Masterclass: Operative Management of Finger Carpometacarpal Fracture-Dislocations

Key Takeaway
This masterclass provides a comprehensive, intraoperative walkthrough for managing finger carpometacarpal (CMC) fracture-dislocations. Fellows will learn intricate surgical anatomy, precise patient positioning, and granular step-by-step execution from incision to definitive fixation. Emphasizing critical pearls, pitfalls, and postoperative care, this guide ensures a deep understanding of technique, neurovascular protection, and complication management for these challenging hand injuries.
Comprehensive Introduction and Patho-Epidemiology
Carpometacarpal (CMC) joint fracture-dislocations of the fingers represent a formidable challenge within hand trauma surgery, demanding a high index of suspicion, meticulous diagnostic acumen, and exacting surgical precision. Often presenting as subtle abnormalities on initial emergency department radiographs, these injuries are notoriously prone to being missed or misdiagnosed as simple sprains. The failure to recognize and appropriately manage the disruption of the transverse and longitudinal arches of the hand invariably leads to a cascade of debilitating sequelae, including chronic pain, post-traumatic arthritis, marked loss of grip strength, and severe functional impairment. As orthopedic surgeons, our mandate is to aggressively identify these complex injury patterns and restore the delicate architectural framework of the hand to prevent long-term disability.
The pathogenesis of these injuries is rooted in the disruption of the highly specialized articulations between the metacarpal bases and the distal carpal row. A finger CMC joint fracture-dislocation typically manifests as either an intra-articular fracture at the metacarpal base, an avulsion fracture of the corresponding carpal bone, or a pure ligamentous dislocation. The fracture component can involve the base of the metacarpal itself or the articular surfaces of the trapezoid, capitate, or hamate. Given the immense forces transmitted through these joints during power grip and axial loading, the resultant pathoanatomy is often a complex amalgamation of bony comminution and profound ligamentous instability, particularly affecting the dorsal capsuloligamentous complex.
These injuries are broadly categorized by their primary mechanism of injury, which dictates the resulting fracture pattern and displacement vector. Type 1 injuries, which constitute the vast majority of presentations, result from a longitudinal load applied to a flexed metacarpal. This mechanism typically produces a dorsal displacement of the ring and small fingers as a unified block relative to the hamate. The force vector shears the metacarpal bases dorsally, often resulting in a pure dislocation or, more commonly, a marginal avulsion fracture of the dorsal lip of the hamate or the dorsal base of the metacarpal.

Conversely, Type 2 injuries are generated by a direct, high-energy axially directed force along the longitudinal axis of the extended metacarpals. This mechanism is significantly less common but inherently more destructive, often creating a severely comminuted fracture of the articular surface with impaction of the subchondral bone. Severe crushing injuries or high-velocity trauma can lead to multiple, divergent dislocations and diffuse, highly comminuted fractures throughout the entire CMC region, completely obliterating the structural integrity of the carpal arch.


Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the osteology and articular relationships of the CMC joints is non-negotiable for successful operative intervention. The CMC joints connect the metacarpals to the distal carpal row, but the shape, degree of constraint, and biomechanical function vary drastically across the hand. The index and middle finger CMC joints form the rigid central pillar of the hand. These are highly constrained, interlocking articulations; the index metacarpal articulates primarily with the trapezoid in a mortise-and-tenon fashion, while the middle metacarpal keys into the capitate. This rigid construct is essential for providing a stable post against which the thumb can pinch and is crucial for the efficient transfer of longitudinal forces from the hand to the radius.

