This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set EA6994)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
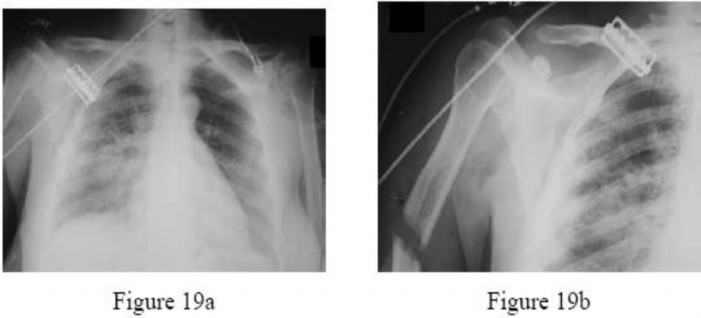
Figure 19bFigures 19a and 19b are the radiographs of a 32-year-old woman who has sustained multiple injuries after being struck by a motor vehicle while riding a bicycle. She is intubated on arrival and remains tachycardic and hypotensive. Pulses are hard to palpate but the right hand is somewhat cooler to touch than the left hand. She has a large open wound over the upper arm. What is the most important predictor of outcome with these injuries?
1
Open wound size
2
Open wound contamination
3
Time to débridement
4
Adequacy of débridement
5
Neurovascular status
No detailed explanation provided for this question.
QUESTION 2 OF 50
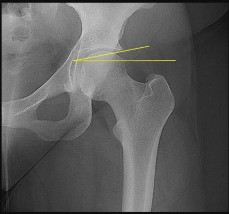
A 21-year-old collegiate female cross-country athlete reports right hip pain that begins about 12 miles into a run, followed by pain resolution when she discontinues running. However, each time she tries to resume a running program, she experiences recurrence of pain deep in the anterior groin. A plain radiograph and MRI scan are shown in Figures 8a and 8b. Management should consist of
1
cessation of running and implementation of cross training until healing is complete.
2
a bone scan, skeletal survey, and chest radiographs to assess for other sites of involvement.
3
a radioisotope injection and scintinigraphic-guided percutaneous biopsy.
4
percutaneous fixation with multiple cannulated screws.
5
excision, bone grafting, and internal fixation.
The history is consistent with a stress fracture. Findings on the plain radiograph are marginal, but the MRI scan shows evidence of stress reaction in the medial neck of the femur (compression side). A lesion on the compression side is not normally at risk for displacement and usually can be managed nonsurgically. A bone scan would further identify the lesion but is not necessary. A skeletal survey and chest radiograph are used in staging a tumor. Radioisotope injection and guided biopsy are sometimes used for osteoid osteomas.
REFERENCES: Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Lynch SA, Renstrom PA: Groin injuries in sport: Treatment strategies. Sports Med 1999;28:137-144.
QUESTION 3 OF 50
-Bacterial resistance to antibiotics in biofilm is an example of
1
avoidance.
2
decreased susceptibility.
3
inactivation.
4
mutation.
No detailed explanation provided for this question.
QUESTION 4 OF 50
of 100
Figures 1 and 2 are the clinical photograph and radiograph of a newborn who is seen for evaluation of his feet. A rigid rocker bottom foot is present with dorsal foot crease. The most appropriate next step in management is
1
serial casting with talonavicular reduction and fixation and Achilles tenotomy.
2
operative release at age 18 months.
3
tendon transfer after age 18 months.
4
observation, physical therapy, and transition into an ankle foot orthosis.
■ Congenital vertical talus is a rare condition in which the navicular is dorsally dislocated on the talus. There is also hindfoot equinus and valgus, resulting in the rocker bottom appearance. Fifty percent of cases are associated with other conditions (arthrogryposis, chromosomal abnormalities, skeletal dysplasia, myelomeningocele). Once the diagnosis is confirmed, usually on a plantar flexion lateral radiograph (the first MT does not align with the first metatarsal), treatment with serial casting described by Dobbs and associates is instituted. Once the talus lines up with the first metatarsal, surgical reduction of the talonavicular joint with pinning and Achilles tenotomy are done to correct the deformity.
QUESTION 5 OF 50
Pseudoaneurysms differ from true aneurysms in that:
1
Pseudoaneurysms are expansile.
2
Pseudoaneurysms occur secondary to trauma.
3
Pseudoaneurysms have a fibrous wall.
4
Pseudoaneurysms frequently occur in the ulnar artery.
Pseudoaneurysms occur secondary to penetrating trauma and have a fibrous wall, compared to true aneurysms that have all the elements of an arterial wall.
QUESTION 6 OF 50
Slide 1 Slide 2 Slide 3
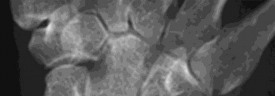
A 55-year-old man has severe wrist pain with erythema and soft tissue swelling. The plain radiograph is shown in Slide 1 and a biopsy specimen is shown in Slide 2 and Slide 3. Which of the following would be the best treatment:
1
Debridement and antibiotics
2
Nonsteroidal anti-inflammatory medications
3
External beam irradiation
4
Wide resection and wrist fusion
5
Thumb basal joint arthroplasty
The plain radiographs show a destructive lesion in the wrist in the distal radius and at the scaphotrapezial joint. The joint spaces are preserved. The histology shows the features of gout: acellular amorphous tissue, macrophages, and giant cells.
Gout is caused by the deposition of monosodium urate crystals in tissues typically around joints. Common locations include the great toe, heel, ankle, and knee. In approximately 50% of patients, the first attack is in the great toe. Gout commonly occurs inside a joint for two reasons:
The synovial fluid is a poorer solvent than plasma
Lower temperatures (as in peripheral joints) favor crystallization
Neutrophils ingest the crystals and then release potent lysosomal enzymes. Histologically, the tophi have several features: Acellular amorphous material
Macrophages
Foreign body giant cells
The first line of treatment is nonsteroidal anti-inflammatory medications. Correct Answer: Nonsteroidal anti-inflammatory medications
QUESTION 7 OF 50
of 100
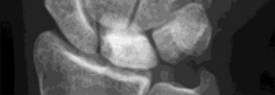
Figures 37a through 37c are the radiographs of a 45-year-old construction worker who has severe wrist pain. He has failed nonsurgical measures and requests surgery. The most appropriate surgical option is
1
bone graft with fixation of the scaphoid.
2
proximal row carpectomy.
3
scaphoid excision with 4-corner fusion.
4
total wrist joint replacement.
The radiographs show a long-standing scaphoid nonunion with avascular necrosis and collapse of the proximal pole. This is referred to as a scaphoid nonunion advanced collapse wrist. He also has advanced arthritis of the capitolunate joint. This patient has a physically demanding occupation, so the best option for him is scaphoid excision with 4-corner fusion. Proximal row carpectomy would be inappropriate because of the advanced arthritis of the capitolunate joint. This procedure’s success is reliant upon normal cartilage/joint articulation of the capitate and lunate fossa of the distal radius. A total wrist replacement is not appropriate for a man with a physically demanding job. Finally, the patient has a long-standing scaphoid nonunion with advanced proximal pole collapse. Therefore, bone grafting with fixation is not an option at this point.
