Orthopedic Board Prep MCQs: Arthroplasty, Trauma & Oncology | Part 72

Key Takeaway
This page offers Part 72 of an OITE and ABOS Orthopedic Board Review quiz. It features 100 high-yield MCQs, verified by Dr. Mohammed Hutaif, designed for orthopedic residents and surgeons. Content mirrors AAOS exam formats, focusing on Arthroplasty, Fracture, Knee, Revision, and Tumor to ensure comprehensive board preparation.
About This Board Review Set
This is Part 72 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 72
This module focuses heavily on: Arthroplasty, Fracture, Knee, Revision, Tumor.
Sample Questions from This Set
Sample Question 1: At the time of revision total knee arthroplasty, the surgeon is trialing the knee and finds that it extends fully and is stable in flexion with a 23-mm trial spacer; however, the patella is impinging on the polyethylene spacer. No augments ...
Sample Question 2: A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as...
Sample Question 3: A 68-year-old woman undergoes hemiarthroplasty for a proximal humerus fracture. What post-operative motion should be limited as it puts the most stress on the lesser tuberosity fragment fixation?...
Sample Question 4: -A 39-year-old woman jammed her long finger playing softball 24 hours ago. She is unable to actively extend the proximal interphalangeal joint; however, when the joint is brought passively into full extension, she is able to maintain that p...
Sample Question 5: What term best describes the process involved when a growth factor produced by an osteoblast stimulates the differentiation of an adjacent undifferentiated mesenchymal cell during fracture repair?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
At the time of revision total knee arthroplasty, the surgeon is trialing the knee and finds that it extends fully and is stable in flexion with a 23-mm trial spacer; however, the patella is impinging on the polyethylene spacer. No augments were used on the femur or the tibia because the components fit well without them. What is the most appropriate action at this time?
Explanation
REFERENCES: Laskin RS: Joint line position restoration during revision total knee replacement. Clin Orthop Relat Res 2002;404:169-171.
Yoshii I, Whiteside LA, White SE, et al: Influence of prosthetic joint line position on knee kinematics and patellar position. J Arthroplasty 1991;6:169-177.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 100
A 68-year-old woman is undergoing a cementless medial/lateral tapered femoral placement during a total hip arthroplasty and the surgeon notices a small crack forming in the anteromedial femoral neck with final implant insertion. The most appropriate management should include which of the following?
Placement of a cerclage cable around the femoral neck above the lesser trochanter
Removal of the implant, placement of a cable around the femoral neck above the lesser trochanter, and reinsertion of the implant
Removal of the press-fit implant and cementing of the same femoral stem
Final seating of the cementless femoral component without additional measures
Removal of the cementless femoral component and placement of a revision modular taper- fluted femoral stem
DISCUSSION: The recognized treatment of the proximal periprosthetic fracture is first to identify its extent and then to optimize the correction. Removing the implant seems logical to accomplish the identification. Several studies indicate that proximal cerclage wiring is adequate to create a “barrel hoop” stability of the proxima l femur. The postoperative management may also include protected weight bearing and periodic radiographs.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Warren PJ, Thompson P, Fletcher MD: Transfemoral implantation of the Wagner SL stem: The abolition of
subsidence and enhancement of osteotomy union rate using Dall-Miles cables. Arch Orthop Trauma Surg 2002;122:557-560.
Your Source for Lifelong Orthopaedic Learning
Question 2
A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as
Explanation
REFERENCE: Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120.
Question 3
A 68-year-old woman undergoes hemiarthroplasty for a proximal humerus fracture. What post-operative motion should be limited as it puts the most stress on the lesser tuberosity fragment fixation?

Explanation
Question 4
- A 39-year-old woman jammed her long finger playing softball 24 hours ago. She is unable to actively extend the proximal interphalangeal joint; however, when the joint is brought passively into full extension, she is able to maintain that position. Management should consist of
Explanation
Question 5
What term best describes the process involved when a growth factor produced by an osteoblast stimulates the differentiation of an adjacent undifferentiated mesenchymal cell during fracture repair?
Explanation
REFERENCES: Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
Zuscik MJ, Drissi MH, Reynolds PR, et al: Molecular and cell biology in orthopaedics, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 6
Which of the following is considered the most useful screening method for the evaluation of protective foot sensation in a patient with diabetes mellitus?
Explanation
REFERENCES: Pinzur MS, Shields N, Trepman E, Dawson P, Evans A: Current practice patterns in the treatment of Charcot foot. Foot Ankle Int 2000;21:916-920.
Smith KD, Emerzian GJ, Petrov O: A comparison of calibrated and non-calibrated 5.07 nylon monofilaments. Foot Ankle Int 2000;21:852-855.
Question 7
An 80-year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 8
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis in the setting of reaction to metal debris?
Explanation
Question 9
Which of the following statements regarding conus medullaris syndrome is most accurate?
Explanation
REFERENCES: Haher TR, Felmly WT, O’Brien M: Thoracic and lumbar fractures: Diagnosis and management, in Bridwell KH, Dewald RL, Hammerberg KW, et al (eds): The Textbook of Spinal Surgery, ed 2. New York, NY, Lippincott Williams & Wilkins, 1977, pp 1773-1778.
Reitman CA (ed): Management of Thoracolumbar Fractures. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 35-45.
Question 10
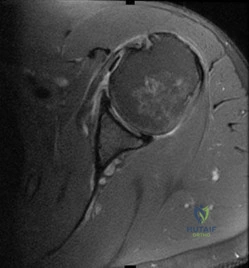
A 45-year-old man reports a history of a popping sensation and pain in the right shoulder while lifting boxes 6 months ago. The pain has persisted with loss of motion of the shoulder. Radiographs and MRI scans are shown in Figures 47a through 47d. Which of the following studies is likely to produce a significant positive result? Review Topic

