Orthopedic Board Review MCQs: Foot & Ankle, Spine, & Trauma | Part 63

Key Takeaway
This page offers Part 63 of 100 verified, high-yield MCQs for orthopedic surgeons & residents preparing for AAOS/ABOS board exams and OITE. Modeled on official formats, these questions, focusing on Foot, Fracture, and Tendon, include clinical explanations to enhance your exam readiness.
About This Board Review Set
This is Part 63 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 63
This module focuses heavily on: Foot, Fracture, Tendon.
Sample Questions from This Set
Sample Question 1: A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuri...
Sample Question 2: During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?...
Sample Question 3: Which of the following areas of the vertebral segment has the highest ratio of cortical to cancellous bone? Review Topic...
Sample Question 4: What is the primary benefit of using rhBMP-2 instead of autogenous bone graft inside an anterior spinal fusion cage?...
Sample Question 5: The use of posting (a wedge added to the medial or lateral side of an insole) is useful to balance forefoot or hindfoot malalignment. Assuming normal subtalar joint pronation, what is the maximum amount of recommended hindfoot posting?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?
Explanation
REFERENCES: Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, pp 632-635.
Question 2
During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?
Explanation
REFERENCES: Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
Wapner K, Pavlock GS, Hecht PJ, Naselli F, Walther R: Repair of chronic Achilles tendon rupture with flexor hallucis longus tendon transfer. Foot Ankle Int 1993;14:443-449.
Question 3
Which of the following areas of the vertebral segment has the highest ratio of cortical to cancellous bone? Review Topic
Explanation
Question 4
What is the primary benefit of using rhBMP-2 instead of autogenous bone graft inside an anterior spinal fusion cage?
Explanation
REFERENCE: Burkus JK, Gornet MF, Dickman CA, et al: Anterior lumbar interbody fusion using rhBMP-2 with tapered interbody cages. J Spinal Disord Tech 2002;15:337-349.
Question 5
The use of posting (a wedge added to the medial or lateral side of an insole) is useful to balance forefoot or hindfoot malalignment. Assuming normal subtalar joint pronation, what is the maximum amount of recommended hindfoot posting?
Explanation
REFERENCES: Donatelli RA, Hurlbert C, Conaway D, et al: Biomechanics foot orthotics: A retrospective study. J Orthop Sports Phys Ther 1988;10:205-212.
Michaud TM: Foot Orthoses and Other Forms of Conservative Foot Care. Baltimore, MD, Williams & Wilkins, 1993, pp 61-65, 186.
Root MC, Orien WP, Weed JH: Normal and Abnormal Function of the Foot. Los Angeles, CA, Clinical Biomechanics Corporation, 1977, vol 2, pp 29-33.
Question 6
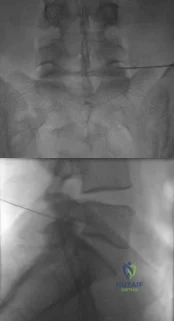
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?

Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 7
A 13-year-old boy has had pain and swelling in his ankle for the past several months. Based on the radiograph, MRI scan, and biopsy specimen shown in Figures 77a through 77c, what is the best course of action?
Explanation
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 247-264.
Lin PP, Thenappan A, Deavers MT, et al: Treatment and prognosis of chondroblastoma. Clin Orthop Relat Res 2005;438:103-109.
Question 8
A 64-year-old man with a history of diabetes mellitus underwent open reduction and internal fixation of a displaced ankle fracture 8 weeks ago. Examination now reveals recent onset erythema, warmth, and swelling of the midfoot. Radiographs are shown in Figures 23a through 23d. What is the most likely reason for the swelling of the foot?
Explanation
REFERENCE: Connolly JF, Csencsitz TA: Limb threatening neuropathic complications from ankle fractures in patients with diabetes. Clin Orthop 1998;348:212-219.
Question 9
After the athlete undergoes the appropriate treatment of the postsurgical complication and recovers without further incident, which muscle most likely will be last to experience return of function?
Explanation
This patient sustained an eccentric contracture (muscle lengthening while contracting) of his biceps muscle while trying to stop a defender from getting around him. This in turn caused failure of the distal biceps tendon, as evidenced by pain in the antecubital fossa, lack of elbow supination strength, and his positive biceps active test finding (supination/pronation of the forearm showing no motion of the biceps muscle belly). Eccentric contractors have the highest
potential for building strength but also are at highest risk for injury. Concentric (muscle shortening with contraction), isometric (no change in muscle length with contracture), and isokinetic (constant velocity of muscle contraction with a variable force) do not describe the mechanism detailed.
The loss of distal biceps attachment will result in loss of elbow supination strength in flexion (the biceps is the only supinator to cross the elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared to the 2-incision technique. The most troubling complication for most surgeons is the development of a PIN palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABC nerve injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button.
Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The EIP is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC followed by the ECU, EDQ, and, finally, the EIP.
RESPONSES FOR QUESTIONS 26 THROUGH 27
Anterior tibial artery
Posterior tibial artery
Superficial peroneal nerve
Deep peroneal nerve
Match the neurovascular structure at risk (listed above) with the compartment undergoing fasciotomy (listed below).
Question 10
A 35-year-old female runner reports progressive vague aching pain involving her midfoot. Her pain is most notable when running. She denies specific injury. Examination reveals minimal swelling and localized tenderness over the dorsal medial midfoot and navicular. Radiographs and an MRI scan are shown in Figures 37a through 37c. What is the most appropriate management?
Explanation
REFERENCES: Lee A, Anderson R: Stress fractures of the tarsal navicular. Foot Ankle Clin 2004;9:85-104.
Coughlin M: Tarsal navicular stress fractures. Tech Foot Ankle Surg 2002;1:112-122.
Question 11
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?
Explanation
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
Question 12
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
REFERENCES: Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186.
Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
Question 13
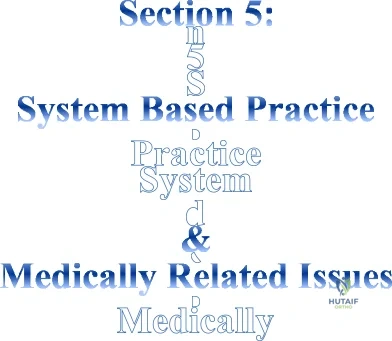
03 A 37 year-old woman with thoracic back pain has had hemoptysis and dyspnea for the past month. A thoracic spine radiograph shows a compression fracture of T-9 and a mass in the right lung. What is the best course of action?
Explanation

Here is an algorithm from OKU 6 Tumors of the Spine pp 723-736

This question gives you the history, skips right over physical exam and goes into plain films. With this patient’s history of hemoptysis and dyspnea and a lung mass, the next steps in this patients work-up would include the competion of initial work-up, metastatic work-up, then pre-operative planning. Goals of treatment are to 1) protect or restore neurologic function, 2) control pain,

