

Comprehensive Introduction and Patho-Epidemiology
The evolution of orthopedic oncology has been defined by a relentless pursuit to replace ablative amputations with durable, functional limb-salvage reconstructions. Proximal and total femur resections, coupled with endoprosthetic reconstruction, represent the zenith of this surgical evolution. Historically, massive neoplastic involvement of the femur—whether from primary bone sarcomas or aggressive metastatic carcinoma—necessitated hip disarticulation or translumbar amputation, procedures fraught with profound psychological devastation and dismal functional outcomes. Today, the modern orthopedic oncologist wields an armamentarium of modular megaprostheses, advanced imaging modalities, and sophisticated soft-tissue reconstruction techniques, transforming what was once a desperate salvage effort into a highly standardized, albeit incredibly complex, reconstructive masterclass.
Epidemiologically, the femur is the most frequent site for both primary malignant bone tumors and skeletal metastases. Osteosarcoma and Ewing sarcoma exhibit a distinct predilection for the femoral metadiaphysis in the pediatric and adolescent populations, while chondrosarcoma frequently targets the proximal femur in adults. Furthermore, the proximal femur is the most common long bone affected by metastatic dissemination from breast, prostate, lung, renal, and thyroid carcinomas. The pathophysiology of these lesions dictates our surgical approach. Primary sarcomas expand radially, compressing surrounding normal tissue to form a reactive pseudocapsule, which must be resected en bloc with a continuous cuff of normal tissue to achieve negative oncologic margins (R0 resection). Conversely, metastatic lesions often present with catastrophic structural failure—the pathologic fracture—which contaminates the local tissue compartments with tumor cells, necessitating wider resections and more complex reconstructions.


The decision to proceed with a proximal or total femur replacement is never made in isolation; it requires a meticulously coordinated multidisciplinary approach. Neoadjuvant chemotherapy, the standard of care for high-grade osteosarcoma and Ewing sarcoma, induces tumor necrosis, reduces the inflammatory pseudocapsule, and facilitates margin-negative resections. However, these systemic therapies simultaneously compromise host immunity and wound healing, significantly elevating the risk of postoperative infection—the dreaded Achilles heel of megaprosthetic reconstruction. Furthermore, preoperative radiation, often utilized for soft tissue sarcomas or localized metastatic disease, severely damages the microvascular network of the skin and muscle flaps, demanding meticulous tissue handling and, frequently, the recruitment of vascularized soft-tissue transfers to ensure adequate implant coverage.
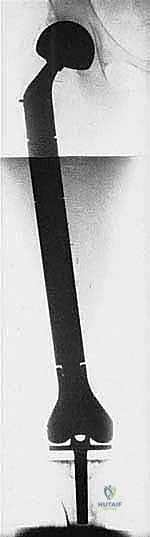
Ultimately, the goal of this procedure transcends mere tumor extirpation; it is the restoration of biomechanical stability, the preservation of limb length, and the facilitation of immediate postoperative mobilization. The shift from custom-cast, monoblock implants to highly versatile, modular titanium and cobalt-chrome systems has revolutionized our ability to adapt to intraoperative realities. We can now intraoperatively fine-tune leg length, femoral version, and joint offset, tailoring the reconstruction to the specific anatomic and biomechanical demands of the patient. This chapter will dissect every nuance of this formidable procedure, equipping the reconstructive surgeon with the knowledge required to navigate the perilous anatomical landscape of the femur and execute a flawless endoprosthetic reconstruction.


