OITE & ABOS Orthopedic Board Prep: Hip, Ankle, Fracture & Arthroplasty MCQs Part 100

Key Takeaway
This page offers Part 100 of a comprehensive orthopedic surgery board review quiz. Authored by Dr. Mohammed Hutaif, it features 100 high-yield MCQs, modeled on OITE and AAOS exams. Designed for orthopedic residents and surgeons, it provides interactive study and exam modes to master critical topics for board certification.
About This Board Review Set
This is Part 100 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 100
This module focuses heavily on: Ankle, Arthroplasty, Fracture, Hip.
Sample Questions from This Set
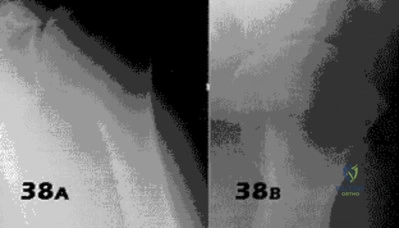
Sample Question 1: A 46-year-old woman had an ankle fracture and ORIF 6 years ago. She had subsequent removal of some of the hardware, but her pain has persisted (Figures 44a and 44b)....
Sample Question 2: The anterior approach to the hip (iliofemoral or Smith-Peterson) puts which of the following anatomic structures at greatest risk?...
Sample Question 3: A 60-year-old woman has activity-related hip pain after undergoing arthroplasty 5 years ago. She has severe Parkinsonism and denies fevers or chills. Radiographs are shown in Figures 45a and 45b. What is the most likely cause of her pain?...
Sample Question 4: What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered?...
Sample Question 5: Figure 12 shows the radiograph of a 55-year-old man who has severe, painful osteoarthritis of the left hip and is scheduled to undergo a left total hip arthroplasty. History reveals that he underwent a right total hip arthroplasty 5 years a...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 46-year-old woman had an ankle fracture and ORIF 6 years ago. She had subsequent removal of some of the hardware, but her pain has persisted (Figures 44a and 44b).

Explanation
Patients younger than 40 years of age who have ankle arthritis pose an ongoing clinical challenge. Nonsurgical treatment should be maximized, although distraction arthroplasty can be used in an effort to delay the need for fusion.
One of the strongest indications for ankle arthroplasty is a preexisting hindfoot fusion with a goal to retain some ankle/hindfoot motion. Ankle fusion is perhaps the most predictable surgical treatment for a relatively young, active patient with ankle arthritis. Moreover, there are concerns regarding implant loosening when performing TAA in active patients.
Outcome after syndesmosis ORIF has been linked to the quality of the reduction at the index procedure. Syndesmotic malreduction that is severe necessitates osteotomy and revision ORIF.
RECOMMENDED READINGS
Sagi HC, Shah AR, Sanders RW. The functional consequence of syndesmotic joint malreduction at a minimum 2-year follow-up. J Orthop Trauma. 2012 Jul;26(7):439-43. doi: 10.1097/BOT.0b013e31822a526a. PubMed PMID: 22357084. View Abstract at PubMed
Smith NC, Beaman D, Rozbruch SR, Glazebrook MA. Evidence-based indications for distraction ankle arthroplasty. Foot Ankle Int. 2012 Aug;33(8):632-6. Review. View Abstract at PubMed
Kim BS, Knupp M, Zwicky L, Lee JW, Hintermann B. Total ankle replacement in association with hindfoot fusion: Outcome and complications. J Bone Joint Surg Br. 2010 Nov;92(11):1540-7. doi: 10.1302/0301-620X.92B11.24452. PubMed PMID: 21037349. View Abstract at PubMed
Daniels TR, Younger AS, Penner M, Wing K, Dryden PJ, Wong H, Glazebrook M. Intermediate-term results of total ankle replacement and ankle arthrodesis: a COFAS multicenter study. J Bone Joint Surg Am. 2014 Jan 15;96(2):135-42. doi: 10.2106/JBJS.L.01597. View Abstract at PubMed
Question 2
The anterior approach to the hip (iliofemoral or Smith-Peterson) puts which of the following anatomic structures at greatest risk?
Explanation
Brachial plexopathy following shoulder taping and application of countertraction
Brachial plexopathy on neck extension for surgical access
Spinal cord injury on neck extension for surgical access
Ulnar neuropathy due to tightly wrapped or malpositioned upper extremities
Cerebral hypoperfusion due to elevation of the head of the bed PREFERRED RESPONSE 1
(SBQ12TR.83) A 45-year-old male sustains the fracture seen in Figure A. He is scheduled for open reduction and internal fixation using the Smith-Peterson approach. After dissection through the superficial intermuscular plane, a moderate amount of bleeding is noted in the surgical field. What vessel was likely injured?

Ascending branch of the lateral femoral circumflex artery
Medial femoral circumflex artery
Obturator artery
Superficial external pudendal artery
Femoral vein
Question 3
A 60-year-old woman has activity-related hip pain after undergoing arthroplasty 5 years ago. She has severe Parkinsonism and denies fevers or chills. Radiographs are shown in Figures 45a and 45b. What is the most likely cause of her pain?
Explanation
REFERENCES: Harris WH, McCarthy JC, O’Neill DA: Femoral component loosening using contemporary techniques of femoral cement fixation. J Bone Joint Surg Am 1982;64:1063-1067.
Callaghan JJ, Rosenberg AG, Rubash H (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 960, 1228-1229.
Maloney WJ, Schmalzreid T, Harris WH: Analysis of long-term cemented total hip arthroplasty retrievals. Clin Orthop Relat Res 2002;405:70-78.
Question 4
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered?
Explanation
REFERENCES: Ludwig S, Zarro CM: Complications encountered in the management of patients with ankylosing spondylitis, in Vaccaro AR, Regan JJ, Crawford AH, et al (eds): Complications of Pediatric and Adult Spine Surgery. New York, NY, Marcel Dekker, 2004,
pp 279-290.
Wu CT, Lee ST: Spinal epidural hematoma and ankylosing spondylitis: Case report and review of the literature. J Trauma 1998;44:558-561.
Question 5
Figure 12 shows the radiograph of a 55-year-old man who has severe, painful osteoarthritis of the left hip and is scheduled to undergo a left total hip arthroplasty. History reveals that he underwent a right total hip arthroplasty 5 years ago that remains pain-free. Based on the preoperative radiograph, the patient is at greatest risk for what complication?
Explanation
REFERENCE: Ranawat CS, Rodriguez JA: Functional leg-length inequality following total hip arthroplasty. J Arthroplasty 1997;12:359-364.
Question 6
An 81-year-old man with severe low back pain reports right extensor hallucis longus and anterior tibialis weakness and difficulty urinating over the past 24 hours. He has a temperature of 101 degrees F (38.3 degrees C). MRI scans are shown in Figures 31a and 31b. Management should consist of
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Reihsaus E, Waldbaur H, Seeling W: Spinal epidural abscess: A meta-analysis of 915 patients. Neurosurg Rev 2000;23:175-204.
Question 7
- The familial occurrence of Legg-Calve-Perthes disease may, in some cases, be attributed to
Explanation
Question 8
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
Explanation
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.
Question 9
What is the most likely complication after surgical treatment in this scenario?
Explanation
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, and internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through as seen in this patient.
The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The 4 muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the 4 rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation.
This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Brighton sign findings would be negative), a posterior capsular shift with rotator interval closure is indicated. If a patient has excessive glenoid retroversion, a posterior opening-wedge osteotomy is appropriate.
The most common complication seen after arthroscopic posterior labral repair is stiffness, followed by recurrent instability and degenerative joint disease.
