Score: 0%
Advanced Orthopedic Mock Exam (Set FE4DA6)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
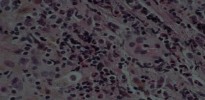
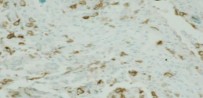
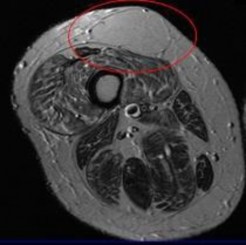
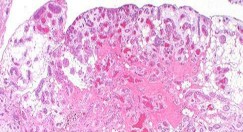
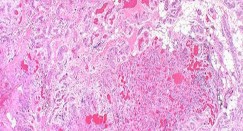
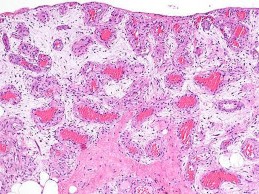
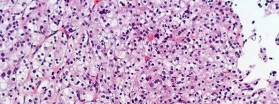
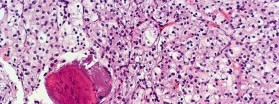
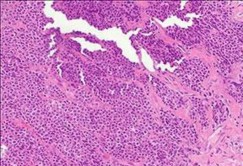
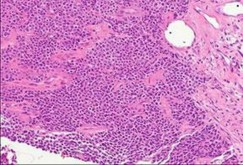
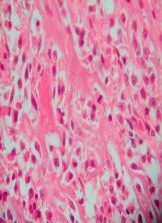
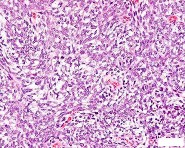
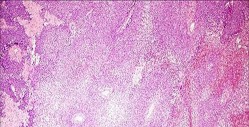
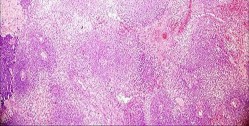
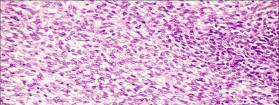
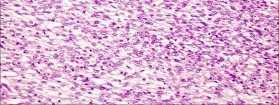
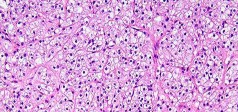
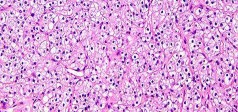
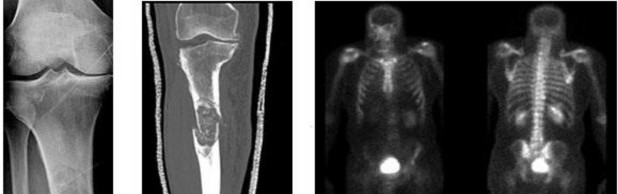
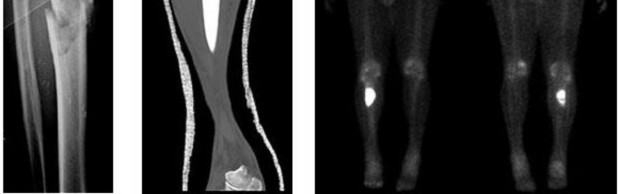
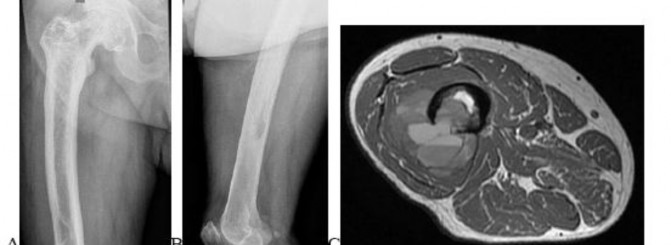
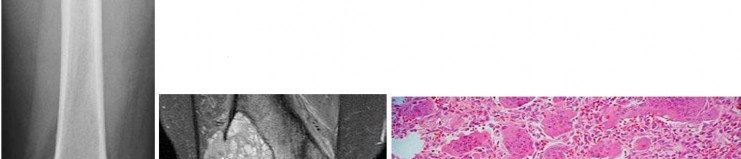
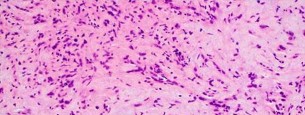
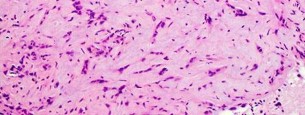
Figures 16a and 16b show the radiographs of a 2-year-old boy who has right arm swelling and pain. He also has multiple scalp lesions and chronic ear pain that has failed to respond to antibiotics. A biopsy specimen is shown in Figure 16c. Figure 16d shows an immunohistochemical stain with CD1a. What is the most likely diagnosis?


1
Langerhans' cell histiocytosis
2
Aneurysmal bone cyst
3
Ewing's sarcoma
4
Osteomyelitis
5
Ollier's enchondromatosis
No detailed explanation provided for this question.
QUESTION 2 OF 50
The periosteal vessels supply what portion of the cortical bone blood circulation:
1
5% to 10% of the inner endosteal surface
2
10% to 20% of the inner endosteal surface
3
1% to 5% of the outer periosteal surface
4
15% to 20% of the outer periosteal surface
5
30% to 50% of the outer periosteal surface
The periosteal vessels supply 15% to 20% of the outer periosteal surface. There are three defined blood supplies:
Nutrient vessel entering in the diaphysis
Metaphyseal vessels from the periarticular vessels (geniculate vessels) Periosteal vessels supply the outer 15% to 20% of the cortex
Nutrient vessel entering in the diaphysis
Metaphyseal vessels from the periarticular vessels (geniculate vessels) Periosteal vessels supply the outer 15% to 20% of the cortex
QUESTION 3 OF 50
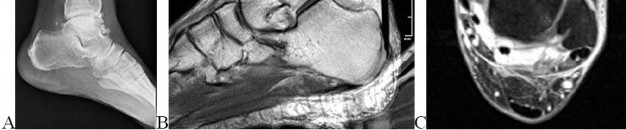
Figures 23a and 23b show
2. radiographs of a 52-year-old man
3. with diabetes who has had purulent
4. drainage from the medial side of his
5. right great toe for 3 weeks. He was
6. recently started on insulin.
7. Examination reveals a good dorsalis
8. pedis pulse but poor sensation from
9. the malleoli to the toes. Treatment
10. should consist of
11. 1- amputation of the great toe.
12. 2- bone culture and 6 weeks of IV
13. antibiotics.
14. 3- joint aspiration and 2 weeks of IV
15. antibiotics.
16. 4- excision interphalangeal arthroplasty.
17. 5- excision of infected bone and
18. interphalangeal joint arthrodesis.
2. radiographs of a 52-year-old man
3. with diabetes who has had purulent
4. drainage from the medial side of his
5. right great toe for 3 weeks. He was
6. recently started on insulin.
7. Examination reveals a good dorsalis
8. pedis pulse but poor sensation from
9. the malleoli to the toes. Treatment
10. should consist of
11. 1- amputation of the great toe.
12. 2- bone culture and 6 weeks of IV
13. antibiotics.
14. 3- joint aspiration and 2 weeks of IV
15. antibiotics.
16. 4- excision interphalangeal arthroplasty.
17. 5- excision of infected bone and
18. interphalangeal joint arthrodesis.
1
radiographs of a 52-year-old man
2
with diabetes who has had purulent
3
drainage from the medial side of his
4
right great toe for 3 weeks. He was
5
recently started on insulin.
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Penn I: Infections in the diabetic foot, in Samarco GJ (ed): The Foot in Diabetes. Philadelphia, PA, Lea & Febiger, 1991, pp 109-121. Wagner FW: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981, pp 66-122.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Penn I: Infections in the diabetic foot, in Samarco GJ (ed): The Foot in Diabetes. Philadelphia, PA, Lea & Febiger, 1991, pp 109-121. Wagner FW: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981, pp 66-122.
#
QUESTION 4 OF 50
A 64-year-old woman who underwent a successful total hip arthroplasty (THA) 2 years ago now reports a painful hip. A radiograph is shown in Figure 44. Laboratory evaluation includes an erythrocyte sedimentation rate (ESR) of 65 mm/h (0-30 mm/h) and a C-reactive protein of 5.4 mg/L (< 0.8 mg/L). What is the next step in management?
1
Ultrasound examination
2
Technetium bone scan
3
Indium-labeled WBC scan
4
Hip joint aspiration
5
Two-stage revision surgery
DISCUSSION: Hip joint aspiration, with analysis of the cell count, differential, and culture greatly aids in the diagnosis of infection in THA. Aspiration is indicated in this patient because both the ESR and C-reactive protein are elevated, and the radiograph shows well-fixed components without evidence of loosening. Technetium and Indium-labeled WBC scans have less specificity and sensitivity respectively, and may not be necessary if the diagnosis is confirmed by joint aspiration. Two-stage revision surgery may be the treatment of choice if infection is confirmed, but it is not the next step in this patient.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL American Academy of Orthopedic Surgeons, 2006, pp 475-503.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL American Academy of Orthopedic Surgeons, 2006, pp 475-503.
QUESTION 5 OF 50
Recurrence of hallux valgus deformity after corrective surgery has been shown to be related to which of the following?
1
Inversely correlated with presence of bipartite fibular sesamoid
2
Associated with residual increased tibial sesamoid displacement
3
Associated with squared lateral first metatarsal shape
4
Unrelated to preoperative 1-2 intermetatarsal angle
5
Unrelated to preoperative hallux valgus angle
DISCUSSION: Okuda and associates have studied the factors associated with the recurrence of hallux valgus deformity following correction with proximal first metatarsal osteotomy. The factors that they found associated with recurrence of deformity postoperatively are a rounded shape to the lateral first metatarsal head, severe lateral displacement of the tibial sesamoid, an increased preoperative 1-2 intermetatarsal angle, and an increased preoperative hallux valgus angle. The reported rate of recurrence of deformity after proximal first metatarsal osteotomy is 4% to 11%. PREFERRED RESPO: 2 Question 79 A 33-year-old woman has had plantar first metatarsophalangeal joint pain for 3 years. Examination reveals that she is tender under the medial sesamoid. She has no swelling or ecchymosis. The first metatarsophalangeal joint motion is equal and stable bilaterally. Radiographically, there is some fragmentation of the medial sesamoid with increased density in some of the fragments. Various orthotic and shoe modifications have failed to provide relief. What is the most appropriate management?
Medial sesamoid stress fractures with fragmentation that have not responded to nonsurgical management have done well after sesamoid excision. Excision of both sesamoids is not recommended. A first metatarsophalangeal joint arthrodesis is not going to resolve the issue of weight loading on the stress fractured, fragmented sesamoid. Open reduction can be considered if there are two large fragments without osteonecrosis. Corticosteroid injection is not going to provide long-term relief.Shoe modifications have already been tried, without relief.
QUESTION 6 OF 50
What is the most common complication following surgical treatment of a displaced talar neck fracture?
1
Osteonecrosis
2
Varus malunion
3
Posttraumatic arthritis
4
Fracture delayed union/nonunion
5
Wound dehiscence/delayed wound healing
The most frequent complication is posttraumatic arthritis. With talar neck fractures,osteonecrosis is relatively common, occurring in up to 50% of patients. Fracture nonunion occurs in 10%to 12% of patients. Varus malunion can occur with medial comminution. Wound dehiscence and deep infection are much less frequently encountered.
QUESTION 7 OF 50
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
1
Posterior capsular ligament
2
Anterior capsular ligament
3
Interclavicular ligament
4
Intra-articular disk
5
Subclavius tendon
In a cadaver ligament sectioning study, the posterior capsular ligament was considered the most important structure for anterior-posterior stability of the sternoclavicular joint. The anterior capsular ligament also helps prevent anterior displacement but not to the same degree as the posterior ligament. The interclavicular ligament provides little support for anteroposterior translation.
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
QUESTION 8 OF 50
Hallux rigidus is associated with:
1
Metatarsus primus elevatus
2
First ray hypermobility
3
Long first metatarsal
4
Flat- or chevron-shaped metatarsal head
5
Bipartate sesamoid
In a large series of patients with hallux rigidus, risk factors were evaluated. The only factor that had a positive correlation with having hallux rigidus was the radiographic shape of the 1st metatarsal head. Metatarsus primus elevatus, first ray hypermobility, or long first metatarsal head were not significantly associated with hallux rigidus.
QUESTION 9 OF 50
Patients treated with zoledronic acid within 90 days of a hip fracture, followed up with annual treatment, will most likely show:
1
Decreased vertebral fractures, no difference in nonvertebral fracture, and no difference in survival
2
Decreased vertebral fractures, decreased nonvertebral fracture, and improved survival
3
No difference in vertebral and nonvertebral fracture and no difference in survival
4
Improved bone mineral density (BMD) but no difference in fracture rate
5
Decreased fracture rate but no difference in survival or BMD
A large prospective, randomized study showed a reduction in vertebral and nonvertebral fractures when patients were treated with intravenous (IV) zoledronic acid within 90 days of a hip fracture, followed up with annual treatment.
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months BMD
  o   12 month: 2.6% vs -1.0%   o   24 month: 4.7% vs -0.7%   o   36 month: 5.5% vs -0.9% Death
  o   Hazard ratio: -0.72 (0.56 to 0.93 C I, P = .01) Adverse advents
  o   Pyrexia: 8.7% vs 3.1%   o   Myalgia: 4.9% vs 2.7%
  o   Bone pain: 3.2% vs 1.0%
C orrect Answer: Decreased vertebral fractures, decreased nonvertebral fracture, and improved survival
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months BMD
  o   12 month: 2.6% vs -1.0%   o   24 month: 4.7% vs -0.7%   o   36 month: 5.5% vs -0.9% Death
  o   Hazard ratio: -0.72 (0.56 to 0.93 C I, P = .01) Adverse advents
  o   Pyrexia: 8.7% vs 3.1%   o   Myalgia: 4.9% vs 2.7%
  o   Bone pain: 3.2% vs 1.0%
C orrect Answer: Decreased vertebral fractures, decreased nonvertebral fracture, and improved survival
QUESTION 10 OF 50
of 100
Figures 26a through 26c are the radiographs of a 34-year-old laborer who injured his wrist in high school and has experienced progressive wrist pain despite use of a splint and medications. Which procedure offers the best long-term prognosis for pain relief and improved function for this patient?



Figures 26a through 26c are the radiographs of a 34-year-old laborer who injured his wrist in high school and has experienced progressive wrist pain despite use of a splint and medications. Which procedure offers the best long-term prognosis for pain relief and improved function for this patient?
1
Scapholunate ligament reconstruction
2
Scaphoid excision and 4-corner fusion
3
Scaphoid-trapezium-trapezoid (STT) arthrodesis
4
Proximal row carpectomy (PRC)
This patient likely sustained a scapholunate ligament injury years prior that has led to arthritic changes. The radiographs demonstrate a stage IV scaphoid lunate advanced collapse (SLAC) wrist. Treatment options for a stage IV SLAC wrist include scaphoid excision with 4-corner fusion, full-wrist fusion, or total wrist arthroplasty. Considering the patient’s age and the arthritic changes about the proximal pole of the capitate, scaphoid excision and intercarpal fusion is the most appropriate procedure. Proximal row carpectomy is not indicated because of this patient’s age and arthritic changes about the proximal pole of the capitate. Wall and associates reported a higher probability of failure with PRC among patients younger than age 40. STT arthrodesis is not indicated because this would lead to increased load through the arthritic radio-scaphoid articulation. Scapholunate ligament reconstruction is not appropriate for this patient because of the wrist arthritic changes, which necessitate a salvage procedure.
RECOMMENDED READINGS
36. [Wall LB, Didonna ML, Kiefhaber TR, Stern PJ. Proximal row carpectomy: minimum 20-year followup. J Hand Surg Am. 2013 Aug;38(8):1498-504. doi: 10.1016/j.jhsa.2013.04.028. Epub 2013 Jun 25. PubMed PMID: 23809467. ](http://www.ncbi.nlm.nih.gov/pubmed/23809467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23809467)
37. [Weiss KE, Rodner CM. Osteoarthritis of the wrist. J Hand Surg Am. 2007 May-Jun;32(5):725-46. Review. PubMed PMID: 17482013. ](http://www.ncbi.nlm.nih.gov/pubmed/17482013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17482013)
CLINICAL SITUATION FOR QUESTIONS 27 THROUGH 30
A 25-year-old teacher has a traumatic fracture-dislocation of the ring finger proximal interphalangeal (PIP) joint. During surgical exploration, comminution of the palmar 60% of the middle phalanx is present, and the dorsal base of the middle phalanx is intact with healthy articular cartilage.
