This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set B658AF)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
A 30-year-old female involved in a severe motor-vehicle collision that requires prolonged extrication. She arrives at a referral trauma center almost 10 hours after her initial injury. She receives tetanus and intravenous antibiotics upon arrival. The patient has an open tibial fracture with significant periosteal stripping and a closed head injury that requires intracranial pressure monitoring. She is cleared for operative intervention by the neurosurgery and trauma surgery services the following morning. She undergoes a thorough debridement, placement of an antibiotic bead pouch, and external fixator placement approximately 18 hours after her injury. She is definitively treated 4 days after her injury with a repeat debridement, gracilis flap and intramedullary nail. Which of the following factors places the patient at increased risk of infection?
1
Free tissue transfer instead of rotational flap
2
Flap coverage at four days after injury
3
Use of an intramedullary nail instead of minimally invasive plating
4
Delay in administration of IV antibiotics
5
Debridement at 15 hours after injury
Intravenous antibiotics are critical to prevent infection in open fractures. Delay in administration of intravenous antibiotics has been linked with increased risk of infection.
Open tibia fractures are associated with high rates of infection. Historically,
early debridement (within 6-8 hours) and early flap coverage (typically defined as less than 72 hours) were thought to minimize the risk of infection. Recent evidence has challenged these findings, with multiple studies demonstrating no significant link between the timing of debridement and rates of infection.
Multiple studies from the Lower Extremity Assessment Project (LEAP) found no significant difference in infection or complication with flap coverage more than 72 hours after injury.
Bhattacharyya et al retrospectively evaluated patients with type IIIB tibial fractures treated with extended use of negative pressure wound therapy. The authors found increased rates of infection beyond 7 days despite the use of negative pressure wound therapy.
Lack et al evaluated the timing of antibiotic administration on infection rates for type III tibial fractures. The authors found increased rates of infection with administration of antibiotics beyond 66 minutes. The authors discuss the possibility of pre-hospital intervention as many severely injured patients have delayed arrival at treatment centers.
Pollak et al prospectively analyzed rates of complication with flap coverage as part of the LEAP study. The authors found no increase in complications with flap coverage beyond 72 hours. The only significant risk for complication was the use of rotational flaps in comminuted or segmental (AO/OTA type C) tibial fractures.
Incorrect answers:
Answer 1: Lower rates of complication, including infection, were seen with free flaps in AO/OTA type C fractures in the study by Pollak et al.
Answer 2: Timing of flap coverage is controversial. Early studies demonstrated increased infection with delay beyond 72 hours, however recent studies using more rigorous statistical analysis do not support these findings.
Answer 3: No study has demonstrated lower infection rates with the use of plating versus nailing in open tibial fractures.
Answer 5: The timing of debridement with open fractures has been shown not to effect the rate of infection in multiple recent studies.
QUESTION 2 OF 50
A 71-year-old woman with coronary artery disease underwent an uncomplicated right total hip arthroplasty for osteoarthritis 12 years ago. Her hip has functioned well until approximately 18 months ago when she noted the spontaneous onset of groin, buttock, and proximal thigh pain that is present at rest and made worse with activity. A radiograph is shown in Figure 15. What is the recommended management at this point?
1
Immediate admission to the hospital and emergent revision hip arthroplasty
2
Reassurance and follow-up if symptoms worsen
3
Repeat radiographs in 1 month
4
Protected weight bearing with urgent revision hip arthroplasty when the patient is medically cleared
5
A prescription for alendronate and reevaluation in 1 year
DISCUSSION: The radiograph shows significant osteolysis with loosening of the femoral component. The patient is symptomatic and surgery is indicated because of the extent of osteolysis and the loose femoral component.
Reassurance and follow-up if symptoms worsen places the patient at risk for further bone loss and periprosthetic fracture. Emergent surgery is not required because the symptoms have been present for more than a year; however, urgent revision hip arthroplasty is recommended when the patient is medically cleared. While there is data to suggest that bisphosphonates may slow the progression of osteolysis in animal modes, there is no clear evidence that bisphosphonate treatment prevents the progression of osteolysis in humans. Additionally, this patient has a loose symptomatic femoral component.
REFERENCES: Chiang PP, Burke DW, Freiberg AA, et al: Osteolysis of the pelvis: Evaluation and treatment. Clin Orthop Relat Res 2003;417:164-174.
Dunbar MJ, Blackley HR, Bourne RB: Osteolysis of the femur: Principles of management. Instr Course Lect 2001;50:197-209.
Rubash HE, Dorr LD, Jacobs JJ, et al: Does alendronate inhibit the progression of periprosthetic osteolysis? Trans
Orthop Res Soc 2004;29:1888.
)
Figure 16a Figure 16b
QUESTION 3 OF 50
of 100
Figures 13a through 13c
1
T-type fracture
2
Anterior column fracture
3
Anterior wall fracture
4
Posterior wall fracture
5
Posterior column and posterior wall fracture
- Posterior wall fracture_
QUESTION 4 OF 50
of 100 38A B
Three months later this patient has continued swelling and giving-way episodes. Figures 38a and 38b are his stress radiographs. This study indicates laxity in which ligament?
1
Anterior talofibular
2
Calcaneal fibular
3
Posterior talofibular
4
Lateral talocalcaneal
- Anterior talofibular
QUESTION 5 OF 50
of 100
What is the advantage of percutaneous pedicle screw fixation over open instrumentation and fusion for a thoracolumbar burst fracture without neurologic deficit?
1
Better clinical outcomes
2
Less blood loss
3
Less pseudarthrosis risk
4
Lower revision surgery rate
A prospective randomized study on short-segment treatment of burst fractures with and without fusion demonstrated similar outcomes at 5 years with lower blood loss in the nonfusion group. There is by definition no fusion performed with percutaneous stabilization, so patients often develop hardware failure. Some surgeons routinely remove instrumentation following percutaneous stabilization, thus revision surgery is common. Clinical outcomes are not improved compared to open methods.
RECOMMENDED READINGS
[Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. Review. PubMed PMID: 24981899. ](http://www.ncbi.nlm.nih.gov/pubmed/24981899)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24981899) [Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomised trial. J Bone Joint Surg Br. 2012 Aug;94(8):1101-6. doi: 10.1302/0301-620X.94B8.28311. PubMed PMID: 22844053. ](http://www.ncbi.nlm.nih.gov/pubmed/22844053)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/22844053)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22844053)
Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone
Joint Surg Am. 2009 May;91(5):1033-41. doi: 10.2106/JBJS.H.00510. PubMed PMID:
[19411450/. ](http://www.ncbi.nlm.nih.gov/pubmed/19411450)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19411450)
RESPONSES FOR QUESTIONS 48 THROUGH 50
1. Fracture displacement or subluxation leading to neurologic injury
2. Symptomatic epidural hematoma
3. Sepsis and death
4. Permanent nerve root injury and neurologic deficit
5. Loss of bowel or bladder control
6. Spinal cord injury
Select the complication listed above that most commonly is associated with the appropriate clinical scenario described below.
QUESTION 6 OF 50
A patient with a transverse femur fracture undergoes statically locked antegrade intramedullary nailing. Postoperatively, the patient appears to have a rotational deformity of greater than 25 degrees. The surgeon informs the patient, who chooses to undergo corrective treatment with removal of distal interlocking screws, rotational correction, and relocking of the screws. The patient goes on to heal
but has persistent hip pain and a limp that does not improve completely after extensive rehabilitation. There is complete healing, no evidence of infection, no hardware issues, no ectopic bone, and rotational studies indicate less than 2 degrees of malrotation. Functional capacity testing reveals the affected abductor and quadriceps function to be about 85% of the uninjured side and the patient returns to work and most of his recreational activities except rock climbing. Two days before the statute of limitations, the patient
files a malpractice suit alleging negligence of surgery, loss of function, consortium, and pain and suffering due to the surgeon's efforts. What action should the surgeon and the defense team take?