Question 10
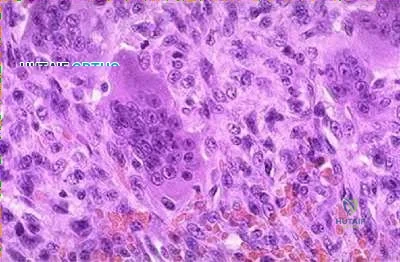
A 19-year-old man has had pain and swelling in his left forearm for the past 8 months. Laboratory studies show a mildly elevated WBC count and erythrocyte sedimentation rate. Radiographs are shown in Figures 58a and 58b, a CT scan is shown in Figure 58c, and T 1 - and T 2 -weighted MRI scans are shown in Figures 58d and 58e, respectively. A biopsy specimen is shown in Figure 58f. Immunohistochemistry demonstrates that the lesion is negative for leukocyte common antigen (CD34). What is the most common cytogenetic translocation associated with this lesion?
Explanation
REFERENCES: Womer R: The cellular biology of bone tumors. Clin Orthop Relat Res 1991;262:12-21.
Yamaguchi U, Hasegawa T, Morimoto Y, et al: A practical approach to the clinical diagnosis of Ewing’s sarcoma/primitive neuroectodermal tumour and other small round cell tumours sharing EWS rearrangement using new fluorescence in situ hybridisation probes for EWSR1 on formalin fixed, paraffin wax embedded tissue. J Clin Pathol 2005;58:1051-1056.
Lazar A, Abruzzo LV, Pollock RE, et al: Molecular diagnosis of sarcomas: Chromosomal translocations in sarcomas. Arch Path Lab Med 2006;130:1199-1207.
Question 11
What is the best surgical approach for the scapular fracture shown in Figure 46?
Explanation
REFERENCES: Kavanagh BF, Bradway JK, Cofield RH: Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-484.
Leung KS, Lam TP: Open reduction and internal fixation of ipsilateral fractures of the scapular neck and clavicle. J Bone Joint Surg Am 1993;75:1015-1018.
Ideberg R: Unusual glenoid fractures: A report on 92 cases. Acta Orthop Scand 1995;66:395-397.
Question 12
A 47-year-old man ruptured his left patellar tendon and twisted his right ankle in a fall. Initial radiographs of the ankle are unremarkable. One week following repair of the left patellar tendon, he reports increased pain with weight bearing in his right ankle. A follow-up radiograph is shown in Figure 38. Management of the ankle injury should consist of
Explanation
REFERENCES: Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Edwards GS Jr, DeLee JC: Ankle diastasis without fracture. Foot Ankle 1984;4:305-312.
Question 13
Figures 82a through 82c show the radiograph and 3-dimensional (3-D) CT scans of a 2-year-old boy whose scoliosis has progressed 15 degrees during the past year. The child is clinically healthy. He has been walking since 11 months of age. An MRI scan of the entire spine revealed no other anomalies. What additional study is indicated? Review Topic
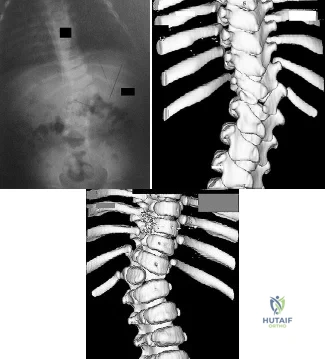
Explanation
Question 14
- A 75-year-old woman who has groin pain states that she had total hip arthroplasty 15 years ago. The radiograph shown in Figure 40 reveals that the left acetabular component is grossly loose. Revision of the acetabular component should include use of a
Explanation
Question 15
A surgeon contemplates performing a hemiarthroplasty (HA) or total hip arthroplasty (THA) for an active, community ambulating 70-year-old female with a displaced femoral neck fracture. Which of the following is true for these options?
Explanation
There are a few differences between THA and HA performed in the setting of displaced FNF. THA has a higher dislocation rate, greater blood loss, requires a larger exposure than HA, and the operation is longer. HA often requires reoperation because of progressive acetabular erosion. Patient outcomes and function are greater following THA than HA.
Florschultz et al. reviewed current management of FNF. They concluded that CRIF / ORIF is indicated for displaced femoral neck fractures in younger individuals, select active elderly, and medically unfit patients. HA is indicated for lower demand ambulatory older patients. THA is indicated for the active elderly and those with preexisting acetabular disease.
Avery et al. reviewed 7-10 year results of an RCT comparing THA with HA. More HA patients had died during follow-up. All surviving patients had polyethylene wear (THA) and acetabular erosion (HA). They concluded that there was lower mortality and a trend towards superior function in patients with a THA in the medium term.
Hedbeck et al. performed a RCT comparing HA and THA. At 4 years, there was improved function and quality of life with THA. They recommend THA in elderly, lucid patients with a displaced FNF.
Incorrect Answers:
Question 16
A 38-year-old woman who tripped and fell on her outstretched arm reports pain with movement. Examination reveals swelling. AP and lateral radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
REFERENCES: Mehdian H, McKee M: Management of proximal and distal humerus fractures. Orthop Clin North Am 2000;31:115-127.
Ring D, Jupiter J, Gulotta L: Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003;85:232-238.
Question 17
Which of the following complications may occur subsequent to resurfacing hip arthroplasty for osteonecrosis of the hip but not after total hip arthroplasty?
Explanation
REFERENCES: Gabriel JL, Trousdale RT: Stem fracture after hemiresurfacing for femoral head osteonecrosis. J Arthroplasty 2003;18:96-99.
Amstutz HC, Campbell PA, Le Duff MJ: Fracture of the neck of the femur after surface arthroplasty of the hip. J Bone Joint Surg Am 2004;86:1874-1877.
Question 18
An 80-year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 19
Which of the following radiographic parameters is most predictive of a poor result following multilevel fusion surgery for adult degenerative scoliosis? Review Topic
Explanation
Question 20
When performing hip arthroscopy, the hip should be placed in neutral to slight internal rotation to protect which of the following structures? Review Topic
Explanation
Question 21
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty?
Explanation
REFERENCES: Visotsky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.
Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
Question 22
Haversian canals are found in the center of an osteon in compact bone. They contain blood vessels and nerves.
Explanation
amputations have several options to optimize ambulation including solid, energy storing, and multi-axial prothesis.
Aaron et al. reviews the important considerations for patient specific prostheses and new developments on the horizon to maximize ambulation in prosthesis users.
Mesenchymal stem cells have the capacity to differentiate into all the following cell types EXCEPT?
Osteoclasts
Chondrocytes
Adipocytes
Osteoblasts
Fibroblasts
Mesenchymal stem cells are multipotent stem cells which retain the ability to self-renew and to form cells of the mesenchymal lineage. They can therefore form muscle, fat, tendon (made from fibroblasts), bone, cartilage, and the marrow stromal cells. Mesenchymal stem cells do not however form osteoclasts, which are formed from the monocyte lineage - from hematopoietic stem cells.
Caterson et al review the use of mesenchymal stem cells in tissue engineering and regeneration of musculoskeletal tissue.
A 60 year-old male was brought into the operating room for total hip replacement. Before making the incision, what precautionary procedure must be performed by the entire staff to minimize surgical error?
Mark the word "No" on the nonoperative extremities
Use intraoperative fluoroscopic imaging
Perform "timeout"
Have blood products ready in the operating room
Use the newest prosthesis
Surgical "timeout" is now part of the standard procedure which must be performed before starting surgery to minimize surgical error such as wrong site surgery.
Which of the following statements regarding articular cartilage is TRUE?
Cartilage is an isotropic material
Most of the water in articular cartilage exists in the deep layer next to the calcified cartilage
Cartilage only heals if the injury does not pass through the tidemark
Calcified cartilage is the only place that type IV collagen is found
Cartilage exhibits stress shielding of the solid matrix components
Cartilage exhibits significant stress shielding of the solid matrix components due to its high water content, the non-compressibility of water, and the structural organization of collagen and proteoglycans. Cartilage is composed of a permeable porous matrix and 65 to 80% of the total weight of articular cartilage is made up of water. A pressure gradient causes the water to flow through the porous-permeable solid matrix. Significant flow of fluid through the solid matrix requires high hydrodynamic pressures because of the low
permeability of the solid matrix.
