Olecranon bursitis The patient has valgus extension overload. This is a spectrum of pathologies, often seen in pitchers, that begins with posteromedial impingement between the medial olecranon and posterior trochlea during forceful elbow extension. As a result, a medial olecranon osteophyte is typically the first notable imaging finding. As pathology increases, there can be progressive damage to the medial collateral ligament (MCL), degeneration of the radiocapitellar articulation, and neuritis of the ulnar nerve. VPMRI is often associated with a large anteromedial coronoid fracture and posterior band MCL rupture. VPLRI occurs when the lateral collateral ligament complex is ruptured. Olecranon bursitis presents with focal swelling or a fluid collection over the posterior aspect of the olecranon.
Correct Answer: Valgus extension overload
Explanation:
A patient sustains a displaced diaphyseal humerus fracture following a motor vehicle accident. Open reduction internal fixation is indicated due to concomitant lower extremity trauma and is planned through an anterior approach. Which intramuscular interval is exploited during the deep dissection of the mid-humerus in this approach?
A. Lateral head of triceps (radial nerve) and brachialis (musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii (musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis (musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis (musculocutaneous nerve)
Question 48:
A 34-year-old male presents with elbow pain after sustaining a ground level fall 2 weeks ago. An injury radiograph is shown in Figure
Options:
- Which of the following provocative maneuvers will most likely be positive?
- Lateral pivot shift test
- Milking maneuver
- Chair rise test
- Posterior drawer test
- Gravity-assisted varus stress test Corrent answer: 5 Figure A demonstrates a fracture of the anteromedial coronoid. Patients with this injury pattern will have feelings of instability with the gravity-assisted varus stress test. Varus posteromedial rotatory instability (VPMRI) of the elbow is caused by a varus and posteromedial rotation force, resulting in rupture of the lateral collateral ligament (LCL) from its humeral origin. The medial coronoid process is subsequently forced against the medial trochlea, which results in fracture of the anteromedial portion. The most sensitive test is the gravity-assisted varus stress test. The arm is abducted to 90° and the patient is asked to flex and extend the elbow. The test is positive for pain, grinding, or instability during range of motion, as the ulnohumeral joint is closed medially by the lack of the buttress from the anteromedial coronoid. Treatment involves surgically addressing the anteromedial facet of the coronoid and repairing the LCL. Steinmann performed a review of coronoid process fractures. He reports that with an anteromedial coronoid fracture, the anteroposterior (AP) radiograph of the elbow will demonstrate progressive narrowing of the joint space from lateral to medial. They conclude that an important determinant of stability is the involvement of the sublime tubercle (insertion point of the MCL). When the sublime tubercle is involved, medial elbow instability is likely. Doornberg et al. performed a retrospective review of coronoid fracture patterns. They found that large fractures of the coronoid were involved with anterior and posterior olecranon fracture/dislocations, small transverse fractures were involved with terrible triad injuries, and anteromedial facet fractures were associated with VPMRI. Doornberg et al. performed a retrospective review of patients with fracture of the anteromedial facet of the coronoid. They report that if the fracture is not specifically treated, patients ultimately developed arthrosis. They report that the coronoid fracture may be secured with a plate, screw, or sutures. They conclude that secure fixation of the coronoid usually restores good elbow function. Figure A is an AP radiograph of the elbow demonstrating a fracture of the anteromedial facet of the coronoid. Illustration A is a fluoroscopic stress view demonstrating ulnohumeral instability due to an associated LCL injury. Illustration B is an AP radiograph demonstrating plate and screw fixation of the coronoid and suture anchor repair of the LCL. Incorrect Answers:
Correct Answer: Chair rise test
Explanation:
positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
OrthoCash 2020
Question 49:
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury? Review Topic
Options:
- C5 root
- C6 root
- Internal carotid artery
- Vertebral artery
- Vagus nerve
Correct Answer: C5 root
Explanation:
The vertebral artery is contained within the vertebral foramen and thus tethered alongside the vertebral body, making it vulnerable to injury if a drill penetrates the lateral wall. The C5 root passes over the C5 pedicle and is not in the vicinity. The C6 root passes under the C5 pedicle but is posterior to the vertebral artery and is only vulnerable at the very posterior-inferior corner. The carotid artery and the vagus nerve are both within the carotid sheath and well anterior.
(SBQ12SP.54) Integrity of the posterior ligamentous complex (PLC) is a critical predictor of spinal fracture stability. Components of the PLC include the supraspinous ligament, interspinous ligament, ligamentum flavum and:
Review Topic
Facet joint capsules
Facet joint capsules, and facet joints
Facet joint capsules, facet joints, and the posterior longitudinal ligament
Facet joint capsules, and the posterior longitudinal ligament
Posterior longitudinal ligament
Components of the PLC include the supraspinous ligament, interspinous ligament, ligamentum flavum and facet joint capsules.
Numerous methods have been used to evaluate for PLC injury. Palpation is unreliable and has low accuracy. Radiographs can show characteristic flexion-distraction fracture patterns with widening or malaligment of the spinous processes. Computed tomography (CT) is more reliable than radiographs to provide indirect evidence of ligament injury. Magnetic resonance image (MRI) can provide direct evidence of soft-tissue injury, making it the preferred method in diagnosing ligamentous injury. However, MRI may not always be utilized due to situations involving emergency operations or contraindications to MRI, such as certain metal implants.
Vaccaro et al. introduced a new classification system for thoracolumbar injuries, TLICS, based on morphological appearance, integrity of the posterior ligamentous complex, and neurological status. They advocate use of the system for nonoperative versus operative decision making and communication between surgeons.
Varccaro et al. sought to determine the accuracy of magnetic resonance imaging (MRI) in diagnosing injury of the posterior ligamentous complex (PLC) in patients with thoracolumbar trauma. Forty-two patients with 62 levels of injury were studied. The sensitivity for the various PLC components ranged from 79% (left facet capsule) to 90% (interspinous ligament). The specificity ranged from 53% (thoracolumbar fascia) to 65% (ligamentum flavum). They concluded that the integrity of the PLC as determined by MRI should not be used in isolation to determine treatment.
Incorrect Answers:
Question 50:
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement? Review Topic
Options:
- Arthroscopic debridement
- Arthroscopic rotator cuff repair
- Hemiarthroplasty with rotator cuff repair
- Total shoulder arthroplasty
- Reverse shoulder arthroplasty
Correct Answer: Reverse shoulder arthroplasty
Explanation:
The patient has end-stage rotator cuff tear arthropathy. The radiograph shows complete proximal humeral migration (acromiohumeral interval of 0 mm), severe glenohumeral arthritis, and acetabularization of the acromion. In addition, she has "pseudoparalysis" with active elevation of only 30 degrees. Reverse shoulder arthroplasty affords her the best opportunity for pain relief and functional improvement. The other procedures have mixed results but typically are better for pain relief than they are for functional gains.
Question 51:
Which treatment of the current fracture will provide the best long-term outcome?
Options:
- Casting it in its current position, which is acceptable alignment
- Closed reduction and casting
- Functional brace because this is a stable fracture
- Open reduction with revision of the current implants
Correct Answer: Open reduction with revision of the current implants
Explanation:
DISCUSSION
Many patients with mild dominant OI (the most common type) appear “normal,” and a diagnosis cannot be made without a careful personal history, family history, and observance of blue sclera. More than 3 fractures during childhood places someone outside of the mean and should merit further investigation. There is no sign of rickets on this radiograph (physeal widening/cupping). Similarly, the history and examination finding of blue sclera in the patient and his mother should raise concern for OI. Many parents of children with OI have inappropriately been accused of abuse despite obvious examination, radiograph, and family history findings that suggest OI. Low-energy mechanisms that create displaced fractures are a hallmark of OI and do not in isolation raise suspicion for nonaccidental trauma.
Based on the history and examination, mild-form OI caused by a defect in the type I collagen gene is most likely. Defects in type II collagen genes affect articular cartilage and cause epiphyseal dysplasia. Defects in the LEPRE cause severe-form OI involving clinically bowed limbs, marked short stature, and white sclera. There is no sign on radiographs of rickets, so severe vitamin D deficiency is not present. The history, examination, and radiographs all point toward OI/osteoporosis rather than nonaccidental trauma.