RECOMMENDED READINGS
36. [Wall LB, Didonna ML, Kiefhaber TR, Stern PJ. Proximal row carpectomy: minimum 20-year followup. J Hand Surg Am. 2013 Aug;38(8):1498-504. doi: 10.1016/j.jhsa.2013.04.028. Epub 2013 Jun 25. PubMed PMID: 23809467. ](http://www.ncbi.nlm.nih.gov/pubmed/23809467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23809467)
37. [Weiss KE, Rodner CM. Osteoarthritis of the wrist. J Hand Surg Am. 2007 May-Jun;32(5):725-46. Review. PubMed PMID: 17482013. ](http://www.ncbi.nlm.nih.gov/pubmed/17482013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17482013)
CLINICAL SITUATION FOR QUESTIONS 27 THROUGH 30
A 25-year-old teacher has a traumatic fracture-dislocation of the ring finger proximal interphalangeal (PIP) joint. During surgical exploration, comminution of the palmar 60% of the middle phalanx is present, and the dorsal base of the middle phalanx is intact with healthy articular cartilage.
QUESTION 11 OF 50
An otherwise healthy man has Dupuytrenâs disease, which involves his small finger with 40° proximal interphalangeal joint involvement. The preferred surgery in this patient is:
1
Partial fasciectomy
2
Arthrodesis
3
Arthroplasty
4
Osteotomy
5
Fasciotomy with skin grafting
A partial fasciectomy is the preferred surgery in this situation. It is recommended that involved fascial cords be resected rather than performing prophylactic fasciectomies. C are must be taken to preserve the neurovascular bundles. Arthrodesis, arthroplasty, and osteotomies are salvage procedures meant for recurrent disease. Fasciotomy has been recommended for elderly patients
who cannot tolerate a long operation.
who cannot tolerate a long operation.
QUESTION 12 OF 50
A 13-year-old gymnast has had recurrent right elbow pain for the past year. She denies any history of trauma. Rest and anti-inflammatory drugs have failed to provide relief. Examination reveals no localized tenderness and only slight loss of both flexion and extension (10 degrees). What is the most likely diagnosis?
1
Recurrent valgus overload (medial collateral ligament sprain)
2
Posterior lateral rotatory instability
3
Biceps tendinitis
4
Medial epicondylitis
5
Osteochondritis of the capitellum
Osteochondritis of the capitellum is characterized by pain, swelling, and limited motion. Catching, clicking, and giving way also can occur. It commonly affects athletes who participate in competitive sports with high stresses, such as pitching or gymnastics.
REFERENCES: Krijnen MR, Lim L, Willems WJ: Arthoscopic treatment of osteochondritis dissecans of the capitellum: Report of 5 female athletes. Arthroscopy 2003;19:210-214.
Schenck RC, Goodnight JM: Osteochondritis dissecans. J Bone Joint Surg Am 1996;3:439-456.
REFERENCES: Krijnen MR, Lim L, Willems WJ: Arthoscopic treatment of osteochondritis dissecans of the capitellum: Report of 5 female athletes. Arthroscopy 2003;19:210-214.
Schenck RC, Goodnight JM: Osteochondritis dissecans. J Bone Joint Surg Am 1996;3:439-456.
QUESTION 13 OF 50
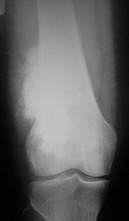
Figure 74 shows the radiograph of an 84-year-old woman who reports severe right knee pain. At the time of total knee arthroplasty, she is found to have gross insufficiency and attenuation of the medial collateral ligament (MCL) complex. Optimal management should consist of

1
primary repair of the MCL and use of a posterior stabilized total knee arthroplasty (TKA) prosthesis.
2
augmentation of the MCL with a collagenous tissue scaffold and use of a posterior stabilized TKA
prosthesis.
3
complete release of the lateral collateral ligament (LCL) and use of a posterior stabilized TKA prosthesis.
4
lateral unicompartmental arthroplasty.
5
use of a varus-valgus constrained TKA prosthesis.
DISCUSSION: Patients with severe valgus deformity may have near complete attenuation of the MCL. Attempts at ligament repair or reconstruction at the time of TKA can have unpredictable outcomes, leading to an unstable TKA. Although there may be a role for trying to reconstruct the ligament in conjunction with a nonconstrained implant in young patients with long life expectancies, in elderly patients a constrained prosthesis can provide varus-valgus stability with a predictable outcome. In younger patients, there is concern that the extra prosthetic constraint may shorten the longevity of the prosthetic fixation. In older patients, the constrained implant is likely to last a lifetime, with several studies documenting excellent survivorship (96%) at 10 years. Complete release of the LCL will leave the knee grossly unstable medially and laterally, and could necessitate a hinged prosthesis.
REFERENCES: Lachiewicz PF, Soileau ES: Ten-year survival and clinical results of constrained components in primary total knee arthroplasty. J Arthroplasty 2006;21:803-808.
Anderson JA, Baldini A, MacDonald JH, et al: Primary constrained condylar knee arthroplasty without stem extensions for the valgus knee. Clin Orthop Relat Res 2006;442:199-203.
Figure 75
QUESTION 14 OF 50
of 100
A 72-year-old man with diabetic neuropathy and 5 degrees of valgus talar tilt; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
A 72-year-old man with diabetic neuropathy and 5 degrees of valgus talar tilt; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
1
Ankle replacement
2
Ankle fusion
3
Tibiotalocalcaneal fusion
4
Total contact cast
5
Intra-articular steroid injection
Arthritis of the ankle and hindfoot can pose challenges. Depending upon patient age, comorbidities, and alignment, a variety of surgical interventions may be offered. A total ankle replacement may be considered for patients older than 60 years of age who have minimal misalignment and low-demand lifestyles. In all other cases, ankle fusion must be considered. The nonsurgical care of ankle arthritis includes anti-inflammatory medication, intra-articular steroid injections, bracing with customized products such as the Arizona brace, or a molded foot and ankle orthosis.
Patients with diabetes and Charcot arthropathy may be treated nonsurgically with total-contact casting during acute and active or "hot" phases and accommodative shoes during consolidation and stable or "cool" phases. When the patient has recurrent ulcers or major anatomy changes, surgical intervention must be considered. Tibiotalocalcaneal fusion helps to realign the foot and ankle and make it more braceable in the setting of ankle and hindfoot Charcot disease.
RECOMMENDED READINGS
Patients with diabetes and Charcot arthropathy may be treated nonsurgically with total-contact casting during acute and active or "hot" phases and accommodative shoes during consolidation and stable or "cool" phases. When the patient has recurrent ulcers or major anatomy changes, surgical intervention must be considered. Tibiotalocalcaneal fusion helps to realign the foot and ankle and make it more braceable in the setting of ankle and hindfoot Charcot disease.
RECOMMENDED READINGS
QUESTION 15 OF 50
Figures 21a and 21b show the clinical photograph and radiograph of a 15-year-old girl who has a deformity of her feet. Her parents are concerned because there is a family history of Charcot-Marie-Tooth disease. The patient reports some mild instability of the ankle and has noticed mild early callosities; however, she is not having any significant pain. Coleman block testing reveals a forefoot valgus and supple hindfoot. She has weakness to eversion and dorsiflexion. Initial management should consist of
1
dorsiflexion osteotomy of the first metatarsal with peroneus longus to brevis transfer.
2
plantar fasciotomy with dorsiflexion osteotomy of the first metatarsal and calcaneal osteotomy.
3
a stretching and strengthening physical therapy program and accommodative inserts.
4
observation.
5
calcaneal osteotomy, dorsiflexion osteotomy of the first metatarsal, peroneus longus to brevis transfer, plantar fascia release, Achilles tendon lengthening, and midfoot osteotomy.
Initial management of a young patient with a cavovarus deformity of the foot and a family history of Charcot-Marie-Tooth disease should focus on mobilization and strengthening of the weakening muscular units and an accommodative insert. Surgical intervention should be delayed until progression of the deformity begins to cause symptoms and/or weakness of the muscular units, resulting in contractures of the antagonistic muscle units.
REFERENCES: Pinzur MS: Charcot’s foot. Foot Ankle Clin 2000;5:897-912.
Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
REFERENCES: Pinzur MS: Charcot’s foot. Foot Ankle Clin 2000;5:897-912.
Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
QUESTION 16 OF 50
Sclerostin and dickkopf-1 (Dkk-1) are direct inhibitors of what pathway related to bone and/or cartilage regulation?
1
Bone morphogenetic protein (BMP)/SMAD pathway
2
Receptor activator of nuclear factor kappa beta (RANK)/RANK ligand (RANKL) pathway
3
Wnt/Beta-catenin (ß-catenin) pathway
4
Parathyroid hormone (PTH) pathway
#
**
Dkk-1 and sclerostin are proteins that inhibit the binding of the Wnt molecule to receptors LRP5/6. In the absence of sclerostin and Dkk-1, Wnt binds to its receptor, which in turn inhibits phosphorylation of the ß-catenin. The unphosphorylated ß-catenin then builds up in the cytoplasm of the cell, allowing it to be transported to the nucleus of the cell. Once in the nucleus, ß- catenin will lead to upregulation of a series of proteins involved in osteoblast formation differentiation. Knocking out or inhibiting sclerostin or Dkk-1 results in increased bone mass secondary to constitutive activation of the Wnt/ß- catenin pathway. The other responses are not directly affected by Dkk-1 or sclerostin. RANKL and RANK are expressed on osteoblasts and osteoclasts, respectively, and are involved in osteoblast-mediated osteoclast activation. BMPs work through SMADs to cause osteoblastic differentiation, and there is reported crosstalk between the Wnt and BMP pathways (but this is an indirect link). Finally, PTH at physiologic levels binds to osteoblasts, causing a series of events that lead to osteoblast-mediated osteoclast activation and subsequent increased bone resorption.
Dkk-1 and sclerostin are proteins that inhibit the binding of the Wnt molecule to receptors LRP5/6. In the absence of sclerostin and Dkk-1, Wnt binds to its receptor, which in turn inhibits phosphorylation of the ß-catenin. The unphosphorylated ß-catenin then builds up in the cytoplasm of the cell, allowing it to be transported to the nucleus of the cell. Once in the nucleus, ß- catenin will lead to upregulation of a series of proteins involved in osteoblast formation differentiation. Knocking out or inhibiting sclerostin or Dkk-1 results in increased bone mass secondary to constitutive activation of the Wnt/ß- catenin pathway. The other responses are not directly affected by Dkk-1 or sclerostin. RANKL and RANK are expressed on osteoblasts and osteoclasts, respectively, and are involved in osteoblast-mediated osteoclast activation. BMPs work through SMADs to cause osteoblastic differentiation, and there is reported crosstalk between the Wnt and BMP pathways (but this is an indirect link). Finally, PTH at physiologic levels binds to osteoblasts, causing a series of events that lead to osteoblast-mediated osteoclast activation and subsequent increased bone resorption.
QUESTION 17 OF 50
Figures 38a and 38b show the AP and lateral radiographs of a 12-year-old baseball pitcher who has pain in his right dominant elbow. Management should consist of
1
gentle range of motion and ultrasound.
2
cast immobilization and a bone stimulator.
3
elimination of offending activities and cross-training.
4
arthroscopy with excision of the pathologic portion.
5
MRI for assessment of accompanying ligamentous instability.
The patient has a stress fracture of the olecranon; therefore, the most appropriate management is modification of activities below the threshold of symptoms to allow for healing. Ultrasound provides no benefit, and immobilization is not necessary. MRI is not necessary because there is no associated ligamentous injury. Arthroscopy is not indicated.
REFERENCES: Cabanela ME, Morrey BF: Fractures of the olecranon, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 2000, pp 365-379.
Nuber GW, Diment MT: Olecranon stress fractures in throwers: A report of two cases and a review of the literature. Clin Orthop 1992;278:58-61.
REFERENCES: Cabanela ME, Morrey BF: Fractures of the olecranon, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 2000, pp 365-379.
Nuber GW, Diment MT: Olecranon stress fractures in throwers: A report of two cases and a review of the literature. Clin Orthop 1992;278:58-61.
QUESTION 18 OF 50
A hockey player had a puck hit his foot. Radiographs taken immediately after the game were negative. He still has persistent pain 5 days after the injury and difficulty weight bearing. What is the best next step?
1
Repeat radiographs
2
Full clearance to return to play
3
Bone scan
4
MRI scan
Ice hockey injuries demand a thorough assessment because they have the potential to be significant. In hockey players, bone injuries in the foot and ankle can be missed or improperly diagnosed through routine radiographic imaging. MRI can display bone injuries that are not found radiographically; this is because _some fractures and contusions involve the medial ankle and midfoot bones._
QUESTION 19 OF 50
1236) Which of the following structures is at risk during proximal dissection of a single lateral perifibular approach for compartment syndrome of the leg?
1
Common peroneal nerve
2
Superficial peroneal nerve
3
Deep peroneal nerve
4
Anterior tibial artery
5
Lateral inferior genicular artery
The perifibular approach is carried out through a straight lateral incision beginning just posterior and parallel to the fibula from the fibular head to the tip of the lateral malleolus. At the proximal end of the incision, the common peroneal nerve must be identified and protected. Elevation of the soleus off the posterior fibula ensures proper deep compartment release. The anterior edge of the incision is then retracted to expose the anterior and lateral compartments, and at this point, care must be taken to avoid the superficial
peroneal nerve as it exits the fascia of the lateral compartment and runs anteriorly in the distal third of the leg.
The referenced article by Whitesides is a review of compartment syndrome pathology, diagnosis, and treatment.
peroneal nerve as it exits the fascia of the lateral compartment and runs anteriorly in the distal third of the leg.
The referenced article by Whitesides is a review of compartment syndrome pathology, diagnosis, and treatment.
QUESTION 20 OF 50
A 12-year-old boy has multiple exostoses (osteochondromas). What is the most likely pattern of inheritance in this condition:
1
Autosomal recessive
2
Autosomal dominant
3
X-linked recessive
4
X-linked dominant
5
Almost always a spontaneous mutation
Multiple exostoses is transmitted in an autosomal dominant pattern. This condition is transmitted by both sexes with incomplete penetrance in females. This condition is more common in males.
QUESTION 21 OF 50
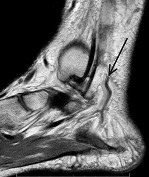
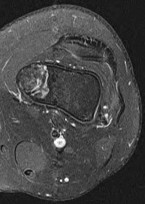
A sagittal MRI scan of the hindfoot and ankle is shown in Figure 86. The arrow points to what structure? ](http://www.orthobullets.com/anatomy/10122/blank)
1
Posterior tibial artery
2
Peroneal artery
3
Flexor hallucis longus
4
Posterior tibial nerve
5
Calcaneal artery
No detailed explanation provided for this question.
QUESTION 22 OF 50
of 100
Despite adequate medical management, the patient continues to experience leg pain that interferes with even the lowest demands of daily living. You recommend prophylactic intramedullary nailing of the tibia with interlocking screws. Prior to the surgery, you should recommend
Despite adequate medical management, the patient continues to experience leg pain that interferes with even the lowest demands of daily living. You recommend prophylactic intramedullary nailing of the tibia with interlocking screws. Prior to the surgery, you should recommend
1
an echocardiogram.
2
an endocrinology consultation.
3
a serum calcium level.
4
a repeat nuclear bone scan.
