Score: 0%
Advanced Orthopedic Mock Exam (Set B29D06)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
of 100
A 73-year-old woman has back and leg pain. Imaging reveals a lumbar degenerative scoliosis. Nonsurgical management, consisting of physical therapy, medications, and injections, has failed. During the surgical planning, dual-energy x-ray absorptiometry is performed, and her T-score returns as -2.6. Intraoperative options to help reduce the risk of instrumentation failure include
A 73-year-old woman has back and leg pain. Imaging reveals a lumbar degenerative scoliosis. Nonsurgical management, consisting of physical therapy, medications, and injections, has failed. During the surgical planning, dual-energy x-ray absorptiometry is performed, and her T-score returns as -2.6. Intraoperative options to help reduce the risk of instrumentation failure include
1
teriparatide injection.
2
multilevel interbody fusion.
3
augmentation of pedicle screws with polymethylmethacrylate (PMMA).
4
iliac crest bone graft.
■
Instrumentation of the osteoporotic spine is becoming more common as the population ages. Some intraoperative options to reduce pedicle screw failure rates include augmenting the pedicle screw with PMMA, using a fenestrated screw designed for injection of the PMMA through the screw, and using hydroxyapatite coated screws. Teriparatide is a parathyroid hormone analogue used as a second-line treatment for osteoporosis. Preoperative administration potentially can increase bone quality. Postoperative administration of teriparatide has been shown to increase lumbar fusion rates. In the setting of osteoporosis, multilevel interbody fusion can increase the risk of implant subsidence. Although iliac crest bone graft is the gold standard graft used to obtain fusion, it does not have immediate impact on the rate of implant failure in osteoporosis.
Instrumentation of the osteoporotic spine is becoming more common as the population ages. Some intraoperative options to reduce pedicle screw failure rates include augmenting the pedicle screw with PMMA, using a fenestrated screw designed for injection of the PMMA through the screw, and using hydroxyapatite coated screws. Teriparatide is a parathyroid hormone analogue used as a second-line treatment for osteoporosis. Preoperative administration potentially can increase bone quality. Postoperative administration of teriparatide has been shown to increase lumbar fusion rates. In the setting of osteoporosis, multilevel interbody fusion can increase the risk of implant subsidence. Although iliac crest bone graft is the gold standard graft used to obtain fusion, it does not have immediate impact on the rate of implant failure in osteoporosis.
QUESTION 2 OF 50
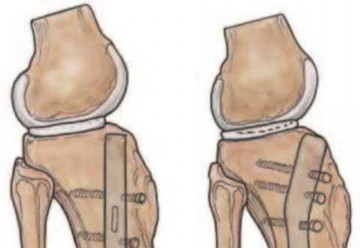
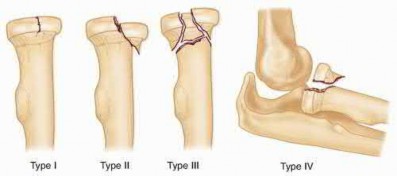
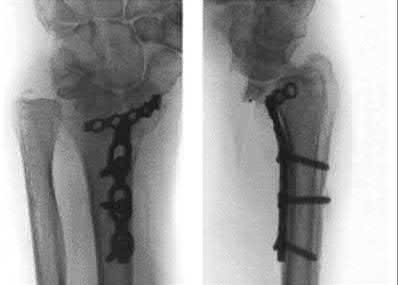
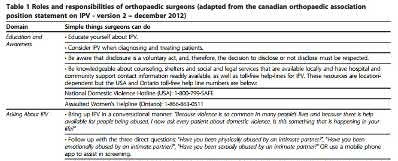
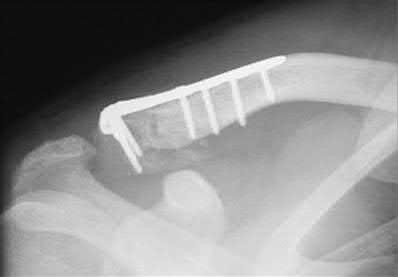
Figure 94 shows the lateral radiograph of an 80-year-old woman who is an independent ambulator and has a supracondylar periprosthetic fracture around the knee. What is the most appropriate management for this patient?
1
Closed reduction and nonsurgical management
2
Open reduction and internal fixation using a distal femoral locking plate
3
Open reduction and internal fixation using an intramedullary rod
4
Revision total arthroplasty using distal femoral allograft
5
Revision total knee arthroplasty using distal femoral replacement
DISCUSSION: A supracondylar femoral periprosthetic fracture that is a reducible or an irreducible fracture with poor distal bone stock and in the vicinity of loose or malpositioned components (type III) is very difficult to treat. One of the treatment options for patients with a loose femoral component and poor bone stock is the use of distal femoral replacement. The distal femoral replacement can be performed with relative ease, expediency, and is best suited for elderly or sedentary patients.
REFERENCES: Kassab M, Zalzal P, Azores GM, et al: Management of periprosthetic femoral fractures after total knee arthroplasty using a distal femoral allograft. J Arthroplasty 2004;19:361-368.
Kim KI, Egol KA, Hozack WJ, et al: Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res
2006;446:167-175.
REFERENCES: Kassab M, Zalzal P, Azores GM, et al: Management of periprosthetic femoral fractures after total knee arthroplasty using a distal femoral allograft. J Arthroplasty 2004;19:361-368.
Kim KI, Egol KA, Hozack WJ, et al: Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res
2006;446:167-175.
QUESTION 3 OF 50
Hepatocellular necrosis has been observed with high levels of in the body.
1
Al
2
Co
3
Cr
4
V
5
Ni
Hepatocellular necrosis often occurs in response to high levels of metal in the body, as observed after acute ingestion of Cr (VI) in humans
QUESTION 4 OF 50
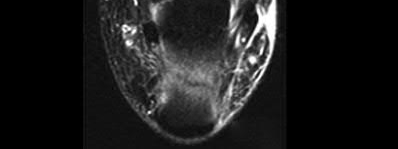
Surgical repair of the injury shown in the MRI scans in Figures 1 through 4 through a single-incision approach has a higher incidence of
33
33
1
heterotopic ossification.
2
posterior interosseous nerve injury.
3
secondary surgery.
4
lateral antebrachial cutaneous nerve injury.
The MRI scans show a distal biceps tendon avulsion with significant retraction. When addressing these injuries, a single-incision approach has been associated with an increased risk of lateral antebrachial cutaneous nerve injury. A two-incision approach has been associated with an increased risk of heterotopic ossification, second surgeries and posterior interosseous nerve injury.
34
34
QUESTION 5 OF 50
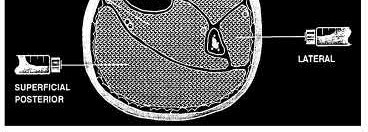
Which of the following leg muscles often has its own fascial envelope (separate compartment):
1
Anterior tibialis muscle
2
Posterior tibialis muscle
3
Peroneus longus muscle
4
Flexor digitorum longus muscle
5
Flexor hallucis longus muscle
Of the four compartments, the deep posterior compartment is the most difficult to release. The surgeon must release the soleus muscle from the tibia to decompress the deep posterior compartment.
The tibialis posterior muscle often has its own fascial sheath in the deep posterior compartment. When a surgeon releases the deep posterior compartment, this fascial sheath (if present) should be released.
The tibialis posterior muscle often has its own fascial sheath in the deep posterior compartment. When a surgeon releases the deep posterior compartment, this fascial sheath (if present) should be released.
QUESTION 6 OF 50
Figures below depict the radiographs obtained from a 60-year-old man with instability and pain 1 year after
primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to
3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1%
neutrophils. No growth of organisms is seen on routine culture. What is the best next step?

primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to
3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1%
neutrophils. No growth of organisms is seen on routine culture. What is the best next step?
1
Revision total knee arthroplasty with extensor mechanism allograft
2
Revision total knee arthroplasty with liner change and primary quadriceps repair
3
Resection knee arthroplasty and arthrodesis with antegrade nail
4
Two-stage revision total knee arthroplasty with extensor mechanism allograft
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results
show no signs of infection, so a single-stage procedure is preferred.
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results
show no signs of infection, so a single-stage procedure is preferred.
QUESTION 7 OF 50
Which of the following statements best characterizes a Dega osteotomy as a distinct osteotomy from a Salter osteotomy:
1
The Dega osteotomy is stabilized by threaded pins.
2
The Dega osteotomy lengthens the ipsilateral limb.
3
The Salter osteotomy hinges upon the triradiate cartilage.
4
The Dega osteotomy hinges upon the medial pelvic cortex.
5
The Dega osteotomy should only be done after triradiate cartilage closure.
The Dega osteotomy, originally described in Poland in 1964, is an incomplete transiliac osteotomy. The medial pelvic cortex is largely preserved, and the osteotomy hinges upon this point. Both osteotomies are best performed in young children, before triradiate cartilage closure. The Salter osteotomy is stabilized by pins, so the Dega needs no internal fixation. The Salter osteotomy lengthens the limb because it is a complete osteotomy.
QUESTION 8 OF 50
of 100
The patient fails nonsurgical treatment. What is the best next step?
The patient fails nonsurgical treatment. What is the best next step?
1
CT scan
2
MRI
3
Bone scan
4
Laboratory studies: complete blood count (CBC) with differential, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), antinuclear antibody (ANA), and rheumatoid factor (RF)
- CT scan
QUESTION 9 OF 50
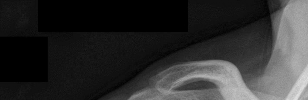
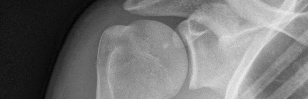
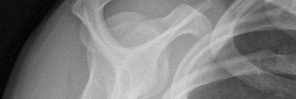
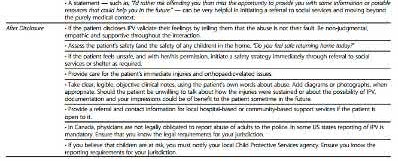
Figures 1 and 2 are the most recent radiographs of an 18-year-old high school student who sustains an anterior shoulder dislocation playing recreational football. He has a low Beighton score on physical examination. He was closed reduced and underwent a course of physical therapy but had a second dislocation playing recreational basketball. What is the most appropriate course of treatment, with the lowest complication rate, to prevent further dislocation?


1
Arthroscopic Bankart procedure
2
Physical therapy
3
SAWA shoulder brace
4
Latarjet procedure
The patient has recurrent instability and is at a high rate of further dislocations due to his young age. Therefore, therapy and bracing are unlikely to decrease his dislocation rate. The radiographs are normal, and there is no Hill-Sachs lesion or bony Bankart lesion. His instability severity index score is 3, and; therefore, a bony procedure such as Latarjet is not necessary. Furthermore, the rate of complication following a Latarjet procedure, especially nerve
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
QUESTION 10 OF 50
A 13-year-old girl with idiopathic adolescent scoliosis has a 32° right thoracolumbar curve. Her Risser sign is 1. Her curve measured 29° 4 months ago. You recommend:
1
Observing until the curve reaches 34°
2
Ordering a magnetic resonance image of the spine
3
Physical therapy to control the curve
4
Electrical stimulation to the paraspinal muscles
5
A thoracolumbosacral orthosis
Idiopathic scoliosis in skeletally immature patients should be braced if it is greater than 30° and significant growth remains (estimated by a Risser sign of 0, 1, or 2). Studies have shown that patients with idiopathic scoliosis without atypical findings do not need magnetic resonance imaging. Physical therapy and electrical stimulation have been shown not to have any effect on the progression of idiopathic scoliosis.
QUESTION 11 OF 50
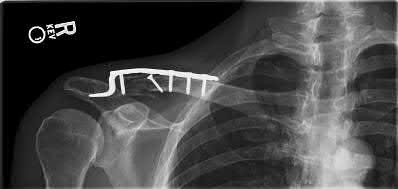
A 51-year-old man sustains the injury shown in the MRI scan in Figures 1 and 2 following a fall. After a thorough discussion regarding risks and benefits, he elects to proceed with surgery. What is the most appropriate surgical treatment for his fracture?
1
Open reduction internal fixation with locking plate
2
Intramedullary (IM) nail
3
Hemiarthroplasty
4
Closed reduction and percutaneous pinning
The patient has sustained a complex proximal humerus fracture with head split component and multiple articular fragments. When the articular surface is significantly compromised, arthroplasty procedures are favored. The only procedure listed that addresses the damaged humeral head is hemiarthroplasty, making it the correct response. Although a possible option, ORIF would be difficult due to the fragmented humeral head, and there would be a high risk for fracture collapse or avascular necrosis. IM nailing will not provide enough control of the fracture pieces, nor will it replace the damaged articular surface. Closed reduction is not an option given the complex nature of the fracture.
QUESTION 12 OF 50
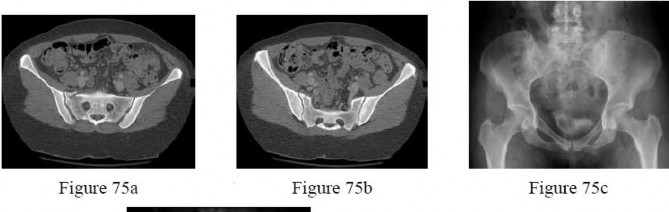
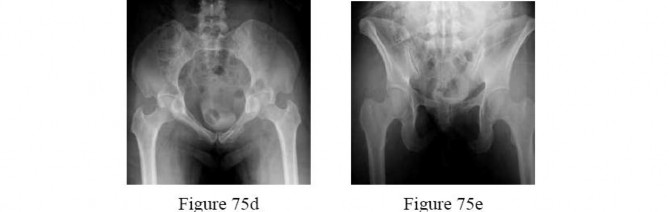
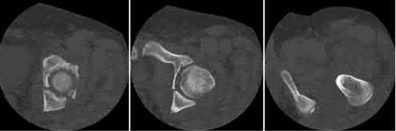
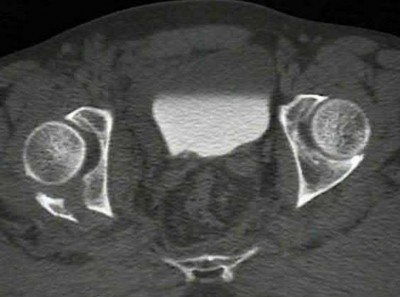
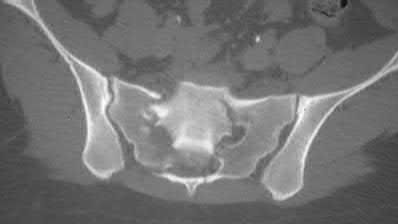
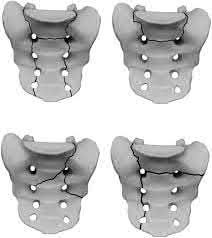
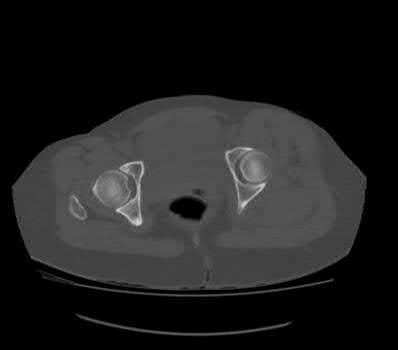
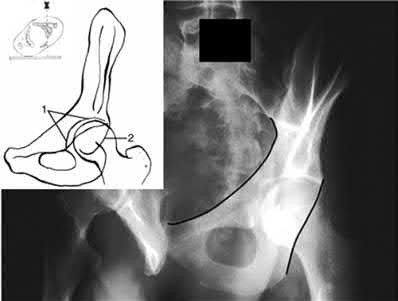
- are the CT scans and radiographs of a 56-year-old man who is a restrained driver involved in a motor vehicle accident in which his car is struck at 35 mph. He has pain to the right buttock and groin regions. Examination reveals that he is neurologically intact and has no evidence of other injuries. What is the most appropriate management at this time?
1
Anterior pelvic external fixation
2
Iliosacral screw fixation on the right side
3
Open reduction and internal fixation of the sacrum
4
Bed rest for 1 to 2 weeks, followed by non-weight-bearing on the right side for 4 weeks
5
Immediate mobilization and weight bearing as tolerated on the right lower extremity
No detailed explanation provided for this question.
QUESTION 13 OF 50
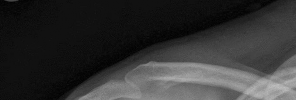
Figure 1 is the radiograph of a 13-year-old right-hand dominant male baseball pitcher who presents with new onset right shoulder pain. Over the past month, he has participated in several tournaments. He was unable to complete his most recent game secondary to continued pain while throwing. Examination reveals a healthy, adolescent male in no apparent distress. Range-of-motion examination of the bilateral shoulders is symmetric with mild pain at the end points of motion. He reports pain on palpation over the lateral aspect of his deltoid. What pathologic process is most likely responsible for this patient's pain?
1
Posterior capsular tightness
2
Excessive humeral retroversion
3
Internal impingement of the articular side of supraspinatus
4
Microtrauma to proximal humeral physis
48
The clinical vignette describes a 13-year-old boy with Little Leaguers’ shoulder. This is an injury to the proximal humerus growth plate specifically involving the hypertrophic zone of the physis. This condition is considered a Salter-Harris 1 injury to the proximal humerus physis and most commonly affects male throwing athletes ages 11 to 16. The proximal humerus growth plate closes between the ages of 18 to 21. The mechanism of injury involves microtrauma to the growth plate from exposure to excessive rotational torque and distraction forces during the late cocking; early acceleration and deceleration phases of throwing, respectively. High pitch counts have been implicated as risk factors for injury. The diagnosis is frequently made clinically; however, radiographs of the shoulder may reveal widening of the proximal humeral physis in comparison with the contralateral side. Treatment includes cessation of throwing for 3 to 6 months. The patient should be asymptomatic prior to return to a throwing program. Physical therapy and a program of guided return to throwing that enforces proper pitching mechanics can be helpful during a return to play. Following established pitch counts and allowing for appropriate rest before throwing can help to prevent future recurrence.
The clinical vignette describes a 13-year-old boy with Little Leaguers’ shoulder. This is an injury to the proximal humerus growth plate specifically involving the hypertrophic zone of the physis. This condition is considered a Salter-Harris 1 injury to the proximal humerus physis and most commonly affects male throwing athletes ages 11 to 16. The proximal humerus growth plate closes between the ages of 18 to 21. The mechanism of injury involves microtrauma to the growth plate from exposure to excessive rotational torque and distraction forces during the late cocking; early acceleration and deceleration phases of throwing, respectively. High pitch counts have been implicated as risk factors for injury. The diagnosis is frequently made clinically; however, radiographs of the shoulder may reveal widening of the proximal humeral physis in comparison with the contralateral side. Treatment includes cessation of throwing for 3 to 6 months. The patient should be asymptomatic prior to return to a throwing program. Physical therapy and a program of guided return to throwing that enforces proper pitching mechanics can be helpful during a return to play. Following established pitch counts and allowing for appropriate rest before throwing can help to prevent future recurrence.
QUESTION 14 OF 50
What is the treatment of choice for the injury shown in Figures 20a through 20c?
1
Closed reduction and a short arm cast
2
Splinting in a functional position and early motion
3
Closed or open reduction and internal fixation with Kirschner wires
4
Open reduction and internal fixation with mini-fragment screws
5
Primary arthrodeses of the carpometacarpal joints
The radiographs show multiple carpometacarpal dislocations. Reduction is often obtainable but difficult to maintain. Internal fixation is required to maintain the reduction, preferably with Kirschner wires. Closed reduction and percutaneous pinning is preferred by some surgeons. Others recommend open reduction to remove irreconstructable osteochondral fragments from the individual joints and to ensure correct reduction of the carpometacarpal joints. Kirschner wires are removed at 6 to 8 weeks.
REFERENCES: Prokuski LJ, Eglseder WA Jr: Concurrent dorsal dislocations and fracture-dislocations of the index, long, ring, and small (second to fifth) carpometacarpal joints. J Orthop Trauma 2001;15:549-554.
Lawlis JF III, Gunther SF: Carpometacarpal dislocations: Long-term follow-up. J Bone Joint Surg Am 1991;73:52-59.
REFERENCES: Prokuski LJ, Eglseder WA Jr: Concurrent dorsal dislocations and fracture-dislocations of the index, long, ring, and small (second to fifth) carpometacarpal joints. J Orthop Trauma 2001;15:549-554.
Lawlis JF III, Gunther SF: Carpometacarpal dislocations: Long-term follow-up. J Bone Joint Surg Am 1991;73:52-59.
QUESTION 15 OF 50
Longevity of traditional total hip arthroplasty in young patients is limited by:
1
Implant failure
2
Infection
3
Fracture
4
Osteolysis and aseptiCloosening
5
Limited range of motion
Although implant failure, infection, and fracture occur with extended lifetime of hip implants, polyethylene wear debris and eventual aseptiCloosening are the most commonly recognized limitation in the survival of total hip arthroplasty. Limited range of motion is a less common presentation for implant failure in the hip
QUESTION 16 OF 50
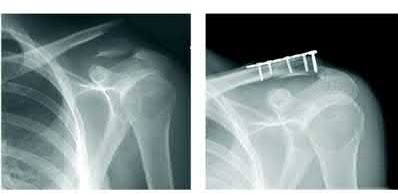
Figures 1 through 3 are the radiographs of a 55-year-old woman who fell on her outstretched right arm, resulting in acute elbow pain and swelling. On examination, she has lateral elbow bruising and tenderness, with a mechanical block to forearm supination and pronation. She has no medial tenderness. During surgery through a direct lateral approach, the surgeon observes a completely bare lateral epicondyle and surgical repair is performed, resulting in a stable and congruent joint. Initial postoperative rehabilitation should include
1
3 weeks of cast immobilization.
2
elbow extension exercises with the forearm supinated.
3
elbow extension exercises with the forearm pronated.
4
elbow extension exercises with the forearm in neutral rotation.
Radial head fractures are thought to occur as a result of valgus posterolateral rotary load across the elbow, although the mechanism can certainly vary. Minimally or nondisplaced fractures without any clinical instability or block to motion can often be successfully managed non-surgically. Fractures with >2 mm of displacement or fragments that block motion require surgical repair. A critical aspect during surgery is identifying concomitant injury to the lateral collateral ligament complex (LCL). When encountered, the LCL is most often avulsed from its origin at the lateral epicondyle, resulting in a bare area. After the radial head is either repaired or replaced (Figures 4 and 5), the LCL should
16
be repaired back to its anatomic origin. Postoperatively, the surgeon must communicate to the therapist that elbow extension exercises should be performed with the forearm in pronation as a result of the compromised LCL, as this position places the least stress on the ligamentous repair. Elbow extension exercises in supination or neutral are recommended for compromise of the medial collateral ligament, or combined medial and lateral ligament injury, respectively. Without any medial elbow bruising, swelling, or tenderness, it is unlikely that the patient has an injury to the medial collateral ligament.
16
be repaired back to its anatomic origin. Postoperatively, the surgeon must communicate to the therapist that elbow extension exercises should be performed with the forearm in pronation as a result of the compromised LCL, as this position places the least stress on the ligamentous repair. Elbow extension exercises in supination or neutral are recommended for compromise of the medial collateral ligament, or combined medial and lateral ligament injury, respectively. Without any medial elbow bruising, swelling, or tenderness, it is unlikely that the patient has an injury to the medial collateral ligament.