The other answers are incorrect because cartilage is anisotropic, most of the water is located in the superficial layers, it only heals if the injury does pass through the tidemark, type X collagen is found in calcified cartilage and is thought to be involved in mineralization. Type IV collagen is found in the basal lamina.
A 38-year-old patient presents 6 months after intramedullary nailing of a distal third tibia fracture with symptoms consistent with complex regional pain syndrome. During the early stage of the disease he was treated with intermittent splinting, elevation and massage, contrast baths, and transcutaneous electrical nerve stimulation. Despite these modalities, he continues to have severe and debilitating symptoms. Which of the following treatment options is indicated as a second line of treatment?
Long leg cast immobilization for 3 months
Walking boot with non weight bearing for three months
Exchange nailing to stimulate healing response to the limb
Epidural spinal cord stimulator
Surgical sympathectomy of the affected limb
Complex regional pain syndrome is a chronic progressive disease of unknown etiology characterized by pain, swelling and skin changes. If nonoperative modalities fail, a surgical sympathectomy of the affected limb is indicated.
The first line of treatment is physical therapy including intermittent splinting, elevation and massage, contrast baths, and transcutaneous electrical nerve stimulation. Aggressive passive range-of-motion exercises should be avoided. If nonoperative modalites fail and symptoms remain severe, a surgical sympathectomy of the affected limb is indicated.
Keys to successful treatment include early clinical suspicion and treatment. Late CRPS is highly refractory to treatment and often results in permanent disability.
Two forms of Complex regional pain syndrome exist: 1) Reflex sympathetic dystrophy
- which does not demonstrate nerve lesions, and 2) Causalgia - which is associated with damage to peripheral nerves. Diagnostic criteria include:
Major criteria: intense and prolonged pain, swelling, stiffness, and discoloration (vasomotor disturbances).
Minor criteria: trophic changes, osseous demineralization, temperature changes, and palmar fibromatosis.
Tran et al present their systemic review of 41 RCTs of the research regarding treatment of CRPS. Their data suggest that only bisphosphonates offer clear medicinal benefits in the treatment of CRPS. Evidence regarding a beneficial effect of lumbar sympathetic blocks, gabapentin, and physical therapy is lacking. As such, these authors advocate for further study thru well-designed RCTs to better evaluate appropriate and effective treatment strategies.
You are planning an intramedullary nail to treat a geriatric patient with a peritrochanteric femur fracture. Which of the following preoperative considerations is correct regarding your implant?
The radius of curvature of an intramedullary nail is generally greater than the radius of curvature of the femur
Closed section nails have less stiffness than slotted nails
The medial/lateral nail starting point relative to the greater trochanter does not affect varus/valgus position in the fracture
The bending stiffness of your nail is proportional to the second power of the radius
Intramedullary nails allow for mostly direct intramembranous bone healing
The radius of curvature of an intramedullary nail is generally greater than the radius of curvature of the femur, which is why anterior distal femur
penetration is a known complication of intramedullary nailing procedures.
Egol et al. evaluated the radius of curvature of 948 femurs (474 matched pairs) and compared those data with current intramedullary nails. He found the average femoral anterior radius of curvature was 120 cm (± 36 cm)
whereas the radius of curvature of the intramedullary nails ranged from 186 to 300 cm.
The other answers are incorrect because closed section nails have more stiffness than slotted nails. The starting position on the greater trochanter greatly affects the post- operative varus/valgus of the fracture. Intramedullary nails allow for mostly indirect enchondral bone healing due to relative motion at the fracture site.
All of the following antibiotics function by interfering with protein synthesis by inhibiting ribosomes EXCEPT
gentamicin
tobramycin
vancomycin
erythromycin
linezolid
Gentamicin and tobramycin are aminoglycosides that function by inhibition of bacterial protein synthesis via irreversible binding to ribosomal subunits. Erythromycin functions by binding to the 50s subunit of the bacterial 70s rRNA complex and thereby inhibits protein synthesis. Linezolid binds to the 23s portion of the ribosomal subunit and inhibits protein synthesis. In contrast, Vancomycin acts by inhibiting proper cell wall synthesis and does not inhibit the ribosome.
The bending rigidity of the implant shown in Figure A is proportional to what power of the measured radius of the implant?
Question 23
When a patient has recurrent anterior shoulder instability, a bony glenoid reconstructive procedure should be considered in which clinical setting?
Explanation
in collision athletes.
Question 24
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
REFERENCES: Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 51.
Question 25
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?
Explanation
REFERENCES: Robinson CM, Aderinto J: Posterior shoulder dislocations and
fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Cicak N: Posterior dislocation of the shoulder. J Bone Joint Surg Br 2004;86:324-332.
Question 26
A 47-year-old woman has had medial ankle pain and swelling for the past 3 months. She recalls no specific injury, and casting and nonsteroidal anti-inflammatory drugs have failed to provide relief. Examination reveals a pes planus with heel valgus that is passively correctable. Radiographs show no evidence of arthritis. An MRI scan is shown in Figure 16. What is the most appropriate surgical procedure to alleviate her pain?
Explanation
REFERENCES: Myerson MS, Corrigan J: Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon transfer and calcaneal osteotomy. Orthopedics 1996;19:383-388.
Mosier-LaClair S, Pomeroy G, Manoli A II: Operative treatment of the difficult stage 2 adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:95-119.
Question 27
During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this athlete be managed?
Explanation
hours before being allowed to participate. Also, all lesions must be dry and crusted and at least 120 hours of antiviral therapy should have been instituted.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 301-309.
Johnson R: Herpes Gladiatorium and other skin diseases. Clin Sports Med 2004;23:473-484.
Question 28
..One week after closed reduction of a primary anterior shoulder dislocation, a 25-year-old athlete should be counseled that
Explanation
A 65-year-old man experienced 6 years of worsening shoulder pain. Examination demonstrates stiffness and crepitus with range of motion, but full rotator cuff strength in all planes. Radiographs show advanced shoulder osteoarthritis, and an MRI scan ordered by the patient's primary care physician shows an intact rotator cuff.
Question 29
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
REFERENCES: Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393.
Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Kostuik JP, Valdevit A, Chang HG, et al: Biomechanical testing of the lumbosacral spine. Spine 1998;23:1721-1728.
Question 30
An otherwise healthy 33-year-old man who works in construction reports a 3-month history of knee pain. Radiographs are shown in Figures 9a and 9b. An axial T 1 -weighted MRI scan with contrast, an angiogram, and histologies are shown in Figures 9c through 9f. What is the most likely diagnosis?
Explanation
REFERENCES: Sheth DS, Yasko AW, Raymond AK, et al: Conventional and dedifferentiated parosteal osteosarcoma: Diagnosis, treatment, and outcome. Cancer 1996;78:2136-2145.
Lewis VO, Gebhardt MC, Springfield DS: Parosteal osteosarcoma of the posterior aspect of the distal part of the femur: Oncological and functional results following a new resection technique. J Bone Joint Surg Am 2000;82:1083-1088.
Question 31
In infantile idiopathic scoliosis, which of the following factors suggests progression? Review Topic
Explanation
Question 32
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?
Explanation
REFERENCE: Baxter DE, Pfeffer GB, Thigpen M: Chronic heel pain: Treatment rationale. Orthop Clin North Am 1989;20:563-569.
Question 33
A 55-year-old man has had progressive right shoulder pain for the past 2 years. Examination reveals active elevation to 120 degrees, external rotation to 20 degrees, and internal rotation to the sacrum. AP and axillary radiographs are shown in Figures 23a and 23b. Which of the following procedures would result in the most predictable long-term pain relief?
