Score: 0%
Advanced Orthopedic Mock Exam (Set B3CDB8)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
of 100
Which structure is most at risk when exposing the most lateral aspect of the medial window (identified by the arrows in Figure 30)? 29

Which structure is most at risk when exposing the most lateral aspect of the medial window (identified by the arrows in Figure 30)? 29
1
Corona mortis
2
Tibial division, sciatic nerve
3
Sciatic nerve, peroneal division
4
Fifth lumbar nerve root
5
Kocher-Langenbeck approach
- Corona mortis
QUESTION 2 OF 50
A mutation in which of the following genes causes a disturbance in normal limb outgrowth patterning:
1
C BFA1
2
C OMP
3
C OL1A1
4
P63
5
VDR3
P63 is an important factor in normal limb outgrowth patterning. The other factors are involved with common disorders:
C BFA1: C leidocranial dysplasia
C OMP: Multiple epiphyseal dysplasia
C OL1A1: Osteogenesis imperfecta (easy to remember type I collagen) VDR3: Osteoporosis (easy to remember vitamin D receptor)
C orrect Answer: P63
C BFA1: C leidocranial dysplasia
C OMP: Multiple epiphyseal dysplasia
C OL1A1: Osteogenesis imperfecta (easy to remember type I collagen) VDR3: Osteoporosis (easy to remember vitamin D receptor)
C orrect Answer: P63
QUESTION 3 OF 50
A patient with deficient anteroinferior bone stock undergoes a Latarjet procedure that transfers a portion of the coracoid to the glenoid rim and secures it with two screws. After surgery, the patient reports numbness on the anterolateral forearm. To verify the diagnosis, what muscle should be tested for strength?
1
Axillary
2
Abductor pollicis brevis
3
Supinator
4
Triceps
5
Biceps
A Latarjet procedure is similar to a Bristow procedure, but with the Latarjet procedure a larger portion of the coracoid is transferred to the scapular neck at the anteroinferior glenoid. As in a Bristow procedure, if the fragment is pulled or twisted during the dissection or during fixation, the musculocutaneous nerve can be injured. With loss of biceps function, elbow flexion and forearm supination will be weaker.
REFERENCES: Ho E, Cofield RH, Balm MR, Hattrup SJ, Rowland CM: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
Boardman ND 3rd, Cofield RH: Neurologic complications of shoulder surgery. Clin Orthop 1999;368:44-53.
Allain J, Goutallier D, Glorion C: Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 1998;80:841-852.
REFERENCES: Ho E, Cofield RH, Balm MR, Hattrup SJ, Rowland CM: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
Boardman ND 3rd, Cofield RH: Neurologic complications of shoulder surgery. Clin Orthop 1999;368:44-53.
Allain J, Goutallier D, Glorion C: Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 1998;80:841-852.
QUESTION 4 OF 50
If the scan shows metastatic, noncontiguous lesions throughout the thoracic spine without epidural spinal cord compression with no known primary lesion, what is the next step in establishing a diagnosis?
1
Open biopsy of the spine lesion
2
Image-guided biopsy
3
Bone marrow aspirate of the ilium
4
CT scan of the chest, abdomen, and pelvis
5
Urine electrolytes
_
_
_
QUESTION 5 OF 50
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of
1
excision of the distal clavicle.
2
open reduction and internal fixation with intramedullary partial threaded pins.
3
open reduction and internal fixation with a reconstruction plate, screws, and bone grafting.
4
bone grafting and use of heavy sutures to secure the clavicle to the coracoid.
5
observation and nonsteroidal anti-inflammatory drugs.
The radiograph shows a displaced type II distal clavicle fracture with nonunion. Because the patient’s symptoms are minimal, the injury can be treated like a grade III acromioclavicular separation. Present management should consist of ice, anti-inflammatory drugs, activity modification, and perhaps physical therapy. If nonsurgical management fails to provide relief, the surgical options are varied with no uniformity in the literature regarding surgical treatment of this injury.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Craig EV: Fractures of the clavicle, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 428-482.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Craig EV: Fractures of the clavicle, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 428-482.
QUESTION 6 OF 50
When nonvascularized cortical allografts lose mechanical strength during the first year following surgery, it is most likely due to:
1
Revascularization
2
Failure of the graft to incorporate
3
Infection
4
Complex regional pain syndrome
5
Failure to provide initial structural support
Nonvascularized cortical grafts may provide immediate structural support but lose mechanical strength over the first few months. Loss of mechanical strength is due to the revascularization process, which causes osteoporosis and subsequent graft weakening. The process requires resorption of at least some graft bone to allow ingrowth of blood vessels and takes a significantly longer period of time in cortical bone than in cancellous bone
QUESTION 7 OF 50
Which of the following describes the inheritance pattern of Gaucher's disease:
1
Autosomal dominant
2
Autosomal recessive
3
X-linked dominant
4
X-linked recessive
5
Sporadic
Structural defects are usually transmitted by an autosomal-dominant pattern. In contrast, with metabolic or enzyme deficiencies, the condition is usually transmitted in an autosomal-recessive pattern.
Remember the major autosomal-recessive conditions: Sickle cell disease
Osteogenesis imperfecta (Types II, III)
Hypophosphatasia Homocystinuria Gaucher's disease
Remember the major autosomal-recessive conditions: Sickle cell disease
Osteogenesis imperfecta (Types II, III)
Hypophosphatasia Homocystinuria Gaucher's disease
QUESTION 8 OF 50
Exposure of tendons to ciprofloxacin in vitro causes all of the following except:
1
A decrease in fibroblast proliferation
2
An increase in proteoglycan synthesis
3
A decrease in proteoglycan synthesis
4
An increase in matrix degrading proteolytic activity
5
A decrease in collagen synthesis
C iprofloxacin was shown to cause a decrease in fibroblast proliferation, proteoglycan synthesis, and collagen synthesis. Matrix degrading proteolytic activity was increased.
QUESTION 9 OF 50
What is the most common complication after surgical management of chronic exertional compartment
syndrome (CECS) in the pediatric (≤18 years) population?
syndrome (CECS) in the pediatric (≤18 years) population?
1
Recurrent CECS
2
Infection
3
Neurologic dysfunction
4
Hematoma or seroma formation
No detailed explanation provided for this question.
QUESTION 10 OF 50
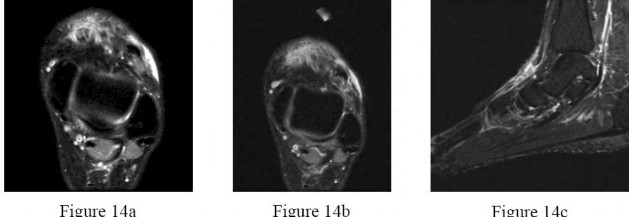
Figures 14a through 14c are the MRI scans of a 37-year-old woman who sustained a traumatic laceration to the anterior aspect of the ankle. The wound was closed in the emergency department. On examination,she has a foot drop and ambulates with a steppage gait. With successful surgical repair, what is the most common long-term residual?
---

---
1
Numbness in the foot
2
Persistent foot drop
3
Persistent ankle pain
4
Decreased dorsiflexion strength
5
Use of an ankle-foot orthosis for ambulation
Anterior tendon disruption has been described in association with direct trauma, gout,inflammatory arthritis, local steroid injections, and diabetes. When a
rupture is accurately diagnosed in younger, healthy, active patients, surgical repair has been recommended. Surgical repair results in improved patient satisfaction; however, isokinetic testing has shown decreased dorsiflexion and inversion strength compared with the uninvolved side. Numbness can result from missed superficial nerve laceration. Persistent foot drop and use of an ankle-foot orthosis are more frequently seen in chronic missed injuries or with nonsurgical management.
---
rupture is accurately diagnosed in younger, healthy, active patients, surgical repair has been recommended. Surgical repair results in improved patient satisfaction; however, isokinetic testing has shown decreased dorsiflexion and inversion strength compared with the uninvolved side. Numbness can result from missed superficial nerve laceration. Persistent foot drop and use of an ankle-foot orthosis are more frequently seen in chronic missed injuries or with nonsurgical management.
---
QUESTION 11 OF 50
Which of the following drugs is a selective estrogen receptor modulator:
1
Fosamax (alendronate sodium tablets, Merck & Co., Inc.)
2
Progestin
3
Aredia (pamidronate disodium for injection, Novartis Pharmaceuticals Corporation)
4
Evista (raloxifene, Eli Lilly and Company)
5
Alendronate sodium
A new class of selective estrogen receptor modulator acts as an antagonist in breast tissue and an agonist in bone. Raloxifene selectively stimulates estrogen receptors in bone and is an antagonist in breast tissue.
Progestin used in conjunction with estrogen opposes the action of estrogen and lowers the risk of endometrial cancer that might occur with estrogen therapy alone.
Aredia, Fosamax, and alendronate are biphosphonates that inhibit osteoclasts, thereby decreasing bone resorption.Correct
Answer: Evista (raloxifene, Eli Lilly and Company)
Progestin used in conjunction with estrogen opposes the action of estrogen and lowers the risk of endometrial cancer that might occur with estrogen therapy alone.
Aredia, Fosamax, and alendronate are biphosphonates that inhibit osteoclasts, thereby decreasing bone resorption.Correct
Answer: Evista (raloxifene, Eli Lilly and Company)
QUESTION 12 OF 50
A 15-day-old boy presents with deformity of the right hand. The boy was delivered prematurely and underwent an urgent arterial switch for transposition of great vessels. The patient is in stable condition. He has a radial club hand, and because the radial head cannot be palpated, total absence of radius is suspected. The thumb is absent and the index finger has camptodactyly. The forearm is short compared to the left side, and the patient flexes his elbow upon stimulation. Spontaneous finger motion is also present. A thorough physical examination is performed and a set of investigations is ordered. The results are as follows: complete blood count 10,000 mcu/L; platelet 254 254×103 mcu/L; neutophils 50%; Hb 14.2 mg/dL; lymphocytes
40%; Hct 45; and monocytes 10%. No renal abnormalities were noted on ultrasonogram of the abdomen. A radiograph of the spine is normal.
Diagnosis is:
40%; Hct 45; and monocytes 10%. No renal abnormalities were noted on ultrasonogram of the abdomen. A radiograph of the spine is normal.
Diagnosis is:
1
Vertebral defects, anal atresia, tracheoesophageal fistula with esophageal atresia, and radial and renal anomalies (VATER)
2
Abnormalities of vertebrae, anus, cardiovascular tree, trachea, esophagus, renal system, and limb buds (VAC TERL)
3
Thrombocytopenia absent radii (TAR) syndrome
4
Holt-Oram syndrome
5
Fanconiâs anemia
The patient has a radial club hand with a cardiac defect. Because the spine radiograph is normal, the diagnosis cannot be VATER or VAC TERL anomaly as both involve vertebrae. Blood work up is normal, making this diagnosis Holt-Oram syndrome.
QUESTION 13 OF 50
The chances of an arthroplasty revision becoming re-infected by a different organism or the initial infection after a two-stage revision is approximately:
1
5%
2
10%
3
20%
4
40%
5
50%
In one series, 23% of arthroplasty revisions became re-infected by a different organism even after a two-stage revision. However, re-infection is usually, although not always, caused by the same microorganism that caused the initial infection. Once the white blood cell count, sedimentation rate, and C-reactive protein count return to normal, it is usually safe to re-implant the prosthesis
QUESTION 14 OF 50
Using a 5° angle trunk rotation (ATR) as a positive screening threshold for detection of curves with a C obb angle over 20° is characterized by:
1
A high degree of sensitivity and specificity
2
A high degree of sensitivity but low specificity
3
A high degree of specificity but low sensitivity
4
A low degree of sensitivity and specificity
5
No predictable relationship to C obb angle
Use of a 5° ATR threshold for detection of curves with a C obb angle over 20° has a sensitivity of 98%, but a specificity of only
64%.
64%.
QUESTION 15 OF 50
Figure 24 shows the radiograph of a 10-year-old boy who sustained a valgus injury to the knee. Examination reveals grade III medial laxity. Initial management should consist of
1
an MRI scan.
2
stress radiographs of the knee.
3
activities as tolerated.
4
a hinged range-of-motion brace.
5
a knee immobilizer.
Based on the mechanism of injury and findings of medial laxity, the most likely diagnosis is injury to either the growth plate or the medial collateral ligament. With the open physeal plate, this area of injury is presumed present until proven otherwise; therefore, stress radiographs should be obtained before implementing any treatment or ordering more extensive and expensive tests.
REFERENCES: DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994,
vol 3, pp 406-432.
Clanton TO, DeLee JC, Sanders B, Neidre A: Knee ligament injuries in children. J Bone Joint Surg Am 1979;61:1195-1201.
Torg JS, Pavlov H, Morris VB: Salter-Harris type III fracture of the medial femoral condyle occurring in the adolescent athlete. J Bone Joint Surg Am 1981;63:586-591.
REFERENCES: DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994,
vol 3, pp 406-432.
Clanton TO, DeLee JC, Sanders B, Neidre A: Knee ligament injuries in children. J Bone Joint Surg Am 1979;61:1195-1201.
Torg JS, Pavlov H, Morris VB: Salter-Harris type III fracture of the medial femoral condyle occurring in the adolescent athlete. J Bone Joint Surg Am 1981;63:586-591.
QUESTION 16 OF 50
A 16-year-old female high school soccer player presents with more than one year of bilateral anterior and lateral lower extremity pain, tightness and a heavy feeling in her lower legs that starts 5 minutes after she begins running and resolves about 10 to 15 minutes after she stops. She describes feeling as though her foot slaps down on the ground when she is running. She failed extensive nonsurgical management and was ultimately indicated for surgery. At the time of endoscopically assisted treatment of this condition, damage to the structure identified by an asterisk in Figure 1 would result in what complication?
21
21
1
Postoperative hematoma
2
Medial leg numbness
3
Weakness of foot eversion
4
Dorsal foot numbness
chronic exertional compartment syndrome is commonly seen in running athletes and causes a constellation of lower leg pain, weakness and/or
numbness/paresthesias. It is an exercise-induced condition that is thought to result from muscle swelling during activity and
resultant hypoperfusion to the muscles and nerves within the compartment. The description of this patient, with symptoms in the anterior and lateral areas of her lower legs and the foot slap that she describes, indicates symptoms localized to the anterior and lateral compartments as opposed to posterior compartment symptoms. The anterior and lateral compartments would have been released in this patient. The structure seen lays between two released muscular compartments over the intermuscular septum and is the superficial peroneal nerve, which pierces the fascia 10 to 12 cm proximal to the tip of the lateral malleolus.
The structure that would cause medial leg numbness would be injury to the saphenous nerve. Her symptom description is not consistent with posterior compartment syndrome, and these compartments would not have been released at the time of surgery. The structure is not a blood vessel.
numbness/paresthesias. It is an exercise-induced condition that is thought to result from muscle swelling during activity and
resultant hypoperfusion to the muscles and nerves within the compartment. The description of this patient, with symptoms in the anterior and lateral areas of her lower legs and the foot slap that she describes, indicates symptoms localized to the anterior and lateral compartments as opposed to posterior compartment symptoms. The anterior and lateral compartments would have been released in this patient. The structure seen lays between two released muscular compartments over the intermuscular septum and is the superficial peroneal nerve, which pierces the fascia 10 to 12 cm proximal to the tip of the lateral malleolus.
The structure that would cause medial leg numbness would be injury to the saphenous nerve. Her symptom description is not consistent with posterior compartment syndrome, and these compartments would not have been released at the time of surgery. The structure is not a blood vessel.
QUESTION 17 OF 50
The lateral arm flap is based on what arterial supply?
1
Posterior radial collateral
2
Anterior radial collateral
3
Brachial
4
Subscapular
5
Circumflex scapular
The lateral arm flap is based on the posterior radial collateral artery, a branch of the profunda brachial artery.
REFERENCES: Katsaros J, Tan E, Zoltie N: The use of the lateral arm flap in upper limb surgery. J Hand Surg 1991;16:598-604.
Katsaros J, Schusterman M, Beppu M, et al: The lateral upper arm flap: Anatomy and clinical applications. Ann Plast Surg 1984;12:489-499.
REFERENCES: Katsaros J, Tan E, Zoltie N: The use of the lateral arm flap in upper limb surgery. J Hand Surg 1991;16:598-604.
Katsaros J, Schusterman M, Beppu M, et al: The lateral upper arm flap: Anatomy and clinical applications. Ann Plast Surg 1984;12:489-499.
QUESTION 18 OF 50
Six weeks after open reduction internal fixation of a closed tibial pilon fracture, a patient has a draining wound with surrounding erythema and swelling. Radiographs show lucency around screws. What is the most appropriate treatment sequence?
1
Start IV antibiotics, obtain wound swab for culture, perform irrigation and debridement and retain hardware
2
Start IV antibiotics, obtain deep soft tissue and bone cultures in OR, perform irrigation and debridement and remove hardware
3
Obtain wound swab for culture, start IV antibiotics, perform irrigation and debridement and remove hardware
4
Obtain deep bone and soft tissue cultures in OR, start IV antibiotics, perform irrigation and debridement and remove hardware
Management of acutely infected wounds is primarily surgical. Osteomyelitis frequently involves Orthopaedic hardware, which would ideally be removed or replaced given biofilm involvement. Multiple operative cultures of fluid collections, soft tissues and bone should routinely be obtained. Culture yield is highest if cultures are obtained before empiric antibiotic treatment is started. Tissue samples are greatly preferred to swabs, which are notoriously inaccurate.
QUESTION 19 OF 50
of 100
The asterisks on Figures 98a through 98c represent which anatomic structure?
A
B
C



The asterisks on Figures 98a through 98c represent which anatomic structure?
A
B
C
1
Medial head of the gastrocnemius
2
Lateral head of the gastrocnemius
3
Semimembranosus
4
Popliteus
The popliteus muscle arises from the posteromedial part of the tibia, and the tendon continues to attach to the lateral femoral condyle. The tendon is an intra-articular, extra synovial structure coursing through the popliteus hiatus, then deep to the fibular collateral ligament before inserting in the anterior portion of the popliteal sulcus.
RECOMMENDED READINGS
1. Clarke HD, Scott WN, Insall JN, et al. Anatomy. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:3-66.
2. Miller TT: Magnetic resonance imaging of the knee. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:201-224.
RECOMMENDED READINGS
1. Clarke HD, Scott WN, Insall JN, et al. Anatomy. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:3-66.
2. Miller TT: Magnetic resonance imaging of the knee. In: Insall JN, Scott WN, eds. Surgery of the Knee. Vol 1. 4th ed. Philadelphia, PA: Churchill Livingstone; 2006:201-224.
QUESTION 20 OF 50
A 37-year-old man has had isolated chronic knee swelling for the past 6 months. He denies any history of specific trauma. Examination reveals a large effusion with a stable knee, but the remainder of the examination is normal. Plain radiographs are unremarkable. An MRI scan reveals a large effusion without meniscal injury. An arthroscopic image of the suprapatellar pouch is shown in Figure 23. What is the most likely diagnosis?
1
Septic arthritis
2
Chondromalacia of the medial femoral condyle
3
Synovial cell sarcoma
4
Rheumatoid arthritis
5
Pigmented villonodular synovitis (PVNS)
The history and physical examination are consistent with a monoarticular joint condition but not typical of joint sepsis. The arthroscopic appearance of brownish proliferative synovium is typical of PVNS. PVNS is a monoarticular synovial disease of unknown etiology and is treated with total synovectomy. The proliferative synovitis is not consistent with chondromalacia. Synovial cell sarcoma is an extracapsular disease. Rheumatoid arthritis typically is polyarticular, and the synovial appearance is not associated with hemosiderin deposition.
REFERENCES: Flandry FC, Hughston JC, Jacobson KE, Barrack RL, McCann SB, Kurtz DM: Surgical treatment of diffuse pigmented villonodular synovitis of the knee. Clin Orthop 1994;300:183-192.
Zvijac JE, Lau AC, Hechtman KS, Uribe JW, Tjin-A-Tsoi EW: Arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 1999;15:613-617.
REFERENCES: Flandry FC, Hughston JC, Jacobson KE, Barrack RL, McCann SB, Kurtz DM: Surgical treatment of diffuse pigmented villonodular synovitis of the knee. Clin Orthop 1994;300:183-192.
Zvijac JE, Lau AC, Hechtman KS, Uribe JW, Tjin-A-Tsoi EW: Arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 1999;15:613-617.
QUESTION 21 OF 50
_AL-Madena Copy_
A 220-lb high school basketball player injured his knee while landing after a rebound. Figure 61 shows a lateral view of the knee. This fracture is associated with which of the following complications?
A 220-lb high school basketball player injured his knee while landing after a rebound. Figure 61 shows a lateral view of the knee. This fracture is associated with which of the following complications?
1
Limb-length discrepency
2
Varus deformity of the proximal tibia
3
Compartment syndrome
4
Genu procurvatum
5
Ligamentous instability of the knee
There is a high incidence of compartment syndrome seen in type III tibial tubercle fractures. Fasciotomy should be considered at the time of initial repair. Type III tibial tubercle fractures extending through the joint are often associated with meniscal injuries, which must be repaired. Delayed complications included recurvatum and refracture. Its association with Osgood-Schlatter’s disease has not been proven. This is a fracture that occurs in later adolescence, so significant limb-length discrepencies are unusual after this fracture.
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fracture of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Sponseller PE, Beaty JH: Fractures and dislocations about the knee, in Rockwood CA, Wilkins KE,
Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott Raven, 1996, pp 1273-1281.
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fracture of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Sponseller PE, Beaty JH: Fractures and dislocations about the knee, in Rockwood CA, Wilkins KE,
Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott Raven, 1996, pp 1273-1281.
QUESTION 22 OF 50
The clinical photograph of the hand of a 72-year-old woman who sustained a
2. laceration of the flexor pollicis longus in her thumb is shown in Figure 45. She
3. cannot actively flex the interphalangeal joint. Which pulley, in addition to the
4. oblique pulley, has been lacerated?
