This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set ECD517)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
Which combination of muscle weakness is typically associated with hereditary sensory motor neuropathy:
1
Anterior tibial, extensor hallucis longus
2
Peroneus longus, extensor hallucis brevis
3
Gastrocnemius, peroneus brevis
4
Posterior tibial, extensor digitorum brevis
5
Anterior tibial, peroneus brevis
The peroneus brevis is usually the first muscle to atrophy. Varying patterns of loss of the other muscles of the lower extremity include the anterior tibial and, in particular, the intrinsic foot muscles. Weakness in these muscles accounts for the cavus and the claw foot deformities noted in patients with hereditary sensory motor neuropathy.
QUESTION 2 OF 50
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
1
Inferior glenohumeral ligament
2
Middle glenohumeral ligament
3
Superior labrum
4
Subscapularis tendon
5
Supraspinatus tendon
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury.
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
QUESTION 3 OF 50
A 15-year-old diver has had persistent, activity-related low back pain for the past 2 months. He denies any history of trauma. Examination reveals that the pain is localized to the lumbosacral junction, and there are no radicular symptoms. The pain is worse with back extension. Neurologic examination is normal, as are AP, lateral, and oblique radiographs of the lumbosacral spine. Further evaluation should include
1
flexion and extension radiographs of the lumbosacral spine.
2
diskography.
3
an MRI scan of the lumbosacral spine.
4
a bone scan with single proton emission computed tomography (SPECT).
5
a renal ultrasound.
Spondylolysis may develop as a stress fracture resulting from repetitive hyperextension during athletic activities. In young people, the pars interarticularis is thin, the neural arch has not yet reached maximum strength, and the intravertebral disk is less resistant to shear. While clinical symptoms may lead to the suspicion of spondylolysis, radiographic confirmation may be difficult in early cases. Plain radiographs may be negative initially, and the plain MRI scan may not offer good visualization of the pars. A bone scan with SPECT is very sensitive initially. CT scans with regular axial and reverse-gantry angled cuts may help determine the type of fracture and the course of treatment.
REFERENCES: Congeni J, McCulloch J, Swanson K: Lumbar spondylolysis: A study of natural progression in athletes. Am J Sports Med 1997;25:248-253.
Harvey CJ, Richenberg JL, Saifuddin A, Wolman RL: The radiological investigation of lumbar spondylolysis. Clin Radiol 1998;53:723-728.
QUESTION 4 OF 50
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
1
Impingement injection test
2
Lift-off test
3
Weakness with “empty-can” abduction test
4
Load-and-sift maneuver
5
MRI with contrast
Postoperative subscapularis detachment can be identified with a positive lift-off test that reveals weakness in internal rotation. This complication does not necessarily compromise the anterior capsule repair. The load-and-sift maneuver and articular contrast studies may be normal. Supraspinatus tests for impingement and weakness should be negative.
REFERENCES: Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
QUESTION 5 OF 50
of 100
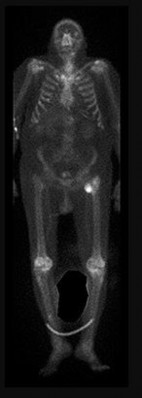
Figures 12a and 12b are a recent radiograph and a whole-body bone scan of an 81-year-old man who has hip pain and difficulty walking. His medical history is significant for obesity, hypertension, chronic kidney disease, and coronary artery disease. An examination demonstrates
moderate tenderness with passive range of motion of the left hip and an inability to actively flex the left hip against gravity. What is the best next step?
1
Dynamic hip screw
2
Long cephalomedullary nail
3
Staging studies
4
Toe-touch weight-bearing activity for 6 weeks
This patient has no known history of active malignancy. The radiograph shows a lesser trochanteric avulsion fracture (a fracture routinely associated with an underlying neoplasm). The bone scan reveals no other bone lesions. The femur fracture is statistically most likely to occur because of metastatic disease, but, without other evidence of metastasis, a primary bone sarcoma is possible, and biopsy is recommended before surgical fixation. Observation of this fracture, which is pathognomonic for neoplastic disease, is strongly discouraged.
RECOMMENDED READINGS
17. Adams SC, Potter BK, Mahmood Z, Pitcher JD, Temple HT. Consequences and prevention of inadvertent internal fixation of primary osseous sarcomas. Clin Orthop Relat Res. 2009 Feb;467(2):519-25. doi: 10.1007/s11999-008-0546-3. Epub 2008 Oct 21. PubMed PMID: 18937020.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18937020)
18. [Herren C, Weber CD, Pishnamaz M, Dienstknecht T, Kobbe P, Hildebrand F, Pape HC. Fracture of the lesser trochanter as a sign of undiagnosed tumor disease in adults. Eur J Med Res. 2015 Sep 4;20:72. doi: 10.1186/s40001-015-0167-8. PubMed PMID: 26336955. ](http://www.ncbi.nlm.nih.gov/pubmed/26336955)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26336955)
19. Rouvillain JL, Jawahdou R, Labrada Blanco O, Benchikh-El-Fegoun A, Enkaoua E, Uzel M. Isolated lesser trochanter fracture in adults: an early indicator of tumor infiltration. Orthop Traumatol Surg Res. 2011 Apr;97(2):217-20. doi: 10.1016/j.otsr.2010.11.005. Epub 2011 Feb 26. PubMed PMID:
[21354885/. ](http://www.ncbi.nlm.nih.gov/pubmed/21354885)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21354885)
QUESTION 6 OF 50
During a posterior cruciate ligament (PCL)-retaining total knee arthroplasty, a critical principle to remember
is to
1
accurately tension the PCL.
2
use bony resection to adjust the joint line.
3
maintain a small amount of residual deformity.
4
use intraoperative fluoroscopy to ensure femoral roll back.
Maintenance of the joint line and accurately tensioning the PCL are critical in the proper execution of a PCL-retaining total knee arthroplasty. Appropriate tension helps ensure femoral rollback and avoid stiffness or instability. Raising the joint line to help ensure full extension should be avoided in cruciate- retaining knees, because doing so creates an unfavorable kinematic environment. The three important principles of surgical technique needed to maintain appropriate tensioning of the PCL include 1) choosing the proper femur size to reproduce the native femoral anterior/posterior dimension, 2) reproducing the joint line by resecting as much tibia from the healthy side as will be replaced by the smallest thickness of the tibial component and, 3) ensuring that full extension is achieved by soft-tissue releases and not by taking additional distal femur, as may be done in a posterior stabilized approach. Another important principle is to re-create the natural degree of the patient’s posterior tibial slope to avoid tightness in
flexion.