Question 14
A 19-year-old linebacker for a collegiate football team has had two episodes of bilateral arm tingling and weakness after tackling; the symptoms resolved after 30 minutes of rest. Three follow-up neurologic examinations have been normal. Cervical spine CT and MRI scans are shown in Figures 13a through 13c. What is the next best step in management?
Explanation
REFERENCES: Torg JS, Naranja RJ Jr, Pavlov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Cantu RC: The cervical spinal stenosis controversy. Clin Sports Med 1998;17:121-126. Crowl AC, Kong JF: Cervical Spine, in Johnson DL, Mair SD (eds): Clinical Sports Medicine. Philadelphia, PA, Mosby Elsevier, 2006, pp 143-149.
Question 15
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
Question 16
A 59-year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 17
-Figure is the radiograph of a 55-year-old veteran who developed avascular necrosis after a traumatic hip dislocation. He was treated with hemiarthroplasty 10 years ago and also has posttraumatic stress disorder and chronic pain. He has had multiple spinal surgeries and takes 30 mg of methadone daily. He now has severe groin pain and is unable to ambulate. Laboratory studies showed a C-reactive protein level of 0.2 mg/L (reference range, 0-3 mg/L), erythrocyte sedimentation rate of 50 mm/h (reference range, 0-20 mm/h), hip aspiration of 500/mm3 white blood cell count, 50% polynucleated cells, 30%monocytes, and 20% lymphocytes What is the most likely cause of his hip pain?
Explanation
Question 18
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
Explanation
REFERENCES: Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.
Question 19
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms? Review Topic
Explanation
Question 20
Which of the following is considered a potential advantage of arthroscopic repair for anterior instability of the shoulder? Review Topic
Explanation
Question 21
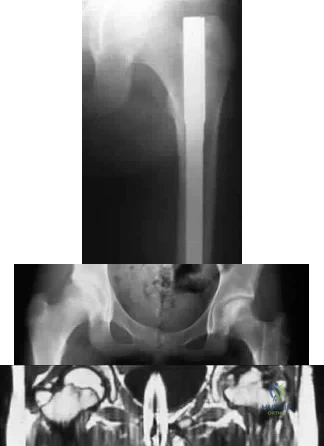
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?
Explanation
REFERENCES: Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
DiCaprio MR, Enneking WF: Fibrous dysplasia: Pathophysiology, evaluation, and treatment.
J Bone Joint Surg Am 2005;87:1848-1864.
Question 22
The space available for the cord is an important determinant in neurologic recovery. Recent analysis suggests that the most reliable radiographic predictor for neurologic recovery after surgery in patients with rheumatoid arthritis and paralysis is a preoperative
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 273-279.
Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Wattenmaker I, Concepcion M, Hibberd P, Lipson S: Upper airway obstruction and perioperative management of the airway in patients managed with posterior operations on the cervical spine for rheumatoid arthritis. J Bone Joint Surg Am 1994;76:360-365.
Question 23
Which of the following statements best describes the instantaneous axis of rotation (IAR) for the functional spinal unit? Review Topic
Explanation
Question 24
Which of the following patients is considered the most appropriate candidate for selective dorsal rhizotomy?
Explanation
REFERENCES: Peacock WJ, Arens LJ, Berman B: Cerebral palsy spasticity: Selective posterior rhizotomy. Pediatr Neurosci 1987;13:61-66.
Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
Mooney JF III, Millis MB: Spinal deformity after selective dorsal rhizotomy in patients with cerebral palsy. Clin Orthop 1999;364:48-52.
Question 25
A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient? Review Topic
Explanation
Question 26
Which of the following changes occur in the spinal cord and the spinal canal when the cervical spine moves from neutral to full flexion?
Explanation
REFERENCES: Breig A: Biomechanics of the Central Nervous System: Some Basic Normal and Pathologic Phenomena. Stockholm, Sweden, Almquist and Wiksell, 1960.
Ghanayem AJ, Zdeblick TA, Panjabi MM: Biomechanics of nonacute cervical spine trauma, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 103-105.
Question 27
During total hip arthroplasty, what characteristic of irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene should provide a more wear-resistant construct than traditional gamma- irradiated (2.5-4 Mrad)-in-air polyethylene mated with the same head?
Explanation
Highly cross-linked polyethylene makes material resistant to adhesive wear. Abrasive wear from third bodies does not decrease wear. The fatigue strength of such material is inferior to that of traditional polyethylene, and its resistance to creep is the same, if not lower, than that of traditional polyethylene.
Question 28
A 25-year-old farm worker sustained a grade III open fracture of the midshaft of the left tibia after falling from a ladder. Which of the following antibiotic regimens is best for this patient?
Explanation
REFERENCES: Holton PD, Mader J, Nelson CL, Osmon DR, Patzakis MJ: Antibiotics for the practicing orthopaedic surgeon. Instr Course Lect 2000;341:36-42.
Wilkins J, Patzakis M: Choice and duration of antibiotics in open fractures. Orthop Clin North Am 1991;22:433-437.
Question 29
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan? Review Topic
Explanation
Question 30
What is the most significant benefit of percutaneous transforaminal lumbar interbody fusion (TLIF) vs open posterior lumbar interbody fusion (PLIF)?
Explanation
Humphreys and associates in a retrospective review of TLIF vs PLIF found fusion rates, surgical time, and length of hospital stay were similar with both procedures. The only benefits associated with TLIF were less blood loss and preservation of the paraspinal muscle sleeve. Manos and associates in a cadaver study found no difference in the volume of disk material evacuated or the area of endplate exposed in either procedure.
RECOMMENDED READINGS
Humphreys SC, Hodges SD, Patwardhan AG, Eck JC, Murphy RB, Covington LA. Comparison of posterior and transforaminal approaches to lumbar interbody fusion. Spine (Phila Pa 1976). 2001 Mar 1;26(5):567-71. PubMed PMID: 11242386. View Abstract at PubMed
Manos R, Sukovich W, Weistroffer J: Transforaminal lumbar interbody fusion: Minimally invasive versus open disc excision and endplate preparation. Presented at the 12th International Meeting of Advanced Spine Techniques, Banff, Alberta, Canada, July 7-9, 2005.
Question 31
Which of the following is an advantage of using blocking screws for tibial nailing?

Explanation
Krettek found that medial and lateral blocking screws can increase the primary stability of distal and proximal metaphyseal fractures after nailing and can be an effective tool for selected cases that exhibit malalignment and/or instability by decreasing mechanically measured deformation.
In a later clinical study, Krettek found that after using blocking screws, tibial healing was evident radiologically at a mean of 5.4 months with a decreased rate of malunions.
Ricci also found that blocking screws are effective to help obtain and maintain alignment of fractures of the proximal third of the tibial shaft treated with intramedullary nails.
Question 32
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?
Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the
inability to gain purchase for extraction.
Question 33
A 14-year-old boy is seen for back pain. Radiographic evaluation reveals a grade III isthmic spondylolisthesis. What measurement is most useful in predicting the likelihood of progression?
Explanation
REFERENCES: Huang RP, Bohlman HH, Thompson GH, et al: Predictive value of pelvic incidence in progression of spondylolisthesis. Spine 2003;28:2381-2385.
Mac-Thiong JM, Wang Z, de Guise JA, et al: Postural model of sagittal spino-pelvic alignment and its relevance for lumbosacral developmental spondylolisthesis. Spine 2008;33:2316-2325.