QUESTION 17 OF 50
Dupuytrenâs cord tissue is characterized by what change from normal:
1
An increase in type II collagen
2
A decrease in type III collagen
3
An increase of type III collagen
4
Abnormal collagen crosslinks
5
Increased hyaluronidase
C ompared to normal palmar fascia, the fibrous bands in Dupuytrenâs disease have an increased ratio of type III to type I
collagen, and an overall increase in the amount of type III collagen.
collagen, and an overall increase in the amount of type III collagen.
QUESTION 18 OF 50
of 100
Based on this patient's MR images, at which location would you expect to find altered sensation?
Based on this patient's MR images, at which location would you expect to find altered sensation?
1
Medial side of left leg
2
Medial side of left foot
3
Dorsum of left foot
4
Lateral aspect of left foot
- Lateral aspect of left foot
QUESTION 19 OF 50
A 30-year-old black woman presents with complaints of pain in the tip of her right index finger. The pain started approximately 6 months ago and becomes intense in cold weather. She also states that her nail on the index finger does not look as good as the others despite regular manicures. You notice a bluish discoloration and ridging of the nail. The nail is not split, but it appears clubbed. The patient does not have a history of respiratory or hemodynamic disease and appears healthy. The nail is exquisitely tender on pressure, but no mass is palpable. Two-point discrimination is intact and capillary refill is good. Radiographs do not reveal bony destruction, but you notice pressure indentation over the distal phalanx. The joint space is preserved, and the
patient has full range of motion. Based on your clinical diagnoses, the histological findings will include which of the following:
patient has full range of motion. Based on your clinical diagnoses, the histological findings will include which of the following:
1
Well-formed vascular channels with nonmyelinated nerve endings
2
Mucous islands with blood vessels
3
Giant cells filled with inflammatory cells in the interstitium
4
Negatively birefringent cystals
5
Amorphous calcium in pseudocapsule
Glomus tumors consist of well-formed vascular channels with nonmyelinated nerve endings. Glomus tumors are not associated with mucous islands or giant cells. Negatively birefringent crystals are found in patients with gout. The presentation of this patient does not suggest gout. Amorphous calcium in a pseudocapsule is diagnostic of calcinosis. C alcinosis occurs intracutaneoulsy or subcutaneously. These deposits can be tender but are not effected by changes in weather, as are glomus tumors.
QUESTION 20 OF 50
When treating a proximal tibia fracture, the surgeon decides to
(1) use blocking screws in the proximal fragment, and (2) pick the intramedullary nail based on the location of the Herzog curve. Which of the following combinations will best prevent the classic deformity associated with this fracture?
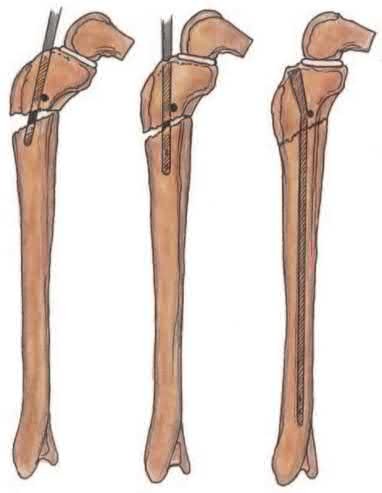
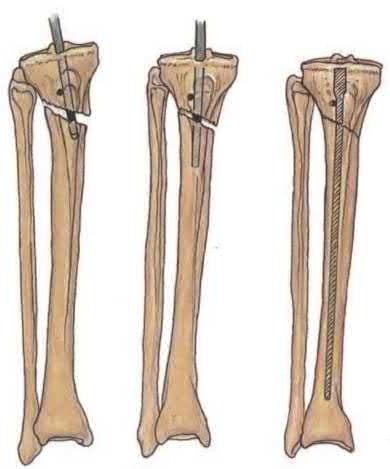

(1) use blocking screws in the proximal fragment, and (2) pick the intramedullary nail based on the location of the Herzog curve. Which of the following combinations will best prevent the classic deformity associated with this fracture?
1
Place blocking screws medial and posterior to the nail. Use a nail with a Herzog curve proximal to the fracture site.
2
Place blocking screws medial and posterior to the nail. Use a nail with a Herzog curve distal to the fracture site.
3
Place blocking screws lateral and posterior to the nail. Use a nail with a Herzog curve proximal to the fracture site.
4
Place blocking screws lateral and posterior to the nail. Use a nail with a Herzog curve distal to the fracture site.
5
Place blocking screws lateral and anterior to the nail. Use a nail with a Herzog curve proximal to the fracture site.
Proximal tibial fractures develop an apex anterior (procurvatum) and valgus malalignment. Blocking (poller) screws should be placed in the concavity of the deformity, thus posterior and lateral to the nail. The Herzog curve should be proximal to the fracture site.
Up to 58% of proximal tibial fractures are malaligned. Malalignment arises because the nail fits loosely in the wide metaphyses and cannot control alignment. Without close fit of the nail at the fracture site, the nail will not align the fracture independent of a stable reduction and careful nail path. Blocking screws serve to reduce the size of the proximal metaphyseal canal and guide final nail passage.
Stinner et al. discuss strategies in proximal tibial fracture nailing. They describe an accurate starting point (using the twin peaks AP view or fibular bisector AP view, and flat plateau lateral view). They emphasize fracture reduction prior to reaming and implant placement.
Hiesterman reviewed nailing of extra-articular proximal tibial fractures. Techniques described include blocking screws, unicortical plating, using a universal distractor, nailing in flexion/locking in extension, semiextended nailing (including percutaneous suprapatellar quads-splitting approaches), multiple proximal interlocking screws (>=3).
Illustration A shows placement of a coronal blocking screw. Illustration B shows placement of a sagittal blocking screw. Illustration C shows the effect of the Herzog curve. A more distal Herzog curve leads to a "wedge" effect and fracture displacement whereas a proximal Herzog curve contains the fracture.
The "wedge" effect occurs as the nail is seated and impinges on the posterior cortex of the distal segment accentuating an apex anterior deformity because of the effective widening of the nail above the bend and posterior force on the distal segment to match the nail shape.
Incorrect Answers:
Answers 1, 2, 4, 5: Blocking screws in the proximal fragment should be lateral and posterior to the nail. The Herzog curve should be proximal to the fracture site.
Up to 58% of proximal tibial fractures are malaligned. Malalignment arises because the nail fits loosely in the wide metaphyses and cannot control alignment. Without close fit of the nail at the fracture site, the nail will not align the fracture independent of a stable reduction and careful nail path. Blocking screws serve to reduce the size of the proximal metaphyseal canal and guide final nail passage.
Stinner et al. discuss strategies in proximal tibial fracture nailing. They describe an accurate starting point (using the twin peaks AP view or fibular bisector AP view, and flat plateau lateral view). They emphasize fracture reduction prior to reaming and implant placement.
Hiesterman reviewed nailing of extra-articular proximal tibial fractures. Techniques described include blocking screws, unicortical plating, using a universal distractor, nailing in flexion/locking in extension, semiextended nailing (including percutaneous suprapatellar quads-splitting approaches), multiple proximal interlocking screws (>=3).
Illustration A shows placement of a coronal blocking screw. Illustration B shows placement of a sagittal blocking screw. Illustration C shows the effect of the Herzog curve. A more distal Herzog curve leads to a "wedge" effect and fracture displacement whereas a proximal Herzog curve contains the fracture.
The "wedge" effect occurs as the nail is seated and impinges on the posterior cortex of the distal segment accentuating an apex anterior deformity because of the effective widening of the nail above the bend and posterior force on the distal segment to match the nail shape.
Incorrect Answers:
Answers 1, 2, 4, 5: Blocking screws in the proximal fragment should be lateral and posterior to the nail. The Herzog curve should be proximal to the fracture site.
QUESTION 21 OF 50
At which of the following sites is 25 hydroxyvitamin D3 converted into the active hormone 1,25 dihydroxyvitamin D3:
1
Skin
2
Liver
3
Kidney
4
Parathyroid hormone
5
Small intestine
Vitamin D3 is converted into its active form in the proximal tubules of the kidney. The active form is 1,25 dihydroxyvitamin D3. Remember that the liver performs the conversion to 25 hydroxyvitamin D3 and the kidney further hydroxylates to 1,25
dihydroxyvitamin D3. Correct Answer: Kidney
dihydroxyvitamin D3. Correct Answer: Kidney
QUESTION 22 OF 50
The gold standard for the diagnosis of avascular necrosis of the femoral head is:
1
Bone scan
2
Routine roentgenogram
3
MagnetiCresonance image
4
Segmented bone collapse
5
Elevated sedimentation rate
The gold standard for the diagnosis of avascular necrosis is magnetiCresonance imaging. Changes can be seen earliest with this technique before there are changes on routine roentgenogram and even before a patient is symptomatic
QUESTION 23 OF 50
A 68-year-old man underwent a primary total hip arthroplasty 2 years ago for a femoral neck fracture. His early postoperative course was unremarkable, but he notes some aching in the thigh since surgery. His symptoms have gotten worse over the last year, such that he now has activity-related thigh pain that limits his walking ability. An AP hip radiograph is shown in Figure 9. What is the most appropriate surgical management?

1
No surgery is indicated
2
Revision of the acetabular component
3
Revision of the femoral component
4
Psoas tendon tenotomy
5
Strut grafting of the femur to stiffen the bone near the tip of the implant
DISCUSSION: The radiograph shows a loose femoral component with failure of osseous integration.
There is a reactive radiolucent line around the fiber mesh portion of the implant, hypertrophy of the bone under the collar, and a pedestal formation at the distal tip of the implant, all of which indicate failure of bone ingrowth. If
bone ingrowth had occurred, there would be stress shielding of bone under the collar.
REFERENCES: Engh CA, Massin P, Suthers KE: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop Relat Res 1990;257:107-128.
Lieberman JR, Huo MH, Schneider R, et al: Evaluation of painful hip arthroplasties: Are technetium bone scans necessary? J Bone Joint Surg Br 1993;75:475-478.
Vresilovic EJ, Hozack WJ, Rothman RH: Radiographic assessment of cementless femoral components: Correlation with intraoperative mechanical stability. J Arthroplasty 1994;9:137-141.
Figure 10
QUESTION 24 OF 50
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. Radiographs of the player’s right ankle confirm there are no fractures. With a lateral talar tilt test result of 19°, which additional structure is most likely damaged?
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. Radiographs of the player’s right ankle confirm there are no fractures. With a lateral talar tilt test result of 19°, which additional structure is most likely damaged?
1
Deltoid ligament
2
Calcaneofibular ligament
3
Anterior tibiofibular ligament
4
Posterior tibiofibular ligament
The anterior drawer test is performed with the ankle in 10° of plantar flexion, which results in the greatest amount of translation. The test investigates the integrity of the anterior talofibular ligament with a key distance of translation being 8 to 10 mm. While the patient is sitting and has her knees flexed over the edge of a table or bench, the physician uses one hand to stabilize the distal leg and with the other hand applies an anterior force to the heel in an attempt to gap the talus anteriorly from under the tibia. The
anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization _and a guided rehabilitation program that emphasizes proprioceptive stability._
anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization _and a guided rehabilitation program that emphasizes proprioceptive stability._
QUESTION 25 OF 50
of 100
Which relationship is noted for the structure identified by the arrow in Figure 22b? 24
Which relationship is noted for the structure identified by the arrow in Figure 22b? 24
1
The anterolateral and posteromedial bundles are relaxed in mid flexion and tensioned in high flexion.
2
The anterolateral and posteromedial bundles are tensioned in mid flexion and tensioned in high flexion.
3
The anterolateral bundle is tensioned in mid flexion, and the posteromedial bundle is tensioned in both extension and high flexion.
4
The posteromedial bundle is tensioned in mid flexion, and the anterolateral bundle is tensioned in both flexion and extension.
- The anterolateral bundle is tensioned in mid flexion, and the posteromedial bundle is tensioned in both extension and high flexion.
QUESTION 26 OF 50
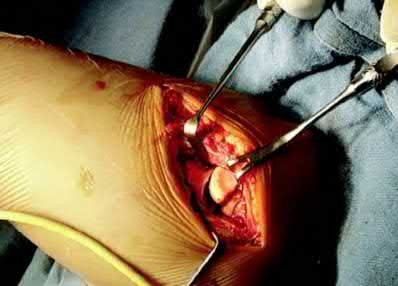
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
1
Brachial artery
2
Median nerve
3
Posterior interosseous nerve
4
Lateral antebrachial cutaneous nerve
5
Antecubital vein
The most commonly injured neurovascular structure during an anterior approach for the repair of a distal biceps tendon rupture is the lateral antebrachial cutaneous nerve. This structure is located lateral to the biceps tendon and in a superficial location just deep to the subcutaneous layer. The antecubital vein is medial and superficial with the brachial artery and median nerve also medial to the biceps tendon but deep to the common flexors. The posterior interosseous nerve is deep within the supinator muscle and can be injured in the deep dissection or through the posterior approach when using a two-incision approach.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Ramsey ML: Distal biceps tendon injuries: Diagnosis and management. J Am Acad Orthop Surg 1999;7:199-207.
QUESTION 27 OF 50
In either a ceramic-on-highly-cross-linked polyethylene (HXPE) or metal- on-HXPE component, increasing the ball head size leads to
1
decreased polyethylene wear.
2
decreased risk for corrosion.
3
increased primary arc of motion.
4
increased offset.
Increasing the size of the ball head increases the primary arc of motion prior to impingement and the jump distance prior to dislocation, assuming an acetabular component abduction of less than 90 degrees. Although HXPE has demonstrated decreases in linear wear rates even with ball head sizes larger than 28 mm, volumetric wear remains a concern. A larger ball head size does not significantly change offset, and larger metal ball heads are not associated with decreased risk for corrosion.
3
3
QUESTION 28 OF 50
of 100
Figure 1 is the radiograph of a 12-month-old girl with a history of type 3 fibroblast growth factor receptor mutation, rhizomelic shortening of the limbs, and dwarfism who is noted to have a thoracolumbar kyphosis (TLK) of 25°. Spontaneous resolution of her thoracolumbar kyphosis is closely associated with

Figure 1 is the radiograph of a 12-month-old girl with a history of type 3 fibroblast growth factor receptor mutation, rhizomelic shortening of the limbs, and dwarfism who is noted to have a thoracolumbar kyphosis (TLK) of 25°. Spontaneous resolution of her thoracolumbar kyphosis is closely associated with
1
appropriate developmental motor progress.
2
absence of ventriculoperitoneal shunt.
3
foramen magnum decompression.
4
gender.
■
Achondroplasia is a skeletal dysplasia caused by a genetic mutation in the type-3 fibroblast growth factor receptor gene, which leads to abnormal endochondral ossification. Some, but not all physical features of achondroplasia include rhizomelic shortening of the limbs, midface hypoplasia, frontal bossing, lower extremity malalignment, hyperlordosis and TLK (defined as a Cobb angle of 20° or more centered at T12 and L1).
Thoracolumbar kyphosis is a characteristic feature of achondroplasia and thought to be a result of developmental motor delay and hypotonia and disproportionate head size relative to a small chest size. Most patients with achondroplasia develop TLK at about sitting age. Studies have shown that most cases of TLK resolve spontaneously within a year after patients start to walk. Studies suggest that approximately 30% of early TLK cases persist, and a third of these cases progress into severe deformities. Apical vertebral translation, percentage of apical vertebral wedging for vertebral height, and developmental motor delay (not sitting by age 14 months and not walking independently by age 30 months) are shown to be risk factors for TLK to persist. Presence of a vertriculoperitoneal shunt, hydrocephalus, foramen magnum decompression, gender, lumbar lordosis were not associated with unresolved TLK. Although the magnitude of the thoracolumbar kyphosis at presentation(>25°) is cited as a risk factor in some studies, this is not verified in other studies.
QUESTION 29 OF 50
The superficial peroneal nerve is at risk during distal screw fixation using a LISS plating technique for fracture fixation.
A 24-year-old motorcyclist is brought in as a polytrauma after striking a tree at 65 mph. He is found to have injuries involving the chest, abdomen, pelvis, as well as a left open femoral shaft fracture. He undergoes resuscitation in the trauma bay. Which of the following parameters best supports proceeding with irrigation, debridement and external fixation as opposed to immediate reamed intramedullary nailing?
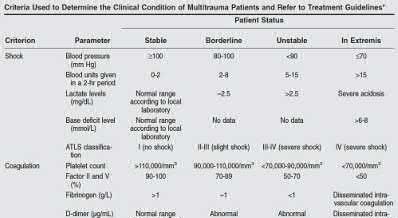
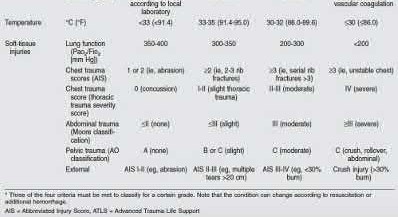
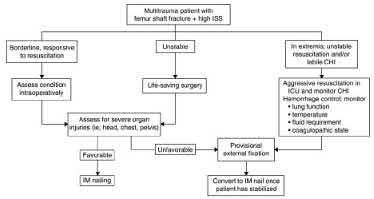



















































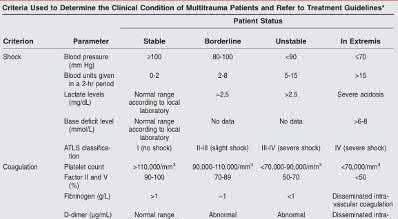























































































































































A 24-year-old motorcyclist is brought in as a polytrauma after striking a tree at 65 mph. He is found to have injuries involving the chest, abdomen, pelvis, as well as a left open femoral shaft fracture. He undergoes resuscitation in the trauma bay. Which of the following parameters best supports proceeding with irrigation, debridement and external fixation as opposed to immediate reamed intramedullary nailing?
1
Temperature = 35.5°C (95.9°F)
2
Fractures of ribs 2-3 with left apical pneumothorax
3
Grade IV liver laceration with SBP = 85 mmHg
4
Left superior and inferior pubic ramus fractures
5
Lactate = 2.3 mg/dL
Significant abdominal trauma with evidence of hemorrhagic shock (SBP 2.5 mg/dL), coagulopathy (platelet count 2.5 mg/dL would be an unstable parameter.
A 92-year-old female sustains the injury shown in Figure A to her nondominant extremity as the result of a non-syncopal ground-level fall. She denies any previous injury or pain of the elbow, and her medical history is significant only for osteoporosis and hypothyroidism. What is the most appropriate treatment for her injury?
This patient has a displaced, intra-articular, comminuted olecranon fracture. Comminution is an indication for plate fixation.
Most displaced olecranon fractures are treated operatively. Options include tension band constructs, intramedullary screws, plate and screw fixation or fragment excision with triceps advancement. Any construct relying on interfragmentary compression (tension band, intramedullary screws) requires a non-comminuted fracture pattern. Plate fixation is indicated in the setting of comminution, extension past the coronoid, or in the setting of associated instability.
Bailey et al. retrospectively reviewed 25 patients who underwent plate fixation of displaced olecranon fractures. Twenty-two of 25 patients had good or excellent outcomes. Five of 25 patients (20%) of patients required plate removal for symptomatic hardware. The authors concluded that plate fixation
was an effective treatment for displaced olecranon fractures, with good functional outcomes.
Figure A shows a displaced, comminuted olecranon fracture without evidence of propagation past the coronoid.
Incorrect answers:
. All displaced olecranon fractures should be considered for internal fixation. Displacement alone does not direct choice of implant.
Answer 2. Intra-articular extension is an indication for surgery to re-establish articular congruity but does not dictate implant selection.
Answer 3. Extension distal to the coronoid is an indication for plate fixation but there is no evidence of such extension on the radiograph shown
Answer 4. This fracture is comminuted, without a distinct fracture line.
A 35-year-old male was involved in a high speed motorcycle accident. He has a closed head injury, bilateral pulmonary contusions and splenic rupture. His orthopaedic injuries are shown in Figure A. He has a blood pressure of 90/50 mm Hg and a heart rate of 115, despite aggressive resuscitation. An arterial blood gas reveals that his blood lactate is 3.5 and base deficit is -6 mmol/L. Following successful closed reduction of the right hip in the operating room with a percutaneous inserted Schantz pin, what is the next most appropriate treatment for his orthopaedic injuries?
1) Bilateral open reduction and internal fixation
2) Open reduction internal fixation on the right, reamed intramedullary nailing on the left
3) Temporizing external fixation on the right, open reduction and internal fixation on the left
4) Bilateral reamed intramedullary nailing
5) Bilateral temporizing external fixation
This patient presents with features of hemodynamic instability and a high injury severity score. The next most appropriate treatment would be temporizing external fixation bilaterally. This patient meets the criteria for damage control orthopaedics.
Damage control orthopaedics is an approach that contains and stabilizes orthopaedic injuries so that the patient's overall physiology does not undergo further inflammatory insult. As a result, external fixation of femoral shaft fracture and pelvic stabilization is an effective treatment under this strategy. Other indications include vascular injury and severe open fracture.
Pallister et al. reviewed the effects of surgical fracture fixation on the systemic inflammatory response to major trauma. They show that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure. However, early fracture surgery increases the post-traumatic inflammatory response, which
carries a higher complication rate compared to temporary fixation.
Tisherman et al. created clinical guidelines for the endpoints of resuscitation. Level I data found that standard hemodynamic parameters do not adequately quantify the degree of physiologic derangement in trauma patients. The initial base deficit, lactate level, or gastric pH should be used to stratify patients with regard to the need for ongoing fluid resuscitation.
Pape et al. retrospectively reviewed the impact of early total care vs. damage control orthopaedics in the treatment of femoral shaft fractures in polytrauma patients. They found a significantly higher incidence of acute respiratory distress syndrome (ARDS) with intramedullary nailing (15.1%) compared to external fixation (9.1%) when DCO subgroups were compared.
Figure A is a pelvic AP radiograph showing a right hip fracture-dislocation with an ipsilateral femoral shaft fracture. On the left side there is a displaced pertrochanteric hip fracture.
Incorrect Answers:
Answer 1-3: Open reduction internal fixation would not be indicated in damage control orthopaedics.
Answer 4: Bilateral reamed intramedullary nailing would be indicated in early total care of these injuries. As this patient is hemodynamically unstable, with a high injury severity score and bilateral lung contusions, damage control orthopaedics would be indicated.
Which of the following has been shown to be the greatest risk factor for refracture after implant removal from a radial shaft?
1) Removal of locking screws
2) Removal of small fragment plates
3) Removal of metaphyseal implants
4) Removal of implants less than 1 year after insertion
5) Removal of protective splinting from limb earlier than 10 weeks postoperatively
Removal of implants earlier than 1 year after insertion is a risk factor for refracture of the bone after implant removal.
The risk of refracture after hardware removal is multifactorial. Multiple
variables have been studied such as protective splinting for 6 weeks after hardware removal, waiting 12 months or more prior to hardware removal, and the location of the fracture. The variable that seems to correlate most with the risk of refracture is a diaphyseal location of the initial fracture. Large fragment plates (4.5 mm), when removed, are also at higher risk for refracture in the forearm.