Detailed Surgical Anatomy and Biomechanics
Before a single incision is made, the operating surgeon must possess a granular, three-dimensional understanding of the femoral anatomy and its surrounding neurovascular topography. The proximal femur is a complex biomechanical nexus, and its resection profoundly alters the force vectors acting across the hip joint. The intracapsular location of the femoral neck is of paramount oncologic significance. Tumors arising in or extending to the femoral neck can rapidly contaminate the hip joint via the synovial fluid. The ligamentum teres, an often-underappreciated structure, serves as a direct vascular and lymphatic conduit for transarticular skip metastases to the acetabular fovea. While true intra-articular tumor spill is relatively rare in the absence of a pathologic fracture, any preoperative clinical or radiographic suspicion of capsular invasion mandates an extra-articular resection of the hip joint—a significantly more morbid procedure involving the en bloc resection of the acetabulum.
The Abductor Mechanism and Pelvic Stability
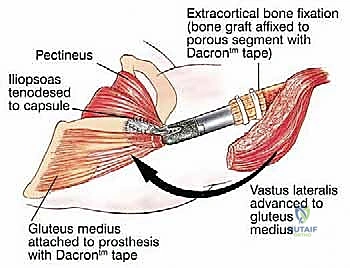
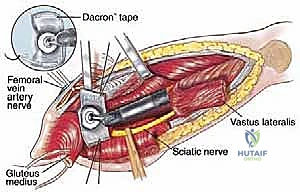
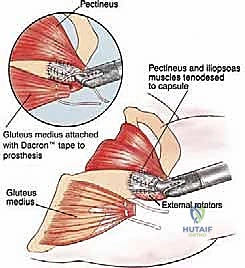
The greater trochanter is the absolute keystone of coronal plane pelvic stability, serving as the insertion site for the gluteus medius and minimus muscles. Resection of the proximal femur invariably sacrifices this bony attachment, rendering the patient profoundly susceptible to Trendelenburg gait and, more disastrously, prosthetic dislocation. The biomechanical imperative of this operation is the meticulous preservation and subsequent reattachment of these tendinous stumps. During the approach, the surgeon must identify the tendinous insertions, tag them with heavy, non-absorbable locking sutures (e.g., #5 Ethibond or FiberWire), and reflect them superiorly. Later, these tendons must be rigidly secured to the trochanteric buildup of the megaprosthesis, often utilizing synthetic meshes (like a Trevira tube) or specialized metallic claw attachments to facilitate soft-tissue ingrowth and restore the abductor moment arm.



Neurovascular Topography: The Femoral Triangle and Sciatic Nerve
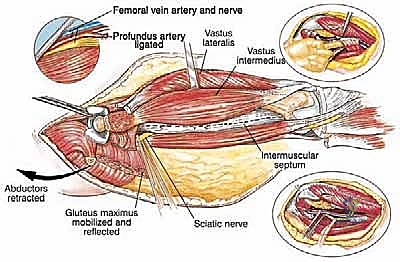
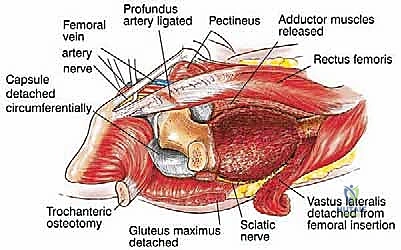
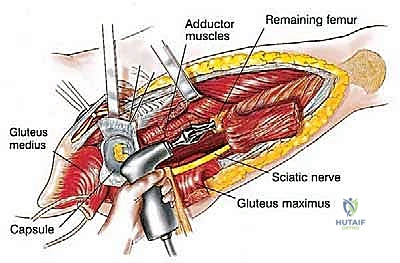
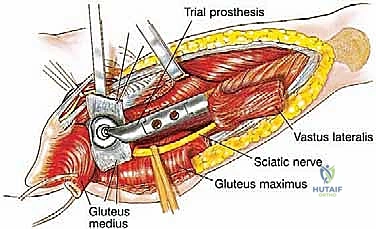
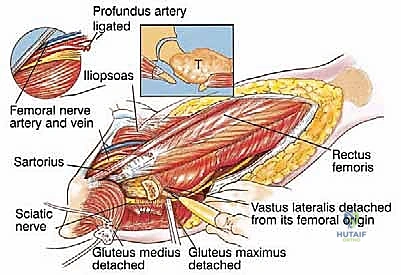
Navigating the medial and posterior aspects of the femur requires absolute precision. Anteriorly, the femoral triangle houses the femoral artery, vein, and nerve. Large, aggressive sarcomas of the proximal medial femur frequently displace or directly encase the profunda femoris artery, which branches laterally from the common femoral artery approximately 4 cm distal to the inguinal ligament. Ligation and en bloc resection of the profunda femoris are often oncologically necessary. While well-tolerated in the pediatric population due to robust collateralization, profunda ligation in older adults with peripheral vascular disease can precipitate catastrophic limb ischemia. Posteriorly, the sciatic nerve descends deep to the gluteus maximus and rests upon the short external rotators. As a tumor expands posteriorly, it typically pushes the external rotators outward, creating a tenuous, stretched barrier between the tumor pseudocapsule and the nerve. Early identification, neurolysis, and continuous protection of the sciatic nerve from the greater sciatic notch to the popliteal fossa are non-negotiable steps in total femur resection.
Distal Femur and Extensor Mechanism Considerations
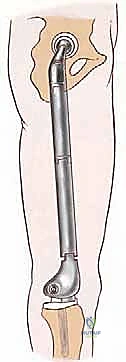
When a total femur replacement is indicated, the anatomical considerations extend to the knee joint and the extensor mechanism. The vastus lateralis, originating from the linea aspera and greater trochanter, is carefully elevated off the lateral intermuscular septum. During this elevation, multiple robust perforating branches from the profunda femoris must be systematically identified, clamped, and ligated to prevent massive postoperative hematoma. Distally, the knee joint capsule must be evaluated. If the distal femoral tumor has breached the articular cartilage or if a pathologic fracture has resulted in a malignant hemarthrosis, an intra-articular resection is contraindicated. In such scenarios, the surgeon must perform an en bloc extra-articular resection of the knee, removing the distal femur, the entire joint capsule, the patella, and the proximal tibial articular surface as a single, uncontaminated specimen, followed by reconstruction with a rotating-hinge knee megaprosthesis.