Explanation
Question 11
Synovitis of the MTP joints with eventual hyperextension deformity of the MTP is a common toe deformity seen with RA.
Explanation
Jin et al conducted a meta-analysis regarding polymorphisms in the 5' flank of COL1A1 gene and the conflicting results relating to osteoporosis. They found that the COL1A1 Sp1 polymorphism is associated with a modest reduction in BMD and an increased risk of fracture.
The attached review by Huang and Kung discusses the multiple genetic and environmental determinants of osteoporosis and illustration A (from a different review by these same authors) lists the known genes currently associated with osteoporosis.
The greatest biomechanical difference between unicortical and bicortical locking screws is seen when what force is applied?
Compression
Torsion
Distraction
Bending on the side of the plate
Bending on the surface perpendicular to the plate
Torsion force has the largest biomechanical difference between unicortical locked screws and bicortical locked screws.
The first referenced article by Roberts et al noted that by replacing the farthest unicortical
screws (3 per side of the fracture) with bicortical locking screws, torsion resistance was increased by over 50%.
The second referenced article by Fulkerson et al noted decreased resistance to all applied forces with unicortical screws in a comminuted fracture model, and recommended against their use in such a fracture.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
You are planning surgery on a 54-year-old female with the tibial plateau fracture seen in figures A and B. After reduction of the joint surface you plan to fill the void with a bone-graft substitute to prevent joint collapse. Which of the following bone-graft substitutes
disappears most quickly in vivo?
Collagen-based matrices
Calcium phosphate
Calcium sulfate
Synthetic calcium sulfate and tri-phosphate mixture
Coraline hydroxyapatite
Calcium sulfate disappears in vivo quickly, usually within 4-12 weeks. Calcium phosphate and coraline hydroxyapatite are resorbed slowly, somewhere between 1-10 years, depending on the manufacturer. Synthetics that combine calcium sulfate and phosphate
resorb quicker than calcium phosphate but slower than calcium sulfate. Collagen-based matrices show quick resorption of the collegen but slow resorption of their hydroxyapatite coating. Walsh et al. examined the in vivo response of calcium sulfate pellets alone or in combination with autogenous bone graft in a sheep model. They found excellent bone formation in defects filled with calcium sulfate pellets. Immunostaining for various cytokines (BMP-2, BMP-7, PDGF, or TGF-beta)
showed elevated levels in the newly formed bone. They proposed that the local environment acidity was responsible for breakdown of the calcium sulfate. Watson evaluated 8 patients with comminuted tibial metaphyseal fractures treated with an injectable calcium sulfate. They found that bone regrowth was observed in all patients and the bone substitute almost completely resorbed by
months. Bucholz reviewed the biochemical, biomechanical, and longevity characteristics of the common bone substitutes.
Which of the following Figures shows a fixation construct achieving absolute stability?
Figure A shows percutaneous pinning, Figure B shows locked bridge plating, Figure C shows intramedullary nailing, Figure D shows lag fixation and neutralization plating, and Figure E shows external fixation. All except Figure D show relative stability constructs.
Absolute stability is a construct seen in Figure D, where lag screws and a neutralization plate are shown in a postoperative clavicle. No micromotion is seen with this technique, and healing is by primary (Haversian) healing, as opposed to the other four constructs, which have relative stability and heal via callus formation. The first reference, the AO Principles textbook, covers this in depth.
The second reference by Claes et al notes that bone can still heal with bone (as opposed to fibrous union) with strain rates up to 15%.
Which immunoglobulin subtype does the rheumatoid factor target?
IgA
IgE
IgM
IgG
Rheumatoid factor does not target an immunoglobulin
Rheumatoid factor is an auto-antibody most commonly seen with rheumatoid arthritis. The presence of rheumatoid factor can also indicate generalized autoimmune activity unrelated to rheumatoid arthritis (e.g. tissue or organ rejection). Rheumatoid factor is itself an IgM antibody that is directed against the Fc portion of IgG antibody. Rheumatoid factor (IgM) attaches to IgG to form immune complexes which are deposited in tissues like the kidney and contribute to the overall disease process in rheumatoid arthritis.
James et al. assessed the occurrence and predictive factors for orthopaedic surgery in an cohort of patients with rheumatoid arthritis. Risk factors for surgery varied but the authors found that decreased inflammatory markers during the first year after diagnosis decreased the risk for subsequent surgery.
The positive predictive value is defined as which of the following?
True positives / (true positives + true negatives)
False negatives / (false negatives + true positives)
False positives / (false positives + false negatives)
(True positives + false positives) / (true negatives + false negatives)
True positives / (true positives + false positives) Corrent answer: 5
The positive predictive value is defined as the true positives divided by the sum of the positive results (true positive and false positive). It is also defined as the probability that a patient with a positive test actually has the disease; it is dependent on prevalence of disease.
The referenced articles by Wojtys and Kuhn et al are two of a series of medical statistics review papers.
An 85-year-old woman undergoes the treatment seen in Figure A for a displaced left femoral neck fracture. During wound closure, the patient becomes hypoxic and hypotensive. Despite aggressive resuscitation efforts, she passes away three hours later in the intensive care unit. The autopsy findings seen in
Figure B from the patient's lungs are most likely the result of which of the following
Reaming for the femoral component
Insertion of a femoral component after cement pressurization
Utilization of undersized broaches during canal preparation
Inadequate beta blockade
Use of spinal anesthesia
The clinical scenario is consistent with fat emboli syndrome. Figure A, shows a cemented bipolar hemiarthroplasty while Figure B shows marrow embolization into the lungs.
Studies have shown that intramedullary pressure and fat embolization are greatest during pressurization of cement and implant insertion.
Intramedullary pressure is influenced by size, shape, sharpness and insertion rate of an implant. Pressurization during cementing of a femoral component generates a large degree of pressure over a much wider surface area than in the other methods described of femoral canal instrumentation or preparation, as the entire femoral canal is
pressurized at one time. This results in the highest degree of marrow embolization to the lungs resulting in hypoxia.
Dobrjanski et al studied which variables affected intramedullary pressurization and found that lower implant insertion speed, lower hammering force, a
rubber- compared with steel-tipped hammer and a larger synthetic bone-to- implant radial gap reduced intramedullary pressure generated in a femur module.
Sustained compression applied to a growth plate under experimental conditions has what effect?
No effect
Accelerated longitudinal growth
Decelerated longitudinal growth
Decelerated apposition growth
Decreased bending strength of the bone
The Heuter-Volkmann Law states that compression across the growth plate slows longitudinal growth.
Stokes et al demonstrated that sustained compression across the growth plate can decrease longitudinal growth by 40%. Tension across the physis increases growth, but to a lesser degree.
A 13-year-old girl with a displaced proximal tibia fracture is brought into the emergency department by her adult cousin. The
fracture needs surgical management. The child is living with her cousin's family while her parents are in Germany. While the child speaks fluent English, her cousin and her parents are German-only speaking. How should you consent this patient?
No consent is needed given the urgent nature of the injury, proceed with surgery
Talk with the cousin, using the child as a translator
Talk with the cousin, using a German-translator
Call the parents in Germany, using the child as a translator over the phone
Call the parents in Germany, using a German-translator over the phone
This is an urgent (not emergent) clinical senario, and as such, the child needs to have
formal consent by speaking with her parents using a German- translator.
Wenger and Lieberman discuss the problems and potential solutions surrounding the process of informed consent in patients who either personally lack capacity to make decisions or in patients who require surrogates (like minors) to make treatment decisions.
Lindseth reviews the ethical issues encountered in pediatric orthopaedics and the problems associated with these decisions. Specifically pediatric consent is confounded because the person giving the consent is not the person who will bear the consequences of the treatment.
What is the primary mode of bisphosphonate excretion?
Renal
Gastrointestinal
Liver
Skin
Pulmonary
Bisphosphonates are a broad class of medicines used to treat osteoporosis and Paget's disease. They work by inhibiting osteoclast-mediated resorption after being absorbed into the inorganic phase of bone and taken up by osteoclasts. The paper by Lin et al provides a nice review of bisphosphonates and describe their appropriate use in enhancing bone density in patients with structurally
flawed bone. They describe the mechanism of action of bisphosphonates as pyrophosphate analogues and their renal mechanism of excretion, thus, prohibiting their use in patients with renal insufficiency. Rosier discusses the role of the orthopaedic surgeon in the diagnosis and treatment of patients with osteoporosis, now referred to as the "own the bone" initiative. Central to the treatment of osteoporosis are bisphosphonates and the anti-RANKL
monoclonal antibody, Denosumab.
The 2009 AAOS Clinical Guideline on prevention of pulmonary embolism in patients undergoing total hip or knee arthroplasty recommends classifying patients as having either a "standard" or "elevated" risk of bleeding complications. The presence of all of the following qualify a patient as having an "elevated" risk of major bleeding EXCEPT?
History of hemophilia
History of protein C deficiency
History of a recent gastrointestinal bleed
History of a recent hemorrhagic stroke
History of Von Willebrand's Disease
The 2009 AAOS Clinical Guideline on prevention of pulmonary embolism in patients undergoing total hip or knee arthroplasty recommends that all patients pre-operatively should be classified as either having an elevated or standard risk of bleeding and either an elevated or standard risk of pulmonary embolism.
A history of a bleeding disorder (e.g., hemophilia, Von Willebrand's Disease), recent GI bleed, or hemorrhagic stroke qualifies a patient as having an elevated risk of major bleeding.
A history of hypercoagulable state (such as protein C deficiency) or previous documented pulmonary embolism qualifies a patient as having an elevated risk of pulmonary embolism. Type of thromboembolism prophylaxis is recommended by weighing risk of major bleeding vs risk of PE. For those patients with a known contraindication to anticoagulation an IVC filter is considered. Mechanical prophylaxis is recommended across all risk (low to
high risk of either bleeding or pulmonary embolism) groups undergoing total hip or total knee arthroplasty. The detailed AAOS guidelines can be found on the AAOS website.
The evidence based clinical recommendations are presented in the reference by Johanson et al.
In consideration of a prosthetic knee, each of the following are advantages of choosing a polycentric knee with fluid control over a constant friction knee EXCEPT:
Allows variations in cadence
Flexes in a more controlled manner
Lighter in weight
Improved stance control allows less energy expenditure
Overall length of the limb is shortened during initiation of a step reducing the risk of stumbling
Single axis, constant friction knees function as a simple hinge. They are light, durable, and much cheaper prostheses making them ideal for growing children who will need multiple prostheses before reaching adulthood. This prosthesis allows only a single speed of walking, and relies solely on alignment for stance phase stability. Polycentric knees offer each of the advantages stated above making it a more ideal prosthesis for the active adult. Disadvantages of the polycentric knee include cost, weight, and more sophisticated maintenance.
Tang et al reviews the current prosthetic options for leg and foot amputees. Illustration A demonstrates a single axis knee prosthesis.
Illustration B demonstrates a polycentric knee prosthesis.
Which of the following biologic agents commonly used to treat rheumatoid arthritis (RA) DOES NOT target tumor necrosis factor- alpha (TNF-alpha)?
Infliximab
Rituximab
Etanercept
Golimumab
Adalimumab
Rituximab is a chimeric monoclonal antibody against the protein CD20, which is primarily found on the surface of immune system B cells. Rituximab is used in combination with methotrexate to treat RA that has not responded to one or more types of treatment, including anti-tumor necrosis factor (TNF) blockers.
In rheumatoid arthritis, and other chronic inflammatory conditions, cytokines produced by activated T-cells/macrophages contribute to the pro-inflammatory state. TNF-alpha is thought to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat RA are directed towards blocking TNF-alpha or its receptors. These drugs are able to reduce inflammation and stop disease progression.
Elliot et al. evaluated the safety and efficacy of infliximab in 20 patients with active RA in an open phase I/II trial lasting 8 weeks. They found that treatment with anti-TNFa was safe, well tolerated and resulted in significant clinical and laboratory improvements.
Illustration A depicts five commonly used anti-TNF alpha biologic agents for the treatment of rheumatoid arhtirits with their usual dosing regimens.
Incorrect Answers:
Receptor activator of nuclear-factor kappa-B ligand (RANKL) is
an important regulator of bone resorption. Which of the following cells is the MAJOR source of RANKL in bone remodelling?
Osteoclasts
Osteoblasts
Integrins
T cells
Macrophages
RANKL, a key osteoclastogenic protein, is expressed by osteoblasts and binds to the RANK receptor on osteoclast precursor cells.
The binding of RANKL to RANK on osteoclast precursor cells drives their differentiation into mature osteoclasts (multinucleated giant cells). Mature osteoclasts bind to the bone surfaces via integrins and resorb bone via their ruffled border within Howship's lacunae. Osteocytes orchestrate bone resorption and bone deposition by controlling osteoclast and osteoblast activity. Osteoblasts release RANKL to induce osteoclast differentiation, while
osteoblasts release osteoprotegerin (OPG) to downregulate osteoclastogenesis. Osteocytes also release fibroblast growth factor-23 (FGF-23), BMPs and sclerostin to regulate osteoblast activity. Antibodies to RANKL and Sclerostin have both been shown to increase bone density.
Compton et al. reviewed osteocyte function and the emerging importance of sclerostin, which is a glycoprotein. Sclerostin is predominantly secreted by osteocytes under physiologic conditions to act as an important negative regulator of bone mass through inhibition of bone formation by osteoblasts.
Illustration A demonstrates local bone milieu. It depicts the interplay between osteocytes, osteoblasts, and osteoclasts via the factors described above.
Incorrect answers:
A 45-year-old woman with rheumatoid arthritis is being scheduled for a total knee athroplasty in 2 weeks. She is currently taking sulfasalazine, Penicillamine, and etanercept, a tumor necrosis factor inhibitor (aTNF-a). What changes should be made to her medication regimen prior to surgery?
Discontinuation of all three medications 1 weeks prior to surgery
Discontinuation of sulfasalazine 1 weeks prior to surgery, continuation of etanercept and penicillamine
Continuation of sulfasalazine, penicillamine, and etanercept
Continuation of sulfasalazine and penicillamine, discontinuation of etanercept 1 week prior to surgery
Continuation of penicillamine, discontinuation of sulfasalazine and etanercept 1 week prior to surgery
Anticytokine disease-modifying antirheumatic drugs (DMARD) have become increasingly popular in the treatment of RA. Immunosuppression and the risk of infection are potential complications for all anti-TNF-alpha medications. Current recommendations for cessation of immunosuppressive therapy are when the drug concentrations are at their lowest levels which include the following: 3 days after etanercept injection; 2 weeks prior to infliximab infusion; 10 days after adalimumab injection. Medications such as sulfasalazine and penicillamine may be continued during the pre and post- operative period. Recent evidence and guidelines such as those reviewed by Keith's paper, suggest that anti-TNF-alpha medications should be stopped 4 weeks prior to surgery.
Giles et al report in their case control series an increased infection rate of RA patients undergoing an orthopaedic procedure who were on TNF-a inhibitors as opposed to patients on more traditional treatment regimens like methotrexate and prednisone.
Which of the following supplements affects blood clotting through its effect on platelets?
Ginkgo
Vitamin D
Ephedra
St. John's Wort
Selenium
Ginkgo and ginseng are two common supplements used in the general population that have inhibitory effects of platelet function. Adverse peri- operative complications consisting of increased bleeding and hematoma formation have been reported with the use of these two herbal supplements. The most commonly used supplements that could have an effect in the peri- operative period include echinacea, ephedra, garlic, ginkgo, ginseng, kava, St John's wort, and valerian. Bleeding has been shown to be effected by garlic, ginkgo, and ginseng; cardiovascular instability from ephedra; and hypoglycemia from ginseng. Kava and valerian have pharmacodynamic herb- drug interactions that can increase the sedative effect of anesthetics. St John's wort has been shown to alter the metabolism of certain drugs used in the perioperative period.
Ang-Lee et al review common supplements used today and their potential anesthesia/operative effects. The article places emphasis on proper history taking of not only medications but also supplements which is often times left out of documentation.
The femur radiograph of a healthy 25-year-old female is compared to the femur radiograph of a healthy 85-year-old female. Which of the following best describes the 25-year-old's femur?
Increased cortical thickness and a smaller medullary canal volume
Decreased cortical thickness and a larger medullary canal volume
Equivalent cortical thickness and medullary canal volume
Increased cortical thickness and larger medullary canal volume
Decreased cortical thickness and a smaller medullary canal volume
As the human body ages the cortical thickness/area decreases and subsequently the diameter/volume of the medullary canal increases. Therefore, a young healthy 25- year-old woman should have thicker cortices and a smaller medullary canal volume than her counterpart at 85 years. A decreased cortical bone area is linked to increased fracture risk.
Stein et al studied femurs from subjects aged 21-92 years of age. They found that a reduction in cortical area was seen in older specimens and this change was more
pronounced in female specimens.
Wrong Answers:
Which of the following is NOT a described complication of corticosteroid injections?
