Pediatric Forearm Shaft Fractures: Flexible Intramedullary Nailing Masterclass

Key Takeaway
This masterclass provides an exhaustive, real-time guide to flexible intramedullary nailing for pediatric forearm shaft fractures. We cover essential anatomy, meticulous preoperative planning, and a granular, step-by-step intraoperative execution from a surgeon's perspective. Fellows will learn precise techniques, critical pearls, potential pitfalls, and comprehensive postoperative management protocols for optimal patient outcomes.
Introduction and Epidemiology
Forearm shaft fractures represent the third most common fracture encountered in the pediatric population, accounting for approximately forty percent of all pediatric fractures. The bimodal distribution of these injuries typically peaks first in early childhood (ages 5 to 8) due to low-energy falls, and subsequently in early adolescence (ages 11 to 14) associated with higher-energy sports, recreational activities, and increased body mass. Historically, closed fracture care with manipulation and cast immobilization has been highly successful in the large majority of children who sustain forearm shaft fractures, particularly for incomplete, greenstick, or plastic deformation fracture patterns.
However, the management paradigm shifts significantly as patients approach skeletal maturity. For children who are eight to ten years of age and older presenting with complete, displaced fracture patterns, the limits of acceptable displacement—specifically regarding angulation, rotation, and translation—become markedly more strict. In this demographic, the remaining growth potential is often insufficient to reliably remodel significant residual deformity. Consequently, the likelihood of surgical intervention increases to restore anatomic alignment, preserve forearm rotation, and prevent long-term functional deficits.
Over the past two decades, intramedullary fixation, primarily utilizing titanium elastic nails (TENs) or elastic stable intramedullary nailing (ESIN), has emerged as the gold standard for pediatric unstable forearm shaft fractures. This technique operates on the principle of relative stability, offering a minimally invasive approach that preserves the fracture hematoma and vital periosteal blood supply. By establishing three-point biomechanical fixation within the medullary canal, ESIN provides sufficient stability to maintain alignment during osseous union while avoiding the extensive soft tissue stripping associated with traditional plate osteosynthesis.

