This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set FF5036)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
of 100
Figures 1 and 2 are the radiographs after attempted reduction of an injury in a 9-year-old girl. Which anatomic structure is most likely to be interposed?
1
Brachialis muscle
2
Radial nerve
3
Median nerve
4
Ulnar nerve
■ The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.
QUESTION 2 OF 50
of 100
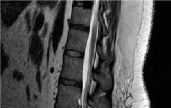
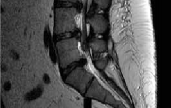
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
1
less intraoperative blood loss.
2
an increased rate of recurrent disk herniation.
3
a shorter length of hospital stay.
4
a higher rate of surgical complications.
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
[PubMed PMID: 24442183. ](http://www.ncbi.nlm.nih.gov/pubmed/24442183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24442183)
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
[22404142/. ](http://www.ncbi.nlm.nih.gov/pubmed/22404142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22404142)
[Lee P, Liu JC, Fessler RG. Perioperative results following open and minimally invasive single-level lumbar discectomy. J Clin Neurosci. 2011 Dec;18(12):1667-70. doi: 10.1016/j.jocn.2011.04.004. Epub 2011 Sep 25. PubMed PMID: 21944927. ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21944927)
[Shamji MF, Bains I, Yong E, Sutherland G, Hurlbert RJ. Treatment of Herniated Lumbar Disk by Sequestrectomy or Conventional Diskectomy. World Neurosurg. 2013 Feb 20. pii: S1878-8750(13)00352-5. doi: 10.1016/j.wneu.2013.02.066. [Epub ahead of print] Review. PubMed PMID: 23454687. ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23454687)
[Wang H, Huang B, Li C, Zhang Z, Wang J, Zheng W, Zhou Y. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon's training level of minimally invasive spine surgery. Clin Neurol Neurosurg. 2013 Oct;115(10):1987-91. doi: 10.1016/j.clineuro.2013.06.008. Epub 2013 Jul 2. PubMed PMID: 23830496. ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23830496)
Soliman J, Harvey A, Howes G, Seibly J, Dossey J, Nardone E. Limited microdiscectomy for lumbar disk herniation: a retrospective long-term outcome analysis. J Spinal Disord Tech. 2014 Feb;27(1):E8-E13. doi: 10.1097/BSD.0b013e31828da8f1. PubMed PMID: 23563332.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23563332)
[Radcliff K, Hilibrand A, Lurie JD, Tosteson TD, Delasotta L, Rihn J, Zhao W, Vaccaro A, Albert TJ, Weinstein JN. The impact of epidural steroid injections on the outcomes of patients treated for lumbar disc herniation: a subgroup analysis of the SPORT trial. J Bone Joint Surg Am. 2012 Aug 1;94(15):1353-8. doi: 10.2106/JBJS.K.00341. PubMed PMID: 22739998. ](http://www.ncbi.nlm.nih.gov/pubmed/22739998)[View](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
QUESTION 3 OF 50
A collegiate football player who sustained a blow to the head during the first quarter of a game is confused for several minutes after the hit but does not lose consciousness. He had two similar episodes in games earlier in the season. When should he be allowed to return to play?
1
Immediately
2
In the second half
3
In 1 week
4
In 4 weeks
5
Next season
Using the traditional concussion grading scale, the patient sustained a grade I concussion because he did not lose consciousness and his abnormal cognitive level lasted less than 1 hour. If this was the player’s first concussion, theoretically he could return to play later in the game provided that he had no confusion, headache, or associated symptoms. However, because it was the third concussion for the year, participation in contact sports should be terminated for the season.
REFERENCES: Guskiewwicz KM, Barth JT: Head injuries, in Schenk RC Jr (ed): Athletic Training and Sports Medicine. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 143-167.
Kelly JP, Rosenberg JH: Diagnosis and management of concussion in sports. Neurology 1997;48:575-580.
QUESTION 4 OF 50
Which of the following is an advantage of unreamed nailing of the tibia compared to reamed nailing?
1
Less surgical time
2
Lower risk of nonunion
3
Lower rate of malunion
4
Faster time to union
5
Less secondary procedures to achieve union
The debate between reamed versus unreamed intramedullary nailing of the tibia continues. Although unreamed nailing was proposed for open fractures to minimize infection, its simplicity made it appealing for closed fractures. However, most studies to date show that the only advantage of unreamed nailing is less surgical time. All studies show higher nonunion rates with increased hardware failure and increased time to union for unreamed nailing. Even in open fractures graded up to Gustilo Grade IIIA, the reamed tibial nail performs better.
REFERENCES: Larsen LB, Madsen JE, Hoiness PR, et al: Should insertion of intramedullary nails for tibial fractures be with or without reaming? A prospective, randomized study with 3.8 years’ follow-up. J Orthop Trauma 2004;18:144-149.
Blachut PA, O’Brien PJ, Meek RN, et al: Interlocking intramedullary nailing with or without reaming for the treatment of closed fractures of the tibial shaft: A prospective randomized study. J Bone Joint Surg Am 1997;79:640-646.
QUESTION 5 OF 50
of 100
Which statement best characterizes the injured structure in Figures 65a through 65d?
1
The structure is extrasynovial, contains significant innervation, and is highly
62
vascularized.
2
The structure is extrasynovial, does not contain significant innervation, and is not highly vascularized.
3
The structure is intrasynovial, contains significant innervation, and is not highly vascularized.
4
The structure is intrasynovial, does not contain significant innervation, and is not highly vascularized.
- The structure is intrasynovial, contains significant innervation, and is not highly vascularized.
QUESTION 6 OF 50
Patients with homocystinuria phenotypically resemble patients with:
1
Achondroplasia
2
Larsen's syndrome
3
Marfan syndrome
4
Gaucher's disease
5
Noonan's syndrome
Patients with homocystinuria may phenotypically resemble patients with Marfan syndrome. Patients with homocystinuria and
Marfan syndrome are tall with long limbs, arachnodactyly, scoliosis, chest wall deformities, and lens dislocations.
Achondroplasia is characterized by short stature, frontal bossing, and rhizomelic shortening of the limbs. Larsen's syndrome is a disorder characterized by short stature and multiple joint dislocations.
Gaucher's disease is a lysosomal storage disease characterized by accumulation of cerebroside in cells of the reticuloendothelial system. As in patients with homocystinuria, patients with Gaucher's disease have osteoporosis, however, they do not develop any of the other phenotypic features seen in homocystinuria.
Noonan's syndrome effects boys and clinical features include short stature, a webbed neck, and cubitus valgus deformities.
