OITE & ABOS Orthopedic Board Prep MCQs: Foot & Ankle, Trauma & Shoulder | Part 110

Key Takeaway
This page presents a professional orthopedic board review quiz, Part 110. It features 100 verified, high-yield multiple-choice questions (MCQs) for orthopedic residents and surgeons preparing for OITE, AAOS, and ABOS certification exams, with detailed explanations and flexible modes.
About This Board Review Set
This is Part 110 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 110
This module focuses heavily on: Ankle, Foot, Fracture, Nerve, Shoulder.
Sample Questions from This Set
Sample Question 1: The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?...
Sample Question 2: A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsifl...
Sample Question 3: Which of the following findings is more suggestive of neurogenic rather than vascular claudication in the differential diagnosis of leg pain?...
Sample Question 4: A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel’s sign at the proximal aspect of the ...
Sample Question 5: A 23-year-old woman with recurrent anterior instability undergoes an open Bankart procedure. Six months after surgery the patient reports shoulder...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?
Explanation
REFERENCES: Perren SM, Claes L: Biology and mechanics of fracture management, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000,
pp 7-32.
deBoer P: Diaphyseal fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 93-104.
Mast J, Jakob R, Ganz R: Planning and Reduction Techniques in Fracture Surgery. Berlin, Springer-Verlag, 1989.
Question 2
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
REFERENCES: Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.
Question 3
Which of the following findings is more suggestive of neurogenic rather than vascular claudication in the differential diagnosis of leg pain?
Explanation
Question 4
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel’s sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
REFERENCES: Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 5
A 23-year-old woman with recurrent anterior instability undergoes an open Bankart procedure. Six months after surgery the patient reports shoulder

Explanation
Question 6
In the anterior cruciate ligament (ACL)-deficient knee, which of the following variables has the highest correlation with the development of arthritis?
Explanation
REFERENCES: O’Brien WR: Degenerative arthritis of the knee following anterior cruciate ligament injury: Role of the meniscus. Sports Med Arthroscopy Rev 1993;1:114-118.
Fetto JF, Marshall JL: The natural history and diagnosis of anterior cruciate ligament insufficiency. Clin Orthop 1980;147:29-38.
McDaniel WJ Jr, Dameron TB Jr: The untreated anterior cruciate ligament rupture. Clin Orthop 1983;172:158-163.
Question 7
Figures 11a and 11b show the clinical photograph and radiograph of a newborn. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Heyman CH, Herndon CH, Heiple KG: Congenital posterior angulation of the tibia with talipes calcaneus. J Bone Joint Surg Am 1959;41:476-488.
Hofmann A, Wenger DR: Posteromedial bowing of the tibia: Progression of discrepancy in leg lengths. J Bone Joint Surg Am 1981;63:384-388.
Question 8
Bioabsorbable polymers are used in a wide range of orthopaedic devices, including anchors, staples, pins, plates, and screws. What is the primary drawback for bioabsorbable implants?
Explanation
REFERENCES: Ambrose CG, Clanton TO: Bioabsorbable implants: Review of clinical experience in orthopedic surgery. Ann Biomed Eng 2004;32:171-177.
Bergsma JE, de Bruijn WC, Rozema FR, et al: Late degradation tissue response to poly
(L-lactide) bone plates and screws. Biomaterials 1995;16:25-31.
Question 9
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. Radiographs of the player’s right ankle confirm there are no fractures. With a lateral talar tilt test result of 19°, which additional structure is most likely damaged?
Explanation
anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
Question 10
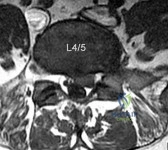
A 32-year-old male presents with left leg pain and weakness. An axial image from his MRI is shown in Figure A. Which of the following physical exam findings would be most consistent with this MRI finding. Review Topic
Explanation
radiculopathy.
While nerve root innervation shows some variability by patient, L5 is "characteristically" responsible for the sensation to the dorsal aspect of the foot, ankle dorsiflexion (tibialis anterior - along with L4), great toe extension (EHL), and hip abduction (gluteus medius).
Suri et al. reported on specific physical exam findings that significantly increased the likelihood of nerve root impingement at specific lumbar levels. They found: L2 was associated with decreased anterior thigh sensation. L3 was associated with a positive femoral stretch test. L4 was associated with a blunted patellar reflex, decreased medial ankle sensation or a positive crossed femoral stretch test. L5 was associated with was associated with decreased hip abductor strength.
Luri et al. reported 8-year follow up on the patients in the spine patient outcomes research trial who underwent surgical vs. conservative care for treatment of lumbar herniated disc. They found that patients who underwent surgical treatment had superior results that were maintained at 8 years compared to patients who underwent conservative management.
Figure A is an axial MRI at the L4/5 disc space that shows a left paracentral disc herniation compressing the descending L5 nerve root. Illustration A identifies the structures in the MRI image. Illustration B demonstrates the dermatome, reflex and motor function associated with the L4, L5 and S1 nerve root.
Incorrect Answers:
(SBQ13PE.102) An 26-year-old male presents to your office complaining of bilateral hip and low back pain. On physical examination, he has 10 degree bilateral hip flexion contractures. An AP pelvis radiograph is demonstrated in figure A. Which of the following findings is consistent with this patient's presentation? Review Topic

A positive flexion, adduction, internal rotation (FADDIR) test
A history of untreated slipped capital femoral epiphysis (SCFE)
A thrombophilia
Normal serum ESR and CRP
Positive Human Leukocyte Antigen B27 (HLA-B27)
The patient has large joint arthralgia and sacroiliac joint sclerosis on AP pelvis radiograph, which is consistent with ankylosing spondylitis. Patients with ankylosing spondylitis have positive Human Leukocyte Antigen B27 (HLA-B27).
Ankylosing spondylitis (AS) is a seronegative spondyloarthropathy that affects the axial skeleton as well as large joints including the hips and knees. The most common initial site of pain is the sacroiliac (SI) joint, and is demonstrated as sacroiliitis on pelvic radiograph. Hip involvement is common, and typically manifests as hip pain and flexion contracture. Serologic studies will be typically be negative for rheumatoid factor, but positive for HLA-B27 in 90% of patients.
Kubiak et. al. review orthopaedic management of AS. Common orthopaedic manifestations include SI joint pain, hip flexion contractures, and stiffness of the cervical and lumbar spine. They report that laboratory analysis of patients with active disease will typically demonstrate mild elevation of ESR, CRP, and WBC. Patients with chronic AS may demonstrate a normocytic anemia. If HLA-B27 is negative, a high clinical suspicion should still be maintained.
Gensler et al. review the different clinical conditions that compose of juvenile-onset spondyloarthritis. They report on the different spondyloarthritides includes ankylosing spondylitis, reactive arthritis, arthropathy associated with inflammatory bowel disease, and that associated with psoriasis. They emphasize that the appearance of sacroiliac joint and spinal disease in the form of ankylosing spondylitis usually takes 5–10 years after initial symptom presentation, and therefore, a definite diagnosis can take several years leading to a delay in diagnosis.
Figure A is an AP pelvis radiograph of a skeletally mature individual demonstrating sclerosis of the SI joint indicative of sacroiliitis. Illustration A shows a axial CT image of the patient in the stem. Sclerosis and bone erosion can be seen in the sacroiliac joint.
Incorrect Answers:
osteonecrosis Answer 3: A infarctions,
of
the
femoral
epiphysis.
thrombophilia may have
osseous manifestations such as bone
which
are
not
evident
on
this
image.
Question 11
An acetabular fracture with all segments of the articular surface detached from the intact posterior ilium is defined as what fracture pattern?