Peri-implant fractures occur because of a difference in elasticity between the bone with implants and the bone adjacent to it without implants. This is particularly important in the setting of osteoporotic bone in which the difference in elasticity and rigidity will be much more pronounced than in normal bone. Load-sharing implants are preferred when possible. The original fracture occurred proximal to the current fracture in the middle of the plated bone and looks healed with no sign of infection.
This fracture is in unacceptable alignment with subluxation of the radiocapitellar joint. The plates are bent, so closed reduction will not solve the alignment problem. In early childhood, load-sharing implants (flexible rods or wires) should be used to solve the elasticity mismatch that contributed to the current fracture.
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a through 51c are the radiographs of an 8-year-old boy with a shoulder deformity and limited cervical range of motion. He has no significant medical problems and plays baseball, pitching with his right arm. His active shoulder abduction is 180 degrees on the left and 150 degrees on the right.
Question 52:
A 27-year-old man sustains a displaced femoral neck fracture and undergoes urgent open reduction internal fixation. What is the most prevalent complication after this injury?
Options:
- Flexion contracture
- Hip instability
- Nonunion
- Abductor lurch
- Osteonecrosis
Correct Answer: Flexion contracture
Explanation:
DISCUSSION: Femoral neck fractures in young patients are difficult to treat, and AVN is a significant concern. Despite advances in both imaging and implants, this injury often leads to functional impairment.
Haidukewych et al followed treatment of femoral neck fractures in young patients. They found almost 10% of displaced fractures were associated with the development of nonunion, where as 27% were associated with the development of osteonecrosis. Their results were influenced by fracture displacement and the quality of reduction. Varus malreduction most closely correlates with failure of fixation after reduction and cannulated screw fixation.
Swiontkowski reviews both the treatment and post operative complications in intracapsular hip fractures. In this Current Concept Review, the rate of AVN was discussed as being related to the pre-operative degree of displacement seen on radiographs.
Incorrect Responses:
Question 53:
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?
Options:
- Interphalangeal joint fusion
- Intercalary tendon graft
- Silicone rod placement
- Primary flexor pollicis longus repair
- Flexor digitorum superficialis transfer
Correct Answer: Flexor digitorum superficialis transfer
Explanation:
DISCUSSION: The patient has a chronic flexor tendon laceration. There are options to restore motion and strength; therefore, fusion is not necessary. Full range of motion is present so the soft tissues are suitable for a tendon transfer. A transfer of the flexor digitorum superficialis of the ring finger to the insertion of the flexor pollicis longus on the distal phalanx provides good results with a one-stage operation.
REFERENCES: Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Posner MA: Flexor superficialis tendon transfers to the thumb: An alternative to the free tendon graft for treatment of chronic injuries within the digital sheath. J Hand Surg Am 1983;8:876-881.
Question 54:
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Options:
- use of an electrical bone stimulation unit.
- open reduction and internal fixation with a dynamic compression plate placed superiorly and autogenous bone grafting.
- open reduction and internal fixation with a dynamic compression plate placed inferiorly and autogenous bone grafting.
- intramedullary screw fixation.
- partial claviculectomy.
Correct Answer: open reduction and internal fixation with a dynamic compression plate placed superiorly and autogenous bone grafting.
Explanation:
DISCUSSION: The patient has a symptomatic painful atrophic midclavicular nonunion, and the treatment of choice is rigid internal fixation with a dynamic compression plate and autogenous bone grafting. A tension band effect is desired and achieved by placing the plate superiorly. Excellent success rates of 90% to 100% have been reported using this technique. Intramedullary screw fixation without bone grafting has a decreased success rate. Partial claviculectomy is not a preferred option.
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 55:
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient?
Options:
- Radial collateral ligament
- Posterior bundle of the ulnar collateral ligament
- Anterior bundle of the ulnar collateral ligament
- Flexor carpi ulnaris
- Pronation teres
Correct Answer: Anterior bundle of the ulnar collateral ligament
Explanation:
DISCUSSION: The anterior bundle of the ulnar collateral ligament of the elbow is the primary constraint to valgus force of the elbow. In pitchers and in overhead athletes, injury to this portion of the ligament results in valgus instability. Reconstruction of the anterior band of the ulnar collateral ligament is necessary in many elite athletic throwers to allow them to return to this competitive activity.
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Cain EL, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.
Rettig AC, Sherrill C, Snead DS, et al: Nonoperative treatment of ulnar collateral ligament injuries in
throwing athletes. Am J Sports Med 2001 ;29:15-17.
/
Figure 55a Question 55
A 22-year-old male basketball player has had knee pain for the past 3 months. He denies any history of trauma. He has symptoms of catching but no locking. He has rested for 2 weeks but symptoms returned when he resumed sporting activities. T
r
and T
2
-weighted MRI scans are shown in Figures 55a and 55b. What is the most likely diagnosis?
Locked lateral meniscus tear
Anterior cruciate ligament tear
Ganglion cyst of the anterior cruciate ligament
Synovial osteochondromatosis
Pigmented villonodular synovitis PREFERRED RESPONSE: 3
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T
2
sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.
Question 56:
In a statement put forth by AAOS, the role of the orthopaedic surgeon in the face of domestic and family abuse includes all of the following EXCEPT: Review Topic
Options:
- Be aware that he or she may be the first physician to be caring for the victims
- Ensure that they maintain comprehensive and accurate medical records documenting the events and examinations
- Care should resume once the patient's social situation is evaluated and assessed
- Transfer an elderly victim who is in immediate danger to a hospital emergency department and notify the emergency department physician of the transfer and the reasons for your concern
- Advocate for appropriate legislation and public policy
Correct Answer: Be aware that he or she may be the first physician to be caring for the victims
Explanation:
Regardless of the social situation, the orthopaedic surgeon's primary role is to proceed and offer expeditious and appropriate care for the patient's injuries.
The statement put forth by the AAOS implores the orthopaedic surgeon to be aware of the integral components to identify, document, and care for minors, elders, and/or partners who are victims of domestic abuse.
Zilmer et al. in a JAAOS review and the basis for the AAOS statement emphasizes the ability to identify abuse, which includes, but is not limited to frequent/multiple injuries, temporal abnormalities in multiple injuries, frequent visits/utilization of the emergency department, and/or unusual injuries/fracture patterns not consistent with the clinical picture. Meticulous documentation is of paramount importance, in addition to communicating your concerns to the appropriate emergency department personnel.
Incorrect answers:
Question 57:
A 71-year-old man has worsening left hip pain and is indicated for a left total hip arthroplasty (THA). Figure 1 shows a preoperative plan for the patient. The patient is scheduled for a left THA using a direct anterior approach with the pictured implants. If this plan is followed as pictured, what is the likely outcome for this patient? Figure could not be loaded
Options:
- Successful THA with significant shortening of the operative limb
- Compromised THA with a high likelihood of persistent trochanteric bursitis
- Successful THA with significant lengthening of the operative limb
- Compromised THA with a Trendelenburg gait and hip instability The focus should be on the pictured plan. This shows a medialized cup and a stem that has insufficient offset (distance between the center of rotation and a line down the center of the femoral shaft) to recreate the patient’s anatomy. The cup sets the hip center of rotation (dot in the middle of the cup), and the femoral head reduces to this point. In this patient, inadequate offset could lead to a decrease in abductor efficiency and a Trendelenburg gait and even worse dislocation due to component impingement and/or muscular insufficiency. Compromised THA with a high likelihood of persistent trochanteric bursitis would be accurate if too much offset was restored for the patient. Regarding limb lengths, it appears the height of the implant is sufficient and as it stands would likely not change the leg lengths much at all. The concepts of limb length and offset restoration are critical to performing a successful THA and limiting adverse events and poor outcomes from an acquired limb length discrepancy, limb instability or persistent trochanteric bursitis.
