Full Question & Answer Text (for Search Engines)
Question 1:
Fractures that have a high specificity for child abuse include all of the following except:
Options:
- C orner fractures
- Rib fractures
- Scapular fractures
- Sternal fractures
- Spiral femur fractures
Correct Answer: Spiral femur fractures
Explanation:
Even though a spiral pattern suggests a rotational force, spiral fractures of the femur are not specific for abuse. All of the other patterns are highly specific although not absolutely diagnostic.
Question 2:
The differential diagnosis of abuse in a child with a long bone fracture includes all of the following conditions except:
Options:
- Myelodysplasia
- C ongenital insensitivity to pain
- Rickets
- C opper deficiency
- Metaphyseal dysplasia
Correct Answer: Metaphyseal dysplasia
Explanation:
All of the diagnoses except metaphyseal dysplasia place patients at increased risk of fracture, and therefore could be confused with nonaccidental injury.
Question 3:
Among children with nonossifying fibromas, a risk of pathologic fracture exists mainly when a lesion exceeds what minimum percentage of a boneâ s diameter:
Options:
Correct Answer: 50%
Explanation:
In a series from the Mayo clinic, all pathologic fractures associated with nonossifying fibromas in the lower extremity occurred in lesions larger than 50% of the transverse diameter.
Question 4:
In a bowed tibia, the tensile stress during weightbearing is greatest at which point:
Options:
- The apex on the convex side
- The apex on the concave side
- The proximal joint surface
- The distal joint surface
- There is never a tensile stress on a tibia.
Correct Answer: The apex on the convex side
Explanation:
The moment becomes tensile at the apex on the convex side of a tibial bow, in contrast to the normal compressive stress in a straight diaphysis. The moment is equal to load multiplied by distance from the axis of load.
Question 5:
Which of the following medications has not been shown to increase the risk of osteopenia or osteoporosis:
Options:
- Glucocorticoids
- Antacids containing aluminum
- Phenytoin
- Phenobarbital
- Pamidronate
Correct Answer: Pamidronate
Explanation:
Pamidronate, a bisphosphonate, increases bone density by inhibiting resorption. All of the medications listed as possible answers decrease bone density.
Question 6:
A 7-year-old gymnast complains of pain in her medial midfoot. Radiographs reveal that the navicular is narrower and more sclerotic on this side than the other. The midfoot appears somewhat flattened. Your next step is to recommend:
Options:
- Open biopsy
- Electrical stimulation
- Percutaneous drilling
- Intravenous pamidronate
- Observation with rest as needed
Correct Answer: Observation with rest as needed
Explanation:
The condition described best resembles Kohlerâ s disease, or avascular necrosis of the tarsal navicular. This disease has a natural history of spontaneous improvement with time, and biopsy is not needed. Rest improves symptoms, although it is probably not mandatory. Sometimes with severe pain, a cast may help to speed improvement of symptoms.
Question 7:
Which part of the body is removed last in a posterior vertebral column resected via a posterior approach:
Options:
- The lamina
- The pedicles
- The anterior wall of the vertebral body
- The posterior vertebral cortex
- The transverse process
Correct Answer: The posterior vertebral cortex
Explanation:
To protect and stabilize the neural elements, the posterior vertebral cortex is left intact to be resected last.
Question 8:
An 18-year-old man has chronic pain in his right thigh, which is foreshortened with an increased anterior bow (Slides). What is the most likely diagnosis:
Options:
- Chronic osteomyelitis
- Osteogenesis imperfecta
- Pagetâ s disease
- Multiple enchondromas
- Fibrous dysplasia
Correct Answer: Fibrous dysplasia
Explanation:
This patient has polyostotic fibrous dysplasia. The diffuse enlargement in width is atypical for osteogenesis imperfecta or infection. Pagets disease is associated with increased sclerosis. Enchondromas produce more localized changes in the bones than fibrous dysplasia.
Question 9:
This infant was born with an anomaly of the left lower extremity (Slides). What is the most likely diagnosis:
Options:
- Clubfoot
- Proximal focal femoral deficiency
- Fibular hemimelia
- Tibial hemimelia
- C ongenital pseudarthrosis of the tibia
Correct Answer: Tibial hemimelia
Explanation:
This infant has tibial hemimelia, which is a complete absence of the tibia with resultant inversion of the foot. The presence of an intact fibula causing focal lateral prominence, a shortened but complete femur, and absence of a visible tibia rule out a diagnosis of clubfoot, proximal focal femoral deficiency, fibular hemimelia, and congenital pseudarthrosis of the tibia.
