OITE & ABOS Orthopedic Exam MCQs: Spine, Arthroplasty & Fracture Part 102

Key Takeaway
This page offers Part 102 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review. It features 50 high-yield MCQs designed for orthopedic residents and surgeons preparing for board certification. Utilize interactive Study or Exam modes to enhance your knowledge and readiness for exams.
OITE & ABOS Orthopedic Exam MCQs: Spine, Arthroplasty & Fracture Part 102
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 14-year-old gymnast presents with progressive lower back pain and is diagnosed with an L5-S1 isthmic spondylolisthesis. Which of the following statements regarding her spino-pelvic parameters is most accurate concerning the etiology of her condition?
Explanation
Question 2
During a primary total knee arthroplasty for osteoarthritis, trial components are placed. Examination reveals that the knee is perfectly balanced in full extension but is significantly tight in 90 degrees of flexion. Which of the following is the most appropriate step to balance the knee?
Explanation
Question 3
A 35-year-old male is involved in a motorcycle accident. Radiographs reveal an anteroposterior compression (APC) type II pelvic ring injury. Which of the following posterior pelvic ligamentous structures is characteristically disrupted in this specific injury pattern?
Explanation
Question 4
A 45-year-old man presents with right arm pain radiating to his thumb. Examination reveals weakness in wrist extension and an absent brachioradialis reflex. A clinical image representing his pathology is shown. Which of the following cervical nerve roots is most likely compressed?

Explanation
Question 5
A 55-year-old highly active male underwent a primary total hip arthroplasty 2 years ago using a ceramic-on-ceramic bearing. He is very satisfied with his pain relief but complains of an audible 'squeaking' noise from the hip when rising from a chair. Which of the following factors is most strongly associated with this complication?
Explanation
Question 6
A 28-year-old man sustains a displaced, vertically oriented (Pauwels Type III) femoral neck fracture. Which of the following fixation constructs is shown biomechanically to provide the greatest stability against the high shear forces in this fracture pattern?
Explanation
Question 7
A 22-year-old male sustains a traumatic cervical spine injury. On examination 48 hours later, he has motor function graded as 3/5 or higher in more than half of the key muscles below the neurological level of injury. He has intact light touch and pinprick sensation in the sacral segments (S4-S5). Based on the ASIA (American Spinal Injury Association) Impairment Scale, how is this injury classified?
Explanation
Question 8
A surgeon utilizes the direct anterior approach for a total hip arthroplasty. To safely access the hip joint, an internervous plane is developed superficially. Which two nerves supply the muscles that form the boundaries of this superficial surgical interval?
Explanation
Question 9
A 62-year-old woman presents with sudden inability to actively flex the interphalangeal joint of her right thumb 8 months after undergoing open reduction and internal fixation of a distal radius fracture with a volar locking plate. What is the most likely cause of her current presentation?
Explanation
Question 10
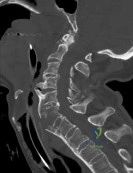
An 82-year-old male with severe COPD, coronary artery disease, and prior myocardial infarction falls and sustains a Type II odontoid fracture with 2 mm of posterior displacement. He is neurologically intact. A representative image is shown. Which of the following is the most appropriate treatment to minimize mortality while managing this fracture?

Explanation
Question 11
A 60-year-old woman with a history of a metal-on-metal total hip arthroplasty performed 8 years ago presents with new-onset groin pain and a palpable anterior thigh mass. Inflammatory markers are normal. MRI demonstrates a thick-walled cystic mass communicating with the joint. What is the classic histopathological finding associated with this condition?
Explanation
Question 12
A 42-year-old male twists his ankle. Radiographs show a transverse fracture of the medial malleolus and a vertical fracture of the lateral malleolus extending proximally from the joint line. A representative radiograph is shown. According to the Lauge-Hansen classification, what was the position of the foot and the deforming force at the time of injury?
Explanation
Question 13
A 68-year-old male complains of bilateral leg and buttock pain that worsens with prolonged standing and walking. His symptoms improve when he leans forward over a shopping cart. Examination reveals normal lower extremity pulses. Which of the following characteristics most reliably differentiates his neurogenic claudication from vascular claudication?
Explanation
Question 14
A 65-year-old male presents with a painful total knee arthroplasty 3 years postoperatively. His serum ESR is 45 mm/hr and CRP is 18 mg/L. Joint aspiration yields a white blood cell count of 4,500 cells/µL with 75% PMNs. Which of the following synovial fluid biomarkers currently offers the highest specificity for confirming a periprosthetic joint infection in this patient?
