This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set F2EBEA)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
of 100
Figure 4
1
Curettage and/or grafting
2
Radiofrequency ablation
3
Intravenous (IV) antibiotics
4
Incision, drainage, and IV antibiotics
5
Neoadjuvant chemotherapy followed by surgical reconstruction
- Radiofrequency ablation
QUESTION 2 OF 50
of 100
Denosumab, the human monoclonal antibody that specifically binds and inactivates receptor activator of nuclear factor-kB ligand (RANKL), is commonly used in the setting of metastatic disease. Its cell surface receptor is expressed by
1
mature osteoclasts only.
2
mature osteoblasts only.
3
both osteoclast precursors and mature osteoclasts.
4
both osteoblast precursors and mature osteoblasts.
Bone remodeling involves both osteoblasts and osteoclasts. RANKL, a member of the tumor necrosis factor (TNF) family, is a key regulator of osteoclast formation and function. The receptor of RANKL, RANK, is expressed by both osteoclast precursors and mature osteoclasts. Denosumab inhibits the binding of RANKL to RANK, decreasing osteoclastogenesis and bone-resorption by mature osteoclasts.
Osteoblasts produce osteoprotegerin, which stimulates osteoclasts to induce apoptosis by acting as a decoy for RANKL, preventing the binding of RANKL to RANK. Osteoprotegerin also binds to other TNF-related apoptosis-inducing ligands and other TNF members including TNF-a, TNF-B, and CD40 ligand. Denosumab does not bind to any other TNF members.
Breast cancer metastases produce cytokines that induce osteoblasts to express elevated levels of RANKL, stimulating osteoclastogenesis via binding to RANK and activating downstream signaling pathways to osteoclast precursors, causing further bone resorption. Measurements of bone product turnover (including N-telopeptide) decrease during treatment with denosumab.
RECOMMENDED READINGS
12. [Gül G, Sendur MA, Aksoy S, Sever AR, Altundag K. A comprehensive review of denosumab for bone metastasis in patients with solid tumors. Curr Med Res Opin. 2016 Jan;32(1):133-45. doi: 10.1185/03007995.2015.1105795. Epub 2015 Nov 25. PubMed PMID: 26451465. ](http://www.ncbi.nlm.nih.gov/pubmed/26451465)[View Abstract ](http://www.ncbi.nlm.nih.gov/pubmed/26451465)[at](http://www.ncbi.nlm.nih.gov/pubmed/26451465)
[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26451465)
13. [De Castro J, García R, Garrido P, Isla D, Massuti B, Blanca B, Vázquez J. Therapeutic Potential of Denosumab in Patients With Lung Cancer: Beyond Prevention of Skeletal Complications. Clin Lung Cancer. 2015 Nov;16(6):431-46. doi: 10.1016/j.cllc.2015.06.004. Epub 2015 Jun 25. Review. PubMed PMID: 26264596. ](http://www.ncbi.nlm.nih.gov/pubmed/26264596)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26264596)
RESPONSES FOR QUESTIONS 26 THROUGH 31
1. Ultrasound
2. MRI with and without contrast
3. Chest CT scan and whole-body bone scan
4. Positron emission tomography (PET)
5. Presurgical radiation therapy
6. Marginal resection
7. Transverse incisional biopsy centered over the mass
8. Incisional biopsy centered over the mass in line with the long axis of the limb
9. Sentinel node biopsy
10. Core needle biopsy
For each clinical scenario or question below, select the most appropriate evaluation or treatment step listed above.
QUESTION 3 OF 50
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?**
1
Contact between the rotator cuff and the posterior-superior labrum
2
Anterior instability
3
A ganglion cyst of the spinoglenoid notch
4
Osteonecrosis of the humeral head
5
Posterior subluxation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity.
REFERENCES: Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
McFarland EG, Hsu CY, Neira C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
QUESTION 4 OF 50
A 16-year-old female basketball player sustains a re-tear of her anterior cruciate ligament (ACL) reconstruction. Her physical examination reveals a 3+ Lachman and 2+ pivot shift. Her range of motion is 10° of hyperextension to 130° of flexion. Radiographs reveal her ACL inclination angle to be 50°, tibial slope, 7°, and her physes are closed. What finding has been associated with an increased risk graft failure?
59
1
Hyperextension
2
Flexion
3
Tibial slope
4
ACL inclination angle
There are numerous risk factors for ACL reconstruction failure. These include increased tibial slope, younger age, higher activity level, increased preoperative hyperextension and increased preoperative instability (increased Lachman/pivot shift). In this case, the patient had increased hyperextension, and a normal tibial slope and inclination angle. Of the hoices, hyperextension is her most identifiable risk factor for potential ACL graft failure. Correct answer : A
QUESTION 5 OF 50
You are commencing a repair of an acute rupture of the Achilles tendon that occurred 8 days previously in a 32-year-old recreational tennis player. Fibrillation of the tendon ends is noted. The following is most important to maximize the ultimate outcome of the repair:
1
Resection of the frayed tendon end, and end-to-end apposition
2
Incorporation of the plantaris tendon in the repair
3
Repair of the tendon with the foot in slight equinus
4
Augmentation of the repair with a facial turn down flap
5
Repair with the tendon ends at normal resting tension
Repair of the Achilles tendon at its normal resting length is critical. The frayed tendon ends should not be excised, since this will force a repair with the foot in equinus. The resting tension of the repair can be compared with the position of the opposite limb that should be prepared into the operative field.
QUESTION 6 OF 50
An 18-year-old female collegiate soccer player presents with right knee pain and swelling after a noncontact pivoting injury during a game. Four years prior, she underwent successful anterior cruciate ligament (ACL) reconstruction with hamstring autograft on the same knee. Physical examination and MRI scan are consistent with ACL graft rupture without associated meniscal tears. What statement can be made about the graft options in counseling this patient on revision ACL reconstruction?
1
Two-year sports function, as measured by International Knee Documentation Committee (IKDC), is better with allograft.
2
At 1-year follow-up, there is greater knee laxity with the use of autograft.
3
There is a higher infection rate with autograft.
4
Risk of graft rerupture is higher with allograft.
Based upon large multicenter studies and registries including the MARS group and Danish registry, re-tear rates after revision ACL reconstruction are higher when allograft is used as compared with autograft. Sport function, as assessed by the IKDC, is better with the use of autograft. Furthermore, no differences in retear rates or function have been shown between soft tissue and bone patellar tendon bone autograft. 26
QUESTION 7 OF 50
Following calcaneus fracture, risk factors for later need for subtalar arthrodesis due to painful posttraumatic arthritis include all of the following except:
1
Bohlerâs angle 75% of patients
2
Are least at risk for penetrating the joint capsule over the anterolateral aspect of the ankle
3
C annot be olive wires because of a higher risk for pin-tract infection
In cadaver specimens, the anterolateral capsular reflection of the ankle joint extended proximally the highest with an average of
9.3 mm and a maximum of 12.2 mm. There was a 100% communication between the distal tibia-fibula joint and the ankle joint.
