Full Question & Answer Text (for Search Engines)
Question 1:
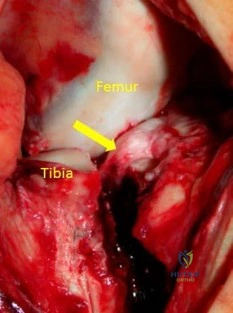
A 22-year-old woman sustains the injury seen in Figure 12 as a result of a motor vehicle crash. What factor is most closely associated with development of osteonecrosis?
Options:
- Reduction quality
- Time from injury to surgery
- Presence or absence of a capsulotomy
- Type of implant used for internal fixation
- Location of the fracture within the femoral neck
Correct Answer: Reduction quality
Explanation:
A displaced femoral neck fracture in a young patient is considered a surgical urgency and prompt anatomic reduction and internal fixation is recommended. There are a few studies that have specifically looked at the rate of osteonecrosis in this patient population. A review of femoral neck fractures in patients ages 15 to 50 years revealed that the incidence of osteonecrosis in displaced fractures was 27% compared with 14% in nondisplaced fractures. The quality of the reduction also influenced the rate of osteonecrosis. Time to reduction, type of implant, presence or absence of capsulotomy, and location of the fracture are not associated with osteonecrosis risk.
(SBQ12TR.90) A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management?
Review
Topic
MRI angiography of leg
Four-compartment fasciotomy
Follow-up examination the following day
Continued monitoring and serial examinations
EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam.
An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy. However, the treatment of early compartment syndrome should be to initially improve the limbs perfusion pressure gradient. This can be done by treating underlying factors such as hypotension, coagulopathy, or vascular compromise due to either a true vascular injury or artificially by external compression. Frequent reassessment is then critical to effectively manage these patients. If clinical diagnosis persists despite these efforts, urgent fasciotomy would be considered.
McQueen looked at 116 patients with tibial diaphyseal fractures who had continuous monitoring of anterior compartment pressure for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of 30 mmHg is a more reliable indicator of compartment syndrome.
White et al. looked at 101 patients with tibial fractures with satisfactory Delta P measurements. THey found that patients with elevated intramuscular pressures >30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P <30 mm Hg.
Figure A shows a Shatzker V tibial plateau fracture. Figure B shows fixation of fracture seen in Figure A.
Incorrect Answers:
30 mm Hg or persistently elevated absolute compartment pressures.. Answer 3: It would not be appropriate to leave this patient with impending compartment syndrome.
(SBQ12TR.57) A 56-year-old right hand dominant attorney falls from standing and sustains the closed injury shown in Figure A. The treating surgeon elects to fix her fracture using a plate and screw construct. Based on the available imaging, which of the following fracture characteristics best justifies this fixation choice?
Fracture displacement
Intra-articular fracture extension
The fracture extends distal to the coronoid
Oblique fracture line
Fracture comminution
This patient has a displaced, intra-articular, comminuted olecranon fracture. Comminution is an indication for plate fixation.
Most displaced olecranon fractures are treated operatively. Options include tension band constructs, intramedullary screws, plate and screw fixation or fragment excision with triceps advancement. Any construct relying on inter-fragmentary compression (tension band, intramedullary screws) requires a non-comminuted fracture pattern. Plate fixation is indicated in the setting of comminution, extension past the coronoid, or in the setting of associated instability.
Bailey et al. retrospectively reviewed 25 patients who underwent plate fixation of displaced olecranon fractures. Twenty-two of 25 patients had good or excellent outcomes. Five of 25 patients (20%) of patients required plate removal for symptomatic hardware. The authors concluded that plate fixation was an effective treatment for displaced olecranon fractures, with good functional outcomes.
Figure A shows a displaced, comminuted olecranon fracture without evidence of propagation past the coronoid.
Incorrect answers:
congruity but does not dictate implant selection. Answer 3. Extension distal to the coronoid is an indication for plate fixation but there is no evidence of such extension on the radiograph shown Answer 4. This fracture is comminuted, without a distinct fracture line.
Question 2:
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury? Review Topic
Options:
- Inlet and outlet views of the pelvis to better delineate the injury
- Angiography
- Laparotomy
- Open reduction and internal fixation of the pelvis
- Placement of a pelvic binder around the patient
Correct Answer: Placement of a pelvic binder around the patient
Explanation:
This hypotensive patient has an obvious open book injury of the pelvic ring on the AP pelvis radiograph and further radiographs are not needed prior to the initiation of treatment. Although angiography may be indicated if he does not respond to stabilization of his pelvis and fluid/blood administration, temporary stabilization of the pelvis with a sheet or binder should be performed first because it is simple, quick, and has been shown to be effective. This patient does not need a laparotomy at this point since the FAST examination did not show any free intra-abdominal fluid and his chest radiograph was unremarkable, leaving the most likely source of bleeding the pelvic fracture. Open reduction with internal fixation of a pelvic injury is not indicated in an acutely ill patient.
Question 3:
Figures 23a and 23b show the AP and lateral radiographs of a 67-year-old woman who has severe left knee pain when ambulating. History reveals that she underwent primary total knee arthroplasty 7 years ago. The patient reports increasing deformity over the past several years and uses a knee brace and a cane. Examination reveals that she walks with a varus thrust and has an uncorrectable varus deformity with valgus force. What is the primary reason for implant failure?
Options:
- Osteolysis
- Polyethylene wear
- Tibial component fixation failure
- Modular tibial component failure
- Posterior cruciate ligament retention
Correct Answer: Tibial component fixation failure
Explanation:
DISCUSSION: Both cemented and cementless total knee arthroplasties depend on adequate fixation of the tibial component to promote long-term survivorship. An effective stem and adequate peripheral fixation of the tibial component to the cancellous-cortical portion of the proximal tibia are necessary for cementless fixation. Peripheral screws and pegs can serve as adjunctive fixation to decrease micromotion and shear forces and allow bone ingrowth to occur. Careful preparation of the proximal tibial surface can minimize fixation failure. Cemented fixation of the tibial stem should be performed in addition to the plateau. Osteolysis, polyethylene wear, and failure at the insert/tray locking mechanism have not occurred. Posterior cruciate ligament retention has not caused the tibial component fixation failure.
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 275-279.
Question 4:
A 24-year-old professional male soccer player has lower abdominal pain on exertion. He has pain with resisted hip adduction and with sit-ups. There is no palpable inguinal hernia with a Valsalva maneuver. Nonsurgical management has failed to provide relief. After ruling out malignancies, what is the next most appropriate step in management? Review Topic
Options:
- Additional nonsurgical management
- Referral to a sports hernia surgeon
- Ultrasound of the scrotum
- CT of the pelvis
- Cortisone injection
Correct Answer: Referral to a sports hernia surgeon
Explanation:
The patient has a sports hernia or athletic pubalgia. The exact nature of this pathology is not well understood. MRI scans are not very helpful in making a diagnosis. In high-performance athletes who have failed to respond to nonsurgical management, surgical intervention is needed to strengthen the anterior pelvic floor. Additional nonsurgical management at this point will not improve symptoms. Cortisone injection will not strengthen the pelvic floor. CT scan of the pelvis is valuable to rule out bony injuries such as osteitis pubis. Ultrasound of the scrotum will have no additional diagnostic use in management of this patient.
Question 5:
Figures below show the radiographs obtained from a 19-year-old woman with a 3-year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?
Options:
- Hip arthroscopy with labral repair B. Reverse periacetabular osteotomy C. Varus rotational osteotomy
- Open surgical dislocation with rim trimming
Correct Answer: Open surgical dislocation with rim trimming
Explanation:
DISCUSSION:
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 6:
A 12-year-old girl has had pain in her right knee for 1 month that started as activity-related and progressed to night pain. Radiographs are shown in Figures 16a and 16b, and a biopsy specimen is shown in Figure 16c. What is the recommended treatment?
Options:
- Resection of the distal femur and postoperative chemotherapy
- Preoperative chemotherapy followed by radiation therapy, then resection of the distal femur
- Preoperative chemotherapy followed by surgical resection of the lesion and postoperative chemotherapy
- Preoperative chemotherapy followed by radiation therapy, resection of the distal femur, then postoperative chemotherapy
- Resection of the distal femur followed by radiation therapy
Correct Answer: Preoperative chemotherapy followed by surgical resection of the lesion and postoperative chemotherapy
Explanation:
DISCUSSION: This is a classic appearance for an osteosarcoma. The radiographs reveal a mixed osteolytic and osteoblastic lesion in a skeletally immature patient in the distal right femoral metaphysis. The pain pattern with progressive symptoms leading to the presence of night pain is also typical for this condition. The biopsy specimen reveals pleomorphic cells and the presence of osteoid. The current standard of care in the treatment of osteosarcoma is neoadjuvant chemotherapy followed by surgical resection or amputation followed by additional postoperative chemotherapy. Osteosarcoma is not radiosensitive.
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 205.
Question 7:
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of
Options:
- open reduction and internal fixation.
- a short leg cast for 6 weeks.
- ankle arthroscopy, removal of the fragment, and drilling of the base of the lesion.
- ankle arthroscopy and internal fixation.
- functional ankle rehabilitation that emphasizes range of motion, peroneal strengthening, and proprioceptive training.
Correct Answer: ankle arthroscopy, removal of the fragment, and drilling of the base of the lesion.
Explanation:
DISCUSSION: Osteochondral fractures involving the talar dome have been classified based on radiographic and MRI findings. A nondisplaced and incomplete fracture may be treated effectively with a short leg cast and no weight bearing for 6 weeks. This patient has a complete, separated, and displaced osteochondral fragment involving the midlateral talar dome that will most likely cause pain, mechanical symptoms, and effusion if treated nonsurgically. In addition, there is very little bone remaining on the fragment, making the likelihood of healing with open reduction and internal fixation problematic. The treatment of choice includes arthroscopy, removal of the loose fragment, curettage or drilling of the base, and a rehabilitation program that emphasizes peroneal strengthening, range of motion, and proprioceptive training.
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Baker CL, Morales RW: Arthroscopic treatment of tranchondral talar dome fractures: A long-term follow-up study. Arthroscopy 1999;15:197-202.
Question 8:
-The World Health Organization Fracture Risk Assessment Tool (FRAX) calculates which fracture risk?
Options:
- year risk for hip fracture
- year risk for distal radius fracture
- year risk for any fragility fracture
- year risk for hip fracture
- year risk for distal radius fracture
Correct Answer: year risk for hip fracture
Question 9:
A patient who underwent a total knee arthroplasty (TKA) 4 years ago reports acute knee pain 2 days following dental surgery. Knee joint aspiration demonstrates 40000 white blood cells/µL with 90% neutrophils. An aspirate culture grows peptostreptococcus. Treatment should consist of
Options:
- intravenous (IV) antibiotics only.
- arthroscopic debridement and IV antibiotics.
- irrigation, debridement, polyethylene liner exchange, and IV antibiotics.
- stage exchange and IV antibiotics.
Correct Answer: irrigation, debridement, polyethylene liner exchange, and IV antibiotics.
Explanation:
DISCUSSION
This patient has an acute hematogenous infection of a TKA. Irrigation, debridement, polyethylene liner exchange, and IV antibiotics remain the treatments of choice. However, failure of this approach has been reported in 20% to 60% of cases in various series, particularly when methicillin-resistant streptococcus aureus or methicillin-resistant streptococcus epidermis is isolated.
Question 10:
A 62-year-old patient is seen for routine follow-up after undergoing cementless total hip arthroplasty 2 years ago. The patient reports limited range of motion that severely affects daily activities. A radiograph is shown in Figure 51. Management should now consist of
Options:
- observation only.
- nonsteroidal anti-inflammatory drugs and protected weight bearing.
- irradiation to the affected area.
- surgical excision.
- surgical excision and postoperative irradiation.
Correct Answer: surgical excision and postoperative irradiation.
Explanation:
DISCUSSION: The patient has symptomatic postoperative heterotopic ossification after total hip arthroplasty. Postoperative prophylactic treatments include nonsteroidal anti-inflammatory drugs (usually indomethacin) or low-dose irradiation. The heterotopic ossification shown here is quite mature; therefore, nonsurgical management will not be successful. Surgical excision of grade III or IV heterotopic ossification should be followed with postoperative irradiation to minimize the chances of recurrence.
REFERENCES: Ayers DC, Evarts CM, Parkinson JR: The prevention of heterotopic ossification in high-risk patients by low-dose radiation therapy after total hip arthroplasty. J Bone Joint Surg Am 1986;68:1423-1430.
Healy WL, Lo TC, DeSimone AA, et al: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595.
Question 11:
A study is proposed in which 50 patients with osteonecrosis of the knee are compared with 23 patients without osteonecrosis in terms of their alcohol consumption levels. This is an example of what type of study?
Options:
- Case control
- Cohort
- Cross-sectional
- Randomized
- Longitudinal
Correct Answer: Case control
Explanation:
In a case control study, all the subjects are selected based on whether they have (cases) or do not have (controls) the disease or outcome of interest. Case control studies are retrospective as they always look back to see how a certain risk factor may be different between the two groups. The main aspect of a cross-sectional study is that it is designed to look at a representative sample of the entire population of interest at a single point in time. Longitudinal studies follow groups of subjects over a period of time. A cohort study follows a particular group in relation to an event, studying them at intervals in time and uses objective outcome criteria. In a randomized controlled study, subjects are divided randomly into control and experimental groups to balance both the known and unknown differences between the groups.
Question 12:
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and
Options:
- distraction interpositional arthroplasty.
- elbow arthrodesis.
- conversion to a resection arthroplasty.
- conversion to semiconstrained elbow arthroplasty.
- revision to unconstrained total elbow arthroplasty.
Correct Answer: conversion to semiconstrained elbow arthroplasty.
Explanation:
DISCUSSION: An unconstrained prosthesis dislocation is a disconcerting problem that is not easily resolved; however, revision to a semiconstrained prosthesis would best achieve both pain relief and stability. Removal of the components and distraction arthroplasty or conversion to a resection arthroplasty are options, but the results would be unpredictable with regards to pain relief, postoperative motion, or elbow stability. Arthrodesis is poorly tolerated. With revision to another unconstrained prosthesis, there is the risk of continued redislocation because of chronic ligamentous insufficiency.
REFERENCES: Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Morrey BF, King GJ: Revision of failed total elbow arthroplasty, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 685-700.
Question 13:
Figure 16 shows the clinical photograph of a 3-month-old infant with a foot deformity that has been nonprogressive since birth. Examination reveals that the deformity corrects actively and with passive manipulation. There is no associated equinus. Management should consist of
Options:
- serial casting.
- UCBL orthotics.
- abductor hallucis lengthening.
- observation and parental reassurance.
- corrective shoes.
Correct Answer: observation and parental reassurance.
Explanation:
DISCUSSION: The patient has bilateral metatarsus adductus deformities. In a long-term follow-up study by Farsetti and associates, deformities that were passively correctable spontaneously resolved and no treatment was required. More rigid deformities were successfully treated with serial manipulation, with good results in 90%. There were no poor results. Therefore, observation is the management of choice for passively correctable deformities. In feet that are more rigid, serial manipulation and casting is the management of choice.
REFERENCE: Farsetti P, Weinstein SL, Ponseti IV: The long-term functional and radiographic outcomes of untreated and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265.