5. 1- A-1
6. 2- A-2
7. 3- A-3
8. 4- A-4
9. 5- A-5
2. laceration of the flexor pollicis longus in her thumb is shown in Figure 45. She
3. cannot actively flex the interphalangeal joint. Which pulley, in addition to the
4. oblique pulley, has been lacerated?
5. 1- A-1
6. 2- A-2
7. 3- A-3
8. 4- A-4
9. 5- A-5
1
laceration of the flexor pollicis longus in her thumb is shown in Figure 45. She
2
cannot actively flex the interphalangeal joint. Which pulley, in addition to the
3
oblique pulley, has been lacerated?
4
1- A-1
5
2- A-2
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Doyle JR, Blythe WF: Anatomy of the flexor tendon sheath and pulleys of the thumb. J Hand Surg 1977;2:149-151.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Doyle JR, Blythe WF: Anatomy of the flexor tendon sheath and pulleys of the thumb. J Hand Surg 1977;2:149-151.
#
QUESTION 23 OF 50
A 29-year-old man reports severe knee instability and popliteal pain. History reveals that he had polio of the left lower extremity as a child and has been brace-free his entire life. Examination reveals that he walks with 40° of knee hyperextension and has a fixed ankle equinus deformity of 30° . He has no active motors about the knee or ankle. Which of the following methods will provide knee stability and pain relief?
1
Knee-ankle-foot orthosis with locking joints
2
Knee and ankle fusion
3
Soft-tissue release of the ankle and a locked knee orthosis
4
Soft-tissue release of the ankle and a knee-ankle-foot orthosis with a locked ankle and drop-lock knee joint
5
Ankle fusion and a knee-ankle-foot orthosis
The ankle equinus allows the patient to keep his weight-bearing line anterior to the axis of the hyperextended knee joint. With time, pain has developed because of continued stretching and now incompetence of the posterior capsule of the knee joint. Several soft-tissue and bony procedures have been designed to provide knee stability in this situation; however, the results have been either short-lived or inconsistent. Tenodeses, capsular plications, and bony blocks have had limited success and generally fail over time. Current orthotic technology makes soft-tissue release and orthotic control the most predictable option. To decrease the hyperextension moment on the knee joint, the ankle deformity also must be corrected. The most predictable method of achieving stability and diminished pain during walking is with soft-tissue release of the ankle and a knee-ankle-foot orthosis with a locked ankle and drop-lock knee joint.
REFERENCE: Michael JW: Lower limb orthoses, in Goldberg B, Hsu JD (eds): Atlas of Orthoses and Assistive Devices. St Louis, MO, Mosby, 1997, pp 209-224.
REFERENCE: Michael JW: Lower limb orthoses, in Goldberg B, Hsu JD (eds): Atlas of Orthoses and Assistive Devices. St Louis, MO, Mosby, 1997, pp 209-224.
QUESTION 24 OF 50
Which of the following statements best characterizes the natural history of metatarsus adductus in a newborn:
1
Metatarsus adductus is likely to become fixed if not treated with casts.
2
Metatarsus adductus is likely to become fixed if not treated by 6 months.
3
Metatarsus adductus is likely to become fixed if not surgically corrected.
4
Metatarsus adductus is likely to later develop hindfoot equinus.
5
Most infants will improve spontaneously.
Virtually all patients with metatarsus adductus will improve with time in the absence of active treatment.
C asts are not needed for the majority of cases because spontaneous improvement is by far the most common outcome. Reverse last shoes are not needed in the majority of patients with metatarsus adductus.
Most patients will not need surgery.
Equinus of the hindfoot is not part of the pathology in metatarsus adductus.
C asts are not needed for the majority of cases because spontaneous improvement is by far the most common outcome. Reverse last shoes are not needed in the majority of patients with metatarsus adductus.
Most patients will not need surgery.
Equinus of the hindfoot is not part of the pathology in metatarsus adductus.
QUESTION 25 OF 50
of 100
The video in Figure 56 depicts a 20-year-old right-hand-dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted. What is the most appropriate course of treatment?

The video in Figure 56 depicts a 20-year-old right-hand-dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted. What is the most appropriate course of treatment?
1
Triangular fibrocartilage complex (TFCC) repair
2
Lunotriquetral fusion
3
Distal radioulnar joint (DRUJ) tenodesis
4
Extensor carpi ulnaris (ECU) tendon sheath reconstruction
Upon examination, this patient is exhibiting dislocation of the ECU tendon because of a disrupted sheath. He has failed nonsurgical measures, so surgery that would involve either direct repair or reconstruction of the tendon sheath is indicated. An option for reconstruction is to use a portion of the extensor retinaculum as a sheath substitute. Deepening of the ECU tendon groove at the distal ulna with direct repair of the sheath is another option, although a 2016 paper by Ghatan and associates did not find depth of the groove as a risk factor for subluxation. TFCC repair, lunotriquetral fusion, and DRUJ tenodesis are not appropriate because the examination clearly shows ECU tendon dislocation. TFCC and lunotriquetral ligament tears can occur along with ECU tendon dislocation, but no other examination findings suggest these conditions for this patient.
RECOMMENDED READINGS
4. [MacLennan AJ, Nemechek NM, Waitayawinyu T, Trumble TE. Diagnosis and anatomic reconstruction of extensor carpi ulnaris subluxation. J Hand Surg Am. 2008 Jan;33(1):59-64. doi: 10.1016/j.jhsa.2007.10.002. PubMed PMID: 18261666. ](http://www.ncbi.nlm.nih.gov/pubmed/18261666)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18261666)
5. [Allende C, Le Viet D. Extensor carpi ulnaris problems at the wrist--classification, surgical treatment and results. J Hand Surg Br. 2005 Jun;30(3):265-72. Epub 2005 Apr 7.](http://www.ncbi.nlm.nih.gov/pubmed/15862366)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15862366)
6. [Inoue G, Tamura Y. Surgical treatment for recurrent dislocation of the extensor carpi ulnaris tendon. J Hand Surg Br. 2001 Dec;26(6):556-9. PubMed PMID: 11884112. ](http://www.ncbi.nlm.nih.gov/pubmed/11884112)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11884112)
7. [Ghatan AC, Puri SG, Morse KW, Hearns KA, von Althann C, Carlson MG. Relative Contribution of the Subsheath to Extensor Carpi Ulnaris Tendon Stability: Implications for Surgical Reconstruction and Rehabilitation. J Hand Surg Am. 2016 Feb;41(2):225-32. doi: 10.1016/j.jhsa.2015.10.024. Epub 2015 Dec 12. PubMed PMID: 26691954. ](http://www.ncbi.nlm.nih.gov/pubmed/26691954)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26691954)
RECOMMENDED READINGS
4. [MacLennan AJ, Nemechek NM, Waitayawinyu T, Trumble TE. Diagnosis and anatomic reconstruction of extensor carpi ulnaris subluxation. J Hand Surg Am. 2008 Jan;33(1):59-64. doi: 10.1016/j.jhsa.2007.10.002. PubMed PMID: 18261666. ](http://www.ncbi.nlm.nih.gov/pubmed/18261666)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18261666)
5. [Allende C, Le Viet D. Extensor carpi ulnaris problems at the wrist--classification, surgical treatment and results. J Hand Surg Br. 2005 Jun;30(3):265-72. Epub 2005 Apr 7.](http://www.ncbi.nlm.nih.gov/pubmed/15862366)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15862366)
6. [Inoue G, Tamura Y. Surgical treatment for recurrent dislocation of the extensor carpi ulnaris tendon. J Hand Surg Br. 2001 Dec;26(6):556-9. PubMed PMID: 11884112. ](http://www.ncbi.nlm.nih.gov/pubmed/11884112)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11884112)
7. [Ghatan AC, Puri SG, Morse KW, Hearns KA, von Althann C, Carlson MG. Relative Contribution of the Subsheath to Extensor Carpi Ulnaris Tendon Stability: Implications for Surgical Reconstruction and Rehabilitation. J Hand Surg Am. 2016 Feb;41(2):225-32. doi: 10.1016/j.jhsa.2015.10.024. Epub 2015 Dec 12. PubMed PMID: 26691954. ](http://www.ncbi.nlm.nih.gov/pubmed/26691954)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26691954)
QUESTION 26 OF 50
Which of the following types of bone behaves in an isotropiCmanner when loaded in different directions:
1
Lamellar bone
2
Woven bone
3
Cortical bone
4
Cancellous bone
5
Plexiform bone
Woven bone is immature bone that is found in newborns, fracture callus, and the metaphyses of growing bone. In woven bone, the collagen fibers are oriented in a completely random fashion. When woven bone is loaded, it performs in an isotropiCmanner. The other types of bone (lamellar, cortical, cancellous, and plexiform) contain collagen that is oriented along the long axis of the bone and cause the bone to perform anisotropically.
QUESTION 27 OF 50
What is the most common complication following surgical treatment of a displaced talar neck fracture?
1
Osteonecrosis
2
Varus malunion
3
Posttraumatic arthritis
4
Fracture delayed union/nonunion
5
Wound dehiscence/delayed wound healing
The most frequent complication is posttraumatic arthritis. With talar neck fractures,osteonecrosis is relatively common, occurring in up to 50% of patients. Fracture nonunion occurs in 10%to 12% of patients. Varus malunion can occur with medial comminution. Wound dehiscence and deep infection are much less frequently encountered.
QUESTION 28 OF 50
-What is the optimal initial treatment for his orthopaedic injuries?
1
Irrigation and débridement of the open fracture and reamed intramedullary nailing of the femoral and tibial fractures
2
Irrigation and débridement of the open fracture, reamed intramedullary nailing of the femur,and external fixation of the tibia
3
Irrigation and débridement of the open fracture and external fixation of both fractures
4
Irrigation and débridement of the open fracture, a reamed femoral nail, and an unreamed tibial nail
5
Irrigation and débridement of the open fracture in the ICU and a calcaneal traction pin
No detailed explanation provided for this question.
QUESTION 29 OF 50
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
1
lateral placement, directly within the temporalis muscle.
2
within the lateral third of the superior orbital rim.
3
lateral to the superior orbital rim.
4
medial third of the superior orbital rim.
5
lateral between the temporalis muscle and zygomatic temporal nerve.
Halo fixation is the most rigid form of cervical orthosis but complications can arise from improper placement of the fixation pins. A relatively safe zone for anterior pin placement is located 1 cm above and within the lateral third of the superior orbital rim. This position avoids the supraorbital and supratrochlear nerves over the medial one third of the orbit. The more lateral positions in the temporal fossa have very thin bone and can interfere with the muscles of mastication.
QUESTION 30 OF 50
A 34-year-old otherwise healthy male is involved in a motor vehicle collision and sustains the injuries shown in the images below. His initial lactate is 8 and blood pressure is 90/50. He receives 2 liters
of normal saline followed by 2 units of crossmatched packed red blood cells, plasma and platelets. His repeat lactate just prior to being taken to the operating room is 7. What is the most appropriate treatment at this time?


of normal saline followed by 2 units of crossmatched packed red blood cells, plasma and platelets. His repeat lactate just prior to being taken to the operating room is 7. What is the most appropriate treatment at this time?
1
Unreamed femoral intramedullary nailing; open reduction and internal fixation of the pelvis
2
External fixation of the femur and pelvis
3
Reamed intramedullary nailing of the femur; external fixation of the pelvis
4
External fixation of the femur; open reduction and internal fixation of the pelvis
5
Splinting of the femur and external fixation of the pelvis.
The patient has multiple injuries including pelvic trauma resistant to initial resuscitative measures as evidenced by the persistently elevated lactate. External fixation of both the femur and pelvis should be employed at this time to avoid additional insult to a patient with evidence of end-organ hypoperfusion.
Early total care versus stabilization and eventual definitive fixation remains controversial. Indications to employ DCO include an injury severity score (ISS)
>40 without thoracic trauma, ISS>20 with thoracic trauma, severe pelvic/abdominal injuries and hemorrhagic shock, bilateral femur fractures, pulmonary contusions, and a base deficit >2/. Early definitive fixation can cause a "second hit" and increase the risk for acute respiratory distress syndrome (ARDS) and multi-organ failure.
D'Alleyrand et al. review the current evidence and practical applications of early appropriate care. They conclude that controversy continues regarding which "borderline" patients benefit from DCO and the ideal timing of fracture fixation surgery. They state that patients with closed head injuries, poor response to resuscitation, and poor ventilator parameters are good candidates for DCO.
Pape et al. review the timing of fracture fixation in polytrauma patients. They conclude that DCO, which uses external fixation as a primary tool, is most appropriate for patients in severe hemorrhagic shock or any other life-threatening condition.
Figure A demonstrates a pelvic ring injury with widening of pubic symphysis, associated anterior column acetabular fracture, and widening of the left SI joint. Figure B demonstrates a comminuted femoral shaft fracture.
Incorrect Answers:
Answers 1, 3, 4: All have definitive fixation of either the pelvis or femur that may lead to a "second hit".
Answer 5: Splinting of the femur would limit the ability to mobilize the patient.
Additionally, continued motion at the fracture site may potentiate local and systemic inflammation.
Early total care versus stabilization and eventual definitive fixation remains controversial. Indications to employ DCO include an injury severity score (ISS)
>40 without thoracic trauma, ISS>20 with thoracic trauma, severe pelvic/abdominal injuries and hemorrhagic shock, bilateral femur fractures, pulmonary contusions, and a base deficit >2/. Early definitive fixation can cause a "second hit" and increase the risk for acute respiratory distress syndrome (ARDS) and multi-organ failure.
D'Alleyrand et al. review the current evidence and practical applications of early appropriate care. They conclude that controversy continues regarding which "borderline" patients benefit from DCO and the ideal timing of fracture fixation surgery. They state that patients with closed head injuries, poor response to resuscitation, and poor ventilator parameters are good candidates for DCO.
Pape et al. review the timing of fracture fixation in polytrauma patients. They conclude that DCO, which uses external fixation as a primary tool, is most appropriate for patients in severe hemorrhagic shock or any other life-threatening condition.
Figure A demonstrates a pelvic ring injury with widening of pubic symphysis, associated anterior column acetabular fracture, and widening of the left SI joint. Figure B demonstrates a comminuted femoral shaft fracture.
Incorrect Answers:
Answers 1, 3, 4: All have definitive fixation of either the pelvis or femur that may lead to a "second hit".
Answer 5: Splinting of the femur would limit the ability to mobilize the patient.
Additionally, continued motion at the fracture site may potentiate local and systemic inflammation.
QUESTION 31 OF 50
of 100
Figures 39a and 39b are the radiographs of a 60-year-old woman with elbow pain at the extremes of motion; occasional locking; flexion/extension, 30-130; pronation/supination, 60/70; and no pain on forearm rotation. She injured her elbow as a teenager and had surgery at that time. What is the best next step?


Figures 39a and 39b are the radiographs of a 60-year-old woman with elbow pain at the extremes of motion; occasional locking; flexion/extension, 30-130; pronation/supination, 60/70; and no pain on forearm rotation. She injured her elbow as a teenager and had surgery at that time. What is the best next step?
1
Debridement, capsular excision, and loose body removal
2
Unconstrained total elbow arthroplasty (TEA)
3
Radial head excision
4
Elbow arthrodesis
This patient appears to have sustained a lateral condyle fracture as a young adult. She was treated with surgical repair and now has posttraumatic arthritis. The best treatment, especially in the setting of mechanical symptoms, is debridement with capsular excision to regain motion and loose body removal. Radial head excision is not indicated because she has no pronation/supination loss or pain with forearm rotation. Elbow arthrodesis is severely limiting because of an associated inability to perform activities of daily living. Unconstrained TEA is more effectively used as a salvage for an older person who has failed debridement and has mid arc motion pain. Unconstrained elbow arthroplasty mandates near-normal elbow bony architecture and intact and normal collateral ligaments, both of which may be compromised in this case.
RECOMMENDED READINGS
48. [Papatheodorou LK, Baratz ME, Sotereanos DG. Elbow arthritis: current concepts. J Hand Surg Am. 2013 Mar;38(3):605-13. doi: 10.1016/j.jhsa.2012.12.037. Epub 2013 Feb 5. Review. PubMed PMID: 23391361. ](http://www.ncbi.nlm.nih.gov/pubmed/23391361)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23391361)
49. [Ring D. Instability after total elbow arthroplasty. Hand Clin. 2008 Feb;24(1):105-12. doi: 10.1016/j.hcl.2007.11.002. Review. PubMed PMID: 18299024. ](http://www.ncbi.nlm.nih.gov/pubmed/18299024)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18299024)
RECOMMENDED READINGS
48. [Papatheodorou LK, Baratz ME, Sotereanos DG. Elbow arthritis: current concepts. J Hand Surg Am. 2013 Mar;38(3):605-13. doi: 10.1016/j.jhsa.2012.12.037. Epub 2013 Feb 5. Review. PubMed PMID: 23391361. ](http://www.ncbi.nlm.nih.gov/pubmed/23391361)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23391361)
49. [Ring D. Instability after total elbow arthroplasty. Hand Clin. 2008 Feb;24(1):105-12. doi: 10.1016/j.hcl.2007.11.002. Review. PubMed PMID: 18299024. ](http://www.ncbi.nlm.nih.gov/pubmed/18299024)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18299024)
QUESTION 32 OF 50
A 32-year-old man has a closed mid-shaft spiral humeral fracture after a fall. After a discussion of his treatment options, he wants to proceed with surgical management. When counseling him about open reduction internal fixation (ORIF) versus intramedullary nailing (IMN), what is the primary difference in outcomes between the two procedures?
1
Lower rate of iatrogenic radial nerve injury with ORIF
2
Lower rate of shoulder complications with
3
Higher rate of union with ORIF
4
Higher rate of infection with ORIF
There has been an abundance of studies designed to compare ORIF with IMN of humeral shaft fractures. When the most well-designed and rigorous studies are pooled and reviewed, the only consistent difference that can be found is a higher incidence of shoulder complications with IMN compared with ORIF. No significant differences have been shown with regard to nerve injury, union, or infection.
Recommended reading:
1. [Carroll EA, Schweppe M, Langfitt M, Miller AN, Halvorson JJ. Management of humeral shaft fractures. J Am Acad Orthop Surg. 2012 Jul;20(7):423-33. doi: 10.5435/JAAOS-20-07-423. Review. PubMed PMID: ](https://www.ncbi.nlm.nih.gov/pubmed/22751161)22751161.
2. [Zhao JG, Wang J, Wang C, Kan SL. Intramedullary nail versus plate fixation for humeral shaft fractures: a systematic review of overlapping meta-analyses. Medicine (Baltimore). 2015 Mar;94(11):e599. doi: 10.1097/MD.0000000000000599. Review. PubMed PMID: ](https://www.ncbi.nlm.nih.gov/pubmed/25789949)[2578994](https://www.ncbi.nlm.nih.gov/pubmed/25789949)
Recommended reading:
1. [Carroll EA, Schweppe M, Langfitt M, Miller AN, Halvorson JJ. Management of humeral shaft fractures. J Am Acad Orthop Surg. 2012 Jul;20(7):423-33. doi: 10.5435/JAAOS-20-07-423. Review. PubMed PMID: ](https://www.ncbi.nlm.nih.gov/pubmed/22751161)22751161.
2. [Zhao JG, Wang J, Wang C, Kan SL. Intramedullary nail versus plate fixation for humeral shaft fractures: a systematic review of overlapping meta-analyses. Medicine (Baltimore). 2015 Mar;94(11):e599. doi: 10.1097/MD.0000000000000599. Review. PubMed PMID: ](https://www.ncbi.nlm.nih.gov/pubmed/25789949)[2578994](https://www.ncbi.nlm.nih.gov/pubmed/25789949)
QUESTION 33 OF 50
A regimen of ankle bracing and supervised physical therapy:
1
Has no beneficial effect on stage II posterior tibial tendon dysfunction
2
Is helpful in relieving the pain symptoms associated with stage II posterior tibial tendon dysfunction but does not increase strength
3
C an significantly relieve pain and increase strength in stage II posterior tibial tendon dysfunction
4
Is only useful for postoperative rehabilitation after flexor digitorum longus tendon transfer and medial slide calcaneal osteotomy
5
Prevents patients from requiring surgery in only 11% of cases
In a study performed by Alvarez and colleagues, 47 patients with stage I or II posterior tibial tendon dysfunction were treated nonoperatively with either a hinged ankle-foot orthosis or foot orthosis and a supervised physical therapy program. After 10 therapy visits, 83% of patients had successful subjective and functional outcomes. Eighty-nine percent of patients were satisfied with the outcome of nonoperative treatment. This included significant improvement in visual analog scale scores and increased strength, concentrically and eccentrically. In this study, 11% of patients failed conservative treatment and required surgery.
QUESTION 34 OF 50
**ONLINE ORTHOPEDIC MCQS TRAUMA 9**
**1**. A 26-year-old woman sustained a nondisplaced femoral neck fracture and treatment consisted of use of percutaneous cannulated screws. At her 3-month follow-up visit, she reports hip pain and is unable to ambulate. A radiograph is shown in Figure 1. What is the next most appropriate treatment?
**1**. A 26-year-old woman sustained a nondisplaced femoral neck fracture and treatment consisted of use of percutaneous cannulated screws. At her 3-month follow-up visit, she reports hip pain and is unable to ambulate. A radiograph is shown in Figure 1. What is the next most appropriate treatment?
