This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set CD23EE)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
of 100
What is the best next step? 1- Knee aspiration
1
Blood cultures
2
Indium-labeled WBC scan
3
Pelvic radiographs
- Blood cultures
QUESTION 2 OF 50
Figures 1 through 3 depict the radiographs obtained from a 76-year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?
1
CT scan to assess component rotational alignment
2
Knee aspiration with cell count/cultures, CRP, ESR
3
Revision knee arthroplasty with intraoperative frozen section
4
Technetium-99m bone scan
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a
concern. 81
QUESTION 3 OF 50
A 27-year-old male competitive soccer player reports a 1-year history of pain in the adductor region that has prevented him from playing. Examination reveals tenderness about the adductor attachment to the pelvis, and pain at the same site with resisted contraction of the adductors. There is no tenderness over the hip joint and no signs of a sports hernia. Radiographs are normal. MRI does not show any evidence of enthesopathy. What is the next best step in management?
1
Hip arthroscopy
2
Corticosteroid injection
3
Percutaneous adductor tenotomy
4
Bone scan
5
Rheumatology consultation
DISCUSSION: Schilders and associates reported their results of treating adductor-related groin pain in competitive athletes. They reported that a single corticosteroid injection into the pubic cleft can be expected to provide at least 1 year of relief of adductor-related groin pain in a competitive athlete with normal findings on MRI. In contrast, when there is evidence of enthesopathy on MRI in this competitive- athlete population, these injections are not therapeutic and are associated with a high likelihood of recurrence of symptoms. Hip arthroscopy is generally reserved for intra-articular problems. Percutaneous adductor tenotomy is not indicated for this condition. A bone scan is unlikely to provide any useful information for clinical decision-making. Rheumatology consultation is also not indicated in the absence of any evidence of inflammatory arthropathy.
REFERENCES: Schilders E, Bismil Q, Robinson P, et al: Adductor-related groin pain in competitive athletes: Role of adductor enthesis, magnetic resonance imaging, and entheseal pubic cleft injections. J Bone Joint Surg Am 2007;89:2173-2178.
Robinson P, Barron DA, Parsons W, et al: Adductor-related groin pain in athletes: Correlation of MR imaging with clinical findings. Skelet Radiol 2004;33:451-457.
QUESTION 4 OF 50
Examination of an 18-year-old professional soccer player who was forcefully kicked across the shin while attempting a slide tackle reveals a marked effusion and limited motion of the knee. The tibia translates 12 mm posterior to the femoral condyles when the knee is held in 90 degrees of flexion. There is no posteromedial or posterolateral instability. Management should consist of
1
early reconstruction of all injured structures.
2
knee immobilization in 30 degrees of flexion for 2 to 4 weeks.
3
knee immobilization in full extension for 2 to 4 weeks.
4
protected weight bearing and intense hamstring strengthening.
5
no weight bearing, followed by a gradual return to sports.
The patient has an acute grade III posterior cruciate ligament injury. The majority of grade I and II injuries can be treated with protected weight bearing and quadriceps rehabilitation, and most patients can return to sports within 2 to 4 weeks. In contrast, grade III injuries require immobilization in full extension for 2 to 4 weeks to protect the posterior cruciate ligament and the other posterolateral structures presumed to be damaged. The mainstay of postinjury rehabilitation for all posterior cruciate ligament injuries is quadriceps strengthening exercises, which have been shown to counteract posterior tibial subluxation.
REFERENCES: Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Posterior Cruciate Ligament Injuries in Principles and Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott, Williams and Wilkins, 2000.
QUESTION 5 OF 50
A 23-year-old national team rower reports pain over the radial dorsum of the forearm that is made worse with flexion and extension of the wrist during competition. His primary physician initially diagnosed de Quervain’s tenosynovitis, and a subsequent corticosteroid injection into the first dorsal compartment at the wrist provided no relief. The patient continues to report pain and audible crepitus that is noted 5 cm proximal to the wrist joint, on the radial aspect. What structures are involved in the continued pathology?
1
Abductor pollicis brevis and extensor pollicis brevis
2
Abductor pollicis brevis and extensor pollicis longus
3
Abductor pollicis longus and extensor pollicis brevis
4
Abductor pollicis longus and extensor pollicis longus
5
Adductor pollicis and extensor pollicis longus
DISCUSSION: Intersection syndrome is also known as “squeakers wrist,” “oarsmen wrist,” and crossover tendinitis. It occurs where the first and second dorsal wrist compartment structures pass over one another, resulting in fibrosis, muscular changes, and inflammation of the bursa in this area. The structures involved are the abductor pollicis longus and extensor pollicis brevis (first dorsal compartment) that pass across the second compartment structures (extensor carpi radialis brevis and extensor carpi radialis longus). An audible “squeak” is occasiona**l** y heard at the intersection point, which is approximately 4 to 5 cm proximal to the proximal dorsal wrist crease.
REFERENCES: Grundberg AB, Reagan DS: Pathologic anatomy of the forearm: Intersection syndrome. J Hand Surg Am 1985; 10:299-302.
Thorson E, Szabo RM: Common tendinitis problems in the hand and forearm. Orthop Clin North Am 1992;23:65-74.
Williams JG: Surgical management of traumatic non-infective tenosynovitis of the wrist extensors. J Bone Joint Surg Br 1977;59:408-410.
Wood MB, Dobyns JH: Sports-related extraarticular wrist syndromes. Clin Orthop Relat Res 1986;202:93-102.
QUESTION 6 OF 50
Figure 1 is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence?
1
Sclerotherapy
2
Shave excision with cautery
3
Cryotherapy
4
Wide surgical excision
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision (Figures below) is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.