Explanation
radiographic findings consistent with a both column acetabular fracture can be seen in Illustration A (AP), Illustration B (obturator oblique), and Illustration C (iliac oblique).
Question 12
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
Explanation
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 13
What is the most common causative bacteria in septic arthritis in children?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, p 2109.
Jackson MA, Nelson JD: Etiology and medical management of acute suppurative bone and joint infections in pediatric patients. J Pediatr Orthop 1982;2:313-323.
Question 14
Figures 1 through 3 are the radiographs of a 27-year-old man who has had wrist pain since falling 1 day ago. Which treatment offers the best prognosis for prevention of carpal collapse and progressive arthritis?

Explanation
Although this patient’s history includes a recent fall, the radiographs show evidence of a scaphoid nonunion with carpal collapse but no arthritis. Obtaining union of the scaphoid is important to prevent progressive carpal collapse and arthritic changes. ORIF with bone graft is most appropriate to obtain union and correct the collapse deformity. Screw fixation with volar wedge graft often is performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal
row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
Question 15
CLINICAL SITUATION Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities. Based on the radiographs shown in Figures 1 and 2, her tibia is a

Explanation
Question 16
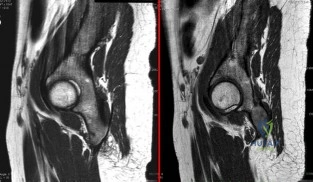
- A right-handed, 53 year old man reports pain in the left shoulder following a fall on an abducted externally rotated shoulder 3 months ago. Examination reveals pain on elevation and tenderness localized to the anterior aspect of the shoulder. Results of the lift-off test are inconclusive due to limited internal rotation. Figure 2 shows the T1-weighted axial image from an MRI-arthrogram. Treatment should include
Explanation
Question 17
- A 19-year-old man sustains a complete spinal cord injury at the C7 level as a result of diving into a lake. He has a blood pressure of 90/50 mm Hg, a pulse of 60/min, and respirations of 20/min. These values most likely signify
Explanation
Question 18
A 65-year-old man has a painful right hip mass that has been growing for several years. A radiograph, CT scan, and photomicrograph are shown in Figures 56a through 56c. What is the most appropriate treatment?
Explanation
REFERENCES: Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530.
Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome.
J Bone Joint Surg Am 1999;81:326-338.
Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 19
A 7-year-old boy sustained an acute puncture wound of the foot after stepping barefoot on a piece of glass 1 day ago. His mother states that she is not sure if she got the piece of glass out; however, she reports that his immunizations are up-to-date. Examination reveals that the wound is slightly erythematous, less than 1 mm in length on the heel, and is not currently draining. What is the next most appropriate step im management?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-205.
DeCoster TA, Miller RA: Management of traumatic foot wounds. J Am Acad Orthop Surg 1994;2:226-230.
Question 20
Which of the following variables has been shown to have the greatest influence on the higher rate of anterior cruciate ligament (ACL) tears in women when compared to men for similar sports?
Explanation
REFERENCES: Harmon KJ, Ireland ML: Gender differences in noncontact anterior cruciate ligament injuries. Clin Sports Med 2000;19:287-302.
Arendt EA: Knee injury patterns among men and women in collegiate basketball and soccer. Am J Sports Med 1995;23:694-701.
Rozzi SL, Lephart SM, Gear WS, Fu FH: Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. Am J Sports Med 1999;27:312-319.
Question 21
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of
Explanation
REFERENCE: Callahan BC, Georgopoulos G, Eilert RE: Hemivertebral excision for congenital scoliosis. J Pediatr Orthop 1997;17:96-99.
Question 22
When using highly cross-linked ultra-high molecular weight polyethylene as an articulating surface for total knee arthroplasty, what property of the material raises concern?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowlegde Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 193-199.
Question 23
Hamstring lengthening and posterior transfer of the rectus femoris will be most successful in a patient with cerebral palsy who has which of the following gait abnormalities?
Explanation
REFERENCES: Gage JR, Perry J, Hicks RR, Koop S, Werntz JR: Rectus femoris transfer to improve knee function of children with cerebral palsy. Dev Med Child Neurol 1987;29:159-166.
Sutherland DH, Santi M, Abel MF: Treatment of stiff-knee gait in cerebral palsy: A comparison by gait analysis of distal rectus femoris transfer versus proximal rectus release. J Pediatr Orthop 1990;10:433-441.
Question 24
A 63-year-old woman is seen 10 weeks after sustaining a closed minimally displaced distal radius fracture. She has been in a short-arm cast and reports minimal pain but notes that she is having difficulty using her thumb. An extensor pollicis longus (EPL) tendon rupture is suspected. Which examination finding would confirm lack of EPL function?
Explanation
As many as to 5% of patients with a nondisplaced distal radius fracture experience EPL rupture. The extensor pollicis brevis (EPB) tendon often attaches to the extensor hood and sometimes continues more distally, providing weak metacarpophalangeal extension even in the setting of EPL disruption. However, because of the vector of its pull, the EPB cannot extend the thumb dorsal to the plane of the palm. A positive Froment sign is noted when flexion of the thumb interphalangeal joint with an attempted key pinch is caused by adductor pollicis weakness from ulnar nerve dysfunction. Compression of the median nerve in the carpal tunnel affects the recurrent motor branch of the abductor pollicis brevis, leading to thenar atrophy. The flexor pollicis longus tendon (FPL) is intact so the patient would not have difficulty flexing the thumb with the palm flat.
Question 25
A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the medial collateral and anterior and posterior cruciate ligaments, as well as the posterior lateral corner. What is the most appropriate first step to rule out a vascular injury?
Explanation
REFERENCES: Miranda FE, Dennis JW, Veldenz HC, et al: Confirmation of the safety and accuracy of physical examination in the evaluation of knee dislocation for injury of the popliteal artery: A prospective study. J Trauma 2002;52:247-252.
Mills WJ, Barei DP, McNair P: The value of the ankle-brachial index for diagnosing arterial injury afterknee dislocation: A prospective study. J Trauma 2004;56:1261-1265.
Question 26
When the great toe deviates into a valgus position, the action of the abductor hallucis muscle becomes one of
Explanation
REFERENCES: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 27
Figure 11 shows the anatomic dissection of the medial side of the knee joint after removal of the superficial fascia. The arrow is pointing to what structure?
Explanation
REFERENCES: Pagnani MJ, Warner JJ, O’Brien SJ, Warren RF: Anatomic considerations in harvesting the semitendinosus and gracilis tendons and a technique of harvest. Am J Sports Med 1993;21:565-571.
Warren LF, Marshall JL: The supporting structures and layers on the medial side of the knee: An anatomical analysis. J Bone Joint Surg Am 1979;61:56-62.
Question 28
Figure 13a shows the radiograph of a 9-year-old girl who sustained complete transverse fractures of the radial and ulnar shafts while in-line skating. A manipulative closed reduction is performed, and the result is seen in Figure 13b. What is the next most appropriate step in management?
Explanation
REFERENCES: Price CT, Scott DS, Kurzner ME, Flynn JC: Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
Vittas D, Larsen E, Torp-Pedersen S: Angular remodeling of midshaft forearm fractures in children. Clin Orthop 1991;265:261-264.
Question 29
Figures 122a and 122b are the radiographs of a 79-year-old woman with a 2-year history of progressively worsening right hip pain. She had a right total hip arthroplasty 7 years prior. An infection workup is negative. She opts for revision surgery; the most appropriate surgical plan to address her femoral component is
Explanation
The patient’s radiographs show loosening of the cemented femoral stem and varus remodeling of the femur. An extended trochanteric osteotomy is necessary because attempting to extract the existing prosthesis and implant another prosthesis without an osteotomy is likely to cause a proximal femoral fracture. Also, an osteotomy would facilitate atraumatic removal of the stem and cement. Cementless fixation is likely to produce a more predictable long-term outcome than cemented fixation for the revision implant.
Question 30
Reconstruction of the injured structure is performed. After surgery, the patient initially notes limitation in motion, and later develops recurrent instability of the knee. Which factor most likely contributed to the development of instability?
Explanation
The anteromedial bundle originates on the anterior and proximal aspect of the lateral femoral condyle and inserts on the anteromedial aspect of the anterior cruciate ligament (ACL) footprint on the proximal tibia. The posterolateral bundle originates posterior and distal to 63 the anteromedial bundle and inserts on the posterolateral aspect of the tibial footprint. The fibers are parallel when the knee is in an extended position. As the knee moves into flexion,
the fibers of the anteromedial bundle rotate externally with respect to the posterolateral bundle. The anteromedial bundle is tensioned in both flexion and extension. The posteromedial bundle is tensioned in extension, but relaxes as the knee moves into flexion.
The lateral meniscus is more commonly injured with an acute injury to the ACL. The medial meniscus is injured more commonly when the ACL is chronically unstable.
The ACL is an intra-articular and intrasynovial structure. It is innervated by posterior articular branches from the tibial nerve. Innervation of the ACL involves several types of mechanoreceptors (Ruffini, Pacini, Golgi tendon, and free-nerve endings) that may contribute to proprioceptive function of the knee and modulation of quadriceps function.
Injury to the ACL is predominantly associated with instability to anterior translation of the tibia in extension. The ACL plays a secondary role to limit internal rotation of the tibia, and a loss of ACL stability is confirmed by the reduction of the tibia from a position of anterior translation and internal rotation (pivot shift). The radiographs demonstrate anterior placement of the femoral tunnel. The convex shape of the lateral femoral condyle can make it more difficult to visualize the anatomic femoral origin of the ACL. Failure to identify the
anatomic footprint can result in anterior placement of the femoral tunnel. Anterior ACL graft placement can result in its impingement against the posterior cruciate ligament and early limitation of knee flexion. Over time, impingement on the graft may result in stretching of the graft and recurrent knee instability symptoms.
RECOMMENDED READINGS
Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. Epub 2005 Oct 19. Review. PubMed PMID: 16235056. View Abstract at PubMed
Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Oct;14(10):982-92. Epub 2006 Aug 5. Review. PubMed PMID: 16897068. View Abstract at PubMed
Question 31
A 35-year-old rock climber sustains an L1 burst fracture from a 30-foot fall while climbing. He sustained no other fractures or serious injuries. He is neurologically intact and has minimal posterior tenderness without increased spinous process separation on examination. Radiographs reveal kyphosis of 20 degrees between T12 and L2 with 30% vertebral height loss. A CT scan shows 55% canal compromise. What is the most appropriate management? Review Topic
Explanation
Question 32
- An infected total knee replacement with symptoms occurring within 4 weeks of surgery and no radiographic signs of osteomyelitis would be best managed with
Explanation
Arthroscopic debridement not recommended secondary to missing cutaneous tracks and soft tissue/muscle involvement.
Question 33
A 35-year-old woman who runs long distance has had posterior calf tenderness for the past 3 months. A clinical photograph is shown in Figure 10a, and MRI scans are shown in Figures 10b and 10c. Management at this point should consist of
Explanation
REFERENCES: Alfredson H, Pietila T, Jansson P, Lorentzon R: Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med 1998;26:360-366.
Angermann P, Hougaard D: Chronic Achilles tendinopathy in athletic individuals: Results of nonsurgical treatment. Foot Ankle Int 1999;20:304-306.
Question 34
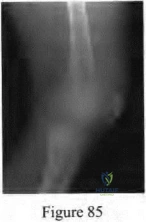
A 25 year-old-male presents with the injury seen in Figure A. Which of the following would be a contraindication to closed management with a functional brace?