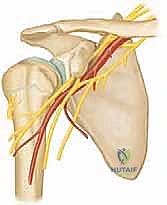
Surgical Anatomy and Biomechanics
The forearm represents a complex, largely nonsynovial, two-bone joint that facilitates a high-amplitude range of motion, typically allowing roughly 180 degrees of pronosupination. The mechanical axis of forearm rotation passes obliquely from the center of the radial head proximally to the fovea of the ulnar head distally. The interosseous membrane (IOM) spans the space between the radius and ulna, playing a critical role in longitudinal load transfer and dynamic stability.
In the fully supinated anteroposterior plane, the radius exhibits a natural lateral bow, which is biomechanically critical for clearing the ulna during pronation. The ulna, conversely, is relatively straight acting as the stable axis around which the radius rotates. In the lateral plane, both bones maintain a predominantly straight alignment. Restoration of the maximum radial bow—typically located at the middle-to-distal third junction of the diaphysis—is a critical surgical objective. Failure to restore this anatomic contour correlates directly with a mechanical block and subsequent loss of forearm rotation.
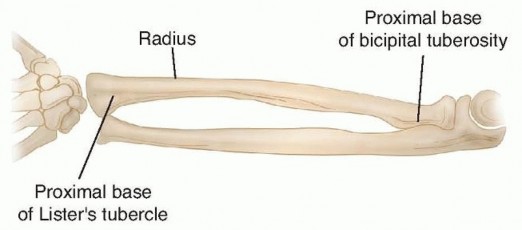
Anatomically, the diaphysis of the radius extends from the most proximal aspect of the tubercle of Lister—approximating the distal metaphyseal-diaphyseal junction—to the proximal base of the bicipital tuberosity. The shaft of the ulna corresponds to these same longitudinal landmarks. In the unfractured state, the normal orientation of the radial styloid and bicipital tuberosity is slightly less than 180 degrees from one another, whereas the ulnar styloid and coronoid process approximate a true 180-degree relationship.
Deforming Muscular Forces
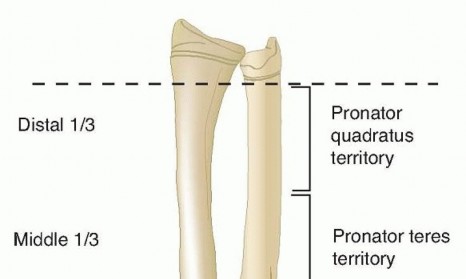
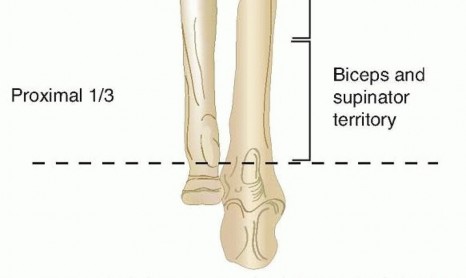
Classically, forearm shaft fractures are divided into three anatomic zones, which offer insight into the predictable deforming forces acting upon the fractured segments. Understanding these forces is paramount for executing successful closed reduction maneuvers:
1. Proximal Third (Biceps and Supinator Region): Fractures proximal to the insertion of the pronator teres result in the proximal fragment being flexed and strongly supinated by the biceps brachii and supinator muscles. The distal fragment is pronated by the pronator teres and pronator quadratus.
2. Central Third (Pronator Teres Region): Fractures in the middle third, distal to the pronator teres insertion, result in a proximal fragment that is maintained in neutral rotation (the supinating forces of the biceps/supinator are balanced by the pronating force of the pronator teres). The distal fragment is pronated by the pronator quadratus.
3. Distal Third (Pronator Quadratus Region): Fractures here typically result in the proximal fragment being pronated, while the distal fragment is drawn proximally and volarly by the brachioradialis and digital flexors.
Natural History of Remodeling
The remodeling potential of the pediatric forearm shaft is robust but finite. Spontaneous correction of malaligned shaft fractures in young children occurs via three primary mechanisms:
* Adjacent physes produce "straight bone" via normal longitudinal growth, gradually distancing the deformity from the joint.
* Physeal orientation adapts to correct the mechanical axis via the Hueter-Volkmann law (increased compression inhibits physeal growth, while decreased compression stimulates growth).
* True diaphyseal shaft remodeling occurs via Wolff's law, where bone remodels in response to the mechanical stresses placed upon it (resorption on the convex side and deposition on the concave side).
Remodeling is most effective in the plane of joint motion (sagittal plane) and in younger patients (< 8 years old). Rotational malalignment and mid-diaphyseal translation exhibit minimal to no remodeling potential, regardless of age.

Indications and Contraindications
The decision to proceed with intramedullary fixation of forearm shaft fractures relies heavily on patient age, fracture pattern, and the ability to achieve and maintain an acceptable closed reduction. While absolute indications are rare, relative indications are heavily weighted by the predictable loss of function associated with malunion in older children and adolescents.
Single-bone forearm shaft fractures must be evaluated with high suspicion for associated radioulnar joint disruptions, specifically Galeazzi (distal radius fracture with distal radioulnar joint disruption) or Monteggia (proximal ulna fracture with radial head dislocation) fracture-dislocations. These complex patterns almost universally require operative stabilization to restore joint congruity and prevent chronic instability.


| Parameter | Operative Indications (Intramedullary Nailing) | Non-Operative Indications (Closed Reduction and Casting) |
|---|---|---|
| Patient Age | > 10 years old (limited remodeling potential) | < 8 years old (high remodeling potential) |
| Angulation | > 10 degrees in children > 10 years; > 15-20 degrees in younger children | < 10 degrees in older children; < 15-20 degrees in younger |
| Rotation | > 30 degrees of malrotation | < 30 degrees of malrotation |
| Translation | Complete displacement (100% off-ended) lacking cortical contact | > 50% cortical apposition |
| Fracture Pattern | Segmental fractures, floating elbow, polytrauma, open fractures | Simple transverse, short oblique, or greenstick fractures |
| Clinical Course | Loss of acceptable reduction in cast; refracture | Stable reduction maintained over serial radiographic follow-up |
Contraindications to elastic intramedullary nailing include active local or systemic infection. Relative contraindications involve fracture locations that are extremely proximal or extremely distal (metaphyseal fractures), where an intramedullary nail fails to provide adequate three-point fixation within the diaphysis, leading to a "bell-clapper" effect and loss of reduction. Furthermore, severe comminution or significant bone loss may preclude the use of flexible nails, as they do not provide rigid axial stability and cannot prevent shortening; such cases necessitate rigid plate osteosynthesis.