1
Bone grafting and revision open reduction and internal fixation
2
Hemiarthroplasty
3
Dynamic hip screw without angular correction
4
Valgus intertrochanteric osteotomy
5
Core decompression
Femoral neck fracture nonunion is a challenging problem for orthopaedic surgeons. Vertical fractures are more prone to nonunion due to shear stress rather than compressive forces across the fracture site. Several authors have suggested these fractures are more common in young adults due to injury type and bone composition. It is widely regarded that an effort should be made to salvage the femoral head if vascularity remains. The most common method to treat this complication is valgus intertrochanteric osteotomy of the femur. This functionally makes a vertical fracture more horizontal, converting shear into compressive forces. It also helps correct the varus position of the fracture nonunion.**
**
**
Scientific References
- : Hartford JM, Patel A, Powell J: Intertrochanteric osteotomy using a dynamic hip screw for femoral neck nonunion. J Orthop Trauma 2005;19:329-333.**
**Mathews V, Cabanela ME: Femoral neck nonunion treatment. Clin Orthop Relat Res 2004;419:57-64.**
**2****. Which of the following choices best describes the fracture pattern shown in Figures
2a through 2c?
1- Anterior column
2- Anterior wall
3- Posterior column
4- Both column
5- Transverse
PREFERRED RESPONSE: 3**
**DISCUSSION: The fracture pattern shown in the radiographs is a fracture of the posterior column. The only line interrupted on the AP pelvis is the ilioischial line. The obturator oblique view shows that the iliopectineal line is intact as is the outline of the posterior wall. The iliac oblique view shows an interruption of the ilioischial line and an intact anterior wall. Therefore, this fracture is a fracture of the posterior column.**
**REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.**
**Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1009-1149.**
**3****. The correct starting point for an external fixation half pin placed into the anterior inferior iliac spine (AIIS) is labeled by what letter in Figure 3?**
1- A
2- B
3- C
4- D
5- E
**PREFERRED RESPONSE: 1**
**DISCUSSION: Half pins placed in the AIIS are an alternative to pins placed in the iliac crest.
A strong pillar of bone runs from the AIIS to the posterior iliac crest and less soft tissue is typically present in this area. The starting point is best seen on an obturator outlet view. The obturator outlet view is a combination of the pelvic outlet view and the obturator view of Judet and Letournel. The beam is rotated “over the top” of the patient since the iliac wing is externally rotated as well as cephalad to best visualize this column of bone running from the AIIS to the posterior iliac spine. This corridor of bone will appear as a teardrop. Once the correct view is obtained, the pin should be started at least 2 cm proximal to the hip joint to avoid placing a pin within the hip capsule. Blunt dissection and a guide sleeve should be used to prevent damage to the lateral femoral cutaneous nerve. An iliac oblique view is used after the pin has been partially inserted to make sure the pin is passing superior to the superior gluteal notch, and an obturator inlet view can be used at the completion of the procedure to make sure the pin is contained within the bone for its entire length.**
**REFERENCES: Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273.**
**Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.**
**Kim WY, Hearn TC, Seleem O, et al: Effect of pin location on stability of pelvic external fixation. Clin Orthop Relat Res 1999;361:237-244.**
**4****. Figures 4a and 4b show the radiographs of a 53-year-old woman who was injured in a fall. After initial closed reduction, what is the preferred treatment for this fracture?
1- Open reduction and internal fixation of the radial head and immobilization
2- Medial collateral ligament repair
3- Radial head replacement, ulnar nerve transposition, and external fixation
4- Coronoid repair, radial head replacement, and lateral ligamentous repair
5- Nonsurgical management in a hinged elbow brace
PREFERRED RESPONSE: 4**
**DISCUSSION: This elbow fracture-dislocation involves a radial head fracture, coronoid fracture, and ulnohumeral dislocation (terrible triad). Several algorithms exist for treatment; surgical treatment is indicated. The treatment should address the radial head. Studies have shown replacement to be superior to repair in comminuted fractures. The coronoid may be addressed in unstable cases at the time of radial head excision and replacement. Lateral ligamentous repair is carried out during closure of the lateral elbow capsule. Medial ligamentous repair also may be undertaken but usually in concert with bony repair. Hinged external fixation remains an option when instability exists following bony and soft-tissue repair. Acute ulnar nerve transposition is rarely indicated.**
**REFERENCES: Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.**
**Pugh DM, Wild LM, Schemitsch EH, et al: Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am 2004;86:1122-1130.**
**5****. A 25-year-old semiprofessional football player sustains a hyperextension injury to the left foot. He is unable to bear weight. Examination reveals tenderness along the midfoot with swelling and plantar ecchymosis. Radiographs are negative. What is the next step in evaluation of this patient?
1- CT
2- MRI
3- Standing radiographs
4- Measurement of compartment pressures
5- Bone scan
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has a suspected Lisfranc sprain based on the plantar ecchymosis. The first step in diagnosis is a dynamic radiographic study. This should include a physician-assisted midfoot stress examination or standing weight-bearing radiographs to evaluate for displacement. There is no evidence of compartment syndrome, and a bone scan, CT, and MRI are expensive tests that are not warranted.**
**REFERENCES: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.**
**Hunt SA, Ropiak C, Tejwani NC: Lisfranc joint injuries: Diagnosis and treatment. Am J Orthop 2006;35:376-385.**
**6****. A 52-year-old woman slips in her bathroom and strikes her right hand on a cabinet.
She notes swelling, ecchymosis, and pain with attempted motion. There are no open wounds. Radiographs are shown in Figures 5a through 5c. What is the most
appropriate treatment?
1- Immobilization of the hand with the metacarpophalangeal (MCP) joints in flexion and the interphalangeal (IP) joints in extension
2- Immobilization of the hand with the MCP joints in extension and the IP joints in extension
3- Percutaneous pinning of the proximal phalanx
4- Open reduction and internal fixation of the proximal phalanx
5- Early motion and pain management
PREFERRED RESPONSE: 1**
**DISCUSSION: Nondisplaced transverse fractures of the phalanges are stable. Immobilization in the intrinsic plus position will prevent MCP joint stiffness. Displaced oblique fractures are more at risk for instability.**
**REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.**
**Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.**
**7****. A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?
1- Closed reduction and long arm cast immobilization
2- Closed reduction and short arm cast immobilization
3- Closed reduction and percutaneous pinning
4- Open reduction and internal fixation with Kirschner wires
5- Open reduction and internal fixation with a headless, cannulated compression screw
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has a scaphoid fracture involving the proximal pole. Surgical treatment is recommended for such fractures because of the prolonged period of cast immobilization necessary and the increased risk of delayed union, nonunion, and/or osteonecrosis with nonsurgical management. A cannulated compression screw, inserted in the central scaphoid via a dorsal approach, is biomechanically advantageous and provides greater stability for fracture healing than Kirschner wires. Recently, good outcomes have been reported with arthroscopic-assisted percutaneous fixation of nondisplaced or minimally displaced scaphoid fractures.**
**REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.**
**Chan KW, McAdams TR: Central screw placement in percutaneous screw scaphoid fixation: A cadaveric comparison of proximal and distal techniques. J Hand Surg Am 2004;29:74-79.**
**Bedi A, Jebson PJ, Hayden RJ, et al: Internal fixation of acute non-displaced scaphoid waist fractures via a limited dorsal approach: An assessment or radiographic and functional outcomes. J Hand Surg Am 2007;32:326-333.**
**McCallister WV, Knight J, Kaliappan R, et al: Central placement of the screw in simulated fractures of the scaphoid waist: A biomechanical study. J Bone Joint Surg Am 2003;85:72-77.**
**8****. A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
1- Irrigation and debridement, external fixation of the ankle and foot, traction and pinning of the femur, open reduction and internal fixation of the forearm
2- Irrigation and debridement, external fixation of the ankle, foot, and femur, splinting of the forearm
3- Irrigation and debridement and open reduction and internal fixation of the ankle and foot, intramedullary nailing of the femur, open reduction and internal fixation of the forearm
4- Irrigation and debridement and open reduction and internal fixation of the ankle and foot, intramedullary nailing of the femur, splinting of the forearm
5- Irrigation and debridement, external fixation of the foot and ankle, intramedullary nailing of the femur, open reduction and internal fixation of the forearm
PREFERRED RESPONSE: 2**
**DISCUSSION: The patient appears to be a borderline or unstable surgical patient following her initial trauma and spleenectomy (high base excess and low urine output). She needs continued resuscitation and minimal additional blood loss. This is best accomplished with irrigation and debridement of the ankle, external fixation of the ankle, foot, and femur, and splinting of the forearm. A traction pin for the femoral fracture will not control bleeding as well as an external fixator. Intramedullary nailing of the femur and open reduction and internal fixation of the forearm would be appropriate in patients that are euvolemic and stable.**
**REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.**
**Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416.**
**Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.**
**Renaldo N, Egol K: Damage-control orthopaedics: Evolution and practical applications.
Am J Orthop 2006;35:285-291.**
**9****. A 45-year-old man who is a smoker has a significant hemothorax and bilateral closed femoral fractures. On insertion of a chest tube, 1,100 mL of blood was returned. He has had 75 mL of chest tube output over the last 2 hours while being resuscitated in the ICU. His base deficit is now 2 and his urine output has been 3 mL/kg over the last hour. What is the next most appropriate step in management?
1- Continued skin traction
2- Skeletal traction of both femurs
3- External fixation of both femurs
4- Intramedullary nailing of one femur and external fixation and delayed nailing for the other femur
5- Intramedullary nailing of both femurs
PREFERRED RESPONSE: 5**
**DISCUSSION: Although this patient had a hemothorax, the bleeding has stopped and he has been resuscitated to a euvolemic status with a small base deficit and good urine output. External fixation of both femurs is an option but an unnecessary step in the treatment algorithm.**
**REFERENCES: Nork SE, Agel J, Russell GV, et al: Mortality after reamed intramedullary nailing of bilateral femur fractures. Clin Orthop Relat Res 2003;415:272-278.**
**Pape HC, Zelle BA, Hildebrand F, et al: Reamed femoral nailing in sheep: Does irrigation and aspiration of intramedullary contents alter the systemic response? J Bone Joint Surg Am 2005;87:2515-2522.**
**10****. A 47-year-old woman falls and sustains a direct blow to her middle finger. She notes pain and swelling and is unable to move the proximal interphalangeal (PIP) or distal interphalangeal (DIP) joints. Radiographs are shown in Figures 8a through 8c. Proper management should consist of
1- closed reduction and splinting in metacarpophalangeal (MCP) and PIP joint extension.
2- closed reduction and splinting in MCP joint flexion and PIP joint extension.
3- reduction and percutaneous intramedullary Kirschner wire fixation.
4- reduction and lag screw fixation.
5- buddy taping and early range of motion.
PREFERRED RESPONSE: 4**
**DISCUSSION: The oblique nature of the fracture and extension of the fracture to the condyles implies an unstable fracture. Lag screw fixation provides an excellent chance of union, and the ability to start early range of motion.**
**REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.**
**Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.**
**11****. Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in
a cast?
1- Elbow stiffness
2- Nonunion
3- Osteonecrosis
4- Varus malunion from overgrowth
5- Fishtail deformity
PREFERRED RESPONSE: 2**
**DISCUSSION: The radiographs show a lateral condyle fracture with 2 mm of displacement. As opposed to other pediatric elbow fractures, lateral condyle fractures have a higher incidence of nonunion. This may be due to minimal metaphyseal bone on the distal fragment, the intra-articular nature of the fracture, or from further displacement when treated nonsurgically. These fractures with 2 mm and greater of displacement should be treated with reduction and stabilization. Osteonecrosis and fishtail deformity may be seen in very rare cases of lateral condyle fractures. The incidence is certainly less than the rates of nonunion seen in nonsurgically treated fractures with 2 mm and greater of displacement. Varus malunion from overgrowth and elbow stiffness are more likely seen in fractures treated surgically.**
**REFERENCES: Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207.**
**Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.**
**Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.**
**12****. Which of the following is most commonly associated with an open clavicular fracture?
1- Scapulothoracic dissociation
2- Closed head injury
3- Calcaneus fracture
4- Pelvic ring injury
5- Open tibial fracture
PREFERRED RESPONSE: 2**
**DISCUSSION: Open clavicular fractures are rare and result from high-energy trauma. In a series of 20 patients with open clavicular fractures, 13 (65%) sustained a closed head injury. Fifteen (75%) had associated pulmonary injuries and 35% had a cervical or thoracic spine fracture. Only one demonstrated scapulothoracic dissociation. Screening for pulmonary and closed head injuries should be considered in the setting of traumatic open clavicular fractures.**
**REFERENCE: Taitsman LA, Nork SE, Coles CP, et al: Open clavicle fractures and associated injuries. J Orthop Trauma 2006;20:396-399.**
**13****. A 22-year-old woman injures her neck in a motor vehicle accident. Examination reveals no sensory or motor function below T8. Radiographs and an MRI scan show a burst fracture at T7. Forty-eight hours later, the bulbocavernosus reflex is present but there is no evidence of motor or sensory recovery in the lower extremities. What is the most likely diagnosis?
1- Spinal shock
2- Anterior cord syndrome
3- Cauda equina syndrome
4- Complete cord syndrome
5- Brown-Sequard syndrome
PREFERRED RESPONSE: 4**
**DISCUSSION: Spinal shock typically ends after 48 hours with the return of reflexes, including the bulbocavernosus reflex. Lack of motor or sensory recovery in the lower extremities with the return of reflexes generally indicates a complete cord syndrome.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.**
**Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1132-1133.**
**14****. A 26-year-old man falls off a motorcycle and injures his left wrist. There are no open wounds and the neurovascular examination is normal. Radiographs are shown in Figures 10a and 10b. Definitive management should consist of
1- closed reduction and casting.
2- external fixation and percutaneous pinning of the distal radius.
3- open reduction and internal fixation of the distal radius.
4- open reduction and internal fixation of the distal radius and open repair of the ulnar styloid.
5- nonbridging external fixation of the distal radius.
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has a high-energy injury with resultant comminution of the distal radius metaphysis. Cast immobilization is likely to lead to radial shortening and angulation due to the comminution. Similarly, while external fixation and pinning has been successful in the past, some loss of radial length and volar angulation is typically noted. Present plate fixation devices for the distal radius employing locking screw technology have a superior ability to resist radial shortening and dorsal angulation. Fixation of the ulnar styloid is warranted when there is distal radioulnar joint instability or significant displacement of the styloid. This is more likely to occur with a fracture at the base of the styloid. In this instance, the distal radioulnar joint does not appear to be disrupted.**
**REFERENCES: May MM, Lawton JN, Blazar PE: Ulnar styloid fractures associated with distal radius fractures: Incidence and implications for distal radioulnar joint instability. J Hand Surg Am 2002;27:965-971.**
**Nana AD, Joshi A, Lichtman DM: Plating of the distal radius. J Am Acad Orthop Surg 2005;13:159-171.**
**15****. Which of the following studies best increases the ability to diagnose femoral neck fractures in patients with femoral shaft fractures?
1- MRI
2- Fine-cut CT scan
3- Bone scan
4- AP radiograph of the femur
5- AP radiograph of the pelvis
PREFERRED RESPONSE: 2**
**DISCUSSION: Tornetta and associates and Yang and associates found that nearly half of all femoral neck fractures associated with femoral shaft fractures were being missed at their institution. On the basis of the delayed diagnosis of these injuries, a best-practice protocol was developed by the attending trauma surgeons for the evaluation of the femoral neck in patients with a femoral shaft fracture. This protocol includes a preoperative AP internal rotation radiograph of the hip, a fine-cut (2-mm) CT scan through the femoral neck (as a part of the initial trauma scan), and an intraoperative fluoroscopic lateral evaluation of the hip just prior to fixation of the femoral shaft. In addition, postoperative AP and lateral radiographs of the hip are made in the operating room to specifically evaluate the femoral neck before the patient is awakened. They found that fine-cut CT (2 mm was the best screening tool in this group of patients) identified 12 of the 13 fractures, whereas 8 of the 13 fractures were visible on the dedicated preoperative AP internal rotation hip radiographs.**
**REFERENCES: Tornetta P III, Kain MS, Creevy WR: Diagnosis of femoral neck fractures in patients with a femoral shaft fracture: Improvement with a standard protocol. J Bone Joint Surg Am 2007;89:39-43.**
**Yang KH, Han DY, Park HW, et al: Fracture of the ipsilateral neck of the femur in shaft nailing: The role of CT in diagnosis. J Bone Joint Surg Br 1998;80:673-678.**
**16****. The axis of forearm rotation occurs between what two anatomic points?
1- Radial head, radial styloid
2- Radial head, ulnar styloid
3- Radial head, ulnar head
4- Coronoid, sigmoid notch
5- Coronoid, radial styloid
PREFERRED RESPONSE: 3**
**DISCUSSION: Forearm rotation results from a complex interaction of osseous articulations and soft tissues including the radiocapitellar articulation, proximal and distal radioulnar joints, the interosseous membrane, and the adjacent forearm muscles. The rotation occurs around a longitudinal forearm axis extending from the center of the radial head proximally through the foveal region of the ulnar head distally.**
**REFERENCES: Werner FW, An KN: Biomechanics of the elbow and forearm. Hand Clin 1994;10:357-373.**
**Tynan MC, Fornalski S, McMahon PJ, et al: The effects of ulnar axial malalignment on supination and pronation. J Bone Joint Surg Am 2000;82:1726-1731.**
**17****. Figure 11 shows the radiograph of a 26-year-old man with type I diabetes mellitus who was struck by a motor vehicle. What is the most common complication associated with this pelvic fracture?
1- Infection
2- Sciatic nerve palsy
3- Heterotopic ossification
4- Deep venous thrombosis
5- Degenerative arthritis
PREFERRED RESPONSE: 4**
**DISCUSSION: The most common complication following acetabular or pelvic ring injury is deep venous thrombosis (DVT). Without prophylaxis, rates of DVT are as high as 70% to 80%. With prophylaxis, the rates are around 10%. Infection rates in surgical repair of acetabular fractures are relatively low but a history of diabetes mellitus and a significant Morel-Lavalle lesion certainly increase the risk. However, even with these two complicating factors, the rates of infection are still lower than 10%. Sciatic nerve palsy rates from the injury alone approach 20% and iatrogenic injury is usually less than 2%. Degenerative changes to the hip following this injury approach 20% to 25%, even with an anatomic reduction.**
**REFERENCES: Geerts WH, Code KI, Jay RM, et al: A prospective study of venous thromboembolism after major trauma. N Engl J Med 1994;331:1601-1606.**
**Steele N, Dodenhoff RM, Ward AJ, et al: Thromboprophylaxis in pelvic and acetabular trauma surgery: The role of early treatment with low-molecular-weight heparin. J Bone Joint Surg Br 2005;87:209-212.**
**18****. Which of the following factors is a significant predictor of reoperation following open reduction and internal fixation of intertrochanteric fractures with a sliding-compression hip-screw device?
1- Standard obliquity fracture pattern
2- Tip-apex distance of 15 mm
3- Fracture through the lateral femoral cortex
4- Sliding-compression hip-screw device with a two-hole side plate
5- Fracture of the lesser trochanter
PREFERRED RESPONSE: 3**
**DISCUSSION: As shown by Palm and associates from the Hip Fracture Study group, the integrity of the lateral femoral cortex in intertrochanteric hip fractures is a significant predictor of reoperation. Baumgartner and associates have shown that a tip-apex distance of greater than 25 mm is associated with a high risk of femoral head cut-out. Lastly, intertrochanteric hip fractures can be described as standard obliquity or reverse obliquity when describing the fracture pattern. Mechanistically, a reverse obliquity pattern is important to recognize because it reflects the presence or absence of a lateral buttress to which the proximal fracture fragment may compress.**
**REFERENCES: Palm H, Jacobsen S, Sonne-Holm S, et al: Integrity of the lateral femoral wall in intertrochanteric hip fractures: An important predictor of a reoperation. J Bone Joint Surg Am 2007;89:470-475.**
**Sadowski C, Lübbeke A, Saudan M, et al: Treatment of reverse oblique and transverse intertrochanteric fractures with use of an intramedullary nail or a 95 degrees screw-plate:
A prospective, randomized study. J Bone Joint Surg Am 2002;84:372-381.**
**Baumgaertner MR, Curtin SL, Lindskog DM, et al: The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am 1995;77:1058-1064.**
**19****. Following fixation of a displaced intra-articular fracture of the distal humerus through a posterior approach, what is the expected outcome?
1- Development of arthritic changes at 1 year
2- Restoration of full elbow range of motion
3- Loss of approximately 25% of elbow flexion strength
4- Posterolateral rotatory instability
5- Olecranon nonunion
PREFERRED RESPONSE: 3**
**DISCUSSION: Following repair of a displaced intra-articular distal humerus fracture, the ability to regain full elbow range of motion is rare. Recent reports of olecranon osteotomy have yielded healing rates of between 95% to 100%. According to McKee and associates, patients can be expected to have residual loss of elbow flexion strength of 25%.**
**REFERENCES: McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.**
**Ring D, Jupiter JB, Gulotta L: Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003;85:232-238.**
**20****. A 15-year-old boy falls from his bicycle and sustains an injury to his elbow. Prereduction radiographs are shown in Figure 12a. Closed reduction is performed without difficulty and postreduction radiographs are shown in Figure 12b. What is the next most appropriate step in treatment?
1- Conversion to cast immobilization for 6 weeks
2- Application of an articulated external fixator
3- Begin early motion as soon as pain resolves
4- Open reduction
5- MRI to assess ligament integrity
PREFERRED RESPONSE: 4**
**DISCUSSION: Elbow dislocations in children are rare injuries and usually result from a fall on an outstretched arm. The incidence of these injuries increases as patients age and concurrently the incidence of supracondylar humerus fractures decreases. In adolescent patients, simple elbow dislocations are treated with splint immobilization and the initiation of physical therapy once comfortable. The practitioner must be aware of structures that may get caught in the joint on reduction. These include the median nerve as well as the medial epicondyle. In this patient, the radiographs reveal a medial epicondyle fracture. Postreduction radiographs show the joint to be incongruous secondary to intra-articular displacement. At this point, the most appropriate treatment is to perform an open reduction and repair of the medial epicondyle fragment.**
**REFERENCES: Rasool MN: Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-1058.**
**Beaty JH: Fractures and dislocations about the elbow in children. Instr Course Lect 1992;41:373-384.**
**21****. A 7-year-old boy is seen in the emergency department with an isolated and displaced supracondylar humerus fracture and absent radial and ulnar pulses. Despite a moderately painful attempt at realignment, examination reveals that his hand remains pulseless. What is the next most appropriate step in management?