Figure 22a Figure 22b
Question 34
Which of the following clinical findings is most often seen with the MRI scan findings shown in Figures 19a through 19c? Review Topic
Explanation
Question 35
The patient develops an inability to dorsiflex her foot 2 days after surgical intervention while she is sitting in a chair after physical therapy. Initial treatment should consist of
Explanation
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis.
This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis, observation for 1 year would not be appropriate.
The psoas is the anatomic structure that runs anterior to the acetabulum. The femoral neurovascular structures are at risk if the retractor is placed anterior and inferior to the psoas tendon.
The patient develops a foot drop 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MR imaging or a CT scan may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be decreased by flexing the surgical knee and positioning the bed flat.
Question 36
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of
Explanation
shown some healing response with callus formation, but these techniques are not successful
in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions
of the clavicle.
REFERENCES: Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 37
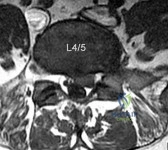
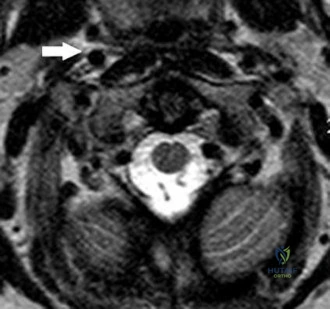
A 32-year-old male presents with left leg pain and weakness. An axial image from his MRI is shown in Figure A. Which of the following physical exam findings would be most consistent with this MRI finding. Review Topic
Explanation
radiculopathy.
While nerve root innervation shows some variability by patient, L5 is "characteristically" responsible for the sensation to the dorsal aspect of the foot, ankle dorsiflexion (tibialis anterior - along with L4), great toe extension (EHL), and hip abduction (gluteus medius).
Suri et al. reported on specific physical exam findings that significantly increased the likelihood of nerve root impingement at specific lumbar levels. They found: L2 was associated with decreased anterior thigh sensation. L3 was associated with a positive femoral stretch test. L4 was associated with a blunted patellar reflex, decreased medial ankle sensation or a positive crossed femoral stretch test. L5 was associated with was associated with decreased hip abductor strength.
Luri et al. reported 8-year follow up on the patients in the spine patient outcomes research trial who underwent surgical vs. conservative care for treatment of lumbar herniated disc. They found that patients who underwent surgical treatment had superior results that were maintained at 8 years compared to patients who underwent conservative management.
Figure A is an axial MRI at the L4/5 disc space that shows a left paracentral disc herniation compressing the descending L5 nerve root. Illustration A identifies the structures in the MRI image. Illustration B demonstrates the dermatome, reflex and motor function associated with the L4, L5 and S1 nerve root.
Incorrect Answers:
(SBQ13PE.102) An 26-year-old male presents to your office complaining of bilateral hip and low back pain. On physical examination, he has 10 degree bilateral hip flexion contractures. An AP pelvis radiograph is demonstrated in figure A. Which of the following findings is consistent with this patient's presentation? Review Topic

A positive flexion, adduction, internal rotation (FADDIR) test
A history of untreated slipped capital femoral epiphysis (SCFE)
A thrombophilia
Normal serum ESR and CRP
Positive Human Leukocyte Antigen B27 (HLA-B27)
The patient has large joint arthralgia and sacroiliac joint sclerosis on AP pelvis radiograph, which is consistent with ankylosing spondylitis. Patients with ankylosing spondylitis have positive Human Leukocyte Antigen B27 (HLA-B27).
Ankylosing spondylitis (AS) is a seronegative spondyloarthropathy that affects the axial skeleton as well as large joints including the hips and knees. The most common initial site of pain is the sacroiliac (SI) joint, and is demonstrated as sacroiliitis on pelvic radiograph. Hip involvement is common, and typically manifests as hip pain and flexion contracture. Serologic studies will be typically be negative for rheumatoid factor, but positive for HLA-B27 in 90% of patients.
Kubiak et. al. review orthopaedic management of AS. Common orthopaedic manifestations include SI joint pain, hip flexion contractures, and stiffness of the cervical and lumbar spine. They report that laboratory analysis of patients with active disease will typically demonstrate mild elevation of ESR, CRP, and WBC. Patients with chronic AS may demonstrate a normocytic anemia. If HLA-B27 is negative, a high clinical suspicion should still be maintained.
Gensler et al. review the different clinical conditions that compose of juvenile-onset spondyloarthritis. They report on the different spondyloarthritides includes ankylosing spondylitis, reactive arthritis, arthropathy associated with inflammatory bowel disease, and that associated with psoriasis. They emphasize that the appearance of sacroiliac joint and spinal disease in the form of ankylosing spondylitis usually takes 5–10 years after initial symptom presentation, and therefore, a definite diagnosis can take several years leading to a delay in diagnosis.
Figure A is an AP pelvis radiograph of a skeletally mature individual demonstrating sclerosis of the SI joint indicative of sacroiliitis. Illustration A shows a axial CT image of the patient in the stem. Sclerosis and bone erosion can be seen in the sacroiliac joint.
Incorrect Answers:
osteonecrosis Answer 3: A infarctions,
of
the
femoral
epiphysis.
thrombophilia may have
osseous manifestations such as bone
which
are
not
evident
on
this
image.
Question 38
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Craig EV: Fractures of the clavicle, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 428-482.
Question 39
A 20-year-old football player has immediate pain in the midfoot and is unable to bear weight after an opposing player lands on the back of his plantar flexed foot. AP and lateral radiographs are shown in Figures 4a and 4b. Management should consist of
Explanation
REFERENCES: Bellabarba C, Sanders R: Dislocations of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1539-1558.
Murphy GA: Fractures and dislocations of the foot, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby, 1998, vol 2, pp 1956-1960.
Question 40
Figures below demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. A further work-up reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MRI with MARS. Revision THA is recommended. The most common complication following revision of a failed metal-on- metal hip arthroplasty is
Explanation
Question 41
Intramembranous ossification during fracture repair is characterized by absence of which of the following elements?
Explanation
REFERENCES: Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Buckwalter JA, Einhorn TA, Bolander ME: Healing of the musculoskeletal tissues, in Rockwood CA Jr, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 261-276.
Question 42
A 36-year-old man sustains blunt chest trauma, an open right femur fracture, and a closed left tibia fracture following a high-speed MVC. Upon presentation to the emergency room, blood pressure is 80/40, HR 135, and urine output is .4 cc/kg/hr. Fluids and blood products are administered, and the patient is transferred to the ICU for further care. Which of the following indicates adequate resuscitation has been achieved?