Pre Operative Planning and Patient Positioning
Thorough preoperative planning begins with high-quality, orthogonal anteroposterior and lateral radiographs of the entire forearm, strictly including the wrist and elbow joints. This is mandatory to fully characterize the fracture geometry and rule out associated Monteggia or Galeazzi variants, which would fundamentally alter the surgical approach.
Nail Sizing and Selection
Appropriate nail diameter is critical for achieving a stable interference fit within the medullary canal. The standard rule dictates that the maximum diameter of a single elastic nail should be approximately 40% (or roughly one-third to one-half) of the narrowest diameter of the diaphysis measured on the AP and lateral radiographs. For the pediatric forearm, this typically translates to nail diameters ranging from 1.5 mm to 2.5 mm, depending on the patient's size. Both the radius and ulna should ideally be instrumented with nails of the same diameter to ensure balanced biomechanical forces and prevent asymmetric tensioning of the interosseous membrane, although slight variations are acceptable if anatomic constraints dictate.

Patient Positioning and Setup
The patient is placed supine on the operating table. The operative extremity is positioned on a radiolucent hand table to allow unencumbered fluoroscopic imaging in multiple planes. A non-sterile tourniquet is applied to the proximal arm but is often not inflated unless a formal open reduction becomes necessary.
The fluoroscopy unit (C-arm) is typically brought in either parallel to the arm board or perpendicular from the foot of the table, depending on surgeon preference and operating room layout. It is imperative to confirm that clear AP and lateral images of the entire forearm, wrist, and elbow can be obtained prior to surgical prep and drape. The surgeon should be able to visualize the entire length of the bone to ensure the nail does not inadvertently breach the cortex or cross a physis.

