Surgical Secrets: Anatomy of the Deep Palmar Space Revealed

Key Takeaway
This article provides essential research regarding Surgical Secrets: Anatomy of the Deep Palmar Space Revealed. The anatomy of the deep palmar space describes a potential area within the central compartment of the palm. Situated between the flexor tendons and the interosseous/adductor pollicis muscles, it is crucial for surgical understanding. This deep space is further divided into medial (midpalmar) and lateral (thenar) spaces by the oblique septum, which is significant for classifying deep palmar infections.
Surgical Secrets Anatomy of the Deep Palmar Space Revealed
Introduction and Epidemiology
The intricate anatomy of the hand, while enabling unparalleled dexterity and function, simultaneously creates complex fascial planes and potential spaces highly susceptible to localized pathology. Among these, the deep palmar space holds significant surgical relevance, often representing a critical area for severe infections, post-traumatic sequelae, and less commonly, tumorous conditions. Understanding the precise three-dimensional architecture of these spaces is paramount for the orthopedic surgeon, enabling accurate diagnosis, judicious pre-operative planning, and meticulous surgical intervention to preserve delicate neurovascular structures and long-term hand function.
Deep palmar space infections, though less common than superficial hand infections, carry a disproportionately high risk of significant morbidity, including widespread tissue necrosis, septic tenosynovitis, joint destruction, and severe functional impairment if not promptly and effectively managed. These infections frequently arise from direct penetrating trauma, spread from contiguous structures like flexor tendon sheaths (Kanavel's signs), or extension from dorsal hand infections. Delays in diagnosis, often due to the deep-seated and sometimes subtle presentation, can lead to aggressive tissue destruction and difficult salvage procedures. Epidemiological data highlight that younger, active individuals are frequently affected, often through occupational or recreational hand injuries, underscoring the socio-economic impact of these conditions. A thorough grasp of the surgical anatomy is thus not merely academic but directly impacts patient outcomes.
Surgical Anatomy and Biomechanics
The palm is an anatomically complex region subdivided into distinct compartments by robust fibrous septa originating from the palmar aponeurosis and inserting onto the metacarpals. These septa serve to compartmentalize intrinsic muscles and neurovascular structures, but also unfortunately delineate pathways for infection spread and potential areas for compartment syndrome.
Overall Palmar Compartmentation
Two primary septa dictate the major divisions of the palm: the thenar septum and the hypothenar septum. The thenar septum arises from the palmar aponeurosis and extends radially to insert onto the first metacarpal. Its function is to separate the three muscles comprising the thenar eminence (abductor pollicis brevis, flexor pollicis brevis, opponens pollicis) from the more central palmar structures. Correspondingly, the hypothenar septum originates from the ulnar side of the palmar aponeurosis and inserts into the fifth metacarpal, effectively isolating the three hypothenar muscles (abductor digiti minimi, flexor digiti minimi brevis, opponens digiti minimi) from the central compartment. This arrangement creates three primary longitudinal compartments within the palm: a thenar compartment, a hypothenar compartment, and a central compartment.

Central Compartment Structures
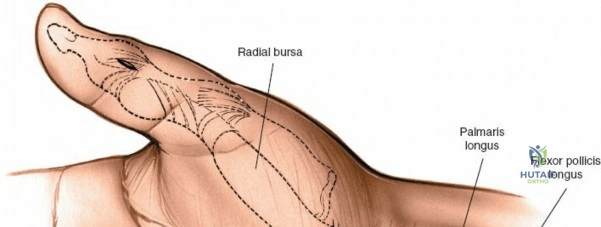
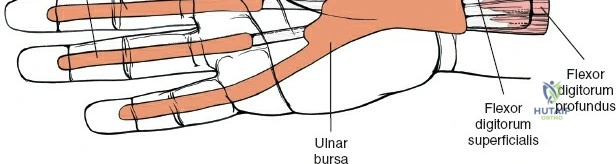
The central compartment is perhaps the most critical from a functional and pathological perspective. It houses a multitude of vital structures: the long flexor tendons to the fingers, the adductor pollicis muscle (although sometimes considered part of the thenar space boundary), the digital nerves and vessels, and the superficial and deep palmar arches. Within this central compartment lies a crucial potential deep space. This space is situated between the superficial layer of flexor tendons and their associated lumbricals (volarly) and the deeper layer consisting of the interosseous muscles and the adductor pollicis muscle (dorsally). This deep palmar space is not a single, unified cavity but is further subdivided by a crucial anatomical partition.