1
Settle the case because the surgeon made an error that resulted in unnecessary surgery, and thus the case is indefensible.
2
Settle the case because they are likely to lose the case, and it would be cheaper to settle than to defend.
3
Defend the case alleging that there was no error, and no damages, and that the patient is malingering.
4
Defend the case because despite there being an error, the error was corrected and there were little or no damages compared with expected outcomes.
5
Contact the patient directly to discuss why he is suing and attempt an amicable resolution.
#
**
To establish negligence, certain criteria must be met. 1) A duty was owed by the surgeon (in this case, yes, a relationship was established). 2) The duty was breached, where the provider failed to meet the standard of care (there
was a technical error, but it was corrected). 3) The breach caused an injury. In this case, the patient had an outcome that was very acceptable, as
documented with outcome studies, for femur fractures. Also, the rotational error and locking distally would have had little impact on the hip, whereas antegrade nailing itself is expected to result in some objective impairment of the hip in some patients. 4) Damages were incurred as a result. In this case, the patient returned to work and could not rock climb which could be reasonably expected with a femur fracture in some patients, and cannot be causally linked to the corrective surgery. For all practical purposes, the patient had a very acceptable outcome. Thus, settling the case for an error would be rather permissive and the important issue is that the surgeon recognized the problem, addressed it, and fulfilled his or her postoperative responsibility. The case is very defendable, and thus it is unlikely to be lost. Defending the case and alleging no error is incorrect because there was an error. The surgeon should never function outside of his or her legal counsel once a suit is filed.
QUESTION 7 OF 50
Which of the following is the atypical mycobacterium that infects a penetrating wound sustained in an aquatic environment:
1
Mycobacterium avium
2
Mycobacterium marinum
3
Mycobacterium aquaticum
4
Mycobacterium tuberculosis hominis
5
Mycobacterium chelorei
Tuberculosis is the most common chronic infection found in the hand. Mycobacterium marinum is the atypical mycobacterium that can infect a wound sustained in a marine environment, freshwater lake, or tropical fish tanks. It is also called swimming pool granuloma or fish tank granuloma.
QUESTION 8 OF 50
of 100
The success of proximal interphalangeal (PIP) joint arthroplasty for arthritis at the index finger PIP joint is dependent upon
1
ulnar collateral ligament stability.
2
radial collateral ligament stability.
3
use of a nonconstrained prosthesis.
4
use of a dorsal surgical approach.
PIP joint arthroplasty is a surgical treatment option for patients with PIP joint arthritis. However, this procedure is dependent upon radial collateral ligament stability, even when a 1-piece silicone implant is used. A key pinch or pinching the thumb tip to the radial aspect of the index finger middle phalanx places tremendous load on the radial collateral ligament of the index PIP joint. Presurgical instability, surgical technique, and surgical dissection are important variables; arthroplasty may threaten the integrity of the ligament. As a result, most surgeons will recommend PIP joint fusion for the index finger, which plays a role in key pinch, and will offer PIP joint arthroplasty for the long and ring fingers, for which there is less thumb-to-side pinching and motion is a priority.
Arthrodesis limits motion but is associated with better reliability over the long term compared to arthroplasty for the PIP joint of the index finger. Infection is no more likely at the index PIP joint than at any other joint. Although a silicone (1-piece) arthroplasty may help in cases of collateral ligament instability, it is not required if the radial collateral ligament can be preserved or satisfactorily reconstructed. Both volar and dorsal approaches for PIP arthroplasty have been described without producing conclusive evidence demonstrating superiority of 1 approach over the other.
RECOMMENDED READINGS
44. Pellegrini VD Jr, Burton RI. Osteoarthritis of the proximal interphalangeal joint of the hand: arthroplasty or fusion? J Hand Surg Am. 1990 Mar;15(2):194-209. PubMed PMID: 2133611.
45. Branam BR, Tuttle HG, Stern PJ, Levin L. Resurfacing arthroplasty versus silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2007 Jul-Aug;32(6):775-88. PubMed PMID: 17606054.
CLINICAL SITUATION FOR QUESTIONS 72 THROUGH 77
Figures 72a through 72b are the radiographs of a 45-year-old man who has severe right wrist pain and paresthesias in the median nerve distribution following a fall from a ladder.
QUESTION 9 OF 50
of 100
The above surgery was performed with recombinant human bone morphogenetic protein-2 (rhBMP-2). She reports immediate relief of her leg pain and is discharged home on postoperative day 2. The patient reports new-onset radicular pain and weakness in her leg 1 year later. Figures 22a and 22b are her postoperative CT myelogram images. What is the most likely cause of her pain? 22A B
1
Excessive retraction of the traversing nerve root
2
Bony overgrowth from the use of BMP protein in the disk space
3
Osteomyelitis with compression of the nerve roots
4
Inadequate decompression after surgery
Transient thigh pain after lateral, transpsoas interbody fusion is common and generally lasts for less than 3 months. Transpsoas interbody fusion with slip reduction can result in indirect spinal decompression and often obviates the need for a laminectomy for most patients. Complications with this approach are comparable to those experienced with open surgery, but the hospital stay is generally shorter.
Use of BMP in interbody devices has also become common. The images above show heterotopic bone growth into the spinal canal causing nerve compression. This complication is more commonly encountered after posterior lumbar interbody fusions.
RECOMMENDED READINGS
Oliveira L, Marchi L, Coutinho E, Pimenta L. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements.
[Spine (Phila Pa 1976). 2010 Dec 15;35(26 Suppl):S331-7. doi: 10.1097/BRS.0b013e3182022db0. PubMed PMID: 21160397. ](http://www.ncbi.nlm.nih.gov/pubmed/21160397)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21160397) Cummock MD, Vanni S, Levi AD, Yu Y, Wang MY. An analysis of postoperative thigh symptoms after minimally invasive transpsoas lumbar interbody fusion. J Neurosurg Spine. 2011 Jul;15(1):11-8. doi: 10.3171/2011.2.SPINE10374. Epub 2011 Apr 8. PubMed PMID:
[21476801.](http://www.ncbi.nlm.nih.gov/pubmed/21476801)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21476801)
[Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011 Jan 1;36(1):26-32. doi: 10.1097/BRS.0b013e3181e1040a. PubMed PMID: 21192221. ](http://www.ncbi.nlm.nih.gov/pubmed/21192221)[View](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Wong DA, Kumar A, Jatana S, Ghiselli G, Wong K. Neurologic impairment from ectopic bone in the lumbar canal: a potential complication of off-label PLIF/TLIF use of bone morphogenetic protein-2 (BMP-2). Spine J. 2008 Nov-Dec;8(6):1011-8. Epub 2007 Nov 26. PubMed PMID: 18037352.](http://www.ncbi.nlm.nih.gov/pubmed/18037352)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18037352)
[Chen NF, Smith ZA, Stiner E, Armin S, Sheikh H, Khoo LT. Symptomatic ectopic bone formation after off-label use of recombinant human bone morphogenetic protein-2 in transforaminal lumbar interbody fusion. J Neurosurg Spine. 2010 Jan;12(1):40-6. doi: 10.3171/2009.4.SPINE0876. PubMed PMID: 20043763.](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)[View ](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)
Rouben D, Casnellie M, Ferguson M. Long-term durability of minimal invasive posterior transforaminal lumbar interbody fusion: a clinical and radiographic follow-up. J Spinal Disord Tech. 2011 Jul;24(5):288-96. doi:10.1097/BSD.0b013e3181f9a60a. PubMed PMID:
[20975594.](http://www.ncbi.nlm.nih.gov/pubmed/20975594)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20975594)
QUESTION 10 OF 50
A collegiate rower reports the sudden onset of right chest pain while rowing. The athlete states that the pain is worse with deep inspiration and coughing. Examination reveals localized tenderness over the posterolateral corner of the eighth rib. What is the most likely diagnosis?