QUESTION 7 OF 50
Which of the following is a significant side effect of biphosphonates (e.g., alendronate):
1
Pruritus
2
Dizziness
3
Peripheral edema
4
Esophagitis and dyspepsia
5
Light sensitivity
The most significant side effect of biphosphonates is esophagitis and dyspepsia. Biphosphonates must be taken on an empty stomach with no oral intake for 30 minutes. In addition, patients should remain upright
QUESTION 8 OF 50
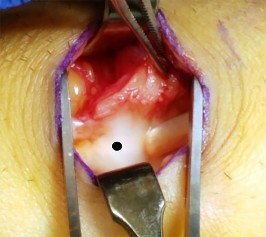
Figures 1 and 2 show the intraoperative photographs obtained during surgical treatment for de Quervain tendonitis. For orientation purposes, dorsal is at the top. Figure 1 is obtained just after the initial first extensor compartment release, and Figure 2 shows the floor of the first extensor compartment. If the structure marked by the black dot is not addressed, the most common postoperative problem would be
1
persistent pain.
2
tendon subluxation.
3
altered sensation.
4
tendon rupture.
The black dot identifies an accessory compartment of the extensor pollicis brevis (EPB) tendon. The incidence of accessory EPB compartment in patients undergoing surgical treatment for de Quervain syndrome ranges from 46% to 60%. Failure to release this compartment at the time of initial surgery can cause persistent postoperative pain. The patient would not experience altered sensation if this compartment were not released. Altered sensation would most commonly occur following injury to the dorsal radial sensory nerve branch during surgery. EPB tendon subluxation also would not occur should the accessory compartment not be released. For EPB tendon subluxation to occur, its own compartment would need to be released first. Finally, EPB tendon rupture would be an extremely uncommon complication of failure to release the accessory compartment.
QUESTION 9 OF 50
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
1
2 to 3
2
4 to 5
3
6 to 7
4
7 to 8
5
9 to 10
DISCUSSION: In the normal adult, the distance between the basion and the tip of the dens is 4 mm to 5 mm. Any distance greater than 5 mm is considered abnormal. This is one way to detect occipitocervical dissociation other than using the Power’s ratio, which relies on an anterior dislocation.
REFERENCES: Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Wholey MH, Browner AJ, Baker HL Jr: The lateral roentgenogram of the neck: With comments on the atlanto odontoid-basion relationship. Radiol 1958;71:350-356.
QUESTION 10 OF 50
A 20-year-old woman with spastic hemiplegia is evaluated for function and hygiene issues with her right wrist. Her wrist has a resting posture of 90° of flexion and can be passively extended to 65° of flexion. Her fingers are flexed into her palm but can be passively extended with the wrist at 95°. What treatment is likely to provide the most durable result for improved hygiene, function, and cosmesis?
1
Flexor carpi ulnaris to extensor carpi radialis brevis transfer
2
Fractional lengthening of the wrist and finger flexor tendons
3
Wrist arthrodesis with proximal row carpectomy
4
Botulinum toxin injection
The patient has a static deformity of the wrist with a fixed flexion deformity of more than 45°. Soft-tissue procedures such as those referenced in options A and B would not be sufficient to address the degree of contracture. Additionally, Botulinum toxin injections would not provide relief for capsular contractures. Wrist arthrodesis combined with a proximal row carpectomy has been shown to provide a functional and _cosmetic alternative for patients with severe wrist flexion contractures._
QUESTION 11 OF 50
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of
1
referral to a pitching coach to improve throwing mechanics.
2
a weight-training program that concentrates on rotator cuff strengthening.
3
rest until symptoms have resolved, followed by a gradual return to pitching.
4
a metabolic work-up.
5
cessation of pitching until the physis is closed.
The patient has the classic signs of Little Leaguer’s shoulder, with findings that include pain localized to the proximal humerus during the act of throwing and radiographic evidence of widening of the proximal humeral physis. Examination usually reveals tenderness to palpation over the proximal humerus, but the presence of any swelling, weakness, atrophy, or loss of motion is unlikely. The treatment of choice is rest from throwing for at least 3 months, followed by a gradual return to pitching once the shoulder is asymptomatic.
REFERENCES: Carson WG Jr, Gasser SI: Little Leaguer’s shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
QUESTION 12 OF 50
When performing capsular releases during shoulder arthroplasty for the treatment of glenohumeral joint osteoarthritis, what anatomic landmark indicates the location of the axillary nerve as it begins to travel from anterior to posterior?
1
Inferior border of the subscapularis
2
Insertion of the pectoralis major onto the humerus
3
Insertion of the latissimus dorsi tendon onto the humerus
4
Lateral margin of the conjoint tendon
The axillary nerve originates from the posterior cord of the brachial plexus. It passes down the anteroinferior aspect of the subscapularis, courses posteriorly beneath the glenoid and inferior capsule, then wraps around the humerus from posterior to anterior on the deep surface of the deltoid. In the setting of glenoid and humeral head deformity, the inferior border of the subscapularis can be a useful landmark to ensure the nerve is appropriately protected intraoperatively.
QUESTION 13 OF 50
Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of
1
cast immobilization.
2
splinting with a bone stimulator.
3
excision of the fracture fragment.
4
arthroscopically assisted percutaneous fixation.
5
trephination of the fibrous union.
The patient’s chronic symptoms are associated with a fracture of the base of the hook of the hamate; therefore, the treatment of choice is simple excision of the fracture fragment, with reasonable expectations of functional return. Acute fractures may be difficult to treat because of the high incidence of nonunion, but once nonunion is discovered, nonsurgical management usually is unsuccessful. Bone grafting may be a surgical alternative, but successful outcomes with percutaneous fixation or trephination of the fibrous union have not been reported.
REFERENCES: Geissler WB: Carpal fractures in athletes. Clin Sports Med 2001;20:167-188.
Rettig ME, Dassa GL, Raskin KB, Melone CP Jr: Wrist fractures in the athlete: Distal radius and carpal fractures. Clin Sports Med 1988;17:469-489.
QUESTION 14 OF 50
A 15-year-old boy presented with inability to elevate his right shoulder and flex his elbow. He sustained a fall from an all-terrain vehicle 8 weeks ago. He landed on the right shoulder and twisted his neck. Radiographs of the skull, chest, cervical and thoracic spine, and shoulder were normal. There was no loss of consciousness, chest pain, or breathing difficulties. The patient was observed in the hospital until stable and referred for follow-up in the hand clinic at 4 weeks. An electromyelogram (EMG) was scheduled. C linical examination revealed weakness of deltoid, supraspinatus, infraspinatus, teres minor, biceps, brachialis, brachioradialis, and extensor carpi radialis longus. The remainder of his forearm musculature was preserved and he could
grasp, release, and pinch. Sensations were decreased along the distribution of the axillary nerve. There was 3 cm wasting of his arm and 2 cm of the forearm. Tinelâs sign is positive around the clavicle. Hornerâs signs are absent and his arm lies against the body. The EMG report showed fibrillation potentials in the weak muscles. The patient can now flex his elbow. When asked to demonstrate, he flexes his wrist and pronates his forearm to swing his elbow into flexion.
