This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set BD61F5)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
of 100
Which nerve is most commonly injured after total knee arthroplasty?
1
Tibial nerve
2
Superficial peroneal nerve
3
Infrapatellar branch of the saphenous
nerve 52
4
Sartorial branch of the saphenous nerve
The tibial or peroneal nerves usually are not injured during total knee arthroplasty. Incidence of peroneal nerve damage is highest in knees with a valgus deformity and an associated flexion contracture attributable to nerve stretch. This nerve injury occurs in as many as 9% of patients undergoing knee arthroplasty. Tibial nerve injury is a rare occurrence and usually an iatrogenic transection injury. The infrapatellar branch of the saphenous nerve and its nerve plexus is commonly injured after the medial parapatellar approach, and altered sensation attributable to injury is reported in up to 70% of cases. Injury typically manifests as numbness inferior to the patella. The sartorial branch of the saphenous nerve provides sensation distal to the knee and is uncommonly injured with a medial parapatellar approach. These concepts are illustrated in video 57, “Selective Exposures in Orthopaedic Surgery: The Knee, 2nd Edition.”
RECOMMENDED READINGS
1. Clarke HD, Bush-Joseph CA, Wolf BR. Selective Exposures in Orthopaedic Surgery: The Knee, 2nd Edition [DVD]. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2012.
2. [Hunter LY, Louis DS, Ricciardi JR, O'Connor GA. The saphenous nerve: its course and importance in medial arthrotomy. Am J Sports Med. 1979 Jul-Aug;7(4):227-30. PubMed PMID: 474860.](http://www.ncbi.nlm.nih.gov/pubmed/474860)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/474860)
3. [Mistry D, O'Meeghan C. Fate of the infrapatellar branch of the saphenous nerve post total knee arthroplasty. ANZ J Surg. 2005 Sep;75(9):822-4. PubMed PMID: 16174002.](http://www.ncbi.nlm.nih.gov/pubmed/16174002)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16174002)
4. [Schinsky MF, Macaulay W, Parks ML, Kiernan H, Nercessian OA. Nerve injury after primary total knee arthroplasty. J Arthroplasty. 2001 Dec;16(8):1048-54. PubMed PMID: 11740762.](http://www.ncbi.nlm.nih.gov/pubmed/11740762)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11740762)
QUESTION 2 OF 50
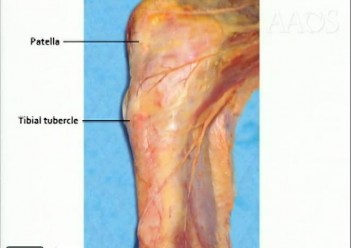
A 60-year-old man with previous right knee injury now has progressive pain over the last 2 years, despite physical therapy, low impact exercise and steroid injection. Figures 1 and 2 show his current radiographs. What is the best next step?
1
Posterior stabilized total knee arthroplasty (TKA)
2
Arthroscopic debridement with osteochondral autograft transplant
3
Constrained TKA
4
Hinged knee arthroplasty
Traditionally, patients with tibiofemoral arthritis and previous patellectomy have been treated with posterior-stabilized knee arthroplasties. There have been some reports suggesting that cruciate-retaining knee arthroplasties may have similar results. This patient has advanced tibiofemoral arthritis, and the only reasonable option listed is posterior stabilized knee arthroplasty. Constrained knee replacement offers no advantage in the absence of varus/valgus instability. The patient does not have knee instability and would not require a hinged prosthesis. 50
QUESTION 3 OF 50
Which of the following activities can improve posterior capsular contractures?
1
Theraband exercises to strengthen the external rotator
2
Latissimus pull-down exercises to the chest
3
Seated rows
4
Internal rotation stretch at 90 degrees abduction with scapular stabilization
5
Bench press with wide grip
Posterior capsule stretching is performed in the cross-chest and behind the back positions. Stretching in internal rotation in the abducted shoulder will further stretch the posterior capsule. Wide grip stretch, and anterior capsule and strengthening exercises will not necessarily stretch the capsule.
REFERENCES: Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Kibler WB, McMullen J, Uhl J: Shoulder rehabilitation strategies, guidelines, and practice. Op Tech Sports Med 2000;8:258-267.
QUESTION 4 OF 50
of 100
The patient in Figure 99 has pain at the first MTP joint.
1
Proximal phalangeal osteotomy alone
2
Proximal metatarsal osteotomy with a modified McBride procedure
3
Distal metatarsal osteotomy with a modified McBride procedure
4
First tarsometatarsal fusion with a modified McBride procedure
5
First metatarsophalangeal fusion
General principles can be used as bunion surgery guidelines even though there is extensive debate on the topic. A distal metatarsal osteotomy is most appropriate for patients with mild deformity and no transfer metatarsalgia. A proximal osteotomy potentially can correct more severe
deformities. A lapidus procedure, or tarsometatarsal fusion, provides the highest potential to correct deformity plus the advantage of stabilizing the first tarsometatarsal joint and limiting or eliminating transfer metatarsalgia. A first MTP fusion is most appropriate for patients with severe first MTP arthrosis.
RECOMMENDED READINGS
1. [Easley ME, Trnka HJ. Current concepts review: hallux valgus part II: operative treatment. Foot Ankle Int. 2007 Jun;28(6):748-58. Review. PubMed PMID: 17592710.](http://www.ncbi.nlm.nih.gov/pubmed/17592710)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17592710)
2. [Coughlin MJ, Shurnas PS. Hallux rigidus. Grading and long-term results of operative treatment. J Bone Joint Surg Am. 2003 Nov;85-A(11):2072-88. PubMed PMID: 14630834. ](http://www.ncbi.nlm.nih.gov/pubmed/14630834)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14630834)
QUESTION 5 OF 50
What complication is associated with the use of epidural morphine and steroid paste after laminectomy?
1
Surgical site infection
2
Arachnoiditis
3
Urinary retention
4
Disk space infections
5
Nerve irritation
Kramer and associates conducted a retrospective review during an
“epidemic” period to identify the risk factors associated with a sudden increase in the rate of surgical site infections. They found in a multivariate analysis that the use of morphine nerve paste resulted in a 7.6-fold increase in postoperative surgical wound débridement, and an 11% rate of surgical site complications. There is no evidence in the literature verifying the incidence of postoperative urinary retention and arachnoiditis.
QUESTION 6 OF 50
Placing the starting point for an antegrade femoral nail too anterior to the axis of the medullary canal can most commonly lead to what intraoperative complication?
1
Nail incarceration
2
Loss of locking screw trajectory into the lesser trochanter
3
Creation of a recurvatum deformity
4
Iatrogenic fracture of the proximal fragment
5
Decrease in hoop stresses
Usage of an anterior starting point that is too anterior leads to creation of significant hoop stresses in the proximal segment, potentially leading to iatrogenic fracture of the proximal segment. The referenced study by Johnson et al reviews the topic of femoral bursting and he notes that even shifting 6mm too far anteriorly can lead to proximal femoral fracture creation. He also reported that overreaming the canal by at least 0.5mm diameter is necessary to decrease hoop stresses throughout the femur, likely due to a mismatch in the radius of curvature of the femur and intramedullary nail.