Question 14:
Figure 35 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?
Options:
- Transforming growth factor-beta (TGF-ß), bone morphogenetic protein-2 (BMP-2), latent membrane protein 1
- Tissue inhibitor of matrix metallo-proteinase-1 (MMP-1), growth and development factor-5, noggin
- Gremlin, MMP, biglycan
- Tumor necrosis factor-alpha (TNF-a), Interleukin-1 (IL-1), MMP
Correct Answer: Tumor necrosis factor-alpha (TNF-a), Interleukin-1 (IL-1), MMP
Explanation:
DISCUSSION
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-a, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-ß, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
RECOMMENDED READINGS
Kim HT, Yoon ST, Jarrett C. Articular cartilage and intervertebral disk. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:23-33.
Hoyland JA, Le Maitre C, Freemont AJ. Investigation of the role of IL-1 and TNF in matrix degradation in the intervertebral disc. Rheumatology (Oxford). 2008 Jun;47(6):809-14. doi: 10.1093/rheumatology/ken056. Epub 2008 Apr 8. PubMed PMID: 18397957.
View Abstract
at PubMed
Gruber HE, Ingram JA, Hanley EN Jr. Immunolocalization of MMP-19 in the human intervertebral disc: implications for disc aging and degeneration. Biotech Histochem. 2005 May-Aug;80(3-4):157-62. PubMed PMID: 16298901.
View Abstract at PubMed
Question 15:
A 52-year-old woman slips in her bathroom and strikes her right hand on a cabinet. She notes swelling, ecchymosis, and pain with attempted motion. There are no open wounds. Radiographs are shown in Figures 5a through 5c. What is the most appropriate treatment?
Options:
- Immobilization of the hand with the metacarpophalangeal (MCP) joints in flexion and the interphalangeal (IP) joints in extension
- Immobilization of the hand with the MCP joints in extension and the IP joints in extension
- Percutaneous pinning of the proximal phalanx
- Open reduction and internal fixation of the proximal phalanx
- Early motion and pain management
Correct Answer: Immobilization of the hand with the metacarpophalangeal (MCP) joints in flexion and the interphalangeal (IP) joints in extension
Explanation:
DISCUSSION: Nondisplaced transverse fractures of the phalanges are stable. Immobilization in the intrinsic plus position will prevent MCP joint stiffness. Displaced oblique fractures are more at risk for instability.
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.
Question 16:
The spring ligament of the foot connects what two bones?
Options:
- Tibia and talus
- Talus and navicular
- Talus and calcaneus
- Calcaneus and cuboid
- Calcaneus and navicular
Correct Answer: Calcaneus and navicular
Explanation:
DISCUSSION: The spring ligament is also known as the calcaneonavicular ligament and connects the calcaneus to the navicular. This ligament supports the talar head and is an important anatomic supporting structure of the medial longitudinal arch of the foot.
REFERENCES: Choi K, Lee S, Otis JC, et al: Anatomical reconstruction of the spring ligament using peroneus longus tendon graft. Foot Ankle Int 2003;24:430-436.
Davis WH, Sobel M, DiCarlo EF, et al: Gross, histological and microvascular anatomy and biomechanical testing of the spring ligament complex. Foot Ankle Int 1996;17:95-102.
Question 17:
A 72-year-old man injured his right shoulder after tripping over a chair leg. Radiographs obtained in the emergency department reveal an isolated anterior dislocation. After successful closed reduction, the patient has recurrent anterior instability and is unable to elevate the arm. What is the most likely cause of the recurrent instability?
Options:
- Infection of the anterior glenoid labral detachment
- Anterior glenoid fracture
- Axilllary nerve palsy
- Occult surgical neck fracture
- Rotator cuff tear
Correct Answer: Rotator cuff tear
Explanation:
DISCUSSION: A rotator cuff tear is the most common cause of recurrent instability following a first-time dislocation in patients older than age 40 years. Dislocations occur through a posterior mechanism rather than by an isolated labral avulsion or a Bankart lesion as seen in younger patients.
REFERENCES: Nevaiser RJ, Nevaiser TJ: Recurrent instability of the shoulder after age 40.
J Shoulder Elbow Surg 1995;4:416-418.
Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294.
Question 18:
In the anterior cruciate ligament-deficient knee, what structure provides an important secondary restraint to anterior tibial translation? Review Topic
Options:
- Anterior horn of the lateral meniscus
- Posterior cruciate ligament
- Posterior horn of the medial meniscus
- Popliteus tendon
- Quadriceps muscle
Correct Answer: Posterior horn of the medial meniscus
Explanation:
Cadaveric studies have demonstrated the important role of the posterior horn of the medial meniscus in stabilizing the anterior cruciate ligament-deficient knee with significantly greater resultant force in the medial meniscus when subjected to anterior tibial loads. The posterior horn of the medial meniscus is thought to limit anterior tibial translation by acting as a buttress by wedging against the posterior aspect of the medial femoral condyle. The other soft tissues mentioned do not play any significant role in prevention of anterior tibial translation in the anterior cruciate ligament-deficient knee.
Question 19:
Figure 9 is the clinical photograph of a 68-year-old woman 10 days after undergoing primary total knee replacement. She is experiencing hemarthrosis, discoloration, and bruising of the soft tissue about the knee; her history includes persistent serous drainage. This clinical appearance likely is associated with
Options:
- failure to use a tourniquet.
- failure to use a drain.
- use of low-molecular-weight heparin (LMWH).
- use of regional anesthesia.
Correct Answer: use of low-molecular-weight heparin (LMWH).
Explanation:
DISCUSSION
Certain anticoagulants are associated with an increased risk for wound complications. Two studies showed an increase in postsurgical bleeding and wound drainage following use of LMWH. Other investigators have associated use of anticoagulants such as LMWH with an increased incidence of persistent wound drainage and subsequent infection. Current evidence does not support a significant difference in complication rates with and without the use of wound drains or a tourniquet. Regional anesthesia has been associated with less blood loss than general anesthesia and is not associated with a difference in wound complication incidence.
Question 20:
A 40-year-old man sustains a fall while mountain biking and presents with a posterior elbow fracture-dislocation. The elbow is reduced in the ER and noted to be grossly unstable with varus and valgus stress. Imaging demonstrates a two part radial head fracture involving 40% of the articular surface and a fracture involving less than 10% of the coronoid tip. He is taken to the OR for surgical reconstruction. After fixation of the radial head and repair of the LCL complex, the elbow is fluoroscopically examined and noted to be unstable with valgus stress. The elbow is ranged and dislocates at less than 45 degrees of flexion with the forearm in full supination. What is the next best step in management?
Options:
- Application of a hinged external fixator
- Conversion to radial head arthroplasty
- Open reduction internal fixation of the coronoid fragment
- Repair of the medial collateral ligament
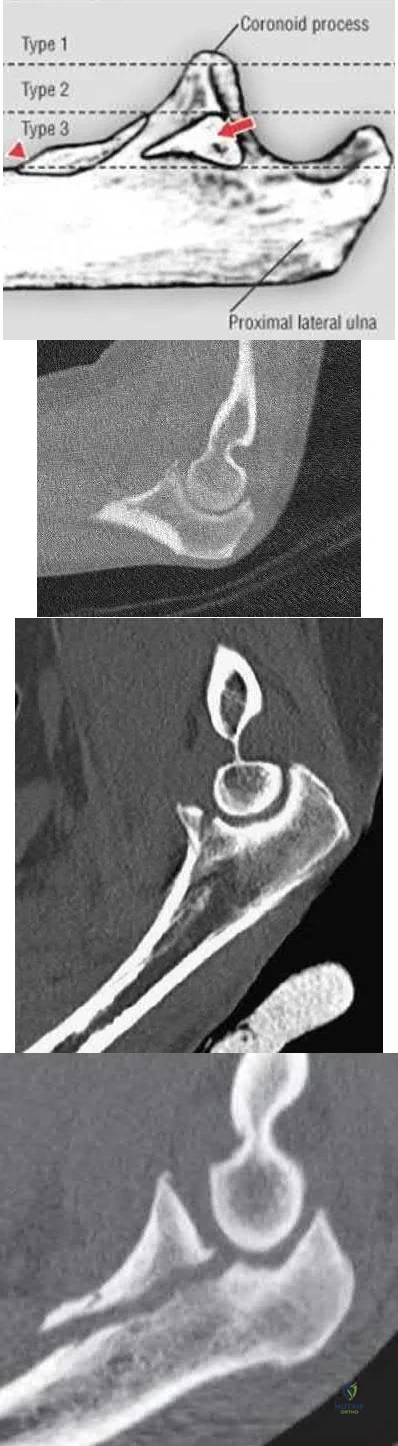
- Splint at 90 degree flexion and full pronation Corrent answer: 4 This patient has persistent elbow instability likely secondary to medial collateral ligament (MCL) rupture and therefore should undergo repair of the MCL, followed by repeat fluoroscopic examination. Small coronoid fractures involving less than or equal to 10% of the coronoid tip do not confer major elbow instability and do not necessitate repair. Terrible triad injuries of the elbow are characterized by: 1. Radial head fracture, 2. Coronoid fracture, and 3. Elbow dislocation. Whether to surgically address the coronoid fracture depends on the size of the fragment (Reagan-Morrey types I-III; Illustration A) as well as elbow stability. Reagan and Morrey suggested that small fractures of the coronoid tip (type I) involving less than 10% of the coronoid may represent anterior capsule avulsions; however, recent cadaveric studies demonstrate that the capsule inserts more distally on the tip and that small fractures often do not contain capsule insertion. Gross elbow instability in the presence of a type I fracture is most likely due to an independent MCL injury and NOT the coronoid avulsion. Surgical repair of type I fractures has not been shown to affect stability and may detrimentally affect elbow range of motion. Matthew et al reviewed the terrible triad injury of the elbow. While the coronoid process provides substantial resistance to posterior subluxation, small fractures involving 10% of the coronoid process have been shown to have little effect on elbow stability. In a cadaveric study of a simulated terrible triad injury, when residual instability was present after radial head repair or arthroplasty and lateral ulnar collateral ligament (LUCL) repair, repair of the MCL was more effective than fixation of small coronoid fractures in restoring elbow stability. However, the authors note that in clinical series of terrible triad injuries, most coronoid fragments were larger than 10%, suggesting that fixation of the coronoid process is usually part of the treatment of terrible triad injuries. Papatheodorou et al performed a retrospective analysis of 14 patients with acute terrible triad injuries and type I or type II coronoid fractures who underwent radial head fixation or arthroplasty and LUCL repair without coronoid fixation. Intraoperative stability was confirmed under fluoroscopy. At 2 year follow up, none of the patients demonstrated elbow instability. Mean elbow flexion-extension was 123 and forearm rotation 145. The authors concluded that terrible triad injuries with type I or II coronoid fractures can be treated without coronoid fixation when intraoperative stability is restored with radial head repair or arthroplasty and LUCL repair. Illustration A demonstrates the Regan-Morrey classification of coronoid fractures. Type I fractures involve < 10% of the coronoid tip and do not result in significant elbow instability. Type II fractures involve < 50% of the coronoid and may result in elbow instability secondary to loss of the anterior bony buttress that resists posterior displacement of the ulna, as well as loss of the anterior capsule insertion. These fractures are often repaired, particularly when associated with elbow instability. Type III fractures involve > 50% of the coronoid and often contain the insertion of the anterior band of the MCL (red arrow). The insertion of the brachialis (red triangle) may also be involved resulting in proximal displacement of the fracture fragment. Surgical repair of type III fractures is necessary to reconstitute the MCL and restore elbow stability. Illustration B is a CT scan of a type I coronoid fracture. Illustration C is a CT scan of a type II coronoid fracture. Illustration D is a CT scan of a type III coronoid fracture. Incorrect Answers:
Correct Answer: Splint at 90 degree flexion and full pronation Corrent answer: 4 This patient has persistent elbow instability likely secondary to medial collateral ligament (MCL) rupture and therefore should undergo repair of the MCL, followed by repeat fluoroscopic examination. Small coronoid fractures involving less than or equal to 10% of the coronoid tip do not confer major elbow instability and do not necessitate repair. Terrible triad injuries of the elbow are characterized by: 1. Radial head fracture, 2. Coronoid fracture, and 3. Elbow dislocation. Whether to surgically address the coronoid fracture depends on the size of the fragment (Reagan-Morrey types I-III; Illustration A) as well as elbow stability. Reagan and Morrey suggested that small fractures of the coronoid tip (type I) involving less than 10% of the coronoid may represent anterior capsule avulsions; however, recent cadaveric studies demonstrate that the capsule inserts more distally on the tip and that small fractures often do not contain capsule insertion. Gross elbow instability in the presence of a type I fracture is most likely due to an independent MCL injury and NOT the coronoid avulsion. Surgical repair of type I fractures has not been shown to affect stability and may detrimentally affect elbow range of motion. Matthew et al reviewed the terrible triad injury of the elbow. While the coronoid process provides substantial resistance to posterior subluxation, small fractures involving 10% of the coronoid process have been shown to have little effect on elbow stability. In a cadaveric study of a simulated terrible triad injury, when residual instability was present after radial head repair or arthroplasty and lateral ulnar collateral ligament (LUCL) repair, repair of the MCL was more effective than fixation of small coronoid fractures in restoring elbow stability. However, the authors note that in clinical series of terrible triad injuries, most coronoid fragments were larger than 10%, suggesting that fixation of the coronoid process is usually part of the treatment of terrible triad injuries. Papatheodorou et al performed a retrospective analysis of 14 patients with acute terrible triad injuries and type I or type II coronoid fractures who underwent radial head fixation or arthroplasty and LUCL repair without coronoid fixation. Intraoperative stability was confirmed under fluoroscopy. At 2 year follow up, none of the patients demonstrated elbow instability. Mean elbow flexion-extension was 123 and forearm rotation 145. The authors concluded that terrible triad injuries with type I or II coronoid fractures can be treated without coronoid fixation when intraoperative stability is restored with radial head repair or arthroplasty and LUCL repair. Illustration A demonstrates the Regan-Morrey classification of coronoid fractures. Type I fractures involve < 10% of the coronoid tip and do not result in significant elbow instability. Type II fractures involve < 50% of the coronoid and may result in elbow instability secondary to loss of the anterior bony buttress that resists posterior displacement of the ulna, as well as loss of the anterior capsule insertion. These fractures are often repaired, particularly when associated with elbow instability. Type III fractures involve > 50% of the coronoid and often contain the insertion of the anterior band of the MCL (red arrow). The insertion of the brachialis (red triangle) may also be involved resulting in proximal displacement of the fracture fragment. Surgical repair of type III fractures is necessary to reconstitute the MCL and restore elbow stability. Illustration B is a CT scan of a type I coronoid fracture. Illustration C is a CT scan of a type II coronoid fracture. Illustration D is a CT scan of a type III coronoid fracture. Incorrect Answers:
Explanation:
Question 21:
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?
Options:
- Debulking
- Wide resection with vascular and nerve grafting
- Above-elbow amputation
- Chemotherapy
- Radiation therapy
Correct Answer: Chemotherapy
Explanation:
DISCUSSION: The patient has infantile fibrosarcoma. For unresectable lesions, the treatment of choice is chemotherapy with vincristine, actinomycin-D, and cyclophosphamide, followed by excision if there is an adequate decrease in the size of the lesion.
