Extensor Tendon Centralization: A Masterclass in Sagittal Band Repair & Reconstruction
Key Takeaway
Join us in the OR for an in-depth masterclass on extensor tendon centralization. We'll meticulously cover the anatomy of the MCP joint, crucial preoperative planning, and detailed surgical execution for both direct sagittal band repair and advanced reconstruction techniques. Learn to identify and manage traumatic "boxer's knuckle" injuries, ensuring optimal patient outcomes and avoiding common pitfalls.
Alright, fellows, gather around. Today, we're tackling a fascinating and often debilitating injury: traumatic extensor tendon subluxation at the metacarpophalangeal (MCP) joint. This is what's colloquially known as "boxer’s knuckle," and it’s a type II injury; a full dislocation, where the tendon completely leaves the condyle and rests between the metacarpal heads, is classified as type III. Understanding the nuances of this condition, from its subtle presentation to the intricate anatomy, is paramount for successful intervention.
Understanding the Pathology: Subluxation vs. Dislocation
First, let's clarify our terms. Extensor digitorum tendon instability at the MCP joint is typically subdivided into two categories:
* Subluxation: This is when the extensor tendon laterally displaces, with its border reaching beyond the midline of the metacarpal head, but critically, it remains in contact with the condyle during full MCP joint flexion.
* Dislocation: This describes a more severe condition where the extensor tendon is fully displaced into the groove between the metacarpal heads, losing contact with the condyle.
It's crucial to remember that not all sagittal band injuries lead to extensor tendon subluxation. Our clinical examination, which we'll discuss, is key to identifying true instability. Factors like the patient's symptoms and the time elapsed since injury significantly influence our treatment approach.
Comprehensive Surgical Anatomy: The Extensor Mechanism
Let's review the critical anatomy of the digital extensor mechanism at the MCP joint level. This is a complex and dynamic system, and a thorough understanding is your foundation for success here.
The primary components include:
* The Extensor Tendon: This is the main player, responsible for extending the digit.
* Sagittal Bands: These are the primary stabilizers. Often referred to as the "shroud" ligament, they envelop the extensor tendons, centering them over the MCP joint during flexion, preventing bowstringing during hyperextension, and controlling tendon excursion. They insert onto the volar plate overlying the MCP joint.
* Volar Plate: A strong fibrocartilaginous structure that reinforces the MCP joint capsule volarly.
Beyond these, the broader extensor retinacular system includes:
* Triangular Ligament: Located between the lateral bands.
* Transverse Retinacular Ligament: Contributes to the extensor mechanism.
* Oblique Retinacular Ligament: Found at the proximal interphalangeal (PIP) joint level.
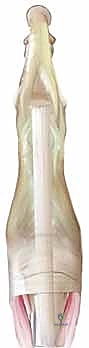
FIG 1 • A. Anatomic representation of the extensor mechanism including the sagittal bands within the digit. DIP, distal interphalangeal joint; PIP, proximal interphalangeal joint; MP, metacarpophalangeal joint.
The sagittal bands are dynamic structures. When the MCP joint is in neutral extension, they are oriented perpendicular to the tendon. The greatest tension on these bands occurs with wrist and MCP flexion, coupled with radioulnar deviation.
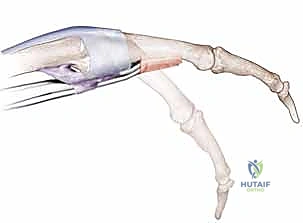
FIG 1 • B. Functional depiction of the sagittal band. The sagittal bands connect the extensor tendon to the base of the proximal phalanx and volar plate, thereby extending the MP joint.
Key Anatomical Pearls:
