Score: 0%
Advanced Orthopedic Mock Exam (Set F85282)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
Which of the following statements is true concerning the changes seen in human articular cartilage as a person ages (normal cartilage):
1
Progressive increase in chondroitin 4-sulfate
2
Progressive decrease in chondroitin 6-sulfate
3
Progressive decrease in collagen concentration
4
Progressive increase in collagen concentration
5
Progressive increase in keratan sulfate concentration
There are several important points concerning aging and articular cartilage. The collagen content increases quickly after birth, attaining adult levels, and then it does not materially change. The water level is high in immature individuals but remains constant in the adult. In contrast to the stable levels of collagen and water, the proteoglycan composition changes:
Chondroitin 4-sulfate levels progressively decrease. Chondroitin 6-sulfate levels progressively increase.
Keratan sulfate levels progressively increase in the human. At age 30, the level increases to 25% to 50% of proteoglycan content.
Aggregation decreases with advancing age.
Chondroitin 4-sulfate levels progressively decrease. Chondroitin 6-sulfate levels progressively increase.
Keratan sulfate levels progressively increase in the human. At age 30, the level increases to 25% to 50% of proteoglycan content.
Aggregation decreases with advancing age.
QUESTION 2 OF 50
of 100
Which factor leads to the worst long-term prognosis in slipped capital femoral epiphysis (SCFE), most likely requiring total hip arthroplasty (THA)?
Which factor leads to the worst long-term prognosis in slipped capital femoral epiphysis (SCFE), most likely requiring total hip arthroplasty (THA)?
1
Avascular necrosis (AVN)
2
Age at onset of SCFE
3
Slip severity or slip angle
4
Femoral acetabular impingement (FAI) with degenerative changes
■
In patients identified and treated for a SCFE, the most devastating complication is AVN. The most likely indication for a total joint replacement in patients with SCFE is the presence of AVN or chondrolysis. The severity of slip, presence of FAI, and/or degenerative changes may increase the possibility of requiring a THA, but typically at an older age than patients with AVN. The age of onset of SCFE has not been found to be directly related to complications or outcomes, such as the development of AVN.
In patients identified and treated for a SCFE, the most devastating complication is AVN. The most likely indication for a total joint replacement in patients with SCFE is the presence of AVN or chondrolysis. The severity of slip, presence of FAI, and/or degenerative changes may increase the possibility of requiring a THA, but typically at an older age than patients with AVN. The age of onset of SCFE has not been found to be directly related to complications or outcomes, such as the development of AVN.
QUESTION 3 OF 50
All of the following factors increase the rigidity of an external fixator except:
1
Increased individual pin diameter
2
Increased pin number
3
Increased bone-to-rod distance
4
Increased pin group separation
5
Separating half pins by 45°
There are many factors that increase the rigidity of an external fixator, including: Increased pin diameter
Increased pin number Decreased bone-to-rod distance Increased pin group separation Separating half pins by 45°
Increasing the bone-to-rod distance decreases the rigidity of the system. The fracture gap is also important. The fracture gap should be minimized for excellent bone apposition.
Increased pin number Decreased bone-to-rod distance Increased pin group separation Separating half pins by 45°
Increasing the bone-to-rod distance decreases the rigidity of the system. The fracture gap is also important. The fracture gap should be minimized for excellent bone apposition.
QUESTION 4 OF 50
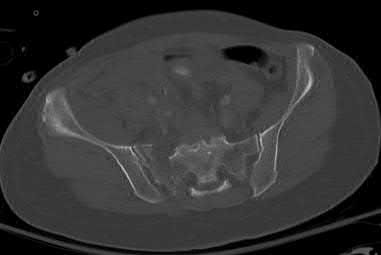
A 65-year-old female presents with the injury seen in Figures A and B after a motor vehicle collision. She is hemodynamically unstable and undergoes emergent pelvic supra-acetabular external fixation followed by laparotomy. She is now hemodynamically stable and cleared for surgery. She has no evidence of neurologic deficit on examination. Which of the following factors is a relative contraindication to open reduction and plating of her posterior pelvic injury from an anterior approach?

1
Sacral fracture
2
Prior laparotomy
3
Supra-acetabular external fixtator
4
Parasymphyseal fractures
5
Ipsilateral proximal femur fracture
An anterior approach to the sacroiliac (SI) joint is indicated with displaced SI joint dislocations that cannot be reduced with closed or percutaneous techniques. One contraindication to anterior exposure of the SI joint is comminuted sacral fracture patterns.
Posterior pelvic ring injuries that are unable to be reduced by closed techniques may require open reduction via anterior or posterior approaches. Relative contraindications to anterior approach include comminuted sacral fractures, morbid obesity, iliac wing external fixation, and ipsilateral diverting colostomy. In the presence of a comminuted sacral fracture, aggressive medial dissection would be required and would place the L5 nerve root at risk.
Simpson et al describe their initial results with open reduction and internal fixation of the SI joint via an anterior exposure in a series of 16 patients. They note that sacral alar comminution is a contraindication to the anterior approach
Jones provides an overview of the operative treatment of posterior pelvic ring injuries. He demonstrates reduction and fixation techniques via both anterior and posterior exposures.
Incorrect Answers:
Answer 2: Prior laparotomy is not a contraindication to open anterior approach if the bowel is in continuity and there is no evidence of wound infection Answer 3: Supracetabular external fixation does not interfere with anterior approach to the SI joint
Answer 4: Anterior pelvic ring injuries such as parasymphyseal fractures do not affect the choice of approach
Answer 5: An ipsilateral proximal femur fracture does not affect the choice of approach
Posterior pelvic ring injuries that are unable to be reduced by closed techniques may require open reduction via anterior or posterior approaches. Relative contraindications to anterior approach include comminuted sacral fractures, morbid obesity, iliac wing external fixation, and ipsilateral diverting colostomy. In the presence of a comminuted sacral fracture, aggressive medial dissection would be required and would place the L5 nerve root at risk.
Simpson et al describe their initial results with open reduction and internal fixation of the SI joint via an anterior exposure in a series of 16 patients. They note that sacral alar comminution is a contraindication to the anterior approach
Jones provides an overview of the operative treatment of posterior pelvic ring injuries. He demonstrates reduction and fixation techniques via both anterior and posterior exposures.
Incorrect Answers:
Answer 2: Prior laparotomy is not a contraindication to open anterior approach if the bowel is in continuity and there is no evidence of wound infection Answer 3: Supracetabular external fixation does not interfere with anterior approach to the SI joint
Answer 4: Anterior pelvic ring injuries such as parasymphyseal fractures do not affect the choice of approach
Answer 5: An ipsilateral proximal femur fracture does not affect the choice of approach
QUESTION 5 OF 50
Figures 1 and 2 show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?
7
7
1
Retain the components and implant a tibial strut allograft.
2
Revise the tibial component with a metaphyseal cone and metaphyseal uncemented stem.
3
Revise the tibial component with a metaphyseal cone and a press-fit diaphyseal-engaging stem.
4
Revise the tibial component with a long cemented diaphyseal-engaging stem.
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and
5
They also assist in obtaining correct limb alignment. Short metaphyseal- engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
8
9
9
QUESTION 6 OF 50
After sustaining a muscle contusion injury, prolonged immobilization leads to
1
increased tensile stiffness.
2
increased granulation tissue production.
3
improved recovery of tensile strength.
4
reduced incidence of myositis ossificans.
No detailed explanation provided for this question.
QUESTION 7 OF 50
Figure 6 shows the radiograph of a 72-year-old woman who underwent a primary total hip arthroplasty
17 years ago. She now reports groin pain. Optimal surgical management should consist of which of the following?
17 years ago. She now reports groin pain. Optimal surgical management should consist of which of the following?
1
Synovectomy and polyethylene liner exchange
2
Synovectomy, polyethylene liner exchange, and femoral stem revision
3
Synovectomy and complete acetabular revision
4
Synovectomy, bone grafting of lytic lesions, and retention of the components and polyethylene liner
5
Revision of all components with synovectomy
Polyethylene wear is evident due to the superiorly eccentric position of the femoral head within the acetabulum. Despite proximal femoral osteolysis, the component appears well fixed, as does the acetabulum. The acetabular component appears to be well positioned. Therefore, an isolated synovectomy and polyethylene liner exchange is indicated. If the hip is stable, there is no need for more extensive revision work.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 521-528.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 521-528.
QUESTION 8 OF 50
of 100
An otherwise healthy 47-year-old woman has numbness and weakness in her bilateral lower legs. Her physical examination reveals an ataxic gait and +3/4 patella and Achilles reflexes. Her upper extremity neurological examination is normal. Her MRI scans are shown in Figures 1 through

An otherwise healthy 47-year-old woman has numbness and weakness in her bilateral lower legs. Her physical examination reveals an ataxic gait and +3/4 patella and Achilles reflexes. Her upper extremity neurological examination is normal. Her MRI scans are shown in Figures 1 through
1
What additional test would best help you plan her treatment?