Explanation
REFERENCES: Cofield RH, Frankle MA, Zuckerman JD: Humeral head replacement for glenohumeral arthritis. Semin Arthroplasty 1995;6:214-221.
Levine WN, Djurasovic M, Glasson JM, Pollock RG, Flatow EL, Bigliani LU: Hemiarthroplasty for glenohumeral osteoarthritis: Results correlated to degree of glenoid wear. J Shoulder Elbow Surg 1997;6:449-454.
Matsen FA III: Early effectiveness of shoulder arthroplasty for patients who have primary glenohumeral degenerative joint disease. J Bone Joint Surg Am 1996;78:260-264.
Question 34
Figure 49 shows a histologic section of the lung in a patient who died during total hip arthroplasty. What unexpected finding is seen in the pulmonary capillaries?
Explanation
23 patients. Fat and marrow embolization during preparation of the femur or cementing of the femoral component was believed to be responsible for the cardiopulmonary collapse that occurred during arthroplasty. Although fat and marrow emboli were found in the pulmonary capillaries of most of the patients on autopsy, this histologic section shows two particles of cement in the pulmonary capillaries.
REFERENCES: Parvizi J, Holiday AD, Ereth MH, et al: The Frank Stinchfield Award. Sudden death during primary hip arthroplasty. Clin Orthop 1999;369:39-48.
Patterson BM, Healy JH, Cornell CN, et al: Cardiac arrest during hip arthroplasty with a cemented long-stem component: A report of seven cases. J Bone Joint Surg Am
1991;73:271-277.
Question 35
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
Explanation
REFERENCES: Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med 2005;33:492-501.
Ford KR, Meyer GD, Hewett TE: Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exer 2003;35:1745-1750.
Question 36
Figure 39 shows the radiograph of a 4-month old infant who has been undergoing weekly casting since birth for a congenital equinovarus deformity. Management should now consist of
Explanation
REFERENCES: Lehman WB, Atar D: Complications in the management of talipes equinovarus, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992,
pp 135-136.
Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002,
pp 927-935.
Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990,
pp 2461-2564.
Question 37
Giant cell tumors of bone can occur in many different areas throughout the body. All of the following are common locations for giant cell tumors of bone EXCEPT?
Explanation
Giant cell tumors are one of the more common tumors in young adults 22-40 years of age. There is much argument as to whether giant cell tumors arise in the metaphysis or the epiphysis, but most authors agree that giant cell tumors are very uncommon in the diaphysis. The most common sites of giant cell tumors in bone, which are the distal radius, sacrum, distal femur, proximal tibia and proximal humerus. Treatment typically involves intralesional curettage with adjuvant treatment (e.g., phenol, hydrogen peroxide, argon beam, etc).
Williams et al undertook a prospective study to evaulate the recurrence rate of giant cell tumors of the hand and they found that soft tissue extension of the tumor significantly increased the rate of local recurrence. This finding is significant because multiple previous studies have demonstrated similar higher recurrence rates for giant cell tumors with soft tissue extension in other areas like around the knee and the distal radius.
Illustration A are radiographs classic for a giant cell tumor showing a large lytic metaphseal-epiphyseal lesion in the distal femur. Illustration B is an axial CT of the distal femur showing the lytic giant cell tumor, abutting and fracturing the subchondral bone. Illustration C is histology classic for a giant cell tumor where the nuclei of the multi-nucleated giant cells look identical to the nuclei of the stromal cells.
Incorrect Answers:


What is the most appropriate treatment for a 65-year-old female with a 100-pack-year tobacco history who presents with a new painful lytic lesion in her femoral diaphysis?
Antegrade femoral nailing with reamings sent to pathology for analysis
Antegrade femoral nailing with adjuvant radiotherapy to the lesion 3
. Minimally invasive plating of the femur for stabilization and open cementation of the lesion
Referral to medical oncology for chemo-radiotherapy
Lesion biopsy with further treatment based on the results of the biopsy
New lesions which are not diagnosed by imaging and require surgical intervention need to have an appropriate biopsy with treatment dictated by the results of the biopsy. While this patient has a significant tobacco history, incorrect treatment of this lytic bone lesion could affect both her overall morbidity and mortality. As an example, a lytic high-grade chondrosarcoma may look exactly like a metastatic lesion but requires wide surgical excision, not just stabilization of an impending pathological fracture. Intramedullary nailing of a chondrosarcoma would spread the tumor the entire length of the bone and likely require a major amputation, not a limb salvage operation.
A 14-year-old child is referred to your office for evaluation of a tibia lesion found incidentally after a minor ankle injury. A radiograph of the child's ankle is shown in Figure A. What treatment do you suggest?

Endocrine consultation secondary to associated endocrine abnormalities
Surgical consultation secondary to associated gastrointestional cancers
Short leg cast and non-weight bearing for a minimum of 6 weeks
Open biopsy and tumor staging
Routine followup of tibial lesion
The radiograph is classic for a non-ossifying fibroma given the classic eccentric position, sclerotic margin, and benign appearance. Other than routine followup for the tibial lesion, this child requires no subsequent treatment. Marks and Bauer review the diagnosis, imaging, and treatment of many different fibrous tumors of bone and review the diagnostic imaging criteria specific to each subclass of bony fibrous tumors.
The chromosomal translocation t(X;18)is found in which of the following conditions?
Myxoid liposarcoma
Synovial Sarcoma
Osteosarcoma
Ewing's Sarcoma
Clear cell sarcoma
Synovial sarcoma is a rare soft tissue sarcoma with biphasic features of both spindle cell and epithelial differentiation. Synovial sarcoma is a rare high-grade tumor that spreads along fascial planes and, thus, can be much more widespread than apparent on initial evaluation. Males are more commonly affected than females with a ratio of 1.1:1. Synovial sarcoma is characterized by a specific chromosomal translocation t(X;18)(p11;q11) that is observed in more than 90% of cases. The t(X;18)(p11;q11) translocation fuses the SYT gene from chromosome 18 to either of 2 homologous genes at Xp11, either SSX1 or SSX2. The fusion proteins SYT-SSX1 and SYT-SSX2 function as aberrant transcriptional regulators, resulting in either activation of protooncogenes or inhibition of tumor suppressor genes.
Kawai et al found that SYT-SSX fusion transcripts are a defining diagnostic marker of synovial sarcomas. These fusion transcripts may yield important independent prognostic information and provide important information for different types of treatment.
Incorrect Answers
Question 38
Which of the following best describes the resultant forces on an increased offset stem when compared with a standard offset stem?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Hurwitz DE, Andriaacchi TP: Biomechanics of the hip, in Callaghan J, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven , 1998.
Pauwels F: Biomechanics of the Normal and Diseased Hip. New York, NY, Springer-Verlag, 1976.
Question 39
A 32-year-old man sustains a pilon fracture which is treated initially with a spanning external fixator, as shown in figure A. He is now 3 weeks from injury and skin swelling has subsided significantly. What is the most appropriate definitive treatment?

Explanation
OrthoCash 2020
Question 40
Which of the following medications may have a negative effect on bone healing following fracture?
Explanation
REFERENCES: Gerstenfeld LC, Thiede M, Seibert K, et al: Differential inhibition of fracture healing by non-selective and cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs. J Orthop Res 2003;21:670-675.
Harder AT, An YH: The mechanisms of the inhibitory effects of nonsteroidal anti-inflammatory drugs on bone healing: A concise review. J Clin Pharmacol 2003;43:807-815.
Question 41
03 A 26-year-old woman has chronic toe pain after hitting a bedpost 3 months ago. A radiograph is shown in Figure 27. Her injury represents an avulsion of the

Explanation
The EDB originates on the distal lateral and superior surface of the calcaneus and inserts on the
lateral aspect of the flexor digitorum longus tendon and also on to the base of the proximal phalanx of the first through fourth toes. There is no EDB tendon to the fifth toe. If an EDB laceration is easily identified at the time of an EDL repair, than it may be repaired as well, otherwise repair of the EDL alone is sufficient.