* Radial Sagittal Band Predominance: Traumatic injury to the sagittal bands, particularly the radial sagittal band, is the most common cause of extensor tendon instability. While ulnar-sided injuries are reported, they are far less frequent. Interestingly, the radial sagittal band is often thinner and longer than its ulnar counterpart, which may contribute to its higher susceptibility to injury.
* Distinction from Collateral Ligaments: The sagittal bands are anatomically and physiologically distinct from the deeper collateral ligaments of the MCP joint. Don't confuse them during your assessment or dissection.
* Lumbrical Muscles: These muscles originate on the flexor digitorum profundus (FDP) tendon and traverse the radial aspect of the digit, inserting into the extensor expansion. They function to flex the MCP joint and extend the interphalangeal (IP) joint through the lateral bands. We must be mindful of them during our approach.
* Intermetacarpal Ligaments: These stout ligaments originate and insert on adjacent metacarpal necks. They pass dorsal to the lumbrical tendons and volar to the interosseous tendons. While not directly involved in the extensor mechanism, they provide stability to the metacarpal arch.
* Neurovascular Risks: During our dorsal approach, we must be acutely aware of the sensory branches of the radial nerve (dorsal digital nerves) and, less commonly, the ulnar nerve. These nerve branches lie subcutaneously and are highly vulnerable to iatrogenic injury during skin incision and superficial dissection. Meticulous, sharp dissection and careful retraction are your best friends here.
Natural History and Pathogenesis
Instability of the extensor tendon is relatively rare in non-rheumatoid patients. This chapter specifically deals with traumatic subluxation; inflammatory conditions, like rheumatoid arthritis, lead to sagittal band attenuation and atraumatic subluxation, which requires different treatment protocols.
Mechanism of Injury:
* A direct blow to a flexed MCP joint is the most common mechanism.
* Injury can also result indirectly from forced flexion or directly from shear forces across the sagittal band.
* Other mechanisms include forceful deviation of the digit against resistance, usually with the MCP joint extended.
* In open injuries, the sagittal band is typically lacerated. Laceration of the junctura tendinum can also contribute to subluxation.
Extensor tendon subluxation typically occurs with at least 50% disruption of the proximal sagittal band. This causes the extensor tendon to no longer remain centralized over the MCP joint through flexion, but rather subluxate ulnarly. The long finger is most commonly injured, possibly due to the cross-sectional diameter, extent of distal attachment, and length of its sagittal band.
If these injuries are neglected, patients will experience ongoing symptoms that may worsen over time. The extensor tendon can become fixed in the valley between the metacarpal heads, leading to loss of extension and deviation of the digit. These chronic cases almost always require surgical intervention.
Patient History and Physical Findings
A critical aspect of treatment involves understanding the circumstances surrounding the injury. For open injuries, we need to determine if it was a bite, which significantly increases the risk of contamination and infection.
Acute Injury Signs and Symptoms:
* Localized pain over the involved MCP joint.
* Swelling over the involved MCP joint.
* Limited motion.
* Limited or deviated MCP joint extension, or both.
* Weak MCP extension.
* A potentially painful snapping of the tendon over the MCP joint with active flexion.
* Ulnar deviation deformity and difficulty adducting (or abducting in the case of the index) the affected finger, either acutely or chronically.

