Orthopedic Surgery Board Review MCQs: Fracture, Nerve & Shoulder | OITE/AAOS Part 73

Key Takeaway
This page is Part 73 of an interactive MCQ quiz for orthopedic surgeons and residents. It features 100 verified, high-yield questions in OITE/AAOS board exam format, covering Fracture, Nerve, and Shoulder. Designed for rigorous AAOS/ABOS board preparation and review.
About This Board Review Set
This is Part 73 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 73
This module focuses heavily on: Fracture, Nerve, Shoulder.
Sample Questions from This Set
Sample Question 1: Which of the following is an advantage of using blocking screws for tibial nailing?...
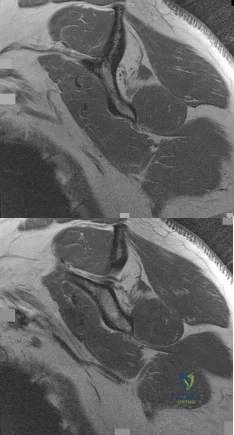
Sample Question 2: Figures 45a and 45b show sagittal T1-weighted MRI scans of a 35-year-old man who has had dominant extremity shoulder pain and weakness for the past 6 months. He denies any history of injury. Examination reveals full range of active and pass...
Sample Question 3: The decision to perform fasciotomy of the fingers for a hand compartment syndrome is most appropriately made using...
Sample Question 4: The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?...
Sample Question 5: An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following is an advantage of using blocking screws for tibial nailing?

Explanation
Krettek found that medial and lateral blocking screws can increase the primary stability of distal and proximal metaphyseal fractures after nailing and can be an effective tool for selected cases that exhibit malalignment and/or instability by decreasing mechanically measured deformation.
In a later clinical study, Krettek found that after using blocking screws, tibial healing was evident radiologically at a mean of 5.4 months with a decreased rate of malunions.
Ricci also found that blocking screws are effective to help obtain and maintain alignment of fractures of the proximal third of the tibial shaft treated with intramedullary nails.
Question 2
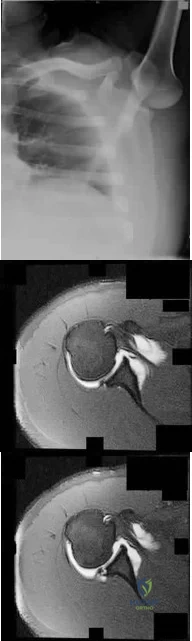
Figures 45a and 45b show sagittal T1-weighted MRI scans of a 35-year-old man who has had dominant extremity shoulder pain and weakness for the past 6 months. He denies any history of injury. Examination reveals full range of active and passive motion, negative Hawkins and Neer impingement signs, 5/5 abduction strength, 3+/5 external rotation strength with arm adducted at his side, and negative belly press, Hornblower's sign, Gerber lift-off, and O'Brien's test. Radiographs are unremarkable. An MR arthrogram shows no rotator cuff or labral tears and no paralabral cysts. What is the next most appropriate step in management? Review Topic
Explanation
Question 3
The decision to perform fasciotomy of the fingers for a hand compartment syndrome is most appropriately made using
Explanation
Compartment syndrome of the hand can result from a variety of factors, including a traumatic event such as crush injury, fracture, vascular insult, a high-pressure injection injury, or an insect or spider bite. The treatment involves decompressive fasciotomy of the involved compartments. The diagnosis of hand compartment syndrome is determined by history, examination, and objective testing. Patients experience pain out of proportion to the injury, along with swelling and tense skin. Pain may occur with passive motion of the metacarpophalangeal joints as the intrinsic muscles are stretched. Invasive intracompartmental pressures can be measured in the compartments of the hand but not in the fingers. Arterial Doppler studies assess arterial blood flow, and an abnormality would be a late finding. MRI would show edema of the hand and fingers, but the decision to perform surgical release is less likely made from the findings. The most appropriate method of determining the need for finger fasciotomy is the history and physical examination.
Question 4
The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?
Explanation
REFERENCES: McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Lister GD, McGregor IA Jackson IT: The groin flap in hand injuries. Injury 1973;4:229.
Question 5
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
REFERENCES: Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Mohler LR, Hanel DP: Closed fractures complicated by peripheral nerve injury. J Am Acad Orthop Surg 2006;14:32-37.
Question 6
All of the following are factors associated with transfer of patients to Level 1 trauma centers EXCEPT:

Explanation
Question 7
An elderly woman with radiographic evidence of spinal stenosis reports difficulty walking and calf pain that is relieved by rest and a change of position. The most likely cause of pain is ischemia of the
Explanation
Question 8
When compared with patients having a body mass index (BMI) lower than 35, patients with a BMI above 40 who undergo primary total hip arthroplasty (THA) and total knee arthroplasty (TKA) are likely to have
Explanation
The obesity epidemic is increasing, and the number of patients with a BMI higher than 35 undergoing THA and TKA also is growing. Controversy exists over the optimal BMI cutoff and the ability to perform joint replacements safely in patients who are morbidly obese. Several clinical series and national database analyses have shown that morbidly obese patients undergoing THA or TKA are at increased risk for wound complications as well as 30-day and 90-day readmissions. These patients’ incisions are typically larger because of the size of the soft-tissue envelope. Although the clinical scores following successful THA or TKA often are lower than the scores of controls, the overall changes in clinical function and satisfaction are equivalent in nonobese and obese patients.
Question 9
A 7-year-old boy is seen in the emergency department with an isolated and displaced supracondylar humerus fracture and absent radial and ulnar pulses. Despite a moderately painful attempt at realignment, examination reveals that his hand remains pulseless. What is the next most appropriate step in management? Review Topic
Explanation
and vascular assessment. Angiography is not required in isolated injuries as the level of the vessel compromise is always at the site of the fracture. When blood flow is not restored, the next best step in treatment is to proceed urgently to the operating room. A formal closed reduction and pinning is performed, and then the vascular status is reassessed. Exploration and vascular repair is required if the hand is cool, white, and without pulses.
Question 10
A 57-year-old man with type II diabetes mellitus was successfully treated for a first occurrence forefoot full-thickness (Wagner II) diabetic foot ulcer underlying the third metatarsal head with associated hammertoe with a series of weight-bearing total contact casts. There was no evidence of osteomyelitis. The ulcer is now fully healed. He is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. What is the next most appropriate step in management?
Explanation
REFERENCES: Pinzur MS, Slovenkai MP, Trepman E, et al: Guidelines for diabetic foot care: Recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int 2005;26:113-119.
Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.
Question 11
Which of the following is the primary mechanism of polyethylene wear in the hip?
Explanation
26-/28-mm heads (1-mm increase in size increased volumetric wear by 10%). The wear at the articulating surface was characterized by highly worn polished areas superiorly and less worn areas inferiorly separated by a ridge. Abrasion was very common, occurring after adhesion and plastic deformation of polyethylene fibrils, and abrasion secondary to third-body wear. Wear rates decreased with longer survival of components, indicating a “bedding in” phenomenon, arguing against oxidative and fatigue wear. Crevice corrosion occurs in fatigue cracks with low oxygen tension (under screw heads, etc). Oscillatory fretting consists of cyclical abrading of the outer surface from small movements. Fatigue and delamination is predominant in total knee arthroplasty where stresses are maximum just below the surface of the polyethylene component, causing fatigue over time with subsequent delamination. In contrast, hip wear occurs primarily at the surface of the polyethylene component.
REFERENCES: Jasty M, Goetz DD, Bragdon CR, et al: Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg Am 1997;79:349-358.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53.
Bell CJ, Walker PS, Abeysundera MR, et al: Effect of oxidation on delamination of
ultrahigh-molecular-weight polyethylene tibial components. J Arthroplasty 1998;13:280-290.
Sutula LC, Collier JP, Saum KA, et al: The Otto Aufranc Award: Impact of gamma sterilization on clinical performance of polyethylene in the hip. Clin Orthop 1995;319:28-40.
Question 12
-Figures 10a and 10b are the sagittal and coronal MRI scans of a 5-year-old boy who noticed “clicking” in his right knee. His family denied any trauma, but admitted that the child was active and fell frequently.Birth and developmental history were unremarkable, and specifically negative for other musculoskeletal conditions. On physical examination, there was no warmth, tenderness, or erythema, or effusion. The child had an audible and palpable clunk when the knee was taken from a position of extreme flexion to full extension. There was no anterior, posterior, medial, or lateral instability on examination or medial or lateral joint line tenderness. The child had not been systemically ill. Radiographs were unrevealing.What is the most likely diagnosis?
Explanation

Question 13
An otherwise healthy 30-year-old man undergoes right shoulder arthroscopic Bankart repair under regional anesthesia using an interscalene brachial plexus block. In the recovery room, he reports mild difficulty breathing and his chest radiograph shows a high riding diaphragm on the right side. His peripheral oxygenation is 97% on 2 liters of oxygen by nasal cannula. What is the most appropriate management?
Explanation
Question 14
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?
Explanation
REFERENCES: McMinn RMH, Hutchings RT, Logan BM: Color Atlas of Foot and Ankle Anatomy. Weert, Netherlands, Wolfe Medical Publications, 1982, p 50.
Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea & Febiger, 2000, pp 963, 966.
Question 15
Which of the following best describes the most common anatomic variation seen in the glenoid labrum and the middle glenohumeral ligament in the anterosuperior quadrant of the shoulder?
Explanation
REFERENCES: Rao AG, Kim TK, Chronopoulos E, et al: Anatomical variants in the anterosuperior aspect of the glenoid labrum. J Bone Joint Surg Am 2003;85:653-659.
Ilahi OA, Labbe MR, Cosculluela P: Variants of the anterosuperior glenoid labrum and associated pathology. Arthroscopy 2002;18:882-886.
Williams MM, Snyder SJ, Buford D: The Buford complex-The “cord-like” middle glenohumeral ligament and absent anterosuprior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 16
Which of the following patients is more likely to have an overall poorer outcome following a lower extremity amputation?
Explanation
Question 17
A 47-year-old woman has an asymptomatic pelvic mass that was discovered on routine gynecologic examination. A radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 7a through 7d. Metastatic work-up is negative. Treatment should consist of
Explanation
REFERENCES: Springfield DS, Gebhardt MS, Mcguire MH: Chondrosarcoma: A review. J Bone Joint Surg Am 1996;78:141-149.
Marco RA, Gitelis S, Brebach GT, Healey JH: Cartilage tumors: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:292-304.
Question 18
Halo treatment for preadolescent children typically requires the use of which of the following? Review Topic
Explanation
Question 19
Calcitonin acts as an antiresorptive agent by
Explanation
REFERENCE: Lane JM, Nydick M: Osteoporosis: Current modes of prevention and treatment. J Am Acad Orthop Surg 1999;7:19-31.
Question 20
- A 47-year-old woman who reports mild, aching pain in her knee has no history of trauma. Examination of the knee is normal. Figure 23a shows the AP radiograph. A bone scan shows increased uptake at this site only. Figure 23b shows the CT scan, and Figure 23c shows the histology from the CT scan-guided needle biopsy. Treatment should include
Explanation
The modern technique for the removal of a giant cell tumor involves wide decortication of all the bone overlying the area of the tumor. The cavity is filled with methylmethacrylate bone cement and covered with demineralized bone matrix to stimulate the restoration of strong cortical
boundaries. The other procedures are much more invasive and not necessary to treat a low-grade neo-plastic lesion such as a giant cell tumor. Fewer complications and better functional results have been found after intralesional excision and insertion of methylmethacrylate than other techniques.
Question 21
Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 degrees of pronation. The interosseous space and distal radioulnar joint are stable. Management should consist of
Explanation
REFERENCES: Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Esser RD, Davis S, Taavao T: Fractures of the radial head treated by internal fixation: Late results in 26 cases. J Orthop Trauma 1995;9:318-323.
Question 22
A 15-year-old right-handed pitcher reports shoulder pain after throwing. His symptoms have been present for 3 months and have been getting progressively worse. Clinical examination shows no atrophy of the shoulder muscles, but he has pain with resisted motion of the shoulder, especially internal rotation. Radiographs are shown in Figures 73a and 73b. What is the next step in the evaluation and treatment of his shoulder pain? Review Topic

Explanation
Question 23
The tibiofibular overlap used to diagnose syndesmotic diastasis on an AP view is most commonly measured between the
Explanation
REFERENCES: Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Stiehl JB: Ankle fractures with diastasis. Instr Course Lect 1990;39:95-103.
Question 24
Radiographs shown in Figures 1 through 3 show two different prosthetic design variations of the same knee implant. When compared with the design of right knee prosthesis, the left can be expected to have a
Explanation
Question 25
In a patient with a C5-6 herniation, the most likely sensory deficit will be in the
Explanation
REFERENCE: Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 26
A 13-year-old girl is referred for a painful progressive valgus deformity of the right knee. Examination reveals an antalgic gait with an obvious valgus deformity. The right distal femur has a palpable, tender mass with erythema and warmth. Figures 4a and 4b show a clinical photograph and a radiograph. Management should consist of
Explanation
REFERENCES: Enneking W: Principles of musculoskeletal oncologic surgery, in Evarts C (ed): Surgery of the Musculoskeletal System. New York, NY, Churchill Livingston, 1990.
Herring JA: General principles of tumor management, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, from the Texas Scottish Rite Hospital for Children, ed 3. Philadelphia, PA, WB Saunders, 2002, pp 1897-1900.
Question 27
Which of the following accurately describes the biosynthetic materials tricalcium phosphate (TCP) and hydroxyapatite?
Explanation
500 µm.
REFERENCES: Lane JM, Bostrom MP: Bone grafting and new composite biosynthetic graft materials. Instr Course Lect 1998;47:525-534.
Walsh WR, Chapman-Sheath PJ, Cain S, et al: A resorbable porous ceramic composite bone graft substitute in a rabbit metaphyseal defect model. J Orthop Res 2003;21:655-661.
Question 28
What factor is associated with a high risk of developing pseudotumors after metal-on-metal hip resurfacing?
Explanation
Question 29
What is the most likely late complication associated with cementless total knee replacement?
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Question 30
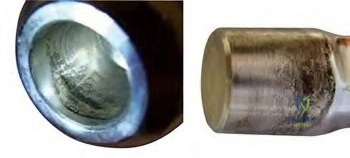
In performing a posterior stabilized total knee arthroplasty (TKA), which component malpositioning is associated with the wear damage shown in this tibial component retrieval (Figure 172)?
Explanation
The tibial polyethylene insert shows anterior post wear damage from anterior CAM-post impingement in a posterior stabilized knee. It is associated with excessive femoral component flexion and excessive posterior tibial slope in a TKA construct. It is not associated with coronal plane alignment.
Question 31
A football player who injured his right lower extremity during a game could not get up and reported extreme pain. The initial sideline evaluation showed a probable anterior cruciate, posterior cruciate, and lateral collateral ligament rupture with a very unstable knee. He also reports pain in his ankle and is unable to dorsiflex the ankle. He has limited sensation over the dorsum of his foot. Examination reveals no swelling of the ankle and no pain with passive range of motion of the ankle. What is the most likely diagnosis? Review Topic
Explanation
Question 32
The posterior horn of the medial meniscus receives its primary blood supply from what artery? Review Topic
Explanation
Question 33
What is the structure indicated by the letter “A” in Figure 21?
Explanation
REFERENCES: Morrey BF: Anatomy of the elbow joint, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1993, p 30.
O’Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 34
An 18-year-old collegiate football player injures his right shoulder during a tackle. He reports pain and numbness in the shoulder and numbness radiating to his fingers. His symptoms improve within 15 minutes and he has no residual symptoms. This condition is best known as Review Topic
Explanation
Question 35
-What is the diagnosis?
Explanation
Salter-Harris type II fracture of the proximal humerus
Question 36
A patient with deficient anteroinferior bone stock undergoes a Latarjet procedure that transfers a portion of the coracoid to the glenoid rim and secures it with two screws. After surgery, the patient reports numbness on the anterolateral forearm. To verify the diagnosis, what muscle should be tested for strength?
Explanation
REFERENCES: Ho E, Cofield RH, Balm MR, Hattrup SJ, Rowland CM: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
Boardman ND 3rd, Cofield RH: Neurologic complications of shoulder surgery. Clin Orthop 1999;368:44-53.
Allain J, Goutallier D, Glorion C: Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 1998;80:841-852.
Question 37
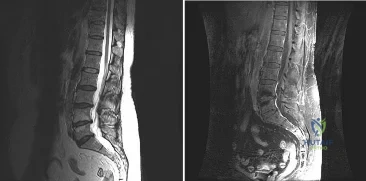
A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T2-weighted MRI scan is shown in Figure 13a, and a contrast enhanced T1-weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient’s symptoms? Review Topic
Explanation
pseudomeningocele is not present. A revision diskectomy is useful for recurrent radiculopathy but would not be helpful for degenerative low back pain.
(SBQ12SP.29) A 17-year-old female is undergoing posterior instrumented fusion from T5-T12 for adolescent idiopathic scoliosis. At the time of the correction maneuver, the neurophysiologist notifies you of a 60% decrease in somatosensory evoked potential (SSEP) amplitude throughout bilateral lower extremities. Which of the following is an acceptable approach to manage this finding? Review Topic
Immediate wake-up test with examination for clonus
Drop the mean arterial pressure (MAP) to ~60mmHg
Discontinue instrumentation and optimize MAP to 85mmHg or greater
Immediate infusion of intravenous corticosteroids
Modification of the anesthesia plan to include inhalational agents only followed by repeated SSEP testing
The patient has a significant drop in SSEP amplitudes at the completion of the corrective maneuver. The most appropriate response is to raise the MAP to 85 mmHg or greater, discontinue the instrumentation, re-evaluate the SSEPs, and if there is no improvement, to consider reversing the reduction of the deformity.
Intra-operative neurophysiologic monitoring is an effective method to monitor insults to the spinal cord and its exiting roots during spinal instrumentation. The common measurements include SSEPs, which monitor sensory potentials transmitted through the dorsal column system, and motor-evoked potentials (MEPs), which monitor motor response to a trans-cranial stimulus. Decreases in amplitude and latency of the circuits are recorded, however diminished signal amplitudes are more sensitive for neurologic injury, and decreases of of >50-60% being highly concerning. The wake-up test involves reversal of anesthesia so that an intra-operative neurologic examination can be performed.
Devlin et al. reviewed the basic science and practice of neurophysiologic monitoring in spine surgery. They proposed an algorithmic approach to managing intraoperative alerts which include discontinuation of inhalational anesthetics, increasing the MAP to >90 mmHg, discontinuing instrumentation, and performing a wake-up test if neurologic signals fail to normalize.
Herdmann et al. reviewed the practice of neurophysiologic monitoring and the effects of anesthesia upon signal transduction. They report that anesthesia affecting a neuron's intrinsic excitability can alter the results of monitoring. Inhalational anesthetics and decreased MAPs can be responsible for decreased amplitudes.
Vitale et. al. developed a consensus-based intraoperative checklist for management of lost neuromonitoring signals. In this checklist, the first steps across the surgical and anesthetic teams should include: stop the case and announce signal losses to the room, optimize the mean arterial pressure, discuss the status of anesthetic agents, and discuss reversible surgical actions just prior to signal loss.
Incorrect
Question 38
Figure 1 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder with loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in
Explanation
A. better glenoid exposure than with stemmed prostheses.
B. reliable use in four-part proximal humerus fracture reconstruction.
C. use in proximal humeral malunion without the need for an osteotomy.
D. improved long-term survivorship profile.
Question 39
A 45-year-old woman has had intense pain in her foot for the last 3 days. She also reports a mild fever and difficulty with shoe wear. Examination reveals a swollen, slightly erythematous warm foot with tenderness at the great toe metatarsophalangeal joint and pain with passive motion of the joint. An AP radiograph is shown in Figure 13. Which of the following will best aid in determining a definitive diagnosis?