1
Intercostal muscle strain
2
Rib stress fracture
3
Pneumothorax
4
Costochondritis
5
Empyema
A rib stress fracture, the most common injury to the thorax in rowing athletes, generally occurs during periods of intense training with a low stroke rate and heavy loads. It is characterized by the sudden onset of sharp, localized chest pain while rowing. The fifth through the ninth rib is generally affected, and the diagnosis is best established with a bone scan. An intercostal muscle strain generally has an insidious onset and may be poorly localized. Costochondritis affects the anterior costochondral junction. A pneumothorax and an empyema can cause nonlocalized chest pain but are associated with respiratory distress and systemic physical findings.
REFERENCES: Karlson KA: Rib stress fractures in elite rowers. Am J Sports Med 1998;26:516-520.
Holden DL, Jackson DW: Stress fractures of the ribs in female rowers. Am J Sports Med 1985;13:342-348.
QUESTION 11 OF 50
Advantages of plain film radiograph in diagnosis and treatment of femoral acetabular impingement do NOT include:
1
Visualization of cam impingement lesion
2
Detection of labral injury
3
Observation of joint space narrowing
4
Detection of developmental dysplasia of the hip (DDH)
5
Assessment for pincer impingement
Plain film radiographs can successfully detect cam and pincer impingement and cartilage space narrowing, as well as allow quantified measurement of femoral head coverage. A magnetiCresonance arthrogram is necessary, however, to successfully visualize labral pathology.
QUESTION 12 OF 50
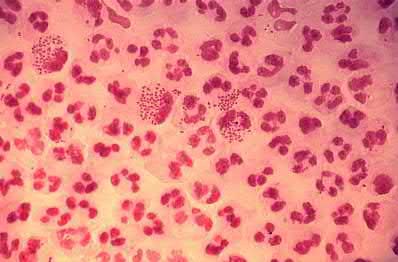
A 26-year-old female presents to the emergency department with right knee pain, swelling, and inability to ambulate for 3 days. She was previously very active and notes no trauma to the knee. Knee range of motion is limited to a 20-degree arc of motion with an obvious large effusion. Radiographs are shown in figure A. Right knee synovial aspiration demonstrates 65,000 WBC with 92% PMNs and no crystals. Upon further questioning, she endorses new vaginal discharge following a new sexual encounter. Given this clinical scenario, which of the following accurately describes the expected causative pathogen?
1
Gram-positive cocci in chains
2
Gram-positive cocci in grape-like clusters
3
A combination of intracellular and extracellular gram-negative diplococci
This young otherwise healthy female patient has a history concerning for Neisseria gonorrhea septic arthritis of the right knee. The expected morphology is a combination of intracellular and extracellular gram-negative diplococci.
Septic arthritis of the knee is diagnosed with a combination of history, physical examination, and aspiration results. In young otherwise healthy patients with a presentation consistent with acute monoarticular septic arthritis, sexual history should be obtained as suspicion should be very high for a diagnosis of gonococcal septic arthritis. Accurate diagnosis of gonococcal septic arthritis is important as it directs antibiotic treatment to include ceftriaxone (or cefotaxime, or ceftizoxime). Treatment typically includes some form of arthroscopic drainage most commonly through arthroscopic or open irrigation and debridement or less commonly serially aspirations.
Favero et al. reviewed 42 patients diagnosed with septic arthritis from their rheumatology clinic. They found patients under 60 years of age were more frequently affected by joint disease and had lower synovial white blood cell count than patients >60/. They conclude the recent increased therapeutic
aggressiveness in rheumatology patients may have increased the frequency of joint disease and lower synovial white blood cell counts in patients younger than 60.
Frazee et al. reviewed 109 synovial fluid samples sent from the emergency department over a 15 month period. They found 12 positive cases of septic arthritis 50% were from MRSA with 33% from MSSA. They concluded that in this emergency department population MRSA was the most common cause of community-acquired adult septic arthritis.
Figure A shows a lateral non-weight bearing x-ray of the right knee with a large knee effusion. Illustration A shows a histologic slide with a combination of intracellular and extracellular gram-negative diplococci consistent with Neisseria gonorrhea.
Incorrect Answers:
Answer 1: Gram-positive cocci in chains most accurately describes streptococcal morphology.
Answer 2: Gram-positive cocci in grape-like clusters describes staphylococcal morphology.
Answer 4: Extracellular, facultative anaerobe, gram-negative bacilli all describe the characteristics of Escherichia or E. coli morphology.
Answer 5: Extracellular, aerobic, gram-negative bacilli all describe the characteristics of pseudomonal morphology.
QUESTION 13 OF 50
Which of the following is the reported incidence of nerve injuries following total shoulder arthroplasty:
1
Less than 1%
2
Between 1% and 2%
3
Between 2% and 4%
4
Between 4% and 5%
5
Greater than 10%
The reported incidence of nerve injuries following shoulder arthroplasty is 4.3%. Correct Answer: Between 4% and 5%
QUESTION 14 OF 50
Results of a study demonstrating no difference between treatments when a difference truly exists is an example of which of the following?
1
Statistical insignificance
2
Type I error
3
Type II error
4
Fragile p-values
5
Negative predictive value
#
**
A type II error (also known as a beta error) occurs when results demonstrate that two groups are similar when, in reality, they are different (with regard to the statistic being measured). Type I errors show that a difference exists when, in reality, no difference exists. A statistically insignificant result may lead an investigator to conclude that no difference exists between two groups; this may be correct (and therefore not a type II error). The concept of
`fragile` p-values is that small sample sizes may result in wide variability of p- values with only one change in a data point for a given group. This singular change could be a chance occurrence, but it still can affect the statistical significance of the outcomes analysis.
Fragility of p-values is limited by increasing sample sizes. Negative predictive value is the
proportion of patients with negative test results who are correctly diagnosed.
QUESTION 15 OF 50
Indications for high tibial osteotomy include all of the following except:
1
10° to 15° of varus deformity on weight-bearing radiographs
2
90° preoperative range of motion
3
Flexion contracture less than 15°
4
60° preoperative range of motion
5
Age younger than 60 years
Indications for a high tibial osteotomy include age younger than 60 years, 10° to 15° varus deformity, 90° preoperative arCrange of motion, and flexion contracture less than 15°
QUESTION 16 OF 50
of 100
A 20-year-old collegiate pitcher sustains a medial collateral ligament (MCL) rupture of his throwing elbow for which surgical reconstruction is necessary. The goal of surgery is anatomic restoration of the MCL. Which statement best describes the kinematics of the native MCL?
1
The posterior bundle demonstrates the greatest change in tension from flexion to extension.