Explanation
Question 15
A 28-year-old comatose male is admitted to the ICU following a motor vehicle accident resulting in a closed tibia fracture. His blood pressure is 100/60 mmHg. Intracompartmental pressure monitoring of the anterior compartment of the injured leg reads 35 mmHg. What is the most appropriate next step in management?
Explanation
Question 16
A 65-year-old man with type 2 diabetes presents with neck stiffness and mild dysphagia. Radiographs demonstrate flowing ossification along the anterolateral aspect of four contiguous vertebral bodies in the cervical spine. The intervertebral disc spaces are preserved, and the sacroiliac joints are normal. A representative image is shown. What is the most likely diagnosis?

Explanation
Question 17
A 72-year-old female sustains a posterior dislocation of her total hip arthroplasty 4 weeks postoperatively. The surgery was performed via a posterior approach. After successful closed reduction, what is the most appropriate bracing strategy to prevent a recurrent posterior dislocation?
Explanation
Question 18
A 45-year-old pedestrian is struck by a car. Radiographs and CT reveal a depressed fracture of the lateral tibial plateau accompanied by a transverse fracture line separating the condyles from the tibial shaft (metaphyseal-diaphyseal dissociation). A representative image is shown. According to the Schatzker classification, what type of fracture is this?
Explanation
Question 19
A 35-year-old female falls from a horse and sustains a T12 burst fracture. On CT, there is 40% canal compromise, but the posterior ligamentous complex (PLC) is intact. She has 5/5 strength in all lower extremity myotomes, normal sensation, and intact bowel/bladder function. What is her Thoracolumbar Injury Classification and Severity (TLICS) score, and what is the recommended treatment based on this score?
Explanation
Question 20
A 68-year-old male undergoes a primary total knee arthroplasty for severe valgus osteoarthritis (25 degrees of valgus deformity). In the recovery room, he is noted to have a foot drop and decreased sensation over the dorsum of his foot. What is the most appropriate initial management for this complication?
Explanation
Question 21
A 35-year-old male is brought to the trauma bay after a high-speed motor vehicle collision. He is intubated and sedated. A lateral cervical spine radiograph shows a Basion-Dens Interval (BDI) of 14 mm and Basion-Axial Interval (BAI) of 15 mm. What is the most appropriate definitive management?
Explanation
Question 22
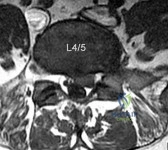
A 45-year-old male presents with severe right anterior thigh pain and weakness in knee extension. An MRI of the lumbar spine reveals a far-lateral (extraforaminal) disc herniation at the L3-L4 level. Which nerve root is most likely compressed by this specific pathology?
Explanation
Question 23
A patient sustains a sacral fracture with a vertical fracture line passing directly through the neural foramina. According to the Denis classification, what zone is this fracture, and what is the approximate risk of neurologic injury?
Explanation
Question 24
A 68-year-old male presents with bilateral hand clumsiness, difficulty walking, and intermittent neurogenic claudication of the lower extremities. Physical exam shows hyperreflexia in the lower extremities, a positive Hoffman sign, and diminished reflexes in the upper extremities. An MRI demonstrates severe cervical stenosis at C4-C6 with cord signal change, as well as severe lumbar stenosis at L3-L5. When planning surgical intervention, what is the generally recommended approach?
Explanation
Question 25
A 72-year-old female presents with a loose right total hip arthroplasty. Radiographs demonstrate superior migration of the acetabular component by 3.5 cm, with massive osteolysis extending medial to the Kohler line and complete destruction of the inferior aspect of the teardrop. This acetabular defect is best classified as:
Explanation
Question 26
During a primary total knee arthroplasty, the surgeon performs a trial reduction and notes lateral patellar subluxation during flexion without the tourniquet inflated. Which of the following technical errors could most likely contribute to this finding?
Explanation
Question 27
A 68-year-old male presents with a painful total knee arthroplasty 6 weeks after index surgery. Aspiration reveals synovial WBC of 45,000 cells/µL with 92% PMNs. Cultures grow methicillin-sensitive Staphylococcus aureus. Radiographs confirm a loose tibial component with a wide radiolucent line. Which of the following is an absolute contraindication to Debridement, Antibiotics, and Implant Retention (DAIR)?