Correct Answer: Compromised THA with a Trendelenburg gait and hip instability The focus should be on the pictured plan. This shows a medialized cup and a stem that has insufficient offset (distance between the center of rotation and a line down the center of the femoral shaft) to recreate the patient’s anatomy. The cup sets the hip center of rotation (dot in the middle of the cup), and the femoral head reduces to this point. In this patient, inadequate offset could lead to a decrease in abductor efficiency and a Trendelenburg gait and even worse dislocation due to component impingement and/or muscular insufficiency. Compromised THA with a high likelihood of persistent trochanteric bursitis would be accurate if too much offset was restored for the patient. Regarding limb lengths, it appears the height of the implant is sufficient and as it stands would likely not change the leg lengths much at all. The concepts of limb length and offset restoration are critical to performing a successful THA and limiting adverse events and poor outcomes from an acquired limb length discrepancy, limb instability or persistent trochanteric bursitis.
Explanation:
Figure 1 is the radiograph of a 73-year-old woman who had a right hip arthroplasty one year prior. Her BMI is 48. Postoperative radiographs at 6 weeks showed early stem subsidence of 4 mm compared with intraoperative radiographs. The current radiographic findings likely resulted from the
A. spinal fusion.
B. BMI and implant size.
C. mismatch between the metaphysis and diaphysis.
D. modular neck prosthesis.
Question 58:
In patients without spondylolisthesis or scoliosis undergoing laminectomy for lumbar spinal stenosis, spinal fusion is generally recommended if
Options:
- a dural tear is repaired.
- more than one level requires decompression.
- less than one half of each facet is removed bilaterally.
- the pars interarticularis is fractured.
- the patient is a smoker.
Correct Answer: the pars interarticularis is fractured.
Explanation:
DISCUSSION: With the notable exception of fusion for degenerative spondylolisthesis and scoliosis, there is a paucity of evidence on the indications for spinal fusion in patients undergoing laminectomy for spinal stenosis. However, it is generally recommended that if the spine is destabilized (for example by removal of one complete facet joint or by an iatrogenic pars fracture), spinal fusion should be considered. Although fusion can be considered for a very long laminectomy, a two-level laminectomy does not represent, by itself, a clear indication for the addition of a spinal fusion. The repair of a dural tear and the use of nicotine by the patient play no role in the determination of whether or not to add fusion to a laminectomy procedure.
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 299-409.
Fischgrund JS, Mackay M, Herkowitz HN, et al: 1997 Volvo Award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 59:
Following application of topical lidocaine, copious arterial bleeding is noted from the region of 1 neurovascular bundle, and the digit remains cool and pale. What is the best next step?
Options:
- Intraoperative arteriogram
- Wound closure and observation
- Ligation of the digital artery
- Primary repair of the digital artery
Correct Answer: Primary repair of the digital artery
Explanation:
DISCUSSION
Used with permission from Benson LS, Williams CS, Kahle M. Dupuytren’s contracture. J Am Acad Surg. 1998
Jan-Feb;6(1):24-35. Review
The spiral cord seen in Dupuytren disease arises from the confluence of abnormal fascial thickening of the spiral bands, lateral digital sheet, and Grayson’s ligament. The orientation of these contributing structures results in a continuous band of fibrous tissue spiraling around the neurovascular bundle. As the developing spiral cord contractures from distal to proximal, the cord itself becomes increasingly linear and shorter, causing displacement of the neurovascular bundle both centrally and superficially. This displacement of the neurovascular bundle brings it closer to the skin and midline, making it more vulnerable to surgical trauma.
Studies have demonstrated a high association between a PIP joint flexion contracture and a spiral cord (Figure 52). Spiral cords are also seen in association with a soft, fleshy mass between the proximal digital flexion crease and distal palmar crease in the interdigital space referred to as an interdigital soft-tissue mass. This represents displacement of normal subcutaneous tissues by contracture of the diseased fascia associated with the spiral cord. Dupuytren diathesis, MCP joint contracture, and the presence of knuckle pads are not indicative of a spiral cord.
A complication following surgical treatment of Dupuytren contracture is trauma to the neurovascular bundle. This can be a consequence of blunt or sharp trauma. In the case of traumatic stretch injury from retraction, vasospasm may develop. The treatment of vasospasm includes flexion, warming the digit, and application of topical medication to treat vasospasm. Allowing the newly extended digit to flex is an important first step, particularly in the case of chronic and severe PIP joint contractures. In these cases, the vessel may have shortened over time, and full extension may cause intimal trauma and secondary vasospasm. Cold is also a stimulus for reactive vasospasm, so warming the digit with warm saline irrigation can be helpful. Finally, topically applied lidocaine (without vasoconstrictive additives) can help diminish vasospasm and lead to digital reperfusion. Phentolamine is useful in cases of prolonged vasospasm secondary to administration of anesthetics containing epinephrine. Streptokinase is a thrombolytic agent that may be useful in treatment of embolic or thrombotic vascular disease. Systemic heparin is useful for digital vessel repair but should not be necessary to treat simple vasospasm.
Copious bleeding in the region of the neurovascular bundle following palmar fasciectomy is an indication of potential arterial trauma. In the setting of arterial laceration, direct repair is necessary, particularly when the digit is dysvascular. This means that both digital vessels are involved or that the intact vessel is insufficient to adequately perfuse the digit. During surgery, the vessels can be directly visualized, and arteriography is unlikely to add additional information of value. Streptokinase is not indicated in this situation because it is useful for thrombolysis rather than vascular repair. Ligation of a traumatized digital artery might be appropriate for a digit that is otherwise well perfused; however, this is not appropriate in the setting of a dysvascular digit. Direct suture of the arterial laceration or segmental grafting necessary to restore adequate digital perfusion in this scenario.
RECOMMENDED READINGS
Rayan GM. Dupuytren disease: Anatomy, pathology, presentation, and treatment. J Bone Joint Surg Am. 2007 Jan;89(1):189-98. Review. PubMed PMID: 17256226.
View Abstract at PubMed
Watson HK, Paul H Jr. Pathologic anatomy. Hand Clin. 1991 Nov;7(4):661-8. Review. PubMed PMID: 1769988.
View Abstract at PubMed
Jones NF, Huang JI. Emergency microsurgical revascularization for critical ischemia during surgery for Dupuytren's contracture: a case report. J Hand Surg Am. 2001 Nov;26(6):1125-8. PubMed PMID: 11721263.
View Abstract at PubMed
Question 60:
What is the typical axial plane transverse angulation of the thoracic pedicles?
Options:
- 5 degrees medial at T 1 and T 2 ; 10 degrees from T3 to T10
- 5 degrees lateral at T 1 ; neutral at T 2 ; 5 degrees medial from T3 to T12
- 10 degrees medial from T1 to T10; 15 degrees medial at T11 and T12
- 10 degrees medial from T 1 to T12
- 25 degrees medial at T 1 ; 15 degrees at T 2 ; and 10 degrees medial from T3 to T10
Correct Answer: 25 degrees medial at T 1 ; 15 degrees at T 2 ; and 10 degrees medial from T3 to T10
Explanation:
DISCUSSION: Thoracic pedicles typically are angled 25 degrees medially at T
1
so the
starting point is more lateral. T
2
angles about 15 degrees, and then the pedicles average about
5 to 7 degrees down to T10. At T11 and 12, the angulation is minimal.
REFERENCES: Weinstein L: Pediatric Spine Principles and Practice. New York, NY, Raven Press, 1994, pp 1659-1681.
Lenke LG, Orchowski J: Segmental posterior spinal instrumentation: Thoracic spine to sacrum, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 537-552.