RECOMMENDED READINGS
23. [Weiss KE, Rodner CM. Osteoarthritis of the wrist. J Hand Surg Am. 2007 May-Jun;32(5):725-46. Review. PubMed PMID: 17482013.](http://www.ncbi.nlm.nih.gov/pubmed/17482013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17482013)
24. [Shah CM, Stern PJ. Scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC) wrist arthritis. Curr Rev Musculoskelet Med. 2013 Mar;6(1):9-17. doi: 10.1007/s12178-012-9149-4. PubMed PMID: 23325545. ](http://www.ncbi.nlm.nih.gov/pubmed/23325545)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23325545)
QUESTION 8 OF 50
of 100
Figure 50 is the radiograph of a 19-year-old woman who injured her left knee while playing soccer 4 days ago. She was cutting to her right, was tackled on the inside of her left knee, and felt a pop. She has no history of prior injury to her knee. Which structure attaches at the site of the avulsion fracture?
The knee ALL is a fibrous band at the anterolateral aspect of the knee. It first was reported by Segond and also is known as the lateral capsular ligament, mid-third lateral capsular ligament, and anterior band of the lateral collateral ligament. It is thought to be injured with varus and internal rotation. It is associated with a torn anterior cruciate ligament 75% of the time and it is located in the third layer on the anterolateral side of the knee. It is 90% collagen I, with some collagen III and VI. The ALL originates at the lateral epicondyle between the lateral collateral ligament and popliteal tendon. It runs obliquely down and forward, inserting in the lateral meniscus and lateral aspect of the proximal tibia. Its role in rotational stability is debated but certainly worthy of consideration, especially in revision knee surgery.
The iliotibial band inserts on Gerdy’s tubercle. A portion of the ALL may insert on the lateral meniscus; however, a lateral meniscus tear is not directly associated with avulsion fractures. The fibular collateral ligament inserts on the fibular head.
RECOMMENDED READINGS
14. Macchi V, Porzionato A, Morra A, Stecco C, Tortorella C, Menegolo M, Grignon B, De Caro R. The anterolateral ligament of the knee: a radiologic and histotopographic study. Surg Radiol Anat. 2015 Oct
[17/. [Epub ahead of print] PubMed PMID: 26476833.](http://www.ncbi.nlm.nih.gov/pubmed/26476833)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26476833)
15. Kennedy MI, Claes S, Fuso FA, Williams BT, Goldsmith MT, Turnbull TL, Wijdicks CA, LaPrade RF. The Anterolateral Ligament: An Anatomic, Radiographic, and Biomechanical Analysis. Am J Sports Med. 2015 Jul;43(7):1606-15. doi: 10.1177/0363546515578253. Epub 2015 Apr 17. PubMed
[PMID: 25888590. ](http://www.ncbi.nlm.nih.gov/pubmed/25888590)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25888590)
RESPONSES FOR QUESTIONS 51 THROUGH 57
Figure 51 a- h
a b c
h
d
e
f
g
QUESTION 9 OF 50
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
What represents the best indication for surgical management of the humeral shaft fracture in this patient? ---
---
1
Radial nerve palsy
2
Extensive fracture comminution
3
Polytraumatized patient
4
Distal third diaphyseal fracture
The patient sustained a comminuted extra-articular distal humeral diaphyseal fracture. In isolation, this fracture would still be amenable to an attempt at closed treatment. His radial nerve palsy alone does not warrant open management, as early exploration has not shown a significant benefit in a closed fracture. In addition, despite the comminution and distal extent of the fracture, it is still amenable to closed treatment, though it may be at higher risk for malunion. However, in this patient with multiple lower extremity injuries, fixation of the humerus can facilitate early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
QUESTION 10 OF 50
What factor highly correlates with poor outcomes after surgery for femoroacetabular impingement?
1
Age <20
2
Tonnis grade 2
3
Prominence of the femoral head in cam impingement
4
The patient is a professional athlete
A systematic review of case studies looking at the results of surgical treatment for femoroacetabular impingement shows good results for most patients, with the exception of those with preoperative radiographs showing osteoarthritis or Outerbridge grade III or grade IV cartilage damage noted intraoperatively. Both Byrd and Jones and Philippon and associates have shown good surgical results for this condition among professional athletes. Likewise, Fabricant and associates demonstrated good surgical results among adolescent patients with an average age of 17.6 years.
QUESTION 11 OF 50
of 100
If aspiration findings are negative or equivocal, the diagnosis can be established with
1
arthroscopy.
2
a bone scan.
3
a serum white blood cell level.
4
a C-reactive protein level.
- arthroscopy._
QUESTION 12 OF 50
Figure 1 is the radiograph of a 22-year-old man who underwent an open reduction and pinning of a perilunate dislocation 10 weeks ago. The hardware has been removed. What is the best next step?
1
Observation
2
Vascularized bone grafting to the lunate
3
Core decompression of the radius and ulna
4
Immobilization
Lunate or perilunate dislocations are usually treated with open reduction and internal fixation through a dorsal or combined dorsal and volar approach. A high index of suspicion is necessary when treating patients who sustain multiple trauma because as many as 25% of lunate or perilunate dislocations are missed initially. The radio dense appearance of the lunate seen in Figure 1 is an example of transient ischemia of the lunate that can occur following treatment of lunate and perilunate dislocations. It has been reported in up to 12.5% of cases. This usually is seen between 1 and 4 months post injury with a relative radio density of the lunate. This appearance of the lunate should not be over treated and usually is a benign self-limiting event. Surgery is not indicated at this time; the incorrect responses are treatment options for Kienbock disease. Treatment of the lunate or perilunate dislocation involves initial gentle closed reduction followed by open reduction, ligamentous and bone repair, and internal fixation. Median nerve dysfunction is common, and a simultaneous carpal tunnel release is often performed. Early treatment seems to produce better results, but good results have been reported when treatment is delayed for up to 6 months. The many questions regarding treatment of this problem involve the use of capsulodesis to supplement intercarpal ligament repair, repair/stabilization of the lunotriquetral interval vs no treatment of that articulation, and intercarpal fixation techniques. In delayed cases, proximal row carpectomy when the head of the capitate is intact and total wrist fusion if there are degenerative changes have been used. Chondral injuries are common, may not be recognized on radiographs, and may negatively affect longterm outcomes. Even when treatment is optimal, this injury is associated with a guarded prognosis and possible permanent partial loss of wrist motion and grip strength. At 10-year follow-up, radiographs will often demonstrate degenerative changes, but these changes do not always substantially negatively affect _hand function._
QUESTION 13 OF 50
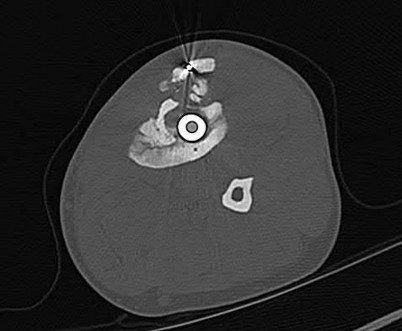
Figures A-D are the radiographs and CT images from a 32-year-old diabetic man who was treated with an intramedullary nail following an open tibial shaft fracture 13-months ago. He continues to have pain in the leg. Despite a course of IV antibiotics, his laboratory markers remain elevated. What is depicted by the arrow in figure D?