Deluca et. al reported on a case series of patients who sustained a refracture of a forearm after implant removal. They noted that radiolucency at the site of the original fracture was seen in most refractured patients when the plate was removed. They also recommend delaying implant removal to two years after insertion to minimize risk.
Rumball et. al reported that the incidence of refracture after forearm implant removal is 6% in their series. They found that early removal, lack of postoperative immobilization, and plate size are the most critical risk factors for refracture.
Illustration A shows a forearm with evidence of refracture after implant removal.
Incorrect Answers:
Answer 1: Removal of locking screws does not increase the risk of refracture. Answer 2: Removal of large fragment plates (4.5mm) are at increased risk of refracture as compared to small fragment plates (3.5mm).
Answer 3: Metaphyseal implant removal has a decreased risk of refracture compared to diaphyseal implant removal.
Answer 5: Protective splinting for 6 weeks is all that is generally recommended for these patients.
A 23-year-old male arrives to the trauma bay after a motorcycle crash caused by a drive-by shooting. The patient is awake and alert and following commands. Vital signs include a blood pressure of 145/90 and a heart rate of 117bpm. Initial lactate is reported as 2.4 mmol/L. The patient has 2 rib fractures on the right with a clear chest radiograph. The patient is neurovascularly intact with a 4cm transverse wound over the medial ankle. Figures A, B and C exhibit his orthopaedic injuries. What is the most appropriate management?
1) Irrigation, debridement and placement external fixator right ankle, external fixation femur and intramedullary fixation tibia
2) Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and tibia
3) Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and external fixation tibia
4) Irrigation, debridement and placement external fixator right ankle, femur and tibia
5) Irrigation, debridement and external fixation right ankle and skeletal traction
The patient is relatively hemodynamically stable. In this case the femur and tibia should be definitively fixed while the open ankle fracture can be irrigated and debrided and placed in a spanning external fixator, temporizing for later definitive fixation.
Aside from an elevated heart rate and mildly elevated lactate (normal
Figure A is an anterior-posterior (AP) radiograph of a 27-year-old male who was a bicyclist struck by a motor vehicle. He was intubated in the field and unresponsive in the trauma slot. Ultrasound of his abdomen is positive for blood and he is brought to the operating room emergently for an exploratory laparotomy. He is found to have ischemic bowel and a grade 4 liver laceration. His lactate is 9.0 mg/dL. Which figure represents the next appropriate step in regard to his pelvic ring injury?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
The radiograph exhibits an elevated left hemipelvis with complete sacroiliac disruption, which can be temporized with placement in skeletal traction.
The patient is unstable, as indicated by an elevated lactate level. The most appropriate next step is temporizing skeletal traction to reduce the left hemipelvis.
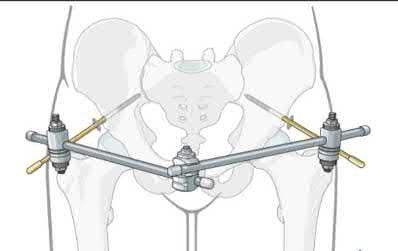
Langford et al. review the initial diagnosis, evaluation and resuscitation in the management of pelvic fractures. Reduction of pelvic volume can be achieved with pelvic binders and temporizing external fixation for anterior posterior compression (APC) and/or lateral compression (LC) fracture patterns, while skeletal traction can help do the same in vertical shear patterns.
Matullo et al. review the uses of skeletal traction in orthopaedic trauma, where lower extremity skeletal traction can be an efficient, fast, easy way to help reduce pelvic volume in vertical shear injuries, especially when the patient is unstable and not cleared for definitive fixation.
Figure A exhibits an elevated left hemipelvis indicative of a vertical shear injury and complete SI disruption. Figure B is an example of a pelvic binder. Figure C is a pelvic reconstruction plate. Figure D is a schematic of an anterior pelvic external fixator. Figure E is a schematic drawing of a patient in lower extremity
skeletal traction. Figure F is a radiograph exhibiting S1 and S2 sacroiliac (SI) screws.
Incorrect answers:
Answer 1: A pelvic binder would not be helpful in this scenario and actually may worsen the deformity.
Answer 2: Definitive plate fixation of the anterior pelvis will be needed, but only when the patient is adequately resuscitated.
Answer 3: An anterior external fixator may actually do more harm than good as it may require more time than placing skeletal traction, and also have difficulty controlling the posterior pelvis from the front.
Answer 5: Percutaneous SI screws may be placed later, once the patient is resuscitated and stable.
A 38-year-old man is involved in a motor vehicle collision and suffers the grossly open injury shown in Figure A. He subsequently undergoes irrigation and debridement and placement of an external fixator. In Figure B, if the proximal pin is placed at the red circle as compared to the black circle, the patient is at increased risk for which of the following?
1) Foot drop
2) Injury to the anterior tibial artery
3) Septic arthritis
4) Flexion contracture of the knee
5) Patellar tendon rupture
The patient is at increased risk of septic arthritis when placing the proximal tibial pin too proximal due to penetration of the joint capsule. Pin site flora can track into the joint and lead to a septic knee.
Tibial external fixators can be used to temporize tibial shaft, pilon, and ankle fractures not ready for definitive management due to soft tissue concerns and/or practice of damage control orthopaedics. Intracapsular placement of fixator pins can lead to septic arthritis. The capsular reflection typically extends 14 mm distal to the subchondral line.
DeCoster et al. reported a cadaveric dissection study for safe placement of proximal tibia pins and determined that the capsule inserts 14 mm below the articular surface along the posteromedial and posterolateral surfaces. For fractures requiring extremely proximal pin placement, they recommend
anterior cortex penetration only at least 6 mm distal to articular surface.
Reid et al. investigated safe transtibial pin placement using MRI and cadaveric and volunteer knees. They found that pin placement 14 mm distal to subchondral bone will result in low likelihood of capsular penetration.
Figure A is an AP radiograph showing a segmental middle third tibia/fibula fracture. Figure B is a lateral diagram of the tibia showing potential sites of proximal pin placement.
Incorrect Answers:
Answer 1: Foot drop would occur secondary to common peroneal nerve injury, which is not at risk with very proximal pin placement.
Answer 2: The anterior tibial artery is not at risk with very proximal pin placement.
Answer 4: The knee is free to move and therefore should not develop a flexion contracture secondary to the external fixator.
Answer 5: Patellar tendon rupture is not complication of external fixator pin placement in the tibia.
Figures A and B are radiographs of a 43-year-old, right-hand dominant, male that injured his arm in a motor vehicle accident. What would be an absolute indication for surgical fixation of his injury?
1) Radial nerve palsy
2) Intra-articular extension
3) 2mm fracture distraction, 5 degrees of rotational malignment
4) Ipsilateral proximal both bone forearm fracture
5) Bilateral fracture
This patient has a humeral shaft fracture. An absolute indication for surgery would include a floating elbow, i.e. ipsilateral both bone forearm fracture.
The primary causes of humeral fractures include motor vehicle accidents, falls, or violent injury. Almost all cases are treated non-operatively with functional bracing. The absolute indications for surgical management include: ipsilateral vascular injury, severe soft-tissue injury, open fracture, compartment syndrome, and associated ipsilateral forearm fracture, ie, floating elbow. The relative indications for surgical management include: segmental fracture, intraarticular extension, significant fracture distraction, bilateral humeral fracture, inability to maintain acceptable alignment, and polytrauma.
Klenerman et al. reviewed non-operative treatment of humeral shaft fractures. They showed that acceptable results could be achieved even after 20° of
anterior bowing, 30° of varus angulation, 15° of malrotation, and 3 cm of shortening.
Carroll et al. reviewed the management of humeral shaft fractures. They state the indications for operative fixation to be polytraumatic injuries, open fractures, vascular injury, ipsilateral articular fractures, floating elbow injuries, and fractures that fail nonsurgical management. Surgical techniques include external fixation, open reduction and internal fixation, minimally invasive percutaneous osteosynthesis, and antegrade or retrograde intramedullary nailing
Figure A and B shows a comminuted mid-shaft humeral fracture with intraarticular extension.
Incorrect Answers:
Answer 1,2,3,5: These associated injuries are NOT an absolute indication for surgery. An area of controversy is the occurrence of new-onset radial nerve injuries after closed manipulation. However, the current algorithm does not support early open nerve exploration and fixation.
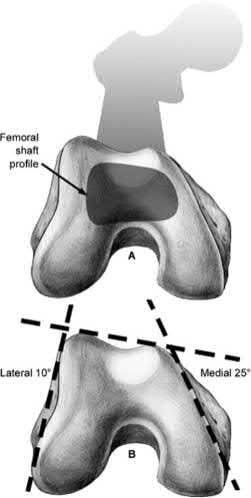
Which of the following findings is a contraindication in retrograde nailing of a periprosthetic distal femur fracture around a total knee arthroplasty?
1) Posterior-stabilized total knee implant
2) Cruciate retaining total knee implant
3) Spiral fracture pattern
4) Distal femoral replacement
5) Knee flexion contracture of 15 degrees
A distal femoral replacement (TKA) implant will generally preclude placement of a retrograde nail due to the long stem on the femoral component.
Supracondylar femur fractures above a well-fixed TKA component are increasingly common. These fractures are often treated with a lateral locking plate, but can also be treated with a retrograde nail in certain circumstances. An important factor in determining if nailing is a viable option are knowing the TKA implant and it's design. In addition, if the TKA component is known, the maximum size of reamer head and nail can be determined preoperatively from the size of the femoral 'box'.
Schutz et al report on a prospective multicenter study of 112 patients who underwent fixation of a distal femur fracture with the LISS system. They report that 90% of fractures went on to union and they attribute all of the failures to either the high-energy nature of particular fractures or a lack of experience in applying the plate in an appropriate pattern. They also note that primary grafting of these fractures is not necessary.
Illustration A shows a periprosthetic femur fracture treated with a retrograde nail.
Incorrect Answers:
1: A posterior-stabilized implant can be treated with an intramedullary nail in many circumstances but can be technically challenging, depending on the components.
2: A cruciate retaining TKA is not a contraindication to use of a retrograde nail. 3: A spiral pattern periprosthetic supracondylar femur fracture can be treated with a femoral nail.
5: A knee flexion contracture will often provide the flexion necessary for access to the box of the femoral component. A knee extension contracture, however, can preclude access to this box for placement of a nail.
A patient falls and sustains the isolated injury seen in Figures A and B. The surgical plan includes open reduction and internal fixation with a small mini-fragment plate using a direct lateral approach. During the approach, the forearm was placed in a fully pronated position. What would be the correct position of the forearm during plate application?
1) Full pronation
2) 25 degrees pronation
3) Neutral
4) 25 degrees supination
5) Full supination
Using the lateral approach (Kocher or Kaplan), the correct placement of the arm should be in a neutral position so that the plate can be placed on the bare area of the proximal radius.
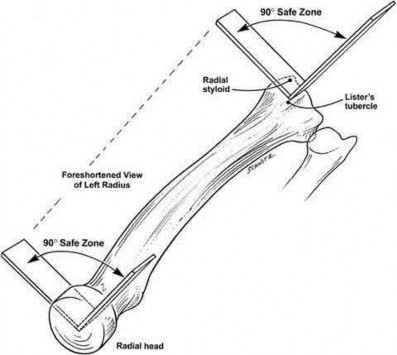
Displaced radial head fractures with less than 3 fragments can be amendable to open reduction internal fixation. The methods of fixation include buried or headless screws, if placed at the articular surface, or posterolateral plating, if placed in the bare area. The safe zone for plating is located at a 90-110 arc from the radial styloid to Lister's tubercle with the arm in neutral rotation. This position helps to avoid impingement of ulna against the plate with forearm rotation. It should be noted that during the approach, that the forearm should be fully pronated to avoid injury to the posterior interosseous nerve.
Mathew et al. reviewed the concepts of terrible triad injuries of the elbow. Radial head fractures are treated conservatively when there is an isolated minimally displaced (less than 2mm) fracture with no mechanical block to motion. Open reduction internal fixation is used for Mason II or III fractures with
A 38-year-old male is involved in a high speed motor vehicle collision. He has a Glasgow Coma Scale of 13 and receives 2 liters of fluid en route to the emergency department. Upon evaluation in the emergency department, he is found to have a bilateral femoral shaft fractures, a right ankle fracture, and a left both bone forearm fracture. He also has 2 left sided rib fracture and a grade II liver laceration. His heart rate is 130 and blood pressure is 85/50. All of the following
would be indications to practice damage control orthopaedics in this patient except:
1) Bilateral femur fractures
2) Rib fractures
3) Lactate of 5.2
4) Urine output of 20 cc/hr
5) Heart rate and blood pressure
Rib fractures without evidence of further thoracic trauma would not be an indication to practice damage control orthopaedics. This patient is underresuscitated based on his lactate level, urine output, and vital signs and definitive management should be delayed.
Damage control orthopaedics is the practice of delaying definitive management of fractures and utilizing temporary stabilization (such as an external fixator) until a patient has recovered from the initial physiologic insult of trauma.
Patients are at increased risk for perioperative complications such as ARDS and multi-system organ failure during the acute period after polytrauma. In addition to underresuscitation, other indications to practice damage control orthopaedics include: injury severity score>40 (or >20 with thoracic trauma), bilateral femoral fractures, hypothermia below 35 degrees Celsius, and pulmonary contusions.
Pape et al. (2007) studied the incidence of acute lung injuries in polytrauma patients undergoing either intramedullary nailing or external fixation and later definitive fixation of femoral shaft fractures. They found that patients undergoing immediate intramedullary nailing were nearly 6.7 times more likely to have acute lung injury
The Canadian Orthopedic Trauma Society studied the effect of reamed versus unreamed femoral nailing on incidence of ARDS for femoral shaft fractures in trauma patients using a randomized controlled study. They found no difference between the groups.
Pape et al. also examined the pathophysiological cascades that accompany soft tissue injuries of the extremities, abdomen, and pelvis and recommend a more comprehensive for evaluation of patients with these injuries.
Incorrect Answers:
Answer 1: Bilateral femur fractures are an indication to practice damage control orthopaedics and delay definitive fixation
Answers 3,4,5: All of these answers suggest that the patient is underresuscitated. Definitive fixation should be delayed
The anterior intrapelvic (modified Stoppa) approach is most appropriate for which of the following fractures?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The anterior intrapelvic (AIP) or modified Stoppa approach provides access to the quadrilateral plate, which is a common location for fracture displacement in associated both column acetabulum fractures as seen in Figure D.
Compared to the traditional ilioinguinal approach, the modified Stoppa with a lateral window can offer comparable access to the quadrilateral plate, which can allow for its use in associated both column fracture patterns.
de Peretti et al. prospectively followed 25 patients with both column fractures
treated via an iliofemoral approach. Results led the authors to not recommend the extensile approach for both column fractures due to lack of efficiency and high complication rates.
Alonso et al. compared the extensile iliofemoral and triradiate approaches, and both reported acceptable results. However, concerning were the relatively high rates of heterotopic ossification, despite prophylaxis.
Bible al. performed a cadaver study to quantify the amount of access provided by the modified Stoppa approach. This approach provides access to approximately 80% of both the inner pelvis, and the quadrilateral plate, however, comparison to the ilioinguinal approach was not performed.
Shazar et al., in a cohort comparison between the ilioguinal and Stoppa approaches, noted better visualization and potential improve fracture reduction via the Stoppa approach for both column fractures. However, this study was limited in its retrospective and relative observer bias.
Figure A depicts a posterior wall fracture dislocation with concomitant femoral neck fracture. Figure B is an iliac oblique view which depicts a posterior column fracture. Figure C exhibits a posterior column + posterior wall fracture. Figure D depicts acetabular fracture with protrusio. Figure E exhibits a posterior wall fracture.
Incorrect answers:
Answers 1,2,3, and 5: Posterior sided injuries, especially for these injuries, would probably be best approached via the Kocher-Langenback approach. Surgical dislocation with a trochanteric slide may help visualization in answer 1.
Figure A is a radiograph of a 75-year-old woman that fell onto her non-dominant shoulder from a standing height. She was treated nonoperatively for 9 months but continues to complain of pain when she elevates her arm. In patients with this type of fracture pattern, what factor has the greatest impact on fracture healing?
1) Hand dominance
2) Angulation of fracture
3) Smoking
4) Early physical therapy
5) Diet
This patient has an impacted varus proximal humerus fracture. Smoking has been shown to increase the nonunion risk up to 5.5 times with these fractures.
Impacted varus proximal humerus fractures can be managed effectively with non-operative care. The major factors that influence non-union are age and smoking. Solid bony union can be seen in 93-98% of patients at 1 year, with more than 97% of people returning to pre-injury level of function. The angulation of fracture, hand dominance and physical therapy does not seem to influence bone union or functional outcomes with this fracture pattern.
Court-Brown et al. looked at the outcomes of impacted varus fractures. They determined that the age of the patient was the major factor in overall outcome. They showed that the best results occurred in younger patients, but results deteriorate with advancing age. Physical therapy was not found to
impact outcome.
Hanson et al. showed that impacted varus fractures can be successfully managed with non-operative care. They found that overall fracture displacement had a minor impact of fracture healing and functional outcome. The predicted risk of delayed union and nonunion was 7% with patients that smoke. This was 5.5 times greater than non-smokers.
Figure A shows an AP radiograph of a varus angulated proximal humerus fracture. This radiograph shows delayed atrophic union.
Incorrect Answers:
Answers 1,2,4: These factors do not have a significant influence on bone healing.
Answer 5: Diet has shown to improve bone healing but this does not have the greatest impact.
A 26-year-old male epileptic patients presents with right shoulder pain and deformity after a grand mal seizure. After medical stabilization, he denies previous injury to his shoulder. Pre-reduction and post-reduction radiographs of the shoulder are shown in Figures A-C, respectively; physical examination reveals a normal upper extremity neurovascular examination. After shoulder immobilization, what would be the next most appropriate step in management of this patient?
1) Abduction brace for three weeks, followed by therapy
2) Right shoulder MR arthrogram
3) Open reduction and internal fixation
4) Hemiarthroplasty
5) Early range of motion
This patient has presented with a fracture dislocation of the right shoulder. After urgent closed reduction, this patient requires open reduction internal fixation of the proximal humerus, and greater tuberosity fracture fragment in particular.
Isolated greater tuberosity fractures may be associated with shoulder dislocations. Careful review of imaging is critical to identify fracture lines that may extend into the humeral neck and head. If these extensions go undetected, catastrophic propagating fractures may occur during closed reduction maneuvers. Treatment is usually with open reduction internal fixation (ORIF). Young patients with proximal humerus fractures should be treated more aggressively with ORIF as compared to elderly patients. Another example would be a severely impacted valgus proximal humeral fracture in a young patient.
Erasmo et al. examined of 82 cases of humerus fracture dislocations treated with the lateral locking plates. Overall outcomes were excellent to good based on standard scoring systems. Complications included avascular necrosis (12%), varus positioning of the head (4.8%), impingement syndrome (3.6%), secondary screw perforation (3.6%), non-union (2.4%) and infection (1.2%).
Robinson et al. looked at severely impacted valgus proximal humeral fractures treated with open reduction internal fixation in young patients. Anatomic reduction is required with lateral plating to re-establish the normal head/neck angle. Good to excellent results can be achieved with fixation methods.
Figure A shows an anterior fracture-dislocation of the right shoulder. Figure B and C show post-reduction radiographs with a congruent glenohumeral joint. Displacement of the greater tuberosity (GT) fragment is greater than 5mm.
Incorrect Answers:
Answer 1: The GT fragment is displaced more than 5-10mm which would warrant surgical reduction and stabilization of the fracture.
Answer 2: MR arthrogram may be indicated to rule out an intra-capsular soft-tissue injury. However, this would not be warranted prior to fixation of the fracture.
Answer 4: Hemiarthroplasty would be indicated in some 4-part proximal humerus fractures or elderly patients. Considering this patient's age and valgus impaction of the fracture, ORIF would be most appropriate.
Answer 5: Early range of motion would be warranted AFTER fixation of the fracture.
Pelvic packing can be performed to temporarily treat a hemodynamically unstable patient with a pelvic ring fracture. Which of the following is the preferred location of the skin incision to perform pelvic packing?
1) Right anterior superior iliac spine (ASIS) to mid-symphysis, left lateral window incision
2) Left ASIS to mid-symphysis, right lateral window incision
3) Subumbilical incision
4) ASIS to ASIS bilaterally
5) Pararectus incision
The preferred skin incision location is a subumbilical incision, 6-8cm extending upwards from the pubic symphysis towards the umbilicus; this allows access to all of the appropriate areas for pelvic packing.
Following skin incision, the rectus fascia is then divided in the midline which allows for access to both sides of the bladder for packing deep in the pelvic
brim. On each side, 3 lap pads are placed from sacroiliac joint to the retropubic space, all placed below the level of the pelvic brim.
Hak et al. review the options for emergent treatment in life threatening hemorrhage secondary to pelvic fractures. The authors offer several options for emergent treatment, which includes the use of pelvic binders, the placement of external fixators, pelvic packing and interventional angiography. Goals include reduction of pelvic volume and stopping rapid hemorrhage to save a patient's life. Pelvic packing, properly performed, is done through a subumbilical incision, as described above.
Osborn et al. retrospectively reviewed and compared emergent pelvic packing to angiography in hemorrhagic pelvic fracture clinical scenarios. The authors noted comparable results in mortality with a noted decrease in need for post-procedure transfusions in the pelvic packing group.
Cothren et al. reported their outcomes following an institutional algorithmic change from pelvic ex-fix/angiography to pelvic packing and ex-fix. Since their institutional change, the authors noted a significant decrease in transfusions, need for angiography and mortality.
Incorrect answers:
Answers 1,2: While these approaches may give access to the pelvic brim, each only give access to one side; one needs to circumferentially access and pack the pelvis.
Answer 4: An ASIS to ASIS skin incision is an unnecessary dissection with too many important structures that lie very close to the skin, including the femoral vessels.
Answer 5: A pararectus incision is an alternative approach to access the quadrilateral plate for acetabular fractures and does not play a role in pelvic packing.
A 28-year-old man is brought by ambulance to the emergency department after falling from the roof of his home four hours ago. Upon initial evaluation, he has visible deformities of his bilateral lower extremities and a positive FAST exam. Heart rate is 135, blood pressure 85/58, and urine output is 40 cc over 3 hours. According to ATLS guidelines, what percentage of his blood volume has this patient likely lost?
1/.
1) 30-40%
2) 40-50%
3) >50%
This patient has likely lost 30-40% of his blood volume and is likely in stage III hemorrhagic shock on the basis of his heart rate, blood pressure, and urine output.
Initial assessment of a trauma patient should involve evaluation of airway, breathing and circulation. An average adult has approximately 5 L of circulating blood volume. Class III and IV hemorrhagic shock, approximated by loss of greater than 30% of blood volume, typically requires resuscitation with fluids and blood products. Lactate level (normal 100 and diminished urine output
4, 5: Blood loss of greater than >40% typically leads to heart rate >140, decreased blood pressure and negligible urine output.
Which of the following fracture patterns would be most appropriately treated with open reduction and internal fixation with posteromedial and lateral plates via dual incisions?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The patient in Figure D has a bicondylar tibial plateau fracture with a posteromedial fracture fragment, which is an indication for lateral and posteromedial plating via dual incisions.