Deep Palmar Space Division by the Oblique Septum
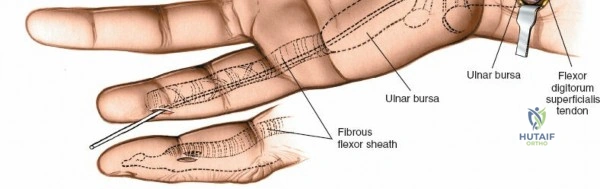
The deep palmar space is bifurcated into two distinct, separate entities: a medial component, traditionally referred to as the midpalmar space, and a lateral component, known as the thenar space. This critical anatomical division is orchestrated by the oblique septum. This septum arises from the connective tissue sheath surrounding the flexor tendons of the middle finger and courses radially and dorsally to attach to the palmar surface of the middle metacarpal. This fibrous partition is the fundamental anatomical basis for the clinical observation that deep palmar infections manifest as two distinct and often isolated pathologies, requiring separate surgical approaches. (This aligns with the clinical division highlighted by the original source's reference 43).
Midpalmar Space Medial Deep Palmar Space
The midpalmar space is the larger and more medially located of the two deep palmar spaces. Its precise boundaries are essential for surgical access and containment of pathology.
* Volar (Superficial) Boundary: Formed by the flexor tendons of the middle, ring, and little fingers, along with the second, third, and fourth lumbrical muscles, all covered by the palmar aponeurosis and overlying skin.
* Dorsal (Deep) Boundary: Composed of the interosseous muscles and the palmar surfaces of the metacarpals (specifically the second, third, and fourth).
* Radial Boundary: Defined by the oblique septum, which separates it from the thenar space.
* Ulnar Boundary: The hypothenar septum, which forms the radial border of the hypothenar compartment.
* Proximal Boundary: Continuously communicates with the carpal tunnel, making it a common pathway for infection spread from the wrist or tenosynovitis.
* Distal Boundary: Communicates with the lumbrical canals leading into the fingers, providing another route for infection propagation.
The primary contents of the midpalmar space include the long flexor tendons of the middle, ring, and small fingers, their associated lumbrical muscles (2nd, 3rd, 4th), and crucially, the deep palmar arterial arch and its accompanying deep branch of the ulnar nerve.
Thenar Space Lateral Deep Palmar Space
The thenar space is the more laterally situated deep palmar space, located radially to the oblique septum. Its boundaries delineate its surgical access and the critical structures contained within.
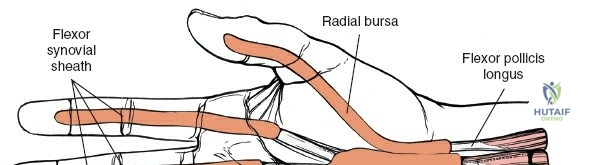
* Volar (Superficial) Boundary: Composed of the flexor pollicis longus (FPL) tendon, the first lumbrical muscle, and the deep aspect of the thenar muscles (specifically the adductor pollicis).
* Dorsal (Deep) Boundary: The adductor pollicis muscle, which also forms part of its ulnar boundary.
* Radial Boundary: Formed by the thenar septum, which separates it from the thenar muscle compartment.
* Ulnar Boundary: Defined by the oblique septum (separating it from the midpalmar space) and the deep aspect of the adductor pollicis.
