Comprehensive Guide to Scaphoid Volar Approach: Anatomy, Indications & Surgical Technique
Key Takeaway
The scaphoid volar approach is a surgical technique for treating scaphoid fractures and nonunions. It provides direct access to the scaphoid, crucially preserving its dorsal blood supply, which is vital for healing and preventing avascular necrosis. It's indicated for various pathologies and offers a more aesthetic scar.
Introduction and Epidemiology
Scaphoid fractures represent the most common carpal bone fracture, accounting for 60-70% of all carpal injuries. Their unique anatomy, precarious blood supply, and complex biomechanical role in wrist kinematics render their management challenging, with a notable propensity for nonunion and avascular necrosis. The scaphoid acts as an intercalated segment within the carpus, articulating with the radius, lunate, capitate, and trapezium, making it crucial for maintaining carpal stability and motion.
Epidemiologically, these injuries predominantly affect young, active males between the ages of 15 and 30 years. The classic mechanism of injury is a fall on an outstretched hand with the wrist in forceful hyperextension and radial deviation. Because the scaphoid spans both the proximal and distal carpal rows, it is subjected to significant shear and bending forces during axial loading.
The volar approach to the scaphoid is a well-established surgical technique, offering direct access to the scaphoid tubercle, waist, and distal pole. Its primary advantages include preservation of the critical dorsal blood supply to the proximal pole and a more aesthetically favorable scar. While historically favored for distal pole and waist fractures, its utility has expanded to include challenging nonunions, particularly those involving the volar column, and for placement of long compression screws that traverse the entire scaphoid. Understanding the precise anatomical relationships and meticulous surgical technique is paramount to optimize outcomes and mitigate potential complications.
Surgical Anatomy and Biomechanics
The scaphoid is a boat-shaped carpal bone situated in the distal row of the carpus, acting as a link between the proximal and distal carpal rows. Its unique orientation, lying at approximately a 45-degree angle to the long axis of the forearm in both the sagittal and coronal planes, contributes to its vulnerability to injury and the complexity of its surgical exposure.
Scaphoid Vascularity
The scaphoid blood supply is predominantly retrograde, arising from the radial artery. This anatomical quirk is the primary driver of proximal pole avascular necrosis following fracture.
- Dorsal Carpal Branch: The main blood supply (70-80%) originates from the dorsal carpal branch of the radial artery. This vessel typically enters the scaphoid through multiple foramina along the dorsal ridge, supplying the proximal two-thirds of the bone. Preservation of this dorsal vascularity is a significant advantage of the volar approach, as no dorsal soft tissue stripping is required.
- Volar Carpal Branches: Smaller branches from the volar radial artery supply the scaphoid tubercle and distal pole. While less substantial, these contributions are vital for the viability of the distal scaphoid.
- Nutrient Foramina: The density of nutrient foramina is higher distally, diminishing towards the proximal pole, contributing to the higher incidence of avascular necrosis in proximal pole fractures.
Neurovascular Structures of the Volar Wrist
The volar wrist anatomy is intricate and requires careful dissection to avoid iatrogenic morbidity.
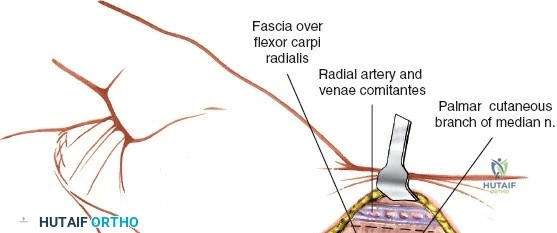
- Radial Artery: The radial artery runs radially to the flexor carpi radialis tendon in the distal forearm and wrist. It lies deep to the abductor pollicis longus and extensor pollicis brevis tendons in the anatomic snuffbox. During the volar approach, it is a primary structure at risk, positioned just radial to the flexor carpi radialis tendon sheath, requiring meticulous retraction.