Bicondylar tibial plateau fractures are typically treated with open reduction internal fixation. Studies have shown that the posteromedial fragment is common in bicondylar tibial plateau fractures. Standard lateral implants do not gain adequate screw purchase in posteromedial bone. Posteromedial incisions using the interval between the semimembranosus and medial head of the gastrocnemius can be used to gain access to the fragment and provide exposure to place a posteromedial plate.
Barei et al. reviewed 57 OTA C-type bicondylar tibial plateau fractures, and found the presence of a posteromedial fragment in 74% of cases. They suggest
the use of alternate methods of fixation for the posteromedial fragment rather than lateral fixed-angle plates alone.
Higgins et al. reviewed 111 patients with bicondylar tibial plateaus that underwent CT scan evaluation. They found the incidence of a posteromedial fragment in 59% of the patients and on average accounted for 25% of the articular surface.
Barei et al. reviewed 83 patients treated with dual incisions for fixation of bicondylar tibial plateau fractures. They found deep infections in 8.4% of patients. Satisfactory articular reduction was found in 62% of patients, satisfactory coronal alignment in 91% of patients, satisfactory sagittal alignment in 72%, and satisfactory condylar width in 98%.
Figure A shows an AP and lateral radiograph of a split/depressed lateral tibial plateau fracture. Figure B shows an AP and lateral radiograph of a proximal third tibial shaft fracture with a proximal fibula fracture. Figure C shows an AP and lateral radiograph of a medial plateau fracture with articular depression. Figure D shows an AP and lateral radiograph of a bicondylar tibial plateau fracture. Figure E shows an AP and lateral radiograph of a tibial tubercle fracture in a tibia with open physes.
Incorrect Answers:
Answer 1: Schatzker II tibial plateau fractures can be treated with a single lateral plate.
Answer 2: Proximal third tibial shaft fractures can be treated with an intramedullary nail or percutaneous plating
Answer 3: Schatzker IV tibial plateau fractures can be treated with a single medial or posteromedial plate.
Answer 5: Tibial tubercle fractures in children can be treated with anterior to posterior screws.
Figure A shows the radiographs of a 87-year-old patient after a fall from standing. He lives in a nursing home and uses a walker to transfer from bed to chair. His past medical history includes recurrent urinary tract infections, congestive heart failure, angina and diabetes. Which of the following factors is associated with the best postoperative outcome in this patient?
1) Immediate surgical intervention
2) Postoperative epidural analgesia
3) Postoperative antibiotics
4) Pre-operative medical optimization
5) Choosing total hip arthroplasty instead of hemiarthroplasty
Geriatric patient with hip fractures tends to have a number of coexisting medical conditions that impact surgical risk. A successful pre-operative medical evaluation has the greatest impact on surgical outcomes in this patient population.
Patients with complex past medical histories are at great risk of complications with surgery. This helped to drive the formation of the ASA classification system as a way to score patients out of 5 based on their anesthetic and surgical risks. Patients with significant systemic disease (ASA III and IV) have shown to demonstrate poorer outcomes as compared to patients with less severe medical comorbidities (ASA I and II).
Egol et al. looked at factors that impact the outcomes of hip fractures in geriatric patients. They showed that cardiac and pulmonary complications were most frequent complications post-operatively. It was stated that early mobilization and pre-operative evaluations have the greatest impact on outcomes.
Parvizi et al. looked at the thirty-day mortality following hip arthroplasty for acute fracture. They reviewed a database of 7774 consecutive patients that underwent hip arthroplasty for the treatment of an acute fractures. The overall mortality was 2.4%. Risk factors were found to be cemented implants, female patients, elderly patients, and patients with cardiorespiratory comorbidities.
Roberts et al reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. Although pre-operative medial optimization was not mentioned in this review, there is strong evidence to support an interdisciplinary care program for patients with hip fractures.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Answer 1: Most studies have shown an association between operative delay of
more than 24-48 hours and a higher 1-year mortality rate. However, In patients with with more than 3 medical comorbidities, medical optimization has a greater impact on post-operative outcomes than time to surgery.
Answer 2: Post-operative epidural anaesthesia has shown to decrease postoperative delirium but does not affect 30-day mortality.
Answer 3: Postoperative antibiotics have not shown to reduce the 30-day mortality.
Answer 5: Total hip arthroplasty has shown to improved functional outcomes at 1 year compared with hemiarthroplasty. However, there has been no change in mortality.
A 36-year-old male sustains severe injuries as a result of a motor vehicle collision. After 5 days, the patient is stabilized and transferred to your facility for continued management. After obtaining appropriate imaging, including the images shown in Figures A, B and C the patient should be given which of the following mobility restrictions?
1) Touch-down weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
2) Weight bearing as tolerated on the left lower extremity, non-weightbearing on the right lower extremity
3) Non-weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
4) Touch-down weight bearing on the left lower extremity, weight bearing as tolerated on the right lower extremity
5) Weight bearing as tolerated on the left lower extremity, weight bearing as tolerated on the right lower extremity
Figures B and C shows a stable, impacted lateral compression (LC) type I injury, which can be treated with immediate mobilization without restrictions. The right lower extremity has a pilon fracture, which should be treated with non-weight bearing.
LC-I injuries are stable patterns, as they involve an impaction injury to the anterior sacrum, which has some inherent stability. In addition, the posterior sacro-iliac (SI) soft tissue structures remain intact, which provides critical stability during immediate mobilization.
The reference by Tile is a review article on the principles of management of these injuries, and he reviews how the Tile classification system is important to help determine surgical need and where the stabilization is required. For the stable LC-1 type injury, no fixation is required.
Incorrect Answers:
Answer 1: A patient cannot do touch-down weight bearing on one side and non-weightbearing on the other side simultaneously.
Answer 3: The LC-I injury pattern is stable and can undergo immediate weightbearing as tolerated.
Answer 4: The LC-I pattern is stable and would allow immediate weightbearing, and the right pilon fracture would require non-weightbearing. Answer 5: The right pilon fracture would require non-weightbearing at this time.
A 24-year-old male sustains the fracture dislocation shown in Figure A. How is this fracture pattern best classified?
1) Moore I
2) Moore II
3) Schatzker III
4) Schatzker V
5) OTA type 41B3
Figure A shows a Moore Type II fracture. Moore type II fractures consist of fractures involving the entire tibial condyle, where the fracture line begins in the opposite compartment and extends across the tibial eminence.
A number of classification systems are used to describe tibial plateau fractures. The main classification systems that are widely used include Schatzker, AO/OTA, Hohl and Moore. The Moore classification describes high energy fracture-subluxation injuries of the knee. This is thought to have clinical implications as the type of fracture pattern can indicate an associated soft-
tissue injury.
Moore retrospectively reviewed over a 1000 proximal tibia fractures to devise a classification systems based on the characteristic of five types of tibia plateau fracture patterns. He believed this system helped to better understand knee instability and concomitant soft-tissue injury. For example, Moore Type III fractures (rim avulsion) are associated with a high rate of neurovascular injury.
Figure A shows a fracture involving the entire tibial condyle. Illustration A shows a schematic diagram of the Moore classification (I - V). Illustration B shows a table that describes the Moore classification (I - V).
Incorrect Answers:
Answer 1: Moore Type I is a coronal split fracture of the medial tibia plateau which displaces distally. It does not cross over to the contralateral side of the eminence.
Answer 3: Schatzker Type III is a pure lateral plateau depression.
Answer 4: Schatzker Type V is a bicondylar fracture where the metaphysis and diaphysis remain intact.
Answer 5: OTA type 41B3 is a partial articular fracture with a split-depression of the unilateral plateau.
A 19-year-old male football player plants and twists his right lower extremity sustaining a spiral fracture of his distal third tibial shaft. Of the following images, which is most commonly associated with distal third spiral tibial shaft fractures.
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The patient has a spiral distal tibial shaft fracture. Spiral distal tibial shaft fractures are commonly associated with intraarticular fracture extension, usually in the form of a posterior malleolus fracture.
Spiral distal third tibial shaft fractures need to be evaluated for intraarticular extension prior to operative management. As this can be missed on x-rays, a CT scan of the ankle is recommended to identify this associated injury. This is important when intramedullary fixation is used for definitive management, as nail insertion can displace a previously non displaced intraarticular fracture.
Anteroposterior screw fixation prior to nailing may be useful in these cases.
Boraiah et al. found that in 62 patients with spiral distal tibial fractures, 39% (24 patients) had a posterior malleolus fracture. They recommended CT evaluation of the ankle to prevent missed intraarticular fractures.
Hou et al. found a posterior malleolus fracture in 9.7% (28 out of 288 cases) of patients with tibial shaft fractures. They recommended CT or MRI evaluation of the ankle prior to surgery.
Figure A shows an axial CT scan of a right ankle with a posterior malleolus
fracture. Figure B shows an AP radiograph of a right ankle with a vertical medial malleolus fracture. Figure C shows a coronal CT scan of a right ankle with a Tillaux fracture. Figure D shows a sagittal CT scan of a right ankle with a comminuted talus fracture. Figure E shows a lateral radiograph of a right knee showing a knee dislocation. Illustration A shows an AP radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration B shows a lateral radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration C shows a sagittal CT of a distal third spiral/oblique tibial shaft fracture with a posterior malleolus fracture.
Incorrect Answers:
Answer 2: Vertical medial malleolar fractures are not typically associated with distal third tibial shaft fractures.
Answer 3: Juvenile Tillaux fractures occur typically in patients with open physes. They do not occur in patients with closed physes, and are not associated with tibial shaft fractures.
Answer 4: Spiral/oblique tibial shaft fractures are not associated with talus fractures.
Answer 5: Knee dislocations are considered high energy injuries, and are not associated with tibial shaft fractures.
What would be the most appropriate treatment for this patient at this time?
1) Observation only
2) Referral to physiotherapy
3) MRI spine and hip
4) Total hip arthroplasty
5) Intramedullary femoral nail
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had
been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers
Answer 1: Symptomatic lateral femoral cortical stress fractures, known as "dreaded black lines", should be treated with early stabilization to prevent subtrochanteric fracture.
Answer 2: Referral to physiotherapy would not be indicated.
Answer 3: Symptoms are related to a subtrochanteric stress fracture, which has been identified on radiograph. MRI would not be indicated.
Answer 4: This patient has mild arthritis. Treatment with a long bridging femoral stem may stabilize the fracture, However, the gold standard treatment would be intramedullary nailing.
A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2
weeks. Which of the following would be an indication for surgical management?
1) Age greater than 70 years.
2) Fracture pattern in Figure A
3) Significant medical comorbidities.
4) Fracture pattern in Figure B
5) Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:
Answers 1, 2, 3, and 5 are all factors that would favor non-operative management for a proximal humerus fracture.
A 37-year-old male arrives to the trauma slot following a high-speed motorcycle crash. His Glasgow Coma score is 14 and his only orthopaedic injury is exhibited in Figure A. His current vital signs are a BP of 90/60, HR 120, and a lactate of 2.5 mMol/L. Other findings include a grade 1 splenic laceration and bilateral pulmonary contusions seen on chest radiograph. Which of the following has been suggested as an indication to perform damage control orthopedic care?
1) HR >110
2) Bilateral pulmonary contusions seen on chest radiograph
3) SBP = 90mmHg
4) Unilateral femur fracture
5) Lactate = 2.5 mMol/L
Pulmonary contusion severe enough to be diagnosed on chest radiograph alone is an indicator that the patient may benefit from damage control orthopaedics (DCO).
Despite the patient's overall stable nature, suffering pulmonary injury severe enough to be seen on x-ray alone suggests that temporary stabilization with staged definitive fixation may avoid potential morbidity.
Pape et al. review the evolution and balance of early total care (ETC) and DCO. Summarizing the literature, the authors report several standalone indicators that would justify DCO regardless of stable status. This includes: Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with chest trauma, multiple injuries with severe pelvic/abdominal trauma/ hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs alone, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater.
Figure A exhibits a right femoral shaft fracture. Illustration A exhibits a summarized table stating the criterion used to determine the condition of a polytrauma patient. (Table from Pape et al, PMID: 19726738)
Incorrect answers:
Answer 1: Heart rate alone (even elevated severely) is not an indicator to
implement DCO.
Answer 3: A systolic BP of 90 mmHg is not an indicator to implement DCO. A SBP of 70mmHg or lower may indicate a patient in extremis (along with other parameters) indicating the benefits of DCO.
Answer 4: A unilateral femur fracture alone in a stable patient is not an indicator of DCO; a patient with bilateral femur fractures, however, may benefit from DCO.
Answer 5:A lactate of 2.5 mMol/L, while slightly elevated, does not warrant DCO. A lactate value of greater than 6 alone would indicate the need for DCO.
A 24-year-old patient presents after a fall from the balcony of a third story building in which he landed on his feet. He reports lumbar back pain and numbness in his perineum region. Radiographs of his hips and pelvis are seen in Figure A, while CT images are shown in Figures B and C. How is this fracture pattern best classified?
1) Young-Burgess APC Type II
2) Young-Burgess LC Type I
3) "U" Type Spinopelvic Dissociation
4) Denis Zone-I
5) Denis Zone-II
This patient has a Denis zone-III "U" Type Spinopelvic Dissociation of the sacrum.
The Denis classification system for sacral fractures is based on anatomical fracture zones. Zone-III fractures involve the spinal canal and have a high rate of associated neurologic injury. It is important to recognize bilateral sacral
fractures with a transverse component, as this often causes spinopelvic discontinuity and possible cauda equina. The lack of mechanical continuity between the spine and pelvis will most likely require reduction and fixation for initial stability. There may also be a need for sacral decompression with fixation mechanisms given the onset of neurologic symptoms.
Mehta et al. reviewed sacral fractures. They report that patients with a transverse sacral fracture involving more proximal sacral segments (S1, S2, or S3) tend to have a higher prevalence of bladder dysfunction than do those involving distal sacral segments (S4 or S5).
Schildhauer et al. report the best way to visualize Denis zone-III "U" type fractures is to obtain a lateral view of the sacrum or sagittal reformatted images with a CT scan. Standard pelvic radiographs often miss this injury.
Figure A shows an AP pelvis with suggestion of sacral irregularities. No fracture pattern can be indentified. Figures B and C show CT scan images showing a "U" Type fracture pattern with angulation and translational displacement of the cephalad and caudad parts of the sacrum. Illustration A shows examples of complex sacral Denis zone-III fractures.
Incorrect Answers:
Answer 1: APC Type II fractures do not classify fracture extensions into the sacral canal. The posterior SI ligaments are considered intact. There is usually disruption of sacrospinous and sacrotuberous ligaments.
Answer 2: LC Type I is an oblique or transverse ramus fracture and ipsilateral anterior sacral ala compression fracture.
Answer 4,5: Figures A-C demonstrate a "U" type fracture of the sacrum.
A 55-year-old male presents with the radiographs seen in Figures A and B after falling off his bike. Physical examination reveals an isolated, closed elbow injury. His limb is neurovascularly intact. Which complication would be most likely with surgical fixation of this injury?
1) Ulnar neuropathy
2) Posterior interosseous nerve injury
3) Early loss of fixation
4) Elbow flexion contracture
5) Avascular necrosis
This patient is presenting with a comminuted capitellar and trochlear fracture. If treated with open reduction internal fixation, the most likely post-operative complication would be elbow stiffness or contracture.
An axial compression force transmitted by the radial head to the capitellum with the elbow in a semiflexed position can result in a shear fracture of the anterior portion of the capitellum. AP, lateral, and radiocapitellar radiographs are recommended to identify these injuries. The lateral X-ray may reveal the “double arc” sign, which represents extension of the capitellum fracture into the trochlea. Extension of the fracture into the trochlea has important implications into the surgical approach to these injuries.
Ruchelsman et al. retrospectively reviewed the outcomes of sixteen patients with capitellar fractures treated with open reduction internal fixation. They found the presence of greater flexion contractures at the time of follow-up in elbows with Type-IV capitellar fractures. All fractures healed, and no elbows had instability or weakness with fixation.
Ring et al. retrospectively reviewed the outcomes of twenty one distal humerus articular fractures that were reduced and stabilized with implants buried beneath the articular surface. Ten patients required a second operation: (6) release of an elbow contracture; (2) treatment of ulnar neuropathy; (1) removal of hardware; (1) early loss of fixation.
Figures A and B show AP and lateral radiographs of the elbow with a comminuted fracture of the capitellum and trochlea. Note the “double arc” sign on the lateral view. Illustrations A and B show open reduction internal fixation of the fracture. Note fixation with multiple interfragmentary screws.
Incorrect Answers:
Answers 1,2,3,5: All of these may be complications with this surgery. These complications are not as common as elbow contracture or stiffness.
Figure A shows a radiograph of a 30-year-old male who underwent fixation of a left leg injury just over two years ago. He presents with persistent pain and drainage from the distal wound despite 4 months of oral antibiotics. He has no systemic symptoms. He has a past medical history of Grave's disease and Irritable Bowel Syndrome. What would be the best management at this stage?
1) Chronic suppressive, culture-directed, antibiotic therapy
2) Above knee amputation
3) Endocrine consultation, irrigation and debridement, removal of hardware and negative-pressure wound therapy
4) Irrigation and debridement, removal of hardware, over-reaming medullary canal, external fixation and culture-directed antibiotics
5) Irrigation and debridement, retention of hardware, acute bone grafting and culture-directed antibiotics
This is a case of fracture nonunion in the setting of chronic osteomyelitis and infected hardware. The best treatment option available would be irrigation and debridement, removal of hardware, ring external fixator and culture directed antibiotics.
The management of infected nonunion in the setting of chronic osteomyelitis is technically demanding. The aims of treatment are to eradicate the infection and obtain bone union. Non-surgical options are largely unsuccessful in patients with draining chronic osteomyeltis in the setting of infected hardware and nonunion. Surgical options involve incision and debridement of necrotic tissue followed by reconstruction of bone and possible soft tissue (to provide
healthy viable coverage). The most common techniques are ringed fixator/circular frames, staged intramedullary device with or without external fixator, free tissue transfer, or radical debridement, bone grafting, and fixation.
Motsitsi et al. reviewed the management of infected nonunion of long bones. They suggest that the Ilizarov technique is regarded as a standard treatment in infected nonunion of the tibia. When there is bone defect after debridement, the bone can be shortened or treated with bone transport.
Egol et al look at a series of patients with chronic osteomyelitis. Limb salvage should be attempted in all patients. The presence of a chronic draining sinus requires surgical debridement and culture directed antibiotics. Infected hardware should be removed. A two-stage strategy is the best and well-proven treatment option.
Figure A shows a intramedullary nail in the left tibia. There is a moderate amount of bone loss at the fracture site with mixed sclerotic bone suggestive of osteomyelitis.
Incorrect Answers:
Answer 1: Chronic suppressive therapy would be considered in a patient that is unable to undergo surgical intervention
Answer 2: Amputation is a primary option for patients unable to undergo lengthy or multiple surgical interventions.
Answer 3: After removing the hardware, the fracture non-union will need to be stabilized.
Answer 5: This patients has a chronic infection that requires radical bone debridement and local infection control. The use of acute bone grafting in a single stage procedure in the distal 1/3 tibia (poor blood supply) is less ideal, especially in the setting of infection.
A 32-year-old male sustained the injury seen in Figure A after a motor vehicle accident. Which of the following factors is most predictive of mortality with this type of injury?
1) Fracture classification
2) Number of blood transfusions in the first 24 hours
3) Gender
4) Time to operative fixation
5) Use of pelvic binders
The best predictors of mortality with pelvic ring fractures include older age and hemodynamic shock at presentation. The amount of blood transfused indicates the severity of hemodynamic instability.
Pelvic ring fractures are typically high energy, blunt injuries. The leading cause of mortality with these injuries is hemorrhage and hemodynamic instability.
The most common source of hemorrhage include venous injury (80%), which is usually caused by a shearing injury of posterior thin walled venous plexus and bleeding cancellous bone. Other sources of hemorrhage include arterial injury (10-20%) from the superior gluteal artery (posterior ring injury, anterior posterior compression [APC] pattern), internal pudendal artery (anterior ring injury, lateral compression [LC] pattern) and obturator artery.
Smith et al. found fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased Injury Severity Scores (ISS) scores. Deaths were most commonly from exsanguination (24 hours).
Starr et al. demonstrated that age and shock on presentation were most predictive of mortality after pelvic ring injury.
Figure A shows a APC III pelvic fracture. Illustration A shows a table describing the Young-Burgress classification of pelvic ring fractures.
Incorrect Answers:
Answers 1,3-5: Gender, fracture pattern, time to operative fixation or use of pelvic blinders do not correlate directly with mortality.
Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?
1) Early range of motion
2) Hinged elbow brace for 4 weeks
3) Repair lateral collateral ligament
4) Remove and upsize implant
5) Remove and downsize implant
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intra-operatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by
>or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
Answer 1: Early range of motion is supported after radial head arthroplasty. However, the next most appropriate step in this scenario would be the intraoperative assessment for radiohumeral joint overstuffing.
Answer 2: Hinged braces may be used in the post operative period. However, overstuffing the radiohumeral joint is of first priority.
Answer 3: There is no indication in this question for lateral collateral ligament repair
Answer 4: Removing the implant and upsizing the radial head would be the opposite of what is needed in this scenario.
Aside from improving the intramedullary nail starting point in Figure A, the use of blocking screws could have been used at the time of fixation to prevent this post-operative deformity. What would have been the correct orientation of these screw(s) in the proximal fragment?
1) Medial only
2) Lateral only
3) Anterior and medial
4) Posterior and medial
5) Posterior and lateral
The clinical presentation is consistent with a malunion of a proximal one-third tibia fracture with a valgus and procurvatum deformity. The correct orientation of Poller blocking screws to help prevent this malalignment would be in the posterior and lateral aspects of the metaphyseal fragment.
Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to
prevent valgus deformity. The semiextended position of the knee for nail insertion also helps to eliminate the tendency for the fracture to flex, due to the avoidance of excessive knee flexion during the reduction.
Stedtfeld et al. describes the mechanical model for blocking screws. They state that two or more blocking screws can be placed in each plane (AP and lateral) alongside the nail to create a narrow canal for the nail. This allows for multiple points of fixation and realignment of the bone as the nail is passed.
Lindvall et al looked at a series of 56 extra-articular proximal tibial fractures treated with intramedullary nailing or percutaneous locked plating. Neither nailing or plating these fractures showed a distinct advantage in the overall outcomes. Apex anterior malreduction however was the most prevalent form of malreduction in both groups.
Lang et al. looked at a series of proximal third tibia fracture treated with intramedullary nailing. They reported that posterior tibial comminution will also contribute to apex anterior angulation. They states this occurs when the fracture hinges on the intact cortex anteriorly during nail insertion.
Figure A shows a proximal one third tibia fracture treated with an intramedullary nail. There is malreduction of the fracture with valgus and procurvatum deformity.
Incorrect Answers:
Answer 1: would prevent varus malalignment Answer 2: would prevent valgus malalignment alone
Answer 3: would prevent varus and recurvatum malalignment Answer 4: would prevent varus and procurvatum malalignment
When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
1) A fracture of the radial head requiring ORIF
2) A highly comminuted radial head fracture requiring radial head arthroplasty or resection
3) An MCL injury requiring repair
4) A type I avulsion fracture of the coronoid
5) An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture.
Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:
Answers 1, 2, 3: Radial head fractures, and MCL injuries are not seen in varus/posteromedial mechanisms. They are seen in terrible triad elbow injuries which are due to valgus and posterolateral rotatory forces.
Answer 4: The coronoid fracture seen in these injuries is an anteromedial facet fracture, and not an avulsion fracture of the tip of the coronoid.
A 26-year-old female presented to the emergency department with the injury seen in Figure A after an awkward fall while intoxicated. She undergoes closed reduction and repeat radiographs are seen in Figure B. After a normal physical examination, including ranging the hip from 0-90 degrees, which of the following options would be the next most appropriate step in management?
1) Femoral skeletal traction
2) CT scan
3) Hip spica cast application
4) Observation only
5) Serial neurovascular examinations
This patient has presented with a posterior left hip dislocation. The next most appropriate step would be performing a post-reduction CT scan to assess for joint reduction and congruity, associated fractures, or loose bodies.
Hip dislocations occur most commonly in young patients with high energy trauma. They are usually classified as simple or complex, with complex dislocations being those with associated fractures of the acetabulum or proximal femur. Urgent close reduction should occur within 6 hours from the time of injury. Post reduction CT scans must be performed for all traumatic hip dislocations to look for fractures or impacted areas of the femoral head or acetabulum, as well as incongruent reductions and free intra-articular joint fragments.
Calkins et al. looked at measurements of the posterior acetabulum on CT scans (the Acetabular Fracture Index) after hip dislocations to evaluate for hip stability. Hips were found to be unstable if less than 34% of the remaining posterior acetabulum was present after dislocation. Hips with greater than 55% were stable. In between 34 and 55% were indeterminate.
Moed et al. found that posterior wall fractures involving less than 20% of the posterior wall were considered stable. Fractures involving more than 40%-50% were unstable, leaving a wide range of posterior wall fractures classified as indeterminate.
Figure A shows a left posterior hip dislocation. Figure B shows a reduced left hip with no obvious fracture. Illustration A shows an axial CT scan image of the left hip. There is no acetabular fracture identified.
Incorrect Answers:
Answer 1: Femoral skeletal traction would be considered if there was an associated acetabular fracture or loose body.
Answer 3: Hip spica casts are not used with these injuries.
Answer 4: Observation would be considered after the CT scan is performed. Answer 5: There was no mention of neurovascular injury. This patient has a normal neurovascular examination. There is no fracture or risk of hematoma formation. This would not be necessary.
A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management?
1) MRI angiography of leg
2) Four-compartment fasciotomy
3) Follow-up examination the following day
4) Continued monitoring and serial examinations
5) EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) 30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P
A 10-year-old girl suffers a displaced tibia fracture. Initial numbness over the dorsum of the the foot resolved following an anatomic closed reduction and placement in a long leg cast performed in the emergency room. The cast was placed with the the ankle dorsiflexed just above neutral to prevent equinus contracture and then the cast and padding was adequately bivalved. Overnight, the patient began experiencing recurrent numbness and paresthesias in her exposed toes and a slight increase in her pain at the fracture site. Your next best step would be:
1) Repeat closed reduction under conscious sedation
2) Selective compartment fasciotomies
3) External fixation and compartment monitoring
4) 4-compartment fasciotomies with fracture fixation done emergently
5) Modify the cast to reposition the ankle into slight plantarflexion
Circumferential casting with the ankle dorsiflexed can cause increased intracompartmental pressures in the leg. However, this patient's cast has been adequately bivalved during initial cast placement. Therefore, the next best step is cast modification to allow the ankle to assume an angle between neutral and 30 degrees of plantar flexion and further reducing the compartment pressure.
Tibia fractures are one of many common underlying etiologies for the development of compartment syndrome in the leg. Fracture reduction as well as eliminating circumferential dressings are important early preventative steps to take. Bivalving casts - including splitting the cast padding - is often indicated in fractures of long bones that are treated with initial casting. While casting patients in a plantigrade or dorsiflexed position reduces the risk of equinus contractures and holds the ankle mortise reduced, dorsiflexing the ankle has been shown to increase the intracompartmental pressures throughout the leg compartments.
Weiner et al. placed pressure monitors into the anterior and deep posterior compartments in healthy volunteers to measure the effects of casting on compartment pressures. They found that the intramuscular pressures were lowest with the ankle positioned between plantigrade and a resting plantar flexion position (0-37 degrees), and that bivalving the cast reduced the pressures 33-47%.
Illustration A shows the needle trajectories for compartment pressure monitoring in the leg. This should be performed within 5 cm of the fracture to get accurate peak pressures.
Incorrect Answers:
Answers 1, 3: The stem does not suggest that the reduction was lost, so neither repeating a closed reduction or placement of an external fixator is indicated at this time.
Answers 2, 4: While suspicion should remain elevated for the development of compartment syndrome, simple conservative measures such as cast modification are ideal first steps to avoid onset of compartment syndrome. The clinical vignette given does not portray clinical compartment syndrome requiring emergent fasciotomy. It would be reasonable to maintain a high level of suspicion given the injury, but non-invasive cast modification is a simple, safe and quick first step.
A 35-year-old male horseback rider was bucked into the air and then landed forcefully with his perineum on the saddlehorn of the saddle. At a one year follow-up, the only long term sequela of his injuries is erectile dysfunction. Which radiographic injury seen in Figures A-E is most commonly associated with this complication?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
This patient has sustained a saddle-horn injury to the pelvis. An anterior posterior compression (APC) injury is the most common pelvic injury associated with this mechanism.
Saddle-horn injury to the pelvis occurs when a horseback rider is bucked into the air and then lands forcefully with his or her perineum on the saddlehorn of the saddle. The bony injury to the pelvis usually consists of a diastasis of the pubic symphysis with/without subsequent widening of the sacroiliac joints. The
majority of patients are able to return close to their pre-injury level of employment and activity after these injuries. However, sexual dysfunction is a common complication with this injury. Sexual dysfunction can be due to urethral, vascular, neurologic, and psychogenic injuries.
Collinge et al. looked at a series of male patients with injuries to the perineum after coming into contact with the saddle or saddle horn on a horse. Eighteen of the twenty patients were found to have sexual dysfunction at the time of the latest follow-up. A multi-disciplinary approach to these patients is needed when treating pelvic injuries.
Cannada et al. surveyed 71 women of childbearing age who had a pelvic fracture. She found that half the patients reported physical genitourinary complaints with 38 percent of women noting new onset pain with intercourse. In terms of psychological impact, they showed that 45 percent of patients answered affirmatively to decreased interest in intercourse and decreased orgasm frequency after the injury.
van Nieuwenhoven et al. describe three equestrians who suffered from straddle injuries with symphysis diastasis and rupture of sacroiliac ligaments after falls or kicks from horses. They show that these presumed low-energy injuries can cause extremely severe injuries to the pelvis itself and to the adjacent organs.
Figure A shows a Burgess APC Type II pelvic fracture. Figure B shows left ASIS avulsion fracture. Figure C shows a left hip dislocation. No pelvic fracture is identified. Figure D shows a subacute superior/inferior pubic rami fracture.
Figure E shows a right femoral neck fracture.
Incorrect Answers:
Answers 2,3,4,5: Any pelvic or lower limb fracture can cause a disruption in a patients activities of daily living. This may include sexual dysfunction, for both men and women. The injury pattern that has the greatest potential for sexual dysfunction are APC type pelvic injuries.
A 31-year-old male driver was involved in a high-speed motor vehicle accident. His injuries include a left subdural hematoma (Abbreviated Injury Score [AIS]=4), left segmental femur fracture (AIS=3), ruptured spleen (AIS=4), nasal fracture (AIS=2), fractured left ribs 4 to 7 (AIS=2), and a closed pelvic ring fracture (AIS=3). What is his Injury Severity Score (ISS)?
1/. 18
1) 25
2) 33
3) 41
4) 48
This patients Injury Severity Score (ISS) is 41. In this patient, the highest AIS scores were from the head (AIS=4), abdomen (AIS=4) and pelvis (AIS=3).
Therefore, the calculation for the ISS score was 4^2 + 4^2 + 3^2 = 41.
The ISS score is calculated as the sum of the square values from the highest Abbreviated Injury Score [AIS] scores in the three most severely injured ISS body regions. ISS scores range from 1 to 75. A single score of 6 on any AIS region results in automatic score of 75. ISS scores > 15 are associated with mortality of 10%.
Poole et al. found that the AIS and ISS appropriately reflect the impact of extraskeletal injuries in patients with femur fractures, but they do not adequately reflect the increased morbidity associated with multiple lower extremity fractures.
Balogh et al. aimed to compare the scoring efficacy of the injury severity score (ISS) and the new injury severity score (NISS) in predicting post-injury outcomes. They found that multiple orthopaedic injuries, as used in the NISS system, had a significantly greater impact on reported poor post-injury outcomes. They suggest that NISS should replace the traditional ISS when grading trauma related outcomes.
Illustration A shows a table of the various ways to score injury severity in trauma patients.
Incorrect Answers:
Answers 1,2,3,5: ISS = A^2 + B^2 + C^2, where A, B, C are the AIS scores of the three most severely injured ISS body regions. The only correct answer is ISS=41.
A 60-year-old otherwise healthy female sustains the fracture in Figure A. Immediate surgical treatment would most likely prevent which of the following complications?
1) Malunion.
2) Regional osteopenia.
3) Skin necrosis.
4) Posttraumatic arthritis.
5) Refracture.
The patient has a calcaneal tuberosity fracture. The Achilles tendon is attached to the displaced fragment, which can cause soft tissue compromise and skin necrosis if not treated promptly.
Displaced calcaneal tuberosity and tongue-type calcaneus fractures have a high incidence of wound complications if not treated urgently. Recommended management includes surgical fixation often performed percutaneously. Lag screws are typically directed from the posterior superior tuberosity inferiorly and distal. In cases of skin sloughing and skin necrosis, flaps may be needed.
Gardner et al. reviewed 139 tongue-type calcaneus fractures, and found that 21% had some degree of posterior skin compromise. Additionally, there was a statistically significant increase in posterior skin compromise with delayed presentations.
Hess et al. reviewed 3 cases of calcaneal tuberosity avulsion fractures that let to skin necrosis because of a delay in treatment.
Tornetta reviewed the indications for percutenaous treatment of calcaneus fractures, and found it was successful and most useful in tongue-type calcaneus fractures.
Figure A shows a lateral radiograph of a R ankle showing a calcaneal tuberosity fracture. Illustration A shows an AP radiograph of a R ankle following percutaneous reduction and internal fixation of the calcaneus fracture with two cannulated screws. Illustration B shows a lateral radiograph of a R ankle showing interval reduction and fixation of the calcaneus fracture. Illustration C shows a clinical photograph of posterior skin compromise associated with a calcaneal tuberosity fracture.
Incorrect Answers:
Malunion, regional osteopenia, posttraumatic arthritis, and refracture risk would not be significantly altered with immediate surgical intervention as opposed to operative management within a reasonable time frame.
When elevating the joint surface in the injury pattern seen in Figure A, what material has the highest compressive strength when filling the metaphyseal void?
1) Calcium phosphate
2) Tricalcium phosphate
3) Cancellous autograft
4) Cancellous allograft
5) rhBMP-7
Figure A illustrates a depressed lateral tibial plateau. One of the key components of fixing a depressed articular segment is maintaining the reduction.
Trenholm et al reviewed an experimental study where a split depression (Schatzker II) fracture was created in a cadaveric model. The stiffness of the elevated fragment in cadavers using calcium phosphate cement versus cancellous bone graft as support showed no difference, but calcium phosphate cement was found to have greater compressive strength than cancellous bone alone.
The review article by Hak reviews the composition, advantages, and disadvantages of commerically available bone graft substitutes.
Incorrect answers:
2: Tricalcium phosphate is a bone graft substitute that is osteoconductive, but has less compressive strength.
3-4: Cancellous bone has less compressive strength than calcium phosphate. 5: rhBMP-7 is not used as a bone filling agent in this instance, as it is typically provided on a easily compressible collagen sponge.
A 42-year-old male sustains multiple abdominal injuries along with the fractures shown in Figures A and B. Which of the following factors is most useful to determine the patient's resuscitation and ability to undergo early definitive fixation of these two fractures?
1) Pulse pressure
2) Respiratory rate
3) Urine output
4) Platelet count
5) Base deficit
The base deficit, or lactate level, has been shown to best reflect the resuscitation status and survival after trauma.
Normalization of hemodynamic parameters does not accurately reflect the resuscitation status and a patient can be in compensated shock (occult tissue hypoperfusion) despite normalization of the heart rate and blood pressure. The use of temporizing measures with delayed definitive fracture treatment has been shown to decrease systemic complications in these patients with occult hypoperfusion.
Crowl et al. performed a retrospective study of 127 patients with femoral shaft fractures undergoing intramedullary nailing, assessing for occult hypoperfusion. Patients with occult hypoperfusion preoperatively had a twofold increase in postoperative complications and significant increase in postoperative infections.
Tisherman et al. present a review of hemodynamic parameters and their use in assessment of resuscitation. They report that hyperlactatemia is common among critically ill patients, and lactate levels and their trend may be reliable markers of illness severity and mortality. Therefore, measurement of blood lactate is recommended to stratify patients based on the need for fluid resuscitation and the risks of multiple organ dysfunction syndrome and death. They conclude that lactate is a reliable indicator of sepsis severity and a marker of resuscitation; however, it is an unreliable quantitative marker of tissue hypoxia/hypoperfusion.
Pallister et al. present a review of the effect of early stabilization of long bone fractures. They note that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure, both of which are caused by activation of the systemic inflammatory response. This activation results in tissue recruitment of and injury by circulating polymorphonuclear leukocytes.
Figure A is a radiograph showing a femoral shaft fracture, while Figure B shows an open tibial shaft fracture.
Incorrect Answers:
Answers 1-4: Normalization of these factors does not always predict adequate resuscitation.
Interleukin-6 levels have been shown to be a reliable measure of which of the following?
1) Osteoporosis
2) Severity of injury
3) Sarcomatous tumor burden
4) Bone turnover
5) Hyperparathyroidism
Interleukin-6 (IL-6) is a proinflammatory cytokine that is increased according to the level of injury sustained and acts to activate the host immune system. In addition, new literature exists to indicate its high sensitivity and specificity for detecting infection in total joint arthroplasty.
Overactivation of the immune system and cytokines can lead to systemic inflammatory response syndrome (SIRS), which results in end-organ damage, including small-vessel vascular damage; this would lead to parenchymal cell death from hypoxic insult.
Keel et al. report that immediate and early trauma deaths are determined by brain injuries or significant blood loss, while late mortality is caused by secondary brain injuries and host defense failure. The secondary effects are characterized by local and systemic release of pro-inflammatory cytokines, arachidonic acid metabolites, proteins of the contact phase and coagulation systems, complement factors and acute phase proteins, as well as hormonal mediators.
Pape et al. investigated the effect of surgeries as a "second-hit" phenomenon. They found that surgery on days 2-4 was associated with a greater amount of postoperative organ dysfunction than if the secondary surgery was done on days 5-8. They also found a significant association between IL-6 values above 500pg/dL at the time of surgery and development of multiple organ failure.
Sears et al. review the effect of the inflammatory response to trauma and the development of complications (death, multiple organ failure). They report that IL-6 and the HLA-DR2 molecules currently appear to have the most potential for use in predicting outcomes in trauma patients.
Illustration A is a diagram that shows some of the effects of IL-6 production.
Incorrect Answers:
1,3-5: IL-6 levels are not known to be reliably altered by these factors.
A 31-year-old male sustained a displaced proximal humerus fracture after a motor vehicle accident. Which of the following factors has the lowest association with humeral head ischemia in these injuries?
1) Four-part fracture
2) Head-splitting fracture
3) Neck fracture with a long calcar segment
4) Disrupted medial periosteal hinge
5) AO type C3 fracture
A long calcar fracture segment, also known as the posteromedial metaphyseal head extension, is a good prognostic sign against the development of osteonecrosis in displaced proximal humerus fractures.
The humeral head is directly supplied by the anterior and posterior humeral circumflex arteries. Disruption of these vessels can result in humeral head osteonecrosis. Fracture patterns with long medial metaphyseal segments (greater than 8 mm) have not shown to critically disrupt the vascular supply to the humeral head causing osteonecrosis. Other factors shown to be protective against osteonecrosis after trauma include an intact medial hinge and simple fracture patterns.
Hertel et al. examined the factors predictive of osteonecrosis of the humeral
head after fracture. These include four-part fragments, angular displacement
>45 degrees of the head, displacement of the tuberosities greater than 10 mm, glenohumeral fracture-dislocation, and head-splitting fractures.
In Hertel's second paper and follow up study they noted that the initial post-fracture humeral head ischemia does not predict development of necrosis.
Illustration A shows an example of a long and short calcar fracture segment. Illustration B shows the AO classification of proximal humerus fractures.
Incorrect Answers:
Answers 1,2,4,5: All these factors are predictive of osteonecrosis.
A 50-year-old female has been diagnosed with osteomyelitis of her left tibia. The infection is isolated to the meduallary canal of the bone, and her past medical history is significant for heavy smoking and chronic venous stasis. Based on the clinical staging of osteomyelitis, what would be her Cierney-Mader classification?
1) Stage 2A
2) Stage 1B
3) Stage 1C
4) Stage 3B
5) Stage 4C
The Cierny-Mader classification is a clinical classification based on clinical and anatomic features. This patient's Cierny-Mader classification is Stage 1B.
The Cierney-Mader classification system characterizes osteomyelitis in one of four anatomic stages. Stage 1 is confined to the medullary cavity of the bone. Stage 2 involves only cortical bone. Stage 3 is a localized infection to cortical and medullary bone. However, the bone remains stable. Stage 4 involves the entire thickness of the bone, with loss of bone stability. The Cierny-Mader system also sub-characterizes patients as A, B, or C. The [A} patients have no systemic or local immune compromising factors. The [B] patients have one or more systemic or local compromising factors. The [C] patients are severely immunocompromised and treatment will lead to greater morbidity than the infection.
Mader et al. described the treatment algorithm of osteomyelitis using the Cierny-Mader classification. Treatment involves both antibiotic and surgical debridement. For type 1 infection, thorough intramedullary reaming and unroofing is usually performed.
Illustration A shows a table for the Cierny-Mader classification. Illustration B shows a schematic illustration of the anatomical involvement of osteomyelitis using the Cierny-Mader classification.
Incorrect Answers:
Answer 1: This would be a cortical infection only in a healthy patient. Answer 3: This would be a medullary cavity infection only in a severely compromised patient.
Answer 4: This would be a localized infection to cortical and medullary bone in a patient with one or more systemic or local compromising factors.
Answer 5: This would be a diffuse infection involving the entire bone in a severely compromised patient.
A 68-year-old female sustains a fall to her dominant arm and sustains the fracture seen in Figure A. She undergoes uneventful open reduction internal fixation with a locked plate and screw construct. Which of the following radiographs (Figures B, C, D, E, or F) show the most common complication associated with this treatment modality?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
Figure B shows screw penetration of the articular surface, which is the most common complication following locked plate and screw fixation.
Inadequate fixation, typically in the humeral head, subsequently fails leading to varus deformity and screw penetration. This most commonly occurs in fixation for 3 and 4 part fractures, but can also occur following fixation for 2 part fractures.
Egol et al. retrospectively reviewed 51 patients following locked plating of 3-and 4-part proximal humerus fractures, they found 16% had screw penetration. The authors recommended ensuring appropriate number and length of the screws placed to prevent cut-out.
Brunner et al. reviewed 158 proximal humerus fractures. They found at 1 year follow-up noted 14% screw penetration rate. They recommended close followup to monitor for cut-out.
Figure A shows a 3-part proximal humerus fracture. Figure B exhibits varus cut-out and screw penetration. Figure C exhibits non-union and fixation failure. Figure D exhibits avascular necrosis and complete head collapse. Figure E (arrow) exhibits changes consistent with heterotopic ossification.
Figure F exhibits non-union and fixation failure at the level of the shaft.
Incorrect answers:
Answer choice 2/5 (figure C/F): Non-union and fixation failure can also occur, but at a relatively low rate.
Answer choice 3 (Figure D): Avascular necrosis also occurs, but at a lower rate than screw penetration.
Answer choice 4 (Figure E): Heterotopic ossification (arrow) can occur but is rare.
Figure A shows an acute, isolated and closed, left knee injury in a 40-year-old male struck by a motor vehicle. What would be the most
appropriate surgical fixation for this injury?
1) Definitive external fixation
2) Temporary external fixation then lateral percutaneous screws
3) Lateral nonlocking plate +/- bone graft substitutes
4) Medial and lateral locking plate +/- bone graft substitutes
5) Lateral percutaneous screws with assisted arthroscopy
This patient has sustained a Schatzker 2 (AO/OTA Type B) fracture of the lateral tibial plateau. The most appropriate treatment of this fracture would be fixation with a lateral nonlocking plate +/- bone graft substitute.
Displaced, widened and depressed tibia plateau fractures are an indication for operative intervention. The aim of surgery is to restore anatomic articular congruity, length, alignment and rotation of the proximal tibia. This is best achieved by (1) direct reduction of the articular surface, and (2) fixation of the interfragmentary piece with a plate and screw construct, which provides subarticular support, interfragmentary compression, and prevents shearing of the fracture. In patients with good bone quality, this is best achieved with an undercontoured lateral nonlocking plate in buttress mode.
Karunakar et al. showed that there was no significant difference between split depression tibial plateau fractures (Shatzker II) fixed with either (1) buttress plate with rafting screws versus (2) periarticular plate with built in rafting screw hole options.
Gardner et al. examined 62 consecutive Schatzker type II fractures with radiographs and MRIs preoperatively. They found that joint depression greater than 6mm and widening of greater than 5mm was associated with a lateral meniscal injury over 80% of the time.
Figure A provided a sequence of coronal CT scan images of a left knee. There is a lateral split depression tibial plateau fracture with significant joint
depression, articular impaction and condylar widening.
Incorrect Answers:
Answer 1: Definitive external fixation of tibial plateau fractures may be considered in patients who are unable to tolerate definitive surgery, severe open fractures, infections, or significant bone loss.
Answer 2: Temporary external fixation would be considered in patients with significant soft tissue injury.
Answer 4: Locking plates do not provide buttress effect when used in pure locking mode. In addition, locking plates add significant incremental cost to the procedure. Medial plating would support a bicondylar fracture.
Answer 5: Screws alone are unlikely to be adequately stable in this patient. Although not commonly employed, knee arthroscopy is considered by some surgeons to be a valuable method to assist in obtaining the best articular surface reduction during surgery.
An otherwise healthy young adult male sustains a transverse radial shaft and ulna fracture. He undergoes definitive surgical fixation with two non-locking compression plates (LCPs) as shown in Figure A. What is the principle of this fixation technique on bone healing?
1) Absolute stability with direct healing by callus formation
2) Relative stability with indirect healing by callus formation
3) Absolute stability with direct healing by internal remodeling
4) Relative stability with indirect healing by internal remodeling
5) Absolute stability with endochondral bone formation
Definitive surgical fixation for a simple transverse both bone forearm fracture would include open reduction and internal fixation with absolute stability with direct healing by internal remodelling (i.e., primary bone healing). The radius is fixed with a 7-hole 3.5mm LC-DCP plate in compression mode. The ulna was fixed with a 8-hole 3.5mm LC-DCP neutralization plate with (2) lag screws.