1- Order an urgent angiogram and then proceed to the OR.
2- Repeat the reduction in the emergency department and reassess.
3- Perform open reduction through an anterior approach.
4- Perform closed reduction and pinning in the OR and reassess the vascular status.
5- Perform arterial repair and then stabilize the fracture.
PREFERRED RESPONSE: 4**
**DISCUSSION: Displaced supracondylar humerus fractures in children may have associated vascular compromise. Decreased blood flow may be due to vessel injury, entrapment within the fracture site, kinking from fracture displacement, or from vessel spasm. Optimal initial treatment in the emergency department includes gentle realignment of the limb and vascular assessment. Angiography is not required in isolated injuries as the level of the vessel compromise is always at the site of the fracture. When blood flow is not restored, the next best step in treatment is to proceed urgently to the operating room. A formal closed reduction and pinning is performed, and then the vascular status is reassessed. Exploration and vascular repair is required if the hand is cool, white, and without pulses.**
**REFERENCES: Ay S, Akinci M, Kamiloglu S, et al: Open reduction of displaced pediatric supracondylar humeral fractures through the anterior cubital approach. J Pediatr Orthop 2005;25:149-153.**
**Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.**
**Dormans JP, Squillante R, Sharf H: Acute neurovascular complications with supracondylar humerus fractures in children. J Hand Surg Am 1995;20:1-4.**
**22****. A 28-year-old cowgirl was injured while herding cattle 1 week ago. A radiograph and CT scans are shown in Figures 13a through 13c. What is the most appropriate management for this injury?
1- Nonsurgical management and gradual weight bearing as tolerated
2- Nonsurgical management and restricted weight bearing
3- Placement of a pelvic binder
4- Open reduction and internal fixation of the symphysis
5- Open reduction and internal fixation of the symphysis and iliosacral screws
PREFERRED RESPONSE: 1**
**DISCUSSION: The patient has an AP I pelvic ring disruption with minimal symphyseal widening. The best treatment is nonsurgical management and weight bearing as tolerated. This will help close the anterior pelvic ring during the healing process. Pelvic binders are excellent for acute treatment of widely displaced pelvic fractures but are not recommended for long-term use. Open reduction and internal fixation is not indicated for this injury and furthermore, the posterior ring is not injured.**
**REFERENCES: Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96.**
**Templeman DC, Schmidt AH, Sems SA, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.**
**Tile M: Management, in Tile M: Fractures of the Pelvis and Acetabulum, ed 2. Philadelphia, PA, Williams and Wilkins, 1995, pp 108-134.**
**23****. As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
1- AIDS
2- Polytrauma
3- Pelvic fracture
4- Pilon fracture
5- Acute myocardial infarction (AMI)
PREFERRED RESPONSE: 4**
**DISCUSSION: Pollak and associates found that the average SF-36 score for patients who sustained a pilon fracture was significantly lower than patients with diabetes mellitus, AIDS, hypertension, asthma, migraines, pelvic fracture, polytrauma, and AMI. Moreover, patients having undergone pilon fixation scored lower on all but three of the SF-36 scales (vitality, mental health, and emotional health).**
**REFERENCE: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.**
**24****. A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb “feels” different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?
1- Serial physical examinations
2- Angiography
3- Duplex ultrasound examination
4- Ankle-brachial index (ABI)
5- Measurement of compartment pressures
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient initially has a distal third femoral fracture and a pulseless limb. The first step is to reduce the fracture and reassess the vascular status. Although the pulse returns, it feels different than the quality of the pulse in the contralateral uninjured extremity. There is a risk of a vascular injury with this fracture pattern due to tethering of the femoral vessels at the adductor hiatus; therefore, the vascular status needs further assessment since the pulses are not symmetrical. A physical examination is not very accurate in assessing whether a vascular injury is present; therefore, serial examinations are not appropriate. Angiography is very sensitive and specific but is time consuming and can cause complications secondary to the dye and the arterial puncture required to perform it. Duplex ultrasound is effective but is very operator-dependent and may not be available 24 hours a day. The ABI is easily performed and has been shown to be sensitive and specific. If the value is greater than 0.9, the negative predictive value is 99% and when the value is less than 0.9, it is 95% sensitive and 97% specific for a major arterial injury. It has been shown to be useful for blunt lower extremity injuries as well as knee dislocations.**
**REFERENCES: Levy BA, Zlowodzki MP, Graves M, et al: Screening for extremity arterial injury with the arterial pressure index. Am J Emerg Med 2005;23:689-695.**
**Abou-Sayed H, Berger DL: Blunt lower-extremity trauma and politeal artery injuries: Revisiting the case for selective arteriography. Arch Surg 2002;137:585-589.**
**Mills WJ, Barei DP, McNair P: The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: A prospective study. J Trauma 2004;56:1261-1265.**
**25****. What is the most appropriate treatment for a 50-year-old woman who sustains the injury shown in Figures 14a and 14b?
1- Total elbow arthroplasty
2- Functional hinge bracing
3- Long arm casting
4- Crossed Kirschner wires
5- Dual column plates
PREFERRED RESPONSE: 5**
**DISCUSSION: This intra-articular distal humerus fracture with displacement at the joint surface is best treated with surgical fixation. The most biomechanically sound construct is two plates applied to either column 180 degrees from one another. Elbow arthroplasty is most appropriate for low demand elderly patients.**
**REFERENCES: Schemitsch EH, Tencer AF, Henley MB: Biomechanical evaluation of methods of internal fixation of the distal humerus. J Orthop Trauma 1994;8:468-475.**
**McCarty LP, Ring D, Jupiter JB: Management of distal humerus fractures. Am J Orthop 2005;34:430-438.**
**Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement: Surgical technique. J Bone Joint Surg Am 2005;87:41-50.**
**26****. A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury?
1- Inlet and outlet views of the pelvis to better delineate the injury
2- Angiography
3- Laparotomy
4- Open reduction and internal fixation of the pelvis
5- Placement of a pelvic binder around the patient
PREFERRED RESPONSE: 5**
**DISCUSSION: This hypotensive patient has an obvious open book injury of the pelvic ring on the AP pelvis radiograph and further radiographs are not needed prior to the initiation of treatment. Although angiography may be indicated if he does not respond to stabilization of his pelvis and fluid/blood administration, temporary stabilization of the pelvis with a sheet or binder should be performed first because it is simple, quick, and has been shown to be effective. This patient does not need a laparotomy at this point since the FAST examination did not show any free intra-abdominal fluid and his chest radiograph was unremarkable, leaving the most likely source of bleeding the pelvic fracture. Open reduction with internal fixation of a pelvic injury is not indicated in an acutely ill patient.**
**REFERENCES: Kreig JC, Mohr M, Ellis TJ, et al: Emergent stabilization of pelvic ring injuries by controlled circumferential compression: A clinical trial. J Trauma 2005;59:659-664.**
**Croce MA, Magnotti LJ, Savage SA, et al: Emergent pelvic fixation in patients with exsanguinating pelvic fractures. J Am Coll Surg 2007;204:935-942.**
**Routt ML Jr, Falicov A, Woodhouse E, et al: Circumferential pelvic antishock sheeting:
A temporary resuscitation aid. J Orthop Trauma 2002;16:45-48.**
**27****. A 7-year-old girl is hit by a motor vehicle and sustains the isolated ipsilateral injuries shown in Figures 16a and 16b. What is the optimal definitive method of treatment?
1- Spica cast immobilization
2- Rigid reamed nailing of the femur and a short leg cast
3- Flexible nailing of the femur and tibia
4- Reamed nails of the femur and tibia
5- Spanning external fixator
PREFERRED RESPONSE: 3**
**DISCUSSION: The child has isolated ipsilateral femoral shaft and tibial shaft fractures. Spica cast immobilization is unlikely to accommodate for shortening and alignment in this child with multiple levels of injury. In this instance, efforts should be made to mobilize a least one level of the limb; therefore, treatment should include flexible nailing of the femur and tibia. Rigid reamed nails are not indicated in this young patient secondary to risk of a growth arrest and osteonecrosis of the proximal femur.**
**REFERENCES: Poolman RW, Kocher MS, Bhandari M: Pediatric femoral fractures:
A systematic review of 2422 cases. J Orthop Trauma 2006;20:648-654. **
**Anglen JO, Choi L: Treatment options in pediatric femoral shaft fractures. J Orthop Trauma 2005;19:724-733.**
**Beaty JH: Operative treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 2005;434:114-122.**
**28****. What is the most common cause of errors that harm patients?
1- Communication breakdown
2- Equipment breakdown
3- Nursing competence
4- Patient noncompliance
5- Physician competence
PREFERRED RESPONSE: 1**
**DISCUSSION: The AMA report identified communication breakdown as the most common cause of errors that harm patients. It is extremely important to learn to communicate effectively with your patients. Understanding cultural and language differences helps avoid communication errors.**
**REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.**
**American Medical Association ethical force program report: “Improving communication - Improving care”, 2006**
**http://www.ama-assn.org/ama/pub/category/16245.html.**
**29****. A 220-lb 20-year-old man was involved in a motor vehicle accident. His work-up reveals that he has multiple long bone fractures as well as a splenic injury that is currently being managed nonsurgically. His initial blood pressure in the trauma bay was 70/30 mm Hg. After receiving 4 liters of fluid and 3 units of packed red blood cells, his blood pressure is currently 110/70, his heart rate is 100, his urine output is 90 mL/h (normal 0.5 to 1 mL/kg/h), and his core temperature is 97.9 degrees F (36.5 degrees C). At this point, the patient’s resuscitation can be described as which of the following?
1- Complete based on the normalization of his blood pressure, urine output, and heart rate
2- Cannot be determined based on the data presented
3- Incomplete based on his fluid requirements calculated using his initial blood pressure as a measure of blood volume loss
4- Incomplete since he will need surgery on the long bone fractures and should be “tanked up” prior to losing blood in the operating room
5- Incomplete based on his heart rate
PREFERRED RESPONSE: 2**
**DISCUSSION: Although the end points of resuscitation are still unclear, what is known is that normalization of the standard hemodynamic parameters (blood pressure, heart rate, and urine output) is not adequate. Up to 85% of patients with normal hemodynamic parameters can still have inadequate tissue oxygenation or uncompensated shock. The initial base deficit, lactate level, or gastric pHi can be used to stratify patients for resuscitation needs, risks of death, and multiple organ failure (level 1 evidence). The time it takes to normalize the base deficit, the lactate level, or gastric pHi, can predict survival (level 2 evidence). Patients who have been in uncompensated shock (abnormal vital signs) should have their resuscitation monitored using data other than vital signs.**
**REFERENCES: Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: Endpoints of resuscitation. J Trauma 2004;57:898-912.**
**Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury,
a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.**
**Englehart MS, Schreiber MA: Measurement of acid-base resuscitation endpoints: Lactate, base deficit, bicarbonate or what? Curr Opin Crit Care 2006;12:569-574.**
**30****. A 30-year-old man who sustained a work-related injury 6 weeks ago reports persistent back and left-sided buttock pain that has been attributed to lumbar transverse process fractures. A pelvic radiograph and CT scans obtained 2 days ago are seen in Figures 17a through 17c. What is the best treatment for his injury?
1- Continued nonsurgical management
2- Posterior open reduction and internal fixation with tension band plating
3- Posterior iliosacral screws
4- Anterior open reduction and internal fixation
5- Anterior open reduction and internal fixation and posterior fixation
PREFERRED RESPONSE: 5**
**DISCUSSION: Fortunately, surgical treatment of sub-acute pelvic ring injuries is relatively uncommon as acute management has become more common. Delayed reconstruction of pelvic ring malunion and impending malunion is rare. Nonsurgical management may have a role as long as the hemipelvis does not flex, shorten, and/or externally rotate. The AP pelvic radiograph suggests that all three motions are happening in this patient. These are just a few of the indications to repair the pelvic ring and this is best done with anterior and posterior fixation. Anterior symphyseal plating will help correct most of the deformity. Posterior fixation can and should be added to lessen the forces on the anterior ring reconstruction when repair is performed in a sub-acute or delayed fashion. Posterior fixation can help obtain a more anatomic reduction and helps decrease the risk of anterior hardware failure.**
**REFERENCES: Mears DC: Management of pelvic pseudarthroses and pelvic malunion. Orthopade 1996;25:441-448.**
**Matta JM, Dickson KF, Markovich GD: Surgical treatment of pelvic nonunions and malunions. Clin Orthop Relat Res 1996;329:199-206.**
**McLaren AC, Rorabeck CH, Halpenny J: Long-term pain and disability in relation to residual deformity after displaced pelvic ring fractures. Can J Surg 1990;33:492-494.**
**31****. A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches
1- less than 10%.
2- 30%.
3- 50%.
4- 70%.
5- greater than 90%.
PREFERRED RESPONSE: 5**
**DISCUSSION: Mortality following trauma that requires surgical intervention for head, chest, and abdominal injury exceeds 90%. The type of pelvic fracture is a predictor of associated injury, blood requirements, and overall mortality. AP III pelvic fractures require the most blood, and are associated with significant abdominal trauma and shock. Lateral compression pelvic fractures are more associated with head, chest, and occasionally abdominal trauma, and mortality often occurs from associated injuries.**
**REFERENCES: Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements and outcome. J Trauma 1989;29:981-1000.**
**Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center. J Trauma 1997;42:695-700.**
**Gilliland MD, Ward RE, Barton RM, et al: Factors affecting mortality in pelvic fractures.
J Trauma 1982;22:691-693.**
**32****. A 19-year-old collegiate baseball player injures the ring finger on his dominant hand while sliding headfirst into second base. He reports that he is unable to actively flex or extend the distal interphalangeal joint of the finger. Radiographs are shown in Figures 19a and 19b. What is the anatomic lesion leading to this injury?
1- Rupture of the terminal extensor tendon
2- Avulsion of the volar plate
3- Rupture of the sagittal bands
4- Rupture of the spiral oblique retinacular ligaments
5- Rupture of the profundus insertion
PREFERRED RESPONSE: 5**
**DISCUSSION: The radiographs reveal a bony avulsion of the flexor profundus insertion (Jersey finger). The large bony fragment classifies this as a Leddy type III injury. The bony fragment has retracted to the level of the annular pulley (A4).**
**REFERENCES: Leddy JP, Packer JW: Avulsion of the insertion of the profundus tendon insertion in athletes. J Hand Surg 1977;2:66-69.**
**Leddy JP: Avulsions of the flexor digitorum profundus. Hand Clin 1985;1:77-83.**
**33****. A 72-year-old man was involved in an automobile accident 4 weeks ago. Initially he noted pain about his nondominant left shoulder, which resolved within a few weeks after the accident. He now describes trouble with gripping and carrying items in his left hand. Radiographs are shown in Figures 20a through 20c. His signs and symptoms are the result of injury to which of the following ligaments?
1- Volar scapholunate interosseous
2- Dorsal scapholunate interosseous
3- Long radiolunate
4- Short radiolunate
5- Dorsal intercarpal
PREFERRED RESPONSE: 2**
**DISCUSSION: The radiographs reveal a gap between the scaphoid and lunate bones, indicative of disruption of the scapholunate ligament complex. The three components of the complex are the dorsal scapholunate ligament, the volar (or palmar) scapholunate ligament, and the proximal fibrocartilaginous membrane, listed in decreasing yield strength. Disruption of the stout dorsal interosseous ligament is required for scapholunate dissociation to occur.**
**REFERENCES: Berger RA: The ligaments of the wrist: A current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63-82.**
**Cohen MS, Taleisnik J: Direct ligamentous repair of scapholunate dissociation with capsulodesis augmentation. Tech Hand Up Extrem Surg 1998;2:18-24.**
**34****. To avoid an injury to the L5 nerve root when placing an S1 sacroiliac screw, what area of the sacrum should be avoided on the lateral C arm image shown in Figure 21?**
1- A
2- B
3- C
4- D
5- E
**PREFERRED RESPONSE: 1**
**DISCUSSION: Safe placement of a sacroiliac screw depends on excellent imaging of and understanding of pelvic anatomy. There are variations in the anatomy of the upper sacrum. Patients with dysplasia of the sacrum can have “in-out-in” screws placed that exit the ilium, pass anterior to the sacral ala, and injure the L5 nerve root. To make sure that this does not occur, a lateral image of the sacrum is used to ensure that the starting point is in the “safe zone.” The starting point needs to be below the iliac cortical density (ICD) which parallels the sacral alar slope. This will prevent placing screws into the recessed ala of patients with a dysplastic sacrum. The triangular area anterior to the ICD is labeled A in the figure, B represents the sacral canal,
C is S2, D is the anterior border of the sacrum, and E represents the greater sciatic notches.**
**REFERENCES: Routt ML Jr, Simonian PT, Agnew SG, et al: Radiographic recognition of the sacral alar slope for optimal placement of iliosacral screws: A cadaveric and clinical study.
J Orthop Trauma 1996;10:171-177.**
**Kellam JF, Mayo K: Pelvic ring disruptions, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1052-1108.**
**35****. An otherwise healthy 37-year-old man fell off the flatbed of a delivery truck and landed directly on his dominant left hand. Surgical stabilization of a distal radius fracture is performed. An intraoperative radiograph is shown in Figure 22. What is the next most appropriate step in management?
1- Immobilization of the wrist in ulnar deviation for 4 weeks before starting range-of-motion exercises
2- In situ Kirschner wire fixation of the carpal bones for 6 weeks
3- Extending the volar incision used for fracture fixation and repairing the injured structures in addition to percutaneous Kirschner wire fixation
4- Performing a separate dorsal incision and repairing the injured structures in addition to percutaneous Kirschner wire fixation
5- Arthroscopic repair of the injured structures and percutaneous Kirschner wire fixation
PREFERRED RESPONSE: 4**
**DISCUSSION: The intraoperative radiograph reveals a scapholunate ligament disruption. Repair of the stout dorsal scapholunate interosseous ligaments is required. Interestingly, the results of scapholunate ligament injuries associated with distal radius fractures appear to be superior to those of isolated ligament injuries.**
**REFERENCES: Smith DW, Henry MK: Comprehensive management of soft-tissue injuries associated with distal radius fractures. J ASSH 2002;3:153-164.**
**Fernandez DL, Wolfe SW: Distal radius fractures, in Green DP, Hotchkiss RN, Pederson WC,
et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 693.**
**36****. A 36-year-old woman is placed in a short arm cast for a nondisplaced extra-articular distal radius fracture. Seven weeks later she notes the sudden inability to extend her thumb. What is the most likely cause of her condition?
1- Posterior interosseous nerve palsy
2- Cervical disk herniation
3- Entrapment of the flexor pollicis longus tendon
4- Rupture of the extensor pollicis longus tendon
5- Metacarpophalangeal joint dislocation
PREFERRED RESPONSE: 4**
**DISCUSSION: A recent review of 200 consecutive distal radius fractures noted that the overall incidence of extensor pollicis longus rupture was 3%. The causes are believed to be mechanical irritation, attrition, and vascular impairment. The fracture is usually nondisplaced and the patient notes weeks to months after injury the sudden, painless inability to extend the thumb. Treatment involves extensor indicis proprius tendon transfer or free palmaris longus tendon grafting.**
**REFERENCES: Skoff HD: Postfracture extensor pollicis longus tenosynovitis and tendon rupture: A scientific study and personal series. Am J Orthop 2003;32:245-247.**
**Bonatz E, Kramer TD, Masear VR: Rupture of the extensor pollicis longus tendon. Am J Orthop 1996;25:118-122.**
**Helal B, Chen SC, Iwegbu G: Rupture of the extensor pollicis longus tendon in undisplaced Colles’ type of fracture. Hand 1982;14:41-47.**
**37****. In Gustilo type III open tibial diaphyseal fractures, which of the following factors is associated with an increased risk of a poor functional outcome?
1- Soft-tissue coverage within 3 days of injury
2- Bone grafting 3 months after injury
3- Wound debridement within 6 to 24 hours from injury
4- Definitive treatment with external fixation
5- Free tissue transfer for soft-tissue coverage
PREFERRED RESPONSE: 4**
**DISCUSSION: According to the published outcomes analyses from the Lower Extremity Assessment Project (LEAP) study group of patients prospectively followed for 2 to 7 years, definitive fixation with an intramedullary nail has shown improved outcomes when compared to definitive external fixation. The findings showed that the timing of wound debridement (within 6 hours from injury as compared to within 6 to 24 hours), the timing of soft-tissue coverage
(3 days or less from injury as compared to more than 3 days), and the timing of bone grafting after injury (within or after 3 months) did not impact the infection or union rates and had no effect on functional outcome. The LEAP study has shown at 7-year follow-up that patients who are definitively treated with external fixation have a significantly longer time to union, poorer functional outcomes, longer time to achieve full weight bearing, and more time in the hospital. **
**REFERENCES: Webb LX, Bosse MJ, Castillo RC, et al: Analysis of surgeon-controlled variables in the treatment of limb-threatening type-III open tibial diaphyseal fractures. J Bone Joint Surg Am 2007;89:923-928.**
**38****. Figures 23a and 23b show the radiographs of a 75-year-old woman who sustained an injury to her nondominant hand. Initial treatment should consist of
1- closed reduction and splinting.
2- open reduction and internal fixation through a volar approach.
3- external fixation and Kirschner wire fixation.
4- intrafocal pinning and casting.
5- acceptance of alignment and bracing.
