This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set EE0B0A)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
The most common soft tissue sarcoma of the foot and ankle is:
1
Primitive neuroectodermal tumor
2
Malignant fibrous histiocytoma
3
Liposarcoma
4
Epithelioid sarcoma
5
Synovial sarcoma
Malignant melanoma is the most common soft tissue malignancy of the foot; however, synovial sarcoma is the most common soft tissue sarcoma. There may be a long duration of presence of the mass, with or without growth of the lesion. When one evaluates a patient with a small or large soft tissue mass on the foot, synovial sarcoma should be considered in the differential diagnosis.
QUESTION 2 OF 50
During an anterior approach to the shoulder, what is the most likely arterial structure to be encountered in the superior extent of the deltopectoral interval (just distal to the anterior edge of the clavicle)? ](http://www.orthobullets.com/approaches/12009/closed--2016-oite-85-day-study-plan)
1
Acromial branch of the thoracoacromial artery
2
Axillary artery
3
Arcuate artery
4
Suprascapular artery
5
Subclavian artery
No detailed explanation provided for this question.
QUESTION 3 OF 50
of 100
Figure 50a is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence?
1
Sclerotherapy
2
Shave excision with cautery
3
Cryotherapy
4
Wide surgical excision
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.
RECOMMENDED READINGS
55. [Quitkin HM, Rosenwasser MP, Strauch RJ. The efficacy of silver nitrate cauterization for pyogenic granuloma of the hand. J Hand Surg Am. 2003 May;28(3):435-8. PubMed PMID: 12772100. ](http://www.ncbi.nlm.nih.gov/pubmed/12772100)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12772100)
56. [Giblin AV, Clover AJ, Athanassopoulos A, Budny PG. Pyogenic granuloma – the quest for optimum treatment: audit of treatment of 408 cases. J Plast Reconstr Aesthet Surg. 2007;60(9):1030-5. Epub 2007 May 2. PubMed PMID: 17478135.](http://www.ncbi.nlm.nih.gov/pubmed/17478135)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17478135)
QUESTION 4 OF 50
of 100
A 13-year-old boy is complaining of elbow and wrist pain following a fall off a bike. Radiographs are taken in the emergency department (Figures 1 through 4). The wrist injury is unstable, and the patient is taken to the operating room for closed reduction and pinning of the distal radius fracture, closed treatment of the proximal fractures. Subsequent to surgery, the patient is noted to have increased irritability and progressively requires more IV pain medication throughout the night. He is anxious, argumentative, and refuses to comply with neurovascular assessments of his upper extremity. What is the best next step in treatment for this patient?
1
Provide diazepam (Valium) for anxiety and muscle spasms
2
Continue with ice, elevation, anti-inflammatory drugs to improve pain and swelling
3
Measure compartment pressures within the volar and dorsal forearm compartments
4
Return to the operating room for emergent volar and dorsal compartment fasciotomies
■ This patient is manifesting the signs of acute compartment syndrome (ACS). In the pediatric population, the 5 P's are less reliable signs of ACS. Instead, pediatric patients manifest increasing analgesic requirements, agitation, and anxiety in the evolution of ACS. Given this patient's clinical signs and risk factors for developing ACS (increased age/adolescence, male predominance, multiple fractures within an extremity), the appropriate treatment is to proceed with emergent forearm fasciotomies.
Administering diazepam (Valium) for the anxiety only masks the underlying condition, which may result in a poorer prognosis if the diagnosis is further delayed. Providing ice and elevation may be useful to diminish swelling and pain, but will not successfully treat the compartment syndrome. Importantly, the diagnosis of ACS is primarily a clinical one. Measuring compartment pressures may be more useful to help confirm or rule out the diagnosis in an obtunded child or one with severe mental/communication difficulty.
QUESTION 5 OF 50
Which of the following is the most likely origin for the greater medullary artery:
1
Lower cervical segmental
2
Middle thoraciCsegmental
3
Upper lumbar segmental
4
Upper thoraciCsegmental
5
Lower thoraciCsegmental
The major part of the blood supply of the spinal cord is provided by the medullary or radicular arteries. The only feeder for the lower thoraciCspinal cord is the greater medullary artery or artery of Adamkiwicz (T9-T11). One should remember that in the spine, the right-sided approach is preferred to avoid the aorta and segmental artery of Adamkiwicz
QUESTION 6 OF 50
Which subtype of Ehlers-Danlos syndrome (EDS) is caused by lysyl hydroxylase deficiency:
1
EDS type I
2
EDS type II
3
EDS type III
4
EDS type IV
5
EDS type VII
Many of the mutations responsible for the differing subtypes of Ehlers-Danlos syndrome (EDS) have not been identified (EDS types I, II, and III). Lysyl hydroxylase deficiency has been identified as the cause of type IV. A mutation in type I collagen has been identified as the cause of EDS VII.
QUESTION 7 OF 50
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be**
1
a program of shoulder strengthening exercises.
2
decompression of the nerve at the spinoglenoid notch.
3
decompression of the nerve at the transverse suprascapular ligament.
4
release of the fascial elements of the muscle tethering the nerve.
5
arthroscopy, repair of the posterior labrum lesion, and an anterior capsular shift.