Restoration of the radial bow, length, and alignment in conjunction with primary bone healing would optimize the restoration of pronation/supination in the forearm. Compression plating and anatomic reduction of articular fractures are examples of absolute stability. Casting, bridge plating, external fixation, and intramedullary nailing provide relative stability, with secondary bone healing resulting.
Moed et al. reviewed 56 patients with open diaphyseal forearm fractures treated with immediate internal fixation. The complications included deep infection in 2 patients and non-union in 6. This study indicated immediate stable plate fixation was a beneficial method of treatment for open diaphyseal forearm fractures.
Jones et al. discussed current literature on treating adult diaphyseal forearm fractures with open reduction internal fixation versus intramedullary nailing, and concluded a randomized prospective study is needed. They stated current literature is inconclusive.
Figure A shows a both bone forearm fracture fixed with absolute stability. The radius is fixed with a 7-hole 3.5mm LC-DCP plate in compression mode. The ulna was fixed with a 8-hole 3.5mm LC-DCP neutralization plate with (2) lag screws.
Incorrect Answers:
Answers 1-2, 4-5: Absolute stability is a biological process of osteonal bone remodelling. This is predominantly intramembranous ossification. Enchondral bone formation occurs in non-rigid fracture healing (secondary bone healing).
A 27-year-old man sustains a tibial plateau fracture as pictured in Figure A-D. Which combination of fixation constructs and stability
would optimize his outcome?
1) Intramedullary nailing for a relative stability construct
2) Posteromedial buttress plating for an absolute stability construct
3) Locked lateral plating an absolute stability construct
4) Medial antiglide plating for a relative stability construct
5) Spanning external fixation for an absolute stability construct
Intraarticular tibial plateau fractures require absolute stability constructs to maintain anatomic joint reductions without callus formation. This condylar split fracture is ideally treated with buttress fixation at the apex of the fracture to avoid the high likelihood of shear failure with a laterally placed fixed-angle construct.
Tibial plateau fractures in young adults are high energy injuries, and the condylar split components of the fractures occur due to shear failure. The mechanism of failure - axial loading combined with a varus or valgus moment with the knee extended or flexed - dictates the orientation of the condylar split fracture line(s). There are multiple fracture classification schemes that assist with surgical decision making, particularly with placement of buttress plate fixation to resist shear failure. Articular impaction and joint depression must also be addressed.
Bai et al. performed a biomechanical study on fresh cadavers to simulate residual articular step-offs after fixation. With a >5 mm step-off, contact pressures increased over 200%.
AO guidelines of tibial plateau fracture management are discussed in depth in AO Principles of Fracture Management, and up-to-date principles can be found on the AO surgery reference. Anatomic reduction and absolute stability are important elements of all intraarticular proximal tibia fractures.
Figures A and B are injury films of a tibial plateau fracture with a large posterior split of the medial condyle. Figure C shows an axial CT cut displaying the same fracture. Illustrations A-C show how the injury was treated. Through a posterior incision, an under-contoured anti-glide plate was used to reduce the fracture at the apex. Subsequently, a pre-contoured posteromedial buttress plate was placed to maintain the reduction. The articular reduction was finalized with rafting screws outside of the plating construct to optimize the angle of subchondral support.
Incorrect Answers:
Answers 1, 4: Relative stability is inappropriate for intraarticular fractures that require anatomic reductions
Answer 3: Laterally-based locked plating for a medial condyle fracture creates large moments about the screw-plate interface, and the construct is apt to fail in shear
Answer 5: Spanning external fixation is most commonly used for temporizing tibial plateau fractures when significant soft tissue is present - in the absence of additional fixation for a hybrid construct, it would provide relative stability
Surgical fixation with absolute stability would be most appropriate for which of the following fracture patterns?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Anatomic reduction and fixation with absolute stability is appropriate for articular fractures, such as posterior malleolar ankle fractures with significant joint involvement.
Compression plating and anatomic reduction of periarticular fractures yield absolute stability. Fractures treated with absolute stability achieve primary bone healing. Posterior malleolar ankle fractures comprising greater than 25% of the joint and non-comminuted lateral malleolar ankle fractures are typically treated with internal fixation to achieve absolute stability. Casting, bridge plating, external fixation, and intramedullary nailing provide relative stability, with secondary bone healing resulting. In fractures with significant comminution and in lower extremity diaphyseal long bone fractures, relative stability is employed.
Gardner et al. surveyed members of the Orthopaedic Trauma Association (OTA) and American Orthopaedic Foot and Ankle Society (AOFAS) regarding treatment of posterior malleolus ankle fractures. They found that size influenced decision making, with 97% electing to treat those posterior malleolus fractures that comprised 50% of the joint. The most common used
approach was the posterolateral approach, which utilizes the interval between the flexor hallucis longus and peroneals.
Forsberger et al. reviewed 45 consecutive patients treated with surgical fixation of the posterior malleolus through the posterolateral approach. This approach allowed excellent exposure with few soft tissue complications.
De Vries et al. reviewed 45 patients with ankle fractures that had a posterior malleolar component. Those patients that had the posterior malleolar fragment fixed did not have statistically better functional scores than those who did not have the fragment fixed. They concluded that those patients with fragment sizes less than 25% did not require fixation and had good functional outcomes at 13 year follow-up.
Figure A shows an AP and lateral radiograph of a right comminuted distal third radial shaft fracture. Figure B shows an AP and lateral radiograph of a lateral and posterior malleolar ankle fracture in addition to a deltoid rupture. Figure C shows an AP and lateral radiograph of a comminuted middle third tibial shaft fracture. Figure D shows an AP radiograph of a minimally displaced greater trochanter fracture. Figure E shows an AP and lateral radiograph of a pediatric distal radial metaphyseal fracture. Illustration A shows an AP, mortise, and lateral radiograph of a posterior and lateral malleolus ankle fracture treated with open reduction and internal fixation.
Incorrect answers:
Answer 1: Significant comminuted radial shaft fractures are treated with bridge plating, which would achieve relative stability.
Answer 3: Diaphyseal tibial fractures are treated with intramedullary nailing, which achieves relative stability.
Answer 4: Minimally displaced greater trochanter fractures are treated nonoperatively.
Answer 5: Pediatric distal radius fractures are typically treated with closed reduction and casting, which achieves relative stability.
Figures A and B are radiographs of a 72-year-old male who presented to hospital 3 days after an unwitnessed fall. He presents with pain and the inability to mobilize since the fall. The patient lives independently and has no significant past medical history. Physical examination reveals an alert and oriented patient. This is an isolated injury with no other focal or systemic deficits. What would be the most important investigation to be obtained before taking this patient to the operating room?
1) Pelvic inlet and outlet views
2) CT head
3) Duplex ultrasound of both lower extremities
4) CT hip and pelvis
5) MRI hip and pelvis
The most appropriate investigation to order in this patient would be a duplex ultrasound of both lower extremities.
Immobilized elderly patients with a delay of more than two days from the fracture to presentation at the hospital are at a higher risk of deep-vein thrombosis (DVT). The risk can be higher in patients with factors that predispose to clot formation, such as malignancy. Patients with a delayed presentation to hospital should be investigated for DVT. The most common screening modality is duplex ultrasound of both lower extremities.
Hefley et al. looked at the effect of delayed admission to the hospital on the preoperative prevalence of DVT associated with hip fractures. They found that 6 out of 11 patients with a delay of more than two days between the fracture and admission to the hospital had evidence of thrombosis. They conclude all patients with delayed admission, after a hip fracture, should be evaluated for DVT preoperatively.
Figure A and B are AP and lateral radiographs that show a displaced left subcapital hip fracture.
Incorrect Answers:
Answer 1: There is no indication of pelvic inlet and out views. Generally speaking, pelvic inlet and outlet views assess the pelvic ring and pelvic bone stock, which are normal in this patient.
Answer 2: CT head would be indicated after an unwitnessed fall if the patient admitted to head injury, had neurological symptoms or acute focal/systemic deficits on exam. None of these are present in this patient.
Answer 4 and 5: A CT or MRI of the hip and pelvis are not indicated in a displaced fracture, but may be useful in diagnosing nondisplaced fractures.
A 67-year-old female sustains the injury shown in Figure A after a trip and fall. When discussing the outcomes of surgery with the patient, which of the following statements is true?
1) Post-surgical mortality rates are significantly lower after total hip arthroplasty compared to hemiarthroplasty
2) Internal fixation shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to arthroplasty
3) Bipolar hemiarthroplasty shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to unipolar hemiarthroplasty
4) A delay in surgery greater than 48 hours is acceptable if the patient has multiple medical comorbiditiesm which are not fully optimized
5) Dislocation rates are equivalent between total hip arthroplasty and hemiarthroplasty
Moderate evidence supports that hip fracture surgery within 48 hours of admission is associated with better outcomes. However, patients with significant medical comorbidity should be fully optimized before surgery.
Although several studies have shown a benefit to surgery within 48 hours, no definitive time frame has been elucidated. The majority of literature has shown improved outcomes in regards to pain, complications, and length of stay with early surgery. Patients with significant medical comorbidities have been shown to have the highest mortality rates.
Moran et al. aimed to determine whether a delay in surgery for hip fractures had an affect on postoperative mortality among elderly patients. In an observational study of 2660 patients, they showed that mortality following hip fracture surgery was 9% at 30-days, 19% at 90-days, and 30% at 12-months.
Patients with medical comorbidities had 2.5 times the risk of death within 30-days of surgery. In addition, individuals who had surgery delayed beyond 4 days had increased mortality at 90-days and 12-months.
Papakostidis et al. examined the timing of internal fixation of intracapsular fractures of the neck of femur on the development of late complications, particularly osteonecrosis of femoral head (ONFH) and non-union. They showed no benefit of early surgery on incidence of AVN. However, delay of internal fixation of more than 24 hours showed increased rates of non-union.
Figure A shows a displaced right femoral neck fracture. Incorrect Answers:
Answer 1: Patients treated with hemiarthroplasty or total hip arthroplasty
demonstrated no statistically significant difference in mortality.
Answer 2: Arthroplasty consistently has better outcomes compared to internal fixation for the treatment of unstable/displaced (Garden III and IV) femoral neck fractures in elderly patients.
Answer 3: Outcomes of unipolar and bipolar hemiarthroplasty for unstable femoral neck fractures are similar.
Answer 5: Dislocation rates are higher with total hip arthroplasty compared to hemiarthroplasty.
An 87-year-old female sustains the injury shown in Figure A after a fall from standing. At baseline, she ambulates with a walker in her home and lives with a 24-hour home health aide. She has a past medical history of stroke and mild dementia. Following medical optimization, what is the most appropriate treatment modality?
1) Intramedullary nail
2) Hemiarthroplasty
3) Closed reduction percutaneous pinning
4) Total hip arthroplasty
5) Sliding hip screw
At baseline, with minimal ambulatory status and dependence on a 24-hour home health aide, the best treatment choice is hemiarthroplasty.
Arthroplasty is the gold standard for displaced femoral neck fractures in the elderly. In community ambulators with relative independent lives, total hip arthroplasty (THA) is recommended. For minimal ambulator, hemiarthroplasty is recommended.
van den Bekerom et al. randomized 252 patients over 70-years-old to either THA or hemiarthroplasty for displaced femoral neck fractures. With increased blood loss, operative time and dislocation risk, they did not recommend THA unless there was good preoperative ambulatory status, and/or pre-existing osteoarthritis or rheumatoid arthritis.
Figure A exhibits a displaced femoral neck fracture
Incorrect answers:
Answers 1, 3, 5 are not the treatment standards for displaced femoral neck fractures in the elderly.
Answer 4 is incorrect because the patient is minimally ambulatory at baseline with little independence.
A 20-year-old female arrives to the trauma bay following a motor vehicle accident. She was a restrained driver and has bilateral chest tubes placed in the trauma slot. Initial laboratory values are significant for a hematocrit of 45.5 g/dL and a lactate of 7 mmol/L. Both lower extremities exhibit grossly open wounds. Radiographs are shown in Figure A and B. What is the best initial management of her orthopaedic injuries?
1) Irrigation and debridement of left femur and right tibia with bilateral external fixator placement
2) Irrigation and debridement of left femur and right tibia with left external fixator placement and right tibial intramedullary nail placement
3) Irrigation and debridement of left femur and right tibia with left femoral and right tibial intramedullary nail placement
4) Irrigation and debridement of left femur and right tibia with left femur open reduction and internal fixation and right tibial intramedullary nail placement
5) Irrigation and debridement of left femur and right tibia with bilateral long leg splint placement
Presenting as an unstable patient, damage control orthopaedics (DCO) should be performed by placing bilateral external fixators following irrigation and debridement.
Signs of clinical instability include an elevated lactate level as well as injuries to both lungs, necessitating bilateral chest tubes. Furthermore, while the patient is young and her hematocrit reflects a 'normal' number, more likely is a hypovolemic state due to bilateral open long bone injuries. Resuscitation is required and early total care (ETC) should be avoided.
Pape et al. review the early data regarding DCO and ETC. Identification of patients in extremis, borderline, unstable or stable patients is critical to determining appropriate management. Adequate resuscitation, by tracking lactate, as well as full evaluation of the multiply injured patient is crucial in determining application of DCO versus ETC. DCO is necessary as a temporizing stage to improve mortality in critically injured patients.
Renaldo and Egol revisit the evolution of trauma care where early, acute treatment evolved to ETC, and again to the development and implementation of DCO and staged fixation. Reviewing the initial post-traumatic inflammatory response, the authors review literature that supports the implementation of DCO in the unstable patient, especially the role of the 'second hit' phenomenon and the spike in inflammatory cascade that occurs between days 2-5 following injury.
Figure A is a lateral x-ray of a comminuted, displaced, open distal femur fracture. Figure B is an anteroposterior radiograph of a spiral, oblique, open tibia fracture.
Incorrect Answers:
Answers 2-4: Due to the elevated lactate levels and unstable nature of the patient, DCO should be applied via placement of external fixators. Definitive fixation at this time could worsen the patient's acute condition and subsequent
morbidity and mortality.
Answer 5: This patient, while unstable, is not in extremis, therefore temporary skeletal stabilization should be placed with external fixators.
Figure A is a radiograph of a 31-year-old male cyclist who was struck by a vehicle. Physical examination revealed a 2 cm opening in the skin over the anteromedial leg. He was treated operatively with an unreamed intramedullary nail. What outcome can be expected using this operative modality when compared with reamed intramedullary nailing?
1) Higher rates of nonunion
2) Higher rates of malunion
3) Higher rates of infection
4) Lower rates of infection
5) No difference
The best definitive surgical fixation option for an open fracture of the tibia would be either a reamed or unreamed intrameduallary nail.
Treatment of open tibia fractures require immediate antibiotics and early
irrigation and debridement. Surgical fixation options are vast, but largely based on the severity of injuries both locally or systemically. External fixation devices are mainly used for provisional fixation in polytrauma patients or definitively in proximal or distal metaphyseal fractures. Plating may be used in a staged fashion after a period of external fixation. The most common fixation method is intramedullary nailing. The use of a reamed or unreamed nail technique does not affect union rates, infection rates, or need for additional surgeries in open tibia fractures.
Bhandari et al conducted a multicenter, blinded randomized trial of 1319 adults in whom a tibial shaft fracture was treated with either reamed or unreamed intramedullary nailing. When comparing outcomes in open and closed injuries at twelve months, they found a benefit for reamed intramedullary nailing in patients with closed fractures, but found no difference between approaches in patients with open fractures.
Finkenmeier et al conducted a randomized controlled study of reamed vs. unreamed nails in open and closed tibia fractures (excluding Grades IIIB and IIIC). They found that the use of reamed insertion of IM nails for the treatment of closed tibia fractures lead to an earlier time to union without increased complications. The authors reported no differences in infection rate, compartment syndrome rate, or percent needing additional surgeries to obtain union. More secondary procedures were needed with unreamed nails in closed fractures only.
Figure A shows a mid-shaft tibia fracture. Incorrect Answers:
Answers 1, 2, 3, 4: All prospective studies show no difference in the rates of
non-union, malunion, or infection when using a reamed or unreamed nails to treat open tibia fractures.
A 27-year-old male presented to the trauma bay following a motor vehicle crash and was diagnosed with a comminuted open tibia fracture. He was subsequently treated with an irrigation and debridement, and un-reamed intramedullary nail. At 4 months followup, despite some signs of healing, the fracture is not fully united. Which of the following is true?
1) Patient should be scheduled for exchange nailing.
2) Use of an un-reamed nail increased this patients risk of infection.
3) Use of an un-reamed nail increased this patient's risk of non-union.
4) Patient should continue to be observed without intervention.
5) Use of an un-reamed nail decreased this patient's risk of infection.
Tibia fractures, open or closed, when treated with an intramedullary nail can take 6 months or longer to achieve clinical and radiographic healing, and should be observed for at least 6 months before secondary intervention is considered.
Open tibia fractures should be managed with debridement and irrigation initially. The choice of definitive fixation between reamed and unreamed nailing remains controversial. Recent randomized controlled studies have examined the outcomes of reamed and unreamed nailing for both closed and open tibia shaft fractures.
Bhandari et al. present a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. Surgeons participating in the study were mandated to delay intervention for delayed union/nonunion until 6 months after the initial procedure. The authors found that many tibia fractures in both the reamed and unreamed nailing groups progressed to union without secondary intervention with this 6 month delay.
Finkemeier et al. present a prospective randomized trial of tibia fractures treated with reamed or un-reamed intramedullary nails. For closed fractures they found a higher rate of union at 4 months in the reamed group, but no difference at 6 or 12 months. There was no difference in union rates for open fractures at any time point. They found no differences in other variables such as infection or compartment syndrome.
Incorrect answers:
Answer 1: This fracture has signs of healing at 4 months, and should continue to be observed until at least 6 months before a secondary operation is considered.
Answers 2 and 5: There is no difference in infection risk between reamed and un-reamed nails for open tibia fractures
Answer 3: There is no difference in rate of eventual union between reamed and un-reamed nails for open tibia fractures.
A 27-year-old male sustains a type I open both bone forearm fracture as seen in Figure A. During irrigation and debridement a 1 cm of cortex is removed leaving a segmental gap. Which of the following adjuvants is recommended to supplement your internal fixation?
1) Bone grafting
2) Tricalcium phosphate
3) Calcium phosphate
4) Calcium sulphate
5) BMP-3
Bone grafting in the primary fixation of fractures is typically limited to those with segmental defects. While the increased surface area of a comminuted fracture may aid in the healing potential, the segmental defect is a limiting factor to fracture healing. Calcium sulphate, tricalcium phosphate, BMP-3, and calcium phosphate are not indicated in this clinical picture. BMP-2,4,6, and 7 all have osteoinductive activity but BMP-3 does not demonstrate osteoinductive activity.
In their retrospective review of 198 fracture, Wright et. al found BG was not indicated for comminuted open fracture, and only recommend BG when there is a segmental bone defect.
Wei et. al also performed a retrospective review of 64 fractures in 49 patients and found BG was not indicated for comminuted open fracture, and only recommend BG when there is a segmental defect.
Finally, Schemitsch and Richards determined that optimal outcome post forearm fracture depends on restoration of the radial bow.
A 30-year-old female falls onto her outstretched arm and sustains the injury shown in Figures A and B. After intra-articular lidocaine injection, her elbow range of motion is 30°-95° extension/flexion, 45° supination, 65° pronation. There is no wrist tenderness and the radius pull test is symmetric to the contralateral forearm. What is the most appropriate treatment?
1) Fragment excision via the extensor carpi ulnaris / anconeus approach
2) Internal fixation with headless compression screws via the brachialis / pronator teres approach
3) Internal fixation with a periarticular plate via the extensor carpi ulnaris /
anconeus approach
4) Radial head arthroplasty via the brachialis / pronator teres approach
5) Sling and early elbow range of motion
This patient has a Mason type III radial head fracture composed of two articular fragments with a mechanical block to motion and should be treated with open reduction internal fixation (ORIF) using a lateral approach to the radial head.
Treatment of radial head fractures depends on fracture anatomy, elbow/forearm motion and ipsilateral forearm injury. Minimally displaced fractures with no mechanical block to motion (Type I; see Illustration C) are most common and are treated with a sling and early motion. Displaced fractures with one fragment (Type II) and block to motion are often managed with ORIF. Fragments less than ~30% of the articular surface may be excised, provided there is no concern for ipsilateral forearm instability. Displaced multi-fragmentary fractures (Type III) are usually managed with radial head arthroplasty, but may be treated with ORIF in young patients with less than three fragments.
Ring et al. performed a retrospective study of 56 patients who underwent radial head ORIF. Patients with more than three articular fragments had significantly poorer patient outcome scores, loss of forearm rotation and required more secondary procedures to ultimately resect the radial head. The authors concluded that ORIF is effective for fractures with less than three articular fragments and that fractures with three or more fragments are better managed with prosthetic replacement.
Ruchelsman et al. reviewed radial head and neck fractures. Choice of treatment is impacted by fragment number, size (percentage of articular disc), comminution and stability, as well as radiocapitellar alignment and block to motion. When feasible, ORIF allows restoration of anatomic congruity and initiation of early motion. Radial head arthroplasty is preferred for radial head fractures with multiple fragments or if stable fixation cannot be ensured.
Figures A and B are the AP and lateral radiographs of the left elbow showing a displaced complete articular radial head fracture with two articular fragments [Ruchelsman et al.]. Illustrations A and B are fluoroscopic images showing subsequent fixation of the fracture with a periarticular plate [Ruchelsman et al.]. Illustration C is the Mason classification of radial head fractures.
Illustration D is an intraoperative photograph showing exposure of the radial head fracture via the Kocher approach (extensor carpi ulnaris / anconeus
interval).
Incorrect Answers:
Answer 1: While the patient has no evidence of ipsilateral distal radioulnar joint or interosseous membrane injury (no wrist tenderness, normal radius pull test), fragment excision is reserved for partial articular fractures involving less than 30% of the articular surface. Complete radial head resection can lead to long-term elbow dysfunction and should be reserved for elderly, low-demand patients.
Answer 2: Using the medial approach to the elbow for an isolated radial head procedure is not appropriate. ORIF can be performed with either headless compression screws or periarticular plates. Use of headless compression screws has been associated with improved postoperative ROM compared to plates.
Answer 4: Using the medial approach to the elbow for an isolated radial head procedure is not appropriate. Radial head arthroplasty should be reserved for older patients and fractures with three or more articular fragments.
Answer 5: Nonoperative treatment is not appropriate for this patient with a displaced fracture and mechanical block to motion.
What nerve is most at risk when applying the external fixator shown in Figure A using a minimally invasive fluoroscopic technique of pin insertion?
1) Ilioinguinal nerve
2) Obturator nerve
3) First branch of the femoral nerve
4) Lateral femoral cutaneous nerve
5) Superior gluteal nerve
Pelvic external fixation with supraacetabular pins through the AIIS can be utilized to stabilize a pelvic fracture. While using this technique, care must be taken not to injure the lateral femoral cutaneous nerve (LFCN). Gardner et al describe the technique for placement of supraacetabular external fixation pins and state that pins in this location are more stable biomechanically compared to other locations in the iliac crest. Grothaus et al performed a cadaveric study to determine the anatomic detail and variation of the LFCN and the distances it traveled from various landmarks.The found the nerve to potentially be at risk as far as 7.3 cm medial to the anterior superior iliac spine along the inguinal ligament and as much as 11.3 cm distal on the sartorius muscle from the anterior superior iliac spine. Riina et al performed a cadaveric study to define the neurovascular structures at risk with the placement of anterior-posterior locking screws in the proximal femur. They found that risks to the neurovascular structures during anterior-posterior locking in the proximal femur are diminished if locking is performed above the level of the lesser trochanter.