Local flare in surrounding tissues
Apoptosis of myocytes
Skin pigmentation changes
Fat atrophy
Facial flushing
Corticosteroids have not been shown to cause apoptosis of myocytes when injected extra-articularly. Each of the other answers have been described.
Cole and Schumacher provide a review of current uses of corticosteroid injections, and emphasize that how accurately the injection is placed affects the outcome.
Kumar and Newman report prospectively on 672 patients who received 1147 intra- and extra-articular injections. Their overall complication rate was low (16%) with injection site pain (mild) and bleeding constituting the majority of cases. There were 4 instances of fat atrophy in the extra-articular group, and
cases of syncope or dizziness in the intra-articular group. They did not discuss the efficacy of their injections.
A surgeon chooses a periarticular locking plate with unicortical proximal locking screws for an extra-articular distal femur fracture as seen in Figure A. Compared to an identical construct with bicortical unlocked proximal screw fixation, the periarticular locking plate with unicortical locking screws has which biomechanical properties?
Greater torsional and axial fixation strength
Less torsional but greater axial fixation strength
Equal torsional and axial fixation strength
Greater torsional but less axial fixation strength
Less torsional and axial fixation strength
Unicortical locking plates have characteristically less torsional strength than bicortical locking plates and bicortical non-locking plates. Axial strength is improved with locking plate fixation.
Zlowodzki et al studied the LISS periarticular locking plate with unicortical proximal fixation in a distal femur model and found superior axial fixation strength (134%) but worse torsional strength (68%) compared to a fixed angle blade plate with non- locking bicortical screw fixation.
Locked plating was reviewed by Haidukewych and Ricci which highlighted the added cost, unique complications, and they recommended the use of locked plating only in situations when unlocked constructs have demonstrated poor outcomes.
In rat models looking at the effect of malnutrition on fracture healing, amino acid supplementation in a nutritionally deprived rat increases all of the following EXCEPT
Serum albumin
Body mass
Quadriceps total protein content
Fracture callus mineralization
Insulin-like growth factor 1 (IGF-1) mRNA expression
The study by Hughes et al found that essential amino acid supplementation (glutamine, arginine, and taurine) following femoral fracture in a protein- malnourished rat model increases serum albumin, body mass, quadriceps total protein content, and fracture callus mineralization. Expression of IGF-1 and
IGF-2, myosin, actin, and VEGF mRNA were all significantly decreased in the amino acid supplemented group compared to the malnourished group. The malnourished group is thought to have upregulation of mRNA expression in attempt to increase the amount of protein product that is translated, however the lack of amino acid building blocks in the malnutrition group was a barrier to appropriate protein synthesis.
The study by Day et al created a malnourished rat femur fracture model by administering a 6% protein diet. They found that administering a 20% protein diet in the post-fracture period yielded a greater cross-sectional area of the
fracture callus and callus stiffness compared to the 6% protein malnourished group.
The statistical power of a study is best defined by?
1 - probability of type-II (beta) error
True positive/(true positive + false negative)
True negative/(false positive + true negative)
1 - probability of type-I (alpha) error
[True positive/(true positive + false negative)] / false-positive rate
The power of a study is an estimate of the probability of finding a significant association in a research study when one truly exists. The power is defined by
1 - probability of type-II (beta) error, and is often set at 80%. For example, a power of 80% means that if the intervention works, the study has an 80% chance of detecting this and a 20% chance of randomly missing it. A type-II or beta error occurs when one falsely concludes that there is no significant association when there actually is an association (resulting in a false-negative study that rejects a true alternative hypothesis). The type-II or beta error can be determined if Type I error rate and sample size are known. A type-I or alpha error occurs when a significant association is found when there is no true association (resulting in a false-positive study that rejects a true null hypothesis). The alpha level refers to the probability of a type-I (alpha) error and is usually set for most studies at 0.05. Answer 2 is the formula for sensitivity. Answer 3 is the formula for specificity. Answer 5 is the formula for the positive likelihood ratio. The references by
Kocher and Wojtys are excellent reviews of basic biostatistic principles.
A 55-year-old female with a history of metastatic breast cancer develops shoulder pain without any trauma. Which of the following is involved with the findings shown in Figures A and B?
IL-4
RANK
TNF-alpha
OPG
Sox-9
Osteoclastic bone resorption is the final common mechanism for osteolysis, whether due to a pathologic lytic lesion, macrophage activation in particle wear, or normal remodeling. The RANK-RANKL mechanism controls the coupling of osteoblast and osteoclast activation. Figures A and B show an osteolytic lesion in the humerus in a patient with known metastatic breast carcinoma.
RANKL is expressed from osteoblasts and bone-marrow stromal cells. When RANKL binds to the RANK receptor (receptor/activator of NF-[kappa]B) on the cell membrane of osteoclasts it stimulates differentiation from osteoclast progenitor cells to mature osteoclasts. Mature osteoclasts proceed with osteoclastic bone resporption.
Osteoprotegerin (OPG) acts as a decoy receptor by binding to RANKL and blocking the interaction between RANKL and the RANK-receptor and consequently inhibiting osteoclast formation and
activation.
Illustration A depicts the RANK/RANKL involvement in tumor metastatic spread.
Laboratory values of a normal serum calcium and parathyroid hormone can be found in which of the following disease states?
Primary hyperparathyroidism
Type I vitamin D deficient rickets
Type II vitamin D deficient rickets
X-linked hypophosphatemic rickets
Nutritional rickets
Hypophosphatemic rickets is caused by the inability of kidney proximal tubules to reabsorb phosphate due to a mutated PHEX gene, found on the X chromosome. PHEX is thought to protect extracellular matrix glycoproteins from proteolysis. Hypophosphatemic rickets shares many clinical similarities with nutritional rickets but shows PTH levels that are not elevated, even with calcium and phosphate abnormalities.
Pettifor reviews the advances in molecular genetics in the understanding and possible treatments in tumour-induced osteomalacia/rickets.
The review article by Carpenter discusses the X-linked disorder including its clinical manifestations, the wide spectrum of disease severity, and complications of the disease in adult patients.
Illustration A is a table that details the laboratory values associated with each type of rickets.
An 80 year-old female undergoes ORIF of her hip fracture without any complications. A hospitalist consult was obtained for medical clearance pre- operatively, and she was diagnosed with osteoporosis. Which of the following treatment scenarios will lead to the best management of the patient's osteoporosis?
Schedule a follow-up appointment with the patients primary care physician to initiate therapy
Order a physical therapy consult and initiate an exercise plan
Have the patient meet with a nutritionist to increase her calcium and vitamin D intake
Start bisphosphonates, and have the patient follow-up with her primary care physician
Perform a metabolic work-up as an inpatient, and set-up an appointment in an osteoporosis clinic
The initiation of appropriate osteoporosis treatment following hip fractures occurs at a surprisingly low rate. Physical therapy and dietary changes are not appropriate initial treatments for osteoporosis, and bisphosphonate therapy should be prescribed by the physician who will be following and managing the patient's osteoporosis.
Miki et al performed a prospective randomized trial where they compared the rates of osteoporosis treatment initiation. The percentage of patients who were on pharmacologic treatment at 6 months post-injury was 58% in the group whose treatment was directed by the orthopedic surgeon and osteoporosis clinic, and 29% when managed by the primary care physician alone.
The elements chromium, molybdenum, and cobalt are basic components of which of the following implant materials?
Aluminum oxide
Cobalt alloy
Stainless steel
PMMA
Tantalum
Cobalt alloys are extremely strong and are well-suited to applications requiring longevity. Strength of the implant is improved by the addition of molybdenum. Corrosion resistance is addressed by the addition of chromium, which also increases the hardness of the implant.
Incorrect Answers:
Which of the following scenarios of treatment of a humerus fracture best achieves low strain at the fracture site and high stiffness of the treatment construct?
Functional bracing of a transverse midshaft fracture
Comminuted midshaft fracture with locked bridge plating
Short oblique fracture with interfragmentary lag screw and locked neutralization plate
Uniplane external fixation of a spiral open fracture
Oblique fracture with intramedullary nail fixation
Strain in fractures is calculated by dividing the interfragmentary movement by the size of the fracture gap. Strain must be very low (2%) for primary bone healing to occur, and should be less than 10% for secondary bone healing to occur. Stiffness refers the ability of the construct to resist movement under applied loads. Answer 3 describes a situation where primary bone healing is
the goal. For this to occur, there must be no significant gapping at the fracture site, there must be low strain between fracture fragments, and the construct must be stiff.
None of the other answers would accomplish this. Functional bracing and intramedullary fixation both accomplish healing through formation of fracture callus, or secondary healing. A comminuted fracture treated with locked bridge plating relies on less stiffness to allow for secondary healing between fragments. However, since there are many fracture fragments, the strain is distributed among them and therefore remains low. A uniplane external fixator is very unlikely to accomplish low strain and high stiffness in this setting.
A 67-year-old man complains of low-grade fevers and calf pain 2 weeks following a total knee arthroplasty. What is the next appropriate step in management of this patient?
Plethysmography of lower extremity
MRI of lower extremity
CT angiography of lower extremity
Venous ultrasonography
Knee aspiration to evaluate for septic joint
Venous ultrasonography is the next best step in this patient's management, due to the clinical picture of a deep venous thrombosis. The most sensitive and specific recommended diagnostic procedure is a venous ultrasonography.
In their multi-center study, Haut et al. hypothesized that admission to trauma centers that use duplex ultrasound more frequently would independently predict increased DVT reporting for individual patients. They indeed found that trauma centers ultrasound practice was an independent predictor of DVT diagnosis for individual patients, controlling for patient-level risk factors, but concluded the elevated DVT rates at these centers were due to surveillance bias. As such, they recommend that surveillance for DVT should not be considered as a quality control measure in the care of trauma patients.
A patient undergoes closed reduction of a bimalleolar ankle fracture dislocation by the ER physician and is sent to your clinic for evaluation. You evaluate the patient and schedule him for surgery. According to the 2009 guidelines, which of the following scenarios would meet criteria for coding the encounter as a new patient?
You injected his knee in the office almost 3 years ago for osteoarthritis, and have not seen him since
He had an arthroscopic operation by your partner 4 years ago
You were consulted 1 year ago for shoulder pain when he was hospitalized for chronic renal failure
He was seen by your partner in clinic for a herniated disk 2 years ago, but had no procedures performed
You performed a hip replacement on him 12 years ago, and his last follow- up was 18 months ago at which time he was doing well
Only answer two is correct. The 2009 guidlines clarify that the patient can be defined as new only if he has not been seen by anyone in the physician's same group practice and of the same specialty in the past 3 years. Hand and sports medicine specialists with a CAQ, however, are an exception and are allowed to bill for patients already seen by other orthopedists in the same group as new
patients. This scenario would not qualify as a consultation, since the orthopedic surgeon
is taking over care of the patient's problem and is not merely offering advice to another physician who is already caring for the patient. Consultations do not have the same 3 year time qualification. However, Medicare and many other insurers no longer recognize consultation codes.
All the following medications binds reversibly to the enzyme COX-1 EXCEPT
Meloxicam
Diclofenac
Indomethacin
Naproxen sodium
Aspirin
Aspirin binds irreversibly to the cyclooxygenase enzyme. Aspirin acetylates platelet cyclooxygenase and permanently inhibits thromboxane (TX) A2 production leading to its antiplatelet effects. The other NSAID's listed above bind reversibly with COX-1.
Patrono et al discuss the pharmokinetics and platelet effect of both low dose and regular dose aspirin. Nonsteroidal anti-inflammatory drugs compete dose- dependently with arachidonate for binding to platelet cyclooxygenase.
In the treatment of patients with rheumatoid arthritis, TNF-alpha is blocked by which of the following agents?
Tocilizumab
Anakinra
Etanercept
Abatacept
Rituximab
Etanercept is a biochemically designed soluble p75 tumor necrosis factor receptor immunoglobulin G fusion protein, which blocks the downstream
effects of TNF.
Methotrexate is a chemotherapy agent used to inhibit lymphocytes. Gold inhibits monocytes, while sulfasalazine is an anti-inflammatory decreasing the production of
prostaglandins and leukotrienes. Rituximab inhibits B-cells as it
is a monoclonal antibody to CD20 antigen. Anakinra (Kineret) is a recombinant IL-1 receptor antagonist. Abatacept (Orencia) is a selective costimulation modulator that binds to CD-80 and CD-86 (inhibits T cells). Tocilizumab (Actemra)is an IL-6 receptor inhibitor (2nd line treatment for poor response to TNF-antagonist therapy).
Pisetsky wrote an editorial in NEJM discussing the development of TNF blockers through research, and the potential for the use of Etanercept in patients with juvenile RA through its inhibition of lymphotoxin-alpha.
Which of the following medications when combined with methotrexate has been shown to be more effective than methotrexate alone in the treatment of rheumatoid arthritis?
Nitrofurantoin
Rifampin
Azithromycin
Erythromycin
Doxycycline
Tetracycline was initially used in the treatment of rheumatoid arthritis (RA) because Mycoplasma was thought to be the causative agent. It was later found that tetracyclines have biologic effects on the inflammatory and immunologic cascade by inhibiting collagenase activity. Collagenase is an enzyme involved
in breaking down macromolecules in the connective tissue, contributing to the pathologic changes of RA.
In a prospective study, O'Dell et al found that initial therapy with methotrexate plus doxycycline was superior to treatment with methotrexate alone. Furthermore, similar results for low-dose and high-dose doxycycline suggested that antimetalloproteinase effects were more important than the antibacterial effects.
When using C-arm fluorocopy, patient radiation exposure will be increased with which of the following?
The extremity is positioned closer to the image intensifier
A larger body part is imaged compared to a smaller body part
Use of radiation beam collimation
Mini C-arm fluroscopy is used instead of large C-arm fluroscopy
Decreased duration of imaging
Patient radiation exposure will be increased if a larger body part is imaged compared to a smaller body part.
The first study by Giordano et al used radiation dosimeters for large and mini c-arm machines. They found that elevated exposure levels can be expected when larger body parts are imaged, when the extremity is positioned closer to the x-ray source, and when the large c-arm is used over the mini c-arm.
The second study by Giordano et al also used dosimeters for a mini c-arm and found that the surgical team is exposed to minimal radiation during routine
use of mini-c-arm fluoroscopy, except when they are in the direct path of the radiation beam. They list factors to decrease radiation exposure to patient and surgeon including: minimizing exposure time, reducing exposure factors, manipulating the x-ray beam with collimation, orienting the fluoroscopic beam in an inverted position relative to the patient, strategic positioning of the surgeon within the operative field, judicious use of protective shielding during imaging, and maximizing the distance of the surgeon from the radiation beam.
Illustration A shows that arrangement #1 has the body part half-way between the radiation source and image intensifier. Arrangement #2 has the the image intensifier acting as an arm table for the body part with the radiation source further away. Arrangement #1 has more radiation exposure than #2. The distance between the x-ray tube and the body part is doubled in arrangement
#2 compared to arrangement #1. This increased distance correlates to a reduction in exposure according to the inverse square law (reduction in radiation intensity with greater distance from the x-ray source).
You are seeing a 13-year-old girl for asymptomatic flat feet and recommend observation. In educating this patient/family about general bone health, you recommend what amount of daily dietary calcium for your patient?
Question 12
Examination of a supine patient in which the hip is abducted, externally rotated, and flexed is referred to as
Explanation
REFERENCES: Watkins RG: History, physical examination, and diagnostic tests for back and lower extremity problems, in Watkins RG (ed): The Spine in Sports. St Louis, MO, Mosby, 1996, Chapter 7.
Hoppenfeld S: Physical Examination of the Spine and Extremities. East Norwalk, CT, Appleton-Century-Crofts, 1976, Chapter 9.
Question 13
A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann’s sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervical kyphosis in the neutral position, with restoration of lordosis on extension. Which of the following procedures is most likely to result in poor long-term results?
Explanation
REFERENCES: Albert TJ, Vaccaro A: Postlaminectomy kyphosis. Spine 1998;23:2738-2745.
Truumees E, Herkowitz HN: Cervical spondylotic myelopathy and radiculopthy. Instr Course Lect 2000;49:339-360.
Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 14
Histologic studies of surgically resected tissue in lateral epicondylitis demonstrate which of the following findings? Review Topic
Explanation
Question 15
A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the clavicle distal to a line drawn vertically to the coracoid process. Management should consist of
Explanation
REFERENCES: Robinson CM, Cairns DA: Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-782.
Deafenbaugh MK, Dugdale TW, Staeheli JW, et al: Nonoperative treatment of Neer type II distal clavicle fractures: A prospective study. Contemp Orthop 1990;20:405-413.
Question 16
Total hip arthroplasty is most appropriate for the injury shown in Figure A for which of the following patients?