2
Flexion / extension radiographs of the thoracic spine
3
CT scan of the thoracic spine
4
MRI scan of the cervical spine
5
Pulmonary function test
■
The patient has thoracic disk herniation. This is causing significant compression of her spinal cord. Her symptoms and physical examination are consistent with myelopathy. Given the patient’s symptoms, surgical treatment is most appropriate. A significant number of thoracic disk herniations will calcify, which can alter the surgical approach. A CT scan (or CT myelogram) is the best way to detect calcification. Flexion extension images, while helpful, may not detect the calcified disk. Instability in the thoracic spine is uncommon. Given the patients hyperreflexia, lumbar pathology contributing to the patient’s complaints is unlikely. Pulmonary function tests may be considered for patients requiring a transthoracic approach, but they are unlikely to be abnormal in an otherwise healthy patient.
The patient has thoracic disk herniation. This is causing significant compression of her spinal cord. Her symptoms and physical examination are consistent with myelopathy. Given the patient’s symptoms, surgical treatment is most appropriate. A significant number of thoracic disk herniations will calcify, which can alter the surgical approach. A CT scan (or CT myelogram) is the best way to detect calcification. Flexion extension images, while helpful, may not detect the calcified disk. Instability in the thoracic spine is uncommon. Given the patients hyperreflexia, lumbar pathology contributing to the patient’s complaints is unlikely. Pulmonary function tests may be considered for patients requiring a transthoracic approach, but they are unlikely to be abnormal in an otherwise healthy patient.
QUESTION 9 OF 50
Placement of the most distal interlocking screw seen in the radiographs in Figures 1 and 2 poses a risk to the nerve that controls what motor function?
1
Elbow flexion
2
Thumb interphalangeal (IP) joint extension
3
Index finger proximal IP joint flexion
4
Index finger metacarpophalangeal (MCP) joint abduction
9
The most distal locking screw in this intramedullary nail construct was placed from anterior to posterior, passing through the distal portion of the biceps and brachialis muscle bellies. The median nerve, along with the brachial artery, is at risk as it lies between these 2 muscles. Malrotation of the nail, producing a more anteromedial starting point for the screw, can lead to a path that intersects with the nerve. Blunt dissection and soft-tissue protection is warranted with this screw placement. Median nerve injury would affect innervations of the flexor digitorum superficialis and profundus to the index finger (among other motors). Although the dissection violates the muscle belly of these 2 elbow flexors, measurable weakness is not typically seen. The radial nerve has already provided function to triceps (elbow extension) proximal to this level and lies sufficiently lateral to be more of a concern with a lateral screw placement (thumb IP extension). The ulnar nerve (index MCP abduction) is further medial at this level and would be at considerably lower risk than the median.
The most distal locking screw in this intramedullary nail construct was placed from anterior to posterior, passing through the distal portion of the biceps and brachialis muscle bellies. The median nerve, along with the brachial artery, is at risk as it lies between these 2 muscles. Malrotation of the nail, producing a more anteromedial starting point for the screw, can lead to a path that intersects with the nerve. Blunt dissection and soft-tissue protection is warranted with this screw placement. Median nerve injury would affect innervations of the flexor digitorum superficialis and profundus to the index finger (among other motors). Although the dissection violates the muscle belly of these 2 elbow flexors, measurable weakness is not typically seen. The radial nerve has already provided function to triceps (elbow extension) proximal to this level and lies sufficiently lateral to be more of a concern with a lateral screw placement (thumb IP extension). The ulnar nerve (index MCP abduction) is further medial at this level and would be at considerably lower risk than the median.
QUESTION 10 OF 50
All of the following factors are important to achieve primary osteonal healing during plate fixation except:
1
AnatomiCreduction
2
Rigid fixation
3
Adequate vascular supply
4
Moderate-to-high strain levels
5
Very low strain levels
In primary osteonal bone healing, osteoclasts cut channels across the bone contact sites and blood vessels, and osteoblasts fill in the gap with new bone.
To achieve osteonal healing, there must be an anatomiCreduction with rigid fixation, an adequate blood supply, and the amount of motion at the fracture site must be very small to none (very low strain levels).
Moderate-to-high strain levels occur if there is motion at the osteosynthesis site. This motion results from poor fixation (lack of rigidity) or excessive loading during the healing period. High strain levels in the gap favor the formation of granulation tissue rather than bone.
To achieve osteonal healing, there must be an anatomiCreduction with rigid fixation, an adequate blood supply, and the amount of motion at the fracture site must be very small to none (very low strain levels).
Moderate-to-high strain levels occur if there is motion at the osteosynthesis site. This motion results from poor fixation (lack of rigidity) or excessive loading during the healing period. High strain levels in the gap favor the formation of granulation tissue rather than bone.
QUESTION 11 OF 50
A 63-year-old right-hand dominant woman has a history of gradually progressive atraumatic right shoulder pain. She describes a constant nagging pain that radiates to her deltoid insertion and difficulty with overhead activities. Her examination and imaging studies confirm a rotator cuff tear. What is the mostly likely initiating anatomic location of her tear?
1
Anterior portion of the supraspinatus tendon adjacent to the biceps tendon
2
15 mm posterior to the biceps tendon near the supraspinatus/infraspinatus junction
3
Superior portion of the subscapularis tendon
4
30 mm posterior to the biceps tendon near the supraspinatus/infraspinatus junction 51
Fundamental to understanding the pathogenesis of rotator cuff tears is an appreciation of the likely initiation site of the disease process. Although authors initially postulated that rotator cuff tears originated in the anterior margin of the supraspinatus tendon near the biceps tendon, recent research has challenged this notion. Kim and associates analyzed 360 full-thickness or partial-thickness rotator cuff tears using ultrasonograms. They separated stratified tears based on their anteroposterior size and whether they were partial- or full-thickness tears. The mean width and length of tear size was 16.3 mm and 17 mm, respectively. Histograms showed that the most common tear location for all tears regardless of size was approximately 15 mm posterior to the biceps tendon. This corresponds to the center of the rotator crescent initially described by Burkhart and associates. This location is described as being more susceptible to degeneration secondary to its diminished vascular supply and mechanical properties. The rotator cable is an arch-shaped thick bundle of fibers that is thought to shield the crescent from stress.
QUESTION 12 OF 50
The most common complication after resection of a plantar fibromatosis is:
1
A recurrent fibroma
2
Infection
3
Wound dehiscence
4
Injury to the medial plantar nerve
5
Injury to the lateral plantar nerve
The most common complication after resection of plantar fibromatosis is recurrence. Although other complications (nerve injury and wound dehiscence) do occur, they occur less frequently. The most reliable treatment for plantar fibromatosis is observation and shoe wear modification if the lesion is painful.
QUESTION 13 OF 50
Which of the following statements is true regarding soft tissue sarcomas:
1
Soft tissue sarcomas frequently metastasize to bone.
2
Patients with soft tissue sarcomas of the hand have worse prognosis than patients with similar tumors in other extremities.
3
Soft tissue sarcomas present as a painful mass in the hand.
4
Overall prognosis is better with radical resection than wide excision.
5
Soft tissue sarcomas can be "shelled out".
Soft tissue sarcomas in the hand present as painless lesions, do not metastasize to bone, and although local control is better with radical resection, there is no improvement in overall survival when compared to wide excision. Soft tissue sarcomas should not be "shelled out."
QUESTION 14 OF 50
As the most direct and predictable preoperative diagnostiCtest for hip infection, the false-positive rate for hip aspiration is:
1
0%
2
0% to 15%
3
15% to 25%
4
25% to 40%
5
40% to 50%
Hip aspiration has a false-positive rate of 0% to 15%. Many authors have warned against its routine use before revision surgery
QUESTION 15 OF 50
of 100
A 4-year-old girl who has midlumbar myelomeningocele and hydrocephalus is being evaluated for her uneven gait. A hip examination reveals a right hip dislocation. Bilateral hips are pain-free with full range of motion and no fixed deformity. What is the most appropriate course of action?
A 4-year-old girl who has midlumbar myelomeningocele and hydrocephalus is being evaluated for her uneven gait. A hip examination reveals a right hip dislocation. Bilateral hips are pain-free with full range of motion and no fixed deformity. What is the most appropriate course of action?
1
Obtain standing AP pelvis to evaluate the hips; plan open reduction of the right hip when the patient starts having hip pain
2
Obtain supine AP pelvis to evaluate the hips; plan open reduction of the right hip as soon as possible
3
Inform the family that the dislocated hip will not limit the ability to ambulate and will not benefit from reduction
4
Inform the family that the patient's ambulatory potential is poor due to the hip dislocation, which cannot be treated successfully
■
A child with midlumbar myelomeningocele, without other lesions, would be expected to have the ability to ambulate, though delayed. She has a high likelihood of hip dislocations because of lack of function of the abductor muscles. The presence or absence of hip dislocation does not affect ambulatory ability; the child is already walking. The best course of action is education of the family and therapist as to the minimal effect that a hip dislocation has in these patients. A shoe lift or brace buildup can address leg length discrepancy; in a hip without contractures, no other treatment is needed.