Explanation
Indications for operative management of humeral shaft fractures are limited given the high rates of union and ability of adjacent joints to compensate for deformity. Intact muscular tone is necessary to effect bony apposition in closed treatment with a functional brace. The absence of neurologic and muscle function in patients with a flail extremity leads to increased rates of nonunion and malunion.
Rutgers and Ring conducted a retrospective review of patients managed with functional bracing of humeral shaft fractures at a single institution. The authors found a 90% overall union rate, with maintenance of shoulder and elbow motion. They caution though, that 29% of their proximal third fractures went on to nonunion.
Figure A demonstrates an AP radiograph of a comminuted humeral shaft fracture with varus alignment.
Incorrect Answers:
Question 35
A 14-year-old boy has failed physical therapy management for Scheuermann kyphosis, and an extension thoracolumbosacral orthosis brace is recommended. The boy and his parents are told that the brace will force his thoracic spine into normal sagittal alignment and put the anterior vertebral bodies of the thoracic segment into tension, which will induce bone growth and normalization of wedge-shaped vertebrae. What name is associated with this process?
Explanation
remodels in response to mechanical stress, with the correlate that increased stress causes increased growth, and decreased stress leads to bone loss.
Question 36
Which of the following muscle tendons inserts just lateral to the long head of biceps tendon on the proximal humerus?
Explanation
REFERENCE: Bal GK, Basamania CJ: Pectoralis major tendon ruptures: Diagnosis and treatment. Tech Shoulder Elbow Surg 2005;6:128-134.
Question 37
What is the goal of surgical treatment in this scenario?
Explanation
This patient has a metastatic neuroendocrine tumor. Surgical treatment should prioritize palliation of her symptoms. She has high-grade spinal cord compression without neurologic signs or symptoms. Steroids are beneficial for patients with high-grade spinal cord compression caused by tumors, and these drugs should be administered in the acute setting. This patient was appropriately initially treated with conventional radiation. However, she is not a candidate for further radiation because of spinal cord tolerance limits and insufficient clearance between the tumor and spinal cord. Consequently, stereotactic radiation is not an option.
The goal of surgical treatment of this tumor should be palliation of her symptoms rather than cure. A costotransversectomy approach offers the advantage of ventral and dorsal spinal cord access, which is necessary in this case. A sternotomy or transthoracic approach would offer ventral access, but dorsal access would be less than optimal.
RECOMMENDED READINGS
Rose PS, Buchowski JM. Metastatic disease in the thoracic and lumbar spine: evaluation and management. J Am Acad Orthop Surg. 2011 Jan;19(1):37-48. Review. PubMed PMID: 21205766.View Abstract at PubMed
Rades D, Abrahm JL. The role of radiotherapy for metastatic epidural spinal cord compression. Nat Rev Clin Oncol. 2010 Oct;7(10):590-8. doi: 10.1038/nrclinonc.2010.137. Epub 2010 Aug
Question 38
What is the most appropriate surgical treatment for a stage III symptomatic scapholunate advanced collapsed (SLAC) wrist?
Explanation
REFERENCES: Ashmead DT IV, Watson HK, Damon C, et al: Scapholunate advanced collapse wrist salvage. J Hand Surg Am 1994;19:741-750.
Sauerbier M, Trankle M, Linsner G, et al: Midcarpal arthrodesis with complete scaphoid excision and interposition bone graft in the treatment of advanced carpal collapse (SNAC/SLAC wrist): Operative technique and outcome assessment. J Hand Surg Br 2000;25:341-345.
Question 39
What significant structure is most at risk during a posterior approach of the Achilles tendon near its musculotendinous junction?
Explanation
REFERENCES: Webb J, Moorjani N, Radford M: Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-477.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Question 40
Figures 28a and 28b show the sagittal and axial lumbar MRI scans of a 72-year-old man who reports dull aching back pain that spreads to his legs, calves, and buttocks. He has had the pain for several years and it is precipitated by standing and walking and relieved by sitting. His symptoms have been worsening over the past year and he notes that he is leaning forward while walking to help relieve his symptoms. He has had no treatment to date. What is his prognosis if he chooses to pursue nonsurgical management for this condition?
Explanation
REFERENCES: Amundsen T, Weber H, Nordal HJ, et al: Lumbar spinal stenosis: Conservative or surgical management? A prospective 10-year study. Spine 2000;25:1424-1435.
Hilibrand AS, Rand N: Degenerative lumbar stenosis: Diagnosis and management. J Am Acad Orthop Surg 1999;7:239-249.
Tadokoro K, Miyamoto H, Sumi M, et al: The prognosis of conservative treatments for lumbar spinal stenosis: Analysis of patients over 70 years of age. Spine 2005;30:2458-2463.
Question 41
Suprapatellar intramedullary nailing for tibia fractures when compared to infrapatellar nailing is associated with
Explanation
Question 42
Figures 23a and 23b show the MRI scans of a 50-year-old woman who has increasing gait disturbance. She reports three falls in the past week. Examination reveals hyperreflexia, motor weakness in the biceps and triceps, and a positive Hoffman’s sign. What is the most appropriate treatment plan?
Explanation
REFERENCES: Emery SE, Bohlman HH, Bolesta MJ, et al: Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy: Two to seventeen-year follow-up. J Bone Joint Surg Am 1998;80:941-951.
Ferguson RJ, Caplan LR: Cervical spondylotic myelopathy. Neurol Clin 1985;3:373-382.
Herkowitz HN: A comparison of anterior cervical fusion, cervical laminectomy, and cervical laminoplasty for the surgical management of multiple level spondylotic radiculopathy. Spine 1988;13:774-780.
Question 43
A 45-year-old man feels a pop in the anterior aspect of his elbow while lifting furniture. He denies any antecedent pain or injury. Which examination method is best for diagnosing a distal biceps rupture?
Explanation
Question 44
Which of the following terms describe a rehabilitative exercise in which the foot is mobile and the motion of the knee is independent of hip and ankle motion?
Explanation
Question 45
A patient has a tibial shaft fracture and is suspected of having a compartment syndrome involving the deep posterior compartment. Associated signs and symptoms would include paresthesias over the
Explanation
Question 46
- What is the primary mechanism of wear of polyethylene acetabular components?
Explanation
Question 47
Figure A is an AP radiograph of a 68-year-old man who presents to clinic with shoulder pain and dysfunction. On examination of his shoulder, he has pseudoparalysis with attempt at forward elevation and a positive hornblower's sign while demonstrating normal belly press test. Treatment should consist of: Review Topic