In stark contrast, the ring and small finger CMC joints exhibit a highly mobile, gliding articulation with the hamate. This mobility—allowing approximately 15 degrees of flexion-extension at the ring finger and up to 30 degrees at the small finger—is biomechanically essential. It permits the ulnar border of the hand to cup and conform around objects, facilitating a powerful and dynamic grip. However, this inherent lack of osseous constraint makes the ulnar CMC joints significantly more susceptible to dislocation. Furthermore, the extensor carpi ulnaris (ECU) tendon inserts robustly onto the dorsoulnar base of the fifth metacarpal. In the setting of a fracture-dislocation, the ECU acts as a relentless deforming force, continuously pulling the fifth metacarpal proximally and dorsally, complicating reduction and necessitating rigid fixation.
The ligamentous architecture stabilizing these joints is complex, comprising dorsal, volar, and interosseous ligaments. The dorsal CMC ligaments are significantly thicker and stronger than their volar counterparts. Consequently, when a deforming force drives the metacarpal bases dorsally, the strong dorsal ligaments often remain intact, instead avulsing a fragment of bone from the metacarpal base or the carpus, creating the classic fracture-dislocation pattern. The volar ligaments, while thinner, provide essential restraint against volar subluxation, while the robust intermetacarpal ligaments tether the metacarpal bases to one another, often causing adjacent metacarpals to dislocate as a single unit, particularly the fourth and fifth.
Protecting critical neurovascular structures is paramount during the dorsal surgical approach. The deep motor branch of the ulnar nerve is exquisitely vulnerable in this region. It courses around the base of the hook of the hamate and runs transversely across the volar surface of the proximal metacarpals to innervate the intrinsic musculature. It can be injured at the time of the initial trauma by a displaced bony fragment or iatrogenically during deep dissection, over-penetration of a drill bit, or aberrant placement of a K-wire. Furthermore, the dorsal cutaneous branches of the ulnar and radial nerves arborize extensively across the surgical field. Meticulous soft tissue handling is required, as iatrogenic laceration of these sensory branches frequently results in debilitating, painful neuromas that can severely compromise the functional outcome of an otherwise technically successful surgery.
Exhaustive Indications and Contraindications
The overarching philosophy in managing CMC fracture-dislocations is that anatomic restoration of the articular surface and rigid stabilization of the carpal arch are absolutely critical to preventing rapid-onset post-traumatic arthritis and chronic grip weakness. Because the natural history of an untreated or inadequately reduced CMC fracture-dislocation is progressive joint subluxation and severe functional impairment, the threshold for operative intervention is exceedingly low. Non-operative management is strictly reserved for the rare, truly non-displaced fracture that demonstrates absolute stability under fluoroscopic stress examination—a scenario that is an exception rather than the rule in high-energy hand trauma.
Absolute indications for immediate or urgent operative intervention include open fracture-dislocations, injuries associated with vascular compromise or acute compartment syndrome of the hand, and irreducible dislocations where soft tissue interposition (such as the extensor tendons or joint capsule) blocks closed reduction. Furthermore, any fracture-dislocation that is unstable following closed reduction—defined by the inability to maintain anatomic alignment without continuous manual pressure—mandates surgical fixation. Poly-traumatized patients also benefit from early rigid fixation of hand injuries to facilitate immediate mobilization and upper extremity weight-bearing during their broader rehabilitation.
Relative indications encompass delayed presentations (injuries recognized several weeks post-trauma) where closed reduction is no longer feasible due to early callus formation and soft tissue contracture. In these cases, open reduction and internal fixation (ORIF), potentially combined with corrective osteotomies or primary arthrodesis depending on the degree of articular cartilage damage, is indicated. Additionally, injuries in high-demand laborers or elite athletes strongly favor operative fixation to guarantee anatomic restoration and expedite return to full functional capacity, minimizing the risk of recurrent instability.
Contraindications to operative management are primarily relative and patient-specific. Severe, unoptimized medical comorbidities that preclude safe anesthesia administration represent a primary contraindication. Active, untreated local infections overlying the surgical site necessitate delaying internal fixation until the soft tissue envelope is sterilized. In severely low-demand, non-ambulatory patients, or those with profound baseline cognitive impairment who cannot comply with post-operative rehabilitation and pin-care protocols, a trial of non-operative cast immobilization may be considered, accepting the high likelihood of a malunion and subsequent deformity.
| Category | Operative Indications | Contraindications |
|---|---|---|
| Absolute | Open fractures, Irreducible dislocations, Vascular compromise, Compartment syndrome | Active local soft tissue infection, Medically unstable for anesthesia |
| Relative | Unstable post-closed reduction, High-demand athlete/laborer, Delayed presentation (>3 weeks) | Low-demand/bedbound patient, Severe non-compliance, Severe osteopenia (modifies fixation choice) |
| Radiographic | >1-2mm articular step-off, Any dorsal subluxation, Loss of metacarpal cascade | Truly non-displaced, stable fracture (rare) |
Pre-Operative Planning, Templating, and Patient Positioning
The operative journey begins with an exhaustive clinical examination and meticulous preoperative planning. A systematic physical examination must assess the entire upper extremity to rule out concomitant injuries. Locally, the hand will exhibit significant dorsal swelling, point tenderness over the affected CMC joints, and a loss of the normal metacarpal cascade. A pronounced rotational deformity of the fingers when making a fist is a hallmark of metacarpal shortening or malrotation. Critically, the neurovascular status must be documented prior to any intervention. The function of the deep motor branch of the ulnar nerve is assessed by testing the strength of the first dorsal interosseous muscle (resisted index finger abduction); preoperative documentation is vital to differentiate trauma-induced neuropathy from an iatrogenic injury post-operatively.
Accurate radiographic imaging is the cornerstone of the preoperative plan, yet standard views are notoriously deceptive. Standard Posteroanterior (PA) views often fail to demonstrate the true extent of the injury due to the overlapping osseous structures of the transverse metacarpal arch. A conventional PA radiograph of the hand creates an oblique projection of the index and middle finger CMC joints when focusing on the ulnar digits, obscuring subtle subluxations.