QUESTION 7 OF 50
Exposure of tendons to ciprofloxacin in vitro causes all of the following except:
1
A decrease in fibroblast proliferation
2
An increase in proteoglycan synthesis
3
A decrease in proteoglycan synthesis
4
An increase in matrix degrading proteolytic activity
5
A decrease in collagen synthesis
C iprofloxacin was shown to cause a decrease in fibroblast proliferation, proteoglycan synthesis, and collagen synthesis. Matrix degrading proteolytic activity was increased.
QUESTION 8 OF 50
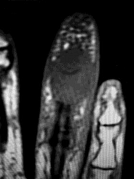
Figures 1 through 4 show the radiographs and MRI obtained from a 40-year-old man who has a 6-week history of ring finger pain, redness, and swelling after puncturing the finger with a toothpick. Purulent drainage from the puncture wound site grew _Eikenella corrodens_. The patient was initially treated with oral antibiotics for 10 days and then intravenous (IV) antibiotics for 3 weeks. What is the best next step in treatment? ---
---
---
---
1
Continued IV antibiotics for 4 weeks
2
Continued oral antibiotics for 6 weeks
3
Bone scan, biopsy, and metastatic work-up
4
Surgical débridement along with antibiotics
This patient has a septic distal interphalangeal joint, which was treated with antibiotics alone. As a result, the patient developed osteomyelitis with bone destruction and abscess. The best way to treat this problem is to perform surgical débridement of bone and soft tissue, along with abscess drainage and an appropriate antibiotic regimen. Antibiotic treatment without surgery would not be successful in eliminating this particular infection. Bone scan with biopsy is not the correct option, because this problem is an infection _and not a tumor, and MRI already has provided enough diagnostic information._
QUESTION 9 OF 50
of 100
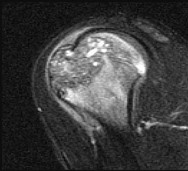
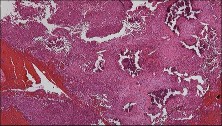
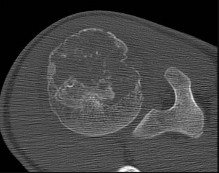
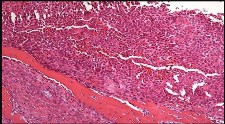
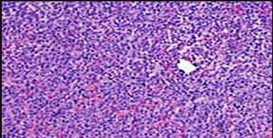
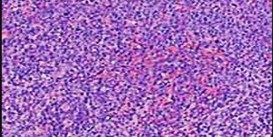
Figures 48a through 48e are the MR image, radiograph, CT scan, and biopsy specimens of a 14-year-old boy with right shoulder pain without antecedent trauma. What is the most likely diagnosis?
1
Unicameral bone cyst
2
Eosinophilic granuloma
3
Chondrosarcoma
4
Chondroblastoma
Imaging reveals a destructive mineralized lesion of the epiphysis and metaphysis in a skeletally immature patient. Epiphyseal lesions include chondroblastoma in skeletally immature patients and giant-cell tumors in skeletally mature patients. The histology confirms the diagnosis with the presence of multinucleated giant cells, “chicken-wire” calcifications, and chondroid islands. Chondrosarcoma would look histologically more aggressive than this and is unusual in children. Unicameral bone cysts do not have mineralization and are typically confined to the metaphysis radiologically. Eosinophilic granuloma can mimic many different lesions radiographically and can occasionally be found in the epiphysis of children, but the histology does not demonstrate classic Langerhans cells.
RECOMMENDED READINGS
34. Wold LE, Unni KK, Sim FH, Sundaram M, Adler C-P, eds. _Atlas of Orthopedic Pathology_. 2nd edition. Philadelphia PA: Saunders; 2003:232:237.
35. [De Mattos CB, Angsanuntsukh C, Arkader A, Dormans JP. Chondroblastoma and chondromyxoid fibroma. J Am Acad Orthop Surg. 2013 Apr;21(4):225-33. doi: 10.5435/JAAOS-21-04-225. Review. PubMed PMID: 23545728.](http://www.ncbi.nlm.nih.gov/pubmed/23545728)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23545728)
CLINICAL SITUATION FOR QUESTIONS 49 AND 50
Figure 49 is the radiograph of a 22-year-old woman with pain and snapping about the knee. Her husband does not have this condition.
QUESTION 10 OF 50
of 100
An 18-year-old woman who plays high school volleyball (Figure 44)
1
Ligamentous reconstruction
2
Meniscal repair
3
Meniscectomy
4
Immobilization
Figure 41 is a coronal MR image demonstrating a medial collateral ligament (MCL) tear. MCL injuries usually are treated with immobilization for 4 to 6 weeks. Surgical treatment is recommended only in cases of persistent valgus laxity or rotatory instability after bracing. Subacute or chronic medial instability associated with cruciate injury is also an indication for surgery.
Figures 42 and 43 are MR images demonstrating lateral meniscal tears. In Figure 42, the coronal view shows a tear through the white-white zone in a discoid lateral meniscus. Because of the location of the tear, this patient is treated with arthroscopic partial meniscectomy. In Figure 43, the lateral view reveals a bucket handle tear of the lateral meniscus that is treated with repair. Figure 44 is an axial MR image demonstrating characteristic bony edema over the medial patella and lateral femoral condyle after an acute lateral patellar dislocation. Immobilization is also recommended for first-time acute patellar dislocations. Surgical treatment for a first-time patellar dislocation is recommended only when a displaced osteochondral fragment is present.
RECOMMENDED READINGS
1. Asik M, Sen C, Taser OF, Alturfan AK, Sozen YV. Discoid lateral meniscus:
41
diagnosis and results of arthroscopic treatment. Knee Surg Sports Traumatol Arthrosc.
[2003 Mar;11(2):99-104. Epub 2003 Jan 25. PubMed PMID: 12664202. ](http://www.ncbi.nlm.nih.gov/pubmed/12664202)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/12664202)[ ](http://www.ncbi.nlm.nih.gov/pubmed/12664202)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12664202)
2. [Jacobson KE, Chi FS. Evaluation and treatment of medial collateral ligament and medial-sided injuries of the knee. Sports Med Arthrosc. 2006 Jun;14(2):58-66. Review. PubMed PMID: 17135948. ](http://www.ncbi.nlm.nih.gov/pubmed/17135948)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17135948)
3. Laible C, Stein DA, Kiridly DN. Meniscal repair. J Am Acad Orthop Surg. 2013 Apr;21(4):204-13. doi: 10.5435/JAAOS-21-04-204. Review. PubMed PMID:
[23545726.](http://www.ncbi.nlm.nih.gov/pubmed/23545726)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23545726)
4. [Palmu S, Kallio PE, Donell ST, Helenius I, Nietosvaara Y. Acute patellar dislocation in children and adolescents: a randomized clinical trial. J Bone Joint Surg Am. 2008 Mar;90(3):463-70. doi: 10.2106/JBJS.G.00072. PubMed PMID: 18310694. ](http://www.ncbi.nlm.nih.gov/pubmed/18310694)[View](http://www.ncbi.nlm.nih.gov/pubmed/18310694)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18310694)
QUESTION 11 OF 50
The hereditary pattern for Holt-Oram syndrome is:
1
Autosomal recessive
2
Autosomal dominant
3
Sex-linked recessive
4
Sex-linked dominant
5
Sporadic
Holt-Oram syndrome is inherited in an autosomal dominant manner.