QUESTION 7 OF 50
A 15-year-old boy presented with inability to elevate his right shoulder and flex his elbow. He sustained a fall from an all-terrain vehicle 8 weeks ago. He landed on the right shoulder and twisted his neck. Radiographs of the skull, chest, cervical and thoracic spine, and shoulder were normal. There was no loss of consciousness, chest pain, or breathing difficulties. The patient was observed in the hospital until stable and referred for follow-up in the hand clinic at 4 weeks. An electromyelogram (EMG) was scheduled. C linical examination revealed weakness of deltoid, supraspinatus, infraspinatus, teres minor, biceps, brachialis, brachioradialis, and extensor carpi radialis longus. The remainder of his forearm musculature was preserved and he could
grasp, release, and pinch. Sensations were decreased along the distribution of the axillary nerve. There was 3 cm wasting of his arm and 2 cm of the forearm. Tinelâs sign is positive around the clavicle. Hornerâs signs are absent and his arm lies against the body. The EMG report showed fibrillation potentials in the weak muscles. The patient can now flex his elbow. When asked to demonstrate, he flexes his wrist and pronates his forearm to swing his elbow into flexion.
The least helpful test in further management of this patient is:
1
Magnetic resonance imaging (MRI)
2
C omputed tomography (C T) scan of the neck
3
Repeat electromyelogram (EMG) after 4 weeks
4
Somatosensory evoked potential (SSEP)
5
C areful neurological examination
C omputed tomography scan of the cervical spine will not show the pseudomeningoceles nor provide any information on brachial plexus. C omputed tomography may be needed in case of a suspected neck injury but does not form part of a brachial plexus work up.
QUESTION 8 OF 50
A 65-year-old woman landed on her nondominant left shoulder in a fall. An AP radiograph is shown in Figure 39. Management should consist of
1
closed reduction and immobilization.
2
closed reduction and percutaneous pinning.
3
open reduction and internal fixation.
4
humeral hemiarthroplasty with tuberosity repair.
5
total shoulder arthroplasty.
The radiograph reveals a four-part fracture-dislocation of the proximal humerus. Humeral hemiarthroplasty and tuberosity repair is the treatment of choice because the risk of osteonecrosis is high after attempted repair of this injury. Glenoid resurfacing is reserved for acute fractures in which there is significant preexisting glenoid arthrosis, such as in patients with rheumatoid arthritis.
REFERENCES: Neer CS II: Displaced proximal humeral fractures: II. Treatment of three- and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Robinson CM, Page RS, Hill RM, et al: Primary hemiarthroplasty for treatment of proximal humeral fractures. J Bone Joint Surg Am 2003;85:1215-1223.
QUESTION 9 OF 50
All of the following implants offer adequate fracture fixation of the injury shown in Figure A EXCEPT:
1
Trochanteric entry point cephalomedullary nail
2
Piriformis fossa entry point cephalomedullary nail
3
Dynamic hip screw
4
Fixed angle blade plate
5
95 degree dynamic condylar screw
Currently, cephalomedullary nails are used widely for reverse obliquity fractures because they limit medialization of the shaft fragment unlike sliding hip screws.
The Haidukewych et al study quoted demonstrated the superiority of fixed angle devices such as blade-plates or dynamic condylar screws over the sliding (or dynamic) hip screws. Reverse obliquity intertrochanteric fractures of the femur are recognized as biomechanically different from standard intertrochanteric fractures. The rate of failure of internal fixation for this fracture pattern was higher than the rates in most reports of internal fixation of intertrochanteric fractures devices.
QUESTION 10 OF 50
The first branch of the lateral plantar nerve innervates the
1
interossei.
2
quadratus plantae.
3
flexor digitorum brevis.
4
abductor hallucis brevis.
5
abductor digiti quinti.
The first branch of the lateral plantar nerve innervates the abductor digiti quinti, and more distal branches of the lateral plantar nerve supply the quadratus plantae and the interossei. The medial plantar nerve supplies the abductor hallucis brevis and the flexor digitorum brevis.
REFERENCES: Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983,
pp 325-328.
QUESTION 11 OF 50
A 22-year-old female dancer presents with left hip pain progressing over 6 months. Physical examination reveals pain with hip flexion, adduction and internal rotation and positive external log roll. Radiographs reveal crossover sign with positive posterior wall sign, and positive ischial spine sign. Center- edge angle (CEA) is 19°. MRI scan shows acetabular labral tear. She has failed attempts at nonsurgical management. What is the most appropriate surgical treatment?
63
1
Arthroscopic acetabular rim-trimming to correct retroversion deformity
2
Arthroscopic labral repair
3
Surgical dislocation with acetabuloplasty and labral advancement
4
Reverse periacetabular osteotomy
The patient demonstrates true acetabular retroversion, with deficient posterior and lateral coverage. While acetabular rim-trimming may be indicated for correction of retroversion deformities in volume-sufficient acetabulae, the risk of creating a secondary instability may preclude this treatment in volume- deficient hips (CEA <20, positive posterior wall sign). Arthroscopic and open techniques of acetabular rim-trimming have reported good results, equaling survivorship for periacetabular osteotomy at 5 years, but 10-year results suggest an advantage to periacetabular osteotomy for correction of retroversion.
QUESTION 12 OF 50
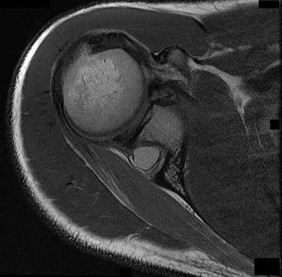
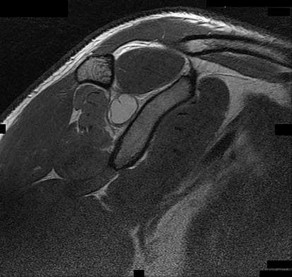
A previously healthy 22-year-old male presents to the hospital after a motor vehicle accident. His injuries include a closed head injury, flail chest, intra-abdominal bleed and right femoral shaft fracture. Which of the following conventional indicators would support the role for "damage control orthopaedics" as opposed to "early total care" in the clinical decision making process of his femur fracture management?
1
Lactate level = 1.9 mmol/L
2
Fibrinogen = 1.1 g/dL
3
Platelet count = 20,000 per mcL
4
Urine output = 50 cc/hr
5
Base deficit = 2 mmol/L
Previously healthy, poly-trauma patients, presenting with platelet counts of
<70,000 will fall into the pathophysiological category of 'in extremis'. This will
support the role of damage control orthopaedics in the decision making process of this patients fracture management.