Radiographs are unnecessary in the management of the hip dislocation in myelomeningocele. Surgery has been shown to convert supple, painless dislocated hips into stiff, painful hips that have a high likelihood of redislocation. Though the dislocation is not recommended for treatment, this does not preclude the ability to safely ambulate and undergo therapy, which is not harmful to the condition.
A child with midlumbar myelomeningocele, without other lesions, would be expected to have the ability to ambulate, though delayed. She has a high likelihood of hip dislocations because of lack of function of the abductor muscles. The presence or absence of hip dislocation does not affect ambulatory ability; the child is already walking. The best course of action is education of the family and therapist as to the minimal effect that a hip dislocation has in these patients. A shoe lift or brace buildup can address leg length discrepancy; in a hip without contractures, no other treatment is needed.
Radiographs are unnecessary in the management of the hip dislocation in myelomeningocele. Surgery has been shown to convert supple, painless dislocated hips into stiff, painful hips that have a high likelihood of redislocation. Though the dislocation is not recommended for treatment, this does not preclude the ability to safely ambulate and undergo therapy, which is not harmful to the condition.
QUESTION 16 OF 50
Biomechanical in vitro studies of double-row anchor fixation of rotator cuff tears show what initial advantage over single-row anchor fixation?
1
Increased peak-to-peak elongation
2
Decreased stiffness
3
Higher ultimate tensile load
4
Decreased contact area
5
Increased conditioning elongation
DISCUSSION: Biomechanical in vitro studies of double-row fixation of rotator cuff tears during cyclic loading and tensile loading to failure have demonstrated that double-row fixation results in a higher ultimate tensile load when compared to single-row fixation. Peak-to-peak elongation, stiffness, and conditioning
elongation for double-row fixation were all similar to single-row fixation. These initial findings, however, may or may not lead to improved clinical outcomes.
REFERENCES: Ma CB, Comerford L, Wilson J, et al: Biomechanical evaluation of arthroscopic rotator cuff repairs: Double-row compared with single-row fixation. J Bone Joint Surg Am 2006;88:403-410. Kim DH, El
Attrache NS, Tibone JE, et al: Biomechanical comparison of single-row versus double-row suture anchor technique for rotator cuff repair. Am J Sports Med 2006;34:407-414.
elongation for double-row fixation were all similar to single-row fixation. These initial findings, however, may or may not lead to improved clinical outcomes.
REFERENCES: Ma CB, Comerford L, Wilson J, et al: Biomechanical evaluation of arthroscopic rotator cuff repairs: Double-row compared with single-row fixation. J Bone Joint Surg Am 2006;88:403-410. Kim DH, El
Attrache NS, Tibone JE, et al: Biomechanical comparison of single-row versus double-row suture anchor technique for rotator cuff repair. Am J Sports Med 2006;34:407-414.
QUESTION 17 OF 50
Which of the following tumor metastasizes to lungs:
1
Squamous cell carcinoma
2
Basal cell carcinoma
3
Soft tissue sarcoma
4
Schwannoma
5
Actinic keratosis
Squamous cell carcinoma and basal cell carcinoma do not commonly metastasize to the lungs. Actinic keratoses are premalignant lesions that progress into squamous cell carcinomas. Schwannomas are common benign nerve tumors.
QUESTION 18 OF 50
Which of the following factors predisposes patients undergoing lateral ankle reconstruction to surgical failure?
1
Low functional demand
2
Anatomic reconstruction
3
Cavovarus foot deformity
4
Planovalgus foot deformity
5
History of acute instability (preoperative)
Bony malalignment such as hindfoot varus, first ray plantar flexion, or cavovarus foot deformity renders patients more susceptible to chronic lateral ankle sprains and can cause failure of isolated lateral ankle reconstruction. Planovalgus foot deformity principally strains the medial ankle ligamentous structures. Low functional demand patients, as well as patients with a preoperative history of acute traumatic ankle instability and patients undergoing anatomic reconstruction all have decreased rates of surgical failure with lateral ankle ligament reconstruction.
QUESTION 19 OF 50
Which of the following has been associated with an increased likelihood of stress shielding after cementless total hip arthroplasty?
1
Use of titanium alloy femoral components
2
Use of proximally fixed femoral components
3
Use of distally fixed femoral components
4
Use of press-fit stems in patients with narrow intramedullary canals
5
Use of plasma sprayed components
DISCUSSION: Although stress shielding has not been associated with adverse clinical outcomes to date, it is a commonly observed process after cementless total hip arthroplasty. Factors that increase the magnitude of stress shielding include the use of distally fixed cobalt-chrome stems, particularly in patients with osteoporosis. Large diameter femoral components (larger than 18 mm in diameter) have also been associated with an increased prevalence of stress shielding.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
QUESTION 20 OF 50
of 100
Staging for patients with this diagnosis necessitates which study or studies?
Staging for patients with this diagnosis necessitates which study or studies?
1
CT scan of the chest and a bone scan
2
Skeletal survey
3
Bone marrow aspirate
4
Bone marrow biopsy
- CT scan of the chest and a bone scan_
QUESTION 21 OF 50
Which of the following abnormalities has been observed in a higher than expected frequency in patients with metal-on-metal hip bearings?

1
Renal cell carcinoma
2
Leukocyte chromosomal aberrations
3
Carcinomas of the gastrointestinal tract
4
Soft-tissue sarcomas
5
Thyroid carcinoma
Metal-on-metal hip bearings have been associated with very low rates of wear and are commonly used in North America and Europe. Patients with these bearings have higher levels of metal ions (particularly cobalt and chromium) in the bloodstream than patients with bearings made of other materials. Although many researchers have been concerned that these ions may predispose to cancer, there has been no evidence that patients with metal-on-metal bearings are developing sarcomas or carcinomas with higher frequency than the general population. However, there has been mixed data as to whether hematopoietic malignancies are slightly more prevalent in patients with metal-on-metal bearings. Two recent reports have found chromosomal abnormalities, such as translocations and aneuploidy, to be increased in patients with metal-on-metal hip bearings. The clinical consequences of these changes, if any, remain unknown.
REFERENCES: Dunstan E, Ladon D, Whittingham-Jones P, et al: Chromosomal aberrations in the peripheral blood of patients with metal-on-metal hip bearings. J Bone Joint Surg Am 2008;90:517-522. Ladon D, Doherty A, Newson R, et al: Changes in metal levels and chromosome aberrations in the peripheral blood of patients after metal-on-metal hip arthroplasty. J Arthroplasty 2004:19:78-83.
Visuri T, Pukkala E, Paavolainen P, et al: Cancer risk after metal on metal and polyethylene on metal total hip
arthroplasty. Clin Orthop Relat Res 1996:329:S280-S289. Question 61
A 73-year-old woman with a history of type II diabetes mellitus undergoes a total hip arthroplasty for osteoarthritis. She continues to have serosanguinous wound drainage from the midportion of the incision 12 days after surgery. What is the most appropriate treatment at this time?
1. Return to the operating room for debridement and irrigation with removal of all implants and immediate reimplantation
2. Return to the operating room for open debridement and irrigation, exchange of the polyethylene
insert, followed by appropriate antibiotics based on intraoperative culture results
3. Hip spica pressure dressing and a 2-week course of oral antibiotics
4. Hip aspiration for culture, followed by a 2-week course of appropriate IV antibiotics based on
culture results
5. Hip aspiration for culture, followed by a 6-week course of appropriate IV antibiotics based on culture results
PREFERRED RESPONSE: 2
DISCUSSION: This patient has an acute postoperative deep infection, with prolonged drainage at 12 days postoperatively. Even without other signs or symptoms of infection, the prolonged drainage this far out after surgery is concerning for an acute postoperative infection. The most appropriate treatment at this point is open debridement with retention of the implants. Modular parts, if present, are exchanged. Oral or IV antibiotics alone are generally inadequate to treat the infection, and this form of management alone would result in a missed opportunity to potentially cure the infection. Removal of all implants at this point is not required because early aggressive debridement within the first 2 weeks after surgery offers a reasonable outcome. After 4 to 6 weeks of symptoms, results of debridement are less favorable and removal of the implants is usually required.
REFERENCES: Crockarell JR, Hanssen AD, Osmon DR, et al: Treatment of infection with debridement and retention of the components following hip arthroplasty. J Bone Joint Surg Am 1998;80:1306-1313. Hanssen AD, Osmon DR: Assessment of patient selection criteria for treatment of the infected hip arthroplasty. Clin Orthop Relat Res 2000;381:91 -100.