2
The posterior bundle is isometric.
3
The anterior bundle becomes tight in flexion and lax in extension.
4
The anterior and posterior bundles are isometric.
The anterior bundle is the most important portion of the complex when treating valgus instability of the elbow. The ligament originates from the anteroinferior surface of the medial epicondyle. The anterior bundle inserts on the medial border of the coronoid at the sublime tubercle.
The anterior bundle of the ulnar collateral ligament (UCL) is the primary restraint to valgus stress, and the radial head is a secondary restraint. With anterior bundle sectioning, the resultant instability is most substantial between 60 and 70 degrees and is lowest at full extension and full flexion. True lateral radiographs reveal that the flexion-extension axis, or center of rotation, of the elbow lies in the center of the trochlea and capitellum. The origin of the anterior bundle of the UCL lies slightly posterior to the rotational center of the elbow. The anterior bundle is further divided into an anterior band and a posterior band. The eccentric origin of these anterior bundle components in relation to the rotational center through the trochlea creates a CAM effect during flexion and extension. The anterior band tightens during extension, and the posterior band tightens during flexion. This reciprocal tightening of the 2 functional components of the anterior bundle allows the ligament to remain taut throughout the full range of flexion.
Cadaver dissection studies have identified the origin and insertion of both the medial and lateral stabilizing elbow ligaments. The anterior bundle of the MCL is isometric throughout the flexion/extension arc of motion, making Response 3 incorrect. The posterior bundle of the MCL elongates with elbow flexion, so Responses 2 and 4 are incorrect. The posterior bundle of the MCL also demonstrates the most change in length from extension to flexion of all the elbow ligaments.
RECOMMENDED READINGS
24. [Hotchkiss RN, Weiland AJ. Valgus stability of the elbow. J Orthop Res. 1987;5(3):372-7. PubMed PMID: 3625360.](http://www.ncbi.nlm.nih.gov/pubmed/3625360)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3625360)
25. [Morrey BF, An KN. Functional anatomy of the ligaments of the elbow. Clin Orthop Relat Res. 1985 Dec;(201):84-90. PubMed PMID: 4064425.](http://www.ncbi.nlm.nih.gov/pubmed/4064425)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4064425)
26. [Schwab GH, Bennett JB, Woods GW, Tullos HS. Biomechanics of elbow instability: the role of the medial collateral ligament. Clin Orthop Relat Res. 1980 Jan-Feb;(146):42-52. PubMed PMID: 7371268. ](http://www.ncbi.nlm.nih.gov/pubmed/7371268)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7371268)
CLINICAL SITUATION FOR QUESTIONS 79 THROUGH 81
Figure 79 is the radiograph of a 65-year-old active, right-hand-dominant woman with a 6-month history of right shoulder pain, motion loss, and progressive weakness after undergoing a hemiarthroplasty to address osteoarthritis 1 year ago. She denies recent trauma to her right shoulder and denies constitutional symptoms. Her surgical wound site is benign. She can actively forward flex to 90 degrees and abduct to 60 degrees. Passive forward flexion and abduction are 150 degrees and 90 degrees, respectively.
QUESTION 17 OF 50
of 100
What is the most common site of nerve compression in radial tunnel syndrome?
1
Fibrous bands anterior to the radiocapitellar joint
2
Recurrent radial vessels
3
Medial edge of the extensor carpi radialis brevis (ECRB)
4
Proximal aponeurotic edge of the supinator (arcade of Frohse)
Radial tunnel syndrome occurs as the result of radial nerve compression at 5 potential sites. These are the fibrous bands anterior to the radiocapitellar joint, the radial recurrent vessels (known as the leash of Henry), the medial edge of the ECRB, the proximal aponeurotic edge of the supinator (arcade of Frohse), and the distal edge of the supinator. The arcade of Frohse is the most common site of compression. The chief discomfort is deep, aching pain in the dorsoradial proximal forearm. Motor and sensory symptoms usually are absent. This condition often is seen when pain persists after surgery for lateral epicondylitis. Lateral epicondylitis and radial tunnel syndrome coexist 5% of the time.
Examination findings are tenderness 4 cm distal to the lateral epicondyle, pain with resisted supination, and pain with resisted long finger extension. Electromyogram/nerve conduction study and MRI results usually are normal. A steroid injection can be diagnostic and also may provide temporary relief of symptoms. Surgery involves decompression of all potential areas of compression and allows good to excellent results in only 50% to 90% of cases. Symptoms may take 9 to 18 months to resolve after surgery.
RECOMMENDED READINGS
19. Lawrence T, Mobbs P, Fortems Y, Stanley JK. Radial tunnel syndrome. A retrospective review of 30 decompressions of the radial nerve. J Hand Surg Br. 1995 Aug;20(4):454-9. PubMed PMID: 7594982.View Abstract at PubMed
20. Lubahn JD, Cermak MB. Uncommon nerve compression syndromes of the upper extremity. J Am Acad Orthop Surg. 1998 Nov-Dec;6(6):378-86. Review. PubMed PMID: 9826421.
**CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 21**
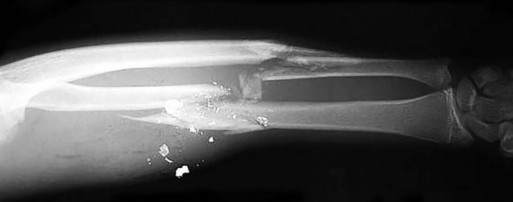
Figures 18a and 18b are the radiographs of a 31-year-old man with an isolated 9-mm gunshot injury to his right forearm. The entry and exit holes are smaller than 1 cm. Motor and sensory function in his right wrist and hand are intact. In the emergency department, the wounds are irrigated and dressed, a long-arm splint is applied, intravenous cefazolin is administered, and a tetanus vaccination is provided. Over the ensuing 2 hours, he experiences increasing pain in his right forearm and new numbness in his right hand. His radial and ulnar arteries remain palpable at the wrist level, and capillary refill is less than 1 second over the digital pulps.
QUESTION 18 OF 50
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. This patient elects nonsurgical treatment and later experiences persistent instability. Examination reveals an asymmetric Dial test finding and a varus thrust during ambulation. Which osteotomy and correction appropriately addresses this chronic instability pattern? ---
1
Distal femoral/opening lateral wedge osteotomy
2
Distal femoral/closing lateral wedge osteotomy
3
High tibial osteotomy; opening medial wedge with increased tibial slope
4
High tibial osteotomy; closing lateral wedge with decreased tibial slope
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used.
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
QUESTION 19 OF 50
of 100
Figures 32a through 32c are the radiograph and CT scans of a 75-year-old smoker with hypertension who sustained a ground-level fall without loss of consciousness with impact to her
left upper extremity 1 week ago. She states that she lived independently at home with her husband prior to her fall. What is the most appropriate next step?