Question 61:
Figure 82 is the MRI scan of a 15-year-old boy who has had knee pain with running for 5 months. Radiographs show an osteochondritis dissecans (OCD) lesion of the medial femoral condyle. What is the most appropriate treatment? Review Topic
Options:
- Arthroscopic or open reduction and internal fixation
- Arthroscopic loose body removal
- Activity restriction for up to 9 months
- Subchondral drilling
Correct Answer: Arthroscopic or open reduction and internal fixation
Explanation:
OCD is an acquired lesion of the subchondral bone. Patients with OCD initially report nonspecific pain and variable amounts of swelling. Initial radiographs help identify the lesion and establish the status of the physes. An MRI scan is useful for assessing the potential for the lesion to heal with nonsurgical treatment. Nonsurgical treatment is appropriate for small, stable lesions in patients with open physes and focuses on activity restriction for 3 to 9 months. Surgical treatment is necessary for unstable or detached lesions. Stable lesions with intact articular cartilage can be treated with subchondral drilling to stimulate vascular ingrowth, with radiographic healing at an average of 4.4 months. Fixation is indicated for unstable or hinged lesions, and stabilization of the fragment can be achieved using a variety of implants through an arthroscopic or open approach. The fragment should be salvaged and the normal articular surface restored whenever possible.
Question 62:
A 42-year-old man sustained a fracture of the distal radius with subsequent stiffness in the ipsilateral shoulder. Despite a 6-month program of range-of-motion exercises, external rotation at the side is limited to 10 degrees. Attempts at closed manipulation are unsuccessful. Treatment should now consist of
Options:
- open release of the posterior capsule.
- arthroscopic release of the rotator cuff interval.
- arthroscopic release of the anteroinferior capsule.
- open subscapularis lengthening.
- open extra-articular release.
Correct Answer: arthroscopic release of the rotator cuff interval.
Explanation:
DISCUSSION: When external rotation at the side is limited, the most likely diagnosis is contracture of the rotator cuff interval, including the superior glenohumeral and coracohumeral ligaments. Therefore, the treatment of choice is arthroscopic release of the rotator cuff interval.
REFERENCE: Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
Question 63:
What nerve is at the highest risk for injury with a percutaneous repair of an Achilles tendon injury?
Options:
- Posterior tibial
- Calcaneal
- Intermediate branch of the superficial peroneal
- Lateral plantar
- Sural
Correct Answer: Sural
Explanation:
DISCUSSION: Cadaver and clinical studies have shown that the sural nerve is at the highest risk for injury with a percutaneous repair of the Achilles tendon.
REFERENCE: Hockenbury RT, Johns JC: A biomechanical in vitro comparison of open versus percutaneous repair of tendon Achilles. Foot Ankle 1990;11:67-72.
Question 64:
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What is the underlying cause of the pathology noted in the figures?
Options:
- Genetic mutation
- Recurrent trauma
- Shallow intercondylar notch
- Congenital abnormality
Correct Answer: Congenital abnormality
Explanation:
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment
of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.
Question 65:
Fixed hyperextension of the metatarsophalangeal joint is associated with
Options:
- dorsal subluxation of the interossei.
- dorsal subluxation of the lumbricals.
- fibrosis of the plantar plate.
- attenuation of the extensor longus tendon.
- extrinsic flexor paralysis.
Correct Answer: dorsal subluxation of the interossei.
Explanation:
DISCUSSION: Claw toe and hammer toe deformities are associated with dorsal subluxation of the interossei, which can no longer serve to flex the metatarsophalangeal joint. The extensor digitorum longus then loses its tenodesing effect on the proximal interphalangeal and distal interphalangeal joints and works unopposed to extend the metatarsophalangeal joint and the proximal phalanx. Without the antagonistic action of the extensor digitorum longus, the extrinsic flexors become unopposed flexors of the proximal and distal interphalangeal joints.
REFERENCES: Marks RM: Anatomy and pathophysiology of lesser toe deformities. Foot Ankle Clin 1998;3:199-213.
Myerson MS, Shereff MJ: The pathological anatomy of claw and hammer toes. J Bone Joint Surg Am 1989;71:45-49.
Question 66:
A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?
Options:
- Functional rehabilitation and return to play when he has pain-free range of motion
- Immobilization in internal rotation for 6 weeks
- Immobilization in internal rotation for 3 weeks, followed by 3 weeks of supervised rehabilitation
- Immobilization with the arm in neutral rotation
- Immobilization with the arm in 30 degrees of external rotation
Correct Answer: Immobilization with the arm in 30 degrees of external rotation
Explanation:
DISCUSSION: Recent evidence has shown that the position of immobilization of the shoulder after a dislocation influences the reduction of the Bankart lesion. In an MRI study in patients who sustained an anterior dislocation, the Bankart lesion was reduced to the glenoid anatomically with the arm in 30 degrees of external rotation. Subsequently, a clinical follow-up study has shown a reduction in recurrence rates when the arm is immobilized in external rotation compared to internal rotation.
REFERENCES: Itoi E, Hatakeyama Y, Kido T, et al: A new method of immobilization after traumatic anterior dislocation of the shoulder: A preliminary study. J Shoulder Elbow Surg 2003;12:413-415.
Itoi E, Sashi R, Minagawa H, et al: Position of immobilization after dislocation of the glenohumeral joint: A study with use of magnetic resonance imaging. J Bone Joint Surg Am 2001;83:661-667.
Question 67:
Which modality has the broadest application for the reduction of postsurgical transfusion?
Options:
- Regional anesthesia
- Tranexamic acid (TXA) administration
- Reduced transfusion trigger
- Hypotensive anesthesia
Correct Answer: Tranexamic acid (TXA) administration
Explanation:
DISCUSSION:
TXA is easy to administer, inexpensive, and safe for virtually all patients. Multiple studies have demonstrated transfusion rates lower than 3% for total knee arthroplasty and lower than 10% for total hip arthroplasty. Regional and hypotensive anesthesia effectively reduce transfusion; however, they cannot be used in as wide a range of patients as can TXA. A reduced transfusion trigger must be considered along with patient symptoms when determining the need for transfusion.
Question 68:
High periosteal signal; normal marrow T1 signal; high marrow T2 signal
Options:
- In 1995, Fredrickson and colleagues classified stress fractures into four grades based upon bone scans: Grade 1 Â Â Â Â Â Small ill-defined cortical area of mildly increased activity
- Grade 2     Well-defined cortical area of moderately increased cortical                     activity
- Grade 3Â Â Â Â Â Wide, cortical-medullary area of increased activity Grade 4Â Â Â Â Â Transcortical area of intensely increased activity
Correct Answer: In 1995, Fredrickson and colleagues classified stress fractures into four grades based upon bone scans: Grade 1 Â Â Â Â Â Small ill-defined cortical area of mildly increased activity
Explanation:
(3786) Q2-7568:
Which of the following treatment methods is used for the majority of patients with a stress fracture:
Question 69:
A 67-year-old woman has persistent anterior thigh and knee pain after undergoing total knee arthroplasty 1 year ago. Examination and radiographs reveal no problems in the knee, mild hip flexor weakness (grade 4+), and decreased sensation over the anterior thigh including and proximal to the incision. MRI of the lumbar spine will most likely reveal which of the following findings?
Options:
- Posterolateral herniated nucleus pulposus at L3-4
- Posterolateral herniated nucleus pulposus at L4-5
- Degenerative disk disease at L3-4 and L4-5 with no significant facet hypertrophy
- Degenerative spondylolisthesis at L3-4 with central and foramenal stenosis
- Degenerative spondylolisthesis at L4-5 with central stenosis
Correct Answer: Degenerative spondylolisthesis at L3-4 with central and foramenal stenosis
Explanation:
DISCUSSION: Degenerative spondylolisthesis at L3-4 is the most likely diagnosis. This spondylolisthesis would result in foraminal stenosis affecting the third lumbar root and leading to anterior thigh and knee pain and hip flexor weakness. L4-5 spondylolisthesis would impinge on the L4 root in the foramen. Degenerative disk disease without hypertrophy is unlikely to have root impingement. Posterolateral herniations typically affect the inferior root and are less common in this age group.
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 250.
Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 70:
After sustaining a muscle contusion injury, prolonged immobilization leads to Review Topic
Options:
- increased tensile stiffness.
- increased granulation tissue production.
- improved recovery of tensile strength.
- reduced incidence of myositis ossificans.
Correct Answer: increased granulation tissue production.