Explanation
RTSA can improve pain and function in shoulders with forward elevation pseudoparalysis secondary to rotator cuff tear arthropathy. Following arthroplasty, the deltoid alone can restore overhead elevation but it does not address active external rotation deficit. LDT is a well described procedure for treatment of irreparable posterosuperior rotator cuff tear. Combining RTSA and LDT can address both deficits and in select patients yields significant pain relief and restoration of function.
Walch et al found that hornblower's sign had 100% sensitivity and 93% specificity for irreparable degeneration of teres minor.
Puskas et al present clinical outcomes of RTSA combined with LDT for treatment of chronic combined pseudoparesis of elevation and external rotation of the shoulder in 40 patients. At a mean follow-up of 53 months, the author report excellent clinical outcomes.
Figure A demonstrates a proximal migration of the humerus resulting in femoralization of the humeral head and acetabularization of the acromion from a massive rotator cuff tear.
Incorrect answers:
Question 48
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 49
What is the main mechanism for nutrition of the adult disk?
Explanation
REFERENCES: Biyani A, Andersson GB: Low back pain: Pathophysiology and management. J Am Acad Orthop Surg 2004;12:106-115.
Urban JG, Holm S, Maroudas A, et al: Nutrition of the intervertebral disc: Effect of fluid flow on solute transport. Clin Orthop 1982;170:296-302.
Park AE, Boden SD: Intervertebral disk: Form and function, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 50
During primary total knee arthroplasty, the trial components are in place. The extensor space is tight, but the flexion space is normal. What is the best gap balancing solution?
Explanation
REFERENCES: Vince KG: Revision knee arthroplasty technique. Instr Course Lect 1993;42:325-339.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 513-536.
Question 51
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?
Explanation
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79:1653-1662.
Question 52
A prospective randomized trial is conducted to test the efficacy of Vitamin C versus placebo in treating patients who develop chronic regional pain syndrome (CRPS) after distal radius fractures. At first follow-up, the rates of CRPS are 1% and 9% in the study and placebo group, respectively. Which statistical test is most appropriate to determine significance?
Explanation
Data can be classified as numerical (continuous) or categorical (proportional). Responses to such questions as "What is your major?" or Do you own a car?" are categorical because they yield data such as "biology" or "no." In contrast, responses to such questions as "How tall are you?" or "What is your G.P.A.?" are numerical. When comparing two independent means from numeric data, a t-test is performed. However, if categorical data is being compared, the chi-square test will determine if the proportions are really different.
Kocher et al. review basic clinical epidemiology and biostatistics relevant to orthopaedic surgery. Amongst other things, they describe that data can be summarized in terms of measures of central tendency, such as mean, median, and mode, and in
terms of measures of dispersion, such as range, standard deviation, and percentiles. Illustration A shows an algorithm for determining which test to use for varying data.
Incorrect Answers:
Question 53
During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?
Explanation
REFERENCES: Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
Wapner K, Pavlock GS, Hecht PJ, Naselli F, Walther R: Repair of chronic Achilles tendon rupture with flexor hallucis longus tendon transfer. Foot Ankle Int 1993;14:443-449.
Question 54
A 14-year-old patient has sustained a complete ACL tear of his right knee. Which of the following options has shown to be the most limiting factor for access to pediatric orthopaedic management in the United States?
Explanation
Access to pediatric orthopaedic management has been well investigated. Numerous Level 4 studies have shown that orthopaedic offices in urban and rural areas prefer treating patients with private insurance over patients with Medicaid.
Iobst et al. telephoned 100 urban and rural orthopaedic outpatient offices to schedule an appointment for a 10-year-old patient with a forearm fracture. They showed that 8/100 offices would schedule an appointment within 1 week to the child with Medicaid insurance, as compared to 36/100 that gave an appointment to a child with private insurance.
Pierce et al. contacted 42 orthopaedic practices to schedule an appointment for a 14-year-old patient with an ACL injury. They showed that 38/42 offices scheduled an appointment for the child within 2 weeks with private insurance. This compared to 6/42 that scheduled an appointment for a similar child with Medicaid.
Incorrect Answers:
Question 55
Use of prophylactic knee bracing in contact sports participants results in which of the following?
Explanation
REFERENCES: Albright JP, Powell JW, Smith W, et al: Medial collateral ligament knee sprains in college football: Effectiveness of preventive braces. Am J Sports Med 1994;22:12-18.
Najibi S, Albright JP: The use of knee braces: Part 1. Prophylactic knee braces in contact sports. Am J Sports Med 2005;33:602-611.
Question 56
Figure 23 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain? Review Topic
Explanation
Question 57
A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment should now consist of
Explanation
REFERENCES: Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibial physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Gruber HE, Phieffer LS, Wattenbarger JM: Physeal fractures: Part II. Fate of interposed periosteum in a physeal fracture. J Pediatr Orthop 2002;22:710-716.
Question 58
Figure 37 shows the clinical photograph of a 1-day-old infant who weighed 10.25 lb at birth. Examination reveals an absent right Moro reflex and limited active motion of the right shoulder, elbow, and wrist, but flexion of the fingers. Passive range of motion of the shoulder and elbow is normal. What is the most likely diagnosis?
Explanation
REFERENCES: Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:997-1001.
Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667.
Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:668-677.
Question 59
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. What is the primary cause of a cam deformity?
Explanation
Question 60
A patient has a C6 spinal cord injury. Following stabilization of the spine, the patient should be advised that their expected maximum level of function
Explanation
Question 61
What is the most common reason an individual with a malignant soft-tissue tumor in the extremities seeks medical attention?
Explanation
REFERENCES: Brouns F, Stas M, De Wever I: Delay in diagnosis of soft tissue sarcomas. Eur J Surg Oncol 2003;29:440-445.
Rougraff B: The diagnosis and management of soft tissue sarcomas of the extremities in the adult. Curr Probl Cancer 1999;23:1-50.
Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 62
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time?
Explanation
REFERENCES: Lyons MK, Atkinson JL, Wharen RE, et al: Surgical evaluation and management of lumbar synovial cysts: The Mayo Clinic Experience. J Neurosurg
2000;93:53-57.
Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.
Epstein NE: Lumbar laminectomy for the resection of synovial cysts and coexisting lumbar spinal stenosis or degenerative spondylolisthesis: An outcome study. Spine 2004;29:1049-1055.
Question 63
Figures 33a and 33b show the radiographs of a 10-year-old girl who reports a 4-month history of medial foot pain after she was kicked while playing soccer. The pain is worse with activity and partially relieved by rest. Examination reveals tenderness directly over a prominent navicular tuberosity. Management should consist of
Explanation
REFERENCES: Sella EJ, Lawson JP, Ogden JA: The accessory navicular synchondrosis. Clin Orthop 1986;209:280-285.
Bennett GL, Weiner DS, Leighley B: Surgical treatment of symptomatic accessory tarsal navicular. J Pediatr Orthop 1990;10:445-449.
Question 64
A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month followup appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph is shown in Figure 21. What is the most likely diagnosis? Review Topic