QUESTION 7 OF 50
A 65-year-old woman with a history of diabetes mellitus and plantar ulcers has an erythematous and swollen right foot and ankle. Despite IV antibiotics, the erythema spreads to her lower calf within 24 hours. She has a systolic blood pressure of 80/55 mm Hg and a pulse rate of 120. Laboratory studies show a creatinine level of 1.5 mg. Initial management should consist of
1
continued IV antibiotics and observation.
2
hyperbaric oxygen treatment.
3
rapid IV fluid boluses.
4
surgical debridement.
5
whirlpool therapy.
Necrotizing fasciitis is an aggressive and rapidly spreading soft-tissue infection, usually caused by group A beta-hemolytic Streptococcus pyogenes. Presentation is typical of a rapidly ascending cellulitis, recalcitrant to antibiotic treatment. Differentiation between cellulitis and impetigo is difficult, and success depends on a high level of suspicion. The skin and subcutaneous tissues are affected, with sparing of the muscles. Septic shock and multi-organ system failure can be fatal. Treatment is aggressive surgical debridement with broad-spectrum antibiotics. Repeat irrigation and debridement may be necessary. Hyperbaric oxygen studies have shown inconsistent results.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 199-205.
Fontes RA Jr, Ogilvie CM, Miclau T: Necrotizing soft-tissue infections. J Am Acad Orthop Surg 2000;8:151-158.
QUESTION 8 OF 50
Which of the following blood vessels supplies the majority of the scaphoid:
1
Superficial palmar branch of the radial artery (volar)
2
Radial artery
3
Dorsal carpal branch of the radial artery (dorsal)
Gelberman and Menon used injection studies to demonstrate that the majority of scaphoid blood flow stems from branches of the radial artery entering the scaphoid at the distal pole. Of these, the branch entering the dorsal ridge supplies 70% to 80% of the intraosseous vascularity of the scaphoid bone. The proximal pole is completely dependent on the intraosseous blood supply and is vulnerable to avascular necrosis when fracture disrupts this vascular source.
QUESTION 9 OF 50
Which of the following rotator cuff tears is the simplest to repair:
1
U-shaped tear
2
L-shaped tear
3
Crescent-shaped tear
4
Vertical cleavage tear
5
Parrot-beak tear
Crescent-shaped tears are the simplest of all tears to repair and demonstrate minimal retraction and excellent mobility. They can be repaired directly to the bone with minimal tension. The anchors are placed percutaneously using a spinal needle. Suture passing techniques are then used and the rotator cuff is tied down. Vertical cleavage and parrot-beak tears refer to meniscal injuries in the knee
QUESTION 10 OF 50
Excessive anteversion of the acetabular cup may lead to:
1
Cup medialization
2
Posterior implant impingement
3
Leg length discrepancy
4
Premature osteolysis
5
Dislocation with excessive internal rotation
Excessive anteversion leads to anterior dislocation due to posterior component impingement. This most commonly occurs through extension and external rotation of the lower extremity. Excessive anteversion has little or no direct effect on medialization of the cup, leg length disparity, or premature osteolysis
QUESTION 11 OF 50
When evaluating a patient with a lumbar burst fracture, the integrity of the posterior ligamentous complex must be evaluated. Which of the following is a complete and accurate list of the components of the posterior ligamentous complex?
1
Supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joint capsules
Supraspinous ligament, interspinous ligament, and ligamentum flavum
4
Supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joints
5
Supraspinous ligament, interspinous ligament, ligamentum flavum, facet joint capsules, facet joints, and the posterior longitudinal ligament
DISCUSSION: The components of the posterior ligamentous complex are the supraspinous ligament,interspinous ligament, ligamentum flavum, and the facet joint capsules. Recent studies have emphasized the importance of the posterior ligamentous complex. The Thoracolumbar Injury Classification and Severity Score (TLICS) is a classification system that allows for efficient and effective classification of thoracolumbar spine injuries. It evaluates three characteristics of the injury:
No detailed explanation provided for this question.
QUESTION 12 OF 50
The virus associated with the most immune reactions is:
1
Adeno-associated virus
2
Gutted adenovirus
3
Adenovirus
4
Retrovirus
5
Herpes simplex virus
Adenoviral vectors can cause inflammatory reaction due to immune activation, an event linked to the first death related to gene therapy. This occurred in September 1999 at the University of Pennsylvania in a clinical trial in which an 18-year-old patient received infusion of more than a trillion adenoviral vectors directed to his liver, which triggered a systemiCinflammatory response that became uncontrollable, leading to organ failure and death. Newer-generation gutted or gutless adenovirus vectors are nonimmunogenic
QUESTION 13 OF 50
of 100
Indicates the anterior center edge angle
1
Figure 51a
2
Figure 51b
3
Figure 51c
4
Figure 51d
5
Figure 51e
- Figure 51d_
QUESTION 14 OF 50
of 100
Regarding the anteromedial and posterolateral bundles of the injured structure, which relationship is the most accurate?
1
Parallel in extension and externally rotated in flexion
61
2
Parallel in extension and internally rotated in flexion
3
Externally rotated in extension and parallel in flexion
4
Internally rotated in extension and parallel in flexion
- Parallel in extension and externally rotated in flexion
QUESTION 15 OF 50
A 25-year-old female presents to the emergency room for the fourth time in the last week. She has vague complaints of extremity pain. Physical examination by a male ER resident has been limited each visit because she is terrified of the pain that the clinician may cause. On physical examination, she is withdrawn and frightened.
Regions of ecchymosis are noted throughout chest and abdomen. She has requested multiple radiographs, MRI and CT scans. Today's imaging (radiographs, MRI, CT scan) has been unrevealing. What is the most likely diagnosis?
1
Malingering
2
Complex regional pain syndrome
3
Anxiety disorder
4
Intimate partner violence
5
Fibromyalgia
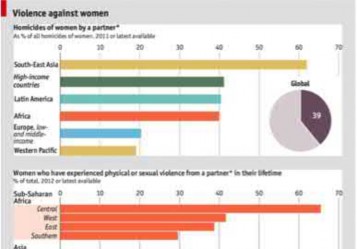
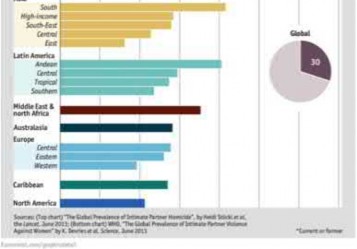
Based on the history and clinical presentation, the most likely diagnosis is intimate partner violence.
Domestic violence or intimate partner violence can be in the form of mental or physical abuse, neglect or abandonment. Close to 25% of women will experience domestic violence. Risk factors include young age (19-29 years of age), females, pregnancy and lower socioeconomic status. Affected patients will have repeated visits to the emergency room, find reasons to stay in a treatment facility for an extended period of time and constantly seek approval
of their partner.