Explanation
Shock is an abnormality of the circulatory system that results in inadequate organ perfusion and tissue oxygenation. This leads to anaerobic metabolism with the development of lactic acidosis and oxygen debt. Shock is either classified as compensated or uncompensated. Compensated shock exists when there is evidence of ongoing inadequate tissue perfusion despite the normalization of blood pressure, heart rate, and urine output. Uncompensated shock occurs when there is inadequate tissue perfusion and abnormal blood pressure, heart rate, and urine output. Thus, a patient may have normal vital signs but still be in a state of compensated shock that requires additional resuscitation.
Porter et al. review the optimal end points of resuscitation in trauma patients. They conclude that using traditional end points such as blood pressure, urine output and heart rate, may leave up to 85% of patients in "compensated" shock. They urge the use of lactate, base deficit, and gastric intramucosal pH as appropriate end points of resuscitation.
Roberts et al. discuss various aspects of damage control orthopaedics in the multiply injured trauma patient. Although they do not discuss the end points for resuscitation, they note that they presence of shock is a clinical parameter associated with adverse outcomes in the trauma patient.
Incorrect answers:
Question 43
The artery of Adamkiewicz (arteria radicularis, arteria magna) is most commonly found on the
Explanation
REFERENCES: Stambaugh J, Simeone F: Vascular complication in spine surgery, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1715.
Lazorthes G: Arterial vascularization of the spinal cord. J Neurosurg 1971;35:253-262.
Question 44
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function. A pathognomonic radiographic feature of this injury is a

Explanation
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 45
What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty?
Explanation
REFERENCES: Chin PY, Sperling JW, Cofield RH, et al: Complications of total shoulder arthroplasty: Are they fewer or different? J Shoulder Elbow Surg 2006;15:19-22.
Hasan SS, Leith JM, Campbell B, et al: Characteristics of unsatisfactory shoulder arthroplasties. J Shoulder Elbow Surg 2002;11:431-441.
Question 46
A 10-year-old girl was thrown over the handlebars of her bicycle and landed directly on her left shoulder. She was treated with a figure-of-8 strap and analgesics. Follow-up examination 2 weeks later reveals that the lateral end of the clavicle is superiorly dislocated relative to the acromion. A radiograph of the shoulder shows calcification lateral to the coracoid process at the level of the acromion, and the clavicle is superiorly displaced. Management should consist of
Explanation
REFERENCES: Falstie-Jensen S, Mikkelsen P: Pseudodislocation of the acromioclavicular joint. J Bone Joint Surg Br 1982;64:368-369.
Havranek P: Injuries of the distal clavicular physis in children. J Pediatr Orthop 1989;9:213-215.
Question 47
What is the typical axial plane transverse angulation of the thoracic pedicles?
Explanation
starting point is more lateral. T2 angles about 15 degrees, and then the pedicles average about
5 to 7 degrees down to T10. At T11 and 12, the angulation is minimal.
REFERENCES: Weinstein L: Pediatric Spine Principles and Practice. New York, NY, Raven Press, 1994, pp 1659-1681.
Lenke LG, Orchowski J: Segmental posterior spinal instrumentation: Thoracic spine to sacrum, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 537-552.
Question 48
A patient undergoes a simple excision of a 3-cm superficial mass in the thigh at another institution. The final pathology reveals a leiomyosarcoma, without reference to the margins. What is the recommendation for definitive treatment?
Explanation
a reexcision of the tumor bed is recommended.
REFERENCE: Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 49
An 18-month-old boy with obstetric brachial plexus palsy is being evaluated for limited right shoulder motion. Physical therapy for the past 6 months has failed to result in improvement of the contracture. Which of the following studies is necessary prior to any shoulder reconstruction?
Explanation
REFERENCES: Waters PM: Update on management of pediatric brachial plexus palsy.
J Pediatr Orthop B 2005;14:233-244.
Waters PM, Bae DS: Effect of tendon transfers and extra-articular soft-tissue balancing on glenohumeral development in brachial plexus birth palsy. J Bone Joint Surg Am
2005;87:320-325.
Moukoko D, Ezaki M, Wilkes D, et al: Posterior shoulder dislocation in infants with neonatal brachial plexus palsy. J Bone Joint Surg Am 2004;86:787-793.
Question 50
A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted radial head fracture, and an elbow dislocation. What is the most appropriate treatment?

Explanation
Question 51
The anterior approach to the hip (iliofemoral or Smith-Peterson) puts which of the following anatomic structures at greatest risk?
Explanation
Brachial plexopathy following shoulder taping and application of countertraction
Brachial plexopathy on neck extension for surgical access
Spinal cord injury on neck extension for surgical access
Ulnar neuropathy due to tightly wrapped or malpositioned upper extremities
Cerebral hypoperfusion due to elevation of the head of the bed PREFERRED RESPONSE 1
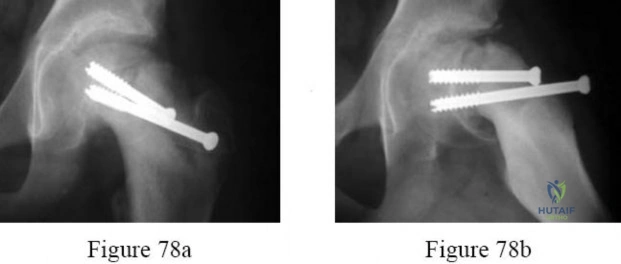
(SBQ12TR.83) A 45-year-old male sustains the fracture seen in Figure A. He is scheduled for open reduction and internal fixation using the Smith-Peterson approach. After dissection through the superficial intermuscular plane, a moderate amount of bleeding is noted in the surgical field. What vessel was likely injured?

Ascending branch of the lateral femoral circumflex artery
Medial femoral circumflex artery
Obturator artery
Superficial external pudendal artery
Femoral vein
Question 52
When elevating the arm, the ratio of scapulothoracic to glenohumeral motion over the total range of motion is best described as
Explanation
REFERENCES: Inman VT, Saunders JR, Abbott LC: Observations of the function of the shoulder joint. Clin Orthop 1996;330:3-12.
Freedman L, Munro RH: Abduction of the arm in the scapular plane: Scapular and glenohumeral movements. J Bone Joint Surg Am 1966;18:1503.
Question 53
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 54
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman with a soft endpoint, varus laxity at 30 degrees, and a positive dial test at 30 degrees that dissipates at 90 degrees of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome? Review Topic
Explanation
(SBQ12SP.35) A 16-year-old male football player is tackled into the ground during a game. He comes to the sideline with unilateral upper extremity pain, burning dysesthesias, and muscle weakness. Several minutes later, his symptoms resolve. In this scenario, what muscles are most likely to be affected? Review Topic
Deltoid and biceps
Triceps
Wrist flexors
Finger flexors
Interossei
This patient presents with a 'burner' or 'stinger,' a transient unilateral neurapraxia that most commonly involves the biceps, deltoid and rotator cuff muscles.
Hypotheses for the mechanism of neurapraxia in stingers include nerve root compression in the neural foramen as a result of extension and compression, traction on the brachial plexus or a direct blow to the plexus. C5-C6 is the most commonly involved level, indicating root injury or upper trunk brachial plexus injury. Unilateral and transient symptoms are required for diagnosis. Bilateral 'stinger' symptoms of numbness, tingling, and weakness are consistent with cervical spinal cord neurapraxia. Return to play in contact sports is contraindicated with bilateral symptoms prior to MRI evaluation of the cervical spine.
Shannon et al. review burner syndrome in athletes. They emphasize that criteria for return to play are based on a complete and thorough neurologic and physical exam. Normal strength and sensation in both upper extremities as well as a normal cervical spine exam (including range of motion, compression, Spurling's, Adson's, and resistive head pressures) are required for return to play. Any positive findings mandate withdrawal of the player from competition.
Illustration A shows hypothesized areas of involvement by mechanism according to
Shannon et al. A, Extension-ipsilateral compression. B, Flexion-contralateral flexion (traction) or direct trauma.
Incorrect Answer Answer Answer
2:
3:
4:
Wrist Finger
Triceps
flexors flexors
C7 C7 C8
Question 55
Figure 21 is the intraoperative fluoroscopic image of a 40-year-old man who felt a pop during a twisting injury to his right ankle. He underwent open reduction and internal fixation (ORIF) of a bimalleolar ankle fracture. During the surgery the medial and lateral malleoli fractures were reduced and rigidly was internally fixed. Following fracture fixation, which additional test is recommended to ensure mortise stability?