Explanation
Displaced femoral neck fractures can present a challenge to treat. In younger patients with good bone stock a closed vs. open reduction and internal fixation should be attempted. For active older patients a total hip arthroplasty is the best option, especially if there is pre-existing arthritis in the injured hip. THA provides the best function with the least pain and less need for repeat surgery (compared to hemiarthroplasty). For low-demand or debilitated patients, for patients older than age 80, or for those who can not reliably follow hip precautions a hemiarthroplasty provides the lowest risk of dislocation, and thus would be the treatment of choice.
Macaulay et al. present a prospective randomized trial of patients with femoral neck fractures treated with THA vs hemiarthroplasty. They found that functional outcomes and patient satisfaction were higher in the THA group without significant increased risk of complications. Inclusion criteria required patients to be over age 50, be a community ambulator, and were excluded for presence of dementia.
Abboud et al. retrospectively reviewed patients treated with THA for osteoarthritis and compared them to patients treated with THA for a femoral neck fracture. They found no significant difference between the two groups for outcomes or complications.
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture.
Incorrect Answers:
Question 17
Which local treatment option is most appropriate?
Explanation
This patient has a pathologic femur fracture. Her history of antecedent pain in the context of a previously well-functioning implant suggests that a new process such as dedifferentiation of a long-standing lesion may have occurred. The initial radiograph reveals a well-mineralized lesion within the intramedullary canal with punctate calcifications. This by itself suggests an enchondroma or low-grade chondrosarcoma. It is important to note that enchondromas in the long bones rarely cause pathologic fractures. This is not the case when they are present in the hands and feet, where enchondromas frequently have a more aggressive radiologic appearance and pose higher risk. Radiographic findings concerning for malignant dedifferentiation of an enchondroma
include cortical thinning or breach, a soft-tissue mass, or periosteal elevation. The pathologic fracture obscures the ability to identify these hallmarks of malignant degeneration.
Multiple myeloma, renal cell carcinoma, and osteolysis are all typically radiolucent. Implant-associated osteolysis lesions are commonly multiple and periarticular. The histopathology reveals a cartilage tumor. The chondroid tissue appears to be low grade. However, in an adjacent region there is a high-grade component seen both on the low-power view and the second higher-power sample that does not resemble cartilage. This is highly suggestive of a dedifferentiated chondrosarcoma. This component signifies that a portion of the original tumor (low-grade chondrosarcoma), which resembled the tissue of origin, converted into a different cell lineage with more aggressive properties (nearly any type of high-grade sarcoma). Dedifferentiated chondrosarcoma is a highly aggressive malignancy, with average 5-year survivals of less than 50%. As with most sarcomas, the most likely site of metastatic dissemination of chondrosarcoma is pulmonary. Consequently, standard staging entails a high-resolution CT scan of the lungs.
Serum protein electrophoresis and a skeletal survey are used for diagnosis of multiple myeloma. Positron emission tomography/CT fusion scans are used at many centers in the staging of osteosarcoma, but their role in chondrosarcoma staging is an emerging modality that is being investigated. Radiation is not typically used for local treatment of extremity chondrosarcoma. Extended curettage is not appropriate for a high-grade lesion such as this. Revision arthroplasty alone does not address the tumor. Wide resection is the local treatment of choice for high-grade chondrosarcoma; because of the fracture, this patient may require an amputation to achieve wide margins.
RECOMMENDED READINGS
Henderson ER, Pala E, Angelini A, Rimondi E, Ruggieri P. Dedifferentiated peripheral chondrosarcoma: a review of radiologic characteristics. Sarcoma. 2013;2013:505321. doi: 10.1155/2013/505321. Epub 2013 Mar 25. PubMed PMID: 23589702. View Abstract at PubMed
Grimer RJ, Gosheger G, Taminiau A, Biau D, Matejovsky Z, Kollender Y, San-Julian M, Gherlinzoni F, Ferrari C. Dedifferentiated chondrosarcoma: prognostic factors and outcome from a European group. Eur J Cancer. 2007 Sep;43(14):2060-5. Epub 2007 Aug 27. View Abstract at PubMed
Mavrogenis AF, Gambarotti M, Angelini A, Palmerini E, Staals EL, Ruggieri P, Papagelopoulos PJ. Chondrosarcomas revisited. Orthopedics. 2012 Mar 7;35(3):e379-90. doi: 10.3928/01477447-20120222-30. PubMed PMID: 22385450. View Abstract at PubMed
Flemming DJ, Murphey MD. Enchondroma and chondrosarcoma. Semin Musculoskelet Radiol. 2000;4(1):59-71. Review. PubMed PMID: 11061692. View Abstract at PubMed
Question 18
When comparing arthroscopic lavage and knee debridement with placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?
Explanation
Excluding a diagnosis of meniscal tear, loose body, or mechanical derangement, treating knee osteoarthritis of indeterminate cause with arthroscopic lavage and debridement has been found to provide no discernable benefit to offset the risk of surgery. The effects of arthroscopy have not been clinically significant in the vast majority of patient-oriented outcomes measures for pain and function at multiple
times between 1 week and 2 years after surgery.
Question 19
Which of the following anatomic structures are in contact with internal impingement in the throwing athlete?
Explanation
85% of patients undergoing arthroscopy for various indications in one study. Internal impingement is defined as impingement of the posterior-superior rotator cuff between the humerus and posterior-superior glenoid rim. Symptomatic internal impingement is felt to be due to the frequency and magnitude of the impingement in throwers.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 252.
Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40.
Question 20
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include
Explanation
REFERENCES: Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459.
Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Skrzynski MC, Biermann JS, Montag A, Simon MA: Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1996;78:644-649.
Question 21
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. Stress radiographs show a 2-mm medial physeal widening with valgus stress. What is the best initial treatment strategy for this patient?
Explanation
Question 22
0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care? Review Topic
Explanation
Question 23
Osteochondritis dissecans of the capitellum is a source of elbow pain and most commonly occurs in what patient population?
Explanation
REFERENCES: Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med 1998;26:520-523.
Takahara M, Ogino T, Fukushima S, et al: Nonoperative treatment of osteochondritis dissecans of the humeral capitellum. Am J Sports Med 1999;27:728-732.
Question 24
What is the most common complication following metatarsal osteotomy for a bunion deformity in an adolescent?
Explanation
Physeal arrest of the first metatarsal-“While an open epiphysis cannot be considered an absolute contraindication to an osteotomy in either the proximal phalanx, or proximal first metatarsal, it is
important at surgery to determine the exact location of the metaphyseal epiphysis to avoid injury.” Pg. 307 Mann, Surgery of Foot and Ankle.
In studies performed by Blais et. Al. A females full foot growth is usually achieved by 14 years and at 12 years an average less than 1 cm of total foot growth remains with less than 50% of this growth at the proximal epiphysis. Males’ terminal growth expected at 16 years of age with 3cm left at 12 years and approximately 1.5 cm of metatarsal growth.
Most studies show recurrence of Hallux Valgus deformity after surgical correction in the juvenile as inordinately high.
Question 25
Which of the following types of ultra-high molecular weight polyethylene has been associated with the poorest clinical performance?
Explanation
REFERENCES: Wright TM, Rimnac CM, Stulberg SD, et al: Wear of polyethylene in total joint replacements: Observations from retrieved PCA knee implants. Clin Orthop 1992;276:126-134.
Landy MM, Walker PS: Wear of ultra-high molecular-weight polyethylene components of 90 retrieved knee prostheses. J Arthroplasty 1988;3:S73-S85.
Skyrme AD, Mencia MM, Skinner PW: Early failure of the porous-coated anatomic cemented unicompartmental knee arthroplasty: . A 5- to 9-year follow-up study. J Arthroplasty 2002;17:201-205.
Question 26
A healthy 16-year-old boy has had increasing pain in the right knee for the past 3 months. Examination reveals warmth and swelling around the distal femur. Radiographs and an MRI scan are shown in Figures 51a through 51c, and a biopsy specimen is shown in Figure 51d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 205.
Question 27
A right-handed 20-year-old college baseball pitcher has had a 6-month history of vague right elbow pain while pitching. Examination reveals full flexion of the elbow and a loss of only a few degrees of full extension. The elbow is stable, but palpation reveals tenderness over the olecranon. Plain radiographs are inconclusive. MRI and CT scans are shown in Figures 20a and 20b. Management should consist of
Explanation
REFERENCES: Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99.
Griffin LY (ed): Orthopaedic Knowledge Uupdate: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 191-203.
Question 28
A 40-year-old female recreational basketball player notes pain deep within her shoulder that occurs with activity. Pain began insidiously 6 months previously. She has completed a physical therapy program, and an intra-articular corticosteroid injection provided excellent temporary relief. Physical examination shows symmetric range of motion of her shoulder. She has a positive O'Brien’s active compression test. There is no pain with cross-arm adduction or tenderness to palpation over the acromioclavicular joint. Resisted abduction is nonpainful and strong. MRI shows increased signal in the substance of the superior labrum, low-grade bursal surface fraying of the supraspinatus, and mild degenerative changes within the acromioclavicular joint. What is the best treatment option?
Explanation
Question 29
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes?
Explanation
REFERENCES: Canale ST, Beaty JH: Operative Pediatric Orthopaedics. St Louis, MO, Mosby Year Book, 1991, pp 357-385.
Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Question 30
- A consecutive series of 50 patients is randomized to receive either treatment A or treatment B. At a 10-year follow up, patient satisfaction with treatment is measured. Which of the following statistical calculations will provide the most information regarding the magnitude of possible differences between the two groups of patients?
Explanation
Question 31
Figures 91a through 91c are the radiographs of a 10-year-old boy who has a 6-month history of progressive heel pain. The patient is a year-round soccer player and now experiences pain with most every step. What is the most appropriate management?

