Full Question & Answer Text (for Search Engines)
Question 1:
What is the most common anatomic location for chondrosarcoma?
Options:
- Hand
- Distal femur
- Proximal humerus
- Spine
- Pelvis
Correct Answer: Pelvis
Explanation:
DISCUSSION: The most common anatomic location of chondrosarcoma is the pelvis (30%), followed by the proximal femur (20%). Chondrosarcomas appear in the shoulder girdle in 15% of patients but rarely affect the spine or hands.
REFERENCES: Marcove RC, Mike V, Hutter RV, et al: Chondrosarcoma of the pelvis and upper end of the femur: An analysis of factors influencing survival time in one hundred and thirteen cases. J Bone Joint Surg Am 1972;54:561-572.
Simon MA, Springfield DS, et al: Chondrosarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 276.
Question 2:
- Which of the following advantages does the use of a vascularized fibula graft have over a nonvascularized fibula graft?
Options:
- Begins to remodel and hypertrophy more quickly
- Provides a better scaffold for osteoconduction
- Reduces the risk of early fracture
- Reduces technical difficulty
- Lowers donor site morbidity
Correct Answer: Begins to remodel and hypertrophy more quickly
Explanation:
A vascularized fibula graft, because its osteogenic potential remains unhampered by loss of vascularity it will begin to remodel and hypertrophy more quickly. Both types of grafts would act equivocably as scaffolding for osteoconduction. Early risk of fracture is increased if the nonvascularized fibula graft is over 12 centimeters in length as compared to a vascularized graft.
And a vascularized graft requires greater technical skills and a larger dissection to isolate the vascular pedicle with associated increased donor site morbidity.
Question 3:
- A 39-year-old woman jammed her long finger playing softball 24 hours ago. She is unable to actively extend the proximal interphalangeal joint; however, when the joint is brought passively into full extension, she is able to maintain that position. Management should consist of
Options:
- Open repair of the central slip of the extensor mechanism
- Open repair of the terminal tendon of the extensor mechanism
- Closed splinting with the proximal interphalangeal joint
- Closed splinting with the proximal interphalangeal joint in 30 degrees of flexion
- Closed splinting with the proximal interphalangeal joint in 45 degrees of flexion
Correct Answer: Closed splinting with the proximal interphalangeal joint
Explanation:
Disruption of the central slip of the extensor tendon at the PIP joint with volar migration of the lateral bands will result in the so-called boutonniere deformity, which includes loss of extension at the PIP joint and compensatory hyperextension at the DIP joint. The lesion is most often secondary to closed blunt trauma with acute forceful flexion at the PIP joint. This produces avulsion of the central slip from its insertion on the dorsal base of the middle phalanx with or without fracture and/or laceration of the extensor tendon at its insertion. In closed injuries the characteristic boutonniere deformity may not be apparent at the time of injury and may not be noted until 10 to 21 days after injury. Two diagnostic tests that are useful in early recognition of this lesion are: (1) a 15 deg to 20 deg or greater loss of active extension of the PIP joint when the wrist and MP joint are fully flexed and (2) extravasation of intraarticular radiopaque dye dorsal and distal to the PIP joint. Weak extension against resistance has also been noted to be a helpful diagnostic finding. Treatment in acute cases before fixed contractures have occurred may be achieved by progressively splinting the PIP joint into full extension and at the same time performing active and passive flexion exercises of the DIP joint. In a closed boutonniere deformity operative intervention is indicated under two circumstances. (1) when the central slip has been avulsed with a bone fragment which is lying free over the PIP joint and (2) a long-standing boutonniere deformity in a young person.
Question 4:
Osteoporotic vertebral compression fractures are associated with
Options:
- neurologic deterioration in 33% of patients.
- osteomalacia in 50% of patients.
- a further fracture risk rate of 20%.
- chronic pain in 75% of patients.
- a 2-year mortality rate that is less than that associated with hip fractures.
Correct Answer: a further fracture risk rate of 20%.
Explanation:
DISCUSSION: Osteoporotic vertebral compression fractures are associated with neurologic complications in less than 1% of patients. After the initial fracture however, patients have a 20% risk of further fractures. The mortality rate of patients with vertebral fractures exceeds that of patients with hip fractures when they are followed beyond 6 months.
REFERENCES: Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Lindsay R, Silverman SL, Cooper C, et al: Risk of new vertebral fracture in the year following a fracture. JAMA 2001;285:320-323.
Kado DM, Duong T, Stone KL, et al: Incident vertebral fractures and mortality in older women: A prospective study. Osteoporos Int 2003;14:589-594.
Question 5:
Sclerostin and dickkopf-1 (Dkk-1) are direct inhibitors of what pathway related to bone and/or cartilage regulation?
Options:
- Bone morphogenetic protein (BMP)/SMAD pathway
- Receptor activator of nuclear factor kappa beta (RANK)/RANK ligand (RANKL) pathway
- Wnt/Beta-catenin (β-catenin) pathway
- Parathyroid hormone (PTH) pathway DISCUSSION.Dkk-1 and sclerostin are proteins that inhibit the binding of the Wnt molecule to receptors LRP5/6. In the absence of sclerostin and Dkk-1, Wnt binds to its receptor, which in turn inhibits phosphorylation of the β-catenin. The unphosphorylated β-catenin then builds up in the cytoplasm of the cell, allowing it to be transported to the nucleus of the cell. Once in the nucleus, β-catenin will lead to upregulation of a series of proteins involved in osteoblast formation differentiation. Knocking out or inhibiting sclerostin or Dkk-1 results in increased bone mass secondary to constitutive activation of the Wnt/β-catenin pathway.The other responses are not directly affected by Dkk-1 or sclerostin. RANKL and RANK are expressed on osteoblasts and osteoclasts, respectively, and are involved in osteoblast-mediated osteoclast activation.BMPs work through SMADs to cause osteoblastic differentiation, and there is reported crosstalk between the Wnt and BMP pathways (but this is an indirect link). Finally, PTH at physiologic levels binds to osteoblasts, causing a series of events that lead to osteoblast-mediated osteoclast activation and subsequent increased bone resorption.
Correct Answer: Wnt/Beta-catenin (β-catenin) pathway
Explanation:
RESPONSES FOR QUESTIONS 3 THROUGH 6
Adhesive wear
Abrasive wear
Fatigue wear
Delamination
For each scenario below, please choose the most likely dominant mechanism of wear from the list
above.
Question 6:
The usual presentation of traumatic subscapularis tears is most often seen after forced
Options:
- internal rotation.
- external rotation.
- extension.
- abduction.
- forward flexion.
Correct Answer: external rotation.
Explanation:
DISCUSSION: The typical mechanism of injury is a fall and the patient grasps something to prevent the fall. This maneuver forces the arm into external rotation against resistance.
REFERENCES: Kreuz PC, Remiger A, Erggelet C, et al: Isolated and combined tears of the subscapularis tendon. Am J Sports Med 2005;33:1831-1837.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 7:
A 42 year-old-woman who underwent surgery for lumbar scoliosis 2 years ago now has fixed sagittal plane imbalance and severe back pain. Which of the following is considered a contraindication to isolated pedicle subtraction osteotomy for the treatment of iatrogenic flatback syndrome in this patient?
Options:
- Anterior pseudarthrosis
- Prior laminectomy at the osteotomy level
- Sagittal decompensation of more than 20 cm on standing lateral radiographs
- Kyphosis at the thoracolumbar junction
- Vascular calcification at the osteotomy site
Correct Answer: Anterior pseudarthrosis
Explanation:
DISCUSSION: Pedicle subtraction osteotomy is the preferred osteotomy technique for the treatment of many patients with iatrogenic flatback syndrome. In the presence of an anterior pseudarthrosis, however, it must be done in conjunction with an anterior procedure. Prior laminectomy is not a contraindication. Significant correction, usually averaging about 30°, can be obtained through each osteotomy. Osteotomies should be performed at L2 or below in the presence of kyphosis at the thoracolumbar junction. The pedicle subtraction technique is preferred with vascular calcifications because it does not lengthen the anterior column, which could risk vascular injury.
REFERENCES: Potter BK, Lenke LG, Kuklo TR: Prevention and management of iatrogenic flatback deformity. J Bone Joint Surg Am 2004;86:1793-1808.
Bridwell KH, Lenke LG, Lewis SJ: Treatment of spinal stenosis and fixed sagittal imbalance. Clin Orthop 2001;384:35-44.
Question 8:
A 23-year-old man reports a 6-year history of recurrent instability in the right dominant shoulder. He has not undergone surgery and has essentially stopped all of his sporting activities. On examination, he has instability and apprehension in the midrange of motion (abduction of 45 to 60 degrees with external rotation) and a palpable clunk representing a transient dislocation over the anterior glenoid rim. A three-dimensional CT scan is shown in Figure 31. What is the most appropriate surgical intervention to provide him with reliable stability postoperatively? Review Topic
Options:
- Arthroscopic Bankart surgery
- Bony glenoid augmentation procedure
- Subscapularis advancement
- Open capsular shift
- Hemiarthroplasty
Correct Answer: Bony glenoid augmentation procedure
Explanation:
In the setting of significant anteroinferior glenoid bone deficiency (greater than 20% to 25%), both open and arthroscopic Bankart repairs have demonstrated higher rates of failure. Bony glenoid augmentation procedures such as the Bristow-Latarjet, which describe coracoid transfers to reconstruct the deficient glenoid, have led to decreased rates of recurrent shoulder instability. In this scenario, the patient has a significant loss of glenoid bone. There are also several clues in the history to suspect bone deficiency: multiple recurrences, a long history of recurrence, and instability in the midranges of motion. A bony augmentation procedure such as the Latarjet has been well-described to provide a well functioning and stable shoulder joint. A hemiarthroplasty is not indicated in the absence of arthritis. Subscapularis advancement will not address the bone loss.
Question 9:
What is the preferred treatment of displaced distal clavicle fractures in children less than eight years old?
Options:
- Closed reduction and pinning of the fracture
- Open reduction and plating
- Sling immobilization
- Coracoclavicular ligament reconstruction
- Open reduction and suture fixation
Correct Answer: Closed reduction and pinning of the fracture
Explanation:
DISCUSSION: Pediatric distal clavicle fractures are typically treated non-operatively because of the great osteogenic capacity of the intact inferior periosteum. The coracoclavicular ligaments remain attached to the periosteum and new bone fills any remaining bony gaps within the periosteal sleeve. Recent articles by Nenopoulos et al recommend sling immobilization for the majority of fractures (84%) and only attempt surgical fixation for children >8 years old with severely displaced fractures (>2 cortical diameters). They found excellent function with conservative treatment and union in all fractures. Surgical care resulted in improved cosmetic appearance.
Question 10:
Figure 7 shows the CT scan of a 25-year-old soccer player who has had posterior ankle pain with plantar flexion for the past 2 years. Immobilization has failed to provide relief. He is ambulatory. Management should consist of
Options:
- a local steroid injection into the flexor hallucis longus tendon sheath.
- range-of-motion exercises.
- open reduction and internal fixation.
- nonsteroidal anti-inflammatory drugs.
- excision of the fragment.
Correct Answer: excision of the fragment.
Explanation:
DISCUSSION: An os trigonum is usually asymptomatic, but this accessory bone has been associated with persistent posterior ankle pain, which has been described as os trigonum syndrome. This usually affects athletes and ballerinas. Forced plantar flexion leads to impingement of the os trigonum against the posterior tibial plafond, and flexor hallucis tendinitis may develop. It may be difficult to differentiate a fractured trigonal process from the os trigonum. MRI may reveal bone marrow edema that may aid in the diagnosis of os trigonum syndrome. Steroid injections may lead to tendon rupture. The results of excision of a symptomatic os trigonum through a posteromedial or lateral approach are favorable, with a rapid return to full function. The main complication of this procedure is sural nerve injury with a lateral approach.
REFERENCES: Hedrick MR, McBryde AM: Posterior ankle impingement. Foot Ankle Int 1994;15:2-8.
Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Question 11:
Duchenne’s muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?
Options:
- X-linked
- Autosomal-dominant
- Autosomal-recessive
- Chromosomal duplication
- Chromosomal deletion
Correct Answer: X-linked
Explanation:
DISCUSSION: Patients with Duchenne’s muscular dystrophy show progressive muscular weakness because of the absence of dystrophin and have the clinical picture of progressive muscle weakness. The condition is an X-linked genetic disease.
REFERENCES: Fitzgerald RH, Kaufer H, Malkani AL: Orthopaedics. St Louis, MO, Mosby Year Book, 2002, pp 1573-1583.
Smith SA, Swaiman HF: Muscular dystrophies, in Swaiman KF, Ashwall S (eds): Pediatric Neurology Principles and Practice, ed 3. St Louis, MO, Mosby, 1999, pp 1235-1237.
Question 12:
The spinal cord terminates as the conus medullaris at what vertebral level in adults? Review Topic 1 T12
Options:
Correct Answer: L2
Explanation:
The spinal cord anatomy changes at the thoracolumbar junction. The spinal cord terminates as the conus medullaris at the lower portion of L1 in women and the pedicle of L1 in men.
Question 13:
- A 50-year-old alcoholic man has erythema and swelling in his entire dominant upper extremity. He has a WBC of 15,000/mm3, a temp of 101 oF (38.3 oC), and a blood pressure of 90/60 mm Hg. After hemodynamic stabilization, the cellulitic forearm is longitudinally incised dorsally and volarly. The forearm muscles are normal in appearance; however, the subcutaneous fat is necrotic. A culture will most likely reveal
Options:
- Bacteroides
- coli
- Staph. aureus
- group A streptococcus
- Clostridium perforingens
Correct Answer: group A streptococcus
Explanation:
Necrotizing fasciitis is frequently caused by strep infections. Cellulitis, which is an inflammatory infection of the subcutaneous tissues, is usually due to Staph or Strep infections (Haemophilus is also seen in children). Significant Streptococcal infections include erysipelas, which produces a progressively enlarging red, raised painful plaque, severe toxicity, fever, leukocytosis and bacteremia; Necrotizing fasciitis produces XXXXX. Clostridium perforingens typically causes gas gangrene (which can also develop from gram neg. and strep infections), presenting as progressive pain, distal edema, and a malodorous serosanguinous discharge.