* Proximal Boundary: Extends proximally towards the carpal tunnel, though less direct communication than the midpalmar space.
* Distal Boundary: Communicates with the first web space (between the thumb and index finger), providing a common pathway for infections, although clinical tracking along the first lumbrical is noted to be rare.
The primary contents of the thenar space are the flexor pollicis longus tendon and the first lumbrical muscle. The deep motor branch of the ulnar nerve and radial artery branches lie in close proximity to its boundaries and must be meticulously protected during surgical interventions.

Surgical Implications of Anatomy
The precise anatomical boundaries and interconnections of these deep palmar spaces have profound surgical implications. Infections originating in the flexor tendon sheaths can track proximally into the carpal tunnel and then spread into the midpalmar space. Similarly, dorsal hand infections, especially those of the web spaces, can penetrate volarly into the thenar space. The presence of the oblique septum is crucial, as it typically prevents direct communication between the midpalmar and thenar spaces, meaning a localized infection usually remains confined to one unless there is severe tissue destruction or iatrogenic breach during surgery. Recognition of these pathways is essential for anticipating the spread of pathology and planning appropriate drainage incisions. Moreover, the proximity of vital neurovascular structures, particularly the deep palmar arch and the branches of the median and ulnar nerves, demands a thorough understanding of their location to prevent iatrogenic injury during surgical access.
Indications and Contraindications
Surgical intervention in the deep palmar space is a critical decision driven by the nature and extent of the pathology, patient comorbidities, and the potential for severe functional compromise.
Indications for Operative Intervention
- Confirmed Deep Palmar Space Abscess: The primary indication for surgical drainage. This is often suggested by clinical signs of fluctuance, severe pain, swelling, erythema, and functional loss, and confirmed by advanced imaging such as ultrasound or MRI demonstrating a well-defined fluid collection within either the midpalmar or thenar space.
- Progressive Infection Despite Non-Operative Management: If cellulitis or a suspected early infection fails to respond to appropriate intravenous antibiotics, elevation, and splinting within 24-48 hours, surgical exploration and debridement are warranted to prevent further spread and tissue destruction.
- Compromise of Neurovascular Structures: Evidence of impending or existing neurovascular compromise due to pressure from an expanding collection (e.g., ischemia of digits, paresthesias, motor weakness) constitutes an urgent surgical indication.
- Infections Involving Flexor Tendons (Septic Tenosynovitis with Extension): While flexor tenosynovitis has its own management protocols, if the infection has clearly extended from the tendon sheath into the deep palmar spaces, drainage of both is necessary.
- Severe Trauma with Open Contamination: Deep penetrating injuries to the palm often require surgical exploration, thorough debridement, and irrigation to prevent deep space infection, especially if foreign bodies are present.
- Tumors Requiring Excision: While less common, certain benign or malignant tumors (e.g., lipomas, nerve sheath tumors, sarcomas) located within the deep palmar spaces may necessitate surgical excision.
Contraindications for Operative Intervention
- Early Cellulitis Without Abscess Formation: Localized erythema, warmth, and tenderness without signs of fluctuance or imaging evidence of pus collection are typically managed initially with conservative measures including antibiotics, elevation, and splinting. Surgical intervention at this stage may lead to unnecessary tissue disruption and increased risk.
- Significant Patient Comorbidities: Severe uncontrolled medical conditions (e.g., unstable cardiac disease, uncorrected coagulopathy) that significantly increase the risk of anesthesia and surgery may necessitate a more conservative, medical management approach, although this is rare for limb-threatening infections.
- Localized Infection Amenable to Non-Operative Management: Superficial infections, paronychia, or felon that have not tracked into the deep spaces can often be managed with local drainage and antibiotics without extensive palmar exploration.