Detailed Surgical Approach and Technique
The procedure typically involves closed reduction and percutaneous or mini-open intramedullary nailing. The sequence of fixation is generally dictated by the fracture pattern; the less displaced or more easily reducible fracture is often stabilized first to provide a stable column, facilitating the reduction of the second bone.
Ulnar Nailing Technique
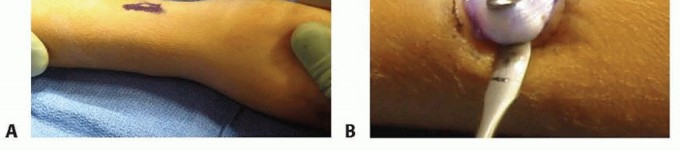
- Entry Point Localization: The entry point for the ulna is located on the lateral aspect of the proximal ulnar metaphysis, approximately 1 to 2 cm distal to the olecranon apophysis. This lateral entry avoids the ulnar nerve medially and the olecranon bursa posteriorly.
- Incision and Preparation: A 1 cm longitudinal incision is made. Blunt dissection is carried down to the periosteum using a hemostat to protect cutaneous nerves.
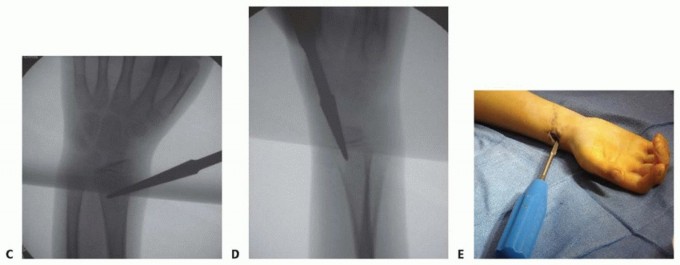
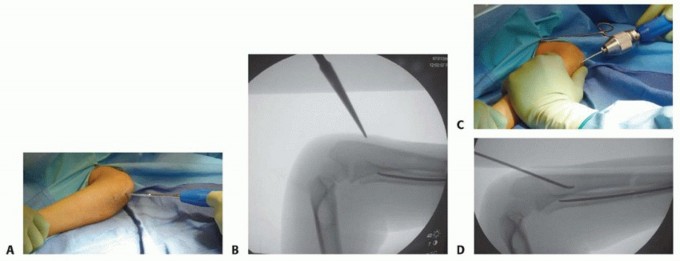
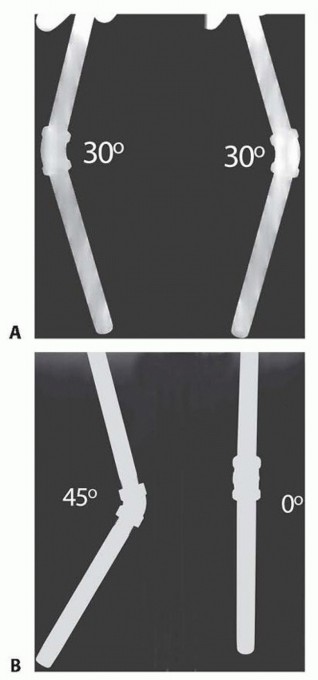
- Cortical Fenestration: An awl or drill is used to breach the near cortex. The instrument is initially directed perpendicular to the bone to prevent skiving, then lowered to a 45-degree angle relative to the longitudinal axis of the shaft to create an oblique track, facilitating smooth nail insertion.
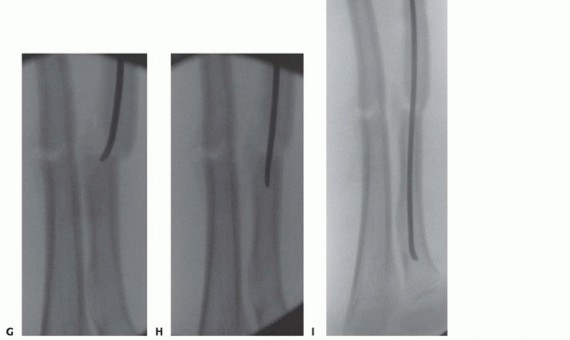
- Nail Passage: The selected titanium elastic nail, pre-bent with a slight curve at the tip to aid in navigation and reduction, is introduced into the medullary canal. It is advanced using a T-handle chuck with oscillating movements to the level of the fracture.
- Fracture Reduction: Closed reduction maneuvers are performed. The nail tip can be used as a "joystick" to manipulate the proximal fragment into alignment with the distal segment.
- Crossing the Fracture: Once aligned, the nail is advanced across the fracture site into the distal metaphysis, stopping just short of the distal ulnar physis to prevent growth arrest.

Radial Nailing Technique
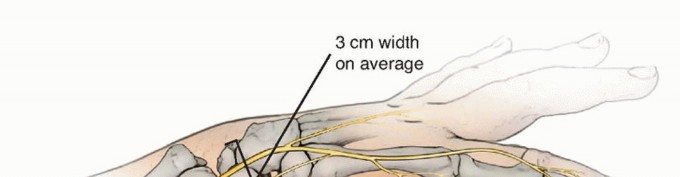
- Entry Point Localization: The radius is typically approached distally. The entry point is on the lateral aspect of the distal radius, approximately 1.5 to 2 cm proximal to the distal radial physis, safely out of the joint capsule.
- Incision and Nerve Protection: A 1 to 2 cm longitudinal incision is made over the lateral distal radius. Meticulous blunt dissection is mandatory in this region to identify and protect the branches of the superficial radial nerve (SRN), which are highly susceptible to iatrogenic injury.
- Cortical Fenestration: Similar to the ulna, an awl or drill creates an oblique entry hole proximal to the physis, taking care not to violate the growth plate.
- Nail Passage and Reduction: The pre-bent radial nail is advanced retrogradely to the fracture site. The radial bow must be respected; the concavity of the nail should align with the natural concavity of the radius. The nail is contoured prior to insertion to recreate the maximum radial bow.
- Crossing the Fracture: The nail is advanced across the fracture into the proximal radial metaphysis, stopping distal to the proximal radial physis and the bicipital tuberosity.