Question 14:
What is the most common primary malignant tumor of bone in childhood?
Options:
- Periosteal chondroma
- Ewing’s sarcoma
- Osteosarcoma
- Chondrosarcoma
- Rhabdomyosarcoma
Correct Answer: Osteosarcoma
Explanation:
DISCUSSION: Osteosarcoma is the most common primary malignant tumor of bone in childhood, followed by Ewing’s sarcoma. Rhabdomyosarcoma is a soft-tissue sarcoma of childhood. Chondrosarcoma rarely occurs in childhood. Osteochondromas are benign tumors of the bone.
REFERENCES: Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 226.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 15:
-A 42-year-old man has increasing pain and, to a lesser extent, some occasional left knee instability.Several years earlier he sustained a noncontact twisting injury to his knee. He had some initial soreness and pain but was able to resume his normal activities while avoiding sports. On examination, the patient has medial joint line pain, a grade 2+ Lachman, and a slight varus thrust. His radiographs reveal mild-tomoderate medial compartment osteoarthritis with varus alignment. What surgical treatment strategy likely will alleviate his pain?
Options:
- Distal femoral osteotomy
- Unicompartmental knee replacement
- High tibial osteotomy (HTO), lateral closing wedge
- HTO, medial opening wedge with decreased tibial slope DISCUSSION-This patient had a previous anterior cruciate ligament (ACL) and posterolateral complex injury. With chronic instability and osteoarthritis, the best option is HTO with a decrease in the tibial slope to reduce anterior laxity. Distal femoral osteotomy is better suited to address valgus malalignment. The lateral closing-wedge osteotomy would not allow for adequate correction of the tibial slope. Unicompartmental knee replacement is not indicated when there is ligament instability. If the patient continues to experience instability following correction of the varus malalignment, reconstruction of the ACL and posterolateral corner would be appropriate at that time.
Correct Answer: HTO, medial opening wedge with decreased tibial slope DISCUSSION-This patient had a previous anterior cruciate ligament (ACL) and posterolateral complex injury. With chronic instability and osteoarthritis, the best option is HTO with a decrease in the tibial slope to reduce anterior laxity. Distal femoral osteotomy is better suited to address valgus malalignment. The lateral closing-wedge osteotomy would not allow for adequate correction of the tibial slope. Unicompartmental knee replacement is not indicated when there is ligament instability. If the patient continues to experience instability following correction of the varus malalignment, reconstruction of the ACL and posterolateral corner would be appropriate at that time.
Explanation:
RESPONSES FOR QUESTIONS 69 THROUGH 71
Bone-patella tendon-bone autograft (10 mm)
Soft-tissue allograft (8 mm)
Quadruple hamstring autograft (10 mm)
For each of the following, please select the preferred response from the choices above.
Question 16:
Figure 17 shows the radiograph of an 11-year-old boy with Duchenne muscular dystrophy who has been nonambulatory for the past 2 years. Management of the spinal deformity should consist of
Options:
- wheelchair modifications and custom-molded inserts.
- posterior fusion with instrumentation.
- anterior and posterior fusion.
- observation and reexamination in 6 months.
- thoracolumbosacral orthosis bracing.
Correct Answer: posterior fusion with instrumentation.
Explanation:
DISCUSSION: The presence of any curve greater than 20 degrees in a nonambulatory patient with Duchenne muscular dystrophy is an indication for posterior fusion with instrumentation. Because of progressive cardiomyopathy and pulmonary deficiency, waiting until the curve is larger can increase the risk of pulmonary or cardiac complications during or following surgery. There is some disagreement as to whether all such fusions must extend to the pelvis. Bracing or other nonsurgical management is ineffective and is not indicated in this situation.
REFERENCES: Sussman M: Duchenne muscular dystrophy. J Am Acad Orthop Surg 2002;10:138-151.
Mubarek SJ, Morin WD, Leach J: Spinal fusion in Duchenne muscular dystrophy: Fixation and fusion to the sacropelvis? J Pediatr Orthop 1993;13:752-757.
Question 17:
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. If present, what is the most likely complication after surgical treatment in this scenario?
Options:
- Recurrent instability
- Degenerative joint disease
- Shoulder stiffness
- Axillary nerve injury
Correct Answer: Shoulder stiffness
Explanation:
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through, as seen in this patient. The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion, at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The four muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the four rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation. This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Beighton sign findings would be negative), a posterior capsular shift with rotator interval closure is indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate. The most common complication seen after arthroscopic posterior labral repair is stiffness, followed by recurrent instability
and degenerative joint disease.
Question 18:
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?
Options:
- pulselessness
- palor
- paresthesia
- paralysis
- increasing analgesia requirement
Correct Answer: pulselessness
Explanation:
DISCUSSION: Although pain, pallor, paresthesia, paralysis, and pulselessness are all possible signs and symptoms of compartment syndrome in children with fractures, studies have shown increasing analgesia requirement is more sensitive.
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
Question 19:
A 10-year-old boy who is active in soccer has had activity-related heel pain for the past 3 months. Examination reveals tenderness over the posterior heel and a tight Achilles tendon. Radiographs demonstrate a 2-cm cyst in the anterior body of the calcaneus. His physes have not closed. Based on these findings, what is the most appropriate management?
Options:
- Bone scan
- Curettage and bone grafting of the cyst
- Cast immobilization
- Observation with reduced activity
- Skeletal survey
Correct Answer: Observation with reduced activity
Explanation:
DISCUSSION: The most likely diagnosis is Sever’s disease, which is considered either an apophysitis or a para-apophyseal stress fracture. It is common in athletic children and is associated with a tight Achilles tendon. Cast immobilization may be necessary if activity reduction fails. Calcaneal cysts are quite common and do not require any further diagnostic testing or treatment unless they occupy the full width of the calcaneus or one third of the length of the calcaneus.
REFERENCES: Ogden JA, Ganey TM, Hill JD, et al: Sever’s injury: A stress fracture of the immature calcaneal metaphysis. J Ped Orthop 2004;24:488-492.
Pogoda P, Priemel M, Linhart W, et al: Clinical relevance of calcaneal bone cysts: A study of 50 cysts in 47 patients. Clin Orthop Relat Res 2004;424:202-210.
Question 20:
A patient undergoes the procedure shown in Figure A. This patient is most likely to be Review Topic
Options:
- year-old man with subtalar arthritis
- year-old girl with congenital vertical talus
- year-old male with talocalcaneal coalition involving less than 50% of middle facet and hindfoot valgus
- year-old male with cavovarus foot and Charcot-Marie-Tooth disease
- year-old male with equinovalgus foot and spastic diplegic cerebral palsy
Correct Answer: year-old man with subtalar arthritis
Explanation:
The procedure shown is subtalar arthroereisis. It is used as an adjunct spacer/distractor following tarsal coalition excision if hindfoot valgus remains following resection.
In the pediatric population, arthroereisis is one option to restore the alignment of the hindfoot after talocalcaneal coalition. Hindfoot deformity correction is required because resection of the coalition alone will often increase the hindfoot valgus
deformity. The arthroereisis implant prevents this valgus collapse. Another alternative to correct the hindfoot valgus deformity is a calcaneal lateral column lengthening osteotomy.
Khoshbin et al. reviewed the long-term outcomes of coalition resection in 24 patients (32 coalitions). Resected talocalcaneal (TC) coalitions had less inversion/eversion postoperatively than resected calcaneonavicular (CN) coalitions but there was no difference in outcome scores. They obtained favorable results when even resecting talocalcaneal coalition with >50% involvement of the middle facet and hindfoot valgus angles >16 °, which were considered historical contraindications to resection.
Zaw et al. reviewed tarsal coalitions. Radiographic signs of CN coalition include the anteater sign (elongated anterior calcaneal process), decreased CN gap, reverse anteater sign (elongated lateral navicular) and hypoplastic lateral talar head. Radiographic signs of TC coalition include obliterated middle facet on a Harris view (osseous coalition), irregular cortices/dysplastic sustentaculum tali on a Harris view (nonosseous), C-sign on a lateral view, talar beaking, short talar neck with concave inferior surface, narrow posterior facet, and non-visibility of the middle facet.
Giannini et al. reviewed subtalar arthroereisis with coalition resection in 14 feet in patients aged 9-18 years. They achieved 57% excellent, 21% good and 21% fair results. Regarding pain, 86% had improvement and 14% had no change. Regarding ROM, 93% had improvement, and 7% had no change. Better scores were seen in patients <14 years.
Figure A shows the implantation of an arthroereisis implant in the sinus tarsi. Illustration A comprises coronal CT images of talocalcaneal coalition.
Incorrect Answers:
Question 21:
In the anterior cruciate ligament (ACL)-deficient knee, which of the following variables has the highest correlation with the development of arthritis?
Options:
- Duration of time since the injury
- Patient age
- Additional ligament injury
- Degree of laxity
- Meniscal integrity
Correct Answer: Meniscal integrity
Explanation:
DISCUSSION: Ample evidence supports an increased rate of degenerative arthritis in the ACL-deficient knee. Several variables play a role in the development of the arthritis, but the integrity of the meniscus has been shown to be the single most important factor.
REFERENCES: O’Brien WR: Degenerative arthritis of the knee following anterior cruciate ligament injury: Role of the meniscus. Sports Med Arthroscopy Rev 1993;1:114-118.
Fetto JF, Marshall JL: The natural history and diagnosis of anterior cruciate ligament insufficiency. Clin Orthop 1980;147:29-38.
McDaniel WJ Jr, Dameron TB Jr: The untreated anterior cruciate ligament rupture. Clin Orthop 1983;172:158-163.
Question 22:
For halo traction, what is the preferred site for anterior pin placement?
Options:
- Below the head equator, above the supraorbital ridge, and 3.5 cm lateral to the midline
- Below the head equator, above the supraorbital ridge, and 4.5 cm lateral to the midline
- Below the head equator, below the supraorbital ridge, and 4.5 cm lateral to the midline
- Above the head equator, above the supraorbital ridge, and 3.5 cm lateral to the midline
- Above the head equator, above the supraorbital ridge, and 4.5 cm lateral to the midline
Correct Answer: Below the head equator, above the supraorbital ridge, and 4.5 cm lateral to the midline
Explanation:
DISCUSSION: The safe zone for anterior halo pin insertion is marked laterally by the anterior border of the temporalis muscle (to avoid penetration of this muscle and relative thin cortex of the skull). Medially, the pin should be placed 4.5 cm lateral to the midline to avoid injury to the supraorbital nerve or the frontal sinus. The safe area is marked superiorly by the head equator to avoid cephalad migration of the pin and inferiorly by the supraorbital ridge to prevent displacement or penetration into the orbit.
REFERENCE: Ebraheim NA, Lu J, Biyani A, Brown JA: Anatomic considerations of halo pin placement. Am J Orthop 1996;25:754-756.
Question 23:
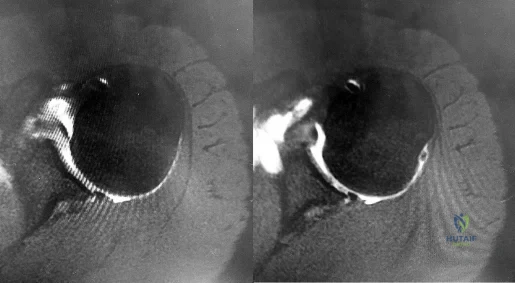
If the site of the pathologic lesion is revealed in Figure 54f and not in Figure 54e after traumatic anterior shoulder dislocation, the mechanism of shoulder injury is likely
Options:
- axial loading of the glenohumeral joint.
- isolated hyperabduction.
- combined 45-degree abduction and external rotation.
- combined hyperabduction and external rotation.
Correct Answer: combined hyperabduction and external rotation.
Explanation:
DISCUSSION
For patients with anterior shoulder instability, most commonly, a Bankart lesion, or detachment of the anteroinferior labrum with the attached inferior glenohumeral ligament from the glenoid rim is found. A medialized anteroinferior capsulolabral attachment (ALPSA lesion) is a common finding in shoulders with chronic anterior instability. The anterior band of the inferior glenohumeral ligament is tightest with the arm in 90 degrees of abduction with the shoulder externally rotated, creating a “hammock” that supports the humeral head. At 45 degrees of shoulder
abduction, the capsuloligamentous components of the shoulder are at their loosest, resulting in the most total superior-inferior translation.
During traumatic anterior glenohumeral dislocation, associated injuries commonly occur. In a prospective database of 3633 patients who sustained a traumatic anterior glenohumeral dislocation, 13.5% had a neurologic deficit following reduction, the majority of which were injuries to the axillary nerve. The injuries typically were sensory but not motor deficits and resolved spontaneously over time. These isolated axillary nerve injuries were more common in young, athletic patients. Associated rotator cuff tears and greater tuberosity fractures are commonly associated with shoulder dislocation as well and are more common in patients 60 years of age and older.
Large, engaging posterior humeral head Hill-Sachs lesions are associated with increased rates of recurrent shoulder instability. At the time of surgical arthroscopy, the Hill-Sachs lesion should be assessed for engagement with the glenoid. In the absence of significant glenoid bone loss, some patients with engaging Hill-Sachs defects may be suitable for combined Bankart repair and Hill-Sachs remplissage at the time of surgery. When these procedures are combined, patients have an approximate 10-degree decreased shoulder external rotation with the arm at the side and in abduction when compared to the contralateral, uninjured shoulder. Rates of recurrent dislocation and return to sport are comparable to those for patients undergoing Bankart repair alone.
Humeral avulsion of the glenohumeral ligaments (HAGL) has become a well-recognized cause of recurrent shoulder instability and is reported in 1% to 9% of patients. HAGL lesions can occur in isolation or, more commonly, may be associated with other abnormalities such as a tear of the rotator cuff, Bankart lesion, Hill-Sachs deformity, or labral tear. Recurrence of shoulder instability is more likely to occur if there is failure to identify a HAGL lesion. HAGL lesions can result from trauma in the setting of combined hyperabduction and external rotation. This is in contrast to a Bankart lesion, which is a result of trauma when the shoulder is hyperabducted without substantial associated rotation.