QUESTION 8 OF 50
of 100
A 45-year-old man has had 3 months of increasing upper back pain, “balance" issues, and heaviness in his legs. His physical examination reveals a normal neurological examination, but he is noted to be anemic. His MRI scans and biopsy specimen are shown in Figures 1 through
1
He is determined to have a Spinal Instability Neoplastic Score (SINS) of 6. After biopsy, what is the most appropriate treatment at this time?

2
Laminectomy
3
Laminectomy with posterior spinal fusion
4
Enbloc vertebral resection and reconstruction
5
Radiation of the lesion
■ The MRI scan reveals a large posterior element tumor, which is compressing the spinal cord. Multiple lesions within the spinal column are consistent with multiple myeloma. Myeloma is a radiosensitive tumor. Additionally, he has a SINS of 6. This score helps the treating physician determine the tumor-related instability of the vertebral column to guide the decision for operative management. A SINS of 0-6 is thought to be stable; 7-12, potentially stable, and >13, unstable. Appropriate treatment in a neurologically intact patient with a radiosensitive tumor with a low SINS would be radiation treatment versus surgical treatment, despite the degree of spinal cord compression.
QUESTION 9 OF 50
of 100
Which surgical procedure should be considered for treatment of chronic plantar fasciitis?
1
Endoscopic or open plantar fasciotomy
2
Heel spur excision
3
Achilles tendon lengthening
4
Extensile approach, medial and plantar, to include release of tarsal tunnel and complete plantar fasciotomy
Imaging studies in the evaluation of plantar fasciitis should always include weight-bearing foot radiographs to reveal alignment and exclude calcaneal stress fracture, tumor, subtalar arthritis, and insertional posterior spurs. MRI is occasionally indicated in problematic cases. Ultrasound can be helpful to evaluate thickening and disease in the proximal plantar fascia. Ultrasound is quick and much more cost effective than MRI. Laboratory screenings to evaluate inflammatory arthritis are indicated only for patients with bilateral heel pain who may be more likely to have systemic disease.
In the nonsurgical treatment of plantar fasciitis, high-impact loading exercises may make the condition worse. Corticosteroid injections may provide short-term relief only and can occasionally cause plantar fascia rupture. They should be used with caution. PRP injections are expensive and currently not covered by insurance. Studies have not demonstrated long-term pain relief with PRP. Plantar fascia-specific stretching has been shown more effective than Achilles tendon stretching alone.
Surgical treatment is indicated for fewer than 5% of patients. It is not necessary to resect the heel spur because the spur is not attached to the plantar fascia and rarely contributes to a patient's pain. The open extensile approach is associated with a much longer recovery than the open or endoscopic approaches and is no longer justified. Multiple studies have demonstrated the efficacy of endoscopic and open plantar fasciotomy techniques.
RECOMMENDED READINGS
Bader L, Park K, Gu Y, O'Malley MJ. Functional outcome of endoscopic plantar fasciotomy. Foot Ankle Int. 2012 Jan;33(1):37-43. doi: 10.3113/FAI.2012.0037. PubMed PMID:
[22381234.](http://www.ncbi.nlm.nih.gov/pubmed/22381234)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22381234)
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
[372/. PubMed PMID: 24860133.](http://www.ncbi.nlm.nih.gov/pubmed/24860133)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860133)
QUESTION 10 OF 50
-A tendon repair is thought to be weakest during which phase of tendon healing?
1
Inflammatory
2
Proliferation
3
Maturation
4
Remodeling
No detailed explanation provided for this question.
QUESTION 11 OF 50
Which of the following is not considered a part of the triangular fibrocartilage complex:
1
Ulnolunate ligament
2
Palmar radioulnar ligament
3
Dorsal radioulnar ligament
4
Radiolunate ligament
5
Ulnotriquetral ligament
The triangular fibrocartilage complex is made up of the dorsal and palmar radioulnar ligaments, the meniscal homologue, the articular disk, the ulnolunate, and the ulnotriquetral ligaments. The radiolunate ligament is not part of the complex.
QUESTION 12 OF 50
Urgent closed reduction of ankle fracture-dislocations using intraarticular lidocaine injection:
1
Provides a similar degree of analgesia compared to conscious sedation
2
Requires more time to perform the reduction and splint the leg than with conscious sedation
3
Results in inferior reduction of ankle deformity compared to conscious sedation
4
Requires frequent repeat reduction procedures due to persistent fracture malalignment
5
Is painful due to distension of the joint capsule
A prospective randomized study compared intraarticular lidocaine injection to conscious sedation for analgesia during reduction of ankle fracture-dislocations. There was no difference in the amount of analgesia provided by the two methods. Time for reduction and splinting was less in the local anesthetic group. Quality of reduction was similar in both groups.
QUESTION 13 OF 50
What is the most appropriate indication for replantation in an otherwise healthy
35-year-old man?
1
Isolated transverse amputation of the thumb through the middle of the nail bed
2
Isolated transverse amputation of the index finger through the proximal phalanx
3
Isolated transverse amputation of the ring finger through the proximal phalanx
4
Isolated transverse amputation of the hand at the level of the wrist
5
Forearm amputation with a 10-hour warm ischemia time
Vascular anastamoses are exceedingly difficult with amputations distal to the nail fold as the digital vessels bifurcate or trifurcate at this level, and little functional benefit is gained compared to other means of soft-tissue coverage. Single digit amputations, other than
the thumb, are a relative contraindication for replantation. Replantations at the level of the proximal phalanx lead to poor motion of the proximal interphalangeal joint. In a healthy
active adult, an amputation through the wrist is an appropriate situation to proceed with a replantation. A transverse forearm amputation is a good indication with a warm ischemia time
of less than 6 hours.
Scientific References
: Urbaniak JR: Replantation, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1085.
Boulas HJ: Amputations of the fingers and hand: Indications for replantation. J Am Acad Orthop Surg 1998;6:100-105.
QUESTION 14 OF 50
A genetiCmutation accounts for the manifestations of achondroplasia. Which of the following proteins has a genetiCmutation that has been linked to achondroplasia:
1
Fibroblast growth factor (FGF) receptor 3
2
Type I collagen
3
Fibrillin
4
Type II collagen
5
Cartilage oligomeriCmatrix protein (COMP)
The genetiCdefect in achondroplasia involves fibroblast growth factor (FGF) receptor 3.