Explanation
REFERENCES: Wise CM, Agudelo CA: Diagnosis and management of complicated gout. Bull Rheum Dis 1998;47:2-5.
Harris MD, Siegel LB, Alloway JA: Gout and hyperuricemia. Am Fam Physician 1999;59:925-934.
Question 40
Figure 50 shows the MRI scan of a 20-year-old female college soccer player with knee pain. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 41
below depicts the radiograph obtained from a year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of below reveals
Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 42
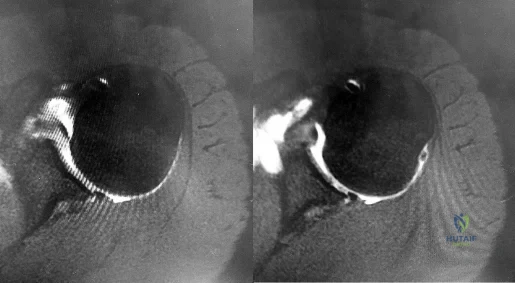
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. If present, what is the most likely complication after surgical treatment in this scenario?
Explanation
and degenerative joint disease.
Question 43
A 20-year-old man has a large soft-tissue mass behind his knee. MRI scans are shown in Figures 10a through 10c. Figure 10d shows a clinical photograph of his chest. The patient’s condition is most likely a result of a defect in what gene?
Explanation
REFERENCES: Theos A, Korf BR, American College of Physicians, et al: Pathophysiology of neurofibromatosis Type 1. Ann Intern Med 2006;144:842-849.
Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002.
Question 44
Which of the following is true regarding changes in the vascularity of the adult intervertebral disc with age? Review Topic
Explanation
The intervertebral disc is composed of an outer structure called the annulus fibrosis and an inner structure called the nucleus pulposus. The annulus fibrosis is composed
of type 1 collagen, water, and proteoglycans. The inner nucleus pulposus is composed of type 2 collagen, water, and proteoglycans. Intervertebral discs are avascular with capillaries terminating at the end plates. The nucleus pulposus receives nutrition primarily through diffusion through blood vessels within the endplate.
Roberts et al. review the histology and pathology of the intervertebral disc. They note that at birth, the cartilagenous end plates have large vascular channels through them as well as vascular channels through the annulus. Soon after birth, these vascular channels close with none remaining at the end of the first decade of life. However, with age, more blood vessels grow into the disc from the outer annulus fibrosis in response to degenerative changes.
Illustration A is a diagram of the vascular supply in an adult intervertebral disc. Incorrect Answers:
Question 45
A 25-year-old male presents to the emergency department with a mangled lower extremity that is not salvageable. He undergoes transfemoral amputation. Three months later the patient presents to the office with the limb sitting in an abducted position. What important step was forgotten during the amputation?

Explanation
Question 46
A 58-year-old man has anterior knee pain after undergoing total knee arthroplasty for osteoarthritis 2 years ago. He denies any history of trauma. A Merchant view is shown in Figure 20. What is the most likely cause of his pain?
Explanation
REFERENCES: Reuben JD, McDonald CL, Woodard PL, Hennington LJ: Effect of patella thickness on patella strain following total knee arthroplasty. J Arthroplasty 1991;6:251-258.
Hsu HC, Luo ZP, Rand JA, An KN: Influence of patellar thickness on patellar tracking and patellofemoral contact characteristics after total knee arthroplasty. J Arthroplasty 1996;11:69-80.
Greenfield MA, Insall JN, Case GC, Kelly MA: Instrumentation of the patellar osteotomy in total knee arthroplasty: The relationship of patellar thickness and lateral retinacular release. Am J Knee Surg 1996;9:129-131.
Question 47
Examination of a 41-year-old man who was thrown from a motorcycle reveals that both legs appear externally rotated and there is bruising in the perineal area. He has a blood pressure of 80/40 mm Hg, a pulse rate of 140/min, a respiratory rate of 25/min, and he appears confused. Following administration of 4 L of saline solution and 2 units of packed red blood cells, he has a blood pressure of 80/40 mm Hg, a pulse rate of 160/min, and a respiratory rate of 25/min. The abdominal assessment for intraperitoneal blood is negative. An AP radiograph shows an anteroposterior compression injury with 7 cm of symphysis diastasis but no posterior displacement in the sacroiliac joints. What is the next most appropriate step in management?
Explanation
REFERENCES: Bassam D, Cephas GA, Ferguson KA, Beard LN, Young JS: A protocol for the initial management for unstable pelvic fractures. Am Surg 1998;64:862-867.
Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 217-226.
Mucha P Jr, Welch TJ: Hemorrhage in major pelvic fractures. Surg Clin North Am 1988;68:757-773.
Question 48
What is the primary limiting membrane and mechanical support for the periphery of the physis?
Explanation
REFERENCES: Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
Asher MA (ed): Orthopaedic Knowledge Update 1. Chicago, IL, American Academy of Orthopaedic Surgeons, 1984, pp 15-28.
Question 49
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What is the most appropriate course of action for this patient’s condition?
Explanation
diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
Question 50
A 55-year-old man is about to undergo right total hip arthroplasty. A preoperative AP pelvis radiograph is shown in Figure below. The final acetabular component and polyethylene liner are implanted. With the broach in place, the surgeon trials a standard offset neck and neutral length femoral head. The leg lengths are approximately equal, but the hip is unstable. What is the best next step?
Explanation
The radiograph shows that this patient has a high offset varus femoral morphology of both hips. Preoperative templating would identify this, and the surgeon should choose an implant system that has extended offset options to help match the native anatomy and biomechanics and minimize the risk of instability. Trialing a high offset neck, rather than a standard offset neck, is the next most appropriate step. Depending on the design of the implant system, this step can be accomplished by direct medialization of the femoral head, which would not affect leg length, or by lowering the neck angle, which would affect the leg length and would require a longer femoral head, because the leg lengths had previously been equal. Placement of a longer femoral head would likely improve hip stability but would also make the leg length uneven, which is a common cause of dissatisfaction after total hip arthroplasty. An offset acetabular liner also increases the leg length and does not correct the issue, which is on the femoral side. Trochanteric
advancement is sometimes used as a treatment for instability but would be inappropriate as the next step in this setting.
Question 51
A 24-year-old man who plays golf noted the immediate onset of pain on the ulnar side of his hand and has been unable to swing a club for the past 6 weeks after striking a tree root with his club during his golf swing. Examination reveals full motion of the wrist, diminished grip strength, and tenderness over the hypothenar region. A CT scan of the hand and wrist is shown in Figure 26. Management should consist of
Explanation
REFERENCES: Carroll RE, Lakin JF: Fracture of the hook of the hamate: Acute treatment. J Trauma 1993;34:803-805.
Whalen JL, Bishop AT, Linscheid RL: Nonoperative treatment of acute hamate hook fractures. J Hand Surg Am 1992;17:507-511.
Question 52
Which of the following is an advantage of unreamed nailing of the tibia compared to reamed nailing?
Explanation
REFERENCES: Larsen LB, Madsen JE, Hoiness PR, et al: Should insertion of intramedullary nails for tibial fractures be with or without reaming? A prospective, randomized study with 3.8 years’ follow-up. J Orthop Trauma 2004;18:144-149.
Blachut PA, O’Brien PJ, Meek RN, et al: Interlocking intramedullary nailing with or without reaming for the treatment of closed fractures of the tibial shaft: A prospective randomized study. J Bone Joint Surg Am 1997;79:640-646.
Question 53
What type of medial collateral ligament tear heals the most reliably? Review Topic
Explanation
Question 54
Which of the following nerves travels with the deep palmar arch?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 166-169.
Question 55
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?
Explanation
REFERENCE: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, pp 98-100.
Question 56
Figure 10 shows the radiograph of an active 75-year-old woman who reports severe leg pain after a fall. Management should consist of
Explanation
REFERENCES: Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Montijo H, Ebert FR, Lennox DA: Treatment of proximal femur fractures associated with total hip arthroplasty. J Arthroplasty 1989;4:115-123.
Question 57
Which of the following is considered the treatment of choice for a 3-cm chondroblastoma of the distal femoral epiphysis with no intra-articular extension?
Explanation
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748.
Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 58
The best definitive treatment for this patient’s left knee is
Explanation
This patient now has a major fixed flexion contracture and severe varus alignment and instability. Infection of the knee joint has to be ruled out. The radiograph shows all the hallmarks of Charcot arthropathy, including disintegration and fragmentation of the joint with major deformity. Infection of the knee joint and contiguous osteomyelitis still have to be ruled out. The clinical and radiographic findings are highly suggestive of a Charcot neurogenic arthropathy associated with uncontrolled diabetes. This patient is an unsuitable candidate for total knee arthroplasty (TKA) because he is noncompliant regarding his diabetes and has had a previously infected native joint that now is associated with Charcot arthropathy. He is nonambulatory. The failure rate of TKA or knee arthrodesis is extremely high in this setting. He will best be served with observation or amputation depending upon his symptom severity.
Question 59
-A 10-year-old boy sustained a displaced Salter-Harris type II supination/plantar flexion fracture of the left ankle. He underwent closed reduction under conscious sedation; however, postreduction radiographs showed continued 5-mm anterior widening of the tibial physis. What is the most likely cause of the widening?
Explanation
Question 60
During anatomic medial patellofemoral ligament (MPFL) reconstruction, the surgeon notes that the graft is becoming too tight with greater knee flexion. What is the most likely cause?
Explanation
Question 61
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?
Explanation
REFERENCES: Brodsky AE, Khalil MA: Talar compression syndrome. Am J Sports Med 1986;14:472-476.
Wredmark T, Carlstedt CA, Bauer H, Saartok T: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Question 62
Which of the following structures is at risk during proximal dissection of a single lateral perifibular approach for compartment syndrome of the leg?

Explanation
Question 63
A patient has a C6 spinal cord injury. Following stabilization of the spine, the patient should be advised that their expected maximum level of function
Explanation
Question 64
A 20-year-old college pitcher reports the recent onset of decreased velocity and posterior shoulder pain. He states that it takes him longer to loosen up but denies any mechanical symptoms. When compared to his non-throwing shoulder, glenohumeral examination of his throwing shoulder will most likely reveal which of the following findings? Review Topic
Explanation
Question 65
An axillary nerve lesion may cause weakness in the deltoid and the
Explanation
REFERENCE: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs. New York, NY, Harper & Row, 1969.
Question 66
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Explanation
REFERENCES: Michelson JD, Magid D, Ney DR, et al, Examination of the pathologic anatomy of ankle fractures. J Trauma 1992;32:65-70.
Marsh JL, Saltzman CL: Ankle fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 2001-2090.
Question 67
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
Explanation
REFERENCES: Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815.
Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Moro JK, Werier J, MacDermid JC, et al: Arthroplasty with a metal radial head for unreconstructable fractures of the radial head. J Bone Joint Surg Am 2001;83:1201-1211.
Question 68
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?
Explanation
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
Question 69
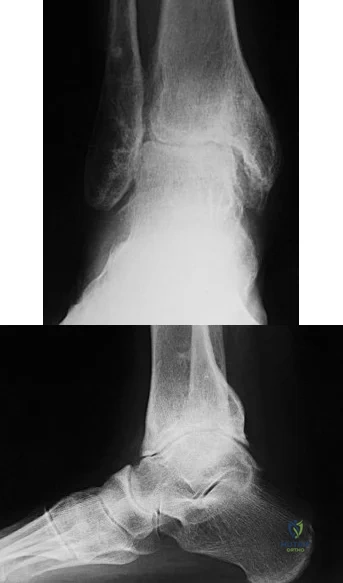
Figures 20a and 20b are the radiographs of a 56-year-old woman who runs a horse farm. She has a 2-year history of increasing ankle pain and swelling without previous treatment. Which treatment is most appropriate at this time?
Explanation
This patient has end-stage ankle arthritis. A short course of NSAIDs may provide pain and inflammation relief. Bracing with either an ankle-foot orthosis or Arizona brace can reduce pain by offloading the ankle joint. Ankle fusion is a reliable procedure for treatment of end-stage ankle arthritis and is especially recommended for active people after it is determined that nonsurgical measures no longer provide adequate relief. Arthroscopic debridement and cheilectomy may be indicated for bony impingement and mild arthritis with little articular cartilage loss. The long-term results of ankle distraction arthroplasty are not yet well defined but likewise would be reserved for scenarios in which nonsurgical measures no longer provide adequate relief. The patient must be able to wear a thin-wire external fixator for 3 months.
RECOMMENDED READINGS
Abidi NA, Neufeld SK, Brage ME, Reese KA, Sabharwal S, Paley, D. Ankle arthritis. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:159-193.
Saltzman CL: Ankle arthritis, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle. Philadelphia, PA, Mosby Elsevier, 2007, vol 1, pp 929-932.
Question 70
When harvesting iliac crest bone graft during a posterior spinal decompression and fusion, injury to what structure can result in painful neuromas or numbness over the skin of the buttocks?
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins 1998, pp 770-773.
Kurz LT, Garfin SR, Booth RE Jr: Harvesting autogenous iliac bone grafts: A review of complications and techniques. Spine 1989;14:1324-1331.
Mrazik J, Amato C, Leban S, et al: The ilium as a source of autogenous bone grafting: Clinical considerations. J Oral Surg 1980;38:29-32.
Question 71
A 23-year-old man reports a 6-year history of recurrent instability in the right dominant shoulder. He has not undergone surgery and has essentially stopped all of his sporting activities. On examination, he has instability and apprehension in the midrange of motion (abduction of 45 to 60 degrees with external rotation) and a palpable clunk representing a transient dislocation over the anterior glenoid rim. A three-dimensional CT scan is shown in Figure 31. What is the most appropriate surgical intervention to provide him with reliable stability postoperatively?
Explanation
A bony augmentation procedure such as the Lataijet has been well-described to provide a well functioning and stable shoulder joint. A hemiarthroplasty is not indicated in the absence of arthritis. Subscapularis
advancement will not address the bone loss.
REFERENCES: Hovelius L, Sandstrom B, Sundgren K, et al: One hundred eighteen Bristow-Latarjet repairs for recurrent anterior dislocation of the shoulder prospectively followed for fifteen years: Study I— clinical results. J Shoulder Elbow Surg 2004;13:509-516.
Schroder DT, Provencher MT, Mologne TS, et al: The modified Bristow procedure for anterior shoulder instability: 26-year outcomes in Naval Academy midshipmen. Am J Sports Med 2006;34:778-786.
Itoi E, Lee SB, Berglund LJ, et al: The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: A cadaveric study. J Bone Joint Surg Am 2000;82:35-46.
Question 72
A 15-year-old boy has had pain in the right shoulder for the past 3 months. He denies any history of trauma and has no constitutional symptoms. Examination reveals a large firm mass in the proximal arm. A radiograph and MRI scan are shown in Figures 27a and 27b. Biopsy specimens are shown in Figures 27c and 27d. Management should consist of
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 232-233.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-196.
Question 73
..Figures 78a and 78b are the radiographs of a 47-year-old right-hand-dominant woman who has a 3-month history of gradually progressive right shoulder pain. She reports no previous trauma, but does report pain at night and with activity such as weight training. Examination demonstrates active and passive range of motion to be 110 degrees forward elevation, external rotation to 20 degrees, and internal rotation to the sacrum. The next treatment step should include

Explanation
Rotator cuff and scapular stabilizer strengthening exercises
Diagnostic and therapeutic corticosteroid injection
Arthroscopic debridement
Completion of rotator cuff tear, repair, and biceps tenotomy
Acromioplasty
Repair of rotator cuff and superior labrum anterior to posterior (SLAP) repair
Repair of subscapularis tendon and biceps tenodesis
Question 74
You are counseling a 55-year-old woman for a right carpal tunnel release. What can you tell her about the treatment benefit (grip strength and paresthesia relief) 1 year after surgery compared with continued splinting, NSAID use, physical therapy, and a single steroid injection?
Explanation
Gerritsen and associates, Hui and associates, and Jarvik and associates compared the effectiveness of surgical versus nonsurgical treatment for the relief of carpal tunnel symptoms. All three studies showed that surgery was superior for the relief of paresthesias and the improvement of grip strength. According to the American Academy of Orthopaedic Surgeons Clinical Guidelines on the Treatment of Carpal Tunnel Syndrome, strong evidence supports the assertion that surgical treatment of carpal tunnel syndrome should have a greater treatment benefit at 6 and 12 months than splinting, NSAIDs, physical therapy, and a single steroid injection. The other choices, including no change in grip strength and
paresthesias, decrease in grip strength and increase in paresthesias, and increase in grip strength and paresthesias, are not supported by the evidence.
Question 75
-A 15-year-old boy underwent open reduction and internal fixation for a tibial tubercle fracture. The next morning he had dramatically increased pain, hypotension, ascending rash, and fever to 103°F. What is the most appropriate course of action?
Explanation

Question 76
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
REFERENCES: Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186.
Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
Question 77
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 78
A 58-year-old woman sustained a ruptured Achilles tendon 1 year ago, and management consisted of an ankle-foot orthosis. She now reports increasing difficulty with ambulation and increasing pain. An MRI scan shows a 6-cm defect in the right Achilles tendon. Management should now consist of
Explanation
REFERENCE: Myerson MS: Achilles tendon ruptures. Instr Course Lect 1999;48:219-230.
Question 79
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?
Explanation
REFERENCES: Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 80
A 40-year-old man fell off of a ladder at work sustaining the injury shown in Figures A and B. On examination, his skin is intact, but the pulses in his foot are absent. Following closed reduction and splinting, what would be the next best step?

Explanation

OrthoCash 2020
Question 81
Delayed-onset muscle soreness (DOMS) is initially evident at the muscle tendon junction and can spread throughout the entire muscle. It is primarily associated with what type of exercise? Review Topic
Explanation
Question 82
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of
Explanation
REFERENCES: Jakob RP, Miniaci A, Anson PS, et al: Four-part valgus impacted fractures of the proximal humerus. J Bone Joint Surg Br 1991;73:295-298.
Resch H, Povacz P, Frohlich R, et al: Percutaneous fixation of three- and four-part fractures of the proximal humerus. J Bone Joint Surg Br 1997;79:295-300.
Question 83
During fracture healing, granulation tissue tolerates the greatest strain before failure so that mature bone can eventually bridge the fracture gap during healing. What is the definition of strain?
Explanation
The mechanical environment at the fracture site has a major influence on fracture healing. Granulation tissue can withstand higher strain, which stabilizes the mechanical environment and forms a scaffold on which cartilage and bone eventually form; this occurs after strain decreases incrementally. Optimal healing, however, depends on duration, rate, timing and type of mechanical influence. Bone is formed by osteoblasts that are adapted to the very low strains of over 1% change in length. Osteoblast synthesis and proliferation is stimulated at uniaxial strain of between 0.3% and 2.8%. It is known that limited inter-fragmentary movement of 0.2 mm to 1 mm is optimal for fracture healing, resulting in promotion of callus and increase in rigidity. Excessive movement, on the other hand, prolongs fracture healing. Researchers have identified that tissue strain of 2% is suitable for primary bone healing and secondary bone healing takes place at tissue strain of 2-10%. Strain of 10-100% results in fibrous tissue formation and 100% strain to non-union. This is known as Perren's theory.
Stokes published a review article on the effects of stress on bone healing and growth, and notes the importance of the 'Hueter-Volkmann Law' (growth is retarded by increased mechanical compression, and accelerated by reduced loading in comparison with normal values) in bone growth. Stokes also notes that sustained compression of physiological magnitude inhibits growth by 40% or more, while distraction increases growth rate by a much smaller amount.
Illustration A shows an example of a stress-strain curve, with several key definitions labeled on the diagram.
Incorrect Answers:
Question 84
Figure 83a shows an axillary radiograph and Figures 83b and 83c show axial MR arthrograms of a 20-year-old collegiate offensive lineman who has shoulder pain while pass-blocking. He sustained a shoulder injury 3 months earlier when he "jammed it." Prior to this injury, he denies any pain or instability in either shoulder. Despite undergoing rehabilitation with a physical therapist and trainer and abstaining from playing for 6 weeks, he is currently unable to play because of his symptoms. Examination reveals full active range of motion, a positive jerk test which reproduces his symptoms, and a grade 2 posterior translation of the humeral head with load and shift testing which also reproduces his symptoms. What is the best management option to allow him to return to his pre-injury function next season? Review Topic
Explanation
Question 85
An otherwise healthy 50-year-old man who is a smoker undergoes a posterior spine fusion with instrumentation for spondylolisthesis. What can the patient do to minimize his risk for pseudarthrosis?
Explanation
Question 86
The patient does well initially but returns for the 4-month postsurgical evaluation with ongoing stiffness and pain despite going to physical therapy twice weekly and working on motion at home. She is unable to bear weight comfortably. What is the best next step?
Explanation
In a skeletally immature patient with OCD and minor symptoms, the lesion can be observed and healing obtained with activity limitations if the cartilage is stable (but this cannot be determined radiographically or clinically). Activity restriction and serial follow-up are appropriate if an MRI reveals a stable lesion. MRI is indicated when there is concern that a lesion may be unstable. Surgical treatment depends on MRI findings.
Observation is recommended for OCD lesions in growing patients for 6 months because healing has been observed. Early surgical procedures, although they may be needed in the future, are not appropriate for patients with well-controlled symptoms.
If symptoms continue for longer than 6 months, arthroscopic drilling is not indicated for unstable OCD. The appropriate treatment is OCD fixation. Debridement is not appropriate with a stable lesion.
Evaluation of the fixation and stability of the lesion with advanced imaging after weight bearing and therapy initiation is the most appropriate option. Manipulating the knee without determining whether the stiffness is attributable to subsidence of the fixation or mechanical block is not appropriate. After 4 months, aspiration of a hematoma (if still present) would not yield much benefit. More therapy is not likely to be useful when a patient is attending therapy regularly and working on a home program.