Explanation:
Increased granulation tissue production occurs with prolonged immobilization following contusion injury; this condition may lead to myositis ossificans. Prolonged immobilization can lead to contraction of scar, poor structural organization of the regenerating muscle, and, ultimately, scar tissue. In a study by J◻rvinen and associates, muscles immobilized following contusion injury were pulled to failure at tensile strengths much lower than tolerated by mobilized limbs. In addition, there is a decrease in tensile stiffness.
Question 71:
A 20-year-old collegiate football player sustains an injury to his left foot 3 weeks before the start of the fall season. Examination reveals localized tenderness over the lateral midfoot and normal foot alignment. Radiographs are shown in Figures 28a through 28c. What is the treatment of choice?
Options:
- Intramedullary screw fixation
- Onlay bone graft
- Application of a walking boot with weight bearing as tolerated
- Application of a short leg cast with weight bearing as tolerated
- Application of a short leg cast and non-weight-bearing
Correct Answer: Intramedullary screw fixation
Explanation:
DISCUSSION: Due to the relatively high incidence of delayed union and nonunion associated with this mildly displaced Jones-type fracture, and the temporal proximity to his playing season, intramedullary screw fixation is the treatment of choice in this collegiate athlete to best ensure healing and expedite his return to football. If nonsurgical management were elected, application of a non-weight-bearing short leg cast would be appropriate since a higher likelihood of healing is expected with it versus a short leg walking cast. The risk of recurrent fracture of fractures that heal with nonsurgical management has reportedly been high (approximately 30%).
REFERENCES: Quill GE: Fractures of the proximal fifth metatarsal. Orthop Clin North Am 1995;26:353-361.
Torg JS, Balduini FC, Zelko RR, et al: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.
Dameron TB Jr: Fractures of the proximal fifth metatarsal: Selecting the best treatment option.
J Am Acad Orthop Surg 1995;3:110-114.
Question 72:
The patient develops an inability to dorsiflex her foot 2 days after surgical intervention while she is sitting in a chair after physical therapy. Initial treatment should consist of
Options:
- lying completely supine in bed.
- remaining seated and placing the postsurgical leg on a stool.
- transferring back to bed with the head of the bed no lower than 60 degrees.
- transferring back to bed with the head of the bed level and the surgical knee flexed.
Correct Answer: transferring back to bed with the head of the bed level and the surgical knee flexed.
Explanation:
DISCUSSION
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis.
This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis, observation for 1 year would not be appropriate.
The psoas is the anatomic structure that runs anterior to the acetabulum. The femoral neurovascular structures are at risk if the retractor is placed anterior and inferior to the psoas tendon.
The patient develops a foot drop 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MR imaging or a CT scan may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be decreased by flexing the surgical knee and positioning the bed flat.
Question 73:
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by
Options:
- a posterior-lateral approach.
- a lateral approach.
- a medial approach.
- an anterior-medial approach.
- rigid cast immobilization.
Correct Answer: a lateral approach.
Explanation:
DISCUSSION: In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by the use of a direct lateral approach to the ankle. The superficial peroneal nerve and its branches exit the fascial hiatus approximately 9 cm to 10 cm proximal to the tip of the distal fibula with a range of 4 cm to 13 cm, and their course is typically anterior to the midlateral plane of the fibula. However, small branches may course across the surgical plane directly laterally. A posterior-lateral approach diminishes the risk of injury to the superficial peroneal nerve and its branches; however, by moving farther posterior, the sural nerve and its branches may be at increased risk. Cast immobilization may injure the cutaneous nerves about the ankle; however, the risks are greater with surgical intervention. A medial or anterior-medial approach to the ankle will not injure the superficial peroneal nerve at the ankle level.
REFERENCES: Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Miller SD: Ankle fractures, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1341-1366.
Question 74:
A 21-year-old woman has a nontraumatic rupture of the Achilles tendon. Which of the following commonly prescribed medications has been associated with this condition?
Options:
- Ibuprofen
- Fluoroquinolones
- Bisphosphonates
- Metoprolol
- Simvistatin
Correct Answer: Fluoroquinolones
Explanation:
DISCUSSION: Fluoroquinolones have been associated with increased rates of tendinitis, with special predilection for the Achilles tendon. Tenocytes in the Achilles tendon have exhibited degenerative changes when viewed microscopically after fluoroquinolone administration. Recent clinical studies have shown an increased relative risk of Achilles tendon rupture of 3.7. The other listed drugs have no known increase in tendon rupture rates nor tendinitis.
REFERENCES: van der Linden PD, van de Lei J, Nab HW, et al: Achilles tendinitis associated with fluoroquinolones. Br J Clin Pharmacol 1999;48:433-437.
Bernard-Beaubois K, Hecquet C, Hayem G, et al: In vitro study of cytotoxicity of quinolones on rabbit tenocytes. Cell Biol Toxicol 1998;14:283-292.
Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Question 75:
-An infant was born with complex syndactyly involving all 4 fingers of both hands, short and deformed thumbs, and similar syndactyly involving both feet. In addition, an altered facial appearance was noted with protruding eyes, a towered cranium, and midface hypoplasia. This appearance is characteristic of which syndrome?
Options:
- Apert
- Poland
- Holt-Oram
- VACTERRL
- Thrombocytopenia-absent radius (TAR)
Correct Answer: Apert
Question 76:
A 71-year-old woman with coronary artery disease underwent an uncomplicated right total hip arthroplasty for osteoarthritis 12 years ago. Her hip has functioned well until approximately 18 months ago when she noted the spontaneous onset of groin, buttock, and proximal thigh pain that is present at rest and made worse with activity. A radiograph is shown in Figure 15. What is the recommended management at this point?
Options:
- Immediate admission to the hospital and emergent revision hip arthroplasty
- Reassurance and follow-up if symptoms worsen
- Repeat radiographs in 1 month
- Protected weight bearing with urgent revision hip arthroplasty when the patient is medically cleared
- A prescription for alendronate and reevaluation in 1 year
Correct Answer: Protected weight bearing with urgent revision hip arthroplasty when the patient is medically cleared
Explanation:
DISCUSSION: The radiograph shows significant osteolysis with loosening of the femoral component. The patient is symptomatic and surgery is indicated because of the extent of osteolysis and the loose femoral component.
Reassurance and follow-up if symptoms worsen places the patient at risk for further bone loss and periprosthetic fracture. Emergent surgery is not required because the symptoms have been present for more than a year; however, urgent revision hip arthroplasty is recommended when the patient is medically cleared. While there is data to suggest that bisphosphonates may slow the progression of osteolysis in animal modes, there is no clear evidence that bisphosphonate treatment prevents the progression of osteolysis in humans. Additionally, this patient has a loose symptomatic femoral component.
REFERENCES: Chiang PP, Burke DW, Freiberg AA, et al: Osteolysis of the pelvis: Evaluation and treatment. Clin Orthop Relat Res 2003;417:164-174.
Dunbar MJ, Blackley HR, Bourne RB: Osteolysis of the femur: Principles of management. Instr Course Lect 2001;50:197-209.
Rubash HE, Dorr LD, Jacobs JJ, et al: Does alendronate inhibit the progression of periprosthetic osteolysis? Trans
Orthop Res Soc 2004;29:1888.
)
Figure 16a Figure 16b
Question 77:
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?
Options:
- Excessive anteversion of the humeral component
- Excessive anteversion of the glenoid component
- Excessive posterior capsular laxity
- Anterior capsular laxity
- Use of an oversized humeral head
Correct Answer: Excessive posterior capsular laxity
Explanation:
DISCUSSION: Anteversion of the humeral component may result in anterior instability of the component. Posterior instability after total shoulder arthroplasty is usually the result of some combination of the following factors: untreated anterior soft-tissue contractures, excessive posterior capsular laxity, and excessive retroversion of the humeral and/or glenoid components.
REFERENCES: Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
Wirth MA, Rockwood CA Jr: Complications of total shoulder replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Question 78:
All of the following are characteristic of synovium affected by rheumatoid arthritis (RA) EXCEPT:
Options:
- Prominent intimal hyperplasia
- Decreased apoptosis
- Increased angiogenesis
- Disruption of the basement membrane
- Abundant lymphocytes
Correct Answer: Prominent intimal hyperplasia
Explanation:
The basement membrane is not disrupted in rheumatoid arthritis-affected synovial tissue, as synovium lacks a true basement membrane.