Explanation
Following ORIF of a known osseous injury, stress testing of the syndesmosis is recommended, especially for pronation-external rotation injuries. The Cotton test applies a laterally directed force to the fibula to assess for widening of the distal tibiofibular joint space. A positive Cotton test result indicates that syndesmotic stabilization is indicated. The Thompson test is used to determine Achilles tendon integrity. The squeeze test is a clinical, not intraoperative, assessment of syndesmotic injury. The anterior drawer test assesses the integrity of the anterior talofibular ligament.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Pakarinen H, Flinkkilä T, Ohtonen P, Hyvönen P, Lakovaara M, Leppilahti J, Ristiniemi J. Intraoperative assessment of the stability of the distal tibiofibular joint in supination-external rotation injuries of the ankle: sensitivity, specificity, and reliability of two clinical tests. J Bone Joint Surg Am. 2011 Nov 16;93(22):2057-61. doi: 10.2106/JBJS.J.01287. PubMed PMID:
Question 56
What is a known risk factor for lateral distal femoral locking plate failure when used for the fixation of comminuted extra-articular fractures?
Explanation
Implant failure is common in distal femur fractures stabilized with plate fixation. Contributors to failure include a short working length of the construct, plate-screw density more than 0.5 and short plate lengths. This will lead to failure as it causes increased strain on the plate over a short segment, and
does not allow enough motion at the fracture site to form bone for healing by secondary intention.
Ricci et al. reviewed 355 cases of distal femur plate fixation. 64 patients (19%) required reoperation to promote union, including 30 that had a planned staged bone grafting. Risk factors for proximal implant failure included open fracture, smoking, increased body mass index, and shorter plate length.
Kregor et al. reviewed 119 patients with distal femoral plate fixation. They found that 93% fractures healed without acute bone grafting. Complications included 5 losses of proximal fixation, 2 nonunions, and 3 acute infections.
Illustration A is an AP of the distal femur demonstrating a comminuted distal femur fracture which has failed fixation with a laterally based distal femur locking plate. It has undergone varus collapse which is a common mechanism of failure for these injuries. Illustration B is a series of AP radiographs of the distal femur of the same patient that was revised to an intramedullary retrograde nail. Illustration C and D show the concepts of plate length, plate-to-screw density and the working length of the plate.
Incorrect Answers:

OrthoCash 2020
Question 57
Acute redislocation of the glenohumeral joint is a complication that occurs following a first-time dislocation. This is most often seen with
Explanation
REFERENCES: Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment.
J Bone Joint Surg Am 2002;84:1552-1559.
Bigliani LU, Newton PM, Steinmann SP, et al: Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. J Sports Med 1998;26:41-45.
Question 58
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Explanation
REFERENCES: Michelson JD, Magid D, Ney DR, et al, Examination of the pathologic anatomy of ankle fractures. J Trauma 1992;32:65-70.
Marsh JL, Saltzman CL: Ankle fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 2001-2090.
Question 59
Which of the following statements describing chordomas is false?
Explanation
REFERENCE: Casali PG, Stacchiotti S, Sangalli C, et al: Chordoma. Curr Opin Oncol 2007;19:367-370.
Question 60
A 78-year-old man being seen for routine follow-up studies reports mild to moderate pain in his left arm. The patient has a history of lung cancer and severe heart disease. A radiograph and a bone scan are shown in Figures 36a and 36b. Treatment should consist of
Explanation
REFERENCE: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 61
The superior glenohumeral ligament primarily restrains
Explanation
REFERENCES: Warner JJ, Deng XH, Warren RF, et al: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy Orthopaedic Surgeons, 1994, pp 165-177.
Question 62
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 505-520.
Question 63
Figures 85a through 85c are the sagittal and axial CT scans and sagittal T2 MR image of a 21-year-old man who was thrown from his motocross bike earlier in the day. He now has significant low-back pain; however, he is neurologically intact and has no trouble voiding urine. A standing plain radiograph obtained the next day is shown in Figure 85d. Treatment should involve A B C D

Explanation
Disruption of the posterior ligamentous complex is an important determinant of the stability of a burst fracture. This patient is neurologically intact and his MR images do not reveal posterior ligamentous complex (PLC) disruption. The standing radiograph confirms that overall alignment is acceptably and relatively preserved. Nonsurgical treatment with or without a brace is acceptable in this scenario; however, the patient should not be cleared to resume full activity until fracture healing, which may be as long as 3 months after the date of injury. Anterior or posterior surgery should be reserved for patients with PLC disruption, neurological injury, or, in some cases, multiple trauma.
RECOMMENDED READINGS
Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. View Abstract at PubMed
Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Zeiller SC, Anderson DG, Bono CM, Stock GH, Brown AK, Kuklo T, Oner FC. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine (Phila Pa 1976). 2005 Oct 15;30(20):2325-33. PubMed PMID: 16227897. View Abstract at PubMed
Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Lehman RA Jr, Anderson DG, Bono CM, Kuklo T, Oner FC. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005 Jun;18(3):209-15. PubMed PMID: 15905761.View Abstract at PubMed
RESPONSES FOR QUESTIONS 86 THROUGH 89
Proximal junctional kyphosis (PJK)
Adjacent segment degeneration
Intraoperative neurological injury
Postsurgical wound infection
Please select the complication listed above that most commonly is associated with a clinical scenario described below.
Question 64
Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
Explanation
A. Inability to flex the distal interphalangeal joint of the index finger
B. Positive Froment’s sign
C. Weakness with wrist extension
D. Decreased capillary refill
Question 65
What is the preferred treatment of a symptomatic curly toe deformity in a 6-year-old child?
Explanation
REFERENCES: Hamer A, Stanley D, Smith TW: Surgery for curly toe deformity: A
double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood.
J Bone Joint Surg Br 1984;66:770-771.
Question 66
-Use of the shorter, anterior screw may result in
Explanation
Question 67
What is the most appropriate management at this time? Review Topic