1
Involucrum
2
Sequestrum
3
Callus
4
Avascular necrosis
5
Malignant bone tumor
The arrow is indicating a sequestrum, or area of devitalized bone that serves as a nidus for chronic infection.
Osteomyelitis is an infection of bone characterized by progressive inflammatory destruction and the apposition of new bone. Despite surgical debridement and long-term antibiotics, the recurrence rate of chronic osteomyelitis in adults is 30%, with S. aureus being the most common organism. A sequestrum is devitalized bone that serves as a nidus for infection, while an involucrum is newly formed bone around this area of bony necrosis. In cases of chronic osteomyelitis, irrigation and debridement with the elimination of the sequestrum, followed by organism-specific antibiotics are indicated. Any non-essential hardware should be removed; however, bony stability is required for the successful eradication of infection.
Jaeblon et al. review the use of polymethylmethacrylate as a delivery vehicle for antibiotics while simultaneosuly eliminating dead space. The authors discuss elution from both the surface and the pores of the cement as well as the microcracks within it. They conclude that tobramycin is favored due to its
broad and antipseudomonal coverage, as well as the fact that it potentiates the elution of other antibiotics within the cement such as vancomycin.
Masri et al. prospectively reviewed the surgical outcomes of 49 patients undergoing a modified 2-stage exchange arthroplasty for infected total hip and knee arthroplasties using an antibiotic-loaded acrylic cement prosthesis. They reported on the intra-articular concentrations of tobramycin and vancomycin at the time of removal. The authors concluded that the dose of vancomycin in the cement did not influence the elution of either tobramycin or vancomycin and recommend the use of at least 3.6 g of tobramycin and 1 g of vancomycin per package of bone-cement.
McNamara et al. review the utility of vancomycin. The authors report on its increased use due to the growing resistance of many gram-positive bacteria to β-lactam antibiotics. They conclude that unlike penicillins and cephalosporins, cross-resistance with vancomycin does not develop, and that while it possesses activity against nearly all gram-positive bacteria, it is not useful against gram-negative bacilli.
Nana et al. review the high affinity of microorganisms to adhere to foreign materials commonly used in orthopedics, including cobalt-chromium, titanium, polyethylene, and polymethylmethacrylate (PMMA) cement by forming biofilms. They discuss that S. aureus and S. epidermidis are the most common biofilm-forming bacteria found in orthopedics and, when combined with P. aeruginosa, represent nearly 75% of biofilm infections. The authors conclude that while no current guidelines exist for treating these infections, recent studies have shown that biofilm growth can be fully inhibited when PMMA is mixed with both daptomycin and gentamicin.
Figures A and B are the AP and lateral radiographs of a tibial shaft infected nonunion treated initially with an intramedullary nail.
Figure C is the axial CT scan demonstrating an infected nonunion of previous tibial shaft fracture.
Figure D demonstrates a sequestrum, or infected dead bone, as indicated by the black arrow. The surrounding new reactive bone, or involucrum, is seen superficial to the sequestrum.
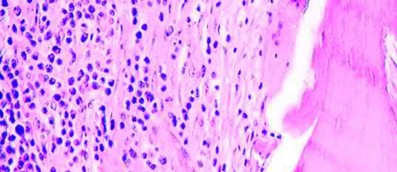
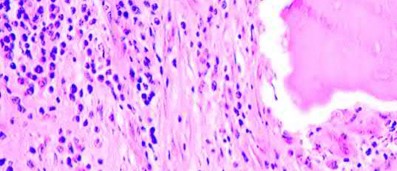
Illustration A is a histologic image of chronic osteomyelitis, anucelar osteocytes with fibrosis of marrow and chronic inflammatory cells (lymphocytes).
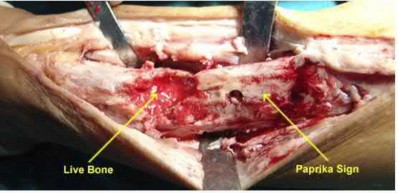
Illustration B demonstrates the "paprika sign," or punctate bleeding seen with viable bone, suggesting adequate bone debridement.
Incorrect Answers:
Answer 1: Involucrum is the newly formed bone around an area of bony necrosis.
Answer 3: There is little callus on the axial CT scan, which is atypical for a tibial shaft fracture treated with IMN fixation.
Answer 4: Avascular necrosis would be atypical following intramedullary nail fixation of tibial shaft fracture.
Answer 5: Malignancy should always be on the differential with infection, and a biopsy should be obtained. However, given the history and clinical presentation infection is more likely.
QUESTION 14 OF 50
Which of the following problems is most common in achondroplasia:
1
Atlantoaxial instability
2
Basilar invagination
3
Symptomatic kyphosis
4
Thoracolumbar stenosis
5
Spondylolisthesis
Symptomatic stenosis of the thoracic and lumbar spine is seen in almost half of all achondroplastic patients, although not all patients require surgery.
Atlantoaxial instability is rare in achondroplasia, although it is not uncommon in other dysplasias. Basilar invagination is not present in achondroplasia.
Kyphosis is often transient in achondroplasia and rarely persists beyond the second year. Kyphosis is rarely symptomatic. Spondylolisthesis is rare in achondroplasia.
QUESTION 15 OF 50
of 100
If this lesion occurred in the spine, which features would most likely be present?
1
Syrinx and paralysis
2
Spondylolisthesis and radiculopathy
3
Epidural abscess and fever
4
Scoliosis and paraspinal pain
The images and clinical history support a diagnosis of osteoid osteoma, which most commonly occurs in adolescence. Although these lesions can be seen in any bone, they are usually located in the femur and tibia. The significant inflammatory response to this tumor is secondary to high levels of prostaglandin production. Characteristic night pain is relieved with nonsteroidal anti-inflammatory drugs (NSAIDs) or by aspirin.
Radiographic images show thickened bone and a small central nidus. Thin-cut CT scan is the imaging of choice to visualize the nidus. A bone scan is associated with uptake but is not specific. Treatment options include expectant management with NSAIDs and observation under the premise that these lesions eventually burn out. Contemporary treatment involves RFA. Historically, these lesions were treated with en bloc resection; however, this technique has largely fallen out of favor because of the high efficacy and comparative low morbidity associated with RFA.
When an osteoid osteoma occurs in the spine, it is located in the posterior elements, and paraspinal pain and scoliosis often are present.