The other answers refer to:
Osteogenesis imperfecta Type I collagen
Marfan syndrome Fibrillin
Spondyloepiphyseal
dysplasia Type II collagen
Pseudoachondroplasia Cartilage oligomeriCmatrix protein (COMP) Correct Answer: Fibroblast growth factor (FGF) receptor 3
QUESTION 15 OF 50
of 100
An 18-month-old girl was treated at the age of 4 months with medial open reduction of a unilateral developmental hip dislocation.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
- Absence of the proximal femoral epiphysis secondary ossification center
QUESTION 16 OF 50
Lyme disease is caused by which of the following organisms or mechanisms:
1
Group A Streptococcus
2
Borrelia burgdorferi
3
Vibrio vulnificus
4
Group B Streptococcus
5
Autoimmune disorder of unknown etiology
Lyme disease was initially thought to be an idiopathic autoimmune disorder; however, in the 1970s, researchers at Yale University identified Borrelia burgdorferi as the cause of the disease. The disease is transmitted by a deer tick known as Ixodes ricinusi.
Group A streptococcal pharyngitis may be followed by rheumatic fever, but not Lyme disease.
Vibrio vulnificus is the organism responsible for severe soft tissue infections in patients who are exposed to fresh-water shellfish. Group B Streptococcus is a common etiologic agent for necrotizing fasciitis.
QUESTION 17 OF 50
Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a
successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?
1
Open reduction and internal fixation (ORIF) of the fracture
2
Removal of the current stem, femur ORIF, and insertion of a longer revision stem
3
Femur ORIF with cables and strut graft, leaving the current stem in situ
4
Femur ORIF combined with reimplantation of the primary component
The fracture has occurred around the stem, representing a Vancouver type B fracture, and the stem is clearly loose, making it a type B2 fracture. The appropriate treatment is removal of the loose in situ stem; ORIF of the femur using cerclage wires, cables, or a plate; and insertion of a longer revision stem such as a tapered fluted modular titanium or fully porous coated cylindrical stem to bypass the fracture. All of the other options are incorrect, because they represent inappropriate treatment options for a Vancouver type B2 fracture.
QUESTION 18 OF 50
of 100
A 35-year-old man has substantial pain at the base of his dominant right thumb. Orthosis use, anti-inflammatory medication, and corticosteroid injections have failed to improve his symptoms. Which condition is a contraindication to the surgery shown in the radiograph (Figure 38)?
1
Lack of hyperextension of the thumb metacarpophalangeal (MCP) joint
2
Scapholunate advance collapse
3
Arthritis of the scaphotrapezial-trapezoid (STT) joint
4
Bilateral disease
There are multiple surgical options for treatment of symptomatic thumb carpometacarpal (CMC) joint arthritis, including trapeziectomy with or without suspensionplasty and with or without tendon interposition, prosthetic replacement, or arthrodesis. However, for a young manual laborer, a more robust solution is required so he can withstand the rigors of occupational activities. Arthrodesis of the CMC joint provides good pain relief but a relatively high nonunion rate (8%-21%). Presence of STT arthritis is a contraindication to CMC fusion because the STT joint will undergo increased stresses following CMC fusion, which will cause early failure of the surgical intervention. Bilateral thumb CMC fusions can be performed, and bilateral disease is not a contraindication to this procedure. Concomitant wrist arthritis does not preclude CMC fusion because this can be addressed with scaphoid excision and partial wrist fusion, which is not compromised by CMC fusion. Lack of MCP joint hyperextension does not preclude CMC fusion; substantial MCP hyperextension should be addressed at the time of arthroplasty for CMC arthritis with MCP fusion or volar capsulodesis.
RECOMMENDED READINGS
25. [Rizzo M, Moran SL, Shin AY. Long-term outcomes of trapeziometacarpal arthrodesis in the management of trapeziometacarpal arthritis. J Hand Surg Am. 2009 Jan; 34(1):20-6. doi: 10.1016/j.jhsa.2008.09.022. PubMed PMID: 19121726.](http://www.ncbi.nlm.nih.gov/pubmed/19121726)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19121726)
26. [Goldfarb CA, Stern PJ. Indications and techniques for thumb carpometacarpal arthrodesis. Tech Hand Up Extrem Surg. 2002 Dec;6(4):178-84. PubMed PMID: 16520598. ](http://www.ncbi.nlm.nih.gov/pubmed/16520598)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16520598)
QUESTION 19 OF 50
A loose body is encountered during a left knee arthroscopy in the posterolateral compartment. In the arthroscopic photograph shown in Figure 17, the posterior aspect of the lateral femoral condyle is shown on the right and the posterolateral capsule is shown on the left. The arthroscope is placed in what anatomic interval to visualize this loose body?
1
Between the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL)
2
Between the ACL and the lateral femoral condyle
3
Between the PCL and the medial femoral condyle
4
Between the lateral collateral ligament (LCL) and the lateral femoral condyle
5
Between the medial collateral ligament (MCL) and the medial femoral condyle
DISCUSSION: The arthroscopic photo shows a grasper removing a loose body from the posterolateral compartment through an accessory posterolateral portal. The blunt arthroscopic trocar is placed through the intercondylar notch in the direction of the posterior horn of the lateral meniscus. The trocar passes between the ACL and the posterior aspect of the lateral femoral condyle into the posterolateral compartment.
REFERENCES: Wu WH, Richmond JC: Arthroscopy of the knee: Basic setup and techniques, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott-Raven, 2003, pp 215-216. Kramer DE, Bahk MS, et al: Posterior knee arthroscopy: Anatomy, technique, application. J Bone Joint Surg Am 2006;88:110-121.
QUESTION 20 OF 50
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
Postoperative radiographs are shown in Figures 3 and
1
How does the plate function?