Shields et al. reviewed factors influence outcome in treatment of patients affected by domestic violence. They found that positive outcomes were associated with interdisciplinary approaches to management. This included better history assessment, providing written documentation regarding intervention and better access to information on community resources.
Illustration A is a chart documenting the frequency of female domestic violence throughout the world as of 2012.
Incorrect Answers
Answers 1, 2, 3, 5: These conditions are not consistent with this patient’s history.
QUESTION 16 OF 50
Transfer of the extensor hallucis longus tendon to the first metatarsal and arthrodesis of the hallux interphalangeal joint is indicated for which of the following deformities:
1
A 36-year-old patient with a cavus foot following a compartment syndrome
2
A 20-year-old patient with a flexible cavovarus deformity
3
C orrection of hallux varus deformity
4
C orrection of a laceration of the extensor hallucis longus
5
A 42-year-old patient with C harcot-Marie-Tooth disease and pes planovalgus deformity
C orrection of the claw hallux and first metatarsal equinus deformity may be accomplished by transfer of the extensor hallucis longus tendon and arthrodesis of the hallux interphalangeal joint. Once the deformity of the forefoot is fixed (e.g., following a compartment syndrome), the extensor hallucis longus tendon can no longer dorsiflex the first metatarsal. Although C harcot-Marie- Tooth disease is often associated with a cavus foot, the transfer is not indicated when a planovalgus foot is present.
QUESTION 17 OF 50
Based on the best available evidence, what is the maximum number of days at which a successful manipulation can be performed following collagenase injection?
1
7
2
5
3
3
4
1
In the original clinical trial, the authors performed manipulation at 24 to 72 hours following the collagenase injection for Dupuytren disease. Evidence now suggests that up to 7 days is a safe and well-_tolerated interval for manipulation following collagenase injection._
QUESTION 18 OF 50
Which of the following findings on a neuromuscular examination is not characteristic of spasticity:
1
Hyperreflexia
2
C lonus
3
Velocity-dependent resistance
4
Writhing movements
5
Muscle contracture
Spasticity is a hallmark of upper motor lesions. Spasticity is characterized by hyperreflexia, clonus, and velocity-dependent resistance. After early childhood, muscle contracture also develops. Writhing movements are characteristic of athetosis, not spasticity.
QUESTION 19 OF 50
A magnetic resonance image of a 7-year-old girl shows a line of high-signal intensity within the cord on T2 sequences that parallels the ventral surface of the cord and appears as a syrinx. However, on the axial images and on the T1 sequences, this finding is not evident. The most likely diagnosis is:
1
C ollapsing syrinx
2
Gibbs artifact
3
Motion artifact
4
Ependymoma
5
Astrocytoma
A Gibbs artifact is a linear focus in the cord on T2-weighted images that parallels the ventral aspect of the cord and mimics a syrinx. The Gibbs artifact is due to the linear interface between two tissues of differing signal intensity. It is not seen on axial images or T1-weighted images.
Motion artifact is a blurring of the image due to patient motion, respiration, or cerebral spinal fluid pulsation. Ependymoma and astrocytoma are seen on both the axial and the sagittal images.
QUESTION 20 OF 50
Androgens prevent bone resorption. Receptors for androgens are found on which of the following cells:
1
Osteoclasts
2
Osteoclast precursor cells
3
Osteoblasts
4
Osteocytes
5
Mast cells
Osteoblasts have receptors for androgens. Although androgens prevent bone resorption and may increase bone mass, the process is not understood at this time
QUESTION 21 OF 50
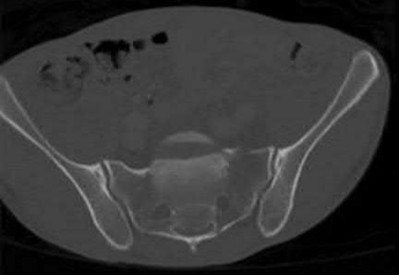
A 25-year-old female was involved in a high-speed motor vehicle accident and sustained the injuries shown in Figures A-C. Which of the following provides the most stable fixation construct?
1
Triangular osteosynthesis
2
Bilateral iliosacral screws
3
Anterior pelvic ring plating with bilateral iliosacral screw fixation
4
Transsacral bar fixation
5
Posterior tension band fixation
This patient has sustained a U-type sacral fracture. The most stable fixation is triangular osteosynthesis, also referred to as lumbopelvic fixation.
This patient has sustained a spinopelvic dissociation, which occurs when there are multiplanar fracture lines in both the horizontal and vertical planes. This creates an unstable situation with the upper part of the sacrum attached to the lumbar spine and the lower part of the sacrum remaining attached to the pelvis. There are many treatment options for this condition including open or percutaneous iliosacral screw osteosynthesis, tension band transiliac plate osteosynthesis, transiliac bars, and local plate osteosynthesis. If a neurologic defect is present, a sacral decompression with laminectomies is recommended.
Schildhauer et al. performed a retrospective study to report the results of sacral decompression and lumbopelvic fixation in neurologically impaired patients with highly displaced, comminuted sacral fracture-dislocations resulting in spinopelvic dissociation. They found 19 patients who were treated with open reduction, sacral decompression, and lumbopelvic fixation. They concluded that lumbopelvic fixation provided reliable fracture stability, and that
neurological outcomes were influenced by the completeness of the injury and the presence of sacral root disruption.
Schildhauer et al. performed a biomechanical comparison of triangular osteosynthesis and the standard iliosacral screw osteosynthesis for unstable transforaminal sacral fractures in both the immediate postoperative situation and in the early postoperative weight-bearing period. They concluded that triangular osteosynthesis for unstable sacral fractures provided significantly greater stability than iliosacral screw fixation under in vitro cyclic loading conditions.
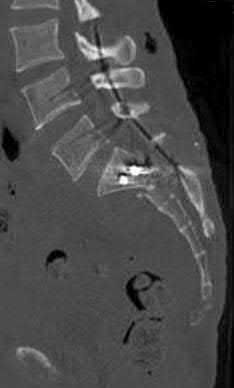
Figure A is an AP radiograph of the pelvis demonstrating a paradoxical inlet that occurs due to the kyphotic deformity of the sacrum. Figure B is an axial CT demonstrating a U-type sacral fracture. Figure C is a sagittal CT demonstrating the same U-type sacral fracture. The kyphotic deformity is well visualized on this image. Illustration A is an AP radiograph of the same patient after surgical treatment with triangular osteosynthesis. Illustrations B & C are coronal and sagittal CTs demonstrating the same. Illustration D is a volume-rendered 3D image of the same patient demonstrating a U-type sacral fracture. Illustration E demonstrates the various multiplanar sacral fractures: A: H-Type, B: Y-Type, C: T-Type, D: U-Type.