RECOMMENDED READINGS
14. [Volkmer D, Sichlau M, Rapp TB. The use of radiofrequency ablation in the treatment of musculoskeletal tumors. J Am Acad Orthop Surg. 2009 Dec;17(12):737-43. Review. PubMed PMID: 19948698. ](http://www.ncbi.nlm.nih.gov/pubmed/19948698)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19948698)
15. [Donahue F, Ahmad A, Mnaymneh W, Pevsner NH. Osteoid osteoma. Computed tomography guided percutaneous excision. Clin Orthop Relat Res. 1999 Sep;(366):191-6. PubMed PMID: 10627735. ](http://www.ncbi.nlm.nih.gov/pubmed/10627735)[View](http://www.ncbi.nlm.nih.gov/pubmed/10627735)[ ](http://www.ncbi.nlm.nih.gov/pubmed/10627735)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10627735)
16. [Boscainos PJ, Cousins GR, Kulshreshtha R, Oliver TB, Papagelopoulos PJ. Osteoid osteoma. Orthopedics. 2013 Oct 1;36(10):792-800. doi: 10.3928/01477447-20130920-10. Review. PubMed PMID: 24093694. ](http://www.ncbi.nlm.nih.gov/pubmed/24093694)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24093694)
QUESTION 16 OF 50
of 100
The patient is treated with emergent open reduction and internal fixation via a lateral approach to the distal femur. The peroneal nerve is found intact but is under pressure by a proximal bone fragment. After fixation, there is near-anatomic fracture reduction and no tension on the nerve. The patient is comfortable at a postsurgical check 4 hours later. Her toes
are warm and pink and there is no pain with passive dorsiflexion/plantar flexion of the toes. However, she continues to have absent first web space sensation, diminished dorsal foot sensation, and absent toe/ankle dorsiflexion. What is the best next step?
1
Return to surgery emergently for 4-compartment fasciotomy because she has a compartment syndrome and the nerve will not otherwise recover
2
Return to surgery urgently within the next few days for nerve exploration and potential microsurgical repair (vs cable grafting) to the damaged nerve to speed repair
3
Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 3 months after surgery
4
Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 12 months after surgery
- Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 3 months after surgery
QUESTION 17 OF 50
of 100
A 65-year-old man with ankylosing spondylitis has a fall from a standing height. He previously had minimal range of motion in his cervical spine, but now notices he is better able to extend his head. He is seen in the emergency department and released with a soft collar for use as needed.
1
Fracture displacement or subluxation leading to neurologic injury
2
Symptomatic epidural hematoma
3
Sepsis and death
4
Permanent nerve root injury and neurologic deficit
5
Loss of bowel or bladder control
- Fracture displacement or subluxation leading to neurologic injury
QUESTION 18 OF 50
-A 38-year-old woman is polytraumatized in a motor vehicle crash. She has multiple injuries including a unilateral femur fracture. The patient is felt to be borderline and, although she is currently stable,she could potentially deteriorate quickly. Which of the following parameters has been suggested as an indicator of which patients would benefit from damage control?
1
Normothermia
2
Hemoglobin of less than 9 g/dL
3
Unilateral lung contusion evident on CT only
4
Injury severity score of greater than 40 without thoracic injury
5
Injury Severity Score of less than 18 with a pulmonary contusion
No detailed explanation provided for this question.
QUESTION 19 OF 50
of 100
Cross-over sign
1
Figure 51a
2
Figure 51b
3
Figure 51c
4
Figure 51d
5
Figure 51e
- Figure 51c
QUESTION 20 OF 50
Which of the following is an effective medication for osteopetrosis:
Interferon gamma-1 is the only treatment for osteopetrosis that is approved by the Food and Drug Administration
QUESTION 21 OF 50
of 100
Figures 92a and 92b are the reconstruction radiographs of a 16-year-old boy with a high-grade conventional osteosarcoma of his right proximal tibia. He has completed neoadjuvant
chemotherapy. Wide resection, endoprosthetic proximal tibia replacement, a medial gastrocnemius flap, and a split-thickness skin graft were performed. The preferred postsurgical knee rehabilitation regimen is
1
therapist-directed passive and active assisted range of motion exercises from 0 to 90 degrees.
2
immobilization in full extension for 6 weeks with therapist-directed gait training and isometric exercises.
3
use of an immediate continuous passive motion machine set at 0 to 90 degrees followed by outpatient physical therapy.
4
use of a knee immobilizer for 2 weeks followed by home use of a continuous passive motion machine (set at 0 to 90 degrees).
This patient underwent resection of the patellar tendon insertion onto the proximal tibia. The residual tendon is sutured to the prosthesis with augmentation of the repair by the medial gastrocnemius flap. Immobilization for 6 weeks in full extension is preferred to permit healing of the tendon repair and prevent patella alta with associated extensor lag. Cast, splint, or brace are all acceptable options for the initial immobilization. Risk for knee stiffness with such immobilization is low because all of the distal knee ligamentous and capsular attachments are transected with resection. Two weeks of immobilization may be adequate for flap and skin graft healing, but this amount of time is inadequate for patellar tendon healing. Continuous passive motion vs therapist-
directed range of motion has not been rigorously compared for proximal tibia replacement. Responses 1 and 2 include early motion.
RECOMMENDED READINGS
89. [Eckardt JJ, Matthews JG 2nd, Eilber FR. Endoprosthetic reconstruction after bone tumor resections of the proximal tibia. Orthop Clin North Am. 1991 Jan;22(1):149-60. PubMed PMID: 1992431. ](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[View](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[ ](http://www.ncbi.nlm.nih.gov/pubmed/1992431)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1992431)
90. [Jentzsch T, Erschbamer M, Seeli F, Fuchs B. Extensor function after medial gastrocnemius flap reconstruction of the proximal tibia. Clin Orthop Relat Res. 2013 Jul;471(7):2333-9. doi: 10.1007/s11999-013-2851-8. Epub 2013 Feb 20. PubMed PMID: 23423620. ](http://www.ncbi.nlm.nih.gov/pubmed/23423620)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23423620)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23423620)
91. [Mavrogenis AF, Pala E, Angelini A, Ferraro A, Ruggieri P. Proximal tibial resections and reconstructions: clinical outcome of 225 patients. J Surg Oncol. 2013 Mar;107(4):335-42. doi: 10.1002/jso.23216. Epub 2012 Jul 17. PubMed PMID: 22806768. ](http://www.ncbi.nlm.nih.gov/pubmed/22806768)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22806768)
QUESTION 22 OF 50
Slide 1
A 56-year-old patient sustained an ankle fracture 3 years ago that was treated with closed reduction and cast immobilization. Since the injury, she has experienced pain upon ambulation and ankle stiffness. On examination, the range of motion of the ankle is 5° of dorsiflexion and 30° of plantarflexion. C repitus with motion is not present, but the patient does experience severe pain. A radiograph is presented (Slide). The recommended procedure to alleviate the patientâs pain and improve function is:
1
Total ankle replacement
2
Ankle arthrodesis
3
Ankle arthroscopy and joint debridement
4
Osteotomy of the fibula
5
Anterior ankle cheilectomy, Achilles lengthening, and joint debridement
The arthritis in this joint is not severe, but there is joint malalignment associated with a short and externally rotated fibula. Joint malalignment is correctable with a lengthening and rotational (internal) osteotomy of the fibula with bone graft. Joint debridement, either open or arthroscopic, is not effective in the management of posttraumatic ankle arthritis. Arthrodesis and arthroplasty are not necessary at this stage.