Heckman JD: Fractures and dislocation of the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds):Rockwood and Green’s Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 2166-2169.
Coughlin MJ: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 787-788.
back to this question next question
Question 42
A 21-year-old throwing athlete has persistent shoulder pain. Figures 73a and 73b are arthroscopic photographs taken from a posterior viewing portal and an anterior viewing portal. During which phase of the throwing motion did the injury most likely occur? Review Topic
Explanation
Rotator cuff tears in throwing athletes may be the result of either tensile or compressive forces. Tensile failure is believed to be the result of repetitive eccentric contractions. Compressive failure is thought to result from direct contact of the articular side of the rotator cuff between the greater tuberosity and posterior glenoid. Compressive failure results in tearing of the posterior supraspinatus and anterior infraspinatus, in contrast to the more common partial tearing of the anterior supraspinatus seen in the general population. In addition to tearing of the articular side of the rotator cuff, compressive forces also contribute to the peel-back mechanism and resultant avulsion of the posterosuperior labrum and biceps anchor. Articular-sided posterior supraspinatus and infraspinatus tears in combination with posterosuperior labral and biceps anchor detachment has been termed internal impingement. It is believed to be the primary result of either posterior capsular contracture (GIRD) or anterior capsular laxity.
Question 43
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
REFERENCES: Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Conn RA, Colfield RH, Byer DE, Lindstromberg JW: Interscalene block anesthesia for shoulder surgery. Clin Orthop 1987;216:94-98.
Question 44
A 65-year-old woman with rheumatoid arthritis is undergoing revision total knee arthroplasty (TKA) during which the medial collateral ligament (MCL) is damaged. Suture anchors are used to attempt primary repair, and a varus-valgus constrained insert also is used. Postsurgically she experiences instability that does not respond to bracing with a 3+ opening to valgus stress (Figure 120). What is the most appropriate surgical option?
Explanation
MCL repair or reconstruction may be considered in younger, more active patients, but this intervention is technically demanding and produces variable results. Rotating-hinge TKA is associated with good results in a number of small series that include cases performed with MCL insufficiency or absence. A rotating hinge is preferable over a fixed hinge because of decreased stresses on implants imposed by fixed-hinge devices.
Question 45
When comparing arthroscopic and open rotator cuff repairs, which of the following tears shows a decreased recurrent tear rate in the open versus the arthroscopic group? Review Topic
Explanation
Question 46
A 23-year-old man has pain and a callus beneath the second metatarsal head. Initial management should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 163-173.
Mizel MS, Yodlowski ML: Disorders of the lesser metatarsophalangeal joints. J Am Acad Orthop Surg 1995;3:166-173.
Question 47
An 8-year-old girl has asymmetry on a forward bend test of the spine. She is asymptomatic and has a normal clinical neurologic examination. Radiographs are shown in Figures 22a and 22b. What should be the next step in her work-up? Review Topic
Explanation
Question 48
Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Coughlin MJ, Mann RA: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby-Year Book, 2000, pp 150-269.
Skalley TC, Myerson MS: The operative treatment of acquired hallux varus. Clin Orthop 1994;306:183-191.
Question 49
A 62-year-old woman reports diffuse aches and pains of the hip and pelvis. She denies any significant trauma but does have a history of chronic anemia. Figure 17a shows a radiograph of the pelvis, and Figures 17b and 17c show T 2 -weighted MRI scans. What is the most likely diagnosis?
Explanation
REFERENCE: Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA,
WB Saunders, 2002, pp 2189-2216.
Question 50
A concern when choosing irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene rather than lower dose–irradiated (4 Mrad) polyethylene is related to its inferior resistance to
Explanation
The higher the dose of radiation to the polyethylene, the higher the amount of cross-linking. Adhesive and abrasive wear resistance increases with an increase in cross-linking. However, fatigue properties of the material are decreased when polyethylene is melted (to remove free radicals) during the cross-linking process. Creep (deformation without wear) is also slightly increased with cross-linking of polyethylene.
Question 51
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Explanation
Question 52
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis? Review Topic
Explanation
Question 53
What is the most common cause of early failure for patellofemoral arthroplasty?
Explanation
REFERENCES: Lonner JH: Patellofemoral arthroplasty. J Am Acad Orthop Surg 2007;15:495-506. Argenson JN, Flecher X, Parratte S, et al: Patellofemoral arthroplasty: An update. Clin Orthop Relat Res 2005;440:50-53.

Question 54
The risk of local recurrence after surgical resection of a soft-tissue sarcoma is most closely related to
Explanation
REFERENCES: Lewis JJ, Leung D, Heslin M, Woodruff JM, Brennan MF: Association of local recurrence with subsequent survival in extremity soft tissue sarcoma. J Clin Oncol 1997;15:646-652.
Meterissian SH, Reilly JA Jr, Murphy A, Romsdahl MM, Pollock RE: Soft-tissue sarcomas of the shoulder girdle: Factors influencing local recurrence. Distant metastases and survival. Ann Surg Oncol 1995;2:530-536.
Question 55
The fracture shown in Figure 32 is strongly indicative of what diagnosis?
Explanation
REFERENCES: Kocher MS, Kasser JR: Orthopaedic aspects of child abuse. J Am Acad Orthop Surg 2000;8:10-20.
Kleinman PK, Marks SC, Blackbourne B: The metaphyseal lesion in abused infants: A radiologic-histopathologic study. Am J Roentgenol 1986;146:895-905.
Question 56
Which of the following is considered a risk factor for the development of low back pain?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 627-643.
Question 57
What structure (arrow) is shown in Figure 24?
Explanation
REFERENCES: Onibokun A, Khoo LT, Holly L: Anterior retroperitoneal approach to the lumbar spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 101-105.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 58
A 40-year-old man with amyloidosis injured his left knee while walking. Figure 17a shows an AP radiograph that was obtained 2 weeks after the injury. The radiograph shown in Figure 17b was obtained after the patient wore a hinged knee brace for 3 months. A clinical photograph is shown in Figure 17c. What is the most likely diagnosis?
Explanation
REFERENCES: Drennan D, Fahey J, Maylahn D: Important factors in achieving arthrodesis of the Charcot knee. J Bone Joint Surg Am 1971;53:1180-1193.
Soudry M, Binazzi R, Johanson N, et al: Total knee arthroplasty in Charcot and Charcot like joints. Clin Orthop 1986;208:199-204.
Buxbaum JN: The systemic amyloidoses. Curr Opin Rhemutol 2004;16:67-75.
Question 59
A 19-year-old soccer player feels a pop in his knee while making a cut and notes the development of an effusion over several hours. Examination reveals medial joint line tenderness, but the knee is stable to manual stress testing of all ligaments. Examination under anesthesia confirms a stable knee. What is the most critical factor in determining healing after repair of the lesion shown in Figure 14?
Explanation
REFERENCES: DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
Henning CE, Lynch MA, Clark JR: Vascularity for healing of meniscus repairs. Arthroscopy 1987;3:13-18.
Question 60
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
REFERENCES: Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Clanton TO, Coupe KJ: Hamstring strains in the athlete: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:237-248.
Question 61
Lumbar disk replacement has been shown to offer which of the following results?
Explanation
REFERENCES: Geisler FH, Blumenthal SL, Guyer RD, et al: Neurological complications of lumbar artificial disc replacement and comparison of clinical results with those related to lumbar arthrodesis in the literature. J Neurosurg Spine 2004;1:143-154.
Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 62
A 22-year-old professional baseball pitcher has had pain in the axillary region of his dominant shoulder for the past several weeks. While throwing a pitch during a game, he notes a sharp pulling sensation with a “pop” in his shoulder. Examination the following day reveals tenderness along the posterior axillary fold and pain and weakness with resisted extension of the shoulder. What is the most likely cause of his symptoms?