Explanation
Question 28
A 58-year-old male presents with severe groin pain 6 years after an uncomplicated primary THA using a cobalt-chrome head on a titanium stem with a highly cross-linked polyethylene liner. His serum cobalt level is 8 ppb and chromium is 1 ppb. MRI with MARS reveals a large cystic mass communicating with the joint space. What is the most likely diagnosis?
Explanation
Question 29
A 45-year-old male sustains an acetabular fracture in a motor vehicle collision.
Representative radiographs demonstrate disruption of both the anterior and posterior columns. A 'spur sign' is clearly visible on the obturator oblique view. Which of the following is the most likely diagnosis?
Explanation
Question 30
A 35-year-old female sustains a complex bicondylar tibial plateau fracture. The CT scan reveals a large posteromedial shear fragment extending to the joint line. Which of the following surgical approaches provides the most direct and optimal access for anti-glide or buttress plating of this specific fragment?
Explanation
Question 31
A 25-year-old male sustains a vertically oriented (Pauwels type III) femoral neck fracture. Which of the following fixation constructs provides the greatest biomechanical stability for this high-shear fracture pattern?
Explanation
Question 32
A 40-year-old male sustains a high-energy closed tibial pilon fracture, as demonstrated in the representative clinical image showing severe soft tissue swelling and clear fracture blisters. What is the most appropriate initial management?
Explanation
Question 33
A 30-year-old male sustains a C1 burst (Jefferson) fracture. An open-mouth odontoid radiograph demonstrates lateral displacement of the C1 lateral masses. According to the Rule of Spence, what total combined overhang of the C1 lateral masses on the C2 articular facets suggests a rupture of the transverse atlantal ligament (TAL)?
Explanation
Question 34
A 14-year-old gymnast presents with chronic low back pain. Radiographs (representative example shown below) demonstrate a Grade II isthmic spondylolisthesis at L5-S1.
Despite 6 months of nonoperative management, her pain persists and she has developed bilateral L5 radiculopathy. What is the most appropriate surgical treatment?
Explanation
Question 35
A 55-year-old male with medial compartment osteoarthritis of the knee is being evaluated for a unicompartmental knee arthroplasty (UKA). Which of the following is historically and contemporarily considered an absolute contraindication to a medial UKA?
Explanation
Question 36
During a complex revision total hip arthroplasty to extract a well-fixed, fully porous-coated cylindrical femoral stem, the surgeon decides to perform an extended trochanteric osteotomy (ETO). The osteotomy is correctly performed by:
Explanation
Question 37
A 28-year-old male sustains a Gustilo-Anderson Type IIIB open fracture of the distal third of the tibial shaft. After thorough debridement and skeletal stabilization, a 6 cm x 4 cm soft tissue defect with exposed bone devoid of periosteum remains. Which of the following soft tissue coverage options is most appropriate?
Explanation
Question 38
A 65-year-old female sustains a dorsally displaced distal radius fracture (Colles type). A volar approach (modified Henry) is planned for open reduction and internal fixation. During the approach, the interval is developed between the flexor carpi radialis (FCR) and the radial artery. Which muscle must be incised and elevated from the radius to expose the fracture site?
Explanation
Question 39
A 55-year-old male presents with worsening gait instability and fine motor dysfunction in his hands. MRI of the cervical spine demonstrates severe central canal stenosis at C4-C5 with T2-weighted hyperintensity in the spinal cord. Which of the following MRI findings is associated with the poorest prognosis for neurologic recovery after decompressive surgery?
Explanation
Question 40
A 24-year-old snowboarder sustains a hyperdorsiflexion injury to his ankle. Radiographs show a talar neck fracture with subluxation of the subtalar joint, but the tibiotalar joint remains congruous. According to the Hawkins classification, what type is this fracture, and what is the approximate rate of avascular necrosis (AVN)?
Explanation
Question 41
A 68-year-old female undergoes a primary posterior-stabilized total knee arthroplasty. During trial reduction with the thinnest available polyethylene insert, the knee is found to be symmetrically tight in both full extension and 90 degrees of flexion. What is the most appropriate next step to achieve a balanced gap?
Explanation
Question 42
An 82-year-old male presents to the emergency department after a ground-level fall. Imaging reveals a displaced Anderson D'Alonzo Type II odontoid fracture. His medical history is significant for severe COPD on home oxygen and congestive heart failure. He is neurologically intact. Which of the following is the most appropriate management strategy?
Explanation
Question 43
During an ilioinguinal approach for the open reduction and internal fixation of an anterior pelvic ring fracture, the surgeon encounters brisk arterial bleeding near the superior pubic ramus. Which of the following vascular structures or anastomoses is the most likely source of this bleeding?