QUESTION 23 OF 50
An active 18-year-old patient reports severe left hip pain that prevents her from playing lacrosse. An AP radiograph of the pelvis is shown in Figure 73. What is the most appropriate option for this patient?
1
Activity modification
2
Hip fusion
3
Periacetabular osteotomy
4
Femoral osteotomy
5
Total hip arthroplasty
DISCUSSION: The patient has developmental dysplasia of the hip (DDH). There is anterolateral deficiency of the acetabulum as is evidenced by the increased acetabular index and the reduced center- edge angle. The patient has some arthritis of the hip with narrowing of the joint space and cyst formation visible on the radiograph. Although all of the mentioned choices may be acceptable treatments for dysplasia of the hip, periacetabular osteotomy is the best and most appropriate option for this young patient. Periacetabular osteotomy allows correction of the problem and can even improve the joint space as the new region of the acetabulum is rotated into the weight-bearing region. Hip fusion is very poorly tolerated by young patients, especially women. Femoral osteotomy alone is unlikely to address the problem because the major problem is on the acetabular side. Although the patient has arthritis, because of the young age of the patient, prosthetic replacement is not an attractive option. The outcome of periacetabular osteotomy even for patients with moderate arthritis has been favorable, deferring the need for total hip arthroplasty by a mean of 6.5 years.
REFERENCES: Weinstein SL, Mubarak SJ, Wenger DR: Developmental hip dysplasia and dislocation: Part 1. Instr Course Lect 2004;53:523-530.
Parvizi J, Burmeister H, Ganz R: Previous Bernese periacetabular osteotomy does not compromise the results of total hip arthroplasty. Clin Orthop Relat Res 2004;423:118-122.
Figure 74
QUESTION 24 OF 50
of 100
What is the most likely complication after surgical treatment of this injury?
1
Osteonecrosis of the fragment
2
Deep infection
3
Persistent stiffness at 2 years
4
Growth arrest of the capitellar physis
- Persistent stiffness at 2 years_
QUESTION 25 OF 50
of 100
A 68-year-old undergoes surgery for adult scoliosis with sagittal imbalance that necessitates a large kyphotic correction.
1
Proximal junctional kyphosis (PJK)
2
Adjacent segment degeneration
3
Intraoperative neurological injury
4
Postsurgical wound infection
- Proximal junctional kyphosis (PJK)
QUESTION 26 OF 50
Which of the following is considered an advantage of the tibial inlay fixation compared to transtibial tunnel technique when used in posterior cruciate ligament reconstruction?
1
Less invasive
2
Superior published clinical results
3
Decreased surgical time
4
Elimination of the critical 90-degree turn at the tibial aperture of the tunnel
5
Improved cosmesis
DISCUSSION: One of the most difficult aspects of posterior cruciate ligament reconstruction is placement of the tibial tunnel and passing of the graft through this tunnel. The tibial inlay technique requires a posteromedial approach to the tibia whereby the graft is directly fixed to the posterior aspect of the tibia. This obviates the need for a tibial tunnel. This technique has never been shown to be less invasive, more cosmetic,
or require decreased surgical time. It has also never been shown in a published level I study to have superior clinical results. However, it does eliminate the need for the 90-degree critical “killer” turn and passing of the tibial graft through the tibial tunnel which may lead to graft failure.
REFERENCES: McAllister DR, Petrigliano FA: Diagnosis and treatment of posterior cruciate ligament injuries. Curr Sports Med Rep 2007;6:293-299.
Cosgarea AJ, Jay PR: Posterior cruciate ligament injuries: Evaluation and management. J Am Acad Orthop Surg 2001;9:297-307.
QUESTION 27 OF 50
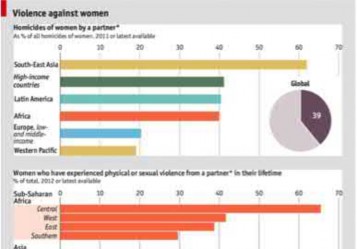
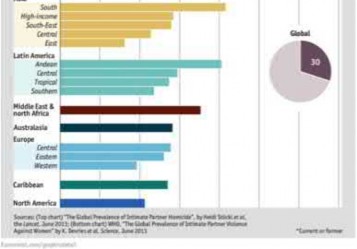
A 25-year-old female presents to the emergency room for the fourth time in the last week. She has vague complaints of extremity pain. Physical examination by a male ER resident has been limited each visit because she is terrified of the pain that the clinician may cause. On physical examination, she is withdrawn and frightened.
Regions of ecchymosis are noted throughout chest and abdomen. She has requested multiple radiographs, MRI and CT scans. Today's imaging (radiographs, MRI, CT scan) has been unrevealing. What is the most likely diagnosis?
1
Malingering
2
Complex regional pain syndrome
3
Anxiety disorder
4
Intimate partner violence
5
Fibromyalgia
Based on the history and clinical presentation, the most likely diagnosis is intimate partner violence.
Domestic violence or intimate partner violence can be in the form of mental or physical abuse, neglect or abandonment. Close to 25% of women will experience domestic violence. Risk factors include young age (19-29 years of age), females, pregnancy and lower socioeconomic status. Affected patients will have repeated visits to the emergency room, find reasons to stay in a treatment facility for an extended period of time and constantly seek approval
of their partner.
Shields et al. reviewed factors influence outcome in treatment of patients affected by domestic violence. They found that positive outcomes were associated with interdisciplinary approaches to management. This included better history assessment, providing written documentation regarding intervention and better access to information on community resources.
Illustration A is a chart documenting the frequency of female domestic violence throughout the world as of 2012.
Incorrect Answers
Answers 1, 2, 3, 5: These conditions are not consistent with this patient’s history.
QUESTION 28 OF 50
The normal porosity of trabecular bone is:
1
10%
2
20%
3
30%
4
40%
5
50% to 90%
Trabecular bone is arranged as a series of interconnecting small plates and rods. The porosity may vary between 50% to 90%. This porosity is secondary to the spaces between the trabecular pieces of bone rather than voids in the actual pieces of trabecular bone.
The normal porosity of cortical bone is 10%. Cortical bone porosity occurs because of the Haversian and Volkman canals and, to a lesser extent, from the ostocyte lacunae and canaliculi.
QUESTION 29 OF 50
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?**
1
Contact between the rotator cuff and the posterior-superior labrum
2
Anterior instability
3
A ganglion cyst of the spinoglenoid notch
4
Osteonecrosis of the humeral head
5
Posterior subluxation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity.
REFERENCES: Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
McFarland EG, Hsu CY, Neira C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
QUESTION 30 OF 50
A 7-year-old boy has a swollen and deformed right arm after falling off his bicycle. Radiographs reveal a completely displaced posterolateral supracondylar humeral fracture. Examination reveals a warm, pink hand and forearm but absent pulses. What is the next most appropriate step in management?