RECOMMENDED READINGS
Warner JJ, Deng XH, Warren RF, Torzilli PA. Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med. 1992 Nov-Dec;20(6):675-85. PubMed PMID: 1456361.
View Abstract at PubMed
Robinson CM, Shur N, Sharpe T, Ray A, Murray IR. Injuries associated with traumatic anterior glenohumeral dislocations. J Bone Joint Surg Am. 2012 Jan 4;94(1):18-26. doi: 10.2106/JBJS.J.01795. PubMed PMID: 22218378.
View Abstract at PubMed
Visser CP, Coene LN, Brand R, Tavy DL. The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery. A prospective clinical and EMG study. J Bone Joint Surg Br. 1999 Jul;81(4):679-85. PubMed PMID: 10463745.
View Abstract at PubMed
Boileau P, O'Shea K, Vargas P, Pinedo M, Old J, Zumstein M. Anatomical and functional results after arthroscopic Hill-Sachs remplissage. J Bone Joint Surg Am. 2012 Apr 4;94(7):618-26. doi: 10.2106/JBJS.K.00101. PubMed PMID: 22488618.
View Abstract at PubMed
Bui-Mansfield LT, Banks KP, Taylor DC. Humeral avulsion of the glenohumeral ligaments: the HAGL lesion. Am J Sports Med. 2007 Nov;35(11):1960-6. Epub 2007 Apr 9. Review. PubMed PMID: 17420506.
View Abstract at PubMed
Question 24:
An obese (BMI = 35) 72-year-old woman with diabetes mellitus, hyptertension and a 22-pack-year smoking history is scheduled to undergo posterior spinal fusion from T10 to S1 with a pedicle subtraction osteotomy at L3 for the spinal deformity seen in Figure 1. Which of the following risk factors is most predictive of major complication following surgery Review Topic
Options:
- Age > 60 years
- > or = 2 comorbid conditions
- History of tobacco use
- BMI > 30 kg/m²
- Using a pedicle subtraction osteotomy
Correct Answer: > or = 2 comorbid conditions
Explanation:
The patients age (> 60 years) is the most significant risk factor for a major perioperative complication during posterior spinal fusion for adult spinal deformity correction.
The surgical treatment of adult spinal deformity often requires multilevel arthrodesis with complex osteotomies including three column osteotomies such as pedicle
subtraction (PSO) and vertebral column resection (VCR). They can involve both anterior and posterior surgical approaches. Surgical time, blood loss, length of hospital stay, and length of recovery can be greater than it is for the more common degenerative conditions.
Auerbach et al. characterized the risk factors for the development of major complications in patients undergoing 3-column osteotomies for adult spinal deformity correction. They also aimed to determine whether the presence of complications affected the ultimate clinical outcome. They found age > 60 years, > or = 3 comorbid conditions and preoperative sagittal imbalance of = 40mm was associated with a major complication. However, the presence of a major complication did not affect the ultimate clinical outcomes at 2 years or more.
Daubs et al. conducted a retrospective analysis of forty-six patients = 60 years of age who underwent major spinal deformity surgery requiring a minimum 5-level arthrodesis procedure to determine the rate of complication and outcomes. The overall complication rate was 37% and the major complication rate was 20%. Increasing age was a significant factor (p<0.05) in predicting the presence of a complication, while presence of comorbidities was found to have no association.
Figure A is a standing preoperative lateral radiograph of the spine demonstrating a thoracic kyphosis of ~25° and thoracolumbar kyphosis of ~25°. Illustration A demonstrates proper sagittal balance after spinal fusion from T10 to S1 and L3 PSO.
Incorrect Answers:
Question 25:
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?
Options:
- CT
- Limited bone scan
- MRI
- Joint aspiration
- Functional capacity examination
Correct Answer: MRI
Explanation:
DISCUSSION: Based on these findings, the most likely diagnosis is a rotator cuff injury and probable tear; therefore, MRI is the study of choice. CT is preferred for articular fractures. A bone scan is nonspecific and can identify inflammation or occult fracture. Joint aspiration is not likely to identify an effusion. Physical therapy and a functional capacity examination are used to identify weakness during recovery prior to a return to work or sports.
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 26:
When considering a flexor digitorum longus tendon transfer as part of the surgical treatment in patients with symptomatic flatfoot deformity caused by posterior tibial tendon insufficiency, which of the following patients is the most appropriate candidate?
Options:
- A 45-year-old woman with a hypermobile foot
- A 45-year-old man with a rigid hindfoot valgus deformity
- A thin 55-year-old woman with mild hemiparesis affecting the symptomatic foot from a previous stroke
- An active 55-year-old woman with a progressively worsening supple hindfoot valgus
- A moderately obese 70-year-old woman with a supple hindfoot
Correct Answer: An active 55-year-old woman with a progressively worsening supple hindfoot valgus
Explanation:
DISCUSSION: Transfer of the flexor digitorum longus tendon is a common technique combined with other procedures to treat patients with posterior tibial tendon insufficiency. However, it is contraindicated in patients with a fixed hindfoot deformity, hypermobility, or neuromuscular compromise. It is relatively contraindicated in patients who are obese, and those older than age 60 to 70 years.
REFERENCES: Pedowitz WJ, Kovatis P: Flatfoot in the adult. J Am Acad Orthop Surg 1995;3:293-302.
Mann RA: Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 167-296.
Question 27:
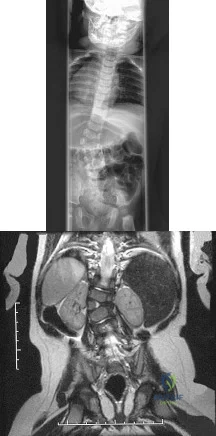
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show
Options:
- an elevated thyroid-stimulating hormone level.
- an elevated estrogen level.
- elevated blood urea nitrogen and creatinine levels.
- a growth hormone deficiency.
- normal laboratory values.
Correct Answer: normal laboratory values.
Explanation:
DISCUSSION: The patient has a slipped capital femoral epiphysis (SCFE) at a younger than average age (average age 13.5 years for boys and 12.0 years for girls); therefore, an etiology that is not idiopathic must be considered. Hypothyroidism can result in a SCFE, but these children typically fall into the category of less than the 10th percentile for height. SCFE may develop in children with a growth hormone deficiency who have undergone hormonal replacement. Osteodystrophy caused by chronic renal failure may result in a SCFE, but the bone quality is markedly osteopenic on radiographs and the children are chronically ill with both low height and weight percentiles. An elevated estrogen level results in physeal closure and is protective to physeal slippage. Therefore, this child will most likely have normal laboratory values.
REFERENCES: Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Question 28:
When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more than the extension space?
Options:
- Iliotibial band
- Popliteus tendon
- Lateral collateral ligament
- Lateral head of the gastrocnemius
Correct Answer: Popliteus tendon
Explanation:
DISCUSSION:
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point,
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 29:
A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Initial treatment should consist of
Options:
- early mobilization only.
- surgical reconstruction of medial and lateral collateral ligaments.
- active motion in a hinged brace from 30° to 120°.
- application of hinged external fixator with early mobilization.
Correct Answer: early mobilization only.
Explanation:
This is a simple (no associated fracture) elbow dislocation. Such dislocations can be treated with closed reduction followed by mobilization after 5 to 7 days to avoid stiffness, provided the elbow is stable through a full arc of motion at the time of reduction. If the elbow is unstable but has a short arc of stability, then using a hinged brace in the stable arc may be considered. (Note: It may be necessary to splint the elbow in pronation if the medial collateral ligament [MCL] is intact and the lateral collateral ligament [LCL] is disrupted, or in supination if the LCL is intact but the MCL disrupted.) Surgical reconstruction of the LCL and MCL may be required only if the elbow does not have a stable arc at the time of reduction. If unstable after reconstruction,
application of a hinged external fixator may be considered.
Question 30:
Which of the following statements most accurately describes the layers of articular cartilage?
Options:
- The superficial zone has condensed proteoglycan and sparse collagen.
- The intermediate zone transition is the thinnest layer and the chondrocytes are oriented tangentially.
- The basal zone (middle, radial, deep) contains flattened chondrocytes.
- Tidemark is found only in joints and not in the growing cartilage cap of an enchondroma.
- Tidemark is more prominent in newborn joints.
Correct Answer: Tidemark is found only in joints and not in the growing cartilage cap of an enchondroma.
Explanation:
DISCUSSION: Normal articular cartilage is composed of three zones that are based on the shape of the chondrocytes and the distribution of the type II collagen. The tangential zone has flattened chondrocytes, condensed collagen fibers, and sparse proteoglycan. The intermediate zone is the thickest layer with round chondrocytes oriented in perpendicular or vertical columns paralleling the collagen fibers. The basal layer is deepest with round chondrocytes. The tidemark is deep to the basal layer and separates the true articular cartilage from the deeper cartilage that is a remnant of the cartilage anlage, which participated in endochondral ossification during longitudinal growth in childhood. The tidemark divides the superficial uncalcified cartilage from the deeper calcified cartilage and also is the division between nutritional sources for the chondrocytes. The tidemark is the zone in which chondrocyte renewal took place in childhood. The tidemark is found only in joints and not in the cap of an enchondroma. It is seen most prominently in the adult, nongrowing joint.
REFERENCE: Schiller AL: Pathology of osteoarthritis, in Kuettner KE, Goldberg VM (eds): Osteoarthritic Disorders. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995,
pp 95-101.
Question 31:
Type II collagen in nondiseased adult human articular cartilage has a half-life that is generally
Options:
- several months.
- 6 months.
- 1 year.
- 10 years.
- more than 25 years.
Correct Answer: more than 25 years.
Explanation:
DISCUSSION: Type II collagen in articular cartilage is amazingly stable. This is important to know because matrix homeostasis generally is associated with minimal synthesis and degradation of type II collagen. Passive glycation has a consistent rate and occurs over decades. The relative amount of glycation in cartilage with age has been used as a measure of stability. Also, the rate of racemization of aspartic acid from the L to D form occurs spontaneously at a very slow rate. The relative stability of collagen can be estimated by calculating the percentage of D aspartic acid per dry weight of type II collagen.
REFERENCES: Maroudas A, Palla G, Gilav E: Racemization of aspartic acid in human articular cartilage. Connect Tissue Res 1992;28:161-169.
Verzijl N, DeGroot J, Thorpe SR, et al: Effect of collagen turnover on the accumulation of advanced glycation end products. J Biol Chem 2000;275:39027-39031.
Question 32:
Fixed hyperextension of the metatarsophalangeal joint is associated with
Options:
- dorsal subluxation of the interossei.
- dorsal subluxation of the lumbricals.
- fibrosis of the plantar plate.
- attenuation of the extensor longus tendon.
- extrinsic flexor paralysis.
Correct Answer: dorsal subluxation of the interossei.
Explanation:
DISCUSSION: Claw toe and hammer toe deformities are associated with dorsal subluxation of the interossei, which can no longer serve to flex the metatarsophalangeal joint. The extensor digitorum longus then loses its tenodesing effect on the proximal interphalangeal and distal interphalangeal joints and works unopposed to extend the metatarsophalangeal joint and the proximal phalanx. Without the antagonistic action of the extensor digitorum longus, the extrinsic flexors become unopposed flexors of the proximal and distal interphalangeal joints.
REFERENCES: Marks RM: Anatomy and pathophysiology of lesser toe deformities. Foot Ankle Clin 1998;3:199-213.
Myerson MS, Shereff MJ: The pathological anatomy of claw and hammer toes. J Bone Joint Surg Am 1989;71:45-49.
Question 33:
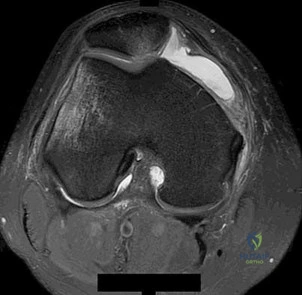
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Options:
- The flexor digitorum longus tendon is ruptured.
- The posterior tibial tendon has a normal appearance.
- The posterior tibial tendon has a physiologic amount of fluid in its sheath.
- The posterior tibial tendon is completely ruptured and retracted (type III tear).
- The posterior tibial tendon has a chronic longitudinal split with enlargement (type II tear).
Correct Answer: The posterior tibial tendon has a chronic longitudinal split with enlargement (type II tear).
Explanation:
DISCUSSION: The MRI scans reveal an enlarged posterior tibial tendon, with degenerative signal within the tendon and an excessive amount of fluid in its sheath. This is a type II tear, as noted by Conti and associates, which is the most commonly seen tear.
REFERENCES: Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 34:
Following ankle arthroscopy performed through a posterolateral portal, a patient notes numbness on the lateral half of the heel pad of the foot. What is the most likely injured structure?
Options:
- Sural nerve
- Lateral plantar nerve
- Lateral calcaneal nerve
- First branch of the lateral plantar nerve
- Deep peroneal nerve
Correct Answer: Lateral calcaneal nerve
Explanation:
DISCUSSION: The lateral calcaneal nerve is a branch of the sural nerve that runs along the lateral border of the Achilles tendon to innervate the lateral heel pad. Ankle arthroscopy involves posterior portals that hug the Achilles tendon to avoid the main trunks of the sural nerve and tibial nerve; however, the lateral calcaneal branch remains potentially vulnerable. The first branch of the lateral plantar nerve is actually a medial structure that partially innervates the plantar fascia and the abductor digiti quinti. The deep peroneal nerve is anterior to the ankle.
REFERENCES: Sitler DF, Amendola A, Bailey CS, et al: Posterior ankle arthroscopy:
An anatomic study. J Bone Joint Surg Am 2002;84:763-769.
Sarrafian SK: Anatomy of the Foot and Ankle, Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, p 361.
Question 35:
Figures 31a and 31b show the radiograph and MRI scan of an otherwise normal 3-month-old infant who has a spinal deformity. MRI reveals no intraspinal anomalies. What is the next step in management? Review Topic
Options:
- Posterior spinal fusion with instrumentation
- Anterior-posterior hemiepiphysiodesis
- Brace management
- Cardiac and renal evaluation
- Hemivertebrectomy and fusion
Correct Answer: Cardiac and renal evaluation
Explanation:
Congenital scoliosis in an infant warrants evaluation of the renal, cardiac, and neurologic systems because frequently there is concurrent pathology. Progression in this instance is possible but not certain; therefore, progression must be documented prior to any surgical intervention. Close observation with serial radiographs every 4 to 6 months is appropriate. All of the surgical options listed may be reasonable choices in the future, but cardiac evaluation is the most important issue at this time.