Question 10:
This child with tibial hemimelia does not have a proximal tibial remnant (Slides). The preferred treatment is:
Options:
- Knee disarticulation
- Femoral-fibular fusion with Syme disarticulation
- Centralization of the fibula at the knee and ankle
- Syme disarticulation
- Rotationplasty
Correct Answer: Knee disarticulation
Explanation:
If the proximal tibial remnant is absent, the prospect of a functionally useful extension at the knee is nil. Disarticulation at the knee is the best option for this patient.
Question 11:
Which of the following Risser signs most accurately describes the patient presented (Slide):
Options:
- Risser 1
- Risser 2
- Risser 3
- Risser 4
- Risser 5
Correct Answer: Risser 4
Explanation:
Despite its biologic variability, the Risser sign is one of the most useful indicators of maturity used in the management of pediatric spine disorders. The Risser sign is a depiction of the progressive ossification and fusion of the iliac apophysis, which begins anterolaterally and finishes posteromedially. The initial ossification (Risser 1) begins just after the peak height velocity, after triradiate cartilage closure, and approximately at the time of menarche. The completion of ossification and fusion usually takes 1½ to 2 years in girls and 2 to 3 years in boys. As the iliac apophysis matures and Risser 4 is reached, the Risser sign becomes a sclerotic line that is whiterâ than the adjacent ilium. Risser 0 and Risser 5 may be difficult to
distinguish except that the cranial border of the ilium in Risser 0 is wavy or ruffled, while it is smooth and sclerotic in Risser 5.
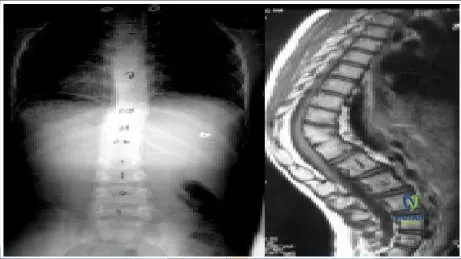
Question 12:
A 15-year-old boy presents with a spinal curvature and no other known disorders (Slide). His curve is 105° and corrects to 70° with traction. His neurologic examination is normal. The best treatment method would be:
Options:
- Observation until medical problems develop
- Brace until maturity
- Anterior endoscopic fusion and instrumentation
- Anterior open fusion and instrumentation
- Anterior and posterior fusion with posterior instrumentation
Correct Answer: Anterior and posterior fusion with posterior instrumentation
Explanation:
A large, rigid curve like this requires an anterior release and fusion to obtain flexibility. The anterior release should be followed by a posterior fusion with instrumentation either on the same day or after a period of traction. Anterior instrumentation alone increases the risk of cut out and incomplete correction.
Question 13:
Numerous braces are available for controlling spinal deformities in growing children. Which type of brace is presented here (pic):
Options:
- Boston brace
- C harleston brace
- Milwaukee brace
- Wilmington brace
- Providence brace
Correct Answer: Milwaukee brace
Explanation:
The Milwaukee brace is the first modern scoliosis brace to demonstrate efficacy and to achieve widespread use. The Milwaukee brace is a cervicothoracolumbar orthosis. All of the other braces listed are thoracolumbosacral orthoses.
The Boston brace is prefabricated and is selected from measurements taken of the patient. The C harleston brace is a night-only brace and bends the patient to reverse the curve. The Wilmington brace is made of thermoplastic material for rapid, on-site fabrication. The Providence brace is made using computer-assisted machining to help achieve maximal correction.
Question 14:
A patient has idiopathic scoliosis measuring 62° thoracic convex to the right and 40° lumbar convex to the left (Slide). The sagittal film shows a relatively decreased thoracic kyphosis and decreased lumbar lordosis. The patient is 13 years old and is 2 months postmenarchal. Which of the following treatments is most appropriate:
Options:
- Milwaukee brace treatment
- Posterior fusion from T4 to L2
- Posterior fusion from T4 to L3
- Posterior fusion from T4 to L4
- Posterior fusion from T4 to L5
Correct Answer: Posterior fusion from T4 to L2
Explanation:
This curve may be classified as a King type II or III. The curve is too large for bracing. Only the thoracic curve must be fused. Because the stable vertebra is L2, the fusion does not need to go below this level. Other acceptable options include anterior thoracic instrumentation and fusion from T4 to T12 or posterior instrumented fusion to L1.