- an endocrinology consultation._
QUESTION 23 OF 50
Which of the following commercially available cements has the lowest tensile strength value:
1
Palacos-R (Biomet, Warsaw, IN)
2
Sulfix-60 (Sulzer, Austin, TX)
3
Simplex P (Stryker, Kalamazoo, MI)
4
CMW3 (Wright Medical Technology, Inc, Arlington, TN)
5
Zimmer Dough (Zimmer, Warsaw, IN)
Zimmer Dough has the lowest value of tensile strength; however, all of the above are FDA-approved cements and of sufficient quality
QUESTION 24 OF 50
A 34-year-old male has persistent anterolateral ankle pain after a snowboarding injury 1 week ago and is unable to bear weight. Three good quality radiographic views of the ankle are negative for fracture or other abnormalities. What is the next best step in management?
1
Short leg cast application
2
Bone scan
3
MRI of ankle
4
Diagnostic injection
5
Repeat radiographs
Fractures of the lateral process of the talus are frequently overlooked and should always be considered in the differential diagnosis of ankle pain in snowboarders. The common mechanism for fracture is dorsiflexion of the ankle and eversion of the hindfoot.
The reference by Vlahovich et al is a case report of a talus fracture in a snowboarder and argues the importance of CT scans in evaluating these injuries as radiographs may fail to show the injury and amount of displacement and comminution of the fracture.
The reference by Tucker et al is a review of the literature which emphasized the importance of early diagnosis to avoid long term complications. They recommend short leg casting for nondisplaced fractures and surgery for displaced or comminuted fractures.
The reference by Vlahovich et al is a case report of a talus fracture in a snowboarder and argues the importance of CT scans in evaluating these injuries as radiographs may fail to show the injury and amount of displacement and comminution of the fracture.
The reference by Tucker et al is a review of the literature which emphasized the importance of early diagnosis to avoid long term complications. They recommend short leg casting for nondisplaced fractures and surgery for displaced or comminuted fractures.
QUESTION 25 OF 50
When performing a total knee replacement, posterior stability can be achieved by all of the following except:
1
Soft tissue
2
The implant
3
Retention of posterior cruciate ligament
4
Resection of the posterior cruciate ligament
5
Resection of the anterior cruciate ligament
Posterior stability can be achieved through the soft tissues or the implant. The posterior cruciate ligament can be retained and posterior instability can still be achieved. The anterior cruciate ligament plays no role in posterior stability and is always resected during a total knee replacement
QUESTION 26 OF 50
The flap shown in the clinical photograph seen in Figure 51 is based on what
arterial supply?
arterial supply?
1
Superficial circumflex iliac
2
Femoral lateral accessory
3
Inferior epigastric
4
Inferior inguinal
5
Lateral obturator
The groin flap is based on the superficial circumflex iliac artery, an axial flap that has been a mainstay of providing soft-tissue coverage of the upper extremity. Flaps as large as 35 cm in length and 15 cm in width have been reported. An advantage of the flap is that when used as a pedicle flap, the donor site can be closed directly. A disadvantage of the flap is that it can be quite bulky and can have a thick layer of subcutaneous fat. The superficial circumflex iliac artery travels lateral and superficial to the fascia and below and parallel to the inguinal ligament. It is helpful to elevate the fascia at the medial border of the sartorius muscle to include the deep and superficial branches of the artery for improved flap survival.
REFERENCES: McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Lister GD, McGregor IA Jackson IT: The groin flap in hand injuries. Injury 1973;4:229.
REFERENCES: McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Lister GD, McGregor IA Jackson IT: The groin flap in hand injuries. Injury 1973;4:229.
QUESTION 27 OF 50
of 100
A
B
C
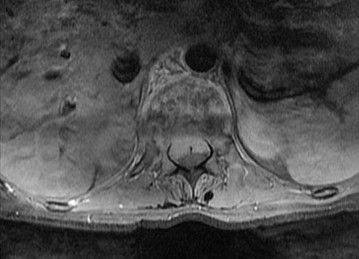
What is the appropriate first step when confirming the diagnosis of a neurologically intact, 73-year-old man who has the images shown in Figures 25a through 25c?




A
B
C
What is the appropriate first step when confirming the diagnosis of a neurologically intact, 73-year-old man who has the images shown in Figures 25a through 25c?
1
Order a prostate-specific antigen (PSA) level
2
Perform a 2-level corpectomy and reconstruction with tissue sent for pathologic analysis
3
Fine-needle aspiration
4
Bone scan
The radiograph and MR images show an osteoblastic lesion in the T9 and T8 vertebral bodies. In an older man, this finding most likely reveals metastatic prostate cancer. The first and least invasive diagnostic step is to order a PSA level. Gleave and associates found in a retrospective review of patients with prostate cancer that isolated levels of PSA lower than 10 to 20 micrograms per liter are rarely associated with bone metastasis. Vis and associates documented that 10-year prostate cancer survival in a screened population was higher than 60%, and in an unscreened population it was 24%. In a neurologically intact patient with no evidence of neural compression or instability, surgery is not indicated. Fine-needle aspiration may be performed, but the diagnostic yield in a blastic lesion is low. A bone scan may be indicated to complete the metastatic workup, but it will not aid in the diagnosis of tissue source.
RECOMMENDED READINGS
[Gleave ME, Coupland D, Drachenberg D, Cohen L, Kwong S, Goldenberg SL, Sullivan LD. Ability of serum prostate-specific antigen levels to predict normal bone scans in patients with newly diagnosed prostate cancer. Urology. 1996 May;47(5):708-12. PubMed PMID: 8650870. ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[View ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8650870)
[Vis AN, Roemeling S, Reedijk AM, Otto SJ, Schröder FH. Overall survival in the intervention arm of a randomized controlled screening trial for prostate cancer compared with a clinically diagnosed cohort. Eur Urol. 2008 Jan;53(1):91-8. Epub 2007 Jun 12. PubMed PMID: 17583416. ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17583416)
Cronen GA, Emery SE. Benign and malignant lesions of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:351-366.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
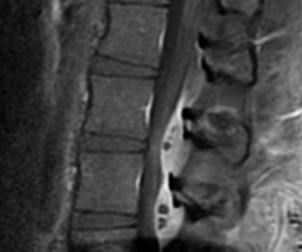
Figures 26a and 26b are the MR images with gadolinium enhancement of a 40-year-old man who arrives at the emergency department with a 4-day history of fevers and severe back pain without radiation. He is normotensive at presentation with a heart rate of 86 beats per minute. Upon examination he is neurologically intact with normal sensory and motor function. He has a history of alcohol and cocaine abuse. His white blood cell (WBC) count is 12000 (reference range [rr], 4500-11000 /µL) and his C-reactive protein (CRP) level is 100 mg/L (rr, 0.08-3.1 mg/L)
RECOMMENDED READINGS
[Gleave ME, Coupland D, Drachenberg D, Cohen L, Kwong S, Goldenberg SL, Sullivan LD. Ability of serum prostate-specific antigen levels to predict normal bone scans in patients with newly diagnosed prostate cancer. Urology. 1996 May;47(5):708-12. PubMed PMID: 8650870. ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[View ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8650870)
[Vis AN, Roemeling S, Reedijk AM, Otto SJ, Schröder FH. Overall survival in the intervention arm of a randomized controlled screening trial for prostate cancer compared with a clinically diagnosed cohort. Eur Urol. 2008 Jan;53(1):91-8. Epub 2007 Jun 12. PubMed PMID: 17583416. ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17583416)
Cronen GA, Emery SE. Benign and malignant lesions of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:351-366.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
Figures 26a and 26b are the MR images with gadolinium enhancement of a 40-year-old man who arrives at the emergency department with a 4-day history of fevers and severe back pain without radiation. He is normotensive at presentation with a heart rate of 86 beats per minute. Upon examination he is neurologically intact with normal sensory and motor function. He has a history of alcohol and cocaine abuse. His white blood cell (WBC) count is 12000 (reference range [rr], 4500-11000 /µL) and his C-reactive protein (CRP) level is 100 mg/L (rr, 0.08-3.1 mg/L)
QUESTION 28 OF 50
At which of the following distances can surgeons expect to have no radiation exposure from scatter from a fluoroscopy unit:
1
6 in
2
1 ft
3
2 ft
4
3 ft
5
6 ft
Radiation exposure decreases by a factor of 4 when a surgeon doubles the distance from the radiation beam. No radiation exists 6 ft from a fluoroscopy unit.Correct Answer: 6 ft
QUESTION 29 OF 50
of 100
Disruption of which anatomic structure is necessary for the second-toe pathology to occur?
Disruption of which anatomic structure is necessary for the second-toe pathology to occur?
1
Collateral ligaments
2
Intrinsic flexor tendons
3
Extrinsic extensor tendons
4
Plantar plate
- Plantar plate
QUESTION 30 OF 50
ORTHOPEDIC MCQS ONLINE 014 PATHOLOGY
..External beam radiotherapy

































































































..External beam radiotherapy
1
should include the instrumented femur and periacetabular area.
2
should include the femur only.
3
should include the acetabulum only.
4
is contraindicated for this patient.
..: 3- CT scan of the chest, abdomen, and pelvis. PREFERRED RESPONSE2…: 1- Metastatic adenocarcinoma
…: 4- Complex total hip arthroplasty
PREFERRED RESPONSE4 …: 1- should include the instrumented femur and periacetabular area.
..Li-Fraumeni syndrome (LFS) is associated with
1) multiple hemangiomas.
2) multiple hereditary osteochondromatosis.
3) soft-tissue sarcomas.
4) neurofibromatosis.
- soft-tissue sarcomas.
..A 60-year-old woman has a proximal femur fracture. A permeative, lytic defect is recognized at the fracture site. Appropriate imaging studies are performed and show no other lesions. What is the next treatment step?
1) Cephalomedullary nail
2) Standard antegrade intramedullary nail
3) Resection and arthroplasty reconstruction
4) Open biopsy
- Open biopsy
CLINICAL SITUATION FOR QUESTIONS 7 THROUGH 9
…Based on the images and histopathology, how is this patient best treated?
1) Chemotherapy and external beam radiotherapy
2) Resection
3) Resection and chemotherapy
4) External beam radiation alone
…: 3- Chordoma PREFERRED RESPONSE14…: 2- Resection
…A 56-year-old podiatrist with a negative past medical history had anterior knee pain after an injury. His radiographs, CT scan, and T1-weighted sagittal and fat-saturated axial MR images are shown in Figures 15a through 15e, respectively. After arthroscopic partial medial menisectomy, the patient was turned to the prone position and an open posterior arthrotomy and excision was performed. Low-power and high-power hematoxylin and eosin stained histologic specimens are shown in Figures 15f and 15g, respectively. Based on the history, radiographs, CT scan, MRI scans, and histologic findings, what is the most likely diagnosis?
1) Localized pigmented villonodular synovitis (PVNS)
2) Biphasic synovial sarcoma
3) Nodular fasciitis
4) Synovial hemangioma
- Synovial hemangioma
CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 19
Figures 16a and 16b are the right femur radiographs of a 59-year-old man who has severe pain in his right distal thigh and knee with no significant trauma and an inability to bear weight. Blood tests demonstrate anemia, serum protein electrophoresis/urine protein electrophoresis findings are negative, and electrolyte levels are within defined limits.
..Approximately what percentage of the time does an unknown primary cancer get identified as part of a full metastatic work-up that includes radiographs; blood tests; a CT scan of the chest, abdomen and pelvis; whole-body bone scan; and biopsy of the metastatic focus?
1) 45%
2) 65%
3) 85%
4) 100%
..: 3- Biopsy of the fracture site
PREFERRED RESPONSE 18..: 3- Distal femoral resection with megaprosthesis PREFERRED RESPONSE 19..: 3- 85%...
CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 23
Figures 20a and 20b are the radiographs of an 83-year-old active, independent, and healthy woman who has experienced 2 months of right lower thigh and knee pain. Her pain increased progressively over the course of several weeks. While exiting a car she “bumped” her knee against the door, felt a “crack,” and developed excruciating pain. She could no longer ambulate and was brought to the hospital.
..What is the most likely site of metastatic disease in patients with this diagnosis?
1) Liver
2) Lungs
3) Brain
4) Kidneys
-: 4- Enchondroma
PREFERRED RESPONSE21-..: 4- Dedifferentiated chondrosarcomas
PREFERRED RESPONSE22-..: 3- Above-the-knee amputation with wide surgical margin PREFERRED RESPONSE23-..: 2- Lungs
..A 14-year-old boy has had wrist pain for 3 weeks. Radiographs are shown in Figures 24a and 24b. His MRI scans are shown in Figures 24c through 24f. Representative histology is shown in Figures 24g through 24i. The most likely diagnosis is
1) aneurysmal bone cyst.
2) fibrous dysplasia.
3) giant-cell tumor.
4) osteoblastoma.
- osteoblastoma.
RESPONSES FOR QUESTIONS 25 THROUGH 29
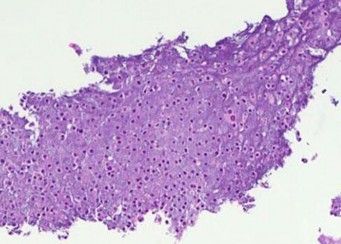
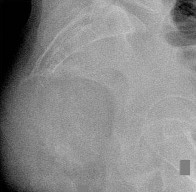
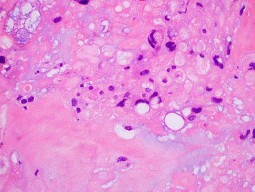
..Figure 30a is the radiograph taken in the emergency department of a 20-year-old man with pain and swelling in his right-dominant arm. His MRI scan is seen in Figure 30b, and his histopathology is shown in Figure 30c. What is the most likely diagnosis?
1) Ewing sarcoma
2) Langerhans cell histiocytosis
3) Osteosarcoma
4) Osteomyelitis
- Ewing sarcoma
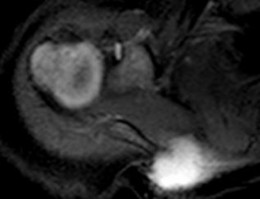
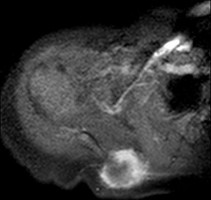
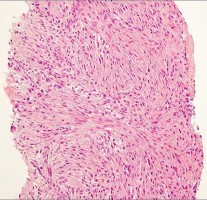
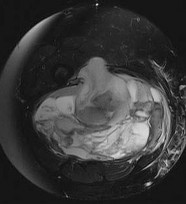
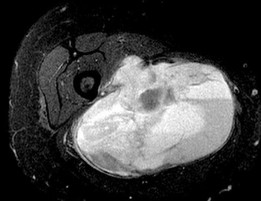
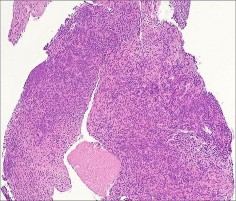
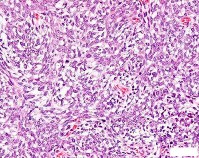
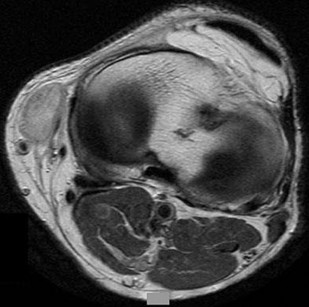
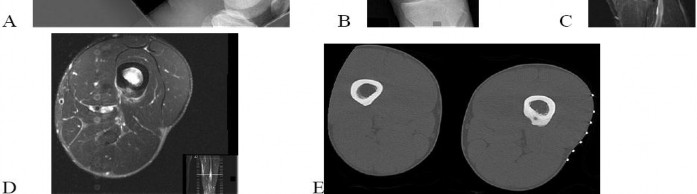
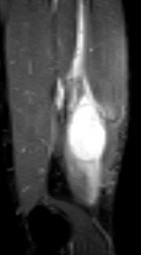
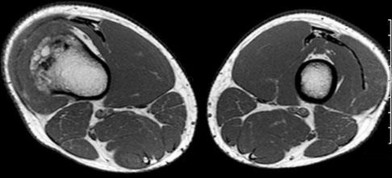
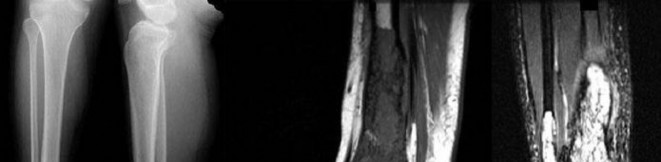
..An 18-year-old woman has had a right thigh mass for “a long time.” She has found it increasingly difficult to ambulate. Her medical history is unremarkable, with the exception of hypertension. On clinical examination, a fullness is appreciated in the popliteal fossa. The neurovascular status of the distal extremity is intact. Anteroposterior and lateral radiographs are shown in Figures 31a and 31b. A lateral T2-weighted MRI scan is shown in Figure 31c. The histology is seen in Figure 31d. What is the most likely diagnosis?