Question 87
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
Question 88
- A patient sustained a joint depression-type fracture of the calcaneus that healed despite lack of treatment. The loss of dorsiflexion the patient is now experiencing is most likely the result of
Explanation
Question 89
In addition to pain, which of the following factors are considered most predictive of the risk of pathologic fracture?
Explanation
REFERENCES: Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 90
Contraindications to cervical laminectomy as a treatment for cervical spondylotic myelopathy include which of the following findings?
Explanation
REFERENCES: Malone DG, Benzyl EC: Laminotomy and laminectomy for spinal stenosis causing radiculopathy or myelopathy, in Clark CR (ed.): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 817-825.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 673-680.
Question 91
Figure 1 is the MRI scan of a patient with recurrent knee instability, which persists after a period of nonsurgical treatment. Anatomic reconstruction of the torn ligament is recommended. What radiographic finding is the most important independent predictor of recurrent instability following surgery?
Explanation
Question 92
2ppb and chromium levels were 2.2ppn. 23 patients were revised to titanium sleeve with ceramic heads and all had improvement of their symptoms and a decrease in their metal ion levels.
Explanation
OrthoCash 2020
A 66-year-old patient is planning to undergo a right total knee arthroplasty. Figure A demonstrates the preoperative radiograph. Placing the components in a kinematic alignment (compared to neutral mechanical alignment) would result in which of the following?

Increased aseptic loosening
Varus tibial cuts and valgus femoral cuts
Lower rates of patient satisfaction
Decreased ROM
Increased reoperation rate
Kinematic alignment total knee arthroplasty is based on component placement to recreate a patient's natural anatomy. In the case of this patient, this would involve varus tibial cuts and valgus femoral cuts.
Kinematic alignment total knee arthroplasty is based on the principle of re-establishing a patient's natural anatomy. Many patients develop constitutionally varus or valgus knee alignment, in which placement of the arthroplasty components in relative varus or valgus positions would lead to symmetric mediolateral loading of the implants. This principle is further based on the idea that placing the components in neutral alignment may align the limb in an abnormal position to the patient, which may lower patient satisfaction. For varus knees, this implies varus tibial cuts with valgus femoral cuts.
Bellemans et al. performed an observational study of 250 asymptomatic study participant to determine what percentage of the population has constitutionally varus knee alignment. The authors found that 32% of males and 17.2% of females had constitutionally varus aligned knees. Furthermore, constitutionally varus knees were associated with greater physical activity during the second decade of life, believed to be secondary to Heuter-Volkmann loading of the open physis.
Lee et al. performed a systematic review of the literature comparing neutral alignment and kinematic alignment arthroplasty. Generally, the literature supported that ROM, KSS and WOMAC scores were equivalent, if not better, in kinematically aligned knees. Further, tibial components were in more varus and femoral components in more valgus. There were no differences in reoperation rates.
Figure A demonstrates a mechanical axis view radiograph with varus alignment of bilateral knees and medial compartment osteoarthritis. Illustration A demonstrates the difference in bone cuts between neutral alignment and kinematic alignment arthroplasty.
Incorrect Answers:

OrthoCash 2020
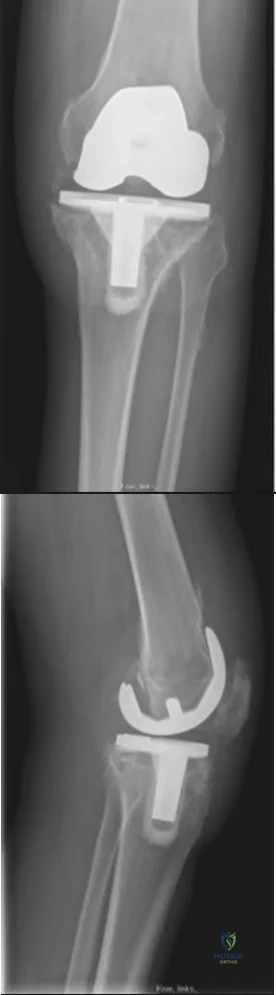
A 68-year-old patient with diabetes progressively worsening left knee pain of 6 months duration. They underwent a left total knee arthroplasty 7 years ago. Figures A-B demonstrate the current radiographs. Aspiration of the left knee demonstrated 11,500 WBCs and 94% neutrophils. Aspiration cultures grew methicillin-resistant Staphylococcus aureus. What would be the best treatment approach for this patient?
Knee arthrodesis
Long-term antibiotic suppression
One-stage revision arthroplasty
Two-stage revision arthroplasty
Above knee amputation Corrent answer: 4
The patient has several medical comorbidities and is presenting with a chronic prosthetic joint infection with a virulent organism (MRSA). The best treatment option at this time would be a two-stage revision arthroplasty.
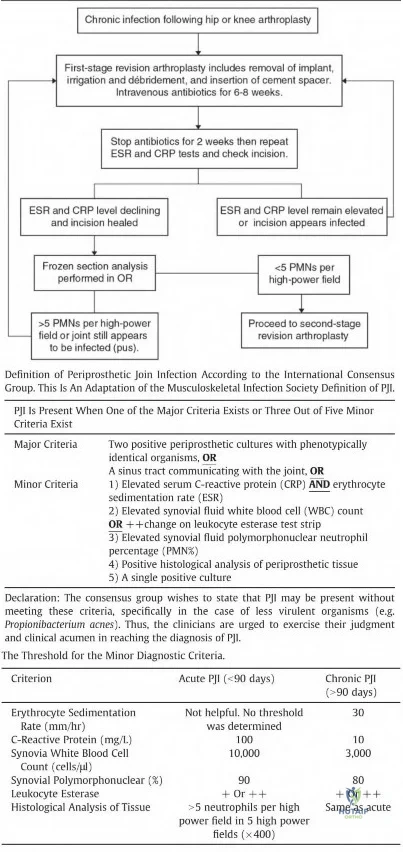
Chronic prosthetic joint infections occur greater than 3-6 weeks from surgery and result in biofilm formation over the prosthesis, making antibiotic treatment alone ineffective for infection eradication. Diagnosis is based on the MSIS criteria, with chronic infections being suggested with CRP greater than 10, ESR greater than 30, and synovial WBCs greater than 1,100. Two-stage revision arthroplasty is the current gold standard in the United States for treating chronic prosthetic joint infections.
Kuzyk et al. 2014 reviewed two-stage revision arthroplasty for chronic periprosthetic joint infections. The authors stated that there is no consensus on laboratory and histology criteria to confirm eradication prior to proceeding with the second stage. The authors recommend holding IV antibiotics for two weeks and repeated inflammatory markers to evaluate whether to proceed with the second stage and to perform frozen section at the time of the procedure.
Nguyen et al. 2016 reviewed one-stage revision arthroplasty for the treatment of periprosthetic joint infections. The authors reported that in select patients, one-stage revision arthroplasty can have equal if not better outcomes compared to two-stage revision with less surgical morbidity and improved functional outcomes. They concluded that one-stage revision arthroplasty can be successful in patients that are not immunocompromised, minimal medical comorbidities, known pathogen prior to surgery, non-polymicrobial, no virulent pathogen (MRSA), and with good soft tissue coverage.
Figures A and B demonstrate AP and lateral radiographs of the right with radiolucencies present around the tibial and femoral prosthesis. Illustration A demonstrates a treatment algorithm proposed by Kuzyk et al. for proceeding with the second stage of a two-stage revision. Illustration B demonstrates the Musculoskeletal Infection Society diagnostic criteria for a prosthetic joint infection. Illustration C depicts specific lab values for diagnosing a prosthetic joint infection.
Incorrect Answers:
OrthoCash 2020
A 77-year-old patient presents with progressively worsening right hip pain and limp. The patient underwent a right revision total hip arthroplasty 15 years ago and is now unable to ambulate due to the pain and feels as if the hip is unstable. The patient's radiograph is shown in Figure 1. Which of the following is the appropriate classification and best treatment approach for this patient?

Paprosky 2A; multihole cup with posterior column plating
Paprosky 2B; antiprotrusio cage with structural allograft
Paprosky 3A; distraction arthroplasty
Paprosky 3B; custom triflange cup
Paprosky 3B; cemented cup Corrent answer: 4
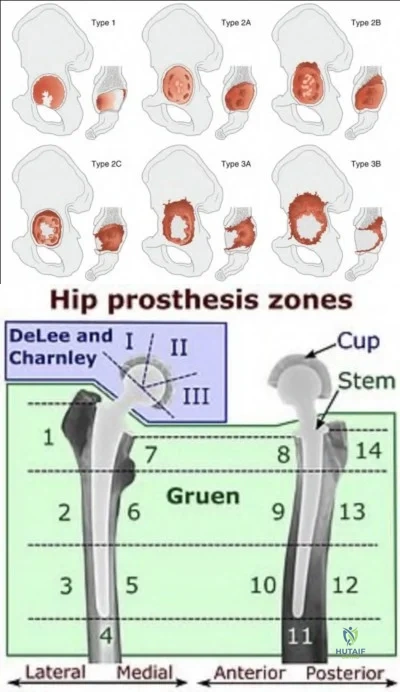
The patient is presenting with pelvic discontinuity due to severe acetabular bone loss and superomedial cup migration consistent with Paprosky 3B
acetabular deficiency and pelvic discontinuity. Revision to a custom triflange cup would be a viable treatment approach.
Pelvic discontinuity in revision total hip arthroplasty is a rare treatment challenge due to extensive bone loss from osteolysis and prior surgery. Typically, the cup migrates superomedial towards the pelvic viscera and can place neurovascular structures at greater risk. This defect is classified as type 3B in the Paprosky classification. Treatment involves restoring pelvic stability through the healing of the anterior and posterior columns as well as reconstituting hip biomechanics with custom triflange cups, posterior column plating, distraction arthroplasty, or augments with highly porous cups.
Taunton et al. performed a multicenter retrospective review of 57 patients that underwent reconstruction of pelvic discontinuity with a custom triflange cup.
The authors found that 81% of patients had a stable implant and healed discontinuity at final follow-up with implant cost being comparable to off-the-shelf options. The authors concluded that that custom triflange cup provides adequate fixation with good outcomes at a comparable cost to other fixation methods.
Jenkins et al. performed a retrospective review of 58 hips, of which 11 had pelvic discontinuity, that underwent revision with a tantalum porous cup and augments. The authors reported a high rate of radiolucency in Delee and Charnley zone III and implant failure in patients with pre-operative pelvic discontinuity that were revised with this technique. The authors recommend the use of alternative or adjunctive fixation in patients with pelvic discontinuity.
Regis et al. performed a retrospective review of 18 patients that underwent revision with antiprotrusio cage and bulk allograft for pelvic discontinuity. The authors found a 72.2% survival rate at 16.6 years with cases of failure demonstrating graft resorption and acetabular loosening. The authors suggested that bulk allografting with antiprotrusio cages provide an effective means to address pelvic discontinuity.
Figure A demonstrates an AP radiograph of the pelvis with pelvic discontinuity. Illustration A depicts the Paprosky classification system. Illustration B depicts the DeLee and Charley as well as the Gruen zones.
Incorrect Answers:
pelvic discontinuity in such a manner to allow for healing of the anterior and posterior columns. Furthermore, cemented cups are associated with high loosening rates.
OrthoCash 2020
A 75-year-old male sustains a ground-level fall while ambulating at home. The patient has been optimized for surgical intervention. Both prosthetic components are deemed to be stable. How would you classify this fracture and what is the appropriate treatment plan?

Vancouver B1; ORIF with a lateral locking plate
Vancouver C; revision of femoral stem from hip component
Vancouver C; retrograde intramedullary nail
Vancouver B2; revision to long stem total knee component
Vancouver C; ORIF with a lateral locking plate Corrent answer: 5
This patient has a Vancouver C periprosthetic fracture about stable total hip and knee arthroplasties (an interprosthetic fracture) which can be appropriately fixed with a lateral locked plate spanning the entire femur.
The success of prosthetic surgery has led to an increase in the percentage of the population having more than one prosthetic implant. This, combined with an increase in the average life expectancy and functional requirements for the elderly, has led to a higher incidence of periprosthetic and interprosthetic fractures. Treatment must be determined and assessed according to the type of fracture, the stability of the prosthesis, the bone quality and the general condition of the patient. When the implants are stable plate fixation spanning both of the prostheses has shown favorable results. Some surgeons advocate for nail/plate combination fixation in these interprosthetic fractures in an attempt to allow early weight-bearing.
Froberg et al. reviewed 60 consecutive periprosthetic Vancouver B1 or C fractures, all fixed with plate osteosynthesis. There were a total of 8 reoperations, 4 of which were for infection and 3 for fixation failure. They conclude that locking-plate osteosynthesis of periprosthetic Vancouver type B1 and C fractures gives good results in terms of fracture union. It appears that spanning of the prosthesis to avoid stress-rising areas is important for successful treatment. Infection remains the major cause of failure.
Hoffmann et al. reviewed interprosthetic femoral fractures, defined as fractures between an ipsilateral total knee and hip arthroplasty. 27 patients were designated as having interprosthetic fractures and were treated with locked plating. They conclude that locked plating can achieve satisfactory results. Additional soft tissue damage can be prevented by submuscular plate insertion. Treatment of type B fractures resulted in significantly greater nonunion rate.
Matlovich et al. reviewed fifty-seven patients treated for supracondylar periprosthetic femur fracture with either a locking plate (n = 38) or IM nail (n
= 19). There was no statistical difference between groups in the meantime to fully weight bear, the incidence of postoperative pain, range of motion, use of gait aids, time to full radiographic union, or the overall radiographic alignment of a healed fracture. Despite this, they add caution is recommended in using IM nails for fractures below the flange where limited fixation may increase the risk of nonunion.
Figure A demonstrates a Vancouver C interprosthetic fracture with well-fixed total hip and knee components.
Illustration A is an example of another patient status-post ORIF of an interprosthetic femur fracture.
Incorrect answers:

OrthoCash 2020
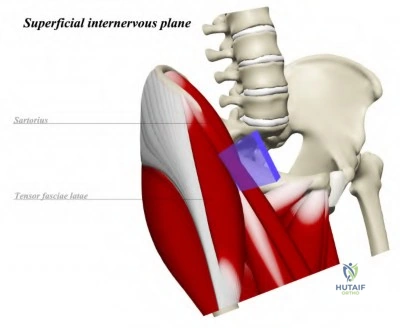
A 61-year-old man with left hip OA presents to clinic for persistent left hip pain despite a trial of conservative therapy. The decision is made to proceed with total hip arthroplasty via a direct anterior approach. Which of the following correctly describes the superficial internervous plane of this approach?
Rectus femoris (femoral n.) & tensor fascia lata (superior gluteal n.)
Tensor fascia lata (femoral n.) & sartorius (superior gluteal n.)
Rectus femoris (femoral n.) & gluteus medius (superior gluteal n.)
Sartorius (femoral n.) & gluteus medius (superior gluteal n.)
Sartorius (femoral n.) & tensor fascia lata (superior gluteal n.) Corrent answer: 5
The direct anterior approach to the hip is performed using the internervous interval between the sartorius (femoral n.) and tensor fascia lata (superior gluteal n.) superficially.
Total hip arthroplasty using a direct anterior approach has become increasingly
popular, with many studies showing good long-term results. It is performed through the internervous plane between the femoral nerve and superior gluteal nerve, superficially between the sartorius and TFL, and deep between the rectus femoris and gluteus medius. Advantages of the direct anterior approach include preservation of the abductor mechanism and decreased dislocation rates compared to the posterior approach. However, this approach has a steep learning curve and its use is limited in obese patients with a large pannus. Additionally, this approach places the lateral femoral cutaneous nerve at risk and may lead to increased intraoperative fracture rates.
Bohler et al. published a review on the direct anterior approach to the hip. They report that this approach allows for direct visualization of the acetabulum and offers a complete intermuscular and internervous access to the hip joint.
They found that the approach allows for decreased muscular trauma, intraoperative blood loss, and post-operative rehabilitation.
Post et al. published a review on the indications, technique, and results of the direct anterior approach for THA. They report that the steep learning curve and complications unique to this approach (fractures and nerve damage) have been well described; however, the incidence of these complications decreases with greater surgeon experience.
Illustration A is a diagram depicting the superficial internervous plane of the direct anterior approach to the hip.
Incorrect Answers:
OrthoCash 2020
A 45-year-old male presents with increasing left groin pain. He has a history of bilateral hip avascular necrosis and underwent bilateral hip resurfacing arthroplasties 3 years ago. He is a recreational runner and recently ran a 10-kilometer race several weeks ago. Figure A demonstrates an AP radiograph of his pelvis. Serum testing demonstrated a cobalt level of 10 mcg/L (reference 0.8
- 5.1 mcg/L) and chromium level of 7 mcg/L (reference 0.5 - 2.5 mcg/L). What is the likely cause of the patient's symptoms?
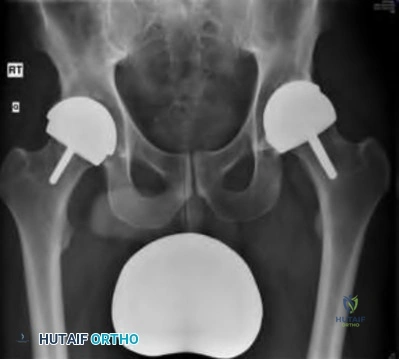
Iliopsoas tendonitis
Edge-loading
Prosthetic joint infection
Increased activity-related wear
Femoral neck stress fracture Corrent answer: 2
The patient is presenting with increased left hip pain after bilateral Birmingham Hip Resurfacing (BHR) arthroplasties and elevated ion levels consistent with metallosis. The most likely cause of metallosis in this patient is the edge-loading of the implant.
Hip resurfacing arthroplasty is a bone preserving procedure that is favorable in young male patients and utilizes metal-on-metal articulations. Metallosis is, therefore, a concerning complication of these implants and can result in pseudotumor formation and subsequent destruction of the hip abductors.
Patients presenting with a painful prosthesis should be screened with metal ion levels as well as a metal artifact reduction sequence MRI. Possible causes of metallosis include edge-loading, component malpositioning, third bodywear, impingement, and sensitivity to cobalt.
Brooks performed a retrospective review of patients undergoing BHR with regards to outcomes. The author found a 0.23% rate of metallosis in the study population, with all cases being attributed to edge-loading. The author recommended a preoperative CT scan and lateral pelvic radiographs to prevent component malposition and better identify surgical candidates.
Matharu et al. performed a prospective cohort study examining metal ion levels in patients with bilateral BHRs. The authors found that cobalt, chromium, cobalt-chromium ratio, and maximum cobalt and chromium levels to be significantly higher in patients with metallosis. They recommended using a cut-off of 5.7 mcg/L for cobalt and 5.5 mcg/L for chromium for metallosis in patients with bilateral BHRs.
Figure A demonstrates an AP radiograph of a pelvis with bilateral BHR implants and an increased inclination angle of the left acetabular component.
Incorrect Answers:
OrthoCash 2020
An ambulatory 57-year-old man with post-polio syndrome presents for follow-up of his right knee pain. He has failed all nonoperative measures for his right knee pain. On exam, he hyperextends to 15° and flexes to 120° with global instability of the knee. He has maintained antigravity strength in the right limb. Radiographs are shown in Figures A and B. What is the best treatment option for this patient?