REFERENCE: Kurkchubasche AG, Halvorson EG, Forman EN, Terek RM, Ferguson WS: The role of preoperative chemotherapy in the treatment of infantile fibrosarcoma. J Pediatr Surgery 2000;35:880-883.
Question 22:
Which of the following anatomic structures are in contact with internal impingement in the throwing athlete?
Options:
- Humerus and posterior-superior glenoid
- Humerus and anterior inferior glenoid
- Humerus and acromion
- Biceps and acromion
- Rotator cuff and acromion
Correct Answer: Humerus and posterior-superior glenoid
Explanation:
DISCUSSION: Internal impingement occurs in the late cocking phase of throwing with humeral head abduction and maximal external rotation. It is a physiologic phenomenon occurring in
85% of patients undergoing arthroscopy for various indications in one study. Internal impingement is defined as impingement of the posterior-superior rotator cuff between the humerus and posterior-superior glenoid rim. Symptomatic internal impingement is felt to be due to the frequency and magnitude of the impingement in throwers.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 252.
Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40.
Question 23:
A patient who underwent a total knee arthroplasty for osteoarthritis 18 months ago now reports the sudden development of pain in the ipsilateral knee. Radiographs and examination of the knee are unremarkable. Aspiration of the synovial fluid 3 days later reveals a WBC count of 1,500/mm 3 . The cells consist of 30% neutrophils and 70% monocytes. Culture results will not be available for several days. The patient has not been on antibiotics prior to this point. Based on these findings, what is the most appropriate management?
Options:
- Arthrotomy, debridement, and polyethylene exchange
- One-stage exchange arthroplasty
- Two-stage exchange arthroplasty
- Parenteral antibiotics
- Nonsurgical management without antibiotics
Correct Answer: Nonsurgical management without antibiotics
Explanation:
DISCUSSION: Synovial fluid analysis is a very sensitive tool for detecting infection in total knee arthroplasties. Several studies have demonstrated that an absolute leukocyte count in the synovial fluid of less than 1,700 to 2,500/mm
3
is an accurate predictor of absence of infection. Similarly, a differential cell count of the WBCs demonstrating less than 50% to 60% neutrophils is an accurate predictor of absence of infection. If both parameters are normal, it is unlikely that the patient has an infection. The three surgical options are contraindicated based on the normal examination findings and laboratory parameters. Similarly, antibiotics should be avoided. The work-up should include tests to evaluate noninfectious sources of knee pain and sources of referred knee pain.
REFERENCES: Trampuz A, Hanssen AD, Osmon DR, et al: Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med 2004;117:556-562.
Mason JB, Fehring TK, Odum SM, et al: The value of white blood cell counts before revision total knee arthroplasty. J Arthroplasty 2003;18:1038-1043.
Kersey R, Benjamin J, Mason B: White blood cell counts and differential in synovial fluid of aseptically failed total knee arthroplasty. J Arthroplasty 2000;15:301-304.
Question 24:
Which of the following choices best describes the fracture pattern shown in Figures 2a through 2c?
Options:
- Anterior column
- Anterior wall
- Posterior column
- Both column
- Transverse
Correct Answer: Posterior column
Explanation:
DISCUSSION: The fracture pattern shown in the radiographs is a fracture of the posterior column. The only line interrupted on the AP pelvis is the ilioischial line. The obturator oblique view shows that the iliopectineal line is intact as is the outline of the posterior wall. The iliac oblique view shows an interruption of the ilioischial line and an intact anterior wall. Therefore, this fracture is a fracture of the posterior column.
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1009-1149.
Question 25:
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?
Options:
- Pain during sitting; flexion abduction and external rotation of the hip
- Groin pain; pain with internal rotation and adduction while supine with the hip and knee flexed 90°
- Clicking; abductor lurch
- Buttock pain; pain with hip extension, adduction, and external rotation while prone
Correct Answer: Groin pain; pain with internal rotation and adduction while supine with the hip and knee flexed 90°
Explanation:
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge score cannot be determined presurgically.
Question 26:
A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of
Options:
- anterior diskectomy and fusion at C4-C5.
- immobilization in a Philadelphia collar and voluntary flexion and extension radiographs when awake.
- occipital-cervical fusion with instrumentation.
- halo immobilization for 12 weeks.
- left C6 superior facetectomy and posterior fusion at C6-C7 with instrumentation.
Correct Answer: occipital-cervical fusion with instrumentation.
Explanation:
DISCUSSION: The CT scans reveal an occipital-cervical dissociation with subluxation of the occipitocervical joints bilaterally. Definitive management should consist of an occipital-cervical fusion with instrumentation. Immobilization in a Philadelphia collar is inadequate for this highly unstable injury, and halo immobilization, while affording adequate temporary immobilization, is not appropriate definitive management for this ligamentous injury. The patient does not have an injury at C4-C5 or C6-C7.
REFERENCES: Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries.
J Am Acad Orthop Surg 2002;10:271-280.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 27:
A 9-year-old boy has lateral right knee pain. An MRI scan shows a discoid lateral meniscus with a partial tear in its central portion. Treatment should consist of Review Topic
Options:
- arthroscopic saucerization of the meniscus.
- lateral total menisectomy.
- meniscal transplant.
- arthroscopy and repair of the central tear.
- casting for 6 weeks followed by physical therapy.
Correct Answer: arthroscopic saucerization of the meniscus.
Explanation:
A tear of the mid portion of a stable discoid lateral meniscus should be treated with a partial menisectomy with saucerization. Lateral total menisectomy is contraindicated because of the poor long-term results following this procedure. Meniscal transplant and casting do not have a role in this scenario, although meniscal repairs may be needed for peripheral meniscal instability.
Question 28:
Figures 36a and 36b show the MRI scans of a 15-year-old girl who has had pain and recurrent hemarthrosis in the knee for the past year. Plain radiographs are normal. What is the most likely diagnosis?
Options:
- Hemangioma of the knee
- Hemophilia
- Discoid lateral meniscus
- Torn medial meniscus
- Pauciarticular-type juvenile rheumatoid arthritis (JRA)
Correct Answer: Hemangioma of the knee
Explanation:
DISCUSSION: In pediatric patients who have pain and recurrent hemarthrosis in the knee, hemangioma is often seen as an internal derangement of the knee, and long delays in diagnosis are common. An MRI scan is noninvasive and will best aid in diagnosis. In this patient, the MRI scan shows a hemangioma with no evidence of meniscal injury or discoid meniscus. Hemophilia is unlikely because the patient is female. The presence of hemarthrosis makes JRA an unlikely diagnosis.
REFERENCE: Price NJ, Cundy PJ: Synovial hemangioma of the knee. J Pediatr Orthop 1997;17:74-77.
Question 29:
A year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
Options:
- Patellar clunk syndrome
- Flexion gap instability
- Polyethylene wear
- Femoral component malrotation
Correct Answer: Patellar clunk syndrome
Explanation:
DISCUSSION:
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 30:
A 58-year-old woman sustained a ruptured Achilles tendon 1 year ago, and management consisted of an ankle-foot orthosis. She now reports increasing difficulty with ambulation and increasing pain. An MRI scan shows a 6-cm defect in the right Achilles tendon. Management should now consist of
Options:
- continued use of an ankle-foot orthosis.
- direct repair of the Achilles tendon.
- V-Y repair of the Achilles tendon.
- transfer of the plantaris tendon.
- Achilles tendon turndown with flexor hallucis longus tendon transfer.
Correct Answer: Achilles tendon turndown with flexor hallucis longus tendon transfer.
Explanation:
DISCUSSION: With a gap of less than 4 cm, a V-Y repair would be appropriate without a tendon transfer. For gaps greater than 5 cm, a lengthening with augmentation is the most appropriate treatment. Therefore, the treatment of choice is an Achilles tendon turndown with flexor hallucis longus tendon transfer. The plantaris tendon is not a strong enough repair, and direct repair is not possible given the large defect in the Achilles tendon. Continued use of the ankle-foot orthosis will not provide adequate relief for this patient.
REFERENCE: Myerson MS: Achilles tendon ruptures. Instr Course Lect 1999;48:219-230.
Question 31:
A 22-year-old male cyclist was struck by a car. He complains of right knee pain and swelling, as well as reduced sensation and weakness in his right foot. His leg compartments are soft and not tender. Distal pulses in the extremity are palpable. Radiographs of the knee, as shown in Figures A and B, were taken after a closed reduction maneuver was performed. What would be the next best step in management of this patient?
Options:
- Non-operative managment, but arrange for early follow-up in clinic
- Intra-compartmental pressure measurements
- Ankle-brachial index measurements
- Knee spanning external fixation
- Open reduction internal fixation
Correct Answer: Non-operative managment, but arrange for early follow-up in clinic
Explanation:
This patient presents with a Schatzker IV tibia plateau fracture with lower extremity neurologic deficits. The next best step would be to investigate for an acute vascular injury with ankle-brachial index measurements.
Fracture-dislocations of the knee must be suspected with all Schatzker type IV injuries as this fracture pattern is usually associated with high energy trauma. Identifying this injury should prompt a thorough assessment of the neurovascular structures across the knee. After closed reduction and emergent immobilization of the knee, ankle brachial indices (ABI) must be immediately performed. If <0.9, further vascular testing is warranted, such as MR or CT angiography.
Berkson et al. reviewed high energy tibia fractures. They state that Schatzker Type IV fractures typically requires more energy than corresponding lateral plateau fractures, due to denser bone on the medial side.
Chang et al. described an anatomic sub-classification of Schatzker IV fractures. They describe Group 1* fractures as classic medial unicondylar fractures. Group 2* fractures are complicated variants characterized by medial condyle fractures with lateral plateau extension. Usually these have articular impaction of the centroposterior lateral plateau.
Figures A and B show AP and lateral radiographs of the knee demonstrating a classic medial unicondylar Schatzker IV fracture. Note the anterior subluxation of the tibia in relation to the femur. Illustration A shows the multiple CT images of this fracture pattern.
Incorrect Answers:
Question 32:
New computer scanning technology for socket design has achieved which of the following improvements in amputee care?
Options:
- Improved socket fit
- Reduced skin breakdown from excessive pressure on the residual limb
- Reduced the time of socket fabrication
- Reduced the cost of prosthetic devices
- Decreased pain at the limb socket interface
Correct Answer: Reduced the time of socket fabrication
Explanation:
One of the new technologies available to the prosthetist is the use of digital scanners to obtain a model of the residual limb. Typically, a digital image of the residual limb is obtained by either running a wand over the surface anatomy, allowing the computer program to record the shape, or by using a ring-type scanner that does not make contact with the residual limb but records the shape by bouncing a laser beam off the limb. In either instance, the end result is a digital image that can then be viewed and modified on the computer to improve the weight-bearing aspects of a socket shape or take pressure off sensitive bony areas. The final shape is then carved out of a foam block for use in the socket fabrication process. Computer-aided socket design is still dependent on input from the prosthetist, and therefore does not represent an improvement in overall socket fit. Digital scanning works well on specific types of devices, such as transfemoral sockets, where there is more soft tissue relative to bone. The scanner does not have the ability to detect the density of tissue beneath the scanned surface. Heterotopic ossification and other anomalies will be missed if a thorough examination of the underlying anatomy is neglected. Therefore, the advantages of using scanning technology are for producing and fabricating a socket shape quickly, storing the shape digitally for future use, and increasing efficiency with a plasterless facility.
Question 33:
A 56-year-old man with poorly controlled diabetes mellitus has rapidly developing and advancing erythema, warmth and swelling with bullae formation on the left lower extremity. These findings appear to be advancing proximally several millimeters per hour. Culture results are most likely to reveal
Options:
- group A Streptococcus.
- Methicillin-resistant staphylococcus aureus.
- Clostridium.
- polymicrobial infection.
Correct Answer: polymicrobial infection.
Explanation:
Discussion: Necrotizing fasciitis (NF) results in the death of the body's soft tissue. It is a severe disease of sudden onset that spreads rapidly. Symptoms include red or purple skin in the affected area, with severe pain, fever, and vomiting. The most commonly affected areas are the limbs and perineum. Early diagnosis is difficult as the disease often looks like a simple superficial skin infection in the early stages. While a number of laboratory and imaging modalities can raise the suspicion for necrotizing fasciitis, the gold standard for diagnosis is a surgical exploration in the setting of high suspicion. When in doubt, a small "keyhole" incision can be made into the affected tissue. If a finger easily separates the tissue along the fascial plane,
the diagnosis is confirmed and an extensive debridement should be performed. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score can be utilized to risk stratify people who have signs of cellulitis and determine the likelihood of necrotizing fasciitis being present. It uses six serologic measures, including C-reactive protein, total white blood cell count, hemoglobin, sodium, creatinine and glucose.
Polymicrobial synergistic infection was the most common cause of necrotizing fasciitis (48 patients; 53.9%) with streptococci and enterobacteriaceae being the most common isolates. Group-A streptococcus was the most common cause of monomicrobial necrotizing fasciitis. The most common associated comorbidity was diabetes mellitus (63 patients; 70.8%).
Question 34:
A 72-year-old woman falls onto her left hip after tripping over a curb during her daily 3-mile walk. An injury radiograph is shown in Figure A. What is the best long term solution?
Options:
- Cannulated screws
- Valgus intertrochanteric osteotomy
- Unipolar hemiarthroplasty
- Bipolar hemiarthroplasty
- Total hip arthroplasty
Correct Answer: Unipolar hemiarthroplasty
Explanation:
THA is the best long term solution for displaced femoral neck fractures (FNF) in active elderly patients.
The aims of surgery for FNF in elderly patients are immediate pain relief, rapid mobilization, and low complications and revision. THA has best pain relief, fewer reoperations, best survivorship and is most cost-effective but has longer operative/anesthetic time, blood loss, higher infection rate, and potential instability compared with HA.
Healy and Iorio examined the optimal treatment for elderly FNF. They compared internal fixation (120 patients) with arthroplasty (HA, 43 patients; THA, 23 patients). There was no different in reoperation or mortality rates between the 2 groups, but arthroplasty was more cost effective, had independent living, and longer interval to reoperation/death. THA had less pain, better function, and lower rates of reoperation than HA, and was most cost-effective. They concluded that THA was the best treatment.
Yu et al. performed a meta-analysis of randomized controlled trials to determine whether THA or hemiarthroplasty (HA) was superior. They found that THA had lower risk of reoperation (RR = 0.53), higher risk of dislocation (RR = 1.99), and
higher functional scores at 1 and 4 years. There was no difference in mortality, infection and complication rates.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Question 35:
Which of the following descriptions is true regarding APC-II (anterior-posterior compression) pelvic injuries as classified by Young and Burgess?
Options:
- Pubic symphysis diastasis, intact anterior sacroiliac ligaments, intact sacrotuberous ligament, intact posterior sacroiliac ligaments
- Pubic symphysis diastasis, torn anterior sacroiliac ligaments, intact sacrotuberous ligament intact posterior sacroiliac ligaments
- Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, intact
- posterior sacroiliac ligaments
- Pubic symphysis diastasis, torn anterior sacroiliac ligaments, torn sacrotuberous ligament, intact posterior sacroiliac ligaments
- Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, torn posterior sacroiliac ligaments
Correct Answer: Pubic symphysis diastasis, intact anterior sacroiliac ligaments, intact sacrotuberous ligament, intact posterior sacroiliac ligaments
Explanation:
DISCUSSION: APC II injuries are unstable injuries and occur as a result of high-energy trauma. Anatomic structures which are injured or torn include the pubic symphysis, anterior iliosacral ligaments, and the sacrotuberous ligaments. The posterior sacroiliac ligaments are spared in APC-II injuries, and differentiate an APC-II injury from an APC-III injury, in which the posterior ligaments are also torn.