- Superficial Radial Nerve: While primarily a dorsal risk, branches of the superficial radial nerve supplying sensation to the radial aspect of the hand and thumb can be inadvertently injured during skin incision or superficial dissection if the incision extends too far radially or proximally.
- Palmar Cutaneous Branch of the Median Nerve: This sensory nerve arises from the median nerve approximately 5-7 cm proximal to the wrist crease and traverses superficially, radial to the palmaris longus tendon. It is susceptible to injury during initial skin incision and subcutaneous dissection if an overly radial or oblique incision is utilized.
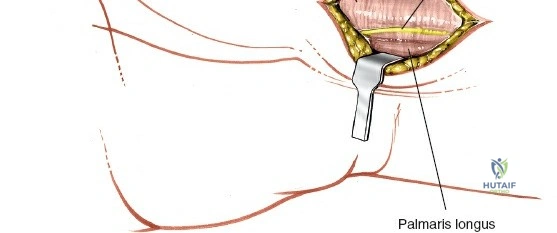
- Flexor Carpi Radialis Tendon: This tendon serves as a key landmark. It lies between the radial artery radially and the palmaris longus ulnarly. The sheath is incised longitudinally to gain access to the underlying structures.
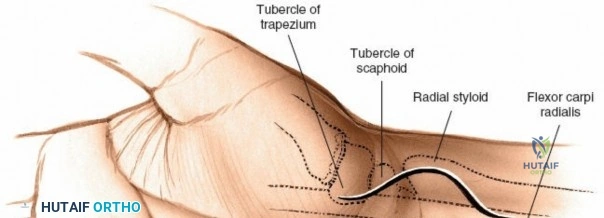
- Scaphoid Tubercle: This palpable prominence on the volar aspect of the wrist is a crucial landmark for initiating the surgical incision and facilitating the identification of the distal pole during the superficial dissection phase.
Carpal Kinematics and Ligamentous Anatomy
The scaphoid is almost entirely covered by articular cartilage, leaving limited surface area for ligamentous attachments and vascular ingress. Volarly, the robust radioscaphocapitate ligament and the long radiolunate ligament provide critical support. The radioscaphocapitate ligament crosses the waist of the scaphoid and acts as a fulcrum around which the scaphoid rotates. During the volar approach, this ligament must be divided to expose the scaphoid waist and subsequently repaired with meticulous precision to prevent postoperative carpal instability, specifically volar intercalated segment instability.
Indications and Contraindications
The decision to proceed with operative fixation of a scaphoid fracture via a volar approach depends on fracture location, displacement, chronicity, and patient-specific functional demands. The volar approach is the gold standard for waist fractures, distal pole fractures, and nonunions with a humpback deformity requiring volar wedge structural grafting. Conversely, fractures of the proximal pole are universally approached dorsally due to the proximal fragment's inaccessibility from the volar side without extensive, destabilizing soft tissue release.
| Clinical Scenario | Operative Indications | Non Operative Indications |
|---|---|---|
| Acute Scaphoid Waist Fracture | Displacement > 1mm, intrascaphoid angle > 35 degrees, radiolunate angle > 15 degrees, high-demand athlete | Nondisplaced, stable fractures in compliant patients |
| Distal Pole Fracture | Intra-articular displacement, symptomatic nonunion | Minimally displaced avulsion fractures |
| Proximal Pole Fracture | Almost all require surgery (Dorsal approach preferred) | Extremely rare to treat non-operatively due to high AVN risk |
| Scaphoid Nonunion | Humpback deformity, cystic changes, avascular necrosis, pain, weakness | Unfit for surgery, asymptomatic established nonunion (rare) |
| Delayed Presentation | Presentation > 4 weeks post-injury with any displacement | Strictly nondisplaced with radiographic signs of early healing |
Contraindications to the volar approach include isolated proximal pole fractures, severe radiocarpal arthritis (scaphoid nonunion advanced collapse stages II-III) where salvage procedures are indicated, and active volar soft tissue infection.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for achieving anatomic reduction and stable fixation. The complex three-dimensional anatomy of the scaphoid demands advanced imaging beyond standard orthogonal radiographs.