1) Aneurysmal bone cyst
2) Osteosarcoma
3) Periosteal lipoma
4) Parosteal osteosarcoma
- Osteosarcoma
CLINICAL SITUATION FOR QUESTIONS 32 THROUGH 36
A 68-year-old woman is referred for left thigh pain. Her medical history includes Hypertension, diabetes, and adenocarcinoma of the breast treated with surgery, chemotherapy, and radiation 3 years ago. She currently is on aromatase therapy. She is unable to ambulate secondary to pain, is limited to a walker, and requires narcotic medications. She has no other pain but agrees to your recommendation that she urgently be sent to the hospital.
..Which intervention should be added to this patient’s care to best prevent future skeletally related events (SRE)?
1) Inferior vena cava (IVC) filter placement
2) Bisphosphonates
3) External beam radiation
4) Tc-99 whole-body bone scan at regular intervals
…: 3- Further imaging PREFERRED RESPONSE 33-..: 3- Location of the lesion PREFERRED RESPONSE 34-…: 2- 15%
PREFERRED RESPONSE 35…..:4- Lung carcinoma, breast carcinoma, multiple myeloma PREFERRED RESPONSE 36-…: 2- Bisphosphonates
..Figures 37a and 37b are the lateral and anteroposterior (AP) radiographs of a 60-year-old man with a remote history of renal cell cancer. A needle biopsy of the lesion is shown in Figure 37c. The bone destruction that occurs in this process is a result of
1) tumor cells.
2) cytokines secreted by the tumor.
3) host bone osteoblasts.
4) osteoprotegerin.
.
- cytokines secreted by the tumor
..Figures 38a and 38b are the histopathology of an otherwise healthy 31-year-old man who had a growing mass excised from his forearm with local anesthetic and no preoperative imaging. The mass was documented to be subfascial and larger than 5 cm.
What is the best local treatment option?
1) Observation
2) Radiation only
3) Chemotherapy only
4) Re-excision and radiation
- Re-excision and radiation
…Figure 39a is the anteroposterior radiograph of a 51-year-old man who has had a painless soft-tissue mass on his left wrist for 2 months. MR sequences are shown in Figures 39b through 39d. A biopsy was performed and shown in a low-power hematoxylin and eosin photomicrograph in Figure 39e. The most appropriate treatment for this lesion is
1) a diet that reduces uric acid production.
2) wide local resection followed by radiotherapy.
3) marginal excision.
4) observation until the mineralization matures, and then excision and radiotherapy to prevent recurrence.
- marginal excision.
CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 43
Figures 40a through 40c are the radiograph, bone scan, and histology of a 68-year-old man who has had 3 months of pain in his left thigh with weight bearing. He has no history of cancer and no illnesses.
..The orthopaedic surgeon obtains tissue with the histology shown in Figure 40c. Treatment should consist of
1) surgical stabilization.
2) surgical stabilization and radiation.
3) excision and endoprosthesis.
4) radiation.
- …..: 1- malignant.
PREFERRED RESPONSE 41..,,,,,,,: 1- CT scan of the chest, abdomen and pelvis. PREFERRED RESPONSE 42………: 2- biopsy.
PREFERRED RESPONSE 43……….: 2- surgical stabilization and radiation.
..First-line treatment recommendations include
1) synovectomy.
2) arthrocentesis, compressive wrap, and rest.
3) en bloc resection.
4) intra-articular radioactive nucleotide injection.
- pigmented villonodular synovitis (PVNS). PREFERRED RESPONSE: 1- synovectomy.
RESPONSES FOR QUESTIONS 47 THROUGH 52
…Figure 53 is the emergency department radiograph of a 7-year-old boy who has pain and is unwilling to use his right arm after a fall on the playground. What is the most appropriate initial treatment?
1) Nonsurgical treatment of the fracture
2) Aspiration and injection with methylprednisolone
3) Curettage and augmentation with bone cement and internal fixation
4) Further imaging and biopsy
- Nonsurgical treatment of the fracture
..Figure 54 is the CT scan of a 70-year-old man with progressive neck pain; there is no history of trauma, and examination is notable only for mildly decreased cervical range of motion. He is neurologically intact. He has monoclonal gammopathy of undetermined significance that has been stable for many years. Current serum protein electrophoresis is unchanged. History and examination reveal no other causes for his pain. What is the next step in clinical management?
1) Corpectomy and anterior fusion
2) Radiation therapy followed by multiple myeloma protocol chemotherapy
3) CT-guided biopsy
4) CT scan of the chest, abdomen, and pelvis
- CT scan of the chest, abdomen, and pelvis
…A 27-year-old incarcerated man was found to have a fungating mass on his anterolateral right proximal thigh. A clinical photograph is shown in Figure 55a. T1- and T2-weighted coronal MRI scans are shown in Figures 55b and 55c. The hematoxylin and eosin and CD34 stained histology are shown in Figures 55d and 55e. What is the most likely diagnosis?
1) Squamous cell carcinoma
2) Melanoma
3) Dermatofibrosarcoma protuberans (DFSP)
4) Desmoid tumor
- Dermatofibrosarcoma protuberans (DFSP)
..Figures 56a and 56b are the axial short tau inversion recovery and T1 with contrast images of a 7-month-old infant who is found to have a right scapular soft-tissue mass. On examination, the mass is hard. A biopsy was performed and is shown in Figure 56c (hematoxylin and eosin, 400x). What is the optimal treatment for this patient?
1) Intralesional excision 2- Marginal excision
2) Wide excision 4- Observation
- Wide excision
…Figures 57a through 57d show the radiographs and T1- and T2-weighted MRI scan sequences of the proximal femur of a 60-year-old man with progressive thigh pain. A review of radiographs taken 3 years ago reveals that the lesion is new. The biopsy specimen is shown in Figure 57e; staging studies show no other lesions, and local imaging confirms the process is confined to bone (no soft-tissue mass). The next treatment step should include
1) hip disarticulation.
2) radiotherapy.
3) ifosfamide-based chemotherapy.
4) wide resection and reconstruction.
- wide resection and reconstruction.
…The characteristic translocation and genes involved in extraskeletal myxoid chondrosarcoma is
1) t(11;12) EWS;FLI1
2) t(12;16) TLS;CHOP.
3) t(9;22)EWS;CHN.
4) t(9;22) BCR-ABL.
.
- t(9;22) EWS;CHN
.Figures 59a and 59b are the axial T2 and T1 with contrast MRI scans of a 32-year-old woman who has a 10-year history of pain and a 1-year history of progressive swelling in her right leg. The histopathology is shown in Figure 59c. A radiograph of her leg showed no mineralizations or osseous erosions. The chromosomal abnormality that is associated with this disease is
1) t(11;22).
2) t(2;13).
3) t(X;18).
4) t(12;16).
- t(X;18).
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
A 45-year-old woman has an enlarging buttock mass. The mass is 12 cm and nonpainful. The patient first noticed it about 6 months after she had a low-impact fall. The general surgeon evaluating the patient felt this mass could be either a lipoma or a hematoma. The patient underwent a surgical procedure to remove the mass.
..What is the most common detrimental impact of an unplanned excision of a high-grade soft-tissue sarcoma?
1) Decreased mortality
2) Decreased recurrence
3) Increased wound complications
4) Increased functional outcome
-,…: 2- Imaging studies (MRI scan or CT scan) PREFERRED RESPONSE 61….: 1- Meticulous hemostasis and closure PREFERRED RESPONSE 62…..: 3- No imaging was obtained before surgery. PREFERRED RESPONSE 63…..: 3- Increased wound complications
CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 66
Figures 64a through 64c are the radiograph, MRI scan, and histology of a 53-year-old man with medial knee pain and swelling below the knee.
..Histology of the lesion is shown in Figure 64c. The best next treatment step is
1) radiation.
2) radiation and surgery.
3) chemotherapy.
4) observation.
- Translocation x;18 PREFERRED RESPONSE: 4- Biopsy
PREFERRED RESPONSE: 2- radiation and surgery.
..A 26-year-old woman has had a slow-growing and painful mass at the base of her ring finger for several months. Radiographs of the affected digit show no mineralization or erosions of the underlying bone. An axial T1 MRI scan is shown in Figure 67a, and a corresponding short tau inversion recovery image is shown in Figure 67b. A coronal T1 MRI scan with contrast is shown in Figure 67c. The best next treatment step is
1) referral to a sarcoma center.
2) observation.
3) excisional biopsy.
4) marginal excision.
- referral to a sarcoma center.
..What is the most specific immunohistochemistry staining pattern that confirms the diagnosis of desmoid tumor?
1) Membranous beta-catenin staining
2) Nuclear beta-catenin staining
3) Nuclear SMAD4 staining
4) Vimentin positivity
- Nuclear beta-catenin staining
…A 30-year-old woman has progressive gait instability, back pain, and urinary retention. Figures 69a and 69b show the axial T2 and postcontrast MRI scans taken at the level of T11, and Figure 69c shows the sagittal T1-weighted image. Representative histology is shown in Figure 69d. The patient remains ambulatory, but symptoms have
progressed during the last week and she is beginning to feel weakness in her legs. Examination is notable for decreased rectal tone, lower-extremity hyperreflexia and clonus, and 4/5 motor strength throughout the lower extremities. What is the most appropriate treatment recommendation for this patient?
1) Margin-free en bloc spondylectomy of T11
2) Radiation therapy
3) Radiation therapy followed by anterior corpectomy and fusion
4) Transpedicular decompression and posterior stabilization followed by radiation therapy
- Transpedicular decompression and posterior stabilization followed by radiation therapy
…Giant-cell tumor of bone usually involves the epiphysis of long bones. What is the next most common type of tumor involving this anatomical location?
1) Conventional chondrosarcoma
2) Aneurysmal bone cyst
3) Chondroblastoma
4) Osteoblastoma
- Chondroblastoma
CLINICAL SITUATION FOR QUESTIONS 71 THROUGH 73
Figures 71a through 71e are the radiographs, MRI scan, and CT scans of a 14-year-old-boy who has cyclical pain in his thigh. His symptoms began approximately 6 months ago. He complains of increased pain when he runs and also of pain that wakes him at night. This pain is relieved by nonsteroidal anti-inflammatory drugs (NSAIDs).
…What is the etiology of the pain associated with this lesion?
1) Prostaglandin production
2) Gram-positive cocci
3) Osteoclast activation
4) Loss of structural integrity of the bone
- Osteoid osteoma PREFERRED RESPONSE: 2- radiofrequency ablation. PREFERRED RESPONSE: 1- Prostaglandin production
...Figure 74 is the radiograph of an 11-year-old boy with pain in his left arm. Prognosis is most influenced by
1) stage at presentation.
2) grade at presentation.
3) response to neoadjuvant chemotherapy.
4) histologic subtype.
- stage at presentation.
..Figures 75a through 75d are the radiograph, CT scan, bone scan, and biopsy of a 45-year-old man who has had a several-month history of progressive pain in his right hip and groin region. Based on these images and histology, what is the most appropriate treatment?
1) Wide resection
2) Curetting and bone grafting
3) Percutaneous cementation and radiotherapy
4) Chemotherapy and radiotherapy
- Wide resection
..Figure 76 is the radiograph of a 77-year-old patient with a history of myeloma who has had severe arm pain after opening a jar. Pain was present for 3 months prior to injury. The most biomechanically stable construct for this fracture is
1) intramedullary nailing (IMN).
2) IMN and cement.
3) plate.
4) plate and cement.
- plate and cement.
CLINICAL SITUATION FOR QUESTIONS 77 THROUGH 79
Figures 77a through 77c are the radiograph and MRI scans of a 45-year-old woman who enjoys dancing and has had left ankle pain for approximately 1 month with minimal trauma. She has slightly limited ankle dorsiflexion with a mechanical block with pain.
..The patient undergoes recommended surgery and minimal joint damage is found. How should she be counseled regarding her future prognosis?
1) High risk for local recurrence, moderate risk for metastases
2) High risk for local recurrence, no risk for metastases
3) Low risk for local recurrence, moderate risk for metastases
4) Low risk for local recurrence, no risk for metastases
- Synovial metaplasia
PREFERRED RESPONSE: 2- TA, EHL, anterior tibial artery, deep peroneal nerve, EDL PREFERRED RESPONSE: 4- Low risk for local recurrence, no risk for metastases
..Figures 80a through 80d are the radiographs and MRI scans of a 16-year-old girl who requires crutches because she is unable to bear weight on her right lower extremity. The pain has progressed over 2 months despite nonsurgical treatment.
Treatment at this point should include
1) continued observation.
2) aspiration and injection with methylprednisolone.
3) curettage and grafting.
4) wide margin resection.
- curettage and grafting.
..A previously healthy 60-year-old woman has a T5 pathologic compression fracture secondary to metastatic renal cell carcinoma. She has myelopathy with severe pain upon sitting from a supine position. The adjacent thoracic levels are unaffected. On MRI scan, there is minimal space available for the cord because of epidural involvement. What is the optimal treatment method at this time?
1) Surgical decompression and instrumented fusion
2) Surgical decompression without fusion
3) Image-guided intensity-modulated radiation therapy
4) Chemotherapy
- Surgical decompression and instrumented fusion
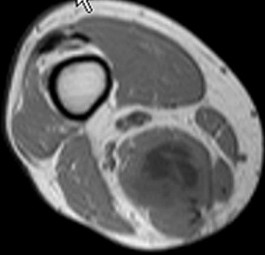
..Figures 82a and 82b are the MRI scans consisting of a T2 coronal sequence and axial T1 pulse sequence of a 38-year-old man who has had right thigh pain and a mass for 4 months since he pulled his hamstring. The presumed diagnosis considering his clinical history and evaluation of the MRI scan was hematoma and the mass was evacuated. The histology is shown in Figures 82c and 82d. Next treatment steps should include
1) physical therapy to accelerate healing and improve function.
2) a complete hematologic work-up to evaluate a bleeding disorder.
3) tumor bed excision and radiation to reduce local recurrence.
4) radiotherapy to complete definitive treatment of this problem.
- tumor bed excision and radiation to reduce local recurrence.
….Figures 83a through 83c are the radiograph and MRI scans of a 16-year-old girl who had posterior knee pain after a dance recital 3 weeks ago; the pain resolved 1 week ago with ibuprofen use. What is the appropriate treatment for this patient?
1) Biopsy and resection of lesion
2) Observation and serial radiographs
3) Tc-99 whole-body bone scan and fine-cut CT scan
4) Evaluation by a pediatric oncologist
- Observation and serial radiographs
CLINICAL SITUATION FOR QUESTIONS 84 THROUGH 86
Figures 84a and 84b are the CT and MRI scans of a 17-year-old girl with a painful lumbosacral scoliosis that has been present for 12 months. Examination is notable only for pain over the left sacral region and a postural scoliosis leaning away from this side.
..With treatment, the spinal deformity is expected to
1) spontaneously resolve.
2) remain stable and nonprogressive.
3) respond in proportion to the family’s compliance with brace treatment.
4) resolve in the coronal plane and progress in the sagittal plane.
- is likely to respond to percutaneous intervention.
PREFERRED RESPONSE: 1- uses nonsteroidal anti-inflammatory or aspirin medications. PREFERRED RESPONSE: 1- spontaneously resolve.