QUESTION 12 OF 50
ProsthetiCplacement in a cement-filled canal creates highest peak elevations in pressure when:
1
Using a cement restrictor
2
Using a retrograde filling
3
Using mechanical pressurization
4
Inserting the prosthesis late in the setting phase
5
Inserting the prosthesis early, while the cement is extremely soft
ProsthetiCplacement in the cement-filled femoral canal creates transiently higher peak elevations in pressure when inserted late in the setting phase. It creates higher pressures than those obtained with a cement restrictor, retrograde filling, or mechanical pressurization
QUESTION 13 OF 50
A 72-year-old man injured his right shoulder after tripping over a chair leg. Radiographs obtained in the emergency department reveal an isolated anterior dislocation. After successful closed reduction, the patient has recurrent anterior instability and is unable to elevate the arm. What is the most likely cause of the recurrent instability?
1
Infection of the anterior glenoid labral detachment
2
Anterior glenoid fracture
3
Axilllary nerve palsy
4
Occult surgical neck fracture
5
Rotator cuff tear
A rotator cuff tear is the most common cause of recurrent instability following a first-time dislocation in patients older than age 40 years. Dislocations occur through a posterior mechanism rather than by an isolated labral avulsion or a Bankart lesion as seen in younger patients.
REFERENCES: Nevaiser RJ, Nevaiser TJ: Recurrent instability of the shoulder after age 40.
J Shoulder Elbow Surg 1995;4:416-418.
Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294.
QUESTION 14 OF 50
The treatment of stenosing tenosynovitis should include all of the following except:
1
Release of the A1 pulley.
2
Release of the A1 pulley and flexor tendon tenosynovectomy.
3
Splinting and nonsteroidal anti-inflammatory drugs (NSAIDs).
4
Steroid injections between the flexor tendon and the A1 pulley.
5
Release of the A1 and A2 pulleys.
The A2 pulley should not be released as part of the treatment for trigger finger. Its presence, along with the A4 pulley, is important in maintaining efficient flexor tendon function. The pathology usually involves the A1 pulley and its release is usually all that is necessary.
Other modalities include NSAIDs, splinting, tenosynovectomy, and steroid injections.
QUESTION 15 OF 50
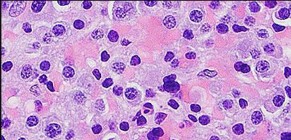
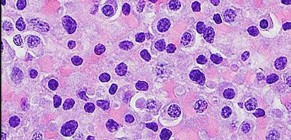
of 100 Figures 88a through 88d are the radiographs and biopsy specimens of a 65-year-old woman with a history of breast cancer who has been experiencing 6 weeks of increasing left hip pain. She denies any injury. What is the most likely diagnosis?
1
Metastatic breast cancer
2
Myeloma
3
Fibrous dysplasia
4
Osteosarcoma
Radiographs reveal a destructive lesion. A differential diagnosis would include metastatic disease, myeloma, lymphoma, or primary sarcoma of bone. Histology shows sheets of plasma cells with eccentric nuclei, coarsely clumped nuclear chromatin, and a perinuclear halo. This pathology is consistent with myeloma. Metastatic disease would reveal nests of epithelia cells in a fibrous
background. Fibrous dysplasia would reveal irregular bony trabecular without rimming osteoblasts. Osteosarcoma would reveal malignant cells making osteoid.
RECOMMENDED READINGS
80. [Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011 Mar 17;364(11):1046-60. doi: 10.1056/NEJMra1011442. Review. PubMed PMID: 21410373. ](http://www.ncbi.nlm.nih.gov/pubmed/21410373)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21410373)
81. Swerdlow S, Campo E, Harris N, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, eds. _WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues_ , 4th ed. Lyon, France: IARC Press; 2008.
QUESTION 16 OF 50
All of the following are characteristic of hemangiomas except:
1
70% of hemangiomas are visible by 4 weeks of age
2
70% of hemangiomas regress by 7 years of age
3
Hemangiomas are three times more common in woman than men
4
All cavernous hemangiomas regress by 12 years of age
5
None of the above
C avernous hemangiomas are noninvoluting hemangiomas and require surgical excision.
QUESTION 17 OF 50
A 25-year-old male presents to the emergency department with a mangled lower extremity that is not salvageable. He undergoes transfemoral amputation. Three months later the patient presents to the office with the limb sitting in an abducted position. What important step was forgotten during the amputation?
1
Beveling the distal femur
2
Saving the patella
3
Allowing the sciatic nerve to retract deep into the soft tissue
4
Myodesis of the adductors
5
Timely fitting of orthosis
Prior to the late 80’s, techniques for transfemoral amputation sacrificed the hip adductor muscles resulting in unopposed abductor forces. Amputation with an abducted femur leads to an increase in side lurch and higher energy consumption. Gottschalk in ’99 showed that myodesis of the adductor magnus through drill holes in the lateral femur preserved maximum muscle force and provided a mechanical advantage for the adductors of the thigh. This resulted in maintenance of the normal anatomic alignment of the femur and a balance between the abductor and adductor mechanisms of the hip, thus providing patients with improved control and easier prosthesis fit.
QUESTION 18 OF 50
of 100
The most appropriate treatment of this lesion involves
1
radiofrequency ablation (RFA).
2
wide resection and hemicortical allograft reconstruction.
3
prophylactic internal fixation followed by radiation.
4
local debridement and an infectious disease consultation.
- radiofrequency ablation (RFA)._
QUESTION 19 OF 50
A patient with deficient anteroinferior bone stock undergoes a Latarjet procedure that transfers a portion of the coracoid to the glenoid rim and secures it with two screws. After surgery, the patient reports numbness on the anterolateral forearm. To verify the diagnosis, what muscle should be tested for strength?
1
Axillary
2
Abductor pollicis brevis
3
Supinator
4
Triceps
5
Biceps
A Latarjet procedure is similar to a Bristow procedure, but with the Latarjet procedure a larger portion of the coracoid is transferred to the scapular neck at the anteroinferior glenoid. As in a Bristow procedure, if the fragment is pulled or twisted during the dissection or during fixation, the musculocutaneous nerve can be injured. With loss of biceps function, elbow flexion and forearm supination will be weaker.
REFERENCES: Ho E, Cofield RH, Balm MR, Hattrup SJ, Rowland CM: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
Boardman ND 3rd, Cofield RH: Neurologic complications of shoulder surgery. Clin Orthop 1999;368:44-53.
Allain J, Goutallier D, Glorion C: Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 1998;80:841-852.
QUESTION 20 OF 50
of 100
A 7-year-old boy is treated for a femoral shaft fracture with flexible intramedullary (IM) nailing. At 2 years postoperative, 1.5-cm overgrowth of the injured side is noted. Which factors increase the risk of overgrowth?
1
Length stable fracture pattern and nail canal diameter ratio <0.8
2
Length stable fracture pattern and nail canal diameter ratio ≥0.8
3
Length unstable fracture pattern and nail canal diameter ratio <0.8
4
Length unstable fracture pattern and nail canal diameter ratio ≥0.8
■ The incidence of leg-length discrepancy following IM nailing of femoral shaft fractures ranges from 8% to 20% related either to overgrowth or shortening through the fracture site. Overgrowth may be related to greater fracture instability and hyperemia, which stimulates the physis. Length unstable fracture patterns and decreased "canal fill" by the flexible nails (nail canal diameter ratio <0.8) have both been associated with femoral overgrowth.