1
Angiography
2
Immediate closed reduction and casting in extension
3
Surgical exploration and repair of the artery, followed by skeletal stabilization
4
Closed reduction and pinning, followed by reassessment of the vascular status
5
Magnetic resonance angiography (MRA)
The incidence of vascular injury in supracondylar humeral fractures is directly related to the degree and direction of displacement. Significant posterior lateral displacement tends to result in brachial artery and median nerve injuries, and posterior medial displacement may lead to radial nerve injury. The brachial artery is always injured at the level of the fracture; therefore, angiography or MRA will not assist in locating the injury. The treatment of choice is surgical reduction and stabilization of the fracture, followed by reassessment of the vascular status. If the hand is pink and warm or pulses can be detected with doppler, it is reasonable to follow the extremity closely after surgery. If the arm becomes pulseless and white, immediate anterior exploration of the arm is indicated. The artery is often entrapped in the fracture and once extricated, will provide adequate blood flow. If the artery is injured, a primary repair or vein graft is needed.
REFERENCES: Shaw BA: The role of angiography in assessing vascular injuries associated with supracondylar humerus fractures remains controversial. J Pediatr Orthop 1998;18:273.
Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Schoenecker PL, Delgado E, Rotman M, et al: Pulseless arm in association with totally displaced supracondylar fracture. J Orthop Trauma 1996;10:410-415.
QUESTION 31 OF 50
Assuming that the fracture shown in this radiograph (Figure
1
is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active


2
metacarpophalangeal (MP) joint extension.
3
proximal interphalangeal (PIP) joint extension.
4
MP flexion.
5
PIP joint flexion.
This is a transverse proximal phalanx fracture with apex volar angulation. The fracture displaces into an apex volar angulated position under the pull of the central slip on the distal fragment and the interossei insertions at the base of proximal phalanx. Although it is possible to lose motion in flexion or extension of the MP or PIP joints, the biomechanics will not allow full extension of the PIP joint. If allowed to heal in apex palmar malunion, the predicted corresponding extensor lags are for a 10-degree lag at 16 degrees of angular deformity, a 24-degree lag at 27 degrees of deformity, and a 66-degree lag at 46 degrees of deformity. These fractures usually can be treated with closed reduction with or without percutaneous _pinning. With surgical treatment, there may be loss of motion both at the MP and PIP joints._
QUESTION 32 OF 50
Which of the following actions increases radiation exposure to patients and personnel when using fluoroscopy?
1
The use of lead glasses, thyroid shield, and a lead apron with a equivalent lead thickness of 0.25 mm
2
Orienting the cathode ray tube beneath the patient with the image intensifier receptor as close to the patient as possible
3
Limiting the beam on time to only what is clinically important
4
The use of continuous fluoroscopy to ensure proper placement of implants
5
Orienting the beam in the opposite direction of the working team and keeping the team outside a 6-foot radius from the fluoroscopy machine
Continuous fluoroscopy and cineradiography exposes the patient and personnel to markedly increased levels of direct and scatter radiation exposure.
Continuous fluoroscopy should be limited to only what is absolutely needed for safe completion of the procedure. By orienting the cathode ray tube beneath the patient and placing the image intensifier as close as clinically possible to the patient,scatter radiation exposure to the personnel is minimized.
QUESTION 33 OF 50
Figures 9a and 9b show the radiographs of a 28-year-old woman who sustained a head injury and a closed injury, without soft-tissue compromise, to her right lower extremity in a motor vehicle accident. Appropriate management of the foot injury should include
1
external fixation with a circular frame.
2
open reduction and internal fixation with screws.
3
closed reduction and percutaneous pinning.
4
closed reduction and cast immobilization.
5
amputation.
The displaced talar neck fracture should be treated with open reduction and internal fixation using screws. Closed reduction and casting will not maintain position, and percutaneous pinning is not able to maintain reduction to allow union. External fixation and amputation are not necessary for this injury unless there is severe soft-tissue loss.
REFERENCE: Adelaar RS: Fractures of the talus. Instr Course Lect 1990;39:147-156.
QUESTION 34 OF 50
With respect to the safety of allogeneic transfusions, which of the following infectious diseases is not tested for during routine laboratory blood screening?
1
Human immunodeficiency virus (HIV)
2
Hepatitis C
3
Lyme disease
4
Syphilis
5
West Nile virus encephalitis
DISCUSSION: Routine screening of donated blood usually includes screening for Hepatitis B, Hepatitis C, syphilis, HIV-1 (responsible for AIDS), HIV-2, and West Nile virus. Several bloodbome diseases that are not routinely screened for during blood donation include Lyme disease, malaria, babesiosis, and Chagas disease. Because routine blood bank practices do not include screening for all potential bloodbome diseases, surgeons should be aware of the possibility of disease transmission.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 217-224.
QUESTION 35 OF 50
Slide 1 Slide 2
A 9-year-old boy has a history of multiple fractures. He presents with left leg pain following a minor fall. His anteroposterior
(Slide 1) and lateral (Slide 2) plain radiographs are shown. The most likely genetiCdefect would be:
1
FGF receptor 3
2
Type I collagen
3
Cartilage oligomeriCmatrix protein
4
Fibrillin
5
Type II collagen
The anteroposterior and lateral radiographs show thinned cortices and a gentle S-shaped curve of the tibia. The overall alignment of the tibia, as well as the physes, is normal. These are the radiographiCfeatures of osteogenesis imperfecta.
In osteogenesis imperfecta, the genetiCdefect involves type I collagen. Type I collagen is made up of two alpha-1 chains and one alpha-2 chain in a triple helix. Glycine is the smallest amino acid and is crucial for coiling of the triple helix. Mutations in the
glycine chain lead to severe forms of osteogenesis imperfecta. One should also remember the Silence classification:
Type Inheritance Sclera Severity
I AD Blue Mild form, normal teeth
II AR Blue Lethal form, die early
III AR Normal Severe, progressively deforming
IV AD Normal Moderately severe
Biphosphonate therapy can be used to slow bone remodeling and increase bone mass. With regard to the incorrect choices:
FGF receptor 3 is associated with achondroplasia. Fibrillin is associated with Marfan's syndrome.
Type II collagen is associated with spondyloepiphyseal dsyplasia.
Cartilage oligomeriCmatrix protein is associated with pseudoachondroplasia. Correct Answer: Type I collagen
QUESTION 36 OF 50
of 100
What is the likelihood of this patient’s children having a similar condition?
1
No different than the likelihood among the general population
2
25% only if her partner is similarly affected; if not, no different than the population average
3
50%
4
100%
- 50%_
QUESTION 37 OF 50
Which of the following statements is true regarding Lyme disease:
1
C ardiac and neurologic symptoms are the most common manifestations of the disease.
2
Arthritic symptoms primarily affect large joints and a majority of patients are cured with antibiotic therapy.
3
The characteristic skin rash occurs late in the disease and can be permanently disfiguring.
4
Arthritic symptoms often do not fully resolve with antibiotic treatment, with a majority of patients progressing on to a rheumatoid-like destructive arthritis.
5
Lyme disease is easy to diagnose and a majority of cases are picked up after a few weeks.
Approximately 60% of patients develop arthritic symptoms that primarily affect large joints. The prognosis for most patients is good after treatment with antibiotics.