[](https://cdn.mycrowdwisdom.com/aaos/test_resources/2018trauma/Trauma18ChooQ123F2.jpg)
[](https://cdn.mycrowdwisdom.com/aaos/test_resources/2018trauma/Trauma18ChooQ125F1.jpg)
[](https://cdn.mycrowdwisdom.com/aaos/test_resources/2018trauma/Trauma18ChooQ125F2.jpg)
2
Neutralization
3
Compression
4
Bridging
5
Buttressing
The patient sustained a comminuted extra-articular distal humeral diaphyseal fracture. In isolation, this fracture would still be amenable to an attempt at closed treatment. His radial nerve palsy alone does not warrant open management, as early exploration has not shown a significant benefit in a closed fracture. In addition, despite the comminution and distal extent of the fracture, it is still amenable to closed treatment, though it may be at higher risk for malunion. However, in this patient with multiple lower extremity injuries, fixation of the humerus can facilitate early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
QUESTION 21 OF 50
Place the following strategies for treating deep infection in total hip replacement in order of their effectiveness from 1 to 4, with
1 being the most effective. 1. No antibiotics 2. SystemiCantibiotics alone 3. AntibiotiCbone cement alone 4. AntibiotiCbone cement plus systemiCantibiotics
1
1,2,3,4
2
2,4,3,1
3
4,2,3,1
4
3,2,4,1
5
4,3,2,1
According to Espehaug and colleagues in their assessment of 10,905 primary cemented total knee replacements, the most effective strategy is antibiotic-bone cement plus systemiCantibiotics followed by systemiCantibiotics alone, antibiotic-bone cement alone, and no antibiotics
QUESTION 22 OF 50
A previously healthy 22-year-old male presents to the hospital after a motor vehicle accident. His injuries include a closed head injury, flail chest, intra-abdominal bleed and right femoral shaft fracture. Which of the following conventional indicators would support the role for "damage control orthopaedics" as opposed to "early total care" in the clinical decision making process of his femur fracture management?
1
Lactate level = 1.9 mmol/L
2
Fibrinogen = 1.1 g/dL
3
Platelet count = 20,000 per mcL
4
Urine output = 50 cc/hr
5
Base deficit = 2 mmol/L
Previously healthy, poly-trauma patients, presenting with platelet counts of
<70,000 will fall into the pathophysiological category of 'in extremis'. This will
support the role of damage control orthopaedics in the decision making process of this patients fracture management.
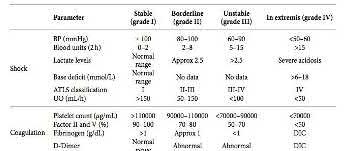
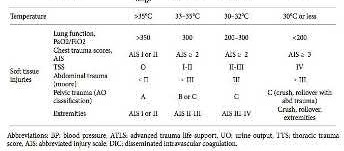
Damage control orthopaedics (DCO) is a staged approach for the management of polytrauma patients. It is most ideal for trauma patients that are clinically unstable or in extremis. In these patients, immediate surgery is thought to cause a “second hit” phenomenon, which may lead to ARDS, multi-organ failure, or even death. A patient is classified as 'unstable' or 'in extremis', if he or she meets the criteria in at least three of the four pathophysiological parameters; blood pressure <90mmHg, platelets count <70,000, temperature
<32°C and major soft tissue injuries.
Pape et al. (2005) described four classes of patients, based on their clinical status: stable, borderline, unstable, and in extremes. The term “borderline” was coined to describe a patient who is categorized as stable before surgery, but is at significant risk of unexpected deterioration and organ dysfunction postoperatively.
Pape et al. (2009) outlined that stable patient can undergo early definitive fracture fixation as necessary. In contrast, unstable patient should be resuscitated and adequately stabilized with temporary fixation before receiving definitive orthopaedic care.
Illustration A shows a table outlining the classification system used by Pape to classify patients into their clinical status of stable, borderline, unstable, and in extremes.
Incorrect Answers:
Answer 1: Lactate level = 1.9 mmol/L (normal range <2.5 mmol/L) would classify this patient into a stable category.
Answer 2: Fibrinogen = 1.1 g/dL (normal range >1 g/dL) would classify this patient into a stable category.
Answer 4: Urine output = 50 cc/hr (normal range >150 cc/hr)would classify this patient into a borderline category.
Answer 5: Base deficit = 2 mmol/L (normal range -2 to +2 mmol/L) would classify this patient into a stable category.
QUESTION 23 OF 50
What finding would most likely be present on an AP radiograph of a nondislocated elbow with an anteromedial coronoid fracture?
1
A “fleck” sign
2
The AP radiograph would appear normal
3
Equal joint spaces between the medial trochlea and the coronoid
4
Progressive narrowing of the joint space from lateral to medial between the medial trochlea and the coronoid
5
Progressive narrowing of the joint space from medial to lateral between the medial trochlea and the coronoid
No detailed explanation provided for this question.
QUESTION 24 OF 50
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
1
semiconstrained total elbow arthroplasty.
2
ulnohumeral arthroplasty and anterior and posterior capsular releases.
3
closed reduction and external fixation.
4
open reduction, heterotopic bone excision, anterior and posterior capsular releases, and a hinged elbow fixator.
5
open reduction, heterotopic excision, anterior and posterior capsular releases, and pin fixation across the joint for 3 weeks.
In a young individual with a chronic dislocation of the elbow and heterotopic bone formation, the treatment of choice is open reduction, heterotopic bone excision, anterior and posterior capsular releases, and a dynamic hinged fixator to begin protected early postoperative range of motion. It is important to understand that the fixator protects the reconstruction and allows early range of motion, but it does not maintain the reduction and should not be expected to do so. Pin fixation across the elbow delays early motion and is not recommended. Total elbow arthroplasty is not indicated, and ulnohumeral arthroplasty is for a primary arthritic condition.
REFERENCES: Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
QUESTION 25 OF 50
of 100
How long does it generally take for patients to return to preinjury levels of activity after sustaining this injury?
1
1 to 2 months
2
3 to 4 months
3
6 to 8 months
4
2 to 3 years
The treatment of Achilles tendon rupture has changed during the last 5 to 10 years as a better understanding of optimal rehabilitation emerges. Patients are encouraged to weight bear much sooner (2 weeks) than previously allowed. Early weight bearing is not associated with an increased risk for rerupture with surgical or nonsurgical treatment. The primary risk associated with surgery is a wound-healing problem. Achilles ruptures generally are preceded by tendinosis and an eccentric contraction of the muscle sufficient for tearing. Athletes who expect to return to their preinjury level of function should anticipate 6 months of recovery time.