The most important indication for early exploration in this patient is:
1
Absence of biceps function at 3 months
2
Absence of biceps function with return of extensor carpi radialis longus (EC RL) power at 4 months
3
Presence of trick movements
4
Subluxation of humeral head on radiographs
5
Weakness of the supraspinatus
An important indication for early exploration is the recovery of a distally supplied muscle, EC RLâC 6, in the absence of a proximally supplied muscle, bicepsâC 5. Trick movements are adaptive movements employed by the patient by recruiting other muscles, for example, the use of flexor-pronator as elbow flexors in this patient. Bony deformity is a late sequelae and biceps recovery at 3 months is important in obstetric brachial palsy.
QUESTION 15 OF 50
A 35-year-old man who has had a 6-month history of low back pain and tenderness now reports worsening pain and stiffness in the hips and entire back. An AP radiograph of the pelvis demonstrates fusion of the sacroiliac joints bilaterally. What is the next most appropriate step in management?
1
Anesthetic injections in both sacroiliac joints
2
Sacroiliac fusion with plate fixation
3
Anti-inflammatory medications, physical therapy, and HLA-B27 testing
4
Patient reassurance and follow-up as needed
5
Immediate bilateral sacroiliac joint aspiration and culture
The patient has a classic presentation of early ankylosing spondylitis. Sacroiliac joint fusion is the earliest radiographic finding and is typically followed by cephalad spinal progression. Early treatment of ankylosing spondylitis consists of nonsteroidal anti-inflammatory drugs and physical therapy to preserve spinal motion. HLA-B27 testing is positive in most (about 95%) patients; however, it is not pathognomonic because it can be positive with other conditions. Considering the progressive nature of this disease, further work-up in a patient with potential ankylosing spondylitis is not warranted. Sacroiliac joint anesthetic injections and sacroiliac fusion are not recommended treatments for early ankylosing spondylitis. Aspiration of the sacroiliac joints can be done if sacroiliac joint infection is suspected;however, in the absence of fever or other constitutional symptoms, infection is unlikely.
QUESTION 16 OF 50
Kinematic testing of patellofemoral motion demonstrates that malalignment that produces increased Q angle causes a shift of the patella laterally in the trochlear groove and is most pronounced during what phase of the flexion arc?
1
0 to 15 degrees
2
20 to 30 degrees
3
40 to 90 degrees
4
100 to 120 degrees
5
130 to 140 degrees
DISCUSSION: Dynamic patellofemoral joint contact measurements on cadaveric knees with simulated increased Q angle demonstrated that forces shifted to the lateral facet. The lateral shift in the patella was most pronounced from 40 to 90 degrees of flexion. At lower degrees of flexion, the lateral shift was significantly less. At higher degrees of flexion, the continued shift of the patella was not as pronounced.
REFERENCES: Ramappa AJ, Apreleva M, Harrold FR, et al: The effects of medialization and anteromedialization of the tibial tubercle on patellofemoral mechanics and kinematics. Am J Sports Med 2006;34:749-756.
Huberti HH, Hayes WC: Patellofemoral contact pressure: The influence of q-angle and tendofemoral contact. J Bone Joint Surg Am 1984;66:715-724.
QUESTION 17 OF 50
of 100
A 24-year-old man is involved in a motor vehicle collision. A CT scan of the cervical spine shows the injury in Figures 1 and
1
He had a normal motor and sensory examination. What is the most appropriate treatment option for this injury?

2
Immobilization in a cervical collar
3
Halo traction
4
Anterior cervical diskectomy and fusion or posterior cervical instrumentation and fusion C4-C5
5
Anterior cervical diskectomy and fusion or posterior cervical instrumentation and fusion C3-C4, C4-C5
■ The figures show a unilateral floating mass fracture of C4 with horizontalization of the C4 facet on the left side and <25% anterior listhesis at C4-C5. These injuries are considered 2 level injuries; therefore, the injury in this patient is a C3-C4 and C4-C5 injury. Nonoperative treatment has been found to be unsuccessful in managing these injuries and lead to subluxation over time. Surgical fixation of the two involved levels, either anteriorly or posteriorly is acceptable. Surgical treatment of only one of the levels may leave the instability at the second level unaddressed.
QUESTION 18 OF 50
A 32-year-old soccer player presents with severe right ankle pain and inability to bear weight after sustaining a slide-tackle injury during a game. Radiographs are shown in Figures A and B. Given the nature of his injury, he is taken for surgical reduction and fixation. Following medial malleolar fixation, the syndesmosis is addressed. All of the following are true regarding the most appropriate intraoperative technique for anatomic syndesmotic reduction EXCEPT:
1
The axis of the reduction clamp should parallel the anatomic trans-syndesmotic angle
2
The lateral tine of the clamp should be seated just posterior to the lateral malleolar ridge
3
The medial tine should be placed on the anterior third of the tibia on a true lateral fluoroscopic view of the ankle
4
The reduction clamp should be placed 1-2cm proximal to the tibial plafond
5
The surgeon should apply judicious compression under fluoroscopic visualization to avoid over-compression of the syndesmosis
When placing a clamp across the syndesmosis to facilitate reduction, the lateral tine should be placed directly on the lateral malleolar ridge. Placing the lateral tine either more anteriorly or posteriorly has been shown to result in sagittal malreduction from fibular translation.
Syndesmotic reduction has proven to be technically challenging, with reportedly greater than 50% of cases resulting in malreduction. Provisional reduction is most often attained via a pointed reduction clamp. Placement of the lateral tine is outlined above. The medial tine should be placed at the anatomic midportion of the medial tibia, which can be confirmed
fluoroscopically as the anterior third of the tibia on a true lateral view of the ankle. It is important to maintain the axis of the clamp parallel to the joint line and to the anatomic syndesmotic angle. The clamp should furthermore be maintained 1-2cm proximal to the mortise, at the level of the incisura, to avoid deformation or undue translation of the fibula. Lastly, over-compression of the syndesmosis has been demonstrated, though the clinical implications remain controversial.