Damage control orthopaedics (DCO) is a staged approach for the management of polytrauma patients. It is most ideal for trauma patients that are clinically unstable or in extremis. In these patients, immediate surgery is thought to cause a “second hit” phenomenon, which may lead to ARDS, multi-organ failure, or even death. A patient is classified as 'unstable' or 'in extremis', if he or she meets the criteria in at least three of the four pathophysiological parameters; blood pressure <90mmHg, platelets count <70,000, temperature
<32°C and major soft tissue injuries.
Pape et al. (2005) described four classes of patients, based on their clinical status: stable, borderline, unstable, and in extremes. The term “borderline” was coined to describe a patient who is categorized as stable before surgery, but is at significant risk of unexpected deterioration and organ dysfunction postoperatively.
Pape et al. (2009) outlined that stable patient can undergo early definitive fracture fixation as necessary. In contrast, unstable patient should be resuscitated and adequately stabilized with temporary fixation before receiving definitive orthopaedic care.
Illustration A shows a table outlining the classification system used by Pape to classify patients into their clinical status of stable, borderline, unstable, and in extremes.
Incorrect Answers:
Answer 1: Lactate level = 1.9 mmol/L (normal range <2.5 mmol/L) would classify this patient into a stable category.
Answer 2: Fibrinogen = 1.1 g/dL (normal range >1 g/dL) would classify this patient into a stable category.
Answer 4: Urine output = 50 cc/hr (normal range >150 cc/hr)would classify this patient into a borderline category.
Answer 5: Base deficit = 2 mmol/L (normal range -2 to +2 mmol/L) would classify this patient into a stable category.
QUESTION 13 OF 50
of 100
Stieda fracture
1
Figure 13a.
2
Figure 13b
3
Figure 13c
4
Figure 13d
5
Figure 13e
- Figure 13e
QUESTION 14 OF 50
The gold standard for the diagnosis of avascular necrosis of the femoral head is:
1
Bone scan
2
Routine roentgenogram
3
MagnetiCresonance image
4
Segmented bone collapse
5
Elevated sedimentation rate
The gold standard for the diagnosis of avascular necrosis is magnetiCresonance imaging. Changes can be seen earliest with this technique before there are changes on routine roentgenogram and even before a patient is symptomatic
QUESTION 15 OF 50
of 100
Which radiographic parameter is fixed as an adult (Figures 1 through 4)?
1
Figure 1
2
Figure 2
3
Figure 3
4
Figure 4
■ Pelvic incidence is a fixed sagittal parameter in adults. Figure 3 represents the pelvic incidence. Figure 1 represents the pelvic tilt. Figure 2 is an indirect way of measuring the sacral slope, as sacral slope = pelvic incidence - pelvic tilt. Figure 4 represents the sacral slope.
QUESTION 16 OF 50
A 21-year-old male is brought to the emergency department after being involved in gang-related violence. A radiograph of his pelvis is shown in Figure A. The patient is hemodynamically stable. Which of the following imaging modalities is the next best step in evaluating this patient for the most common associated injury?
1
Ultrasound bladder to exclude bladder perforation
2
CT abdomen to exclude bowel perforation
3
MRI pelvis to exclude genital injuries
4
CT angiogram exclude laceration of major vessels
5
CT acetabulum to exclude intra-articular foreign body
Low velocity gunshot wounds (GSW) to the hip are most commonly associated with bowel perforation. Consultation with general surgery (or in some facilities, trauma surgery) is necessary to exclude this.
The incidence of GSW is increasing and it is the 2nd leading cause of death in young males in the US after motor vehicle accidents. The incidence of a GSW to the buttock is approximately 8% of all GSW to the extremities. Potential complications of pelvic and acetabular GSW include septic arthritis, enterocutaneous, enteroacetabular, and vesicoacetabular fistulas, infected nonunion, malunion, and injuries to the iliac vessels. The presence or absence of intra-abdominal injuries affects treatment and outcome.
Bartkiw et al. reviewed 2808 GSW and found 1235 associated fractures including 42 fractures of the hip and pelvis. Ten orthopaedic operative
procedures were performed in 7 patients. Associated nonorthopaedic injuries included 15 small/large bowel perforations (36%), 7 vessel lacerations (17%), and 2 urogenital injuries (5%) that required surgery.
Najibi et al. reviewed 39 GSW to acetabulum. They found 32 simple and 7 associated fracture patterns. The most common simple and associated patterns were anterior column and both column, respectively. Bowel injuries were the most common associated injures (42%). Predictors of poor outcome include high-velocity missile, involvement of acetabular dome, abdominal injury, nerve injury, vascular injury, and male gender. Deep infection was associated with primary anastomosis of bowel injury and an associated fracture pattern.
Figure A shows a GSW to the right hip with acetabular fracture and visible bullet fragment.
Incorrect Answers:
Answers 1, 3, 4: Urogenital and vascular injuries are not as common as bowel injuries.
Answer 5: Intraarticular bullet fragments should be removed to prevent lead toxicity (plumbism), which arises from fragments dissolving in synovial fluid. Other reasons for removal include prevention of third body wear, joint sepsis and lead arthropathy. It is not the priority in this case and exclusion of bowel injury must take precedence.
QUESTION 17 OF 50
A 21-year-old professional baseball player has had painful catching and stiffness in his dominant right elbow for the past year. Examination reveals a flexion contracture of 2 degrees and mild pain with full elbow flexion. Radiographs are shown in Figures 33a and 33b. The most effective management should consist of**
1
reconstruction of the medial collateral ligament.
2
a short period of rest followed by a gradual return to activity.
3
physical therapy and dynamic extension splinting.
4
arthroscopic removal of the loose body.
5
a corticosteroid injection.
The radiographs show osteochondritis dissecans of the capitellum and a loose body in the anterior compartment. Arthroscopic removal is indicated because symptoms referable to the loose body are present.
REFERENCES: Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Shaughnessy WJ, Bianco AJ: Osteochondritis dissecans, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 282-287.