Explanation
(SBQ12TR.54) A 37-year-old male cashier is shot in the leg. He sustains the injury shown in Figures A and B, and is subsequently taken to the operating room for intramedullary nailing. Figure C shows a radiograph of the nail starting point (*). What complication is most likely to result?

Varus malunion
Nonunion
Valgus malunion
Malrotation
Superficial peroneal nerve injury
This patient is presenting with a comminuted fracture of the proximal third of the tibia. He is appropriately undergoing intramedullary nail fixation, however, the start point illustrated in Figure C is too medial and often leads to a valgus malunion.
Intramedullary nail fixation is more technically demanding in proximal tibial fractures than diaphyseal fractures. The valgus deformity is due to imbalanced muscle forces on the proximal fragment, which are then accentuated by a start point that is too medial. An apex anterior (procurvatum) deformity can also occur and results from the pull of the patellar tendon or a posteriorly directed nail that deflects off the posterior tibial cortex and rotates the proximal fragment. The ideal starting point for proximal tibial fractures is slightly lateral to the medial aspect of the lateral tibial spine on a true AP x-ray and very proximal and just anterior to the anterior margin of the articular surface.
Nork et al. reported the results of intramedullary nailing of proximal tibial fractures with emphasis on techniques of reduction. Various techniques were found to be successful including attention to the proper starting point, the use of unicortical plates, and the use of a femoral distractor applied to the tibia.
Lowe et al. describe surgical techniques for complex proximal tibial fractures. They describe the extended leg position, use of a femoral distractor, temporary plate fixation, blocking (Poller) screws, and use of percutaneous clamps as means to achieve reduction during fixation.
Figure A and B show an AP and lateral radiograph of a comminuted extra-articular fracture through the proximal third of the tibia. Figure C demonstrates a start point that is too medial (represented by the asterisk) for intramedullary nail fixation. Illustration A and B show the ideal start point for intramedullary nail fixation of the tibia on AP and lateral radiographs.
Incorrect Answers:
Varus malunion is more likely to occur in midshaft tibia fractures with an intact fibula.
Nonunion after a proximal tibial fracture treated with intramedullary nailing is less common than malunion.
Malrotation occurs most commonly after IM nailing of fractures through the distal third of the tibia.
The superficial peroneal nerve is at risk during distal screw fixation using a LISS plating technique for fracture fixation.
Question 65
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, p 1550.
Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 212-214.
Kaplan FS, August CS, Fallon MD, et al: Successful treatment of infantile malignant osteopetrosis by bone-marrow transplantation: A case report. J Bone Joint Surg Am 1988;70:617-623.
Question 66
A 7-year-old girl is hit by a motor vehicle and sustains the isolated ipsilateral injuries shown in Figures 16a and 16b. What is the optimal definitive method of treatment? Review Topic