A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?
1) Sural nerve injury
2) Tethering of the flexor hallucis longus by fracture fragments
3) Medial plantar nerve neuropathy
4) Weakness of the tibialis posterior
5) Unrecognized foot compartment syndrome
Contracture of the intrinsic flexor muscles of the foot can be the result of unrecognized foot compartment syndrome. Foot compartment syndrome is a known complication of calcaneus fractures.
Myerson reported 3/43 patients in his series below had chronic foot compartment syndrome. There are 9 compartments in the foot: (1) medial, (2) superficial, (3) lateral, (4) adductor, (5-8) four interossei, and (9) calcaneal.
The plantar fascia limits the space available for hematoma and swelling, causing damage to the intrinsic flexors of the foot (particularly the lumbricals and interossei), resulting in clawtoes.
A 25-year-old male sustains a closed elbow dislocation after falling during a soccer game. Two months later, the patient continues to complain of pain and instability. Radiographs and physical exam are concerning for posteromedial instability. Which of the following fracture patterns is most consistent with this diagnosis?
1) Coronoid tip
2) Coronoid anteromedial facet
3) Radial head
4) Olecranon
5) Capitellar impaction injury
of coronoid fractures, they indicate that identification of anteromedial facet injuries is often difficult and that treatment should be instituted promptly to limit persistent instability and subsequent arthritis.
Illustration A shows an AP radiograph of the affected elbow. An event of posteromedial instability is evidenced by the fracture through the anteromedial facet of the coronoid. Illustrations B and C show the AP and lateral radiographs of a patient who developed significant arthrosis after inadequate treatment of varus posteromedial rotatory instability.
Incorrect answers
Answers 1, 3, 5: These injuries may be seen as the sequlae of posterolateral rotatory instability.
Answer 4: Large coronoid fractures are seen in olecranon fracture-dislocations around the elbow.
A 7-year old boy presents to the emergency room following a ATV accident with complaints of left pelvic pain. In the emergency room he is alert and oriented and is hemodynamically stable. On physical exam he is unable to bear weight on his left lower extremity. There is no tenderness to palpation at the posterior pelvis. A radiograph is performed and shown in Figure A and CT examination shows the posterior ring is stable and age-appropriate. What is the most appropriate treatment for this injury pattern?
1) Nonoperative management with weight bearing as tolerated
2) Percutaneous sacroiliac screw
3) Pelvic external fixation
4) Anterior pelvic ring plating
5) Anterior and posterior pelvic ring plating
The clinical presentation is consistent for a mildly displaced parasymphyseal fracture in a pediatric patient with an open triradiate cartilage. Weight bearing as tolerated is the most appropriate treatment.
In skeletally immature pelvic ring fractures, the majority of cases can be treated nonoperatively. Open reduction and internal fixation is required for acetabular fractures with >2 mm of fracture displacement and for any intraarticular or triradiate cartilage fracture displacement >2 mm. External fixation is necessary for pelvic ring displacement of >2 cm to prevent limb-length discrepancies.
Holden et al. emphasize that children with open triradiate cartilage have
different fracture patterns than do children whose triradiate cartilage has closed. They report because of the immaturity of the pelvis, the iliac wing is weaker than the elastic pelvic ligaments, resulting in bone failure before pelvic ring disruption has a chance to occur. For this reason fractures usually involve the pubic rami and iliac wings and rarely require surgical treatment.
Spiguel et al. reviewed 2850 pediatric trauma admissions at their institution and reviewed cases with a pelvic ring fracture. They found that although pelvic fractures are an uncommon injury in pediatric trauma patients, the morbidity associated with these injuries is significant. They report while the majority of pelvic fractures in children are treated nonoperatively, more than one-half of these patients have concomitant injuries requiring operative management.
Figure A shows an inferior rami fracture in a pediatric patient with an open triradiate cartilage.
Incorrect Answers:
Answers 1,3,4,5: These treatment options are not appropriate in a stable pelvic ring fracture in a child with open triradiate cartilage.
A 75-year-old-male presents after being struck by a vehicle while crossing the street. He complains of right leg pain, and physical exam reveals no evidence of an open fracture. Initial radiographs are shown in Figures A and B, and intramedullary nailing of the fracture is planned. What is the proper blocking screw technique to prevent apex anterior and valgus deformity of the fracture?
1) Insertion of blocking screws lateral and posterior to the nail
2) Insertion of blocking screws medial and posterior to the nail
3) Insertion of blocking screws lateral and anterior to the nail
4) Insertion of blocking screws medial and anterior to the nail
5) Insertion of blocking screws medial, lateral, and posterior to the nail
Apex anterior and valgus deformity of the proximal tibia fracture can be prevented by inserting blocking screws lateral and posterior to the nail in the proximal segment.
Blocking screws may be used to prevent deformity when performing intramedullary fixation of proximal tibia fractures. Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to prevent valgus deformity. Stability screws can be placed prior to insertion of the nail to prevent deformity during nail passage, or after nail insertion to prevent postoperative deformity from developing.
Ricci et al. describe the technique and results of using blocking screws and intramedullary nails to treat patients with fractures of the proximal third of the tibial shaft. Post-operatively, all patients in their series had less than 5 degrees
of angular deformity in the planes in which blocking screws were used to control alignment. At 6 months follow-up, 10/11 patients maintained this alignment.
Figures A and B demonstrate a segmental tibial shaft fracture. Illustration A shows an intraoperative fluoroscopic image demonstrating insertion of the blocking screws intraoperatively. Illustrations B and C show post-operative radiographs demonstrating placement of the blocking screws and adequate alignment of the proximal segment.
A 36-year-old man sustains blunt chest trauma, an open right femur fracture, and a closed left tibia fracture following a high-speed MVC. Upon presentation to the emergency room, blood pressure is 80/40, HR 135, and urine output is .4 cc/kg/hr. Fluids and blood products are administered, and the patient is transferred to the ICU for further care. As an alternative to lactate and base deficit measurements, which of the following would best indicate adequate resuscitation has been achieved?
1) Systolic blood pressure > 120
2) Heart rate between 60-100
3) Urine output equals 0.4 cc/kg/hr
4) Gastric intramucosal pH of 7.4
5) Potassium between 3.5-4.5
Of the following variables, only a normal gastric mucosal pH (>7.3) is associated with restoration of tissue oxygenation.
Shock is an abnormality of the circulatory system that results in inadequate organ perfusion and tissue oxygenation. This leads to anaerobic metabolism
with the development of lactic acidosis and oxygen debt. Shock is either classified as compensated or uncompensated. Compensated shock exists when there is evidence of ongoing inadequate tissue perfusion despite the normalization of blood pressure, heart rate, and urine output. Uncompensated shock occurs when there is inadequate tissue perfusion and abnormal blood pressure, heart rate, and urine output. Thus, a patient may have normal vital signs but still be in a state of compensated shock that requires additional resuscitation.
Porter et al. review the optimal end points of resuscitation in trauma patients. They conclude that using traditional end points such as blood pressure, urine output and heart rate, may leave up to 85% of patients in "compensated" shock. They urge the use of lactate, base deficit, and gastric intramucosal pH as appropriate end points of resuscitation.
Roberts et al. discuss various aspects of damage control orthopaedics in the multiply injured trauma patient. Although they do not discuss the end points for resuscitation, they note that they presence of shock is a clinical parameter associated with adverse outcomes in the trauma patient.
Incorrect answers:
Answers 1-3: A patient may have normalized blood pressure, heart rate, and urine output but may still be in a state of compensated shock requiring further resuscitation.
Answer 5: Potassium levels do not assess adequate resuscitation
A 32-year-old man sustains the knee injury seen in Figure A after falling from a ladder. Which of the following options is the most biomechanically stable and appropriate definitive surgical treatment?
1) Spanning knee external fixation
2) Lateral plateau locking plate
3) Posteromedial locking plate
4) Lateral plateau percutaneous lag screws and posteromedial plate
5) Lateral plateau and posteromedial plating
The above clinical scenario is consistent with a bicondylar tibial plateau fracture. Bicondylar tibial plateau fractures are best definitively treated with dual incision technique using separate lateral plateau and posteromedial plates.
Yoo et al perfored a biomechanical study comparing locking and nonlocking single and dual plating constructs in maintaining posteromedial fragment reduction in a bicondylar tibial plateau fractures. They found that the posteromedial fracture fragment tolerated higher loads with a posteromedial conventional plate construct. The superiority of this dual plating construct may be caused by unreliable penetration of the posteromedial fragment by the lateral locking screws alone.
Zeng et al also performed a biomechanical study comparing the biomechanical strength of four different fixation methods for the posteromedial tibial plateau split fracture. The four following constructs: anteroposterior lag-screws, an anteromedial limited contact dynamic compression plate (LC-DCP), a lateral locking plate, or a posterior T-shaped buttress plate were studied. They found that the posterior-based buttress plating technique was the most biomechanically stable fixation method allowing the least amount of fracture subsidence for posteromedial split tibial plateau fractures.
Figure A shows an AP radiograph of a bicondylar tibial plateau. Illustration A shows a post-operative radiograph following the dual-plating technique for bicondylar tibial plateau fractures.
Incorrect answers:
Answer 1: External fixation is not the most appropriate definitive care for bicondylar tibial plateau fractures.
Answers 2-4: Not as biomechanically stable as dual plating technique for bicondylar tibial plateau fractures.
A 35-year-old male sustains a closed tibial shaft fracture after falling from 12 feet. Which of the following measurements would be concerning for an evolving compartment syndrome?
1) Intraoperative anterior compartment measurement of 29, with preoperative diastolic pressure 58
2) Preoperative anterior compartment measurement of 25, with preoperative diastolic pressure of 60
3) Intraoperative anterior compartment measurement of 25, with intraoperative diastolic pressure of 54
4) Intraoperative anterior compartment measurement of 28, with intraoperative diastolic pressure of 72
5) Preoperative anterior compartment measurement of 22, with mean arterial pressure of 70
A delta P (diastolic blood pressure minus compartment pressure measurement)of
A 44-year-old male is involved in a motorcycle collision and presents with the radiographs shown in Figure A. A CT scan is obtained which shows intra-articular extension of the fracture, and lateral locked plating with intercondylar lag screw fixation is planned. Which of the following is important intra-operatively to ensure that the
intercondylar screws are contained within the bone and are of appropriate length?
1) AP fluoroscopic imaging with the leg in 30 degrees of internal rotation
2) AP fluoroscopic imaging with the leg in 30 degrees of external rotation
3) AP fluoroscopic imaging with the knee in full extension
4) Lateral fluoroscopic imaging with the knee in 30 degrees of internal rotation
5) Lateral fluoroscopic imaging with the knee in 15 degrees of flexion
Figure A illustrates a comminuted distal femur fracture. AP fluoroscopic imaging with the leg in 30 degrees of internal rotation is important to prevent intercondylar screw prominence.
Hardware irritation is a common post-operative complication of distal femoral plate fixation. Two common sites of pain are laterally where the iliotibial band is in contact with the plate, and medially where intercondylar screws may penetrate the cortex if they are of inappropriate length. Iliotibial irritation most commonly presents with activities requiring knee flexion and extension. It is important to remember that the lateral metaphysis of the distal femur is angulated 10 degrees from the sagittal plane, and the medial metaphysis is angulated 25 degrees from the sagittal plane. Therefore, if a straight AP view is obtained, a distal screw can appear to be inside the bone even if it is too long. In order to assess the exact length of the screw, one must obtain an AP view with 30° internal rotation of the lower extremity.
Gwathmey et al discuss distal femoral fractures in their review article. They state that the goal of surgical management is to promote early knee motion while restoring the articular surface, maintaining limb length and alignment,
and preserving the soft-tissue envelope with a durable fixation that allows functional recovery during bone healing. They describe a variety of surgical exposures, techniques, and implants developed to treat these injuries, including intramedullary nailing, screw fixation, and periarticular locked plating, possibly augmented with bone fillers.
Illustration A demonstrates the sagittal plane angulation of the medial and lateral cortex of the distal femur. Illustration B shows a knee in external rotation, with the intercondylar screw appearing to be of appropriate length. Illustration C shows the knee in internal rotation, which indicates that the screw is penetrating the medial cortex.
A 68-year-old male falls onto his outstretched hand and suffers the injury shown in Figures A and B. He undergoes operative treatment of his fracture, and immediate post-op radiographs are shown in Figure C. Two weeks later he presents with significantly increased pain and deformity. He denies any new trauma, and has followed all postoperative activity restrictions. Current radiographs are shown in Figure D and a clinical photograph of the affected wrist is shown in Figure E. Which of the following is the most likely cause for failure of fixation in this patient?
1) Failure to support the lunate facet with fragment specific fixation
2) Use of a non-locking plate
3) Lack of volar tilt restoration
4) Lack of radial styloid column plating
5) Use of only three bicortical screws in the intact radial shaft proximally
The failure of this patient's fixation post-operatively is caused by failure to support the lunate-facet fragment noted on the injury radiographs.
The stability of comminuted fractures of the distal part of the radius with volar fragmentation is determined not only by the reduction of the major fragments but also by the reduction of the small volar lunate fragment. The distal volar lunate fragment is the site of origin of the strong volar radiolunate ligaments which insert onto the lunate, and so displacement of this small piece volarly will allow the lunate and the rest of the carpus to subluxate volarly. The unique anatomy of this fragment may prevent standard fixation devices for distal radial fractures from supporting the entire volar surface effectively, as a standard volar plate cannot capture this small distal piece without risking injury to the flexor tendons. Fragment specific fixation of the volar lunate facet fragment with commercially available small plates, or with a tension-band construct or augmentation with K-wires may be required to reduce and stabilize this fragment.
Harness et al. reported on a cohort of 7 patients with a volar shearing fracture of the distal radius who lost fixation of a volar lunate facet fragment with subsequent carpal displacement after open reduction and internal fixation. Five patients underwent revision surgery with adequate results. The authors concluded that with regards to lunate facet fracture fragments, it is preferable to recognize the complexity of the injury prior to the initial surgical intervention and to plan accordingly to prevent early post-operative failure.
Taylor et al. compared the biomechanical stability of a fixed-angle volar plate versus a fragment specific fixation system in the treatment of an intraarticular, dorsally comminuted distal radius fracture model. They found that both fixed-angle volar plate and fragment-specific fixation systems performed comparably in a simulated early postoperative motion protocol. Fragment-specific fixation had improved stiffness characteristics only with respect to the smaller ulnar-sided fragment.
Figures A and B show a shearing radiocarpal-fracture subluxation with small lunate-facet fracture. Figure C shows an immediate post-operative radiograph. Figure D shows subluxation of the radiocarpal joint caused by failure to support lunate-facet fragment. Figure E shows the clinical appearance of a volarly subluxated wrist.
Incorrect Answers:
Answer 2: The use of a non-locking plate in this situation did not directly lead to the failure of fixation, and applying a similar construct with locking fixation
would not have prevented volar subluxation of the lunate facet fragment. Answer 3: Volar tilt was grossly restored post-operatively.
Answer 4: Radial styloid plating would not have prevented volar subluxation of the lunate facet fragment.
Answer 5: Three bicortical screws in the intact radial shaft proximally is adequate fixation.
Which of the following is most commonly associated with both simple and complex elbow dislocations?
1) radial head fracture
2) radial neck fracture
3) loss of terminal extension
4) repeat dislocation
5) coronoid base fracture
Elbow dislocations are classified as either simple (no associated fracture) or complex (associated fracture). The goal of treatment is a stable joint that tolerates early motion. The initial range of motion is the stable arc found on postreduction examination. Studies have demonstrated a better outcome when simple elbow dislocations are treated non-surgically rather than with surgical repair. Simple elbow dislocations usually have an excellent outcome (return of functional range of motion with normal strength). A loss of terminal extension is the most common sequelae.
Ross et al. reported on 20 patients with simple closed posterior elbow dislocations who were treated with immediate active ROM under close supervision. They found a final arc of motion of -4 to 139 degrees, with final motion reached a mean of 19 days after dislocation. Only 1 patient had recurrent instability.
A 36-year-old female sustains a knee injury after falling from a ladder onto her flexed knee; she cannot do a straight leg raise after a lidocaine injection into her knee. A radiograph is shown in Figure A. Which of the following treatment options has been shown to have the best outcomes with this injury?
1) Long leg cast
2) Hinged knee brace use with functional rehabilitation protocol
3) Open treatment with internal fixation or excision with patellar tendon advancement
4) Distal patellar resection and allograft reconstruction
5) Placement of a cerclage wire from patella to proximal tibia
The clinical presentation is consistent with and inferior pole patella fracture. Open reduction and internal fixation or excision with patellar tendon advancement is the most appropriate treatment of this injury pattern.
Whenever possible, salvage of the inferior pole through open reduction internal fixation is favored over simple excision and patellar tendon advancement, as this has been shown to be associated with improved outcomes. This is not always possible, however, and pole resection can be performed if the inferior comminution precludes fixation. Inferior outcomes of the partial distal patellectomy and patellar tendon advancement are (aside from the possible resulting patella baja) probably not directly related to the patellofemoral articulation. On the undersurface, the proximal 75% of the patella is covered with articular cartilage; however, the distal 25% is not, and does not articulate with the femoral trochlea.
Kastelec et al. performed a retrospective review of ORIF v. pole resection followed over 4.6 years postoperatively. There was a significant increase (better) in patellofemoral score with ORIF; significant differences in knee pain,
tolerated activity levels, and ROM were also noted. Patella baja was frequently noted with pole resection and correlated with worse functional outcomes.
Matejcic et al. performed a retrospective review of ORIF v. pole resection followed over 5.3 years postoperatively. Results were excellent/good in 90.1% of the ORIF and only 73.1% of the pole resection patients. In addition, significant differences between the groups were noted with regard to knee pain, swelling, level activity, compression pain, range of motion, muscular atrophy, muscular strength, and final patellofemoral score (all better with ORIF).
Figure A is a lateral knee radiograph showing an inferior pole patella fracture.
Which of the following factors increase the risk of nonunion in midshaft clavicle fractures when treated nonoperatively?
1) Sling immobilization
2) Displacement and comminution
3) Age less than 40 years old
4) Immediate motion exercises
5) Male
Robinson et al have shown that lack of cortical apposition, comminution, female gender, and advancing age are the 4 factors that contribute to nonunion.
The Canadian Orthopaedic Trauma Society in a randomized, prospective study showed that for midshaft fracture in adults with 100% displacement, ORIF results in improved DASH and Constant scores (p = 0.001 and p
A 34-year-old male presents after falling off a roof at his job. He has an obvious deformity of his left lower extremity, and injury radiographs are shown in Figures A and B. He has no other injuries. Which of the following definitive treatment algorithms will most likely lead to the best outcomes in this patient?
1) Closed reduction and percutaneous screw fixation of the femoral neck, followed by reamed antegrade nailing of the femur fracture
2) Reamed antegrade nailing of the femoral shaft fracture, followed by open reduction and percutaneous screw fixation of the femoral neck fracture
3) Reamed retrograde nailing of the femoral shaft fracture, followed by closed
reduction and percutaneous screw fixation of the femoral neck
4) Open reduction and screw fixation of the femoral neck, followed by reamed retrograde nailing of the femoral shaft fracture
5) Open reduction and screw fixation of the femoral neck, followed by plating of the femoral shaft fracture
The clinical presentation is consistent with a femoral shaft fracture with an ipsilateral femoral neck fracture. Of the options presented, the most appropriate treatment is open reduction and lag screw fixation of the femoral neck fracture followed by reamed retrograde nailing of the femoral shaft fracture.
Ipsilateral femoral neck/shaft fractures are an uncommon injury estimated to occur in 2-6% of all femoral shaft fractures. It is generally agreed upon that due to the potentially devastating complications of the femoral neck fracture in young patients, the neck fracture should be treated first and the shaft fracture second. Anatomic reduction of the femoral neck fracture is paramount in obtaining successful healing, and therefore open reduction is recommended in the setting of fracture displacement. Provisional reduction of the femoral neck fracture, followed by antegrade nailing with subsequent addition of definitive fixation of the femoral neck is also acceptable.
Peljovich et al. present a review article on ipsilateral femoral neck and shaft fractures. The treatment algorithm they propose consists of first treating the femoral neck fracture, and then addressing the femoral shaft fracture with retrograde nailing. They also highlight the risk and benefits of each treatment approach.
Watson et al. reviewed 13 patients who had healing complications after undergoing surgical fixation of their ipsilateral femoral neck and shaft fractures. They found that lag screw fixation of the femoral neck fracture and reamed intramedullary nailing for shaft fracture stabilization were associated with the fewest complications. Therefore, this approach was recommended as the treatment of choice.
Figures A and B demonstrate an ipsilateral comminuted femoral shaft fracture, and a displaced femoral neck fracture. Illustrations A-C show an example of a femoral shaft fracture with an ipsilateral femoral neck fracture treated with lag screws of the femoral neck fx and retrograde nailing.
Incorrect Answers:
Answer 1: Open reduction of the femoral neck fracture with anatomic
alignment is preferred to closed reduction in this case.
Answer 2,3: The femoral neck fracture should be addressed first.
Answer 5: Nailing of the femoral shaft fracture would be preferred initially in this case to prevent disruption of the biology and fracture healing around the comminuted segments.
During surgical treatment of the most common variation of distal femoral "Hoffa" fractures, which of the following orientations for screw fixation should be used?
1) Medial to lateral screw placement across lateral femoral condyle
2) Anterior to posterior screw placement across medial femoral condyle
3) Medial to lateral screw placement across medial femoral condle
4) Anterior to posterior screw placement across lateral femoral condyle
5) Anterior to posterior screw placement across intercondylar notch
The most common variation of a Hoffa fracture is a coronal fracture of the lateral femoral condyle. The most appropriate screw placement of the above answer choices in the treatment of the most common Hoffa fracture variant would be anterior to posterior screws across the lateral condyle for fixation.
Hoffa fractures are coronally oriented fractures of the femoral condyles, with most occurring in the lateral condyle. They are commonly associated with high-energy fractures of the distal femur and can often be overlooked during the assessment and treatment of distal femur fractures. Hoffa fractures are best evaluated using CT scans.
Nork et al. studied the association of supracondylar-intercondylar distal femoral fractures and coronal plane fractures. Of 202 supracondylar-intercondylar distal femoral fractures, they found coronal plane fractures were diagnosed in 38%. A coronal fracture of the lateral femoral condyle was involved more frequently than the medial condyle. Eighty-five percent of these coronal fractures involved a single lateral femoral condyle.
Holmes et al. looked at five cases of coronal fractures of the femoral condyle. All cases received open reduction and internal fixation with lag screws through a formal parapatellar approach. They reported good results with all fractures healing within 12 weeks without complications with final range of motion at least 0 degrees to 115 degrees.
Illustration A shows sagittal and axial CT scan cuts showing a Hoffa fracture of the lateral femoral condyle. Illustration B shows multiple anterior to posterior, and posterior to anterior oriented screws for ORIF of the Hoffa fracture.