QUESTION 18 OF 50
A 16-year-old female swimmer reports several episodes of atraumatic glenohumeral instability that occur with different arm positions. Examination reveals generalized ligamentous laxity and a positive sulcus sign, and her shoulder can be subluxated both anteriorly and posteriorly. Initial management should consist of
1
a strengthening program for the rotator cuff and scapular muscles.
2
arthroscopic thermal capsulorrhaphy.
3
an inferior capsular shift.
4
a glenoid osteotomy.
5
a Putti-Platt repair.
The patient has multidirectional instability (MDI). It has been reported that a high percentage of patients with MDI respond to a properly structured exercise program that is continued for at least 3 to 6 months. If nonsurgical management fails to provide relief, stabilization with an inferior capsular shift procedure has been effective in a high percentage of patients. Unidirectional repairs, such as the Putti-Platt procedure, are unsuitable for correcting MDI. Thermal capsulorrhaphy has been reported to have a very high failure rate
(greater than 50%) for treating MDI.
REFERENCES: Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1992;74:890-896.
Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Pollock RG, Owens JM, Flatow EL, et al: Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am
2000;82:919-928.
Miniaci A, Birnie J: Thermal capsular shrinkage for treatment of multidirectional instability of the shoulder. J Bone Joint Surg Am 2003;85:2283-2287.
QUESTION 19 OF 50
A 45-year-old male undergoes open reduction internal fixation for a displaced olecranon fracture as shown in Figure A. What is the most common complication for this type of fixation?
1
anterior interosseous nerve palsy
2
osteomyelitis
3
implant failure
4
symptomatic implants
5
avascular necrosis
The most common complication of an olecranon fracture treated with tension band wiring is symptomatic implants. This is largely related to the
subcutaneous nature of the olecranon.
Macko and Szabo encountered a high incidence of complications related to the technique of tension-band wire fixation of displaced fractures of the olecranon in a five-year retrospective study of twenty patients. They reported that the most frequent complication of this construct is symptomatic prominence of the hardware which is usually due to improper seating at the time of surgery.
Other complications reported include loss of fixation, skin breakdown, and infection.
Hume and Wiss reported on 41 patients randomized to tension band wiring and plate fixation. They note that there was no difference in regards to elbow motion postoperatively, but plating required more operative time. Plating of these fractures resulted in a significantly increased rate of good clinical and radiographic results.
Figure A shows an AP and lateral radiograph of an olecranon fracture treated with tension-band wiring.
Incorrect Answers:
Answer 1: This is a possibility with overpenetration of the wires through the anterior ulnar cortex, but not a common finding.
Answer 2: This is not a common finding with this treatment method. Answer 3: Although implant failure is a possibility with this technique, this is not the most common complication.
Answer 5: Avascular necrosis of the proximal ulna is not a common complication of this injury or treatment method.
QUESTION 20 OF 50
A 32-year-old ballet dancer sustains a distal radius fracture, and is subsequently closed reduced and casted. She presents 11 months later with the radiograph seen in Figure A, complaining of significant wrist pain. What is the appropriate surgical treatment at this time?
1
Distal radius corrective osteotomy
2
Total wrist arthrodesis
3
Proximal row carpectomy
4
Scaphoid excision and four corner fusion
5
Interposition arthroplasty
The lateral wrist radiograph in Figure A shows significant dorsal angulation of the distal radius with a maintained joint space. The most appropriate surgical treatment for this patient would include corrective osteotomy of the distal radius, as there is no evidence of degenerative changes. If degenerative changes would be present, a salvage procedure such as total wrist arthrodesis would become an option.
The referenced article by Fernandez recommended distal radius corrective osteotomy with bone grafting and internal fixation for the following indications:
1) manually active patients who had a symptomatic extra-articular malunion of the distal end of the radius causing angulation of more than 25 to 30 degrees in either the frontal or sagittal plane without significant degenerative changes in the wrist joint (such as narrowing of the joint space, intra-articular incongruency, subchondral sclerosis, and osteophytic reaction) and in whom it
was thought that the result of either a Darrach procedure or shortening osteotomy of the ulna would be uncertain because the deformity of the radius would not be corrected, and 2) patients who wished to have the deformity corrected even though they had adequate function of the wrist.
QUESTION 21 OF 50
-are the radiographs of a 58-year-old right-hand dominant woman who fell from a standing height directly onto her left shoulder and now reports left shoulder pain and is unable to elevate her arm. She has a normal sensory examination. The patient refuses any type of surgical intervention.What factor will have the greatest impact on her outcome at 1 year?
1
Age
2
Bone quality
3
Hand dominance
4
Initial angulation of fracture
5
Use of a physical therapy program
No detailed explanation provided for this question.
QUESTION 22 OF 50
A 13-year-old girl has hip pain and the inability to bear weight. On anteroposterior and lateral hip radiographs the femoral head is displaced inferiorly and posteriorly by 50% of its diameter. Recommended treatment includes:
1
C losed reduction and immobilization in a spica cast
2
Traction followed by internal fixation
3
Open reduction and pin fixation
4
Metaphyseal osteotomy and internal fixation
5
In situ fixation with screw(s)
In situ fixation has results superior to any of the other methods.
Besides being extremely cumbersome, spica cast treatment carries significant risk of redisplacement and chondrolysis. There is no indication for traction in this situation.
The amount of displacement can be accepted as long as it is stabilized.
Metaphyseal osteotomy carries a risk of avascular necrosis. It should only be undertaken in grade III slips.
QUESTION 23 OF 50
A patient with a severe nickel allergy and degenerative joint disease of the hip would be best served by which of the following prosthetic options?
1
Cemented titanium stem, ceramic (alumina) head, and press-fit titanium cup
2
Cemented cobalt-chrome stem, ceramic (alumina) head, and press-fit cobalt-chrome cup
3
Press-fit titanium stem, cobalt-chrome head, and press-fit titanium cup
4
Press-fit titanium stem, titanium head, and press-fit titanium cup
5
Press-fit titanium stem, ceramic (alumina) head, and cementless titanium cup
DISCUSSION: Nickel is present in cobalt-chrome and stainless steel alloys used in orthopaedic surgery; therefore, these materials are not well suited for nickel-sensitive patients. Nickel is not present in titanium alloys or in ceramic components. Titanium is therefore the material of choice for the femoral and acetabular component.