Incorrect Answers:
Answers 2, 3, 4, & 5: Though all of these may be treatment options for treating this injury, triangular osteosynthesis is the most stable fixation construct.
QUESTION 22 OF 50
Pediatric flexor tendon injuries of the upper extremity differ from adult flexor tendon injuries in which of the following ways?
1
Delayed presentation is not common.
2
A staged repair is never necessary.
* **##### **22 • American Academy of Orthopaedic Surgeons**
**
3
Six to eight weeks of postoperative immobilization is recommended.
4
Cooperation with occupational therapy can be difficult.
5
The use of Botulinum is contraindicated.
DISCUSSION: Pediatric flexor tendon injuries have several remarkable distinctions from those in adults. Delayed presentation is more common in children, at times requiring staged flexor tendon reconstruction. Three to four weeks of postoperative immobilization following acute repair is recommended in children as opposed to early motion protocols used in adults. Temporary paralytic agents (botulinum toxin type A) have also been shown to facilitate the rehabilitation phase of flexor tendon care in very young children.
REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2008, p 675.
QUESTION 23 OF 50
Slide 1 Slide 2 Slide 3
A 44-year-old obese man presents for treatment of acute ankle pain. He does not have a history of trauma or a systemic history of note. His opposite foot has had multiple episodes of acute pain in the past, lasting from 3 to 5 days. On examination, the
ankle is warm, swollen, and exquisitely tender to palpation and any range of motion (Slide1, Slide 2, and Slide 3). C oncerned about the source of pain, you aspirate the joint and send the sample for analysis. You expect to find:
1
Gram-positive cocci
2
Gram-negative rods
3
Normal joint fluid
4
Sodium monourate crystals
5
A high red cell count
This patient most likely has an acute attack of gout. The prior episodes of foot pain and the sudden onset lasting 5 days for each bout is characteristic. The ankle is not a common location for gout (the most frequent site is the hallux metatarsophalangeal joint). The treatment should consist of injection of a corticosteroid into the joint and administration of appropriate oral anti-inflammatory medication.
QUESTION 24 OF 50
Figures 43a and 43b are the MRI scans of a 54-year-old woman who reports a 2-year history of progressive shooting and burning-type pain in the posteromedial ankle. What is the most appropriate management?
1
Needle aspiration
2
Tarsal tunnel release
3
Incisional biopsy
4
Surgical excision
5
Referral to an orthopaedic surgeon specializing in oncology
The MRI scans show a bright, homogeneous mass (white arrow) on the T2-weighted images consistent with a ganglion cyst, which is likely emanating from the flexor digitorum longus tendon sheath. Because of the neuritic symptoms from the tibial nerve, the patient is best managed with surgical excision. Whereas needle aspiration can provide temporary relief by mass decompression, the location of the lesion in this instance, adjacent to the tibial nerve and posterior tibial artery, makes this option less optimal. Although the cyst is deep to the flexor retinaculum, which necessitates a tarsal tunnel release to access the lesion, release of the flexor retinaculum alone will not likely provide full resolution of symptoms. Incisional biopsy is indicated for potentially malignant lesions, which also makes referral to an orthopaedic surgeon specializing in oncology in this case unnecessary.
QUESTION 25 OF 50
of 100
A 4-year-old boy with recent onset of limping and right hip pain is diagnosed with Perthes disease. His radiographs reveal femoral head epiphysis fragmentation and partial collapse consistent with lateral pillar classification B and mild lateral extrusion. His prognosis strongly correlates with his
1
sex.
2
age at the onset of disease.
3
orthopaedic management.
4
ability to bear weight on the extremity.
■ Legg-Calve-Perthes disease (LCPD) is a childhood disorder of unknown etiology that can produce permanent deformity of the femoral head. Although LCPD can affect a wide range of children, it is most commonly seen in children aged 5 to 8 years. The male to female ratio is approximately 5:1, and bilateral disease occurs in 10% to 15% of patients. Treatment of patients with LCPD requires an understanding of the natural history of the disease, prognostic factors, and the effectiveness of various treatment methods.
Some of the prognostic indicators of outcome in patients with LCPD includes extent of the femoral head deformity and loss of hip joint congruity at maturity (Stulberg classification), age at onset, lateral pillar height at the fragmentation stage (lateral pillar classification), and premature physeal closure.
Existing studies show a difference in outcome depending on patient age at disease onset. Most patients in whom disease onset occurs younger than age 6 years achieve Stulberg I/II hips at maturity regardless of the type of treatment. These studies show no added benefits in outcome with surgical management in this age group. The treatment results for children aged 6 to 8 years are less clear, though treatment compared with no treatment (brace, range of motion, surgery) may yield better results. For children in whom disease onset occurs older than age 8 years, surgery compared with nonsurgical treatment could be beneficial for the lateral pillar B and B/C border groups but not for patients classified as group C.
QUESTION 26 OF 50
A 21-year-old female cross-country runner is brought to the medical tent after completing her run. The race took place during an unseasonably warm day in August. The patient is disoriented upon her arrival to the tent and cannot state the exact date. What is the next most appropriate course of action?
37
1
Administration of intravenous fluids
2
Immediate transport by ambulance to the closest hospital
3
Immersion in a cold-water ice bath
4
Temperature check with an oral thermometer
The patient is suffering from heat stroke due to the neurologic changes noted by confusion (can not state the date). This is a medical emergency and should be treated with immediate cold-water ice bath immersion and temperature monitoring with a rectal thermometer. Administration of IV fluids is controversial and is not first-line treatment for heat stroke. Transport to a hospital should be delayed until immediate cooling has been achieved and rectal temperature begins to decrease.
QUESTION 27 OF 50
Slide 1 Slide 2
The following image (Slide 1) depicts:
1
The removal of congenital pseudoarthrosis of the tibia
2
A vascularized iliaCautograft
3
A fibular autograft
4
The harvesting of the vascularized fibula from the contralateral leg
5
A fibular autograft for spinal fusion
The image depicts the harvesting of a vascularized fibula from the contralateral leg, which is then used to move a defect in congenital pseudoarthrosis of the tibia on the opposite side. The following image (Slide 2) shows clinical union 3.5 years later
QUESTION 28 OF 50
What are the potential benefits of performing a lesser tuberosity osteotomy:
1
Bone-to-bone healing
2
Improved glenoid exposure
3
Ability to detect on radiographs disruption of the anterior repair
4
All of the above
A lesser tuberosity osteotomy allows bone-to-bone healing as well as facilitates glenoid exposure. Moreover, disruption of the anterior repair is immediately evident on postoperative radiographs with the appearance of a displaced lesser tuberosity.