QUESTION 21 OF 50
Figure 1 is the MRI scan of a 25-year-old left-hand dominant minor league pitcher with a 6 month history of progressive left elbow pain during pitching. He fails nonoperative treatment and undergoes surgery to address the problem. What is the most common complication of this procedure?
1
Ulnar nerve neuropraxia
2
Flexor pronator mass avulsion
3
Posterolateral rotatory instability
4
Symptomatic hardware
The MRI scan shows evidence of a medial collateral ligament (MCL) tear. In a patient with a chronic MCL injury that has failed non-operative treatment, MCL reconstruction would be indicated. Initial MCL reconstruction technique involved routine transposition of the ulnar nerve and detachment of the flexor- pronator mass. Subsequent.
technique modifications have been made to minimize complications by avoiding routine ulnar nerve transposition and performing a muscle-splitting approach. Despite these improvements, transient ulnar nerve neuropraxia remains the most common complication, and patients should be counseled about its occurrence pre-operatively. Flexor pronator mass avulsion is more likely with a muscle-detaching approach, but is not more common than ulnar nerve neuropraxia. Posterolateral rotatory instability is a complication of lateral collateral ligament repair or reconstruction, not medial collateral ligament reconstruction. Symptomatic hardware is not a common complication from this procedure 56
QUESTION 22 OF 50
Figure 60 is the radiographs of a patient who underwent surgery to alleviate pain under her second metatarsal that is worsened by wearing high heel shoes. What is the most common complication of the osteotomy shown in the radiographs?
1
Osteonecrosis
2
Nonunion of the osteotomy
3
Significant transfer lesions
4
Metatarsophalangel (MTP) arthritis
5
Dorsiflexion contracture at the MTP joint
The radiographs show a Weil osteotomy that is used to treat metatarsalgia, which is often associated with severe claw toes. The most common complication is a floating toe, or dorsiflexion contracture
at the MTP joint. This is because the interossei muscles move dorsally with respect to the axis of the MTP joint due to depression of the plantar fragment and that the center of rotation is altered after the osteotomy. Multiple studies have shown that the floating toe is the main complication and that the other listed complications rarely occur with this type of osteotomy.
QUESTION 23 OF 50
What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?
1
True lateral
2
Lateral in 30 degrees of pronation
3
Lateral in 30 degrees of supination
4
Posteroanterior in 30 degrees of pronation
5
Carpal tunnel
The pisotriquetral joint is best seen on a lateral view in 30 degrees of supination. The carpal tunnel view provides visualization of the joint but to a lesser extent. The other views do not provide clear and accurate visualization.
REFERENCES: Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
Steinmann SP, Linsheid RL: Pisotriquetral loose bodies. J Hand Surg 1997;22:918-921.
**related link****[ortho mcqs bank](https://hutaifortho.com/?sid=23)**
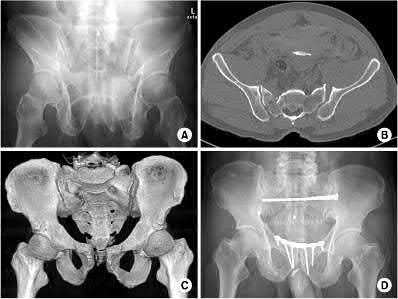
1250) Based on the Young and Burgess classification of pelvic ring injuries, an anterior-posterior compression type II injury does not result in disruption of which of the following?
1
pubic symphysis
2
anterior sacroiliac ligaments
3
posterior sacroiliac ligaments
4
sacrospinous ligament
5
sacrotuberous ligament
The posterior sacroiliac ligaments are not disrupted in an APC type II pelvic fracture.
Young and Burgess classification of pelvic ring injuries is largely based on the mechanism and energy of injury. An APC type I involves slight widening of
pubic symphysis and/or anterior sacroiliac (SI) joint. An APC II is a continuation of this force, and additionally involves a disrupted anterior SI joint, as well as sacrotuberous and sacrospinous ligaments. An APC III also involves disrupted posterior SI ligaments, causing complete SI joint disruption with potential translational and rotational displacement.
The reference by Young et al is a classic article that describes the Young and Burgess classification of pelvic ring injuries. They retrospectively analyzed pelvic ring radiographs and discussed four patterns of injury: anteroposterior compression, lateral compression, vertical shear, and a complex/combined pattern.
The reference by Burgess et al is a validation of the aforementioned classification and study, as they reviewed 210 consecutive patients who sustained a pelvic ring injury. They validated the classification scheme and found that overall blood replacement averaged: lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units. Overall mortality was: lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear, 0%; combined mechanical, 18.0%.
Illustration A shows an APC-II injury pattern - (a) is an outlet radiograph, (b) is an axial CT cut, (c) is a 3-D CT cut, and (d) is a representative fixation construct.
Incorrect answers:
1,2,4,5: An APC - 2 pelvic ring injury involves injury to all of these structures.
QUESTION 25 OF 50
A 10-year-old soccer player has bilateral heel pain and reports that the pain is worse during and immediately after sports. Examination reveals that the calcaneal tuberosities are painful to palpation bilaterally. What is the most likely diagnosis?
1
Plantar fasciitis
2
Calcaneal apophysitis
3
Achilles tendinitis
4
Calcaneal bursitis
5
Stress fractures of the calcanei
Calcaneal apophysitis (Sever’s disease) is a common cause of heel pain in children who are active in sports. The symptoms are most commonly bilateral and will often respond to a gastrocnemius-soleus complex stretching program. In addition, rest, anti-inflammatory drugs, and heel pads for the shoe may be prescribed. There is no effect on the long-term growth of the calcaneus.
REFERENCES: Micheli LJ, Ireland ML: Prevention and management of calcaneal apophysitis in children: An overuse syndrome. J Pediatr Orthop 1987;7:34-38. 500.
A 46-year-old man reports occasional squeaking of his hip 2 years after undergoing an uneventful total hip arthroplasty. History reveals no pain, physical examination cannot reproduce audible squeaking, and radiographs show appropriate implant position. What is the most appropriate management?
1
Revise the cup bearing to polyethylene
2
Revise the cup bearing to polyethylene and replace the femoral head with a metal design
3
Increase the cup abduction angle
4
Decrease the cup abduction angle
5
Continue routine follow-up and observation
DISCUSSION: In the absence of component malpositioning, hip pain, or other compelling reasons to reoperate, a squeaking ceramic bearing is not an indication for revision surgery. The patient can be reassured and observed.
Hopefully, with a better understanding of acoustic phenomena following ceramic total hip arthroplasty, this complication can be minimized.
REFERENCES: Yang CC, Kim RH, Dennis DA: The squeaking hip: A cause for concem-disagrees. Orthopedics
2007;30:739-742.
Walter WL, O’Toole GC, Walter WK, et al: Squeaking in ceramic-on-ceramic hips: The importance of acetabular component orientation. J Arthroplasty 2007;22:496-503.
Figure 80a Figure 80b
QUESTION 27 OF 50
An L3 radiculopathy is best differentiated from a femoral neuropathy by testing what muscle? ](http://www.orthobullets.com/anatomy/10065/adductor-longus)
1
Quadriceps
2
Adductor longus
3
Iliacus
4
Sartorius
5
Psoas
No detailed explanation provided for this question.
QUESTION 28 OF 50
What is the most common cause of persistent pain after excision of a Morton neuroma?