RECOMMENDED READINGS
13. [Vosseller JT, Ellis SJ, Levine DS, Kennedy JG, Elliott AJ, Deland JT, Roberts MM, O'Malley MJ. Achilles tendon rupture in women. Foot Ankle Int. 2013 Jan;34(1):49-53. doi: 10.1177/1071100712460223. PubMed PMID: 23386761. ](http://www.ncbi.nlm.nih.gov/pubmed/23386761)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23386761)
14. [Tallon C, Maffulli N, Ewen SW. Ruptured Achilles tendons are significantly more degenerated than tendinopathic tendons. Med Sci Sports Exerc. 2001 Dec;33(12):1983-90. PubMed PMID: 11740288. ](http://www.ncbi.nlm.nih.gov/pubmed/11740288)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11740288)
15. [Willits K, Amendola A, Bryant D, Mohtadi NG, Giffin JR, Fowler P, Kean CO, Kirkley A. Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation. J Bone Joint Surg Am. 2010 Dec 1;92(17):2767-75. doi: 10.2106/JBJS.I.01401. Epub 2010 Oct 29. PubMed PMID: 21037028. ](http://www.ncbi.nlm.nih.gov/pubmed/21037028)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21037028)
QUESTION 26 OF 50
Slide 1
An 83-year-old woman presents for treatment of a painful second toe deformity. The hallux, the bunion, and the third toe are not painful. A fixed crossover toe deformity is present (Slide), with a dislocation of the second metatarsophalangeal joint noted radiographically. Which procedure is likely to give the patient rapid pain relief:
1
Arthrodesis of the hallux metatarsophalangeal joint and resection arthroplasty of the second proximal interphalangeal joint
2
Osteotomy of the second toe and metatarsal
3
Shortening osteotomies of the second and third metatarsals and interphalangeal arthroplasty
4
Amputation of the second toe at the metatarsophalangeal joint
5
Resection arthroplasty of the hallux metatarsophalangeal joint
In this age group, amputation of the second toe is a reasonable treatment. It is not possible to correct the second toe deformity without correction of the hallux, either by arthrodesis or arthroplasty at the metatarsophalangeal joint. The hallux is
asymptomatic, which is common in this age group, and the simplest treatment is to amputate the toe.
QUESTION 27 OF 50
of 100
An 11-month-old boy is being evaluated for scoliosis. Radiographs reveal a right thoracic curve of 20° with a rib-vertebral angle difference of 16°. What is the most appropriate next step in management?
1
A total spine MRI should be obtained, followed by serial casting
2
A thoracolumbosacral orthosis (TLSO) should be fabricated for this patient and used 23 hrs/day
3
The patient does not require any intervention or follow-up for this normal finding and can be discharged from follow-up
4
A repeat examination and PA radiograph should be obtained in 3 months
■ Infantile scoliosis has both resolving and progressive forms. If the rib-vertebral angle difference of Mehta is not >20 degrees, and the curve is mild at presentation, repeat imaging with a standing film in 3 months is recommended to determine if the curve is of the resolving type.
MRI in younger than age 12 months can fail to detect a tethered cord; as it requires sedation, it can be appropriately delayed until the second image to avoid unnecessary risk. A TLSO is not appropriate initial treatment for infantile scoliosis. While the patient still has a curve, he should be followed to ensure resolution.
QUESTION 28 OF 50
Slide 1
A 43-year-old construction worker presents for treatment of ankle pain. The patient recounts a fall from a height that caused an ankle fracture 2 years ago. The fracture was treated with closed reduction and cast immobilization for 5 months. He experiences pain upon ambulation and is unable to work. On examination, the range of ankle motion is 5° dorsiflexion and 20° plantarflexion. There is no crepitus with motion, but severe pain is present. A radiograph is presented (Slide 1). The recommended procedure to alleviate pain and improve function is:
1
Total ankle replacement
2
Ankle arthrodesis
3
Arthroscopy ankle and joint debridement
4
Osteotomy of the tibia and fibula
5
Anterior ankle cheilectomy, Achilles lengthening, and joint debridement
The arthritis in this joint is not severe, but there is joint malalignment associated with a short and externally rotated fibula and a marked valgus tibiotalar deformity. Although arthrodesis or total ankle replacement may be considered as treatment for some patients, this patient is not a good candidate for these procedures because he does not have severe arthritis. The deformity must be corrected with an osteotomy of the tibia and fibula. Although an opening wedge osteotomy may be considered, a closing wedge procedure is easier to perform and has a higher rate of healing.
QUESTION 29 OF 50
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of
1
arthroscopic synovectomy.
2
humeral arthroplasty.
3
unconstrained total shoulder arthroplasty.
4
constrained total shoulder arthroplasty with a fixed-fulcrum prosthesis.
5
glenohumeral arthrodesis.
Unconstrained total shoulder arthroplasty has been found to yield satisfactory results in a high percentage of patients with rheumatoid involvement of the glenohumeral joint. Pain relief has been more predictable with total shoulder arthroplasty than humeral arthroplasty, and a glenoid component is favored when there is sufficient glenoid bone stock and an intact rotator cuff. Constrained or fixed-fulcrum devices have an unacceptably high failure rate because of loosening. Glenohumeral arthrodesis is avoided when the deltoid or rotator cuff is functioning because the functional results after arthroplasty are superior when compared with results of arthrodesis. Arthroscopic synovectomy may be helpful in early stages of the disease before extensive cartilage damage has occurred.
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Kelly IG, Foster RS, Fisher WD: Neer total shoulder replacement in rheumatoid arthritis. J Bone Joint Surg Br 1987;69:723-726.
QUESTION 30 OF 50
of 100
Figures 1 and 2 are the radiographs of a 75-year-old patient who has a 1-year history of progressive low back pain. He reports difficulty ambulating, inability to sit for extended periods, and pain when arising from a seated position. His medical history is positive for coronary artery disease, type II diabetes, depression, and mild obesity (BMI 32). His surgical history is positive for a lumbar fusion 3 years previously. Laboratory studies show normal CBC and metabolic profile. HgbA1C is 6.3. What factor is most predictive of his perceived clinical outcome after revision surgery?
1
Intraoperative cervical spine fluid leak
2
Postoperative infection
3
Depression status
4
Intraoperative blood loss requiring transfusion
■ Patient satisfaction ratings are increasingly viewed as important parameters for functional outcomes, as well as in delivering quality care. Psychosocial influence, however, plays a paramount role in perceived outcomes. Affective disorders like depression have a highly significant negative effect on patient-related outcomes and self-interpretation of health status. Verla and associates reported outcomes after fusion surgery and used SF-36, Visual Analog Scale, and Oswestry Disability Index scores before and at 1 and 2 years, postoperatively. They also specifically looked at patients who sustained complications (major and minor). The results showed no lasting effects from complications on patients' overall interpretation of health status.
QUESTION 31 OF 50
Which is the best match in surface topography when performing an osteochondral autograft transplantation procedure from the distal femur to the talar dome for an osteochondral lesion of the talus:
1
From the superior-medial femoral condyle to the antero-medial talar dome
2
From the inferior-medial femoral condyle to the postero-medial talar dome
3
From the superior-lateral femoral condyle to any position on the medial talar dome
4
From the inferior-medial femoral condyle to the centro-medial talar dome
5
From the inferior-lateral femoral condyle to the antero-medial talar dome
In a magnetic resonance imaging topography study looking for the best corresponding shape of the articular surface between the non-weightbearing femoral condyle and the medial talar dome, plugs from the supero-lateral femoral condyle had the best fit with osteochondral lesions of the medial talus in the anterior, central, and posterior zones.