Normal synovium consists of two layers, the intimal and the sublining, and two types of cells, type A and B. In RA, the following changes to the synovium are seen: 1) hyperplasia, with the intimal lining increasing from two cell layers to 10-20 layers 2) decreased apoptosis of the lining 3) increased angiogenesis and 4) abundant lymphocytes around vessels, forming lymphoid follicles.
The synovial pannus is invasive granulation tissue that contains fibroblast-like synoviocytes, but few inflammatory cells. The synovial cells in the pannus have anchorage-independent growth and invasive capabilities, allowing them to directly attack and destroy articular cartilage.
Koch et al. note that the possible contributions of angiogenesis to the proliferation of the inflammatory synovial pannus and the ingress of inflammatory leukocytes into the synovial tissue in RA have been extensively studied. Relevant angiogenesis inducers seen in RA include FGF-2, VEGF, TGFß, TNFa, IL-1, IL-8, VCAM-1, among others. Modulation of angiogenesis may be a viable therapeutic option for RA in the future.
Incorrect Answers:
Question 79:
A patient sustains a displaced scapular neck fracture. What is the internervous plane for a posterior approach to the glenohumeral joint?
Options:
- lateral pectoral-axillary
- subscapular-musculocutaneous
- suprascapular-axillary
- long thoracic-spinal accessory
- suprascapular-subscapular
Correct Answer: lateral pectoral-axillary
Explanation:
CORRECT
DISCUSSION: Surgical fixation of a scapular neck fracture is performed via the Judet approach, a posterior approach to the scapula/glenoid. The internervous plane is between the infraspinatus (suprascapular nerve) and the teres minor (axillary nerve). As outlined by Ball et al, the posterior branch of the axillary nerve has intimate association with the inferior aspects of the glenoid and shoulder joint capsule, which may place it at particular risk during a posterior approach to the shoulder.
Question 80:
Figures 1 and 2 are of a 51-year-old man who underwent open reduction and internal fixation of a right proximal humerus fracture with concomitant rotator cuff repair. Within 1 year, he develops heterotopic ossification, for which he undergoes excision and hardware removal. Postoperatively, he was noted to have progressive atrophy in the shoulder and anterior humeral head subluxation with attempted shoulder abduction. What nerve was damaged during the most recent procedure?
Options:
- Suprascapular
- Radial
- Anterior branch of axillary
- Spinal accessory (cranial nerve XI)
Correct Answer: Anterior branch of axillary
Explanation:
EXPLANATION:
This patient has a deficiency of the anterior deltoid muscle, resulting in inferior subluxation of the humerus with associated glenohumeral instability. Axillary nerve injury during shoulder surgery accounts for 6% to 10% of brachial plexus injuries. In the posterior scapular region, the axillary nerve terminates by dividing into two main branches: the posterior terminal branch, which provides motor innervation to the teres minor and posterior deltoid muscles, and the anterior terminal branch, which provides motor innervation to the anterior and middle portions of the deltoid muscle. The deltoid determines the silhouette
of the shoulder and is a stabilizer of the humeral head.
Question 81:
Radiotherapy for palliative pain control as the risk for pathological fracture is very small
Options:
- Open incisional biopsy
- Chemotherapy and surgical stabilization with intramedullary nailing of the tibia
- Radiotherapy and surgical stabilization with intramedullary nailing of the tibia
Correct Answer: Radiotherapy and surgical stabilization with intramedullary nailing of the tibia
Explanation:
Treatment for musculoskeletal oncology depends on a correct tissue diagnosis, which in this patient requires an open incisional biopsy. Despite the concern that this lesion may represent a metastasis from lung carcinoma, without tissue diagnosis, treatment cannot ensue. Regarding concerns for pathologic fracture, this patient would be best managed with no weight bearing until a diagnosis can be determined. If this lesion is a sarcoma, then despite the patient's pain and risk of pathologic fracture, neo-adjuvant chemotherapy and wide surgical resection will be needed for the best chance at local control and patient survival. While intramedullary nailing of the tibia and sending canal reamings to pathology may either appear appropriate or be performed at
some centers, this procedure may contaminate the entire bone with tumor and make limb salvage nearly impossible if this is a sarcoma. If the incisional biopsy shows carcinoma, then intramedullary nailing with adjuvant radiotherapy would be completely appropriate.
Question 82:
Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow? Review Topic
Options:
- Infraspinatus
- Teres minor
- Subscapularis
- Long head of triceps
- Latissimus dorsi
Correct Answer: Teres minor
Explanation:
The sagittal T1-weighted MRI scan is useful for interpreting the quality of muscle. The arrow is pointing to the teres minor.
Question 83:
Use of titanium elastic nailing for treatment of pediatric femur fractures is associated with a higher complication rate among
Options:
- patients younger than age 6.5.
- patients who bear weight immediately after surgery.
- patients weighing more than 50 kg (110 pounds).
- patients with grade 1 open transverse midshaft fractures.
Correct Answer: patients weighing more than 50 kg (110 pounds).
Explanation:
DISCUSSION
Studies of titanium elastic nailing for femur fractures demonstrated a higher rate of complications, including angular deformity and construct failure, among patients weighing more than 50 kg (100 pounds). Other methods of fixation are recommended for these patients. Flexible nails are not commonly needed, but they also are not associated with a higher complication rate in children younger than age 6.5. Titanium elastic nailing works well in closed or minimally open transverse midshaft fractures, even in the setting of early or immediate weight bearing.
Video 8a
Video 8b
Question 84:
A 53-year-old woman has severe neck and left shoulder pain after a rollover motor vehicle accident. Radiographs and a CT scan of the cervical spine are shown in Figures 34a through 34c. Management should consist of
Options:
- a soft cervical collar.
- a rigid cervical collar.
- halo vest immobilization for 3 months.
- simple midline (Rogers) wiring.
- lateral mass plate fixation at C4-C6.
Correct Answer: lateral mass plate fixation at C4-C6.
Explanation:
DISCUSSION: The plain radiographs show a horizontal orientation of the C5 facet joint. The CT scan through C5 reveals an ipsilateral pedicle and lamina fracture (floating facet). This injury involves two adjacent motion segments and is extremely unstable. Lateral mass plates, with or without the purchase of the “floating facet,” provide the best means of stabilization and should include the facet above (C4) and below (C6) the level of injury. Orthotic immobilization is insufficient for this particular injury. Halo vest treatment does not control the subaxial spine well and is of limited value. While simple midline (Rogers) wiring provides some tension band restoration, it is not optimal for rotational control. The use of lateral mass plates provides rotational stability. Another option would be anterior fusion and plating, which would save cervical segments.
REFERENCES: Levine AM, Mazel C, Roy-Camille R: Management of fracture separations of the articular mass using posterior cervical plating. Spine 1992;17:S447-S454.
Levine AM: Facet fractures and dislocations, in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 360-362.
Whitehill R, Richman JA, Glaser JA: Failure of immobilization of the cervical spine by the halo vest: A report of five cases. J Bone Joint Surg Am 1986;68:326-332.
Garvey TA, Eismont FJ, Roberti LJ: Anterior decompression, structural bone grafting, and Caspar plate stabilization for unstable cervical spine fractures and/or dislocations. Spine 1992;17:S431-S435.
Question 85:
Which of the following anatomic structures are in contact with internal impingement in the throwing athlete? Review Topic
Options:
- Humerus and posterior-superior glenoid
- Humerus and anterior inferior glenoid
- Humerus and acromion
- Biceps and acromion
- Rotator cuff and acromion
Correct Answer: Humerus and posterior-superior glenoid
Explanation:
Internal impingement occurs in the late cocking phase of throwing with humeral head abduction and maximal external rotation. It is a physiologic phenomenon occurring in 85% of patients undergoing arthroscopy for various indications in one study. Internal impingement is defined as impingement of the posterior-superior rotator cuff between the humerus and posterior-superior glenoid rim. Symptomatic internal impingement is felt to be due to the frequency and magnitude of the impingement in throwers.