1
Tarsal tunnel syndrome
2
Painful plantar scar formation
3
Metatarsophalangeal joint synovitis
4
Presence of an amputation stump neuroma
5
Inadequate resection of an interdigital neuroma
The most frequent cause of recurrent pain after neuroma excision is tethering of the common digital nerve to the plantar skin by plantar-directed branches of the nerve, possibly preventing retraction of the nerve, due to inadequate resection of the neuroma. These plantar branches were not found to be present 4 cm proximal to the transverse metatarsal ligament. Therefore, an effort should be made to cut the nerve at this level.
QUESTION 29 OF 50
of 100
A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?
1
Medical management with intravenous (IV) antibiotics and observation
2
CT-guided aspiration of the abscess before initiating antibiotics
3
Surgical decompression and IV antibiotics
4
Blood cultures and re-evaluation in 24 hours
Epidural abscess is a serious and potentially disastrous condition. Although medical management is effective in some situations, surgical decompression is considered urgent with the presence of a neurological deficit. Medical management can be considered in the case of a neurologically intact patient, particularly when the microorganism has been identified. If medical management is chosen, careful observation and serial examination for neurologic deterioration is required. Surgical decompression is indicated if a patient's neurologic status worsens or if medical management failure is noted. Additionally, diabetes, a CRP level higher than 115 mg/L, WBC higher than 12500/µL , and bacteremia have proven predictive of medical treatment failure. This patient would be a better candidate for urgent surgical decompression and subsequent IV antibiotics than for medical management.
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683/. ](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
CLINICAL SITUATION FOR QUESTIONS 96 AND 97
Figures 96a and 96b are the CT scans of a 32-year-old man who was thrown from his motorcycle. He has humeral shaft and femoral shaft fractures. A secondary survey reveals substantial tenderness to his lower thoracic spine. He is awake and alert and his movement is limited by pain secondary to the extremity fractures. He is otherwise neurologically intact.
A B
QUESTION 30 OF 50
In the upright standing position, approximately what percent of the vertical load is borne by the lumbar spine facet joints?
1
0%
2
20%
3
40%
4
60%
5
80%
DISCUSSION: Direct measurement and finite element modeling results show that
approximately 20% of the vertical load is borne by the posterior structures of the lumbar
spine in the upright position.
Scientific References
: Adams MA, Hutton WC: The effect of posture on the role of the apophyseal joints in resisting intervertebral compressive forces. J Bone Joint Surg Br 1980;62:358-362.
Goel VK, Kong W, Han JS, Weinstein JN, Gilbertson LG: A combined finite element and optimization investigation of lumbar spine mechanics with and without muscles. Spine 1993;18:1531-1541.
QUESTION 31 OF 50
A young gymnast fell awkwardly onto an outstretched hand during a competition. At the time of impact, his forearm was positioned in supination. Axial and posterolateral forces were loaded along the forearm into the elbow and the elbow underwent a significant valgus thrust. What injury pattern is most likely to result from the combination of these forces at the elbow?
1
Extension-type supracondylar fracture
2
Flexion-type supracondylar fracture
3
Anterior olecranon fracture dislocation
4
Coronoid fracture, olecranon fracture and elbow dislocation
5
Coronoid fracture, radial head fracture and elbow dislocation
The combination of valgus, axial, and posterolateral rotatory forces (forearm supination) can result in a "terrible triad" injury of the elbow.
The key features of a terrible triad injury include a radial head fracture, coronoid fracture, and dislocation of the elbow. Disruption of the lateral collateral ligament complex often concomitantly occurs. While restoration of the bony anatomy is important for static stability, the key primary stabilizer that needs to be addressed is the lateral collateral ligament complex. In acute
injuries LCL repair may be possible. In chronic injury, LCL reconstruction would need to be considered.
O'Driscoll et al. 1991, examined 5 patients with recurrent posterolateral rotatory instability of the elbow. They showed that by applying supination of the forearm with a valgus moment and an axial compression force to the elbow while it is flexed from full extension, this can demonstrate posterolateral rotatory instability of the elbow. The elbow is reduced in full extension and must be subluxated as it is flexed in order to obtain a positive test result (a sudden reduction of the subluxation).
O'Driscoll et al. 1992 looked at a cadaveric study of the elbow. They showed that external rotation and valgus moments with axial forces resulted in posterior dislocations in 12 of the 13 specimens when the anterior medial collateral ligament (AMCL) remained intact. Clinically, it valgus stability in pronation is demonstrated, the AMCL can be assumed to be intact.
Illustration A and B shows radiographs of a terrible triad injury. There is posterolateral dislocation of the elbow with associated radial head fracture, coronoid fracture.
Incorrect Answers:
Answer A: Extension-type supracondylar fractures typically occur with FOOSH injuries with posteriorly directed forces.
Answer B: Flexion-type supracondylar fractures typically occur with the elbow in flexion with an anterior directed force.
Answer C: Anterior olecranon fracture dislocation typically occurs with a direct high-energy blow that is applied to the posterior aspect of the forearm with the elbow in 90° flexion.
Answer D: Coronoid fracture, olecranon fracture and lateral collateral ligament injury typically occur with the arm positioned in supination, axial and VARUS moment forces.
QUESTION 32 OF 50
A 21-year-old football player reports increasing pain and a deformity involving his chest after colliding with another player during a scrimmage. Imaging studies confirm an anterior sternoclavicular dislocation. Management should consist of
1
reconstruction of the sternoclavicular capsule.
2
symptomatic nonsurgical treatment.
3
medial clavicle excision.
4
medial clavicle excision with capsular imbrication.
5
medial clavicle excision and rhomboid ligament reconstruction.
For the patient with an anterior sternoclavicular dislocation, the most appropriate initial treatment should be symptomatic. Surgical options are usually contraindicated because the incidence of intraoperative and postoperative complications is high. A deformity from an anterior sternoclavicular dislocation is usually well tolerated. Return to play is allowed when symptoms resolve.
REFERENCES: Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 477-525.
Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
QUESTION 33 OF 50
A patient with stress fracture has a transcortical area of intense uptake on the technetium bone scan. Which of the following findings would most likely be present on the magnetic resonance imaging (MRI) scan:
1
Normal periosteal signal; normal marrow signal on T1; high marrow signal on T2
2
Normal periosteal signal; low marrow signal on T1; high marrow signal on T2
3
Normal periosteal signal on T2; low marrow signal on T1; high marrow signal on T2
4
High periosteal signal on T2; low marrow signal on T1; high marrow signal on T2
5
High periosteal signal on T2; low marrow signal on T1; normal marrow signal on T2
In 1995, Fredrickson and colleagues classified stress fractures into four grades based upon bone scans:
Grade 1     Small ill-defined cortical area of mildly increased activity Grade 2     Well-defined cortical area of moderately increased cortical                     activity
Grade 3Â Â Â Â Â Wide, cortical-medullary area of increased activity
Grade 4Â Â Â Â Â Transcortical area of intensely increased activity
In a grade 4 stress fracture, the corresponding MRI will show: High periosteal signal on T2-weighted images
Low signal on T1-weighted images, often with a liner low signal line representing the fracture line
High signal on T2-weighted images, often with a liner low signal line representing the fracture line
C orrect Answer: High periosteal signal on T2; low marrow signal on T1; high marrow signal on T2
QUESTION 34 OF 50
of 100
Figure 29 is the radiograph of a 12-year-old female gymnast with elbow pain.