1
Hemiarthroplasty
2
Initial sling immobilization with subsequent physical therapy
3
Open reduction and internal fixation
4
Reverse total shoulder arthroplasty (rTSA)
The radiographs and CT scans indicate a 4-part left proximal humerus fracture with tuberosity comminution. Based upon her preinjury level of activity and current imaging studies, nonsurgical management is not the correct option to restore her ability to perform activities of daily living, including hygiene care. There has been enthusiasm among surgeons regarding the use of the reverse shoulder prosthesis as the primary mode of surgical treatment of certain 3- and 4-part proximal humerus fractures. The main attribute of this implant is its ability to achieve functional shoulder forward flexion and abduction regardless of tuberosity healing, position, and degree of comminution. Nevertheless, repair and union of the greater tuberosity fragment during rTSA demonstrate improved external rotation, clinical outcomes, and patient satisfaction than outcomes achieved after tuberosity resection, nonunion, or resorption. Based upon this patient’s age and imaging findings, an rTSA would provide pain relief and improved function with complication rates similar to those associated with hemiarthroplasty. Open reduction with internal fixation would not be a viable option because of the high probability for a dysvascular head, increased risk for nonunion, and potential for revision surgery, including arthroplasty. Hemiarthroplasty for 4-part proximal humerus fractures remains a viable option for patients younger than 70 years of age with minimal tuberosity comminution and an intact rotator cuff who can comply with a postsurgical rehabilitation program. Most studies indicate significant pain relief with this modality with significant variation in functional outcomes. In this clinical scenario, the patient’s injury may not be best served with hemiarthroplasty because of uncertainty regarding functional outcome.
RECOMMENDED READINGS
34. [Jobin CM, Galdi B, Anakwenze OA, Ahmad CS, Levine WN. Reverse shoulder arthroplasty for the management of proximal humerus fractures. J Am Acad Orthop Surg. 2015 Mar;23(3):190-201. doi: 10.5435/JAAOS-D-13-00190. Epub 2015 Jan 28. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/25630370)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25630370)
35. [Bufquin T, Hersan A, Hubert L, Massin P. Reverse shoulder arthroplasty for the treatment of three- and four-part fractures of the proximal humerus in the elderly: a prospective review of 43 cases with a short-term follow-up. J Bone Joint Surg Br. 2007 Apr;89(4):516-20. ](http://www.ncbi.nlm.nih.gov/pubmed/17463122)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17463122)
36. [Cuff DJ, Pupello DR. Comparison of hemiarthroplasty and reverse shoulder arthroplasty for the treatment of proximal humeral fractures in elderly patients. J Bone Joint Surg Am. 2013 Nov 20;95(22):2050-5. doi: 10.2106/JBJS.L.01637. PubMed PMID: 24257664.](http://www.ncbi.nlm.nih.gov/pubmed/24257664)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24257664)
37. [Boyle MJ, Youn SM, Frampton CM, Ball CM. Functional outcomes of reverse shoulder arthroplasty compared with hemiarthroplasty for acute proximal humeral fractures. J Shoulder Elbow Surg. 2013 Jan;22(1):32-7. doi: 10.1016/j.jse.2012.03.006. Epub 2012 May 29. ](http://www.ncbi.nlm.nih.gov/pubmed/22652065)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22652065)
QUESTION 20 OF 50
A 25-year-old female presents to the emergency room for the fourth time in the last week. She has vague complaints of extremity pain. Physical examination by a male ER resident has been limited each visit because she is terrified of the pain that the clinician may cause. On physical examination, she is withdrawn and frightened.
Regions of ecchymosis are noted throughout chest and abdomen. She has requested multiple radiographs, MRI and CT scans. Today's imaging (radiographs, MRI, CT scan) has been unrevealing. What is the most likely diagnosis?
1
Malingering
2
Complex regional pain syndrome
3
Anxiety disorder
4
Intimate partner violence
5
Fibromyalgia
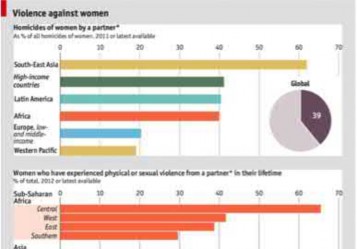
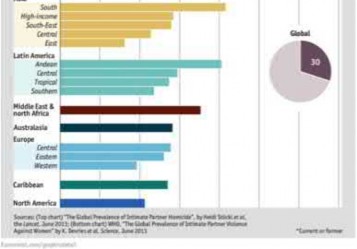
Based on the history and clinical presentation, the most likely diagnosis is intimate partner violence.
Domestic violence or intimate partner violence can be in the form of mental or physical abuse, neglect or abandonment. Close to 25% of women will experience domestic violence. Risk factors include young age (19-29 years of age), females, pregnancy and lower socioeconomic status. Affected patients will have repeated visits to the emergency room, find reasons to stay in a treatment facility for an extended period of time and constantly seek approval
of their partner.
Shields et al. reviewed factors influence outcome in treatment of patients affected by domestic violence. They found that positive outcomes were associated with interdisciplinary approaches to management. This included better history assessment, providing written documentation regarding intervention and better access to information on community resources.
Illustration A is a chart documenting the frequency of female domestic violence throughout the world as of 2012.
Incorrect Answers
Answers 1, 2, 3, 5: These conditions are not consistent with this patient’s history.
QUESTION 21 OF 50
A 70-year-old man undergoes removal of an infected total hip arthroplasty (THA) and insertion of an
articulating antibiotic-loaded spacer to treat a deep periprosthetic hip infection. While in a nursing home receiving intravenous antibiotics 3 weeks after surgery, the patient trips and falls. Examination reveals swelling in the mid and distal thigh, intact skin and neurovascular structures, and severe pain with knee
or hip movement. Radiographs of the femur are shown in Figures 1 through
1
What is the most appropriate treatment for the fracture below the implant?
2
Balanced traction to address concern for persistent infection with reoperation
3
Open reduction and internal fixation of the fracture with a lateral plate and screws
4
Removal of the articulating spacer and revision to a longer-stem antibiotic-loaded articulating spacer
5
Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement
This patient has a type C periprosthetic femoral fracture. The articulating spacer is not involved in the fracture, which is well distal to the implant. The most appropriate treatment is open reduction and internal fixation of the fracture. Traction is not appropriate for this fracture because the injury can be treated surgically despite the history of previous hip infection. Traction would also be needed for at least 5 weeks and would delay the surgical treatment of the periprosthetic fracture until the time of second-stage revision THA. The fracture is fairly distal, and revision to a longer antibiotic-loaded implant or uncemented stem is not suitable for this fracture pattern, because it extends well past the isthmus. A femoral stem in the distal fragment would provide little stability for the fracture. Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement is not appropriate, because it would be premature to reimplant the man's hip while he is still receiving treatment for a deep hip infection.
QUESTION 22 OF 50
Computer navigation in total knee arthroplasty (TKA) has demonstrated which of the following?
1
Decreased cost
2
Improved clinical outcomes
3
Fewer outliers in terms of component position
4
Improved longevity
5
Decreased surgical time
DISCUSSION: Computer navigation has been shown to improve the accuracy of placement of TKA components with fewer outliers. However, the surgical time and cost are increased. No studies to date have demonstrated improved clinical outcomes or implant survivorship.
REFERENCE: Haaker RG, Stockheim M, Kamp M, et al: Computer-assisted navigation increases precision of component placement in total knee arthroplasty. Clin Orthop Relat Res 2005;433:152-159.