Cruciate retaining knee with ligamentous reconstruction
Robotic-assisted posterior stabilized total knee arthroplasty
Distal femoral osteotomy with total knee arthroplasty
Hinged total knee arthroplasty
Above-knee amputation
The best treatment for this patient with post-polio syndrome is a hinged total knee arthroplasty.
Patients affected by the 1950 poliomyelitis outbreak are now approaching an age where degenerative knee changes are impacting their quality of life. These patients often have global instability and significant hyperextension deformity and require a hinged prosthesis. Any less constrained components put the patient at risk for continued instability and early failure. Patients with maintained antigravity strength in the operative limb may have improved outcomes in the setting of post-polio syndrome.
Gan et al. reviewed 16 knee replacement in patients with post-polio syndrome and degenerative knee changes. They found an improvement in the mean of all outcomes scoring measures including the AKSS, Oxford knee scores, AKSS pain scores, and SF-36 scoring. They concluded that primary knee arthroplasty for patients with post-polio syndrome shows a good improvement in patients quality of life and decreases pain.
Giori et al. retrospectively reviewed 16 patients with a history of poliomyelitis and a history of primary total knee arthroplasty. They found four cases of recurrent instability, two of which had a preoperative hyperextension deformity of 20 degrees. They concluded that pain and knee scores improved in these patients and that recurrent instability or functional deterioration occurred more often in the most severely affected knees. They recommend consideration of hinged arthroplasty or arthrodesis in this challenging subgroup of patients.
Figures A and B are AP and lateral radiographs of the right knee showing and severe valgus-hyperextension deformity and degenerative changes in a post-polio limb. Illustrations A and B show an AP and lateral postoperative radiograph following a hinged arthroplasty.
Incorrect Answers:

OrthoCash 2020
When compared to a median parapatellar approach which of the following approaches may lead to higher rates of component malposition?
Quadriceps sparing
Lateral parapatellar
Midvastus
Quadriceps snip
V-Y turndown
A quadriceps-sparing approach has been found to lead to a high rate of component malpositioning.
Improvements in surgical instrumentation and techniques drove surgeons to perform total knees replacement in a less invasive manner. One such technique was the quadriceps-sparing approach which uses minimal subluxation of the patella and special side cutting instruments. This technique was thought to lead to quicker recovery due to the minimal disturbance of the extensor mechanism however, studies have shown that it may lead to statistically significant higher rates of component malposition when compared to a traditional median parapatellar approach.
Kazarian et al. reviewed the outcomes of the quadriceps-sparing (QS) approach compared to a median parapatellar(MP) approach for total knee arthroplasty. They found statistically and clinically significant disadvantages to the QS approach including femoral and mechanical axis outliers, increased surgical time, and increased tourniquet time. They concluded the QS approach does not demonstrate any clinically significant advantages and leads to higher rates of component malalignment.
Kelly et al. randomized 42 consecutive total knee patients to either median parapatellar (MP) approach or a vastus splitting (VS) approach. They found a statistically significant increase in the rate of lateral release and blood loss in the MP approach but showed no difference in functional parameters, tourniquet time, or patellar resurfacing. They conclude the VS approach is a reasonable alternative to the MP approach and may lead to lower rates of lateral releases without impairment of quadriceps function.
Liu et al. compared outcomes of the minimally invasive midvastus (MV) and
subvastus (SV) approaches compared to a traditional median parapatellar (MP) approach for total knee arthroplasty. They found the number of days needed to perform a straight leg raise was significantly longer following MP compared to SV or MV approaches. They conclude that further studies should be performed to assess the outcomes of the various minimally invasive approaches for total knee arthroplasty.
Illustration A shows four different approaches for a total knee arthroplasty including three minimally invasive approaches.
Incorrect Answers:

OrthoCash 2020
A 66-year-old patient that underwent a right total knee arthroplasty approximately 4 years ago presents with worsening right knee pain over the last 48 hours. The patient has a history of rheumatoid arthritis and recently underwent a dental procedure a week ago. Labs were significant for CRP of 212, ESR 105, and a WBC count of 11K. Aspiration yielded a milky-looking fluid with 55K nucleated cells with 97% PMN. Radiographs are shown in Figures A and B. What is the next best step?
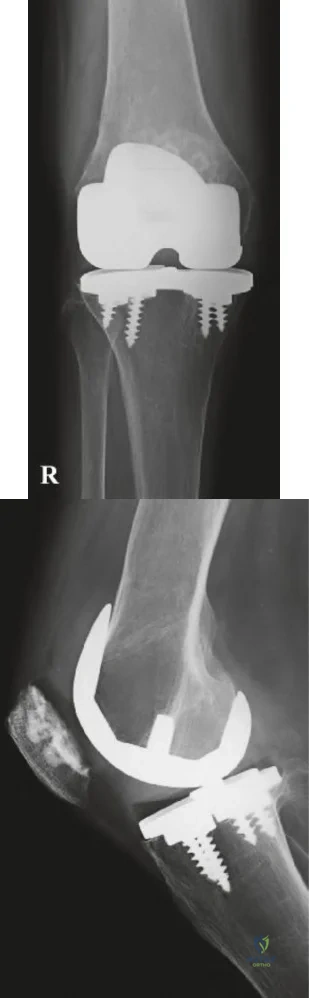
Surgical intervention after cultures finalize
Repeat aspiration of the knee and send for alpha-defensin
Begin IV antibiotics and re-evaluate in 24-48 hours
Proceed with surgical intervention now
IR guided drain placement Corrent answer: 4
The patient is presenting with an acute hematogenous prosthetic joint infection, which requires surgical treatment as soon as safely possible.
Periprosthetic joint infections (PJI) are generally managed surgically. Diagnosis is composed of a battery of findings as established by the Musculoskeletal Infection Society (MSIS), which requires the presence of one of two major criteria or four of six minor criteria (Illustration A). Acute infections can often be treated with irrigation and debridement with polyethylene exchange (IDPE), whereas chronic infections are best managed with a two-stage revision.
Buller et al. performed a retrospective study looking at variable affecting the success of IDPE treatment for PJI. The authors found that infections with MRSA or VRE, higher ESR levels, symptoms longer than 3 weeks, and previous joint infections were strong risk factors for failure of IDPE. The authors
concluded that patients presenting with these characteristics may be best treated with a two-stage revision rather than IDPE.
Figures A and B are AP and lateral radiographs of a right knee with a stable appearing total knee arthroplasty prosthesis. Illustration A is a table that depicts the 2011 MSIS criteria for diagnosing prosthetic joint infections.
Incorrect Answers:
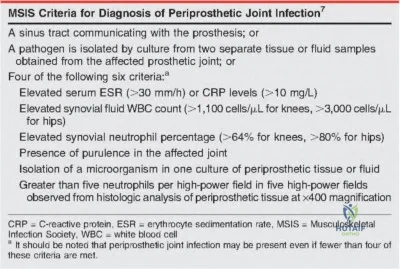
OrthoCash 2020
A 63-year-old patient with a previous right TKA 4 years ago presents with worsening pain in the right knee. The patient reports that pain is worsened when starting physical activity, but is also present at night. Two weeks prior to presentation the patient was given a 1-week course of oral antibiotics for cellulitis affecting the right knee. Serum labs were significant for a CRP of 11 mg/L and an ESR of 35 mm/hr. Synovial fluid analysis revealed 1,000/µL nucleated cells with 85% PMNs and no evidence of crystals. Synovial cultures were negative for any bacterial or fungal growth. Synovial alpha-defensin is positive. Figures A and B are the AP and lateral
radiographs of the right knee. The patient opts to undergo a revision total knee arthroplasty. What is the best management at this point?
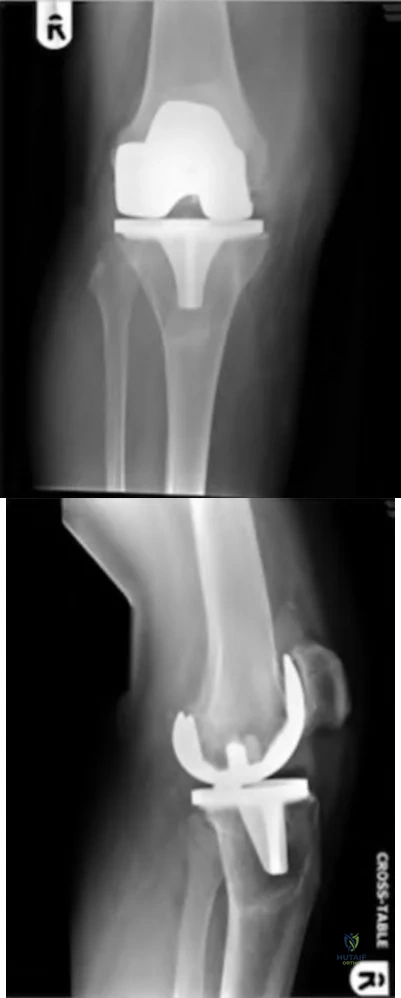
Femoral component revision
Tibial component revision
Polyethylene component revision
One-stage revision of both the femoral and tibial components
Two-stage revision of both the femoral and tibial components Corrent answer: 5
The patient is presenting with increasing knee pain consistent with either septic or aseptic loosening of the prosthesis. Serum and synovial labs are not diagnostic for an infection, but there is a positive synovial alpha-defensin suggesting the presence of a chronic prosthetic joint infection.
Prosthetic joint infections are diagnostic challenges as there is no single confirmatory test. Rather, diagnosis is composed of a conglomerate of physical and laboratory findings as laid forth by the Musculoskeletal Infection Society criteria. Diagnosis can be made by either the presence of one major criterion or four minor criteria. Synovial alpha-defensin is a new assay that tests for the presence of an antimicrobial peptide that is part of the innate immune system. Recent studies have suggested a high sensitivity and specificity of this test for prosthetic joint infections, even with prior antibiotic administration. Treatment involves two-stage revision arthroplasty with culture-specific antibiotics for at least six weeks. Reimplantation of a prosthesis is done with infection eradication is confirmed.
Shahi et al. performed a retrospective diagnostic study looking at whether prior antibiotic administration affected synovial alpha-defensin levels. The authors found that alpha-defensin was not affected by prior antibiotic administration. The authors concluded that since many patients with PJI will present with prior antibiotic administration, alpha-defensin may be an ideal diagnostic adjunctive test.
Frangiamore et al. performed a prospective cohort study on the sensitivity and specificity of alpha-defensins in diagnosing prosthetic joint infections. The authors found that alpha-defensin has a sensitivity and specificity of 100% and 98%, respectively, for diagnosing PJI in single-stage and first-stage revisions. The authors concluded that alpha-defensin has the potential as a useful adjunct in diagnosing PJI.
Figures A and B demonstrate AP and lateral radiographs of the right knee with loosening of the tibial and femoral components. Illustration A depicts the MSIS criteria for the diagnosis of PJI.
Incorrect Answers:
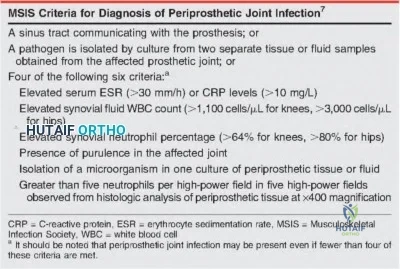
OrthoCash 2020
Of the following, which has the highest strength of recommendation according to the AAOS Clinical Practice Guidelines (CPG) for Surgical Management of Osteoarthritis of the Knee?
Preoperative physical therapy improves pain and physical function postoperatively
Tourniquet use during total knee arthroplasty (TKA) decreases short-term postoperative function
Continuous passive motion (CPM) after TKA improves outcomes
Rehabilitation started on the day of TKA reduces length of hospital stay
Surgical navigation should be used because there is a decrease in pain and functional outcomes
Rehabilitation started on the day of TKA decreasing length of stay has been deemed a "strong recommendation" by the AAOS.
Postoperative management following TKA is an important aspect of achieving an optimal outcome following total knee arthroplasty. The general recommendation is that patients should work with a physical therapist on the
day of surgery or as early as possible as it will decrease pain and improve function. Early rehabilitation is felt to also decrease the length of stay.
Recommendations against cryotherapy machines and CPM are moderate and strong, respectively, as they do not appear to improve outcomes.
McGrory et al. present the AAOS CPG's for surgical management of osteoarthritis of the knee. Strong evidence supports postoperative rehabilitation started on the day of surgery, which has been shown to decrease the length of stay. Moderate evidence supports rehabilitation starting the day of surgery compared to postoperative day 1 reduced pain and improves function. Various other preoperative and intraoperative topics are reviewed for the corresponding strength of recommendation.
Incorrect Answers:
OrthoCash 2020
A 62-year-old patient that underwent a right hip resurfacing arthroplasty 3 years ago develops worsening right hip pain over the past 6 months. The pain is present at all times, including at night. The patient does not walk with a Trendelenburg gait and does not have reproducible pain on hip examination. Laboratory inflammatory markers from 1 week ago were erythrocyte sedimentation rate of 66 mm/hr (reference <20 mm/hr), C-reactive protein of 22 mg/dL (reference <2.5 mg/dL), cobalt 0.5 µg/L (reference <0.7 µg/L), and chromium of 0.4 µg/L (reference <0.4 µg/L). Figure A demonstrates an AP radiograph of the pelvis. What is the next best step in management?

Physical therapy
Routine follow-up
Arthrocentesis with synovial fluid analysis
stage revision
Metal artifact reduction sequence MRI Corrent answer: 3
The patient is presenting with a painful right hip after a metal-on-metal arthroplasty with recent elevated inflammatory markers and normal metal ion levels. The best next step in diagnostic workup would include an arthrocentesis with synovial fluid analysis.
Diagnosis of chronic prosthetic joint infections is challenging due to the requirement of a conglomerate of physical and laboratory findings for the diagnosis. The most common presenting symptom is pain in the affected joint, but there may be draining sinus tracts and systemic inflammatory signs.
Work-up should start with serum inflammatory markers, which if elevated should prompt an arthrocentesis with synovial fluid analysis. If the diagnosis is still not clear a repeat aspiration can be performed or frozen section performed in the operating room. It is important in aspiration of metal on metal joints to request manual cell counts as the metal debris can often result in faulty automated counts.
Connelly et al. performed a prospective cohort study of indications for performing metal artifact reducing sequence (MARS) MRI on patients with metal-on-metal hip resurfacing arthroplasty. They found that elevated cobalt and chromium were the strongest predictors for an adverse local tissue reaction and using 1.15 ppb of Co and 1.09 ppb for chromium as cut-offs for
performing a MARS MRI.
Yi et al. performed a retrospective study evaluating the diagnostic accuracy of serologic and synovial tests for PJI in MoM hip arthroplasty. The authors found that a high rate of inaccurate reporting of MoM aspirations, with 35% of inaccurate reports having a synovial WBC count >3000 suggesting a false positive for infection. The authors concluded that using synovial WBC >4350 and PMN >85% provided greater diagnostic sensitivity and specificity than standard MSIS criteria.
Figure A demonstrates an AP pelvis radiograph with a stable appearing right hip resurfacing arthroplasty.
Incorrect answers:
OrthoCash 2020
Compared to a cruciate retaining knee prosthesis, an anterior stabilized prosthesis has what effect on the contact area and what effect on the stability in PCL deficient knees?
Decreased contact area; increased stability
Increased contact area; increased stability
No change in contact area; no change in stability
Decreased contact area; decreased stability
Increased contact area; decreased stability Corrent answer: 2
An anterior stabilized knee prosthesis is composed of highly conformed polyethylene component with a large anterior lip, which prevents anterior translation of the femur on the tibia. The high conformity of the polyethylene component increases the contact area of the implant.
In arthroplasty, several factors can affect wear characteristics and stability at the bearing surface. Articular surfaces that are more congruous decrease the contact stresses at the surface by dispersing the joint reactive forces across a greater area. There are drawbacks to this as the articular surface is less anatomic and can prevent the natural roll back kinematics in total knee arthroplasty. New prosthesis designs with a large anterior lip formed on the bearing can be used to stabilize the knee in the absence of a functional PCL without sacrificing bone stock for the box cut and potential patellar complications.
Peters et al. performed a retrospective cohort study of total knee arthroplasty outcomes between cruciate retaining prostheses in intact PCL knees and anterior stabilized bearing prostheses in PCL deficient knees. They found that anterior stabilized bearing prostheses had similar knee society scores, radiographic alignment, component loosening, and major complications but had a significantly lower number of revisions performed. They concluded that the use of anterior stabilized bearings is an effective implant to stabilize PCL deficient knees.
Brockett et al. performed a biomechanical study that examined wear characteristics of poly-ether-ether-ketone (PEEK) and carbon fiber reinforced PEEK (CFR-PEEK) and compared to ultra-high molecular weight polyethylene (UHMWPE). It was found that PEEK had worse wear characteristics compared to UHMWPE, specifically with increasing contact pressures, decreased contact surface, and increased cross-shear. However, CFR-PEEK had similar wear performance as UHMWPE, but there were increased wear characteristics with increasing shear and contact pressure. They concluded that CFR-PEEK may be a potential alternative bearing surface in arthroplasty, but further investigation is needed to determine it's role in less conforming bearing due to the increased shearing wear.
Illustration A depicts the design of a cruciate retaining total knee prosthesis and an anterior stabilized total knee prosthesis.
Incorrect Answers:
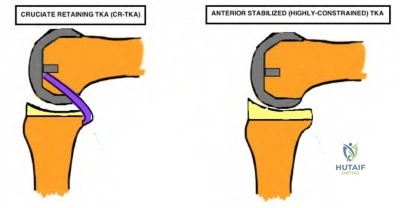
OrthoCash 2020
Resection of the posterior cruciate ligament during total knee arthroplasty simulates which of the following techniques below?
Excessive distal femur resection
Excessive distal femur augmentation
Excessive posterior femur resection
Excessive posterior femur augmentation
Oversized femoral component Corrent answer: 3
Posterior cruciate ligament (PCL) resection during total knee arthroplasty (TKA) results in a relative increase in the flexion gap compared to the extension gap. This effect simulates excessive posterior femur resection, which also results in an increased flexion gap.
The PCL acts as a central stabilizer to prevent posterior subluxation, allows femoral condyle roll back on the tibial plateau during flexion, and permits clearance of the tibia in high degrees of flexion to improve the mechanical efficiency of the extensor mechanism. The PCL may be preserved or resected during TKA. Biomechanical studies have demonstrated that after PCL resection, the flexion gap increases significantly compared with the extension gap. This has implications on gap balancing during posterior-stabilizing (PS) TKA, as the flexion gap must match the extension gap.
Park et al. performed a study to investigate the change in the medial-lateral gap in flexion and extension after PCL resection in severely deformed knees and its effect on bone resection, rotation, and size of the femoral component. They reported that after PCL resection, the flexion gap increased significantly compared with the extension gap. They concluded that PCL resection in PS-TKA designs necessitates an increase in the size of the femoral component to
balance the resulting gap mismatch.
Sierra et al. published an article on the surgical technique differences between cruciate-retaining (CR) and PS TKA designs. They reported that PCL resection selectively opens the flexion space approximately 2mm more than the extension space, resulting in some flexion instability. They recommended that in PS-TKA, surgeons must avoid flexion instability due to an extra large flexion space caused by PCL sacrifice and postoperative knee flexion contracture by underresection of the distal femur.
Incorrect Answers:
OrthoCash 2020
A 70-year-old healthy woman presents with recurrent left prosthetic hip dislocations after undergoing total hip arthroplasty 6 months ago. Workup for infection has been negative. Radiographs from her visit today are depicted in Figure A. Which of the following will most definitively prevent further dislocations?