..Figures 87a through 87e are the radiograph, MRI scans, and biopsy specimen of an 83-year-old woman who is experiencing pain in her distal thigh with activity and at night. She has undergone total hip arthroplasty for hip osteoarthritis. The most appropriate treatment is
1) external beam radiation.
2) curetting and cementation.
3) radiofrequency ablation.
4) wide local resection.
- wide local resection.
CLINICAL SITUATION FOR QUESTIONS 88 through 92
Figures 88a and 88b are the radiographs of a 70-year-old woman with a remote history of localized renal cell carcinoma. She has insidious onset of right shoulder pain that worsens with any activity and at night. She appears otherwise healthy.
..Oncologic outcome for this patient
1) is influenced by extraosseous tumor extension.
2) is more favorable if the lesion is solitary.
3) involves a predictable rapid demise.
4) hinges on the presence or absence of gene amplification.
- CT scan of the chest, abdomen, and pelvis.
PREFERRED RES: 3- Should be performed if the lesion is solitary, but not necessarily if multifocal PREFERRED RESPONSE: 4- resection and reconstruction.
PREFERRED RESPONSE: 3- inhibits vascular endothelial growth factor (VEGF) pathways. PREFERRED RESPONSE: 2- is more favorable if the lesion is solitary.
..Figures 93a and 93b are the MRI scans of a 24-year-old man with painless, persistent swelling in his left knee without any trauma. What is the best next treatment step?
1) Arthroscopic anterior synovectomy and posterior open resection
2) Arthroscopic anterior synovectomy only
3) Radiation therapy and wide excision
4) Observation
- Arthroscopic anterior synovectomy and posterior open resection
..What biopsy technique for a posterior thigh sarcoma is associated with the highest risk for adverse outcome?
1) Transverse incision open biopsy
2) Core needle biopsy
3) Fine-needle aspirate
4) Longitudinal incision open biopsy
- Transverse incision open biopsy
..A 60-year-old woman with a history of breast cancer has a rapidly enlarging arm mass. The lesion is situated outside of the prior irradiation field, but within an area of heavy lymphedema involvement. Needle biopsy reveals a high-grade sarcoma. What is the most likely diagnosis?
1) Lymphangiosarcoma
2) Acral myxoinflammatory fibroblastic sarcoma
3) Hemangioendothelioma
4) Hemangiopericytoma
- Lymphangiosarcoma
RESPONSES FOR QUESTIONS 96 THROUGH 100
..Figures 106a and 106b are the T1 sagittal and T2 coronal images of a 41-year-old woman who has been experiencing electric shock-type radiating pain over her right ankle for 4½ years. Her biopsy specimen is shown in Figure 106c. What is the best next treatment step?
1) Marginal excision
2) Wide excision
3) Wide excision and radiation
4) Observation
- Marginal excision
..Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man. While walking, he collapsed and was unable to ambulate because of pain and deformity in his right leg. What is the most appropriate next step?
1) Staging studies to assess the extent of disease
2) Immediate stabilization of the fracture with an intramedullary nail
3) Curetting and bone culture
4) Segmental resection of the tibia and allograft reconstruction
- Staging studies to assess the extent of disease
RESPONSES FOR QUESTIONS 108 THROUGH 111
..Figures 112a and 112b are the anteroposterior and lateral radiographs of a 65-year-old man who has a significant history of tobacco abuse and a 6-week history of right thigh pain. Axial and sagittal MRI scans are seen in Figures 112c and 112d. His MR angiogram is shown in Figure 112e. A biopsy of a lesion is shown in Figure 112f. What is the most likely diagnosis?
1) Secondary sarcoma in a pre-existing condition
2) Angiosarcoma
3) Metastatic lung carcinoma
4) Fibrous dysplasia
- Secondary sarcoma in a pre-existing condition
CLINICAL SITUATION FOR QUESTIONS 113 THROUGH 116
Figures 113a and 113b are the radiographs of a 68-year-old-man who has increasing pain in his left groin with weight-bearing activities and a Trendelenburg gait. Radiographs reveal a lytic lesion of the greater trochanter. An initial diagnosis of adenocarcinoma of the lung was made 1 year before this presentation. His lung cancer treatment consisted of partial lobectomy and postsurgical radiation therapy.
..Staging studies show no other lesions and surgical treatment is planned; when should a biopsy be performed?
1) Before surgery
2) Intraoperatively after instrumentation
3) After surgery (reamings/curettings sent)
4) No biopsy is needed
- Positron emission tomography (PET) scan PREFERRED RESPONSE: 3- Curettage, cementation, and internal fixation PREFERRED RESPONSE: 4- resection and prosthetic reconstruction.
PREFERRED RESPONSE: 1- Before surgery
CLINICAL SITUATION FOR QUESTIONS 117 THROUGH 120
Figures 117a through 117c are the radiographs and MRI scan of a 16-year-old boy who has had a persistent fullness in his thigh since being kicked while playing soccer 4 weeks ago. He states that initially the area was painful, but now all symptoms other than the mass have resolved.
Findings of multiple lesions in multiple skeletal sites may be associated with
1) decreased risk for malignancy.
2) a characteristic chromosomal translocation.
3) soft-tissue hemangiomas.
4) limb deformity and short stature.
- Osteochondroma
PREFERRED RESPONSE: 1- benign and simply can be observed with serial radiographs. PREFERRED RESPONSE: 4- growth beyond skeletal maturity.
PREFERRED RESPONSE: 4- limb deformity and short stature.
..Figure 121a is the axial T1 MRI scan and Figure 121b is the coronal T1 MRI scan of an 85-year-old man who has a mass in his medial thigh. The mass was present for years and recently grew. His biopsy specimen is shown in Figure 121c. What is the best treatment for this patient?
1) Chemotherapy and wide local resection
2) Wide local resection and radiotherapy
3) Marginal excision
4) Observation and reimaging in 6 months
- Wide local resection and radiotherapy
..What tumor commonly metastasizes to regional lymph nodes?
1) Fibromyxoid sarcoma
2) Epithelioid sarcoma
3) Leiomyosarcoma
4) Liposarcoma
- Epithelioid sarcoma
..A 64-year-old woman has significant right arm pain associated with a destructive proximal humeral bone lesion with an associated soft-tissue mass. Her medical history includes carcinoma of the breast treated 8 years ago with modified radical mastectomy, hormone receptor-based chemotherapy, and 45 Gy of radiation with 8 subsequent disease-free years. Biopsy reveals a high-grade osteogenic sarcoma. What factor is most likely related to her current disease?
1) Presence of metastatic disease
2) Dosage of radiation treatment
3) Type of prior surgical procedure
4) Type of chemotherapy given
- Dosage of radiation treatment
..Figures 124a and 124b are the MRI scans of a 25-year-old woman who has a painful mass in her left gluteal and thigh region. Her biopsy specimen is seen in Figure 124c. What is the most likely diagnosis?
1) Desmoid fibromatosis
2) Extraskeletal Ewing sarcoma
3) Metastatic breast cancer
4) Lymphoma
- Desmoid fibromatosis
CLINICAL SITUATION FOR QUESTIONS 125 THROUGH 128
A 45-year-old woman has increasing knee pain with activity and at rest. Her radiograph, MRI scan, and histology are shown in Figures 125a through 125c.
..The cell that directly causes osteolysis in this lesion is
1) giant cell.
2) stromal cell.
3) osteoblast.
4) fibroblast.
- benign aggressive. PREFERRED RESPONSE: 4- chest radiograph.
PREFERRED RESPONSE: 1- extended intralesional curettage. PREFERRED RESPONSE: 1- giant cell.
..Figures 129a through 129c are the lateral radiograph of the sacrum, axial CT scan, and a high-power view of a fine-needle biopsy of a 47-year-old man who has buttock pain and constipation. A large mass is palpable on rectal examination. The tumor cell that is the signature of this tumor is known as a(n)
1) giant cell.
2) physaliferous cell.
3) chondroblast.
4) adipocyte.
- physaliferous cell.
..Figures 130a through 130c show the CT scan and T1- and T2-weighted MRI scan sequences of an otherwise healthy 67-year-old woman with progressive left groin pain. Her biopsy specimen is shown in Figure 130d. Staging studies reveal no other lesions. Treatment should include
1) radiotherapy.
2) chemotherapy followed by surgical resection.
3) curettage with adjuvant treatment and grafting.
4) en bloc resection.
- en bloc resection.
..A lateral radiograph (Figure 131a), sagittal short tau inversion recovery MRI scan (Figure 131b), and an axial T1 contrast MRI scan (Figure 131c) were performed on a 15-year-old boy who has injured his right knee twice during the last 5 months. He has a reduced range of motion of the knee and posterior thigh tenderness. A biopsy showed bland spindle cells, giant cells, and blood-filled spaces without endothelial lining. What is the most appropriate treatment?
1) Chemotherapy and wide local excision
2) Chemotherapy and radiotherapy
3) Marginal excision
4) Extended intralesional curettage
- Extended intralesional curettage
CLINICAL SITUATION FOR QUESTIONS 132 THROUGH 134
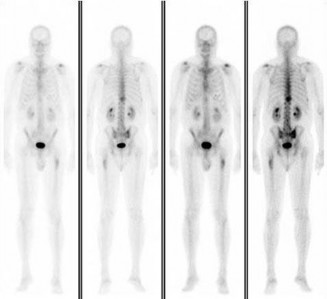
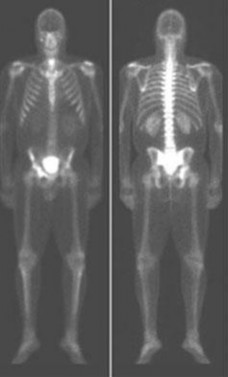
Figure 132 is the bone scan of a 73-year-old man who is referred from his family doctor with diffuse bone pain, fatigue, and right knee pain. Examination is notable for pain with motion about the right knee and mild hyporeflexia.
..Further imaging shows pulmonary metastases without an obvious primary tumor of origin and an incomplete fracture of the right distal femur. A decision is made to surgically treat his distal femur fracture. What is the role of establishing a preoperative histologic diagnosis for this patient?
1) The distal femoral lesion should undergo needle biopsy first.
2) Bone marrow biopsy should be done first.
3) Preoperative biopsy is not necessary because a metastatic process is present.
4) Biopsy is not necessary if the lesion demonstrates a standardized uptake value (SUV) greater than 3 on fluorodeoxyglucose positron emission tomography (PET) imaging.
.
- CT scan of the chest, abdomen, and pelvis and laboratory studies. PREFERRED RESPONSE: 3- intravenous bisphosphonate treatment.
PREFERRED RESPONSE: 3- Preoperative biopsy is not necessary because a metastatic process is present
…: 4- Complex total hip arthroplasty
PREFERRED RESPONSE4 …: 1- should include the instrumented femur and periacetabular area.
..Li-Fraumeni syndrome (LFS) is associated with
1) multiple hemangiomas.
2) multiple hereditary osteochondromatosis.
3) soft-tissue sarcomas.
4) neurofibromatosis.
- soft-tissue sarcomas.
..A 60-year-old woman has a proximal femur fracture. A permeative, lytic defect is recognized at the fracture site. Appropriate imaging studies are performed and show no other lesions. What is the next treatment step?
1) Cephalomedullary nail
2) Standard antegrade intramedullary nail
3) Resection and arthroplasty reconstruction
4) Open biopsy
- Open biopsy
CLINICAL SITUATION FOR QUESTIONS 7 THROUGH 9
…Based on the images and histopathology, how is this patient best treated?
1) Chemotherapy and external beam radiotherapy
2) Resection
3) Resection and chemotherapy
4) External beam radiation alone
…: 3- Chordoma PREFERRED RESPONSE14…: 2- Resection
…A 56-year-old podiatrist with a negative past medical history had anterior knee pain after an injury. His radiographs, CT scan, and T1-weighted sagittal and fat-saturated axial MR images are shown in Figures 15a through 15e, respectively. After arthroscopic partial medial menisectomy, the patient was turned to the prone position and an open posterior arthrotomy and excision was performed. Low-power and high-power hematoxylin and eosin stained histologic specimens are shown in Figures 15f and 15g, respectively. Based on the history, radiographs, CT scan, MRI scans, and histologic findings, what is the most likely diagnosis?
1) Localized pigmented villonodular synovitis (PVNS)
2) Biphasic synovial sarcoma
3) Nodular fasciitis
4) Synovial hemangioma
- Synovial hemangioma
CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 19
Figures 16a and 16b are the right femur radiographs of a 59-year-old man who has severe pain in his right distal thigh and knee with no significant trauma and an inability to bear weight. Blood tests demonstrate anemia, serum protein electrophoresis/urine protein electrophoresis findings are negative, and electrolyte levels are within defined limits.
..Approximately what percentage of the time does an unknown primary cancer get identified as part of a full metastatic work-up that includes radiographs; blood tests; a CT scan of the chest, abdomen and pelvis; whole-body bone scan; and biopsy of the metastatic focus?
1) 45%
2) 65%
3) 85%
4) 100%
..: 3- Biopsy of the fracture site
PREFERRED RESPONSE 18..: 3- Distal femoral resection with megaprosthesis PREFERRED RESPONSE 19..: 3- 85%...
CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 23
Figures 20a and 20b are the radiographs of an 83-year-old active, independent, and healthy woman who has experienced 2 months of right lower thigh and knee pain. Her pain increased progressively over the course of several weeks. While exiting a car she “bumped” her knee against the door, felt a “crack,” and developed excruciating pain. She could no longer ambulate and was brought to the hospital.
..What is the most likely site of metastatic disease in patients with this diagnosis?
1) Liver
2) Lungs
3) Brain
4) Kidneys
-: 4- Enchondroma
PREFERRED RESPONSE21-..: 4- Dedifferentiated chondrosarcomas
PREFERRED RESPONSE22-..: 3- Above-the-knee amputation with wide surgical margin PREFERRED RESPONSE23-..: 2- Lungs
..A 14-year-old boy has had wrist pain for 3 weeks. Radiographs are shown in Figures 24a and 24b. His MRI scans are shown in Figures 24c through 24f. Representative histology is shown in Figures 24g through 24i. The most likely diagnosis is
1) aneurysmal bone cyst.
2) fibrous dysplasia.
3) giant-cell tumor.
4) osteoblastoma.
- osteoblastoma.
RESPONSES FOR QUESTIONS 25 THROUGH 29
..Figure 30a is the radiograph taken in the emergency department of a 20-year-old man with pain and swelling in his right-dominant arm. His MRI scan is seen in Figure 30b, and his histopathology is shown in Figure 30c. What is the most likely diagnosis?
1) Ewing sarcoma
2) Langerhans cell histiocytosis
3) Osteosarcoma
4) Osteomyelitis
- Ewing sarcoma
..An 18-year-old woman has had a right thigh mass for “a long time.” She has found it increasingly difficult to ambulate. Her medical history is unremarkable, with the exception of hypertension. On clinical examination, a fullness is appreciated in the popliteal fossa. The neurovascular status of the distal extremity is intact. Anteroposterior and lateral radiographs are shown in Figures 31a and 31b. A lateral T2-weighted MRI scan is shown in Figure 31c. The histology is seen in Figure 31d. What is the most likely diagnosis?
1) Aneurysmal bone cyst
2) Osteosarcoma
3) Periosteal lipoma
4) Parosteal osteosarcoma
- Osteosarcoma
CLINICAL SITUATION FOR QUESTIONS 32 THROUGH 36
A 68-year-old woman is referred for left thigh pain. Her medical history includes Hypertension, diabetes, and adenocarcinoma of the breast treated with surgery, chemotherapy, and radiation 3 years ago. She currently is on aromatase therapy. She is unable to ambulate secondary to pain, is limited to a walker, and requires narcotic medications. She has no other pain but agrees to your recommendation that she urgently be sent to the hospital.
..Which intervention should be added to this patient’s care to best prevent future skeletally related events (SRE)?