Explanation
Question 68
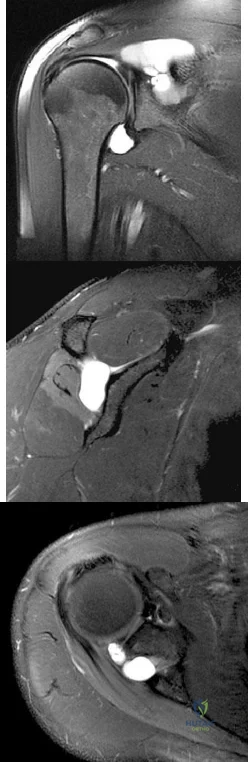
A professional baseball player has had intermittent, mild shoulder pain for the past 2 years. Nonsurgical management has consisted of anti-inflammatory drugs. Examination reveals atrophy of the infraspinatus muscle but not the supraspinatus. There is weakness in external rotation with the arm at his side but not at 90 degrees of abduction. He has no weakness or pain with resisted abduction. Electromyography confirms an isolated lesion of the suprascapular nerve branch to the infraspinatus. He is otherwise neurologically intact. An MRI scan of the shoulder shows no cysts but confirms atrophy of the infraspinatus muscle. What is the next most appropriate step in management?
Explanation
REFERENCES: Cummins CA, Bowen M, Anderson K, et al: Suprascapular nerve entrapment at the spinoglenoid notch in a professional baseball pitcher. Am J Sports Med 1999;27:810-812.
Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Ferretti A, De Carli A, Fontana M: Injury of the suprascapular nerve at the spinoglenoid notch: The natural history of infraspinatus atrophy in volleyball players. Am J Sports Med 1998;26:759-763.
Question 69
Which of the following statements best characterizes polymethylmethacrylate (PMMA) when it is used to secure joint components in bone and to distribute the forces evenly across the bone-implant interface?
Explanation
REFERENCES: Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby, 1998, pp 221-224.
Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 27-33.
Question 70
A 20-year-old college pitcher reports medial elbow pain after 3 innings of hard throwing. He recalls no injury and reports no pain with light throwing. The examination shown in the clinical photograph in Figure 48 reproduces the elbow pain. What is the most likely diagnosis? Review Topic

Explanation
Question 71
Thoracic disk herniations most typically occur at what level of the thoracic spine? Review Topic
Explanation
Question 72
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 73
03 Which of the following findings is the best indication for the use of temporary external fixation of a femoral shaft fracture?

Explanation

These days, femoral shaft fractures at Tulane / Charity are commonly encountered by orthopaedic residents on the night-float team.
Despite the presence of a well-rested 4th year surgeon, definitive orthopaedic fixation is not always the correct answer for each trauma patient.

Tulane defines “Orthopaedic Tunnel Vision” as a condition commonly associated with a young MD at the Bulldog without a proper wing-man, trying to make advances on the wrong patron due to his relatively easy 80-hour work week schedule and a few too many refined hops.

Skeletal Trauma (p. 1967) describes “Orthopaedic Tunnel Vision” as looking at the orthopaedic injury without considering the patient’s injury in general. Femoral shaft fractures are typically high energy injuries which often do not occur in isolation. In these fractures, it is particularly important to not have tunnel vision.

Indications for temporary bridging external fixation includes hemodynamic instability
(ans. 2), acidosis, hypothermjia, hypoxemia, coagulopathy, sepsis or severely contaminated soft tissues that cannot be adequately debrided. Definitive fixation is performed after the general surgical and medical issues have resolved.

The other answer choices, including the type IIIA open fracture are not contraindications to definitive fixation in themselves (typically IM nailing—antegrade or retrograde).
Question 74
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had
Explanation
Question 75
Figures 46a through 46e show the radiographs of a 22-year-old man who injured his wrist in a motorcycle accident. He has no other injuries. What is the best course of action?
Explanation
REFERENCES: Dumontier C, Meyer ZU, Reckendorf G, et al: Radiocarpal dislocations: Classification and proposal for treatment: A review of twenty-seven cases. J Bone Joint Surg Am 2001;83:212.
Bilos ZJ, Pankovich AM, Yelda S: Fracture-dislocation of the radiocarpal joint: A clinical study of five cases. J Bone Joint Surg Am 1977;59:198-203.
Question 76
Figures 20a and 20b are the radiographs of a 19-year-old woman who was involved in a motor vehicle accident. What mechanism of injury is most consistent with the injury?

Explanation
Question 77
A 17-year-old boy underwent open reduction and internal fixation of a navicular fracture 5 days ago. A follow-up examination now reveals a tensely swollen foot with erythema and multiple skin bullae. The patient is febrile and has marked pain with palpation of the entire forefoot and hindfoot. What is the next step in management?
Explanation
REFERENCES: Ault MJ, Geiderman J, Sokolov R: Rapid identification of group A streptococcus as the cause of necrotizing fasciitis. Ann Emerg Med 1996;28:227-230.
McHenry CR, Piotrowski JJ, Pentrinic D, Malangoni MA: Determinants of mortality for necrotizing soft-tissue infections. Ann Surg 1995;221:558-563.
Question 78
The structure that runs just beneath the peroneal tubercle of the calcaneus is the
Explanation
The peroneal tubercle is often a good landmark at which to identify the peroneus longus tendon surgically, and a hypertrophic tubercle has been associated with peroneus longus tendinopathy. Both peroneal tendons curve anteriorly around the tip of the fibula, with the peroneal tubercle separating the 2 tendons at the level of the calcaneus. The peroneus brevis runs in front of the tubercle and the longus behind. The flexor hallucis longus runs through a fibro-osseus tunnel posterior to the hindfoot formed by the posterolateral (os trigonum) and posteromedial tubercle of the talus. The calcaneal fibular ligament attaches to the calcaneus below the posterior facet of the subtalar joint and deep to the peroneal tendons.
RECOMMENDED READINGS
Hyer CF, Dawson JM, Philbin TM, Berlet GC, Lee TH. The peroneal tubercle: description, classification, and relevance to peroneus longus tendon pathology. Foot Ankle Int. 2005 Nov;26(11):947-50. Pub PMID: 16309609.View Abstract at PubMed
Bruce WD, Christofersen MR, Phillips DL. Stenosing tenosynovitis and impingement
of the peroneal tendons associated with hypertrophy of the peroneal tubercle. Foot Ankle Int. 1999 Jul;20(7):464-7. PubMed PMID: 10437932.View Abstract at PubMed
Question 79
Which of the following factors is responsible for causing the distal femur to pivot about a medial axis as the knee moves from full extension into early flexion?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 239-240.
Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, Churchill Livingstone, 1993, pp 1-13.
Question 80
Which structure is shown in Video 27? 27

Explanation
Video 27 shows the medial patellofemoral ligament running from the medial epicondyle of the femur to the medial portion of the patella. The posterior oblique ligament and the superficial medial collateral ligament run from medial epicondyle to the tibia.
RECOMMENDED READINGS
Babb JR, Detterline AJ, Noyes FR. AAOS Orthopaedic Video Theater. The Key to the Knee: A Layer-by-Layer Video Demonstration of Medial and Anterior Aatomy. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:493-568.
Question 81
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
REFERENCES: Montgomery DM, Brower RS: Cervical spondylotic myelopathy: Clinical syndrome and natural history. Orthop Clin North Am 1992;23:487-493.
Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K: Myelopathy hand: New clinical signs of cervical cord damage. J Bone Joint Surg Br 1987;69:215-219.
An HS, Simpson JM: Surgery of the Cervical Spine. Baltimore, MD, Williams and
Wilkins, 1994.
Question 82
.The least gliding resistance for a flexor tendon laceration at the thumb palmar-digital crease as shown inFigure 75 can be achieved with
Explanation