QUESTION 32 OF 50
In what region of the United States is Lyme disease most prevalent:
1
Hawaii
2
Alaska
3
Northeastern United States
4
Lower Midwestern United States
5
Southern United States
Lyme disease is most common in the northern United States, Wisconsin, and C alifornia; however, the disease can occur anywhere. Vector ticks identified in Europe transmit several variations of Lyme disease.
Hawaii, Alaska, the lower midwestern states, and southern states do not have an increased incidence of Lyme diseaseC orrect
Answer: Northeastern United States
QUESTION 33 OF 50
A 21-year-old football player who sustained a direct blow to the posterior hindfoot while making a cut is unable to bear weight on the injured foot. Examination reveals tenderness and swelling of the great toe metatarsophalangeal (MTP) joint. Radiographs are shown in Figures 9a and 9b. What is the most likely diagnosis?
1
Dislocation of the great toe MTP joint
2
Rupture of the volar plate
3
Fracture of the lateral sesamoid
4
Fracture of the lateral sesamoid and rupture of the plantar plate
5
Subluxation of the sesamoids
Turf toe occurs in collision and contact sports in which the athlete pushes off to accelerate or change direction and there is hyperextension of the great toe MTP joint. Typically, there is also axial loading of the posterior hindfoot, which increases the hyperextension of the MTP joint. The most common presentation is pain and swelling of the MTP joint and inability to hyperextend the joint without significant symptoms. With significant force, fractures of the sesmoids and plantar soft tissues can occur. The radiographs do not show a dislocation of the great toe MTP joint because it is concentrically located on both radiographs. However, the radiographs show a fracture of the lateral sesamoid or a diastasis of a bipartite lateral sesamoid. The medial sesamoid is also proximal indicating a rupture of the plantar (volar) plate. Therefore, the most likely diagnosis is a fracture of the lateral sesamoid with rupture of the plantar plate leading to proximal migration of the proximal fragment of the lateral sesamoid and the medial sesamoid.
REFERENCES: Rodeo SA, et al: Diastasis of bipartite sesamoids of the first metatarsophalangeal joint. Foot Ankle 1993;l4:425-434.
Rodeo SA, O’Brien S, Warren RF, et al: Turf toe: An analysis of metatarsal joint sprains in professional football players. Am J Sports Med 1990;18:280-285.
QUESTION 34 OF 50
-Premature arrest following growth plate injury is attributed to what mechanism?
1
Proliferation of the perichondrial ring of LaCroix
2
Initiation of Wolff’s law
3
Disruption of the Heuter-Volkmann principle
4
Vascular invasion across the physis
No detailed explanation provided for this question.
QUESTION 35 OF 50
When performing a Green transfer for cerebral palsy—flexor carpi ulnaris (FCU) to extensor carpi radialis brevis (ECRB)—in addition to improving wrist extension, what other motion may be improved if the FCU is routed around the ulna instead of through the interosseous membrane?
1
Thumb extension
2
Forearm supination
3
Finger extension
4
Forearm pronation
The typical upper extremity deformity in spastic hemiplegic cerebral palsy consists of shoulder internal rotation, elbow flexion, forearm pronation and wrist flexion, and ulnar deviation. The pronation position of the forearm can make bimanual activities more challenging for the child. The wrist flexion and ulnar deviation deformity interferes with finger function and therefore with grasp and release patterns. By transferring the FCU tendon to the ECRB, the deforming force is released, and central wrist extension is augmented. This transfer can lead to a supination moment when it is routed around the ulna to the ECRB insertion on the dorsum of the wrist. Thumb and finger extension are not affected by an FCU-to-ECRB _tendon transfer. Forearm supination, not pronation, is potentially improved with this tendon transfer._
QUESTION 36 OF 50
Figures 1 and 2 are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test, trace effusion, and range of motion from 0 to 85° of knee flexion. Which factor is most contributory to his examination findings?
1
Incorrect graft choice
2
Improper tunnel position
3
Tibial graft-tunnel mismatch
4
Femoral fixation at 80° flexion
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario. 14
QUESTION 37 OF 50
Figures 18a and 18b are the radiographs of an obese 75-year-old man with a rigid acquired flatfoot deformity. What is the best treatment option?
1
Double calcaneal osteotomy
2
Medial calcaneal osteotomy and tendon transfer
3
Lateral column lengthening and tendon transfer
4
Subtalar arthrodesis
5
Triple arthrodesis
For stage III adult-acquired flatfoot deformity characterized by dysfunction of the posterior tibial tendon, rigid valgus deformity of the hindfoot, and arthritic changes of the hindfoot joints,arthrodesis is the favored procedure. In an overweight patient with degenerative changes affecting the subtalar and Chopart joints, triple arthrodesis is the best treatment option. Subtalar arthrodesis only addresses the talocalcaneal joint and continues to render the patient symptomatic in the talonavicular and calcaneocuboid joints. Advanced stage III disease precludes reconstructive procedures involving calcaneal osteotomy and tendon transfer.
QUESTION 38 OF 50
Figures 1 through 4 show the radiographs and MRI obtained from a 40-year-old man who has a 6-week history of ring finger pain, redness, and swelling after puncturing the finger with a toothpick. Purulent drainage from the puncture wound site grew _Eikenella corrodens_. The patient was initially treated with oral antibiotics for 10 days and then intravenous (IV) antibiotics for 3 weeks. What is the best next step in treatment?
1
Continued IV antibiotics for 4 weeks
2
Continued oral antibiotics for 6 weeks
3
Bone scan, biopsy, and metastatic work-up
4
Surgical débridement along with antibiotics
This patient has a septic distal interphalangeal joint, which was treated with antibiotics alone. As a result, the patient developed osteomyelitis with bone destruction and abscess. The best way to treat this problem is to perform surgical débridement of bone and soft tissue, along with abscess drainage and an appropriate antibiotic regimen. Antibiotic treatment without surgery would not be successful in eliminating this particular infection. Bone scan with biopsy is not the correct option, because this problem is an infection _and not a tumor, and MRI already has provided enough diagnostic information._
QUESTION 39 OF 50
A 16-year-old football player reports the acute onset of pain in his left foot. An AP radiograph is shown in Figure
8/. What treatment is most likely to result in successful healing for this injury?
1
Restricted activity
2
Short leg walking cast
3
Short leg cast with no weight bearing
4
Percutaneous fixation with a screw
5
Open reduction and internal fixation with bone grafting
Fractures in this region of the fifth metatarsal have been shown to be prone to delayed union and
nonunion and therefore are most reliably managed with internal fixation. Bone grafting is generally not required.