Figure 62
REFERENCES: Dunstan E, Ladon D, Whittingham-Jones P, et al: Chromosomal aberrations in the peripheral blood of patients with metal-on-metal hip bearings. J Bone Joint Surg Am 2008;90:517-522. Ladon D, Doherty A, Newson R, et al: Changes in metal levels and chromosome aberrations in the peripheral blood of patients after metal-on-metal hip arthroplasty. J Arthroplasty 2004:19:78-83.
Visuri T, Pukkala E, Paavolainen P, et al: Cancer risk after metal on metal and polyethylene on metal total hip
arthroplasty. Clin Orthop Relat Res 1996:329:S280-S289. Question 61
A 73-year-old woman with a history of type II diabetes mellitus undergoes a total hip arthroplasty for osteoarthritis. She continues to have serosanguinous wound drainage from the midportion of the incision 12 days after surgery. What is the most appropriate treatment at this time?
1. Return to the operating room for debridement and irrigation with removal of all implants and immediate reimplantation
2. Return to the operating room for open debridement and irrigation, exchange of the polyethylene
insert, followed by appropriate antibiotics based on intraoperative culture results
3. Hip spica pressure dressing and a 2-week course of oral antibiotics
4. Hip aspiration for culture, followed by a 2-week course of appropriate IV antibiotics based on
culture results
5. Hip aspiration for culture, followed by a 6-week course of appropriate IV antibiotics based on culture results
PREFERRED RESPONSE: 2
DISCUSSION: This patient has an acute postoperative deep infection, with prolonged drainage at 12 days postoperatively. Even without other signs or symptoms of infection, the prolonged drainage this far out after surgery is concerning for an acute postoperative infection. The most appropriate treatment at this point is open debridement with retention of the implants. Modular parts, if present, are exchanged. Oral or IV antibiotics alone are generally inadequate to treat the infection, and this form of management alone would result in a missed opportunity to potentially cure the infection. Removal of all implants at this point is not required because early aggressive debridement within the first 2 weeks after surgery offers a reasonable outcome. After 4 to 6 weeks of symptoms, results of debridement are less favorable and removal of the implants is usually required.
REFERENCES: Crockarell JR, Hanssen AD, Osmon DR, et al: Treatment of infection with debridement and retention of the components following hip arthroplasty. J Bone Joint Surg Am 1998;80:1306-1313. Hanssen AD, Osmon DR: Assessment of patient selection criteria for treatment of the infected hip arthroplasty. Clin Orthop Relat Res 2000;381:91 -100.
Figure 62
QUESTION 22 OF 50
The gold standard for diagnosis of lateral epicondylitis is considered:
1
History and physical examination
2
Plain radiographs
3
Electromyography
4
Magnetic resonance imaging
5
Radionuclear bone scan
The clinical diagnosis of lateral epicondylitis is supported by specific provocative tests. The gold standard for diagnosis is the history and physical examination. Tenderness on examination is localized to the lateral epicondyle, which can radiate into the forearm; the area of maximum tenderness is approximately 2 mm to 5 mm distal and anterior to the midpoint of the lateral epicondyle. There is usually a history of overuse or of a repetitive activity. The pain is aggravated, with the elbow extended, by resisted wrist and finger extension or with passive finger and wrist flexion.
QUESTION 23 OF 50
of 100
The idiopathic form of this condition may be associated with
The idiopathic form of this condition may be associated with
1
absence of the anterior tibial artery.
2
absence of the fibula.
3
duplication of the first ray.
4
postaxial polydactyly.
- absence of the anterior tibial artery.
QUESTION 24 OF 50
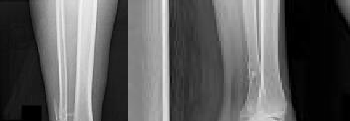
1251) A 25-year-old male involved in a motor vehicle accident sustains multiple injuries. He undergoes operative treatment for his humeral shaft fracture. Figures A and B show his preoperative and postoperative radiographs. The distal interlocks for this implant place which of the following nerves at risk?


1
Radial
2
Ulnar
3
Anterior interosseous
4
Axillary
5
Musculocutaneous
With intramedullary (IM) nailing of the humerus, the distal anterior-to-posterior interlocking screws place the musculocutaneous nerve at high risk for injury as it goes through the coracobrachialis muscle and courses anteriorly along the brachialis (of which it innervates the medial half).
Rupp et al performed a cadaveric study with IM nails utilizing either lateral-to-medial or anterior-to-posterior distal interlocking screws. They showed that anterior-to-posterior screws placed the musculocutaneous nerve at high risk, while lateral-to-medial screws placed the radial nerve at high risk as it courses laterally distally along the humerus.
Rupp et al performed a cadaveric study with IM nails utilizing either lateral-to-medial or anterior-to-posterior distal interlocking screws. They showed that anterior-to-posterior screws placed the musculocutaneous nerve at high risk, while lateral-to-medial screws placed the radial nerve at high risk as it courses laterally distally along the humerus.
QUESTION 25 OF 50
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
1
Brachial artery
2
Median nerve
3
Posterior interosseous nerve
4
Lateral antebrachial cutaneous nerve
5
Antecubital vein
The most commonly injured neurovascular structure during an anterior approach for the repair of a distal biceps tendon rupture is the lateral antebrachial cutaneous nerve. This structure is located lateral to the biceps tendon and in a superficial location just deep to the subcutaneous layer. The antecubital vein is medial and superficial with the brachial artery and median nerve also medial to the biceps tendon but deep to the common flexors. The posterior interosseous nerve is deep within the supinator muscle and can be injured in the deep dissection or through the posterior approach when using a two-incision approach.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
QUESTION 26 OF 50
What is the post-amplification product of reverse transcription polymerase chain reaction (RT-PCR)?
1
RNA
2
DNA
3
Protein
4
Mitochondria
5
Immunoglobulins
#
**
Reverse transcription polymerase chain reaction (RT-PCR) is a variant of polymerase chain reaction (PCR) used in molecular biology to generate many copies of a DNA sequence from fragments of RNA. The RNA strand is first reverse transcribed into its DNA complement, followed by amplification of the resulting DNA using polymerase chain reaction. Polymerase chain reaction amplifies short segments of DNA by using the temperature stable DNA polymerase enzyme.
Reverse transcription polymerase chain reaction (RT-PCR) is a variant of polymerase chain reaction (PCR) used in molecular biology to generate many copies of a DNA sequence from fragments of RNA. The RNA strand is first reverse transcribed into its DNA complement, followed by amplification of the resulting DNA using polymerase chain reaction. Polymerase chain reaction amplifies short segments of DNA by using the temperature stable DNA polymerase enzyme.
QUESTION 27 OF 50
Injuries to the central articular disk portion of the triangular fibrocartilage complex are related to all of the following except:
1
Age
2
Positive ulnar variance
3
Ulnocarpal impingement
4
Scaphoid nonunion
5
Avulsion injuries from the dorsal ligamentous attachments
Scaphoid nonunion is not related to central triangular fibrocartilage complex injuries. A positive ulnar variance is most strongly associated with triangular fibrocartilage complex central disk injuries.
QUESTION 28 OF 50
Which of the following may be beneficial in decreasing the deleterious effects of total muscle ischemia in a patient who has a compartment syndrome:
1
Systemic steroids
2
Hypothermia
3
Elevation of the extremity above the heart
4
Antihypertensive therapy
5
Anticoagulant therapy
Aside from performing a fasciotomy, little can be done for patients with a compartment syndrome. Hypothermia, systemic corticosteroids, and anticoagulation therapy may increase muscle tolerance to ischemia.
Steroids and anticoagulation are not reasonable options because there is an impaired blood supply to the muscle (ie, these agents cannot enter the muscle). Hypothermia can be used to gain some time if immediate fasciotomy cannot be performed.
Steroids and anticoagulation are not reasonable options because there is an impaired blood supply to the muscle (ie, these agents cannot enter the muscle). Hypothermia can be used to gain some time if immediate fasciotomy cannot be performed.
QUESTION 29 OF 50
of 100
A 71-year-old man with long-standing ankle arthrosis who has previously had a subtalar fusion (Figure 42).

A 71-year-old man with long-standing ankle arthrosis who has previously had a subtalar fusion (Figure 42).
1
Tibial and/or fibular osteotomy with open reduction and internal fixation (ORIF)
2
Ankle distraction arthroplasty
3
Ankle fusion
4
Total ankle arthroplasty (TAA)

- Total ankle arthroplasty (TAA)_
QUESTION 30 OF 50
Isolated subtalar fusion:
1
Is not associated with development of ankle or transverse tarsal joint arthritis
2
Is associated only with development of transverse joint arthritis, but the ankle joint is spared
3
Is associated only with development of ankle arthritis, but the transverse tarsal joints are spared
4
Is associated with the development of both ankle and transverse tarsal joint arthritis
5
Is associated with knee joint degenerative arthritis
In 48 subtalar fusions followed for 5 years, 36% of patients developed ankle arthritis and 41% of patients developed transverse tarsal joint arthritis.