Explanation
Question 67
A 15-year-old girl who plays high school basketball has had worsening forefoot pain and swelling that is aggravated by activity for the past 5 weeks. She denies any history of an injury. Examination reveals no deformities. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
walking cast.
REFERENCE: Mann RA, Coughlin MJ: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 413-415.
Question 68
Which of the following is helpful on physical examination to diagnose a fixed posterior shoulder dislocation? Review Topic
Explanation
Question 69
A 51-year-old woman has had progressively increasing right knee pain for the past 6 months. She has a history of metastatic renal cell carcinoma to the lung and the skeletal system. Radiographs are seen in Figures 18a and 18b. The next step in management of the right distal femur lesion should consist of
Explanation
REFERENCES: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Sim FH: Metastatic bone disease of the pelvis and femur. Instr Course Lect 1992;41:317-327.
Question 70
At the time of revision total knee arthroplasty, the surgeon is trialing the knee and finds that it extends fully and is stable in flexion with a 23-mm trial spacer; however, the patella is impinging on the polyethylene spacer. No augments were used on the femur or the tibia because the components fit well without them. What is the most appropriate action at this time?
Explanation
REFERENCES: Laskin RS: Joint line position restoration during revision total knee replacement. Clin Orthop Relat Res 2002;404:169-171.
Yoshii I, Whiteside LA, White SE, et al: Influence of prosthetic joint line position on knee kinematics and patellar position. J Arthroplasty 1991;6:169-177.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 100
A 68-year-old woman is undergoing a cementless medial/lateral tapered femoral placement during a total hip arthroplasty and the surgeon notices a small crack forming in the anteromedial femoral neck with final implant insertion. The most appropriate management should include which of the following?
Placement of a cerclage cable around the femoral neck above the lesser trochanter
Removal of the implant, placement of a cable around the femoral neck above the lesser trochanter, and reinsertion of the implant
Removal of the press-fit implant and cementing of the same femoral stem
Final seating of the cementless femoral component without additional measures
Removal of the cementless femoral component and placement of a revision modular taper- fluted femoral stem
DISCUSSION: The recognized treatment of the proximal periprosthetic fracture is first to identify its extent and then to optimize the correction. Removing the implant seems logical to accomplish the identification. Several studies indicate that proximal cerclage wiring is adequate to create a “barrel hoop” stability of the proxima l femur. The postoperative management may also include protected weight bearing and periodic radiographs.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Warren PJ, Thompson P, Fletcher MD: Transfemoral implantation of the Wagner SL stem: The abolition of
subsidence and enhancement of osteotomy union rate using Dall-Miles cables. Arch Orthop Trauma Surg 2002;122:557-560.
Your Source for Lifelong Orthopaedic Learning
Question 71
A 52-year-old woman who is right hand-dominant sustains an injury to her elbow in a fall. A radiograph is shown in Figure 60. The preferred treatment of this injury pattern should include
Explanation
REFERENCES: Egol KA, Tejwani NC, Bazzi J, et al: Does a Monteggia variant lesion result in a poor functional outcome? A retrospective study. Clin Orthop Relat Res 2005;438:233-238.
Jupiter JB, Leibovic SJ, Ribbans W, et al: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Konrad GG, Kundel K, Kreuz PC, et al: Monteggia fractures in adults: Long-term results and prognostic factors. J Bone Joint Surg Br 2007;89:354-360.
Question 72
Prescribing touch (10 to 15 kg) weight-bearing would be most appropriate in the following scenario?
Explanation
The definition of touch weight bearing (also known as touch-down weight bearing) is ill-defined in the literature. Published data suggest touch weight bearing to be 10 to 15 kg of load applied to ground by the affected limb or less than 20% of body weight. In contrast, partial weight bearing is reported as 20 to 25 kg or 30% to 50% of body weight. Joint reaction forces across the hip have been shown to be lowest with touch weight-bearing. In this scenario, the foot should be flat against the ground so the flexor and extensor musculature that cross the hip are relaxed. With non-weight bearing restrictions, the musculature across the hip will be contracted, which increases contact pressures and joint reaction forces.
Rubin et al. looked at the validity of touch weight-bearing and partial weight bearing regimens. They found that most patients overload the limb up to 50% more than the target weight prescribed.
Lewis et al. showed that maintaining non-weight-bearing position of the involved leg produces increased compressive forces across the hip joint due to activation of the hip flexors compared to restricted weight-bearing.
Incorrect Answers:
Question 73
A 27-year-old man has recurrent right shoulder instability. He first dislocated his shoulder in college while playing rugby and was treated nonsurgically. Since then, he has sustained nearly 1 dozen dislocations and says that his shoulder always feels “loose.” The shoulder recently dislocated in his sleep and while he was putting on clothes. Which factor is a contraindication to an arthroscopic soft-tissue repair?
Explanation
There is much debate in the literature regarding optimal techniques for treatment of shoulder instability. Although some studies suggest that open stabilization may result in lower recurrence rates in contact athletes, this approach is now under scrutiny. Extensive labral involvement (posterior labral involvement in this scenario) is likely more accessible via arthroscopic methods. Although HAGL lesions may be more easily accessible via an open approach (particularly for inexperienced arthroscopists), numerous authors describe successful repair via arthroscopic techniques. Among these responses, the strongest indication for an open approach, including possible bony transfer, is high-grade glenoid bone loss. Although the critical amount of bone loss is a topic of debate, most surgeons and authors suggest a cutoff of 20% to 25%.

CLINICAL SITUATION FOR QUESTIONS 90 THROUGH 92
Figure 90 is the radiograph of a 14-year-old pitcher who plays in a year-round baseball program and has vague pain in his dominant shoulder. The pain occurs with throwing, and it has been worsening for 2 months. Pain typically occurs during the late cocking phase of throwing. He has no tenderness of the rotator cuff and 5/5 rotator cuff strength. His arc of motion is symmetric between his dominant and nondominant arms. The sulcus sign is negative.
Question 74
A 68-year-old male presents with gait instability, clumsiness of the hands, and the MRI images shown in Figure A. You decide to proceed with surgical decompression. When planning your surgical treatment, it is important to note that compared to a posterior approach, the anterior procedure has: Review Topic

Explanation
Cervical myelopathy has a progressive course and therefore if there is evidence of functional impairment surgical decompression is indicated. Either an anterior decompression or posterior decompression can be used depending on a variety of factors including number of levels involved and sagittal alignment of the cervical spine. In general, a posterior approach is used when three or more levels are involved and the spine is in neutral or lordotic alignment.
Fehlings et al. did a prospective study on the risks of complications associated with surgical treatment of cervical myelopathy. They found that combined anterior and posterior procedures had a significantly higher rate of complication than either anterior-only or posterior-only procedures. Posterior procedures had a higher rate of wound infections compared to anterior. They found no statistical difference in the over-all complication rate, incidence of C5 radiculopathy, or dysphagia between an anterior-only or posterior-only procedure.
Fehlings et al. did a prospective study on outcomes following surgical treatment of cervical myelopathy. At one year follow-up they found a significant improvement in mJOA score, Nurick grade, NDI score, and all SF-36v2 dimensions. With the exception of mJOA scores, these improvements were not statistically related to severity of disease.
Liu et al. performed a meta-analysis of outcomes following surgical decompression of cervical myelopathy. They found outcomes following anterior procedures were better than those for posterior procedures when there were less than 3 affected levels. With 3 or greater levels, no statistical difference in outcomes could be found between the two approaches. They note none of their reviewed publications represent high-quality prospective randomized trials.
Figure A is a sagittal MR image of the cervical spine showing multi-level degenerative disease with cord compression consistent with cervical myelopathy.
Incorrect Answers:
Question 75
Results of a study demonstrating no difference between treatments when a difference truly exists is an example of which of the following?
Explanation
fragile p-values is that small sample sizes may result in wide variability of p-values with only one change in a data point for a given group. This singular change could be a chance occurrence, but it still can affect the statisticalsignificance of the outcomes analysis. Fragility of p-values is limited by increasing sample sizes. Negative predictive value is the proportion of patients with negative test results who are correctly diagnosed.
Question 76
The natural history of cervical spondylolytic myelopathy is best described as
Explanation
REFERENCES: Emery SF: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Lees F, Turner JA: The natural history and prognosis of cervical spondylosis. Brit Med J 1963;2:1607-1610.
Clarke E, Robinson PK: Cervical myelopathy: A complication of cervical spondylosis. Brain 1956;79:486-510.
Question 77
Figure 17 shows the AP radiograph of a 5-year old child who has mild short stature and a painless bilateral gluteus medius lurch. Initial work-up should include
Explanation
REFERENCES: Sponseller PD: Skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 269-270.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 689-691.
Question 78
A 20-year-old man sustained an isolated displaced type II odontoid fracture in a motor vehicle accident. He is neurologically intact. Treatment consists of placement in halo traction, and the fracture is reduced. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 193.
Kiovikko MP, Kiuru MJ, Koskinen SK, et al: Factors associated with nonunion in conservatively-treated type-II fractures of the odontoid process. J Bone Joint Surg Br 2004;86:1146-1151.
Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, p 1091.
Fiore AJ, Haid RW, Rodts GE, et al: Atlantal lateral mass screws for posterior spinal reconstruction: Technical note and case series. Neurosurg Focus 2002;12:E5.
Question 79
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of
Explanation
REFERENCES: Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Myerson M, Quill GE Jr: Late complications of fractures of the calcaneus. J Bone Joint Surg Am 1993;75:331.
Question 80
Following resection of malignant tumors, complications related to endoprosthetic reconstruction are most common in what anatomic location?
Explanation
REFERENCE: Horowitz SM, Glasser DB, Lane JM, Healey JH: Prosthetic and extremity survivorship after limb salvage for sarcoma: How long do the reconstructions last? Clin Orthop 1993;293:280-286.
Question 81
With respect to the structure identified by the arrow in Figure 22b, the meniscofemoral 25 ligaments are
Explanation
The stress radiographs demonstrate posterior instability of the right knee in flexion. The MR images demonstrate injury to both the anterior and posterior cruciate ligament (PCL), with the stump identified with the arrow on the MR image (Figure 22b). The PCL has 2 functional bands. The anterolateral bundle originates from the roof of the intercondylar notch. It runs in a posterolateral direction onto the tibial crest between the posterior attachment of the medial and lateral menisci. During a double-bundled posterior ligament reconstruction, the
anterolateral bundle is tensioned with the knee in a position of mid flexion. The posteromedial bundle has a variable pattern of tension both in extension and in high flexion. Tensioning of the posteromedial bundle in extension may contribute to resistance against knee hyperextension.
The meniscofemoral ligaments are variably present. Although 93% of knees have been reported to have at least 1 meniscofemoral ligament present, both ligaments are simultaneously present in approximately 50% of knees. The ligament of Humphrey (anterior meniscofemoral ligament) and ligament of Wrisberg (posterior meniscofemoral ligament) are delineated by their anatomic relationship to the posterior cruciate.
RECOMMENDED READINGS
Amis AA, Bull AM, Gupte CM, Hijazi I, Race A, Robinson JR. Biomechanics of the PCL and related structures: posterolateral, posteromedial and meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2003 Sep;11(5):271-81. Epub 2003 Sep 5. Review. PubMed PMID: 12961064.View Abstract at PubMed
Amis AA, Gupte CM, Bull AM, Edwards A. Anatomy of the posterior cruciate ligament and the meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):257-63. Epub 2005 Oct 14. Review. PubMed PMID: 16228178.
View Abstract at PubMed . 26
Question 82
Spontaneous rupture of the extensor pollicis longus tendon is most frequently associated with which of the following scenarios?