1) Inferior vena cava (IVC) filter placement
2) Bisphosphonates
3) External beam radiation
4) Tc-99 whole-body bone scan at regular intervals
…: 3- Further imaging PREFERRED RESPONSE 33-..: 3- Location of the lesion PREFERRED RESPONSE 34-…: 2- 15%
PREFERRED RESPONSE 35…..:4- Lung carcinoma, breast carcinoma, multiple myeloma PREFERRED RESPONSE 36-…: 2- Bisphosphonates
..Figures 37a and 37b are the lateral and anteroposterior (AP) radiographs of a 60-year-old man with a remote history of renal cell cancer. A needle biopsy of the lesion is shown in Figure 37c. The bone destruction that occurs in this process is a result of
1) tumor cells.
2) cytokines secreted by the tumor.
3) host bone osteoblasts.
4) osteoprotegerin.
.
- cytokines secreted by the tumor
..Figures 38a and 38b are the histopathology of an otherwise healthy 31-year-old man who had a growing mass excised from his forearm with local anesthetic and no preoperative imaging. The mass was documented to be subfascial and larger than 5 cm.
What is the best local treatment option?
1) Observation
2) Radiation only
3) Chemotherapy only
4) Re-excision and radiation
- Re-excision and radiation
…Figure 39a is the anteroposterior radiograph of a 51-year-old man who has had a painless soft-tissue mass on his left wrist for 2 months. MR sequences are shown in Figures 39b through 39d. A biopsy was performed and shown in a low-power hematoxylin and eosin photomicrograph in Figure 39e. The most appropriate treatment for this lesion is
1) a diet that reduces uric acid production.
2) wide local resection followed by radiotherapy.
3) marginal excision.
4) observation until the mineralization matures, and then excision and radiotherapy to prevent recurrence.
- marginal excision.
CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 43
Figures 40a through 40c are the radiograph, bone scan, and histology of a 68-year-old man who has had 3 months of pain in his left thigh with weight bearing. He has no history of cancer and no illnesses.
..The orthopaedic surgeon obtains tissue with the histology shown in Figure 40c. Treatment should consist of
1) surgical stabilization.
2) surgical stabilization and radiation.
3) excision and endoprosthesis.
4) radiation.
- …..: 1- malignant.
PREFERRED RESPONSE 41..,,,,,,,: 1- CT scan of the chest, abdomen and pelvis. PREFERRED RESPONSE 42………: 2- biopsy.
PREFERRED RESPONSE 43……….: 2- surgical stabilization and radiation.
..First-line treatment recommendations include
1) synovectomy.
2) arthrocentesis, compressive wrap, and rest.
3) en bloc resection.
4) intra-articular radioactive nucleotide injection.
- pigmented villonodular synovitis (PVNS). PREFERRED RESPONSE: 1- synovectomy.
RESPONSES FOR QUESTIONS 47 THROUGH 52
…Figure 53 is the emergency department radiograph of a 7-year-old boy who has pain and is unwilling to use his right arm after a fall on the playground. What is the most appropriate initial treatment?
1) Nonsurgical treatment of the fracture
2) Aspiration and injection with methylprednisolone
3) Curettage and augmentation with bone cement and internal fixation
4) Further imaging and biopsy
- Nonsurgical treatment of the fracture
..Figure 54 is the CT scan of a 70-year-old man with progressive neck pain; there is no history of trauma, and examination is notable only for mildly decreased cervical range of motion. He is neurologically intact. He has monoclonal gammopathy of undetermined significance that has been stable for many years. Current serum protein electrophoresis is unchanged. History and examination reveal no other causes for his pain. What is the next step in clinical management?
1) Corpectomy and anterior fusion
2) Radiation therapy followed by multiple myeloma protocol chemotherapy
3) CT-guided biopsy
4) CT scan of the chest, abdomen, and pelvis
- CT scan of the chest, abdomen, and pelvis
…A 27-year-old incarcerated man was found to have a fungating mass on his anterolateral right proximal thigh. A clinical photograph is shown in Figure 55a. T1- and T2-weighted coronal MRI scans are shown in Figures 55b and 55c. The hematoxylin and eosin and CD34 stained histology are shown in Figures 55d and 55e. What is the most likely diagnosis?
1) Squamous cell carcinoma
2) Melanoma
3) Dermatofibrosarcoma protuberans (DFSP)
4) Desmoid tumor
- Dermatofibrosarcoma protuberans (DFSP)
..Figures 56a and 56b are the axial short tau inversion recovery and T1 with contrast images of a 7-month-old infant who is found to have a right scapular soft-tissue mass. On examination, the mass is hard. A biopsy was performed and is shown in Figure 56c (hematoxylin and eosin, 400x). What is the optimal treatment for this patient?
1) Intralesional excision 2- Marginal excision
2) Wide excision 4- Observation
- Wide excision
…Figures 57a through 57d show the radiographs and T1- and T2-weighted MRI scan sequences of the proximal femur of a 60-year-old man with progressive thigh pain. A review of radiographs taken 3 years ago reveals that the lesion is new. The biopsy specimen is shown in Figure 57e; staging studies show no other lesions, and local imaging confirms the process is confined to bone (no soft-tissue mass). The next treatment step should include
1) hip disarticulation.
2) radiotherapy.
3) ifosfamide-based chemotherapy.
4) wide resection and reconstruction.
- wide resection and reconstruction.
…The characteristic translocation and genes involved in extraskeletal myxoid chondrosarcoma is
1) t(11;12) EWS;FLI1
2) t(12;16) TLS;CHOP.
3) t(9;22)EWS;CHN.
4) t(9;22) BCR-ABL.
.
- t(9;22) EWS;CHN
.Figures 59a and 59b are the axial T2 and T1 with contrast MRI scans of a 32-year-old woman who has a 10-year history of pain and a 1-year history of progressive swelling in her right leg. The histopathology is shown in Figure 59c. A radiograph of her leg showed no mineralizations or osseous erosions. The chromosomal abnormality that is associated with this disease is
1) t(11;22).
2) t(2;13).
3) t(X;18).
4) t(12;16).
- t(X;18).
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
A 45-year-old woman has an enlarging buttock mass. The mass is 12 cm and nonpainful. The patient first noticed it about 6 months after she had a low-impact fall. The general surgeon evaluating the patient felt this mass could be either a lipoma or a hematoma. The patient underwent a surgical procedure to remove the mass.
..What is the most common detrimental impact of an unplanned excision of a high-grade soft-tissue sarcoma?
1) Decreased mortality
2) Decreased recurrence
3) Increased wound complications
4) Increased functional outcome
-,…: 2- Imaging studies (MRI scan or CT scan) PREFERRED RESPONSE 61….: 1- Meticulous hemostasis and closure PREFERRED RESPONSE 62…..: 3- No imaging was obtained before surgery. PREFERRED RESPONSE 63…..: 3- Increased wound complications
CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 66
Figures 64a through 64c are the radiograph, MRI scan, and histology of a 53-year-old man with medial knee pain and swelling below the knee.
..Histology of the lesion is shown in Figure 64c. The best next treatment step is
1) radiation.
2) radiation and surgery.
3) chemotherapy.
4) observation.
- Translocation x;18 PREFERRED RESPONSE: 4- Biopsy
PREFERRED RESPONSE: 2- radiation and surgery.
..A 26-year-old woman has had a slow-growing and painful mass at the base of her ring finger for several months. Radiographs of the affected digit show no mineralization or erosions of the underlying bone. An axial T1 MRI scan is shown in Figure 67a, and a corresponding short tau inversion recovery image is shown in Figure 67b. A coronal T1 MRI scan with contrast is shown in Figure 67c. The best next treatment step is
1) referral to a sarcoma center.
2) observation.
3) excisional biopsy.
4) marginal excision.
- referral to a sarcoma center.
..What is the most specific immunohistochemistry staining pattern that confirms the diagnosis of desmoid tumor?
1) Membranous beta-catenin staining
2) Nuclear beta-catenin staining
3) Nuclear SMAD4 staining
4) Vimentin positivity
- Nuclear beta-catenin staining
…A 30-year-old woman has progressive gait instability, back pain, and urinary retention. Figures 69a and 69b show the axial T2 and postcontrast MRI scans taken at the level of T11, and Figure 69c shows the sagittal T1-weighted image. Representative histology is shown in Figure 69d. The patient remains ambulatory, but symptoms have
progressed during the last week and she is beginning to feel weakness in her legs. Examination is notable for decreased rectal tone, lower-extremity hyperreflexia and clonus, and 4/5 motor strength throughout the lower extremities. What is the most appropriate treatment recommendation for this patient?
1) Margin-free en bloc spondylectomy of T11
2) Radiation therapy
3) Radiation therapy followed by anterior corpectomy and fusion
4) Transpedicular decompression and posterior stabilization followed by radiation therapy
- Transpedicular decompression and posterior stabilization followed by radiation therapy
…Giant-cell tumor of bone usually involves the epiphysis of long bones. What is the next most common type of tumor involving this anatomical location?
1) Conventional chondrosarcoma
2) Aneurysmal bone cyst
3) Chondroblastoma
4) Osteoblastoma
- Chondroblastoma
CLINICAL SITUATION FOR QUESTIONS 71 THROUGH 73
Figures 71a through 71e are the radiographs, MRI scan, and CT scans of a 14-year-old-boy who has cyclical pain in his thigh. His symptoms began approximately 6 months ago. He complains of increased pain when he runs and also of pain that wakes him at night. This pain is relieved by nonsteroidal anti-inflammatory drugs (NSAIDs).
…What is the etiology of the pain associated with this lesion?
1) Prostaglandin production
2) Gram-positive cocci
3) Osteoclast activation
4) Loss of structural integrity of the bone
- Osteoid osteoma PREFERRED RESPONSE: 2- radiofrequency ablation. PREFERRED RESPONSE: 1- Prostaglandin production
...Figure 74 is the radiograph of an 11-year-old boy with pain in his left arm. Prognosis is most influenced by
1) stage at presentation.
2) grade at presentation.
3) response to neoadjuvant chemotherapy.
4) histologic subtype.
- stage at presentation.
..Figures 75a through 75d are the radiograph, CT scan, bone scan, and biopsy of a 45-year-old man who has had a several-month history of progressive pain in his right hip and groin region. Based on these images and histology, what is the most appropriate treatment?
1) Wide resection
2) Curetting and bone grafting
3) Percutaneous cementation and radiotherapy
4) Chemotherapy and radiotherapy
- Wide resection
..Figure 76 is the radiograph of a 77-year-old patient with a history of myeloma who has had severe arm pain after opening a jar. Pain was present for 3 months prior to injury. The most biomechanically stable construct for this fracture is
1) intramedullary nailing (IMN).
2) IMN and cement.
3) plate.
4) plate and cement.
- plate and cement.
CLINICAL SITUATION FOR QUESTIONS 77 THROUGH 79
Figures 77a through 77c are the radiograph and MRI scans of a 45-year-old woman who enjoys dancing and has had left ankle pain for approximately 1 month with minimal trauma. She has slightly limited ankle dorsiflexion with a mechanical block with pain.
..The patient undergoes recommended surgery and minimal joint damage is found. How should she be counseled regarding her future prognosis?
1) High risk for local recurrence, moderate risk for metastases
2) High risk for local recurrence, no risk for metastases
3) Low risk for local recurrence, moderate risk for metastases
4) Low risk for local recurrence, no risk for metastases
- Synovial metaplasia
PREFERRED RESPONSE: 2- TA, EHL, anterior tibial artery, deep peroneal nerve, EDL PREFERRED RESPONSE: 4- Low risk for local recurrence, no risk for metastases
..Figures 80a through 80d are the radiographs and MRI scans of a 16-year-old girl who requires crutches because she is unable to bear weight on her right lower extremity. The pain has progressed over 2 months despite nonsurgical treatment.
Treatment at this point should include
1) continued observation.
2) aspiration and injection with methylprednisolone.
3) curettage and grafting.
4) wide margin resection.
- curettage and grafting.
..A previously healthy 60-year-old woman has a T5 pathologic compression fracture secondary to metastatic renal cell carcinoma. She has myelopathy with severe pain upon sitting from a supine position. The adjacent thoracic levels are unaffected. On MRI scan, there is minimal space available for the cord because of epidural involvement. What is the optimal treatment method at this time?
1) Surgical decompression and instrumented fusion
2) Surgical decompression without fusion
3) Image-guided intensity-modulated radiation therapy
4) Chemotherapy
- Surgical decompression and instrumented fusion
..Figures 82a and 82b are the MRI scans consisting of a T2 coronal sequence and axial T1 pulse sequence of a 38-year-old man who has had right thigh pain and a mass for 4 months since he pulled his hamstring. The presumed diagnosis considering his clinical history and evaluation of the MRI scan was hematoma and the mass was evacuated. The histology is shown in Figures 82c and 82d. Next treatment steps should include
1) physical therapy to accelerate healing and improve function.
2) a complete hematologic work-up to evaluate a bleeding disorder.
3) tumor bed excision and radiation to reduce local recurrence.
4) radiotherapy to complete definitive treatment of this problem.
- tumor bed excision and radiation to reduce local recurrence.
….Figures 83a through 83c are the radiograph and MRI scans of a 16-year-old girl who had posterior knee pain after a dance recital 3 weeks ago; the pain resolved 1 week ago with ibuprofen use. What is the appropriate treatment for this patient?
1) Biopsy and resection of lesion
2) Observation and serial radiographs
3) Tc-99 whole-body bone scan and fine-cut CT scan
4) Evaluation by a pediatric oncologist
- Observation and serial radiographs
CLINICAL SITUATION FOR QUESTIONS 84 THROUGH 86
Figures 84a and 84b are the CT and MRI scans of a 17-year-old girl with a painful lumbosacral scoliosis that has been present for 12 months. Examination is notable only for pain over the left sacral region and a postural scoliosis leaning away from this side.
..With treatment, the spinal deformity is expected to
1) spontaneously resolve.
2) remain stable and nonprogressive.
3) respond in proportion to the family’s compliance with brace treatment.
4) resolve in the coronal plane and progress in the sagittal plane.
- is likely to respond to percutaneous intervention.
PREFERRED RESPONSE: 1- uses nonsteroidal anti-inflammatory or aspirin medications. PREFERRED RESPONSE: 1- spontaneously resolve.
..Figures 87a through 87e are the radiograph, MRI scans, and biopsy specimen of an 83-year-old woman who is experiencing pain in her distal thigh with activity and at night. She has undergone total hip arthroplasty for hip osteoarthritis. The most appropriate treatment is
1) external beam radiation.
2) curetting and cementation.
3) radiofrequency ablation.
4) wide local resection.
- wide local resection.
CLINICAL SITUATION FOR QUESTIONS 88 through 92
Figures 88a and 88b are the radiographs of a 70-year-old woman with a remote history of localized renal cell carcinoma. She has insidious onset of right shoulder pain that worsens with any activity and at night. She appears otherwise healthy.
..Oncologic outcome for this patient
1) is influenced by extraosseous tumor extension.
2) is more favorable if the lesion is solitary.
3) involves a predictable rapid demise.
4) hinges on the presence or absence of gene amplification.
- CT scan of the chest, abdomen, and pelvis.
PREFERRED RES: 3- Should be performed if the lesion is solitary, but not necessarily if multifocal PREFERRED RESPONSE: 4- resection and reconstruction.
PREFERRED RESPONSE: 3- inhibits vascular endothelial growth factor (VEGF) pathways. PREFERRED RESPONSE: 2- is more favorable if the lesion is solitary.
..Figures 93a and 93b are the MRI scans of a 24-year-old man with painless, persistent swelling in his left knee without any trauma. What is the best next treatment step?
1) Arthroscopic anterior synovectomy and posterior open resection
2) Arthroscopic anterior synovectomy only
3) Radiation therapy and wide excision
4) Observation
- Arthroscopic anterior synovectomy and posterior open resection
..What biopsy technique for a posterior thigh sarcoma is associated with the highest risk for adverse outcome?
1) Transverse incision open biopsy
2) Core needle biopsy
3) Fine-needle aspirate
4) Longitudinal incision open biopsy
- Transverse incision open biopsy
..A 60-year-old woman with a history of breast cancer has a rapidly enlarging arm mass. The lesion is situated outside of the prior irradiation field, but within an area of heavy lymphedema involvement. Needle biopsy reveals a high-grade sarcoma. What is the most likely diagnosis?