Open Reduction Techniques
If closed reduction cannot be achieved after reasonable attempts (often due to soft tissue interposition, such as muscle, periosteum, or the interosseous membrane), a mini-open reduction is indicated. A small (2-3 cm) incision is made directly over the fracture site. The internervous planes utilized depend on the level of the fracture (e.g., between the extensor carpi radialis brevis and extensor digitorum communis for the middle third of the radius). The interposed tissue is meticulously cleared, the fracture is reduced under direct vision, and the nail is subsequently passed under direct visualization.

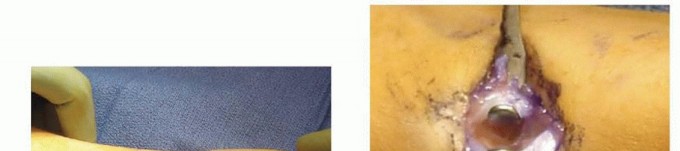
Final Seating and Cutting
Once both nails are across the fracture sites and adequate reduction is confirmed via orthogonal fluoroscopy, the nails are cut. It is imperative to leave approximately 1 to 1.5 cm of the nail protruding from the cortex to facilitate future hardware removal. However, the ends must be carefully bent and buried deep to the subcutaneous tissue to minimize skin irritation, bursa formation, and the risk of extensor tendon rupture.
Complications and Management
While intramedullary fixation of pediatric forearm fractures yields excellent outcomes, complications can occur. Meticulous surgical technique, appropriate implant selection, and adherence to biomechanical principles mitigate many of these risks.

| Complication | Estimated Incidence | Etiology and Clinical Presentation | Salvage and Management Strategies |
|---|---|---|---|
| Symptomatic Hardware | 10% - 15% | Nail ends left too long or insufficiently buried, causing skin irritation, bursa formation, or pain. | Local wound care; early hardware removal once robust radiographic union is confirmed (typically > 6 months). |
| Delayed Union / Nonunion | 1% - 3% | Distraction at the fracture site, inadequate stabilization, failure to achieve cortical contact, or infection. | Observation if asymptomatic and progressing; revision fixation with rigid plate osteosynthesis and autologous bone grafting if established nonunion. |
| Loss of Forearm Rotation | 5% - 10% | Failure to restore the radial bow, unrecognized cross-union (synostosis), or prolonged immobilization. | Aggressive physical therapy; corrective osteotomy if the functional deficit is severe and skeletal maturity is reached. |
| Extensor Pollicis Longus (EPL) Rupture | < 1% | Prominent distal radial nail causing attritional wear on the EPL tendon at Lister's tubercle. | Hardware removal; tendon transfer (e.g., Extensor Indicis Proprius to EPL) for functional restoration. |
| Superficial Radial Nerve Injury | 2% - 5% | Iatrogenic injury during the distal radius approach. Presents as paresthesia, numbness, or painful neuroma. | Observation (most are traction neuropraxias that resolve spontaneously); neuroma excision and capping if chronic and debilitating. |
| Compartment Syndrome | < 1% | High-energy trauma, excessive traction, or bleeding into closed fascial spaces. | Emergent volar and dorsal fasciotomies. High index of suspicion required postoperatively. |
Post Operative Rehabilitation Protocols
Immediate postoperative management typically involves the application of a well-padded long arm cast or a bivalved sugar-tong splint. Despite the internal stability provided by the intramedullary nails, the fixation is considered load-sharing rather than load-bearing. Rotational stability relies partially on supplemental external immobilization, especially in the early phases of healing.
The extremity is immobilized for a period of three to four weeks. At the first postoperative visit (typically 7-10 days), radiographs are obtained to confirm maintenance of reduction, evaluate for any secondary displacement, and monitor soft tissue status.
At three to four weeks, assuming radiographic evidence of early callus formation and clinical stability, the long arm cast is transitioned to a short arm cast or a removable functional splint. Supervised range of motion exercises for the elbow, wrist, and specifically forearm pronosupination are initiated to prevent capsular contracture and tendon adhesions.
Return to full, unrestricted sporting activities is generally delayed until complete radiographic consolidation is evident, typically between three to six months postoperatively, depending on the patient's age and fracture severity.
Hardware removal is a planned secondary procedure in pediatric patients to
Clinical & Radiographic Imaging

You Might Also Like