Explanation
clinically satisfactory.
The referenced article by Gelb is a review of the etiology and treatment of this injury. He reviews the above discussion and findings.
Question 83
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
REFERENCES: Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JS (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 84
A 56-year-old man has had a 2-year history of slowly progressive neck pain and bilateral arm aching. Over the past year, he has noticed intermittent, diffuse numbness in both hands, with decreased grip strength and mild hand clumsiness. He denies any problems with balance. Examination shows a wide-based gait, intrinsic wasting, and a postive Hoffman's sign bilaterally. An MRI scan of the cervical spine is shown in Figure 16. What is the most appropriate treatment? Review Topic

Explanation
Question 85
Performance parameters developed by the Centers for Medicare and Medicaid Services and the Centers for Disease Control and Prevention regarding prophylactic antibiotics include
Explanation
Question 86
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function? Review Topic
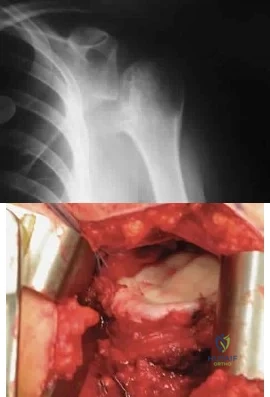
Explanation
Question 87
A 58-year-old woman with rheumatoid arthritis and a severe hindfoot valgus deformity now reports recurrent lateral ankle pain. Examination reveals pain over the fibula and sinus tarsi, with a valgus hindfoot that is passively correctable. Despite the use of an ankle-foot orthosis, this is the second time this problem has occurred. Radiographs and a clinical photograph are shown in Figures 28a through 28c. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Stephens HM, Walling AK, Solmen JD, Tankson CJ: Subtalar repositional arthrodesis for adult acquired flatfoot. Clin Orthop 1999;365:69-73
Easley ME, Trnka HJ, Schon LC, Myerson MS: Isolated subtalar arthrodesis. J Bone Joint Surg Am 2000;82:613-624.
Question 88
- While under a physician’s care, a 45-year-old man verbally abuses the staff and nurses who are attempting to carry out orders. A decision to discharge the patient is best carried out by
Explanation
Question 89
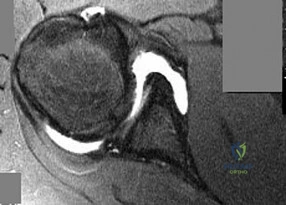
A 22-year-old ballet dancer undergoes hip arthroscopy for increasing hip pain and popping with activity. She experiences complete resolution of signs and symptoms post-operatively. Her pre- and post-operative magnetic resonance sagittal images shown in Figure A (left, pre-operative; right, post-operative). Which of the following pre-operative physical examination findings may have been positive? Review Topic
Explanation
Snapping hip exists in 3 forms: (1) external snapping hip, which is caused by the iliotibial band (ITB) sliding over the greater trochanter, (2) internal snapping hip, and
(3) intraarticular snapping hip, which is caused by loose bodies (traumatic, or from synovial chondromatoses) or labral tears. While painless snapping hip requires no treatment, painful snapping hip may be addressed with activity modification, physical therapy, steroid injections. Surgical release (ITB z-plasty or psoas tenotomy) is indicated if nonoperative management is unsuccessful.
Ilizaliturri et al. evaluated the results of endoscopic iliopsoas tendon release at the lesser trochanter (10 patients) vs endoscopic transcapsular psoas release from the peripheral compartment (9 patients). There were improvements in WOMAC scores in both groups, and no difference between groups. They conclude that both techniques are equally effective.
Marquez Arabia et al. evaluated if the psoas tendon regenerates after tenotomy in 27 patients. At 23 months, they found that tendon regeneration occurred in all patients, to
a mean circumference of 84% of the original. One patient had persistent pain, but all had 5/5 hip flexion strength. They hypothesize that the bulk of iliopsoas muscle fibers attaches directly to the proximal femoral shaft without a tendon, preventing retraction and allowing regeneration to occur easily.
Figure A shows pre- and post-operative arthroscopic psoas tenotomy magnetic resonance sagittal images. Illustration A shows the psoas tendon (white arrows) prior to transection. Illustration B shows the psoas tendon after transection (green arrows, proximal tendon segment; yellow arrows, distal segment). Illustration C and D are diagrams showing release at the level of the lesser trochanter and hip joint respectively.
Incorrect
90 degrees, but full external rotation. Answer 2: Decreased internal rotation and a positive impingement test (forced
flexion, adduction, femoroacetabular Answer 4: These
and internal
rotation) are classic findings
findings may
be found with intra-articular
for cam-type impingement loose bodies.
Question 90
What is the most likely consequence of a vertebral compression fracture associated with osteoporosis?
Explanation
REFERENCES: Heaney RP: The natural history of vertebral osteoporosis: Is low bone mass an epiphenomenon? Bone 1992;13:S23-S26.
Tohmeh AG, Mathias JM, Fenton DC, et al: Biomechanical efficacy of unipedicular versus bipedicular vertebroplasty for the management of osteoporotic compression fractures. Spine 1999;24:1772-1776.
Question 91
Figures 25a and 25b show the radiographs of a 66-year-old man who has had a long history of bilateral painful flatfoot deformities. Examination reveals that his foot is partially correctable passively, albeit with discomfort, and he has an Achilles tendon contracture. An ankle-foot orthosis has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004,
pp 115-120.
Walling AK: Symposium: Adult acquired flatfoot. Clin Orthop 1999;365:2-99.
Question 92
Figure 1 shows the clinical photograph obtained from a child with a congenital difference of the hand. What clinical feature(s) is/are characteristic of this condition?