Question 36:
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Options:
- Superior ulnar collateral
- Inferior ulnar collateral
- Posterior ulnar recurrent
- Brachial
- Ulnar
Correct Answer: Inferior ulnar collateral
Explanation:
DISCUSSION: The superior ulnar collateral, inferior ulnar collateral, and posterior ulnar recurrent arteries provide consistent vascular supply to the ulnar nerve. This supply is segmental in nature. No identifiable direct anastomosis is seen between the superior ulnar collateral and the posterior ulnar recurrent arteries. The inferior ulnar collateral artery provides the only direct vascularization to the nerve and is located in the region just proximal to the cubital tunnel. The segmental nature of the blood supply to the ulnar nerve underscores the importance of its preservation during transposition.
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraneural and intraneural arterial anatomy of the ulnar nerve at the elbow. J Shoulder Elbow Surg 1999;8:17-21.
Question 37:
A 10-year-old girl with a history of an obstetrical brachial plexus palsy has been referred for evaluation. Examination reveals a severe adduction internal rotation contracture of the shoulder and a mild flexion contracture of the elbow. Hand function is normal. Radiographs show mild glenohumeral joint incongruity. To achieve the best functional outcome, management should consist of
Options:
- physical therapy to stretch the tight structures.
- a humeral rotational osteotomy.
- anterior shoulder release and posterior muscle transfers.
- anterior shoulder release.
- shoulder fusion.
Correct Answer: a humeral rotational osteotomy.
Explanation:
DISCUSSION: The patient has an upper plexus palsy (Erb palsy) with severe shoulder contracture. While physical therapy for stretching is the treatment of choice to prevent contracture in the newborn, it is unlikely to be of benefit in the older child with an established contracture. Contracture release alone or in combination with muscle transfers can improve the cosmetic appearance, and in the case of a mild deformity, may also improve function. These procedures are less likely to help when there is deformity of the shoulder joint or when arthritic changes are present. The procedure of choice for an older child with joint deformity is rotational osteotomy of the proximal humerus because it can improve cosmesis and function, even in the face of joint deformity.
REFERENCES: Jahnke AH Jr, Bovill DF, McCarroll HR Jr, James P, Ashley RK: Persistent brachial plexus birth palsies. J Pediatr Orthop 1991;11:533-537.
Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of 20 cases. J Pediatr Orthop 1990;10:442-444.
Goddard NJ, Fixsen JA: Rotation osteotomy of the humerus for birth injuries of the brachial plexus. J Bone Joint Surg Br 1984;66:257-259.
Question 38:
-Figure 39 is the anteroposterior radiograph of a marathon runner who has left groin pain that prevents her from running. She recently got back into her usual running routine after an ankle injury preventedbher from running for several months. She now has pain with any weight bearing. What is the most appropriate treatment option?
Options:
- Hip resurfacing arthroplasty
- Hip arthroscopy with removal of the cam lesion
- Internal fixation of the femoral neck with multiple screws
- Trial of nonsurgical treatment with no weight bearing on the left leg
- Vitamin D level assessment and supplementation with 50000 units weekly
Correct Answer: Internal fixation of the femoral neck with multiple screws
Question 39:
A 32-year-old woman with systemic lupus erythematosus treated with methotrexate and oral corticosteroids reports right groin pain with ambulation and night pain. Examination reveals pain with internal and external rotation and flexion that is limited to 105 degrees because of discomfort. Laboratory studies show a serum WBC of 9.0/mm 3 and an erythrocyte sedimentation rate of 35 mm/h. Figures 5a and 5b show AP and lateral radiographs of the right hip. Further evaluation should include
Options:
- examination under fluoroscopy.
- MRI.
- a bone scan.
- arthrography.
- aspiration and arthrography.
Correct Answer: MRI.
Explanation:
DISCUSSION: The radiographs show Ficat and Arlet stage 2 osteonecrosis. The femoral head remains round, and there are sclerotic changes in the superolateral quadrant. Patients with systemic lupus erythematosus are at risk for osteonecrosis because of prednisone use and the underlying metabolic changes associated with the condition (hypofibrinolysis and thrombophilia). MRI is the best diagnostic method for detecting osteonecrosis, with a greater than 98% sensitivity and specificity. For this patient, an MRI can assess the contralateral hip for any involvement and can quantify the extent of the lesion.
REFERENCES: Mont MA, Jones LC, Sotereanos DG, Amstutz HC, Hungerford DS: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect
2000;49:169-185.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont , IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 40:
The radiographs shown in Figures 1 and 2 reveal squamous cell carcinoma of the thumb involving the distal phalanx. Following biopsy confirmation, what would be the most appropriate course of management?
Options:
- Curettage and bone grafting
- External beam radiation
- Ray amputation of the thumb
- Interphalangeal (IP) joint disarticulation
Correct Answer: Interphalangeal (IP) joint disarticulation
Explanation:
EXPLANATION:
Squamous cell carcinoma of the fingertip/nail region is uncommon but remains the most common malignancy in the hand. A high degree of suspicion is needed to diagnose this condition. Biopsy and radiographs are necessary initially. The subsequent treatment depends on the extent of the lesion at the time of presentation. Treatment can vary from Mohs micrographic surgery (MMS) to digital amputation. Amputation is recommended when bone involvement is present. In this patient, because the distal phalanx tip is involved and no further bone involvement proximally was observed, an amputation at the IP joint level is recommended. More proximal involvement would require a more proximal amputation level. Curettage and bone graft is not appropriate for this malignant lesion. External beam radiation therapy is not a first-line treatment option for this condition. Metastatic spread is uncommon. MMS is inappropriate when bone invasion has occurred.
Question 41:
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?
Options:
- Cobalt-on-polyethylene
- Cobalt-on-cobalt
- Titanium-on-polyethylene
- Stainless steel-on-polyethylene
- Ceramic-on-ceramic
Correct Answer: Ceramic-on-ceramic
Explanation:
DISCUSSION: Alumina ceramic is highly biocompatible when used as a biomaterial for joint arthroplasty implants. It has been shown to have good hardness, low roughness, and excellent wettability, therefore resulting in very low friction. However, it is expensive and limited reports have shown the problem of fracture on impact. The exact role for ceramic articulations is unknown at present.
REFERENCES: Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Sharkey PF, Hozack WJ, Dorr LD, Maloney WJ, Berry D: The bearing surface in total hip arthroplasty: Evolution or revolution, in Price CT (ed): Instructional Course Lectures 49. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 41-56.
Question 42:
A 16-year-old boy who is a competitive basketball player (Figure 43)
Options:
- Ligamentous reconstruction
- Meniscal repair
- Meniscectomy 39
- Immobilization
Correct Answer: Meniscal repair
Question 43:
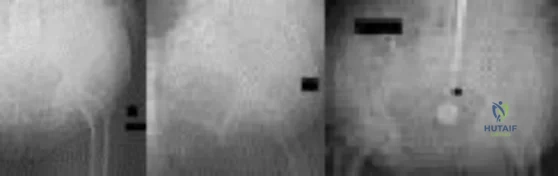
Figure below shows the radiograph obtained from a 76-year-old woman who has sharp pain in her groin, thigh, and buttocks that worsens with activity. She has been dealing with this pain for more than a year but is otherwise healthy. Recently, she has begun to notice night pain. The pain no longer responds to NSAIDs. She would like to be able to dance at her daughter's wedding in 4 months and wonders how best to proceed. What is the best next step?
Options:
- Radiograph-guided steroid injection followed by total hip arthroplasty 6 weeks later
- Total hip arthroplasty
- Physical therapy
- Referral back to her spine surgeon
Correct Answer: Physical therapy
Explanation:
DISCUSSION:
The next best course of action is total hip arthroplasty. The patient is an otherwise healthy woman requesting pain relief and expresses a desire to be dancing in 4 months. She has had more than 6 months of symptoms that are classic hip osteoarthritis symptoms, with pain in the groin and thigh. Severe osteoarthritis is seen in the radiograph as well. NSAIDs are no longer working. Given the objective findings, the subjective reports, and the duration of symptoms, this patient merits surgery. Consideration for steroid injection is reasonable, but given her desire to be dancing in 4 months, an injection would increase her risk of infection if total hip arthroplasty were to be performed within 3 months of the injection.
Question 44:
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?
Options:
- Hypertrophic cardiomyopathy (HCM)
- Sclerosis of the aortic valve without stenosis
- Mild mitral valve regurgitation
- Left ventricular hypertrophy (LVH)
- Functional murmurs
Correct Answer: Hypertrophic cardiomyopathy (HCM)
Explanation:
DISCUSSION: Hypertrophic cardiomyopathy (HCM) accounts for up to 50% of cases of
sudden death in young athletes. HCM phenotype becomes evident by age 13 to 14 years. Those at higher risk include individuals with cardiac symptoms, a family history of inherited cardiac disease, and those with a family history of premature sudden death. Echocardiography is useful for detecting structural heart disease, including the cardiomyopathies and valvular abnormalities. Trained adolescent athletes demonstrated greater absolute left ventricular wall thickness (LVWT) compared to controls. HCM should be considered in any trained adolescent male athlete with a LVWT of more than 12 mm (female of more than 11 mm) and a nondilated ventricle. Adolescent and adult athletes differ with respect to the range of LVWT measurements, as a manifestation of left ventricular hypertrophy (LVH). Differentiating LVH (“athlete’s heart”) from HCM involves looking at additional echocardiographic features. Sharma and associates reported that adolescents with HCM had a small or normal-sized left ventricle (less than 48 mm) chamber size, while those with LVH had a chamber size at the upper limits of normal (52 mm to 60 mm).
REFERENCES: Sharma S, Maron BJ, Whyte G, et al: Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete’s heart and hypertrophic cardiomyopathy. J Am College Cardiol 2002;40:1431-1436.
Maron BJ, Spirito P, Wesley Y, et al: Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med 1986;315:610-614.
Pelliccia A, Culasso F, Di Paolo FM, et al: Physiologic left ventricular cavity dilatation in elite athletes. Ann Intern Med 1999;130:23-31.
Question 45:
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior knee pain, a trace effusion, a 2+ posterior drawer, a grade 1A Lachman, no valgus laxity, and negative dial tests at 30° and 90°. What is the best treatment strategy at this time?
Options:
- Physical therapy with a focus on quadriceps strengthening
- Physical therapy and delayed posterior cruciate ligament (PCL) reconstruction
- PCL reconstruction
- PCL and posterolateral corner reconstruction This patient has likely sustained an isolated PCL injury. The examination is consistent with a grade II injury to the PCL. In patients with isolated PCL injuries, such as this scenario, the best initial option is nonsurgical treatment and return to play as symptoms subside and strength improves. Physical therapy and delayed PCL reconstruction is not the answer because this patient can likely be treated without surgery. The absence of valgus laxity and negative dial testing findings suggest that an injury to the posteromedial and posterolateral corners has not occurred. Initial nonsurgical treatment is indicated for this patient. If he completes rehabilitation and experiences persistent disability with anterior and/or medial knee discomfort or senses the knee is "loose," PCL reconstruction should be considered at that time.
Correct Answer: Physical therapy with a focus on quadriceps strengthening
Explanation:
Figure 1 is the MRI scan of a 61-year-old man who had left shoulder pain with a massive rotator cuff tear. Active forward elevation was 120°. Arthroscopic examination revealed that the rotator cuff tear was irreparable. The articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment option for pain relief in this patient?
A. Biceps tenotomy
B. Loose body removal
C. Latissimus dorsi transfer
D. Reverse total shoulder arthroplasty
Question 46:
An otherwise healthy 75-year-old man has a painful mass in the popliteal fossa of his right knee. A lateral radiograph of the knee, a CT scan of the distal femur, and a histopathologic specimen are shown in Figures 13a through 13c. Management should consist of
Options:
- observation.
- radiation therapy.
- radiation therapy and chemotherapy.
- surgical resection.
- surgical resection and chemotherapy.
Correct Answer: surgical resection.
Explanation:
DISCUSSION: The patient has a parosteal osteosarcoma of the distal femur. The findings of mild knee pain, radiographic evidence of a radiodense mass involving the parosseous space or surface of the distal femur, and histologic findings of a spindle cell lesion forming immature osteoid with little to no necrosis most likely suggest a parosteal osteosarcoma. The treatment of choice is surgical resection.
REFERENCES: Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK: Parosteal osteosarcoma: A clinicopathological study. J Bone Joint Surg Am 1994;76:366-378.
Campanacci M: Bone and Soft Tissue Tumors. New York, NY, Springer-Verlag, 1990, pp 433-454.
Question 47:
- An 8-year-old girl has a supracondylar fracture of the distal humerus. Her neurovascular status is intact. Radiographs show hyperextension of 10 degrees of the distal fragment and an angle between the humeral shaft and capitellar physis (Baumann’s angle) of 88 degrees. Management should consist of
Options:
- Olecranon pin traction
- Closed reduction and pin fixation
- Open reduction and internal fixation
- Cast immobilization in this position
- An arteriogram to rule out an occult intimal tear of the brachial artery
Correct Answer: Closed reduction and pin fixation
Explanation:
Supracondylar fracture of the humerus accounts for 3 percent of childhood fractures. It is the commonest fracture of the elbow region in children and accounts for 80% of elbow injuries. Common complications include cubitus varus, ischemic contracture, and neurovascular lesions. This question chooses closed reduction with Kwire fixation as the correct method of treatment. However, the literature discusses olecranon screw traction and open reduction as legitimate options in treatment. This study recommends olecranon traction for severely displaced fractures left unstable by closed reduction.