Advanced Imaging Modalities
Standard posterior-anterior, lateral, and scaphoid-specific radiographic views often underestimate the degree of displacement and angular deformity. High-resolution computed tomography is the imaging modality of choice. Scans must be reformatted along the true longitudinal axis of the scaphoid (parasagittal and paracoronal planes) rather than the anatomical planes of the wrist. This allows for accurate assessment of the humpback deformity (intrascaphoid angle), comminution, and the exact location of the fracture line. Magnetic resonance imaging is reserved for assessing the vascular status of the proximal pole in cases of established nonunion.
Operating Room Setup
The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded upper arm tourniquet is applied. The fluoroscopy unit (typically a mini C-arm) is brought in perpendicular to the longitudinal axis of the patient, entering from the distal end of the hand table. The monitor should be positioned directly across from the surgeon for ergonomic viewing. The surgeon typically sits in the axilla, with the assistant opposite.
Detailed Surgical Approach and Technique
The volar approach, originally popularized by Russe, provides excellent exposure to the distal two-thirds of the scaphoid. Meticulous execution of each step ensures adequate exposure while minimizing iatrogenic injury.
Incision and Superficial Dissection
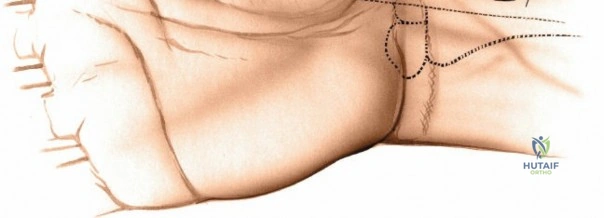
A 4 to 5 cm longitudinal incision is made directly over the flexor carpi radialis tendon, extending distally to the scaphoid tubercle. Some surgeons prefer a slight zigzag or a curved incision crossing the wrist crease obliquely to prevent scar contracture.
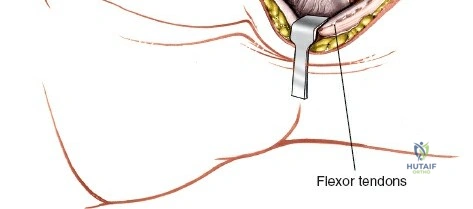
Subcutaneous tissues are bluntly dissected. The palmar cutaneous branch of the median nerve lies ulnar to the flexor carpi radialis tendon and must be protected. The superficial fascia over the flexor carpi radialis tendon is identified, and the tendon sheath is incised longitudinally. The flexor carpi radialis tendon is mobilized and retracted ulnarly. This ulnar retraction is critical as it simultaneously protects the median nerve. The radial artery, located radial to the flexor carpi radialis sheath, is carefully identified and retracted radially.
Deep Dissection and Capsulotomy
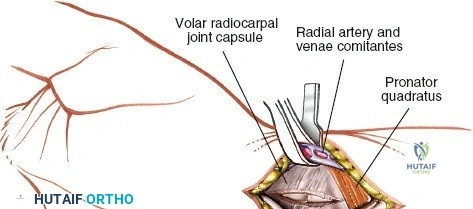
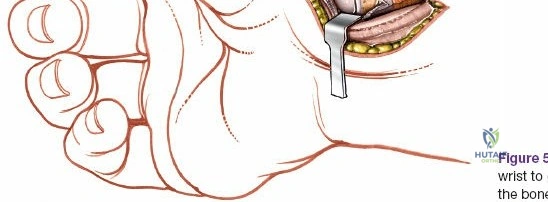
With the flexor carpi radialis tendon retracted ulnarly, the deep posterior layer of the flexor carpi radialis sheath is incised. This exposes the volar wrist capsule and the robust radioscaphocapitate ligament.