Isolated palsy of the infraspinatus portion of the suprascapular nerve is common in volleyball players and is seen frequently in the throwing arm of baseball players. The exact cause is not known, but it may be the result of either tethering or traction on the nerve at the spinoglenoid notch. Synovial cysts in the spinoglenoid notch also can be a cause, but the patient’s negative MRI findings rule out that entity. Because many isolated nerve palsies of the infraspinatus branch are asymptomatic, initial management should always be nonsurgical. Surprisingly, many athletes with this injury can participate fully in sports. Surgical treatment with decompression at the notch is unpredictable and generally is indicated only if nonsurgical management fails.
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Martin SD, Warren RF, Martin TL, Kennedy K, O’Brien SJ, Wickiewicz TL: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
QUESTION 8 OF 50
Residual angulation <30° of the humeral shaft after nonoperative fracture treatment has been shown to have what effect on patient reported outcomes?
1
Angulation in the coronal plane has more effect on functional outcomes than in the sagittal plane.
2
Increased angulation corresponds with worse functional outcomes.
3
Angulation >5° in any plane results in an unacceptable cosmetic result.
4
Residual angulation has no correlation with functional outcomes.
Acceptable angulation of humeral shaft fractures for nonoperative treatment is quite generous due to compensatory motion at the shoulder joint. Traditionally, 20° of anterior-posterior and 30° of varus-valgus angulation is acceptable. Indications for surgery have included angulation outside of this range, open fractures, brachial plexus injury, polytrauma, or other factors that preclude functional bracing. Increased amounts of angulation at the conclusion of healing can result in cosmetic dissatisfaction, but this has not been correlated with any specific degree of angulation, as patient factors are a strong influencer. Increased angulation has not been shown to affect functional outcomes within the angulation range previously described.
QUESTION 9 OF 50
of 100
Figure 89 is the radiograph of this boy 3 months later. The patient and family ask if he can safely play baseball in the spring. He is pain free at this time. What is the best advice?
1
No sports allowed; recommend clavicle bump resection, contouring, and plating
2
No sports allowed; recommend clavicle bump resection (no plate needed)
3
Allow baseball as tolerated and careful follow-up
4
Recommend an electrical stimulator and advise him to change his sport and join the swim team
- Allow baseball as tolerated and careful follow-up
QUESTION 10 OF 50
The net effect of 1,25 dihydroxyvitamin D3 on the calcium and phosphate concentration of the extracellular fluid and serum is:
1
Increased calcium, increased phosphate
2
Increased calcium, decreased phosphate
3
Decreased calcium, decreased phosphate
4
Increased calcium, no effect on phosphate
5
Transient decrease in serum calcium
Parathyroid hormone, the active form of vitamin D (1,25 dihydroxyvitamin D), and calcitonin each have a net effect on calcium and phosphorus concentrations in extracellular fluid and serum:
Net Effect
Parathyroid hormone Increased serum calcium
Decreased serum phosphate
Vitamin D3 (1,25 dihydroxyvitamin D) Increased serum calcium
Increased serum phosphate
Calcitonin Decreased serum calcium
(transient) Correct Answer: Increased calcium, increased phosphate
QUESTION 11 OF 50
The erythrocyte sedimentation rate (ESR) returns to normal how long after a total hip replacement:
1
6 weeks
2
2 months
3
6 months
4
9 months
5
1 year
The ESR takes more than a year to return to normal after a total hip replacement
QUESTION 12 OF 50
Which of the following factors are not related to the success of brace treatment for idiopathic scoliosis?
1
C urve size at start of treatment
2
C urve correction in brace
3
Number of hours worn
4
Gender
5
Positive family history of scoliosis
A lower chance of curve control with brace treatment has been shown with curves greater than 40°, correction of less than 50% in brace, brace worn fewer than 16 hours per day, or male gender. Positive family history has not been shown to be related to curve progression or chance of control.
QUESTION 13 OF 50
A 12-year-old boy has had left thigh pain for the past 4 months. Examination shows lack of internal rotation and abduction, and external rotation with hip flexion. A radiograph is shown in Figure 87. What is the most appropriate treatment?
1
Physical therapy
2
In situ pinning
3
Reduction and percutaneous pinning
4
Surgical dislocation of the hip with reduction under direct vision
5
Spica casting
DISCUSSION: The patient has a stable slipped capital femoral epiphysis (SCFE). Preferred treatment of
stable SCFE is in situ pinning. In situ fixation of stable SCFE has an extremely low rate of osteonecrosis. Gentle postural reduction with hip capsulotomy or surgical dislocation of the hip with reduction has been
aPdvRoEcFaEteRdRfEoDr uRnsEtaSbPlOe NSSCEF: E2.
REFERENCES: Aronson DD, Peterson DA, Miller DV: Slipped capital femoral epiphysis: The case for
2010 Pediatric Orthopaedic Examination ook • 73
internal fixation in situ. Clin Orthop Relat Res 1992;281:115-122.
Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Figure 88a Figure 88b
QUESTION 14 OF 50
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip
pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
1
Cemented left total hip arthroplasty (THA)
2
Cementless left THA with a proximally porous coated femoral stem
3
Hybrid left THA
4
Cementless left THA with a diaphyseal engaging conical femoral stem
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
QUESTION 15 OF 50
-A 20-year-old concert pianist sustained a diaphyseal radius fracture and underwent open reduction and internal fixation 3 years ago. She is thin and reports that the plate is irritating her after playing the piano for an hour or more. She undergoes elective plate removal of the 3.5 mm plate and 2 weeks later she refractures the radius. Which of the following statements is most accurate?