Patient age
Displacement of the radius fracture
Displacement of the ulnar styloid fracture
Position of the ulnar styloid after open reduction and internal fixation of the radius
Stability of the distal radioulnar joint after open reduction and internal fixation of the radius

Question 83
A 42-year-old man sustained the periprosthetic fracture shown in Figures 19a and 19b. The femoral component is well fixed. What is the next most appropriate step in management?
Explanation
REFERENCES: Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Bono JV, McCarthy JC, Thornhill TS, Bierbaum BE, Turner RH (eds): Revision Total Hip Arthroplasty. New York, NY, Springer Verlag, 1999, pp 530-592.
Question 84
A 13-year-old boy has knee pain after sustaining a mild twisting injury while playing basketball 4 weeks ago. Radiographs and MRI scans are shown in Figures 24a through 24d, and biopsy specimens are shown in Figures 24e and 24f. Treatment should consist of
Explanation
REFERENCES: Simon MA, Springfield DS: Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274.
Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 85
A 28-year-old anesthesia resident has aching pain in his dominant right forearm after injuring it while playing basketball 1 week ago. He reports that he is unable to perform regional anesthesia that requires manipulation of a needle. Examination reveals that he is unable to flex the interphalangeal joint of the thumb, and flexion of the distal interphalangeal joint of the index finger is weak. Management should consist of
Explanation
REFERENCES: Miller-Breslow A, Terrono A, Millender LH: Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am 1990;15:493-496.
Stern PJ, Fassler PR: Anterior interosseous nerve compression syndrome, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, 1991, vol 2, pp 983-1002.
Question 86
What muscle is most often encountered during surgical approaches to C5-6?
Explanation
REFERENCES: Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-56.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 87
A 75-year-old female with a longstanding history of brachial plexus palsy 2 . A 63-year-old male with a 6 month history of shoulder pain and inability to abduct past 30 degrees

Explanation
A TSA involves replacement of the humeral head with a metal head and resurfacing of the glenoid to a cemented all-polyethylene surface. In order to achieve optimal results, patients must be selected carefully. Patients with an irreparable rotator cuff tear, non-functioning deltoid, inadequate glenoid bone stock and brachial plexopathy are poor candidates for TSA.
Edwards et al. conducted a multicenter randomized controlled trial to compare TSA versus hemiarthroplasty in patients with primary osteoarthritis of the shoulder. They found that TSA provided better scores for pain, mobility, and activity than hemiarthroplasty at 2 year follow-up. Boileau et al. followed 45 consecutive patients who underwent reverse TSA ( rTSA) for cuff tear arthropathy (CTA), post-traumatic arthritis, and failure of revision arthroplasty. After a mean follow-up of 40 months, they found that the reverse prosthesis improved function and was able to restore active elevation in patients with incongruent cuff-deficient shoulders. They also found that
the results were less predictable and complication and revision rates were higher in patients undergoing revision surgery as compared to those patients undergoing rTSA for CTA.
Illustrations A and B show the preoperative and postoperative x-rays of a patient with characteristic OA of the glenohumeral joint that was treated with TSA.
Incorrect Answers:

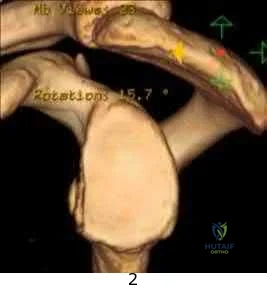
Figure A is a glenoid CT 3D reconstruction of a 26-year-old accountant who has recurrent shoulder instability. His first dislocation occurred after a fall while skiing. He has now sustained his third dislocation, which was reduced in the emergency department prior to being sent to your office. What is the most appropriate definitive treatment?
Immobilization in external rotation for 6 weeks Arthroscopic bony Bankart repair

Arthroscopic Remplissage procedure

Glenoid augmentation using coracoid transfer Glenoid augmentation using tricortical iliac crest graft
This patient has recurrent shoulder instability with a small bony defect of the anterior glenoid and no previous surgery. The most appropriate definitive management in this patient would be arthroscopic bony Bankart repair.
Older (>20 years old), recreational athletes with minor glenoid bone loss (<20 % of the glenoid surface area) may be treated with soft tissue stabilization procedures using suture anchors. Goals of this procedure include tightening and repairing the torn ligament and labrum to the glenoid.
Younger, contact sports athletes with large glenoid defect (>20%) may require bony augmentation type of procedures.
Lynch et al. review the clinical presentation, assessment and treatment algorithm for surgical management of bone loss associated with anterior shoulder instability. While defects larger than 25% of glenoid width should be managed with bony augmentation, they recommend soft-tissue stabilization in smaller defects.
Balg et al. analyzed 131 patients following Bankart procedure and identified following risk factors for failure: age <=20, competitive participation in contact sports, shoulder hyperlaxity, Hill-Sachs on AP radiograph, glenoid bone loss of contour on AP radiograph.
Using human cadaveric shoulders with various anterior glenoid defects sizes, The MOON Shoulder Group compared radiography, MRI and CT to determine the most reliable imaging modality for predicting bone loss. Three-dimensional CT, followed by regular CT were the most reliable and reproducible imaging modalities for predicting glenoid bone loss.
Figure A shows an en face sagittal 3D reconstruction of a glenoid with 10% surface area loss. Incorrect Answers:
A latissimus dorsi tendon transfer is a well established procedure for treatment of massive irreparable posterosuperior rotator cuff tears. All of the following factors have been shown to result in worse clinical outcomes after a transfer EXCEPT?

Nonsynergistic action of the transferred muscle Fatty atrophy of the supraspinatus and infraspinatus Deficiency of the subscapularis

Absence of the coracoacromial ligament Deltoid weakness
A latissimus dorsi tendon transfer can be utilized in patients with a massive, irreperable rotator cuff tear involving the supraspinatus and infraspinatus. It has been reported to relieve pain and improve function in a carefully selected patient population. Those patients with deficiency of the deltoid or subscapularis, nonsynergistic muscle action after transfer, or fatty infiltration of the posterosuperior cuff have worse clinical outcomes. Absence of the CA ligament may allow anterosuperior escape in RC deficient shoulders but has not been shown to lead to worse outcomes after a tendon transfer.
The paper by Warner, et. al demonstrated that poor tendon quality, stage 3/4 muscle fatty degeneration, and detachment of the deltoid insertion each had a statistically significant effect on the Constant score noting that salvage reconstruction of a previous cuff repair had more limited gains as compared to primary. The reference by Ianotti, et. al showed that synchronous in-phase contraction of the transferred latissimus dorsi is associated with a better clinical result while improved preoperative shoulder function and general strength also positively influence the clinical result.
An active 68-year-old woman undergoes an uncomplicated rotator cuff repair with a double-row construct using biocomposite knotless anchors. At her two month follow up, she is noted to have increased shoulder pain, weakness and limited motion. Imaging reveals failure of the rotator cuff repair. What is the most likely mechanism of failure?