Putnam et al. performed a radiographic analysis of the ideal orientation for placement of a syndesmotic reduction clamp. Based on the CT scans of uninjured adult ankles, the authors showed that the trans-syndesmotic axis could be most reliably paralleled by a reduction clamp by placing the lateral tine on the lateral malleolar ridge and the medial tine radiographically within the anterior third of the tibia, anatomically half-way between the anterior and posterior cortices. They further specified that the ideal location was within the central one-third of the distance from the anterior tibial cortex to the anterior fibular cortex.
Cosgrove et al. prospectively evaluated the effect of medial clamp tine positioning on the incidence of syndesmotic malreduction. The authors found that malreduction most often resulted from deviation of the clamp axis from the syndesmotic axis. With the clamp at 1-2cm proximal to the mortise and the lateral tine on the lateral malleolar ridge, the ideal position of the medial tine was within the anterior third of the tibia. The rate of sagittal malreduction increased substantially with increasingly posterior placement of the medial tine. The medial clamp position did not affect coronal plane malreduction.
Gardner et al. review the technical considerations in reduction and fixation of syndesmotic injuries. The authors stress careful positioning of the reduction clamp, advocating that the clamp should be placed from the lateral malleolar ridge to the center of the anteroposterior width of the medial tibia.
Additionally, they note that placement too proximal or distal results in coronal plane deformity of the fibula, and that over-compression of the syndesmosis is certainly possible.
Figure A is the AP radiograph of the left ankle demonstrating a displaced medial malleolar fracture and syndesmotic widening. Figure B is the lateral radiograph of the ipsilateral knee showing an associated proximal fibular fracture.
Illustration A shows the syndesmotic angle and anatomic trans-syndesmotic axis as compared to the AP and lateral fluoroscopic axes. Illustration B shows the ideal positioning of the medial tine within the anterior third of the tibia on a true lateral view of the ankle.
Incorrect answers:
Answer 1: The axis of the reduction camp should parallel that of the trans-syndesmotic axis.
Answer 3: The medial tine is ideally placed within the anterior third of the tibia, and moreover within the central third of the distance between the anterior tibial and fibular cortices on a true lateral view of the ankle.
Answer 4: The clamp is ideally placed 1-2cm proximal to the tibial plafond at the level of the incisura to avoid deformation of the fibula, which has been associated with placement too proximal or distal.
Answer 5: Over-compression of the syndesmosis has been demonstrated radiographically, though the effect on the range of motion and clinical outcomes remains unclear.
QUESTION 19 OF 50
A high school football player asks you about an oral supplement that increases body mass and improves sprint times. He would like to use it to improve performance. What is the most likely agent?
1
Creatine
2
Caffeine
3
Testosterone
4
Human growth hormone
5
Ephedrine
DISCUSSION: The supplement is creatine. Approximately 17% of high school athletes and about 30% of high school football players use creatine. Creatine is a protein synthesized in the liver and the kidney, circulates in the bloodstream, and is incorporated into muscle. Its use is associated with increased muscle mass, short-term improvement in sprinting, and may allow for increased anaerobic resistance performance. Caffeine and ephedrine are taken orally but do not increase muscle mass. Testosterone and human growth hormone are both associated with increased body mass but must be injected.
PREFERRED RESPONSE: 1
REFERENCES: McGuine TA, Sullivan JC, Bernhardt DT: Creatine supplementation in high school football players. Clin J Sports Med 2001 ;11:247-253.
Rawson ES, Gunn B, Clarkson PM: The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res 2001; 15:178-184.
Branch JD: Effect of creatine supplementation on body composition and performance: A meta-analysis.
Int J Sport Nutr Exerc Metab 2003;13:198-226.
QUESTION 20 OF 50
of 100 A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
1
Midsubstance tear of the lateral ulnar collateral ligament
2
Proximal avulsion of the ulnar collateral ligament
3
Proximal avulsion of the lateral ulnar collateral ligament
4
Distal bony avulsion of the ulnar collateral ligament from the sublime tubercle
DISCUSSION:
Classic posterior elbow dislocations result from a posterolateral rotatory mechanism, whereby the hand is fixed (typically on the ground) while the weight of the body creates a valgus and external rotation moment on the elbow. This results first in tearing of the lateral collateral ligament that proceeds medially through the anterior and posterior joint capsules, ending with potential involvement of the ulnar collateral ligament (but this is not universal). McKee and associates assessed the lateral soft-tissue injury pattern of elbow dislocations
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
QUESTION 21 OF 50
Superficial frostbite injuries result in:
1
Minimal tissue loss
2
Significant tissue loss
3
Firm tissue
4
Amputation
5
Hemorrhagic blisters
Superficial frostbite typically involves minimal tissue loss. Patients have pliable skin with sensation. Deep frostbite typically results in significant soft tissue loss with firm anesthetic tissue that forms hemorrhagic blisters.
Increasing the hyaluroniCacid concentration in a joint
4
Decreasing the hyaluroniCacid concentration in a joint
5
Intra-articular steroids do not change synovial fluid characteristics
Intra-articular steroids change synovial fluid characteristics by increasing hyaluroniCacid concentration
QUESTION 23 OF 50
Optimization of early active motion protocols for flexor tendon rehabilitation includes:
1
Multi-strand repair
2
Splinting the digit in extension
3
Using passive flexion of the finger to gain flexibility
4
Therapist hyperextension of the finger
5
Ultrasound as an adjunct
The use of 6- and 8-strand repair techniques allow the flexor tendon repair to withstand the force applied by early active motion protocols. The addition of epitendinous tendon repair also strengthens the repair.
QUESTION 24 OF 50
of 100
22
The lesser or small saphenous vein passes along the sural nerve in the mid calf
1
medially.
2
laterally.
3
anteriorly.
4
posteriorly.
The sural nerve is at risk when incisions are placed near the Achilles tendon musculotendinous junction of the posterior calf. The nerve, which can be easily identified when the vein is visualized, is at risk during Achilles tendon recession procedures, and the vein provides a landmark with which to identify the nerve.
RECOMMENDED READINGS
1. [Eid EM, Hegazy AM. Anatomical variations of the human sural nerve and its role in clinical and surgical procedures .Clin Anat.2011Mar;24(2):237-45.doi: 10.1002/ ca.21068. Epub 2010 Oct 14.PubMed PMID: 20949489.](http://www.ncbi.nlm.nih.gov/pubmed/20949489)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20949489)
2. Hoppenfeld S, deBoer P, Buckley R. Surgical Exposures in Orthopaedics. The Anatomic Approach. Philadelphia, PA: Lippincott Williams &Wilkins 2009:585-622.