Question 48:
A 32-year-old man who sustained a tarsometatarsal (Lisfranc) injury 3 years ago now reports increasing pain in the left foot. Orthotics, nonsteroidal anti-inflammatory drugs, and injections have provided only temporary relief. Examination reveals swelling and tenderness over the tarsometatarsal joints. Radiographs show advanced arthrosis of the first and second tarsometatarsal joints. Management should now include
Options:
- midfoot arthrodesis.
- a rocker sole shoe with orthotic inserts.
- shock wave or orthotripsy.
- an ankle-foot orthosis.
- triple arthrodesis.
Correct Answer: midfoot arthrodesis.
Explanation:
DISCUSSION: The patient has advanced arthrosis of the midfoot, and orthotic management has failed to provide relief. Therefore, the treatment of choice is midfoot arthrodesis. Shock wave treatment has not been shown to be beneficial for arthritis. An ankle-foot orthosis would not be appropriate based on findings of a normal ankle joint. Triple arthrodesis would not be helpful because the hindfoot joint is not affected in a Lisfranc injury.
REFERENCES: Sangeorzan BJ, Veith GR, Hansen ST Jr: Salvage of Lisfranc’s tarsometatarsal joints by arthrodesis. Foot Ankle 1990;10:193-200.
Komenda
GA
, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Question 49:
An active 23-year-old man has right groin pain that increases with sports activity. Examination reveals decreased internal rotation of the affected hip. He has a positive impingement test and radiographs reveal no crossover sign. An MRI scan is most likely to reveal which of the following? Review Topic
Options:
- Abnormal alpha angle and a chondrolabral tear
- Acetabular retroversion
- Heterotopic ossification
- Ankylosing spondylitis
- Coxa varum
Correct Answer: Abnormal alpha angle and a chondrolabral tear
Explanation:
Young patients with hip pain and a positive impingement test are likely to have femoroacetabular impingement. The triad seen in these patients is a reduced concavity at the femoral head-neck junction, which leads to an increase in alpha angle and a chondrolabral tear. MR-arthrogram is the cross-sectional imaging modality of choice. These patients usually have reduced internal rotation and a positive impingement sign. The other findings, though possible, are not the most likely scenario in this young and active patient.
Question 50:
All of the following indicators of resuscitation may be within normal limits for a trauma patient that is in "compensated" shock EXCEPT:
Options:
- Systolic blood pressure
- Urine output
- Heart rate
- Serum lactate
- Mean arterial pressure
Correct Answer: Systolic blood pressure
Explanation:
DISCUSSION: Historically, normal blood pressure, heart rate, and urine output have been endpoints to signal complete resuscitation in the polytrauma patient. The review article by Porter et al states that there is a high incidence of patients (as much as 85%) in "compensated" shock despite normal vital signs and urine output parameters. Compensated shock is secondary to a maldistribution of blood flow and tissue oxygenation as splanchnic organs have less distribution of the cardiac output compared to the heart and the brain. The article by Elliott is also a review, and it states that serum lactate is the best indicator of peripheral organ perfusion and tissue oxygenation. It also states that base deficit and gastric mucosal pH are appropriate end points to determine the complete resuscitation of trauma patients.
Question 51:
A 16-year-old boy with spastic quadriplegic cerebral palsy has been referred for evaluation and management of scoliosis. His parents report increasing problems with sitting balance, positioning, and hygiene because of the deformity. The radiograph shown in Figure 46 reveals a lordoscoliosis of 105° with marked pelvic obliquity. Attempts at correcting the pelvic obliquity on supine bending radiographs show significant rigidity. Management should consist of
Options:
- a thoracolumbosacral orthosis.
- posterior spinal fusion.
- anterior and posterior spinal fusion.
- electrical stimulation.
- wheelchair modifications.
Correct Answer: anterior and posterior spinal fusion.
Explanation:
DISCUSSION: Spinal stabilization is the treatment of choice in patients with severe scoliosis who have progressive positioning, sitting balance, and/or hygiene problems despite maximal nonsurgical management. Pelvic rigidity and marked frontal plane deformity necessitate anterior and posterior procedures so as to maximize correction and fusion.
REFERENCES: Weinstein SL (ed): The Pediatric Spine: Principles and Practice. New York, NY, Raven Press, 1994, pp 977-997.
Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1993, pp 447-459.
Question 52:
What cardiac condition causes most upper extremity emboli?
Options:
- Atrial fibrillation
- Viral cardiomyopathy
- Valvular disease
- Atrial septal defect
Correct Answer: Atrial fibrillation
Explanation:
EXPLANATION:
Atrial fibrillation is responsible for approximately 80% of all upper extremity emboli. All other cardiac conditions listed can cause upper extremity emboli; however, atrial fibrillation is the most common cause. Patients with an upper extremity embolic event should undergo prompt evaluation, with a careful history and physical examination as well as focused laboratory tests for hypercoagulability. Arterial Doppler studies or angiography is/are warranted. Electrocardiogram and echocardiogram are also used to evaluate for potential cardiac abnormalities. Consultation with vascular, radiology, and cardiology personnel is often necessary when patients present with upper extremity emboli. Treatment usually involves anticoagulation, embolectomy if necessary, and treatment for any recognized cardiac
abnormality.
Question 53:
A 15-year-old boy has a mass at the knee. Radiographs show an aggressive tumor involving the proximal tibia, and biopsy findings reveal a high-grade osteosarcoma. Staging studies show that the tumor impinges on the neurovascular bundle. The tumor enlarges during preoperative chemotherapy. Management should now consist of
Options:
- prolonged chemotherapy.
- radiation therapy.
- amputation.
- marginal excision, sparing the neurovascular bundle.
- wide excision, including the neurovascular bundle.
Correct Answer: amputation.
Explanation:
DISCUSSION: Limb salvage procedures have become the usual treatment for even high-grade osteosarcomas. However, tumors associated with pathologic fracture, tumors encasing the neurovascular bundle, and tumors that enlarged during preoperative therapy and are adjacent to the neurovascular bundle require amputation.
REFERENCES: Springfield D: Bone and soft-tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 423-468.
Question 54:
A 77-year-old woman underwent semiconstrained right total elbow arthroplasty 4 weeks ago through a Bryan-Morrey approach. Her recovery was uneventful until 2 days ago when she began her physical therapy session at an outpatient clinic. During resisted extension exercises, she felt a "pop" in her elbow, accompanied with pain and inability to extend her elbow against resistance. What is the most likely cause of her symptoms? Review Topic
Options:
- Fracture of the ulnar component
- Disengagement of the axle of the prosthesis
- Failure of the triceps mechanism repair
- Periprosthetic fracture of the humerus
- Periprosthetic fracture of the ulna
Correct Answer: Failure of the triceps mechanism repair
Explanation:
During a Bryan-Morrey approach for total elbow arthroplasty, the triceps is dissected free from its ulnar insertion and reflected laterally. At the conclusion of the procedure, the triceps tendon is reattached to the ulna through drill holes. Whereas motion can be initiated postoperatively, 6 to 8 weeks of protection are recommended before initiation of resistance exercises to protect the triceps repair. A periprosthetic fracture or component failure is rare in the absence of more significant trauma, and they are usually late complications.
Question 55:
In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
Options:
- Extensor digiti quinti
- Abductor pollicis longus
- Extensor pollicis longus
- Extensor carpi radialis brevis
- Extensor carpi ulnaris
Correct Answer: Extensor digiti quinti
Explanation:
DISCUSSION: The tendon most prone to rupture in a patient with rheumatoid arthritis of the wrist is the extensor digiti quinti. It can be a silent injury since the extensor digitorum communis can provide extension to the fifth finger. The extensor digiti quinti is at high risk since it is overlying the ulnar head where it is prone to attritional rupture (Vaughan-Jackson syndrome).
REFERENCES: Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.
Papp SR, Athwal GS, Pichora DR: The rheumatoid wrist. J Am Acad Orthop Surg
2006;14:65-77.
Question 56:
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension?
Options:
- Removal of hardware with tendon transfer
- Repair of the extensor pollicis longus (EPL) tendon primarily
- Thumb interphalangeal (IP) arthrodesis
- Nonsurgical treatment with cast placement keeping the thumb in a fully extended position for 4 weeks
Correct Answer: Removal of hardware with tendon transfer
Explanation:
EXPLANATION:
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through
view, are useful for avoiding this complication.
Question 57:
The mechanism for the osseous destruction is attributable to
Options:
- avascular necrosis.
- tumor invasion.
- hypervascularity.
- infection.
Correct Answer: hypervascularity.
Explanation:
DISCUSSION
This scenario is a classic example of the development of Charcot foot. A red, swollen, deformed foot without ulceration suggests neuroarthropathy. Normal inflammatory marker findings, no history of fever or chills, and radiographs demonstrating bone loss support the diagnosis. Limb elevation with dramatic reduction in erythema is also characteristic of this disease process and does not occur with infection. Total-contact casting is the cornerstone of treatment for acute Charcot disease. Hemoglobin A1C is an indicator of glucose averaged over a 3-month period, providing the most reliable indication of a patient's ongoing glucose control. The pathophysiology of bone destruction is believed to be hypervascularity of bone. Infection and Charcot disease may develop simultaneously, but the combination is rare.
RECOMMENDED READINGS
Kaynak G, Birsel O, Güven MF, Ogüt T. An overview of the Charcot foot pathophysiology. Diabet Foot Ankle. 2013 Aug 2;4. doi: 10.3402/dfa.v4i0.21117.Print 2013. PubMed PMID: 23919113.
View Abstract at PubMed
Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006 May;27(5):324-9. PubMed PMID: 16701052.
View Abstract at PubMed
Question 58:
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92?
Options:
- Valgus laxity at 30 degrees of knee flexion
- Varus laxity at 30 degrees of knee flexion
- Posterior drawer
- Pivot shift
- Patellar apprehension
Correct Answer: Pivot shift
Explanation:
DISCUSSION: The T
2
-weighted sagittal MRI scan shows the classic “bone bruise” pattern seen with an anterior cruciate ligament (ACL) tear. These lesions are thought to represent subcortical trabecular hemorrhages and are manifested as an increase in signal intensity on T
2
-weighted images and diminished signal intensity on T
r
weighted images. They are classically located in the mid-portion of the lateral femoral condyle and posterior aspect of the lateral tibial plateau. This is due to the fact that an ACL tear typically is the result of a valgus-extemal rotation of the femur on the fixed tibia. This places most of the weight-bearing stress on the lateral femoral condyle, which rotates laterally and impacts the posterior lip of the lateral tibial plateau. This may result in an impaction fracture if the force is great enough, but more frequently causes merely a microfracture of the involved subcortical trabeculae.
REFERENCES: Vellet AP, Marks PH, Fowler PJ, et al: Occult posttraumatic osteochondral lesions of the knee: Prevalence, classification, and short-term sequelae evaluated with MR imaging. Radiology 1991;178:271-276.
Cone R: Imaging sports-related injuries of the knee, in DeLee J, Drez D, Miller M (eds): DeLee & Drez’s Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 2, pp 1595-1652.
Question 59:
During impaction of a cementless acetabular component, the posterior column was fractured and found to be displaced. Which of the following is considered the most appropriate surgical option?
Options:
- Exchange of the cementless cup to a larger component
- Retention of the component and bone grafting of the fracture
- Retention of the component and postoperative weight protection until the posterior column heals
- Removal of the cup, fixation of the posterior column, and application of an antiprotrusio cage
- Removal of the cup and cementing of an all-polyethylene liner
Correct Answer: Removal of the cup, fixation of the posterior column, and application of an antiprotrusio cage
Explanation:
DISCUSSION: Acetabular bone loss presents a challenge during reconstruction. A cementless hemispherical cup can be used in most patients provided that the acetabular rim, particularly the posterior column, is intact. When the posterior column is disrupted, fixation with a reconstruction plate and/or the use of an antiprotrusio cage is recommended. The latter is particularly important when the posterior column is fractured and displaced, such as in this patient. Under these circumstances, reduction of the fracture and application of an antiprotrusio cage is recommended. In this particular type of case, some surgeons may elect to retain the hemispherical cup and apply an antiprotrusio cage over the cup (“cage over cup” technique).
REFERENCES: Berry DJ: Antiprotrusio cages for acetabular revision. Clin Orthop 2004;420:106-112.
Peterson CA, Lewallen DG: Periprosthetic fracture of the acetabulum after total hip arthroplasty. J Bone Joint Surg Am 1996;78:1206-1213.
Question 60:
A homebound 75-year-old woman with diabetes mellitus has had progressive left knee pain and swelling for the past 6 weeks. She is febrile with a temperature of 103 degrees F (39.5 degrees C). History reveals that she underwent arthroplasty 5 years ago. Examination shows passive range of motion of 0 to 100 degrees with no active extension. Knee aspiration reveals purulent fluid with a Gram stain showing gram-negative rods. A radiograph is shown in Figure 27. In addition to IV antibiotics, which of the following management options offers the best chance of a successful outcome?
Options:
- Incision and drainage with repair of the extensor mechanism
- Removal of components and delayed revision knee arthroplasty with an allograft extensor mechanism
- Removal of components and immediate exchange revision total knee arthroplasty
- Removal of components and delayed knee arthrodesis
- Removal of components and delayed revision knee arthroplasty with extensor mechanism repair
Correct Answer: Removal of components and delayed knee arthrodesis
Explanation:
DISCUSSION: The patient has an infected total knee arthroplasty and an interrupted extensor mechanism. A late infection of a total knee arthroplasty in a patient with diabetes mellitus and a virulent organism requires removal of the components, debridement, antibiotic spacers, and surveillance to ensure eradication of the infection. Reconstruction of an incompetent extensor mechanism in an infected knee is extremely unlikely to be successful. Arthrodesis is the procedure of choice if a revision total knee arthroplasty is not likely to succeed. Resection arthroplasty is recommended only as a long-term solution if the patient is medically unable to undergo further surgery.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgery, 2002, pp 513-536.
Hanssen AD, Rand JA: Evaluation and treatment of infection at the site of a total hip or knee arthroplasty. Instr Course Lect 1999;48:111-122.
Question 61:
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Options:
- closed reduction and casting in extension.
- open reduction with suture fixation of the proximal fragment.
- closed reduction, followed by functional bracing.
- open reduction and internal fixation with screws and complete proximal tibial epiphysiodesis.