1
Diaphyseal plate removals are at higher risk of refracture.
2
Postoperative splinting increases the chance of refracture.
3
The patient would not have sustained a refracture if the plate was 4.5 mm.
4
The risk of fracture increased because the plate was removed within 5 years.
5
Waiting 5 years to remove the hardware would have decreased the risk of refracture.
No detailed explanation provided for this question.
QUESTION 16 OF 50
A 22-year-old professional baseball pitcher has had pain in the axillary region of his dominant shoulder for the past several weeks. While throwing a pitch during a game, he notes a sharp pulling sensation with a “pop” in his shoulder. Examination the following day reveals tenderness along the posterior axillary fold and pain and weakness with resisted extension of the shoulder. What is the most likely cause of his symptoms?
1
Type 2 tear of the superior labrum anterior and posterior
2
Tear of the anterior labrum
3
Tear of the subscapularis tendon
4
Tear of the latissimus dorsi tendon
5
Tear of the supraspinatus tendon
Injury to the latissimus dorsi tendon recently has been reported as a cause of pain in the thrower’s shoulder. The etiology of this injury is felt to be eccentric overload during the follow-through of the throwing motion. Recommended management for this unusual injury consists of a short period of rest, followed by physical therapy to restore shoulder motion and strength. Throwing is allowed when the athlete demonstrates full, pain-free motion and good strength and balance of the rotator cuff and scapular rotator muscles. Currently there are no defined indications for surgical repair.
REFERENCES: Schickendantz MS, Ho CP, Keppler L, et al: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains and related injuries.
Magn Reson Imaging Clin N Am 1999;7:39-49.
Livesey JP, Brownson P, Wallace WA: Traumatic latissimus dorsi: Tendon rupture. J Shoulder Elbow Surg 2002;11:642-644.
QUESTION 17 OF 50
-What is the most common anatomic location of the lateral femoral cutaneous nerve?
1
Deep to the psoas muscle
2
Medial to the femoral vein
3
Under the inguinal ligament
4
Adjacent to the femoral nerve
5
Deep to the iliopectineal fascia
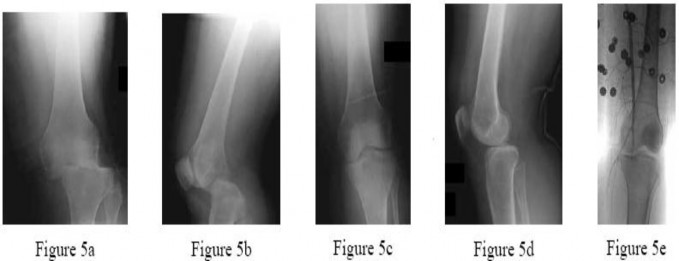
Knee dislocations are known to have a high risk for vascular injury. Although the specific treatment of various combinations of ligamentous injuries is controversial, the need for emergent revascularization is not. In this particular patient, after vascular repair, the most important initial concern is protection of the vascular repair. A spanning external fixator, especially in this patient with gross instability, will allow for easier assessment of vascular status, evaluation of fasciotomy wounds,
and temporary stability of the knee. A cylinder cast can stabilize the knee but will not allow wound assessment or room for inevitable post-injury/postoperative swelling. Diagnostic knee arthroscopy is not necessary, and ligamentous repair/reconstruction should be delayed until the vascular repair is stable. PREFERRED RESPONSE: 1
QUESTION 18 OF 50
The ABER (abducted and externally rotated) position in the shoulder MRI scan shown in Figure 1 can be helpful in identifying a variety of subtle pathologies including rotator cuff tears and capsulolabral injury. While in the ABER position, the humerus and glenoid are seen predominantly in what planes, respectively?
1
Sagittal and coronal
2
Coronal and axial
3
Axial and sagittal
4
Axial and coronal
While in the ABER position in the MRI machine, the MRI technician aligns the cut lines along the axis of the humerus and perpendicular through the glenoid, from superior to inferior. According to this, one might assume that the humerus would be seen in a sagittal plane and the glenoid in an axial plane. However, while the glenoid
does stay fixed in an axial plane, the humerus is externally rotated, resulting in a coronal view of the proximal humerus. All of the other options do not depict the anatomic relationship of the humerus and glenoid properly while in the ABER sequence.
QUESTION 19 OF 50
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. The patient fails an extensive course of physical therapy and is unable to return to baseball. He and his orthopaedic surgeon elect to proceed with surgery. During a repeat evaluation, he has negative sulcus and Beighton sign findings, and radiographs show 5° of glenoid retroversion. What is the most appropriate surgical plan?
1
Arthroscopic infraspinatus tenodesis
2
Arthroscopic posterior labral repair
3
Arthroscopic capsular shift and rotator interval closure
4
Posterior glenoid opening-wedge osteotomy
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through, as seen in this patient. The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion, at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The four muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the four rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation. This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Beighton sign findings would be negative), a posterior capsular shift with rotator interval closure is indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate. The most common complication seen after arthroscopic posterior labral repair is stiffness, followed by recurrent instability
and degenerative joint disease.
QUESTION 20 OF 50
Figures 1 through 3 are the radiographs of a 27-year-old man who has had wrist pain since falling 1 day ago. Which treatment offers the best prognosis for prevention of carpal collapse and progressive arthritis?