FIG 2 • A. Lack of complete active digital extension at the metacarpophalangeal joint associated with a sagittal band disruption.

FIG 2 • B. Ulnar deviation of the long finger associated with a radial sagittal band disruption.
Chronic Injury Signs and Symptoms:
* Pain during MCP joint flexion, such as during grip.
* Localized tenderness and swelling over the injured sagittal band.
Examination Techniques for Extensor Tendon Instability:
1. Visual Assessment: Observe for swelling, open injuries, and obvious tendon displacement. Determine the precise location of the pathology.
2. Palpation: Palpate over the MCP joints and specifically in the groove between the metacarpal heads. Sagittal band injuries typically exhibit pain with superficial palpation directly over the band. In contrast, collateral ligament injury pain is usually deeper, within the groove between the metacarpal heads.
3. Tendon Instability Examination: Ask the patient to actively flex the MCP joint and wrist simultaneously. This position places the maximum ulnar force on the extensor tendon at the MCP joint, effectively demonstrating the degree of instability.
4. Pain Provocation Test: With the distal and proximal IP joints extended and the MCP joint flexed, ask the patient to try to extend the MCP joint against resistance. This can elicit pain and demonstrate weakness or instability.
Imaging and Other Diagnostic Studies
Our initial workup always includes a standard radiographic series: posteroanterior, lateral, and oblique views of the MCP joints. These are crucial to exclude any mechanical or bony pathology that might limit extension or predispose the sagittal band to dislocate. Sometimes, a Brewerton view (AP view with dorsal surface of the fingers touching the cassette and the MCP joints flexed 45 degrees) or stress views are needed to rule out collateral ligament avulsion injuries.
While radiographs are good for bone, they don't show soft tissue well. Magnetic resonance imaging (MRI) has proven successful, especially when physical examination is obscured by swelling or discomfort. An MRI with the injured MCP joint flexed can particularly facilitate the diagnosis by showing the tendon displacement. Acute injuries will demonstrate morphologic and signal intensity abnormalities within and around the sagittal bands on axial T1- and T2-weighted images, including poor definition, focal discontinuity, and focal thickening.
Dynamic ultrasound has also emerged as a useful modality for diagnosing extensor tendon subluxation, especially when swelling makes physical examination challenging.
Differential Diagnosis
Always keep a broad differential in mind:
* MCP joint collateral ligament injury
* Trigger finger
* Ulnar nerve palsy
* Congenital sagittal band deficiency
* Extensor digitorum communis tendon rupture
* Radial nerve injury
* Junctura tendinum disruption
* MCP joint arthritis
Nonoperative Management
Except in special circumstances, such as for professional athletes, conservative therapy should always be our initial approach for acute injuries. In our experience, most symptomatic patients presenting within 3 weeks of injury with acute sagittal band disruptions and extensor tendon instability can be successfully treated nonoperatively.
Conservative Protocol:
* Immobilization: The common objective across various protocols is maintaining the MCP joint in neutral (full extension) for a period of weeks. We typically use a hand-based, custom orthoplast splint holding the involved digit in 0 to 20 degrees of MCP joint flexion.
* Duration: This splint is worn for 4 to 6 weeks, depending on the patient’s progress at 2- and 4-week follow-up visits.
* IP Joint Motion: Crucially, motion of the IP joint should be accommodated and encouraged throughout this period to prevent stiffness.