- open reduction and internal fixation with screws.
Correct Answer: open reduction and internal fixation with screws.
Explanation:
DISCUSSION: Tibial tubercle avulsion is an injury of the adolescent knee that most often occurs just before the end of growth. The fracture usually occurs with jumping, either at push-off or landing. This patient has a type III injury. In type III injuries, the articular surface is disrupted, and meniscal injury and compartment syndrome can occur. Open reduction is the treatment of choice, and anterior fasciotomy should be considered prophylactically at the time of surgery. Although the fracture heals with an anterior epiphysiodesis of the proximal tibia, little growth remains in this patient and no special handling of the physis is warranted.
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 62:
When evaluating articular cartilage, what extracellular matrix component is most closely associated with the deep calcified cartilage zone?
Options:
- Collagen type I
- Collagen type II
- Collagen type X
- Proteoglycan aggrecan
- Hyaluronic acid
Correct Answer: Collagen type X
Explanation:
DISCUSSION: Collagen type X is produced only by hypertrophic chondrocytes during enchondral ossification (growth plate, fracture callus, heterotopic ossification) and is associated with calcification of cartilage in the deep zone of articular cartilage. Collagen type I is the predominant collagen in bone, ligament, and tendon. Collagen type II is the predominant collagen in articular cartilage. Proteoglycan aggrecan and hyaluronic acid are components of the extracellular matrix and are involved in the compressive strength characteristics of articular cartilage.
REFERENCES: Buckwalter JA, Mankin HJ: Articular cartilage: Tissue design and chondrocyte matrix interactions. Instr Course Lect 1998;47:477-486.
Poole AR, Kojima J, Yasuda T, Mwale F, Kobayasai M, Laverty S: Composition and structure of articular cartilage: A template for tissue repair. Clin Orthop 2001;391:S26-S33.
FOR ALL MCQS CLICK THE LINK ORTHO
MCQ BANK
Question 63:
A 75-year-old woman with rheumatoid arthritis and a long history of oral corticosteroid use sustains a comminuted intra-articular distal humerus fracture. What is the best surgical option?
Options:
- Open reduction internal fixation (ORIF) with parallel plates
- ORIF with orthogonal plates and iliac crest bone grafting
- Total elbow arthroplasty (TEA)
- Closed reduction and percutaneous pinning
Correct Answer: Total elbow arthroplasty (TEA)
Explanation:
TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF with TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared with ORIF. TEA was also likely to result in a lower resurgical rate; one- quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA versus ORIF in 24 elderly women. TEA outcomes were again
superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed
reduction and percutaneous pinning studies have not been published on the adult population.
Question 64:
A 57-year-old man reports right hip pain that has been progressive for the past several months. The pain is exacerbated by weight-bearing activities and improves somewhat with rest. A radiograph is shown in Figure 10a and a coronal T 1 -weighted MRI scan is shown in Figure 10b. What is the most likely diagnosis?
Options:
- Osteoarthritis of the hip
- Osteonecrosis of the hip
- Metastatic carcinoma
- Femoral head fracture
- Rheumatoid arthritis of the hip
Correct Answer: Osteonecrosis of the hip
Explanation:
DISCUSSION: These are classic findings of osteonecrosis of the hip. The radiograph reveals the subchondral sclerotic pattern commonly seen in osteonecrosis and is quite extensive in this patient. The MRI scan reveals the typical serpentine-like region of low signal intensity with a central zone where the signal is similar to fat.
REFERENCES: Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA,
WB Saunders, 2002, pp 3160-3162.
Sugano N: Osteonecrosis, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 877-887.
Question 65:
Following operative repair of lower extremity long bone and periarticular fractures, what is the time frame for patients to return to normal automobile braking time?
Options:
- 6 weeks after initiation of weight bearing
- 4 weeks postoperatively
- 8 weeks from the date of injury
- Once full range of motion of the ankle and knee exist
- At the time of bony union
Correct Answer: 6 weeks after initiation of weight bearing
Explanation:
DISCUSSION: According to the first referenced study by Egol et al, appropriate braking time returns at a point 6 weeks after initiation of weightbearing after treatment of lower extremity long bone and periarticular fractures, as examined with a driving simulator. No differences were seen in return of braking time between periarticular fractures and long bone injuries.
The second reference by Egol studied only operatively treated ankle fractures and found that time to appropriate braking returns at 9 weeks postoperatively. Interestingly, no significant association was found between the functional scores and normalization of total braking time.
Question 66:
A deficiency of which of the following is associated with an increased risk of venous thromboembolism?
Options:
- Fibrinogen
- Protein S
- Factor VII
- Factor VIII
- Prothrombin
Correct Answer: Protein S
Explanation:
Protein C and Protein S are endogenous proteins whose action is to inhibit the coagulation cascade. Deficiencies in these proteins are a risk factor for the development of thrombus. Prothrombin is the precursor to thrombin, which is the final common pathway for both the intrinsic and extrinsic coagulation cascade. Thrombin acts to convert fibrinogen to fibrin and thus clot formation.
Question 67:
Which of the following accurately describes the biosynthetic materials tricalcium phosphate (TCP) and hydroxyapatite?
Options:
- The osteoblast is the cell responsible for resorption of hydroxyapatite.
- Once in the body, TCP is partially converted to hydroxyapatite.
- TCP undergoes biologic resorption at a rate 10 times slower than hydroxyapatite.
- TCP is much stronger biomechanically in compression than hydroxyapatite.
- Optimal pore size for both materials appears to be less than 150 µm.
Correct Answer: Once in the body, TCP is partially converted to hydroxyapatite.
Explanation:
DISCUSSION: TCP is resorbed more rapidly, at a rate of 10 to 20 times faster than hydroxyapatite, partially because its larger pore size makes it a weaker substance. It provides significantly less compressive strength than hydroxyapatite. It does partially convert to hydroxyapatite, thus slowing its resorption rate. The absorbing cell of hydroxyapatite is the foreign body giant cell, not the osteoclast. Optimum pore size appears to be between 150 and
500 µm.
REFERENCES: Lane JM, Bostrom MP: Bone grafting and new composite biosynthetic graft materials. Instr Course Lect 1998;47:525-534.
Walsh WR, Chapman-Sheath PJ, Cain S, et al: A resorbable porous ceramic composite bone graft substitute in a rabbit metaphyseal defect model. J Orthop Res 2003;21:655-661.
Question 68:
A 66-year-old man who underwent shoulder arthroplasty 7 years ago reports progressively worsening shoulder pain for the past 4 weeks after hospital discharge for community-acquired pneumonia. He is afebrile and reports no chills or night sweats. Laboratory studies show a white blood cell count of 11,200/mm3 and an erythrocyte sedimentation rate of 25/h. Shoulder radiographs are negative for fracture, dislocation, or signs of implant loosening. What is the most appropriate management? Review Topic
Options:
- Follow-up in 2 weeks with a repeat white blood cell count and erythrocyte sedimentation rate
- Shoulder aspiration with Gram stain and culture of fluid
- Prescription strength nonsteroidal anti-inflammatory drugs
- Physical therapy for shoulder stretching and modalities
- Emergent surgical irrigation, debridement, and revision shoulder arthroplasty
Correct Answer: Shoulder aspiration with Gram stain and culture of fluid
Explanation:
The patient may have hematologic spread of the pulmonary infection to the shoulder arthroplasty; however, further work-up is necessary at this point. The elevated laboratory studies may still be secondary to the pulmonary infection. Aspiration of the shoulder joint with stat Gram stain and culture of the fluid is indicated. If the aspirate shows signs of infection and irrigation and debridement is indicated, complete revision of the well-seated implants may not be necessary. Physical therapy and nonsteroidal anti-inflammatory drugs are not indicated until the possibility of a shoulder infection has been ruled out. A wait of 2 weeks to repeat the laboratory values, in the presence of new shoulder pain, is contraindicated.
Question 69:
A 27-year-old runner training for his first marathon reports lateral knee pain after an unusually long training run. He states that the most significant pain occurs while running downhill. Examination of the patient while he is laying on the unaffected side reveals increased pain when manual pressure is applied to the lateral femoral epicondylar area during knee range of motion of 30° to 45°. What is the most likely diagnosis?
Options:
- Popliteal tendinitis
- Iliotibial band friction syndrome
- Excessive lateral pressure syndrome
- Lateral meniscal tear
- Stress fracture
Correct Answer: Iliotibial band friction syndrome
Explanation:
DISCUSSION: Iliotibial band friction syndrome is one of the most common causes of lateral knee pain in runners. It is caused by increased friction between the iliotibial band and the lateral femoral condyle because of increased tension on the lateral structures. It may be caused by a prominence of the lateral epicondyle or a malalignment of the lower extremity in the runner, including genu varum, tibia vara, heel varus and forefoot supination, or compensating pronation. These structural characteristics can couple with relative muscle imbalance and lead to an altered running gait, enhancing friction between the lateral femoral condyle and the iliotibial band. Management is usually nonsurgical, including stretching of the iliotibial band and strengthening of the hip abductor muscles, with occasional use of cortisone injections or iontophoresis.
REFERENCES: Noble CA: The treatment of iliotibial band friction syndrome. Br J Sports Med 1979;13:51-54.
James SL: Running injuries to the knee. J Am Acad Orthop Surg 1995;3:309-318.
James SL, Jones DV: Biomechanical aspects of distance running, in Cavanagh PR (ed): Biomechanics of Distance Running. Champaign, IL, Human Kinetic Books, 1990, pp 249-269.
Question 70:
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?
Options:
- Fifth metatarsal head lateral ostectomy
- Fifth metatarsal head excision
- Metatarsal osteotomy and fifth metatarsal head ostectomy
- Fifth metatarsal plantar condylectomy
- Fifth metatarsophalangeal Silastic implant arthroplasty
Correct Answer: Metatarsal osteotomy and fifth metatarsal head ostectomy
Explanation:
DISCUSSION: The patient has a bunionette with a large 4-5 intermetatarsal angle. This requires not only ostectomy of the lateral prominence but metatarsal osteotomy to decrease the intermetatarsal angle. Excising the head results in a flail joint and creates the possibility of a transfer lesion. Condylectomy can reduce plantar pressures but does not address the bunionette. The joint surface is well maintained, thus there are no indications for resection.
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Koti M, Maffulli N: Bunionette. J Bone Joint Surg Am 2001;83:1076-1082.
Question 71:
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Options:
- Cemented left total hip arthroplasty (THA)
- Cementless left THA with a proximally porous coated femoral stem
- Hybrid left THA
- Cementless left THA with a diaphyseal engaging conical femoral stem
Correct Answer: Hybrid left THA
Explanation:
DISCUSSION:
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 72:
A 32-year-old recreational basketball player underwent a successful anterior cruciate ligament (ACL) reconstruction using hamstring autograft approximately 15 months ago. His chart notes that he has good functional knee outcome scores as tested by his physical therapist. However, he has not returned to play despite being cleared by his physician 3 months ago. After successful ACL reconstruction, which of the following factors has shown to contribute the greatest influence on a player's decision to return to sport? Review Topic
Options:
- Surgeon's advice not to return
- Persistent knee pain
- Duration of sport participation
- Lifestyle and psychological factors
- Autograft harvasting surgical technique
Correct Answer: Surgeon's advice not to return
Explanation:
Athletes who do not return to their preinjury level of sport after primary ACL reconstruction despite having good knee function are largely influenced by lifestyle and psychological factors.
The return to their preinjury level of sport is frequently expected within 1 year after anterior cruciate ligament (ACL) reconstruction, yet many athletes do not achieve this milestone. Having a previous ACL reconstruction to either knee, poorer hop-test symmetry and subjective knee function, and more negative psychological responses were associated with not returning to the preinjury level sport. Fear of reinjury is considered one of the most common reasons cited for a postoperative reduction in or
cessation of sports participation.
Tjong et al. conducted a qualitative study of 31 patients, aged 18 to 40 years, to understand the factors influencing a patient's decision to return to his or her preinjury level of sport after ACL reconstruction. They found 3 overarching factors what largely influenced their decision to return to the preinjury sport: fear, lifestyle changes, and innate personality traits. This highlighted the importance of recognizing and addressing the psychological factors and lifestyle changes that significantly contribute to a patient's postoperative decision to return to sport.
Ardern et al. investigated the return-to-sport rates at 2 years after ACL reconstruction in athletes. At 2 years after surgery, 66% were playing sport, with 41% playing their preinjury level of sport and 25% playing a lower level of sport. Demographics, physical function, and psychological factors were supported as the most important influencing factors for the return to their preinjury level of sport.
Incorrect Answers:
Question 73:
- A 20-year-old college football player sustains a forceful hyperextension injury to his shoulder 4 months after undergoing an anterior capsular shift. Examination 2 weeks later reveals anterior tenderness. He is unable to lift the dorsum of his hand away from his back. What is the most likely diagnosis?
Options:
- Subscapularis rupture
- Type III SLAP lesion
- Disruption of capsular shift
- Isolated traumatic subluxation
- Injury to the axillary nerve after dislocation
Correct Answer: Subscapularis rupture
Explanation:
Subscapularis rupture is most likely, given weakness with the lift-off test. The injury is usually caused by either forceful hyperextension or external rotation of the adducted arm. Patients will complain of anterior shoulder pain and weakness of the arm when used above and below shoulder level. SLAP lesions usually occur with a fall onto an outstretched arm in abduction and slight forward flexion. No mention was made of shoulder instability (answers 3&4), or deltoid weakness (answer 5).