3. [Aktan Ikiz ZA, Uçerler H, Bilge O. The anatomic features of the sural nerve with an emphasis on its clinical importance. Foot Ankle Int. 2005 Jul;26(7):560-7. PubMed PMID: 16045849.](http://www.ncbi.nlm.nih.gov/pubmed/16045849)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16045849)
QUESTION 25 OF 50
Which of the following methods reduce radiation exposure to a surgeon during fluoroscopic procedures:
1
Avoiding the inverted C -arm position
2
Avoiding collimation of the radiation beam
3
Limiting the use of the foot pedal for controlling the fluoroscopy unit
4
Always standing on the opposite side of the C -arm
5
Increasing the amperage of each exposure
One of the best ways to limit radiation exposure is to increase distance from the C -arm. Surgeons should always stand on the opposite side of the C -arm and remember the following methods for reducing radiation exposure:
Increase distance (doubling distance reduces exposure by a factor of 4) Inverted position of the C -arm (increases distance)
Shielding: 90% attenuated by 0.25-mm apron
C ollimation (reduces the size of the beam)
Foot pedal to control the fluoroscopy unit (decreases the amount of exposure)
QUESTION 26 OF 50
-Figure 81 is the radiograph of a healthy 72-year-old man who has a 3-month history of medial knee pain.He denies any specific trauma. Until 3 months ago when the pain began, he had been an avid runner for many years. Initial treatment should be oral anti-inflammatory medication
1
alone.
2
with food.
3
with a proton pump inhibitor.
4
with glucosamine hydrochloride.
No detailed explanation provided for this question.
QUESTION 27 OF 50
A patient with spina bifida has significant symmetrical calcaneus positioning of both ankles. This is most likely due to:
1
Lack of ambulatory experience
2
Braces that are set in too much dorsiflexion
3
Motor level at L3
4
Motor level at L5
5
Motor level at S1
At motor level L5, dorsiflexors overpower plantarflexors to cause a calcaneus position.
This condition occurs from muscle imbalance. Even with significant ambulation, it will persist. Brace properties do not cause fixed deformity.
At L3, neither dorsiflexors nor plantarflexors of the ankle work. At S1, both dorsiflexors and plantarflexors are well innervated.
QUESTION 28 OF 50
A 50-year-old man who underwent an arthroscopic rotator cuff repair 5 days ago now returns for an early postoperative follow-up because of increasing pain in his shoulder. He reports increasing malaise and has a low-grade fever. Examination reveals no redness or swelling, but he has scant serous drainage from the posterior portal. An emergent Gram stain is positive for gram-positive cocci. The next most appropriate step in management should consist of
1
oral antibiotics and observation.
2
IV antibiotics and observation.
3
immediate arthroscopic debridement and lavage.
4
blood cultures, oral antibiotics, and a reculture in 2 days.
5
aspiration of the joint at his regular follow-up in 7 days if the symptoms increase.
An infection of the shoulder is considered a surgical emergency unless there are medical reasons that a patient cannot be taken to the operating room. If cultures of wound drainage are in question, then an aspiration should be done emergently, not several days later. The hallmark of infection in any major joint is increasing pain out of proportion to what is expected. Drainage occurring 1 to 2 days after an arthroscopic procedure is not normal, and it should be aggressively treated. Delay in diagnosis can result in sepsis and on a delayed basis, postinfectious arthritis. Both the glenohumeral joint and the subacromial space require debridement and irrigation, followed by antibiotics after both areas are cultured.
REFERENCES: Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213.
Settecerri JJ, Pitner MA, Rock MG, Hanssen AD, Cofield RH: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5.
Ward WG, Eckardt JJ: Subacromial/subdeltoid bursa abscesses: An overlooked diagnosis. Clin Orthop 1993;288:189-194.
Ward WG, Goldner RD: Shoulder pyarthrosis: A concomittant process. Orthopedics 1994;17:591-595.
QUESTION 29 OF 50
of 100
Which distal biceps repair technique has the highest load to failure in vitro?
1
Suspensory cortical button (Endobutton)
2
Suture anchor
3
Transosseous suture
4
Interference screw
- Suspensory cortical button (Endobutton)_
QUESTION 30 OF 50
What is the most common complication following surgical treatment of a displaced talar neck fracture?
1
Osteonecrosis
2
Varus malunion
3
Posttraumatic arthritis
4
Fracture delayed union/nonunion
5
Wound dehiscence/delayed wound healing
The most frequent complication is posttraumatic arthritis. With talar neck fractures,osteonecrosis is relatively common, occurring in up to 50% of patients. Fracture nonunion occurs in 10%to 12% of patients. Varus malunion can occur with medial comminution. Wound dehiscence and deep infection are much less frequently encountered.
QUESTION 31 OF 50
A 29-year-old woman is seen in the emergency department with a 24-hour history of severe back and leg pain precipitated by weight-lifting. The patient reports bilateral leg pain and is unable to urinate. She has dense anesthesia in the perineal region on examination. A MRI scan is shown in Figure 38. The patient is taken to surgery urgently. What is her prognosis for recovery? ---
1
Improvement in her pain and sensory symptoms following surgery but may have residual bladder dysfunction
2
Decreased pain following surgery; sensory deficits and bladder function are not likely to improve
3
No change in her symptoms following surgery
4
Complete resolution of pain and will have normal sensation and bladder function following surgery
5
Improvement in her pain and complete return of bladder function following surgery; sensation may not return
The patient with cauda equina syndrome should be taken to surgery urgently to provide the best chance of symptom resolution. However, many studies indicate that patients with cauda equine syndrome do not return to a completely normal status even following urgent surgery. Whereas pain is typically relieved after surgery, other deficits, especially bladder and sexual dysfunction, may persist.Particularly in light of the patient’s severe saddle anesthesia, she may have a poor prognosis for recovery of normal bladder function.
QUESTION 32 OF 50
Posterior cruciate-retaining total knee arthroplasty has been studied by numerous methods including kinematic video fluoroscopy. Which of the following is the best description of typical kinematic behavior?
1
Unpredictable anterior femoral condylar translation from full extension to 90 degrees of flexion
2
Predictable femoral rollback from full extension to 90 degrees of flexion
3
Medial femoral condyle pivot with minimal medial femoral condyle translation and lateral femoral condyle posterior translation in flexion
4
Lateral femoral condyle pivot with minimal medial femoral condyle translation
5
Anterior tibial contact of both the medial and lateral femoral condyles in full extension
DISCUSSION: In vivo fluoroscopic studies have enlightened orthopaedic surgeons as to the actual kinematic performance of the total knee implants. Importantly, many technical factors combine to result in abnormal kinematics after total knee arthroplasty. The typical kinematics of the normal knee are negated by osteoarthritis and the various changes created by the surgeon’s technique. Dennis and associates observed that anterior femoral condylar translation during deep knee flexion was most commonly observed in posterior cruciate-retaining knees.
