
<class='ortho-master-container'
✨ Welcome to Your Orthopedic Oral Examination Station on Humeral Shaft Fractures!
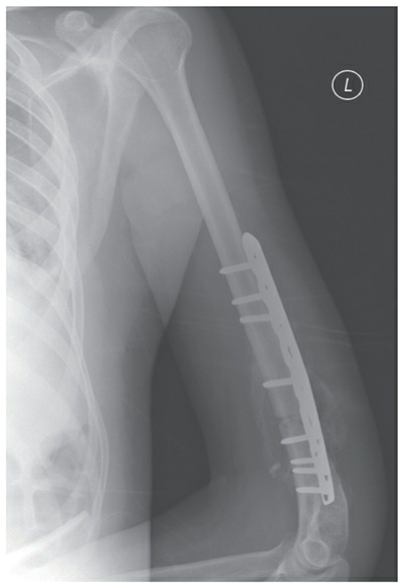
EXAMINER: "Good morning, candidate. You are presented with a 35-year-old male patient who reports left arm pain after slipping and falling on a flexed elbow at work. Here is his initial radiograph."

Station 1: Initial Assessment & Diagnosis
❓ EXAMINER: "Please interpret the X-ray image for me. Describe your findings and classify the type of fracture shown for this patient."
Model Answer:
Certainly, Examiner. The X-ray image (Figure 1) reveals a displaced fracture located in the middle third of the left humerus. There are no signs of dislocation in the left shoulder or elbow joints. Clinically, the patient presented with focal pain and deformity in the left middle humerus, with no pain at the shoulder or elbow joints. Based on these findings, the fracture can be classified as a mid-shaft humerus fracture.
Station 2: Fundamentals - Epidemiology, Anatomy, Mechanism & Evaluation
❓ EXAMINER: "Excellent. Now, provide an overview of the epidemiology and relevant anatomy of humeral shaft fractures, along with their mechanism of injury and key points of clinical and radiographic evaluation."
Model Answer:
Epidemiology:
- **Incidence:** 3-5% of all fractures, with an incidence of 14.5 per 100,000 per year.
- **Demographics:** Bimodal age distribution, affecting young patients with high-energy trauma and elderly, osteopenic patients with low-energy injuries.
- 2-10% are open fractures.
- 60% involve the middle third, 30% proximal third, and 10% distal third of the diaphysis.
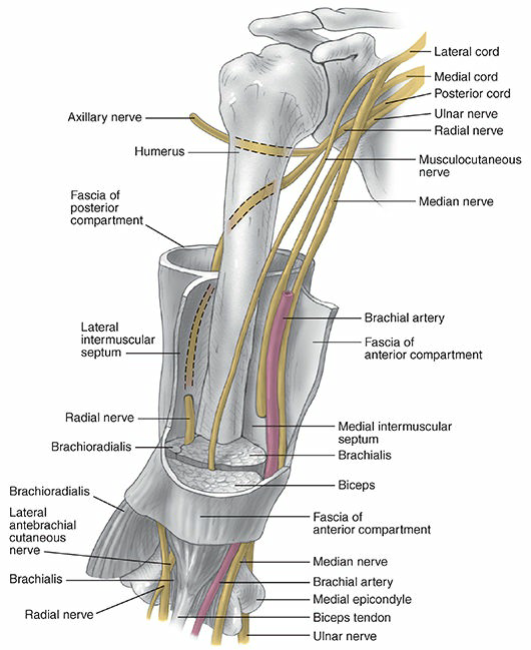
Anatomy:
- **Osteology:** The humeral shaft is cylindrical proximally and becomes triangular distally. The intramedullary canal terminates 2-3 cm proximal to the olecranon fossa.
- **Muscles:** Insertions for pectoralis major, deltoid, coracobrachialis. Origins for brachialis, triceps, brachioradialis.
- **Nerve:** The radial nerve courses along the spiral groove, approximately 14cm proximal to the lateral epicondyle and 20cm proximal to the medial epicondyle.
- **Vascular Supply:** Arises from perforating branches of the brachial artery, with the main nutrient artery entering the medial humerus distal to the midshaft.
Mechanism of Injury:
- **Direct Trauma (most common):** A direct blow or motor vehicle accident resulting in transverse or comminuted fractures.