1
Long-arm cast
2
Percutaneous screw fixation
3
Open reduction and internal fixation (ORIF) with bone graft
4
Proximal row carpectomy
EXPLANATION:
Although this patient’s history includes a recent fall, the radiographs show evidence of a scaphoid nonunion with carpal collapse but no arthritis. Obtaining union of the scaphoid is important to prevent progressive carpal collapse and arthritic changes. ORIF with bone graft is most appropriate to obtain union and correct the collapse deformity. Screw fixation with volar wedge graft often is performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal
row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
QUESTION 21 OF 50
A 12-year-old boy sustains a Salter type II fracture of the proximal humerus during a fall. The fracture has an apex angulation of 40° anteriorly and laterally. The neurovascular examination is normal. The recommended treatment is:
1
Longitudinal traction in abduction followed by slowly bringing the arm into an abduction (airplane) splint
2
C losed reduction and percutaneous pin fixation
3
Open reduction and plate fixation
4
Skeletal traction in abduction with an olecranon pin
5
No formal reduction attempt, rather placement of the arm in a sling
Recommended treatment involves no formal reduction attempt, rather placement of the arm in a sling. This simple treatment is adequate for all patients with at least 2 years of growth remaining. This is due to the tendency to self-align, the remodeling potential, and the ability to tolerate some deformity in the region with no functional consequence.
The abduction splint is cumbersome. It is not necessary because simpler means are effective due to the young age and remodeling potential.
C losed reduction and pin fixation are not needed because adequate remodeling is expected. Any residual deformity is well tolerated in this region. The pins can sometimes cause significant soft tissue irritation in the bulky area of the shoulder. Plate fixation is not feasible because of the open physis. It is also not necessary because simpler means are available. Skeletal traction is not needed because the humerus will align itself better with time in a dependent position.
QUESTION 22 OF 50
What is the most common physical finding in a patient with femoroacetabular impingement (FAI)?
1
Increased external rotation
2
Increased abduction
3
Decreased external rotation
4
Decreased flexion and internal rotation
5
Decreased adduction
DISCUSSION: A loss of flexion and internal rotation are hallmarks of FAI. With the hip flexed 90 degrees, maximal internal rotation testing is also known as the anterior impingement test, causing deep groin pain and
reproduction of symptoms. Occasionally, a posterior impingement test will be positive with extension and external rotation. There are a variety of causes of FAI; however, the pathology limits motion as the femur (cam) and acetabulum (pincer) contact one another. Also, only one location needs to be present, such as cam- type or pincer-type versus both cam-pincer lesions to cause symptoms.
REFERENCES: Philippon MJ, Stubbs AJ, Schenker ML, et al: Arthroscopic management of femoroac- etabular impingement: Osteoplasty technique and literature review. Am J Sports Med 2007;35:1571 -1580, Siebenrock KA, Schoeniger R, Ganz R: Anterior femoroacetabular impingement due to acetabular retro- version: Treatment with periacetabular osteotomy. J Bone Joint Surg Am 2003;85:278 -286. Kubiak-Langer M, Tannast M, Murphy SB, et al: Range of motion in anterior femoroacetabular impingement. Clin Orthop Relat Res 2007;458:117-124.
QUESTION 23 OF 50
A 20-year-old college student sustains a closed distal one-third tibia fracture when he falls while skiing. Which of the following would be the most common fracture pattern and mechanism:
1
Short spiral fracture â torsion
2
Oblique fracture â uneven bending
3
Transverse fracture â pure bending
4
Oblique fracture with a butterfly fragment â bending and compression
5
Segmental fracture â four-point bending
This college student has sustained a low-energy twisting injury, also known as a boot-top injury. The fracture pattern is a short spiral fracture and the mechanism of injury is torsion loading of the tibia.
The other patterns included:
Oblique fracture â uneven bending: This type of injury typically occurs following motorcycle accidents when the tibia is subjected to uneven bending forces.
Transverse fracture â pure bending: This fracture is typical of a soccer injury because the tibia is subjected to pure bending forces.
Oblique fracture with a butterfly fragment â bending and compression: This is a common fracture that occurs with low- and high-speed injuries. These fractures may occur from car bumpers and motorcycles.
Segmental fracture â four-point bending: This pattern is typical of high-energy injury, such as a pedestrian being struck by a car bumper.
QUESTION 24 OF 50
Slide 1
A patient presents with a claw toe deformity (Slide). What is the strongest flexor of the metatarsophalangeal joint, which in this patient is not functioning adequately:
1
Flexor digitorum longus
2
Flexor digitorum brevis
3
Lumbrical
4
Volar plate
5
Interosseous
Although the long and short flexor tendons have some effect albeit indirect on the flexion of the metatarsophalangeal joint, the flexor that acts directly on the joint is the interosseous muscle. Intrinsic atrophy will lead to claw toe deformity.
QUESTION 25 OF 50
of 100
The pediatric service orders an MRI, and findings are unremarkable. Results from the tests ordered above are pending. The clinician should recommend
1
discharge home on crutches with an ibuprofen prescription.
2
discharge home with an oral antibiotic prescription.
3
initiation of intravenous (IV) antibiotics.
4
a knee CT scan.
- initiation of intravenous (IV) antibiotics.
QUESTION 26 OF 50
Which of the following factors most likely has a role in the production of osteoblastic bone metastases:
1
Receptor activator of nuclear factor-kB ligand (RANKL)
2
Parathyroid hormone-related protein (PTHrP)
3
Osteoprotegerin (OPG)
4
Endothelin-1
5
Macrophage inflammatory protein (MIP) 1 alpha
Endothelin-1 likely plays a major role in blastic metastases in breast and prostate cancers. Endothelin-1 stimulates bone formation and the proliferation of osteoblasts.