QUESTION 23 OF 50
A patient with stress fracture has a transcortical area of intense uptake on the technetium bone scan. Which of the following findings would most likely be present on the magnetic resonance imaging (MRI) scan:
1
Normal periosteal signal; normal marrow signal on T1; high marrow signal on T2
2
Normal periosteal signal; low marrow signal on T1; high marrow signal on T2
3
Normal periosteal signal on T2; low marrow signal on T1; high marrow signal on T2
4
High periosteal signal on T2; low marrow signal on T1; high marrow signal on T2
5
High periosteal signal on T2; low marrow signal on T1; normal marrow signal on T2
In 1995, Fredrickson and colleagues classified stress fractures into four grades based upon bone scans:
Grade 1     Small ill-defined cortical area of mildly increased activity Grade 2     Well-defined cortical area of moderately increased cortical                     activity
Grade 3Â Â Â Â Â Wide, cortical-medullary area of increased activity
Grade 4Â Â Â Â Â Transcortical area of intensely increased activity
In a grade 4 stress fracture, the corresponding MRI will show: High periosteal signal on T2-weighted images
Low signal on T1-weighted images, often with a liner low signal line representing the fracture line
High signal on T2-weighted images, often with a liner low signal line representing the fracture line
C orrect Answer: High periosteal signal on T2; low marrow signal on T1; high marrow signal on T2
QUESTION 24 OF 50
The iliopectineal fascia runs between which of the following structures? ](http://www.orthobullets.com/anatomy/10111/femoral-nerve)
1
Iliopsoas muscle and the iliac vessels/femoral nerve
2
Lateral femoral cutaneous nerve and the iliac vessels
3
Iliopsoas muscle/femoral nerve and the iliac vessels
4
Iliac wing and the iliopsoas muscle
5
Pubic symphysis and the iliac vessels
No detailed explanation provided for this question.
QUESTION 25 OF 50
of 100
A 35-year old man has had 8 weeks of progressive midback pain and persistent left thigh pain. He tried chiropractic manipulation and lumbar traction, which were both unsuccessful in pain relief. MRI scans reveal a left-sided L2-L3 foraminal disk herniation. He is subsequently referred to an interventional pain specialist. A left transforaminal epidural injection is scheduled. During the procedure, the patient develops rapid bilateral leg weakness and subsequent paraplegia. Post procedure MRI is shown in Figures 1 and
1
What is the most likely cause of this lesion neurological injury?

2
Epidural hematoma
3
Intra-arterial injection
4
Intravenous injection
5
L2 nerve puncture
■ Complication rates for percutaneous interventional procedures are low (1-2%). Potential risks for epidural injections include dural injury, cerebrospinal fluid leak, infection, nerve puncture, intrathecal injection, and intravascular injection. Furman and associates reported 8% incidence of inadvertent vascular puncture from lumbar transforaminal injection. In this patient, there was injection into an L2 radiculomedullary artery, which ultimately caused catastrophic spinal cord ischemia and infarction. The dominant radiculomedullary artery, artery of Adamkiewicz, is the major blood supply for the anterior cord. Adamkiewicz enters the cord on the left from T9 to L2 level in 85% of people. The MRI scan shown, taken 48 hours after injury, indicates classic cord infarction with hyperintense cord signal on sagittal film. The axial image also shows hyperintense signal, predominantly in the gray matter with "owl's eye" pattern. Epidural hematoma would show a high T2 signal extradural compressive lesion on MRI. Intravenous injections are rarely dangerous. L2 nerve injury from a puncture would cause unilateral L2 nerve pain (dysesthesia), hypoesthesia, and/or palsy.
QUESTION 26 OF 50
Long-term alendronate (Fosamax) use for osteoporosis has been associated
**with which of the following?**
1
Scurvy
2
Detached retina
3
Uterine carcinoma
4
Osteonecrosis of the femoral head
5
Diaphyseal femoral insufficiency fractures
#
**
Alendronate is a bisphosphonate that inhibits the ruffled border of the osteoclast. When used long term, this class of medication prevents the normal bone remodeling process. Long-term use has recently been shown to be associated with insufficiency fractures of the femur. Osteonecrosis of the jaw has been described but not in other anatomic locations. Scurvy occurs because of a lack of vitamin C and use of bisphosphonates is not associated with
uterine cancer or a detached retina.
QUESTION 27 OF 50
In the study design for evaluating the effectiveness of total hip replacement, the endpoint can be only:
1
Revision hip surgery
2
RadiographiCloosening of the implant
3
Any well-defined chosen point, such as revision hip surgery or functional level and pain
4
Pain or functional level
5
Range of motion
In the study design, it is paramount that a universal, well-defined endpoint is chosen. In the well-established Scandinavian Hip Registries, this endpoint is revision total hip arthroplasty. Whether this endpoint is sensitive enough is debatable. For more in- depth studies, several other endpoints, such as pain or postoperative functional level, may also be used
QUESTION 28 OF 50
Initial postoperative management after repair of an acute rotator cuff tear includes
1
active range of motion.
2
active abduction to prevent scarring.
3
passive forward elevation and external rotation within a safe zone determined at surgery.
4
eccentric strengthening exercises.
5
internal rotation behind the back.
In the immediate postoperative period following repair of an acute rotator cuff tear, passive forward elevation and external rotation should be performed within the safe zone determined at surgery. Early active range of motion (prior to tendon healing), internal rotation behind the back, and resistive exercises increase the risk of rupture of the repair.
REFERENCES: Iannotti JP: Full-thickness rotator cuff tear: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Bigliani LU, Cordasco FA, McIlveen ST, et al: Operative repair of massive rotator cuff tears: Long-term result. J Shoulder Elbow Surg 1992;1:120-130.
QUESTION 29 OF 50
of 100
Figures 24a and 24b are the radiographs of a 7-year-old boy who fell off the monkey bars and has a closed injury. His hand appears warm and well perfused with an absent radial pulse. What is the best initial treatment?
1
Immediate open reduction with an anterior approach
2
Immediate open reduction with a posterior approach
3
Obtain an immediate arteriogram
4
Perform closed reduction and reassess perfusion and pulse
In displaced extension-type supracondylar fractures, the neurovascular structures get kinked anteriorly or anteromedially related to the displacement. In almost all cases, there is a spontaneous resolution of this kink following closed fracture reduction.
QUESTION 30 OF 50
A 35-year-old man reports a 2-year history of right groin pain. The pain is made worse with hip flexion, prolonged sitting, and cycling. A radiograph and MRI scan are shown in Figures 16a and 16b. Nonsurgical management has failed to provide relief. What is the best surgical option?
1
Arthroscopic labral debridement
2
Reverse periacetabular osteotomy
3
Resurfacing hip arthroplasty
4
Femoral neck osteochondroplasty and resection of the detached labrum
5
Femoral neck osteochondroplasty and reattachment of the labrum
DISCUSSION: The patient has cam-type femoral acetabular impingement. He still has a well-maintained joint space without significant degenerative changes, and given his age a joint preserving procedure would be the procedure of choice. A reverse periacetabular osteotomy may be considered in a retroverted acetabulum; however, that is not the case here. A femoral neck osteochondroplasty is required to remove the cam of bone and reshape the femoral head- neck junction to improve the femoral head/neck ratio (femoral head offset). Typically, in isolated cam impingement, cartilage damage in the anterior-superior acetabulum precedes labral damage. Labral debridement alone does not address the pathology of impingement. In cases where labral detachment is present, reattachment has been shown to be superior to labral resection.
REFERENCES: Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
Parvizi J, Leunig M, Ganz R: Femoroacetabular impingement. J Am Acad Orthop Surg 2007;15:561-570. Trousdale RT: Acetabular osteotomy: Indications and results. Clin Orthop Relat Res 2004;429:182-187.