- **Indirect Trauma:** A fall on an outstretched arm leading to transverse or oblique fractures, especially in the elderly. Throwing injuries or arm wrestling with rotational forces can cause spiral fractures.
- **Fracture Pattern:** Depends on the force applied (compressive, bending, torsional, or combined).
Clinical Evaluation:
- **Symptoms:** Pain, swelling, deformity, and shortening of the affected arm.
- **Physical Exam:** Essential to examine overall limb alignment. Gross motion with crepitus is often present. A critical pre-operative or pre-reduction neurovascular exam, with particular attention to radial nerve function, must be performed and documented. Serial neurovascular exams and compartment pressures may be needed in extreme swelling.
- Differentiation between soft tissue abrasions and open fractures is important; intra-articular injection of saline may help determine articular extension of open fractures.
Radiographic Evaluation:
- **Views:** AP and lateral radiographs, including the joint above and below the site of injury (shoulder and elbow).
- To obtain true orthogonal views, the patient (not the arm) should be rotated (transthoracic lateral) to prevent distal fragment rotation.
- Traction views may assist in defining severely displaced or comminuted fractures.
- CT, bone scans, and MRI are rarely indicated unless a pathologic fracture is suspected.
Station 3: Classification
❓ EXAMINER: "Describe the classification systems for humeral shaft fractures. What is a Holstein-Lewis fracture, and what is the incidence of radial nerve palsy associated with it?"
Model Answer:
Classification of Humeral Shaft Fractures:
Humeral shaft fractures can be classified descriptively or using the Orthopaedic Trauma Association (OTA) system.
-
**Descriptive Classification:** Categorizes fractures by:
- Open versus closed
- Location (proximal, middle, or distal third)
- Displacement (nondisplaced, displaced)
- Direction and character (transverse, oblique, spiral, segmental, comminuted)
- Intrinsic condition of bone (normal, osteopenic, pathologic)
- Articular extension
-
**OTA Classification:** The humerus is bone number 1, and the shaft is location 2. Fracture patterns are defined as:
- Simple (A)
- Wedge (B)
- Complex (C)
Holstein-Lewis Fracture:
A Holstein-Lewis fracture is a specific spiral fracture of the distal one-third of the humeral shaft. It is commonly associated with neuropraxia of the radial nerve, with an incidence of radial nerve palsy reported at 22%.
Station 4: Treatment - Nonoperative Management
❓ EXAMINER: "What are the overall treatment goals for humeral shaft fractures, and when would you consider nonoperative management? Provide the criteria for acceptable alignment and any absolute or relative contraindications."
Model Answer:
Treatment Goals:
The goals are fracture union with acceptable humeral alignment and the patient's return to their pre-injury level of function.
Nonoperative Indications:
Nonoperative treatment is indicated in the vast majority of humeral shaft fractures, as over 90% heal nonsurgically.
Criteria for Acceptable Alignment:
- < 20° anterior angulation
- < 30° varus/valgus angulation (historically 25° varus or 10° valgus)
- < 3 cm shortening (bayonet apposition)
Varus angulation is common but rarely has functional or cosmetic sequelae, and even angulation beyond these parameters has not been shown to affect function.
Absolute Contraindications to Nonoperative Treatment:
- Severe soft tissue injury or bone loss
- Vascular injury requiring repair
- Brachial plexus injury
- Compartment syndrome
Relative Contraindications to Nonoperative Treatment:
- These generally overlap with relative operative indications (see next section).
- **Note:** Radial nerve palsy is NOT a contraindication to functional bracing.
❓ EXAMINER: "Describe the different nonoperative treatment methods, outlining their principles and ideal applications."
Model Answer:
Nonoperative Treatment Methods:
-
**Hanging Cast:**
- **Principle:** Uses dependency traction by the weight of the cast and arm to effect fracture reduction.
- **Indications:** Displaced midshaft humeral fractures with shortening, particularly spiral or oblique patterns.
- **Disadvantages:** Rarely used as the patient must remain upright or semi-upright. Transverse or short oblique fractures are relative contraindications due to potential for distraction. May be exchanged for functional bracing after early callus formation. Union rates >95%.