QUESTION 31 OF 50
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic reduction best assessed intra-operatively?
---

Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic reduction best assessed intra-operatively?
---
1
By comparing tibiofibular overlap with population norms
2
By comparing tibiofibular clear space with population norms
3
By comparing images with the patient’s contralateral uninjured side
4
By measuring the talocrural angle
The radiographs reveal a trimalleolar ankle fracture dislocation with an associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
9. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
10. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
11. Maximizes the surface area for ankle joint loading
12. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
9. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
10. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
11. Maximizes the surface area for ankle joint loading
12. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
QUESTION 32 OF 50
In comparing high tibial osteomtomy to unicondylar knee arthroplasty (UKA):
1
Patients with high tibial osteotomy recover faster than patients with UKA.
2
High tibial osteotomy has better 10-year results than UKA.
3
High tibial osteotomy has better early results than UKA.
4
High tibial osteotomy is better for patients who work as heavy laborers.
5
High tibial osteotomy has fewer operative complications than UKA.
Although a successful UKA can eliminate pain and improve the patientâs function, heavy labor and high impact athletiCactivities are not encouraged. High tibial osteotomy allows a patient to perform more aggressive activities
QUESTION 33 OF 50
If the structure marked by the tip of the probe in Figure 94 is repaired to the bony glenoid with suture anchors
during an arthroscopic stabilization procedure, what is the most likely result?
during an arthroscopic stabilization procedure, what is the most likely result?
1
Loss of external rotation with the glenohumeral joint abducted 90 degrees
2
Loss of external rotation with the arm at the side of the body
3
Loss of internal rotation with the glenohumeral joint abducted 90 degrees
4
Loss of internal rotation up the back
5
Loss of flexion
DISCUSSION: The probe is on the middle glenohumeral ligament (MGHL), which, in this case, is a cordlike and robust structure, commonly known as a Buford complex. The space between the bony glenoid and the MGHL (in this case, a cord-like Buford complex) is a normal variant and should not be repaired or tightened to the bony glenoid with a soft-tissue anchor or other repair. If this structure is inadvertently repaired, the most common scenario is loss of external rotation with the arm at the side, as the MGHL/ Buford complex becomes tight with the arm in this position. The loss of external rotation is more pronounced with the arm at the side than abducted at 90 degrees as the MGHL/Buford complex becomes tighter with the arm at the side than abducted.
REFERENCES: Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Ide J, Maeda S, Takagi K: Normal variations of the glenohumeral ligament complex: An anatomic study for arthroscopic Bankart repair. Arthroscopy 2004;20:164-168.
Gerber C, Werner CM, Macy JC, et al: Effect of selective capsulorrhaphy on the passive range of motion of
the glenohumeral joint. J Bone Joint Surg Am 2003;85:48-55. Question 95
What allograft has the highest antigenicity when used for ligament reconstruction about the knee?
1. #### Tibialis anterior used for anterior cruciate ligament (ACL) reconstruction
2. #### Tibialis anterior used for posterolateral reconstruction
3. #### Bone-patellar tendon-bone used for ACL reconstruction
4. #### Semitendinosus used for posterior cruciate ligament reconstruction
5. #### Semitendinosus used for medial collateral ligament reconstruction PREFERRED RESPONSE: 3
DISCUSSION: Although theoretically the intra-articular environment is slightly more immune privileged, the role of immunogenicity is related more to bone than soft tissue. Therefore, the bone-patellar tendon- bone used for ACL reconstruction would have the highest risk of immunogenicity if storage techniques and harvest techniques were similar. This also is true for bone plugs associated with meniscal allografts.
REFERENCES: Rodeo SA, Seneviratne A, Suzuki K, et al: Histological analysis of human meniscal allografts: Apreliminary report. J Bone Joint Surg Am 2000;82:1071-1082.
West RV, Hamer CD: Graft selection in anterior cruciate ligament reconstruction. J Am Acad Orthop Surg
2005;13:197-207.
REFERENCES: Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Ide J, Maeda S, Takagi K: Normal variations of the glenohumeral ligament complex: An anatomic study for arthroscopic Bankart repair. Arthroscopy 2004;20:164-168.
Gerber C, Werner CM, Macy JC, et al: Effect of selective capsulorrhaphy on the passive range of motion of
the glenohumeral joint. J Bone Joint Surg Am 2003;85:48-55. Question 95
What allograft has the highest antigenicity when used for ligament reconstruction about the knee?
1. #### Tibialis anterior used for anterior cruciate ligament (ACL) reconstruction
2. #### Tibialis anterior used for posterolateral reconstruction
3. #### Bone-patellar tendon-bone used for ACL reconstruction
4. #### Semitendinosus used for posterior cruciate ligament reconstruction
5. #### Semitendinosus used for medial collateral ligament reconstruction PREFERRED RESPONSE: 3
DISCUSSION: Although theoretically the intra-articular environment is slightly more immune privileged, the role of immunogenicity is related more to bone than soft tissue. Therefore, the bone-patellar tendon- bone used for ACL reconstruction would have the highest risk of immunogenicity if storage techniques and harvest techniques were similar. This also is true for bone plugs associated with meniscal allografts.
REFERENCES: Rodeo SA, Seneviratne A, Suzuki K, et al: Histological analysis of human meniscal allografts: Apreliminary report. J Bone Joint Surg Am 2000;82:1071-1082.
West RV, Hamer CD: Graft selection in anterior cruciate ligament reconstruction. J Am Acad Orthop Surg
2005;13:197-207.
QUESTION 34 OF 50
The incidence of patella component loosening is:
1
4%
2
10%
3
2%
4
8%
5
15%
The incidence of patella component loosening is less than 2%. Factors predisposing to loosening include cementation into deficient bone, component malposition, patellar subluxation or fracture, patellar avascular necrosis, asymmetriCpatellar bone resection, and loosening of other components. Treatment options include observation, component revision, patellectomy or component removal, and patellar arthroplasty if bone stock is sufficient
QUESTION 35 OF 50
of 100
If the patient had an isolated spine injury without neurologic deficit, the most appropriate next step would be
If the patient had an isolated spine injury without neurologic deficit, the most appropriate next step would be
1
anterior corpectomy with percutaneous pedicle screw stabilization.
2
percutaneous pedicle screw stabilization.
3
posterior pedicle screw stabilization with fusion.
4
MRI.
The treatment of thoracolumbar burst fractures has evolved over the years. In the absence of a neurologic deficit or a posterior ligamentous complex injury, nonsurgical treatment is as effective as surgery. The degree of spinal canal compromise is not a risk factor for neurologic symptoms. Similarly, although kyphosis may be a marker of more significant injury, the degree of kyphosis does not correlate with chronic pain. In the setting of a burst fracture, MRI can be used to evaluate the integrity of the posterior ligamentous complex. Polytrauma may be considered a relative indication for surgical intervention in the setting of a stable burst fracture.
RECOMMENDED READINGS
[Rechtine GR 2nd. Nonoperative management and treatment of spinal injuries. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S22-7; discussion S36. Review. PubMed PMID: 16685232. ](http://www.ncbi.nlm.nih.gov/pubmed/16685232)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16685232)
[Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999 Feb 15;24(4):412-5. PubMed PMID: 10065527. ](http://www.ncbi.nlm.nih.gov/pubmed/10065527)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10065527)
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. doi: 10.1016/j.spinee.2012.10.041. Review. PubMed PMID: 24332321.](http://www.ncbi.nlm.nih.gov/pubmed/24332321)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24332321)
RECOMMENDED READINGS
[Rechtine GR 2nd. Nonoperative management and treatment of spinal injuries. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S22-7; discussion S36. Review. PubMed PMID: 16685232. ](http://www.ncbi.nlm.nih.gov/pubmed/16685232)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16685232)
[Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999 Feb 15;24(4):412-5. PubMed PMID: 10065527. ](http://www.ncbi.nlm.nih.gov/pubmed/10065527)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10065527)
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. doi: 10.1016/j.spinee.2012.10.041. Review. PubMed PMID: 24332321.](http://www.ncbi.nlm.nih.gov/pubmed/24332321)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24332321)
QUESTION 36 OF 50
In which of the following osteonecrotiCconditions does the marrow cavity become packed with abnormal cells:
1
Caisson disease
2
Gaucher disease
3
Renal transplantation
4
Pancreatitis
5
ChroniCcorticosteroid administration
There are two conditions that cause osteonecrosis secondary to the marrow cavity becoming packed with abnormal cells â
Gaucher disease and sickle cell disease. There is probable occlusion of the intraosseous arteries with both of these conditions.
With Gaucher disease, the marrow cavity is filled with Gaucher cells (macrophages filled with cerebroside). In sickle cell disease, the marrow cavity is filled with sickled red blood cells.
Gaucher disease and sickle cell disease. There is probable occlusion of the intraosseous arteries with both of these conditions.