Explanation
REFERENCES: Schickendantz MS, Ho CP, Keppler L, et al: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains and related injuries.
Magn Reson Imaging Clin N Am 1999;7:39-49.
Livesey JP, Brownson P, Wallace WA: Traumatic latissimus dorsi: Tendon rupture. J Shoulder Elbow Surg 2002;11:642-644.
Question 63
- Figures 38a & 38b show radiographs of a 40 year old man who underwent a Putti-Platt repair for recurrent dislocations at age 22. He reports increasing pain in the shoulder and limited motion for five years. Examination reveals 130 degrees of elevation and 15 degrees of external rotation. Non-surgical treatment has failed. Treatment should now consist of what?
Explanation
Late onset of pain (average 13 years) was noted following this procedure in a small number of patients. The pain is attributed to excessive G-H compressive forces due to limited external rotation. NSAIDS and PT are first line treatments. If these fail, the authors demonstrated good results with release of the anterior structures. Choices 3 & 4 would probably be reserved for patients older than 50 with more advanced signs of degenerative disease.
Question 64
Figures 9a and 9b are the radiographs of a 19-year-old woman with a painful juvenile bunion. The pathologic findings associated with this deformity include a

Explanation
The radiographs show a hallux valgus deformity with a laterally deviated distal metatarsal articular surface, a large intermetatarsal angle with medial deviation at the first metatarsocuneiform joint, an elongated medial collateral ligament, and a contracted lateral collateral ligament. There is no distal 1-2 transverse intermetatarsal ligament. The distal transverse ligament in the first interspace extends from the second metatarsal to the lateral (fibular) sesamoid, remains intact, and keeps the sesamoids in a lateral position as the first metatarsal head migrates medially.
RECOMMENDED READINGS
Coughlin MJ. Roger A. Mann Award. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int. 1995 Nov;16(11):682-97. PubMed PMID: 8589807.
View Abstract at PubMed
Coughlin MJ, Mann RA. Hallux valgus. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:183-226.
Question 65
Figures 18a through 18c show injuries sustained by a 22-year-old woman after falling 45 feet while mountain climbing. After being airlifted to the nearest trauma center, her arterial blood gas was 7.21, pO2 84, pCO2 48, and delta base -11 mmol/L. Her Hgb is 8.7 and her resuscitation is ongoing. Based on this data, what would be the best management of her orthopaedic injuries?

Explanation
prolonged, invasive surgery. Upper extremity fractures are best managed acutely with splints in this clinical setting. Definitive fracture fixation should be delayed until the patient is adequately resuscitated.
Question 66
A 14-year-old boy is seen for back pain. Radiographic evaluation reveals a grade III isthmic spondylolisthesis. What measurement is most useful in predicting the likelihood of progression?
Explanation
REFERENCES: Huang RP, Bohlman HH, Thompson GH, et al: Predictive value of pelvic incidence in progression of spondylolisthesis. Spine 2003;28:2381-2385.
Mac-Thiong JM, Wang Z, de Guise JA, et al: Postural model of sagittal spino-pelvic alignment and its relevance for lumbosacral developmental spondylolisthesis. Spine 2008;33:2316-2325.
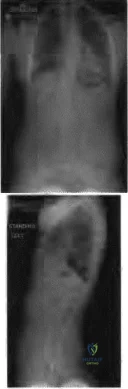
Figure 22a Figure 22b
Question 67
Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implant is shown in Figure 181). He now has increasing hip pain. Radiographs reveal a stable hip arthroplasty and elevated serum cobalt and chromium levels. MR imaging is obtained, and, based on these findings, the patient’s hip is revised. Which corrosion type likely is responsible for this THA failure?
Explanation
Micromotion at the femoral head-neck or stem-neck junction can lead to fretting corrosion. Fretting corrosion is among the most common causes of failure in modular components. Modularity gives surgeons additional intraoperative flexibility but has resulted in corrosion-related failure and an implant recall. Although titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer, resulting in fretting corrosion. This may eventually lead to excessive metal ion formation and painful synovitis that necessitates a revision procedure. Galvanic corrosion is attributable to a mismatch in electrochemical gradients between dissimilar metals. Crevice or pitting corrosion occurs in fatigue cracks because of differences in oxygen tension.
Question 68
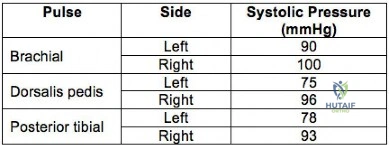
A 32-year-old professional skydiver lands awkwardly during a jump. He presents to the emergency room with bilateral knee injuries. Following successful closed reduction of both extremities, both feet are warm and pulses are present. Bedside doppler assessment is performed and the results are seen in Figure A. What would be the most appropriate next step in treatment?
Explanation
Injury to the popliteal artery is present in 10-40% of knee dislocations (KD). ABI
<0.9 has sensitivity of 87% and specificity of 97% for the diagnosis of arterial disruption. Delayed recognition of an occlusive injury (>8 hours) is likely to result in above knee amputation.
Stannard et al. examined the role of selective arteriography based on serial physical examination. They found arterial injury in 7% (9 out of 134 knees), and abnormal physical findings in 10 patients, with only 1 false positive. They recommend arteriography for patients with decreased pulses, color or temperature, expanding knee hematoma, or an abnormal physical examination prior to presentation in the emergency department.
Mills et al. reviewed the value of ABI for diagnosing arterial injury after knee dislocation. They found that of the 29% with ABI <0.9, all required surgery for arterial injury. Of the remaining patients with ABI >0.9, none had vascular injury. They concluded ABI >0.9 has negative predictive value of 100%.
Nicandri et al. reviewed an algorithm for selective angiography. They recommend the following: (1) Intact pulses and ABI >0.9, observation for 24 hours. (2) Asymmetric pulses or ABI <0.9, arteriogram. (3) Hard signs of vascular injury (absent distal pulses, distal ischemia, active hemorrhage, expanding pulsatile hematoma), surgical exploration.
Figure A is a table showing systolic pressure readings at different sites. To calculate the ABI, the highest measured arterial pressure in the ankle or foot is divided by the higher brachial arterial pressure from both upper extremities.
Incorrect Answers:
Question 69
The parents of a 14-year-old female soccer player are concerned about any future injury. They have been advised that she has the potential to play for the US Olympic team. They are especially concerned about the anterior cruciate ligament (ACL). What should you advise them? Review Topic
Explanation
Question 70
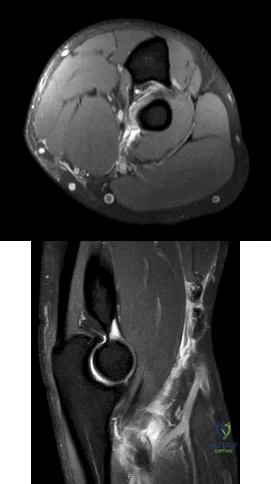
Figures 1 and 2 are the MRI scans of a 35-year-old right-hand dominant man who has right elbow pain after trying to lift a large television at home. An examination reveals ecchymosis, an abnormal hook test, and altered biceps muscle contour. What treatment is most likely to result in a satisfactory and predictable outcome?
Explanation
Question 71
03 An 18 month old child has bilateral “corner fractures” of the distal femoral metaphyses of unknown origin. Following a skeletal survey, the first step in management should consist of
Explanation
back to this question next question
Question 72
A 22-year-old woman sustains the injury seen in Figure 12 as a result of a motor vehicle crash. What factor is most closely associated with development of osteonecrosis?

Explanation
(SBQ12TR.90) A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management? Review Topic

MRI angiography of leg
Four-compartment fasciotomy
Follow-up examination the following day
Continued monitoring and serial examinations
EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam.