Exhaustive Indications and Contraindications
Patient selection is the absolute foundation of successful megaprosthetic reconstruction. The indications for proximal and total femur replacement have expanded significantly over the past two decades, driven by advancements in implant survivorship and soft-tissue management. The classic indication remains the presence of a primary malignant bone sarcoma (osteosarcoma, chondrosarcoma, Ewing sarcoma) exhibiting extensive diaphyseal involvement that precludes the retention of a biomechanically viable segment of host bone. Furthermore, massive metastatic lesions—particularly those from renal cell or thyroid carcinoma, which are highly destructive and hypervascular—that present with impending or actual pathologic fractures are prime indications. In these metastatic scenarios, standard intramedullary nailing or plate osteosynthesis is doomed to fail due to the lack of structural bone stock and the inability of irradiated bone to heal; endoprosthetic replacement offers immediate structural stability and pain relief.
Increasingly, these massive implants are being utilized in the revision arthroplasty setting. Non-oncologic indications include catastrophic periprosthetic fractures (Vancouver Type B3) in the elderly, massive aseptic osteolysis with complete loss of proximal femoral bone stock, and the second stage of a two-stage revision for recalcitrant periprosthetic joint infection (PJI). In these revision scenarios, the soft tissue envelope is often severely compromised by multiple prior surgical approaches, scarring, and chronic inflammation, making the reconstruction exponentially more difficult than in a virgin oncologic case. The surgeon must meticulously assess the viability of the abductor mechanism and the adequacy of the soft-tissue coverage before committing to a megaprosthesis in the revision setting.


Despite the versatility of these implants, stringent contraindications exist and must be respected to avoid catastrophic outcomes. Absolute contraindications include the encasement of the major neurovascular bundle (the superficial femoral artery and sciatic nerve) by the tumor, such that a margin-negative resection would require the sacrifice of these structures, rendering the salvaged limb completely ischemic or insensate. In such cases, hip disarticulation remains the oncologically and functionally superior choice. Uncontrollable, active polymicrobial local infection is an absolute contraindication to one-stage endoprosthetic reconstruction; the presence of gross purulence necessitates a radical debridement and the placement of an antibiotic-loaded cement spacer.
Relative contraindications revolve around the patient's physiologic reserve and the local soft-tissue envelope. Severe medical comorbidities that preclude a prolonged general anesthetic or massive fluid shifts make this highly invasive procedure perilous. Furthermore, extensive cutaneous involvement by the tumor or severe radiation-induced skin changes may preclude primary wound closure. While large soft-tissue defects can be managed with pedicled gastrocnemius flaps or free latissimus dorsi transfers, the necessity of a massive free flap significantly increases the morbidity and complexity of the operation, requiring careful preoperative counseling and the involvement of a highly skilled microvascular plastic surgery team.
| Category | Proximal/Total Femur Endoprosthetic Reconstruction |
|---|---|
| Primary Indications | High-grade primary bone sarcomas (Osteosarcoma, Ewing, Chondrosarcoma) with extensive diaphyseal involvement; Massive metastatic bone disease with impending/actual pathologic fracture; Catastrophic bone loss not amenable to standard osteosynthesis. |
| Revision Indications | Vancouver B3 periprosthetic fractures; Massive aseptic osteolysis; Two-stage reconstruction for recalcitrant periprosthetic joint infection (PJI) with severe bone loss. |
| Absolute Contraindications | Encasement of major neurovascular bundles (SFA, Sciatic Nerve) precluding R0 resection without rendering limb non-functional; Active, uncontrolled local purulent infection; Severe medical comorbidities precluding prolonged anesthesia. |
| Relative Contraindications | Extensive soft tissue/skin compromise requiring massive free tissue transfer; Poor patient compliance/inability to adhere to strict postoperative rehabilitation protocols; Severe untreated peripheral vascular disease. |