To accurately visualize the ring and small finger CMC joints, a True Frontal (AP) view is required. The hand must be positioned in an AP projection with the dorsum flat against the cassette, ensuring the base of the affected metacarpal lies perfectly parallel to the imaging plane. Lateral views are equally critical: a semisupinated lateral optimally profiles the index and middle CMC joints, while a semipronated lateral is essential for visualizing dorsal subluxation of the ring and small finger bases.

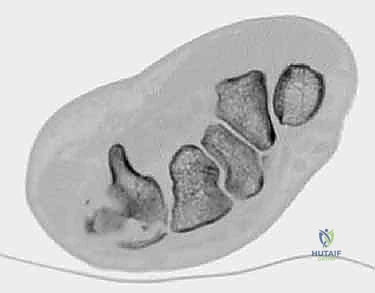
In contemporary orthopedic practice, a high-resolution Computed Tomography (CT) scan is considered indispensable for virtually all complex CMC fracture-dislocations. CT imaging, particularly with 3D reconstructions, provides unparalleled visualization of articular comminution, the size of avulsed fragments, and the exact vector of displacement. It allows the surgeon to map out the fracture lines, determine if the fragments are amenable to screw fixation or require bridging techniques, and identify subtle impaction of the carpal articular surface that would be invisible on plain radiographs.


Patient positioning is standardized to optimize surgical ergonomics and fluoroscopic access. The patient is placed supine with the affected extremity extended on a radiolucent hand table. A well-padded upper arm tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying small articular fragments and protecting delicate neurovascular structures. The C-arm fluoroscopy unit is positioned either parallel or perpendicular to the hand table, allowing for seamless transition between AP, lateral, and oblique views without compromising the sterile field. The surgeon typically sits in the axilla, providing a direct, unobstructed view of the dorsal hand.

Step-by-Step Surgical Approach and Fixation Technique
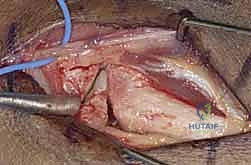
The surgical execution demands a masterful blend of soft tissue respect and rigid biomechanical fixation. A dorsal longitudinal incision is typically employed, centered over the affected CMC joints. For multiple adjacent dislocations (e.g., 4th and 5th digits), a single, slightly curved or straight incision placed in the intermetacarpal valley provides excellent exposure while minimizing skin flap necrosis. Meticulous blunt dissection through the subcutaneous tissues is paramount to identify, mobilize, and protect the dorsal sensory branches of the ulnar and radial nerves, as well as the dorsal venous network, retracting them gently with vessel loops.
Deep exposure requires navigating the extensor tendon compartments. The extensor digitorum communis (EDC) and extensor digiti minimi (EDM) tendons are identified and retracted. The choice of interval depends on the specific joints involved; for the ulnar digits, the interval between the EDC to the ring finger and the EDM provides direct access to the 4th and 5th CMC joints. The dorsal capsule, which is often already torn or avulsed by the injury, is sharply incised longitudinally to expose the articular surfaces. Hematoma and interposed soft tissues are meticulously debrided to allow clear visualization of the fracture margins and the carpal articular facets.


Reduction is achieved through a combination of longitudinal traction applied to the affected digits and direct, firm dorsal-to-volar pressure over the displaced metacarpal bases. If the ECU tendon is acting as a severe deforming force on the 5th metacarpal, a small dental pick or Freer elevator can be used to lever the metacarpal base volarly into its anatomic footprint on the hamate. Once reduced, the joint is provisionally stabilized with 0.045-inch or 0.062-inch Kirschner wires (K-wires). The trajectory of these wires is critical; they can be driven trans-articularly from the metacarpal into the carpus (e.g., 5th metacarpal to hamate) or transversely across the intermetacarpal space into an adjacent, stable metacarpal to re-establish the transverse arch.