REFERENCES: Herrera-Soto JA, Scherb M, Duffy MF, et al: Fractures of the fifth metatarsal in children and adolescents. J Pediatr Orthop 2007;27:427-431.
Fetzer GB, Wright RW: Metatarsal shaft fractures and fractures of the proximal fifth metatarsal. Clin Sports Med 2006;25:139-150.
QUESTION 40 OF 50
A 5-year-old boy is seen in the emergency department with a 2-day history of refusing to walk. Examination shows that he has a temperature of 102.2 degrees F (39 degrees C) and limited range ot motion of the right hip. The AP pelvic radiograph is normal. The WBC count is normal but the C-reactive protein and erythrocyte sedimentation rate (ESR) are elevated. What is the next step in management?
1
IV antibiotics
2
Oral antibiotics
3
Ibuprofen
4
Observation and repeat evaluation in 2 weeks
5
Aspiration of the right hip
The history, physical examination, and laboratory studies suggest a septic hip. Recent studies indicate that a child with elevated ESR, a WBC count of greater than 12,000/mm3, a temperature of greater than 38.5 degrees, and unwillingness to walk is very likely to have septic arthritis of the hip versus toxic synovitis. The best way to confirm the diagnosis is by hip aspiration. No medications should be started until a diagnosis is made. Toxic synovitis is common, but significantly less likely if three of the above criteria are present. This condition usually responds well to ibuprofen, but requires close observation. Septic hips are considered urgent conditions and therefore a repeat evaluation in 2 weeks is inappropriate.
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
QUESTION 41 OF 50
of 100 A 55-year-old man falls from a ladder and dislocates his nondominant shoulder. He undergoes an uncomplicated closed reduction under sedation in the emergency department. Postreduction radiographs reveal a small Hill-Sachs lesion and no other bony abnormalities. Six weeks after the dislocation, the patient has persistent pain at rest and forward elevation and external rotation weakness, but the remaining motor function in the extremity and sensation are intact. What is the best next step?
1
Physical therapy with electrical stimulation and iontophoresis
2
Corticosteroid injection
3
MRI of the shoulder
4
Electromyography (EMG) of the arm
DISCUSSION
For a patient >40 years of age who has persistent pain and weakness isolated to the rotator cuff following an acute anterior shoulder dislocation, an MRI is indicated to evaluate rotator cuff integrity. EMG is not indicated in this case because this patient has no evidence of distal motor functional abnormality and their sensation is intact, thereby making a brachial plexus injury unlikely. Corticosteroid injections and physical therapy
modalities do not adequately address the concern over his potential for having sustained a rotator cuff tear.
QUESTION 42 OF 50
Which of the following is an action of 1,25 dihydroxy vitamin D:
1
Increases synthesis of calcium binding protein
2
C auses kidney tubule cells to absorb calcium
3
Increases bone resorption by directly signaling osteoclasts
4
Increases parathyroid hormone (PTH) production
5
C auses kidney tubule cells to absorb phosphorus
Vitamin D acts on the intestinal to increase calcium absorption. C alcium binding protein synthesis is increased. Vitamin D is an intracellular messenger, acting through the nucleus.
Vitamin D actions:
Increase the efficiency of calcium absorption in the intestine (primarily duodenum) Increases synthesis of calcium binding protein (and others)
Increases passage of calcium through the cell membrane
Moves calcium through the cell cytoplasm and into the circulation
Increases bone resorption by telling the osteoblasts to release receptor activator of nuclear factor -kB ligand
Osteoblasts have vitamin D receptors
Vitamin D receptors exert a negative feedback on 1,25 dihydroxy vitamin D production
Decreases PTH production
QUESTION 43 OF 50
During an anterior retroperitoneal approach to the lumbar spine, what nerve is encountered lying on the anteromedial surface of the psoas muscle? ](http://www.orthobullets.com/anatomy/10053/psoas)
1
Genitofemoral
2
Ilioinguinal
3
Femoral
4
Lateral femoral cutaneous
5
Iliohypogastric
No detailed explanation provided for this question.
QUESTION 44 OF 50
A 21-year-old hockey player who has recurrent shoulder subluxations undergoes an anterior capsulorrhaphy under general anesthesia, and an interscalene block is used to relieve postoperative pain. At the 1-week follow-up examination, he reports loss of sensation over the lateral region of the shoulder and is unable to actively contract the deltoid muscle. The remainder of the examination is normal. What is the best course of action at this time?
1
Early exploration and possible repair of the axillary nerve
2
Urgent electromyography to assess for level of nerve injury
3
Continued normal postoperative care and observation of the nerve injury
4
Consultation with the anesthesiologist regarding a complication of the interscalene block
5
MRI to evaluate for a possible hematoma compressing the neurovascular bundle
The patient has an axillary nerve injury, which is relatively uncommon after surgery for instability. This type of injury generally is the result of a stretch injury rather than transection or a hematoma. Therefore, observation is indicated in the early postoperative period. After approximately 6 weeks, electromyography can be used to confirm and document the point of injury. Interscalene blocks can cause prolonged nerve injury but usually are not limited to the axillary nerve.
REFERENCE: Ho E, Cofield RH, Balm MR, et al: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
QUESTION 45 OF 50
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient?
1
Radial collateral ligament
2
Posterior bundle of the ulnar collateral ligament
3
Anterior bundle of the ulnar collateral ligament
4
Flexor carpi ulnaris
5
Pronation teres
DISCUSSION: The anterior bundle of the ulnar collateral ligament of the elbow is the primary constraint to valgus force of the elbow. In pitchers and in overhead athletes, injury to this portion of the ligament results in valgus instability. Reconstruction of the anterior band of the ulnar collateral ligament is necessary in many elite athletic throwers to allow them to return to this competitive activity.
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Cain EL, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.
Rettig AC, Sherrill C, Snead DS, et al: Nonoperative treatment of ulnar collateral ligament injuries in
throwing athletes. Am J Sports Med 2001 ;29:15-17.
/
Figure 55a Question 55
A 22-year-old male basketball player has had knee pain for the past 3 months. He denies any history of trauma. He has symptoms of catching but no locking. He has rested for 2 weeks but symptoms returned when he resumed sporting activities. Tr and T2-weighted MRI scans are shown in Figures 55a and 55b. What is the most likely diagnosis?
1. #### Locked lateral meniscus tear
2. #### Anterior cruciate ligament tear
3. #### Ganglion cyst of the anterior cruciate ligament
4. #### Synovial osteochondromatosis
5. #### Pigmented villonodular synovitis PREFERRED RESPONSE: 3
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.