Exchange polyethylene liner to a lipped acetabular liner
Exchange polyethylene liner to a thinner liner and increase the size of femoral head component
Cemented acetabular component revision
Uncemented acetabular component revision
Exchange polyethylene liner to a constrained acetabular liner Corrent answer: 4
This patient appears to have a significantly increased acetabular abduction (theta) angle, which places her at a high risk of periprosthetic dislocation. She should undergo revision of her malpositioned acetabular component to prevent further dislocation events.
Variables that help determine stability after total hip arthroplasty (THA) include component design, component position, soft tissue tension, and soft tissue function. The component position comprises of both femoral and acetabular implants. The recommendations are femoral component anteversion of 10-15 degrees, acetabular anteversion of 5-25 degrees, and acetabular abduction of 30-50 degrees. Excessive abduction may result in posterosuperior instability whereas inadequate abduction may result in impingement during flexion as well as inferior instability. Component malposition generally requires revision and cannot be compensated for by abductor strengthening or orthoses.
Dewal et al. retrospectively reviewed THA dislocations to determine the effectiveness of abduction bracing following closed reduction. They observed no significant differences in first-time dislocators or recurrent dislocators with or without the use of abduction braces. They concluded that abduction bracing following closed reduction of THA dislocation is ineffective in preventing re-dislocation.
McCarthy et al. performed a study to investigate cup position angles associated with impingement in a group of subjects during different activities. They reported that true acetabular target for impingement-avoidance is much smaller than previously believed and varies considerably between patients and that certain tasks including low-chair rise and squatting decrease the size of the target zone. As such, they recommended preoperative patient-specific planning and intraoperative execution for placement of the components.
Figure A depicts a THA construct with significantly increased acetabular abduction angle.
Incorrect Answers:
OrthoCash 2020
A 65-year-old woman with a history of right total hip arthroplasty presents with a fall. Her injury radiographs are depicted in Figure A. What are the fracture classification and most appropriate treatment?

Vancouver AG; nonoperative with partial weight bearing
Vancouver AG; open reduction internal fixation with trochanteric claw plate
Vancouver AG; femoral component revision
Vancouver AL; open reduction internal fixation with trochanteric cables
Vancouver B1; open reduction internal fixation with lateral locking plate Corrent answer: 2
This patient has a displaced (> 2cm) greater trochanteric periprosthetic fracture around her previous right total hip arthroplasty (THA). Her fracture is classified in the Vancouver classification as AG, and is best treated with open reduction internal fixation (ORIF) using a trochanteric claw plate.
The Vancouver hip periprosthetic classification system is one of the most useful classifications in the field of orthopaedic surgery, as it can reliably guide decision-making regarding fixation versus revision of the femoral component. Vancouver A fractures confer fractures about the femoral trochanters, with AG and AL fractures depicting greater and lesser trochanters, respectively. While nondisplaced and minimally displaced (<2cm) Vancouver AG fractures may be managed nonoperatively with protected weight-bearing, displaced AG fractures should be treated with ORIF using wires, cables, or claw plates.
Sariyilmaz et al. performed a biomechanical study to compare fixation techniques (cables, trochanteric grip plates, and locking plates) in Vancouver
type AG periprosthetic femoral fractures. They reported that locking plate versus cable fixation and grip plate fixation versus cable fixation showed statistically significant superior results in axial distraction tests. They concluded that Vancouver type AG fractures may be treated with either grip plate fixation or locking plates, with the former ensuring more stable osteosynthesis.
Masri et al. published a review article on the evaluation and management of periprosthetic fractures. They reported that the best outcome is achieved when the surgeon has a thorough understanding of the principles of treatment of periprosthetic fractures with access to various fixation and prosthetic devices. They concluded that the Vancouver classification offers a reproducible description of these factors and easily guides treatment.
Figure A depicts a displaced greater trochanteric periprosthetic fracture. Illustration A depicts the Vancouver periprosthetic hip classification system. Illustration B depicts an example of a Vancouver AG fracture treated with ORIF using a claw plate.
Incorrect Answers:
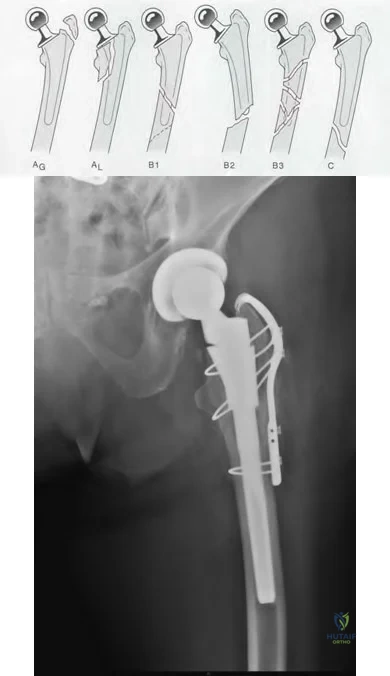
OrthoCash 2020
A 79-year-old man sustains a fall and presents with the injury depicted in Figures A and B. He underwent total knee arthroplasty (TKA) 5 days ago and had been doing well prior to his recent fall. What is the TKA implant design and what is the most appropriate treatment?
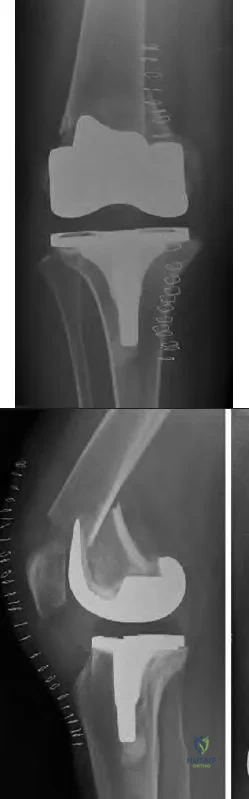
Cruciate-retaining; Open reduction internal fixation with lateral locking plate
Cruciate-retaining; Retrograde femoral nail
Cruciate-retaining; Open reduction internal fixation with medial locking plate
Posterior-stabilized; Open reduction internal fixation with lateral locking plate
Posterior-stabilized; Femoral component revision Corrent answer: 4
The TKA prosthesis in question is a posterior-stabilized (PS) design. Open reduction and internal fixation (ORIF) with a lateral locking plate is a viable treatment option for a periprosthetic femur fracture around the femoral component of a well-fixed PS TKA.
Femoral periprosthetic fractures after TKA may occur following low-energy trauma in osteopenic bone. Nondisplaced fractures with a stable prosthesis may be treated nonoperatively in a cast or brace. The decision for revision of the femoral component is guided by component stability versus loosening, with ORIF and revision arthroplasty indicated, respectively. ORIF options include locked femoral plating or retrograde intramedullary nailing (IMN).
Retrograde IMN is not a viable option for stemmed femoral prosthesis and posterior-stabilized (PS) TKA systems without an open box design.
Haidukewych et al. published an instructional course lecture on periprosthetic
fractures of the hip and knee. They reported internal fixation is indicated for the majority of periprosthetic distal femoral fractures. Both locked plates and retrograde IMNs can provide good outcomes, and that revision arthroplasty is indicated in fractures around loose components, nonunions, or fractures for which internal fixation attempts are likely to fail.
Su et al. published a review on periprosthetic femoral fractures above total knee replacements. They reported that periprosthetic femoral fractures above TKAs can be managed by a variety of methods, including casting, ORIF, external fixation, or revision arthroplasty. They highlighted that classification based on fracture location helps guide treatment. They concluded that IMNs are best for proximal fractures, fixed-angle devices for fractures originating at the component, and revision arthroplasty for very distal fractures or those with component loosening.
Figures A and B depict a periprosthetic femoral fracture originating at the anterior flange of the femoral component of a PS-TKA. Illustrations A and B depict radiographs of the periprosthetic femur fracture after ORIF with a lateral locking plate.
Incorrect Answers:

OrthoCash 2020
A 67-year-old woman presents with chronic right hip pain, exacerbated by long walks. She has limited hip range of motion, particularly in flexion and internal rotation. Radiographs are depicted in Figure A. This is her first time seeking treatment. What is the mechanism of action of a medication strongly recommended for short-term pain relief according to the most recent (2013) AAOS Clinical Practice Guidelines?

Direct action on hypothalamic regulating center with anti-pyretic effects
Binds to cannabinoid receptors in neural tissues
Binds directly to nuclear receptors to interrupt the inflammatory and immune cascade via mRNA changes
Maintains synovial fluid viscosity and supports articular cartilage shock absorption
Inhibits sodium ion channels to inhibit sensory nerve impulse initiation and conduction
This patient presents with right hip osteoarthritis. In the 2013 AAOS Clinical Practice Guidelines (CPG), intraarticular corticosteroids usage in improving function and pain reduction in the short-term for patients with symptomatic osteoarthritis of the hip was strongly recommended. Corticosteroids function by direct binding to nuclear steroid receptors to interrupt the inflammatory cascade through mRNA changes.
The 2013 AAOS CPG for the treatment of symptomatic arthritis discuss both operative and non-operative treatment options and scrutinizes the literature for each modality. Amongst the strong recommendations are weight loss, low impact physical activity, and non-narcotic analgesia including nonsteroidal anti-inflammatory drugs (NSAIDs). Numerous modalities were not supported including the use of prescription opioids, acupuncture, needle lavage, hyaluronic acid, glucosamine and chondroitin, and arthroscopic lavage.
Dieppe et al. published a review article on the management of hip osteoarthritis. They reported that shock absorbing shoe insoles and walking sticks can be of great benefit, while physiotherapy and hydrotherapy should be considered for more severe cases. They recommended simple analgesics such as paracetamol and NSAIDs as first-line treatment, with joint replacement considered in patients with severe pain or disability.
Quinn et al. published a review article on the management of hip osteoarthritis using the AAOS Appropriate Use Criteria (AUC). Evidence-based information, in conjunction with the clinical expertise of physicians, was used to develop the criteria to improve patient care and obtain the best outcomes while considering the subtleties and distinctions necessary in making clinical decisions.
Figure A depicts right hip osteoarthritis with evidence osteophytes, narrowed joint space, and subchondral sclerosis.
Incorrect Answers:
OrthoCash 2020
A 70-year-old man presents with chronic persistent right knee pain and erythema which has been present for 7 weeks after having undergone total knee arthroplasty (TKA) 7 years ago. He is referred after completing a course of oral antibiotics prescribed by his primary care physician, which did not improve his symptoms. His current radiograph is shown in Figure A. Laboratory testing reveals a serum C-reactive protein (CRP) of 50mg/L and an erythrocyte sedimentation rate (ESR) of 67 mm/h. Arthrocentesis is performed and reveals a synovial WBC of 1,500 WBC/uL, with 85% polymorphonuclear cells (PMNs), and negative final cultures. The alpha-defensin test is positive. What is the next best step?

Repeat knee arthrocentesis after 2-week antibiotic holiday
Revision of femoral component without antibiotic therapy
One-stage revision arthroplasty with intravenous antibiotic therapy for 4-6 weeks
Two-stage revision arthroplasty with intravenous antibiotic therapy for 4-6 weeks
Revision of tibial component without antibiotic therapy
Based on the 2018 revised Musculoskeletal Infection Sociecty (MSIS) criteria, the elevated ESR, serum CRP, positive alpha defensin, and elevated PMNs convey a score of 1, 2, 3, and 2, respectively, for a combined score >6. This is diagnostic of a chronic prosthetic joint infection (PJI), for the most supported management strategy is two-stage revision arthroplasty with intravenous (IV) antibiotic therapy for 4-6 weeks.
PJI after TKA is estimated to be 2.5%. The chronicity of the infection determines management. Non-MRSA PJI within 4 weeks of surgery is considered acute and may be treated with irrigation, debridement, polyethylene exchange, component retention, and IV antibiotics, as the organism has purportedly had too little time to form a robust biofilm. PJI occurring more than 4 weeks after TKA is considered chronic and, due to a high likelihood of biofilm formation, requires two-stage revision arthroplasty with IV antibiotic therapy.
Ting et al. reviewed an algorithm-based approach for diagnosis of PJI. They reported that the diagnosis of PJI is made in 90% of patients by ESR and CRP, followed by arthrocentesis if the results are high, with a focus on synovial WBC count, differential, and cultures.
Everhart et al. developed and validated a preoperative surgical site infection (SSI) risk score for primary or revision TKA and hip arthroplasty (THA). They reported that patient comorbidities composing the risk significantly influence SSI risk for primary or revision TKA and THA. They concluded that preoperative SSI risk can be objectively determined by the proposed SSI risk score.
Parvizi et al. most recently presented the 2018 updated MSIS evidence-based criteria for diagnosis of periprosthetic hip and knee infections (Illustration A). The authors updated the original crtieria, expanding and refining the contributions from each of the minor criteria. The authors supported that a score >6 was diagnostic of periprosthetic infection. They concluded that this criteria was 97.7% sensitive and 99.5% specific for diagnosis of prosthetic joint infection.
Figures and Illustrations:
Figure A shows the AP and lateral radiographs of a TKA prosthesis with evidence of osteolysis and marked loosening of the femoral and tibial components.
Illustration A is the updated 2018 MSIS criteria for diagnosis of a PJI.
Incorrect Answers:
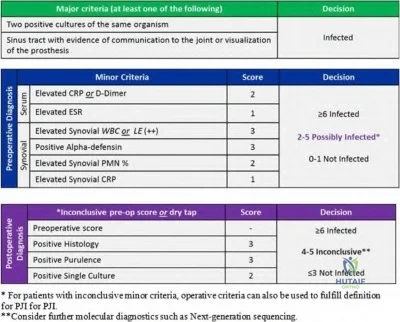
OrthoCash 2020
Figure A depicts the intraoperative findings during a revision total hip arthroplasty (THA) in a patient with chronic pain for the last two years after undergoing his index THA 10 years ago. Workup for infection was negative. The acetabular and femoral components are assessed to be well-fixed intraoperatively. Which of the following describes the best treatment option?
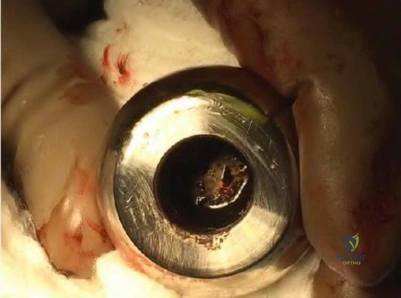
Suppressive intravenous antibiotics
Two-stage revision arthroplasty
Irrigation and debridement
Acetabular component revision
Revision to new ceramic femoral head with titanium sleeve Corrent answer: 5
This patient's symptoms and intraoperative image are consistent with trunnionosis. As the components appear well-fixed, the best treatment is a revision to a ceramic head with a titanium sleeve.
Metal-on-metal (MoM) total hip arthroplasty (THA) has been associated with complications from metal debris and toxicity. Although morse taper technology allows machined taper trunnion to fit with the femoral head, complications have been reported including corrosion at the trunnion, which results in pain and is often associated with adverse local tissue reactions (ALTR). During revision surgery, a ceramic head with a titanium sleeve adaptor is advocated, as an exchange of the metal femoral head to another metal femoral head may result in recurrence of ALTR. Lastly, while no cutoffs for serum cobalt chromium ion levels have been identified as pathognomonic for trunnion corrosion, a serum cobalt level of 1.6 ng/mL (ppb) and greater has been suggested as a threshold for mechanically-assisted crevice corrosion.
Weiser et al. published a current concepts review of trunnionosis in THA. They stated that the complication of trunnionosis in THA is likely underreported since it often causes concurrent osteolysis and loosening, which are more universally accepted diagnoses. They recommended analysis of serum cobalt and chromium ions as well as metal artifact reduction MRI during workup. In revision surgery, they advocated for head and liner exchange, with retention
of the acetabular and femoral components.
Raju et al. published a case series on trunnionosis in metal-on-polyethylene (MoP)THA. They reported three failures (two dissociations of the femoral head from the neck), with the most likely contributing factors to failure being a large femoral head size, high horizontal offset, a low angled neck, and a titanium alloy taper with a cobalt-chromium head. They recommended high vigilance for any alteration of alignment between the femoral head and neck in follow-up radiographs after THA.
Figure A is an intraoperative image depicting severe corrosion at the trunnion in a metal-on-metal THA.
Incorrect Answers:
OrthoCash 2020
Figure A depicts the current radiograph of a 66-year-old man with significant right groin pain after undergoing right total hip arthroplasty (THA) 10 years ago. Revision surgery is planned after infection workup is negative. What is the classification of his diagnosis and what would the most appropriate treatment for the acetabulum?