Operative vs Non Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Infection | - Confirmed deep palmar abscess | - Early cellulitis without fluctuance or imaging-confirmed abscess |
| - Progressive infection despite IV antibiotics (24-48h) | - Localized, superficial infections (e.g., paronychia, felon) without deep spread | |
| - Septic tenosynovitis with deep space extension | - Minor soft tissue infections without systemic signs | |
| Trauma | - Penetrating injury with deep space foreign body | - Superficial lacerations without deep contamination |
| - Severe open hand trauma with gross contamination requiring debridement | - Closed soft tissue injuries | |
| Vascular Compromise | - Impending or existing digital ischemia due to mass effect in deep space | - Resolved vascular compromise following conservative measures |
| Tumors | - Symptomatic or rapidly enlarging deep palmar mass | - Asymptomatic, stable, benign lesions where observation is appropriate |
| Neurovascular Risk | - Documented neurovascular compression by deep space pathology | - Neurological symptoms secondary to non-compressive etiologies |
Pre Operative Planning and Patient Positioning
Meticulous pre-operative planning is crucial for optimizing surgical outcomes and minimizing complications in deep palmar space interventions.
Diagnostic Evaluation
- Clinical Assessment: A thorough history and physical examination are the cornerstones. Assessment includes local pain, swelling, erythema, warmth, tenderness, and crucially, any signs of fluctuance. Functional deficits, such as restricted range of motion or weakness, should be documented. Systemic signs of infection (fever, chills, malaise) are important.
- Laboratory Studies: Complete blood count (CBC) with differential, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) are essential to gauge the systemic inflammatory response. Blood cultures should be obtained in febrile patients or those with systemic toxicity.
- Microbiology: Whenever possible, obtain samples for Gram stain, aerobic and anaerobic cultures, and sensitivities pre-operatively if a superficial purulent collection is accessible. This guides empiric antibiotic therapy.
- Imaging:
- Plain Radiographs: Initial screening to rule out osteomyelitis, periostitis, or the presence of radiopaque foreign bodies.
- Ultrasound: A valuable, non-invasive tool to identify fluid collections, differentiate cellulitis from abscess, and guide aspiration for culture. Can also assess vascular flow.
- Magnetic Resonance Imaging (MRI): The gold standard for delineating the precise extent of deep palmar space infections or tumors. MRI can accurately identify fluid collections, demonstrate inflammation of surrounding soft tissues, and detect bone involvement (osteomyelitis) or tendon sheath involvement (tenosynovitis). It is also excellent for tumor characterization and staging.
- Antibiotic Prophylaxis and Management: Empiric broad-spectrum intravenous antibiotics targeting common hand pathogens (Staphylococcus aureus, Streptococcus species, often including MRSA coverage) should be initiated as soon as deep infection is suspected, ideally after cultures are obtained. This regimen should be tailored based on culture and sensitivity results post-operatively.
Anesthesia and Tourniquet Application
- Anesthesia: Depending on patient factors and the anticipated extent of surgery, regional anesthesia (e.g., axillary block, supraclavicular block) or general anesthesia may be employed. Regional blocks offer excellent post-operative pain control but require a cooperative patient.
- Tourniquet Application: An upper arm pneumatic tourniquet is absolutely essential for creating a bloodless surgical field. This allows for meticulous dissection, clear identification of vital structures, and complete debridement, which is paramount in deep space infections. The tourniquet time should be carefully monitored, typically not exceeding 90-120 minutes.
Patient Positioning
The patient is positioned supine on the operating table. The affected arm is abducted and supported on a specialized hand table, allowing for full access to the palm and dorsum of the hand. The forearm may be pronated for approaches primarily targeting the midpalmar space, or supinated for a thenar space approach via the first web space, to optimize exposure and ergonomics for the surgeon.

Detailed Surgical Approach and Technique
The primary goal of surgery for deep palmar space infections is to adequately drain all purulent material, debride necrotic tissue, and relieve any pressure on vital neurovascular structures, while minimizing damage to functioning tissues.
Principles of Incision and Drainage
- Adequate Exposure: Incisions must provide sufficient access to the entire affected space.
- Complete Debridement: All necrotic and infected tissue must be removed.