Explanation
Question 32
-Which type of cells has been implicated in the process shown inFigure?
Explanation

Question 33
Figure 72 is the MRI scan of a 61-year-old man who had left shoulder pain with a massive rotator cuff tear. Active forward elevation was 120 degrees. Arthroscopic examination revealed that the rotator cuff tear was irreparable. The articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment option? Review Topic
Explanation
Question 34
…Giant-cell tumor of bone usually involves the epiphysis of long bones. What is the next most common type of tumor involving this anatomical location?
Explanation
Figures 71a through 71e are the radiographs, MRI scan, and CT scans of a 14-year-old-boy who has cyclical pain in his thigh. His symptoms began approximately 6 months ago. He complains of increased pain when he runs and also of pain that wakes him at night. This pain is relieved by nonsteroidal anti-inflammatory drugs (NSAIDs).

Question 35
Figure 9 is the clinical photograph of a 68-year-old woman 10 days after undergoing primary total knee replacement. She is experiencing hemarthrosis, discoloration, and bruising of the soft tissue about the knee; her history includes persistent serous drainage. This clinical appearance likely is associated with
Explanation
Certain anticoagulants are associated with an increased risk for wound complications. Two studies showed an increase in postsurgical bleeding and wound drainage following use of LMWH. Other investigators have associated use of anticoagulants such as LMWH with an increased incidence of persistent wound drainage and subsequent infection. Current evidence does not support a significant difference in complication rates with and without the use of wound drains or a tourniquet. Regional anesthesia has been associated with less blood loss than general anesthesia and is not associated with a difference in wound complication incidence.