Question 15:
Which of the following terms best describes the condition shown (Slide):
Options:
- Calcaneovalgus
- Equinovarus
- Posteromedial bow
- Fibular hemimelia
- Metatarsus adductus
Correct Answer: Calcaneovalgus
Explanation:
This patientâ s foot is in calcaneovalgus. Treatment is not required because calcaneovalgus spontaneously resolves.
Question 16:
A 4-year-old boy is brought to the doctor for evaluation of his feet. His mother is concerned that he has no arch. He does not have any pain in his feet, and there are no calluses on the plantar surface. Radiographs of one of the feet are shown below. You recommend:
Options:
- Open reduction of the talocalcaneal joint
- Calcaneal slide osteotomy
- Calcaneal neck lengthening
- Medial arch support
- Observation
Correct Answer: Observation
Explanation:
The radiographs demonstrate a normal appearance of a foot in a young child. The angle between the talus and calcaneus is increased at this age. The arch in a young child is not as well developed as in an older child. The navicular has not ossified yet. No treatment is needed.
Question 17:
A 13-year-old girl is brought to the office for evaluation of her feet. During gait, she has a foot progression angle of 45° outward on each side. Her transmalleolar axis is 20° outward on each side. Her hips have internal rotation in extension of 40° and external rotation in extension of 40°. Her clinically estimated anteversion is 20°. She has popliteal angles of 20° bilaterally and full knee extension during swing. Standing radiographs of the feet are presented. Which factor is most likely to be the cause of her toeing- out:
Options:
- Femoral retroversion
- External tibial torsion
- Dynamic knee torsion
- Forefoot abduction
- Tight hamstrings
Correct Answer: Forefoot abduction
Explanation:
This patient has significant forefoot abduction demonstrated on the standing foot radiographs. The femoral anteversion of 20° is within normal limits for age. The transmalleolar and popliteal angles are also within normal limits. There is no evidence of dynamic knee torsion as a factor in alignment of children.
Question 18:
After being dragged by an automobile, a 7-year-old child sustained injuries to his foot (Slide). Following reconstructive surgery, he is most likely to be left with a permanent deficit in which of the following:
Options:
- Ankle inversion
- Ankle eversion
- Ankle dorsiflexion
- Growth of the distal tibia
- Growth of the navicular
Correct Answer: Ankle dorsiflexion
Explanation:
This patient sustained a dorsal degloving injury. The anterior tibialis tendon is gone, as are some of the toe dorsiflexors. The anterior tibial function is difficult to reconstruct, even after tendon transfer, because of scarring at the insertion site.
Question 19:
What best describes the anomalies depicted (Slide):
Options:
- Incarcerated hemivertebra
- C ongenital hemivertebra
- C ongenital diastematomyelia
- C ongenital hemivertebrae plus bar
- Block vertebra
Correct Answer: C ongenital hemivertebra
Explanation:
The Slide shows two congenital hemivertebrae on the convex side plus a bar on the right side. An incarcerated hemivertebra fits into indentations in the adjacent vertebrae, causing no net deformity. A block vertebra is a pair of fully fused vertebrae usually without significant deformity.
Question 20:
Compared to viral vectors, the advantages of non-viral vectors for gene delivery include all of the following except:
Options:
- Safety
- Less immunogenicity
- More efficiency
- Easier production
- Special packaging cell line
Correct Answer: More efficiency
Explanation:
Due to safety concerns, immunogenicity, and production issues associated with viral vectors, non-viral delivery systems were developed by complexing of genes (DNA) to various chemical formulations. This makes the DNA stable and increases its uptake. They include plasmids, peptides, cationic liposomes, DNA-ligand complexes (recognize specific cell-surface receptors, leading to receptor- mediated uptake), and gene gun (particles of gold coated with DNA, forced into the cells with high velocity bombardment). However, their efficiency is lower than viral vectors.


 distinguish except that the cranial border of the ilium in Risser 0 is wavy or ruffled, while it is smooth and sclerotic in Risser 5.
distinguish except that the cranial border of the ilium in Risser 0 is wavy or ruffled, while it is smooth and sclerotic in Risser 5.



 This patient has significant forefoot abduction demonstrated on the standing foot radiographs. The femoral anteversion of 20° is within normal limits for age. The transmalleolar and popliteal angles are also within normal limits. There is no evidence of dynamic knee torsion as a factor in alignment of children.
This patient has significant forefoot abduction demonstrated on the standing foot radiographs. The femoral anteversion of 20° is within normal limits for age. The transmalleolar and popliteal angles are also within normal limits. There is no evidence of dynamic knee torsion as a factor in alignment of children.