An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy. However, the treatment of early compartment syndrome should be to initially improve the limbs perfusion pressure gradient. This can be done by treating underlying factors such as hypotension, coagulopathy, or vascular compromise due to either a true vascular injury or artificially by external compression. Frequent reassessment is then critical to effectively manage these patients. If clinical diagnosis persists despite these efforts, urgent fasciotomy would be considered.
McQueen looked at 116 patients with tibial diaphyseal fractures who had continuous monitoring of anterior compartment pressure for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of 30 mmHg is a more reliable indicator of compartment syndrome.
White et al. looked at 101 patients with tibial fractures with satisfactory Delta P measurements. THey found that patients with elevated intramuscular pressures >30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P <30 mm Hg.
Figure A shows a Shatzker V tibial plateau fracture. Figure B shows fixation of fracture seen in Figure A.
Incorrect Answers:
30 mm Hg or persistently elevated absolute compartment pressures.. Answer 3: It would not be appropriate to leave this patient with impending compartment syndrome.
(SBQ12TR.57) A 56-year-old right hand dominant attorney falls from standing and sustains the closed injury shown in Figure A. The treating surgeon elects to fix her fracture using a plate and screw construct. Based on the available imaging, which of the following fracture characteristics best justifies this fixation choice?

Fracture displacement
Intra-articular fracture extension
The fracture extends distal to the coronoid
Oblique fracture line
Fracture comminution
This patient has a displaced, intra-articular, comminuted olecranon fracture. Comminution is an indication for plate fixation.
Most displaced olecranon fractures are treated operatively. Options include tension band constructs, intramedullary screws, plate and screw fixation or fragment excision with triceps advancement. Any construct relying on inter-fragmentary compression (tension band, intramedullary screws) requires a non-comminuted fracture pattern. Plate fixation is indicated in the setting of comminution, extension past the coronoid, or in the setting of associated instability.
Bailey et al. retrospectively reviewed 25 patients who underwent plate fixation of displaced olecranon fractures. Twenty-two of 25 patients had good or excellent outcomes. Five of 25 patients (20%) of patients required plate removal for symptomatic hardware. The authors concluded that plate fixation was an effective treatment for displaced olecranon fractures, with good functional outcomes.
Figure A shows a displaced, comminuted olecranon fracture without evidence of propagation past the coronoid.
Incorrect answers:
congruity but does not dictate implant selection. Answer 3. Extension distal to the coronoid is an indication for plate fixation but there is no evidence of such extension on the radiograph shown Answer 4. This fracture is comminuted, without a distinct fracture line.
Question 73
What is the primary concern for arthrodesis of a failed infected total knee arthroplasty using internal fixation?
Explanation
REFERENCE: Windsor RE: Knee arthrodesis, in Insall JN, Windsor R, Kelly M, et al (eds): Surgery of the Knee. New York, NY, Churchill Livingstone, 1993, pp 1103-1116.
Question 74
A 20-year-old collegiate baseball pitcher has persistent deep shoulder pain. Examination reveals normal strength, 130 degrees of external rotation in abduction, 10 degrees of internal rotation in abduction, mild dynamic scapular winging, and equivocal findings on provocative tests for labral tears. Management should consist of
Explanation
REFERENCE: Burkhart SS, Morgan CD, Kibler WB: Shoulder injuries in overhead athletes: The “dead arm” revisited. Clin Sports Med 2000;19:125-158.
Question 75
Pacinian corpuscles are lamellated nerve endings that are responsible for providing the perception of
Explanation
REFERENCE: Sunderland SS: Nerves and Nerve Injuries, ed 2. New York, NY, Churchill Livingstone, 1978, pp 343-347.
Question 76
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 179-191.
Question 77
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
REFERENCES: Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.
Paley D, McMurtry RY: Median nerve compression by volarly displaced fragments of the distal radius. Clin Orthop Relat Res 1987;215:139-147.
Question 78
A healthy 65-year-old woman undergoes anatomic total shoulder arthroplasty to address osteoarthritis (OA). The surgery is uncomplicated. What is the most common indication for future revision?
Explanation
inflammatory arthritis. Infections, periprosthetic fractures, and rotator cuff tears are uncommon. In the population-based study by Matsen and associates, 10% of the revisions were performed for loosening versus
7% for infection and 7% for rotator cuff tearing.
Question 79
At the first postoperative visit after mini-open carpal tunnel release, a patient reports hand weakness. Poor index finger interphalangeal joint extension and metacarpophalangeal joint flexion are present. This finding is most consistent with
Explanation
Complications after carpal tunnel release are relatively uncommon. The clinical picture described above is most consistent with lumbrical muscle weakness secondary to neuropraxia of the proper palmar digital nerve to the index finger supplying motor innervation to that muscle. The recurrent motor branch of the median nerve innervates the thenar musculature and would not present as index finger weakness. A new onset of trigger finger may result from a loss of the pulley effect of the transverse carpal ligament, postoperative tendon inflammation, or previously unrecognized flexor tendon triggering. Flexor digitorum profundus to the index finger lies deep within the carpal tunnel, making its injury unlikely. If it were injured, the result would not be weakness of interphalangeal joint extension.
Question 80
Figures 49a and 49b show MRI scans of the shoulder. What is the most likely diagnosis?
Explanation
REFERENCES: Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29.
Seeger LL, Gold RH, Bassett LW, Ellman H: Shoulder impingement syndrome: MR findings in 53 shoulders. Am J Roentgenol 1988;150:343-347.
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 81
Titanium and its alloys are unsuitable candidates for which of the following implant applications?
Explanation
REFERENCES: McKellop HA, Sarmiento A, Schwinn CP, et al: In vivo wear of titanium-alloy hip prostheses. J Bone Joint Surg Am 1990;72:512-517.
Salvati EA, Betts F, Doty SB: Particulate metallic debris in cemented total hip arthroplasty. Clin Orthop 1993;293:160-173.
Evans BG, Salvati EA, Huo MH, et al: The rationale for cemented total hip arthroplasty. Orthop Clin North Am 1993;24:599-610.
Question 82
Which of the following is most frequently associated with heterotopic ossification about the shoulder?
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 291.
Neer CS: Displaced proximal humerus fractures: Part II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Question 83
A 52-year-old woman underwent open reduction and internal fixation for radial and ulnar shaft fractures 2 months ago. In a second fall she refractured her forearm and required revision surgery with bone grafting. One month after the second operation she notes erythema, swelling, and drainage from the volar radial incision. In addition to antibiotic treatment, management should consist of
Explanation
REFERENCES: Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 53-63.
Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr: Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68:1008-1017.
Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphysis of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169.
Question 84
Figure 19 shows the radiograph of a 6-month-old infant who has limited hip motion. History reveals no complications during pregnancy or delivery. Examination reveals that hip abduction is 45 degrees in flexion bilaterally. The neurologic examination is normal. What is the best course of action?
Explanation
REFERENCE: Castelein RM, Korte J: Limited hip abduction in the infant. J Pediatr Orthop 2001;21:668-670.
Question 85
A 45-year-old man has a draining sinus and recurrent infection of his right total knee arthroplasty. He has had two prior revision surgeries after the primary procedure and three other surgeries before his initial replacement, including a proximal tibial osteotomy and subsequent hardware removal. On clinical examination, he has a draining sinus in the mid portion of his surgical scar and a range of motion of 5° to 85°. AP and lateral radiographs of the right knee are shown in Figures below. During surgery, the femoral component is found to be grossly loose, but the tibial component is well fixed. What is the most appropriate extensile approach that would provide adequate exposure and aid in tibial component extraction?