The mechanism of bone formation is not nearly as well defined as bone destruction in metastatic bone disease. Correct Answe Endothelin-1
QUESTION 27 OF 50
A patient underwent a right hip arthroscopy, CAM resection, and labral repair while positioned supine on a fracture table with a perineal post. The leg was in traction for 4 hours, and no intrasurgical complications were noted. At the 2‐week follow‐up appointment, the patient was experiencing numbness and tingling in the perineum on the surgical side and noted pain predominantly while sitting. What is the likely cause of these symptoms?
25
1
Traction injury to the sciatic nerve
2
Traction injury to the femoral nerve
3
Compression injury to the pudendal nerve
4
Direct injury to the lateral femoral cutaneous nerve
Although all of these responses are known complications related to hip arthroscopy, the symptoms of perineal numbness and pain associated with prolonged traction time indicate a compression injury to the pudendal nerve against the perineal post used to provide counter traction. Perineal numbness usually occurs on the surgical side, with pain in the area of the anus to the penis/clitoris. Pain is predominantly experienced while sitting, but is relieved when sitting on a toilet. Pain can be relieved with a diagnostic pudendal nerve block. This injury is not unique to hip arthroscopy; it also is described in the trauma literature. To prevent compression‐type injuries, a well‐padded post larger than 9 cm in diameter should be positioned against the medial thigh. Traction force should be kept to a minimum and the extremity positioned in slight abduction. Continuous traction time should not exceed 2 hours, with intermittent traction used during prolonged procedures.
QUESTION 28 OF 50
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
1
an elastic bandage, cold packs, and weight bearing as tolerated.
2
non-weight-bearing and a CT scan of the talus.
3
cast immobilization for 10 days, followed by progressive rehabilitation.
4
cast immobilization for 6 weeks, followed by progressive rehabilitation.
5
stirrup splinting, cold packs, and aggressive rehabilitation.
Because there is a significant possibility that the patient may have a fracture of the lateral process of the talus, there is some disagreement as to the best radiographic study to identify this injury. A CT scan is an appropriate diagnostic tool to visualize the fracture and identify any displacement. Displaced lateral process fractures are best treated surgically.
REFERENCES: Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder’s foot and ankle. Am J Sports Med 1998;26:271-277.
Ebraheim NA, Skie MC, Podeszwa DA, Jackson WT: Evaluation of process fractures of the talus using computed tomography. J Orthop Trauma 1994;8:332-337.
QUESTION 29 OF 50
Which of the following clinical findings is commonly associated with symptomatic partial-thickness rotator cuff tears?
1
Negative impingement signs
2
Abnormal lift-off test
3
External rotation lag sign
4
Painful arc with active range of motion
5
Mismatch in active and passive motion
In symptomatic partial-thickness rotator cuff tears, a painful arc with active range of motion is common, impingement signs are usually positive, and the lift-off test is normal. Active and passive range of motion measurements are often equal, although active range of motion can be painful. External rotation lag signs are often seen with larger full-thickness tears.
REFERENCES: Hertel R, Ballmer FT, Lambert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313.
McConville OR, Iannotti JP: Partial thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43.
Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Fukuda H: Partial-thickness rotator cuff tears: A modern view on Codman’s classic. J Shoulder Elbow Surg 2000;9:163-168.
QUESTION 30 OF 50
of 100 Figure 50 is the radiograph of a 68-year-old man who has anterior knee pain 6 months after total knee arthroplasty. His knee is flexed 45 degrees. Anteroposterior and lateral radiographs show satisfactory size and alignment of the components. This patient has knee range of motion from 0 to 75 degrees. What is the most appropriate next step in his evaluation?
1
MR images with metal artifact reduction
2
Dynamic fluoroscopy
3
CT images of the femoral and tibial components
4
30-degree, 60-degree, and 90-degree patellar radiographs
46
The patient’s radiograph demonstrates patellar instability. He has both pain and suboptimal range of motion following knee arthroplasty. Several considerations may contribute to loss of range of motion, but rotational malalignment of the components is a primary consideration for patients with otherwise well-aligned, well-fixed knee arthroplasties complicated by patellar instability. CT images have demonstrated value in evaluation of femoral and tibial component rotational malalignment. Radiographs in variable degrees of flexion are not necessary because the patient has documented patellar instability on his 45-degree flexion radiograph. Dynamic fluoroscopy may demonstrate ligamentous instability, but does not readily demonstrate patellofemoral tracking. Even with use of a metal-suppression technique, MR image artifact limits its usefulness in evaluating this clinical concern.
RECOMMENDED READINGS
1. Peters CL, Crofoot CD. Knee reconstruction and replacement. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:457-471.
2. [Berger RA, Crossett LS, Jacobs JJ, Rubash HE. Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res. 1998 Nov;(356):144-53. PubMed PMID: 9917679.](http://www.ncbi.nlm.nih.gov/pubmed/9917679)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9917679)
3. [Jazrawi LM, Birdzell L, Kummer FJ, Di Cesare PE. The accuracy of computed tomography for determining femoral and tibial total knee arthroplasty component rotation. J Arthroplasty. 2000 Sep;15(6):761-6. PubMed PMID: 11021452.](http://www.ncbi.nlm.nih.gov/pubmed/11021452)[View](http://www.ncbi.nlm.nih.gov/pubmed/11021452)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11021452)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11021452)
4. [Kelly MA. Extensor mechanism complications in total knee arthroplasty. Instr Course Lect. 2004;53:193-9. Review. PubMed PMID: 15116613.](http://www.ncbi.nlm.nih.gov/pubmed/15116613)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15116613)
RESPONSES FOR QUESTION 51 THROUGH 55
Match the image above with the description below.