With Gaucher disease, the marrow cavity is filled with Gaucher cells (macrophages filled with cerebroside). In sickle cell disease, the marrow cavity is filled with sickled red blood cells.
QUESTION 37 OF 50
Early postoperative infections following primary total hip arthroplasty are most likely caused by which
organism?
organism?
1
Staphylococcus epidermidis
2
Streptococcus viridans
3
Propionibacterium acnes
4
Staphylococcus aureus
S aureus is the most common organism cultured in early (fewer than 4 weeks postoperative) periprosthetic infections. Methicillin-resistant S aureus is becoming a more common pathogen in certain patient populations. B hemolytic Streptococcus and some gram-negative infections can also be found in early postoperative infections. S epidermidis, S viridans, and P acnes are more commonly found in late (more
than 4 weeks postoperative) infections.
than 4 weeks postoperative) infections.
QUESTION 38 OF 50
The most common pathogen causing septic arthritis in the hand is:
1
Staphylococcus aureus
2
Streptococci
3
Haemophilus influenzae
4
Mix of gram-negative and gram-positive organisms
5
Atypical mycobacterium
Staphylococcus aureus is the most common pathogen that causes septic arthritis in the hand. The second most common pathogen is streptococcus species infections, which are often the result of trauma. Treatment includes incision and drainage with copius irrigation.
QUESTION 39 OF 50
of 100
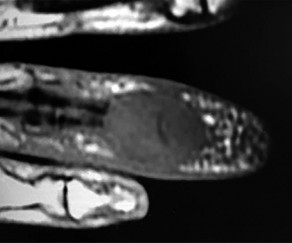
Figures 31a through 31d are the radiographs and MR images of a 52-year-old man who has a 7-week history of right ring finger pain, redness, and swelling. He accidentally stuck his finger with a toothpick 1 week before developing symptoms. There is purulent drainage from the puncture wound site. He was treated with oral antibiotics for 10 days and intravenous (IV) antibiotics for 3 weeks before being seen. Initial cultures grew _Eikenella corrodens_. What is/are the best next step(s)?



Figures 31a through 31d are the radiographs and MR images of a 52-year-old man who has a 7-week history of right ring finger pain, redness, and swelling. He accidentally stuck his finger with a toothpick 1 week before developing symptoms. There is purulent drainage from the puncture wound site. He was treated with oral antibiotics for 10 days and intravenous (IV) antibiotics for 3 weeks before being seen. Initial cultures grew _Eikenella corrodens_. What is/are the best next step(s)?
1
Continued IV antibiotics for 4 weeks
2
Bone scan followed by biopsy of the region
3
Drainage of the abscess with debridement of bone and soft tissue
4
Amputation through the distal interphalangeal (DIP) joint
This patient had a septic DIP joint that was treated with antibiotics alone. As a result, he developed osteomyelitis with bone destruction and an abscess. The correct answer is debridement of both bone and soft tissue with abscess drainage. Antibiotic treatment without surgery would not successfully eliminate this infection. A bone scan and biopsy are not appropriate because this problem is an infection and not a tumor, and the MR imaging provided enough diagnostic information. Amputation is not indicated prior to an attempt to salvage the digit. Amputation through the DIP joint would not remove the infected bone in the middle phalanx and would provide an inadequate level of resection.
RECOMMENDED READINGS
5. [Robinson LG, Kourtis AP. Tale of a toothpick: Eikenella corrodens osteomyelitis. Infection. 2000 Sep;28(5):332-3. PubMed PMID: 11073145. ](http://www.ncbi.nlm.nih.gov/pubmed/11073145)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11073145)
6. [Cuenca-Estrella M, Ramos JM, Esteban J, Soriano F, Vallejo JV. Eikenella corrodens thumb osteomyelitis. Postgrad Med J. 1996 Mar;72(845):188.](http://www.ncbi.nlm.nih.gov/pubmed/8731720)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8731720)
7. [Schmidt DR, Heckman JD. Eikenella corrodens in human bite infections of the hand. J Trauma. 1983 Jun;23(6):478-82. PubMed PMID: 6345799. ](http://www.ncbi.nlm.nih.gov/pubmed/%206345799)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%206345799)
8. [Rayan GM, Putnam JL, Cahill SL, Flournoy DJ. Eikenella corrodens in human mouth flora. J Hand Surg Am. 1988 Nov;13(6):953-6. PubMed PMID: 3066818. ](http://www.ncbi.nlm.nih.gov/pubmed/3066818)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3066818)
RECOMMENDED READINGS
5. [Robinson LG, Kourtis AP. Tale of a toothpick: Eikenella corrodens osteomyelitis. Infection. 2000 Sep;28(5):332-3. PubMed PMID: 11073145. ](http://www.ncbi.nlm.nih.gov/pubmed/11073145)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11073145)
6. [Cuenca-Estrella M, Ramos JM, Esteban J, Soriano F, Vallejo JV. Eikenella corrodens thumb osteomyelitis. Postgrad Med J. 1996 Mar;72(845):188.](http://www.ncbi.nlm.nih.gov/pubmed/8731720)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8731720)
7. [Schmidt DR, Heckman JD. Eikenella corrodens in human bite infections of the hand. J Trauma. 1983 Jun;23(6):478-82. PubMed PMID: 6345799. ](http://www.ncbi.nlm.nih.gov/pubmed/%206345799)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%206345799)
8. [Rayan GM, Putnam JL, Cahill SL, Flournoy DJ. Eikenella corrodens in human mouth flora. J Hand Surg Am. 1988 Nov;13(6):953-6. PubMed PMID: 3066818. ](http://www.ncbi.nlm.nih.gov/pubmed/3066818)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3066818)
QUESTION 40 OF 50
of 100
Which 2 tendons are identified in the dissection shown in Video 92?
Which 2 tendons are identified in the dissection shown in Video 92?
1
Semitendinosus and gracilis
2
Semitendinosus and semimembranosus
3
Semimembranosus and gracilis
4
Semimembranosus and sartorius
- Semitendinosus and gracilis
The demonstration in Video 92 shows the tendons of the semitendinosus and gracilis muscles. They insert on the tibia deep to the sartorial fascia. The semimembranosus inserts more proximal and posterior on the tibia.
RECOMMENDED READINGS
1. Babb JR, Detterline AJ, Noyes FR. AAOS Orthopaedic Video Theater. The Key to the Knee: A Layer-by-Layer Video Demonstration of Medial and Anterior Anatomy. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009.
2. Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:493-568.
The demonstration in Video 92 shows the tendons of the semitendinosus and gracilis muscles. They insert on the tibia deep to the sartorial fascia. The semimembranosus inserts more proximal and posterior on the tibia.
RECOMMENDED READINGS
1. Babb JR, Detterline AJ, Noyes FR. AAOS Orthopaedic Video Theater. The Key to the Knee: A Layer-by-Layer Video Demonstration of Medial and Anterior Anatomy. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009.
2. Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:493-568.
QUESTION 41 OF 50
Optimal treatment for a symptomatic ganglion is:
1
Observation
2
C losed rupture
3
Aspiration
4
Surgical excision
5
C orticosteroid injection
Surgical excision of a symptomatic ganglion, with removal of the entire ganglion stalk and a portion of the joint capsule at its base, reliably relieves pain and has a low recurrence rate (approximately 5%). C losed rupture, while potentially effective, has a recurrence rate of approximately 50%. Ganglions are prone to recur after aspiration, although 3 serial aspirations of a ganglion have been shown to reduce the recurrence rate to about 15%. The addition of corticosteroids to aspiration treatment has not been shown to provide any additional benefit. While observation of painless ganglions is certainly acceptable treatment given their benign prognosis, it is not considered the optimal course for a symptomatic lesion.
QUESTION 42 OF 50
Opioids must be used with caution in infants younger than 3 months of age because of which of the following properties:
1
Increased clearance
2
Increased protein binding
3
Increased hepatic activity
4
Decreased clearance and protein binding
5
Decreased body surface area to mass
Opioids must be used with caution in infants younger than 3 months of age because of decreased clearance and decreased protein binding. This results in greater bioavailability.
QUESTION 43 OF 50
Which of the following is the most common final attribution of back pain in children and adolescents after all appropriate diagnostic studies are performed:
1
Spondylolysis
2
Osteoid osteoma
3
Infection
4
Herniated nucleus pulposus
5
No identifiable cause
The majority of children and adolescents do not have an identifiable cause of back pain after all appropriate tests are performed. Many times the diagnosis is "musculo-ligamentous strain." the most common identified cause is spondylolysis.
QUESTION 44 OF 50
A 65-year-old woman with a history of diabetes mellitus and plantar ulcers has an erythematous and swollen right foot and ankle. Despite IV antibiotics, the erythema spreads to her lower calf within 24 hours. She has a systolic blood pressure of 80/55 mm Hg and a pulse rate of 120. Laboratory studies show a creatinine level of 1.5 mg. Initial management should consist of
1
continued IV antibiotics and observation.