1
Plain radiographs
2
CT scan
3
MRI
4
Arthrogram
- MRI
QUESTION 35 OF 50
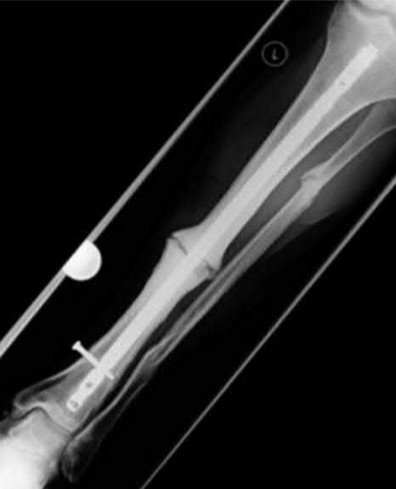
A 25-year-old male presents with the injury seen in Figures A and B following a motorcycle collision. He has an ipsilateral open tibia fracture. No other injuries are noted. He is hemodynamically stable and cleared for operative intervention. What would be the most appropriate definitive treatment for this injury?
1
Reamed unlocked antegrade nailing
2
Unreamed antegrade nailing with dynamic interlocking
3
Reamed unlocked retrograde nailing
4
Reamed retrograde nailing with static interlocking
5
Reamed retrograde nailing with dynamic interlocking
Reamed, statically locked nailing is the standard treatment for diaphyseal femur fractures. In this patient with an ipsilateral lower extremity fracture, retrograde nailing allows for supine positioning to address both injuries.
Antegrade, reamed, statically locked intramedullary nailing is the treatment of choice for the majority of diaphyseal femur fractures. Relative indications for retrograde nailing include multi-injured patients, ipsilateral lower extremity trauma, morbid obesity, and infra-isthmal fracture patterns.
Brumback and Virkus review the current concepts and controversies regarding the management of femoral shaft fractures with reamed and unreamed nailing. The authors highlight the benefits of reaming including deposition of local autograft, stimulation of periosteal blood supply and increased nail diameter.
They note that there is a subset of trauma patients, specifically those with pulmonary injury, that may be adversely affected by nailing.
Figures A and B demonstrate AP and Lateral views of a comminuted mid-diaphyseal femoral shaft fracture. Illustrations A and B demonstrate the same fracture that progressed to uneventful union after treatment with a reamed, statically locked retrograde nail supplemented with blocking screws to correct angular alignment.
Incorrect answers:
Answers 1 and 3: Unlocked nailing is rarely indicated and is mainly of historical significance
Answer 2: Antegrade nailing would not necessarily allow for the tibia fracture to be addressed simultaneously. Dynamic interlocking is contra-indicated in this length unstable fracture pattern
Answer 5: Dyamic interlocking is not typically used for femoral shaft fractures. It would be contra-indicated in this length unstable femur fracture.
QUESTION 36 OF 50
of 100
A 12-year-old boy is diagnosed with osteomyelitis and subperiosteal abscess of the distal tibia demonstrated on the MRI. CRP is 13 mg/l. He is taken to the operating room (OR) for incision and drainage. Intraoperative cultures as well as blood cultures grow methicillin-resistant Staphylococcus aureus (MRSA). On postoperative day 2, he develops swelling in the leg, as well as an increased oxygen requirement. What should be the next step in evaluation?
1
Repeat MRI of the leg
2
CT scan of chest
3
Radiograph of chest
4
Return to the OR for repeat incision and drainage
■ This child has a MRSA osteomyelitis. Many recent studies have shown that these infections are more difficult to treat and are associated with severe complications and longer hospitalizations. They may also require an increased number of surgical procedures to get control of the infection source. Deep venous thrombosis (DVT) and pulmonary embolism, as well as septic emboli to the lungs occur more commonly with MRSA infections. Increased swelling of the leg may be related to the onset of a DVT and venous ultrasonography is an easy and quick study to help determine if a DVT is present. Currently, the patient has an increased oxygen requirement. Helical CT scan is the next best test to evaluate for septic pulmonary emboli. Plain radiograph of the chest is helpful to look for areas of pneumonia but not diagnostic for septic emboli. Repeat MRI of the leg will be abnormal because of the recent surgical procedure and most likely will not add anything diagnostically. Given his clinical improvement and decreasing CRP, a repeat return to the OR is not indicated at this time, although it is not uncommon for children with MRSA infections to require more than one surgical procedure.
QUESTION 37 OF 50
A 32-year-old previously healthy male sustained a closed right tibial shaft fracture 15 months prior that was treated with an unreamed intramedullary nail. The patient presents with persistent
pain in his right leg with radiographs revealing an "elephant's foot" appearance of the bone at the fracture site with gapping on all four cortices on the AP and lateral radiographs. His medical history is significant for type 1 diabetes for which he uses an insulin pump and denies any related issues. Based on this information, what is the most likely underlying cause of the patient's condition?
1
Chronic low-grade infection at the fracture site
2
Insufficient blood supply at the fracture site
3
Lack of stability at the fracture site
4
Low levels of vitamin D
5
Genetic error of collagen metabolism
The patient is presenting with a hypertrophic nonunion after unreamed intramedullary nailing of a closed tibial shaft fracture. The most likely underlying cause for hypertrophic nonunion is insufficient fracture site stability.
Tibial shaft fractures are the most common long bone fracture to be complicated by nonunion. This risk is increased further in the setting of open injuries which can compromise blood flow to the fracture site and increase the chance of a septic nonunion. Hypertrophic nonunions are typically the result of insufficient mechanical stability with otherwise preserved fracture blood supply and healing biology. Radiographs characteristically demonstrate abundant callus formation with lack of cortical union on both AP and lateral radiographs. Surgical treatment involves reamed exchange nailing or adjunctive plate fixation.
Marsh performed a biomechanical and radiographic evaluation of 43 closed tibial shaft fractures managed conservatively. The authors performed serial radiographs and measurements of bending stiffness. They defined three different healing groups in the study, of which, delayed union considered the failure to reach 7 N-m/degree stiffness at 20 weeks from injury, and found that the presence of new periosteal bone formation at 10 weeks was a predictor of prolonged healing. The authors discussed periosteal bone formation as a criterion for the definition of delayed union and lack of periosteal and endosteal healing responses as a definition for nonunion.
Hak reviewed the management of aseptic tibial nonunions. The author discussed that exchange tibial nailing and adjunctive plate fixation both demonstrated high union rates for hypertrophic nonunions. The author cited that the benefit of exchange nailing derived from less soft tissue disruption, increased fracture stability from a larger and stiffer nail, and stimulation of
periosteal blood flow. Alternatively, adjunctive plate fixation permitted retention of the original nail while enabling debridement and direct bone grafting of the nonunion site. The author concluded that treatment should be tailored on a case-by-case basis, as there are now various supported surgical and non-surgical treatment options for aseptic tibial nonunions.
Illustrations A and B are the AP and lateral radiographs of a tibial shaft fracture treated with an intramedullary nail with evidence of hypertrophic nonunion.
Incorrect answers:
Answer 1: The patient has a hypertrophic nonunion, which is associated with optimal healing biology but a lack of stability. There is no evidence of a septic nonunion, which is more often associated with an oligotrophic or atrophic nonunion.
Answer 2: Insufficient blood supply at the fracture site would be associated with an atrophic nonunion.
Answer 4: Insufficient vitamin D levels would most likely result in an atrophic or oligotrophic nonunion.