Question 74:
A 43-year-old woman has a 2-week history of right shoulder pain. She denies any injury to initiate her symptoms but states that she has shoulder pain with range of motion and lifting objects. Examination reveals mild pain with abduction, empty can testing, and with the Neer and Hawkins impingement tests. Her range of motion with the right shoulder reveals passive forward flexion to 90 degrees, abduction to 90 degrees, external rotation at the side to 15 degrees, and internal rotation to her buttock. The uninvolved left shoulder has forward flexion to 160 degrees, abduction to 150 degrees, external rotation at the side to 60 degrees, and internal rotation to T6. Radiographs of the shoulder are normal. What is the next most appropriate step in management? Review Topic
Options:
- Home exercise program
- Sling at all times until her pain decreases
- Closed manipulation under anesthesia
- Arthroscopic rotator cuff repair
- Arthroscopic anterior and posterior capsular release
Correct Answer: Home exercise program
Explanation:
The patient has the recent onset of adhesive capsulitis, which is characterized by loss of both active and passive range of motion. A home exercise program is as helpful as organized therapy to improve her range of motion. While a sling might be appropriate for comfort, continuous use might increase her shoulder stiffness. Surgical treatments, such as a manipulation under anesthesia or arthroscopic capsular release, might be necessary if her motion cannot be restored with physical therapy and home exercises. However, the natural history of idiopathic adhesive capsulitis is self limited and does not usually require surgery. An arthroscopic rotator cuff repair is not indicated because she does not have a rotator cuff tear.
Question 75:
A 10-month-old boy has an untreated developmental hip dislocation.
Options:
- Sclerosis of the proximal femoral epiphysis with subchondral lucency
- Abnormal femoral head-neck junction offset
- Widening of the proximal femoral physis with normal femoral head-neck junction offset
- Absence of the proximal femoral epiphysis secondary ossification center
Correct Answer: Absence of the proximal femoral epiphysis secondary ossification center
Explanation:
DISCUSSION
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.
Question 76:
Figures 29a and 29b show a clinical photograph and radiographs of a patient who sustained an open calcaneus fracture in a motor vehicle accident. The patient received immediate IV antibiotics and an emergent irrigation and debridement. The swelling has subsided by 3 weeks and the medial wound is clean. What do you tell the patient about the likelihood of infection if a formal open reduction and internal fixation via a lateral approach is performed?
Options:
- There is no significant difference between the infection rate for this fracture and a similar closed fracture.
- Due to the risk of infection, open reduction and internal fixation is not recommended for this fracture.
- The infection rate is three to five times more likely with this fracture.
- Due to the risk of infection from a lateral approach, treatment is confined to limited internal fixation or an external fixator.
- The patient will need to undergo 3 weeks of IV antibiotics at home.
Correct Answer: There is no significant difference between the infection rate for this fracture and a similar closed fracture.
Explanation:
DISCUSSION: Multiple authors have shown similar infection rates for grade 1 and 2 open medial fractures and closed fractures that have been treated with an extensile lateral approach and open reduction and internal fixation. Patients only need IV antibiotics for 2 to 3 days after surgery. Formal open reduction and internal fixation is not recommended for grade 3 medial wounds and most lateral wounds.
REFERENCES: Heier KA, Infante AF, Walling AK, et al: Open fractures of the calcaneus: Soft-tissue injury determines outcome. J Bone Joint Surg Am 2003;85:2276-2282.
Buckley RE, Tough S: Displaced intra-articular calcaneal fractures. J Am Acad Orthop Surg 2004;12:172-178.
Question 77:
Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with 2 weeks of pain at the left distal femur, a limp, and an inability to dance. Knee motion is 0 to 135 degrees with minimal pain and there is no effusion. Her temperature is 37.0°C, WBC is 12000 /µL (rr, 4500-11000 /µL), CRP is 0.8 mg/L (rr, 0.08-3.1 mg/L), and ESR is 21 mm/h (rr, 0-20 mm/h).
Options:
- Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
- Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
- Aspiration, cultures, Lyme serology, and oral amoxicillin
- Biopsy, culture, curettage, bone graft, and possible internal fixation
- Physical therapy, ibuprofen, and an antinuclear antibody test
Correct Answer: Biopsy, culture, curettage, bone graft, and possible internal fixation
Explanation:
DISCUSSION
Figures 14a through 14e show a 13-year-old boy with osteomyelitis of the distal tibia and a large subperiosteal abscess. The patient has failed treatment with IV ceftriaxone, and methicillin-resistant Staphylococcus aureus infection is likely. Aspiration, cultures, irrigation and debridement, IV vancomycin, an infectious disease consult, and an evaluation for possible deep vein thrombosis is prudent initial treatment. Figure 15a through 15c show a 7-year-old girl who sustained a deer tick bite while vacationing in Connecticut. She has Lyme arthritis and a Lyme “bulls-eye” rash on the same leg. Aspiration, cultures, Lyme serology, and oral amoxicillin for 30 days is prudent initial treatment. Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with a probable minor fracture via a benign cyst of the distal femur. The geographic cyst may be a nonossifying fibroma, eosinophilic granuloma, Brodie abscess, or simple bone cyst. Biopsy, culture, curettage and bone graft, and possible internal fixation is reasonable initial treatment.
Question 78:
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Options:
- Improvement in range of motion
- Reduction in range of motion
- Increase in extensor mechanism lag
- No differences in motion and strength
Correct Answer: No differences in motion and strength
Explanation:
DISCUSSION:
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 79:
A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
Options:
- she can expect to have good pain relief following surgery.
- active forward elevation and external rotation are reliably obtained postoperatively.
- with her current anterosuperior escape, she is likely to have a poor surgical result.
- postoperatively, significant muscular atrophy in the latissimus dorsi commonly occurs.
- no advancement in glenohumeral arthritic changes should occur following surgery.
Correct Answer: with her current anterosuperior escape, she is likely to have a poor surgical result.
Explanation:
DISCUSSION: Latissimus dorsi tendon transfer is considered a surgical option for treatment in patients with chronic supraspinatus and infraspinatus tendon tears. Preoperative subscapularis function is necessary for good clinical results. Additionally, men with active elevation to shoulder level and active external rotation to 20 degrees have predictably good results. Women with active shoulder elevation limited to below chest level have poor results from this procedure and should not be considered candidates. Postoperatively they lack pain control, active elevation, and active external rotation. Muscular atrophy in the latissimus dorsi does not occur, and glenohumeral arthritic changes frequently develop postoperatively.
REFERENCES: Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am
2006;88:113-120.
Iannotti JP, Hennigan S, Herzog R, et al: Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am 2006;88:342-348.
Question 80:
In patients with suspected hepatitis C, which of the following tests is commonly used to confirm the diagnosis after a positive ELISA screening test?
Options:
- Polymerase chain reaction (PCR)
- Northern blot
- Immunoblot assay
- Microarray
- Proteomics
Correct Answer: Immunoblot assay
Explanation:
DISCUSSION: The basic diagnostic test for hepatitis C (HCV) is detection of an antibody to epitopes on an enzyme-linked immunosorbent anti-HCV assay (ELISA). The currently used ELISA has high sensitivity (92%) and specificity (95%). False positives, however, still occur. The currently used supplemental test for HCV is strip immunoblot assay, which is based on detection of several HCV epitopes on nitrocellulose paper by antibody-capture techniques. Molecular amplification by PCR technology is very sensitive, but difficult to standardize and susceptible to contamination. Microarray and proteomics are relatively recent molecular techniques used for analysis of genes or proteins, respectively. A Northern blot is used to detect mRNA levels of specific genes but is not used in this situation.
REFERENCES: de Medina M, Schiff ER: Hepatitis C: Diagnostic assays. Semin Liver Dis 1995;15:33-40.
McGrory BJ, Kilby AE: Hepatitis C virus infection: Review and implications for the orthopedic surgeon. Am J Orthop 2000;29:261-266.
Question 81:
Figures 1 through 3 demonstrate the radiographs obtained from a 45-year-old construction worker who has wrist pain, loss of motion, and loss of strength. Nonsurgical measures have failed, and the patient requests surgery. What is the best surgical option for this patient?
Options:
- Proximal row carpectomy
- Excision of the proximal pole of the scaphoid
- Bone grafting with fixation of the scaphoid
- Scaphoid excision with four-corner fusion
Correct Answer: Scaphoid excision with four-corner fusion
Explanation:
EXPLANATION:
This patient has a physically demanding occupation. His radiographs show a long-standing nonunion with avascular necrosis and collapse of the proximal pole. This condition is referred to as a scaphoid nonunion advanced collapse wrist (SNAC). He has advanced arthritis of the capitolunate joint, but the radiolunate joint is preserved. The best option for him would be scaphoid excision with four-corner fusion. Proximal row carpectomy, would be incorrect because of the advanced arthritis of the capitolunate joint. This procedure relies on normal cartilage/joint articulation of the capitate as well as of the lunate fossa of the distal radius. Proximal pole scaphoid excision alone would not address the advanced arthritis of the capitolunate joint. Scaphoid fixation with bone grafting would not address the midcarpal arthritis and advanced proximal pole collapse.
Question 82:
A 4-year-old child sustains a spiral fracture to the tibia in an unwitnessed fall. History reveals three other fractures to long bones, and the parents are vague about the etiology of each. There is no family history of bone disease. The parents ask if the child has osteogenesis imperfecta (OI); however, there are no clinical or radiographic indications of this diagnosis. In addition to fracture care, management should include
Options:
- notification of child protective services and hospital admission.
- a punch biopsy of skin for collagen analysis.
- DNA testing for OI.
- calcium, phosphate, and alkaline phosphatase studies.
- placement of intramedullary rods to prevent further fractures.
Correct Answer: notification of child protective services and hospital admission.
Explanation:
DISCUSSION: Child abuse and OI are frequently both in the differential diagnosis of a child with multiple fractures. If OI is suspected, testing is appropriate to confirm this diagnosis. This may include skull radiographs to look for wormian bones and/or fibroblast culturing and collagen analysis of a punch biopsy. Unfortunately, because of the large number of mutations that can yield the disease, DNA testing is not commercially available for OI. In this patient, however, the physician suspects nonaccidental trauma and is legally obligated in most states to notify child protective services. Because the child may be at considerable risk of further injury, hospitalization is indicated to protect the child until child protective services can complete a home investigation and assess the degree of risk. Work-up for both OI and child abuse can be done during the hospitalization.
REFERENCES: Rockwood CA, Wilkins KE, King RE (eds): Fractures in Children. Philadelphia, PA, JB Lippincott, 1984, vol 3, pp 173-175.
Kempe CH, Silverman FN, Stelle BF, Droegemueller W, Silver HK: The battered-child syndrome. JAMA 1962;181:17-24.
Akbarnia BA, Akbarnia NO: The role of the orthopedist in child abuse and neglect. Orthop Clin North Am 1976;7:733-742.
Question 83:
Which of the following primary prognostic factors best predicts the outcome of the knee lesion shown in Figure 22?
Options:
- Location
- Size
- Knee stability
- Patient age
- Degree of pain
Correct Answer: Patient age
Explanation:
DISCUSSION: The patient has osteochondritis dissecans. While location, size, and knee stability are all relevant to the overall prognosis, studies have shown that younger patients with open growth plates have a better prognosis of healing when compared with patients who have closed growth plates. The degree of pain is also relevant to treatment, but it is subjective rather than objective and is not as reliable of a prognostic indicator as age.
REFERENCES: Stanitski CL: Osteochondritis dissecans of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 387-405.
Cahill B: Treatment of juvenile osteochondritis dissecans and osteochondritis dissecans of the knee. Clin Sports Med 1985;4:367-384.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
Question 84:
An 11-year-old boy has had a fever and pain and swelling over the lateral aspect of his right ankle for the past 3 days. Examination reveals warmth, swelling, and tenderness over the lateral malleolus, and he has a temperature of 103.2 degrees F (39.5 degrees C). Laboratory studies show a WBC count of 13,200/mm 3 with 61% neutrophils, an erythocyte sedimentation rate of 112 mm/h, and a C-reactive protein of 15.7. Radiographs and a T 2 -weighted MRI scan are shown in Figures 13a through 13c. Aspiration yields 1 mL of purulent fluid. Management should now consist of
Options:
- oral antibiotics and a follow-up office appointment the next day.
- incision and drainage of the distal fibular metaphysis.
- indium-labeled WBC scan.
- antituberculous medication for 6 months.
- three-phase technetium Tc 99m bone scan.
Correct Answer: incision and drainage of the distal fibular metaphysis.
Explanation:
DISCUSSION: The initial signs and symptoms of acute hematogenous osteomyelitis vary widely but usually include fever, bone pain, and impaired use of the involved extremity. In lower extremity infections, the child may limp or refuse to walk. Examination often reveals bone tenderness. In more advanced cases, erythema, warmth, and swelling may be present. The WBC and neutrophil counts are not always elevated, but the erythocyte sedimentation rate will be abnormal in more than 90% of patients. When the infection is diagnosed early, before a subperiosteal abscess has formed, antibiotics alone may be adequate to treat the infection. This patient has a more advanced infection, however, with the MRI scan revealing a subperiosteal abscess that was confirmed by aspiration. When an abscess is present, surgical drainage is generally indicated to remove devitalized tissue and to enhance the efficacy of the antibiotics. Further studies, such as bone or indium scans, are not necessary and will delay
definitive treatment.
REFERENCES: Scott RJ, Christofersen MR, Robertson WW Jr, et al: Acute osteomyelitis in children: A review of 116 cases. J Pediatr Orthop 1990;10:649-652.
Vaughan PA, Newman NM, Rosman MA: Acute hematogenous osteomyelitis. J Pediatr Orthop 1987;7:652-655.
Question 85:
Which of the following findings is a relative contraindication to primary total knee arthroplasty?
Options:
- Incompetent anterior cruciate ligament
- Incompetent posterior cruciate ligament
- Incompetent extensor mechanism
- Flexion contracture of 20 degrees
- Previous high tibial valgus osteotomy
Correct Answer: Incompetent extensor mechanism
Explanation:
DISCUSSION: Contraindications to primary total knee arthroplasty include active infection, an incompetent extensor mechanism, compromised vascularity in the extremity, and local neurologic disruption affecting the competence of the musculature about the knee. Anterior cruciate, posterior cruciate, or lateral ligament incompetence can be managed with primary total knee arthroplasty. Mild flexion contracture and previous high tibial valgus osteotomy are not contraindications to primary total knee arthroplasty.
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 513-536.
Question 86:
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Options:
- Fourth cervical nerve root
- Upper trunk of the brachial plexus
- Middle trunk of the brachial plexus
- Lateral cord of the brachial plexus
- Axillary nerve
Correct Answer: Upper trunk of the brachial plexus
Explanation:
The athlete has symptoms referable to the axillary, musculocutaneous, and suprascapular nerves resulting from an injury to the upper trunk of the brachial plexus. This portion of the plexus is formed by contributions of the fourth through sixth cervical nerve roots. This area is often contused or stretched following a tackling maneuver that results in either depression of the shoulder from contact at Erb’s point or traction of the upper plexus from forced stretching of the neck to the contralateral side.