Titanium is a poor option for the femoral head due to its susceptibility to abrasive wear. Titanium is also poorly suited to cemented applications in hip arthroplasty because it is less stiff than cobalt-chrome (and stainless steel), and therefore transmits greater stresses to the cement column. Titanium’s poor abrasion resistance can also leave the component susceptible to increased abrasive wear in the event of loosening and micromotion. Therefore, of the options available, a cementless titanium stem and socket with a ceramic head is the best choice. In nickel-sensitive total knee arthroplasty patients, cemented oxidized zirconium femoral components can be used in place of cobalt- chrome, and titanium tibial components (press-fit or cemented) have been used with success.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
QUESTION 24 OF 50
Which of the following is the most common finding in diastematomyelia:
1
C utaneous lesions over the spine
2
Anisomelia
3
Foot deformity
4
Neurologic deficit
5
Widened interpedicular distance
Widened interpedicular distance is the most common finding (94% or greater) in patients with diastematomyelia.
Neurologic deficit is present in 60% to 88% of patients with diastematomyelia.
A cutaneous lesion, such as a dimple or hairy patch, is present in 55% to 79% of patients with diastematomyelia. Anisomelia is present in 53% to 58% of patients with diastematomyelia.
Foot deformities are present in 32% to 52% of patients with diastematomyelia.
QUESTION 25 OF 50
Slide 1
A 33-year-old recreational athlete presents for treatment of chronic ankle pain. He recalls multiple ankle sprains that occurred
10 years ago. He has not undergone any surgical treatment. On examination, his ankle is stable, there is no crepitus on range of motion, and pain is present to palpation of the posterior ankle. A computerized axial tomography is presented (Slide). The surgical procedure most consistent with a rapid recovery and predictable outcome is:
1
Ankle arthrodesis
2
Arthroscopy of the ankle with drilling of the osteochondral defect
3
Osteoarticular autograft procedure
4
C artilage cell harvest with staged debridement of the talus and cartilage cell implantation
5
Osteoarticular allograft procedure
Ankle arthrodesis must be used as a salvage procedure for failed management of the osteochondral lesion of the talus. Although osteoarticular autograft is a popular procedure, the results are variable and unpredictable, particularly in posteromedial lesions. Ankle arthroscopy with transarticular drilling is the most predictable procedure with expected satisfactory results in approximately
80% of patients.
QUESTION 26 OF 50
Figure 1
A 35-year-old man has experienced ankle pain for 7 years. It is associated with giving way and progressive deformity of the foot. He notices that the foot is rolling inward and is becoming flatter. The cause of his condition is:
1
Tarsal coalition
2
Subtalar arthritis
3
Talonavicular arthritis
4
Recurrent ankle sprains
5
Rupture spring ligament
This patient presents with ankle instability and progressively worsening flatfoot, with the hindfoot in valgus. Although a rare condition, this is caused by a talonavicular tarsal coalition, with increasing stress on the ankle likely.
QUESTION 27 OF 50
A 24-year-old man presents for treatment of a painful fifth toe deformity. He had the deformity for 10 years and notes that it is getting progressively worse. On examination, a claw toe deformity is present. There is 90° of fixed hyperextension of the metatarsophalangeal joint, 70° of flexion at the interphalangeal joint, and a painful corn on the distal tip of the phalanx. The patient would like surgical correction. Which procedure is most likely to give him relief of pain and correction of deformity:
1
Flexor tenotomy and extensor tenotomy
2
Dorsal capsulectomy, extensor lengthening, and flexor tenotomy
Subtotal proximal phalangectomy with tendon transfer
C orrection of a fixed claw fifth toe deformity is not an easy procedure. The customary procedures used for correction of other lesser toe deformities are not always successful. In this patient, PIP arthroplasty or arthrodesis alone will not correct this deformity. The deformity requires a subtotal or complete proximal phalangectomy. Although this procedure corrects the deformity, patients must know that they will inevitably have a floppy fifth toe.
QUESTION 28 OF 50
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?
1
Hypertrophic cardiomyopathy
2
Atrial fibrillation
3
Pulmonary embolism
4
Ruptured aorta
5
Mitral valve prolapse
The number one cause of sudden death in the young athlete is myocardial pathology, with hypertrophic cardiomyopathy being most common. Because of cardiac muscle hypertrophy, the ventricular capacity is diminished and can result in decreased cardiac output. During exertional activities, the increased demand may not be able to be met and leads to sudden death. While the other choices can be the cause of sudden death in an otherwise healthy young athlete, their incidence is even more rare.
REFERENCES: Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647.
Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Mills JD, Moore GE, Thompson PD: The athlete’s heart. Clin Sports Med 1997;16:725-737.
QUESTION 29 OF 50
Slide 1 Slide 2 Slide 3
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The most likely complication in this child is:
1
Malignant degeneration
2
C arpal translocation
3
Posterior interosseous neuropathy (PIN) palsy
4
Peroneal nerve palsy
5
Elbow dislocation
Ulnar carpal translocation occurs due to the steep radial articular angulation that occurs due to the tethering effect of a shortened ulna and is already apparent in early stages in the first radiograph. While peroneal palsy is possible due to a proximal fibula lesion, it is less common. Malignant transformation occurs, risk varies with families.