2
hyperbaric oxygen treatment.
3
rapid IV fluid boluses.
4
surgical debridement.
5
whirlpool therapy.
Necrotizing fasciitis is an aggressive and rapidly spreading soft-tissue infection, usually caused by group A beta-hemolytic Streptococcus pyogenes. Presentation is typical of a rapidly ascending cellulitis, recalcitrant to antibiotic treatment. Differentiation between cellulitis and impetigo is difficult, and success depends on a high level of suspicion. The skin and subcutaneous tissues are affected, with sparing of the muscles. Septic shock and multi-organ system failure can be fatal. Treatment is aggressive surgical debridement with broad-spectrum antibiotics. Repeat irrigation and debridement may be necessary. Hyperbaric oxygen studies have shown inconsistent results.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 199-205.
Fontes RA Jr, Ogilvie CM, Miclau T: Necrotizing soft-tissue infections. J Am Acad Orthop Surg 2000;8:151-158.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 199-205.
Fontes RA Jr, Ogilvie CM, Miclau T: Necrotizing soft-tissue infections. J Am Acad Orthop Surg 2000;8:151-158.
QUESTION 45 OF 50
What is the best treatment option for complex proximal humerus fractures in the
low-demand patient population?

low-demand patient population?
1
Hemiarthroplasty
2
Reverse total shoulder arthroplasty
3
Locked-plate fixation
4
Nonoperative treatment
In the recent meta-analysis by Mao and associates, there was no evidence to support the use of any of the operative modalities to treat 3- and 4-part fractures of the proximal humerus in low-demand patients. Although surgeons and patients will differ in their treatment algorithms, the recent meta-analysis showed lower complications with nonoperative treatment for these complex fractures. New treatment modalities involving fibular strut allograft, reverse total shoulder arthroplasty for elderly patients with an incompetent rotator cuff, and locked-plate fixation may prove to be superior to nonoperative treatment in select patient populations. However, not one operation has been shown to be superior to nonoperative treatment in the low-demand patient population with complex proximal humerus fractures.
**Question 15of 100**
**CLINICAL SITUATION**
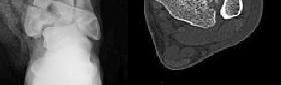
Figure 1 is the radiograph and Figure 2 is the CT image of a 45-year-old woman who fell about 20 feet off her balcony. These images show an isolated, open injury with a 3-cm open medial wound.
The best delayed definitive surgical fixation plan would include
---
1. lateral plating of the fibula and a percutaneous medial column plate.
2. intramedullary fixation of the fibula and an anterolateral tibial plate.
3. open medial column plating, percutaneous screw fixation of the joint, and lateral fibular plating.
4. screw fixation of the medial column with an anterolateral tibial plate and lateral fibular plating
Answer: D
Discussion: The timely administration of antibiotics has been shown to be the best initial treatment to reduce the incidence of infection following an open fracture. Life threatening injuries must first be addressed. But in this isolated open pilon fracture, antibiotics should be initiated early along with tetanus prophylaxis. Reduction and splinting would stabilize the fracture but these interventions should follow antibiotic coverage. Emergency department irrigation is controversial. Closed reduction and splinting, external fixation, CT scan, and delayed open reduction internal fixation would be the preferred sequence of management. External fixation to provide provisional limb stabilization would be indicated in this length unstable C type injury to provide soft tissue stabilization and prevent further chondral injury. Splinting alone would not prevent shortening and would not allow soft tissue recovery. CT scans prior to limb stabilization are not warranted because the patterns make more sense after the restoration of gross length, rotation and alignment in the external fixator. Initial fibular fixation is also not recommended in this case because the location of incisions could affect the definitive surgical tactic. In this multi-fragmentary fibular injury, anatomic reduction would be challenging and malreduction could occur and influence subsequent reconstructions. Delayed open reduction internal fixation is ideal after the resolution of soft tissue swelling.
**Question 15of 100**
**CLINICAL SITUATION**
Figure 1 is the radiograph and Figure 2 is the CT image of a 45-year-old woman who fell about 20 feet off her balcony. These images show an isolated, open injury with a 3-cm open medial wound.
The best delayed definitive surgical fixation plan would include
---
1. lateral plating of the fibula and a percutaneous medial column plate.
2. intramedullary fixation of the fibula and an anterolateral tibial plate.
3. open medial column plating, percutaneous screw fixation of the joint, and lateral fibular plating.
4. screw fixation of the medial column with an anterolateral tibial plate and lateral fibular plating
Answer: D
Discussion: The timely administration of antibiotics has been shown to be the best initial treatment to reduce the incidence of infection following an open fracture. Life threatening injuries must first be addressed. But in this isolated open pilon fracture, antibiotics should be initiated early along with tetanus prophylaxis. Reduction and splinting would stabilize the fracture but these interventions should follow antibiotic coverage. Emergency department irrigation is controversial. Closed reduction and splinting, external fixation, CT scan, and delayed open reduction internal fixation would be the preferred sequence of management. External fixation to provide provisional limb stabilization would be indicated in this length unstable C type injury to provide soft tissue stabilization and prevent further chondral injury. Splinting alone would not prevent shortening and would not allow soft tissue recovery. CT scans prior to limb stabilization are not warranted because the patterns make more sense after the restoration of gross length, rotation and alignment in the external fixator. Initial fibular fixation is also not recommended in this case because the location of incisions could affect the definitive surgical tactic. In this multi-fragmentary fibular injury, anatomic reduction would be challenging and malreduction could occur and influence subsequent reconstructions. Delayed open reduction internal fixation is ideal after the resolution of soft tissue swelling.
QUESTION 46 OF 50
Which of the following proteins or vitamins controls the amount of receptor activator of nuclear factor âkB ligand (RANKL)
produced by osteoblasts:
produced by osteoblasts:
1
Parathyroid hormone
2
25 hydroxyvitamin D3
3
Thyroid hormone
4
1,25 dihydroxyvitamin D3
5
Calcitonin
The active from of vitamin D (1,25 dihydroxyvitamin D3) regulates the control of RANKL production by the osteoblast.
The activation of osteoclasts is a complex process. Surface receptors on the osteoclast precursor cells are called RANK. Receptor activator of nuclear factor âkB ligand (RANKL) is expressed on the surface of osteoblasts/stromal cells. The RANKL proteins leave the osteoblast and attach to the RANK receptor on the osteoclast precursor. Macrophage colony stimulating factor then facilitates the production of active osteoclasts from the osteoclast precursor
The activation of osteoclasts is a complex process. Surface receptors on the osteoclast precursor cells are called RANK. Receptor activator of nuclear factor âkB ligand (RANKL) is expressed on the surface of osteoblasts/stromal cells. The RANKL proteins leave the osteoblast and attach to the RANK receptor on the osteoclast precursor. Macrophage colony stimulating factor then facilitates the production of active osteoclasts from the osteoclast precursor
QUESTION 47 OF 50
of 100
Figure 9 is the radiograph of a 24-year-old amateur marathon runner who has ankle pain. She previously sustained a metatarsal stress fracture. In addition to asking about her training routine and the type of footwear she uses, the orthopaedic surgeon should inquire about this patient's history of nutrition and

Figure 9 is the radiograph of a 24-year-old amateur marathon runner who has ankle pain. She previously sustained a metatarsal stress fracture. In addition to asking about her training routine and the type of footwear she uses, the orthopaedic surgeon should inquire about this patient's history of nutrition and
1
genetics.
2
rheumatology.
3
menstruation.
4
cardiovascular health.
Several studies have reported an increased incidence of stress fractures in female athletes, including fractures of the foot and ankle in runners. The
female athlete triad describes a condition involving decreased bone density, anorexia, and amenorrhea. In addition to asking about this woman's exercise routine, the orthopaedic surgeon should obtain a comprehensive menstrual and dietary history in the context of multiple stress fractures. A review of genetics, rheumatology, and cardiovascular disorders is less likely to generate an etiology.
RECOMMENDED READINGS
Kasser JR, ed. Orthopaedic Knowledge Update 5: Home Study Syllabus. Rosemont, IL: American Academy of Orthopaedic Surgeons; 1996:96-99.
Arendt EA. Osteoporosis in the athletic female: Amenorrhea and amenorrheic osteoporosis. In: Pearl AJ, ed. AOSSM: The Athletic Female. Champaign, IL: Human Kinetics; 1993:41-59. Brukner PD, Khan KM. Clinical Sports Medicine. Sydney: McGraw-Hill; 1991:17.
RESPONSES FOR QUESTIONS 10 THROUGH 13
1. Ankle replacement
2. Ankle fusion
3. Tibiotalocalcaneal fusion
4. Total contact cast
5. Intra-articular steroid injection
Match the appropriate treatment listed above with the patient scenario described below.
female athlete triad describes a condition involving decreased bone density, anorexia, and amenorrhea. In addition to asking about this woman's exercise routine, the orthopaedic surgeon should obtain a comprehensive menstrual and dietary history in the context of multiple stress fractures. A review of genetics, rheumatology, and cardiovascular disorders is less likely to generate an etiology.