Figure 17a Figure 17b Figure 17c
QUESTION 31 OF 50
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Based on the pathology noted, which finding may be found on plain knee radiographs? --- --- --- --- ---
1
Shallow trochlear groove
2
Squaring of the lateral femoral condyle
3
Deepening of the sulcus terminalis
4
Medial joint space narrowing
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment _of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair._
QUESTION 32 OF 50
Examination of an 18-year-old professional soccer player who was forcefully kicked across the shin while attempting a slide tackle reveals a marked effusion and limited motion of the knee. The tibia translates 12 mm posterior to the femoral condyles when the knee is held in 90 degrees of flexion. There is no posteromedial or posterolateral instability. Management should consist of
1
early reconstruction of all injured structures.
2
knee immobilization in 30 degrees of flexion for 2 to 4 weeks.
3
knee immobilization in full extension for 2 to 4 weeks.
4
protected weight bearing and intense hamstring strengthening.
5
no weight bearing, followed by a gradual return to sports.
The patient has an acute grade III posterior cruciate ligament injury. The majority of grade I and II injuries can be treated with protected weight bearing and quadriceps rehabilitation, and most patients can return to sports within 2 to 4 weeks. In contrast, grade III injuries require immobilization in full extension for 2 to 4 weeks to protect the posterior cruciate ligament and the other posterolateral structures presumed to be damaged. The mainstay of postinjury rehabilitation for all posterior cruciate ligament injuries is quadriceps strengthening exercises, which have been shown to counteract posterior tibial subluxation.
REFERENCES: Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Posterior Cruciate Ligament Injuries in Principles and Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott, Williams and Wilkins, 2000.
QUESTION 33 OF 50
A 20-year-old healthy female endurance athlete has lower leg pain and dorsal foot paresthesias after
running for 30 minutes. She has seen another physician and has been ruled out for a bone stress injury. She has tried extensive nonsurgical measures such as shoe modification and an extended period without running. You suspect chronic exertional compartment syndrome and perform intramuscular compartment pressure measurements at three separate time points with the following results:
**Baseline**
**1 Minute**
**5 Minutes**
|||
**Anterior**
7
32
25
**Lateral**
8
29
23
**Superficial Posterior**
12
25
17
**Deep Posterior**
14
22
16
The patient decides to pursue surgical intervention. Which compartments should be released?
1
Anterior and lateral
2
Anterior, lateral, and deep posterior
3
Anterior, lateral and superficial posterior
4
Lateral and superficial posterior
The diagnostic criteria for chronic exertional compartment syndrome is pressure >15 mm Hg at rest, or
>30 mm Hg at 1 minute post exercise, or >20 mm Hg at 5 minutes post-exercise. The anterior and lateral compartments are the only ones that meet strict diagnostic criteria for chronic exertional compartment syndrome. The superficial posterior compartment, although close to meeting criteria, is not responsible _for the patient's symptoms and falls below current thresholds for diagnosis._
QUESTION 34 OF 50
A 65-year-old woman landed on her nondominant left shoulder in a fall. An AP radiograph is shown in Figure 39. Management should consist of
1
closed reduction and immobilization.
2
closed reduction and percutaneous pinning.
3
open reduction and internal fixation.
4
humeral hemiarthroplasty with tuberosity repair.
5
total shoulder arthroplasty.
The radiograph reveals a four-part fracture-dislocation of the proximal humerus. Humeral hemiarthroplasty and tuberosity repair is the treatment of choice because the risk of osteonecrosis is high after attempted repair of this injury. Glenoid resurfacing is reserved for acute fractures in which there is significant preexisting glenoid arthrosis, such as in patients with rheumatoid arthritis.
REFERENCES: Neer CS II: Displaced proximal humeral fractures: II. Treatment of three- and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Robinson CM, Page RS, Hill RM, et al: Primary hemiarthroplasty for treatment of proximal humeral fractures. J Bone Joint Surg Am 2003;85:1215-1223.
QUESTION 35 OF 50
Involvement of what single muscle best distinguishes an L5 radiculopathy from a peroneal neuropathy? ](http://www.orthobullets.com/anatomy/10117/deep-peroneal-nerve)
1
Extensor hallucis longus
2
Extensor digitorum brevis
3
Tibialis anterior
4
Tibialis posterior
5
Peroneus longus
No detailed explanation provided for this question.
QUESTION 36 OF 50
A 75-year-old woman with rheumatoid arthritis and a long history of oral corticosteroid use sustains a comminuted intra-articular distal humerus fracture. What is the best surgical option?
1
Open reduction internal fixation (ORIF) with parallel plates
2
ORIF with orthogonal plates and iliac crest bone grafting
3
Total elbow arthroplasty (TEA)
4
Closed reduction and percutaneous pinning
TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF with TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared with ORIF. TEA was also likely to result in a lower reoperation rate; one-quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA versus ORIF in 24 elderly women. TEA outcomes were again superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed reduction and percutaneous pinning studies have not been published on the adult population. 25
QUESTION 37 OF 50
A well-developed college football player reports swelling and a heaviness in the arm after lifting weights. Examination reveals that distal pulses are normal and equal in both arms. A venogram is shown in Figure 13. What is the most likely cause of this condition?
1
Intimal tearing of the subclavian artery
2
Compression of the subclavian vein by scalene muscle hypertrophy
3
Postural compression of the neurovascular bundle between the clavicle and the first rib
4
A congenital cervical rib
5
Arterial thrombosis induced by repeated overhead activities
The clinical findings indicate venous obstruction without arterial compression, and the venogram reveals occlusion of the subclavian vein, which is most likely the result of thoracic outlet compression. In the developed athlete, scalene muscle hypertrophy (Paget-Schroetter syndrome) causes compression of the subclavian vein. Treatment should consist of thrombolysis followed by decompressive surgery.
REFERENCES: Angle N, Gelabert HA, Farooq MM, et al: Safety and efficacy of early surgical decompression of the thoracic outlet for Paget-Schroetter syndrome. Ann Vasc Surg 2001;15:37-42.
Azakie A, McElhinney DB, Thompson RW, et al: Surgical management of subclavian-vein effort thrombosis as a result of thoracic outlet compression. J Vasc Surg 1998;28:777-786.
QUESTION 38 OF 50
An 18-year-old man is seen in the office because of back pain in the thoracic region. He has a kyphosis of 65°, a slight wedging in the midthoracic spine, and a Risser sign of 4. Recommended treatment includes:
1
A program of strengthening and stretching exercises
2
A Milwaukee brace
3
A Boston brace
4
A posterior spinal fusion
5
An anterior and posterior spinal fusion
Exercises must be the first treatment for this patient because he is too mature for brace treatment.
Brace treatment is not indicated for someone of this skeletal maturity. Surgery is not indicated unless the patient fails conservative treatment.
QUESTION 39 OF 50
Which category of failure of formation anomalies is most often associated with systemic anomalies?
1
Radial deficiencies.
2
Ulnar deficiencies.
3
C entral deficiencies.
4
Transverse deficiencies.
5
Tibial deficiencies
Radial deficiencies are often seen in the later association. which may include cardiac,renal,anorectal and tracheoesphogeal abnormalities.
QUESTION 40 OF 50
A 30-year-old woman sustains a transverse amputation of the distal phalanx of the index finger, leaving exposed bone. What is the most appropriate management of the soft-tissue defect?
1
Dressing changes and healing by secondary intention
2
Split-thickness skin grafting
3
V-Y advancement flap
4
Moberg (volar advancement flap)
5
First dorsal metacarpal artery-island pedicled flap
V-Y advancement flaps are ideal for fingertip amputations that are transverse or dorsal oblique in nature. Healing by secondary intention is contraindicated with exposed bone. Shortening of exposed bone to allow primary skin closure is a possible alternative, as long as significant shortening of the index finger is avoided. A Moberg flap is useful only for distal amputations of the thumb. The first dorsal metacarpal artery-island pedicled flap uses tissue from the dorsum of the proximal index finger, and is typically used to resurface defects of
the thumb.