- Protection of Vital Structures: Meticulous dissection is required to safeguard nerves, vessels, and tendons.
- Effective Drainage: A mechanism for continued drainage (e.g., Penrose drain, open packing) is often necessary.
General Considerations
- Magnification: Use of surgical loupes (2.5x to 4.5x magnification) is highly recommended to enhance visualization of delicate structures.
- Hemostasis: Maintenance of a bloodless field with a tourniquet is critical. Avoidance of electrocautery directly near nerves or tendons is prudent.
Midpalmar Space Drainage
Access to the midpalmar space requires careful consideration of critical neurovascular structures. The goal is to evacuate pus without injuring the digital nerves, vessels, or flexor tendons.
- Incision Options:
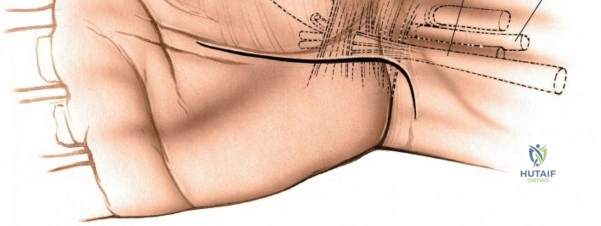
- Transverse Volar Incision: A curvilinear incision made in the distal palmar crease is a common approach. This incision is cosmetically favorable and generally provides good access. It should not extend significantly past the mid-axis of the fourth or second metacarpal to avoid excessive scarring and contracture over flexor tendons.
- Longitudinal Incisions: If more extensive drainage or debridement is required, longitudinal incisions can be made directly over the second, third, or fourth metacarpals in the interosseous interval. Crucially, these incisions must be made carefully and only in the mid-axial line to avoid contracture across flexor creases.
- Dorsal Web Space Incisions: For deeply situated midpalmar abscesses or those extending dorsally, a dorsal incision in the third or fourth web space may provide safe access to drain the space from dorsal to volar, between the metacarpals. This approach may be favored if significant dorsal hand involvement is also present.
- Dissection Technique:
- Skin and Subcutaneous Tissue: Incise the skin and subcutaneous tissue. Avoid deep electrocautery.
- Palmar Aponeurosis: The palmar aponeurosis is encountered next. Carefully incise it longitudinally, respecting the underlying flexor tendons and neurovascular bundles. For a transverse incision, the aponeurosis is incised transversely and then longitudinally between major structures.
- Entering the Space: Once the aponeurosis is opened, the flexor tendons and lumbricals (2nd-4th) are visible. The deep palmar space lies dorsal to these structures. Blunt dissection (e.g., with a curved mosquito hemostat or closed scissors) is used to carefully push the flexor tendons volarly and enter the potential space, aiming towards the metacarpals. Always direct dissection from superficial to deep and radial to ulnar within the midpalmar space.
- Exploration and Debridement: Once entered, purulent material will usually express. Thoroughly explore all recesses of the midpalmar space using a small curette or finger. Remove all necrotic tissue, fibrinous exudates, and foreign bodies. Irrigate the space copiously with sterile saline.
- Drainage: A Penrose drain (or small surgical drain) is typically placed into the deepest part of the space and brought out through a separate stab incision or the primary incision, secured with a skin suture. The primary incision may be left loosely packed with gauze or partially closed with loose sutures to allow for continued drainage and subsequent dressing changes.