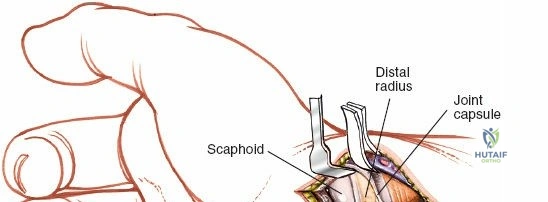
A longitudinal or inverted T-shaped capsulotomy is performed through the radioscaphocapitate ligament to expose the underlying scaphoid. It is absolutely imperative to place heavy non-absorbable tagging sutures in the margins of the divided radioscaphocapitate ligament at this stage. Failure to anatomically repair this ligament during closure will result in postoperative carpal instability. Once the capsule is reflected, the scaphoid tubercle, the waist, and the fracture site are visualized.
Fracture Reduction and Deformity Correction
In acute fractures, a hematoma is evacuated, and the fracture edges are gently debrided with a dental pick or small curette. For nonunions, fibrous tissue and sclerotic bone must be aggressively debrided back to punctate bleeding bone using a high-speed burr or curettes.
Reduction of a scaphoid waist fracture often requires correction of the classic humpback deformity (volar angulation and foreshortening). This is achieved by extending the wrist over a rolled towel, which utilizes the intact dorsal hinge (if present) to open the volar fracture site. Joysticks (0.045-inch Kirschner wires) can be placed in the proximal and distal fragments to manipulate them into anatomic alignment. The reduction is provisionally held with a 0.045-inch K-wire driven from the distal pole toward the proximal pole.
Implant Trajectory and Fixation
Biomechanical studies have definitively shown that a headless compression screw placed down the central longitudinal axis of the scaphoid provides the highest biomechanical stability, greatest resistance to bending forces, and fastest time to union.
Achieving this central axis trajectory from a volar approach requires precise starting point selection. The starting point is typically at the most distal and ulnar aspect of the scaphoid tubercle, often requiring excision of a small portion of the trapezium lip for adequate trajectory.
A guide wire is advanced under multi-planar fluoroscopic guidance. The wire must be perfectly centered in the proximal pole in all views (posterior-anterior, lateral, pronated oblique, and supinated oblique). Once central placement is confirmed, the length is measured. The surgeon must subtract 2 to 4 millimeters from the measured length to ensure the headless screw is completely countersunk beneath the articular cartilage at both ends. The scaphoid is then drilled, and the appropriate length headless compression screw is inserted.
Structural Bone Grafting Techniques
In cases of nonunion with significant bone loss or a persistent humpback deformity after debridement, an interpositional structural bone graft is required. The volar approach facilitates the placement of a volar wedge graft.
Corticocancellous bone is typically harvested from the ipsilateral distal radius volar metaphysis or the iliac crest. The graft is meticulously contoured to fit the defect precisely, restoring the scaphoid's anatomic length and volar alignment. The guide wire for the compression screw is then passed through the distal fragment, through the geometric center of the bone graft, and into the proximal fragment, securing the entire construct.
Complications and Management
Despite meticulous surgical technique, scaphoid fixation carries a risk of significant complications. Early recognition and appropriate salvage strategies are essential for maintaining wrist function.