REFERENCES: Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Atasoy E, Ioakimidis E, Kasdan ML, et al: Reconstruction of the amputated fingertip with a triangular volar flap: A new surgical procedure. J Bone Joint Surg Am 1970;52:921-926.
QUESTION 41 OF 50
Which of the following actions increases radiation exposure to patients and personnel when using fluoroscopy?
1
The use of lead glasses, thyroid shield, and a lead apron with a equivalent lead thickness of 0.25 mm
2
Orienting the cathode ray tube beneath the patient with the image intensifier receptor as close to the patient as possible
3
Limiting the beam on time to only what is clinically important
4
The use of continuous fluoroscopy to ensure proper placement of implants
5
Orienting the beam in the opposite direction of the working team and keeping the team outside a 6-foot radius from the fluoroscopy machine
#
**
Continuous fluoroscopy and cineradiography exposes the patient and personnel to markedly increased levels of direct and scatter radiation exposure. Continuous fluoroscopy should be limited to only what is absolutely needed for safe completion of the procedure. By orienting the cathode ray
tube beneath the patient and placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
QUESTION 42 OF 50
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of
1
external electrical stimulation.
2
external ultrasound stimulation.
3
implanted electrical stimulation.
4
closed reduction and percutaneous fixation.
5
open reduction and internal fixation with bone graft.
The radiograph reveals an atrophic nonunion of the diaphysis of the clavicle. Electrical or ultrasound stimulation may be an option in diaphyseal nonunions that have
shown some healing response with callus formation, but these techniques are not successful
in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions
of the clavicle.
REFERENCES: Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
QUESTION 43 OF 50
C linical improvement following ankle distraction arthroplasty:
1
Typically reaches its maximal improvement by the end of 1 year
2
Is accompanied by major gains in ankle range of motion
3
C an take up to 5 years to reach maximal improvement
4
Is not accompanied by improvement in radiographic joint space
5
Is usually realized within the first month following removal of the frame
Distraction arthroplasty with an Ilizarov external fixator is usually associated with half of the clinical improvement occurring within the first year, and the other half happening over the next 5 years.
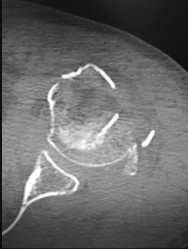
QUESTION 44 OF 50
Which of the following primary prognostic factors best predicts the outcome of the knee lesion shown in Figure 22?
1
Location
2
Size
3
Knee stability
4
Patient age
5
Degree of pain
The patient has osteochondritis dissecans. While location, size, and knee stability are all relevant to the overall prognosis, studies have shown that younger patients with open growth plates have a better prognosis of healing when compared with patients who have closed growth plates. The degree of pain is also relevant to treatment, but it is subjective rather than objective and is not as reliable of a prognostic indicator as age.
REFERENCES: Stanitski CL: Osteochondritis dissecans of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 387-405.
Cahill B: Treatment of juvenile osteochondritis dissecans and osteochondritis dissecans of the knee. Clin Sports Med 1985;4:367-384.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
QUESTION 45 OF 50
Glomus tumors are characterized by all of the following except:
1
Three-quarters of glomus tumors occur in the hand.
2
Pain, point tenderness, and cold sensitivity are clinically present.
3
Glomera are neuromyoarterial apparatuses that regulate sympathetic outflow.
4
Persistence of symptoms for more than 3 months after excision is suggestive of recurrence.
5
None of the above
Glomera are neuromyoarterial apparatuses that regulate temperature.
QUESTION 46 OF 50
Urgent closed reduction of ankle fracture-dislocations using intraarticular lidocaine injection:
1
Provides a similar degree of analgesia compared to conscious sedation
2
Requires more time to perform the reduction and splint the leg than with conscious sedation
3
Results in inferior reduction of ankle deformity compared to conscious sedation
4
Requires frequent repeat reduction procedures due to persistent fracture malalignment
5
Is painful due to distension of the joint capsule
A prospective randomized study compared intraarticular lidocaine injection to conscious sedation for analgesia during reduction of ankle fracture-dislocations. There was no difference in the amount of analgesia provided by the two methods. Time for reduction and splinting was less in the local anesthetic group. Quality of reduction was similar in both groups.
QUESTION 47 OF 50
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
1
Tension pneumothorax
2
Inadvertent epidural injection
3
Inadvertent intravascular injection
4
Laryngeal nerve block
5
Bezold-Jarisch reflex
The beach chair position may cause sudden hypotension and bradycardia as a result of the Bezold-Jarisch reflex. This reflex occurs when venous pooling and increased sympathetic tone induce a low-volume, hypercontractile ventricle, resulting in activation of the parasympathetic nervous system and sympathetic withdrawal. The reported incidence of this phenomenon associated with the sitting position is between 13% to 24%. Left untreated, the result may be cardiac arrest. Pneumothorax or central nervous system toxicity after interscalene block is rare and has an incidence of less than 0.2%. Laryngeal nerve block associated with interscalene nerve block can occur but usually results in hoarseness secondary to ipsilateral vocal cord palsy.
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
QUESTION 48 OF 50
of 100
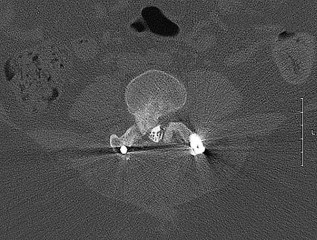
A 73-year-old man goes to the emergency department after tripping and falling down roughly thirteen steps at home. Prior to the injury, the patient had well-controlled medical comorbidities and was independent with all activities of daily living. Figures 1 through 3 show the injury sustained by the patient. What is the most appropriate definitive treatment for this patient?
1
Rigid cervical collar
2
Halo vest
3
Posterior C1-C2 instrumentation and fusion
4
Anterior C2 fixation
■ The patient has a C1 burst fracture, as well as a grossly displaced C2 fracture. Surgical treatment should be considered for this patient who has good baseline function and wellcontrolled medical comorbidities. A cervical collar would not offer adequate stabilization for this fracture. Anterior reduction of this C2 fracture would be difficult, and screw fixation of C2 would not address the C1-C2 instability. A halo vest is considered a relative contraindication in the older patient population. Therefore, posterior C1-C2 fixation is the most appropriate choice.
QUESTION 49 OF 50
-What method of spinal fixation requires the largest force to disrupt the bone-implant interface?
1
Sublaminar cables
2
Laminar hooks
3
Pedicle hooks
4
Pedicle screws
No detailed explanation provided for this question.
QUESTION 50 OF 50
Which of the following methods best aids in diagnosis of an interdigital neuroma?
1
Ultrasound
2
MRI
3
Web space injection
4
Electromyography and nerve conduction velocity studies
5
History and physical examination
History and physical examination are still the gold standard for diagnosis of an interdigital neuroma. Ultrasound and MRI may be helpful adjuncts but are dependent on equipment and operator expertise. Web space injection may be helpful for diagnostic and therapeutic purposes. Electromyography and nerve conduction velocity studies are of little benefit for distal lesions.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 145-147.
Bennett GL, Graham CE, Mauldin DM: Morton’s interdigital neuroma: A comprehensive treatment protocol. Foot Ankle Int 1995;16:760-763.