QUESTION 29 OF 50
of 100
Figures 57a and 57b are the close-up femur radiographs of a 73-year-old man with nonsmall-cell carcinoma of the lung with visceral metastases. He has localized thigh pain at rest and with any
range of motion of the ipsilateral hip or knee. A bone scan shows multiple areas of increased uptake. Other femur images in 2 views show no other lesions. The medical oncologist predicts a survival of 3 months. What is the best next step?
1
Needle biopsy of the femur to confirm the diagnosis
2
Cephalomedullary femur nailing
3
Palliative radiation only
4
Curettage and cementation with plate fixation of the involved femur
A needle biopsy is not needed to confirm a diagnosis of metastatic disease when other sites of disease are present. Cephalomedullary nailing offers a percutaneous option to prophylactically stabilize the impending fracture and to assist in nursing and palliative care. Palliative radiation can be added, but risk for fracture (even with complete bedrest) is nearly 100% according to Mirels’ criteria. An open procedure offers no benefit to intramedullary nail placement.
Recently, CT-based structural rigidity analysis has proven more accurate than Mirels’ scoring for metastatic femoral lesion fracture prediction, but this analysis is unnecessary when the likelihood of progression to fracture is so marked.
RECOMMENDED READINGS
10. [Damron TA, Nazarian A, Entezari V, Brown C, Grant W, Calderon N, Zurakowski D, Terek RM, Anderson ME, Cheng EY, Aboulafia AJ, Gebhardt MC, Snyder BD. CT-based Structural Rigidity Analysis Is More Accurate Than Mirels Scoring for Fracture Prediction in Metastatic Femoral Lesions. Clin Orthop Relat Res. 2016 Mar;474(3):643-51. doi: 10.1007/s11999-015-4453-0. PubMed PMID: 26169800. ](http://www.ncbi.nlm.nih.gov/pubmed/26169800)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26169800)
11. [Mirels H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop Relat Res. 1989 Dec;(249):256-64. PubMed PMID: 2684463. ](http://www.ncbi.nlm.nih.gov/pubmed/2684463)[View](http://www.ncbi.nlm.nih.gov/pubmed/2684463)[ ](http://www.ncbi.nlm.nih.gov/pubmed/2684463)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2684463)
12. [Ward WG, Holsenbeck S, Dorey FJ, Spang J, Howe D. Metastatic disease of the femur: surgical treatment. Clin Orthop Relat Res. 2003 Oct;(415 Suppl):S230-44. PubMed PMID: 14600615.](http://www.ncbi.nlm.nih.gov/pubmed/14600615)[View](http://www.ncbi.nlm.nih.gov/pubmed/14600615)[ ](http://www.ncbi.nlm.nih.gov/pubmed/14600615)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14600615)
QUESTION 30 OF 50
of 100
Figures 74a and 74b are the MR images of a 36-year-old man with a 3-month history of excruciating left leg pain. Which finding upon examination would be most consistent with the MR images?
1
Numbness and pain along the anterolateral thigh and weakness of hip adduction
2
Numbness and pain along the anterolateral calf and weakness of ankle dorsiflexion
3
Numbness and pain along the lateral and plantar aspect of the foot with weakness of ankle plantar flexion
4
Numbness and pain along the medial malleolus and weakness of knee extension
The MR images show a classic posterolateral disk herniation at L5-S1. This location affects the traversing nerve root (at L5-S1, the S1 nerve root). The S1 dermatome innervates the plantar aspect of the foot and primarily contributes to ankle plantar flexion and foot eversion. Hip adduction and quadriceps are controlled via the obturator nerve L2-4 innervation, and ankle dorsiflexion is controlled via L4 or L5 innervation. The L2 and L3 dermatomes provide sensation in the anteromedial thigh, L4 provides sensation along the anterolateral leg down to the medial malleolus, L5 provides sensation along the anterolateral leg to the dorsum of the foot, and S1 provides sensation along the posterior leg to the lateral foot.
RECOMMENDED READINGS
14. [Rhee JM, Schaufele M, Abdu WA. Radiculopathy and the herniated lumbar disk: controversies regarding pathophysiology and management. Instr Course Lect.2007;56:287-99. Review. PubMed PMID: 17472314. ](http://www.ncbi.nlm.nih.gov/pubmed/17472314)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17472314)
15. Mixter WJ, Barr JS. Rupture of the intervertebral disk with involvement of the spinal canal. N Engl J Med. 1934: 211: 210-5.
QUESTION 31 OF 50
The bone avulsion shown in Figure 32 has a high correlation with tearing of the
1
iliotibial band.
2
anterior cruciate ligament.
3
posterior cruciate ligament.
4
lateral collateral ligament.
5
biceps femoris tendon.
As described by Segond in 1987, an avulsion fracture of the lateral tibial plateau is commonly referred to as a Segond fracture. Subsequent to 1987, several authors have also found that the lateral capsular sign represents, but is not limited to, a disruption of the middle third of the lateral capsule and a tear of the anterior cruciate ligament.
REFERENCES: Bach BR, Warren RF: Radiographic indicators of anterior cruciate ligament injury, in Feagin JA (ed): The Crucial Ligaments. New York, NY, Churchill Livingston, 1988, pp 301-327.
Segond P: Recherches cliniques et experimentales sur les epanchements sanguins du genou par entorse. Prog Med (Paris) 1987;7:297.
Johnson LL: Lateral capsular ligament complex: Anatomical and surgical considerations. Am J Sports Med 1979;7:156-160.
QUESTION 32 OF 50
All of the following are true statements regarding elbow involvement in ulnar club hand except:
1
Fifty percent of patients have radial head dislocation.
2
Nearly 50% of aplasia patients have radiohumeral synostosis.
3
Elbow instability worsens with the severity on involvement.
4
The anlage causes radial head dislocation or subluxation.
5
The elbow is usually normal in all hypoplastic patients.
Elbow instability does not correspond with severity of involvement. Fifty percent of patients with total aplasia have radiohumeral synostosis, which provides adequate stability.