Paprosky I; cementless hemispheric cup with screw fixation
Paprosky I; cemented hemispheric cup without screw fixation
Paprosky IIB; cementless hemispheric cup with screw fixation
Paprosky IIIA; cup/cage construct
Paprosky IIIA; triflange reconstruction Corrent answer: 3
This patient demonstrates superior acetabular rim loss and superolateral migration that can be characterized as Paprosky IIB in the Paprosky classification for acetabular bone loss. This may be managed with a hemispheric acetabular cup with screw fixation.
Acetabular bone loss poses a technical challenge in THA. The Paprosky classification for acetabular bone loss helps guide treatment for revision THA. Broadly speaking, Paprosky Type I and II defects may be managed with a porous-coated hemisphere cup secured with screws, and Type III defects managed with reconstruction cages protected with cups, structural augments, or custom triflange implants.
Sheth et al. published a review article on the evaluation and management of acetabular bone loss in revision THA. They reported that appropriate radiographs are key in quantifying acetabular bone loss, and specific classification schemes can assist in identifying bone loss patterns which guide available treatment options. They concluded that depending on the severity of bone loss, treatment may include impaction grafting and acetabular cementation, cementless hemispheric acetabular reconstruction, structural allograft reconstruction, cementless reconstruction with modular porous metal
augments, ring and cage reconstruction, cup-cage reconstruction, and triflange reconstruction.
Paprosky et al. performed a 6-year follow up evaluation study on acetabular defect classification and surgical reconstruction in revision THA. They typed acetabular defects from 1 to 3 and reconstructed with bulk or support allograft depending on the type. They concluded that the size, orientation, and method of fixation of the allografts utilized during revision THA play a pivotal role in the integrity of structural allografts, and stressed the importance of adequate host-bone to ensure solid bone ingrowth.
Dennis et al. published on the outcomes after Paprosky Type III acetabular bone loss reconstructed using custom triflanged acetabular components. They reported stable fixation and reconstruction of periacetabular bone in over 80% of patients at short-term follow up. They recommended that this technique be used with caution in cases of preoperative hemipelvis dissociation unless additional column plating is performed.
Figure A demonstrates Paprosky IIB acetabular bone loss with superolateral migration of the acetabular component. Illustration A depicts the Paprosky classification.
Incorrect Answers:
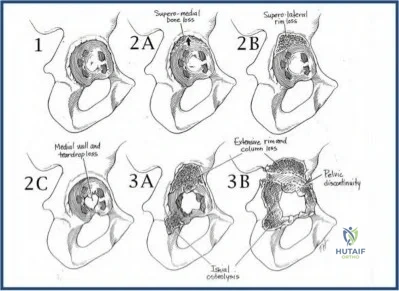
OrthoCash 2020
A 72-year-old male presents with worsening left hip pain 12 years after total hip arthroplasty. On examination, the patient has a Trendelenburg gait with a 3.5 cm leg length discrepancy. The patient denies any fevers or chills. Current radiographs are shown in figure A. Recent ESR and CRP are 21 mm/hr and 1.2 mg/L, respectively. What is the preferred treatment option to address these findings?
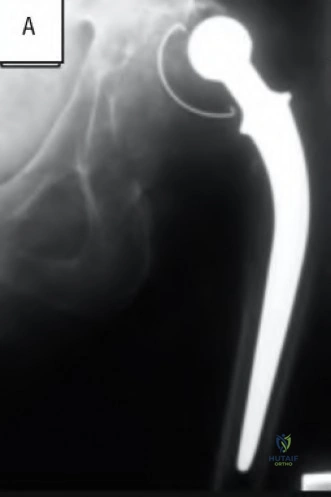
Large porous hemispheric cup with particulate bone graft and augmented with screw fixation
Custom triflanged acetabular component
Cemented large porous hemispheric cup
Metal augments with large porous hemispheric cup and bone grafting combined with screw augmentation
stage revision arthroplasty Corrent answer: 4
The patient is presenting with a Paprosky type IIIA acetabular defect with the migration of the hip center in a superolateral direction. The preferred treatment option would be to provide structural stability of the cup with metal augments combined with bone grafting and cement reinforcement and screw fixation.
Acetabular bone loss can make revision total hip arthroplasty challenging due to lack of structural support of the acetabular cup as well as concerns for bony ingrowth potentially compromising implant longevity. The Paprosky classification was designed to identify the location and degree of acetabular bone loss and thereby to guide treatment of the respective defects. In type IIIA defects there is bone loss of the superolateral acetabulum with greater than 3 cm migration of the center of the femoral head, also described as "up and out." Intraoperatively structural support must be reestablished for the revision cup by either structural allograft or metal augments. Further bone grafting is performed to enhance long term bone ingrowth of the prosthesis.
Sheth et al. performed a literature review on the evaluation and management of acetabular bone loss in revision total hip arthroplasty. The authors reviewed the Paprosky classification for acetabular bone loss and recommended the use of noncemented, porous-coated, hemispheric cups with adjunctive screw fixation in type I, IIA, and IIB defects. For type IIC defects, the authors recommended highly porous, noncemented, hemispheric cups with screw fixation and bone grafting of the medial wall defect. For type IIIA defects, they advocated for the use of metal augments or structural allograft combined with porous hemispheric cups and augmentation with screw fixation and cement.
Lastly, for type IIIB defects, they recommended the use of noncemented acetabular devices combined with structural allograft, structural augments, and a reconstruction cage.
Paprosky et al. performed a retrospective study of patients undergoing revision total hip arthroplasty and proposed a classification system of acetabular bone loss, recommending treatment options for each type. The authors found that of the 147 implants included in the study, only 6 required repeat revision, all of which were type IIIB defects. The authors concluded that adherence to this classification system and the recommended reconstruction techniques can produce acceptable and predictable results in acetabular revision surgery.
Dennis et al. performed a retrospective review of twenty-four patients with Paprosky type IIIB acetabular defects treated with a custom triflanged acetabular component (CTAC). The authors found that of the twenty-four patients treated, three (87.5%) were considered to have radiographic and clinical signs of failure, with one requiring resection arthroplasty. There were two hip dislocations necessitating only closed reduction. The authors concluded that CTAC is an effective means to treat type IIIB acetabular defects, but should be used with caution in cases of pelvic discontinuity unless additional column plating performed.
Figure A is the AP radiograph of a pelvis with a Paprosky type IIIA acetabular defect. Illustration A is the post-op radiograph after reconstruction with metal augments and large porous hemispheric cup. Illustration B is a table with the description of the Paprosky classification. Illustration C is a diagram depicting the Paprosky classification.
Incorrect Answers:
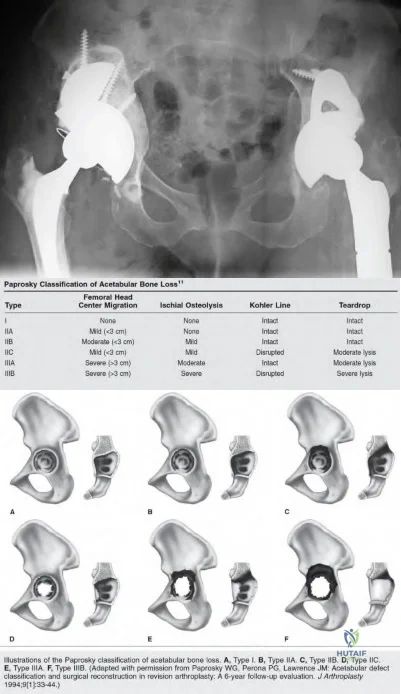
OrthoCash 2020
A 67-year-old woman with poliomyelitis presents with quadriceps weakness and chronic right knee pain for the last 2 years. She is scheduled to undergo right total knee arthroplasty (TKA) after failing nonoperative modalities. Her preoperative radiographs are shown in Figures A and B. What technique should be utilized to optimize her function and to prevent the recurrence of her deformity?
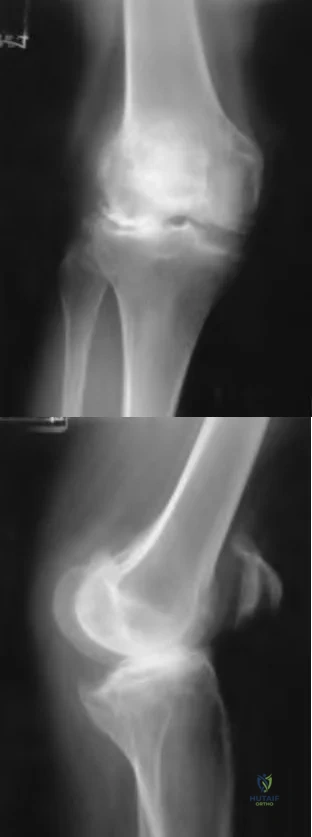
Posterior stabilized design with under-resection of distal femur
Posterior stabilized design with under-resection of proximal tibia
Posterior stabilized design with under-resection of posterior femur
Varus-valgus constrained design
Rotating hinge design
This patient with neuromuscular disease has genu valgum with recurvatum (hyperextension). Of the techniques listed above, utilization of a rotating hinge TKA design would most likely optimize her function and prevent recurrence of her recurvatum deformity because of the implant’s extension stop.
Genu recurvatum is associated with deformities such as genu valgum, ligamentous laxity, and neuromuscular diseases, which are often accompanied by equinus ankle contractures. Knee hyperextension is likely to recur after TKA in patients with neuromuscular disorders such as poliomyelitis due to the bony deformity, muscle weakness, and paralysis seen in these patients. Several strategies to correct knee hyperextension at the time of primary TKA have been described and include posterior capsular plication, proximal and posterior transfer of collateral ligaments, under-resection of distal femur and proximal tibia, and the use of thicker components. In severe cases where ligament integrity is likely compromised, utilization of more constrained prostheses is recommended.
Giori et al. performed a retrospective study of patients with poliomyelitis involving a limb that underwent primary TKA. Complications reported included two periprosthetic fractures, one peroneal nerve palsy, one patellar tendon avulsion, and four cases of recurrent instability, all attributable to the poor bone quality, valgus deformity, patella baja, poor musculature, and attenuated soft tissues observed in knees with poliomyelitis. They concluded that pain and knee scores improved following TKA this cohort of patients and recurrence of instability and progressive functional deterioration is possible postoperatively.
Paratte et al. published an AAOS Instructional Course Lecture on instability after TKA. They reported knee hyperextension before TKA is seen in <1% of patients and is most commonly seen in patients with neuromuscular disease like poliomyelitis. They recommended solutions to be considered for such patients such as distal femur under-resection, distal femoral augmentation blocks with the knee left with a slight flexion contracture, translation of the femoral origins of the medial collateral ligament and lateral collateral ligaments proximally and posteriorly to recreate the normal tightening action during full extension of the knee, and the use of a rotating-hinge total knee prosthesis with an extension stop.
Meding et al. published a review article on the etiology and surgical treatment of genu recurvatum during TKA. They emphasized the importance of diagnosing and elucidating the etiology of the hyperextension deformity prior to surgery since the deformity is known to recur in patients with certain neuromuscular disorders. They recommended a meticulous approach and
avoiding even mild degrees of residual instability in the coronal plane at surgery since this is associated with increased extension in the postoperative period.
Figures A and B depict severe right knee osteoarthritis with valgus and recurvatum deformities. Illustration A depicts a rotating-hinge TKA prosthesis.
Incorrect Answers:

OrthoCash 2020
A 57-year-old man with a history of chronic lower back pain and right hip arthritis is postoperative day 2 from an uncomplicated right total hip arthroplasty with a spinal block. Since the procedure, he has reported persistent pain in his right leg with a focal point in the proximal lateral leg. He has had difficulty getting out of bed for physical therapy due to pain reproduced in his leg. He is voiding but has not yet had a bowel movement. Physical exam is only significant for decreased ankle dorsiflexion strength on the right. Plantarflexion strength remains 5/5 bilaterally. No point tenderness was elicited and Homan's sign is negative. His wound is unremarkable with typical post-operative swelling of the leg and no significant drainage. He has
been receiving ASA 81mg PO daily since surgery and has been wearing compression stockings full-time. Postoperative repeat radiographs of the hip are unremarkable and his hemoglobin is stable. Which of the
following etiologies is most likely responsible for this patient's symptoms?
Residual effect of the spinal block
Lumbar lateral recess stenosis
Gluteal hematoma
Acute post-operative infection
Venous thomboembolism
During total hip arthroplasty, a "double crush" injury can occur to the sciatic nerve in the presence of pre-existing degenerative lumbar spondylosis, leading to persistent pain and post-operative motor weakness. The best study would be a lumbar MRI to evaluate for lumbar spinal stenosis.
Nerve injuries following total hip arthroplasty are rare and usually affect the sciatic nerve. The peroneal branch appears to be the most commonly affected due to its more superficial and lateral position, more the tightly packed fascicles, and greater adherence to the surrounding tissues compared to the tibial division. Lumbar degenerative disc disease commonly occurs in the presence of coxarthrosis, with spinal stenosis being exacerbated by traction neurapraxia during the procedure.
DeHart et al. reviewed nerve injuries and postoperative management. The authors stated that the sciatic nerve is the most commonly injured nerve, with up to 70% of cases have subclinical electrodiagnostic changes. The cause of this is multifactorial, but the vast majority of studies reviewed reported complete spontaneous recovery by 6-12 months. The authors recommend observation of the nerve deficit with ankle-foot-orthosis and follow-up EMG to determine the level of the injury.
Pritchett performed a review of 21 patients that presented with a foot drop after total hip arthroplasty. All patients reported prior back and leg pain prior to the procedure, with post-op MRI demonstrating severe spinal stenosis. The author postulated there to be a double crush phenomenon, with patients undergoing lumbar laminectomy having improvement or complete resolution. The author concluded that select patients presenting with foot drop following THA may benefit from a lumbar laminectomy.
Incorrect Answers:
and paresthesias are uncommon after a spinal block but have been reported with regional anesthesia, such as a sciatic nerve block. Furthermore a spinal would be unlikely to have any residual effect still post-operative day 2.
OrthoCash 2020
A 65-year-old female presents to the clinic with isolated medial-sided left knee pain. She has since exhausted conservative management but remains persistently symptomatic. The physical exam and radiographic work-up demonstrates isolated medial tibiofemoral compartment involvement. After discussion of the surgical options, she undergoes the procedure shown in Figure A. She initially does well but returns to clinic 3 months post-operatively with significantly increased medial-sided knee pain and the injury shown in Figure B. All of the following technical errors likely contributed to this complication EXCEPT?

Excessive force impacting the tibial component
Penetration of the posterior tibial cortex with proximal guide pin
Placement of a peripheral medial cortical guide pin
Tibial resection guide replacement with re-drilling of the two proximal guide holes
Under-sizing of the tibial component Corrent answer: 1
The patient presents with a periprosthetic tibial stress fracture following a medial unicompartmental knee arthroplasty. Excessive force used when impacting the tibial component could potentially lead to intra-operative fracture, but this would be recognized in the acute post-operative period.
With continuing advances in surgical technique, UKA has demonstrated increasingly promising midterm outcomes. However, there are number of technical considerations that directly impact survivorship and the potential for post-operative complications. While aseptic loosening remains the most common mode of early failure necessitating conversion to TKA, literature is replete with reports of early failure secondary to proximal tibia stress fractures. Stress fractures have been linked to a number of largely non-modifiable patient characteristics to include bone quality, but technical errors remain a controllable contributing factor. Recent studies have found that excessive guide pin number and suboptimal placement for the tibial resection guide as well as tibial component undersizing are associated with increased proximal tibial mechanical stress and may result in fracture.
Brumby et al. described a series of tibial plateau stress fractures subsequent to UKA. The authors attributed these to mechanical weakening of the proximal tibia from the guide pin and lug holes drilled for the guide and tibial component, respectively. They noted that this even occurred in some cases with penetration of the medial tibial cortex by a single pin. Stress fractures presented at a median of 8 weeks post-operatively and in all cases required revision to TKA. They recommended post-operative monitoring of patients in whom a guide with 3 or more pins was utilized, or with any peripheral pins that breach the medial tibial cortex.
Vince et al. present a review of the evolution, indications, and outcomes following UKA. The authors specifically highlight guide pin holes as a major contributing factor to periprosthetic fractures. They recommend limiting the number of holes drilled for placement of the tibial resection guides and paying careful attention to placement, specifically with regard to violation of the medial cortex. Furthermore, the authors advocated that a single proximal pin, placed centrally, and the guide secured distally by the ankle clamp would be
sufficient for stability and alignment while avoiding increased stress on the proximal tibia.
Figure A is an AP weight-bearing radiograph of the left knee demonstrating isolated medial tibiofemoral arthritis.
Figure B is a post-operative radiograph of the left knee significant for a medial UKA. Figure C is a follow-up AP radiograph of the left knee demonstrating a periprosthetic fracture involving the medial UKA with significant varus collapse.
Incorrect answers:
OrthoCash 2020
A 65-year-old male presents to your clinic for evaluation of right hip pain. He underwent a right total hip arthroplasty (THA) 20 years prior and was doing very well until 2 years ago. He admits to groin pain when getting up from a seated position. He denies any fevers or chills. Radiograph is shown in Figure A. Which of the following would preclude the patient from undergoing a single-stage surgical intervention without further workup?

Elevated serum cobalt
Metallosis noted intra-operatively
Significantly higher serum cobalt then serum chrome levels
Elevated ESR and CRP
Pseudotumor noted on MRI Corrent answer: 4
An elevated ESR and CRP are screening labs used to determine if further workup is required to rule out a periprosthetic joint infection (PJI). A patient with an elevated ESR and CRP should thus undergo further workup including a joint aspiration prior to consideration of a single-stage revision THA.
The differential diagnosis of pain after THA encompasses a number of etiologies. While radiographs may point to loosening of the stem or the cup, osteolysis or a stress fracture, the first step in management needs to evaluate for a PJI. Accordingly, ESR and CRP are logical next screening steps in the workup. If elevated, additional studies need to be obtained such as joint aspiration with manual diff (to look for elevated synovial WBC, synovial PMNs or a positive culture), immunoassays (alpha-defensive, leukocyte esterase colorimetric strip) and serum IL-6. If the additional workup for infection is negative, it is safe to proceed with a single-stage revision THA. Metal on metal THA have their own set of modes of failure leading to bony erosion and pain.
The majority of these are aseptic and allow for a single-stage revision including metallosis, pseudotumor, and metal hypersensitivity.
Parvizi et al. performed a retrospective cohort study to examine the effectiveness of surgical treatment in treating hip and knee PJI caused by MRSA. They looked at 127 patients with a minimum of 2 years follow-up or until recurrence of PJI. In 35 patients, only an I&D with prosthetic retention was performed while a 2 stage explantation and reimplantation was performed in the other 92 patients. Of those who underwent an I&D and implant retention, only 37% of cases had successful eradication of the infection
whereas two-stage exchange arthroplasty controlled the infection in 75% of hips and 60% of knees in the other 92 patients. Furthermore, cardiac disease was associated with a higher likelihood of failure to control infection in all treatment groups.
Shukla et al. evaluated 87 hips with a PJI that were treated with explantation, antibiotic spacer and 6 weeks of antibiotics. The authors looked at ESR and CRP before reimplantation and obtained synovial WBC at the time of reimplantation. The authors noted 9 hips (10.1%) had persistent infections at the time of re-implantation. The mean ESR, CRP, and synovial fluid WBC count had significantly decreased between stages; however, the ESR remained elevated in 50 patients (62.5%) and the CRP remained elevated in 22 patients (27.5%) in whom the infection had been eradicated. The authors noted that the synovial fluid WBC count was the best test for identifying persistent infection, with an optimum cutoff of 3528 WBCs/microL (sensitivity, 78%; specificity, 96%).
Browne et al. evaluated 37 patients with metal on metal THA or resurfacing arthroplasties who underwent revision to determine the clinical, radiographic, laboratory, intraoperative, and histopathologic findings to determine the cause of failure. Of the 37 patients, 10 were revised due to metal on metal hypersensitivity, 8 due to chronic inflammation with lymphocytic infiltration, 8 with aseptic loosening, 2 with iliopsoas impingement, 3 with femoral neck fracture after resurfacing arthroplasty and 6 due to infection, instability, and periprosthetic fracture. The authors stressed increased awareness of the wide variety of modes of failure associated with metal-on-metal articulations.
Figure A is an AP pelvis showing a characteristic appearance of a metal-on-metal THA with a large femoral head.
Incorrect Answers:
OrthoCash 2020
The use of a high-offset femoral stem leads to which of the following changes with regard to total hip arthroplasty?
Increased joint reactive forces
Increased leg length
Increased risk of acetabular component loosening
Increased soft tissue tension
A higher rate of dislocation Corrent answer: 4
A high-offset femoral stem leads to increased soft tissue tension without affecting leg length.
Femoral offset is defined as the distance from the femoral head center of rotation to the center of the long axis of the femur. Restoration of offset improves overall arthroplasty biomechanics with decreased cup strain and polyethylene wear, decreased dislocation risk, increased hip abductor strength, and lower rates of postoperative limp. The drawback of too much femoral offset is an increased risk of lateral prominence and subsequent trochanteric bursitis.
Lecerf et al. reviewed the femoral offset with regard to total hip arthroplasty. They state femoral offset does correlate closely with the hip abductor lever arm and hip abductor strength. They conclude that femoral offset is important for improved hip function and longevity after total hip arthroplasty.
Flecher et al. reviewed limb lengthening as it pertains to total hip arthroplasty. They discuss methods of assessing limb length including EOS and CT imaging as well as intraoperative robotic or computer assistance. They comment that the expectations of limb function after total hip make it crucial for surgeons to understand the three-dimensional geometry and placement of prostheses.
Illustration A shows an example of a standard and high offset stem and how it maintains leg length while increasing offset.
Incorrect Answers:

OrthoCash 2020
You are currently evaluating a 68-year-old woman who has met indications for a total knee arthroplasty. You finally have finished documenting the patient’s extensively detailed social and family history. As you finish, the patient tells you that she has spoken with her friends regarding her knee and tells you that she wants a prescription for preoperative physical therapy, would like a drain placed, an order for a cryotherapy device and use of a patient-controlled analgesia (PCA), in addition to being mobilized with physical therapy on the day of surgery. As an astute resident you inform the patient that based on the current AAOS clinical practice guidelines (CPG), there is strong evidence against using which of the patient’s request?
Preoperative physical therapy
Drain placement
Cryotherapy device
Postoperative day 0 mobilization
Patient-controlled analgesia
Based on the most recently published AAOS CPG, there is strong evidence to support not using a drain with total knee arthroplasty (TKA) because there is not any difference in complications or outcomes.
The use of a drain was postulated to aid in decreasing postoperative infection, swelling, blood transfusions, hematoma formation, pain, length of hospital stay, and re-operation rates. In addition, their use was meant to improve
postoperative range of motion. However, after review of the high- and moderate-quality studies and with input from the multiple orthopaedic and medical societies, there has not been any clear advantage to the use of drains after unilateral total knee arthroplasty when comparing complication profiles and outcomes.
McGrory et al. published a systematic review on the surgical management of osteoarthritis of the knee. In an effort to improve the surgical management of patients with osteoarthritis, the authors provide 38 evidence-based recommendations on topics specific to the preoperative, perioperative and postoperative treatment of such patients. Additionally, each topic was further classified based on the level of evidence available (limited, moderate, and strong) to support or not support a give recommendation.
MacDonald et al. completed a prospective randomized clinical trial using continuous passive motion (CPM) following TKA. The patients were separated into two separate treatment groups plus a control group. The patients were followed over the course of one year from surgery. Similar to postoperative drain placement following TKA, MacDonald et al. were unable to demonstrate any significant difference in outcomes for CPM versus no CPM.
Incorrect Answers:
OrthoCash 2020
Figure A is the radiograph of a male who fell down the stairs. He is 8 years status post right total hip arthroplasty. All of the following are indications for a proximal femoral replacement EXCEPT?