Figure 56
QUESTION 46 OF 50
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of**
1
local modalities including iontophoresis.
2
quadriceps and iliotibial band stretching exercises.
3
progressive eccentric strengthening exercises.
4
a patellar tendon strap.
5
excision of the abnormal area.
Excision of the affected mucoid degenerative area is considered appropriate management in the Blazina classification system. A finding of phase III indicates persistent pain with or without activities, as well as deterioration of performance. With the appearance of the mucoid degeneration and the vigorous activity level of the intercollegiate basketball player, it is unlikely that nonsurgical management will provide adequate relief. When excising the affected degenerative area, care must be taken to retain normal tendon fibers. The defect in the patellar tendon is closed with absorbable sutures, as is the paratenon. Postoperative rehabilitation involves initial mobilization extension, with progressive range-of-motion and mobilization exercises as tolerated and weight bearing as tolerated. Open chain and isokinetic exercises are delayed until full range of motion and mobility is obtained, generally within 4 weeks. A return to activities is achieved by 80% to 90% of athletes, although there may be occasional activity-related aching for 4 to 6 months after surgery.
REFERENCES: Blazina ME, et al: Jumper’s knee. Orthop Clin North Am 1973;4:665.
Kelly DW, Carter VS, Jobe FW, Kerlan RK: Patellar and quadriceps tendon ruptures: Jumper’s knee. Am J Sports Med 1984;12:375-380.
Krums PE, Ryder B: Operative treatment of patella tendon disorders. Operative Techniques Sports Med 1994;2:303.
Rows J, et al: Patella tendinitis (jumper’s knees). Am J Sports Med 1978;6:362.
QUESTION 47 OF 50
A 28-year-old man who sustained an ankle fracture in a motor vehicle accident underwent open reduction and internal fixation 3 months ago. He continues to report significant ankle pain with ambulation. Radiographs are shown in Figure 26. What is the next most appropriate step in management?
1
Articulated ankle-foot orthosis
2
Revision open reduction and internal fixation of the syndesmosis with debridement of the medial gutter
3
Ankle arthrodesis
4
Syndesmosis arthrodesis
5
Ankle arthroscopy and debridement
The patient sustained a bimalleolar ankle fracture with a syndesmosis disruption. The initial open reduction and internal fixation did not successfully reduce the distal tibiofibular joint. The patient may need a derotational distraction osteotomy of the fibula to reduce the syndesmosis. The other procedures do not address the primary problem of the fibular malunion and syndesmosis malreduction. There is no radiographic evidence of significant arthritis; therefore, ankle arthrodesis is not indicated.
REFERENCE: Heier KA, Walling AK: Treatment of ankle fractures. Foot Ankle Clin 1999;4:521-534.
QUESTION 48 OF 50
of 100
Considering her current symptoms, history, and examination findings, you believe that the most efficacious means with which to address this patient's junctional kyphosis is
1
cervico-thoracic-lumbosacral orthosis to immobilize the kyphosed segment.
2
removal of the posterior instrumentation because she has had a successful fusion.
3
anteroposterior instrumented fusion at T2-3 to address the collapsed interspace.
4
revision posterior instrumentation with extension of the fusion to T1 to span the area of junctional kyphosis.
- revision posterior instrumentation with extension of the fusion to T1 to span the area of junctional kyphosis.
QUESTION 49 OF 50
Figures 1 and 2 are the radiographs of a 24-year-old male wrestler who underwent surgery for recurrent shoulder dislocations using coracoid autograft. At his first postoperative visit, the patient complains of decreased sensation on the lateral aspect of his forearm. The patient’s symptoms are most likely due to injury of the
1
axillary nerve.
2
musculocutaneous nerve.
3
median nerve.
4
radial nerve.
---
--- DISCUSSION:
The patient has undergone a Latarjet procedure as shown in the radiographs. After harvesting the coracoid graft, care must be taken to not place too much tension on or dissect excessively near the musculocutaneous nerve. The nerve is encountered 5 cm distal to the coracoid as it enters the conjoint tendon. The lateral antebrachial cutaneous nerve is the terminal branch of the musculocutaneous nerve and; therefore, injury can cause decreased sensation in the lateral forearm.
QUESTION 50 OF 50
of 100
Figures 33a through 33d are the radiograph, MR images, and biopsy specimen of a 66-year-old woman with a several-month history of an enlarging thigh mass after “pulling a muscle” while playing softball. Several weeks ago her physician aspirated the cyst, but the result is no change. Treatment of this lesion should include
1
embolization.
2
reaspiration and observation.
3
radiation therapy alone.
4
radiation therapy and surgery.

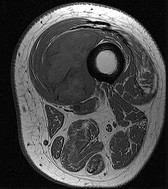
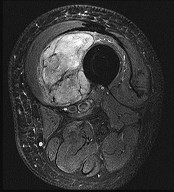
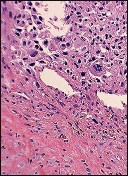
This patient’s imaging and biopsy specimen are consistent with a high-grade undifferentiated pleomorphic sarcoma (UPS). Histologically, UPS is characterized by high cellularity, marked nuclear pleomorphism, abundant mitotic activity (including atypical mitoses), and a spindle cell morphology. Necrosis is common and characteristic of high-grade lesions. Treatment consists of wide surgical excision and, in almost all cases, radiation. Radiation eliminates the need for limb amputation, and there is level I evidence to show that it leads to equivalent rates of survival. Radiation may be delivered either before or after surgery depending on the surgeon’s and multidisciplinary tumor board’s recommendations. There may be a role for presurgical embolization in some cases of high-grade soft-tissue sarcoma, but this is not appropriate as a standalone treatment. Chemotherapy provides limited survival improvement in adults with high-grade soft-tissue sarcomas.
RECOMMENDED READINGS
13. [Bell RS, O'Sullivan B, Davis A, Langer F, Cummings B, Fornasier VL. Functional outcome in patients treated with surgery and irradiation for soft tissue tumours. J Surg Oncol. 1991 Dec;48(4):224-31. PubMed PMID: 1745046. ](http://www.ncbi.nlm.nih.gov/pubmed/1745046)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1745046)
14. [O'Sullivan B, Wylie J, Catton C, Gutierrez E, Swallow CJ, Wunder J, Gullane P, Neligan P, Bell R. The local management of soft tissue sarcoma. Semin Radiat Oncol. 1999 Oct;9(4):328-48. Review. PubMed PMID: 10516380. ](http://www.ncbi.nlm.nih.gov/pubmed/10516380)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10516380)