QUESTION 33 OF 50
The daily elemental calcium requirement for an elderly woman is:
1
500 mg to 700 mg
2
1,200 mg
3
1,500 mg
4
2,000 mg
5
2,500 mg
The guidelines for the daily elemental calcium requirement are as follows:
Children 500 mg to 700 mg
Growth spurt to young adult
(10 to 25 years of age)
1,300 mg
Adult male 750 mg
Adult female
Postmenopausal Elderly Pregnancy Lactation
  Â
1,500 mg
1,200 mg
1,500 mg
2,000 mg
Note: 1 daily equivalent = 250 mg elemental calcium (one glass of milk) Correct Answer: 1,200 mg
QUESTION 34 OF 50
of 100 A 67-year-old man with right shoulder osteoarthritis (OA) remains symptomatic despite a course of nonsurgical treatment. A CT scan of the shoulder shows eccentric posterior glenoid wear with 10° of retroversion. What is the appropriate management of this glenoid bone loss during surgery for an anatomic total shoulder arthroplasty?
1
In situ glenoid component implantation
2
Hemiarthroplasty
3
Eccentric reaming of glenoid
4
Posterior glenoid bone graft
DISCUSSION
Total shoulder arthroplasty (TSA) is superior to hemiarthroplasty for primary OA. The most common complication of TSA is glenoid loosening and malposition, which are common causes of glenoid failure. Glenoid malposition decreases the glenohumeral contact area and subsequently increases contact pressures. Altering the stem version to accommodate glenoid retroversion does not appropriately address soft-tissue balancing. A retroversion of <12° to 15° can be corrected with eccentric reaming without excessively compromising glenoid bone stock and risking glenoid vault penetration by the glenoid component. Posterior
glenoid bone grafting may be considered for glenoid retroversion >15°.
QUESTION 35 OF 50
Which of the following by itself is not an indication for surgery in a child with acute hematogenous osteomyelitis:
1
Fever higher than 38.5°
2
Subperiosteal abscess
3
Presence of a sequestrum
4
Intramedullary abscess
5
Adjacent septic arthritis
Surgery is indicated in situations in which antibiotics alone will not be curative, including subperiosteal abscess, sequestrum, intramedullary abscess, and adjacent septic arthritis. Fever alone is not an indication for surgery.
QUESTION 36 OF 50
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?
1
Continued observation
2
Open reduction and internal fixation of the fracture
3
Excision of the hook of the hamate
4
Carpal tunnel release
5
Guyon’s canal release
Excision of the fracture fragment typically leads to rapid return to function. Fixation techniques are difficult to perform because of the size of the bone; hardware prominence is common. Nerve deficits are not typically noted in this injury. The motor branch of the ulnar nerve in Guyon’s canal must be protected during the surgical approach.
REFERENCES: Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
QUESTION 37 OF 50
What is the function of the rotator cuff during throwing?
1
Limits humeral head translation in the transverse plane but not in the sagittal plane
2
Limits superior migration but not anterior and posterior translation
3
Limits superior migration and anterior and posterior translation
4
Provides little control of superior anterior and posterior translation
5
Creates inferior migration with maximal contraction during acceleration
The coupled action of the rotator cuff prevents superior migration and controls anterior and posterior translation by depressing the humeral head.
Scientific References
: Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
Abrams JS: Special shoulder problems in the throwing athlete: Pathology, diagnosis, and nonoperative management. Clin Sports Med 1991;10:839-861.
QUESTION 38 OF 50
A 35-year-old man sustained a traumatic low ulnar nerve palsy 18 months ago. The extent of the clawing and intrinsic atrophy as well as the active radial deviation are seen in Figures 1 through
1
No hyperextensibility of any of the proximal interphalangeal (PIP) joints is observed. Preoperatively, the patient is not able to fully extend the PIP joints with the wrist in neutral position and the examiner holding the metacarpophalangeal (MCP) joints flexed. Figure 4 shows the intraoperative photograph obtained during the intrinsic reconstruction procedure that is performed. The tendon grafts were inserted distally into the


















2
proximal phalanx.
3
radial lateral bands.
4
first annular pulley.
5
second annular pulley.
Originally, Burkhalter and Strait recommended bony insertion into the proximal phalanx through a drill hole. This procedure does require more surgical dissection and flexes only the MCP joints; thus it cannot extend the PIP joints directly. It does improve clawing in the fingers if the PIPs can extend with preoperative MCP flexion. The ability to extend the PIP joints is evaluated preoperatively using the Bouvier test. With the wrist in neutral position, the examiner holds the MCPs flexed and looks for the ability in that position to actively extend the PIPs. If the patient is able to do so, then the test is considered positive, and this describes "simple" clawing. In such cases, procedures that flex only the MCPs are appropriate. The insertion sites for these procedures include the proximal phalanx, the first annular pulley, and the second annular pulley. If the Bouvier test is negative, then it is best to insert the tendon grafts distally into the lateral bands. This technique has a low chance of leading to hyperextension of the PIP joints, particularly when performed with a wrist extensor motor (which leaves the flexor digitorum superficialis undisturbed) and with no preoperative hyperextensibility of the PIPs.
QUESTION 39 OF 50
Which of the angles depicted in Figure 60 has been found to most closely correlate with a patient’s lumbar lordosis, thoracic kyphosis, and overall sagittal alignment?
1
A
2
B
3
C
4
D
5
A and D
Angle A represents pelvic incidence (PI), a constant anatomic relationship between the pelvis and sacrum. Angle B represents pelvic tilt, and angle C represents sacral slope. Pelvic tilt and sacral slope can change depending on the rotation of the pelvis. Pelvic incidence has been found directly correlate with the magnitude of lumbar lordosis and thoracic kyphosis because it determines the angle at the base
of the spine (the lumbosacral junction). To obtain sagittal balance, the remainder of the spine compensates, resulting in the degree of lumbar lordosis and thoracic kyphosis to maintain an upright posture. Thus, PI must be considered in the evaluation of sagittal balance and potential reconstructive procedures. Angle D represents the T1 angle.
QUESTION 40 OF 50
A 72-year-old woman underwent a primary total hip arthroplasty 14 months ago. She states that the hip has now dislocated four times when rising from a low chair, requiring closed reduction. A radiograph is shown in Figure 3a and a CT scan of her pelvis is shown in Figure 3b. What is the most reliable method for rectifying her instability?
1
Use of an abduction orthosis for 6 weeks
2
Modular exchange of the femoral head to a 36-mm head and a longer neck
3
Modular exchange of the polyethylene liner to a constrained acetabular insert
4
Revision and repositioning of the acetabular component and use of a 36-mm femoral head
5
A physical therapy program stressing abductor strengthening
DISCUSSION: The radiograph shows well-fixed components without evidence of loosening. The CT scan shows severe retroversion of the acetabular component. Revision of the component into the correct amount of anteversion
will most reliably rectify the instability in the face of severe component malposition.
REFERENCES: Parvizi J, Picinic E, Sharkey PF: Revision total hip arthroplasty for instability: Surgical techniques and principles. J Bone Joint Surg Am 2008;90:1134-1142.