<4cm of diaphyseal cortical bone
Age <50 years
Extensive metadiaphyseal proximal bone loss with <4cm of intact isthmic bone
Nonunion of the proximal femur with multiple failed attempts at osteosynthesis
Paprosky IV femoral bone loss Corrent answer: 2
The radiograph demonstrates a Paprosky type IV femoral deficiency. Given the substantial bone loss with limited proximal femoral support, a proximal femoral replacement is recommended.
Postoperative fractures around a total hip prosthesis has an incidence of 0.1% and occurs most commonly at the tip of the stem. Proximal femoral support is important to evaluate following a periprosthetic fracture of the hip. The Paprosky classification of femoral bone loss helps guide treatment. A Paprosky type IIIb or IV femoral deficiency would benefit from either an allograft prosthetic component or a megaprosthesis/modular oncology component.
Additionally, impaction bone grafting is indicated with a large canal and thin cortices for Paprosky IIIb and IV defects. Revising the femur to a proximal
femoral replacement would allow early mobility and provide better fixation, given the substantial bone loss for proximal support and is typically reserved for the elderly or sedentary patient.
Parvizi et al. review the use of a proximal femoral replacement (megaprosthesis) in revision hip surgery. They report that with the increased use of cortical strut grafts to augment host bone, the indications for the use of megaprostheses have narrowed. They conclude that currently, the use of megaprostheses is reserved for elderly or sedentary patients with massive proximal femoral bone loss that cannot be reconstructed by other reconstructive procedures.
Brown et al. tests the inter-observer and intra-observer reliability of this Paprosky classification of femoral bone loss. They report an inter-observer reliability of 0.61, indicating substantial agreement between surgeons. They also show a high intra-observer reliability, indicating substantial to almost perfect agreement. They conclude that there is substantial agreement among experienced arthroplasty surgeons when using the Paprosky Classification to characterize femoral bone loss.
Figure A is the AP radiograph of the right hip which demonstrates a Paprosky type IV femoral deficiency. Illustration A is the Paprosky classification of proximal femoral bone loss.
Incorrect Answers:
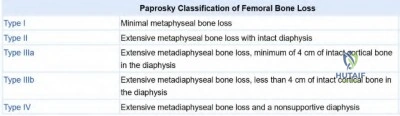
OrthoCash 2020
A healthy, active, 65-year-old male underwent a total knee arthroplasty 1 year ago. He presents to the emergency room after a ground-level fall earlier in the day. On exam, the patient is unable to perform a straight leg raise. Figure A is his current lateral radiograph. What is the most appropriate treatment for this patient?

Immediate active and passive range of motion in a hinged brace
Immobilization for 2 weeks followed by aggressive physical therapy
Cylinder cast for 6 weeks
Open Reduction Internal Fixation
Partial patellectomy
This patient has a displaced patella fracture with a disrupted extensor mechanism; therefore, (4) open reduction internal fixation is the correct answer.
Risk factors for patella fracture following total knee arthroplasty include trauma, the performance of a lateral release, damage to the blood supply, and excessive resection at the time of resurfacing. Indication for non-operative management includes both implant stability and extensor mechanism competency. If the implant is unstable or the extensor mechanism is disrupted a variety of surgical options exist including open reduction internal fixation (ORIF), component revision, partial or complete patellectomy or extensor mechanism allograft.
Konan et al. reviewed the management of periprosthetic total knee fractures. They report that non-operative treatment for periprosthetic patella fractures with an intact extensor mechanism leads to better outcomes when compared to surgery. Surgery is associated with high complication rates, including infection and nonunion. They conclude that regardless of the treatment employed, the goal should be early patient mobilization.
Kuyzk et al. reviewed the management of periprosthetic total knee fractures. They note that periprosthetic patella fractures are the least common type of fracture in this population. Their review concludes that host bone stock is one of the most important factors when determining the revision implant type.
Figure A demonstrates a displaced patella fracture in a patient with a previous total knee arthroplasty.
Incorrect answers
OrthoCash 2020
A 91-year-old, minimally ambulatory male presents with acute on chronic progressive right thigh pain. Fifteen years ago, he underwent a right total hip replacement and he had been having progressive thigh start-up pain over the prior 5 months. He sustained a ground-level fall yesterday and he is now unable to bear any weight on the right leg. His current radiograph is shown in Figure A. His labs, including CBC, ESR, and CRP are all within normal limits. Which of the following represents the most appropriate next step in definitive management?

Revision to a proximal femoral replacement
Open reduction and internal fixation with proximal femoral locking plate and cerclage cables
Revision to a cemented long femoral stem
Open reduction and internal fixation with iliac crest bone grafting
Revision to a cementless long porous-coated femoral stem Corrent answer: 1
The patient has a Vancouver B3 periprosthetic femur fracture and requires revision. Given the extensive amount of bone loss in the proximal segment as well as a loose stem, a proximal femoral replacement would be an appropriate treatment
Post-operative periprosthetic femur fractures are classified based on the Vancouver classification which classifies fractures based on the location of the fracture, implant stability, and bone loss. Vancouver B3 periprosthetic femur fractures are defined as fractures at, around, or just below the stem with significant proximal bone loss/osteopenia or comminution which is unable to allow for reconstruction. In the setting of these injuries, treatment would consist of endoprosthetic proximal femur replacement or replacement with a large proximal femur allograft.
Della Valle et al. discuss the challenges associated with pre-operative planning for femoral revision total hip arthroplasty. The authors provide a classification of femoral bone loss that guides the surgeon in selecting an appropriate method of reconstruction. They conclude that appropriate pre-operative planning is required for the management of femoral implant revision in the setting of fracture, osteolysis, and instability.
Brown et al. reviewed the indications for revision THA to include instability, aseptic loosening, osteolysis, infection, periprosthetic fracture, component malposition, and catastrophic implant failure. They note that femoral component revision presents a complex challenge to the arthroplasty surgeon because of modern implant design as well as bone loss in the proximal femur. They conclude that knowledge of various reconstructive options and the indications for each is necessary to achieve a successful outcome.
Figure A is the radiograph of a periprosthetic femur fracture with extensive proximal femoral bone loss consistent with a Vancouver B3 periprosthetic femur fracture. Illustrations A and B are the radiographs revealing a revision total hip arthroplasty with proximal femur endoprosthetic reconstruction.
Incorrect Answers:
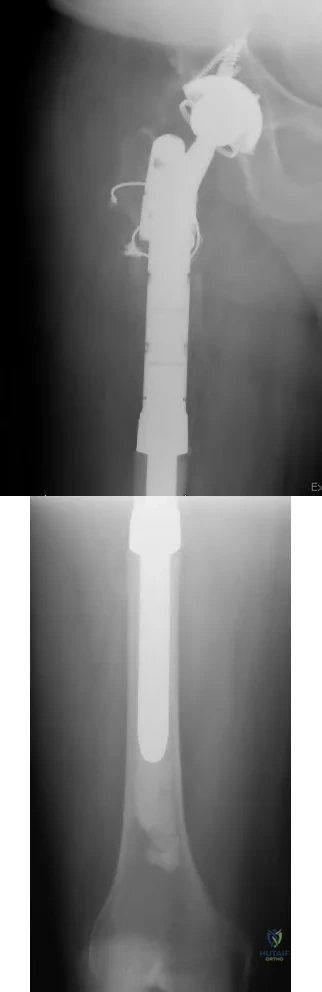
OrthoCash 2020
A 64-year-old male is 6 months out from left total knee arthroplasty. He has had at least two months of pain and swelling to the operative joint. In your initial workup, he is found to have a well-healed surgical incision, a serum CRP of 13mg/L and an ESR of 19mm/h. You perform arthrocentesis, which results in a negative alpha-defensin, synovial WBC of 1000 cells/µL, synovial PMNs of 90%, and synovial CRP of 4mg/L. What is the next best step in management?
Corticosteroid injection
Proceed to OR for histologic examination
Proceed with two stage revision
Proceed with single stage polyethylene exchange with irrigation and debridement
6 weeks of IV antibiotics
The patient has a score of 4 (2 points for elevated serum CRP, 2 points for elevated synovial PMN %) according to Parvizi et al's "The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria". This results in an ‘inconclusive’ determination of whether the patient has a periprosthetic joint infection. The best next step is to proceed to the OR in order to obtain tissue for histologic examination, cultures, and to determine whether purulence is present.
Periprosthetic joint infections can be devastating. Chronic PJI of the hip and knee is typically treated with two-stage revision arthroplasty. The first stage involves removal of the orthopaedic implants, placement of an antibiotic spacer, and at least 6 weeks of intravenous antibiotics. Once there is evidence that the infection has cleared (i.e. serum and synovial analysis), the second stage involves removal of the antibiotic spacer and placement of revision components.
Parvizi et al. updated their definition of PJI in 2018. They kept the major criteria for a chronic periprosthetic joint infection the same (an infection is indicated when 2 positive cultures of the same organism are isolated, or a sinus tract is present), but made several changes to the minor criteria.
Namely, they assign a point criteria in which a score of ≥6 is reliably infected, 2-5 is inconclusive, and 0-1 is not infected. In the case of infection, their recommendation is to proceed with a two-stage revision. If an inconclusive score is met, the recommendation is to proceed to the OR for histologic examination, cultures, and to determine whether purulence is present. The update to the MSIS criteria provides a sensitivity of 97.7% and a specificity of 99.5%.
Parvizi et al. reviewed 54 consecutive THA two-stage revisions. In their review, they determined MRSA to be the most common causative organism: MRSA 27.7%, S.epidermidis 18.4%, followed by MSSA 14.8%. They followed patients for a mean of 32 months, during which 26% had a recurrent infection and 8% developed mechanical failure (loose acetabular or femoral components).
Della Valle et al. made 15 CPGs (clinical practice guidelines) in JAAOS 2010. Among their recommendations: 1) they recommended utilizing serum CRP and ESR in assessing for PJI, 2) they recommended aspiration if serum CRP/ESR are abnormal, 3) if the initial aspiration has unexpected results they recommend repeat aspiration, and 4) 2 week antibiotic holiday before attaining cultures.
Illustration A shows the scoring criteria for the 2018 PJI update.
Incorrect Answers:
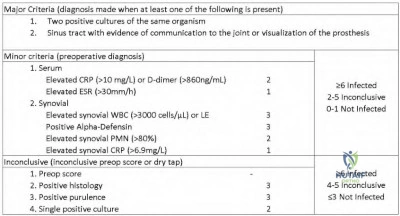
OrthoCash 2020
A 66-year-old male is undergoing a total knee arthroplasty using a fixed bearing posterior stabilized component. During the intraoperative trialing of the components, it is noted that the flexion gap is loose, and the extension gap is appropriate. Compared to a patient with appropriate flexion and extension gaps, this patient would be at an increased risk for which of the following?
Manipulation under anesthesia
Knee hyperextension
Posterior knee dislocation
Anterior knee dislocation
Patella fracture
A loose flexion gap in a posterior stabilized primary total knee arthroplasty can lead to an atraumatic posterior knee dislocation during knee flexion.
A posteriorly stabilized knee has a post built into the polyethylene bearing that articulates with the box of the femoral component in flexion to act as a cam mechanism. It is felt to occur when the patient is in moderate to deep flexion and tibia is able to translate posteriorly. The post becomes locked behind the cam and the patient is unable to extend the knee. The etiology is felt to be related to implant design, soft tissue laxity over time, and surgeon technique.
Clarke et al. review flexion instability as a mode of failure in knee replacements. They describe how this is usually due to a lack of adequate balance at the time of surgery. They also report that revision surgery is usually the only way to correct symptomatic flexion instability.
Lombardi et al. reviewed 15 cases of dislocation in three different implant designs given the statistically significant difference in the rate of dislocation. They found the only significant difference between the group of patients with dislocation was increased flexion. They state the majority of the dislocations occurred prior to a modification in the tibial polyethylene insert of the specific knee design they studied.
Illustration A shows an example of a posteriorly dislocated total knee arthroplasty following a "jumped post" dislocation.
Incorrect Answers:

OrthoCash 2020
A 78-year-old woman who has a history of an uncomplicated right total hip arthroplasty presents after a fall. Figure A is the radiograph obtained in the emergency department. What is the most appropriate treatment for the femoral component?

Retained femoral stem with open reduction internal fixation
Revision femoral stem to an uncemented long stem with strut allograft
Revision femoral stem to a cemented long stem with open reduction internal fixation
Revision femoral stem to an uncemented long stem with open reduction internal fixation
Proximal femoral replacement Corrent answer: 4
In this scenario, the stem is loose with good proximal bone stock. The best option would be revision femoral stem to an uncemented long stem with an open reduction of the fracture.
Operative treatment of periprosthetic fractures is directed by the location of the fracture, the stability of the implant, and remaining bone stock. In circumstances where the femoral implant has loosened or subsided revision to a long stem is recommended. Cemented fixation is less ideal in a fracture scenario given cement interference with fracture healing. After bypassing the fracture with a long stem the fracture is reduced and stabilized to provide an environment for healing and long term durability.
Ko et al. reviewed 14 patients who underwent revision to a Wagner stem
following a B2 periprosthetic fracture. They found all 12 patients who followed up went on to union with 10 achieving good or excellent outcomes. They concluded the Wagner revision stem is a satisfactory prosthesis for Vancouver B2 periprosthetic femur fractures.
Kwong et al. reviewed 143 patients who underwent revision total hip for a proximally compromised femur to a modular cementless femoral stem.
Roughly ~10% of these patients were revised for periprosthetic fracture. They found a 97.2% survival rate and an average Harris hip score of 92. They concluded that the modular cementless diaphyseal engaging revision stem allows for adequate revisions THA for the proximally compromised femur.
Figure A shows a loose femoral component with subsidence and a periprosthetic fracture. Illustration A shows an AP of the right hip following open reduction internal fixation as well as a revision to an uncemented long stem and revision of the acetabular components.
Incorrect Answers:

OrthoCash 2020
A 78-year-old female with end-stage arthritis of the left hip is schedule for a total hip arthroplasty. Her contralateral hip was replaced 4 years prior and a current radiograph is shown in Figure A. Which of the following would be the most effective at preventing the complication shown in the Figure?

Indomethacin treatment for 2 days postoperatively
Leaving 2 drains in place until at least 4 days post-operatively
Postoperative administration of ethylhydroxydiphosphonate
Preoperative administration of radiation therapy 1 week before surgery
Postoperative administration of radiation therapy 8 hours following the surgery
This patient has developed heterotopic ossification (HO) following a total hip arthroplasty. Radiation therapy administered within 24-48 hours postoperatively would best prevent this from forming.
Heterotopic ossification following arthroplasty is relatively rare, but is more common following total hip arthroplasty (THA) as compared to total knee arthroplasty (TKA). Symptoms can range from subtle pain to complete loss of motion. The trigger for HO formation is unknown but this process involves mesenchymal cell stimulation within the muscle and fascia to form osteoblast and osteoid formation. This process begins within 16 hours of the insulting event and continues for over 1 year, maturing into a ossified mass of lamellar bone.
Iorio and Healy discussed management of HO following arthroplasty. They note the most effective treatment at preventing HO is radiation therapy given 6 hours or sooner pre-operatively, or within 4 days post-operatively.
Indomethacin is an alternative to radiation, with variable regimens showing relatively equivalent results. They make a point to note that despite appropriate prophylaxis, 2-5% of individuals still develop HO.
Pelligrini et al. evaluated the outcomes of 2 groups undergoing THA who received either 800 cGy or fractionated 1000 cGy radiation therapy postoperatively. Equivalent outcomes were shown between the groups, as evidenced by 79% disease-free at 6 month follow-up. Of note, the implants used were all cemented which do not rely on bone ingrowth.
Pelligrini and Gregoritch then prospectively followed 2 groups undergoing THA that were randomized to receive either pre- or post-operative radiation therapy. At final 6 month followup, both groups showed similar disease-free rates (73% vs. 76%). This demonstrated that pre-operative radiation was as effective as post-operative, at a time when it's utility was unknown and unstudied.
Figure A shows a radiograph with HO formation nearly completely bridging the hip joint.
Incorrect Answers:
OrthoCash 2020
A 62-year-old woman with a valgus knee as seen in Figures A and B who underwent a primary total knee arthroplasty with a tourniquet presents 5 hours postoperatively with severe pain in the extremity and inability to dorsiflex or plantarflex the ankle. Narcotic pain medication does not improve her symptoms. The knee is flexed and the bandage is loosened and she is re-examined one hour later. On examination, the patient is unable to dorsiflex or plantarflex the foot and the pulses are asymmetric. What is the next most appropriate step in management?

Serial neurologic examinations and EMG in 3 months
Pain service consultation for adductor canal block
Return to the OR for peroneal nerve exploration
Vascular surgery consultation
Thrombectomy
The patient's asymmetric pulses, pain, and loss of motor function are evidence of an acute vascular injury for which an immediate vascular surgery consultation should be obtained.
Acute vascular injury following TKA is a rare but devastating complication that can result in wound healing complications, permanent neurologic injury, and loss of limb. Preoperative knowledge and evaluation of patients at risk for vascular injury allows optimization and potential modifications of surgical techniques to limit the chances of a vascular injury. Early recognition of an injury and consultation with a vascular surgeon is paramount to limit the chances of loss of limb. Patients with pre-existing vascular disease may be better served to have a TKA without the use of a tourniquet. If an injury occurs aggressive revascularization may be indicated for limb salvage.
Calligaro et al. report on their experience with vascular injuries following total hip and total knee arthroplasty in 32 patients, 24 TKA and 8 THA, for a rate of 0.13%. They found 44% of these vascular injuries were noted after the day of surgery and late-diagnosed injuries tended to have a higher rate of fasciotomies and foot drop. They also found thrombectomy alone was only successful in 28% of patients. They concluded that arterial injury after TKA and THA is rare, and aggressive revascularization is often needed for limb salvage.
Smith et al. review arterial injuries following total knee arthroplasty. They state preoperative risk factors of a history of vascular disease, intermittent claudication, ischemic ulcers, rest pain, asymmetric pulses, suspected popliteal aneurysm, radiographic evidence of vascular disease, or prior vascular surgery should alert the orthopedic surgeon of an increased risk for vascular complications following total knee arthroplasty. If performing a TKA on a patient with a history of vascular disease they recommend evaluation by a vascular surgeon and consideration of not using a tourniquet intraoperatively versus a tourniquet with an intravenous dose of heparin.
Ninomiya et al. reviewed the anatomy of the popliteal artery and when it could be injured during various portions of total knee arthroplasty. They state the popliteal artery is lateral to the midline at the tibial plateau in 95% of cadavers. To avoid vessel injury they recommend a preoperative vascular workup for high risk patients, careful placement of posterior retractors, and avoidance of hyperextension of the knee.
Figure A shows an AP and lateral of the knee respectively demonstrating a valgus knee with degenerative changes as well as posterior arterial calcifications.
Incorrect Answers:
OrthoCash 2020
A 70-year-old female patient on chronic steroids for severe lupus presents with worsening bilateral hip pain over the last several years. She has been on chronic corticosteroids for p-ANCA vasculitis. The current radiograph is shown in figure A. Which treatment will have the most reliable pain relief and return of function in this patient?

Vascularized fibular graft
Proximal femoral osteotomy
Core decompression
Total hip arthroplasty
Hip resurfacing arthroplasty Corrent answer: 4
Total hip arthroplasty would provide the most reliable pain relief and return of function in this patient with bilateral femoral head avascular necrosis with collapse.
Hip avascular necrosis, also known as osteonecrosis, leads to progressively worse hip pain and femoral head collapse. Idiopathic avascular necrosis is most common, which is the result of intravascular coagulation. In 80% of
cases, it is bilateral. Core decompression, vascularized fibular autograft, and rotational osteotomies are treatment options for pre-collapse osteonecrosis. Once Total hip arthroplasty or hip resurfacing arthroplasty are treatment options for lesions with femoral head collapse. Hip resurfacing is reserved for young male patients with good femoral bone stock. Total hip arthroplasty is a better option for older, female patients and those with chronic steroid use as there is poorer bone quality.
Jawad et al. reviewed the Ficat classification system for hip osteonecrosis. They described stage 0 as preclinical disease that is suspected when the contralateral hip is affected, stage 1 as preradiographic disease with groin pain, stage 2 as increased femoral head density or cystic lesions with or without a crescent sign, stage 3 occurs when there is the loss of the femoral head contour and stage 4 with complete collapse of the femoral head with associated osteoarthritis. The authors concluded that the Ficat classification system is the most widely used, but has limitations with prognostication of outcomes and reliability among researchers.
Zalavras and Lieberman reviewed the diagnosis and management of hip osteonecrosis. They identified risk factors for developing hip osteonecrosis including trauma, corticosteroid use, excessive alcohol consumption, coagulation disorders, hemoglobinopathies, dysbaric phenomena, autoimmune diseases, storage diseases, smoking, and hyperlipidemia.
Figure A is the AP pelvis radiograph demonstrating bilateral hip avascular necrosis with the collapse of the femoral head. Illustration A is a diagram of a vascularized fibular autograft used for hip avascular necrosis. Vascularized fibular autograft involves the harvesting of a portion of the peroneal artery pedicle. The femoral neck and head are reamed to accommodate the graft, which provides structural support to the subchondral bone. This is fixed with a K-wire or screw. The graft is anastomosed with the lateral femoral circumflex artery. Illustration B is a table of the Ficat classification system.
Incorrect Answers:
increasing vascular flow. It is not effective once femoral head collapse has occurred. It can be augmented with bone morphogenic proteins or bone marrow aspirate.