PREFERRED RESPONSE: 1**
**DISCUSSION: Definitive treatment decisions for displaced distal radius fractures in the elderly are based on a number of factors related to the fracture pattern and patient demographics. The first step in any treatment algorithm is a closed reduction and splinting with reassessment of alignment parameters. This is an extra-articular fracture with dorsal angulation. Low-demand elderly patients can be treated well with accepted minor malreduction.**
**REFERENCES: Handoll HH, Madhok R: Conservative interventions for treating distal radial fractures in adults. Cochrane Database Syst Rev 2003;2:CD000314.**
**Young CF, Nanu AM, Checketts RG: Seven-year outcome following Colles’ type distal radial fracture: A comparison of two treatment methods. J Hand Surg Br 2003;28:422-426.**
**39****. A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been
1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome?
1- His clinical outcome will correlate closely with his initial reduction.
2- His outcome will correlate with his radiographic score on the Ankle Osteoarthritis Score.
3- He will likely require a late ankle arthrodesis.
4- He will demonstrate marked limitations with regard to recreational activities.
5- He will perceive improvements for a period of over 2 years.
PREFERRED RESPONSE: 5**
**DISCUSSION: Marsh and associates retrospectively reviewed 56 tibial plafond fractures and found that the patients perceived improvement in their function and pain for an average of 2.4 years. They demonstrated some limitations in recreational activities but not marked limitations. Patients were unlikely to need a late arthrodesis (13%), and their outcomes did not correlate well with assessments of reduction or arthritis scores.**
**REFERENCE: Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: How do these ankles function over time? J Bone Joint Surg Am 2003;85:287-295.**
**40****. The injury shown in Figure 24 was most likely caused by what mechanism of injury?
1- Anterior posterior compression
2- Lateral compression
3- Vertical shear
4- Combined mechanism
5- Flexion-rotation
PREFERRED RESPONSE: 2**
**DISCUSSION: The CT cut shows a fracture through the posterior portion of the iliac wing or a crescent fracture. This occurs after a laterally directed force is applied to the anterior part of the involved iliac wing.**
**REFERENCE: Kellam JF, Mayo K: Pelvic ring disruptions, in Browner BD, Jupiter JB,
Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1,
pp 1052-1108.**
**41****. A 21-year-old college student fell from a balcony and landed on his outstretched right hand. He is seen in the emergency department 4 hours later and reports wrist pain and diffuse hand numbness. The volar forearm compartment is soft and there is no pain with passive finger extension. Radiographs are shown in Figures 25a and 25b. Definitive treatment should consist of
1- closed reduction and cast immobilization.
2- closed reduction, carpal tunnel release, and cast immobilization.
3- open reduction and ligament repair via a dorsal approach.
4- open reduction and ligament repair via a volar approach.
5- open reduction and ligament repair via dorsal and volar approaches and an extended carpal tunnel release.
PREFERRED RESPONSE: 5**
**DISCUSSION: A spectrum of perilunate injury patterns exists, with the dorsal trans-scaphoid perilunate fracture-dislocation being the most common. Perilunate injuries are highly unstable complex carpal disruptions that are not amenable to closed treatment. Open reduction and internal fixation is necessary to accurately restore carpal alignment via fracture reduction and fixation and intercarpal ligament repair. Controversy exists regarding the need for dorsal or combined dorsal and volar approaches. Based on the radiographic findings of a volar dislocation of the lunate and the associated median nerve injury, the patient requires open reduction and internal fixation via combined dorsal and volar approaches with a concomitant carpal tunnel release.**
**REFERENCES: Herzberg G, Forissier D: Acute dorsal trans-scaphoid perilunate fracture-dislocations: Medium-term results. J Hand Surg Br 2002;27:498-502.**
**Melone CP Jr, Murphy MS, Raskin KB: Perilunate injuries: Repair by dual dorsal and volar approaches. Hand Clin 2000;16:439-448.**
**Herzberg G, Comtet JJ, Linscheid RL, et al: Perilunate dislocations and fracture-dislocations:
A multicenter study. J Hand Surg Am 1993;18:768-779.**
**42****. A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result?
1- Growth arrest of the distal ulna
2- Growth arrest of the distal radius
3- Compartment syndrome
4- Radioulnar synostosis
5- Entrapment of the extensor pollicis longus (EPL) tendon
PREFERRED RESPONSE: 1**
**DISCUSSION: The radiographs show a fracture of the distal radius and ulna physis. The most likely complication is growth arrest of the distal ulna. In contradistinction to physis fractures of the radius (growth arrest incidence of less than 5%), the incidence of growth arrest in the ulna is between 30% and 40%. Entrapment of the EPL tendon and cross union between the two bones is extremely rare.**
**REFERENCES: Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.**
**Cannata G, De Maio F, Mancini F, et al: Physeal fractures of the distal radius and ulna: Long-term prognosis. J Orthop Trauma 2003;17:172-179.**
**Ray TD, Tessler RH, Dell PC: Traumatic ulnar physeal arrest after distal forearm fractures in children. J Pediatr Orthop 1996;16:195-200.**
**Aminian A, Schoenecker PL: Premature closure of the distal radial physis after fracture of the distal radial metaphysis. J Pediatr Orthop 1995;15:495-498.**
**43****. A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?
1- Continue wet-to-dry dressing changes until the wound heals by secondary intention.
2- Perform a volar advancement flap (ie, Moberg flap).
3- Perform a V-Y advancement flap.
4- Perform a thenar flap.
5- Perform a cross-finger flap to the ring finger.
PREFERRED RESPONSE: 1**
**DISCUSSION: The clinical photographs and radiographs reveal a distal phalangeal amputation with soft-tissue coverage over nonexposed bone. This is an ideal circumstance to allow healing by secondary intention with wet-to-dry dressing changes. There are few complications and the aesthetics surpass that of any soft-tissue reconstruction procedure. Volar advancement flaps (Moberg flaps) are limited to small defects about the thumb. A thenar flap will provide good coverage; however, the results are not comparable to simple dressing changes. A V-Y flap is useful when there is more tissue loss dorsally.**
**REFERENCES: Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.**
**Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.**
**44****. A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?
1- Functional bracing
2- Hanging long arm cast immobilization
3- Intramedullary nailing
4- Open reduction and internal fixation, radial nerve exploration
5- External bone stimulator
PREFERRED RESPONSE: 4**
**DISCUSSION: There is a high incidence of partial or complete laceration of the radial nerve with high-energy open fractures of the humeral shaft. The recommended treatment is irrigation and debridement of the fracture followed by open reduction and internal fixation and exploration of the radial nerve. If the nerve is completely lacerated, primary repair may be performed but poor outcomes have been reported. If a large zone of nerve injury is identified, delayed nerve grafting is advocated.**
**REFERENCES: Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high energy humeral shaft fractures. J Hand Surg 2004;29:144-147.**
**Foster RJ, Swiontkowski MR, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.**
**Lowe JB III, Sen SK, Mackinnon SE: Current approach to radial nerve paralysis. Plast Rec Surg 2002;110:1099-1113.**
**45****. Which of the following complications is associated with the use of a short cephalomedullary nail for fixation of intertrochanteric hip fractures?
1- Increased risk of deep venous thrombosis
2- Increased risk of a postoperative ipsilateral femoral fracture
3- Increased blood loss when compared to a sliding-compression hip-screw
4- Increased risk of nonunion
5- Increased mortality
PREFERRED RESPONSE: 2**
**DISCUSSION: Implant-related fractures following hip fracture surgery were reported by Robinson and associates and showed that the risk of an ipsilateral femoral fracture is significantly increased with the use of short cephalomedullary nails as compared to a compression hip screw. The use of short cephalomedullary nails has not been shown to increase the risk of deep venous thrombosis or nonunion. Cephalomedullary nails overall have decreased surgical blood loss when compared to use of sliding-compression hip-screw devices.**
**REFERENCES: Robinson CM, Adams CI, Craid M, et al: Implant-related fractures of the femur following hip fracture surgery. J Bone Joint Surg Am 2002;84:1116-1122.**
**Valverde JA, Alonso MG, Porro JG, et al: Use of the Gamma nail in the treatment of fractures of the proximal femur. Clin Orthop Relat Res 1998;350:55-61.**
**46****. A 19-year-old man sustained the isolated injury seen in Figure 28a. He is adequately resuscitated. A closed reduction was performed in the emergency department, and postreduction radiographs are shown in Figures 28b and 28c. What is the next most appropriate step in management?
1- Urgent open reduction and internal fixation
2- Placement of a knee immobilizer and delayed open reduction and internal fixation
3- Placement of a distal femoral traction pin and delayed open reduction and internal fixation
4- Delayed open reduction and internal fixation
5- Nonsurgical management and restricted weight bearing
PREFERRED RESPONSE: 1**
**DISCUSSION: Incarcerated fragments and nonconcentric reductions are best treated with urgent open reduction, retrieval of the fragments, and internal fixation. Delayed treatment increases the damage to the articular surface, even if traction is applied. There is no role for nonsurgical management with entrapped fragments and nonconcentric reduction of the hip.**
**REFERENCES: Epstein HC, Wiss DA, Cozen L: Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res 1985;201:9-17.**
**Anglen JO, Hughes M: Trochanteric osteotomy for incarcerated hip dislocation due to interposed posterior wall fragments. Orthopedics 2004;27:213-216.**
**47****. The iliopectineal fascia runs between which of the following structures?
1- Iliopsoas muscle and the iliac vessels/femoral nerve
2- Lateral femoral cutaneous nerve and the iliac vessels
3- Iliopsoas muscle/femoral nerve and the iliac vessels
4- Iliac wing and the iliopsoas muscle
5- Pubic symphysis and the iliac vessels
PREFERRED RESPONSE: 3**
**DISCUSSION: The sheath of the psoas muscle or the iliopectineal fascia separates the more lateral iliopsoas muscle and the femoral nerve from the more medially located iliac vessels. This fascia has to be taken down to enter the true pelvis.**
**REFERENCES: Masquelet AC, McCullough CJ, Tubiana R: An Atlas of Surgical Exposures of the Lower Extremity. Philadelphia, PA, JB Lippincott, 1993.**
**Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.**
**Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1109-1149.**
**48****. Which of the following is most predictive of a medial side ankle injury in the presence of a fibula fracture above the level of the joint?
1- Severe medial ankle tenderness
2- Severe medial ankle ecchymosis
3- Stress radiographs showing the medial clear space measuring 6 mm and the superior joint space measuring 3 mm
4- Inability to ambulate
5- Medial ankle swelling
PREFERRED RESPONSE: 3**
**DISCUSSION: Isolated Lauge-Hansen supination-external rotation-type ankle fractures comprise 20% to 40% of ankle fractures and nonsurgical management is effective for managing SER-2 ankle fractures. Tornetta and associates recently showed that medial ankle tenderness, ecchymosis, and swelling are not reliable findings when trying to determine deltoid competence. Stress radiographs showing a medial clear space of greater than 4 mm or one that is also 1 mm greater than the superior joint space, or any lateral talar subluxation are indicative of deltoid incompetence and indicative of a SER-4 ankle fracture.**
**REFERENCES: McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004:86;2171-2178.**
**Kristensen KD, Hansen T: Closed treatment of ankle fractures: Stage II supination-eversion fractures followed for 20 years. Acta Orthop Scand 1985;56:107-109.**
**Michelson JD: Fractures about the ankle. J Bone Joint Surg Am 1995;77:142-152.**
**49****. Figure 29 shows the radiograph of a 10-year-old boy who injured his knee playing football. What is the most appropriate initial treatment?
1- Closed reduction and casting
2- Flexible nailing
3- Blade plate fixation
4- Anatomic reduction and smooth pin fixation with supplemental casting
5- Open or closed reduction and screw fixation
PREFERRED RESPONSE: 4**
**DISCUSSION: Salter type I fractures of the distal femur are quite unstable; therefore, closed reduction and cast immobilization can be expected to result in high rates of redisplacement. Optimal treatment consists of open or closed reduction and smooth pin fixation, and supplemental casting is required to ensure fracture stability. Screw fixation may increase rates of growth plate injury. Blade plate or flexible nail fixation will be challenging to apply and is not necessary.**
**REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.**
**Thomson JD, Stricker SJ, Williams MM: Fractures of the distal femoral epiphyseal plate.
J Pediatr Orthop 1995;15:474-478. **
**Edwards PH Jr, Grana WA: Physeal fractures about the knee. J Am Acad Orthop Surg 1995;3:63-69.**
**50****. A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?
1- Nerve conduction velocity studies and electromyography
2- Extension splinting of the fingers
3- Exploration and repair of the extensor tendon laceration
4- Exploration and repair of the posterior interosseous nerve
5- Observation
PREFERRED RESPONSE: 4**
**DISCUSSION: The clinical photographs indicate that the tenodesis effect of digit flexion with passive wrist extension and digit extension with passive wrist flexion is intact, indicating no discontinuity of the extensor or flexor tendons. The most likely injury is a laceration of the posterior interosseous nerve.**
**REFERENCE: Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 2069.**
**51****. A 42-year-old college professor reports persistent pain at the hypothenar eminence 9 months after falling from his bicycle. Initial radiographs were reportedly normal. Use of a wrist splint for the last 2 months has failed to provide relief. A radiograph obtained by his primary care physician prior to referral is seen in Figure 31. What is the most appropriate treatment?
1- Continued splint immobilization for 6 weeks
2- Pisiform excision
3- Hook of hamate excision
4- Open reduction and internal fixation with bone grafting
5- Lunotriquetral arthrodesis
PREFERRED RESPONSE: 2**
**DISCUSSION: The oblique radiograph of the wrist reveals a displaced fracture of the pisiform that usually occurs following a direct blow or sudden contraction of the flexor carpi ulnaris tendon. Persistent pain secondary to pisotriquetral incongruity and degenerative arthritis warrants pisiform excision, which does not compromise wrist flexion strength. Pisiform fractures are usually missed on routine radiographic views. An oblique or carpal tunnel view can be helpful in visualizing the pisotriquetral joint.**
**REFERENCE: Fleege MA, Jebson PJ, Renfrew DL, et al: Pisiform fractures. Skeletal Radiol 1991;20:169-172.**
**52****. Figures 32a and 32b show the radiographs of a 13-year-old right hand-dominant boy who sustained a closed Salter-Harris type II fracture of the proximal humerus during a hockey game. The shoulder has significant swelling, but is neurovascularly intact. What treatment offers the best chance of reestablishing normal shoulder motion?
1- Closed reduction and application of a shoulder spica cast in the outpatient setting
2- Closed reduction under fluoroscopy and application of a shoulder spica cast in the operating room
3- No active reduction and placement of the upper extremity in a shoulder immobilizer
4- Closed or open reduction and percutaneous pin stabilization
5- Open reduction and internal fixation
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a significantly angulated proximal humerus fracture with a high degree of varus angulation, and rotational malalignment is likely. Failure to correct the varus angulation will result in permanent loss of shoulder abduction because the patient’s age limits bony remodeling. These fractures are inherently unstable due to the inability to control the proximal fracture alignment. Shoulder spica casts have a high rate of redisplacement after treatment. Adequate open or closed reduction and pin fixation in the operating room optimizes alignment and all but eliminates the chance of redisplacement.**
**REFERENCES: Dobbs MB, Luhmann SJ, Gordon JE, et al: Severely displaced proximal humerus epiphyseal fractures. J Pediatr Orthop 2003;23:208-215.**
**Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, p 701.**
**Sarwark JF, King EC, Luhmann SJ: Proximal humerus, scapula, and clavicle, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 703-715.**
**53****. What letter in Figure 33 marks the correct starting point for a transiliac pelvic screw?**
1- A
2- B
3- C
4- D
5- E
**PREFERRED RESPONSE: 1**
**DISCUSSION: Iliosacral screws cannot always be placed safely due to variations in pelvic anatomy. Transiliac bars are an alternative method for fixation but are placed using an open technique. A screw can be placed percutaneously through both iliac wings posterior to the posterior border of the sacrum. The starting point is visualized using a lateral C arm shot and is located on the posterior iliac crest at about the level of the S1 body where the crest has its largest area posterior to the sacrum. This area is labeled A in the figure, B represents the sacral canal, C is S1, D is the area cephalad to the iliocortical density, and E is the anterior border of the sacrum. The radiograph demonstrates a well-placed sacroiliac screw.**
**REFERENCES: Moed BR, Fissel BA, Jasey G: Percutaneous transiliac pelvic fracture fixation: Cadaver feasibility study and preliminary clinical results. J Trauma 2007;62:357-364.**
**Kellam JF, Mayo K: Pelvic ring disruptions, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1052-1108.**
**54****. A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure 34. What is the next most appropriate step in the orthopaedic management of this patient?
1- Axillary view
2- CT of the shoulder
3- Closed reduction
4- Sling and close follow-up
5- Functional brace
PREFERRED RESPONSE: 1**
**DISCUSSION: The next step in the management of this injury is completion of the shoulder trauma series. An axillary radiograph, which can be quickly performed in the emergency department, must be obtained to accurately assess the humeral head relationship to the glenoid. If difficulty is encountered, a “Velpeau” axillary may be substituted. If that fails to elucidate the status of the glenohumeral joint, a CT scan should be obtained.**
**REFERENCE: Simon JA, Puopolo SM, Capla EL, et al: Accuracy of the axillary projection to determine fracture angulation of the proximal humerus. Orthopedics 2004;27:205-207.**
**55****. An 8-year-old girl injures her elbow playing soccer. After attempted reduction in the emergency department, radiographs of the elbow are shown in Figures 35a through 35c. What is the next most appropriate step in treatment?
1- Cast immobilization for 2 weeks followed by early motion
2- Minimal treatment for this congenital radial head dislocation
3- Open reduction and internal fixation
4- Annular ligament reconstruction
5- Attempt a repeat closed reduction
PREFERRED RESPONSE: 3**
**DISCUSSION: Ninety percent of injuries to the proximal radius in children are radial neck fractures, and 50% of these fractures are through the metaphyseal bone. The remaining 50% are Salter-Harris type I or II fractures. These radiographs show a fracture of the radial head and subluxation of the radius anteriorly. Most congenital radial head dislocations are posterior lateral. Nonsurgical treatment modalities are unlikely to be successful due to the wide displacement of the fracture fragments, as well as dislocation of the radial head.**
**REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14. **
**Hashemi-Nejad A, Goddard NJ: Radial head fractures. Br J Hosp Med 1994;51:223-226.**
**Rodriguez Merchan EC: Displaced fractures of the head and neck of the radius in children: Open reduction and temporary transarticular internal fixation. Orthopedics 1991;14:697-700.**
**56****. A 30-year-old woman injured the ring finger of her nondominant hand while playing baseball 5 weeks ago. She now reports pain and limited motion of the proximal interphalangeal (PIP) joint. A lateral fluoroscopy image is shown in Figure 36. Treatment of the PIP joint should consist of
1- closed reduction and percutaneous pinning.
2- implant arthroplasty.
3- arthrodesis.
4- volar plate arthroplasty.
5- resection arthroplasty.
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a neglected PIP joint fracture-dislocation with comminution involving more than 40% of the volar articular surface of the middle phalanx. Volar plate arthroplasty has been advocated for the treatment of acute unstable and chronic dorsal fracture-dislocations. The volar plate is incised laterally and released from the collateral ligaments. The volar fragments of the middle phalanx are removed and a trough is created for advancement of the volar plate, which is secured with sutures secured on the dorsum of the middle phalanx beneath the extensor mechanism.**
**REFERENCES: Dionysian E, Eaton RG: The long-term outcome of volar plate arthroplasty of the proximal interphalangeal joint. J Hand Surg Am 2000;25:429-437.**
**Eaton RG, Malerich MM: Volar plate arthroplasty of the proximal interphalangeal joint: A review of ten years’ experience. J Hand Surg Am 1980;5:260-268.**
**Deitch MA, Kiefhaber TR, Comisar BR, et al: Dorsal fracture dislocations of the proximal interphalangeal joint: Surgical complications and long-term results. J Hand Surg Am 1999;24:914-923.**
**57****. A 19-year-old woman fell onto her nondominant hand 6 weeks ago. Radiographs are shown in Figures 37a and 37b. A decision has been made to treat this fracture surgically. What is the best approach to treat this fracture?
1- Percutaneous pinning of the fracture with Kirschner wires
2- Open reduction and pinning with Kirschner wires
3- Arthroscopic in situ compression screw fixation
4- Reduction and compression screw fixation via a volar approach
5- Reduction and compression screw fixation via a dorsal approach
PREFERRED RESPONSE: 5**
**DISCUSSION: Displaced fractures of the scaphoid are best treated with compression screw fixation. Proximal third fractures (as in this patient) are optimally approached via a dorsal approach to ensure proper reduction and compression. Fractures of the scaphoid waist can be approached either by a volar or a dorsal approach. Kirschner wire fixation is limited to proximal pole fractures that are too small to accommodate the trailing head of a compression screw.**
**REFERENCES: Retting ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole fractures. J Hand Surg Am 1999;24:1206-1210.**
**Filan SK, Herbert TJ: Herbert screw fixation of scaphoid fractures. J Bone Joint Surg Br 1996;78:519-529.**
**58****. Which of the following findings best describes the acetabular fracture shown in
Figure 38?
1- Posterior column with articular impaction and a free fragment
2- Anterior column with articular impaction
3- Posterior wall with an intra-articular fragment
4- Posterior wall with articular impaction and a free intra-articular fragment
5- Posterior wall with articular impaction
PREFERRED RESPONSE: 4**
**DISCUSSION: The CT scan shows a posterior wall fracture with impaction of the articular surface and a free fragment within the joint. Proper treatment of this injury requires not only reduction and fixation of the posterior wall fragment but also removal of the free fragment and elevation of the depressed articular segment.**
**REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.**
**Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1109-1149.**
**59****. In the setting of a proximal tibial plateau fracture and its repair, which of the following materials is an isotropic material?
1- Proximal tibial cortical bone
2- Articular cartilage of the tibial plateau
3- Stainless steel tibial plate
4- Medial or lateral meniscus
5- Calcium phosphate cement
PREFERRED RESPONSE: 3**
**DISCUSSION: An isotropic material is one that has similar mechanical properties regardless of the orientation of the material. Examples of isotropic materials include metals, plastics, and methacrylate. Most biologic tissues are anisotropic, meaning their mechanical properties alter depending on the materials’ orientation to the applied stress.**
**REFERENCE: Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 58-59.**
**60****. A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
1- normal sexual function and normal vaginal childbirth.