Question 87:
A 15-year-old boy has had pain in the right shoulder for the past 3 months. He denies any history of trauma and has no constitutional symptoms. Examination reveals a large firm mass in the proximal arm. A radiograph and MRI scan are shown in Figures 27a and 27b. Biopsy specimens are shown in Figures 27c and 27d. Management should consist of
Options:
- observation.
- steroid injection.
- curettage and bone grafting.
- wide resection with neoadjuvant chemotherapy.
- debridement, irrigation, and intravenous antibiotics.
Correct Answer: curettage and bone grafting.
Explanation:
DISCUSSION: The patient has an aneurysmal bone cyst. The fluid-fluid levels seen on the MRI scan are typical for aneurysmal bone cyst, and the histology is consistent with a cystic lining. Vascular lakes, multinucleated giant cells, reactive bone, fibrovascular tissue, and an absence of atypical cells or numerous mitoses are seen histologically. Aneurysmal bone cysts will typically continue to grow and cause further bone destruction; therefore, observation is not recommended. Steroid injections are not effective. A thorough curettage of the cyst lining and bone grafting are required. Wide resection and chemotherapy are reserved for more aggressive tumors. There is no evidence of infection radiographically or histologically. Telangiectatic osteosarcoma should also be considered in the differential diagnosis; therefore, biopsy is an important part of the work-up.
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 232-233.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-196.
Question 88:
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?
Options:
- Inadequate physical therapy
- Exposure of the periosteum of the lateral ulna during surgery
- Inappropriate location of the suture anchor
- Fixation of the tendon with the forearm fully pronated
- Subluxation of the radial head
Correct Answer: Exposure of the periosteum of the lateral ulna during surgery
Explanation:
DISCUSSION: The radiographs show early ectopic bone formation originating between the ulna and the radius. The development of ectopic bone in this area following a two-incision approach for anatomic repair of the distal biceps tendon is thought to be related to exposure of the periosteum of the lateral ulna during surgery. This can be avoided by the use of a muscle-splitting incision between the extensor carpi ulnaris and common extensor muscles. Full pronation of the forearm allows for the necessary exposure of the radial tuberosity during the procedure and for fixation of the tendon at its maximal length.
REFERENCES: Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 89:
A 16-year-old football player is participating in the second session of two-a-day preseason practices. He complains of dizziness and fatigue. He is brought to the sideline by the athletic trainer where examination demonstrates confusion and disorientation. Ambient temperature is 82°F. What would be the next most appropriate step in his treatment?
Options:
- Rapid cooling via ice bath, cold water and fans
- Transportation via ambulance to a local emergency department
- Rapid rehydration via oral and IV fluids
- Immediate administration of acetaminophen or other anti-pyretics
Correct Answer: Rapid cooling via ice bath, cold water and fans
Explanation:
Heat exhaustion and heat stroke reflect varying degrees of heat illness, with both marked by increased heat production with impaired heat dissipation. Heat exhaustion typically involves a core body temperature between 37°C (98.6°F) and 40°C (104°F) and usually presents with heavy sweating, as well as nausea; vomiting; headache; fainting; weakness; and cold or clammy skin. Fatigue, malaise, and dizziness may occur, but necessary to the diagnosis is normal mentation and stable neurologic status. Heat stroke is defined by a core body temperature >40°C (>104°F) and disturbances of the central nervous system, such as confusion, irritability, ataxia, and even coma. Heat exhaustion is a less urgent scenario and can usually be treated with rest, elevation, and rehydration. Heat stroke, confirmed here by the presence of mental status changes, is a more critical situation. The most important immediate step is rapid body cooling through whatever means are available, as this has been clearly shown to improve outcomes. Ideally, a whole body ice bath would be used, with ice towels, ice packs, cold water, and air fans all utilized if needed. Emergency department transportation and rehydration may be considered as well but are not as important as immediate lowering of body temperature. Anti-pyretics have no role in this process.
Question 90:
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Options:
- Posttraumatic arthritis of the subtalar joint
- Posttraumatic arthritis of the ankle joint
- Malunion of the talus
- Osteonecrosis of the talus
- Complex regional pain syndrome
Correct Answer: Malunion of the talus
Explanation:
DISCUSSION: Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction.
REFERENCES: Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its affects on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Question 91:
The direct anterior (Smith-Peterson) approach to hip arthroplasty is most commonly associated with injury to what nerve?
Options:
- Lateral femoral cutaneous
- Sciatic
- Pudendal
- Superior gluteal
Correct Answer: Lateral femoral cutaneous
Explanation:
DISCUSSION:
Some authors have reported the incidence of lateral femoral cutaneous nerve neuropraxia following hip arthroplasty with the direct anterior approach to be near 80%, but resolution of the sensory deficits has been observed in most patients over time. Femoral nerve palsy has been reported to occur in .64% to 2.3% direct lateral (Hardinge) and anterolateral (Watson-Jones) approaches, and the superior gluteal nerve may be injured with proximal extension of the abductor muscular dissection. The posterior approach has been reported to be associated with sciatic nerve injury, especially in cases of dysplasia. Pudendal nerve injury has not been reported with the anterior, anterolateral, direct lateral, or posterior approaches to hip
arthroplasty. It has been reported following hip arthroscopy and the use of a traction table, however.
Question 92:
Which of the following cannulated screw configurations used in the treatment of subcapital femoral neck fractures is optimal?
Options:
- Inverted triangle pattern with the inferior screw posterior to midline and adjacent to the calcar
- Inverted triangle pattern with the inferior screw anterior to midline and adjacent to the calcar
- Triangle pattern with the superior screw posterior to midline and adjacent to the calcar
- Inverted triangle pattern with the inferior screw posterior to midline and central in the femoral neck
- Inverted triangle pattern with the inferior screw anterior to midline and central in the femoral neck
Correct Answer: Inverted triangle pattern with the inferior screw posterior to midline and adjacent to the calcar
Explanation:
DISCUSSION: The strongest portion of the femoral neck is the posterior inferior neck in the region of the femoral calcar. The optimal biomechanical configuration includes an inverted triangle pattern with the single screw in the posterior inferior aspect of the femoral neck adjacent to the calcar.
Booth et al performed a cadaveric study comparing central versus calcar (cortical-adjacent) fixation. The results demonstrated significant improved stability, load, stiffness, and displacement in all tested parameters for the group with calcar-adjacent screw fixation.
Lindequist and Törnkvist performed a Level 4 study of 72 femoral neck fractures. They found that all 5 of their nonunions had screws placed greater than 3mm from the femoral calcar. Additionally, 16 of 18 fractures healed in the group of displaced fractures where both the fixating screws were placed within 3 mm from the femoral neck cortex.
Gurusamy et al performed a Level 4 study of 395 patients undergoing femoral neck fixation. They found a reduced spread of the screws on the lateral view was associated with an increased risk of nonunion of the fracture.
Illustration A depicts the optimal configuration of an inverted triangle with the single screw being inferior and all of the screws being cortical adjacent.
Question 93:
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management?
Options:
- Incision and drainage of the abscess
- Nonsteroidal anti-inflammatory drugs, physical therapy, and a repeat MRI scan in 6 to 8 weeks
- Open biopsy
- Hematoma evacuation and musculotendinous repair
- Primary wide resection followed by radiation therapy
Correct Answer: Nonsteroidal anti-inflammatory drugs, physical therapy, and a repeat MRI scan in 6 to 8 weeks
Explanation:
DISCUSSION: The history, examination, and MRI scan findings are consistent with a midsubstance partial rupture of the rectus femoris muscle. This is an injury masquerading as a “pseudo tumor.” The lack of an appreciable mass effect on the T
1
-weighted MRI scan, the defined fluid signal on the T
2
-weighted scans, and the lack of significant contrast enhancement after gadolinium are all most consistent with injury rather than a neoplasm. Most of these injuries respond to nonsurgical management; a few will benefit from late debridement and repair if symptoms fail to resolve in 3 to 6 months. The treatment of choice is nonsurgical management with a follow-up MRI scan to verify that the findings are resolving.
REFERENCES: Hughes C IV, Hasselman CT, Best TM, et al: Incomplete, intrasubstance strain injuries of the rectus femoris muscle. Am J Sports Med 1995;23:500-506.
Temple HT, Kuklo TR, Sweet DE, et al: Rectus femoris muscle tear appearing as a pseudotumor. Am J Sports Med 1998;26:544-548.
Question 94:
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
Options:
- splinting for 5 weeks.
- active range-of-motion exercises after 1 to 3 days.
- delayed passive stretching at 2 weeks.
- open medial collateral ligament reconstruction.
- open lateral collateral ligament reconstruction.
Correct Answer: active range-of-motion exercises after 1 to 3 days.
Explanation:
DISCUSSION: The elbow usually is stable after reduction in most elbow dislocations. Ross and associates reported that supervised motion begun immediately after reduction was effective in uncomplicated dislocations. The elbow will become stiff if immobilization is applied for an extended period of time. Immediate open treatment is not indicated for a simple elbow dislocation.
REFERENCES: Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
O’Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
Question 95:
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What other finding may be noted in patients with this diagnosis?
Options:
- Symmetric knee pathology
- Excessive joint laxity
- Recurrent patella instability
- Extra-articular manifestations
Correct Answer: Symmetric knee pathology
Explanation:
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral
discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.
Question 96:
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?
Options:
- Overall kyphosis gradually decreases.
- Overall lumbar lordosis gradually decreases.
- The sagittal vertical line dropped from C7 gradually moves posteriorly relative to the sacrum.
- Cervical scoliosis develops.
- Coronal balance shifts laterally from the midsacrum.
Correct Answer: Overall lumbar lordosis gradually decreases.
Explanation:
DISCUSSION: The primary change that takes place in the aging spine is degeneration of the lumbar disks and loss of the overall lumbar lordosis. This also may be associated with osteopenic-related compression fractures. With these changes, the sagittal vertical line moves anteriorly relative to the sacrum; cervical scoliosis is uncommon and not part of the normal aging process. Overall kyphosis in the thoracic spine gradually increases, but the coronal balance remains essentially the same unless scoliosis develops.
REFERENCES: Gelb DE, Lenke LG, Bridwell KH, et al: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20:1351-1358.
Vedantam R, Lenke LG, Keeney JA, et al: Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine 1998;23:211-215.
Question 97:
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Options:
- Axillary nerve in the posterolateral space
- Dorsal scapular nerve at the medial border of the scapula
- Suprascapular nerve in the scapular notch
- Suprascapular nerve in the spinoglenoid notch
- Subscapular nerve at the rotator interval
Correct Answer: Suprascapular nerve in the spinoglenoid notch
Explanation:
DISCUSSION: Suprascapular deficits, as the result of repetitive forceful internal rotation with overhead ball striking, occur in the spinoglenoid notch. Compression interferes with distal suprascapular nerve innervation to the infraspinatus, while allowing the supraspinatus to function normally. A scapular notch entrapment of this nerve would involve both the supraspinatus and the infraspinatus. The axillary, dorsal scapular, and subscapular nerves do not affect the infraspinatus.
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 98:
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?
Options:
- Observation
- Revision and removal of any remaining gross disease
- Hemipelvectomy
- Exploration and repeat curettage
- Hip disarticulation
Correct Answer: Hemipelvectomy
Explanation:
DISCUSSION: The definitive surgery would be removal of the entire resection bed, and in this case of dedifferentiated chondrosarcoma, a hemipelvectomy was performed. The MRI and CT scans show an aggressive cartilage lesion. The histology, representative of a dedifferentiated chondrosarcoma, shows a bimorphic low-grade cartilage lesion with high-grade spindle cell sarcoma. The cartilage lesion is usually an enchondroma or low-grade chondrosarcoma. The dedifferentiated portion is typically a malignant fibrous histocytoma, osteosarcoma, or fibrosarcoma.
REFERENCES: Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642
Question 99:
Which of the following best describes athletic pubalgia?
Options:
- A syndrome of lower abdominal and adductor pain
- Painful symptoms emanating from the symphysis pubis
- Painful symptoms associated with dysfunction of the iliopsoas tendon
- Stress fracture of the pubic ramus
- Entrapment of the pudendal nerve
Correct Answer: A syndrome of lower abdominal and adductor pain
Explanation:
DISCUSSION: Athletic pubalgia refers to a distinct syndrome of lower abdominal and adductor pain that is mostly commonly seen in high performance male athletes. This condition must be distinguished from others such as painful inflammation of the symphysis pubis, referred to as osteitis pubis. Symptoms attributable to the iliopsoas tendon are most commonly associated with snapping of the tendon. Stress fracture of the pubic ramus may cause symptoms in this area, but it is usually confirmed by imaging studies. Neurapraxia of the pudendal nerve is associated with pressure from the seat in cycling sports and also as a complication associated with traction during surgical procedures.
REFERENCES: Meyers WC, Foley DP, Garrett WE, Lohnes JH, Mandlebaum BR: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Albers SL, Spritzer CE, Garrett WE Jr, Meyers WC: MR findings in athletes with pubalgia. Skeletal Radiol 2001;30:270-277.
Question 100:
An AP radiograph of the pelvis is shown in Figure 4. What muscle attaches to the avulsed fragment of bone identified by the arrow?
Options:
- Short head of the biceps femoris
- Adductor longus
- Pectineus
- Piriformis
- Semitendinosus
Correct Answer: Semitendinosus
Explanation:
DISCUSSION: The radiograph reveals an avulsion of the ischial apophysis, most likely the result of violent contraction of the attached hamstring tendons (semimembranosus, semitendinosus, and long head of the biceps femoris). The short head of the biceps femoris arises from the linea aspera on the posterior femur. The pectineus and adductor longus attach to the pubic portion of the pelvis. The piriformis runs from the sacrum to the femur.
REFERENCES: Woodburne RT (ed): Essentials of Human Anatomy. New York, NY, Oxford University Press, 1978, pp 542-545.
Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.