47
A B
C
D
48
E F
QUESTION 31 OF 50
Which of the following structures is the most important restraint to posterior subluxation of the glenohumeral joint when positioned in 90 degrees of flexion and internal rotation?
1
Subscapularis muscle and tendon
2
Supraspinatus muscle and tendon
3
Middle glenohumeral ligament
4
Inferior glenohumeral ligament
5
Coracohumeral ligament
The posterior band of the inferior glenohumeral ligament is the most important restraint to posterior subluxation of the glenohumeral ligament with the shoulder in 90 degrees of flexion and internal rotation. With the shoulder in external rotation, the subscapularis is an important stabilizer to posterior subluxation. When the shoulder is in neutral rotation, the coracohumeral ligament is the primary stabilizer. The middle glenohumeral ligament functions primarily to resist anterior translation of the shoulder in the midrange of abduction. The supraspinatus muscle and tendon have relatively little contribution to anterior and posterior translation of the glenohumeral joint.
REFERENCES: Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML: Posterior glenohumeral subluxation: Active and passive stabilization in a biomechanical model. J Bone Joint Surg Am 1997;79:433-440.
Flatow EL, Warner JI: Instability of the shoulder: Complex problems and failed repairs: Part I. Relevant biomechanics, multidirectional instability, and severe glenoid loss. Instr Course Lect 1998;47:97-112.
QUESTION 32 OF 50
The most frequent location for osteochondral lesions of the talar dome is:
1
Anterolateral talar dome (Raikin zone 3)
2
Posteromedial talar dome (Raikin zone 7)
3
Lateral talar dome, mid-body (Raikin zone 6)
4
Medial talar dome, mid-body (Raikin zone 4)
5
Anteromedial talar dome (Raikin zone 1)
A survey of 428 osteochondral lesions of the talus was undertaken using a nine zone anatomical grid system to determine the most frequent location in which these lesions occur. Results showed that 62% of lesions occurred in the medial talar dome and
34% over the lateral talar dome. The most frequent location along the medial dome was the mid-body of the talus. Medial lesions were larger in surface area as well as deeper than lateral lesions.
QUESTION 33 OF 50
Which of the following can be seen in the heart of a well-conditioned athlete?
1
Decreased stroke volume
2
Decreased cardiac output
3
Decreased resting heart rate
4
Decreased ventricular wall thickness
5
Decreased vagal tone
DISCUSSION: The well-conditioned heart of an athlete leads to increased ventricular wall thickness which in turn increases the amount of blood ejected from the heart per given stroke (stroke volume). The increased parasympathetic (vagal) tone also leads to a lower (decreased) resting heart rate. Cardiac output is equal to stroke volume x heart rate and is increased during exercise in a well-conditioned athlete.
REFERENCES: Basilico FC: Cardiovascular disease in athletes. Am J Sports Med 1999;27:108-121. Huston TP, Puffer JC, Rodney WM: The athletic heart syndrome. N Engl J Med 1985;313:24-32.
An 18-year-old boxer sustained a blow to his right eye in a boxing match. Examination on the sideline reveals hyphema, reduced visual acuity and color vision, and a visual field cut. What is the next step in management?
1. #### Eye patch and ophthalmology evaluation in 2 days
2. #### Fluorescein eye stain
3. #### Emergent CT
4. #### High-dose systemic steroids
5. #### Observation PREFERRED RESPONSE: 3
DISCUSSION: With the examination demonstrating reduced visual acuity and visual field changes,
2010 Sports Medicine Examination Answer Book • 81
QUESTION 34 OF 50
**CLINICAL SITUATION**
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
Which factors will lead a surgeon to pursue fracture fixation and acute total hip arthroplasty instead of fixation alone? ---
1
Age > 50 years, marginal impaction, posterior wall comminution
2
BMI > 50, femoral head damage, prior hip surgery
3
Posterior wall comminution, worker’s compensation injury, femoral head damage
4
Age > 50 years, history of smoking, diabetes mellitus Discussion: A
The patient sustained a posterior wall fracture dislocation. For acetabular fractures, the position of the limb in space at the time of impact (in terms of the amount of flexion/extension, internal/external rotation, and adduction/abduction) will dictate the fracture pattern. For posterior wall fracture patterns, the limb is in some degree of flexion, adduction, and internal rotation. Other combinations are possible to contribute to an acetabular fracture but not likely to contribute to a posterior wall pattern.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified
posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in . In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage, there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling. Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
QUESTION 35 OF 50
An erythrocyte sedimentation rate (ESR) of what level is considered a good cutoff for guiding an index of suspicion for infection:
1
10 mm/hr
2
20 mm/hr
3
30 mm/hr
4
40 mm/hr
5
60 mm/hr
With an ESR of 30 mm/hr to 35 mm/hr, sensitivities have been reported from 0.60 to 0.96 and specificities from 0.65 to
1
QUESTION 36 OF 50
Which of the following blood vessels supplies the majority of the scaphoid:
1
Superficial palmar branch of the radial artery (volar)
2
Radial artery
3
Dorsal carpal branch of the radial artery (dorsal)
Gelberman and Menon used injection studies to demonstrate that the majority of scaphoid blood flow stems from branches of the radial artery entering the scaphoid at the distal pole. Of these, the branch entering the dorsal ridge supplies 70% to 80% of the intraosseous vascularity of the scaphoid bone. The proximal pole is completely dependent on the intraosseous blood supply and is vulnerable to avascular necrosis when fracture disrupts this vascular source.