2- sexual dysfunction (dyspareunia) and normal vaginal childbirth.
3- normal sexual function and caesarean section childbirth.
4- sexual dysfunction (dyspareunia) and caesarean section childbirth.
5- normal sexual function and caesarean section childbirth until hardware removal.
PREFERRED RESPONSE: 4**
**DISCUSSION: Pelvic trauma in women has been shown to increase the risk of sexual dysfunction and dyspareunia. Additionally, caesarean section childbirth is almost universal following pelvic trauma regardless of whether anterior pelvic hardware is present or not.**
**REFERENCES: Copeland CE, Bosse MJ, McCarthy ML et al: Effect of trauma and pelvic fracture on female genitourinary, sexual, and reproductive function. J Orthop Trauma 1997;11:73-81.**
**Wright JL, Nathans AB, Rivara FP, et al: Specific fracture configurations predict sexual and excretory dysfunction in men and women 1 year after pelvic fracture. J Urol 2006;176:1540-1545.**
**61****. A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?
1- Closed treatment and casting
2- Open reduction and internal fixation
3- Primary subtalar arthrodesis
4- Percutaneous fixation
5- External fixation
PREFERRED RESPONSE: 2**
**DISCUSSION: A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures.**
**REFERENCES: Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.**
**Sanders R: Displaced intraarticular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.**
**Sanders R, Fortin P, DiPasquale T, et al: Operative treatment in 120 displaced intra-articular calcaneal fractures: Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res 1993;290:87-95.**
**62****. A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
1- Radial head resection, open reduction and internal fixation of the coronoid, and medial collateral ligament repair
2- Radial head resection and lateral collateral ligament repair
3- Radial head arthroplasty alone
4- Radial head arthroplasty and lateral collateral ligament repair
5- Radial head arthroplasty, open reduction and internal fixation of the coronoid, and lateral collateral ligament repair
PREFERRED RESPONSE: 5**
**DISCUSSION: The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region.**
**REFERENCES: Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815.**
**Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.**
**Moro JK, Werier J, MacDermid JC, et al: Arthroplasty with a metal radial head for unreconstructable fractures of the radial head. J Bone Joint Surg Am 2001;83:1201-1211.**
**63****. A 30-year-old man is brought to the emergency department after a motor vehicle accident. He has a closed midshaft femoral fracture and an intra-abdominal injury.
He is currently in the operating room and the exploration of his abdomen has been completed. His initial blood pressure was 70/30 mm Hg and is now 90/50 mm Hg after
4 liters of fluid and 2 units of blood. His initial serum lactate was 3.0 mmol/L
(normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C). What is the most appropriate management for the femoral shaft fracture at this point?
1- Reamed intramedullary nailing
2- Traction
3- External fixation
4- Open plating
5- Mast suit
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has several indications that he is not ready for definitive fixation of the femoral shaft fracture at this point. He is cold with a core temperature of 93 degrees F, and hypothermia of less than 95 degrees F (35 degrees C) has been shown to be associated with an increased mortality rate in trauma patients. The patient has also not been resuscitated based on his increasing lactate levels and although controversial, it has been shown that temporary external fixation leads to a lower incidence of multiple organ failure and acute respiratory distress syndrome.**
**REFERENCES: Shafi S, Elliot AC, Gentilello L: Is hypothermia simply a marker of shock and injury severity or an independent risk factor for mortality in trauma patients? Analysis of a large national trauma registry. J Trauma 2005;59:1081-1085.**
**Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.**
**Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-454.**
**64****. A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?
1- MRI scan
2- Physical examination
3- Workers’ compensation status
4- Surgeon availability
5- Patient age
PREFERRED RESPONSE: 2**
**DISCUSSION: The most important criteria in determining the need for surgery following a nondisplaced or minimally displaced tibial plateau fracture is knee stability to varus/valgus stress. Soft-tissue injury noted on MRI may be addressed at a later time following fracture healing. This fracture pattern is amenable to nonsurgical management. Decisions regarding surgical intervention may be made up to 2 weeks after injury.**
**REFERENCE: Lansinger O, Bergman B, Korner L, et al: Tibial condylar fractures: A twenty-year follow-up. J Bone Joint Surg Am 1986;68:13-19.**
**65****. A 100-lb 9-year-old boy has a closed midshaft transverse femoral fracture. The oblique fracture is shortened by 3 cm with a 10-degree varus angulation. Surgical management consists of intramedullary, retrograde flexible titanium nailing. To optimize fracture stability, the surgeon should
1- insert the largest diameter nails possible.
2- place asymmetric nails, with the smaller nail placed medially.
3- impact the distal ends of the nail into the medullary canal.
4- open the fracture to permit anatomic alignment.
5- apply a hinged knee orthosis.
PREFERRED RESPONSE: 1**
**DISCUSSION: The technique of intramedullary nailing with titanium elastic nails is based on the concept of balanced forces across the fracture site with two equally sized nails. Implantation of the largest sized nails possible, with two equally sized nails, maximizes the stiffness at the fracture site, thereby optimizing fracture alignment and stability. Impacting the nails into the medullary canal can impact the fixation by minimizing distal purchase of the nail at the cortical insertion site. Closed reduction commonly permits bony reduction and passage of the nails; open reduction is reserved for inability to align the fracture.**
**REFERENCES: Luhmann SJ, Schootman M, Schoenecker PL, et al: Complications of titanium elastic nails for pediatric femur fractures. J Pediatr Orthop 2003;23:443-447.**
**Lascombes P, Haumont T, Journeau P: Use and abuse of flexible intramedullary nailing in children and adolescents. J Pediatr Orthop 2006;26:827-834.**
**Kasser JR, Beaty JH: Femoral shaft fractures, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 911-916.**
**66****. A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and recently had an intramedullary nail placed for the skeletal injury. Vacuum-assisted closure (VAC) has been used to cover the defect since the injury. The risk of infection developing in the tibia is
1- higher than previous reports because of the use of the wound VAC.
2- related mainly to the location of the soft-tissue defect.
3- related mainly to the timing of soft-tissue coverage.
4- lower than previous reports because of the use of the wound VAC.
5- lower than previous reports because of the intramedullary nailing.
PREFERRED RESPONSE: 3**
**DISCUSSION: The risk of infection in a 3B open tibia fracture is most directly related to the timing of the soft-tissue coverage and less related to the size or location of the wound. The wound VAC does not lower or raise the risk of infection in open fractures. It does appear to increase the window of time to obtain coverage without increasing the risk of infection. Additionally, the wound VAC may decrease the probability of needing free tissue coverage. Intramedullary nailing has not been shown to lower the risk of infection in 3B fractures.**
**REFERENCES: Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.**
**Dedmond BT, Kortesis B, Punger K, et al: The use of negative-pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibia shaft fractures. J Orthop Trauma 2007;21:11-17.**
**Herscovici D Jr, Sanders RW, Scaduto JM, et al: Vacuum-assisted wound closure (VAC therapy) for the management of patients with high-energy soft tissue injuries. J Orthop Trauma 2003;17:683-688.**
**67****. A 12-year-old boy falls from a bicycle. A radiograph of his injured shoulder is shown in Figure 41. What is the optimal method of treatment?
1- Suture of the coracoclavicular ligament
2- Temporary plate fixation across the acromioclavicular joint
3- Immobilization in a shoulder spica cast
4- Sling immobilization
5- Reduction and temporary intramedullary fixation across the acromioclavicular joint
PREFERRED RESPONSE: 4**
**DISCUSSION: The radiograph reveals a distal clavicle fracture. In children, a periosteal sleeve will remain attached to the intact coracoclavicular ligament, and as such, remodeling can be expected. Therefore, nonsurgical management with a sling is preferred. Surgical treatment is not necessary, and a shoulder spica cast offers no advantage over a simple sling.**
**REFERENCES: Bishop JY, Flatow EL: Pediatric shoulder trauma. Clin Orthop Relat Res 2005;432:41-48.**
**68****. The major benefit of irrigation with a castile soap solution over irrigation with bacitracin solution for the treatment of the open fracture shown in Figure 42 can be seen in which of the following outcomes?
1- Decreased rate of postoperative infection
2- Decreased rate of nonunion
3- Decreased rate of primary wound healing problems
4- Decreased rate of reoperation
5- Increased rate of bone healing
PREFERRED RESPONSE: 3**
**DISCUSSION: The mainstay of early treatment of open fractures includes irrigation and debridement. Prior to the development of antibiotics, this was traditionally accomplished with some form of detergent irrigation. Antibiotic irrigation has been in favor more recently but has mixed scientific results related to its use. Results of at least one major study show the use of a nonsterile liquid soap additive (castile soap) is at least as effective as the use of bacitracin with regards to the rate of postoperative infection and fracture healing, and shows a significant decrease in problems with soft-tissue healing.**
**REFERENCE: Anglen JO: Comparison of soap and antibiotic solutions for irrigation of lower-limb open fracture wounds: A prospective, randomized study. J Bone Joint Surg Am 2005;87:1415-1422.**
**69****. A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?
1- Nonsurgical management with weight bearing as tolerated
2- Nonsurgical management with no weight bearing on the left side
3- Nonsurgical management with use of a pelvic binder
4- Open reduction and internal fixation of the anterior pelvis
5- Open reduction and internal fixation of the anterior pelvis with placement of a left-sided percutaneous posterior screw
PREFERRED RESPONSE: 4**
**DISCUSSION: Symphyseal widening of greater than 2.5 cm and less than 5 cm denotes an AP II injury and a rotationally unstable pelvis. An AP II pelvic ring injury is best treated with anterior open reduction and internal fixation. Nonsurgical management is reserved for AP I injuries. Pelvic binders are used only acutely and should not be used for definitive management. Iliosacral screws usually are not necessary in the acute management of AP II injuries.**
**REFERENCES: Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96.**
**Templeman DC, Schmidt AH, Sems AS, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.**
**Tile M: Management, in Tile M: Fractures of the Pelvis and Acetabulum, ed 2. Philadelphia, PA, Williams and Wilkins, 1995, pp 108-134.**
**70****. What vessel is marked with an asterisk in Figure 44?
1- Obturator artery
2- Inferior epigastric artery
3- Superior gluteal artery
4- Internal pudendal artery
5- Lateral sacral artery
PREFERRED RESPONSE: 3**
**DISCUSSION: The superior gluteal artery is a branch of the posterior division of the internal iliac artery and exits the pelvis through the greater sciatic notch. It can be injured as a result of a pelvic ring fracture or acetabular fracture that has a fracture of the posterior column.**
**REFERENCES: Agur AM, Dalley AF (eds): Grant’s Atlas of Anatomy, ed 12. Philadelphia, PA, Lippincott Williams and Wilkins, 2008.**
**Uflacker R: Atlas of Vascular Anatomy: An Angiographic Approach, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006.**
**71****. Figures 45a and 45b show the radiographs of a 14-year-old boy who sustained a distal radius fracture while playing hockey. After 1 year the patient is asymptomatic. Follow-up and comparison radiographs and an MRI scan are shown in Figures 45c and 45d. What is the next most appropriate step in management?
1- Resection of radius growth arrest
2- Performing growth arrest of the ulna
3- Repair of the ulnar styloid fracture
4- Perform lengthening of the radius
5- Continued observation
PREFERRED RESPONSE: 2**
**DISCUSSION: The patient sustained a growth plate fracture of the distal radius and ulna. Although treated with closed reduction and casting, the follow-up radiographs demonstrate shortening of the radius in comparison to the ulna, and the MRI scan confirms thinning of the distal radius growth plate and bony bars consistent with a growth arrest. At this time, the discrepancy in length is too minor to consider lengthening of the radius; in addition, excision of a physeal bar with minimal growth potential is not likely to restore the gross discrepancy. Ulnar styloid fractures are rarely symptomatic and do not require treatment in the asymptomatic patient. Closure of the distal ulna growth plate will prevent further discrepancy between the radius and ulna.**
**REFERENCES: Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.**
**Bae DS, Waters PM: Pediatric distal radius fractures and triangular fibrocartilage complex injuries. Hand Clin 2006;22:43-53.**
**72****. A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient?
1- Chondrolysis
2- Ischemic necrosis of the femoral head
3- Ischemic necrosis of the greater trochanter
4- Femoral neck fracture
5- Trochanteric overgrowth
PREFERRED RESPONSE: 2**
**DISCUSSION: The development of femoral head ischemic necrosis is the iatrogenically created complication in this skeletally immature patient. Placement of a rigid, antegrade intramedullary nail through the piriformis fossa is likely to damage the vascular supply to the femoral head as the vessels ascend the femoral neck on the way to the femoral head. The MRI scan reveals ischemic necrosis with early collapse of the femoral head. The joint space is preserved on the MRI scan, ruling out chondrolysis.**
**REFERENCES: Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516.**
**Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 1997;338:60-73.**
**Kasser JR, Beaty JH: Femoral shaft fractures, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 917-919.**
**73****. A 30-year-old man caught his dominant little finger on the straps of his windsurfing board 10 days ago. He reports swelling about the distal phalanx and has difficulty completely extending the distal interphalangeal joint. A radiograph is shown in
Figure 47. What is the most appropriate treatment for this injury?
1- Extension splinting of the proximal interphalangeal and distal interphalangeal joints
2- Extension splinting of the distal interphalangeal joint
3- Transarticular pinning of the distal interphalangeal joint
4- Extension block pinning of the distal interphalangeal joint
5- Open reduction and internal fixation of the distal phalanx
PREFERRED RESPONSE: 2**
**DISCUSSION: The radiograph reveals a “bony mallet injury.” As the distal phalanx is not volarly subluxated, extension splinting, similar to a classic mallet injury without bony involvement, is appropriate. If there is volar subluxation associated with a large bony fragment, surgical intervention is appropriate.**
**REFERENCES: Baratz ME, Schmidt CC, Hughes TB: Extensor tendon injuries, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 192.**
**Bendre AA, Hartigan BJ, Kalainov DM: Mallet finger. J Am Acad Orthop Surg 2005;13:336-344.**
**74****. A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient’s neurologic recovery can be best determined by
1- myelography with CT.
2- spinal cord-evoked potentials.
3- repeat physical examinations.
4- MRI.
5- electromyography and nerve conduction velocity studies.
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has spinal shock. Steroid administration and MRI are appropriate therapeutic and diagnostic procedures. Myelography with CT is of little value unless there is an unusual skeletal variant. Spinal cord-evoked potentials have no value. The best method to determine the patient’s neurologic recovery is repeated physical examinations over the first 48 to 72 hours.**
**REFERENCES: Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.**
**Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1185-1194.**
**75****. Figures 48a and 48b show the radiographs of a 26-year-old woman who fell down two steps and twisted her foot and ankle. What is the most appropriate treatment for this injury?
1- Open reduction and internal fixation with a mini fragment plate and screws
2- Closed cannulated screw fixation
3- Short leg casting for 6 weeks
4- Hard-soled shoe and weight bearing as tolerated
5- Short leg cast and non-weight-bearing, followed by weight bearing as tolerated for 6 weeks in a fracture brace
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a zone 1 base of the fifth metatarsal fracture (Pseudojones) that represents a less serious injury compared to zone 2 and 3 fractures with regard to healing potential. Treatment is symptomatic and casting is not necessary. These fractures are well treated with a hard-soled shoe for comfort and weight bearing as tolerated. Surgical intervention is not warranted.**
**REFERENCES: Vorlat P, Achtergael W, Haentjens P: Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal. Int Orthop 2007;31:5-10.**
**Wiener BD, Linder JF, Giattini JF: Treatment of fractures of the fifth metatarsal: A prospective study. Foot Ankle Int 1997;18:267-269.**
**Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.**
**76****. A still active 86-year-old pastry chef falls in her kitchen and notes pain and deformity of her little finger. There are no open wounds. Radiographs are shown in Figures 49a and 49b. What is the most appropriate management?
1- Closed reduction and splinting in metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joint extension
2- Closed reduction and splinting in MCP joint flexion and PIP joint extension
3- Reduction and percutaneous fixation
4- Open reduction and internal fixation
5- Buddy taping and early range of motion
PREFERRED RESPONSE: 3**
**DISCUSSION: The fracture of the proximal phalanx is clearly displaced. There is slight comminution at the area of the fracture. Closed reduction is likely to fail due to the forces of the extensor, flexor, and intrinsic mechanisms. Percutaneous fixation, unlike open fixation techniques, avoids likely problems with stiffness.**
**REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.**
**Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.**
**77****. A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient’s family reports that he is a Jehovah’s Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient’s blood pressure becomes unstable. What is the most appropriate action?
1- Consult the ethics committee before giving blood.
2- Use cell saver blood.
3- Ask the patient’s family for consent to give blood.
4- Use plasma expanders.
5- Give the patient blood.
PREFERRED RESPONSE: 4**
**DISCUSSION: Certain medical procedures involving blood are specifically prohibited in the belief system of a Jehovah’s Witness whereas others are not doctrinally prohibited. For procedures where there is no specific doctrinal prohibition, a Jehovah’s Witness should obtain the details from medical personnel and make his or her own decision. Transfusions of allogeneic whole blood or its constituents or preoperative donated autologous blood are prohibited. Other procedures, while not doctrinally prohibited, are not promoted such as hemodilution, intraoperative cell salvage, use of a heart-lung machine, dialysis, epidural blood patch, plasmapheresis, white blood cell scans (labeling or tagging of removed blood returned to the patient), platelet gel, erythropoietin, or blood substitutes. The patient should not be given blood. Plasma expanders should be used first to restore hemodynamic stability. Cell saver blood from an open would is not recommended nor would there likely be enough from an open tibial fracture to salvage. The patient’s family may be expressing their own beliefs rather than the patient’s beliefs and it would be better to ask the patient when he or she is more alert to determine what procedures they would allow. A consult with the ethics committee will unnecessarily delay an intervention that should restore hemodynamic stability.**
**REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.**
**Jehovah’s Witnessess Official Web Site: Medical Care and Blood, 2008, http://www.watchtower.org/e/medical_care_and_blood.htm**
**78****. Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and
1- talectomy.
2- reimplantation of the talus.
3- reimplantation of the talus with acute triple arthrodesis.
4- Syme amputation.
5- transtibial amputation.
PREFERRED RESPONSE: 2**
**DISCUSSION: The radiograph shows a complete extrusion of the talus. Reimplantation of the talus after wound debridement has been reported to be safe and successful, and provides for flexibility with any future reconstructive procedures.**
**REFERENCES: Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424.**
**Brewster NT, Maffulli N: Reimplantation of the totally extruded talus. J Orthop Trauma 1997;11:42-45.**
**79****. An 86-year-old woman sustained a fracture of the humerus and underwent surgical fixation 8 weeks ago. There was no radial nerve function below the elbow after surgery. Radiographs are shown in Figures 51a and 51b. What is the most appropriate management at this time?
1- Nerve conduction velocity studies and electromyography
2- Exploration and grafting of the radial nerve
3- Tendon transfers
4- Observation for another 2 months
5- Removal of the plate, neurolysis of the radial nerve, and intramedullary rodding of the humerus
PREFERRED RESPONSE: 4**
**DISCUSSION: Most radial nerve palsies associated with closed fractures of the humerus resolve spontaneously, including Holstein-Lewis lesions (radial nerve palsy associated with oblique distal third fractures of the humerus). Initial sign of recovery at the brachioradialis may not occur for 4 months. There has been no evidence of deleterious effects occurring during this observation period. There are advocates of early exploration of the nerve. Exploration in the intermediate period between 1 and 4 months is not supported. As overall alignment of the fracture is acceptable, there is no need for hardware exchange until nonunion is clearly identified.**
**REFERENCES: Shao YC, Harwood P, Grotz MR, et al: Radial nerve palsy associated with fractures of the shaft of the humerus: A systematic review. J Bone Joint Surg Br 2005;87:1647-1652.**
**Green DP: Radial nerve palsy, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 112.**
**80****. Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
1- Spiral
2- Oblique
3- Transverse
4- Segmental
5- Comminuted
PREFERRED RESPONSE: 3**
**DISCUSSION: A pure bending force produces a transverse fracture pattern. Spiral fractures are mainly rotational, oblique are uneven bending, segmental are four-point bending, and comminuted are either a high-speed torsion or crush mechanism.**
**REFERENCES: Tencer AF, Johnson KD: Biomechanics in Orthopaedic Trauma: Bone Fracture and Fixation. Philadelphia, PA, JB Lippincott, 1994.**
**Gonza ER: Biomechanical long bone injuries, in Gonza ER, Harrington IJ (eds): Biomechanics of Musculoskeletal Injury. Baltimore, MD, Williams & Wilkins, 1982, pp 1-30.**
**Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, p 297.**
**81****. A 20-year-old man sustained an isolated displaced type II odontoid fracture in a motor vehicle accident. He is neurologically intact. Treatment consists of placement in halo traction, and the fracture is reduced. What is the next most appropriate step in treatment?
1- Conversion to a halo vest
2- Closed reduction and conversion to a halo vest
3- Posterior atlantoaxial arthrodesis
4- Odontoid screw fixation
5- Continued halo immobilization
PREFERRED RESPONSE: 1**
**DISCUSSION: The traditional treatment of a reduced type II fracture is a halo vest. A 20-year-old man will tolerate a halo vest better than the elderly or women. Anterior screw fixation has gained increasing support; however, it too has risks and requires a significant learning curve. More recently, C1 lateral mass screws have become more popular. The long-term results and benefits have not yet been determined.**
**REFERENCES: Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 193.**
**Kiovikko MP, Kiuru MJ, Koskinen SK, et al: Factors associated with nonunion in conservatively-treated type-II fractures of the odontoid process. J Bone Joint Surg Br 2004;86:1146-1151.**
**Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, p 1091.**
**Fiore AJ, Haid RW, Rodts GE, et al: Atlantal lateral mass screws for posterior spinal reconstruction: Technical note and case series. Neurosurg Focus 2002;12:E5.**
**82****. A 38-year-old woman fell from a ladder onto her right hip. The radiographs and
CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?