1) Lymphangiosarcoma
2) Acral myxoinflammatory fibroblastic sarcoma
3) Hemangioendothelioma
4) Hemangiopericytoma
- Lymphangiosarcoma
RESPONSES FOR QUESTIONS 96 THROUGH 100
..Figures 106a and 106b are the T1 sagittal and T2 coronal images of a 41-year-old woman who has been experiencing electric shock-type radiating pain over her right ankle for 4½ years. Her biopsy specimen is shown in Figure 106c. What is the best next treatment step?
1) Marginal excision
2) Wide excision
3) Wide excision and radiation
4) Observation
- Marginal excision
..Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man. While walking, he collapsed and was unable to ambulate because of pain and deformity in his right leg. What is the most appropriate next step?
1) Staging studies to assess the extent of disease
2) Immediate stabilization of the fracture with an intramedullary nail
3) Curetting and bone culture
4) Segmental resection of the tibia and allograft reconstruction
- Staging studies to assess the extent of disease
RESPONSES FOR QUESTIONS 108 THROUGH 111
..Figures 112a and 112b are the anteroposterior and lateral radiographs of a 65-year-old man who has a significant history of tobacco abuse and a 6-week history of right thigh pain. Axial and sagittal MRI scans are seen in Figures 112c and 112d. His MR angiogram is shown in Figure 112e. A biopsy of a lesion is shown in Figure 112f. What is the most likely diagnosis?
1) Secondary sarcoma in a pre-existing condition
2) Angiosarcoma
3) Metastatic lung carcinoma
4) Fibrous dysplasia
- Secondary sarcoma in a pre-existing condition
CLINICAL SITUATION FOR QUESTIONS 113 THROUGH 116
Figures 113a and 113b are the radiographs of a 68-year-old-man who has increasing pain in his left groin with weight-bearing activities and a Trendelenburg gait. Radiographs reveal a lytic lesion of the greater trochanter. An initial diagnosis of adenocarcinoma of the lung was made 1 year before this presentation. His lung cancer treatment consisted of partial lobectomy and postsurgical radiation therapy.
..Staging studies show no other lesions and surgical treatment is planned; when should a biopsy be performed?
1) Before surgery
2) Intraoperatively after instrumentation
3) After surgery (reamings/curettings sent)
4) No biopsy is needed
- Positron emission tomography (PET) scan PREFERRED RESPONSE: 3- Curettage, cementation, and internal fixation PREFERRED RESPONSE: 4- resection and prosthetic reconstruction.
PREFERRED RESPONSE: 1- Before surgery
CLINICAL SITUATION FOR QUESTIONS 117 THROUGH 120
Figures 117a through 117c are the radiographs and MRI scan of a 16-year-old boy who has had a persistent fullness in his thigh since being kicked while playing soccer 4 weeks ago. He states that initially the area was painful, but now all symptoms other than the mass have resolved.
Findings of multiple lesions in multiple skeletal sites may be associated with
1) decreased risk for malignancy.
2) a characteristic chromosomal translocation.
3) soft-tissue hemangiomas.
4) limb deformity and short stature.
- Osteochondroma
PREFERRED RESPONSE: 1- benign and simply can be observed with serial radiographs. PREFERRED RESPONSE: 4- growth beyond skeletal maturity.
PREFERRED RESPONSE: 4- limb deformity and short stature.
..Figure 121a is the axial T1 MRI scan and Figure 121b is the coronal T1 MRI scan of an 85-year-old man who has a mass in his medial thigh. The mass was present for years and recently grew. His biopsy specimen is shown in Figure 121c. What is the best treatment for this patient?
1) Chemotherapy and wide local resection
2) Wide local resection and radiotherapy
3) Marginal excision
4) Observation and reimaging in 6 months
- Wide local resection and radiotherapy
..What tumor commonly metastasizes to regional lymph nodes?
1) Fibromyxoid sarcoma
2) Epithelioid sarcoma
3) Leiomyosarcoma
4) Liposarcoma
- Epithelioid sarcoma
..A 64-year-old woman has significant right arm pain associated with a destructive proximal humeral bone lesion with an associated soft-tissue mass. Her medical history includes carcinoma of the breast treated 8 years ago with modified radical mastectomy, hormone receptor-based chemotherapy, and 45 Gy of radiation with 8 subsequent disease-free years. Biopsy reveals a high-grade osteogenic sarcoma. What factor is most likely related to her current disease?
1) Presence of metastatic disease
2) Dosage of radiation treatment
3) Type of prior surgical procedure
4) Type of chemotherapy given
- Dosage of radiation treatment
..Figures 124a and 124b are the MRI scans of a 25-year-old woman who has a painful mass in her left gluteal and thigh region. Her biopsy specimen is seen in Figure 124c. What is the most likely diagnosis?
1) Desmoid fibromatosis
2) Extraskeletal Ewing sarcoma
3) Metastatic breast cancer
4) Lymphoma
- Desmoid fibromatosis
CLINICAL SITUATION FOR QUESTIONS 125 THROUGH 128
A 45-year-old woman has increasing knee pain with activity and at rest. Her radiograph, MRI scan, and histology are shown in Figures 125a through 125c.
..The cell that directly causes osteolysis in this lesion is
1) giant cell.
2) stromal cell.
3) osteoblast.
4) fibroblast.
- benign aggressive. PREFERRED RESPONSE: 4- chest radiograph.
PREFERRED RESPONSE: 1- extended intralesional curettage. PREFERRED RESPONSE: 1- giant cell.
..Figures 129a through 129c are the lateral radiograph of the sacrum, axial CT scan, and a high-power view of a fine-needle biopsy of a 47-year-old man who has buttock pain and constipation. A large mass is palpable on rectal examination. The tumor cell that is the signature of this tumor is known as a(n)
1) giant cell.
2) physaliferous cell.
3) chondroblast.
4) adipocyte.
- physaliferous cell.
..Figures 130a through 130c show the CT scan and T1- and T2-weighted MRI scan sequences of an otherwise healthy 67-year-old woman with progressive left groin pain. Her biopsy specimen is shown in Figure 130d. Staging studies reveal no other lesions. Treatment should include
1) radiotherapy.
2) chemotherapy followed by surgical resection.
3) curettage with adjuvant treatment and grafting.
4) en bloc resection.
- en bloc resection.
..A lateral radiograph (Figure 131a), sagittal short tau inversion recovery MRI scan (Figure 131b), and an axial T1 contrast MRI scan (Figure 131c) were performed on a 15-year-old boy who has injured his right knee twice during the last 5 months. He has a reduced range of motion of the knee and posterior thigh tenderness. A biopsy showed bland spindle cells, giant cells, and blood-filled spaces without endothelial lining. What is the most appropriate treatment?
1) Chemotherapy and wide local excision
2) Chemotherapy and radiotherapy
3) Marginal excision
4) Extended intralesional curettage
- Extended intralesional curettage
CLINICAL SITUATION FOR QUESTIONS 132 THROUGH 134
Figure 132 is the bone scan of a 73-year-old man who is referred from his family doctor with diffuse bone pain, fatigue, and right knee pain. Examination is notable for pain with motion about the right knee and mild hyporeflexia.
..Further imaging shows pulmonary metastases without an obvious primary tumor of origin and an incomplete fracture of the right distal femur. A decision is made to surgically treat his distal femur fracture. What is the role of establishing a preoperative histologic diagnosis for this patient?
1) The distal femoral lesion should undergo needle biopsy first.
2) Bone marrow biopsy should be done first.
3) Preoperative biopsy is not necessary because a metastatic process is present.
4) Biopsy is not necessary if the lesion demonstrates a standardized uptake value (SUV) greater than 3 on fluorodeoxyglucose positron emission tomography (PET) imaging.
.
- CT scan of the chest, abdomen, and pelvis and laboratory studies. PREFERRED RESPONSE: 3- intravenous bisphosphonate treatment.
PREFERRED RESPONSE: 3- Preoperative biopsy is not necessary because a metastatic process is present
QUESTION 31 OF 50
of 100
A 72-year-old man with a previous contralateral ankle fusion, rheumatoid arthritis, and 5 degrees of valgus; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
A 72-year-old man with a previous contralateral ankle fusion, rheumatoid arthritis, and 5 degrees of valgus; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
1
Ankle replacement
2
Ankle fusion
3
Tibiotalocalcaneal fusion
4
Total contact cast
5
Intra-articular steroid injection
- Ankle replacement
QUESTION 32 OF 50
A patient with stress fracture has a transcortical area of intense uptake on the technetium bone scan. Which of the following findings would most likely be present on the magnetic resonance imaging (MRI) scan:
1
Normal periosteal signal; normal marrow signal on T1; high marrow signal on T2
2
Normal periosteal signal; low marrow signal on T1; high marrow signal on T2
3
Normal periosteal signal on T2; low marrow signal on T1; high marrow signal on T2
4
High periosteal signal on T2; low marrow signal on T1; high marrow signal on T2
5
High periosteal signal on T2; low marrow signal on T1; normal marrow signal on T2
In 1995, Fredrickson and colleagues classified stress fractures into four grades based upon bone scans:
Grade 1     Small ill-defined cortical area of mildly increased activity Grade 2     Well-defined cortical area of moderately increased cortical                     activity
Grade 3Â Â Â Â Â Wide, cortical-medullary area of increased activity
Grade 4Â Â Â Â Â Transcortical area of intensely increased activity
In a grade 4 stress fracture, the corresponding MRI will show: High periosteal signal on T2-weighted images
Low signal on T1-weighted images, often with a liner low signal line representing the fracture line
High signal on T2-weighted images, often with a liner low signal line representing the fracture line
C orrect Answer: High periosteal signal on T2; low marrow signal on T1; high marrow signal on T2
Grade 1     Small ill-defined cortical area of mildly increased activity Grade 2     Well-defined cortical area of moderately increased cortical                     activity
Grade 3Â Â Â Â Â Wide, cortical-medullary area of increased activity
Grade 4Â Â Â Â Â Transcortical area of intensely increased activity
In a grade 4 stress fracture, the corresponding MRI will show: High periosteal signal on T2-weighted images
Low signal on T1-weighted images, often with a liner low signal line representing the fracture line
High signal on T2-weighted images, often with a liner low signal line representing the fracture line
C orrect Answer: High periosteal signal on T2; low marrow signal on T1; high marrow signal on T2
QUESTION 33 OF 50
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?
1
Myositis ossificans
2
Tumoral calcinosis
3
Synovial cell sarcoma
4
Fungal granuloma
5
Hemochromatosis
The radiographic findings are classic for tumoral calcinosis; they are not consistent with myositis ossificans, fungal granuloma, or hemochromatosis. The condition typically appears as large aggregations of dense calcified lobules confined to the surrounding soft tissues. Hyperphosphatemia is a fundamental factor in many patients with this condition. Tumoral calcinosis also occurs in the setting of chronic renal failure when mineral homeostasis is not controlled. The histologic appearance is essentially a foreign body granuloma reaction. Multilocular cysts with purplish amorphous material are surrounded by thick connective tissue capsules. The fibrous walls contain numerous foreign body giant cells. Surgical excision is indicated if the tumor causes discomfort or interferes with function.
REFERENCES: Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Boskey AL, Vigorita VJ, Sencer O, Stuchin SA, Lane JM: Chemical, microscopic, and ultrastructural characterization of the mineral deposits in tumoral calcinosis. Clin Orthop 1983;178:258-269.
REFERENCES: Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Boskey AL, Vigorita VJ, Sencer O, Stuchin SA, Lane JM: Chemical, microscopic, and ultrastructural characterization of the mineral deposits in tumoral calcinosis. Clin Orthop 1983;178:258-269.
QUESTION 34 OF 50
A patient presents for treatment of a dislocated second metatarsophalangeal joint. Radiographs demonstrate the dislocation. In addition to soft tissue balancing, you perform an oblique shortening osteotomy of the second metatarsal head (Weil). The most common complication following this osteotomy is:
1
Recurrent dislocation
2
Avascular necrosis of the metatarsal head
3
Arthritis of the second metatarsophalangeal joint
4
Elevation of the second toe
5
C law toe deformity
The Weil osteotomy is a good procedure to correct deformity about the lesser metatarsophalangeal joint but is associated with potential complications, the most common of which is elevation of the second toe. As a result of shortening and plantar shifting of the metatarsal, the intrinsic muscles shift dorsally and can function as a dorsiflexor of the metatarsophalangeal joint.
QUESTION 35 OF 50
of 100
A 10-month-old boy has an untreated developmental hip dislocation.




A 10-month-old boy has an untreated developmental hip dislocation.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.
Figure 46a
Figure 46b
Figure 46c
Figure 46d
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.
Figure 46a
Figure 46b
Figure 46c
Figure 46d
QUESTION 36 OF 50
of 100
The injury pattern shown in the CT image in Figure 26 is most commonly associated with which mechanism?

The injury pattern shown in the CT image in Figure 26 is most commonly associated with which mechanism?
1
Traction injury.
2
Seizures
3
Collision athletic events
4
Postpolio syndrome
Posterior shoulder dislocations are most commonly the result of seizures and electrical shock. Collision athletic events, postpolio syndrome, and traction injury are rarely associated with posterior shoulder dislocations. The bony defect caused by impaction of the anterior superior humeral head on the posterior glenoid has been referred to as a “reverse Hill-Sachs lesion.”
RECOMMENDED READINGS
1. McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;64:1584-1590.
2. [Kowalsky MS, Levine WN. Traumatic posterior glenohumeral dislocation: classification, pathoanatomy, diagnosis, and treatment. Orthop Clin North Am. 2008 Oct;39(4):519-33, viii. doi: 10.1016/j.ocl.2008.05.008. Review. PubMed PMID: 18803981.](http://www.ncbi.nlm.nih.gov/pubmed/18803981)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18803981)
RECOMMENDED READINGS
1. McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;64:1584-1590.
2. [Kowalsky MS, Levine WN. Traumatic posterior glenohumeral dislocation: classification, pathoanatomy, diagnosis, and treatment. Orthop Clin North Am. 2008 Oct;39(4):519-33, viii. doi: 10.1016/j.ocl.2008.05.008. Review. PubMed PMID: 18803981.](http://www.ncbi.nlm.nih.gov/pubmed/18803981)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18803981)
QUESTION 37 OF 50
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Initial surgical management should consist of
---
---


Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Initial surgical management should consist of
---
---
1
closed reduction and percutaneous screw placement.
2
open reduction internal fixation through an anterior midline approach.
3
spanning external fixation and closed manipulative realignment.
4
ring fixation.
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but
typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but
typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
QUESTION 38 OF 50
What structure is most often injured in a volar proximal interphalangeal joint dislocation?
1
Sagittal bands
2
Central slip
3
Lumbrical
4
Juncturae tendinum
5
Terminal extensor tendon
Closed ruptures of the central slip of the extensor tendon may occur with volar proximal interphalangeal joint dislocation, forced flexion of the proximal interphalangeal joint, or blunt trauma to the dorsum of the proximal interphalangeal joint. The other structures are not typically injured in proximal interphalangeal joint dislocations. Treatment typically requires static splinting of the proximal interphalangeal joint. In the more common dorsal proximal interphalangeal joint dislocation, the volar plate is injured, and early range of motion may be started after reduction.
REFERENCES: Doyle JR: Extensor tendons: Acute injuries, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1925.
Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
REFERENCES: Doyle JR: Extensor tendons: Acute injuries, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1925.
Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
QUESTION 39 OF 50
of 100 A 17-year-old high school football player sustains a traumatic anterior shoulder dislocation, resulting in a small bony Bankart lesion and small Hill-Sachs lesion. The patient undergoes an arthroscopic Bankart repair with incorporation of the bone fragment and returns to play football the following year. He has a recurrent dislocation at football practice but decides to finish the football season before considering additional treatment. He sustains nine additional dislocations, with the last dislocation occurring while sleeping. The patient has eroded one-third of the inferior glenoid surface area. What is the most appropriate surgical treatment?