Anchor fatigue and breakage Anchor pull out from bone

Suture rupture secondary to anchor eyelet abrasion Suture pull out from the repaired tissue

Infection
Rotator cuff repair (RCR) failure most commonly occurs from a failure of the repaired tissue to heal with suture anchor pull out from the repaired tissue.
The overall complication rate of arthroscopic RCR is roughly 10%. Failed RCR most commonly results from failure to heal (19-94%) secondary to poor rotator cuff tissue, insufficient vascularity or poor bone quality. Other causes of RCR failure include surgical complications (deltoid disruption, infection, foreign body reaction, stiffness, neurologic injury), diagnostic errors (missed lesions of the rotator interval, long head of biceps or subscapularis tear), and technical errors (excessive tension due to lack of proper tissue mobilization, anchor pull out secondary to improper anchor placement).
George et al evaluated the causes of failed RCR and results of revision RCR. While results of revision RCR are inferior to primary RCR, arthroscopic repair yields > 60% good or excellent results. Risk factors for poor results following revision RCR include poor tissue quality, detachment of the deltoid origin and multiple previous surgeries.
Diduch et al reviewed the design and composition of various anchors used in arthroscopic shoulder surgery. Current advancements in the field include highstrength polyethylene sutures, new biocompatible anchor materials (PEEK, biocomposite) and modified designs including knotless systems. With improved strength of the current anchors and repair constructs, the most common mode of arthroscopic RCR failure is now related to tissue failure occurring at the tissue-anchor interface.
Cole et al discussed the different primary rotator cuff repair constructs, including single row, double row, transosseous and transosseous equivalent. The authors concluded that construct selection depends on tear acuity, size and tissue quality. For acute tears < 12mm in anteroposterior length, singlerow configuration likely has sufficient strength to maintain the repair and promote healing. For more chronic tears, poor tissue quality, or tears > 1215 mm in the anteroposterior dimension, the authors recommend double-row or transosseous-equivalent repair to better restore the anatomic footprint and provide optimal mechanical stability to achieve healing. Illustration A is an algorithm from George et al detailing the decision-making process when considering revision RCR for a symptomatic failed RCR.
Incorrect Responses
Biocomposite anchors exhibit high load-to-failure and result in fatigue failure less commonly than metal anchors.

A 32-year-old cross-training athlete awakens with severe left neck and shoulder pain after a day of intense upper body training. Aside from a recent viral illness, he is otherwise healthy. His pain improves, but two weeks later he notes significant left shoulder weakness. Examination reveals weakness of shoulder abduction, forward elevation and external rotation with the arm at his side. Radiographs are normal. Electromyography demonstrates 2+ positive sharp waves and fibrillations. Sensory nerve conduction studies show reduced amplitudes. MRI of the brain, cervical spine and shoulder are shown in Figures A-D, respectively. Which of the following is true of his prognosis?

Decompression will result in improved muscle strength and function.

The patient can expect a gradual return of muscle strength without long term functional deficits. Immunomodulators may decrease the number and severity of his relapses. 4 . Arthroscopic repair will result in the best functional outcomes given the patient's high activity level.
Question 88
A patient sustained the injuries shown in the radiographs and clinical photograph seen in Figures 10a through 10c. The neurovascular examination is normal. The first step in emergent management of the extremity injuries should consist of
Explanation
REFERENCES: Sahin V, Karakas ES, Aksu S, et al: Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-529.
Moed BR, WillsonCarr SE, Watson JT: Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am 2002;84:752-758.
Question 89
A 42-year-old patient undergoes resection of the medial clavicle for painful sternoclavicular degenerative joint disease. The postoperative course is complicated by an increase in symptoms, a medial bump, and subjective tingling in the digits. A clinical photograph and radiograph are shown in Figures 20a and 20b. What is the most appropriate procedure at this time?
Explanation
REFERENCES: Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.
Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Question 90
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of
Explanation
REFERENCES: Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Warner JP, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Sammarco VJ: Os acromiale: Frequency, anatomy, and clinical implications. J Bone Joint Surg Am 2000;82:394-400.
Question 91
In a hypothetical study, an investigator uses pedometers to determine that the 20 women in his activity study averaged 2.1 million steps per year, whereas the 20 men averaged 1.8 million. The p-value for this difference was 0.09. Which of the following is a correct interpretation of the outcome of this study?
Explanation
Question 92
Figures 47a and 47b show the CT scans of a patient who reports persistent pain in the sinus tarsi following a fall. The avulsion fracture fragment remains attached to what ligament?
Explanation
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, p 192.
Robbins MI, Wilson MG, Sella EJ: MR imaging of anterosuperior calcaneal process fractures. Am J Roentgenol 1999;172:475-479.
Question 93
Which of the following best describes the relationship of the median nerve to the flexor carpi radialis tendon just proximal to the carpal canal?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Henry A: Extensile Exposure, ed 3. Edinburgh, UK, Churchill Livingstone, 1995, pp 100-107.
Question 94
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?
Explanation
REFERENCE: Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 2069.
Question 95
Arthritic change in cartilage is characterized by which of the following findings?
Explanation
Question 96
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70° of the right knee. The active arc of motion is from 70° to 90°, and the opposite knee has a flexion contracture of 10°. Both hips are dislocated with flexion contractures of 10°, passive hip motion is from 10° to 90° of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
REFERENCES: Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469.
DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Sells JM, Jaffe KM, Hall JG: Amyoplasia, the most common type of arthrogryposis: The potential for good outcome. Pediatrics 1996;97:225-231.
Question 97
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?
Explanation
REFERENCES: Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Meister K: Injuries to the shoulder in the throwing athlete. Part one: Biomechanics, pathophysiology, classification of injury. Am J Sports Med 2000;28:265-275.
Question 98
A 63-year-old man has a feeling of generalized clumsiness in his arms and hands, difficulty buttoning his shirt, and gradually worsening gait instability. During examination, his neck is gently passively flexed to end range while he is seated. The patient describes an electric shock-like sensation that radiates down the spine and into the extremities. This describes which of the following? Review Topic
Explanation
Question 99
A 41-year-old man is involved in a high-speed motor vehicle crash and sustains a closed femoral midshaft fracture and a unilateral pulmonary contusion with a hemothorax, requiring placement of a chest tube. He has an initial blood pressure of 90/50 mm Hg. After receiving two liters of crystalloid, he has a blood pressure of 115/70 mm Hg and a heart rate of 90 bpm. He has normal mentation and does not require ventilator support. An arterial blood gas reveals that his delta base is
Explanation
Question 100
A 42-year-old man reports persistent arm pain after undergoing intramedullary nailing of a humeral shaft fracture 13 months ago. Physical exam shows near normal shoulder and elbow range-of-motion. Infection work-up is normal. A radiograph is shown in Figure
Explanation
Rubel et al in a combined cadaveric and clinical study comparing one versus two plate constructs for humeral nonunions found that the two plate construct was significantly stiffer, but had no difference in healing rate compared with a single plate construct; 92% of the humeral shaft nonunion patients went onto union with rigid plate fixation.
Ring et al successfully treated a cohort of osteoporotic humeral shaft nonunions with locked plating. They
report 100% union rate with locking plate fixation of these humeral shaft nonunions, with use of autograft in >50% of their cases. Subjective shoulder scores were excellent or good in 22 of 24 patients.
Brinker and O'Connor analyzed the current available evidence for exchange nailing of nonunions and could not recommend this treatment for humeral shaft nonunions.
OrthoCash 2020