Thenar Space Drainage
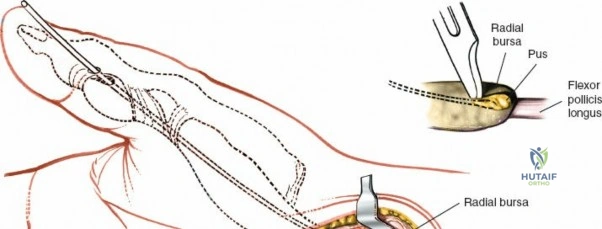
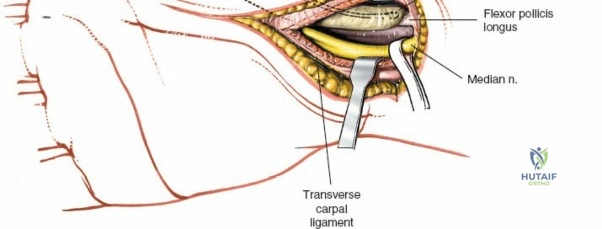
The thenar space is most safely drained via a dorsal approach through the first web space to avoid injury to the motor branch of the median nerve and radial artery.
- Incision Options:
- Dorsal Approach (First Web Space Incision): This is the preferred and safest approach. A longitudinal incision is made along the dorsum of the first web space, just radial to the second metacarpal, extending slightly volar into the web. This allows access to the thenar space from its dorsal aspect.
- Volar Approach (Thenar Crease Incision): Less commonly used due to the high risk of injuring the recurrent motor branch of the median nerve (which lies just superficial to the thenar muscles) and branches of the radial artery. If this approach is necessary (e.g., for direct visualization of a specific volar thenar mass), a short transverse incision parallel to the thenar crease should be used, with extreme caution and meticulous dissection.
- Dissection Technique (Dorsal Approach):
- Skin and Subcutaneous Tissue: Incise the skin and subcutaneous tissue along the chosen line in the first web space.
- Adductor Pollicis: The adductor pollicis muscle is the key deep structure forming the dorsal boundary of the thenar space. Dissection proceeds through the interosseous muscles of the first web space. Blunt dissection is performed carefully along the radial border of the adductor pollicis, gently separating its fibers to access the thenar space.
- Protecting Structures: Be acutely aware of the superficial radial nerve branches and radial artery branches in this area. Dissection should be kept close to the adductor pollicis muscle belly.
- Entering the Space: Once the space is entered, purulence will be observed. The FPL tendon and first lumbrical are located within this space.
- Exploration and Debridement: Explore the space thoroughly, remove necrotic tissue, and irrigate copiously.
- Drainage: A Penrose drain is placed into the thenar space and brought out through the incision. The wound is loosely packed or partially closed.
Post-Drainage Management
Following drainage, the wound is typically left open or loosely packed to allow for ongoing drainage. A sterile dressing is applied, and the hand is placed in a bulky dressing with a splint in a position of function (wrist extended 20-30 degrees, MCPs flexed 70-90 degrees, IPs extended) to promote healing and prevent stiffness. Elevation of the hand is crucial to minimize swelling.
Complications and Management
Despite meticulous surgical technique, complications can arise following deep palmar space interventions. Proactive identification and management are key to optimizing functional recovery.
Common Complications
- Infection Recurrence:
- Incidence: Varies, but can be 5-15%, often due to incomplete drainage, multiloculated abscesses, or resistant organisms.
- Management: Re-exploration, repeat debridement, re-culturing, and adjustment of antibiotic regimen based on sensitivities. Consideration of advanced imaging (MRI) to identify undrained collections.
- Neurovascular Injury:
- Incidence: Direct trauma to digital nerves, branches of the median or ulnar nerves, or palmar arterial arches can occur during dissection. Risk is higher with distorted anatomy due to inflammation or scarring.
- Management: Immediate recognition is paramount. Micro-surgical repair of transected nerves or vessels should be considered. If not immediately recognized, secondary nerve grafting or vascular reconstruction may be necessary. Meticulous surgical technique, proper illumination, and magnification are crucial for prevention.
- Tendon Adhesions and Stiffness:
- Incidence: High, particularly following extensive inflammation and prolonged immobilization. Scar tissue can tether flexor tendons, limiting excursion.
- Management: Aggressive post-operative hand therapy with early active range of motion exercises (as soon as wounds permit), tendon gliding exercises, and dynamic splinting. If severe, recalcitrant adhesions cause significant functional limitation, tenolysis may be considered after several months of conservative treatment and mature scarring.