Pre-Operative Planning, Templating, and Patient Positioning
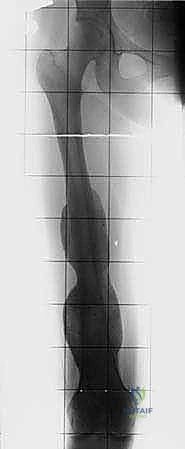
The success or failure of a massive endoprosthetic reconstruction is largely determined before the patient ever enters the operating theater. Meticulous preoperative planning is the cornerstone of this procedure. The imaging suite is our primary intelligence-gathering tool. Full-length, weight-bearing orthogonal plain radiographs of the entire femur, hip, and knee are mandatory to assess overall alignment, leg length discrepancies, and the gross extent of bony destruction. However, the true roadmap for resection is provided by advanced cross-sectional imaging. High-resolution, multi-planar Magnetic Resonance Imaging (MRI) with and without gadolinium contrast is the gold standard for defining the intraosseous extent of the tumor (evaluating for skip metastases within the medullary canal) and delineating the extraosseous soft-tissue mass. The T1-weighted coronal and sagittal sequences are specifically utilized to determine the exact level of the bony osteotomy, aiming for a minimum of 2 to 3 cm of normal marrow beyond the MRI-defined tumor margin.
Angiography and Embolization
For tumors of the proximal femur, particularly highly vascular metastatic lesions (e.g., renal cell carcinoma, thyroid carcinoma) or massive sarcomas extending medially, preoperative CT angiography or conventional catheter angiography is absolutely essential. This maps the iliofemoral vessels, identifies any displacement or encasement of the profunda femoris or superficial femoral artery, and dictates the vascular strategy. If preoperative imaging reveals a highly hypervascular tumor, selective arterial embolization performed 24 to 48 hours prior to surgery is a critical adjunct. Embolization significantly reduces intraoperative blood loss, shrinks the tumor pseudocapsule, and prevents potentially fatal exsanguination during the extensive soft-tissue dissection required for en bloc resection.

Digital Templating and Implant Selection
Modern modular endoprosthetic systems offer unparalleled intraoperative flexibility, but they require precise preoperative digital templating. Using specialized orthopedic software, the surgeon overlays the scaled digital templates onto the patient's CT and plain radiographs. The critical parameters to determine are: 1) The exact resection length required to achieve an R0 margin; 2) The diameter and length of the intramedullary stem for the remaining host bone (deciding between a cemented or press-fit, porous-coated stem based on bone quality and patient age); 3) The required modular body segments to restore anatomic limb length; and 4) The specific trochanteric and articular components. For total femur replacements, the surgeon must also template the distal femoral hinge mechanism and the proximal tibial stem. Despite rigorous templating, the surgeon must ensure that a wide array of backup implant sizes, varying lengths of modular bodies, and different stem diameters are physically present in the operating room, as intraoperative frozen section results may dictate a wider resection than initially planned.
Patient Positioning and OR Setup
The patient is typically placed in the true lateral decubitus position on a radiolucent operating table, with the affected side up. Rigid stabilization using a vacuum beanbag and anterior/posterior pelvic supports is critical, as the procedure involves vigorous manipulation of the limb. Meticulous padding of the dependent axilla (axillary roll), the contralateral fibular head, and all bony prominences is mandatory to prevent devastating neuropraxias during a surgery that can easily exceed 6 to 8 hours. The entire affected extremity, from the costal margin down to the toes, is circumferentially prepped and draped free in a sterile stockinette. This free draping is vital, allowing the surgeon to manipulate the limb through a full range of motion to dislocate the hip, deliver the femur from the wound, and assess the stability and leg length of the final reconstruction. The C-arm fluoroscopy unit must be positioned to enter from the anterior aspect of the patient, allowing seamless AP and lateral imaging of the entire femur without compromising the sterile surgical field.