Question 36
A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, and has internal rotation to the fifth lumbar vertebra. At 6 months, his motion fails to improve. Radiographs are shown in Figures 18a and 18b. What is the best course of action?
Explanation
REFERENCES: Cuomo F, Checroun A: Avoiding pitfalls and complication in total shoulder arthroplasty. Orthop Clin North Am 1998;29:507-518.
Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 37
The fracture shown in Figure 32 is strongly indicative of what diagnosis?
Explanation
REFERENCES: Kocher MS, Kasser JR: Orthopaedic aspects of child abuse. J Am Acad Orthop Surg 2000;8:10-20.
Kleinman PK, Marks SC, Blackbourne B: The metaphyseal lesion in abused infants: A radiologic-histopathologic study. Am J Roentgenol 1986;146:895-905.
Question 38
A 14-year-old boy has failed physical therapy management for Scheuermann kyphosis, and an extension thoracolumbosacral orthosis brace is recommended. The boy and his parents are told that the brace will force his thoracic spine into normal sagittal alignment and put the anterior vertebral bodies of the thoracic segment into tension, which will induce bone growth and normalization of wedge-shaped vertebrae. What name is associated with this process?
Explanation
remodels in response to mechanical stress, with the correlate that increased stress causes increased growth, and decreased stress leads to bone loss.
Question 39
A 50-year-old pipefitter falls from a ladder at work and dislocates his non-dominant shoulder. His MRI scan shows supraspinatus and infraspinatus tears with retraction to the glenoid. He cannot actively raise his arm away from his side. He denies prior shoulder symptoms before his fall. Three weeks of physical therapy have failed to improve his function. Which factor has been demonstrated to result in a poor clinical outcome following surgical intervention?
Explanation
Question 40
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
REFERENCE: Kelly MA: Nonprosthetic management of the arthritic knee, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 245-249.
Question 41
Figure 59 shows properties of a material being tested for use as an implant. What is represented by the portion of the stress-strain curve from point A to point B?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 45-46.
El-Ghannam A, Ducheyne P: Biomaterials, in Mow VC, Huiskes R (eds): Basic Orthopaedic Biomechanics and Mechano-Biology, ed 3. Philadelphia, PA, Lippincott-Raven, 2005, pp 501-503.
Question 42
The risk of progression with congenital kyphosis is greatest with which of the following?
Explanation
REFERENCES: McMaster MJ, Singh H: Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-1383.
Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, p 351.
AL-Madena Copy
Question 43
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?
Explanation
REFERENCES: Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Wu YW, Day SM, Strauss DJ, et al: Prognosis for ambulation in cerebral palsy: A population-based study. Pediatrics 2004;114:1264-1271.
Question 44
An 82-year-old woman fell on her right shoulder 2 days ago. She is alert, oriented, and in mild discomfort. Prior to falling, she lived alone and functioned independently. Examination reveals extensive ecchymosis extending to the midhumeral region. Her neurovascular examination is normal. Radiographs are shown in Figures 41a and 41b. What is the most appropriate management?
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-1089.
Bigliani LU, Flatow EL, Pollock RG: Fractures of the proximal humerus, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, pp 352-354.
Question 45
A “p value” of 4% (p=0.04) indicates that the
Explanation
The p value is the probability that the chance selection of patients might suggest a difference in treatment that was not real. Only with a small p value are we willing to believe that the observed difference in treatment is very likely real and not simply due to chance.
The confidence interval provides a measure of the magnitude of the possible difference between two groups of patients, regardless of whether or not the p value was small. This makes the confidence interval more informative than the p value when different treatments are compared. This is much beyond the scope of this review.
Question 46
A 72-year-old man with a history of Parkinson’s disease, stable coronary artery disease, and mild renal insufficiency is seen for hip arthroplasty. Which of the following is considered the most appropriate bearing of choice?
Explanation
REFERENCES: Bragdon CR, Greene ME, Freiberg AA, et al: Radiostereometric analysis comparison of wear of highly cross-linked polyethylene against 36- vs 28-mm femoral heads. J Arthroplasty 2007;22:125-129.
MacDonald SJ: Metal-on-metal total hip arthroplasty: The concerns. Clin Orthop Relat Res 2004;429:86- 93.
Question 47
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?
Explanation
REFERENCES: Wiesel SW, Rothman RH: Occipito-atlantal hypermobility.
Spine 1979;4:187-191.
Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 50-51.
Question 48
When harvesting iliac crest bone graft during a posterior spinal decompression and fusion, injury to what structure can result in painful neuromas or numbness over the skin of the buttocks?
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins 1998, pp 770-773.
Kurz LT, Garfin SR, Booth RE Jr: Harvesting autogenous iliac bone grafts: A review of complications and techniques. Spine 1989;14:1324-1331.
Mrazik J, Amato C, Leban S, et al: The ilium as a source of autogenous bone grafting: Clinical considerations. J Oral Surg 1980;38:29-32.
Question 49
During the early swing phase of the normal gait cycle, what lower extremity muscle is primarily contracting?
Explanation
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Wootten ME, Kadaba MP, Cochran GV: Dynamic electromyography II: Normal patterns during gait. J Orthop Res 1990;8:259-265.
Question 50
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management? Review Topic

Explanation
Question 51
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis? Review Topic
Explanation
Question 52
A 58-year-old woman who underwent a successful total hip replacement for degenerative arthritis 8 years ago reports groin pain for the past 6 months. A radiograph of the hip is shown in Figure 32. At revision, severe deficiency of the posterior column is noted. What reconstructive option would be most appropriate for the acetabulum?
Explanation
REFERENCES: Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 53
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule? Review Topic
Explanation
Question 54
A 12-year-old male patient is scheduled to undergo femoral lengthening. The 2 techniques at your disposal are (1) femoral lengthening along the mechanical axis of the limb with an external fixator, and (2) femoral lengthening along the anatomical axis of the femur with a telescoping nail. What happens to the mechanical axis of the limb when performing these techniques? Review Topic
Explanation
There is a difference of approximately 7° between the mechanical axis of the limb and the anatomical axis of the femur. Lengthening along the anatomical axis of the femur leads to lateral MAD. Similarly, shortening along the anatomical axis of the femur leads to medial MAD.
Kasis et al. described limb shortening of 4cm using external fixator assistance to dial in compression before fixation with a blade plate. They claimed this allowed correction of any tendency to medialize the mechanical axis of the limb prior to plate fixation.
Burghardt et al. described femoral lengthening over a telescoping nail and found lateral shift of the mechanical axis in 26 of 27 limbs, although many were minor and inconsequential. As a rule of thumb, the mechanical axis will shift about 1 mm laterally for every 1 cm of lengthening.
Illustration A illustrates how when lengthening with an external fixator (left), the mechanical axis can be preserved. On the other hand, when lengthening over a nail
(right), the anatomical axis is preserved, but there is lateral MAD (ISKD, intramedullary skeletal kinetic distractor).
Incorrect Answers:
Question 55
A 21-year-old man has had posterior neck discomfort for the past 6 months. A whole-body bone scan and a cervical single-photon emission CT reveal increased activity at the C7 spinous process. MRI reveals multifocal involvement of the spinous process lamina and facet of C7. A CT-directed needle biopsy reveals osteoblastoma. What is the best course of action?
Explanation
REFERENCES: Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1143-1174.
Ozaki T, Liljenquist U, Hillmann A, et al: Osteoid osteoma and osteoblastoma of the spine: Experience with 22 patients. Clin Orthop 2002;397:394-402.
Question 56
A 60-year-old man who underwent left partial knee arthroplasty 6 months earlier was doing well until he experienced left knee pain and swelling for 4 weeks following a dental procedure. The left knee aspirate was bloody, with a white blood cell count of 8,000 and 70% neutrophils. Culture grew group B Streptococcus ( Granulicatella adiacens ), and serologies were elevated, with an erythrocyte sedimentation rate of 55 mm/h (reference range: 0 to 20 mm/h) and a C-reactive protein level of 24 mg/L (reference range: 0.08 to 3.1 mg/L). What is the best next step?
Explanation
This complication is best addressed with either a single-stage or two-stage total knee arthroplasty. A recent report suggests that a single-stage arthroplasty can be effective, although many surgeons would perform a two-stage procedure with an articulating or static spacer. Arthroscopic would be non-effective, especially given 4 weeks of symptoms. Resection arthroplasty without a spacer would leave an unstable and poorly functioning extremity. Knee fusion should be used as a salvage procedure.
Question 57
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
REFERENCES: Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20.
Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Solomonow M, Baratta R, Zhou BH, et al: The synergistic action of the anterior cruciate ligament and thigh muscles in maintaining joint stability. Am J Sports Med 1987;15:207-213.
Question 58
A B D … C E F G

Explanation
Question 59
When compared with patients having a body mass index (BMI) lower than 35, patients with a BMI above 40 who undergo primary total hip arthroplasty (THA) and total knee arthroplasty (TKA) are likely to have
Explanation
The obesity epidemic is increasing, and the number of patients with a BMI higher than 35 undergoing THA and TKA also is growing. Controversy exists over the optimal BMI cutoff and the ability to perform joint replacements safely in patients who are morbidly obese. Several clinical series and national database analyses have shown that morbidly obese patients undergoing THA or TKA are at increased risk for wound complications as well as 30-day and 90-day readmissions. These patients’ incisions are typically larger because of the size of the soft-tissue envelope. Although the clinical scores following successful THA or TKA often are lower than the scores of controls, the overall changes in clinical function and satisfaction are equivalent in nonobese and obese patients.
Question 60
A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?
Explanation
REFERENCES: Bigliani LU, Flatow EL, McCluskey G, et al: Failed prosthetic replacement for displaced proximal humeral fractures. Orthop Trans 1991;15:747-748.
Boileau P, Krishnan SG, Tinsi L, et al: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412.
Tanner MW, Cofield RH: Prosthetic arthroplasty for fractures and fracture-dislocations of the proximal humerus. Clin Orthop Relat Res 1983;179:116-128.
Question 61
A 56-year-old man has had a 2-year history of slowly progressive neck pain and bilateral arm aching. Over the past year, he has noticed intermittent, diffuse numbness in both hands, with decreased grip strength and mild hand clumsiness. He denies any problems with balance. Examination shows a wide-based gait, intrinsic wasting, and a postive Hoffman's sign bilaterally. An MRI scan of the cervical spine is shown in Figure 16. What is the most appropriate treatment? Review Topic

Explanation
Question 62
Varus malalignment after a talar neck fracture with medial comminution causes a decrease in what motion?