C ardiac and neurologic symptoms occur in a minority of patients, however, they can be the most serious symptoms. Erythema chronicum migrans is the characteristic skin rash. The rash tends to remit with antibiotic treatment and permanent disfigurement is not typically a problem.
Only 1%-2% of pediatric patients develop chronic arthritis.
Lyme disease may be difficult to diagnose because of the numerous possible presentations.
QUESTION 38 OF 50
The primary purpose of osteotomy in the closure of classic exstrophy of the bladder is to:
1
Decrease the tension on the closure of the abdominal wall and bladder
2
Decrease the strain on the sacroiliac joints
3
Prevent degenerative disease of the hip
4
Normalize the gait
5
Allow reconstruction of a normal symphysis pubis
The primary purpose of osteotomy is to improve the chance of a successful urologic reconstruction. This is achieved by decreasing the tension on the closure of the abdominal wall and bladder.
The strain on the sacroiliac joints has not been measured with or without closure; this is not a primary purpose of the osteotomy.
There is no conclusive evidence that the hips are at increased risk of degenerative disease in patients with exstrophy, or that osteotomy will alter the condition.
In patients with exstrophy, the gait progressively normalizes over time. It is not possible to reconstruct a normal symphysis pubis in exstrophy.
QUESTION 39 OF 50
Slide 1
A 55-year-old man presents for treatment of pain in the Achilles tendon. This has been present for 2 years, but has suddenly become much worse. The pain is approximately 6 cm proximal to the insertion. He is unable to push off during walking and has pain when ascending stairs. C linical examination reveals thickening of the tendon, weakness of the gastrocnemius-soleus, and pain upon squeezing the Achilles tendon. The magnetic resonance image is shown. The diagnosis is:
1
Xanthoma
2
Degenerative tendinosis
3
C hronic paratendinitis
4
Acute rupture
5
C hronic rupture
The widening and thickening over a length of the tendon noted clinically and on magnetic resonance image (MRI) is diagnostic of chronic degenerative tendinosis. While paratendinitis may be present simultaneously, limited MRI changes are noted in this condition. Rupture of the tendon may occur and patients with chronic tendinosis should recognize the potential for tendon rupture.
QUESTION 40 OF 50
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
1
Posttraumatic arthritis of the subtalar joint
2
Posttraumatic arthritis of the ankle joint
3
Malunion of the talus
4
Osteonecrosis of the talus
5
Complex regional pain syndrome
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction.
REFERENCES: Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its affects on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
QUESTION 41 OF 50
The bone avulsion shown in Figure 32 has a high correlation with tearing of the
1
iliotibial band.
2
anterior cruciate ligament.
3
posterior cruciate ligament.
4
lateral collateral ligament.
5
biceps femoris tendon.
As described by Segond in 1987, an avulsion fracture of the lateral tibial plateau is commonly referred to as a Segond fracture. Subsequent to 1987, several authors have also found that the lateral capsular sign represents, but is not limited to, a disruption of the middle third of the lateral capsule and a tear of the anterior cruciate ligament.
REFERENCES: Bach BR, Warren RF: Radiographic indicators of anterior cruciate ligament injury, in Feagin JA (ed): The Crucial Ligaments. New York, NY, Churchill Livingston, 1988, pp 301-327.
Segond P: Recherches cliniques et experimentales sur les epanchements sanguins du genou par entorse. Prog Med (Paris) 1987;7:297.
Johnson LL: Lateral capsular ligament complex: Anatomical and surgical considerations. Am J Sports Med 1979;7:156-160.
QUESTION 42 OF 50
Figure 1 is the axial MRI scan of a 45-year-old brick mason who experienced acute right elbow pain after attempting to lift a wheelbarrow. Examination reveals pain and swelling in the antecubital fossa, weakness with forearm supination, and an abnormal hook test. The surgeon performs an anterior repair with two anchors. Three months after surgery, the patient has appropriate strength and range of motion but reports persistent radiating paresthesias along the radial side of the forearm. What is the best next step in management?
1
Exploration of forearm with neurolysis
2
MRI scan of cervical spine
3
Revision distal biceps repair
4
Observation with nonsteroidal anti-inflammatory drugs as needed
This is a classic presentation of an acute traumatic distal biceps tendon rupture. In the dominant extremity of a manual laborer, this injury can result in approximately 40% loss of supination strength. Although not required, an MRI scan can confirm
the diagnosis. In general, a single incision anterior or two incision anterior/ posterior repair can be utilized for surgical intervention with similar success rates. Although the percentage of complications is similar between surgical approaches, the type of complications can vary. Anterior only repairs have a
20
higher risk of traction injury to the lateral antebrachial cutaneous nerve (LABC) secondary to the degree of retraction required for exposure in muscular patients. Posterior repairs have a higher risk for radiographic heterotopic bone formation. Fortunately, most LABC injuries are neuropraxias and resolve with observation, but resolution may take up to 6 months. In this case, ongoing observation is appropriate, with surgical exploration being considered only in chronic cases. Patients should be appropriately counseled about this issue prior to surgery.
QUESTION 43 OF 50
Compared with retention of the native patella in primary total knee arthroplasty, routine patellar
resurfacing is associated with
1
no patellar complications.
2
an increased occurrence of anterior knee pain.
3
a reduced patellar fracture rate.
4
a reduced risk for revision surgery.
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in
large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate
in patients with anterior knee pain.
QUESTION 44 OF 50
An 82-year-old man who underwent a primary total knee arthroplasty 11 weeks ago is now seen following a fall from a standing height. A radiograph is shown in Figure 42. Examination reveals a small abrasion of the skin overlying the anterior aspect of the knee. He is able to actively extend the the knee but has a 10-degree extensor lag. Initial management should include which of the following?
1
A 4-week period of immobilization followed by protected range of motion in a hinged knee brace
2
Use of a cylinder cast for 12 weeks
3
Open reduction and internal fixation of the fracture using a tension band technique 4 Revision of the patellar component
4
Resection of the proximal bony fragment and soft-tissue repair
DISCUSSION: The patient has a periprosthetic fracture of the patella but is able to actively extend his knee. Despite the wide displacement of the fracture fragments, nonsurgical management is recommended given the high risk of complications and problems when open treatment of these fractures is undertaken.
REFERENCES: Ortiguera CJ, Berry DJ: Patellar fracture after total knee arthroplasty. J Bone Joint Surg Am 2002;84:532-540.
Parvizi J, Kim KI, Oliashirazi A, et al: Periprosthetic patella fractures. Clin Orthop Relat Res
2006;446:161-166.
Figure 43a Figure 43b
QUESTION 45 OF 50
Figures below show the radiographs obtained from a 90-year-old woman who is seen in the emergency
department after a fall from a height. She has right hip and thigh pain and is unable to bear weight. Based on this patient's history and imaging, what is the best next step?