-
**Coaptation Splint:**
- **Principle:** Uses dependency traction and hydrostatic pressure for reduction with greater stabilization and less distraction than a hanging cast. Forearm suspended in a collar and cuff.
- **Indications:** Acute treatment of humeral shaft fractures with minimal shortening, and for short oblique or transverse fracture patterns.
- **Disadvantages:** Axillary irritation, potential for splint slippage. May be exchanged for functional bracing 1-2 weeks after injury.
-
**Thoracobrachial Immobilization (Velpeau dressing):**
- **Principle:** Immobilizes the arm against the chest.
- **Indications:** Used in elderly patients or children unable to tolerate other methods; for minimally displaced or nondisplaced fractures.
- Passive shoulder pendulum exercises may start in 1-2 weeks. May be exchanged for functional bracing 1-2 weeks after injury.
-
**Functional Bracing:**
- **Principle:** Uses hydrostatic soft tissue compression to maintain fracture alignment while allowing motion of adjacent joints.
- **Application:** Typically applied 1-2 weeks after injury, after pain/swelling subsides. Consists of anterior and posterior shells with Velcro straps.
- **Success:** Depends on an upright, mobile patient, daily brace tightening, and functioning upper arm musculature.
- **Contraindications:** Massive soft tissue injury, unreliable patient, inability to obtain/maintain acceptable reduction. Sling use may lead to varus angulation.
- **Duration:** Worn for a minimum of 8 weeks or until radiographic union.

Station 5: Treatment - Operative Management
❓ EXAMINER: "When would you consider operative intervention for a humeral shaft fracture? List the absolute and relative indications."
Model Answer:
Absolute Indications for Operative Treatment (ORIF):
- Open fracture
- Vascular injury requiring repair
- Brachial plexus injury
- Ipsilateral forearm fracture (floating elbow)
- Compartment syndrome
- Periprosthetic humeral shaft fractures at the tip of the stem
Relative Indications for Operative Treatment:
- Multiple trauma or associated lower extremity fracture
- Inadequate closed reduction or unacceptable malunion
- Pathologic fractures
- Bilateral humerus fracture
- Segmental fracture
- Intra-articular fracture extension
- Neurologic loss following penetrating trauma
- Radial nerve palsy after fracture manipulation (controversial)
- Nonunion
- Unfavorable body habitus (e.g., morbid obesity, pendulous breasts)
- Chronic shoulder or elbow stiffness (increases risk of nonunion)
- Distraction at fracture site
- Short oblique or transverse fracture pattern
- Severe osteoporotic bone
- Overlying skin compromise limits open approach
❓ EXAMINER: "If you decide on open reduction and internal fixation, what surgical approaches are available for the humeral shaft? Discuss the main fixation techniques and briefly mention postoperative rehabilitation."
Model Answer:
Surgical Approaches to the Humeral Shaft:
- **Anterolateral Approach:** Preferred for proximal third humeral shaft fractures. The radial nerve is identified in the interval between the brachialis and brachioradialis and traced proximally. The brachialis muscle is split for access, and this approach can be extended proximally to the shoulder.
- **Anterior Approach:** Utilizes the muscular interval between the biceps and brachialis muscles.
- **Posterior Approach:** Provides excellent exposure to most of the humerus, including the elbow, but cannot be extended proximally to the shoulder. The muscular interval is between the lateral and long heads of the triceps, with the medial head split. The radial nerve must be identified in the spiral groove, usually at the midportion of the arm, to avoid iatrogenic injury.
Operative Fixation Techniques:
-
**Open Reduction and Internal Fixation (ORIF) with Plates and Screws:** A versatile method for anatomical reduction and stable fixation.
 🔍 Click to enlarge
🔍 Click to enlargeFigure 4: Plate and screw fixation of a distal third humeral shaft fracture. -
**Intramedullary Nailing (IMN):**
- **Relative Indications:** Pathologic fractures, segmental fractures, severe osteoporotic bone, overlying skin compromise limiting open approach, and polytrauma.
 🔍 Click to enlarge
🔍 Click to enlargeFigure 5: Intramedullary nail fixation of a humeral shaft fracture. -
**External Fixation:**
- **Indications:** High-energy complex or comminuted fractures, open fractures, significant soft tissue or bony defects, floating elbow, hemodynamically unstable polytrauma, or concomitant vascular injury.