QUESTION 37 OF 50
What surgical technique has been associated with increased risk for recurrent dislocation after revision total hip arthroplasty?
1
Posterior capsulorrhaphy
2
Use of a jumbo cup
3
Use of a lateralized liner
4
Use of a larger femoral head diameter
When addressing recurrent dislocation after total hip arthroplasty, surgical considerations that must be addressed include approach, soft-tissue tension, component positioning, impingement, head size, and acetabular liner profile. These considerations most often involve tensioning or augmentation of soft tissues, as in capsulorrhaphy or trochanteric advancement; correction of malpositioned components; use of larger femoral head sizes that increase motion before impingement; improving the head-to-neck ratio; and increasing femoral offset. The use of a larger-diameter acetabular component may lead to soft-tissue overgrowth around the liner, causing impingement and increasing the risk for recurrent dislocation.
QUESTION 38 OF 50
Slide 1 Slide 2 Slide 3
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The genetic pattern seen in patients with this type of presentation is:
1
Autosomal recessive
2
Autosomal dominant
3
Sex-linked recessive
4
Sex-linked dominant
5
Sporadic
Multiple hereditary exostoses is inherited in an autosomal-dominant manner with 90% penetrance.
QUESTION 39 OF 50
of 100
Figures 37a through 37c are the radiographs of a 45-year-old construction worker who has severe wrist pain. He has failed nonsurgical measures and requests surgery. The most appropriate surgical option is
1
bone graft with fixation of the scaphoid.
2
proximal row carpectomy.
3
scaphoid excision with 4-corner fusion.
4
total wrist joint replacement.
The radiographs show a long-standing scaphoid nonunion with avascular necrosis and collapse of the proximal pole. This is referred to as a scaphoid nonunion advanced collapse wrist. He also has advanced arthritis of the capitolunate joint. This patient has a physically demanding occupation, so the best option for him is scaphoid excision with 4-corner fusion. Proximal row carpectomy would be inappropriate because of the advanced arthritis of the capitolunate joint. This procedure’s success is reliant upon normal cartilage/joint articulation of the capitate and lunate fossa of the distal radius. A total wrist replacement is not appropriate for a man with a physically demanding job. Finally, the patient has a long-standing scaphoid nonunion with advanced proximal pole collapse. Therefore, bone grafting with fixation is not an option at this point.
RECOMMENDED READINGS
23. [Weiss KE, Rodner CM. Osteoarthritis of the wrist. J Hand Surg Am. 2007 May-Jun;32(5):725-46. Review. PubMed PMID: 17482013.](http://www.ncbi.nlm.nih.gov/pubmed/17482013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17482013)
24. [Shah CM, Stern PJ. Scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC) wrist arthritis. Curr Rev Musculoskelet Med. 2013 Mar;6(1):9-17. doi: 10.1007/s12178-012-9149-4. PubMed PMID: 23325545. ](http://www.ncbi.nlm.nih.gov/pubmed/23325545)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23325545)
QUESTION 40 OF 50
This muscle group demonstrates electrical activity at the time of heel strike:
1
Anterior compartment
2
Intrinsic foot muscles
3
Lateral compartment
4
Deep posterior compartment
5
Medial compartment
The anterior muscle compartment, in particular, the anterior tibialis, is active during heel strike, to maintain foot dorsiflexion, and prevent foot drop during heel strike.
QUESTION 41 OF 50
of 100 During an anterior approach to the bicipital 53
tuberosity, you encounter a nerve overlying the brachioradialis fascia (Figure 58). It provides innervation to the
1
flexor pollicis longus.
2
skin on the anteromedial forearm.
3
skin on the anterolateral forearm.
4
extensor indicis proprius.
The structure shown is the lateral antebrachial cutaneous nerve (LABC). It is the terminal sensory branch of the musculocutaneous nerve and runs superficial to the brachioradialis. It supplies sensation to the anterolateral surface of the forearm. The flexor pollicis longus is innervated by the anterior interosseous nerve. The extensor indicis proprius is innervated by the radial nerve. The LABC does not innervate the skin of the anteromedial forearm. Careful
identification and protection of this nerve is critical to prevent the most common nerve injury during distal biceps repair.
RECOMMENDED READINGS
1. Agur AM. Grant's Atlas of Human Anatomy. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:460.
2. Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1994:118-125.
RESPONSES FOR QUESTIONS 59 THROUGH 61
Please select the image that represents the most appropriate response to the question or statement below.