- Complex Regional Pain Syndrome (CRPS) Type 1:
- Incidence: Variable, but reported in up to 5-10% of hand injuries or surgeries. The inflammatory nature of deep space infections may predispose patients.
- Management: Early recognition of symptoms (pain out of proportion, edema, color/temperature changes). Multidisciplinary approach involving pain management specialists, physical therapists, and occupational therapists. Treatments include nerve blocks, medication (gabapentin, amitriptyline), sympathetic blocks, and graded motor imagery.
- Functional Deficits:
- Incidence: Common, ranging from mild loss of grip strength to severe restriction of digit motion.
- Management: Intensive hand rehabilitation focusing on restoring strength, coordination, and range of motion. Occupational therapy to adapt activities of daily living.
- Scar Contracture:
- Incidence: Especially with transverse palmar incisions or wide dorsal web space incisions if not properly managed.
- Management: Scar massage, silicone sheeting, static/dynamic splinting to counteract contractures. Z-plasty or other reconstructive plastic surgery techniques may be required for severe, functionally limiting contractures.
- Osteomyelitis:
- Incidence: Rare, but can occur if the infection penetrates deeply to involve the metacarpals or phalanges.
- Management: Prolonged, culture-directed intravenous antibiotics. Surgical debridement of infected bone is often necessary, sometimes requiring bone grafting or reconstructive procedures.
Common Complications Incidence and Salvage Strategies
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Infection Recurrence | 5-15% | Repeat I&D, re-culturing, targeted IV antibiotics, imaging (MRI) for residual collections. |
| Neurovascular Injury | <5% | Immediate microsurgical repair if identified intraoperatively; secondary nerve grafting/reconstruction; vascular repair/bypass. |
| Tendon Adhesions & Stiffness | High (20-40%) | Aggressive hand therapy, early mobilization, splinting, tendon gliding exercises; tenolysis for severe, recalcitrant cases. |
| Complex Regional Pain Syndrome | 5-10% | Multidisciplinary pain management, sympathetic blocks, gabapentin/pregabalin, NSAIDs, physical/occupational therapy, desensitization, psychological support. |
| Functional Deficits | Variable (10-30%) | Intensive hand therapy, strengthening, fine motor control exercises, ergonomic modifications, assistive devices. |
| Scar Contracture | 5-10% (severe) | Scar massage, silicone therapy, prolonged splinting; Z-plasty, local flap, or skin grafting for functionally significant contractures. |
| Osteomyelitis | <1% | Prolonged, culture-specific IV antibiotics; surgical debridement of necrotic bone; possibly bone grafting/reconstruction. |
Post Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical component of treatment following deep palmar space surgery, aimed at restoring hand function, preventing stiffness, and minimizing long-term disability. Close collaboration between the surgeon and a certified hand therapist is essential.
Initial Phase 0-7 Days
- Edema Control: Strict elevation of the hand above heart level (e.g., sling or pillow support when supine) is paramount to reduce swelling and pain.
- Immobilization: The hand is typically immobilized in a bulky dressing and a custom-molded static splint in a functional position (wrist extended 20-30 degrees, metacarpophalangeal (MCP) joints flexed 70-90 degrees, interphalangeal (IP) joints extended). This position maintains the collateral ligaments of the MCP joints in a stretched position, preventing shortening and subsequent stiffness. The splint also protects the healing tissues and any drains.
- Wound Care: Regular wound dressing changes are performed, ensuring cleanliness and monitoring for signs of infection. Drain management (if applicable) is crucial, with drains typically removed when output significantly decreases.
- Early Motion: Gentle active range of motion (AROM) exercises for uninvolved joints (shoulder, elbow, wrist flexion/extension) are encouraged to maintain overall limb mobility. Light active finger flexion and extension within the limits of pain and wound integrity may be initiated by the surgeon, particularly for uncomplicated drainage, to prevent tendon adhesions.