Question 86:
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?
Options:
- Patellar sleeve fracture
- Avulsion of the tibial tubercle
- Avulsion of the anterior tibial spine
- Osteochondral fracture of the femoral condyle
- Osteochondral fracture of the patella
Correct Answer: Patellar sleeve fracture
Explanation:
DISCUSSION: This is a typical patellar sleeve fracture. The patellar tendon avulses a portion of the distal bony patella, along with the retinaculum and articular cartilage from the inferior pole of the patella. It is common in children between ages 8 and 10 years. Anatomic reduction and repair of the extensor mechanism are mandatory to reestablish full knee extension.
REFERENCES: Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Question 87:
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior knee pain, a trace effusion, a 2+ posterior drawer, a grade 1+ stable Lachman, no valgus laxity, and negative dial tests at 30 degrees and 90 degrees. What is the best treatment strategy at this time? Review Topic
Options:
- Physical therapy with a focus on quadriceps strengthening
- Physical therapy and delayed posterior cruciate ligament (PCL) reconstruction
- PCL reconstruction
- PCL and posterolateral corner reconstruction
Correct Answer: Physical therapy with a focus on quadriceps strengthening
Explanation:
This patient has likely sustained an isolated PCL injury. The examination is consistent with a grade II injury to the PCL. In this scenario, the best initial option is nonsurgical treatment and return to play as symptoms subside and strength improves. Physical therapy with a focus on quadriceps strengthening and delayed PCL reconstruction is not the answer because this patient can likely be treated without surgery. The absence of valgus laxity and negative dial testing findings suggest that an injury to the posteromedial and posterolateral corners has not occurred. Initial nonsurgical treatment is indicated for this patient. If he completes rehabilitation and experiences persistent disability with anterior and/or medial knee discomfort or senses the knee is "loose," PCL reconstruction should be considered at that time.
Question 88:
Figures below show the radiographs obtained from a 68-year old man with progressively worsening right side hip pain over the last 8 months. He is 6 feet tall, with a BMI of 51 kg/m2 and reports that his index total hip arthroplasty was performed 8 years ago. The preoperative work-up includes negative infectious laboratory results. What is the most appropriate surgical plan for revision of the femoral component in this patient?
Options:
- Superior approach with trochanteric slide
- Direct anterior approach with a chevron modification of the standard greater trochanteric osteotomy
- Lateral approach with a partial greater trochanter osteotomy
- Posterolateral approach with an extended trochanteric osteotomy
Correct Answer: Posterolateral approach with an extended trochanteric osteotomy
Explanation:
DISCUSSION:
Submit Answer
The patient’s radiographs demonstrate varus femoral remodeling around a broken cylindrical, distally fixed femoral stem. Proximal femoral remodeling around loose or fractured stems occurs in 21% to 42% of femoral revisions, based on the definitions outlined by Foran and associates. In definition 1, varus femoral remodeling occurs when the template falls within 2 mm of the endosteal cortex of the metaphysis on templating with a diaphyseal engaging stem. In definition 2, varus femoral remodeling = when the template crosses the lateral femoral cortex proximally. Based on the templating or drawing a line from the isthmus proximally along the lateral cortex, implantation of a straight stem would perforate the cortex proximally, indicating varus femoral remodeling. An extended trochanteric osteotomy would aid in the removal of the well-fixed distal segment and enable the safe insertion of the new femoral component. The approach is not the concern in this case, because extended trochanteric osteotomies have been described from the posterior and direct lateral approaches with excellent outcomes and union rates. The key is that the extended osteotomy is necessary and not a trochanteric slide or standard (shorter or incomplete trochanteric) osteotomy. These types would not provide access to the well-fixed distal stem, nor would they afford a straight tube in which to insert a new femoral component.
Question 89:
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal.
Options:
- Decompression and posterior fusion at L4-L5
- Epidural steroid injection at L4-5
- Nonsteroidal medications and physical therapy for 6 weeks
- Measurement of the ankle-brachial index
- CT myelogram
Correct Answer: Measurement of the ankle-brachial index
Explanation:
The patient has symptoms that are more consistent with vascular claudication than with the pseudoclaudication anticipated from lumbar spinal stenosis. Therefore, the patient is a candidate for further vascular work-up. The radiographs reveal early spinal stenosis and spondylolisthesis at L4-5 but also show significant calcification of the iliac arteries, suggestive of peripheral vascular disease. Vascular claudication is a manifestation of peripheral vascular disease and presents with crampy leg pain that is exacerbated by physical exertion. The pain is easily relieved by standing still or sitting. Unlike pseudoclaudication, a forward-flexed posture and/or sitting does not improve the symptoms. Night pain is common in vascular claudication due to the elevation of the extremities and patients often report pain improvement by hanging their extremities in a dependent position. In evaluation of a patient with suspected vascular claudication, the five “P’s” of vascular insufficiency should be monitored, including pulselessness, paralysis, paresthesia, pallor, and pain. While pain and paresthesias can be common in both vascular claudication and pseudoclaudication, the presence of any of the remaining symptoms is suggestive of vascular disease.
Question 90:
What is the most common nonanesthetic-related reversible cause of changes in intraoperative neurophysiologic monitoring data?
Options:
- Pedicle screw misplacement
- Patient positioning
- Spinal cord ischemia
- Retractor placement
- Hypotension
Correct Answer: Patient positioning
Explanation:
DISCUSSION: Patient positioning that results in local nerve compression, plexus traction, or improper neck alignment is the most common nonanesthetic-related cause of changes in intraoperative neurophysiologic monitoring data during spinal surgery.
REFERENCES: Jones SC, Fernau R, Woeltjen BL: Use of somatosensory evoked potentials to detect peripheral ischemia and potential injury resulting from positioning of the surgical patient: Case reports and discussion. Spine J 2004;4:360-362.
Schwartz DM, Sestokas AK, Hilibrand AS, et al: Neurophysiological identification of position-induced neurologic injury during anterior cervical spine surgery. J Clin Monit Comput 2006;20:437-444.
Question 91:
What factor induces myofibrillar muscle protein synthesis (MPS)? Review Topic
Options:
- Aerobic exercise
- Anabolic hormones (growth hormone/testosterone)
- Resistance exercise above 60% 1-repetition maximum (RM)
- High-repetition exercise at mid intensity (30% 1-RM)
Correct Answer: Resistance exercise above 60% 1-repetition maximum (RM)
Explanation:
Resistance exercise induces myofibrillar MPS that drives muscle hypertrophy. Growth hormone/testosterone does not influence MPS in acute response to exercise or adaptive response of muscle hypertrophy to resistance exercise. Recombinant growth hormone administration does not affect MPS. Anabolic steroids do not drive adaptation in humans; an intrinsic autocrine/paracrine factor and mechanotransduction process is involved. Exercise above 60% 1-RM represents anabolic ceiling. There is a sigmoidal dose response to resistance exercise, maximum MPS occurs at > 60% 1-RM. Aerobic-zone exercise does not result in hypertrophy of skeletal muscle, but it does increase oxidative capacity.
Question 92:
A 65-year-old woman who works as a florist has had pain in her right elbow for the past 6 months after lifting a flowerpot. MRI scans are shown in Figures 55a and 55b. The area of increased signal intensity seen in Figure 55b most likely represents which of the following findings?
Options:
- Hematoma
- Edema
- Soft-tissue sarcoma
- Antecubital lipoma
- Brachial artery aneurysm
Correct Answer: Edema
Explanation:
DISCUSSION: The MRI scans reveal a chronic distal biceps tendinitis. The T
1
-weighted scan shows the anatomic detail of the biceps tendon, and the T
2
-weighted scan shows increased signal caused by edema surrounding the tendon. The T
1
-weighted scan is not consistent with an antecubital lipoma. The chronicity of the lesion makes hematoma unlikely. An aneurysm usually appears with blood flow through the region and is dark on T
1
- and T
2
-weighted scans.
REFERENCES: Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 492-504.
Morrey B: Distal biceps tendon rupture, in Master Techniques in Orthopedic Surgery:
The Elbow, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2002, pp 173-192.