Burgess et al review the classifications of pelvic ring disruptions and their association with mortality. They concluded that APC injuries required more blood replacement and were related to death more often than lateral compression, vertical shear, or combined mechanism pelvic injuries.
Tile studied the anatomy of anterior to posterior pelvic ring injuries. Although the anterior structures, the symphysis pubis and the pubic rami, contribute to 40% to the stiffness of the pelvis, clinical and biomechanical studies have shown that the posterior sacroiliac complex is more important to pelvic-ring stability. The posterior sacroiliac ligamentous complex is more important to pelvic-ring stability than the anterior structures and therefore, the classification of pelvic fractures is based on the stability of the posterior lesion.
Question 36:
Metal-on-metal lumbar disk arthroplasty devices may generate cobalt and chromium ions into the serum of patients after implantation into the lumbar spine. Which of the following statements best represents the levels of the serum ion levels in these patients? Review Topic
Options:
- The serum ion levels are not measureable in these patients.
- The serum ion levels are measureable, but are of negligible value in these patients.
- The serum ion levels measured equal the values measured in the local tissues in total hip arthroplasty metal-on-metal prostheses.
- The serum ion levels measured are much lower in terms of their level to the values measured in total hip arthroplasty metal-on-metal prostheses.
- The serum ion levels measured are similar in terms of their level to the values measured in total hip arthroplasty metal-on-metal prostheses.
Correct Answer: The serum ion levels measured are similar in terms of their level to the values measured in total hip arthroplasty metal-on-metal prostheses.
Explanation:
According to two studies looking at patients with a cobalt-chrome metal-on-metal lumbar disk arthroplasty, serum ion levels in these patients were similar to values measured in patients with total hip arthroplasty metal-on-metal prostheses.
Question 37:
Which of the following statements regarding conus medullaris syndrome is most accurate?
Options:
- Conus medullaris syndrome most commonly accompanies injuries at the T12-L2 region.
- Conus medullaris injury is a lower motor neuron injury, resulting in an excellent prognosis for recovery of bowel and bladder dysfunction.
- The conus medullaris houses the motor cell bodies for the lumbar roots.
- Lower extremity weakness is a common sign of conus medullaris syndrome.
- Autonomic dysreflexia is common.
Correct Answer: Conus medullaris syndrome most commonly accompanies injuries at the T12-L2 region.
Explanation:
DISCUSSION: Conus medullaris syndrome most frequently occurs as a result of trauma or with a disk herniation at L1, resulting in a lower motor neuron syndrome but with a poor prognosis for recovery of bowel and bladder dysfunction. The conus region, as the termination of the spinal cord, contains the motor cell bodies of the sacral roots. The syndrome is usually a sacral level neural injury; therefore, lower extremity weakness is uncommon.
REFERENCES: Haher TR, Felmly WT, O’Brien M: Thoracic and lumbar fractures: Diagnosis and management, in Bridwell KH, Dewald RL, Hammerberg KW, et al (eds): The Textbook of Spinal Surgery, ed 2. New York, NY, Lippincott Williams & Wilkins, 1977, pp 1773-1778.
Reitman
CA
(ed): Management of Thoracolumbar Fractures. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 35-45.
Question 38:
A 30-year-old woman injured the ring finger of her nondominant hand while playing baseball 5 weeks ago. She now reports pain and limited motion of the proximal interphalangeal (PIP) joint. A lateral fluoroscopy image is shown in Figure 36. Treatment of the PIP joint should consist of
Options:
- closed reduction and percutaneous pinning.
- implant arthroplasty.
- arthrodesis.
- volar plate arthroplasty.
- resection arthroplasty.
Correct Answer: volar plate arthroplasty.
Explanation:
DISCUSSION: The patient has a neglected PIP joint fracture-dislocation with comminution involving more than 40% of the volar articular surface of the middle phalanx. Volar plate arthroplasty has been advocated for the treatment of acute unstable and chronic dorsal fracture-dislocations. The volar plate is incised laterally and released from the collateral ligaments. The volar fragments of the middle phalanx are removed and a trough is created for advancement of the volar plate, which is secured with sutures secured on the dorsum of the middle phalanx beneath the extensor mechanism.
REFERENCES: Dionysian E, Eaton RG: The long-term outcome of volar plate arthroplasty of the proximal interphalangeal joint. J Hand Surg Am 2000;25:429-437.
Eaton RG, Malerich MM: Volar plate arthroplasty of the proximal interphalangeal joint: A review of ten years’ experience. J Hand Surg Am 1980;5:260-268.
Deitch MA, Kiefhaber TR, Comisar BR, et al: Dorsal fracture dislocations of the proximal interphalangeal joint: Surgical complications and long-term results. J Hand Surg Am 1999;24:914-923.
Question 39:
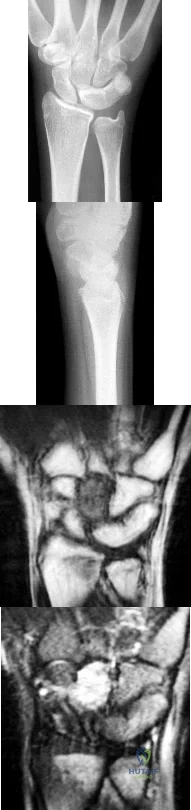
Figures 1 through 4 are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this scenario is
Options:
- capitate excision with interposition arthroplasty.
- capitate proximal pole excision and drilling.
- proximal row carpectomy (PRC).
- vascularized bone graft.
Correct Answer: vascularized bone graft.
Explanation:
EXPLANATION:
This patient has osteonecrosis of the capitate. The MR images show evidence of osteonecrosis with decreased signal on the T1-weighted image. The radiographs are unremarkable, with the exception of lunotriquetral coalition, which does not necessitate treatment. The etiology of osteonecrosis of the capitate may be related to trauma, abnormal Interosseous vascular supply, and hypermobility. Surgery is an option for patients with persistent symptoms despite immobilization. Vascularized bone graft should be considered in this scenario because there is no evidence of capitate collapse or arthritic change about the wrist. Free and local vascularized bone grafts have produced satisfactory results. Capitate excision with interposition arthroplasty is indicated for patients with proximal pole capitate collapse. Total wrist fusion is a salvage procedure and would be considered if there were evidence of collapse and arthritic change.
PRC would leave the capitate articulating with the radius and is not indicated.
Question 40:
Figure 7 shows the CT scan of a 25-year-old soccer player who has had posterior ankle pain with plantar flexion for the past 2 years. Immobilization has failed to provide relief. He is ambulatory. Management should consist of
Options:
- a local steroid injection into the flexor hallucis longus tendon sheath.
- range-of-motion exercises.
- open reduction and internal fixation.
- nonsteroidal anti-inflammatory drugs.
- excision of the fragment.
Correct Answer: excision of the fragment.
Explanation:
DISCUSSION: An os trigonum is usually asymptomatic, but this accessory bone has been associated with persistent posterior ankle pain, which has been described as os trigonum syndrome. This usually affects athletes and ballerinas. Forced plantar flexion leads to impingement of the os trigonum against the posterior tibial plafond, and flexor hallucis tendinitis may develop. It may be difficult to differentiate a fractured trigonal process from the os trigonum. MRI may reveal bone marrow edema that may aid in the diagnosis of os trigonum syndrome. Steroid injections may lead to tendon rupture. The results of excision of a symptomatic os trigonum through a posteromedial or lateral approach are favorable, with a rapid return to full function. The main complication of this procedure is sural nerve injury with a lateral approach.
REFERENCES: Hedrick MR, McBryde AM: Posterior ankle impingement. Foot Ankle Int 1994;15:2-8.
Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Question 41:
During the revision surgical procedure, thoracic pedicle screws are placed. Following placement, triggered electromyography (EMG) is performed by stimulating the pedicle screw heads. During testing the right T2 pedicle screw head returns a threshold of 2 mA. What does this reading indicate?
Options:
- The right T2 pedicle screw is well seated within the pedicle.
- The right T2 pedicle screw has breached the pedicle wall and has violated the costovertebral junction.
- There is a breach in the right T2 pedicle wall, but the screw is not in contact with a neural structure.
- There is a breach in the right T2 pedicle and the screw is in contact with a neural structure.
Correct Answer: There is a breach in the right T2 pedicle and the screw is in contact with a neural structure.
Explanation:
DISCUSSION
This patient has developed a proximal junctional kyphosis following a long posterior fusion performed for treatment of degenerative lumbar scoliosis. Risk factors for proximal junctional kyphosis in the setting of instrumented fusions performed for degenerative scoliosis include advanced age, 360-
degree fusions, extension of fusion constructs to the sacrum, and upper instrumented vertebrae at the level of T1-3. The patient's junctional kyphosis is attributable to failure of the disk and ligamentous structures at T2-3 and would be graded as type I using the classification system of Yagi and associates. Most symptomatic proximal junctional kyphoses are treated with posterior extension of the fusion construct to a more proximal level spanning the kyphosed region. The use of orthoses or simple removal of instrumentation is unlikely to substantively impact symptoms or address the proximal kyphosis. Diabetes and obesity are known factors that increase risk for postsurgical infection following a spine fusion procedure. The most frequent complication following revision surgery for proximal junctional kyphosis, however, is the need for further surgery. In the study by Yagi and associates, 48% of patients who underwent revision surgery for proximal kyphosis developed further adjacent segment degeneration. In the proximal thoracic spine, where the pedicle may be narrow, triggered EMG testing of inserted pedicle screws may be used to assess for violation of the pedicle wall during insertion. In the setting of triggered EMG, thresholds exceeding 10 mA indicate a well-placed pedicle screw. Thresholds lower than 4 mA to 6 mA indicate that a screw is directly contacting a neural structure. Thresholds between 9 mA and 10 mA suggest that a breach of the pedicle may be present, but the screw is not contacting a neural structure.
RECOMMENDED READINGS
Yagi M, Rahm M, Gaines R, Maziad A, Ross T, Kim HJ, Kebaish K, Boachie-Adjei O; Complex Spine Study Group. Characterization and surgical outcomes of proximal junctional failure in surgically treated patients with adult spinal deformity.Spine (Phila Pa 1976). 2014 May 1;39(10):E607-14. doi: 10.1097/BRS.0000000000000266. PubMed PMID: 24525992.
View
Abstract at PubMed
Cammarata M, Aubin CÉ, Wang X, Mac-Thiong JM. Biomechanical risk factors for proximal junctional kyphosis: a detailed numerical analysis of surgical instrumentation variables. Spine (Phila Pa 1976). 2014 Apr 15;39(8):E500-7. doi: 10.1097/BRS.0000000000000222. PubMed
PMID: 24480964.
View Abstract at PubMed
Kim HJ, Lenke LG, Shaffrey CI, Van Alstyne EM, Skelly AC. Proximal junctional kyphosis as a distinct form of adjacent segment pathology after spinal deformity surgery: a systematic review. Spine (Phila Pa 1976). 2012 Oct 15;37(22 Suppl):S144-64. doi: 10.1097/BRS.0b013e31826d611b. PubMed PMID: 22885829.
View Abstract at PubMed
Schoenfeld AJ, Carey PA, Cleveland AW 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: a prognostic study based on 5,887 patients. Spine J. 2013 Oct;13(10):1171-9. doi: 10.1016/j.spinee.2013.02.071. Epub 2013 Apr 9. PubMed PMID:
Question 42:
Which of the following zones of articular cartilage has the highest concentration of proteoglycans?
Options:
- Superficial
- Transitional
- Deep
- Calcified
- Tidemark
Correct Answer: Deep
Explanation:
The fundamental structure of normal adult articular cartilage is divided into four different zones: superficial, transitional, deep, and calcified. These layers vary in chondrocyte morphology, size and orientation of collagen bundles, and water and proteoglycan content. The deep zone has the highest concentration of proteoglycans and the lowest concentration of water. The tidemark is a boundary between the calcified and uncalcified layers of articular cartilage.
Question 43:
A patient underwent an anterior cervical diskectomy and interbody fusion for a C5-6 herniated nucleus pulposus and left C6 radiculopathy 8 months ago. He now reports new onset of severe neck pain and left C6 radicular pain, with wrist extension weakness. The radiograph and CT scan shown in Figures 26a and 26b reveal pseudarthrosis at C5-6. The next step in management should consist of
Options:
- application of a neck brace for 6 to 12 weeks.
- revision anterior diskectomy and interbody fusion with autograft at C5-6.
- revision anterior diskectomy with interbody autograft and anterior plate fixation at C5-6.
- posterior fusion at C5-6.
- posterior foraminotomy at left C6 and posterior fusion at C5-6 with stabilization and autograft.
Correct Answer: posterior foraminotomy at left C6 and posterior fusion at C5-6 with stabilization and autograft.
Explanation:
DISCUSSION: Brodsky and associates reviewed 34 cases of cervical pseudarthrosis after anterior fusion. Seventeen were treated with revision anterior fusion and 17 with posterior foraminotomy and fusion. Good results were seen in 75% of patients who underwent revision anterior surgery, but better results (94%) were seen with posterior surgery, including foraminotomy and stabilization. Tribus and associates reported treatment of 16 patients with pseudarthrosis using revision anterior debridement of the fibrous tissue and fusion with autograft and plates. There was improvement of the neck in 75% of the patients, nonunion in 19%, continued weakness in 28%, and dysphagia in 5%. Farey and associates reported on 19 patients treated with posterior foraminotomy, stabilization, and fusion with a fusion rate of 100%, resolution of arm pain in 94%, resolution of weakness in 100%, and resolution of neck pain in 75%. It would appear that posterior foraminotomy is more effective for relieving arm pain and neurologic deficits associated with pseudarthrosis. Posterior fusion has the most reliable rate of arthrodesis in this setting. Dysphagia is reported in some patients undergoing more extensive anterior dissections required for applying plates. A neck brace is unlikely to aid in healing of pseudarthrosis in a patient who underwent surgery 8 months ago. A neck brace would be most effective within the first 3 months if a delayed union is identified.
REFERENCES: Brodsky AE, Khalil MA, Sassard WR, Neuman BP: Repair of symptomatic pseudarthrosis of anterior cervical fusion: Posterior versus anterior repair. Spine
1992;17:1137-1143.
Tribus CB, Corteen DP, Zdeblick TA: The efficacy of anterior cervical plating in the management of symptomatic pseudarthrosis of the cervical spine. Spine 1999;24:860-864.
Farey ID, McAfee PC, Davis RF, Long DM: Pseudarthrosis of the cervical spine after anterior arthrodesis: Treatment by posterior nerve root decompression, stabilization, and arthrodesis.
J Bone Joint Surgery Am 1990;72:1171-1177.
Question 44:
What is the most common MRI appearance of a malignant soft-tissue sarcoma?