QUESTION 30 OF 50
Which of the following precautionary measures should be taken to prevent a periprosthetiCfracture when removing components from a patient with a previous compression hip screw:
1
Cemented femoral component with cement augmentation of the screw holes and full weight bearing
2
Plate augmentation with circlage wires and protected weight bearing
3
Toe touch weight bearing for 6 weeks
4
Cortical strut allograft and protected weight bearing
5
Bypass the last screw hole with a cemented femoral component by two cortical diameters and protected weight bearing
Stress risers are generated when a screw is removed from the femur, weakening the bone for at least 4 weeks. Larger defects (50%) of the cortical width can reduce torsional strength up to 44%. Bypassing the defect by two cortical diameters with a cemented stem doubles the boneâs strength
QUESTION 31 OF 50
Figures 1 and 2 are the radiographs of a 72-year-old man 5 weeks after a right total knee arthroplasty (TKA). The patient has had continued drainage from a large hematoma in his right knee, despite an irrigation and debridement 4 weeks prior. His physical examination is notable for swelling and erythema with active purulent drainage. Prior operative cultures were negative for growth and repeat aspiration was negative for growth. What is the best next step?
2
1
Resection arthroplasty with a two-stage reconstruction of the knee
2
Resection arthroplasty with a single- stage reconstruction of the knee
3
Irrigation and debridement with a polyethylene insert exchange
4
Removal of components and a knee fusion with antibiotic beads
The patient has an infected TKA that has failed one prior washout. Another irrigation and debridement procedure is not indicated. Knee fusion would be indicated as a limb salvage. Without a known organism, a single-stage reconstruction of the right knee is not advisable. The two-stage reconstruction with an antibiotic spacer as the first stage is the benchmark standard.
QUESTION 32 OF 50
Which of the following muscle groups comprises the mobile wad of the forearm:
Brachioradialis, extensor carpi radialis brevis, extensor digitorum communis
5
Extensor carpi ulnaris, extensor pollicis brevis, extensor digitorum communis
The forearm contains the anterior, dorsal, and mobile wad. The following muscles are located in each compartment: Mobile wad
Brachioradialis
Extensor carpi radialis brevis
Extensor carpi radialis longus
Volar compartment
Flexor carpi ulnaris
Flexor digitorum profundus Flexor digitorum superficialis Palmaris longus
Flexor carpi radialis
Flexor pollicis longus
QUESTION 33 OF 50
of 100 A 61-year-old right-hand-dominant woman falls down the stairs, resulting in a left anteroinferior dislocation and noncomminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation
is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm. What is the most appropriate treatment?
1
Open reduction internal fixation with transosseous sutures
2
Arthroscopic fixation using a suture bridge technique
3
Nonsurgical treatment with early passive range of motion
4
Nonsurgical treatment with sling immobilization for 4 weeks
DISCUSSION
Greater tuberosity fractures and rotator cuff tears associated with a traumatic dislocation are more commonly seen in women >60 years. Greater tuberosity fractures that are displaced <5 mm in the general population and
<3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range
of motion is important to avoid stiffness.
QUESTION 34 OF 50
of 200
Figures 1a and 1b are the recent radiographs of an 82-year-old man with rheumatoid arthritis who underwent total knee arthroplasty (TKA) 18 years ago. These radiographs reveal osteolysis with loosening of the tibial component. Aspiration and laboratory study findings for infection are negative. During the revision TKA, treatment of tibial bone loss should consist of
1
filling the tibial defect with methylmethacrylate.
2
revision of the tibial component with porous metal augmentation.
3
reconstruction with iliac crest bone graft.
4
reconstruction with structural allograft.
No detailed explanation provided for this question.
QUESTION 35 OF 50
of 100
Figures 91a and 91b
1
Chromosome 17 mutation
2
MYH3 mutation
3
Embryonic vascular interruption
4
Infantile vascular interruption
5
Chromosome 11 mutation
- Embryonic vascular interruption
QUESTION 36 OF 50
The clinical variable found to be associated with a higher risk of complications following open reduction and internal fixation of unstable ankle fractures in diabetic patients was:
1
Presence of a severe fracture pattern
2
Presence of an open fracture
3
Insulin-dependent diabetes mellitus
4
Peripheral neuropathy or vasculopathy
5
Presence of nephropathy
A retrospective Level IV study followed 84 patients with diabetes who underwent open reduction internal fixation of unstable ankle fractures. After analyzing multiple patient factors including sex, fracture pattern, open or closed injury, nephropathy, hypertension, vasculopathy, peripheral neuropathy, and diabetic control (insulin-dependent compared with non-insulin- dependent), the only factors that predicted a higher rate of complications were vasculopathy and peripheral neuropathy. There was a 12% rate of postoperative infection and an overall 14% rate of complications.
QUESTION 37 OF 50
In the treatment of all magnitudes of bunionette deformities, what is the most common complication associated with lateral condylectomy of the fifth metatarsal head?
1
Metatarsophalangeal arthrosis
2
Transfer metatarsalgia
3
Recurrent deformity
4
Overcorrection of the deformity
5
Dislocation of the metatarsophalangeal joint
When a lateral condylectomy alone is performed for all bunionette deformities, a high recurrence rate is expected. Lateral condylectomy should be used alone when the primary deformity is an enlarged lateral condyle of the fifth metatarsal head. In cases with significant divergence of the fifth metatarsal shaft in relationship to the fourth metatarsal shaft or with lateral bowing of the distal fifth metatarsal shaft, the lateral fifth metatarsal prominence will not be effectively reduced and recurrent symptoms and deformity are expected. Transfer metatarsalgia and/or dislocation of the metatarsophalangeal joint can infrequently occur with excessive metatarsal head excision. Arthrosis of the metatarsophalangeal joint has not been frequently reported.
REFERENCES: Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465.
Kelikian H: Deformities of the lesser toe, in Kelikian H (ed): Hallux Valgus, Allied Deformities of the Forefoot and Metatarsalgia. Philadelphia, PA, WB Saunders, 1965, pp 327-330.
Kitaoka HB, Holiday AD Jr: Lateral condylar resection for bunionette. Clin Orthop 1992;278:183-192.
QUESTION 38 OF 50
A 75-year-old man has persistent radial sided hand and wrist pain. Radiographs demonstrate severe scaphotrapezial trapezoidal arthritis. His basal joint is unaffected. His pain has failed to improve with bracing, activity modification, and image-guided corticosteroid injection. He has elected surgical treatment. What longterm complication can arise from a distal scaphoid resection?