Explanation
Question 44
A 55-year-old male is 15 years post-operative from a total hip arthroplasty utilizing a highly cross-linked polyethylene (HXLPE) liner. Which of the following best describes the wear and mechanical characteristics of HXLPE compared to conventional ultra-high-molecular-weight polyethylene?
Explanation
Question 45
A 14-year-old female competitive gymnast presents with progressive low back pain and hamstring tightness. Radiographs demonstrate a grade II L5-S1 isthmic spondylolisthesis. She has failed 6 months of comprehensive nonoperative management including physical therapy and bracing. What is the most appropriate surgical intervention?
Explanation
Question 46
A 35-year-old male sustains a displaced Pauwels type III femoral neck fracture in a motor vehicle collision. He is taken to the operating room for open reduction and internal fixation. Which of the following biomechanical constructs provides the most stable fixation for this specific fracture pattern?
Explanation
Question 47
A 65-year-old female presents with a painful total knee arthroplasty 3 years postoperatively. Synovial fluid analysis reveals a WBC count of 3,500 cells/uL with 75% PMNs. An alpha-defensin test is ordered and returns positive. Which of the following best describes the nature and clinical utility of alpha-defensin in diagnosing periprosthetic joint infection (PJI)?
Explanation
Question 48
A 45-year-old male sustains an L1 burst fracture after falling from a height. Neurological examination reveals normal motor and sensory function in the bilateral lower extremities, and normal rectal tone. CT imaging demonstrates a 40% loss of anterior vertebral body height, 15 degrees of local kyphosis, and 25% spinal canal compromise. MRI confirms that the posterior ligamentous complex (PLC) is completely intact. According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is his total score and the generally recommended management?
Explanation
Question 49
A 42-year-old female presents with acute wrist pain and deformity after a fall on an outstretched hand. Radiographs reveal a highly comminuted, intra-articular fracture of the distal radius with a prominent volar marginal fragment and volar subluxation of the carpus.
Which of the following eponymous terms best describes this fracture pattern, and what is the optimal surgical approach for internal fixation?
Explanation
Question 50
A 58-year-old male presents with isolated medial compartment knee osteoarthritis. He is considering a medial unicompartmental knee arthroplasty (UKA). Which of the following conditions represents an absolute contraindication to proceeding with a UKA?
Explanation
Question 51
A 52-year-old male presents with severe radicular pain radiating down his right arm to his middle finger. Neurological examination reveals weakness in elbow extension and wrist flexion. His triceps reflex is 1+ on the right and 2+ on the left. Biceps and brachioradialis reflexes are symmetric and 2+. He has decreased pinprick sensation over the volar aspect of his middle finger. Compression of which cervical nerve root is most likely responsible for these findings?
Explanation
Question 52
A 34-year-old male cyclist is struck by a motor vehicle and presents to the trauma bay. Radiographs demonstrate a displaced midshaft clavicle fracture and a displaced fracture of the ipsilateral scapular neck, representing a 'floating shoulder' injury. Which of the following represents a generally accepted, strong indication for operative fixation of the clavicle (and potentially the scapula) in this setting?
Explanation
Question 53
A 62-year-old female is 8 years post-operative from a metal-on-metal total hip arthroplasty. She presents with new-onset, progressive anterior groin pain and a palpable soft tissue mass. Serum cobalt and chromium levels are elevated. MRI with MARS sequencing reveals a large periarticular cystic mass. Tissue biopsy of the periarticular soft tissues would most likely reveal which of the following characteristic histologic findings?
Explanation
Question 54
A 40-year-old male presents with bilateral leg sciatica, perineal numbness, and new-onset urinary incontinence. An ultrasound bladder scan reveals a post-void residual of 400 mL. MRI confirms a massive L4-L5 central disc herniation severely compressing the thecal sac.
According to current literature, what is the generally accepted critical time threshold for emergent surgical decompression to optimize the chances of full neurologic recovery?
Explanation
Question 55
A 28-year-old male construction worker falls from a ladder and sustains an intra-articular calcaneus fracture. Radiographs show a decreased Bohler's angle and an increased angle of Gissane. He is scheduled for open reduction and internal fixation. Which of the following surgical approaches provides the most comprehensive exposure of the subtalar joint and the lateral wall of the calcaneus?
Explanation
Question 56
During a total hip arthroplasty via a posterior approach, the surgeon inadvertently utilizes a femoral component with significantly less femoral offset than the patient's native anatomy, though leg lengths are perfectly restored. Postoperatively, the patient experiences recurrent posterior dislocations. Decreasing femoral offset contributes to joint instability primarily through which of the following mechanisms?