REFERENCES: Dennis DA, Komistek RD, Mahfouz MR, et al: Multicenter determination of in vivo kinematics after total knee arthroplasty. Clin Orthop Relat Res 2003;416:37-57.
Freeman MA, Pinskerova V: The movement of the normal tibio-femoral joint. J Biomech 2005-38'197- 208.
**42 • American Academy of Orthopaedic Surgeons**
Figure 52
QUESTION 33 OF 50
of 100
Which inheritance pattern has been described for the condition shown in Figures 64a through 64d?
1
Autosomal recessive
2
Autosomal dominant
3
X-linked recessive
4
X-linked dominant
- Autosomal dominant
QUESTION 34 OF 50
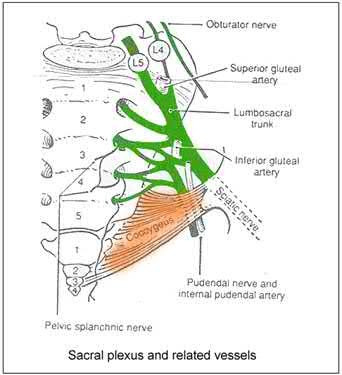
What structure has been described as having a risk of injury with retractor placement on the sacrum during combined acetabular-pelvic ring surgery using the Stoppa approach with a lateral window?
1
External iliac artery
2
Pudendal nerve
3
Corona mortis
4
L5 nerve root
5
Ilioinguinal nerve
Care must be taken when placing a retractor on the anterior aspect of the sacrum, as the L4 and L5 nerve roots are both at risk.
Illustration A shows a diagram of the lumbosacral plexus, indicating the proximity of the L4 and L5 nerve roots to the anterior sacrum and SI joint.
The first referenced article by Atlihan et al reported on the anatomy of the anterior sacroiliac joint and reported that the L4 nerve root is within 1 cm of the joint at its inferior margin.
The second article by Ebraheim et al found that the L4 and L5 nerve roots are 10 mm medial to the sacroiliac joint at the pelvic brim.
QUESTION 35 OF 50
of 100
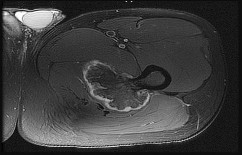
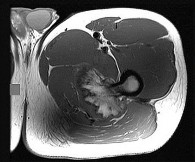
Figures 97a through 97d are the radiographs and MR images of a 21-year-old man with symptoms of a left medial thigh mass. Upon examination, you palpate a firm, fixed, deep, nontender mass of the medial proximal left thigh. No other masses are found during the examination. The patient fears metastatic disease. What is the risk for malignant transformation throughout this patient’s lifetime?
1
0%
2
Less than 1%
3
Less than 15%
4
More than 15%
The images reveal a solitary pedunculated osteochondroma. Malignant degeneration of solitary osteochondromas occurs in fewer than 1% of patients. A reasonable approach would be to inform the patient of the rare (less than 1%) incidence of malignant degeneration and to return for evaluation if symptoms develop or if the patient notices growth of the lesion.
RECOMMENDED READINGS
104. Schwartz AJ. Benign cartilage tumors. In: Biermann JS, ed. _Orthopaedic Knowledge Update Musculoskeletal Tumors 3_. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013:97-106.
105. [Aboulafia AJ, Kennon RE, Jelinek JS. Benign bone tumors of childhood. J Am Acad Orthop Surg. 1999 Nov-Dec;7(6):377-88. Review. PubMed PMID: 11505926.](http://www.ncbi.nlm.nih.gov/pubmed/11505926)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11505926)
QUESTION 36 OF 50
Currently, what is the most common clinical study type in the orthopaedic literature?
1
Level 1 (prospective, randomized trial)
2
Level 2 (cohort trial)
3
Level 3 (retrospective case control)
4
Level 4 (retrospective case series)
5
Level 5 (expert opinion)
#
**
Although a recent push for prospective, randomized trials has been advocated by multiple orthopaedic journals, many studies published continue to be of Level 4 evidence (retrospective case series). Case series represented 64% of all studies reviewed by Freedman and associates in 2001 from the British and American volumes of Journal of Bone and Joint Surgery and from Clinical Orthopaedics and Related Research.
Obremskey and associates published that
58.1% of all studies from nine orthopaedic journals were Level 4 evidence. Further investigation of more current trends is likely warranted with the
current emphasis on publishing higher level-of-evidence studies in orthopaedic journals.
QUESTION 37 OF 50
of 100
A surgeon is performing a revision total hip arthroplasty. Multiple screws are used to stabilize the acetabulum, including screws placed in the anterior superior and posterior superior quadrants. In the postanesthesia care unit, the patient develops a progressive decline in blood pressure. Intraoperative injury to which anatomical structure has most likely occurred?
1
Femoral artery
2
External Iliac artery
3
Superior gluteal artery
4
Inferior gluteal artery
Acetabular screws are commonly used to stabilize the acetabular component. This is particularly true in revision surgery. Wasielewski and associates described a quadrant system for placing screws, and the safest quadrants for screw placement are the posterior superior and posterior inferior quadrants. Placement of screws in the anterior superior quadrant is particularly dangerous because the screws may damage the external iliac artery or vein.
The femoral artery is more anterior and distal and less likely to be damaged by screw placement. The superior and inferior gluteal arteries may be injured but are less likely to be affected by screw placement anteriorly and are more likely to be noted immediately.
RECOMMENDED READINGS
5. Wasielewski RC, Cooperstein LA, Kruger MP, Rubash HE. Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am. 1990 Apr;72(4):501-
[8/. PubMed PMID: 2324135. ](http://www.ncbi.nlm.nih.gov/pubmed/2324135)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2324135)
6. [Wasielewski RC, Crossett LS, Rubash HE. Neural and vascular injury in total hip arthroplasty. Orthop Clin North Am. 1992 Apr;23(2):219-35. Review. PubMed PMID: 1315014. ](http://www.ncbi.nlm.nih.gov/pubmed/1315014)[View Abstract ](http://www.ncbi.nlm.nih.gov/pubmed/1315014)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1315014)
QUESTION 38 OF 50
A 13-year-old pitcher is hit in the left intercostal space by a line drive ball. He collapses, is apneic and unresponsive, and his radial pulse is absent. What is the next step in management?