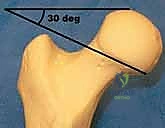
FIG 3 • Typical splint used for the conservative treatment of sagittal band disruption. The interphalangeal joints are free and no more than 30 degrees of metacarpophalangeal joint flexion is allowed.
- Weaning: After 6 weeks of MCP immobilization in extension, the splint is gradually weaned. For sporting endeavors or other heavy activities, the splint is used for another 2 weeks. Buddy taping can provide long-term support as indicated.
- Rehabilitation: Active range-of-motion activities are initiated and slowly progressed to gentle passive flexion of the involved MCP joint. Thereafter, unrestricted use of the hand is promoted. Formal hand therapy is usually not needed unless excessive joint stiffness persists without bony pathology; in such cases, a short course of therapy with modalities can be helpful.
Success rates for conservative treatment vary in the literature, from 44% to 100% of patients being asymptomatic at an average of 13.5 months.
Surgical Management: Indications and Principles
If conservative management fails, or for specific patient profiles, surgery is indicated.
Operative Indications:
* Patients with painful extensor tendon instability presenting more than 3 weeks after the injury.
* Patients whose injury has failed to respond to nonsurgical management and have persistent, painful tendon instability beyond 6 weeks of conservative care.
* Professional athletes and other high-demand individuals, where an accelerated and definitive recovery is paramount.
General Principles:
* Direct Repair vs. Reconstruction: When possible, direct repair of the sagittal band should be performed. However, if tissue deficiency or significant scarring exists, especially in chronic cases (typically beyond 8 weeks), reconstruction will be required. The surgeon must be prepared to perform either.
* Open Injuries: With open injuries, determine if a bite was the cause. If so, MCP joint contamination is highly likely, and surgical irrigation and débridement, along with antibiotic treatment, are absolutely warranted. In severe contamination, delayed sagittal band repair is indicated after the infection is controlled.
Preoperative Planning
Before we even make an incision, careful planning is essential.
Anesthesia:
* Local anesthesia with sedation is often preferred, allowing for intraoperative assessment of tendon stability with patient cooperation (though this can be challenging).
* Regional block (e.g., axillary block) or general anesthesia are also acceptable options, especially for more complex reconstructions or anxious patients.
Patient Positioning:
* The patient is placed supine on the operating table.
* The affected hand is outstretched onto a specialized hand table, ensuring ergonomic access for the surgeon and assistants. This allows for full range of motion of the digit during intraoperative assessment.
* A tourniquet is applied to the arm (or forearm, if a more distal block is used) and inflated to the appropriate pressure (typically 250 mmHg for normotensive patients) to provide a bloodless field, which is critical for identifying delicate structures.
Exposure
Our choice of incision depends on the anticipated pathology and the need for exposure.
-
Curvilinear Incision (for Primary Repair):
- A curvilinear incision is typically placed dorsally over the ulnar aspect of the affected MCP joint. This allows for excellent exposure of the radial sagittal band (most commonly injured) while minimizing the risk of scarring directly over the joint apex.
- This approach is generally preferred for primary sagittal band repair where the pathology is well-localized.
-
Longitudinal Incision (for Reconstruction):
- A longitudinal incision, centered dorsally over the affected MCP joint, provides greater exposure.
- This is generally reserved for reconstructive cases where more extensive dissection, tissue mobilization, or creation of tendon slips is anticipated.
Dissection and Neurovascular Protection:
* After the skin incision, we proceed with careful subcutaneous dissection.
* Identify and protect the sensory branches of the radial or ulnar nerves. These nerves run superficially and are highly vulnerable. Use fine dissecting scissors or a scalpel with a small blade (e.g., 15 blade) and meticulous technique.
* Once through the subcutaneous tissue, the extensor tendon and its surrounding retinacular system are exposed.
* The tear in the sagittal band is then identified.
* Any scar tissue that may impede tendon centralization or repair is meticulously débrided.
* The MCP capsule, which lies deep to the extensor tendon, is usually left undisturbed unless there is concomitant capsular injury or other MCP joint pathology that needs to be addressed.
* If a capsular injury is suspected, a small amount of methylene blue injected into the joint (away from the zone of injury) can help reveal any rents. These defects should be débrided, and the joint thoroughly irrigated. Typically, no capsular repair is necessary after débridement and irrigation.
Primary Repair: Step-by-Step Intraoperative Execution
Now, let's move into the repair phase. This is where precision and an understanding of biomechanics are crucial.
-
Identify and Centralize:
- First, clearly identify the sagittal band disruption. In most cases, this will be a tear of the radial sagittal band, allowing the extensor tendon to subluxate ulnarly.
- Once identified, gently manipulate the extensor tendon to centralize it over the metacarpal head. This provides the correct anatomical position for your repair.