Step-by-Step Surgical Approach and Fixation Technique
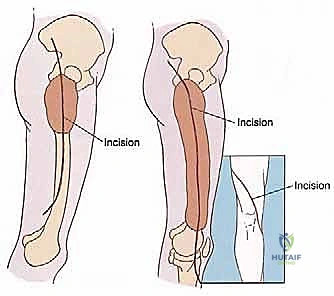
The execution of a proximal or total femur resection is a highly choreographed sequence of anatomical dissection, precise osteotomies, and meticulous reconstruction. The procedure commences with a long, extensile lateral incision. For a proximal resection, the incision begins approximately 5 cm proximal to the greater trochanter, curving gently posterior to the trochanter, and extending distally along the lateral aspect of the thigh, following the longitudinal axis of the femur. For a total femur replacement, this incision is extended distally all the way to the lateral aspect of the tibial tubercle. The subcutaneous tissues are divided in line with the skin incision, and meticulous hemostasis is maintained using electrocautery to minimize postoperative hematoma.
Deep Dissection and Tumor Isolation
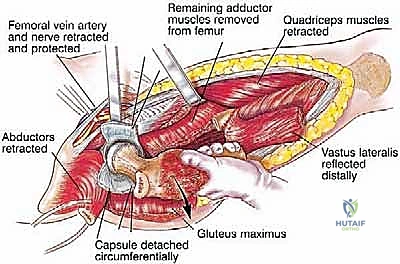
The fascia lata is incised longitudinally. Proximally, the gluteus maximus is split in line with its fibers to expose the short external rotators and the posterior aspect of the hip joint. The sciatic nerve is immediately identified as it emerges from the greater sciatic notch, deep to the piriformis. The nerve is carefully neurolysed, tagged with a vessel loop, and continuously protected throughout the resection. The short external rotators (piriformis, gemelli, obturator internus, quadratus femoris) are transected at their insertions on the femur, leaving a cuff of tissue on the bone to maintain the oncologic margin. Attention is then turned to the critical abductor mechanism. The insertions of the gluteus medius and minimus on the greater trochanter are identified, sharply detached with a robust tendinous cuff, tagged with heavy non-absorbable locking sutures, and reflected superiorly. The iliopsoas tendon is similarly identified at the lesser trochanter, detached, and tagged.

Moving distally, the vastus lateralis is elevated from the lateral intermuscular septum. The surgeon must meticulously identify, clamp, and ligate the multiple perforating branches of the profunda femoris artery that pierce the septum. The medial dissection requires extreme caution. The femoral vessels are retracted anteriorly. If the tumor extends medially, the profunda femoris artery and vein are identified, isolated, and ligated at their origins to allow for safe en bloc resection of the tumor mass. Once the circumferential soft-tissue dissection is complete and the tumor is isolated with wide margins, the hip capsule is incised (assuming no intra-articular involvement), and the hip is dislocated anteriorly.
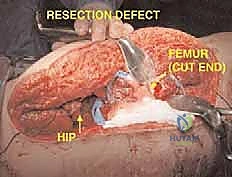
Osteotomy, Preparation, and Reconstruction
Using a sterile ruler and fluoroscopic guidance, the exact level of the femoral osteotomy is marked based on the preoperative MRI templating. The osteotomy is performed using an oscillating saw. The resected specimen is immediately handed off the field, and a marrow scraping from the remaining host bone is sent for stat frozen section analysis to definitively confirm a negative oncologic margin. If the margin is positive, further bone must be resected.


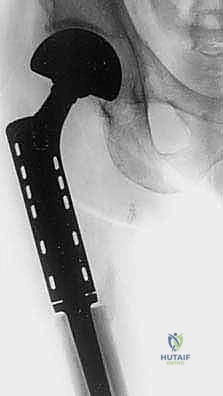
Once margins are cleared, the reconstruction phase begins. The distal femoral canal is sequentially reamed and broached to accept the definitive stem. If a cemented stem is chosen (typical for older patients or irradiated bone), a cement restrictor is placed, the canal is pulsatile lavaged, dried, and polymethylmethacrylate (PMMA) bone cement is injected in a retrograde fashion. The modular prosthesis is then assembled on the back table. The components—stem, intercalary segments, proximal body, and femoral head—are impacted together, ensuring the Morse tapers are clean and dry to prevent fretting and cold welding failures.
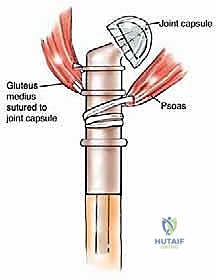
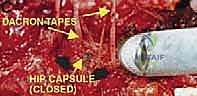
The most critical phase of the reconstruction is the soft-tissue reattachment. The tagged abductor tendons (gluteus medius/minimus) are rigidly secured to the lateral aspect of the proximal prosthetic body. Modern implants feature porous-coated trochanteric buildups and metallic suture loops specifically designed for this purpose. Many surgeons augment this repair by wrapping the proximal prosthesis in a synthetic mesh (e.g., Trevira tube) or an acellular dermal matrix, sewing the host tendons directly into the mesh to promote robust fibrovascular ingrowth. The iliopsoas is similarly reattached to the medial aspect of the prosthesis. Meticulous, multi-layered closure over deep subfascial closed-suction drains is imperative to eliminate dead space and minimize the risk of catastrophic postoperative infection.



















Detailed Chapters & Topics
Dive deeper into specialized chapters regarding proximal-and-total-femur-resection-with-endoprosthetic-reconstruction