1
Protect the airway and use smelling salts
2
Protect the airway, move to the shade, and place in reverse Trendelenburg
3
Protect the airway and protect from seizure activity
4
Protect the airway, start CPR, and prepare to cardiovert
5
Protect the airway, and move patient slowly to a spine board
DISCUSSION: Sudden death in athletes without structural cardiac damage is referred to as commotio cordis. This is an emergency. The immediate priorities are protection of the airway, starting CPR, and early cardioversion as this patient has an arrythmia. It is hypothesized to occur from apnea, vasovagal reflex, or ventricular arrhythmia as reported by Maron and associates from the direct impact of the baseball during a vulnerable part of the cardiac rhythm. Janda and associates reported that soft-core baseballs may not differ from standard baseballs with regard to the risk of fatal chest-impact injury while playing baseball. High survival rates are associated with rapid treatment.
REFERENCES: Maron BJ, Poliac LC, Kaplan JA, et al: Blunt impact to the chest leading to sudden death from cardiac arrest during sports activities. N Engl J Med 1995;333:337-342.
Janda DH, Bir CA, Viano DC, et al: Blunt chest impacts: Assessing the relative risk of fatal cardiac injury from various baseballs. J Trauma 1998;44:298-303.
QUESTION 39 OF 50
A 32-year-old powerlifter who was performing a dead lift 3 days ago noted a sharp pain in the front of his dominant right arm just after beginning to lower the weight. He now reports pain in the anterior aspect of the arm that worsens when he opens a door. Examination reveals moderate ecchymosis and swelling of the forearm and tenderness in the antecubital fossa. The MRI scans are shown in Figures 15a and 15b. If the injury is left unrepaired, the greatest functional deficit will most likely be the loss of
1
elbow extension motion.
2
elbow flexion strength.
3
forearm supination motion.
4
forearm pronation strength.
5
forearm supination strength.
A complete tear of the distal biceps brachii most often occurs from a large, rapid eccentric elbow extension load. A pop or tearing sensation usually occurs, and a palpable defect in the antecubital fossa is often present on examination. The treatment of choice is a direct primary repair by a two-incision technique. If left unrepaired, the most disabling consequence is the loss of forearm supination strength. It is unlikely that significant elbow or forearm motion will be lost if the rupture is left unrepaired and early motion exercises are initiated. Elbow flexion strength tends to return with time, but the loss of forearm supination strength remains problematic.
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Agins HJ, Chess JL, Hoekstra DV, Teitge RA: Rupture of the distal insertion of the biceps brachii tendon. Clin Orthop 1988;234:34-38.
QUESTION 40 OF 50
Water comprises what percentage of bone composition:
1
5% to 8%
2
20%
3
30%
4
40%
5
50%
Bone has the following composition:
Mineral or inorganiCphase 70% Water 5% to 8% OrganiCmatrix 22% to 25% Collagen type I 90% Noncollagenous proteins 5% to 8%
QUESTION 41 OF 50
of 100
The workup to exclude other congenital abnormalities should include evaluation of which systems?
1
Cardiac, renal, and gastrointestinal (GI)
2
Cardiac, renal, and auditory
3
Cardiac, pulmonary, and GI
4
Cardiac, pulmonary, and neural axis
- Cardiac, renal, and auditory
QUESTION 42 OF 50
A 12-year-old girl has the painful foot deformity seen in Figure 79. You advise her that she has juvenile bunions. How do they differ from adult bunions?
1
Metatarsus primus varus
2
Large exostosis
3
Rigidity of the metatarsal phalangeal joint
4
Greater hallux valgus angle than in adult bunions
5
Prominent bursal thickening over the medial eminence
DISCUSSION: The hallmark of the juvenile bunion is metatarsus primus varus. Increased flexibility of
the first metatarsal phalangeal joint leads to increased deformity. The hallux valgus angle is less than the adult bunion. Bursal thickenings and prominence of the medial eminence are less in a juvenile bunion.
REFERENCES: Coughlin MJ: Juvenile bunions, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. Philadelphia, PA, Mosley, 1993, pp 297-339.
Coughlin MJ, Mann RA: The pathophysiology of juvenile bunion. Instr Course Lect 1987;36:123-136.
68 • American Academy of Orthopaedic Surgeons
Figure 80a Figure 80b Figure 80c
QUESTION 43 OF 50
Which of the following describes the inheritance pattern of Duchennes muscular dystrophy:
1
Autosomal dominant
2
Autosomal recessive
3
X-linked dominant
4
X-linked recessive
5
Sporadic
C ommon inheritance patterns that should be known for examinations:
Autosomal dominant
Autosomal recessive
X-linked dominant
X-linked recessive
Achondroplasia Sickle cell Hypophosphatemic rickets Hemophilia (A, B)
SED (congenital) OI (II, III) Duchennes muscular dystrophy
MED Hypophosphatasia Hunters syndrome
Marfanâs syndrome Homocystinuria SED (tarda)
Ehlers-Danlos syndrome Gaucherâs disease Beckerâs muscular dystrophy
Abbreviations: OI (I,IV)=Osteogenesis imperfecta, SED=Spondyloepiphyseal dysplasia, MED=Multiple epiphyseal dysplasia, MHE=Multiple hereditary exostosis
QUESTION 44 OF 50
A patient presents for treatment of a dislocated second metatarsophalangeal joint. Radiographs demonstrate the dislocation. In addition to soft tissue balancing, you perform an oblique shortening osteotomy of the second metatarsal head (Weil). The most common complication following this osteotomy is:
1
Recurrent dislocation
2
Avascular necrosis of the metatarsal head
3
Arthritis of the second metatarsophalangeal joint
4
Elevation of the second toe
5
C law toe deformity
The Weil osteotomy is a good procedure to correct deformity about the lesser metatarsophalangeal joint but is associated with potential complications, the most common of which is elevation of the second toe. As a result of shortening and plantar shifting of the metatarsal, the intrinsic muscles shift dorsally and can function as a dorsiflexor of the metatarsophalangeal joint.
QUESTION 45 OF 50
In congenital lesions characterized by failure of formation of parts, the most functional, without treatment, is/are:
1
Transverse arrest at the wrist.
2
C entral deficiencies.
3
VATER syndrome.
4
Ulnar deficiencies.
5
Radial deficiencies
C entral deficiencies allow a wide grasp, good release and pinch. These are also termed "cleft hand". The other conditions produce greater impairment.
QUESTION 46 OF 50
of 100
A 28-year-old man is subjected to a blast and sustains the fragmentary injury shown in the plain radiographs in Figures 99a and 99b. He lacks distal radial nerve function. His wounds have associated soft-tissue damage, although they do not appear grossly contaminated, and tissue loss would not prevent either primary or delayed closure. Which surgical plan is associated with the lowest rate of revision surgery and complications?