DeWal H, Su E, DiCesare PE: Instability following total hip arthroplasty. Am J Orthop 2003;32:377-382. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
QUESTION 41 OF 50
Which of the following choices is the best for sedating an otherwise healthy child for a fracture reduction:
1
Morphine, diazepam
2
Meperidine, midazolam
3
Fentanyl, diazepam
4
Demerol, phenergan, and thorazine
5
Fentanyl, midazolam
The combination of fentanyl and midazolam is the closest we have to an ideal drug combination for conscious sedation. Both drugs have commercially available antagonists. Fentanyl and midazolam are both quick-onset and short-duration drugs. When using these two drugs together, there is a significant risk of respiratory depression. It is important to monitor patients closely.
QUESTION 42 OF 50
The primary function of structure “A” in Figure 29 is to limit
1
posterior tibial displacement at 90 degrees of flexion.
2
varus knee laxity at 30 degrees of flexion.
3
varus knee laxity at 0 degrees of flexion.
4
anterolateral rotation of the tibia on the femur.
5
posterolateral rotation of the tibia on the femur.
The primary function of the popliteofibular ligament is to resist posterolateral rotation of the tibia on the femur, although it also secondarily resists varus angulation and posterior displacement of the tibia on the femur. The posterior cruciate ligament resists posterior tibial displacement, especially at 90 degrees of flexion. The lateral collateral ligament primarily resists varus displacement at 30 degrees of flexion but also resists posterolateral rotatory displacement with flexion that is less than approximately 50 degrees. The anterior and posterior cruciate ligaments resist varus displacement (along with the lateral collateral ligament) at 0 degrees of flexion. The anterior cruciate ligament primarily resists anterolateral displacement of the tibia on the femur.
REFERENCES: Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
Veltri DM, Deng XH, Torzilla PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
QUESTION 43 OF 50
The thickness of a flexible intramedullary nail used in pediatric femur fractures should be which of the following percentages of the diameter of the femoral isthmus:
1
10%
2
25%
3
40%
4
50%
5
75%
It is recommended that the intramedullary nail be 40% of the diameter of the femoral isthmus.
QUESTION 44 OF 50
Which of the following statements is true concerning atlanto-occipital dislocations in children:
1
The dens-basion distance is greater than 10 mm.
2
The power ratio is greater than 1.0.
3
The injury is not survivable.
4
Spinal cord injury always accompanies this dislocation.
5
No single plain radiographic finding is always diagnostic.
Pediatric atlanto-occipital dislocation is increasing in frequency due to improved emergency care. Although the injuries are sometimes fatal and are often accompanied by severe spinal cord injury, this is not always the case. Although the dens-basion distance should be less than 10 mm and the power ratio should be less than 1 in normals, these are not always abnormal in children with such injuries. C linical and radiographic correlation, with computer tomography or magnetic resonance imaging if needed, are called for to maximize diagnosis.
QUESTION 45 OF 50
A 51-year-old female sustained a comminuted radial head fracture with 4 fragments and an associated elbow dislocation. She was initially closed reduced and splinted with the elbow joint in a reduced position and presents to the orthopedists office 10 days later. In response to the patient's question of what treatment offers the best chance for a good outcome, the surgeon should recommend?
1
Excision of the radial head
2
ORIF of the radial head
3
Continued splinting, no surgery
4
Radial head arthroplasty
5
Hinged external fixation
In the context of elbow instability, optimal treatment of a comminuted radial head fracture with greater than three fragments is with a radial head replacement.
Radial head fractures are often seen in conjunction with injuries such as elbow dislocations and DRUJ instability. Although minimally displaced injuries can be treated non-operatively, an ORIF can be utilized when there is limited comminution of the radial head. Improved outcomes are demonstrated when radial head arthroplasty is used in the setting of greater than 3 fracture fragments.
Ring et al. reviewed 56 patients who had been treated with an ORIF of the
radial head at 48 months after injury. They found that patients had unsatisfactory outcomes for patients who had an ORIF of radial fractures with greater than 3 articular fragments. They recommend ORIF of radial head fractures with 3 or few fragments.
Moro et al. reviewed functional outcomes of patients treated with radial head arthroplasty for un-reconstructible fractures. They found that patients treated with metal radial head implants had mild physical impairment. Short term follow-up indicates that radial head arthroplasty is a reasonable option for severely comminuted radial head fractures.
Illustration A shows a 3D reconstruction of a radial head fracture with a coronal and sagittal split. The presence of 3 fragments portends good outcomes with an ORIF procedure.
Incorrect Answers
Answer 1: Resection is not indicated in this patient to improve her function and optimize outcome
Answer 2: With greater than 3 fragments, better outcomes have been reported with radial head replacement.
Answer 3: Non operative management will likely lead to loss of motion and radiocapitellar arthritis
Answer 5: Hinged external fixation is not indicated in this patient
QUESTION 46 OF 50
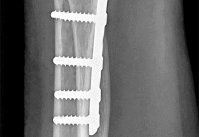
Figures 1 through 3 are the radiographs of a 55-year-old woman who underwent a volar plating of an extra-articular distal radius fracture 2 weeks ago. She is experiencing weakness with flexion of the interphalangeal (IP) thumb joint. IP joint flexion was normal before surgery. What is the best next step? --- --- ---
1
Observation
2
Electromyogram/nerve conduction study (EMG/NCS)
3
CT scan
4
Immediate exploration
Prevalence of flexor tendon rupture after distal radius fracture is between 2% and 12%. The FPL tendon is the most common flexor tendon rupture associated with volar plating. It is usually seen with plates that are distal to the watershed line (W) and with plates extending volar to the critical line (C) (Figure below). The watershed line (W) is the location of the origin of the volar carpal ligaments and the bone prominence
---
at which flexor tendons are most closely opposed to the distal radius (Figure 4). In this scenario, the lateral radiograph shows that the plate is not distal to the watershed line (W) and is between the critical line (C) and the line parallel to the volar cortex of the radius (R). This is the optimal position for the plate. Placement of a volar locking plate distal to the watershed line of the distal radius and excessive plate prominence has been associated with FPL tendon rupture. This patient is only 2 weeks past surgery and there is some FPL function. FPL weakness after volar distal radius plating is common and has been seen in as many as 50% of patients. This usually recovers spontaneously by 2 months, and no treatment is needed. A nerve conduction study would be indicated if an anterior interosseous nerve compression were considered, but it is too early for this test. A CT scan could be obtained to judge the alignment of the fracture fragment and position of the screws, but it is not indicated in this case. Exploration could be performed if an FPL rupture were considered, but, because it is only 2 weeks after surgery, there is some FPL function, the plate is proximal to the watershed line, and immediate exploration is not indicated. If this does not improve after 2 to 3 months, further investigation with ultrasound or MRI would be indicated.