Options:
- Well defined, homogeneous, and deep to fascia
- Well defined, heterogeneous, and deep to fascia
- Ill defined, homogeneous, and deep to fascia
- Ill defined, heterogeneous, and superficial to fascia
- Ill defined, homogeneous, and superficial to fascia
Correct Answer: Well defined, heterogeneous, and deep to fascia
Explanation:
DISCUSSION: The classic MRI appearance of a soft-tissue sarcoma is a well-defined heterogeneous mass deep to the fascia. MRI has greatly enhanced our ability to identify and characterize soft-tissue masses. In many patients, MRI is diagnostic and may obviate the need for biopsy. In other patients, it may indicate with high probability that the mass is malignant and consideration for referral can be made. A common misconception is that sarcomas are infiltrative; therefore, physicians mistakenly exclude the diagnosis of a sarcoma based on a well-defined mass seen on MRI. However, sarcomas grow centrifugally with balloon-like expansion compressing surrounding normal tissue; as such, they appear well defined. Many benign soft-tissue masses such as lipomas are similarly well defined. However, MRI is especially useful in identifying fat. Lipomas appear to be homogeneous masses with fat signal characteristics on all sequences. Ill-defined soft-tissue masses include infection, trauma, and desmoid tumors. Heterogeneity is not unique to malignant tumors but is a characteristic of soft-tissue sarcomas.
REFERENCES: Bancroft LW, Peterson JJ, Kransdorf MJ, Nomikos GC, Murphey MD: Soft tissue tumors of the lower extremities. Radiol Clin North Am 2002;40:991-1011.
Berquist TH, Ehman RL, King BF, et al: Value of MR imaging in differentiating benign from malignant soft-tissue masses: Study of 95 lesions. Am J Roentgenol 1990;155:1251-1255.
Crim JR, Seegar LL, Yao L, et al: Diagnosis of soft tissue masses with MR imaging: Can benign masses be differentiated from malignant ones? Radiology 1992;185:581-586.
Question 45:
-What is the most likely deficit in elbow function resulting from an isolated lesion of the ulnar nerve above the elbow?
Options:
- No elbow deficit
- Weakness of elbow flexion
- Weakness of elbow extension
- Weakness of forearm pronation
- Weakness of forearm supination
Correct Answer: No elbow deficit
Question 46:
Figure 46 shows the MRI scan of a patient who has a mass in the calf that has been fluctuating in size. Radiographs are negative. Which of the following procedures will most quickly aid in confirming the diagnosis?
Options:
- Open biopsy
- Needle aspiration
- Arthroscopy
- CT
- Arthrography
Correct Answer: Needle aspiration
Explanation:
DISCUSSION: The bright signal on the T2-weighted MRI scan suggests fluid. The multiloculated appearance in proximity to the proximal tibiofibular joint suggests that the most likely diagnosis is a ganglion. They typically increase and decrease in size and can be diagnosed by the classic gelatinous fluid obtained through needle aspiration.
REFERENCES: Bianchi S, Abdelwahab IF, Kenan S, Zwass A, Ricci G, Palomba G: Intramuscular ganglia arising from the superior tibiofibular joint: CT and MR evaluation. Skeletal Radiol 1995;24:253-256.
Feldman F, Singson RD, Staron RB: Magnetic resonance imaging of para-articular and ectopic ganglia. Skeletal Radiol 1989;18:353-358.
Question 47:
A 39-year-old man reports low back pain, lower extremity numbness, and urinary retention after being injured in a motor vehicle accident 1 day ago. He is able to walk but is in pain. A straight leg raise results in increased back pain, and examination reveals that perianal sensation is decreased. Placement of a urinary catheter results in 500 mL of urine. What is the next most appropriate step in management?
Options:
- Emergent MRI
- Urology consultation
- Pain control with narcotics
- Pain control with a lumbar epidural steroid injection
- Physical therapy
Correct Answer: Emergent MRI
Explanation:
DISCUSSION: Acute cauda equina syndrome, including saddle hypesthesia and bowel/bladder incontinence, is a red flag that demands emergent evaluation with MRI and urgent surgery if compression is confirmed. Results appear to be improved if surgery is performed within 48 hours. The other treatment approaches listed are not indicated if a cauda equina syndrome
is present.
REFERENCES: Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Shapiro S: Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine 2000;25:348-351.
Kostuik JP, Harrington I, Alexander D, et al: Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am 1986;68:386-391.
Question 48:
Standard guidelines necessitate the use of intraoperative neurophysiological monitoring for patients undergoing surgery for which condition?
Options:
- Primary lumbar disk herniation
- Adolescent idiopathic scoliosis
- Cervical spondylotic myelopathy
- No conditions; there are no official guidelines
Correct Answer: No conditions; there are no official guidelines
Explanation:
DISCUSSION
There are currently no official guidelines on the appropriate use of neuromonitoring in spine surgery. In general, use of neuromonitoring is at surgeon discretion and often is based on the surgeon's perceived risk for neurologic injury during surgery and medicolegal concerns. In most reports,
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090.
View Abstract at PubMed
Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377.
View
Abstract at PubMed
Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334.
View
Abstract at PubMed
Question 49:
Emergent management of acute tooth displacement (luxation) includes
Options:
- delaying replantation until a dentist is present.
- scrubbing the root of the tooth clean with hydrogen peroxide.
- transporting the tooth in a carbonated beverage.
- emergency root canal. §. immediate repositioning or replantation of the tooth.
Correct Answer: delaying replantation until a dentist is present.
Explanation:
DISCUSSION: Avulsed teeth must be replanted immediately to enhance viability of the periodontal ligament cells on the root. With the tooth in place, the athlete should bite down on a towel to maintain stability. The athlete should be taken emergently to a dentist’s office or emergency room. The avulsed tooth should not be handled by the root or scrubbed to remove debris. If immediate replantation is not possible, the tooth should be transported in saline solution, milk, or saliva on gauze.
REFERENCES: Flores MT, Andreasen JO, Bakland LK, et al: Guidelines for the evaluation and management of traumatic dental injuries. Dent Traumatol 2001; 17:97-102.
Ranalli DN, Demas PN: Orofacial injuries from sport preventive measures for sports medicine. Sports Med
2002;2:409-418.
Question 50:
A 72-year-old man was involved in an automobile accident 4 weeks ago. Initially he noted pain about his nondominant left shoulder, which resolved within a few weeks after the accident. He now describes trouble with gripping and carrying items in his left hand. Radiographs are shown in Figures 20a through 20c. His signs and symptoms are the result of injury to which of the following ligaments?
Options:
- Volar scapholunate interosseous
- Dorsal scapholunate interosseous
- Long radiolunate
- Short radiolunate
- Dorsal intercarpal
Correct Answer: Dorsal scapholunate interosseous
Explanation:
DISCUSSION: The radiographs reveal a gap between the scaphoid and lunate bones, indicative of disruption of the scapholunate ligament complex. The three components of the complex are the dorsal scapholunate ligament, the volar (or palmar) scapholunate ligament, and the proximal fibrocartilaginous membrane, listed in decreasing yield strength. Disruption of the stout dorsal interosseous ligament is required for scapholunate dissociation to occur.
REFERENCES: Berger RA: The ligaments of the wrist: A current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63-82.
Cohen MS, Taleisnik J: Direct ligamentous repair of scapholunate dissociation with capsulodesis augmentation. Tech Hand Up Extrem Surg 1998;2:18-24.
Question 51:
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Options:
- Pasteurella
- Streptococcus
- Staphylococcus
- Bacteroides
- Moraxella
Correct Answer: Pasteurella
Explanation:
DISCUSSION: To define bacteria responsible for dog and cat bite infections, a prospective study yielded a median of five bacterial isolates per culture. Pasteurella is most common from both dog bites (50%) and cat bites (75%). Pasteurella canis was the most frequent pathogen of dog bites, and Pasteurella multocida was the most common isolate of cat bites. Other common aerobes included streptococci, staphylococci, moraxella, and neisseria.
REFERENCE: Talan DA, Citron DM, Abrahamian FM, et al: Bacteriologic analysis of infected dog and cat bites. Emergency Medicine Animal Bite Infection Study Group. N Engl J Med 1999;340:85-92.
Question 52:
Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
Options:
- Both CT and MRI have equivalent cost for the patient.
- Both CT and MRI have equivalent safety for the patient.
- Associated soft-tissue damage can be more reliably shown on CT scans.
- Two-dimensional CT scans represent better definition of bone loss than two-dimensional MRI scans. Two-dimensional CT scan is generally accepted as a superior imaging modality for evaluating bone loss in shoulder instability than two-dimensional MRI scan. This advantage is offset by the relatively high radiation dose. Although CT in most situations is less costly, MRI can provide more data regarding associated soft-tissue damage that can be associated with recurrent instability. It should be noted that three-dimensional MRI has recently been shown as equivalent to three-dimensional CT in its ability to identify glenoid bone loss.
Correct Answer: Two-dimensional CT scans represent better definition of bone loss than two-dimensional MRI scans. Two-dimensional CT scan is generally accepted as a superior imaging modality for evaluating bone loss in shoulder instability than two-dimensional MRI scan. This advantage is offset by the relatively high radiation dose. Although CT in most situations is less costly, MRI can provide more data regarding associated soft-tissue damage that can be associated with recurrent instability. It should be noted that three-dimensional MRI has recently been shown as equivalent to three-dimensional CT in its ability to identify glenoid bone loss.
Explanation:
A 43-year-old woman is involved in a motor vehicle collision. She sustains the isolated injury shown in the radiograph in Figure 1. Her neurovascular examination is compromised. What is the most likely deficit?
A. Inability to flex the distal interphalangeal joint of the index finger
B. Positive Froment’s sign
C. Weakness with wrist extension
D. Decreased capillary refill
Question 53:
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Options:
- Need for ankle fusion or arthroplasty
- Return to normal function
- Ankle stiffness without pain
- Severe constant pain and inability to work
- Adversely affected general health status and posttraumatic arthritis
Correct Answer: Adversely affected general health status and posttraumatic arthritis
Explanation:
DISCUSSION: Two recent studies by Pollak and associates and Marsh and associates have focused on function after high-energy tibial plafond fractures. Findings are unfavorable even when anatomic reduction is performed in the best centers and patients are provided excellent rehabilitation. Function improves up to 2 years after injury, but even basic walking skills remain adversely affected. Virtually all patients have long-term adverse general health effects compared to their gender and age-matched peers. Posttraumatic degenerative arthritis is present in most ankles. Patients should be told early about the long-term prognosis, and early vocational/psychological counseling should be given. Despite these adverse outcomes, only a minority of patients require fusion or arthroplasty.
REFERENCES: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: How do these ankles function over time? J Bone Joint Surg Am 2003;85:287-295.
Question 54:
A 20-year-old collegiate baseball pitcher has persistent deep shoulder pain. Examination reveals normal strength, 130 degrees of external rotation in abduction, 10 degrees of internal rotation in abduction, mild dynamic scapular winging, and equivocal findings on provocative tests for labral tears. Management should consist of
Options:
- shoulder arthroscopy and repair of a possible labral tear.
- anterior capsulorrhaphy for subtle anterior instability.
- diagnostic arthroscopy of the glenohumeral joint and arthroscopic subacromial decompression.
- rest from pitching, initiation of a rehabilitation program to restore internal rotation, and scapular stabilization.
- rest from pitching and a corticosteroid injection into the subacromial space.
Correct Answer: rest from pitching, initiation of a rehabilitation program to restore internal rotation, and scapular stabilization.
Explanation:
DISCUSSION: Although management of shoulder pain in the throwing athlete is controversial, there are some general principles. Initial management generally includes rest from throwing, restoring normal joint function, specifically motion and strength as well as eliminating pain. In this patient, examination reveals excessive external rotation and decreased internal rotation. This pattern is common in pitchers; however, the total arc of motion should remain close to 180 degrees in abduction. In this patient, the total arc is 140 degrees. Treatment should first focus on restoring a 180-degree arc with posterior scapular stretching, as well as pain control and muscle rehabilitation. Injections and surgery are generally reserved for patients who fail to respond to rest and rehabilitation.
REFERENCE: Burkhart SS, Morgan CD, Kibler WB: Shoulder injuries in overhead athletes: The “dead arm” revisited. Clin Sports Med 2000;19:125-158.
Question 55:
A 43-year-old woman has had pain in the left hip for the past 2 months. A radiograph, CT scan, MRI scan, and biopsy specimens are shown in Figures 16a through 16e. What is the most likely diagnosis?
Options:
- Osteosarcoma
- Osteochondroma
- Chondrosarcoma
- Chordoma
- Enchondroma
Correct Answer: Chondrosarcoma
Explanation:
DISCUSSION: The imaging studies are consistent with a chondrosarcoma. The radiograph shows a radiolucent lesion in the pelvis, and there are stippled calcifications on the CT scan. The histology shows a low-grade cellular hyaline cartilage neoplasm with stellate, occasionally binucleated chondrocytes. Enchondroma has a more benign histologic appearance.
REFERENCE: Mirra JM, Gold R, Downs J, Eckardt JJ: A new histologic approach to the differentiation of enchondroma and chondrosarcoma of the bones: A clinicopathologic analysis of 51 cases. Clin Orthop 1985;201:214-237.
Question 56:
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?
Options:
- Neurofibromatosis
- Multiple sclerosis
- Cervical spondylotic myelopathy
- Acute poliomyelitis
- Gaucher’s disease
Correct Answer: Neurofibromatosis
Explanation:
DISCUSSION: Muliple neurofibromas result in marked foraminal enlargement as seen on the sagittal MRI scan. Collagen disorders leading to dural ectasia may show similar enlargement, but none of these is listed as a possible answer.
REFERENCES: Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Funasaki H, Winter RB, Lonstein JB, et al: Pathophysiology of spinal deformities in neurofibromatosis: An analysis of seventy-one patients who had curves associated with dystrophic changes. J Bone Joint Surg Am 1994;76:692-700.
Question 57:
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
Options:
- Brachiocephalic
- Innominate
- Subclavian
- Axillary
- Circumflex scapular
Correct Answer: Axillary
Explanation:
DISCUSSION: The axillary artery commences at the first rib as a direct continuation of the subclavian artery and becomes the brachial artery at the lower border of the teres major. The arteriogram reveals a nonfilling defect in the third portion of the artery just distal to the subscapular artery. The complex arterial collateral circulation in this region often permits distal perfusion of the extremity despite injury.
REFERENCE: Radke HM: Arterial circulation of the upper extremity, in Strandness DE Jr (ed): Collateral Circulation in Clinical Surgery. Philadelphia, PA, WB Saunders, 1969, pp 294-307.
Question 58:
What type of nerve palsy is most common following elbow arthroscopy?
Options:
- Transient posterior interosseous
- Transient ulnar
- Transient radial
- Transient median
- Transient medial antebrachial cutaneous
Correct Answer: Transient ulnar
Explanation:
DISCUSSION: Transient ulnar nerve palsy is the most common palsy following elbow arthroscopy. The ulnar nerve is most frequently affected, followed by the radial nerve. Injury to the other nerves has been reported but less frequently.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of elbow arthroscopy.
J Bone Joint Surg Am 2001;83:25-34.
Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 59:
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?