🔍 Click to enlargeFigure 6: External fixation of a humeral shaft fracture sustained secondary to gunshot wound.

Postoperative Rehabilitation:
Range-of-motion exercises for the hand and wrist should be started immediately after surgery. Shoulder and elbow range of motion should be instituted as pain subsides and as permitted by fixation stability.
Station 6: Complications & Radial Nerve Palsy Management
❓ EXAMINER: "What are the common complications associated with humeral shaft fractures and their treatment?"
Model Answer:
Common Complications of Humeral Shaft Fractures:
- **Nonunion:** No callus on radiograph and gross motion at the fracture site at 6 weeks has a 90-100% PPV of going on to nonunion in closed humeral shaft fractures. Overall incidence up to 15%.
- **Malunion:** Varus angulation is common but rarely has functional or cosmetic sequelae due to compensation by arm musculature and adjacent joints. Risk factors include transverse fracture patterns and radial nerve palsy.
- **Radial Nerve Palsy:** Occurs in 8-15% of closed fractures, increasing to 22% in distal one-third fractures. Iatrogenic palsy is most common following ORIF via lateral (20%) or posterior (11%) approaches.
- **Vascular Injury:** Uncommon but serious, especially in proximal and distal thirds, or with penetrating trauma. Brachial artery has highest risk. Constitutes an orthopedic emergency requiring repair within 6 hours.
- **Infection:** Risk associated with open fractures and surgical procedures.
- **Stiffness:** Of shoulder and elbow if not mobilized adequately.
❓ EXAMINER: "Let's delve deeper into radial nerve palsy. What is its incidence, and how would you manage it, both in acute presentation and if it occurs iatrogenically after surgery?"
Model Answer:
Incidence of Radial Nerve Palsy:
- Overall incidence in closed humeral shaft fractures: 8-15%.
- Increased incidence in distal one-third (Holstein-Lewis) fractures: 22%.
- Iatrogenic radial nerve palsy (post-ORIF): most common following lateral approach (20%) or posterior approach (11%).
Management of Radial Nerve Palsy:
The management strategy depends on whether the palsy is primary (at initial presentation) or secondary/iatrogenic (after intervention).
1. Primary Radial Nerve Palsy (at presentation with closed fracture):
- Most primary palsies are **neuropraxias** and recover spontaneously within 3-6 months (up to 90% recovery rate).
- Initial management is typically **nonoperative** (functional bracing for the fracture).
- **Monitoring:** Regular clinical examinations for signs of recovery (e.g., return of wrist/finger/thumb extension). EMG/NCS can be performed at 3-6 weeks to assess reinnervation.
-
**Indications for Exploration:**
- Lack of clinical or electrophysiological recovery by 3-6 months.
- Open fractures with associated nerve palsy (requires immediate exploration).
- Nerve injury associated with vascular injury requiring surgical exploration.
2. Secondary/Iatrogenic Radial Nerve Palsy (after closed reduction or surgery):
- If palsy develops immediately **after closed reduction:** Check reduction; if unsatisfactory or nerve entrapment is suspected, **immediate surgical exploration** is warranted.
- If palsy develops immediately **after ORIF:** **Immediate surgical re-exploration** is usually indicated to identify and address the cause (e.g., nerve impingement by plate/screws, traction injury).
3. General Supportive Management for All Radial Nerve Palsies:
- **Patient Education:** Inform the patient about the expected course of recovery, which can be prolonged.
- **Splinting:** Dynamic wrist extension splint (cock-up splint) to prevent wrist drop deformity and maintain function during recovery.
- **Therapy:** Hand and wrist therapy to maintain passive range of motion and muscle strength.
- **Tendon Transfers:** If no recovery occurs after 6-12 months, or if recovery is incomplete, tendon transfers may be considered to restore lost function.
Conclusion of Station
EXAMINER: "Thank you, candidate. That was a thorough and well-articulated discussion. This concludes your station on Humeral Shaft Fractures. You may now proceed."
Full Topic Review: Humeral Shaft Fractures
📚 Click to Reveal Comprehensive Article Review
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding orthopedic-md-oral-examination-diagnosis-and-management-of-humeral-shaft-fractures