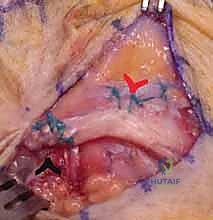
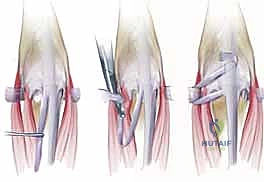
TECH FIG 1 • A. Traumatic extensor tendon dislocation (ulnar) over the metacarpophalangeal (MCP) joint ( arrowhead ) with the MCP joint extended.
<figure class="operative-step-slider my-4 text-center p-3 border rounded shadow-sm bg-light">
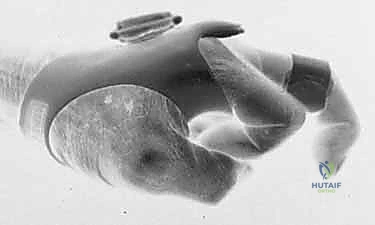
TECH FIG 1 • B. Extensor tendon subluxation over the MCP joint with the joint flexed.
-
Débridement and Preparation:
- Excise any excess or frayed tissue from the edges of the torn sagittal band and from the area between the torn band and the common extensor tendon. This ensures clean, healthy tissue edges for a robust repair.
-
Suture Selection and Technique:
- We'll use a 4-0 or 5-0 nonabsorbable suture, such as Ethibond. Nonabsorbable suture is preferred for its long-term strength, which is essential for stabilizing this dynamic structure.
- The repair is performed using interrupted sutures. We want to achieve a strong, secure repair without excessively tightening the band, which could lead to restricted motion.

TECH FIG 1 • C. Primary repair of the sagittal band with the MCP joint extended.
<figure class="operative-step-slider my-4 text-center p-3 border rounded shadow-sm bg-light">

TECH FIG 1 • E. Primary repair of the deficient sagittal band.
**Surgical Pearl:** Bury the knots where possible. This minimizes irritation to the overlying skin and reduces the risk of suture extrusion or granuloma formation.
-
Optimal Joint Position for Repair:
- Crucially, perform the repair with the MCP joint in 60 to 70 degrees of flexion. This position helps to avoid excessive tension on the repair when the joint is extended and helps prevent postoperative joint stiffness. If you repair it in full extension, you risk overtensioning the repair and limiting flexion postoperatively.
Surgical Warning: Repairing the sagittal band in full MCP extension can lead to significant postoperative stiffness and a high risk of re-tear due to excessive tension during early flexion. Always repair in moderate flexion.
-
Intraoperative Stability Assessment:
- Once the repair is complete, gently flex and extend the MCP joint through its full range of motion.
- Observe the extensor tendon carefully. It should remain perfectly centralized over the metacarpal head throughout the entire arc of motion. If there is any tendency for subluxation, the repair is inadequate, and you must revise it.

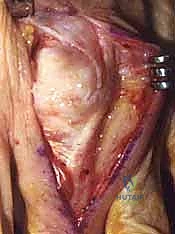
TECH FIG 1 • D. Primary sagittal band repair with the MCP joint flexed. The extensor tendon remains centralized dorsally with flexion.
- Wound Closure:
- Once stability is confirmed, proceed with meticulous wound closure. Close the subcutaneous tissue (if identifiable) with fine absorbable sutures, and then the skin with interrupted 4-0 nylon sutures.
Reconstruction with Extensor Tendon Slip (Carroll/Kilgore Technique) – Our Preferred Method
For chronic injuries, or those with significant tissue loss or scarring where direct repair is not feasible, reconstruction is necessary. This technique, popularized by Carroll and Kilgore, is our preferred method. It involves using a distally based slip of the extensor tendon itself to create a new, functional sagittal band.
-
Assess and Mobilize:
- In chronic cases, the extensor tendon may be scarred down and difficult to mobilize. It may be necessary to release the ulnar sagittal band (if intact but constricting) to mobilize the scarred extensor tendon dorsally and radially, bringing it back to a centralized position.

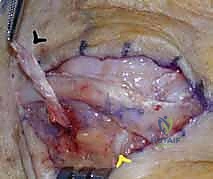
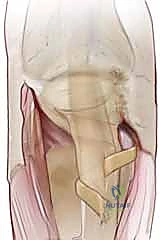
TECH FIG 2 • A. Release of the ulnar sagittal band may be necessary to mobilize the scarred tendon dorsally and radially.
<figure class="operative-step-slider my-4 text-center p-3 border rounded shadow-sm bg-light">

TECH FIG 2 • B. Mobilizing the scarred tendon dorsally and radially.
-
Create the Tendon Slip:
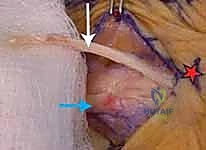
- We will create a distally based radial or ulnar slip from the main extensor digitorum communis (EDC) tendon. The choice of radial or ulnar depends on which sagittal band needs reconstruction (typically radial).
- Carefully incise the EDC tendon longitudinally, approximately 1.5 to 2 cm in length and about 3-4 mm in width, ensuring it remains distally attached. This slip will form our new sagittal band.