Definitive fixation strategy is dictated by the fracture pattern. For simple dislocations or large, non-comminuted avulsion fragments, percutaneous or open K-wire fixation often suffices. However, if a large, distinct articular fragment is present, rigid internal fixation with 1.5mm or 2.0mm lag screws provides superior biomechanical stability and allows for earlier mobilization. In scenarios of severe comminution where screw purchase is impossible, dorsal spanning mini-fragment plates can be utilized in a bridge plating construct to maintain length and alignment while the metaphyseal bone heals. Regardless of the chosen hardware, meticulous fluoroscopic verification in multiple planes is mandatory to confirm anatomic articular reduction and ensure no hardware has penetrated the joint space or compromised the deep motor branch of the ulnar nerve volarly.




Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following CMC fracture-dislocations are not uncommon, primarily due to the high-energy nature of the initial trauma and the delicate anatomy of the region. Post-traumatic arthritis is the most frequent long-term complication, particularly in cases with significant initial articular comminution or residual step-off greater than 1mm. Patients present with chronic, aching pain at the base of the hand, exacerbated by power grip. Salvage management for symptomatic, end-stage arthritis typically involves CMC joint arthrodesis. For the index and middle fingers, arthrodesis is highly successful and well-tolerated due to their naturally rigid nature. However, arthrodesis of the 4th and 5th CMC joints sacrifices their essential mobility, leading to a noticeable decrease in grip strength and dexterity, though it reliably relieves pain.
Hardware-related complications are particularly prevalent when K-wires are utilized. Pin track infections occur in up to 10-15% of cases with percutaneous wires, necessitating aggressive local pin care and oral antibiotics. Deep infections requiring premature hardware removal are rare but devastating. Furthermore, K-wires can migrate, lose fixation, or break, leading to a loss of reduction. If reduction is lost early in the healing phase, revision ORIF with more rigid plate and screw constructs is mandatory. If hardware prominence causes extensor tendon irritation, the hardware must be removed once radiographic union is achieved.
Neurological complications represent a significant source of post-operative morbidity. Iatrogenic injury to the dorsal sensory branches of the radial or ulnar nerves during the surgical approach can result in agonizing neuromas. Prevention through meticulous soft tissue handling is the best strategy; however, established neuromas may require surgical excision and burying of the nerve stump into deep muscle or bone. Injury to the deep motor branch of the ulnar nerve, while rare, results in profound intrinsic muscle weakness. If recognized intra-operatively, primary microscopic repair is indicated; late presentations may require complex tendon transfer surgery to restore pinch and grip mechanics.
Stiffness of the adjacent metacarpophalangeal (MCP) and interphalangeal (IP) joints, along with Complex Regional Pain Syndrome (CRPS), are severe complications driven by prolonged immobilization and aggressive surgical dissection. To mitigate this, rehabilitation protocols must emphasize immediate, unrestricted motion of all non-immobilized joints. If CRPS develops, a multidisciplinary approach involving aggressive hand therapy, neuropathic pain modulators (e.g., gabapentin), and sympathetic nerve blocks is required to salvage hand function.


| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Post-Traumatic Arthritis | 20 - 40% (varies by comminution) | Anatomic articular reduction, rigid fixation | NSAIDs, Injections, CMC Arthrodesis |
| Pin Track Infection | 10 - 15% | Sterile pin insertion, meticulous post-op pin care | Oral antibiotics, premature pin removal if deep |
| Sensory Neuroma | 2 - 5% | Blunt superficial dissection, vessel loop retraction | Neuroma excision, nerve stump burial |
| CRPS / Severe Stiffness | 5 - 10% | Early MCP/IP motion, adequate pain control | Aggressive hand therapy, Sympathetic blocks |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following CMC fracture-dislocation fixation is a delicate balancing act between protecting the fragile osseous repair and preventing debilitating soft tissue contractures. Phase 1 (Weeks 0-2) focuses on strict protection and edema control. Immediately post-operatively, the patient is placed in a bulky, well-padded short-arm volar splint that immobilizes the wrist in slight extension and supports the affected metacarpals, while leaving the MCP and IP joints completely free. The paramount goal during this phase is the immediate, aggressive active range of motion of the fingers and thumb to prevent intrinsic muscle tightness and extensor tendon adhesions. Strict elevation and digital massage are employed to combat edema.
Phase 2 (Weeks 2-6) marks the transition to a more functional, yet protected, state. At the two-week mark, sutures are removed, and the patient is transitioned to