Explanation
The clinical photograph reveals a child with amniotic band syndrome or constriction band syndrome. If a band causes an autofusion of the digits without amputation, acrosyndactyly can occur, as demonstrated in the clinical photograph. Typically, a proximal sinus tract with a distal syndactyly is present. Radial deviation of the thumb can be seen most frequently in Apert syndrome. Cardiac anomalies are associated with many congenital upper extremity differences but are not characteristic of amniotic band syndrome. Ulnar longitudinal deficiency is characterized by hypoplasia or complete absence of the ulna.
Question 93
A 38-year-old man who is an avid tennis player has had persistent pain over the medial aspect of his knee for the past 6 years. He notes that the pain occurs on a daily basis with any significant activity. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 22a and 22b. What is the best course of action?
Explanation
REFERENCES: Nagel A, Insall JN, Scuderi GR: Proximal tibial osteotomy: A subjective outcome study. J Bone Joint Surg Am 1996;78:1353-1358.
Rinonapoli E, Mancini GB, Corvaglia A, et al: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Manifold SG, Kelly MA, Richardson L, et al: Osteotomies about the knee, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 947-961.
Question 94
Figure 50 shows the AP radiograph of an asymptomatic 82-year-old woman who underwent total hip arthroplasty 16 years ago. What is the most likely diagnosis?
Explanation
with polyethylene wear.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 440.
Dowd JE, Sychterz CJ, Young AM, et al: Characterization of long-term femoral-head-penetration rates: Association with and prediction of osteolysis. J Bone Joint Surg Am 2000;82:1102-1107.
Question 95
A 3-year old child from an isolated mountain area is evaluated for multiple medical problems, including vomiting, loss of appetite, polyuria, and failure to thrive. History reveals the child was normal at birth. The parents, who appear healthy, are second cousins and have two other children who are normal. The parents state that they know of another family member who died at age 6 years after a similar medical history. Radiographs of the lower extremities show bowing of the long bones with cupping and widening of the physes. What is the most likely diagnosis?
Explanation
hemolytic anemia, rhabdomyolysis, and hepatocellular injury that began during refeeding and resolved with treatment. The signs and symptoms, pathophysiology, and treatment of refeeding hypophosphatemia are reviewed.
Renal Osteodystrophy-Musculoskeletal complications in patients with chronic renal failure are common and may be related to the disease itself or to treatment. The altered metabolism in patients with chronic renal failure leads to renal osteodystrophy, which consists of osteomalacia and secondary hyperparathyroidism [1]. Erosive changes attributable to secondary hyperparathyroidism may be easily confused with rheumatoid arthritis, seronegative spondyloarthropathies, infection, or even malignancy.
Primary Hyperparathyroidism-Preferential involvement of cortical bone with apparent preservation of cancellous bone in primary hyperparathyroidism was confirmed by percutaneous bone biopsy. Over 80% of patients had a mean cortical width below the expected mean, whereas cancellous bone volume in over 80% of patients was above the expected mean.
Skeletal disease in primary hyperparathyroidism J Bone Miner Res 1989 Jun; 4(3):283-91
Nutritional vitamin D deficiency-Rickets, osteomalacia, and renal osteodystrophy are disorders of the mineralization of bone that result from a lack of available calcium, phosphorus, or both. The diseases that result from numerous mechanisms present with a symptom-sign-radiographic complex with such a high degree of stereotypy that laboratory investigation is often required to distinguish one form from another. The disorders in children, known as rickets, produce bowing and other deformities of the long bones and dwarfism. These disorders are principally related to the profound effect of the deficiency states on the epiphyseal plate; whereas the same disorders in adults produce an often severe osteopenia and pathologic fractures. Because of newer developments in our understanding of the factors affecting calcium-phosphorus
hemostasis and vitamin D metabolism, many of the children and Rickets, osteomalacia, and renal osteodystrophy.
Question 96
A 7-year-old boy is seen in the emergency department with an isolated and displaced supracondylar humerus fracture and absent radial and ulnar pulses. Despite a moderately painful attempt at realignment, examination reveals that his hand remains pulseless. What is the next most appropriate step in management?
Explanation
REFERENCES: Ay S, Akinci M, Kamiloglu S, et al: Open reduction of displaced pediatric supracondylar humeral fractures through the anterior cubital approach. J Pediatr Orthop 2005;25:149-153.
Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Dormans JP, Squillante R, Sharf H: Acute neurovascular complications with supracondylar humerus fractures in children. J Hand Surg Am 1995;20:1-4.
Question 97
Figure 1 is the right hand of a 65-year-old man with a history of hypertension and rheumatoid arthritis. He is taking immunosuppressive disease-modifying antirheumatic drugs (DMARDs) and is seen in the emergency department with rapid progression of erythema from his right thumb to his right arm during the last 12 hours. He is confused, lethargic, and has these vital signs: blood pressure 92/40, respiratory rate 45, temperature 39.7°C, pulse 135, and oxygen saturation 90% on 4 liters of oxygen by face mask. An examination of his right upper extremity reveals black bulla extending from the metacarpophalangeal down to the tip and no capillary refill at the pulp. Immediate treatment should consist of

Explanation
This patient has multiple criteria for necrotizing soft-tissue infection (NSTI, also known as necrotizing fasciitis) including rapidly progressive infection, black bulla, hypotension and hypoxia, and a history of immune compromise. Aggressive emergent debridement including the removal of all necrotic tissue and IV antibiotics can decrease morbidity and mortality. Not all patients will have such obvious NSTI findings. In less clear cases, a scoring system using laboratory values (the Laboratory Risk Indicator for Necrotizing Fasciitis) can help clarify the diagnosis. IV antibiotics are key to treatment as well, but any delay in surgical treatment can increase morbidity and mortality. The black bulla and necrotic-appearing thumb indicate that this infection is not confined to the flexor sheath, therefore irrigation of the tendon sheath alone would be insufficient treatment. Although the thumb is dysvascular, this is because of an infection, and revascularization is not indicated.
Question 98
Which factor is a contraindication to surgical treatment of a symptomatic CAM deformity?
Explanation
Multiple studies have confirmed that CAM or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, CAM deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion was higher than 50% in the subgroup of athletes.
Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in the majority of nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between CAM deformity and hip osteoarthritis, a corresponding link between correction of the deformity and prevention of osteoarthritis has never been proven.
Results of CAM deformity correction, typically including repair of the degenerative labral tear, are much poorer when there is significant joint space loss. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
Question 99
If the quality of the tendon is poor at the lateral attachment of a partial articular side rotator cuff tear (more than 6 mm of footprint exposure or greater than 50% thickness), what should the surgeon do? Review Topic
Explanation
Question 100
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
Explanation
REFERENCES: Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273.
Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Kim WY, Hearn TC, Seleem O, et al: Effect of pin location on stability of pelvic external fixation. Clin Orthop Relat Res 1999;361:237-244.