1
Avascular necrosis of the proximal pole of the scaphoid
2
Dorsal intercalated segment instability (DISI)
3
Volar intercalated segment instability
4
Thumb metacarpophalangeal joint hyperextension
Resection of the distal pole of the scaphoid eliminates the arthritic contact at the scaphotrapeziotrapezoid joint; however, it functionally shortens the scaphoid. Theoretically, the lunate is at equilibrium between the extension moment of the capitate and the triquetrum and the flexion moment of the scaphoid. Shortening the scaphoid allows the extension moment of the triquetrum to predominate, pulling the lunate into extension and creating a DISI deformity. Concomitant capsulodesis or interposition is recommended _by some authors to prevent this complication._
QUESTION 39 OF 50
of 100
Gerdy tubercle
1
Figure 13a.
2
Figure 13b
3
Figure 13c
4
Figure 13d
5
Figure 13e
- Figure 13a
QUESTION 40 OF 50
A 26-year-old woman presents for treatment of painful forefoot deformity. Hallux valgus is present, with a 35° angle, and arthritis of the metatarsophalangeal (MP) joint. The second and third lesser toe MP joints are dislocated with juxta-articular erosions of the fourth metatarsal head noted. The ideal surgical treatment is:
1
Silastic joint replacement of the hallux and osteotomy of the lesser metatarsals
2
Resection arthroplasty of the hallux and silastic arthroplasty of the lesser toe MP joints
3
Arthrodesis of the hallux MP joint and resection of the lesser metatarsal heads
4
Bunionectomy, proximal metatarsal osteotomy, and resection arthroplasty of the lesser MP joints
5
Resection arthroplasties of all the MP joints
For the patient with rheumatoid arthritis, stabilization of the hallux metatarsophalangeal joint is necessary, and a combination bunionectomy and metatarsal osteotomy is unlikely to succeed in the long-term when arthritis is present. Although shortening osteotomies of the lesser toe metatarsals may be considered to reduce the joint dislocations, this procedure has not yet been reported with long-term follow-up. Silastic joint replacement is not a procedure with long-term benefit, and is not indicated for the lesser toes.
QUESTION 41 OF 50
Which of the following is the most common cause of death in children with pelvic fractures:
1
Intrapelvic exsanguination
2
Head injury
3
Pulmonary embolism
4
Multisystem organ failure
5
Spinal cord injury
Head injury is the cause of virtually all mortality in children with pelvic fractures. The rarity of life-threatening intrapelvic hemorrhage is in marked contrast to adults. Pulmonary embolism and multisystem organ failure are rare in children.
QUESTION 42 OF 50
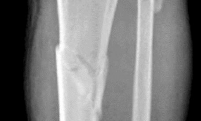
A 53-year-old man sustains a fall while skiing. He experiences immediate pain and deformity in his lower leg just above his ski boot top. Radiographs of his left lower leg are shown in Figures 1 and
1
After discussing operative management with the patient, you choose to proceed with an intramedullary nail. Where should blocking screws be placed to prevent the characteristic deformity of this fracture?





2
Posterior and medial aspect of the proximal fragment
3
Anterior aspect of the proximal fragment and medial half of the distal fragment
4
Posterior and lateral aspect of the proximal fragment
5
Anterior and lateral aspect of the proximal fragment
The patient has sustained a proximal third tibia and fibula fracture, sometimes referred to as a "boot top" fracture when sustained while alpine skiing. These fractures frequently fall into apex anterior and valgus
angulation as shown in the radiographs. Great care needs to be taken during intramedullary nailing to avoid fixing the fracture in a malreduced position. The use of Poller blocking screws in the posterior and lateral aspects of the proximal fragment can help to avoid this complication (posterior screw prevents flexion deformity while lateral screw prevents valgus deformity). Additional technical pearls include starting with a more lateral entry point for the guidewire, placing a provisional unicortical plate prior to nailing to maintain the reduction, or using a suprapatellar entry nail to allow for fixation with the knee in _a semi-extended position._
QUESTION 43 OF 50
of 100
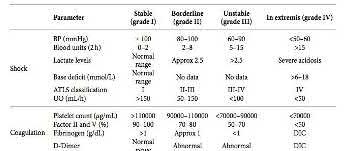
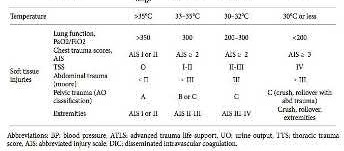
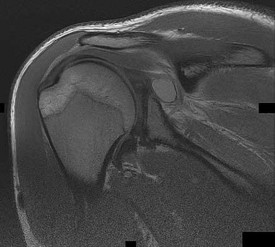
The cystic lesion shown on the MR images in Figures 46a through 46c should cause denervation changes in which muscle? A B
1
Subscapularis
2
Teres major
3
Infraspinatus
4
Supraspinatus
42
The cystic lesion is shown in an area adjacent to the spinoglenoid notch. A space-occupying lesion in this area has the potential to compress the suprascapular nerve as it passes through the spinoglenoid notch to innervate the infraspinatus. Compression of the nerve can cause denervation and atrophy of the infraspinatus muscle. The supraspinatus is innervated by the suprascapular nerve proximal to the compressive lesions and will not undergo atrophy. The subscapularis and the teres major are innervated by the subscapular nerve.
RECOMMENDED READINGS
1. Getz CL, Ramsey ML, Williams GR. Paralabral cysts of the shoulder. In: Galatz LM, ed. Orthopaedic Knowledge Update: Shoulder and Elbow 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:339-344.
2. [Takagishi K, Saitoh A, Tonegawa M, Ikeda T, Itoman M. Isolated paralysis of the infraspinatus muscle. J Bone Joint Surg Br. 1994 Jul;76(4):584-7. PubMed PMID: 8027145.](http://www.ncbi.nlm.nih.gov/pubmed/8027145)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8027145)
QUESTION 44 OF 50
Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implant is shown in Figure 1). He now has increasing hip pain. Radiographs reveal a stable hip arthroplasty and elevated serum cobalt and chromium levels. MR imaging is obtained, and based on these findings, the patient's hip is revised. Which corrosion type likely is responsible for this THA failure?