QUESTION 47 OF 50
of 100
Which nerve is not included in a standard popliteal nerve block?
1
Sural nerve
2
Saphenous nerve
3
Superficial peroneal nerve
4
Deep peroneal nerve
A standard popliteal nerve block is performed with the patient prone. The injection aims for the area at, or close to, the peroneal and tibial nerves. The sural nerve branches distal to the injection site, so this nerve and the superficial peroneal, deep peroneal, and tibial nerves are covered with the injection. The saphenous nerve is in an anteromedial location at knee level and is not close enough to the area covered by the posterior injection to be included in the analgesic effect.
RECOMMENDED READINGS
[Varitimidis SE, Venouziou AI, Dailiana ZH, Christou D, Dimitroulias A, Malizos KN. Triple nerve block at the knee for foot and ankle surgery performed by the surgeon: difficulties and efficiency. Foot Ankle Int. 2009 Sep;30(9):854-9. PubMed PMID: 19755069. ](http://www.ncbi.nlm.nih.gov/pubmed/19755069)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/19755069)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19755069)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19755069)
[Hromádka R, Barták V, Popelka S, Jahoda D, Pokorný D, Sosna A. [Regional anaesthesia of the foot achieved from two cutaneous points of injection: an anatomical study]. Acta Chir Orthop Traumatol Cech. 2009 Apr;76(2):104-9. Czech. PubMed PMID: 19439129. ](http://www.ncbi.nlm.nih.gov/pubmed/19439129)[View](http://www.ncbi.nlm.nih.gov/pubmed/19439129)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19439129)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19439129)
[Tran D, Clemente A, Finlayson RJ. A review of approaches and techniques for lower extremity nerve blocks. Can J Anaesth. 2007 Nov;54(11):922-34. Review. PubMed PMID: 17975239. ](http://www.ncbi.nlm.nih.gov/pubmed/17975239)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17975239)
CLINICAL SITUATION FOR QUESTIONS 42 THROUGH 44
42A
B
Figures 42a and 42b are the radiographs of a 32-year-old man with an accessory navicular, pes planovalgus deformity, and an associated gastrocnemius contracture. He has been treated with custom orthotics and a physical therapy program for several years and has progressed to stage II posterior tibial tendon dysfunction (PTTD). This patient is now interested in surgery. Tendon reconstruction with bony procedure to correct alignment, medializing calcaneal osteotomy with lateral column lengthening, and a subtalar arthroereisis implant are discussed with the patient.
QUESTION 48 OF 50
Which muscles cause the fracture displacement of the proximal fragment shown in figure A?
1
gluteus maximus and adductors
2
gluteus maximus and rectus femoris
3
gluteus medius and hamstrings
4
gluteus medius and iliopsoas
5
rectus femoris and hamstrings
The gluteus medius attaches to the greater trochanter, leading to abduction, while the iliopsoas attaches to the lesser trochanter, leading to flexion. French et al evaluated forty-five Russell-Taylor Type 1B subtrochanteric femoral fractures which were stabilized using an interlocked cephalomedullary nail. The intraoperative complication rate was 13.5%; and the most frequent complication was a varus malreduction. The primary reason for this was failure to counteract the muscle forces acting on the proximal fragment combined with the adducted position of the distal femur during portal creation. This problem can be avoided if the position of the proximal fragment is evaluated carefully and reduced before guidewire insertion.
QUESTION 49 OF 50
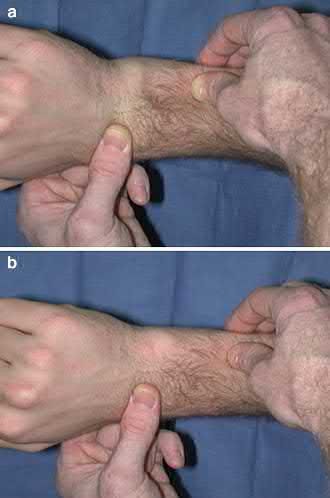
A 45-year-old construction worker sustains a fall and presents with an isolated injury to his upper extremity. Radiographs of the affected wrist are shown in Figure A. After soft tissue swelling subsides, open reduction and internal fixation of the distal radius is performed. Following fixation, a "shuck" test is performed and shows persistent instability of the distal radioulnar joint. Incompetence of which of the following anatomic structures is the most likely etiology of this finding?
1
Radioulnar ligaments of the TFCC
2
Ulnar collateral ligament
3
Fracture fixation
4
Ulnolunate ligament of the TFCC
5
Ulnotriquetral ligament of the TFCC
The patient has sustained a distal radius fracture and concomitant ulnar styloid fracture. The shuck test is performed after fixation of the distal radius to assess the status of the DRUJ, namely the radioulnar ligaments.
Injuries to the DRUJ often occur with distal radius fractures. The presence of an ulnar styloid fracture may signify injury to the DRUJ. After the distal radius has been fixed, the shuck test is performed. This test is completed with the elbow at 90 degrees of flexion, the forearm in neutral rotation, followed by pronation and supination. The examiner attempts to translate the ulnar in the sagittal plane. Excessive sagittal plane ulnar translation signifies DRUJ injury.
Kim et al. review the effect of ulnar styloid nonunion on functional outcome after distal radius ORIF. Of the 91 patients treated with distal radius ORIF, 22% were found to have a nonunion of the ulnar styloid. There was no
difference in wrist functional outcomes, ulnar sided wrist pain, or DRUJ stability.
Sammer et al. reviewed 144 patients undergoing ORIF of the distal radius. The DRUJ was stable in all patients after internal fixation. An ulnar styloid fracture was found in 88 patients. Functional outcome scores were not affected by the presence of an ulnar styloid fracture. Additionally, the size of the fracture, extent of displacement, or healing status did not affect the outcome.
Figure A shows a PA radiograph of the wrist demonstrating a comminuted distal radius fracture with a concomitant ulnar styloid fracture. Illustration A shows an example of the shuck test used to test the DRUJ.
Incorrect Answers:
Answer 2: The ulnar collateral ligament is involved with injuries to the thumb. Answer 3: The shuck maneuver is not utilized to assess stability of the fracture.
Answers 4, 5: The ulnolunate and ulnotriquetral ligament origins are part of the TFCC, but are not the key stabilizers of the DRUJ.
QUESTION 50 OF 50
of 100
This injury is best treated with
1
closed reduction and percutaneous pinning.
2
a short-leg cast with closed reduction.
3
open reduction and internal fixation (ORIF) with Kirschner wires.