Explanation
Extended tibial tubercle osteotomy is an extensile approach to revision total knee arthroplasty that affords excellent exposure and can facilitate removal of tibial sleeves and cones. This patient has had multiple surgeries, including a proximal tibial osteotomy, as well as poor range of motion, patella baja, and a well-fixed metaphyseal sleeve component. Classically, an extended tibial tubercle osteotomy provides outstanding exposure for component removal in the setting of prior high tibial osteotomy and patella baja. For this patient, it is important to recognize the patella baja on the radiographs, as well as the tibial sleeve. In many of these cases the osteotomy provides access to the sleeve to help with extraction, because the stem will not pull through the sleeve or detach from the tray to allow visualization of the sleeve. The extended medial parapatellar approach is just a long medial approach that typically yields good exposure
but would not help with the patella baja or extraction of the tibial sleeve. The quadriceps snip would give good exposure to the knee but would not aid in tibial component removal. Lastly, the medial epicondyle osteotomy could help with exposure and tensioning of the medial complex of the knee but would not help with tibial component extraction.
Question 86
A patient with refractory long head biceps pain in the shoulder undergoes biceps tenotomy. The patient is concerned about possible postoperative deformity and loss of supination strength. Which of the following techniques provides the strongest initial fixation to prevent distal migration?
Explanation
REFERENCES: Ozalay M, Akpinar S, Karaeminogullari O, et al: Mechanical strength of four different biceps tenodesis techniques. Arthroscopy 2005;21:992-998.
Richards DP, Burkhart SS: A biomechanical analysis of two biceps tenodesis fixation techniques. Arthroscopy 2005;21:861-866.
Question 87
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads? Review Topic
Explanation
Question 88
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
in intestinal absorption and an increase in urinary calcium loss. The reduction of
intestinal absorption is accompanied by reduced circulating concentrations of total, but
not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial.
REFERENCES: Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Reid IR: Menopause, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 55-57.
Question 89
Figure 17 shows the radiograph of a 2-year-old girl who sustained a fracture of the femur in a fall while walking with her parents. History reveals that this is her third long bone fracture, having sustained a humerus fracture 1 year ago and a fracture of the opposite femur 9 months ago. There is no family history of any similar problem. Examination reveals distinctly blue sclerae, normal appearing teeth, and no skin lesions. What is the most likely cause of this patient’s disorder?
Explanation
REFERENCES: Kocher MS, Shapiro F: Osteogenesis imperfecta. J Am Acad Orthop Surg 1998;6:225-236.
Sillence DO, Senn A, Danks DM: Osteogenesis imperfecta: An expanding panorama of variants. Clin Orthop 1981;159:11-25.
Cole WG: Etiology and pathogenesis of heritable connective tissue diseases. J Pediatr Orthop 1993;13:392-403.
Question 90
A 10-year-old soccer player has bilateral heel pain and reports that the pain is worse during and immediately after sports. Examination reveals that the calcaneal tuberosities are painful to palpation bilaterally. What is the most likely diagnosis?
Explanation
REFERENCES: Micheli LJ, Ireland ML: Prevention and management of calcaneal apophysitis in children: An overuse syndrome. J Pediatr Orthop 1987;7:34-38. 500.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 91
Figures below show the radiographs obtained from a 75-year-old woman who underwent right total hip arthroplasty in 2009. She did well until last month, when a right posterior hip dislocation occurred after she fell from her bed to the floor. Successful closed reduction was performed. She sustained two more posterior dislocations requiring closed reduction under anesthesia. The surgical report from the index arthroplasty notes a 54-mm monoblock acetabular component with a 28-mm inner diameter compression molded polyethylene and a high offset neck cementless stem with a +8-mm length, 28-mm head. What is the best next step?
Explanation
This patient has demonstrated recurrent instability, and her current implants lack the modularity to upsize and improve the head-neck ratio and range to impingement. Given the monoblock acetabular component and a +7-mm neck length, the best option is revision to a large-diameter femoral head or dual-mobility component. Placement of a hip spica cast and resection arthroplasty are unreasonable. Revision to a longer ball length likely would not solve this recurrent instability pattern.
Question 92
A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of
Explanation
REFERENCE: Clarke CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
Question 93
A quarterback sustains a rough tackle after which he appears confused, has a dazed look on his face and an unsteady gait on standing. He denies loss of consciousness. Reexamination within 10 minutes is normal, the patient is lucid, and he wants to return to play. The coach and the player should be advised that he may
Explanation
REFERENCES: Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Cantu RC: Criteria for return to competition after closed head injury, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby, 1991.
Question 94
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At 1-year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is
Explanation
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 95
A 33-year-old male patient presents with a comminuted open tibia fracture after involvement in a motor vehicle crash. He has a history of smoking but is otherwise healthy. He is given antibiotics, and taken immediately for irrigation and debridement, followed by an un-reamed stainless steel intramedullary nail. Due to bone loss there is a non-circumferential cortical defect measuring 12 mm at the fracture site. All of the following factors in this patient's history and presentation increase his risk for adverse outcome EXCEPT:
Explanation
The treatment of open tibia fractures with intramedullary nailing can be complicated by many factors. High energy mechanism of injury, use of a stainless steel nail,
residual fracture gap greater than 1 cm, and a history of smoking have all been shown to increase the risk of adverse outcome. The use of reamed and un-reamed nails for open tibia fractures have been studied, and no significant difference in outcome has been found.
Schemitsch et al. present data from a prospective randomized trial of tibia fractures treated with reamed or unreamed intrameduallry nails. They found no difference in risk of adverse outcome between reamed and un-reamed nails in open tibia fractures. They did, however, find an increased risk of adverse outcomes in high-energy mechanisms, use of stainless steel (versus titanium) rods, and a residual fracture gap of greater than 1 cm. They comment that their data did not show a significant increase in risk due to history of smoking, but cite other studies that have demonstrated such a relationship.
Bhandari et al. present data from a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. For closed fractures they found a lower rate of primary events (most commonly need for dynamization) in the reamed group. However, they found no difference in outcomes for either technique in open fractures.
Incorrect answers:
Question 96
What cell type causes the bone destruction in metastatic lesions?
Explanation
REFERENCES: Cramer SF, Fried L, Carter KJ: The cellular basis of metastatic bone disease in patients with lung cancer. Cancer 1981;48:2649-2660.
Clohisy DR, Palkert D, Ramnaraine ML, Pekurovsky I, Oursler MJ: Human breast cancer induces osteoclast activation and increases the number of osteoclasts at sites of tumor osteolysis. J Orthop Res 1996;14:396-402.
Question 97
A 12-year-old boy with hemophilia A and no known inhibitors sustains a tibia fracture and has pain with passive motion of the deep toe flexors. Appropriate management should consist of
Explanation
REFERENCES: Dumontier C, Sautet A, Man M, Bennani M, Apoil A: Entrapment and compartment syndromes of the upper limb in haemophilia. J Hand Surg Br 1994;19:427-429.
Carr ME Jr, Loughran TP, Cardea JA, Smith WK, Kuhn JG, Dottore MV: Successful use of recombinant factor VIIa for hemostasis during total knee replacement in a severe hemophiliac with high-titer factor VIII inhibitor. Int J Hematol 2002;75:95-99.
Chuansumrit A, Isarangkura P, Angchaisuksiri P, et al: Controlling acute bleeding episodes with recombinant factor VIIa in haemophiliacs with inhibitor: Continuous infusion and bolus injection. Haemophilia 2000;6:61-65.
Question 98
Compared with retention of the native patella in primary total knee arthroplasty, routine patellar resurfacing is associated with
Explanation
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in
large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate
in patients with anterior knee pain.
Question 99
What is the most common site of nerve compression in radial tunnel syndrome?
Explanation
A. Quadrigia
B. Intrinsic tightness
C. Lumbrical plus deformity
D. Disruption of the tendon repai
Question 100
A 22-year-old man reports that he initially dislocated his shoulder while playing basketball 2 years ago and was subsequently treated with an arthroscopic Bankart repair. Despite appropriate rehabilitation, the patient continues to report recurrent instability. An axillary view radiograph and CT scan are shown in Figures 57a and 57b. What is the most appropriate management at this time? Review Topic

Explanation