Options:
- No weight bearing
- Cortisone injection
- Physical therapy
- Arthroscopic meniscectomy or repair
- Anterior cruciate ligament reconstruction
Correct Answer: Arthroscopic meniscectomy or repair
Explanation:
DISCUSSION: The patient has a locked knee that cannot be fully extended. This is most likely the result of the mechanical block of a bucket-handle tear that has flipped into the notch. Also, the pain may be so severe that the muscle spasm prevents the knee from straightening out. When the patient is anesthetized, the muscle spasm relaxes and the meniscus can be reduced out of the notch. Arthroscopy is the treatment of choice. A meniscal repair is usually possible in large bucket-handle tears because the meniscus is torn in the red-red zone where most of the vascular supply is located. If the handle portion is badly frayed or damaged, a partial meniscectomy should be performed. The classic finding on MRI is a “double PCL sign.” This is due to the flipped portion of the meniscus in the notch.
REFERENCES: Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Bansal P, Deehan DJ, Gregory RJ: Diagnosing the acutely locked knee. Injury 2002;33:495-498.
Question 60:
Figure 6a through 6c
Options:
- Curettage and/or grafting
- Radiofrequency ablation
- Intravenous (IV) antibiotics
- Incision, drainage, and IV antibiotics
- Neoadjuvant chemotherapy followed by surgical reconstruction
- Observation alone
Correct Answer: Incision, drainage, and IV antibiotics
Explanation:
DISCUSSION
Figure 2 depicts a typical unicameral bone cyst with a pathologic fracture. The decision to treat this lesion should be based on the amount of cortical thinning. If these lesions involve a pathologic fracture, many surgeons will treat them nonsurgically to see if the fracture stimulates healing of the cyst. If the cyst wall remains thin or the patient is symptomatic, then treatment is directed at decreasing cyst volume, increasing cortical thickness, and eliminating symptoms. This can be accomplished by curettage and grafting, injection with autogenous bone marrow, or grafting with 1 of the many available bone void fillers. In some cases, internal fixation may be required. This typically is accomplished with flexible intramedullary nails.
Figure 3 shows a typical nonossifying fibroma. These benign lesions are usually incidental findings on a radiograph and often resolve in adulthood. Treatment usually is not required, and these lesions typically do not produce symptoms.
Figure 4 shows an osteoid osteoma of the femoral neck. This is characterized by a central radiolucent nidus surrounded by reactive bone with increased radiodensity. These lesions are painful because of the large amount of prostaglandin they secrete. They temporarily respond to oral anti-inflammatory drugs. Treatment is directed at eliminating the nidus and can be done through curettage, but radiofrequency ablation, which allows for a minimally invasive approach, is often used today.
Figure 5 shows diskitis with vertebral osteomyelitis. The disease is characterized by fever and back pain. Movement is extremely uncomfortable for these children, and they may adopt unusual postures to alleviate pain. The MRI shows involvement of 1 vertebrae and an adjacent disk. Left untreated, this condition often spreads to involve multiple vertebrae and also can cause an epidural abscess. Treatment during the early stages is IV antibiotics. Many orthopaedic surgeons also use bracing to prevent late vertebral collapse.
Figures 6a through 6c show septic arthritis of the ankle with metaphyseal osteomyelitis. The recommended treatment is incision and drainage followed by IV antibiotics. MRI may be considered before surgery to assess for an associated osteomyelitis or abscess that may also necessitate surgical debridement. Increasingly, these scenarios are managed with a rapid transition to oral antibiotics.
Question 61:
A 65-year-old man has had “catching” in front of his knee since he had a total knee arthroplasty 9 months ago. Examination reveals a palpable and audible snap in the anterior aspect of the knee at about 40 degrees of flexion as the knee is being actively extended. A radiograph of the prosthetic knee will most likely show
Options:
- Patella alta
- A metal-backed patella
- Varus malalignment of the knee
- A posterior cruciate-substituting femoral component
- Lateral subluxation of the patella on a Merchant’s view
Correct Answer: A posterior cruciate-substituting femoral component
Explanation:
The patellar “clunk” syndrome is an infrequent complication of TKA. It is diagnosed clinically by a clunking or clicking sensation or sound as the flexed knee is extended usually at about 30-40 degrees of flexion.
Pathologically, the clunk is produced by a suprapatellar fibrous nodule seen superior to the patellar component at re-operation. This nodule has been seen to catch in the intercondylar notch in primarily first generation TKAs. Current component designs have decreased this phenomenon through better engineering of femoral components. Treatment is by arthroscopic debridement or open arthroplasty resection. The nodule may be recurrent.
Question 62:
A 78-year-old man being seen for routine follow-up studies reports mild to moderate pain in his left arm. The patient has a history of lung cancer and severe heart disease. A radiograph and a bone scan are shown in Figures 36a and 36b. Treatment should consist of
Options:
- intramedullary fixation.
- arterial embolization.
- curettage and cementation.
- radiation therapy.
- segmental resection and reconstruction using a diaphyseal metal spacer.
Correct Answer: radiation therapy.
Explanation:
DISCUSSION: The patient has lung cancer metastatic to the left humerus that is mildly to moderately symptomatic. Radiographically, the lesion is small and is not associated with significant cortical destruction. Metastatic lesions in the upper extremity have a lower incidence of pathologic fracture than lesions in the lower extremity.
REFERENCE: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 63:
A 17-year-old javelin thrower reports medial-sided elbow pain and diminished grip strength while throwing. He has decreased sensation in the little and ring fingers of his throwing hand only while throwing. The sensory deficits resolve at rest. Examination of the elbow reveals no instability and full motion. He has a positive Tinel’s sign over the cubital tunnel and a positive elbow flexion test. Radiographs are normal. What is the next most appropriate step in management?
Options:
- Anterior ulnar nerve transposition
- Cortisone injection
- Nighttime elbow extension splinting
- Medial collateral ligament reconstruction
- Ulnar nerve decompression in situ
Correct Answer: Nighttime elbow extension splinting
Explanation:
DISCUSSION: The patient’s symptoms and examination findings are consistent with ulnar neuritis/cubital tunnel syndrome, most probably exacerbated by javelin throwing. The first step includes rest and extension splinting. Surgical intervention should only be considered after failure of nonsurgical management.
REFERENCES: Posner MA: Compressive neuropathies of the ulnar nerve at the elbow and wrist. Instr Course Lect 2000;49:305-317.
Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 65-69.
Question 64:
271 Which of the following factors has been shown to contribute to poor results after anatomic reduction of posterior wall acetabulum fractures?
Options:
- Marginal articular impaction
- Involvement of the weight-bearing dome
- Delay in reduction of hip dislocation of greater than 12 hours
- Size of wall fragment
- Patient age of less than 40 years
- back answer Question 03.271
Correct Answer: Delay in reduction of hip dislocation of greater than 12 hours
Explanation:
Only 30% of posterior-wall acetabular fractures involve a single large fragment. The majority are multifragmentary or have areas of impaction. Unsatisfactory clinical results occur in more than 80% of patients treated nonsurgically. Operative management usually offers the best chance of preserving long-term joint function, but only if an anatomically reconstructed acetabulum can be achieved without complication. The keys to surgical success include maintaining the viability of the fracture fragments and the femoral head itself, using bone grafts and buttress plating to support elevated and comminuted fragments, and protecting the neurovascular structures at risk.
Complications can include sciatic nerve injury (incidence, 3% to 18%), heterotopic ossification (7% to 20%), and osteonecrosis of the femoral head (5% to 8%). Despite the relative simplicity of this acetabular fracture, unsatisfactory outcomes after surgical repair of the posterior wall occur in at least 18% to 32% of cases, results that are worse than for most of the other more complex acetabular fracture patterns.
Moed BR, et al. Results of operative treatment of fractures of the posterior wall of the acetabulum. JBJS AM 2002:84:752-758
Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. JBJS Am 1996;78:1632-1645
back to this question next question
Question 65:
Which sterilization method is expected to produce the most degradation of an allograft used for anterior cruciate ligament reconstruction?
Options:
- Deep freezing
- Supercritical CO2 treatment
- Gamma irradiation with 1.2 Mrad
- Chlorhexidine gluconate 4% cleansing
Correct Answer: Supercritical CO2 treatment
Explanation:
DISCUSSION
A biomechanical study compared unprocessed, irradiated (2.0 Mrad-2.8 Mrad), and supercritical CO2-treated soft-tissue allografts and demonstrated a 27% to 36% decrease in stiffness of the supercritical CO2-treated grafts. No significant difference was found between the irradiated and untreated soft-tissue allografts. Low-dose (1.0 Mrad-1.2 Mrad) gamma irradiation of bone-patellar-tendon-allograft has been shown to produce a 20% decrease in graft stiffness. Deep freezing or cleansing with 4% chlorhexidine gluconate does not appear to adversely affect the biomechanical properties of the allograft tissue.
CLINICAL SITUATION FOR QUESTIONS 43 THROUGH 46
Figures 43a and 43b are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable.
Question 66:
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
Options:
- Coracohumeral
- Superior glenohumeral
- Middle glenohumeral
- Anterior band of the inferior glenohumeral ligament complex
- Posterior band of the inferior glenohumeral ligament complex
Correct Answer: Anterior band of the inferior glenohumeral ligament complex
Explanation:
DISCUSSION: With the arm in the abducted, externally rotated position, the anterior band of the inferior glenohumeral ligament complex moves anteriorly, preventing anterior humeral head translation. Both the coracohumeral ligament and the superior glenohumeral ligament restrain the humeral head to inferior translation of the adducted arm, and to external rotation in the adducted position. The middle glenohumeral ligament is a primary stabilizer to anterior translation with the arm abducted to 45 degrees. The posterior band of the inferior glenohumeral ligament complex resists posterior translation of the humeral head when the arm is internally rotated.
REFERENCES: Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.
Question 67:
An 18-year-old football player has intense pain and is unable to bear weight on the right knee after being tackled from the front. A posterior knee dislocation is reduced on the field. Because the game took place in a remote location, the patient is not examined in the emergency department until 5 hours after the injury. Examination now shows a grossly swollen knee with moderate ischemia in the lower leg. Posterior tibial and dorsalis pedis pulses are diminished. The best course of action should be to
Options:
- obtain an emergent arteriogram.
- obtain an emergent MRI scan.
- perform a thorough examination of the knee ligaments.
- perform surgical repair or bypass of the injured popliteal vessels.
- perform surgical repair or bypass of the injured popliteal vessels and ligament reconstruction.
Correct Answer: perform surgical repair or bypass of the injured popliteal vessels.
Explanation:
DISCUSSION: Vascular injuries occur in approximately 20% to 35% of knee dislocations, of which one third are posterior. Recognition of the vascular injury is essential. Normal pulses or normal capillary refill do not preclude an arterial injury, and arteriography should be considered in all knee dislocations. If the leg is ischemic, the arteriogram should be circumvented and the patient taken directly to the operating room. The risk of muscle fibrosis, contracture, or vascular insufficiency, and the need for amputation increase significantly when ischemia exceeds 6 hours. This patient has ischemia and is considered a vascular emergency. As such, delays for a thorough examination of the ligament, MRI scans, and even an arteriogram are unwarranted. Concurrent ligamentous repair and reconstruction should be deferred until vascular stability has been achieved.
REFERENCES: Kremchek TE, Welling RE, Kremchek EJ: Traumatic dislocation of the knee. Orthop Rev 1989;18:1051-1057.
Reckling FW, Peltier LF: Acute knee dislocations and their complications. J Trauma 1969;9:181-191.
Question 68:
A patient with a cobalt-chromium alloy (Co-Cr) femoral stem has a periprosthetic fracture that is to be fixed with a cable-plate device. The surgeon should make sure that the plate, screws, and cable, respectively, are made of
Options:
- Co-Cr, stainless steel, stainless steel.
- stainless steel, stainless steel, Co-Cr.
- stainless steel, Co-Cr, Co-Cr.
- titanium alloy, titanium alloy, titanium alloy.
- titanium alloy, stainless steel, Co-Cr.
Correct Answer: titanium alloy, titanium alloy, titanium alloy.
Explanation:
DISCUSSION: Contact between metals in a biologic environment leads to galvanic corrosion. Reduction potentials of Co-Cr and stainless steel produce the worst combination of metals in commonly used implants. Because the fixation implants are not intended to contact the existing implant, it is not as great a consideration as the plate and the screws and cables that will directly contact each other.
REFERENCES: Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 119-144.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 69:
What is the recommended treatment of a skeletally immature 12-year-old boy who has an anterior cruciate ligament-deficient knee?
Options:
- Reduced activity, rehabilitation exercises, and functional bracing until the patient is near skeletal maturity
- Bone-patellar tendon-bone autograft reconstruction
- Allograft reconstruction
- Hamstring tendon intra-articular repair using a centrally placed tibial tunnel and an over-the-top femoral attachment
- Extra-articular repair
Correct Answer: Reduced activity, rehabilitation exercises, and functional bracing until the patient is near skeletal maturity
Explanation:
DISCUSSION: Traditional surgeries for anterior cruciate ligament-deficient knees carry the potential risk of premature physeal closure in young athletes. Therefore, most surgeons are reluctant to recommend intra-articular reconstruction using bone tunnels with bone-patellar tendon-bone autografts or hamstring tendons. The current recommendation for young athletes is activity modification, rehabilitation, and functional bracing until the patient is near skeletal maturity. At that time, for the very symptomatic patient, the treatment of choice is intra-articular repair of the anterior cruciate ligament. If a skeletally immature patient continues to have instability despite rehabilitation and bracing, a modification of the femoral tunnel to the over-the-top position will not place the lateral femoral physis at risk for premature closure and deformity. A centrally placed tibial tunnel will minimize the risk of angular deformity and minimize limb-length discrepancy if physeal arrest occurs.
REFERENCES: Barry P: Anterior cruciate ligament injuries, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy. Philadelphia, Pa, WB Saunders, 1997, p 358.
McCarroll JR, Shelbourne KD, Porter DA, Rettig AC, Murray S: Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes: An algorithm for management. Am J Sports Med 1994;22:478-484.
Nottage WM, Matsuura PA: Management of complete traumatic anterior cruciate ligament tears in the skeletally immature patient: Current concepts and review of the literature. Arthroscopy 1994;10:569-573.
Stanitski CL: Anterior cruciate ligament injury in the skeletally immature patient: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:146-158.
Question 70:
A 27-year-old man sustains a displaced femoral neck fracture and undergoes urgent open reduction internal fixation. What is the most prevalent complication after this injury?
Options:
- Flexion contracture
- Hip instability
- Nonunion
- Abductor lurch
- Osteonecrosis
Correct Answer: Flexion contracture
Explanation:
DISCUSSION: Femoral neck fractures in young patients are difficult to treat, and AVN is a significant concern. Despite advances in both imaging and implants, this injury often leads to functional impairment.
Haidukewych et al followed treatment of femoral neck fractures in young patients. They found almost 10% of displaced fractures were associated with the development of nonunion, where as 27% were associated with the development of osteonecrosis. Their results were influenced by fracture displacement and the quality of reduction. Varus malreduction most closely correlates with failure of fixation after reduction and cannulated screw fixation.
Swiontkowski reviews both the treatment and post operative complications in intracapsular hip fractures. In this Current Concept Review, the rate of AVN was discussed as being related to the pre-operative degree of displacement seen on radiographs.