Answer 5: Osteogenesis imperfecta is a genetic defect of collagen that can result in hypertrophic callus formation following fractures. However, this patient does not have a medical history consistent with this diagnosis.
QUESTION 38 OF 50
of 100
A 45-year-old woman has a painless thigh mass that is larger than 5 cm. What is the best next step?
1
Percutaneous biopsy
2
Positron emission tomography (PET)/CT scan
3
Excisional biopsy
4
MRI of the thigh with gadolinium
Masses exceeding 5 cm in size and any deep mass should be evaluated with MRI prior to biopsy or excision to ensure the most viable tissue is sampled and to minimize morbidity and complications from an improperly placed biopsy site. Examinations are unreliable when attempting to determine if a mass is a simple lipoma, and any large or deep mass should be considered a sarcoma until proven otherwise. PET/CT is a staging examination to evaluate for metastatic or multifocal disease. These are expensive tests that should not be ordered prior to MR imaging of the primary lesion. For patients that are unable to obtain an MRI, CT of the mass is the preferred imaging modality.
RECOMMENDED READINGS
11. [Gilbert NF, Cannon CP, Lin PP, Lewis VO. Soft-tissue sarcoma. J Am Acad Orthop Surg. 2009 Jan;17(1):40-7. Review. PubMed PMID: 19136426.](http://www.ncbi.nlm.nih.gov/pubmed/19136426)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19136426)
12. [Damron TA, Beauchamp CP, Rougraff BT, Ward WG Sr. Soft-tissue lumps and bumps. Instr Course Lect. 2004;53:625-37. Review. PubMed PMID: 15116652.](http://www.ncbi.nlm.nih.gov/pubmed/15116652)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15116652)
13. Simon MA. Diagnostic Strategies. In: Simon MA, Springfield D, eds. _Surgery for Bone and Soft Tissue Tumors_. Philadelphia, PA: Lippincott-Raven; 1998:21-30.
CLINICAL SITUATION FOR QUESTIONS 9 THROUGH 11
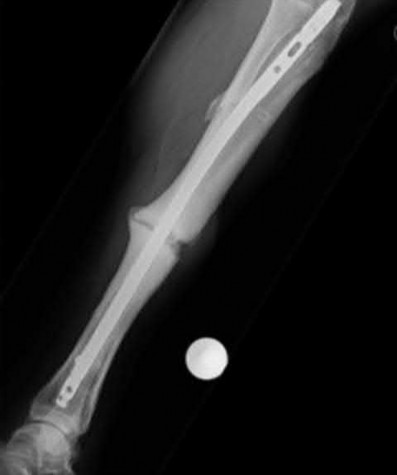
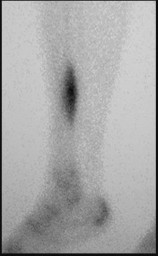
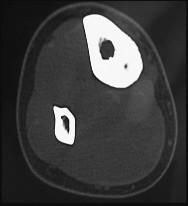
Figures 9a through 9d are the anteroposterior and lateral radiographs, CT scan, and technetium bone scan of a 12-year-old boy who has experienced 7 months of pain in his lower leg. The pain limits his ability to participate in sports and he is having difficulty sleeping. He is afebrile, and laboratory study findings including an erythrocyte sedimentation rate, C-reactive protein, and complete blood count are within normal limits.
QUESTION 39 OF 50
A 30-year-old man who participates in recreational sports reports the spontaneous onset of intermittent pain and swelling about the right knee. Examination reveals a 3+ effusion, with a range of motion of 10° to 60°. He has mild diffuse tenderness but no instability. MRI scans and an arthroscopic view are shown in Figures 39a through 39c. Management should consist of
1
arthroscopic debridement of the articular lesion and resurfacing.
2
knee aspiration and an intra-articular cortisone injection.
3
rheumatologic evaluation.
4
infectious disease evaluation for possible Lyme disease.
5
arthroscopic synovectomy.
The patient has synovial chondromatosis. The MRI scans show multiple small proscribed areas of signal intensity in the gutters and suprapatellar pouch, suggesting very small loose bodies. The arthroscopic view shows the classic appearance of multiple small chondral loose bodies. Synovial chondromatosis is a condition in which the synovium undergoes metaplasia, producing multiple chondral loose bodies that can subsequently ossify. The treatment of choice, removal of the loose bodies and arthroscopic synovectomy, results in a lower incidence of recurrence than other treatment methods.
REFERENCES: Coolican MR, Dandy DJ: Arthroscopic management of synovial chondromatosis of the knee: findings and results in 18 cases. J Bone Joint Surg Br
1989;71:498-500.
Ogilvie-Harris DJ, Saleh K: Generalized synovial chondromatosis of the knee: A comparison
of removal of the loose bodies alone with arthroscopic synovectomy. Arthroscopy
1994;10:166-170.
QUESTION 40 OF 50
A 57-year-old man has had a 2-week history of neck pain. He has no history of radiating symptoms, and has no complaints of numbness or paresthesias. There was no trauma associated with the onset of the pain. Figure 26 shows the MRI scan initially obtained by his family physician. What should the patient be told regarding the prevalence of the MRI findings in his age group?
1
Less than 10%
2
20% to 25%
3
50% to 60%
4
75% to 80%
5
Greater than 95%
The MRI findings reveal age-related degenerative changes in the cervical spine, which is a very common finding in the adult population. Boden and associates evaluated cervical spine MRI findings on 63 asymptomatic subjects, and found that the prevalence of having at least one degenerative disk was approximately 57% in those older than age 40 years.
QUESTION 41 OF 50
What nerve is at greatest risk of harm from the portal shown in Figure 36?
1
Radial
2
Ulnar
3
Median
4
Lateral antebrachial cutaneous
5
Posterior antebrachial cutaneous
The figure shows the anterolateral portal for elbow arthroscopy, and injury to the radial nerve has been reported in conjunction with this portal site. Studies have shown that closer proximity to the radial nerve is associated with more distal portal sites. The lateral and posterior antebrachial cutaneous nerves are both at less risk of injury. The ulnar and median nerves are both fairly remote to this location.
REFERENCES: Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Papilion JD, Neff RS, Shall LM: Compression neuropathy of the radial nerve as a complication of elbow arthroscopy: A case report and review of the literature. Arthroscopy 1988;4:284-286.
Poehling GG, Whipple TL, Sisco L, Goldman B: Elbow arthroscopy: A new technique. Arthroscopy 1989;5:222-224.
QUESTION 42 OF 50
Which finger is most commonly involved in a flexor digitorum profundus (FDP) avulsion injury:
1
Index
2
Middle
3
Ring
4
Small
5
Thumb
An FDP avulsion is caused by forceful extension of the distal interphalangeal (DIP) joint, occurring at the same time as a maximum contraction of the FDP tendon. Jersey finger is often seen in athletes, especially football or rugby players, who commonly get their fingers caught in an opposing playerâs jersey, thus the name. In most cases, this injury affects the ring finger.
QUESTION 43 OF 50
of 100
The patient is treated with emergent open reduction and internal fixation via a lateral approach to the distal femur. The peroneal nerve is found intact but is under pressure by a proximal bone fragment. After fixation, there is near-anatomic fracture reduction and no tension on the nerve. The patient is comfortable at a postsurgical check 4 hours later. Her toes
are warm and pink and there is no pain with passive dorsiflexion/plantar flexion of the toes. However, she continues to have absent first web space sensation, diminished dorsal foot sensation, and absent toe/ankle dorsiflexion. What is the best next step?