54
A B
C D
QUESTION 42 OF 50
Which of the following portions of a gene directly codes for the messenger RNA for eventual translation into proteins on the ribosome:
1
Promoter region
2
Intron
3
Exon
4
Coding region
5
Activator or repressor binding site
The human genome is composed of approximately 30,000 unique genes. Each gene is composed of a promotor or regulator region and a transcriptional or coding region. Regulatory proteins or transcription factors bind to the promoter region of the gene
to signal the beginning of transcription of the DNA into RNA or repress the expression of the gene. The coding region contains both introns and exons. Exon sequences of the gene directly code for the proteins, and the introns are spacers. The intron sequences are enzymatically removed from the newly transcribed messenger RNA by a splicing mechanism
QUESTION 43 OF 50
Figure 1 is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence? ---
1
Sclerotherapy
2
Shave excision with cautery
3
Cryotherapy
4
Wide surgical excision
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision (Figures below) is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.
---
QUESTION 44 OF 50
A 3-year-old girl is brought in for evaluation of leg alignment. She has bilateral foot progression angles of 35° internal. Her thigh-foot angles are 40° internal. Her hip rotation in the prone position is 50° external and 30° internal. The metaphyseal- diaphyseal angle is 2° on each side. Recommended treatment includes:
1
Denis Browne bar with feet 45° outward
2
Bilateral double-upright knee-ankle-foot orthoses
3
Femoral derotation osteotomy
4
Tibial osteotomy
5
Observation
The tibial torsion described has an excellent chance of resolution over time. Observation is indicated.
This child has tibial torsion. The Denis Browne bar has not been proven to affect the natural history of tibial torsion. The knee-ankle-foot orthoses are used for genu varum, which is not the primary problem in this case.
A femoral osteotomy is rarely used to correct femoral anteversion in older children. A tibial osteotomy is rarely used to correct tibial torsion in older children.
QUESTION 45 OF 50
of 100
Figures 1 and 2 are the clinical photograph and radiograph of a newborn who is seen for evaluation of his feet. A rigid rocker bottom foot is present with dorsal foot crease. The most appropriate next step in management is
1
serial casting with talonavicular reduction and fixation and Achilles tenotomy.
2
operative release at age 18 months.
3
tendon transfer after age 18 months.
4
observation, physical therapy, and transition into an ankle foot orthosis.
■ Congenital vertical talus is a rare condition in which the navicular is dorsally dislocated on the talus. There is also hindfoot equinus and valgus, resulting in the rocker bottom appearance. Fifty percent of cases are associated with other conditions (arthrogryposis, chromosomal abnormalities, skeletal dysplasia, myelomeningocele). Once the diagnosis is confirmed, usually on a plantar flexion lateral radiograph (the first MT does not align with the first metatarsal), treatment with serial casting described by Dobbs and associates is instituted. Once the talus lines up with the first metatarsal, surgical reduction of the talonavicular joint with pinning and Achilles tenotomy are done to correct the deformity.
QUESTION 46 OF 50
Which of the following proteins negatively affects osteoclast precursor cells:
1
Receptor activator of nuclear factor-kB (RANK)
2
Osteoprotegerin
3
Bone morphogenetic protein-7
4
C ore binding factor alpha 1 (C bfa1)
5
Parathyroid hormone related protein (PTHrP)
Four proteins that regulate osteoclast activation have been discovered:
1/. RANK binds to a receptor on osteoclast precursor cells and positively effects their final differentiation into osteoclasts.
2/. Osteoprotegerin is a soluble decoy receptor that resembles RANK and inhibits osteoclasts.
3/. Tumor necrosis factor-related activation induced cytokine (TRANC E)
4/. Osteoclast differentiation factor
Note:
C bfa1 is a transcription factor (coded by the C bfa1 gene) that is necessary and sufficient for differentiation of cells into osteoblasts and facilitates chondrocyte differentiation during enchondral bone formation.
QUESTION 47 OF 50
The distinction between a Lauge-Hansen supination-external rotation III injury and a Lauge-Hansen supination-external rotation
IV injury is:
1
A spiral oblique fracture of the lateral malleolus
Posteroinferior tibiofibular ligament (PITFL) disruption or posterior malleolus fracture
4
Deltoid ligament disruption or medial malleolus fracture
5
Anterior talo-fibular ligament disruption
The sequence of injury according to the Lauge-Hansen classification system in supination-external rotation injuries is AITFL disruption, spiral oblique fracture of the lateral malleolus, PITFL disruption or posterior malleolus fracture, and finally stage IV, which is a deltoid ligament disruption or medial malleolus fracture.
QUESTION 48 OF 50
of 100
Figures 1 and 2 are the radiographs of a 21-year-old man who has a long history of thoracic back pain. His lumbar spine is asymptomatic. He has failed prolonged nonsurgical treatment. Surgical correction should consist of
1
anterior release and fusion at T4-10.
2
posterior instrumentation and fusion at T9-L5.
3
posterior instrumentation and fusion at T2-L2.
4
posterior instrumentation and fusion at T6-pelvis.
■ When planning surgical intervention for Scheuermann kyphosis, it is imperative that the instrumentation and fusion extend across the entirety of the deformity. Distally, this means extending across the first lordotic disk space. In this scenario, this disk is the L1-L2 disk, which means the fusion needs to extend to L2. Shorter and longer fusions are not necessary or appropriate.
QUESTION 49 OF 50
of 100
A 47-year-old man undergoes a 3-column osteotomy as part of scoliosis surgery. During closure, somatosensory-evoked potentials decrease.
1
Proximal junctional kyphosis (PJK)
2
Adjacent segment degeneration
3
Intraoperative neurological injury
4
Postsurgical wound infection
- Intraoperative neurological injury
QUESTION 50 OF 50
of 100
Which factor is most important when making a decision regarding surgery with this patient?