Incorrect Responses:
Question 71:
In the posterior approach to the proximal radius (proximal Thompson approach), the supinator is exposed through the interval between what two muscles?
Options:
- Aconeus and extensor carpi ulnaris
- Extensor digitorum comminus and extensor carpi ulnaris
- Extensor digitorum communis and aconeus
- Extensor carpi radialis brevis and extensor digitorum comminus
- Extensor carpi radialis brevis and extensor carpi ulnaris
Correct Answer: Extensor carpi radialis brevis and extensor digitorum comminus
Explanation:
DISCUSSION: The proximal exposure of the radius is most often used for internal fixation of fractures, resection of tumors, or decompression of the posterior interosseous nerve beneath the supinator muscle. The supinator muscle is exposed through the interval between the extensor carpi radialis brevis and the extensor digitorum comminus muscles. This interval can be more easily palpated further distal in the forearm.
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 136-146.
Tubiana R, McCullough C, Masquelet A: An Atlas of Surgical Exposures of the Upper Extremity. London, UK, JB Lippincott, 1990, pp 137-141.
Question 72:
Figures 59a and 59b are the radiographs of a 7-year-old boy who was seen 1 week after he underwent a closed reduction and casting in the emergency department after a fall on an outstretched arm. What is the most appropriate next step for this patient? Review Topic
Options:
- Observation
- Repeat closed reduction and casting
- Open reduction and plate fixation
- Closed reduction and intramedullary nail fixation
Correct Answer: Observation
Explanation:
This child's radiograph shows an acceptably reduced fracture of both the radius and ulna. Generally accepted limits of shaft angulation for cast treatment for girls 8 years of age or younger and boys age 10 or younger are 20 degrees for distal-third, 15 degrees for middle-third, and 10 degrees for proximal-third fractures. Remodeling decreases as one goes from distal to proximal in the forearm. Unless the child's fracture deviates from these criteria, surgical treatment is not necessary. Because of the risk of displacement, however, close follow-up is recommended.
Question 73:
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?
Options:
- Activity modification
- Hinged knee brace
- Partial meniscal excision
- Lateral release
- Physical therapy
Correct Answer: Partial meniscal excision
Explanation:
DISCUSSION: Discoid menisci are rare causes of lateral knee pain in children. Various etiologies have been proposed, including failure of central absorption of the developing meniscus and hereditary transmission. Patients with discoid menisci have pain, clicking, and locking with a loss of active extension on range-of-motion testing. Classification of discoid menisci according to the Watanabe classification include complete, incomplete, and Wrisberg ligament type. The Wrisberg variant contains an abnormal posterior meniscal attachment. MRI is the diagnostic tool of choice, revealing a thick, flat meniscus generally seen in three consecutive MRI images. Symptomatic knees are often associated with a meniscal tear or degeneration and are managed with arthroscopic partial excision to a more normal shape (saucerization).
REFERENCES: Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Bellier G, Dupont JY, Larrain M, et al: Lateral discoid menisci in children. Arthroscopy 1989;5:52-56.
Question 74:
An AP radiograph of the pelvis is shown in Figure 4. What muscle attaches to the avulsed fragment of bone identified by the arrow?
Options:
- Short head of the biceps femoris
- Adductor longus
- Pectineus
- Piriformis
- Semitendinosus
Correct Answer: Semitendinosus
Explanation:
DISCUSSION: The radiograph reveals an avulsion of the ischial apophysis, most likely the result of violent contraction of the attached hamstring tendons (semimembranosus, semitendinosus, and long head of the biceps femoris). The short head of the biceps femoris arises from the linea aspera on the posterior femur. The pectineus and adductor longus attach to the pubic portion of the pelvis. The piriformis runs from the sacrum to the femur.
REFERENCES: Woodburne RT (ed): Essentials of Human Anatomy. New York, NY, Oxford University Press, 1978, pp 542-545.
Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 75:
An 18-year-old man sustains an injury to his lateral ankle after being kicked while playing soccer. He reports persistent pain on the lateral ankle as well as a popping sensation with attempted ankle dorsiflexion and eversion. Which of the following structures anatomically restrains the retracted structure shown in Figure 12?
Options:
- Posterior talofibular ligament
- Calcaneofibular ligament
- Superior peroneal retinaculum
- Inferior peroneal retinaculum
- Peroneal tubercle
Correct Answer: Superior peroneal retinaculum
Explanation:
DISCUSSION: The peroneus brevis and peroneus longus muscles are the main evertors of the hindfoot. As they descend along the posterior fibula, they pass through the retromalleolar sulcus, formed by the concavity of the retromalleolar fibula. This sulcus is deepened by a fibrocartilaginous rim. The superior peroneal retinaculum covers the fibular groove and stabilizes the peroneal tendons within the retromalleolar sulcus. It originates from the posterolateral ridge of the fibula and inserts onto the lateral calcaneus.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 81-89.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 76:
What is the most appropriate orthotic management for the lesion shown in Figure 6?
Options:
- Metatarsal pad
- Morton’s extension orthosis
- Medial longitudinal arch support
- Budin splint
- Viscoelastic heel lift
Correct Answer: Metatarsal pad
Explanation:
DISCUSSION: The figure shows an intractable plantar keratosis (IPK). The keratoma usually forms beneath a bony prominence. This can occur under the sesamoids, most commonly the tibial sesamoid, or under the fibular condyle of a prominent metatarsal head. The initial treatment of an IPK consists of paring down the callused lesion and placing a metatarsal pad proximal to the lesion to provide posting to unload the bony prominence.
REFERENCE: Rudicel SA: Intractable plantar keratoses, in Gould J (ed): Operative Foot Surgery. Philadelphia, PA, WB Saunders, 1994, p 70.
Question 77:
A 43-year-old man who works as a plumber has a painful stiff elbow in his dominant arm. He notes that while he recalls no single event of injury, he thinks the many years of pulling wrenches and soldering pipes have resulted in his problem. He reports that he has pain with any motion in bending his arm and can no longer straighten his elbow. Examination reveals generalized swelling of the elbow, both medial and lateral with a range of motion that lacks 45 degrees of extension and flexes only to 110 degrees. Pronation and supination are also limited to 45 degrees. Audible crepitus is perceived but there is no instability. Radiographs reveal advanced osteoarthritis at the radiocapitellar and ulnohumeral joints with complete loss of articular cartilage. What is the most appropriate initial treatment option? Review Topic
Options:
- Elbow fusion
- Radial head resection
- Total elbow arthroplasty
- Osteophyte resection and capsular release
- Physical therapy with dynamic extension and flexion splints
Correct Answer: Osteophyte resection and capsular release
Explanation:
Osteoarthritis of the elbow is more common in the middle-age laborer such as this plumber, whereas rheumatoid arthritis is more common in older females. Treatment
must respect the physical demands of the patient while trying to preserve joint motion and function with tolerable symptoms. Osteophyte resection and capsular release have offered many patients significant improvement in their symptoms while allowing them to return to most activities. The osteophyte resection and releases can be done effectively by an open or arthroscopic approach. Whereas total elbow arthroplasty would likely result in better and more thorough pain relief, it would not tolerate the occupational demands of this individual. There is no role for physical therapy initially in the face of advanced, painful arthritis associated with long-standing fixed joint contractures. Elbow fusion results in severe loss of function and its indication is rare and usually considered in the face of unmanageable sepsis. Radial head resection may improve symptoms related to the radial capitellar arthritis but would not improve range of motion or end range impingement pain. Also, radial head resection should be avoided in heavy laborers with elbow arthritis because it would lead to increased loads across the arthritic ulnohumeral joint.
Question 78:
Nutritional rickets is associated with which of the following changes in chemical blood level?
Options:
- Low Vitamin D levels
- High to normal calcium levels
- High phosphate levels
- Decreased PTH
- Decreased alkaline phosphatase levels
Correct Answer: Low Vitamin D levels
Explanation:
DISCUSSION: Nutritional rickets is associated with decreased dietary intake of Vitamin D, resulting in low levels of Vitamin D that result in decreased intestinal absorption of calcium
and low to normal serologic levels of calcium. To boost serum calcium levels, there is a compensatory increase in PTH and bone resorption, leading to increased alkaline
phosphatase levels.
REFERENCES: Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
Pettifor J: Nutritional and drug-induced rickets and osteomalacia, in Farrus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 399-466.
Einhorn TA: Metabolic bone disease, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 79:
A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?
Options:
- Fracture
- Patella baja
- Patella alta
- Osteonecrosis
- Maltracking
Correct Answer: Patella baja
Explanation:
DISCUSSION: Patella baja is commonly encountered when converting a high tibial osteotomy (HTO) to a TKA. Patella baja most likely occurs because of scarring. Meding and associates’ study did not show an increased rate of lateral release when converting a knee that had undergone a previous HTO.
REFERENCES: Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA,
JB Lippincott, 2003, vol 2, pp 1265-1271.
Meding JB, Keating EM, Ritter MA, et al: Total knee arthroplasty after high tibial osteotomy:
A comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am 2000;82:1252-1259.
Question 80:
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of
Options:
- repair of the superior labrum.
- isolated supraspinatus repair.
- biceps recentering.
- subscapularis repair and biceps tenodesis.
- subscapularis repair and recentering of the biceps tendon.
Correct Answer: subscapularis repair and biceps tenodesis.
Explanation:
DISCUSSION: The MRI scan reveals a subscapularis tear with a biceps that is out of the groove. Treatment in this patient is most predictable if the subscapularis is repaired. The biceps should either be tenodesed or tenotomized since it is unstable. Recentering of the biceps has been found to be unpredictable. Treatment of these lesions has been shown to have better results if the biceps is either released or tenodesed. This prevents recurrent biceps symptoms that can be source of surgical failure.
REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Deutsch A, Altcheck DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Walch G, Nove-Josserand L, Boileau P, et al: Subluxations and dislocations of the tendon of the long head of the biceps. J Shoulder Elbow Surg 1998;7:100-108.
Question 81:
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Options:
- Erythrocyte sedimentation rate, C-reactive protein, and white blood cell count
- Serum cobalt and chromium ion levels
- MRI with metal artifact reduction sequence (MARS)
- CT of pelvis
Correct Answer: MRI with metal artifact reduction sequence (MARS)
Explanation:
Painful MOM THA and taper corrosion can cause substantial damage to a patient's hip if left untreated. In this case, the workup for a painful MOM THA starts the same as a workup for a painful metal-on-polyethylene bearing couple. Infection must be ruled out in every case with a set of inflammatory markers. If these markers are remotely elevated, this is an indication for joint aspiration. In patients with metal debris, the pathology report often indicates too many cells to count or cellular debris. Metal ion levels do not seem to correlate with prognosis. There are well-functioning patients with high ion levels and poor-functioning patients with low ion levels. Advanced imaging with MARS MRI to evaluate for peritrochanteric fluid collection, a soft-tissue mass, or synovial/capsular hypertrophy will reveal signs of a metal reaction that indicate the need for a revision discussion. A CT scan can show more advanced bony destruction as an indicator of poor prognosis. These films can be used to determine the need for a structural graft or augments for reconstruction of bone loss attributable to metal debris.
Question 82:
The hallucal sesamoids are held together by which of the following structures?
Options:
- Intersesamoid ligament
- Intermetatarsal ligament
- Spring ligament
- Plantar fascia
- Flexor hallucis longus tendon
Correct Answer: Intersesamoid ligament
Explanation:
DISCUSSION: The two sesamoids of the metatarsophalangeal joint are embedded in the tendons of the short flexor of the great toe. They are held together by the intersesamoid ligament and the plantar plate, which inserts on the base of the proximal phalanx of the hallux. The flexor hallucis longus tendon inserts onto the distal phalanx of the great toe. The plantar calcaneonavicular (spring) ligament, by supporting the head of the talus, principally maintains the arch of the foot. The plantar fascia inserts distally onto the skin and to the flexor tendons and transverse metatarsal ligaments at each metatarsophalangeal joint. The intermetatarsal ligament attaches to the base of the second through fifth metatarsals.
REFERENCES: Lewis WH (ed): Gray’s Anatomy of the Human Body, ed 20. Philadelphia, PA, Lea & Febiger, 2000.
Richardson EG: Hallucal sesamoid pain: Causes and surgical treatment. J Am Acad Orthop Surg 1999;7:270-278.
Question 83:
A 75-year-old woman who sustained a fall now reports neck pain and upper extremity weakness. Examination reveals 4 of 5 strength in the upper extremities and 5 of 5 strength in the lower extremities. Radiographs show multilevel degenerative disk disease. An MRI scan is shown in Figure 96. Her clinical presentation is most compatible with which of the following? Review Topic
Options:
- Brachial plexus injury
- Anterior cord syndrome
- Posterior cord syndrome
- Central cord syndrome
- Brown-Séquard syndrome
Correct Answer: Central cord syndrome
Explanation:
The MRI scan shows advanced multilevel degenerative changes and moderate to severe stenosis at C3-C4 and C4-C5 with associated cord signal change. The patient has greater weakness in the upper extremities than in the lower extremities. This pattern is most compatible with central cord syndrome. Patients with brachial plexus injury will have unilateral weakness. Patients with anterior cord syndrome will have greater weakness in the legs than in the arms, and those with Brown-Séquard syndrome will have ipsilateral motor deficits and contralateral pain and temperature deficits.
Question 84:
Which of the following best describes the course of the median nerve at the elbow?
Options:
- Crosses superficial to the ulnar artery, deep to the fibrous arch of the superficialis muscle, deep to the superficial head of the pronator teres muscle
- Crosses superficial to the ulnar artery, deep to the fibrous arch of the superficialis muscle, superficial to the superficial head of the pronator teres muscle
- Crosses deep to the ulnar artery, deep to the fibrous arch of the superficialis muscle, deep to the superficial head of the pronator teres muscle
- Crosses deep to the ulnar artery, deep to the fibrous arch of the superficialis muscle, superficial to the superficial head of the pronator teres muscle
- Crosses deep to the ulnar artery, superficial to the fibrous arch of the superficialis muscle, superficial to the superficial head of the pronator teres muscle
Correct Answer: Crosses superficial to the ulnar artery, deep to the fibrous arch of the superficialis muscle, deep to the superficial head of the pronator teres muscle
Explanation:
DISCUSSION: The median nerve courses superficial to the ulnar artery, deep to the fibrous arch of the superficialis muscle, and deep to the superficial head of the pronator teres muscle. The median nerve lies within the interval between the flexor digitorum superficialis muscle and the flexor digitorium muscle as it progresses toward the wrist.
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
pp 46-47.
Question 85:
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. Figures 4 through 8 are the axial and coronal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
Options:
- prone.
- lateral.
- supine.
- sloppy latera
Correct Answer: supine.
Explanation:
Discussion: Medial plateau fracture dislocations are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the anteroposterior radiograph include an intact lateral column (lateral articular surface still in continuity with tibial shaft), centrolateral articular impaction, shortening, and condylar widening. The medial femoral condyle stays with the fractured medial tibial plateau segment.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 86:
Which of the following factors is most closely associated with early postoperative migration of “stand-alone” lumbar interbody fusion cages?