| Complication | Estimated Incidence | Etiology and Risk Factors | Management and Salvage Strategies |
|---|---|---|---|
| Nonunion | 5-10% (Acute), up to 30% (Revisions) | Inadequate reduction, eccentric screw placement, poor vascularity, smoking | Revision fixation with structural bone grafting (vascularized graft if AVN is present) |
| Avascular Necrosis | 15-30% (Waist), >70% (Proximal Pole) | Disruption of retrograde blood supply, delayed treatment | Vascularized bone grafting (e.g., 1,2 ICSRA), proximal row carpectomy if collapsed |
| Hardware Prominence | 5-15% | Failure to countersink screw, inaccurate measurement | Screw removal after union is achieved |
| Carpal Instability | 2-5% | Failure to repair radioscaphocapitate ligament | Soft tissue reconstruction, partial carpal arthrodesis |
| SNAC Wrist Arthritis | Variable (Depends on union status) | Chronic nonunion leading to altered kinematics and joint wear | Radial styloidectomy, Proximal Row Carpectomy (PRC), Four-corner fusion, Total wrist arthrodesis |
Symptomatic hardware is a frequent complication resulting from the screw head protruding into the scaphotrapezial joint or the tip penetrating the radiocarpal joint. Precise intraoperative fluoroscopy using multiple oblique views is mandatory to confirm that the screw is completely intraosseous. If a patient develops scaphoid nonunion advanced collapse (SNAC), salvage procedures such as proximal row carpectomy or four-corner fusion become necessary, as simple fixation is no longer viable once degenerative articular changes occur.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation must be tailored to the rigidity of the fixation, bone quality, and whether bone grafting was performed. The primary goal is to achieve bony union while preventing debilitating wrist stiffness.
Phase 1 Immobilization (Weeks 0-2):
Immediately postoperatively, the wrist is immobilized in a bulky plaster splint or a short arm thumb spica cast. The wrist is typically positioned in slight extension to relieve tension on the volar capsular repair. Finger range of motion is encouraged immediately to prevent tendon adhesions and reduce edema.
Phase 2 Early Motion and Protection (Weeks 2-6):
At the two-week mark, sutures are removed. If rigid internal fixation was achieved in an acute fracture with excellent bone quality, the patient may be transitioned to a removable thermoplastic thumb spica orthosis. Gentle, active range of motion exercises for the wrist and thumb are initiated under the guidance of a certified hand therapist. Passive stretching and forceful mobilization are strictly contraindicated during this phase. If the surgery involved bone grafting for a nonunion, continuous cast immobilization may be maintained for a full 6 weeks.

Phase 3 Strengthening and Return to Activity (Weeks 6-12+):
At 6 weeks, radiographic evaluation is performed. If early signs of trabecular bridging are visible, the orthosis is discontinued during the day, and progressive strengthening is initiated. Advanced imaging, specifically a fine-cut computed tomography scan along the scaphoid axis, is the definitive gold standard for confirming union before clearing a patient for heavy manual labor or contact sports. Union is generally defined as bridging trabeculae across at least 50% of the fracture cross-section. Return to high-impact activities typically occurs between 10 to 14 weeks, contingent upon CT-confirmed union and restoration of near-normal grip strength.
Summary of Key Literature and Guidelines
The evolution of the volar approach to the scaphoid is deeply rooted in foundational anatomical and biomechanical research.
The seminal work by Gelberman and Menon in 1980 defined the extraosseous and intraosseous vascularity of the scaphoid, definitively proving the retrograde nature of the blood supply. This research forms the biological rationale for utilizing the volar approach to preserve the dominant dorsal carpal branch of the radial artery.
Herbert and Fisher's introduction of the headless compression screw in 1984 revolutionized the operative management of scaphoid fractures. Prior to this, prolonged cast immobilization was the standard, often leading to severe stiffness and high nonunion rates. The Herbert screw allowed for rigid interfragmentary compression beneath the articular surface, facilitating early mobilization.
Biomechanical studies by McCallister et al. have heavily influenced modern surgical technique by demonstrating that screw placement along the central longitudinal axis of the scaphoid provides superior stiffness and load-to-failure compared to screws placed perpendicular to the fracture plane. This central axis concept mandates the precise starting point at the scaphoid tubercle utilized in the modern volar approach.
Current guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH) support operative fixation for all displaced scaphoid fractures (>1mm). Furthermore, there is a growing consensus supporting the surgical fixation of acute, nondisplaced scaphoid waist fractures in young, active patients to accelerate return to work and sport, minimizing the morbidity associated with prolonged cast immobilization. The volar approach remains the workhorse technique for these indications, providing a safe, reliable, and biologically favorable pathway to achieving anatomic reduction and stable fixation.