RECOMMENDED READINGS
Kasser JR, ed. Orthopaedic Knowledge Update 5: Home Study Syllabus. Rosemont, IL: American Academy of Orthopaedic Surgeons; 1996:96-99.
Arendt EA. Osteoporosis in the athletic female: Amenorrhea and amenorrheic osteoporosis. In: Pearl AJ, ed. AOSSM: The Athletic Female. Champaign, IL: Human Kinetics; 1993:41-59. Brukner PD, Khan KM. Clinical Sports Medicine. Sydney: McGraw-Hill; 1991:17.
RESPONSES FOR QUESTIONS 10 THROUGH 13
1. Ankle replacement
2. Ankle fusion
3. Tibiotalocalcaneal fusion
4. Total contact cast
5. Intra-articular steroid injection
Match the appropriate treatment listed above with the patient scenario described below.
QUESTION 48 OF 50
Anterior subluxation in a throwing athlete is most commonly the result of
1
avulsion of the inferior glenohumeral ligament from the glenoid.
2
avulsion of the inferior glenohumeral ligament from the humerus.
3
fracture of the anterior glenoid rim.
4
excessive capsular laxity from microtrauma.
5
a large Hill-Sachs lesion.
Subtle anterior subluxation in the throwing athlete most frequently results from excessive capsular laxity because of repetitive microtrauma. Avulsion of the inferior glenohumeral ligament from the glenoid, or more rarely from the humerus, occurs with macrotrauma. A large Hill-Sachs lesion and a glenoid rim fracture also may result from a traumatic anterior dislocation.
REFERENCES: Kvitne RS, Jobe FW: The diagnosis and treatment of anterior instability in the throwing athlete. Clin Orthop 1993;291:107-123.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1999, pp 961-990.
REFERENCES: Kvitne RS, Jobe FW: The diagnosis and treatment of anterior instability in the throwing athlete. Clin Orthop 1993;291:107-123.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1999, pp 961-990.
QUESTION 49 OF 50
Which of the following deformities is most common after the amputation shown in Figure A?


1
Pes cavus
2
Pes planus
3
Hindfoot valgus
4
Equinovarus
5
Calcaneovalgus
The most common deformity after a midfoot amputation as shown in Figure A is an equinuovarus deformity due to the pull of the Achilles and plantarflexors in face of loss of the common extensors and distal insertion of the tibialis anterior.
Ng et al. review foot and ankle amputations, and review the issues inherent with each amputation level, including prosthesis fitting and use. They also mention that careful repair of all released or transected tendons is needed to maintain a plantigrade foot.
Early reviews the importance of soft tissue balancing with midfoot amputations. They note that the attachment of the resected tendons into the more proximal retained bones is critical for success in restoration of foot position and ambulation capabilities.
Figure A shows a midfoot amputation as the result of trauma. Illustration A shows the lateral view of the amputation, with an obvious equinus deformity.
Incorrect Answers:
Answer 1, 2, 3, 5: Loss of the common extensor tendons of the toes would not lead to the listed deformities.
Ng et al. review foot and ankle amputations, and review the issues inherent with each amputation level, including prosthesis fitting and use. They also mention that careful repair of all released or transected tendons is needed to maintain a plantigrade foot.
Early reviews the importance of soft tissue balancing with midfoot amputations. They note that the attachment of the resected tendons into the more proximal retained bones is critical for success in restoration of foot position and ambulation capabilities.
Figure A shows a midfoot amputation as the result of trauma. Illustration A shows the lateral view of the amputation, with an obvious equinus deformity.
Incorrect Answers:
Answer 1, 2, 3, 5: Loss of the common extensor tendons of the toes would not lead to the listed deformities.
QUESTION 50 OF 50
A 45-year-old male with well-controlled diabetes and hypertension is involved in a high-speed motor vehicle collision. He is complaining of left knee pain only. On physical examination, his skin is intact and his neurovascular examination is normal. His injury films are seen in Figure A. Which of the following places this patient at an increased risk for postoperative infection after open reduction and internal fixation (ORIF)?

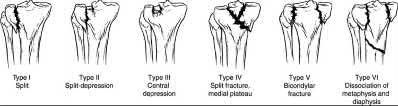
1
Intraoperative time over 3 hours
2
Age
3
Fracture Pattern
4
Medical comorbidities
5
Mechanism of injury
Intraoperative times approaching 3 hours have been associated with an increased risk of infection after undergoing ORIF of tibial plateau fractures.
The optimal treatment for displaced tibial plateau fractures is ORIF. The goals
of care are preservation of the soft tissues, restoration of the mechanical axis, and restoration of the articular surface. These injuries are associated with complications such as infections, arthrofibrosis, malunion/nonunion, and compartment syndromes. Infections have been associated with male gender, smoking, pulmonary disease, bicondylar fracture patterns, and intraoperative time over 3 hours. Modern techniques such as delay of definitive surgery, the use of temporary spanning external fixators, and dual incision approaches have improved the results of ORIF.
Basques et al. performed a database study to identify factors that are associated with short-term outcomes after ORIF of tibial plateau fractures. They examined adverse events (AAE), severe adverse events (SAEs), infectious complications, extended length of stay (LOS), and readmission within 30 days. They found that AAE was associated with increased ASA class and history of pulmonary disease. SAE was associated with male sex and increased ASA class. Infectious complications were associated with male sex, increased ASA class, smoking, pulmonary disease, and bicondylar fracture patterns.
Colman et al. performed a retrospective study to identify the relationship between surgical site infection and prolonged operative time in fractures of the tibial plateau. They found that mean operative time for patients who had an infection was 2.8 hours vs. 2.2 hours for patients without an infection. They also found that compartment syndromes that underwent fasciotomy had a higher infection rate than patients that did not develop this complication. Open fracture grade was also related to infection rate. They concluded that operative times approaching 3 hours and open fractures are related to an increased overall risk for surgical site infection.
Figure A is an AP radiograph of the knee demonstrating an intra-articular split of the lateral tibial plateau (Schatzker 2). Illustration A is an illustration of the Schatzker classification of tibial plateau fractures.
Incorrect Answers:
Answer 2: Age has not been associated with an increased risk of infection after ORIF of the tibial plateau.
Answer 3: An increased risk of infection after ORIF of the tibial plateau has been associated with bicondylar fracture patterns.
Answer 4: Well controlled diabetes and hypertension have not been associated with an increased risk of infection after ORIF of the tibial plateau.
Answer 5: Mechanism of injury has not been associated with an increased risk of infection after ORIF of the tibial plateau.
The optimal treatment for displaced tibial plateau fractures is ORIF. The goals
of care are preservation of the soft tissues, restoration of the mechanical axis, and restoration of the articular surface. These injuries are associated with complications such as infections, arthrofibrosis, malunion/nonunion, and compartment syndromes. Infections have been associated with male gender, smoking, pulmonary disease, bicondylar fracture patterns, and intraoperative time over 3 hours. Modern techniques such as delay of definitive surgery, the use of temporary spanning external fixators, and dual incision approaches have improved the results of ORIF.
Basques et al. performed a database study to identify factors that are associated with short-term outcomes after ORIF of tibial plateau fractures. They examined adverse events (AAE), severe adverse events (SAEs), infectious complications, extended length of stay (LOS), and readmission within 30 days. They found that AAE was associated with increased ASA class and history of pulmonary disease. SAE was associated with male sex and increased ASA class. Infectious complications were associated with male sex, increased ASA class, smoking, pulmonary disease, and bicondylar fracture patterns.
Colman et al. performed a retrospective study to identify the relationship between surgical site infection and prolonged operative time in fractures of the tibial plateau. They found that mean operative time for patients who had an infection was 2.8 hours vs. 2.2 hours for patients without an infection. They also found that compartment syndromes that underwent fasciotomy had a higher infection rate than patients that did not develop this complication. Open fracture grade was also related to infection rate. They concluded that operative times approaching 3 hours and open fractures are related to an increased overall risk for surgical site infection.
Figure A is an AP radiograph of the knee demonstrating an intra-articular split of the lateral tibial plateau (Schatzker 2). Illustration A is an illustration of the Schatzker classification of tibial plateau fractures.
Incorrect Answers:
Answer 2: Age has not been associated with an increased risk of infection after ORIF of the tibial plateau.
Answer 3: An increased risk of infection after ORIF of the tibial plateau has been associated with bicondylar fracture patterns.
Answer 4: Well controlled diabetes and hypertension have not been associated with an increased risk of infection after ORIF of the tibial plateau.
Answer 5: Mechanism of injury has not been associated with an increased risk of infection after ORIF of the tibial plateau.