TECH FIG 2 • C. A distally based radial slip of the extensor tendon is created.
<figure class="operative-step-slider my-4 text-center p-3 border rounded shadow-sm bg-light">
<a href="/media/hutaif_opertive/hutaif-ch59-extensor-tend
Additional Intraoperative Imaging & Surgical Steps



REFERENCES
-
Araki S, Ohtani T, Tanaka T. Acute dislocation of the extensor digitorum communis tendon at the metacarpophalangeal joint. J Bone Joint Surg Am 1987;69A:616–619.
-
Carroll C, Moore JR, Weiland AJ. Posttraumatic ulnar subluxation of the extensor tendons: a reconstructive technique. J Hand Surg Am 1987;12A:227–231.
-
Catalano LW, Gupta S, Ragland R, et al. Closed treatment of nonrheumatoid extensor tendon dislocations at the metacarpophalangeal joint. J Hand Surg Am 2006;31A:242–245.
-
Drape JL, Dubert T, Silbermann P, et al. Acute trauma of the extensor hood of the metacarpophalangeal joint: MR imaging evaluation. Radiology 1994;192:469–476.
-
Hame S, Melone C. Boxer’s knuckle in the professional athlete. Am J Sports Med 2000;28:879–882.
-
Inoue G, Yukihisa T. Dislocation of the extensor tendons over the metacarpophalangeal joints. J Hand Surg Am 1996;21A: 464–469.
-
Ishizuki M. Traumatic and spontaneous dislocation of extensor tendon of the long finger. J Hand Surg Am 1990;15A:967–972.
-
Kilgore ES, Graham WP, Newmeyer WL, et al. Correction of ulnar subluxation of the extensor communis. Hand 1975;7: 272–274.
-
Lopez-Ben R, Lee DH, Nicolodi DJ. Boxer knuckle (injury of the extensor hood with extensor tendon subluxation): diagnosis with dynamic US: report of three cases. Radiology 2003;228:642–646.
-
Milford LW Jr. Retaining Ligaments of the Digit of the Hand. Philadelphia: WB Saunders, 1968:26–27.
-
Pfirrmann CWA, Theumann NH, Botte MJ, et al. MRI Imaging of the metacarpophalangeal joints of the fingers. Radiology 2002;222: 447–452.
-
Rayan GM, Murray D. Classification and treatment of closed sagittal band injuries. J Hand Surg Am 1994;19A:590–594.
-
Rayan GM, Murray D, Chung KW, et al. The extensor retinacular system at the metacarpophalangeal joint: an anatomical and histological study. J Hand Surg Br 1997;22B:585–590.
-
Saldana MJ, McGuire RA. Chronic painful subluxation of the metacarpophalangeal joint extensor tendons. J Hand Surg Am 1986; 11A:420–423.
-
Scheweitzer T, Rayan G. The terminal tendon of the digital extensor mechanism, part I: anatomic study. J Hand Surg Am 2004;29A: 898–902.
-
Segalman KA. Dynamic lumbrical muscle transfer for correction of posttraumatic extensor tendon subluxation. Tech Hand Up Ext Surg 2006;10:107–113.
-
Watson HK, Weinzweig J, Guidera PM. Sagittal band reconstruction. J Hand Surg Am 1997;22A:452–456.
-
Young CM, Rayan GM. The sagittal band: anatomic and biomechanical study. J Hand Surg Am 2000;25A:1107–1113.
You Might Also Like