1- Kocher-Langenbeck
2- Iliofemoral
3- Ilioinguinal
4- Extended iliofemoral
5- Triradiate approach
PREFERRED RESPONSE: 3**
**DISCUSSION: The fracture is an associated both column fracture. The best approach for this fracture is the ilioinguinal. The Kocher-Langenbeck is best for posterior injuries to the acetabulum and some transverse fractures. The iliofemoral alone is limited to high anterior column injuries. The extended iliofemoral and triradiate approaches although useful for this fracture, have a higher rate of complications.**
**REFERENCES: Letournel E: The treatment of acetabular fractures through the ilioinguinal approach. Clin Orthop Relat Res 1993;292:62-76.**
**Matta JM: Operative treatment of acetabular fractures through the ilioinguinal approach:
A 10-year perspective. Clin Orthop Relat Res 1994;305:10-19.**
**83****. A 24-year-old man was thrown from a car and is seen in the emergency department with a Glasgow Coma Scale (GCS) score of 8. A CT scan of the head shows no significant bleeding. The patient is hemodynamically stable. The left femur has the closed injury shown on the radiographs in Figures 53a and 53b. What is the best treatment for this patient?
1- Skin traction for the femur, with a follow-up CT scan of the head in the morning
2- Distal femur skeletal traction, with a follow-up CT scan of the head in the morning
3- External fixation of the femur with delayed intramedullary nailing
4- Intramedullary nailing of the femur
5- Ventriculostomy and external fixation of the femur
PREFERRED RESPONSE: 4**
**DISCUSSION: Treatment of patients with a closed head injury and a femoral fracture remains controversial but recent data suggest that intramedullary nails done acutely with avoidance of intraoperative hypotension did not compromise the outcome related to the head injury. This was especially true for high-level GCS scores. A GCS score of lower than 8 and intraoperative hypotension have been associated with worsening outcomes following acute intramedullary nailing of the femur. Skin traction and distal femur skeletal traction in a young adult man with a femoral fracture is not well tolerated secondary to spasm and pain. External fixation is an option but an unnecessary step in the treatment of this patient. Ventriculostomy is not necessary in stable patients with no significant bleeding on a CT scan of the head.**
**REFERENCES: Starr AJ, Hunt JL, Chason DP, et al: Treatment of femur fracture with associated head injury. J Orthop Trauma 1998;12:38-45.**
**Nau T, Kutscha-Lissberg F, Muellner T, et al: Effects of a femoral shaft fracture on multiply injured patients with a head injury. World J Surg 2003;27:365-369.**
**McKee MD, Schemitsch EH, Vincent LO, et al: The effect of a femoral fracture on concomitant closed head injury in patients with multiple injuries. J Trauma 1997;42:1041-1045.**
**Brundage SI, McGhan R, Jurkovich GJ, et al: Timing of femur fracture fixation: Effect on outcome in patients with thoracic and head injuries. J Trauma 2002;52:299-307.**
**84****. An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes
1- plating of the radial shaft fracture and open repair of the triangular fibrocartilage complex.
2- open reduction and internal fixation of the radius and ulna.
3- plating of the radius with closed reduction and evaluation of the distal radioulnar joint (DRUJ).
4- closed reduction of the radius and DRUJ.
5- plating of the radius and pinning of the DRUJ in pronation.
PREFERRED RESPONSE: 3**
**DISCUSSION: This Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction of the radial shaft and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. If not, either open or closed reduction with pinning is undertaken. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.**
**REFERENCE: Rettig ME, Raskin KB: Galeazzi fracture-dislocation: A new treatment-oriented classification. J Hand Surg Am 2001;26:228-235.**
**85****. A 38-year-old man caught his index finger in a volleyball net. He noted an angular deformity of the finger that was reduced when a teammate pulled on his finger. Three weeks later, he now reports trouble extending his finger. A clinical photograph is shown in Figure 55. What anatomic structure is most likely injured?
1- Spiral oblique retinacular ligament
2- Sagittal bands
3- Volar plate
4- Central slip of the extensor tendon
5- Terminal extensor tendon
PREFERRED RESPONSE: 4**
**DISCUSSION: The clinical photograph shows a classic boutonniere deformity. It is likely that the patient sustained a volar dislocation of the proximal interphalangeal joint, with a concomitant rupture of the central slip insertion of the extensor tendon.**
**REFERENCES: Peimer CA, Sullivan DJ, Wild DR: Palmar dislocation of the proximal interphalangeal joint. J Hand Surg Am 1984;9:39-48.**
**Glickel SZ, Barron OA, Catalano LW: Dislocation and ligament injuries in the digits, in
Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 355.**
**86****. A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in
Figures 56a and 56b. What is the most common complication associated with
surgical intervention?
1- Chronic osteomyelitis
2- Planovalgus hindfoot
3- Plantar nerve entrapment
4- Wound dehiscence
5- Painful hardware
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a severe Sanders type 4 calcaneus fracture. By far the most common complication associated with surgical treatment of calcaneus fractures is wound dehiscence.**
**REFERENCES: Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.**
**Sanders R, Fortin P, DiPasquale T, et al: Operative treatment in 120 displaced intra-articular calcaneal fractures: Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res 1993;290:87-95.**
**87****. A 40-year-old woman sustains a flexion injury to her neck. Physical examination is normal. A lateral radiograph of the cervical spine is shown in Figure 57a. MRI scans of the cervical spine are shown in Figures 57b and 57c. Treatment should include
1- skeletal traction and reduction, followed by a halo jacket and nonsurgical stabilization.
2- skeletal traction, closed reduction, and posterior fixation/fusion.
3- skeletal traction, anterior decompression and fusion, followed by posterior stabilization and fusion.
4- skeletal traction and surgical posterior fusion, followed by anterior decompression and fusion.
5- general anesthesia, closed reduction, and a halo jacket for 3 to 4 months until stable.
PREFERRED RESPONSE: 2**
**DISCUSSION: This is a classic bilateral facet dislocation. When there is no evidence of a disk herniation, treatment should include careful skeletal traction, closed reduction, and posterior fusion. There is no role for anterior procedures. These fractures are unstable and require surgical intervention.**
**REFERENCES: Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1120-1128.**
**Coe JD, Warden KE, Sutterlin CE, et al: Biomechanical evaluation of cervical spinal stabilization methods in a human cadaveric model. Spine 1989;14:1122-1131.**
**88****. Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
1- A primed immune system with an increased risk of a systemic inflammatory response
2- Nothing since they are no longer in uncompensated shock and their vital signs have normalized
3- Higher nonunion rates after fracture fixation
4- Higher infection rates after definitive fracture fixation
5- Higher complication rates after temporizing external fixation of long bone fractures
PREFERRED RESPONSE: 1**
**DISCUSSION: Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a “primed” immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered.**
**REFERENCES: Schulman AM, Claridge JA, Carr G, et al: Predictors of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:795-800.**
**Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: Endpoints of resuscitation. J Trauma 2004;57:898-912.**
**89****. A 66-year-old woman was a restrained passenger in an automobile accident. She sustained a direct blow to her nondominant left hand as the airbag in her automobile deployed and she now reports pain, swelling, and difficulty moving her fingers. Radiographs are shown in Figures 58a and 58b. Appropriate definitive treatment should consist of
1- application of a compressive soft dressing, and aggressive edema control and range-of-motion exercises.
2- plaster immobilization without reduction of the fractures.
3- closed reduction and plaster immobilization.
4- surgical fixation of the middle finger metacarpal and closed treatment of the ring and little finger metacarpals.
5- surgical fixation of all three metacarpal fractures.
PREFERRED RESPONSE: 5**
**DISCUSSION: While most isolated metacarpal fractures can be treated nonsurgically, multiple metacarpal fractures are inherently unstable due to the loss of support that an intact adjacent metacarpal provides; therefore, treatment should consist of surgical fixation of all three metacarpal fractures.**
**REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 286.**
**Faraj AA, Davis TR: Percutaneous intramedullary fixation of metacarpal shaft fractures. J Hand Surg Br 1999;24:76-79.**
**90****. A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient’s mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?
1- Emergent four compartment fasciotomies
2- Emergent four compartment fasciotomies and open reduction and internal fixation of the fracture
3- Elevation of the limb overnight and four compartment fasciotomies in the morning
4- Elevation of the limb overnight and a recheck of compartment pressures in the morning
5- Emergent MRI of the knee and leg
PREFERRED RESPONSE: 2**
**DISCUSSION: The patient has a compartment syndrome based on the firm compartments of the leg and the elevated compartment pressures measured at the diastolic pressure reading. Muscle ischemia occurs quickly when compartment pressures are elevated, and within 6 hours irreversible damage can occur. Emergent fasciotomies permit decompression of all four compartments and reestablishment of vascular supply to the muscles. Stabilization of the fracture prevents further soft-tissue injury.**
**REFERENCE: Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 1057-1061.**
**91****. Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
1- The mean arterial blood pressure is above 90 mm Hg.
2- The pulse pressure has normalized.
3- Urine output is greater than 0.5 to 1 mL/kg/h.
4- Oxygen delivery has been maximized.
5- Aerobic metabolism has been restored in all tissue beds.
PREFERRED RESPONSE: 5**
**DISCUSSION: Shock can be defined as inadequate tissue perfusion. Resuscitation or the resolution of shock is defined as when oxygen debt has been repaid, tissue acidosis is eliminated, and aerobic metabolism has been restored in all tissue beds. The end points for resuscitation are not clearly defined, but occult shock can still be present in the setting of normal vital signs and normal urine output due to selective perfusion of organ systems.**
**REFERENCES: Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: End point of resuscitation. J Trauma 2004;57:898-912.**
**Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury, a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.**
**Englehart MS, Schreiber MA: Measurement of acid-base resuscitation end points: Lactate, base deficit, bicarbonate or what? Curr Opin Crit Care 2006;12:569-574.**
**92****. A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
1- Infection
2- Malunion
3- Loss of forearm rotation
4- Refracture
5- Delayed union/nonunion
PREFERRED RESPONSE: 3**
**DISCUSSION: Healing of forearm fractures in skeletally immature patients is the usual outcome. The use of intramedullary fixation has been reported to result in a lower frequency of refractures when compared to plate osteosynthesis due to the absence of diaphyseal holes after plate removal, which are considered stress risers. Regardless of implant technique, malunion and infection are infrequent. Loss of forearm pronation and supination is a common occurrence in surgically treated fractures due to the higher degree of soft-tissue injury, and periosteal stripping leads to fracture site instability and fracture comminution.**
**REFERENCES: Luhmann SJ, Gordon JE, Schoenecker PL: Intramedullary fixation of unstable both-bone forearm fractures in children. J Pediatr Orthop 1998;18:451-456.**
**Mehlman CT, Wall EJ: Injuries to the shafts of the radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 430-436.**
**93****. A 52-year-old woman who is right hand-dominant sustains an injury to her elbow in a fall. A radiograph is shown in Figure 60. The preferred treatment of this injury pattern should include
1- lateral plating of the proximal ulna and fixation of the radial head.
2- Kirschner wire/tension band fixation of the proximal ulna alone.
3- closed reduction and casting.
4- dorsal plating of the proximal ulna and radial head replacement.
5- total elbow arthroplasty.
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a Bado type 2 variant Monteggia fracture with a radial head fracture. The type 2 variant is associated with a higher nonunion rate and poorer outcomes compared to other Bado-type Monteggia fractures. While it is potentially acceptable to repair the radial head, factors such as higher degrees of comminution and older age lead toward replacement as the treatment of choice. Plate and screw fixation is favored over Kirschner wire/tension band fixation because this is not a simple olecranon fracture. Plate placement in a type 2 fracture is dorsal to counteract very high tensile forces associated with fixation failure.**
**REFERENCES: Egol KA, Tejwani NC, Bazzi J, et al: Does a Monteggia variant lesion result in a poor functional outcome? A retrospective study. Clin Orthop Relat Res 2005;438:233-238.**
**Jupiter JB, Leibovic SJ, Ribbans W, et al: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.**
**Konrad GG, Kundel K, Kreuz PC, et al: Monteggia fractures in adults: Long-term results and prognostic factors. J Bone Joint Surg Br 2007;89:354-360.**
**94****. The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
1- Anterior superior iliac spine
2- Sciatic buttress
3- A column of bone running from the anterior inferior iliac spine (AIIS) to the posterior superior iliac spine (PSIS)
4- The most superior portion of the roof of the acetabulum
5- Iliopectineal line
PREFERRED RESPONSE: 3**
**DISCUSSION: The teardrop can be visualized on the obturator outlet view of the pelvis and represents a thick column of bone that runs from the AIIS to the PSIS. Half pins for eternal fixation frames or screws can be inserted into this column for fixation of fractures.**
**REFERENCES: Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273.**
**Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.**
**Kim WY, Hearn TC, Seleem O, et al: Effect of pin location on stability of pelvic external fixation. Clin Orthop Relat Res 1999;361:237-244.**
**95****. A patient was treated with a revision reamed intramedullary nail for a nonunion 6 months ago. A current radiograph is shown in Figure 62. Based on these findings, what is the most appropriate treatment?
1- Electrical stimulation
2- Bone grafting
3- No weight bearing
4- Bone grafting and compression plating
5- Free vascularized bone transport
PREFERRED RESPONSE: 4**
**DISCUSSION: Nonunions after intramedullary nails are often treated with exchange reamed nailing. In a recent study, this resulted in a union rate of 53%. After failed exchange nailing, bone grafting and compression plating should be used. The other options resulted in less satisfactory results as compared to bone grafting and compression plating.**
**REFERENCES: Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nails for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.**
**Bellabarba C, Ricci WM, Bolhofner BR: Results of indirect reduction and plating of femoral shaft nonunions after intramedullary nailing. J Orthop Trauma 2001;15:254-263.**
**96****. Figure 63 shows the radiographs of a 23-year-old man who sustained a twisting injury at work. Swelling, tenderness, and ecchymosis are noted about the entire midfoot. What associated injury is most likely to be problematic?
1- Peroneal tendon tear
2- Lateral process talus fracture
3- Talar neck fracture
4- Lisfranc injury
5- Deltoid ligament tear
PREFERRED RESPONSE: 4**
**DISCUSSION: This cuboid compression fracture (“nutcracker” injury) is associated with subtle injury to the Lisfranc complex. This diagnosis must be made to ensure proper treatment.**
**REFERENCE: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.**
**97****. A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
1- Posterior column/posterior wall acetabular
2- Associated both column acetabular
3- Transverse plus posterior wall acetabular
4- Anterior column posterior hemitransverse acetabular
5- Anterior column acetabular
PREFERRED RESPONSE: 5**
**DISCUSSION: The radiographs and CT scans reveal an anterior column acetabular fracture. The fracture has quadrilateral plate extension but does not exit out the posterior column. The CT scans confirm an intact posterior column and no wall fracture. A transverse fracture is best seen on the CT scan and runs in the sagittal plane, not the coronal plane.**
**REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 115-140.**
**Beaule PE, Dorey FJ, Matta JM: Letournel classification of acetabular fractures: Assessment of interobserver and intraobserver reliability. J Bone Joint Surg Am 2003;85:1704-1709.**
**98****. A 71-year-old woman who reports long-term use of oral steroids for asthma is referred for treatment of a distal humerus fracture. Radiographs reveal diffuse osteopenia and a severely comminuted intra-articular fracture. What is the most appropriate treatment?
1- Long arm cast immobilization
2- Total elbow arthroplasty
3- Open reduction and internal fixation
4- Osteoarticular allograft
5- Resection arthroplasty
PREFERRED RESPONSE: 2**
**DISCUSSION: Several studies have documented the satisfactory outcomes of total elbow arthroplasty when osteosynthesis is not feasible for fixation of a distal humerus fracture, particularly in the physiologically older patient with low functional demands. Total elbow arthroplasty should be considered when a comminuted intra-articular distal humerus fracture occurs in a woman older than age 65 years, particularly with such associated comorbidities as systemic steroid use, osteoporosis, or rheumatoid arthritis.**
**REFERENCES: Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.**
**Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.**
**Garcia JA, Mykula R, Stanley D: Complex fractures of the distal humerus in the elderly: The role of total elbow replacement as primary treatment. J Bone Joint Surg Br 2002;84:812-816.**
**99****. A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
1- Cast removal and measurement of carpal canal pressure
2- Immediate carpal tunnel release and pinning of the fracture
3- Continued observation
4- Surgical reduction and pinning of the fracture
5- Electromyography/nerve conduction velocity studies
PREFERRED RESPONSE: 2**
**DISCUSSION: The patient has an evolving acute carpal tunnel syndrome. Initial management for this injury is to relieve all external pressure that may elevate the neural compression. Surgical decompression of the median nerve at the carpal tunnel is the optimal intervention. Further nonsurgical interventions (cast removal or further bivalving) are insufficient to alleviate the neural compression.**
**REFERENCES: Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.**
**Paley D, McMurtry RY: Median nerve compression by volarly displaced fragments of the distal radius. Clin Orthop Relat Res 1987;215:139-147.**
**100****. A 25-year-old male polytrauma patient undergoes initial temporary external fixation for a femoral shaft fracture. He is converted to a femoral nail at 7 days. This management can be expected to result in
1- higher infection rates.
2- higher nonunion rates.
3- equal union and infection rates.
4- higher rate of ARDS.
5- higher mortality rate.
PREFERRED RESPONSE: 3**
**DISCUSSION: Recently Harwood and associates investigated the principles of damage control orthopaedics (DCO) as they apply to patients with femoral shaft fractures. When they compared those who underwent initial external fixation of femoral shaft fractures with conversion to an intramedullary nail to those who underwent intramedullary nailing as their initial treatment, they found the following: overall infection rates were comparable in patients receiving DCO versus primary intramedullary fixation; open fracture was an independent risk factor for infection regardless of the treatment method; contamination rates in external fixator pin sites rose considerably when left in place more than 2 weeks and logistic regression analysis suggests that infection rates may increase when conversion to an intramedullary nail occurs after 2 weeks following external fixation; and there was no significant difference in time to union among treatment groups.**
**REFERENCES: Harwood PJ, Giannoudis PV, Probst C, et al: The risk of local infective complications after damage control procedures for femoral shaft fracture. J Orthop Trauma 2006;20:181-189.**
**Roberts CS, Pape HC, Jones AL, et al: Damage control orthopaedics: Evolving concepts in the treatment of patients who have sustained orthopaedic trauma. Instr Course Lect
2005;54:447-462. **
QUESTION 35 OF 50
The preferred means for fixation of patellar components is:
1
Large, central patellar lugs
2
Two parallel patellar lugs
3
Three large patellar-fixation lugs
4
Three small peripheral-fixation lugs
5
One central and two peripheral-fixation lugs
Large, central patellar-fixation lugs remove a significant amount of bone, which contributes to patellar fractures. Three small peripheral-fixation lugs are preferred in most designs
QUESTION 36 OF 50
Which of the following lesions would display a low to moderate signal on T1 weighted images and high signal on T2 weighted images:
1
Lipomas
2
Subcutaneous fat
3
Cortical bone
4
Malignant fibrous histiocytoma
5
Tendons
All soft tissue sarcomas have the same signal sequence - low on T1 weighted images and high on T2 weighted images. It is important to remember the appearances of common tissues on both T1 and T2 weighted images:
 T1 weighted T2 weighted
Fat High Moderate Tendons Low Low Ligaments Low Low Fascial layers Low Low Cortical bone Low Low Muscle Moderate Moderate Normal marrow High Moderate Soft tissue sarcomas Low High
Fluid (ganglions, effusions) Low High
Pigmented villonodular synovitis* Very low Very low
Signal drop out (very low signal on gradient echo sequences) Correct Answer: Malignant fibrous histiocytoma
 T1 weighted T2 weighted
Fat High Moderate Tendons Low Low Ligaments Low Low Fascial layers Low Low Cortical bone Low Low Muscle Moderate Moderate Normal marrow High Moderate Soft tissue sarcomas Low High
Fluid (ganglions, effusions) Low High
Pigmented villonodular synovitis* Very low Very low
Signal drop out (very low signal on gradient echo sequences) Correct Answer: Malignant fibrous histiocytoma
QUESTION 37 OF 50
of 100
What is the chief mechanism of action of parathyroid hormone (PTH) in the treatment of patients with osteoporosis?
What is the chief mechanism of action of parathyroid hormone (PTH) in the treatment of patients with osteoporosis?
1
Reduces resorptive activity of osteoclasts
2
Inhibits receptor activator of nuclear factor kappa-B ligand
3
Stimulates osteoblastic bone formation
4
Acts as a selective estrogen modulator
Recombinant human PTH benefits patients with osteoporosis by stimulating osteoblastic bone formation and reducing osteoblastic apoptosis. Treatment reduces vertebral fractures by 65%. PTH analogs act similarly and reduce vertebral fractures by 47%. Bisphosphonates reduce the resorptive activity of
osteoclasts and cause a dissociation of bone formation and resorption that favors bone formation and reduce vertebral fractures by 50% to 70%. Selective estrogen receptor modulators inhibit bone resorption and reduce vertebral fractures by 35%. Humanized monoclonal antibodies inhibit osteoclast formation and reduce vertebral fractures by 68%.