Explanation
Question 57
A 55-year-old diabetic male with a history of intravenous drug use presents with severe, localized back pain, low-grade fever, and progressive bilateral lower extremity weakness. MRI reveals a dorsal fluid collection in the epidural space from T8 to T10, causing significant spinal cord compression. What is the most common causative organism for this pathology?
Explanation
Question 58
A 45-year-old female pedestrian is struck by a motor vehicle. Radiographs of her right knee demonstrate a displaced fracture of the medial tibial plateau with extension into the metaphysis. The lateral tibial plateau is completely intact.
How is this fracture classified according to the Schatzker classification system?
Explanation
Question 59
A 68-year-old female presents with a painful 'catching' or 'popping' sensation in her knee 14 months after undergoing a posterior-stabilized total knee arthroplasty. She notes the catching occurs consistently as she extends her knee from a flexed position, typically around 30 to 45 degrees of flexion. Which of the following is the underlying pathophysiology of this specific phenomenon?
Explanation
Question 60
A 70-year-old male presents with deteriorating handwriting, difficulty buttoning his shirts, and a progressive, unsteady, broad-based gait. On physical examination, the examiner supports the patient's hand and sharply flicks the volar aspect of the distal phalanx of the patient's middle finger. This maneuver immediately produces rapid, involuntary flexion of the thumb and index finger. What is the name of this clinical sign, and what neurologic localization does it indicate?
Explanation
Question 61
A 68-year-old female presents with progressive clumsiness in her hands and difficulty walking. Radiographs and MRI demonstrate severe cervical spondylosis from C3 to C6 with a rigid 20-degree cervical kyphosis and cord signal changes. Which of the following is the most appropriate surgical approach?
Explanation
Question 62
A 55-year-old male with a metal-on-polyethylene total hip arthroplasty (modular unipolar femoral head) placed 6 years ago presents with new-onset anterior groin pain. Radiographs show well-fixed components. Serum metal ion testing reveals a Cobalt level of 18 ppb and a Chromium level of 1.2 ppb. What is the most likely etiology of his symptoms?
Explanation
Question 63
A 40-year-old male sustains a Schatzker IV tibial plateau fracture extending into the posteromedial quadrant following a motor vehicle collision. Which of the following best describes the optimal fixation strategy for the posteromedial fragment?
Explanation
Question 64
According to the Spine Patient Outcomes Research Trial (SPORT) data regarding the treatment of degenerative spondylolisthesis with spinal stenosis, which of the following statements is most accurate at 4-year follow-up?
Explanation
Question 65
During a primary total knee arthroplasty, the surgeon places the trial components and notes that the knee is perfectly balanced in 90 degrees of flexion, but is symmetrically tight in full extension. Which of the following is the most appropriate intraoperative adjustment?
Explanation
Question 66
A 32-year-old male sustains a high-energy distal femur fracture. CT imaging reveals a coronal plane intra-articular fracture of the lateral femoral condyle (Hoffa fracture).
What is the biomechanically superior method for independent lag screw fixation of this specific fragment?
Explanation
Question 67
A 72-year-old male falls forward striking his face, causing a hyperextension injury to his neck. On examination, he has motor strength of 2/5 in his bilateral upper extremities and 4/5 in his bilateral lower extremities. What is his most likely diagnosis and overall prognosis for ambulation?
Explanation
Question 68
A 60-year-old male presents with a third episode of posterior dislocation following a primary total hip arthroplasty performed via a posterior approach. Which of the following component positions is the most likely culprit contributing to his recurrent posterior instability?
Explanation
Question 69
A 45-year-old female sustains a lateral compression type II (LC-II) pelvic ring injury, which includes a crescent fracture of the posterior ilium. The stability of the remaining posterior sacroiliac complex hinges on which intact ligamentous structure?
Explanation
Question 70
A 12-year-old premenarcheal female presents with a right thoracic curve of 32 degrees.
Radiographs show open triradiate cartilages and a Risser stage of 0. What is the most appropriate management based on the Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST)?
Explanation
Question 71
A 68-year-old male is 3 weeks status post primary total knee arthroplasty. He presents with acute onset of severe knee pain, erythema, and a large effusion. Joint aspiration yields synovial fluid with 65,000 WBC/uL and 95% neutrophils. What is the most appropriate surgical management?