1
Revision arthroscopic Bankart repair with capsular shift
2
Open Bankart repair with capsular shift
3
Repair of infraspinatus tendon into the Hill-Sachs defect (remplissage procedure)
4
Coracoid transfer to the glenoid (Latarjet procedure)
DISCUSSION
A failed bony Bankart repair with multiple dislocations can further erode the anteroinferior glenoid, changing the sagittal morphology of the glenoid into an "inverted pear." Quantitative bone loss is best evaluated by CT scan with 3-D reconstructions and subtraction of the humeral head. MRI and ultrasonography can assist in evaluating soft-tissue injury, but they are not as helpful in determining bone loss compared with a CT scan. An arthrogram alone is not sufficient to evaluate bone loss. Bone loss >30% necessitates glenoid augmentation with either a Latarjet procedure or iliac crest bone grafting. A revision arthroscopic or open Bankart repair with capsular shift or remplissage do not address bone loss. The Latarjet procedure can effectively restore stability with glenoid bone loss and after failed stabilizing procedures. Patients with pain before surgery are
more likely to have pain after surgery. Age and activity level are lesser influences on satisfaction.
QUESTION 40 OF 50
-Reverse total shoulder arthroplasty improves kinematics in the rotator cuff deficient joint by what directional change to the center of rotation?
1
Medial
2
Lateral
3
Posterior
4
Proximal
No detailed explanation provided for this question.
QUESTION 41 OF 50
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. What examination findings are most consistent with the pathology seen in the radiographs?




1
Pain with resisted hip flexion
2
Pain with a half sit-up, plus tenderness at the pubic ramus
3
Pain with a combination of hip flexion, adduction, and internal rotation
4
Tenderness to palpation at the greater trochanter
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater
trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a _periacetabular osteotomy can develop a more retroverted acetabulum as well._
trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a _periacetabular osteotomy can develop a more retroverted acetabulum as well._
QUESTION 42 OF 50
An obese 62-year-old man (BMI 38) who underwent a cementless total hip arthroplasty 14 months ago fell from a ladder and is now unable to bear weight on the extremity. A radiograph from his 3-month visit is shown in Figure 77a and a radiograph from the time of the injury is shown in Figure 77b. Appropriate management includes which
of the following?
of the following?
1
Nonsurgical management with the use of a cast-brace
2
Nonsurgical management with skeletal traction
3
Open treatment with a plate with or without strut allograft
4
Revision of the femoral component to a cemented femoral component that bypasses the fracture site by two cortical diameters
5
Revision of the femoral component to a cementless femoral component that bypasses the
fracture site by at least two cortical diameters
The patient has a Vancouver type B1 fracture of the femur with a well-fixed femoral component. When comparing the two radiographs, the proximal femoral component position has not changed and remodeling is seen around the component. Nonsurgical management is associated with the complications of extended recumbency. As the femoral component is well-fixed, revision of the femoral component is not necessary.
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Ricci WM, Bolhofner BR, Lofitus T, et al: Indirect reduction and plate fixation, without grafting, for
periprosthetic femoral shaft fractures about a stable intramedullary implant. J Bone Joint Surg Am 2005;87:2240-2245.
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Ricci WM, Bolhofner BR, Lofitus T, et al: Indirect reduction and plate fixation, without grafting, for
periprosthetic femoral shaft fractures about a stable intramedullary implant. J Bone Joint Surg Am 2005;87:2240-2245.
QUESTION 43 OF 50
All of the following factors are important to achieve primary osteonal healing during plate fixation except:
1
AnatomiCreduction
2
Rigid fixation
3
Adequate vascular supply
4
Moderate-to-high strain levels
5
Very low strain levels
In primary osteonal bone healing, osteoclasts cut channels across the bone contact sites and blood vessels, and osteoblasts fill in the gap with new bone.
To achieve osteonal healing, there must be an anatomiCreduction with rigid fixation, an adequate blood supply, and the amount of motion at the fracture site must be very small to none (very low strain levels).
Moderate-to-high strain levels occur if there is motion at the osteosynthesis site. This motion results from poor fixation (lack of rigidity) or excessive loading during the healing period. High strain levels in the gap favor the formation of granulation tissue rather than bone.
To achieve osteonal healing, there must be an anatomiCreduction with rigid fixation, an adequate blood supply, and the amount of motion at the fracture site must be very small to none (very low strain levels).
Moderate-to-high strain levels occur if there is motion at the osteosynthesis site. This motion results from poor fixation (lack of rigidity) or excessive loading during the healing period. High strain levels in the gap favor the formation of granulation tissue rather than bone.
QUESTION 44 OF 50
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include
1
ultrasonic stimulation for 3 months.
2
removal of the nail and plate fixation.
3
continued observation.
4
removal of the distal locking screws to dynamize the nail.
5
exchange reamed nailing with bone graft.
The patient has an oligotrophic nonunion of the distal femoral fracture. Although the proximal fracture appears incompletely united, it was stable at exchange nailing. The treatment of choice is exchange reamed nailing to at least 2 mm above the nail in place. Bone grafting is debatable. Recent studies have shown a 70% to 75% success rate with exchange nailing only, so in nonhypertrophic nonunions, bone grafting can be considered. Nonsurgical management consisting of observation or external stimulation runs the risk of implant failure. Plate fixation is acceptable but is considered a second choice because of the need to consider stabilization of the proximal fracture until union is achieved. Also, plate fixation definitely requires bone grafting.
REFERENCES: Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141.
Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Hak DG, Lee SS, Goulet JA: Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma 2000;14:178-182.
REFERENCES: Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141.
Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Hak DG, Lee SS, Goulet JA: Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma 2000;14:178-182.
QUESTION 45 OF 50
Figure 11 shows the radiograph of an 18-year-old soccer player who reports recurrent lateral foot pain after sustaining an inversion injury. History reveals that 6 months ago he had been treated in a non-weight-bearing cast for a fifth metatarsal fracture. Management should consist of**
1
intermedullary fixation.
2
a brace or taping to limit inversion stress.
3
a short leg walking cast or a fracture walker.
4
a non-weight-bearing short leg cast.
5
a rigid orthotic insole, with early motion exercises.
Fractures in this area of the fifth metatarsal have a high incidence of delayed union, nonunion, and recurrence with nonsurgical management. In an acute fracture, prolonged casting in a non-weight-bearing cast may allow for healing; however, in the presence of prolonged symptoms, recurrent fracture, and intermedullary sclerosis, surgical treatment is preferred. Surgery most commonly consists of intermedullary fixation or medullary curettage and bone grafting, followed by application of a non-weight-bearing cast.
REFERENCES: Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff TC, Das M: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.
DeLee JC: Fractures and dislocations of the foot, in Mann R, Coughlin M (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 1465-1503.
REFERENCES: Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff TC, Das M: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.
DeLee JC: Fractures and dislocations of the foot, in Mann R, Coughlin M (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 1465-1503.
QUESTION 46 OF 50
Examination of a 10-year-old girl with a hypoplastic breast and atrophic pectoralis major may also reveal which of the following findings?
1
Absent middle phalanx
2
Absent deltoid muscle
3
Absent radius
4
Contralateral hypoplastic thumb
5
Clubfoot deformity
Poland’s syndrome has four main features: 1) short digits as the result of absence or shortening of the middle phalanx; 2) syndactyly of the short digits usually consisting of a simple, complete type; 3) hypoplasia of the hand and forearm; and 4) absence of the sternocostal head of the pectoralis major on the same side.
REFERENCES: Wilson MR, Louis DS, Stevenson TR: Poland’s syndrome: Variable expression and associated anomalies. J Hand Surg 1988;13:880-882.
Poland A: Deficiency of the pectoralis muscle. Guys Hosp Rep 1841;6:191.
REFERENCES: Wilson MR, Louis DS, Stevenson TR: Poland’s syndrome: Variable expression and associated anomalies. J Hand Surg 1988;13:880-882.
Poland A: Deficiency of the pectoralis muscle. Guys Hosp Rep 1841;6:191.
QUESTION 47 OF 50
of 100
A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
1
Inflammatory elbow arthritis
2
A presurgical flexion-extension elbow arc of approximately 50 degrees
3
Retained distal humerus hardware on presurgical radiographs
4
Evidence of presurgical elbow instability
End-stage posttraumatic or inflammatory elbow arthritis in active, high-demand patients remains difficult to treat. Traditional total elbow arthroplasty is discouraged in this demographic secondary to the concerns about implant longevity. The soft-tissue interposition arthroplasty does not necessitate the same activity and weight restrictions for patients after surgery and remains a reasonable salvage procedure. Larson and Morrey published their findings on 38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in
Mayo Elbow Performance Score in addition to improvement in the flexion-extension arc from 51 degrees to 97 degrees after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability upon examination; retained hardware from prior surgery was not deemed a contraindication.
RECOMMENDED READINGS
5. [Larson AN, Morrey BF. Interposition arthroplasty with an Achilles tendon allograft as a salvage procedure for the elbow. J Bone Joint Surg Am. 2008 Dec;90(12):2714-23. doi: 10.2106/JBJS.G.00768. PubMed PMID: 19047718.](http://www.ncbi.nlm.nih.gov/pubmed/19047718)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19047718)
6. [Nolla J, Ring D, Lozano-Calderon S, Jupiter JB. Interposition arthroplasty of the elbow with hinged external fixation for post-traumatic arthritis. J Shoulder Elbow Surg. 2008 May-Jun;17(3):459-64. doi: 10.1016/j.jse.2007.11.008. Epub 2008 Mar 14. PubMed PMID: 18342545. ](http://www.ncbi.nlm.nih.gov/pubmed/18342545)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18342545)
Mayo Elbow Performance Score in addition to improvement in the flexion-extension arc from 51 degrees to 97 degrees after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability upon examination; retained hardware from prior surgery was not deemed a contraindication.
RECOMMENDED READINGS
5. [Larson AN, Morrey BF. Interposition arthroplasty with an Achilles tendon allograft as a salvage procedure for the elbow. J Bone Joint Surg Am. 2008 Dec;90(12):2714-23. doi: 10.2106/JBJS.G.00768. PubMed PMID: 19047718.](http://www.ncbi.nlm.nih.gov/pubmed/19047718)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19047718)
6. [Nolla J, Ring D, Lozano-Calderon S, Jupiter JB. Interposition arthroplasty of the elbow with hinged external fixation for post-traumatic arthritis. J Shoulder Elbow Surg. 2008 May-Jun;17(3):459-64. doi: 10.1016/j.jse.2007.11.008. Epub 2008 Mar 14. PubMed PMID: 18342545. ](http://www.ncbi.nlm.nih.gov/pubmed/18342545)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18342545)
QUESTION 48 OF 50
of 100
A 65-year-old patient undergoes revision total shoulder arthroplasty. Intraoperative culture results held for 5 days are negative. Five days after surgery, this afebrile patient experiences increasing pain, modest redness, and decreased motion. His postsurgical erythrocyte sedimentation rate is 25 mm/h (reference range, 0-20 mm/h), and his white blood cell level is normal. What is the best next step?



A 65-year-old patient undergoes revision total shoulder arthroplasty. Intraoperative culture results held for 5 days are negative. Five days after surgery, this afebrile patient experiences increasing pain, modest redness, and decreased motion. His postsurgical erythrocyte sedimentation rate is 25 mm/h (reference range, 0-20 mm/h), and his white blood cell level is normal. What is the best next step?
1
Additional imaging
2
Anti-inflammatory medications
3
Physical therapy
4
Ask microbiology to hold the intraoperative cultures for 2 weeks
_Propionibacterium acnes is increasingly recognized as a pathogen in shoulder surgery of all types and a cause of postsurgical shoulder pain. Its presentation often is characterized by pain and only minimally elevated laboratory study results and low-grade clinical findings. Cultures should be held for 2 weeks to identify this organism._
RECOMMENDED READINGS
12. Hudek R, Sommer F, Kerwat M, Abdelkawi AF, Loos F, Gohlke F. Propionibacterium acnes in shoulder surgery: true infection, contamination, or commensal of the deep tissue? J Shoulder Elbow Surg. 2014 Dec;23(12):1763-71. doi: 10.1016/j.jse.2014.05.024. Epub 2014 Aug 29. PubMed PMID:
[25179369/. ](http://www.ncbi.nlm.nih.gov/pubmed/25179369)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25179369)
13. [Matsen FA 3rd, Butler-Wu S, Carofino BC, Jette JL, Bertelsen A, Bumgarner R. Origin of propionibacterium in surgical wounds and evidence-based approach for culturing propionibacterium from surgical sites. J Bone Joint Surg Am. 2013 Dec 4;95(23):e1811-7. doi: 10.2106/JBJS.L.01733. PubMed PMID: 24306704. ](http://www.ncbi.nlm.nih.gov/pubmed/24306704)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24306704)
14. [Sethi PM, Sabetta JR, Stuek SJ, Horine SV, Vadasdi KB, Greene RT, Cunningham JG, Miller SR. Presence of Propionibacterium acnes in primary shoulder arthroscopy: results of aspiration and tissue cultures. J Shoulder Elbow Surg. 2015 May;24(5):796-803. doi: 10.1016/j.jse.2014.09.042. Epub 2014 Dec 4. PubMed PMID: 25483906. ](http://www.ncbi.nlm.nih.gov/pubmed/25483906)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25483906)
CLINICAL SITUATION FOR QUESTIONS 21 AND 22
Figures 21a through 21c are the radiographs of a 45-year-old man following acute trauma.
RECOMMENDED READINGS
12. Hudek R, Sommer F, Kerwat M, Abdelkawi AF, Loos F, Gohlke F. Propionibacterium acnes in shoulder surgery: true infection, contamination, or commensal of the deep tissue? J Shoulder Elbow Surg. 2014 Dec;23(12):1763-71. doi: 10.1016/j.jse.2014.05.024. Epub 2014 Aug 29. PubMed PMID:
[25179369/. ](http://www.ncbi.nlm.nih.gov/pubmed/25179369)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25179369)
13. [Matsen FA 3rd, Butler-Wu S, Carofino BC, Jette JL, Bertelsen A, Bumgarner R. Origin of propionibacterium in surgical wounds and evidence-based approach for culturing propionibacterium from surgical sites. J Bone Joint Surg Am. 2013 Dec 4;95(23):e1811-7. doi: 10.2106/JBJS.L.01733. PubMed PMID: 24306704. ](http://www.ncbi.nlm.nih.gov/pubmed/24306704)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24306704)
14. [Sethi PM, Sabetta JR, Stuek SJ, Horine SV, Vadasdi KB, Greene RT, Cunningham JG, Miller SR. Presence of Propionibacterium acnes in primary shoulder arthroscopy: results of aspiration and tissue cultures. J Shoulder Elbow Surg. 2015 May;24(5):796-803. doi: 10.1016/j.jse.2014.09.042. Epub 2014 Dec 4. PubMed PMID: 25483906. ](http://www.ncbi.nlm.nih.gov/pubmed/25483906)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25483906)
CLINICAL SITUATION FOR QUESTIONS 21 AND 22
Figures 21a through 21c are the radiographs of a 45-year-old man following acute trauma.
QUESTION 49 OF 50
of 100
Figure 1 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?

Figure 1 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?
1
Transforming growth factor-beta (TGF-β), bone morphogenetic protein-2 (BMP-2), latent membrane protein 1
2
Tissue inhibitor of matrix metallo-proteinase-1 (MMP-1), growth and development factor5, noggin
3
Gremlin, MMP, biglycan
4
Tumor necrosis factor-alpha (TNF-α), Interleukin-1 (IL-1), MMP
■
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-α, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-β, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-α, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-β, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
QUESTION 50 OF 50
Surgical repair of the injury shown in the MRI scans in Figures 1 through 4 through a single-incision approach has a higher incidence of
33
33
1
heterotopic ossification.
2
posterior interosseous nerve injury.
3
secondary surgery.
4
lateral antebrachial cutaneous nerve injury.
The MRI scans show a distal biceps tendon avulsion with significant retraction. When addressing these injuries, a single-incision approach has been associated with an increased risk of lateral antebrachial cutaneous nerve injury. A two-incision approach has been associated with an increased risk of heterotopic ossification, second surgeries and posterior interosseous nerve injury.
34
34