Explanation
Herscovici et al review the appropriate management of complex ankle and hindfoot injuries in this instructional course lecture.
Daniels et al performed a cadaveric study where they osteotomized the talar neck and then studied ankle motion with and without removal of a medially based wedge of bone. They found that subtalar eversion was specifically decreased.
Sanders et al found that secondary reconstructive procedures following talar neck fractures were most commonly performed to treat subtalar arthritis or misalignment.
Question 63
Figure 194 is the radiograph of a 71-year-old woman who had a right total hip arthroplasty 4 months ago; now she has tripped and fallen. She is unable to continue weight-bearing activity on her right leg, but denies pain or ambulation issues prior to her fall. She is seen in the emergency department. What is best treatment for this patient?
Explanation
This patient has sustained a periprosthetic hip fracture consistent with a Vancouver B2 pattern. The femoral stem must be revised by bypassing the fracture and simultaneously providing stability through fixation. Method of fixation is dependent upon fracture pattern, and, in this case, the medial fracture fragment is better suited for cerclage fixation. Loosening of the stem precludes simply fixing the fracture with cables, plates, or allograft struts, and there is no need to allow the fracture to heal prior to placing a new stem if the fracture is adequately stabilized with fixation.
CLINICAL SITUATION FOR QUESTIONS 195 THROUGH 197
A 67-year-old woman with osteoarthritis is scheduled for total hip arthroplasty (THA). She has a history of hypertension and stenting for coronary artery disease. She has no surgical history. Her presurgical hemoglobin level is 11.5 g/dL (reference range, 14.0-17.5 g/dL).
Question 64
Which of the following zones of articular cartilage has the highest concentration of proteoglycans?
Explanation
Question 65
A 19-year-old woman fell onto her nondominant hand 6 weeks ago. Radiographs are shown in Figures 37a and 37b. A decision has been made to treat this fracture surgically. What is the best approach to treat this fracture?
Explanation
REFERENCES: Retting ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole fractures. J Hand Surg Am 1999;24:1206-1210.
Filan SK, Herbert TJ: Herbert screw fixation of scaphoid fractures. J Bone Joint Surg Br 1996;78:519-529.
Question 66
Which of the following statements is true regarding the posterior oblique portion of the medial collateral ligament of the elbow? Review Topic
Explanation
The medial ulnar collateral ligament is one of the primary static stabilizers of the elbow and is composed of three parts: anterior, posterior and transverse. The MCL provides resistance to valgus and distractive stresses. The anterior oblique fibers (of the anterior bundle) are the most important against valgus stresses. The posterior bundle is involved elbow contractures and releasing it can yield significant flexion gains, without creating valgus instability.
Morrey et al. performed a pilot study on 4 specimens and found the valgus stability is equally divided among the medial collateral ligament complex, anterior capsule, and bony articulation in full extension; whereas, at 90 degrees of flexion the contribution of the anterior capsule is assumed by the medial collateral ligament which provides approximately 55% of the stabilizing contribution to valgus stress.
Regan et al. was a subsequent study by the same group that found the posterior medial collateral ligament (PMCL) was taut only when the elbow was in a flexed position. Among the collateral ligaments, the anterior (AMCL) was the strongest and stiffest. (Of note, using present terminology these would be referred to as posterior oblique and anterior oblique portions of the medial ulnar collateral complex).
Wada et al. reported a series of open medial releases for post-traumatic elbow contracture and found scarring on the posterior oblique bundle in all cases. Large increases in flexion were achieved by releasing this structure and the capsule without the need for a lateral incision in most cases.
Illustrations A and B show the posterior oblique portion of the medial collateral ligament. Illustration C shows the most recent terminology and identifies the area to be resected for stiffness.
Incorrect Answers:
Question 67
What is the most common arthroscopic finding of internal impingement in an overhead athlete?
Explanation
REFERENCES: Jobe CM: Posterior superior impingement of the rotator cuff on the glenoid rim as a cause of shoulder pain in the overhead athlete. Arthroscopy 1993;9:697-699.
McFarland EG, Hsu C, Neir C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
Question 68
An 8-year-old boy with severe hemophilia A (factor VIII) and no inhibitor is averaging eight transfusions per month for bleeding into the right ankle. Examination shows synovial hypertrophy; range of motion consists of 0° of dorsiflexion and 20° of plantar flexion. The patient’s knees, elbows, and left ankle have no restriction of motion. Standing radiographs of the right ankle are shown in Figure 18. Management should consist of
Explanation
REFERENCES: Greene WB: Synovectomy of the ankle for hemophilic arthropathy. J Bone Joint Surg Am 1994;76:812-819.
Greene WB: Chronic inflammatory arthridities and diseases related to the hematopoietic system, in Drennan JC (ed): The Child’s Foot and Ankle, New York, NY, Raven Press, 1992, pp 461-482.
Question 69
When using a two-incision approach for open reduction and internal fixation of a Hawkins III talar fracture-dislocation involving the talar neck and body, what anatomic structure must be preserved to optimize outcome?
Explanation
REFERENCES: Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.
Question 70
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
REFERENCES: Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
D’Antonio J, Capello W, Manley M, et al: New experience with alumina-on-alumina ceramic bearings for total hip arthroplasty. J Arthroplasty 2002;17:390-397.
Question 71
Intramembranous ossification during fracture repair is characterized by absence of which of the following elements?
Explanation
REFERENCES: Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Buckwalter JA, Einhorn TA, Bolander ME: Healing of the musculoskeletal tissues, in Rockwood CA Jr, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 261-276.
Question 72
Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?
Explanation
REFERENCES: Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 351-360.
Inaba K, Kirkpatrick AW, Finkelstein J, et al: Blunt abdominal aortic trauma in association with thoracolumbar spine fractures. Injury 2001;32:201-207.
Question 73
What is the most appropriate orthosis for hallux rigidus?
Explanation
REFERENCES: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 611.
Watson AD, Wapner KL: Foot and ankle reconstruction, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, p 635.
Question 74
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. Further workup confirms an anterosuperior tear of the acetabular labrum and prominence of the acetabulum. What is the most likely location of a chondral injury associated with these findings?

Explanation
Question 75
A 14-year-old boy has a midshaft fibular lesion. Biopsy results are consistent with Ewing’s sarcoma. Following induction chemotherapy, local control typically consists of
Explanation
REFERENCES: Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodal therapy for the management of primary, nonmetastatic Ewing’s sarcoma of bone: A long-term follow-up of the First Intergroup study. J Clin Oncol 1990;8:1664-1674.
Simon MA, Springfield DS, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 287-297.
Question 76
A 79-year-old woman with a massive rotator cuff tear presents to the emergency department with pain and difficulty moving her arm 7 weeks after undergoing reverse TSA for a displaced 4-part proximal humerus fracture.
Explanation
The complication rate is high after surgical treatment of proximal humerus fractures, particularly in elderly patients with osteoporotic bone. In patients treated with ORIF, common complications include varus malunion (16%), avascular necrosis (10%), screw penetration (8%), and infection (4%). In cases involving a dislocation of the humeral head, avascular necrosis is more common. In patients treated with hemiarthroplasty or TSA, complications include component loosening, infection, and dislocation. TSA is associated with
glenoid loosening in patients with rotator cuff incompetence and should be avoided in these patients. Reverse TSA is a potential solution for this population. Dislocation and postoperative infection are potential complications after reverse TSA.
RECOMMENDED READINGS
Krappinger D, Bizzotto N, Riedmann S, Kammerlander C, Hengg C, Kralinger FS. Predicting failure after surgical fixation of proximal humerus fractures. Injury. 2011 Nov;42(11):1283-
Question 77
A year-old patient fell 3 weeks after undergoing a total hip arthroplasty using cementless fixation of the femoral component. She sustained a comminuted Vancouver type B-2 fracture with displacement of the calcar fragment. What is the best treatment option?
Explanation
The patient has an acute postoperative fracture of the proximal femur with subsidence. It is also common that the stem retroverts relative to the femur. It is most often seen in proximally porous coated stems within 90 days of surgery, one paper found it to occur 0.7% of the time in modern implants. There is always a debate whether this is a missed intraoperative fracture, or a new fracture that has resulted from an event of increased hoop stresses. Removal of the primary stem, placement of a diaphyseal engaging
stem (most frequently a tapered-fluted stem), and cabling of the fracture is the most successful treatment.
Question 78
An 83-year-old woman with a long history of her foot slowly and progressively “turning out” now reports significant ankle pain. History reveals that she has significant cardiac disease and exercise-induced angina. Examination reveals a deficiency in the posterior tibial tendon; however, the hindfoot remains moderately supple. Radiographs reveal a valgus tilt of the tibiotalar joint and early arthrosis. What is the most appropriate orthotic management?
Explanation
REFERENCE: Augustin JF, Lin SS, Berberian WS, et al: Nonoperative treatment of adult acquired flat foot with the Arizona brace. Foot Ankle Clin 2003;8:491-502.
Question 79
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of
Explanation
REFERENCES: Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Warner JJ, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 80
Ulnar collateral ligament (UCL) reconstruction using a modified Jobe technique
Explanation
Certain complications are more strongly associated with the approach and surgical procedure for elbow pathology. With a 2-incision distal biceps repair, heterotopic ossification
with a radial-ulnar synostosis is a concern. This complication can be minimized through irrigation of bone debris and care to avoid dissection between the radius and ulna. With a single-incision distal biceps repair, the lateral antebrachial cutaneous nerve is retracted during the procedure. Numbness on the lateral side of the forearm is common, although often temporary. During arthroscopic debridement for lateral epicondylitis, injury to the radial UCL can occur, leading to posterolateral rotatory instability of the elbow. The modified Jobe technique for UCL reconstruction typically involves an ulnar nerve transposition during the procedure. Numbness and tingling in the fourth and fifth digits are concerns when this procedure is performed.
Question 81
A 56-year-old man who underwent a left total hip arthroplasty 8 years ago is seen following a fall from a standing height. A radiograph obtained at 2 years postoperatively is shown in Figure 55a and a current radiograph obtained in the emergency department is shown in Figure 55b. On further questioning, he reports pain in this thigh for the past 3 years that has been increasing in intensity. Appropriate management at this time includes which of the following?
Explanation
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Springer BD, Berry DJ, Lewallen DB: Treatment of periprosthetic femoral fractures following total hip
arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162. Question 56
A 62-year-old woman who underwent a primary total knee arthroplasty under a combined spinal-epidural anesthetic presents 5 hours postoperatively with severe pain in the extremity that is unresponsive to narcotic pain medication. A tourniquet was used during the procedure. On examination, the patient is unable to dorsiflex or plantar flex the foot and the pulses appear to be asymmetric. What is the next most appropriate step in management?
Discontinuation of the epidural and serial neurologic exams
Loosening of the surgical bandages and elevation of the extremity
MRI of the spine to evaluate for an epidural hematoma
Return to the operating room for angiography and vascular bypass
Return to the operating room for angiography, vascular bypass, and four-compartment fasciotomy PREFERRED RESPONSE: 5
DISCUSSION: The patient has clinical evidence of vascular injury and compartment syndrome. An emergent
vascular consult and a return to the operating room for an angiogram and revascularization are needed. In these situations, thrombectomy alone is often not sufficient and a bypass is typically required. A four-compartment fasciotomy should be done following revascularization of the extremity.
REFERENCES: Calligaro KD, Dougherty MJ, Ryan S, et al: Acute arterial complications associated with total hip and knee arthroplasty. J Vase Surg 2003;38:1170-1177.
Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001;9:253-257.
Ninomiya JT, Dean JC, Goldberg VM: Injury to the popliteal artery and its anatomic location in total knee
arthroplasty. J Arthroplasty 1999;14:803-809.
Question 82
A researcher decides she wants to look at the current total number of patients who have methicillin-resistant Staphylococcus aureus (MRSA) infections in a hospital on 1 particular day. What is the researcher measuring?
Explanation
Question 83
A polytrauma patient sustains a right bicondylar tibial plateau fracture and a right humeral shaft fracture both treated with open reduction, internal fixation. He also underwent statically locked intramedullary nailing of a left femoral shaft fracture. What is the appropriate weightbearing status?