1
Hip revision and implantation of a proximal femoral replacement
2
Hip revision and implantation of a tapered fluted stem
3
Open reduction and internal fixation with a locked plate and allograft struts
4
Erythrocyte sedimentation rate and C-reactive protein laboratory studies
Periprosthetic fracture is the third most common reason (after loosening and infection) for revision surgery after total hip arthroplasty (THA). Late periprosthetic fracture risk is 0.4% to 1.1% after primary
THA and 2.1% to 4% after revision THA. Risk factors for periprosthetic fracture include age over 70 years, decreasing bone mass, and loosening of implants and osteolysis. The risk of concomitant infection in the presence of a periprosthetic fracture is 11%, according to Chevillotte and associates. Obtaining presurgical aspiration or intrasurgical tissue for culture is recommended if concomitant infection is suspected.
QUESTION 46 OF 50
The preferred means for fixation of patellar components is:
1
Large, central patellar lugs
2
Two parallel patellar lugs
3
Three large patellar-fixation lugs
4
Three small peripheral-fixation lugs
5
One central and two peripheral-fixation lugs
Large, central patellar-fixation lugs remove a significant amount of bone, which contributes to patellar fractures. Three small peripheral-fixation lugs are preferred in most designs
QUESTION 47 OF 50
A patient with a history of rheumatoid arthritis reports a painful total hip arthroplasty 3 years after the index procedure. Radiographs reveal loosening of the femoral component. Preoperative blood work shows an erythrocyte sedimentation rate (ESR) of 38 mm/h (normal 0-29 mm/h) and a C-reactive protein (CRP) of 8.9 (0.2- 8.0). What is the most appropriate action at this time?
1
Technetium bone scan
2
Hip aspiration for culture
3
FDG-PET scan
4
Surgery with no further investigations
5
Revision surgery and obtain an intraoperative frozen section
DISCUSSION: The question centers on the appropriate work-up for a failed total hip arthroplasty prior to revision surgery. The preoperative ESR is elevated and the CRP is at the upper end of normal. If either the ESR or CRP is elevated, further investigations are required to exclude infection as a cause of loosening, particularly in a patient only 3 years after the index procedure. A technetium scan alone is nonspecific and will show increased uptake because of the loose femoral component. An intraoperative frozen section is a helpful confirmatory investigation, but whenever possible the diagnosis should be made preoperatively to allow for appropriate surgical planning. Recently, investigators have shown the value of FDG-PET scanning as a useful investigation for diagnosing infection; however, it is no more accurate than the combined use of an ESR and CRP, and does not allow for identification of an infecting organism. At this point, a hip aspiration for culture is the most appropriate investigation.
REFERENCES: Bauer TW, Parvizi J, Kobayashi N, et al: Diagnosis of periprosthetic infection. J Bone Joint Surg Am 2006;88:869-882.
Pill SG, Parvizi J, Tang PH, et al: Comparison of fiuorodeoxyglucose positron emission tomography and (111
)indium-white blood cell imaging in the diagnosis of periprosthetic infection of the hip. J Arthroplasty 2006;21:91-97.
Spangehl MJ, Masri BA, O’Connell JX, et al: Prospective analysis of preoperative and intraoperative investigations for the diagnosis of infection at the sites of two hundred and two revision total hip arthroplasties. J Bone Joint Surg Am 1999;81:672-683.
Figure 5a Figure 5b
QUESTION 48 OF 50
All of the following muscles are innervated by the median nerve except:
1
The ulnar two lumbricals (lumbricals III and IV)
2
Opponens pollicis
3
Abductor pollicis brevis
4
Flexor pollicis brevis
5
Flexor digitorum profundus to the middle finger
Lumbricals 1 and 2 are innervated by the median nerve, in addition to the opponens pollicis brevis, abductor pollicis brevis, and flexor pollicis brevis.
QUESTION 49 OF 50
The clinical variable found to be associated with a higher risk of complications following open reduction and internal fixation of unstable ankle fractures in diabetic patients was:
1
Presence of a severe fracture pattern
2
Presence of an open fracture
3
Insulin-dependent diabetes mellitus
4
Peripheral neuropathy or vasculopathy
5
Presence of nephropathy
A retrospective Level IV study followed 84 patients with diabetes who underwent open reduction internal fixation of unstable ankle fractures. After analyzing multiple patient factors including sex, fracture pattern, open or closed injury, nephropathy, hypertension, vasculopathy, peripheral neuropathy, and diabetic control (insulin-dependent compared with non-insulin- dependent), the only factors that predicted a higher rate of complications were vasculopathy and peripheral neuropathy. There was a 12% rate of postoperative infection and an overall 14% rate of complications.
QUESTION 50 OF 50
of 100
Figures 73a through 73c are the radiographs of a 68-year-old woman with a pathologic left femur fracture. A clinical examination demonstrates a large soft-tissue mass at the fracture site. CT scans of the chest, abdomen, and pelvis reveal numerous enlarged lymph nodes. Frozen section analysis at open biopsy reveals relapsed lymphoma. What is the most appropriate treatment?
1
Antegrade reconstruction nail
2
Antegrade reconstruction nail and distal femur plate fixation
3
Retrograde femoral nail
4
Retrograde femoral nail and proximal femur plate fixation
Retrograde femoral nail fixation is mechanically advantageous for this fracture because it permits fixation distal to that which can be achieved with an antegrade nail. Most modern retrograde nail systems permit placement of multiple distal interlock screws that can be locked in a fixed-angle construct. Lytic bone destruction extends to the femoral condyles, making antegrade femoral nail fixation comparatively unsuitable. Classic orthopaedic oncology principles advise fixation of the entire bone whenever feasible. Evidence indicates that new distant metastasis within a fixated femur is a rare event, and efforts to protect the “whole bone” may not be warranted, especially if they entail additional risk. This argument is stronger regarding lymphoma-associated fractures (vs the more common carcinoma-associated fractures) because chemotherapy and radiation may be used to treat lymphoma with curative rather than palliative intent. Combined plate and nail fixation is not preferred in this scenario. Plate fixation alone or augmented with cement is a viable option
for this this fracture; however, the presence of a large soft tissue would likely necessitate extensive tumor debulking to appropriately place the plate.
RECOMMENDED READINGS
45. [Scholl BM, Jaffe KA. Oncologic uses of the retrograde femoral nail. Clin Orthop Relat Res. 2002 Jan;(394):219-26. PubMed PMID: 11795737.](http://www.ncbi.nlm.nih.gov/pubmed/11795737)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11795737)
46. [Alvi HM, Damron TA. Prophylactic stabilization for bone metastases, myeloma, or lymphoma: do we need to protect the entire bone? Clin Orthop Relat Res. 2013 Mar;471(3):706-14. doi: 10.1007/s11999-012-2656-1. Epub 2012 Oct 27. PubMed PMID: 23104043.](http://www.ncbi.nlm.nih.gov/pubmed/23104043)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23104043)
47. [Xing Z, Moon BS, Satcher RL, Lin PP, Lewis VO. A long femoral stem is not always required in hip arthroplasty for patients with proximal femur metastases. Clin Orthop Relat Res. 2013 May;471(5):1622-7. doi: 10.1007/s11999-013-2790-4. Epub 2013 Jan 30. ](http://www.ncbi.nlm.nih.gov/pubmed/23361930)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23361930)