Options:
- Pseudarthrosis
- Placement of the cage through a posterior approach
- Placement of the cage laparoscopically through an anterior approach
- Use of tapered rather than cylindrical cages
- Use of BMP-2 rather than autograft in the cage
Correct Answer: Placement of the cage through a posterior approach
Explanation:
DISCUSSION: Postoperative migration of lumbar interbody fusion cages is a rare complication. It is most commonly seen after placement of the cages through a posterior approach, with instability of the final construct. It is not associated with the design of the cage, the type of graft used, or a resultant pseudarthrosis.
REFERENCES: McAfee PC: Interbody fusion cages in reconstructive operations on the spine. J Bone Joint Surg Am 1999;81:859-880.
McAfee PC, Cunningham BW, Lee GA, et al: Revision strategies for salvaging or improving failed cylindrical cages. Spine 1999;24:2147-2153.
Question 87:
In the treatment of intra-articular calcaneal fractures, surgical reduction and fixation has been shown to have improved outcomes over nonoperative treatment in all of the following patient groups EXCEPT:
Options:
- Sedentary job
- Sanders IIb fractures
- Women
- Younger age (<29 years old)
- Previous calcaneus fracture
Correct Answer: Sedentary job
Explanation:
DISCUSSION: The referenced study by Buckley et al is a prospective study of intra-articular calcaneus fractures at several trauma centers. They found that overall, the outcomes after nonoperative treatment were not different from those after operative treatment. However, when stratifying groups, women who were managed operatively scored significantly higher on the SF-36 than did women who were managed nonoperatively. Also, patients who were less than twenty-nine years old, had a Böhler angle of 0 degrees to 14 degrees, a comminuted fracture, or a light workload did better after surgery compared with those who were treated nonoperatively.
Question 88:
A 32-year-old amateur bowler has progressive pain in the lateral aspect of the proximal forearm and elbow. Nonsurgical management consisting of a tennis elbow brace, nonsteroidal anti-inflammatory drugs, and activity modification has failed to provide relief. Examination reveals tenderness in the lateral aspect of the proximal forearm and exacerbation of symptoms with resisted finger extension. Radiographs of the elbow reveal no abnormalities. Which of the following studies will aid in diagnosis?
Options:
- MRI of the elbow and forearm
- Bone scan
- Electrodiagnostic studies
- Radial tunnel injection
- Radiographs of the wrist
Correct Answer: Radial tunnel injection
Explanation:
DISCUSSION: It is often difficult to accurately discern between lateral epicondylitis and radial tunnel syndrome. Neither MRI nor a bone scan is likely to reveal abnormalities. Electrodiagnostic studies are often inconclusive, and radial tunnel syndrome often presents without motor weakness. The symptoms of radial tunnel syndrome are expected to improve with an injection of lidocaine into the radial tunnel; therefore, this is the test of choice in this clinical scenario. Radiographs of the wrist will not assist in making the diagnosis.
REFERENCES: Eversmann WW Jr: Entrapment and compression neuropathies, in Green DP (ed): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingston, 1993, pp 1341-1385.
Sarhadi NS, Korday SN, Bainbridge LC: Radial tunnel syndrome: Diagnosis and management. J Hand Surg Br 1998;23:617-619.
Question 89:
A 58-year-old man reports a 2-month onset of groin pain with no history of trauma. Examination reveals that range of motion of the hip is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 20. Treatment should consist of
Options:
- protected weight bearing and anti-inflammatory drugs.
- core decompression of the femoral head.
- vascularized free fibular grafting to the femoral head.
- bipolar hemiarthroplasty of the hip.
- total hip arthroplasty.
Correct Answer: protected weight bearing and anti-inflammatory drugs.
Explanation:
DISCUSSION: The MRI findings show highly increased signal through the entire femoral head and neck on STIR imaging, diagnostic of transient osteoporosis of the femoral head. This disease entity can be seen in middle-aged men, and should be treated nonsurgically. The natural history is that of self-resolution.
REFERENCES: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Urbanski SR, de Lange EE, Eschenroeder HC Jr: Magnetic resonance imaging of transient osteoporosis of the hip: A case report. J Bone Joint Surg Am 1991;73:451-455.
Question 90:
A 61-year-old man reports right hip pain and limited motion after undergoing total hip arthroplasty for posttraumatic arthritis 1 year ago. Figure 6 shows an AP radiograph of the pelvis. To improve motion and relieve pain, management should consist of
Options:
- surgical excision of heterotopic ossification and ethyl hydroxydiphosphonate at a dose of 20 mg/kg of body weight for 3 months.
- surgical excision of heterotopic ossification and irradiation of the right hip in a single dose of 400 Gy postoperatively.
- surgical excision of heterotopic ossification and irradiation of the right hip in a single dose of 700 Gy postoperatively.
- ethyl hydroxydiphosphonate at a dose of 20 mg/kg of body weight for 3 months.
- 25 mg of oral indomethacin administered three times a day for 10 days.
Correct Answer: surgical excision of heterotopic ossification and irradiation of the right hip in a single dose of 700 Gy postoperatively.
Explanation:
DISCUSSION: The patient has symptomatic grade IV Brooker heterotopic ossification. Once the bone has matured, it can be excised. Surgical excision should be combined with postoperative irradiation to avoid recurrence. Pharmacologic and irradiation intervention are not successful beyond the perioperative period unless they are combined with surgical excision of mature heterotopic ossification.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Iorio R, Healy WL: Heterotopic ossification after total hip and total knee arthroplasty: Risk factors, prevention, and treatment. J Am Acad Orthop Surg 2002;10:409-416.
Question 91:
What gene is implicated in spinal muscular atrophy? Review Topic
Options:
- Survival motor neuron I (SMN-I)
- Peripheral myelin protein 22 (PMP22)
- Dystrophin
- Androgen receptor
Correct Answer: Survival motor neuron I (SMN-I)
Explanation:
Deletions in the SMN-I gene are found in 95% to 98% of patients with spinal muscular atrophy. Genetic testing is typically part of the diagnostic workup for spinal muscular atrophy. A positive test result is diagnostic, and, in most cases, eliminates the need for muscle biopsy. The other choices are not associated with spinal muscular atrophy. Defects in PMP22 are the cause of 70% to 80% of cases of Charcot-Marie-Tooth disease. Mutations in the dystrophin gene cause Duchenne muscular dystrophy, and mutations in the androgen receptor cause spinobulbar muscular atrophy (Kennedy's disease).
Question 92:
A year-old woman has severe anterior knee pain. Her radiographs indicate end-stage patellofemoral compartment osteoarthritis. The tibiofemoral compartments are preserved. Extensive nonsurgical treatment has failed to provide relief, and she is offered patellofemoral arthroplasty (PFA). What is the most common long-term mode of failure for PFA using an implant with an onlay prosthesis design?
Options:
- Infection
- Patellar instability
- Aseptic loosening
- Progression of tibiofemoral arthritis
Correct Answer: Progression of tibiofemoral arthritis
Explanation:
DISCUSSION:
Contemporary onlay-design trochlear prostheses in PFA replace the entire anterior trochlear surface. Previous inlay designs were inset within the native trochlea and carried a higher risk of catching and patellar instability, particularly in patients with trochlear dysplasia; they also generally have higher failure rates. The current most common mode of failure is progression of arthritis throughout the knee, in some series as high as 25% at 15 years. Aseptic loosening, particularly of cemented implants, is less common. Infection is an uncommon long-term complication. Patients considering PFA should be advised of the risk of arthritis progression. Many authors routinely obtain a preoperative MRI to assess the status of the tibiofemoral compartments.
Question 93:
When 6 weeks of noninvasive nonsurgical management fails to provide relief for a lumbar disk herniation, a trial of epidural steroid injections is likely to yield which of the following results?
Options:
- Eighty percent to ninety percent of patients report rapid and long-lasting relief of symptoms.
- Patients with extruded disk herniations report greater relief of symptoms than patients with contained herniations.
- Patients with less hydrated disk herniations report the most rapid relief of symptoms.
- Patients may experience temporary relief that lasts a maximum of 6 months.
- The percentage of patients who report significant improvement is similar to that of patients undergoing diskectomy.
Correct Answer: Patients with extruded disk herniations report greater relief of symptoms than patients with contained herniations.
Explanation:
DISCUSSION: Lumbar epidural steroid injections appear to play a role in management of a lumbar disk herniation that has failed to respond to at least 6 weeks of nonsurgical treatment. Approximately 42% to 56% of patients report significant pain relief compared with 92% to 98% of those patients treated with diskectomy. Patients with extruded or sequestered herniations report the greatest and most rapid relief. Similarly, those with well-hydrated disk fragments report rapid relief of symptoms. A smaller percentage of patients report symptom relief compared with those having surgery, but the degree of improvement is similar for both groups and the improvement lasts up to 3 years.
REFERENCES: Butterman GR: Treatment of lumbar disc herniation: Epidural steroid injection compares with discectomy: A prospective, randomized study. J Bone Joint Surg Am 2004;86:670-679.
Butterman GR: Lumbar disc herniation regression after successful epidural steroid injection.
J Spinal Disord Tech 2002;15:469-476.
Question 94:
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include
Options:
- close observation with frequent neurovascular checks.
- emergency angiography.
- emergency exploration of the brachial artery.
- removal of pin fixation and exploration of the brachial artery.
- thrombectomy.
Correct Answer: close observation with frequent neurovascular checks.
Explanation:
DISCUSSION: In a study of over 400 patients with displaced supracondylar fractures, 3.2% of the fractures were associated with the absence of the radial pulse with an otherwise well-perfused hand. Based on this study, a period of close observation with frequent neurovascular checks should be completed before attempting invasive correction of the problem. Because of the satisfactory results with expectant management, angiography, exploration, removal of fixation and exploration, and thrombectomy are contraindicated.
REFERENCE: Sabharwal S, Tredwell SJ, Beauchamp RD, Mackenzie WG, Jakubec DM, Cairns R: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 95:
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management? Review Topic
Options:
- MRI of the spinal axis
- Physical therapy
- A brace for scoliosis
- Observation, with reevaluation in 6 to 12 months
- Posterior spinal fusion from T6 to T12
Correct Answer: MRI of the spinal axis
Explanation:
The patient has an abnormal neurologic exam as shown by the abnormal abdominal reflexes. Furthermore, she has a significant curve and is younger than age 10 years. These findings are not consistent with idiopathic scoliosis. MRI will best rule out syringomyelia or an intraspinal tumor. Bracing and surgery are not indicated for this small curvature prior to obtaining an MRI scan.
Question 96:
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
Options:
- Enhanced neurogenic adaptations
- Advanced myogenic adaptations
- Increased contractile proteins
- Increased short-term energy sources
- Thickening of the connective tissue
Correct Answer: Enhanced neurogenic adaptations
Explanation:
DISCUSSION: Prepubescent athletes gain strength through neurogenic adaptations, including recruitment of motor units, reduced inhibition, and learned motor skills. Myogenic adaptations (muscle hypertrophy) occur after puberty and include increased contractile proteins, thickening of the connective tissue, and increased short-term energy sources such as creatine phosphate.
REFERENCES: Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Micheli LJ: Strength training, in Sullivan JA, Grana WA (eds): The Pediatric Athlete. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 17-20.
Question 97:
A 14-year-old boy is seen for back pain. Radiographic evaluation reveals a grade III isthmic spondylolisthesis. What measurement is most useful in predicting the likelihood of progression?
Options:
- Pelvic incidence
- Slip angle
- Sacral inclination
- Lumbosacral joint angle
- Sagittal rotation
Correct Answer: Slip angle
Explanation:
DISCUSSION: Slip angle has been shown to be highly predictive of the risk for increased slippage in patients with spondylolisthesis. None of the other radiographic parameters listed has been shown to be predictive of the risk for increased slippage.
REFERENCES: Huang RP, Bohlman HH, Thompson GH, et al: Predictive value of pelvic incidence in progression of spondylolisthesis. Spine 2003;28:2381-2385.
Mac-Thiong JM, Wang Z, de Guise JA, et al: Postural model of sagittal spino-pelvic alignment and its relevance for lumbosacral developmental spondylolisthesis. Spine 2008;33:2316-2325.
Figure 22a Figure 22b
Question 98:
Which of the following is indicative of a patient who has been successfully resuscitated following a trauma?
Options:
- Urine output of 0.25 mL/kg/hour
- Lactic acid of 1.9 mmol/L
- Base deficit of -5.5
- Gastric mucosal pH of 6.3
- Pulse pressure of 15
Correct Answer: Urine output of 0.25 mL/kg/hour
Explanation:
DISCUSSION: Rapid fluid resuscitation is the cornerstone of therapy for hypovolemic shock. Fluid should be infused at a rate sufficient to rapidly correct the deficit. If the estimated blood loss is greater than 30% of the total volume(class III), blood replacement is also indicated. In general, a favorable response to fluid replacement therapy includes increased urinary output (at least 0.5ml/kg/hr), improved level of consciousness, increased peripheral perfusion, and changes in vital signs (such as increased BP, increased pulse pressure, and decreased heart rate). Lab values that are important include lactic acid, which is increased if the shock is severe enough to cause anaerobic metabolism, and decreased serum bicarbonate which leads to a negative base deficit. Successful resuscitation in a shock patient will therefore lead to a falling lactate and normalizing pH. Successful resuscitation in a shock patient will therefore lead to a falling lactate (i.e. <2.0mmol/L) and a normalizing pH.
Question 99:
Myodesis of which muscle group is most important for optimal outcome after transfemoral amputation?
Options:
- Abductors
- Adductors
- Hip flexors
- Hip extensors
- Hip external rotators
Correct Answer: Abductors
Explanation:
DISCUSSION: Adductor myodesis is critical for optimal outcome after transfemoral amputation. Pinzur et al. emphasize that when the adductors are not anchored to bone, the hip abductors are able to act unopposed, producing a dynamic flexion-abduction deformity. This deformity prepositions the femur in an orientation that is not conducive to efficient walking. The retracted adductor muscles lead to a poorly cushioning soft-tissue envelope, further complicating prosthetic fitting. Preservation of a functional adductor magnus helps to maintain the muscle balance between the adductors and abductors by allowing the adductor magnus to maintain its power and retain the mechanical advantage for positioning the femur. Preservation is best accomplished with a myodesis.
Question 100:
A 25-year-old student sustains the injury shown in Figures 13a through 13c after falling off a curb. Initial management should consist of
Options:
- weight bearing as tolerated in a hard-soled shoe.
- weight bearing as tolerated in an ankle lacer.
- weight bearing as tolerated in a short leg cast.
- non-weight-bearing in a hard-soled shoe.
- non-weight-bearing in a short leg cast.
Correct Answer: non-weight-bearing in a short leg cast.
Explanation:
DISCUSSION: The radiographs reveal a fracture entering the 4-5 intermetatarsal articulation, consistent with a zone 2 injury. This classically is also referred to as a Jones fracture. The history and radiographic findings indicate this is an acute fracture, which guides management. A zone 1 fracture enters the fifth tarsometatarsal joint, and a zone 3 fracture is a proximal diaphyseal fracture distal to the 4-5 articulation. Initial management is usually nonsurgical and consists of non-weight-bearing in a short leg cast. This method has been shown to result in a better healing rate compared to weight bearing as tolerated.
REFERENCES: Rosenberg GA, Sterra JJ: Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8:332-338.
Lawrence SJ, Botte MJ: Jones’ fracture and related fractures of the proximal fifth metatarsal. Foot Ankle 1993;14:358-365.