Explanation
Question 84
While performing long fusion with osteotomies for a patient with adult scoliosis and sagittal plane deformity, the neurophysiologist reports a change in motor-evoked potentials in the lower extremities. What is the most appropriate next step?
Explanation
The use of intraoperative neuromonitoring is expanding, especially in the setting of deformity surgery. Changes in monitoring are concerning for the possibility of a neurologic injury; however, several other factors can alter signals. These include hypotension, changes in anesthesia depth and medications, the use of paralytic agents, and technical issues such as leads falling out or becoming disconnected. If a change in neuromonitoring signals is noted, these factors should be checked first to rule out false-positive findings. If this does not correct the problem, the wound should be explored to ensure there is no compression on the neural elements. Finally, if the deformity has been corrected, some of the correction can be released in an attempt to improve the signals. A wake-up test is difficult to perform and does not provide specific information regarding the location of the problem or how to correct it. Steroids may be used depending on surgeon preference, but should not be used until neurologic injury is ruled out. Any neuromonitoring changes always necessitate immediate investigation.
RECOMMENDED READINGS
Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. View Abstract at PubMed
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
Review. PubMed PMID: 21102290. View Abstract at PubMed
Question 85
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?
Explanation
REFERENCES: Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129.
Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Thompson JE: Anatomical methods of approach in operations on the long bones of the extremities. Ann Surg 1918;68:309-316.
Question 86
A 13-year-old boy has a mild deformity of the left sternoclavicular joint after being involved in a rollover accident while riding an all-terrain vehicle. Examination in the emergency department reveals that he is hemodynamically stable, and his neurovascular examination is normal. The CT scan shown in Figure 22 was obtained because radiographs were inconclusive. Management should consist of
Explanation
REFERENCES: Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, p 581.
Wirth MA, Rockwood CA Jr: Acute and chronic traumatic injuries of the sternoclavicular joint. J Am Acad Orthop Surg 1996;4:268-278.
Question 87
Acetaminophen is an antipyretic medication. It exerts its pharmacologic effects by inhibiting which of the following enzymes?
Explanation
REFERENCE: Mancini F, Landolfi C, Muzio M, et al: Acetaminophen down-regulates interleukin-1beta-induced nuclear factor-kappaB nuclear translocation in a human astrocytic cell line. Neurosci Lett 2003;353:79-82.
Question 88
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the Review Topic
Explanation
Question 89
Following an acute dislocation of the patella, the risk of a recurrent dislocation is greater if the patient has which of the following findings?
Explanation
REFERENCES: Cash JD, Hughston JC: Treatment of acute patellar dislocation. Am J Sports Med 1988;16:244-249.
Larsen E, Lauridsen F: Conservative treatment of patellar dislocations: Influence of evident factors on the tendency to redislocation and the theraputic result. Clin Orthop
1982;171:131-136.
Question 90
A 17-year-old boy is shot in the left side of the neck at the C5-6 level and sustains an incomplete spinal cord injury that is called a Brown-Sequard syndrome. Which of the following best describes the expected deficits? Review Topic
Explanation
Question 91
Early postoperative infections following primary total hip arthroplasty are most likely caused by which organism?
Explanation
S aureus is the most common organism cultured in early (fewer than 4 weeks postoperative) periprosthetic infections. Methicillin-resistant S aureus is becoming a more common pathogen in certain patient populations. B hemolytic Streptococcus and some gram-negative infections can also be found in early postoperative infections. S epidermidis, S viridans, and P acnes are more commonly found in late (more than 4 weeks postoperative) infections.
Question 92
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an acceptable arrangement?
Explanation
Question 93
Arthritic change in cartilage is characterized by which of the following findings?
Explanation
Question 94
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 376.
Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Waninger KN, Richards JG, Pan WT, et al: An evaluation of head movement in backboard-immobilized helmeted football, lacrosse, and ice hockey players. Clin J Sport Med
2001;11:82-86.
Donaldson WF III, Lauerman WC, Heil B, et al: Helmet and shoulder pad removal from a player with suspected cervical spine injury: A cadaveric model. Spine 1998;23:1729-1732.
Peris MD, Donaldson WF III, Towers J, et al: Helmet and shoulder pad removal in suspected cervical spine injury: Human control model. Spine 2002;27:995-998.
Question 95
A 67-year-old man with right shoulder osteoarthritis (OA) remains symptomatic despite a course of nonsurgical treatment. A CT scan of the shoulder shows eccentric posterior glenoid wear with 10° of retroversion. What is the appropriate management of this glenoid bone loss during surgery for an anatomic total shoulder arthroplasty?
Explanation
glenoid bone grafting may be considered for glenoid retroversion >15°.
Question 96
A 62-year-old runner injured his right ankle 8 weeks ago. He has ongoing lateral ankle pain and swelling that did not improve with 4 weeks of immobilization and 4 weeks of physical therapy. MR images demonstrate a longitudinal tear of the peroneus brevis tendon. Treatment should involve
Explanation
Additional nonsurgical treatment is not beneficial for peroneal tendon tears. Early repair of longitudinal tears reduces risk for progression to a full-thickness tear that would necessitate peroneus brevis to peroneus longus tenodesis. Platelet-rich plasma has no role in peroneal tendon tears.
RECOMMENDED READINGS
Arbab D, Tingart M, Frank D, Abbara-Czardybon M, Waizy H, Wingenfeld C. Treatment of isolated peroneus longus tears and a review of the literature. Foot Ankle Spec. 2014 Apr;7(2):113-8. doi: 10.1177/1938640013514273. Epub 2013 Dec 30. Review. PubMed
PMID: 24381076.View Abstract at PubMed
Coughlin MJ, Schon LC. Disorders of tendons. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014: 1188-1291.
RESPONSES FOR QUESTIONS 71 THROUGH 75
Lapidus procedure
First metatarsophalangeal (MTP) joint arthrodesis and lesser metatarsal head resection
Proximal first metatarsal osteotomy
Distal first metatarsal chevron osteotomy
Biplanar distal first metatarsal osteotomy
Match the appropriate surgical procedure listed above with the clinical scenario described below.
Question 97
A patient undergoes anterior spinal decompression through a left retroperitoneal approach as treatment of an L2 burst fracture. Following surgery, examination reveals the temperature of the right foot is cool when compared with the left foot. Which of the following neurologic structures has most likely been disrupted?
Explanation
Chapter 60, p. 777: “[After sympathetic denervation], at first the blood flow rises markedly because of lost vascular tone, but over a period of says to weeks the blood flow returns to almost normal because of progressive increase tone of the vascular musculature itself, thus compensating for the loss of sympathetic tone.”
Question 98
A 41-year-old woman with diabetes mellitus fell onto her outstretched arm and sustained an injury to the right elbow. Radiographs are shown in Figures 53a and 53b. What is the most appropriate management?

Explanation
Question 99
Figure 20 shows the resting and stress radiographs of a patient who has had pain and feelings of instability after undergoing a total knee arthroplasty 1 year ago. Which of the following ligaments is not functional and is therefore responsible for the patient’s symptoms?
Explanation
REFERENCE: Incavo SJ, Churchill DL: The role of the posterior cruciate ligament in total knee arthroplasty. Techniques Orthop 1999;14:267-273.
Question 100
An 8-year-old boy reports ankle pain after striking the ground with the medial aspect of his foot while attempting to kick a soccer ball. Radiographs reveal slight distal tibial physeal widening but no other abnormalities. In treating this injury, which of the following associated conditions is most likely present but may be missed without careful evaluation?
Explanation
REFERENCES: Phan VC, Wroten E, Yngve DA: Foot progression angle after distal tibial physeal fractures. J Pediatr Orthop 2002;22:31-35.
Brook GJ, Greer RB: Traumatic rotational displacements of the distal tibial growth plate. J Bone Joint Surg Am 1970;52:1666-1668.