1
Return to surgery emergently for 4-compartment fasciotomy because she has a compartment syndrome and the nerve will not otherwise recover
2
Return to surgery urgently within the next few days for nerve exploration and potential microsurgical repair (vs cable grafting) to the damaged nerve to speed repair
3
Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 3 months after surgery
4
Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 12 months after surgery
- Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 3 months after surgery
QUESTION 44 OF 50
..What is the most appropriate treatment if instability is present at the time of evaluation?
1
TEA
2
Distal humeral replacement arthroplasty
3
Arthroscopic release with debridement
4
Soft-tissue interposition arthroplasty
DISCUSSION..The radiographs reveal ulnohumeral arthrosis with relative sparing of the radiocapitellar articulation secondary to underlying osteoarthritis. Arthrosis of the elbow joint in this
young and active patient presents a treatment dilemma for the surgeon. Interposition arthroplasty allows for improved function with pain relief and no weight-lifting restrictions, as required with TEA. This option is an intermediate procedure that preserves bone stock and allows for conversion to a TEA if necessary. Conventional TEA would provide pain relief with improved range of motion, but activity limitation and lifetime weight restrictions make this an undesirable option. Arthroscopic debridement is not an option, considering the previous failure from this modality. Contraindications for soft-tissue interposition arthroplasty include elbow instability, active infection, and pain without motion loss. Common complications associated with this procedure include instability, infection, ulnar neuropathy, bone resorption, and heterotopic bone formation.
Botulinum toxin is used to treat vasospastic disorders of the hand such as the Raynaud phenomenon to improve digital perfusion and reduce pain. Botulinum toxin enables which transmitter to be unopposed, resulting in vasodilation?
1
Substance P
2
Glutamate
3
Rho kinase
4
Nitric oxide
Nitric oxide is the only transmitter listed that is not inhibited by botulinum toxin. Substance P and glutamate are inhibited by botulinum toxin from release by pain nociceptors, thus reducing pain. Fonseca and associates have postulated that botulinum toxin inhibits the RhoA kinase pathway by blocking reactive oxygen species, which in turn does not allow actin/myosin to activate, thus preventing vasoconstriction of smooth muscle. Blocking the RhoA kinase pathway allows the action of nitric oxide to be unopposed, causing vasodilation. Nitric oxide is a potent vasodilator. Thus, botulinum toxin _promotes nitric oxide activity to increase vasodilation._
QUESTION 46 OF 50
What is the most common presenting problem in patients with cauda equina syndrome?
1
Urinary retention
2
Urinary incontinence
3
Saddle numbness
4
Lower extremity numbness and weakness
5
Back and leg pain
In one recent retrospective cohort study of 42 patients with cauda equina syndrome, 83% had low back pain at presentation, 90% had radicular lower extremity pain, 60% had urinary retention, and 55% had urinary incontinence. Objective findings at presentation included 55% with leg weakness, 62% with sensory deficit, 62% with absent ankle jerk reflexes, 76% with perianal sensory deficit, and 50% with decreased rectal tone.
QUESTION 47 OF 50
of 100
While performing long fusion with osteotomies for a patient with adult scoliosis and sagittal plane deformity, the neurophysiologist reports a change in motor-evoked potentials in the lower extremities. What is the most appropriate next step?
1
Perform an immediate wake-up test
2
Continue with the surgery and reassess in 5 minutes
3
Administer intravenous methylprednisolone
4
Ensure that mean arterial blood pressure is 80 or higher
The use of intraoperative neuromonitoring is expanding, especially in the setting of deformity surgery. Changes in monitoring are concerning for the possibility of a neurologic injury; however, several other factors can alter signals. These include hypotension, changes in anesthesia depth and medications, the use of paralytic agents, and technical issues such as leads falling out or becoming disconnected. If a change in neuromonitoring signals is noted, these factors should be checked first to rule out false-positive findings. If this does not correct the problem, the wound should be explored to ensure there is no compression on the neural elements. Finally, if the deformity has been corrected, some of the correction can be released in an attempt to improve the signals. A wake-up test is difficult to perform and does not provide specific information regarding the location of the problem or how to correct it. Steroids may be used depending on surgeon preference, but should not be used until neurologic injury is ruled out. Any neuromonitoring changes always necessitate immediate investigation.
RECOMMENDED READINGS
[Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. ](http://www.ncbi.nlm.nih.gov/pubmed/23116091)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23116091)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116091)
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
[Review. PubMed PMID: 21102290. ](http://www.ncbi.nlm.nih.gov/pubmed/21102290)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21102290)
QUESTION 48 OF 50
**An otherwise healthy 25-year-old man underwent a right**
anterior cruciate ligament reconstruction with a bone-patellar tendon- bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-negative Staphylococcus 5 days postoperatively. The patient has exhibited no evidence of clinical infection and his postoperative course has been uncomplicated during this time. What is the ideal management of this patient?
1
Observation
2
Oral antibiotics for 6 weeks
3
IV antibiotics for 6 weeks
4
Arthroscopic irrigation and debridement with graft retention
5
Arthroscopic irrigation and debridement with graft removal
#
**
The incidence of preimplantation positive cultures of musculoskeletal allografts used for anterior cruciate ligament reconstruction has varied between 4.8% and 13.3%.
Interestingly, in none of the studies evaluating this issue did any of the patients implanted with a "contaminated" graft develop a clinical infection. The results of the current literature suggest that the treatment of
low-virulence organisms is unnecessary if no evidence of clinical infection exists. Preimplantation cultures do not appear to correlate with clinical infection. Therefore, the routine culture of allograft tissue is not recommended.
QUESTION 49 OF 50
Which of the following is not associated with increased risk of stress fractures:
1
Eating disorder
2
Hyperthyroidism
3
Prolonged corticosteroid use
4
Hypothyroidism
5
CeliaCsprue
Any history of frequent or prolonged corticosteroid use, hyperparathyroidism, rheumatoid arthritis, hyperthyroidism, celiaCsprue, previous stress fractures or overuse injuries as well as signs or symptoms of an eating disorder also should draw oneâs attention to the possibility of a reduced bone mass
QUESTION 50 OF 50
A healthy 25-year-old man sustains a grade IIIB open tibial fracture. Following appropriate debridement, irrigation, and stabilization with an external fixator, the soft-tissue injury is shown in Figure 30. What is the most appropriate definitive soft-tissue coverage procedure?
1
Split-thickness skin graft
2
Full-thickness skin graft
3
Soleus rotation flap
4
Medial gastrocnemius rotation flap
5
Free latissimus dorsi flap with microvascular anastomosis
This is a very large near circumferential defect with posterior as well as anterior skin and muscle injury. Bone is exposed. The posterior muscles cannot be rotated since they are part of the zone of injury. The bone and other poorly vascularized areas of this wound would not accept a skin graft. The best chance for limb salvage will be to obtain soft-tissue coverage with a free tissue transfer using the latissimus dorsi.
REFERENCES: Mathes SJ, Nahai F: Vascular anatomy of muscle: Classification and applications, in Mathes SJ, Nahai F (eds): Clinical Application for Muscle and Musculocutaneous Flaps. St Louis, MO, CV Mosby, 1982, p 20.
Bos GD, Buehler MJ: Lower-extremity local flaps. J Am Acad Orthop Surg 1994;2:342-351.