Question 93:
A 5-month-old girl with arthrogryposis has a limb-length discrepancy. Examination and radiographs reveal unilateral hip dislocation. Management should consist of
Options:
- a Pavlik harness.
- observation.
- closed reduction and a spica cast.
- open reduction and femoral shortening.
- open reduction.
Correct Answer: open reduction.
Explanation:
DISCUSSION: In this age group of patients with arthrogryposis, open reduction through a medial approach is generally recommended. Open reduction through an anterior approach is reserved for patients in which a medial approach has failed or for older patients who require simultaneous femoral shortening and/or pelvic osteotomy. Closed treatment of unilateral hip dislocation in association with arthrogryposis is rarely successful. In bilateral hip dislocation associated with arthrogrypsis, the consensus is that the hips are best left unreduced because of the difficulty in obtaining excellent clinical and radiographic results bilaterally.
REFERENCES: Staheli LT, Chew DE, Elliot JS, Mosca VS: Management of hip dislocations in children with arthrogryposis. J Pediatr Orthop 1987;7:681-685.
Szoke G, Staheli LT, Jaffe K, Hall JG: Medial-approach open reduction of hip dislocation in amyoplasia-type arthrogryposis. J Pediatr Orthop 1996;16:127-130.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996.
Question 94:
A 45-year-old man sustains an acute closed posterolateral elbow dislocation. The elbow is reduced, and examination reveals that the elbow dislocates posteriorly at 35 degrees with the forearm placed in supination. What is the best course of action?
Options:
- Cast immobilization for 6 weeks
- Hinged brace with early range of motion in supination
- Hinged brace with early range of motion in pronation
- Primary ligament repair
- Lateral collateral ligament reconstruction with tendon graft
Correct Answer: Hinged brace with early range of motion in pronation
Explanation:
DISCUSSION: Most closed simple dislocations are best managed with early range of motion. Posterior dislocation typically occurs through a posterolateral rotatory mechanism. When placed in pronation, the elbow has greater stability when the medial ligamentous structures are intact. In traumatic dislocations, MRI rarely provides additional information that will affect treatment. In elbows that remain unstable, primary repair is preferred over ligament reconstruction. Cast immobilization increases the risk of arthrofibrosis.
REFERENCE: O’Driscoll SW, Morrey BF, Korinek S, et al: Elbow subluxation and dislocation: A spectrum of instability. Clin Orthop 1992;280:186-197.
Question 95:
Treatment of adhesive capsulitis has a high failure rate when the underlying cause is
Options:
- idiopathic.
- traumatic.
- diabetes mellitus.
- hypothyroidism.
- hyperthyroidism.
Correct Answer: diabetes mellitus.
Explanation:
DISCUSSION: Diabetes mellitus has been associated with resistant cases of adhesive capsulitis. With other causes of onset, adhesive capsulitis frequently responds to nonsurgical management such as stretching exercises or, when this fails, manipulation under anesthesia and/or arthroscopic release. Manipulation is rarely successful for the treatment of adhesive capsulitis associated with diabetes mellitus, and arthroscopic release may be preferred.
REFERENCES: Fisher L, Kurtz A, Shipley M: Association between cheiroarthropathy and frozen shoulder in patients with insulin-dependent diabetes mellitus. Br J Rheumatol 1986;25:141-146.
Janda DH, Hawkins RJ: Shoulder manipulation in patients with adhesive capsulitis and diabetes mellitus: A clinical note. J Shoulder Elbow Surg 1993;2:36-38.
Pollock RG, Duralde XA, Flatow EL, Bigliani LU: The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop 1994;304:30-36.
Question 96:
below depict the radiographs obtained from a year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Options:
- Cemented unipolar hemiarthroplasty B. Cemented bipolar hemiarthroplasty C. Total hip replacement
- Open reduction and internal fixation
Correct Answer: Cemented unipolar hemiarthroplasty B. Cemented bipolar hemiarthroplasty C. Total hip replacement
Explanation:
DISCUSSION:
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 97:
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
Options:
- AIDS
- Polytrauma
- Pelvic fracture
- Pilon fracture
- Acute myocardial infarction (AMI)
Correct Answer: Pilon fracture
Explanation:
DISCUSSION: Pollak and associates found that the average SF-36 score for patients who sustained a pilon fracture was significantly lower than patients with diabetes mellitus, AIDS, hypertension, asthma, migraines, pelvic fracture, polytrauma, and AMI. Moreover, patients having undergone pilon fixation scored lower on all but three of the SF-36 scales (vitality, mental health, and emotional health).
REFERENCE: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 98:
A 74-year-old woman has had acute medial right knee pain for the past 3 months. She denies any history of trauma or previous problems. Coronal and sagittal MRI scans are shown in Figures 11a and 11b. What is the most likely diagnosis? Review Topic
Options:
- Osteoarthritis
- Rheumatoid arthritis
- Medial meniscal tear
- Osteonecrosis
- Transient osteoporosis
Correct Answer: Osteonecrosis
Explanation:
Spontaneous osteonecrosis of the medial femoral condyle is seen in the MRI scans, and is most common in women older than age 60 years. Although usually present in the weight-bearing portion of the medial femoral condyle, spontaneous osteonecrosis has also been described involving the lateral femoral condyle and patella. Most patients are seen postcollapse, and the treatment of choice is arthroplasty. Optimal treatment in precollapse stages is controversial.
Question 99:
Which of the following statements is true regarding the posterior oblique portion of the medial collateral ligament of the elbow? Review Topic
Options:
- Can be released to gain flexion in patients with post-traumatic contracture
- Has the highest tensile strength of any elbow ligament
- Is reconstructed in the Tommy John procedure
- Is the primary ligamentous restraint to valgus force during throwing
- Is responsible for the pivot shift of the elbow
Correct Answer: Is responsible for the pivot shift of the elbow
Explanation:
Addressing flexion in a post-traumatic contracture of the elbow requires releasing the posterior oblique ligament (or band) of the medial ulnar collateral complex.
The medial ulnar collateral ligament is one of the primary static stabilizers of the elbow and is composed of three parts: anterior, posterior and transverse. The MCL provides resistance to valgus and distractive stresses. The anterior oblique fibers (of the anterior bundle) are the most important against valgus stresses. The posterior bundle is involved elbow contractures and releasing it can yield significant flexion gains, without creating valgus instability.
Morrey et al. performed a pilot study on 4 specimens and found the valgus stability is equally divided among the medial collateral ligament complex, anterior capsule, and bony articulation in full extension; whereas, at 90 degrees of flexion the contribution of the anterior capsule is assumed by the medial collateral ligament which provides approximately 55% of the stabilizing contribution to valgus stress.
Regan et al. was a subsequent study by the same group that found the posterior medial collateral ligament (PMCL) was taut only when the elbow was in a flexed position. Among the collateral ligaments, the anterior (AMCL) was the strongest and stiffest. (Of note, using present terminology these would be referred to as posterior oblique and anterior oblique portions of the medial ulnar collateral complex).
Wada et al. reported a series of open medial releases for post-traumatic elbow contracture and found scarring on the posterior oblique bundle in all cases. Large increases in flexion were achieved by releasing this structure and the capsule without the need for a lateral incision in most cases.
Illustrations A and B show the posterior oblique portion of the medial collateral ligament. Illustration C shows the most recent terminology and identifies the area to be resected for stiffness.
Incorrect Answers:
Question 100:
Which of the following is true regarding plating of humeral shaft fractures compared to intramedullary nailing?
Options:
- worse functional results
- higher need for subsequent surgeries
- less blood loss
- higher union rates
- increased postoperative shoulder stiffness
Correct Answer: worse functional results
Explanation:
DISCUSSION: Lin et al found less blood loss with intramedullary nailing than plating, but nailing was also associated with increased shoulder surgery due to disruption of the rotator cuff tendon during insertion. Meekers et al found a higher union rate, better functional results and a lower reoperation rate after plate and screw fixation versus nailing. They concluded that plating was superior in most cases of humeral shaft fracture, except for pathological fractures, very obese patients, and open fractures.