OrthoCash 2020
Medial knee osteoarthritis is associated with which biomechanical change?
Decreased knee flexion moment
Increased knee abduction moment
Increased knee adduction moment
Increased knee extension moment
None of the above Corrent answer: 3
An increased adductor moment during gait is associated with progression of medial knee osteoarthritis.
Altered joint loading during ambulation contributes to the onset and progression of knee osteoarthritis. The external knee adduction moment is considered a surrogate measure for the medial tibiofemoral contact force. An adduction moment is experienced by the knee when the ground reaction force passes medial to the center of the joint. This is seen when the knee has a varus mechanical alignment. An abnormally large peak adduction moment has been linked to increased pain and rate of disease progression. Strategies to decrease the knee adduction moment have been developed such as offloader braces.
Chehab et al. performed a biomechanical, clinical and MRI study on the progression of knee osteoarthritis. They found that the knee adduction and flexion moments were associated with decreases in medial femoral and tibial cartilage thickness, with the knee adduction moment being most associated with diminished medial femoral cartilage thickness and the knee flexion moment being most associated with diminished medial tibial cartilage thickness. They concluded that both knee adduction moment and knee flexion moment increase with medial arthritis and varus alignment, and must be taken into consideration when designing interventions that address knee osteoarthritis progression.
Manal et al. performed a biomechanical study in which they determined knee compartment loading utilizing video-based motion capture and electromyographic (EMG) recordings. They determined that peak adduction moment was the leading predictor of peak medial loading, and that peak knee flexor moment was also a significant predictor of peak medial joint loading.
They concluded that the combined use of peak knee adductor and flexor moments provides a more accurate estimate of peak medial joint loading than the peak adduction moment alone.
Illustration A is a diagram that shows how a knee adduction moment is produced by a varus mechanical alignment.
Incorrect Answers:
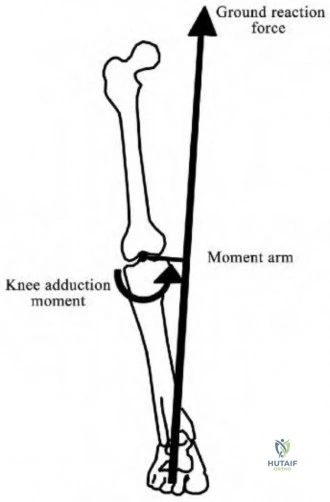
OrthoCash 2020
With regard to a mobile-bearing unicompartmental knee arthroplasty (UKA), which of the following is the most common cause of late (>10 years) failure?
Aseptic loosening
Progression of osteoarthritis
Unexplained pain
Instability
Infection
The most common cause of late failure and revision of unicompartmental knee arthroplasty (UKA) is the progression of osteoarthritis.
Late failure (>10 years) of UKA is most commonly caused by progression of arthritis. Other causes of failure include aseptic loosening, instability, infection, unexplained pain, and polyethylene wear. Interestingly, while TKA saw improved survival with improved polyethylene from the 1990s to the 2000s, UKA did not see a large change in survivorship suggesting that progression of osteoarthritis may be an unmodifiable mode of failure of these implants.
Jennings et al. review medial UKA. They state early medial UKA failures (<5 years) were from aseptic loosening (25%) with the progression of osteoarthritis second at 20%. However midterm and late failures were more commonly due to the progression of osteoarthritis (38 to 40%) with aseptic loosening (29%) and polyethylene wear (10%) as the next most common modes of failure.
Borus et al. reviewed UKA with regard to the evolution of the procedure. They found that at 10 years, one registry study found the progression of arthritis (51%) to be the most common cause of failure. They also cite a study that showed that mobile-bearing UKA tended to fail more from the progression of arthritis while fixed-bearing UKA failed due to tibial component failure.
Incorrect Answers:
OrthoCash 2020
Placement of an acetabular cup with a high inclination angle decreases the stability benefit of which of the following?
Larger femoral head size
Smaller femoral head size
Acetabular cup medialization
Increased femoral offset
Femoral stem anteversion Corrent answer: 1
Placement of an acetabular cup with a high inclination (abduction, theta) angle decreases the benefit of a larger head size by allowing dislocation with minimal translation.
Dislocations following THA occurs in approximately 1-3% of cases with an increased risk following revision surgery. Increased femoral head size improves stability by increasing jump-distance. In addition, an increased head-neck ratio allows a greater arc of motion prior to neck-socket impingement.
However, the increased stability provided by larger head sizes can be negated by other factors, including poor component positioning, poor soft tissue tensioning, and abductor deficiency. The use of a larger femoral head will not compensate for instability caused by a vertically positioned cup or abductor deficiency.
Burroughs et al. performed an in-vitro study evaluating the range of motion and stability in THA with 28, 32, 38, and 44-mm femoral head sizes. They found femoral heads >32-mm provide greater ROM and decreased component impingement. The authors conclude that large femoral heads offer potential in providing greater hip ROM and joint stability.
Kung et al. studied the effect of femoral head size and abductor integrity on dislocation rates in 230 patients who underwent revision THA. Four groups were identified: 1) intact abductor mechanism and 28-mm head, 2) absent abductor mechanism and 28-mm head, 3) intact abductor mechanism and 36-mm head, and 4) absent abductor mechanism and 36-mm head. The dislocation rate was higher with a 28-mm head compared to a 36-mm head when abductors were intact (groups 1 & 3). Dislocation rates were also higher if the abductors were absent, regardless of head size. The authors conclude the use of a large-diameter head does not reduce the rate of dislocation if the abductor mechanism is absent.
Illustration A is a low AP pelvis demonstrating an inclination (abduction, theta) angle of 63º.
Incorrect Answers
increasing the moment arm of the abductors, which is not biomechanically dependent on cup position.
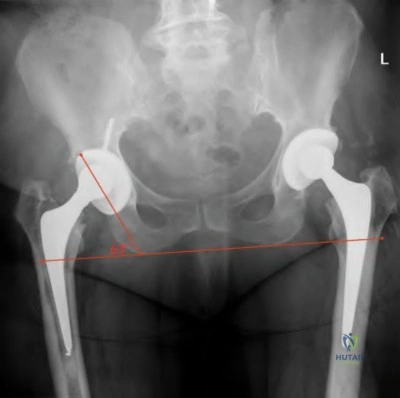
OrthoCash 2020
A 65-year-old woman who underwent left total hip arthroplasty 10 years ago now reports groin pain over the past year. An immediate postoperative (left image) and current radiograph (right image) are shown in Figure A. Laboratory studies show an elevated ESR and CRP. Aspiration results from one day prior shows 500 WBC with 50% neutrophils. She is presently taking oral antibiotics for a upper respiratory tract infection. What is the next most appropriate step in management?

Triple phase bone scan
Repeat aspiration today sent for cell count, gram stain, and culture
Open biopsy and frozen sections
Revision arthroplaty of acetabular component
Repeat aspiration today sent alpha-defensin synovial fluid immunoassay Corrent answer: 5
Oral antibiotics can decrease the yield of aspiration. In this circumstance, the aspiration should be repeated after 2 weeks off antibiotics or a repeat aspiration can be sent for alpha-defensin synovial fluid immunoassay.
The diagnosis of periprosthetic joint infection remains a challenge with no single test with 100% accuracy. The highest accuracy can be achieved with a combination of tests and the knowledge of the pretest probability given the clinical history. Elevated inflammatory markers are an indication to aspirate the joint. Aspiration can yield a false-negative result if the patient is on antibiotics at the time of aspiration (often for UTI, URI, or cellulitis). A repeat aspiration after 2 weeks off antibiotics can yield more accurate information, or an alpha-defensin synovial fluid immunoassay can be performed as these results are not affected by antibiotics.
Della Valle et al. reviewed preoperative and intraoperative evaluation for periprosthetic infection. They state that patients should be off antibiotics for 2 weeks prior to aspiration as being on antibiotics can lead to false-negative results. They state there is no gold standard single test to diagnose a periprosthetic infection so a combination of tests will lead to the highest proportion of correct diagnoses.
Lachiewicz et al. reviewed 142 patients who underwent revision total hip arthroplasty and had a preoperative aspiration. They found no patients were infected if their implant had been in for >5 years and they had a normal ESR. They conclude that all patients with a painful total hip should be aspirated if
<5 years have elapsed from the index surgery or they have an elevated CRP.
Kelly et al. looked at synovial alpha-defensin in cases of an unclear diagnosis of PJI. They retrospectively reviewed 41 cases of possible PJI with prior aspiration and found in patients with recent antibiotic use alpha-defensin correctly diagnosed 83% of patients. They concluded alpha-defensin may be a useful data point in patients with and unclear diagnosis in cases of recent antibiotic use, equivocal laboratory findings, or suspected false-positive or false-negative cultures.
Figure A shows a left total hip with immediate post-op and current radiographs with interval loosening of the acetabular component.
Incorrect Answers:
OrthoCash 2020
An otherwise healthy 62-year-old woman presents 6 months postop from a TKA. For the past 6 weeks, she has noted pain and swelling with one week of drainage from the knee as seen in Figure A. Inflammatory markers and aspiration cell counts are elevated. Which of the following treatments give her the highest chance of eradication of infection?

Chronic lifelong suppressive antibiotic therapy
Urgent debridement, antibiotics, and implant retention (DAIR)
Urgent irrigation and debridement with modular component exchange
stage revision of all components
stage revision of all components Corrent answer: 5
The patient has a confirmed chronic postoperative periprosthetic joint infection (PJI) based on positive aspiration and a draining sinus. A 2-stage revision would give her the best chance of successful eradication.
Chronic PJI are difficult to eradicate without the removal of components due to biofilm on the prosthesis surface. A 2-stage revision with the removal of all components and placement of an antibiotic-eluting spacer and 6 weeks of culture directed IV antibiotics is the gold standard for chronic infections.
Parvizi et al. reviewed the literature on diagnostic strategies for assessing PJI and compared these data to a single large-volume institution's findings. Joint fluid aspirates with high cell counts and high percentage-neutrophils as well as positive FDG-PET scans have high sensitivities for diagnosing periprosthetic infections. While properly performed aspirates and intraoperative cultures
have near-perfect specificities (0.97, 1.0 respectively), they found a 10-14% false-negative rate. They go on to describe their institutional diagnostic protocol defining numerical cutoffs based on predictive value thresholds.
Koyonos et al. performed a single-institution retrospective review of irrigation and debridement alone for various time intervals from index surgery (acute, acute delayed, and chronic). They found irrigation and debridement was an ineffective way to definitively treat PJI for acute post-op infections (<4 wks from surgery 69% failure), acute delayed infections (>4 wks from surgery, 56% failure), and chronic infections (months after index surgery, 72% failure). They concluded that I&D should be reserved for acute onset symptoms with a non-staphylococcal infection in an optimized host with a previously normal total joint arthroplasty.
Figure A shows a draining sinus tract over a standard midline TKA incision. Incorrect Answers:
successful infection eradication compared to 2-stage revision.
OrthoCash 2020
A 62-year-old female is referred to you by your partner for continued groin pain after undergoing an uneventful total hip arthroplasty utilizing the direct anterior approach. On exam, her pain is reproduced with resisted hip flexion. Workup for infection and loosening were negative. Radiographs and CT show well-placed implants. An ultrasound-guided lidocaine injection eliminated her pain completely for one day but returned. When arthroscopically addressing the pathologic structure, in what position should the hip be placed to avoid damaging the nearest major neurovascular structure?
Internal rotation to avoid the sciatic nerve
Internal rotation to avoid the ascending medial femoral circumflex artery
Internal rotation to avoid the femoral neuromuscular bundle
External rotation to avoid the ascending medial femoral circumflex artery
External rotation to avoid the femoral neurovascular bundle
This patient has iliopsoas tendinitis following total hip arthroplasty (THA). The leg should be externally rotated when performing extra-capsular tenotomy to protect the femoral neurovascular bundle.
Hip arthroscopy was a previously daunting procedure given the deep location of the hip joint, limitations of available instrumentation, and close proximity of the peri-articular anatomy. Significant advances in these areas have allowed for safer and more reproducible results in treating common hip pathology.
Iliopsoas tenotomy is now commonly performed but relies heavily on a thorough understanding of the surrounding anatomy. The two most common iliopsoas tenotomy techniques are the trans-capsular and extra-capsular releases. Trans-capsular release involves making a capsulotomy between the anterior labrum and zona orbicularis to access the iliopsoas tendon (Illustration A). The extra-capsular tenotomy is more commonly done following total hip arthroplasty and involves accessing the iliopsoas at the level of the lesser trochanter (Illustration C). Both techniques require slight flexion of the hip and external rotation to bring the tendon towards the surgeon and away from the femoral neurovascular structures.
Robertson and Kelly performed a cadaveric study demonstrating which neurovascular structures are at risk with common arthroscopic portals. The traditional anterior portal (AP) was an average of 15mm from the branches of the lateral femoral cutaneous nerve. They concluded that by shifting the anterior portal further lateral to a longitudinal line drawn from the ASIS, the LFCN is less in danger.
Ilizaliturri et al. performed a prospective trial following two cohorts undergoing either the extra-capsular or trans-capsular iliopsoas tenotomy. They found both cohorts had significant improvements in both groups without significant differences between them. This shows arthroscopic/endoscopic iliopsoas tenotomy to be a safe and reliable procedure.
Illustration A shows the trans-capsular iliopsoas tenotomy. Illustration B is a panel intra-operative photos of this release, showing the subsequent release of the bright white psoas tendon (PT) to reveal the iliac muscle fibers (ZO= zone orbicularis, AHC= anterior hip capsule). Illustration C is an axial MRI at the level of the central compartment, with the femoral neurovascular bundle (arrow) and psoas labelled.
Illustrations D and E demonstrate the extra-capsular iliopsoas tenotomy. Again, note the bright appearance of the psoas tendon before release.
Illustration F is an axial MRI at the level of the lesser trochanter with the femoral neurovascular bundle (arrow) and psoas tendon labelled.
Incorrect Answers:

OrthoCash 2020
A 65-year-old male presents to your clinic with right hip pain. He underwent right metal-on-metal total hip arthroplasty (THA) 20 years prior and had been doing well until 5 years ago. He notes groin pain with ambulation and thigh pain when getting up from a seated position. His radiographs are shown in Figure A. MRI studies with metal artifact reduction sequence reveal a pseudotumor noted in the periprosthetic soft tissues. Which of the following is true with respect to this patient's clinical picture?

The majority of patients with metal-on-metal THA have a pseudotumor
The presence of a pseudotumor is associated with increased implant linear wear rate
The pseudotumors are composed of both macrophages and lymphocytes, with macrophages being predominant
The presence of a pseudotumor is associated with relatively high ratio of serum cobalt to chromium
Observation is recommended given the absence of loosening on radiographs Corrent answer: 2
The patient has a metal-on-metal (MoM) THA with a pseudotumor present on MRI studies. The presence of a pseudotumor is associated with increased linear wear of both the acetabulum and the femoral components.
A pseudotumor is a mass-forming tissue reaction caused by metal-on-metal wear most notably seen in MoM total hip arthroplasty. These lesions are noted in 10-15% of patients with MoM THAs. The etiology is unclear but is thought to be associated with local high wear debris as well an increased hypersensitivity to metal wear. The lesions are lymphocyte-predominant although macrophages are also present throughout. Treatment of patients with hip pain and pseudotumor noted on MRI studies is generally revision to a ceramic-on-polyethylene THA.
Kwon et al. compared the in vivo wear rate of MoM THAs revised due to a pseudotumor compared to those MoM THAs that were revised for other reasons. The authors noted that the pseudotumor group (n = 8) had median linear wear of the femoral component of 8.1 microns/year and the non-pseudotumor group (n =22) had a linear wear rate of 1.79 microns/year. A similar discrepancy was noted for acetabulum wear with 7.36 microns/year in the pseudotumor group compared to 1.28 microns/year in the non-pseudotumor group. The authors conclude that the presence of a pseudotumor is associated with increased wear at the metal-on-metal articulation.
Daniel et al. performed a review of pseudotumors associated with MoM THA. They reviewed the potential causes to include foreign-body reaction, hypersensitivity and wear debris. They discussed that patients with pseudotumors associated with a MoM THA should undergo prompt revision to a nonmetal-on-metal bearing THA since prolonged delay can lead to soft tissue envelope compromise, recurrent dislocations, nerve palsies, and femoral artery stenosis. Furthermore, they also noted that hip function scores for patients who had revision for pseudotumors were significantly worse than those for patients who had MoM THA revision for other reasons.
Figure A is an AP pelvis showing the characteristic appearance of an MoM THA with a large metallic femoral head.
Incorrect Answers:
OrthoCash 2020
A 66-year-old male undergoes the procedure shown in figures A and B. After 4 years, he develops progressive pain and limitations in his daily function that is refractory to conservative measures. He is indicated for conversion to a total knee replacement with almost complete relief of his symptoms postoperatively. What preoperative factor likely led to the subsequent failure?
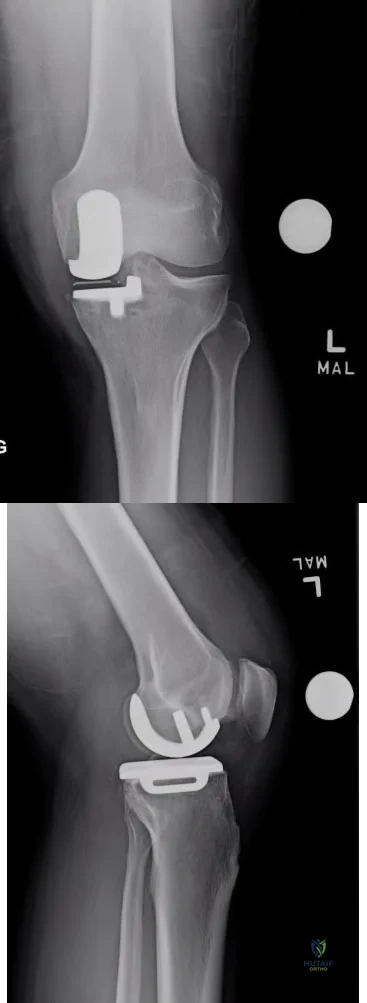
Question 93
Elbow distraction interposition arthroplasty may be most appropriate treatment for which of the following patient profiles? Review Topic
Explanation
Question 94
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What is the underlying cause of the pathology noted in the figures?

Explanation
Question 95
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?
Explanation
REFERENCES: Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, pp 165-201.
Question 96
A 26-year-old man sustained an isolated injury to his left hip joint in a motor vehicle accident. Closed reduction was performed, and the postreduction radiograph is shown in Figure 29. Management should now consist of
Explanation
REFERENCES: Tile M, Olson SA: Decision making: Non operative and operative indications for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 496-532.
Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993, pp 337-339, p 507.
Question 97
One advantage of using onlay strut allograft in femoral revision surgery is that it can
Explanation
REFERENCES: Emerson RH Jr, Malinin TI, Cuellar AD, Head WC, Peters PC: Cortical strut allografts in the reconstruction of the femur in revision total hip arthroplasty: A basic science and clinical study. Clin Orthop 1992;285:35-44.
Pak JH, Paprosky WG, Jablonsky WS, Lawrence JM: Femoral strut allografts in cementless revision total hip arthroplasty. Clin Orthop 1993;295:172-178.
Head WC, Emerson RH Jr, Malinin TI: Structural bone grafting for femoral reconstruction. Clin Orthop 1999;369:223-229.
Question 98
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management?
Explanation
REFERENCES: Hughes C IV, Hasselman CT, Best TM, et al: Incomplete, intrasubstance strain injuries of the rectus femoris muscle. Am J Sports Med 1995;23:500-506.
Temple HT, Kuklo TR, Sweet DE, et al: Rectus femoris muscle tear appearing as a pseudotumor. Am J Sports Med 1998;26:544-548.
Question 99
A 14-year-old gymnast misses her dismount off of the uneven bars, hits the mat face first, and loses consciousness for about 15 seconds. She is dazed and confused for several minutes. She does not complain of pain, numbness, or weakness and she is moving all extremities without deficit. The athlete and coach would like to return to competition that day. What is the best next step?
Explanation
A. Axillary
B. Median
C. Musculocutaneous
D. Radial
Question 100
What factor induces myofibrillar muscle protein synthesis (MPS)? Review Topic
Explanation