Explanation
Question 72
A 25-year-old male sustains a Hawkins type III talar neck fracture following a fall from height. Which of the following accurately describes the pathoanatomy and associated risk of avascular necrosis (AVN) for this fracture pattern?
Explanation
Question 73
An 84-year-old male with multiple medical comorbidities sustains a Type II odontoid fracture after a ground-level fall. He is neurologically intact. Which of the following represents the most appropriate initial management strategy with the lowest risk of severe complications or mortality?
Explanation
Question 74
A 58-year-old female presents with isolated medial compartment osteoarthritis of the knee. She is being considered for a unicompartmental knee arthroplasty (UKA). Which of the following is considered an absolute contraindication for a mobile-bearing UKA?
Explanation
Question 75
A 24-year-old male falls on an outstretched hand and sustains a proximal pole scaphoid fracture.
What is the rationale for using a dorsal surgical approach for internal fixation of this specific fracture pattern?
Explanation
Question 76
When evaluating a patient with a spinal metastasis using the Spinal Instability Neoplastic Score (SINS), which of the following clinical or radiographic features contributes the highest point value to the total score?
Explanation
Question 77
A 70-year-old female with severe rotator cuff tear arthropathy undergoes a reverse total shoulder arthroplasty (RTSA). How does this implant design alter the biomechanics of her shoulder to restore active elevation?
Explanation
Question 78
A 35-year-old roofer falls from a ladder and sustains an intra-articular calcaneus fracture.
The Sanders classification is used for surgical planning. This classification is primarily based on the fracture lines seen on which specific imaging view?
Explanation
Question 79
A 50-year-old male with a history of intravenous drug use presents with severe lumbar back pain, fevers, and new-onset bilateral lower extremity weakness that has rapidly progressed over the last 6 hours. MRI reveals a ventral epidural abscess from L3 to L5 causing severe thecal sac compression. What is the most appropriate definitive management?
Explanation
Question 80
A 65-year-old male presents with severe cervical spondylotic myelopathy and a rigid cervical kyphosis. Surgical planning is undertaken for a posterior cervical fusion. To achieve optimal sagittal alignment and minimize adjacent segment disease, which of the following spinopelvic parameters is most critical to restore?
Explanation
Question 81
During a primary total knee arthroplasty, the surgeon notes that the joint is symmetrically tight in full extension but has symmetric laxity in 90 degrees of flexion. Which of the following is the most appropriate intraoperative adjustment?
Explanation
Question 82
A 35-year-old male sustains a comminuted distal femur fracture (OTA/AO 33-C3) with significant articular involvement. During open reduction and internal fixation utilizing a lateral locked plate, the surgeon recognizes a coronal plane fracture of the medial femoral condyle (Hoffa fragment). What is the optimal fixation strategy for this specific fragment?
Explanation
Question 83
A 45-year-old male presents with acute onset weakness in ankle dorsiflexion and numbness over the dorsal web space of his first and second toes. MRI demonstrates a large, extruded disc herniation in the far-lateral (extraforaminal) zone at the L4-L5 level. Which nerve root is most likely compressed?
Explanation
Question 84
A 55-year-old highly active female underwent a right total hip arthroplasty using a ceramic-on-ceramic bearing 3 years ago. She now complains of a high-pitched squeaking noise during gait, particularly when extending her hip. Which of the following component position factors is most strongly associated with this phenomenon?
Explanation
Question 85
A 42-year-old male sustains a high-energy Schatzker type VI tibial plateau fracture. He presents with massive swelling, fracture blisters, and shortening of the limb. A spanning external fixator is applied. When considering the definitive surgical approach, which structure defines the safe interval for a posteromedial approach to the medial plateau?
Explanation
Question 86
A 68-year-old male with long-standing ankylosing spondylitis sustains a low-energy mechanical fall and complains of new-onset severe neck pain without neurologic deficit. Initial plain radiographs of the cervical spine are read as negative. What is the most appropriate next step in management?
Explanation
Question 87
A 70-year-old female undergoes a primary total hip arthroplasty via a posterior approach. Intraoperatively, she is noted to dislocate anteriorly with the hip in extension, external rotation, and adduction. What is the most likely cause of this specific instability pattern?
Explanation
Question 88
A 25-year-old male is brought to the trauma bay after a severe crush injury to the pelvis. AP pelvis radiograph demonstrates widening of the pubic symphysis to 4 cm and disruption of the right sacroiliac joint. Based on the Young-Burgess classification, this anteroposterior compression (APC) III injury involves complete disruption of all the following ligaments EXCEPT:
Explanation
None