RECOMMENDED READINGS
[Castro-Lionard K, Dargent-Molina P, Fermanian C, Gonthier R, Cassou B. Use of calcium supplements, vitamin D supplements and specific osteoporosis drugs among French women aged 75-85 years: patterns of use and associated factors. Drugs Aging. 2013 Dec;30(12):1029-38. doi: 10.1007/s40266-013-0121-9. PubMed PMID: 24114665. ](http://www.ncbi.nlm.nih.gov/pubmed/24114665)[View](http://www.ncbi.nlm.nih.gov/pubmed/24114665)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24114665)
[Papapoulos S, Makras P. Selection of antiresorptive or anabolic treatments for postmenopausal osteoporosis. Nat Clin Pract Endocrinol Metab. 2008 Sep;4(9):514-23. doi: 10.1038/ncpendmet0941. Review. PubMed PMID: 18714329. ](http://www.ncbi.nlm.nih.gov/pubmed/18714329)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18714329) [Zhang J, Delzell E, Curtis JR, Hooven F, Gehlbach SH, Anderson FA Jr, Saag KG. Use of pharmacologic agents for the primary prevention of osteoporosis among older women with low bone mass. Osteoporos Int. 2014 Jan;25(1):317-24. doi: 10.1007/s00198-013-2444-0. Epub 2013 Aug 28. PubMed PMID: 23982799. ](http://www.ncbi.nlm.nih.gov/pubmed/23982799)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23982799)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23982799)
osteoclasts and cause a dissociation of bone formation and resorption that favors bone formation and reduce vertebral fractures by 50% to 70%. Selective estrogen receptor modulators inhibit bone resorption and reduce vertebral fractures by 35%. Humanized monoclonal antibodies inhibit osteoclast formation and reduce vertebral fractures by 68%.
RECOMMENDED READINGS
[Castro-Lionard K, Dargent-Molina P, Fermanian C, Gonthier R, Cassou B. Use of calcium supplements, vitamin D supplements and specific osteoporosis drugs among French women aged 75-85 years: patterns of use and associated factors. Drugs Aging. 2013 Dec;30(12):1029-38. doi: 10.1007/s40266-013-0121-9. PubMed PMID: 24114665. ](http://www.ncbi.nlm.nih.gov/pubmed/24114665)[View](http://www.ncbi.nlm.nih.gov/pubmed/24114665)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24114665)
[Papapoulos S, Makras P. Selection of antiresorptive or anabolic treatments for postmenopausal osteoporosis. Nat Clin Pract Endocrinol Metab. 2008 Sep;4(9):514-23. doi: 10.1038/ncpendmet0941. Review. PubMed PMID: 18714329. ](http://www.ncbi.nlm.nih.gov/pubmed/18714329)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18714329) [Zhang J, Delzell E, Curtis JR, Hooven F, Gehlbach SH, Anderson FA Jr, Saag KG. Use of pharmacologic agents for the primary prevention of osteoporosis among older women with low bone mass. Osteoporos Int. 2014 Jan;25(1):317-24. doi: 10.1007/s00198-013-2444-0. Epub 2013 Aug 28. PubMed PMID: 23982799. ](http://www.ncbi.nlm.nih.gov/pubmed/23982799)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23982799)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23982799)
QUESTION 38 OF 50
Slide 1
A patient presents with a claw toe deformity (Slide). What is the strongest flexor of the metatarsophalangeal joint, which in this patient is not functioning adequately:
A patient presents with a claw toe deformity (Slide). What is the strongest flexor of the metatarsophalangeal joint, which in this patient is not functioning adequately:
1
Flexor digitorum longus
2
Flexor digitorum brevis
3
Lumbrical
4
Volar plate
5
Interosseous
Although the long and short flexor tendons have some effect albeit indirect on the flexion of the metatarsophalangeal joint, the flexor that acts directly on the joint is the interosseous muscle. Intrinsic atrophy will lead to claw toe deformity.
QUESTION 39 OF 50
A 16-year-old female swimmer reports several episodes of atraumatic glenohumeral instability that occur with different arm positions. Examination reveals generalized ligamentous laxity and a positive sulcus sign, and her shoulder can be subluxated both anteriorly and posteriorly. Initial management should consist of
1
a strengthening program for the rotator cuff and scapular muscles.
2
arthroscopic thermal capsulorrhaphy.
3
an inferior capsular shift.
4
a glenoid osteotomy.
5
a Putti-Platt repair.
The patient has multidirectional instability (MDI). It has been reported that a high percentage of patients with MDI respond to a properly structured exercise program that is continued for at least 3 to 6 months. If nonsurgical management fails to provide relief, stabilization with an inferior capsular shift procedure has been effective in a high percentage of patients. Unidirectional repairs, such as the Putti-Platt procedure, are unsuitable for correcting MDI. Thermal capsulorrhaphy has been reported to have a very high failure rate
(greater than 50%) for treating MDI.
REFERENCES: Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1992;74:890-896.
Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Pollock RG, Owens JM, Flatow EL, et al: Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am
2000;82:919-928.
Miniaci A, Birnie J: Thermal capsular shrinkage for treatment of multidirectional instability of the shoulder. J Bone Joint Surg Am 2003;85:2283-2287.
(greater than 50%) for treating MDI.
REFERENCES: Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1992;74:890-896.
Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Pollock RG, Owens JM, Flatow EL, et al: Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am
2000;82:919-928.
Miniaci A, Birnie J: Thermal capsular shrinkage for treatment of multidirectional instability of the shoulder. J Bone Joint Surg Am 2003;85:2283-2287.
QUESTION 40 OF 50
slide 1 slide 2
A patientâs upper extremity radiographs are shown in Slide 1 and Slide 2. The risk of malignancy in this condition is approximately:
A patientâs upper extremity radiographs are shown in Slide 1 and Slide 2. The risk of malignancy in this condition is approximately:
1
No risk of malignancy
2
5% to 10%
3
25%
4
50%
5
100%
This patient has multiple hereditary exostoses. Note the multiple sessile osteochondromas on the humerus and ulna. A
characteristic bowing deformity of the forearm and pseudo-Madelung deformity of the wrist are also present.
Multiple hereditary exostoses is autosomal dominant. The putative tumor suppressive gene mutation is EXT1, EXT2. The risk of low-grade chondrosarcoma occurring is approximately 10%.
In most patients, the forearm deformity does not cause a major problem and can be treated nonoperatively. Correct Answe 5% to 10%
characteristic bowing deformity of the forearm and pseudo-Madelung deformity of the wrist are also present.
Multiple hereditary exostoses is autosomal dominant. The putative tumor suppressive gene mutation is EXT1, EXT2. The risk of low-grade chondrosarcoma occurring is approximately 10%.
In most patients, the forearm deformity does not cause a major problem and can be treated nonoperatively. Correct Answe 5% to 10%
QUESTION 41 OF 50
Which of the following statements best describes the anatomy of the sartorial branch of the saphenous nerve during medial meniscal repair?
1
The nerve is reliably extrafascial at the joint line.
2
The nerve is anterior to the sartorius.
3
The nerve becomes extrafascial between the gracilis and the semitendinosus.
4
The nerve is anterior to the semitendinosus with the knee in extension.
5
The sartorial branch exits the adductor canal and travels to the anteromedial aspect of the knee.
DISCUSSION: Dunaway and associates reported that the nerve was extrafascial in only 43% of their cadaveric specimens. Therefore, in medial meniscal repair, the nerve may be present during deep dissection. The sartorial branch of the saphenous nerve is posterior to the sartorius; dissection should remain anterior to the sartorius. The branch becomes extrafascial between the gracilis and the sartorius. The nerve is anterior to the semitendinosus with the knee in extension. The infrapatellar branch of the saphenous nerve exits the adductor canal and travels to the anteromedial aspect of the knee.
REFERENCES: Dunaway DJ, Steensen RN, Wiand W, et al: The sartorial branch of the saphenous nerve: Its anatomy at the joint line of the knee. Arthroscopy 2005;21:547-551.
Rodeo SA: Arthroscopic meniscal repair with use of the outside-in technique. Instr Course Lect 2000;49:195-206.
QUESTION 42 OF 50
An 18-year-old male wrestler is injured while picking up an opponent over his head. Witnesses observed his knee buckle out from under him. He is immediately taken to the hospital. On physical examination, his knee is swollen and grossly unstable in multiple planes. Radiographs reveal a located joint without fracture. Distal pulses are palpable. What is the best next step?
67
67
1
Measure compartment pressures.
2
Order a knee MRI scan.
3
Perform ankle-brachial index (ABI).
4
Go to surgery for urgent stabilization of the knee.
Multiple factors need to be considered in the setting of the acutely dislocated knee, but beyond the joint being located, the vascular status of the knee needs to be established to avoid an ischemic limb and possibility of amputation. While palpation for pulses certainly can be performed, an ABI should be performed first in this setting. The patient should be supine and ideally Doppler ultrasonography should be used to detect the pulse. ABI <0.9 has been demonstrated to be 100% sensitive and 100% specific for vascular injury (Mills and associates). Selective angiography can be employed if ABI measures indicate a possible injury. ABI measurements can be affected by existing distal arterial sclerosis or calcification, which would not be expected in this young patient. If pulses are absent or other hard ischemic signs are present, ABI can be foregone for operating room (OR) angiography or an equivalent study to determine the exact location of the vascular injury.
A missed compartment syndrome in the setting of a knee dislocation can be a devastating event leading to ischemia and limb dysfunction or tissue death leading to need for amputation. If a suspected compartment syndrome exists, compartment pressures can be measured directly after ABI, and if needed, compartments can be released in the OR in conjunction with vascular repair (if required). Urgent stabilization can also be done in the OR at the time of vascular repair but is not the most important priority in this setting. Angiograms can be performed in the OR to reduce warm ischemia time if ABI measures are concerning, with vascular repair if indicated. This has been superseded by CT-arteriogram in many trauma centers, which can be performed just prior to OR if indicated.
68
A missed compartment syndrome in the setting of a knee dislocation can be a devastating event leading to ischemia and limb dysfunction or tissue death leading to need for amputation. If a suspected compartment syndrome exists, compartment pressures can be measured directly after ABI, and if needed, compartments can be released in the OR in conjunction with vascular repair (if required). Urgent stabilization can also be done in the OR at the time of vascular repair but is not the most important priority in this setting. Angiograms can be performed in the OR to reduce warm ischemia time if ABI measures are concerning, with vascular repair if indicated. This has been superseded by CT-arteriogram in many trauma centers, which can be performed just prior to OR if indicated.
68
QUESTION 43 OF 50
The abrupt appearance of which of the following collagens heralds the onset of ossification in the physis:
1
Type I
2
Type VI
3
Type X
4
Type II
5
Type IX
The terminal hypertrophiCchondrocytes in the hypertrophiCzone produce Type X collagen. The appearance of Type X collagen heralds ossification. Remember that Type II collagen is the most abundant collagen in the hypertrophiCzone
QUESTION 44 OF 50
Which of the following is the most common cause of osteonecrosis of the femoral head:
1
Corticosteroids
2
Displaced transcervical fracture
3
Nitrogen bubbles
4
Coagulopathies
5
Sickle cell disease
Displaced transcervical fractures of the cervical neck of the femur are the most common cause of osteonecrosis of the femoral head. Although corticosteroid use, nitrogen bubbles, coagulopathies, and sickle cell disease can also cause osteonecrosis, the highest incidence is seen with displaced transcervical fractures
QUESTION 45 OF 50
of 100
A 47-year-old man has left-sided motor weakness in the extensor digitorum longus and extensor hallucis longus, sensory loss in the lateral calf and dorsal foot, and no discernible reflex loss.
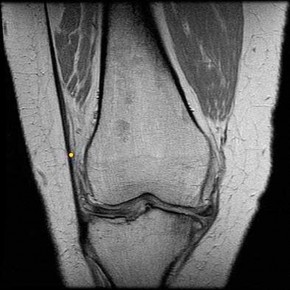
A 47-year-old man has left-sided motor weakness in the extensor digitorum longus and extensor hallucis longus, sensory loss in the lateral calf and dorsal foot, and no discernible reflex loss.
1
Figure 72a Figure 72b
2
Figure 72c Figure 72d
3
Figure 72e Figure 72f
4
Figure 72g Figure 72h
Figures 72a and 72b are the T1-weighted MR images of a disk bulge. Disk bulges are common in asymptomatic people and are not predictive of pathology. Figures 72c and 72d show T1 MR images of a far lateral disk herniation at the L4-L5 level. This would affect the exiting or L4 nerve root. Radicular symptoms would occur at the L4 level. Figures 72e and 72f show an annular tear at the L4-L5 level. This pathology is associated with discogenic low-back pain. Figures 72g and 72h show the T1 MR images of a central lateral disk herniation at the L4-L5 level. This would affect the traversing or L5 nerve root. Radicular symptoms would occur at the L5 level.
RECOMMENDED READINGS
1. [View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15990670)
2. Hoppenfeld S. Physical Exam of the Spine and Extremities. Stamford, CT: Appleton and Lange; 1995.
3. [Madigan L, Vaccaro AR, Spector LR, Milam RA. Management of symptomatic lumbar degenerative disk disease. J Am Acad Orthop Surg. 2009 Feb;17(2):102-11. Review. PubMed PMID: 19202123.](http://www.ncbi.nlm.nih.gov/pubmed/19202123)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19202123)
68
RESPONSES FOR QUESTIONS 76 THROUGH 82
For each MR image above, match the correct structure. The structure is labeled with a yellow dot.
RECOMMENDED READINGS
1. [View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15990670)
2. Hoppenfeld S. Physical Exam of the Spine and Extremities. Stamford, CT: Appleton and Lange; 1995.
3. [Madigan L, Vaccaro AR, Spector LR, Milam RA. Management of symptomatic lumbar degenerative disk disease. J Am Acad Orthop Surg. 2009 Feb;17(2):102-11. Review. PubMed PMID: 19202123.](http://www.ncbi.nlm.nih.gov/pubmed/19202123)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19202123)
68
RESPONSES FOR QUESTIONS 76 THROUGH 82
For each MR image above, match the correct structure. The structure is labeled with a yellow dot.
QUESTION 46 OF 50
An 8-year-old girl has asymmetry on a forward bend test of the spine. She is asymptomatic and has a normal clinical neurologic examination. Radiographs are shown in Figures 22a and 22b. What should be the next step in her work-up?


1
MRI of the cervical thoracic lumbar spine
2
Supine side bending radiographs of the spine
3
Return to the clinic in 12 months with repeat radiographs
4
Anterior and posterior spinal fusion with instrumentation
5
Echocardiogram and renal ultrasound
DISCUSSION: There are several reasons to obtain an MRI of the entire spinal cord of this patient to evaluate for abnormalities. These include her young age and the presence of a left-sided curve. For juvenile scoliosis patients with more than a 20-degree Cobb angle, there is an approximately 20% prevalence of a neurologic abnormality. Therefore, recommendations for work-up include an MRI scan of the entire spine.
REFERENCES: Gillingham BL, Fan RA, Akbamia BA: Early onset idiopathic scoliosis. J Am Acad Orthop Surg 2006;14:101-112.
Gupta P, Lenke LG, Bridwell KH: Incidence of neural axis abnormalities in infantile and juvenile patients with spinal deformity: Is a magnetic resonance image screening necessary? Spine 1998;23:206-210.
**24 • American Academy of Orthopaedic Surgeons**
Figure 23a Figure 23b
REFERENCES: Gillingham BL, Fan RA, Akbamia BA: Early onset idiopathic scoliosis. J Am Acad Orthop Surg 2006;14:101-112.
Gupta P, Lenke LG, Bridwell KH: Incidence of neural axis abnormalities in infantile and juvenile patients with spinal deformity: Is a magnetic resonance image screening necessary? Spine 1998;23:206-210.
**24 • American Academy of Orthopaedic Surgeons**
Figure 23a Figure 23b
QUESTION 47 OF 50
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
1
glenohumeral arthrodesis.
2
total shoulder arthroplasty.
3
humeral arthroplasty.
4
open synovectomy and rotator cuff repair.
5
anterior acromioplasty and rotator cuff repair.
Because the patient has end-stage rheumatoid arthritis with glenoid and rotator cuff deficiency, humeral arthroplasty is the treatment of choice. When a patient has an intact rotator cuff and there is sufficient glenoid bone stock to implant a glenoid component, total shoulder arthroplasty is the preferred method because it appears to provide more predictable pain relief. Glenohumeral arthrodesis is generally avoided when there is a functional deltoid or rotator cuff. Open synovectomy is appropriate in early rheumatoid disease before articular changes are present. Anterior acromioplasty with coracoacromial ligament resection is avoided in patients with rheumatoid arthritis because this procedure compromises the coracoacromial arch and may result in anterosuperior instability.
REFERENCES: Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337.
Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271.
Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Sneppen O, Fruensgaard S, Johannsen HV, Olsen BS, Sojbjerg JO, Anderson NH: Total shoulder replacement in rheumatoid arthritis: Proximal migration and loosening. J Shoulder Elbow Surg 1996;5:47-52.
REFERENCES: Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337.
Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271.
Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Sneppen O, Fruensgaard S, Johannsen HV, Olsen BS, Sojbjerg JO, Anderson NH: Total shoulder replacement in rheumatoid arthritis: Proximal migration and loosening. J Shoulder Elbow Surg 1996;5:47-52.
QUESTION 48 OF 50
A 68-year-old woman reports pain and sensations of instability following a primary total knee arthroplasty 18 months ago. A preoperative radiograph is shown in Figure 39a and postoperative AP and patellar view
radiographs are shown in Figures 39b and 39c. A CT scan shows that the femoral component is internally rotated 8 degrees and the tibial component is internally rotated 4 degrees. Management should include which of the following?
radiographs are shown in Figures 39b and 39c. A CT scan shows that the femoral component is internally rotated 8 degrees and the tibial component is internally rotated 4 degrees. Management should include which of the following?
1
A structured physical therapy program
2
A custom patellar stabilizing brace
3
Modular polyethylene liner exchange to a thicker liner
4
Revision of the femoral and tibial components
5
An open lateral retinacular release
The patient had a valgus knee preoperatively and in these patients, care must be taken to avoid internal rotation of the femoral component that can lead to patellar instability. At the present time she has a completely dislocated patella, evidence of coronal instability on her AP radiograph, and internally rotated femoral and tibial components; therefore, management should consist of revision of both of her components to place them in appropriate external rotation.
REFERENCES: Malo M, Vince KG: The unstable patella after total knee arthroplasty: Etiology, prevention, and management. J Am Acad Orthop Surg 2003; 11:364-371.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 40
The term “paradoxical motion,” used to describe knee kinematics, is best described by which of the following definitions?
1. The patella does not roll forward into the trochlear groove during knee extension.
2. The tibia rolls back on the femur during knee extension.
3. The tibiofemoral contact point moves anteriorly during knee flexion.
4. The posterior cruciate ligament rolls posteriorly with respect to the anterior cruciate ligament during knee extension.
5. The femur rolls back on the tibia during knee flexion.
PREFERRED RESPONSE: 3
DISCUSSION: The term “rollback” describes the posterior movement of the tibiofemoral contact point with knee motion from extension to flexion. Therefore, with “paradoxical rollback” this contact point moves anteriorly. “Paradoxical rollback” is a term used to connote the inability of the anterior cruciate- deficient, posterior cruciate-retaining total knee prosthesis to create normal posterior femoral rollback with knee flexion.
REFERENCES: Dennis DA, Komistek RD, Mahfouz MR: In vivo fluoroscopic analysis of fixed-bearing total knee replacements. Clin Orthop Relat Res 2003;410:114-130.
Incavo SJ, Mullins ER, Coughlin KM, et al: Tibiofemoral kinematic analysis after total knee arthroplasty.
J Arthroplasty 2004;19:906-910.
REFERENCES: Malo M, Vince KG: The unstable patella after total knee arthroplasty: Etiology, prevention, and management. J Am Acad Orthop Surg 2003; 11:364-371.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 40
The term “paradoxical motion,” used to describe knee kinematics, is best described by which of the following definitions?
1. The patella does not roll forward into the trochlear groove during knee extension.
2. The tibia rolls back on the femur during knee extension.
3. The tibiofemoral contact point moves anteriorly during knee flexion.
4. The posterior cruciate ligament rolls posteriorly with respect to the anterior cruciate ligament during knee extension.
5. The femur rolls back on the tibia during knee flexion.
PREFERRED RESPONSE: 3
DISCUSSION: The term “rollback” describes the posterior movement of the tibiofemoral contact point with knee motion from extension to flexion. Therefore, with “paradoxical rollback” this contact point moves anteriorly. “Paradoxical rollback” is a term used to connote the inability of the anterior cruciate- deficient, posterior cruciate-retaining total knee prosthesis to create normal posterior femoral rollback with knee flexion.
REFERENCES: Dennis DA, Komistek RD, Mahfouz MR: In vivo fluoroscopic analysis of fixed-bearing total knee replacements. Clin Orthop Relat Res 2003;410:114-130.
Incavo SJ, Mullins ER, Coughlin KM, et al: Tibiofemoral kinematic analysis after total knee arthroplasty.
J Arthroplasty 2004;19:906-910.
QUESTION 49 OF 50
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20° of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked “A,” the resulting ligament reconstruction will excessively**
1
tighten as the knee extends past 10° of flexion.
2
tighten as the knee flexes past 90°.
3
loosen as the knee extends past 10° of flexion.
4
loosen as the knee flexes past 30°.
5
loosen as the knee flexes past 90°.
If the femoral tunnel is created using guide wire A, it will be too far anterior in the intercondylar notch. The distance between a central tibial insertion for the ACL and an anterior femoral tunnel will progressively increase as the knee is flexed. Therefore, if the graft is tensioned near extension, the ligament will excessively tighten as the knee flexes past 90°. This will result in restricted knee flexion or failure of the graft as full flexion is gained. There will be little effect on the ligament as it extends from 20° to 0° of flexion. If the graft is tensioned in significant flexion (greater than 60°), it will be excessively loose as the knee fully extends.
REFERENCES: Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
REFERENCES: Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
QUESTION 50 OF 50
Which of the following is a risk factor for the development of a postoperative periprosthetiCfracture of the humerus:
1
Diabetes
2
Female gender
3
Age
4
Diagnosis of avascular necrosis
5
Polyethylene-induced osteolysis
Osteolysis, osteopenia, and aggressive cortical reaming have been reported as potential risk factors for the development of a postoperative periprosthetiCfracture