1
Open reduction and intramedullary fixation
2
Primary closure and coaptation splinting
3
Nerve exploration and intramedullary fixation
4
Nerve exploration and internal fixation
Two indications for nerve exploration are open fractures and high-velocity injuries. Nerve exploration under these circumstances can improve outcomes. Intramedullary fixation is associated with higher revision surgery and complication rates vs open reduction and internal fixation. Nonsurgical treatment in the setting of a high-energy injury is associated with a higher nonunion rate.
RECOMMENDED READINGS
10. [Heineman DJ, Poolman RW, Nork SE, Ponsen KJ, Bhandari M. Plate fixation or intramedullary fixation of humeral shaft fractures. Acta Orthop. 2010 Apr;81(2):216-23. doi: 10.3109/17453671003635884. Review. Erratum in: Acta Orthop. 2010 Oct;81(5):647. PubMed PMID: 20170424. ](http://www.ncbi.nlm.nih.gov/pubmed/20170424)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20170424)
11. [Bishop J, Ring D. Management of radial nerve palsy associated with humeral shaft fracture: a decision analysis model. J Hand Surg Am. 2009 Jul-Aug;34(6):991-6.e1. doi: 10.1016/j.jhsa.2008.12.029. Epub 2009 Apr 10. PubMed PMID: 19361935. ](http://www.ncbi.nlm.nih.gov/pubmed/19361935)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19361935)
QUESTION 47 OF 50
A 17-year-old high school football player injures his right ankle during a game. Examination reveals swelling and a closed ankle deformity, with normal foot circulation and sensation. Radiographs are shown in Figures 10a and 10b. In addition to closed reduction, management should include
1
cast immobilization.
2
delayed fixation of the medial malleolus.
3
immediate fixation of the medial malleolus and plating of the fibula.
4
immediate fixation of the medial malleolus, plating of the fibula, and placement of a syndesmotic screw.
5
immediate fixation of the medial malleolus and placement of a syndesmotic screw.
The examination and radiographs reveal a closed fracture-dislocation of the ankle with tibiofibular diastasis. Immediate fixation of the medial malleolus and plating of the fibula are indicated. If residual tibiofibular diastasis occurs with lateral translation of the fibula after plating, a syndesmotic screw is placed to stabilize the syndesmosis. Ankle fracture-dislocations associated with a proximal fibular fracture (Maisonneuve fracture) require syndesmotic fixation, but the fibula is not plated. Unstable ankle fractures require surgical treatment. If swelling is severe (fracture blisters, loss of skin wrinkling), a compressive splint is applied and surgery is delayed for 5 to 7 days.
REFERENCES: Browner BD, Jupiter JB, Levine AM, Trafton PG: Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 1887-1957.
Stiehl JB: Ankle fractures with diastasis. Instr Course Lect 1990;39:95-103.
QUESTION 48 OF 50
of 100
A 21-year-old man learned he had Ewing sarcoma of the right distal femur at age 13. He underwent treatment with neoadjuvant chemotherapy, surgical resection with distal femoral replacement, and adjuvant chemotherapy. He completed treatment at age 14, and subsequent surveillance imaging has shown no evidence of recurrence. He has noted increasing fatigue during the last 3 months, however, and bleeding when he brushes his teeth. An examination is unremarkable with the exception of bilateral pretibial bruising for which the patient does not recall trauma. Which tests will aid in diagnosis?
1
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
2
Serum protein electrophoresis
3
Complete blood count (CBC) with a peripheral smear
4
Platelet aggregation testing and bleeding time
This patient most likely has therapy-associated leukemia, which occurs in approximately 2% of patients who have Ewing sarcoma within 5 years of receiving treatment. Most cases are myelodysplasia or acute myeloid leukemia. Most patients with therapy-associated leukemia
respond poorly to conventional chemotherapies and require allogenic stem cell transplant for cure. Fatigue, gum bleeding, and bruising should raise concern for leukemia in light of his clinical history. A CBC with a peripheral smear will likely reveal an elevated leukocyte count with an abnormal percentage of myeloblasts. ESR and CRP are required to assess for infection of a prosthesis. Fatigue may be associated with chronic infection, but bleeding would be atypical. Platelet aggregation test results may be abnormal for this patient, but this testing is unlikely to reveal a specific diagnosis because drugs and genetic disorders may cause platelet aggregation dysfunction. Serum protein electrophoresis is diagnostic for multiple myeloma, but this patient is the wrong age for this condition and does not have appropriate signs and symptoms. A CBC can demonstrate early findings for leukemia with anemia and platelet suppression despite no blast presence. Of note, 25% of long-term survivors of Ewing sarcoma have findings of cardiotoxicity.
RECOMMENDED READINGS
10. [Bhatia S, Krailo MD, Chen Z, Burden L, Askin FB, Dickman PS, Grier HE, Link MP, Meyers PA, Perlman EJ, Rausen AR, Robison LL, Vietti TJ, Miser JS. Therapy-related myelodysplasia and acute myeloid leukemia after Ewing sarcoma and primitive neuroectodermal tumor of bone: A report from the Children's Oncology Group. Blood. 2007 Jan 1;109(1):46-51. Epub 2006 Sep 19. PubMed PMID: 16985182. ](http://www.ncbi.nlm.nih.gov/pubmed/16985182)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16985182)
11. [Hamilton SN, Carlson R, Hasan H, Rassekh SR, Goddard K. Long-term Outcomes and Complications in Pediatric Ewing Sarcoma. Am J Clin Oncol. 2015 Jan 16. [Epub ahead of print] PubMed PMID: 25599318. ](http://www.ncbi.nlm.nih.gov/pubmed/25599318)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25599318)
QUESTION 49 OF 50
Which of the following is the normal resting pressure in skeletal muscle:
1
0 mm Hg to 8 mm Hg
2
10 mm Hg to 16 mm Hg
3
18 mm Hg to 24 mm Hg
4
24 mm Hg to 30 mm Hg
5
30 mm Hg to 36 mm Hg
Normal resting muscle tissue pressure is between 0 mm Hg and 8 mm Hg. Remember, if one squeezes the muscle or pushes on it, then the compartment pressure increases.
Normal tissues have adequate tissue perfusion with increases in compartment pressure to within 10 mm Hg of the diastolic pressure. In damaged tissue (eg, tibia fracture), perfusion can be impaired when the diastolic pressure reaches within 20 mm Hg of the diastolic pressure.
One should remember that hypotensive patients with extremity injuries are prone to compartment syndromes. Correct Answer: 0 mm Hg to 8 mm Hg
QUESTION 50 OF 50
of 100
She completes the necessary testing and wishes to proceed with revision surgery. The most appropriate surgical option in this scenario involves implant removal and