71
1
Galvanic
2
Pitting
3
Fretting
4
Crevice
Micromotion at the femoral head-neck or stem-neck junction can lead to fretting corrosion. Fretting corrosion is among the most common causes of failure in modular components. Modularity gives surgeons additional intraoperative flexibility but has resulted in corrosion-related failure and an implant recall. Although titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer, resulting in fretting corrosion. This may eventually lead to excessive metal ion formation and painful synovitis that necessitates a revision procedure. Galvanic corrosion is attributable to a mismatch in electrochemical gradients between dissimilar metals. Crevice or pitting corrosion occurs in fatigue cracks because of differences in oxygen tension.
QUESTION 45 OF 50
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course
of action?
1
Immediate MRI of the brain
2
Electromyography and nerve conduction velocity studies
3
Physical therapy and observation
4
Lyme titer
5
Psychiatric consultation
Lateral scapular winging is characteristic of trapezius palsy, whereas medial scapular winging is characteristic of long thoracic nerve palsy. During sports activity, injury to the spinal accessory nerve is rare but may occur with blunt or stretching trauma. Patients often report an asymmetric neckline, drooping shoulder, winging of the scapula, and weakness of forward elevation. Evaluation should include a complete electrodiagnostic examination.
REFERENCES: Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16.
Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27.
Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546.
Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Cohn BT, Brahms MA, Cohn M: Injury to the eleventh cranial nerve in a high school wrestler. Orthop Rev 1986;15:59-64.
QUESTION 46 OF 50
A college athlete on a scholarship has a medical condition that you feel presents a life-threatening risk to him with participation in athletics. Because of the gravity of this decision and the potential effect it can have on the student/athlete’s future, the college asks for your guidance. As the team physician for the college, what is your ethical obligation?
1
Ban the athlete from sports participation.
2
Allow the athlete to participate as it is his constitutional right to do so.
3
Advise the college to revoke the athlete’s college scholarship.
4
Offer no opinion as it is a matter strictly between the college and the athlete.
5
Recuse yourself from all decision making and advise the athlete to get an opinion from a third- party physician who is not employed by the college or university.
DISCUSSION: There is legal precedent for banning a scholarship athlete from participation in college
athletics if the physician feels that it presents a significant physical risk to the athlete. The courts have decided that the athlete has no constitutional right to participate in NCAA sports, and as a team physician you must advise your athlete and the school as to the best course of action. The athlete must be allowed to keep his or her college scholarship.
REFERENCES: Klossner D: NCAA Sports Medicine Handbook, ed 18. Indianapolis, IN, National Collegiate Athletic Association, 2007.
Pearsall AW IV, Kovaleski JE, Madanagopal SG: Medicolegal issues affecting sports medicine practitioners. Clin Orthop Relat Res 2005;433:50-57.
QUESTION 47 OF 50
Which of the following describes the radiographiCfeatures of a bone island:
1
Ovoid, compact, heavily mineralized intramedullary lesion with thorny spicules
2
Large, nodular, heavily mineralized lesion on the surface of the bone
3
Surface lesion with spiculated bone formation
4
Well-demarcated nidus surrounded by a distinct zone of sclerosis
5
Cortically based lytiCmetaphyseal lesion with a sclerotiCborder
Bone islands are also referred to as enostosis. They are usually solitary and composed of dense, compact bone within the medullary cavity. Patients are often asymptomatiCand the bone island is discovered as an incidental finding.
There are three features that may lead to confusion: The lesion may be as large as 3 cm to 5 cm.
The bone scan may show mild activity within the lesion.
Bone islands may grow slowly (approximately 1 mm per year).
The other possible answers describe the radiographiCfeatures of other lesions:
Osteoid osteoma: Well-demarcated nidus surrounded by a distinct zone of sclerosis
Parosteal osteosarcoma: Large, nodular, heavily mineralized lesion on the surface of the bone
Periosteal osteosarcoma:Surface lesion with spiculated bone formation
Non-ossifying fibroma: Cortically based lytiCmetaphyseal lesion with a sclerotiCborder
QUESTION 48 OF 50
The following pair of tendons is affected in De Quervain disease:
1
Extensor pollicis longus and extensor pollicis brevis
2
Abductor pollicis longus and extensor pollicis longus
3
Abductor pollicis brevis and extensor pollicis longus
4
Opponens pollicis and abductor pollicis brevis
5
Abductor pollicis longus and extensor pollicis brevis
De Quervain disease affects the tendons in the first dorsal compartment, the extensor pollicis brevis and the abductor pollicis longus (consisting of 2 to 7 individual tendon slips). The extensor pollicis longus traverses the third dorsal compartment. The abductor pollicis brevis and the opponens pollicis are thenar muscles and do not lie within any of the dorsal compartments.
QUESTION 49 OF 50
A 52-year-old woman has right hip pain and obvious swelling 3 years after undergoing a resurfacing arthroplasty. Her implant consists of a 42-mm femoral component and 48-mm socket. Her components are well positioned, and her metal ion levels are slightly elevated (less than 4 ppm) with a normal erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level. What is the most likely cause of her discomfort?
1
Pseudotumor from a local reaction to metal debris from the bearing surface
2
Chronic periprosthetic infection
3
Impingement of the femoral neck on the edge of the cup
4
Referred pain from lumbar disk disease
This patient likely has a soft-tissue reaction (pseudotumor) related to metal-on- metal articulation. Although the components are well positioned, patient gender and small head size are both known risk factors for failure of hip resurfacing arthroplasties. Metal ion levels are elevated but are not always markedly increased in the setting of a problematic metal-on-metal articulation. The patient should have a metal artifact reduction sequence MR imaging study to confirm the presence of a pseudotumor. Chronic infection is very unlikely in the setting of normal ESR and CRP findings. Impingement and lumbar disk disease would not explain the swelling around the hip.
QUESTION 50 OF 50
of 100
In addition to her planned primary procedure, how can the surgeon best improve this patient's lumbar lordosis?