Intermediate Phase 1-4 Weeks
- Progressive Mobilization: Once acute inflammation has subsided, wound stability is achieved, and pain is controlled, a more aggressive range of motion program is initiated.
- Active and Passive Range of Motion (AROM/PROM): Gradual progression of AROM and PROM exercises for all digits and the wrist. Focus on composite finger flexion, extension, and isolated joint movements.
- Tendon Gliding Exercises: Crucial for preventing flexor tendon adhesions. Specific exercises for differential gliding of FDS and FDP tendons are implemented.
- Blocking Exercises: Used to isolate motion at specific finger joints, strengthening specific muscle groups.
- Scar Management: As the wound heals, scar massage, silicone gel sheeting, or compression garments are introduced to soften and remodel the scar tissue, reducing contracture risk.
- Desensitization: If nerve irritation or hyper-sensitivity is present, desensitization techniques (e.g., varying textures, vibration) are employed.
- Light Functional Activities: Gradual introduction of light, non-resistive functional tasks to encourage natural hand use.
Advanced Phase 4+ Weeks
- Strengthening: Once a near full, pain-free range of motion is achieved, strengthening exercises are initiated. These include grip strengthening (putty, hand exercisers), pinch strengthening, and endurance activities.
- Return to Activity: Progressive return to work-specific, sport-specific, or daily living activities. Occupational therapy focuses on activity modification and ergonomic assessment to prevent re-injury or exacerbation of symptoms.
- Dynamic Splinting: In cases of persistent stiffness or contracture, dynamic splinting may be utilized to provide a prolonged, low-load stretch, aiming to restore terminal range of motion.
- Long-Term Follow-up: Continued monitoring for residual stiffness, pain, or functional limitations. Adjustments to the rehabilitation program are made based on ongoing assessment. Patient education on self-management strategies and prevention of future issues is reinforced.
Summary of Key Literature and Guidelines
The management of deep palmar space pathologies, particularly infections, has evolved significantly with advances in surgical technique, imaging, and antimicrobial therapy. Historically, landmark descriptions by anatomists and surgeons established the compartmentalization of the hand, laying the groundwork for understanding infection spread. The anatomical divisions detailed by the thenar and hypothenar septa, and critically, the oblique septum (as referenced in the original seed by authors 43 and 44), remain the gold standard for surgical decision-making in the deep palm.
Key literature consistently emphasizes the critical importance of early diagnosis and aggressive surgical drainage for deep palmar space infections. Studies have highlighted that delayed intervention correlates directly with increased morbidity, longer hospital stays, and poorer functional outcomes due to irreversible tissue damage, tendon necrosis, or joint destruction. The role of advanced imaging, particularly MRI, has become indispensable in confirming the presence and precise extent of deep-seated abscesses, differentiating them from cellulitis, and guiding surgical planning to ensure complete drainage while minimizing exploration of uninvolved areas.
Current guidelines advocate for a multidisciplinary approach involving orthopedic hand surgeons, infectious disease specialists, and certified hand therapists. Empiric broad-spectrum intravenous antibiotics, tailored to local resistance patterns and adjusted based on intraoperative cultures and sensitivities, form the medical pillar of treatment. Surgical approaches prioritize safe access, meticulous debridement, and avoidance of critical neurovascular structures. The dorsal approach for thenar space drainage and judicious transverse or longitudinal incisions for the midpalmar space are generally favored to minimize iatrogenic damage and subsequent scar contracture.
Post-operative rehabilitation protocols, focusing on early controlled motion, aggressive scar management, and progressive strengthening, are widely accepted as crucial for optimizing functional recovery and preventing long-term stiffness and adhesions. While specific protocols may vary, the underlying principles of protecting healing tissues while promoting movement are universally applied. Continuous research aims to refine diagnostic algorithms, optimize antimicrobial stewardship, and improve rehabilitation strategies to further enhance outcomes for these complex hand pathologies.
Clinical & Radiographic Imaging