A 26-year-old right hand dominant male is involved in a motor vehicle collision and sustains the left humerus injury demonstrated in Figure A. The brachial artery is disrupted and requires urgent attention in the operating room. The patient's preoperative nerve evaluation demonstrates that the patient is unable to initiate extensor carpi radialis longus, extensor carpi radialis brevis, extensor pollicis brevis, extensor digitorum, extensor indicis proprius, and extensor pollicis longus motor activity. What is the most likely etiology for this observed neurologic examination?
1) Neurapraxia of the median nerve
2) Axonotmesis of the radial nerve
3) Neurotmesis of the ulnar nerve
4) Neurotmesis of the radial nerve
5) Axonotmesis of the ulnar nerve
The most likely cause of the radial nerve palsy in a high energy open humerus fracture is laceration or complete disruption of the radial nerve (Neurotmesis).
Neurotmesis is complete disruption of nerve and is associated witn no spontaneous recovery without intervention. Axonotmesis constitutes axon disruption, but the surrounding neural connective tissue is intact and nerve regeneration can occur(Wallerian or antegrade degeneration). Neurapraxias occur often by compression and the axon maintains continuity but local demyelination and ischemia occur.
Ring et al. present a Level 4 study of 24 patients that had radial nerve palsy associated with a humerus fracture. All 6 patients with a transected radial nerve had an open humerus fracture also. The results of primary nerve repair in this circumstance found that there was no recovery in any of the patients.
Foster et al. authored a Level 4 review of 14 patients had a radial nerve palsy and an associated open humerus fracture. 64% of the 14 patients had a radial nerve that was either lacerated or interposed between the fracture fragments. They recommend exploration of the radial nerve in the setting of a radial nerve palsy and concomitant open humerus fracture in contrast to observation of a radial nerve palsy in closed humerus fractures.
Figure A demonstrates an open left humerus fracture.
Incorrect Answers:
Answer 1,3,5: The radial nerve provides distal motor activity to the ECRL, ECRB, EPB, EIP, and EPL.
Answer 2: Axonotmesis of the radial nerve is not the most common form of injury associated with closed or open humerus fractures.
Which of the following is true regarding the center of rotation of angulation (CORA) as it refers to tibial diaphyseal angular deformity?
1) It is the point at which the proximal mechanical axis and distal mechanical axis meet
2) It is the point at which the proximal anatomical axis and proximal mechanical axis meet
3) It is always the point on the cortex at the most concave portion of the deformity
4) It is the point at which the distal anatomical axis and distal mechanical axis meet
5) It is always the point on the cortex at the most convex portion of the deformity
The center of rotation of angulation(CORA) in diaphyseal tibial deformity is defined as the intersection of the proximal mechanical(PMA) or anatomical axis(PAA), and the distal mechanical(DMA) or anatomical axis(DAA).
Angular deformity of the femur or tibia involves angulation not only of the bone but also of its axes. When a bone is divided and angulated, the mechanical and anatomic axis of the bone are also divided into proximal and distal segments.
The pairs of proximal and distal axis lines intersect to form an angle. The point at which the proximal and distal axis lines intersect is called the CORA.
The axis line of the proximal bone segment is called the PMA or PAA, and axis line of the distal segment is called the DMA or DAA. In the tibia, because the mechanical and anatomical axes are almost the same, the PMA and PAA lines overlap, as do the DMA and DAA lines.
Illustration A shows the CORA as it relates to the axes of an angulated tibia.
Incorrect Answers:
2-5:These do not describe the CORA or any other specific anatomical points as they related to long bone deformity.
At long term follow-up, a male who sustains multiple traumatic injuries compared with a premenopausal female, who sustained similar polytrauma, is most likely to have which of the following?
1) Higher quality-of-life scores than females
2) Increased rates of complex regional pain syndrome
3) Require more psychiatric counseling and pharmacologic management than females
4) Take more absentee days at work as a result of illness than females
5) Decreased incidence of lower extremity amputation
Ten or more years after severe polytrauma, premenopausal women, compared to men, demonstrate a higher incidence of posttraumatic stress disorder (PTSD) and take more sick leave time from work.
Depression following polytrauma should be screened for by treating orthopaedic surgeons. Depression commonly arises from a protracted injury and can compound the disability by increasing the perception of more physical illness.
Probst et al. present a Level 4 review of over 600 polytrauma patients. They found that quality-of-life was significantly lower in women (Short form-12 psychologic F = 48.6 +/- 10.8 vs. M = 50.8 +/- 9.4; p = 0.02), but the same rate of women (75.3%) and men (75.4%; p = 0.995) felt well rehabilitated.
Holbrook et al. report a Level 4 study of 1,048 polytrauma patients. They found that females had lower quality-of-life scores and were significantly more likely to develop early combined depression.
Incorrect Answers:
Answer 4: Females take more absentee days at work.
Answers 2, 3, 5: There is no data supporting these answer options.
A 29-year-old healthy Caucasian female presents to the emergency department with her boyfriend with a left anterior shoulder dislocation and several facial abrasions after tripping in the shower approximately three hours prior to arrival. She is 5’7’’ and weights 120 lbs (BMI 18.8). The patient notes that she has not had a menstrual period in three months and that she is training for a long-distance triathlon. Physical examination reveals no other obvious injuries. Basic serum laboratory values are unremarkable. A urine pregnancy test is positive. In addition to treating her shoulder dislocation, the orthopaedic surgeon should
1) Perform a skeletal survey to evaluate for other fractures or dislocations
2) Question the patient in private about the specific details of this injury and her sense of safety in the home
3) Refer the patient to a nutritionist given the patient’s BMI of 18.8
4) Obtain additional laboratory studies and admit the patient to the hospital for treatment of anorexia nervosa
5) Obtain advanced imaging of the shoulder to evaluate for underlying pathologic lesions
for her current injury, it is imperative for health care providers to inquire into the safety of the home environment in potential cases of intimate partner violence (IPV).
Risk factors for female victims IPV include being in the 2nd or 3rd decade of life, current pregnancy, having 1 or more prior children, and low socioeconomic status. Reporting requirements for adult abuse are not standardized amongst most states and physicians must understand the importance of identification and documentation in cases of suspected IPV.
Bhandari et al. state that musculoskeletal injuries are the second most common form of IPV (28%) after head and neck injuries (40%).
Musculoskeletal injuries can be variable, including sprains, fractures, dislocations, and foot injuries.
Della Rocca et al. conducted a survey and found orthopaedic surgeons have several misconceptions regarding victims of IPV and further, nearly half of their survey respondents reported identifying a victim of IPV while only 4% reported that they currently screen their injured female patients for IPV.
Zillmer presents a review of the issues surrounding IPV including proper identification, documentation, appropriate questioning and how to involve community services.
Illustration A shows some basic facts regarding IPV during pregnancy as reported by the CDC. Additional information can be found at the following link.
[htt](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)[p](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)[://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)
Incorrect Answers:
Answer 1. There is no indication for a skeletal survey and it would be inappropriate to subject this pregnant patient to additional radiation.
Answer 3. There is no need to refer a patient to a nutritionist for a normal BMI Answer 4. There is no indication for admission or other laboratory studies in this otherwise healthy patient.
Answer 5. There is no need for advanced imaging in the emergency department in the case of an isolated traumatic shoulder dislocation
A 19-year-old military recruit complains of 7 weeks of right heel pain. He notes the pain is worse with jumping and long distance running. He has completed a course of plantar fascia and Achilles tendon stretching with no significant improvement in his symptoms. He denies constitutional symptoms. On examination, his body mass index is 22, he has a normal foot posture and can perform a single leg heel rise without difficulty. There is no pain with palpation of the lateral border of the foot or with external rotation stress to the midfoot. There is tenderness with medial and lateral compression of the hindfoot and there is a negative syndesmosis squeeze test. There is a negative Tinel's sign at the tibial nerve. Axial and lateral radiographs are shown in Figures A and B. What is the most appropriate next step in management?
1) Heel pad cortisone injection
2) Platelet rich plasma injection and 6 weeks of physical therapy
3) Restricted weight bearing and magnetic resonance imaging of the foot
4) Release of the first branch of the lateral plantar nerve
5) ASTYM or Graston physical therapy techniques to the achilles and plantar fascia
Restricted weight bearing and magnetic resonance imaging of the foot is indicated in this military recruit with a positive heel compression test and suspicion for calcaneal stress fracture.
Calcaneal stress fractures occur as a result of repetitive loading and are more common in females with the female athlete triad (anorexia athletica) of disordered eating, amenorrhea, and osteoporosis. On exam tenderness is obtained with medial and lateral compression of the calcaneus.
Sormaala et al. performed a Level 4 review over 8 years of the Finnish military. They found 34 calcaneal stress fractures with 19 occurring in the posterior part of the calcaneus. Only 15% of the patients had the stress fracture visualized on plain radiography. They conclude that MRI is warranted if plain radiography does not show abnormalities in a physically active patient with exercise-induced pain in the ankle or heel. A nuclear medicine bone scan is also appropriate for diagnosis but MRI may give greater detail.
Gehrmann et al. present a Level 5 review of foot stress fractures. They report that with calcaneal stress fractures the fracture lines are oriented vertically or obliquely in the tuberosity of the calcaneus.
Figures A and B show some sclerosis in the central calcaneus with no evidence of overt fracture and an enthesophyte at the Achilles tendon insertion.
Illustration A and B are T2 sagittal and coronal images demonstrating a stress fracture in the superior calcaneal tuberosity with surrounding edema.
Incorrect Answers:
Answer 1: Heel pad cortisone injections are typically avoided due to risk of fat pad atrophy and are not indicated in calcaneal stress fractures.
Answer 2: Platelet rich plasma is not indicated in calcaneal stress fractures. Answer 4: The patient presents with a negative Tinel's at the tibial nerve and presentation is not consistent with first branch of the lateral plantar nerve entrapment.
Answer 5: ASTYM and Graston physical therapies are not indicated for calcaneal stress fractures.
A 35-year old male is involved in a fall from height and present with the isolated injury shown in Figures A and B. The body of the talus is extruded medially through a large linear open wound. Along with irrigation and debridement, what is the most appropriate definitive management of this injury?
1) Reimplantation of the talar body followed by cast immobilization
2) Reduction of talar body, fracture fixation with smooth Steinman pins, and spanning fixator placement
3) Talar body allograft with internal fixation to native talar head
4) Fragment removal, antibiotic spacer placement and external fixation
5) Reduction of native talar body and ORIF of talar neck fracture
The patient is presenting with a displaced talar neck fracture with extrusion of the talar body. Reimplantation of the talar body and ORIF of the talar neck fracture is the most appropriate treatment.
Talar extrusions are rare injuries and are caused by high energy mechanisms. Complete dislocation without a concomitant fracture is extremely rare. The talus is prone to dislocation as there are no muscular attachments. These injuries need to be treated with anatomic reduction and internal fixation to prevent avascular necrosis and post-traumatic arthritis.
Smith et al. investigated the clinical results and functional outcome after reimplantation of the extruded talus. They concluded that salvage and reimplantation of the talus is a relatively safe procedure with only 2 of the 27 patients developing an infection. No association was found between outcome and associated talar fracture.
Van Opstal et al. reported on two cases of talar extrusions following high energy injuries and reviewed the associated literature. Both cases were treated with wound I&D, reduction and external fixation. After 1 year they had pain free ROM with no signs of AVN or arthritis. Review of the literature showed that anterolateral dislocations are more common than anteromedial. Total talar dislocation is thought to be the endpoint of maximum pronation or supination injuries.
Figures A and B show an extruded talar body in the setting of a Hawkins III talar neck fracture. Illustration A shows a clinical photo of an extruded talus.
Incorrect Answers:
Answer 1: Displaced talar neck fractures should not be treated in a cast, especially open fractures
Answer 2: Definitive treatment of this injury is most effectively accomplished with formal ORIF. Steinman pin fixation is not adequate, even in the presence of an external fixator.
Answer 3: There is no data supporting removal of fragment and use of allograft overuse of native talar body
Answer 4: There is no data supporting removal of the fragment. The associated
Most displaced olecranon fractures are treated operatively. Options include tension band constructs, intramedullary screws, plate and screw fixation or fragment excision with triceps advancement. Any construct relying on interfragmentary compression (tension band, intramedullary screws) requires a non-comminuted fracture pattern. Plate fixation is indicated in the setting of comminution, extension past the coronoid, or in the setting of associated instability.
Bailey et al. retrospectively reviewed 25 patients who underwent plate fixation of displaced olecranon fractures. Twenty-two of 25 patients had good or excellent outcomes. Five of 25 patients (20%) of patients required plate removal for symptomatic hardware. The authors concluded that plate fixation
was an effective treatment for displaced olecranon fractures, with good functional outcomes.
Figure A shows a displaced, comminuted olecranon fracture without evidence of propagation past the coronoid.
Incorrect answers:
. All displaced olecranon fractures should be considered for internal fixation. Displacement alone does not direct choice of implant.
Answer 2. Intra-articular extension is an indication for surgery to re-establish articular congruity but does not dictate implant selection.
Answer 3. Extension distal to the coronoid is an indication for plate fixation but there is no evidence of such extension on the radiograph shown
Answer 4. This fracture is comminuted, without a distinct fracture line.
A 35-year-old male was involved in a high speed motorcycle accident. He has a closed head injury, bilateral pulmonary contusions and splenic rupture. His orthopaedic injuries are shown in Figure A. He has a blood pressure of 90/50 mm Hg and a heart rate of 115, despite aggressive resuscitation. An arterial blood gas reveals that his blood lactate is 3.5 and base deficit is -6 mmol/L. Following successful closed reduction of the right hip in the operating room with a percutaneous inserted Schantz pin, what is the next most appropriate treatment for his orthopaedic injuries?
1) Bilateral open reduction and internal fixation
2) Open reduction internal fixation on the right, reamed intramedullary nailing on the left
3) Temporizing external fixation on the right, open reduction and internal fixation on the left
4) Bilateral reamed intramedullary nailing
5) Bilateral temporizing external fixation
This patient presents with features of hemodynamic instability and a high injury severity score. The next most appropriate treatment would be temporizing external fixation bilaterally. This patient meets the criteria for damage control orthopaedics.
Damage control orthopaedics is an approach that contains and stabilizes orthopaedic injuries so that the patient's overall physiology does not undergo further inflammatory insult. As a result, external fixation of femoral shaft fracture and pelvic stabilization is an effective treatment under this strategy. Other indications include vascular injury and severe open fracture.
Pallister et al. reviewed the effects of surgical fracture fixation on the systemic inflammatory response to major trauma. They show that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure. However, early fracture surgery increases the post-traumatic inflammatory response, which
carries a higher complication rate compared to temporary fixation.
Tisherman et al. created clinical guidelines for the endpoints of resuscitation. Level I data found that standard hemodynamic parameters do not adequately quantify the degree of physiologic derangement in trauma patients. The initial base deficit, lactate level, or gastric pH should be used to stratify patients with regard to the need for ongoing fluid resuscitation.
Pape et al. retrospectively reviewed the impact of early total care vs. damage control orthopaedics in the treatment of femoral shaft fractures in polytrauma patients. They found a significantly higher incidence of acute respiratory distress syndrome (ARDS) with intramedullary nailing (15.1%) compared to external fixation (9.1%) when DCO subgroups were compared.
Figure A is a pelvic AP radiograph showing a right hip fracture-dislocation with an ipsilateral femoral shaft fracture. On the left side there is a displaced pertrochanteric hip fracture.
Incorrect Answers:
Answer 1-3: Open reduction internal fixation would not be indicated in damage control orthopaedics.
Answer 4: Bilateral reamed intramedullary nailing would be indicated in early total care of these injuries. As this patient is hemodynamically unstable, with a high injury severity score and bilateral lung contusions, damage control orthopaedics would be indicated.
Which of the following has been shown to be the greatest risk factor for refracture after implant removal from a radial shaft?
1) Removal of locking screws
2) Removal of small fragment plates
3) Removal of metaphyseal implants
4) Removal of implants less than 1 year after insertion
5) Removal of protective splinting from limb earlier than 10 weeks postoperatively
Removal of implants earlier than 1 year after insertion is a risk factor for refracture of the bone after implant removal.
The risk of refracture after hardware removal is multifactorial. Multiple
variables have been studied such as protective splinting for 6 weeks after hardware removal, waiting 12 months or more prior to hardware removal, and the location of the fracture. The variable that seems to correlate most with the risk of refracture is a diaphyseal location of the initial fracture. Large fragment plates (4.5 mm), when removed, are also at higher risk for refracture in the forearm.
Deluca et. al reported on a case series of patients who sustained a refracture of a forearm after implant removal. They noted that radiolucency at the site of the original fracture was seen in most refractured patients when the plate was removed. They also recommend delaying implant removal to two years after insertion to minimize risk.
Rumball et. al reported that the incidence of refracture after forearm implant removal is 6% in their series. They found that early removal, lack of postoperative immobilization, and plate size are the most critical risk factors for refracture.
Illustration A shows a forearm with evidence of refracture after implant removal.
Incorrect Answers:
Answer 1: Removal of locking screws does not increase the risk of refracture. Answer 2: Removal of large fragment plates (4.5mm) are at increased risk of refracture as compared to small fragment plates (3.5mm).
Answer 3: Metaphyseal implant removal has a decreased risk of refracture compared to diaphyseal implant removal.
Answer 5: Protective splinting for 6 weeks is all that is generally recommended for these patients.
A 23-year-old male arrives to the trauma bay after a motorcycle crash caused by a drive-by shooting. The patient is awake and alert and following commands. Vital signs include a blood pressure of 145/90 and a heart rate of 117bpm. Initial lactate is reported as 2.4 mmol/L. The patient has 2 rib fractures on the right with a clear chest radiograph. The patient is neurovascularly intact with a 4cm transverse wound over the medial ankle. Figures A, B and C exhibit his orthopaedic injuries. What is the most appropriate management?
1) Irrigation, debridement and placement external fixator right ankle, external fixation femur and intramedullary fixation tibia
2) Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and tibia
3) Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and external fixation tibia
4) Irrigation, debridement and placement external fixator right ankle, femur and tibia
5) Irrigation, debridement and external fixation right ankle and skeletal traction
The patient is relatively hemodynamically stable. In this case the femur and tibia should be definitively fixed while the open ankle fracture can be irrigated and debrided and placed in a spanning external fixator, temporizing for later definitive fixation.
Aside from an elevated heart rate and mildly elevated lactate (normal
Figure A is an anterior-posterior (AP) radiograph of a 27-year-old male who was a bicyclist struck by a motor vehicle. He was intubated in the field and unresponsive in the trauma slot. Ultrasound of his abdomen is positive for blood and he is brought to the operating room emergently for an exploratory laparotomy. He is found to have ischemic bowel and a grade 4 liver laceration. His lactate is 9.0 mg/dL. Which figure represents the next appropriate step in regard to his pelvic ring injury?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
The radiograph exhibits an elevated left hemipelvis with complete sacroiliac disruption, which can be temporized with placement in skeletal traction.
The patient is unstable, as indicated by an elevated lactate level. The most appropriate next step is temporizing skeletal traction to reduce the left hemipelvis.
Langford et al. review the initial diagnosis, evaluation and resuscitation in the management of pelvic fractures. Reduction of pelvic volume can be achieved with pelvic binders and temporizing external fixation for anterior posterior compression (APC) and/or lateral compression (LC) fracture patterns, while skeletal traction can help do the same in vertical shear patterns.
Matullo et al. review the uses of skeletal traction in orthopaedic trauma, where lower extremity skeletal traction can be an efficient, fast, easy way to help reduce pelvic volume in vertical shear injuries, especially when the patient is unstable and not cleared for definitive fixation.
Figure A exhibits an elevated left hemipelvis indicative of a vertical shear injury and complete SI disruption. Figure B is an example of a pelvic binder. Figure C is a pelvic reconstruction plate. Figure D is a schematic of an anterior pelvic external fixator. Figure E is a schematic drawing of a patient in lower extremity
skeletal traction. Figure F is a radiograph exhibiting S1 and S2 sacroiliac (SI) screws.
Incorrect answers:
Answer 1: A pelvic binder would not be helpful in this scenario and actually may worsen the deformity.
Answer 2: Definitive plate fixation of the anterior pelvis will be needed, but only when the patient is adequately resuscitated.
Answer 3: An anterior external fixator may actually do more harm than good as it may require more time than placing skeletal traction, and also have difficulty controlling the posterior pelvis from the front.
Answer 5: Percutaneous SI screws may be placed later, once the patient is resuscitated and stable.
A 38-year-old man is involved in a motor vehicle collision and suffers the grossly open injury shown in Figure A. He subsequently undergoes irrigation and debridement and placement of an external fixator. In Figure B, if the proximal pin is placed at the red circle as compared to the black circle, the patient is at increased risk for which of the following?
1) Foot drop
2) Injury to the anterior tibial artery
3) Septic arthritis
4) Flexion contracture of the knee
5) Patellar tendon rupture
The patient is at increased risk of septic arthritis when placing the proximal tibial pin too proximal due to penetration of the joint capsule. Pin site flora can track into the joint and lead to a septic knee.
Tibial external fixators can be used to temporize tibial shaft, pilon, and ankle fractures not ready for definitive management due to soft tissue concerns and/or practice of damage control orthopaedics. Intracapsular placement of fixator pins can lead to septic arthritis. The capsular reflection typically extends 14 mm distal to the subchondral line.
DeCoster et al. reported a cadaveric dissection study for safe placement of proximal tibia pins and determined that the capsule inserts 14 mm below the articular surface along the posteromedial and posterolateral surfaces. For fractures requiring extremely proximal pin placement, they recommend
anterior cortex penetration only at least 6 mm distal to articular surface.
Reid et al. investigated safe transtibial pin placement using MRI and cadaveric and volunteer knees. They found that pin placement 14 mm distal to subchondral bone will result in low likelihood of capsular penetration.
Figure A is an AP radiograph showing a segmental middle third tibia/fibula fracture. Figure B is a lateral diagram of the tibia showing potential sites of proximal pin placement.
Incorrect Answers:
Answer 1: Foot drop would occur secondary to common peroneal nerve injury, which is not at risk with very proximal pin placement.
Answer 2: The anterior tibial artery is not at risk with very proximal pin placement.
Answer 4: The knee is free to move and therefore should not develop a flexion contracture secondary to the external fixator.
Answer 5: Patellar tendon rupture is not complication of external fixator pin placement in the tibia.
Figures A and B are radiographs of a 43-year-old, right-hand dominant, male that injured his arm in a motor vehicle accident. What would be an absolute indication for surgical fixation of his injury?
1) Radial nerve palsy
2) Intra-articular extension
3) 2mm fracture distraction, 5 degrees of rotational malignment
4) Ipsilateral proximal both bone forearm fracture
5) Bilateral fracture
This patient has a humeral shaft fracture. An absolute indication for surgery would include a floating elbow, i.e. ipsilateral both bone forearm fracture.
The primary causes of humeral fractures include motor vehicle accidents, falls, or violent injury. Almost all cases are treated non-operatively with functional bracing. The absolute indications for surgical management include: ipsilateral vascular injury, severe soft-tissue injury, open fracture, compartment syndrome, and associated ipsilateral forearm fracture, ie, floating elbow. The relative indications for surgical management include: segmental fracture, intraarticular extension, significant fracture distraction, bilateral humeral fracture, inability to maintain acceptable alignment, and polytrauma.
Klenerman et al. reviewed non-operative treatment of humeral shaft fractures. They showed that acceptable results could be achieved even after 20° of
anterior bowing, 30° of varus angulation, 15° of malrotation, and 3 cm of shortening.
Carroll et al. reviewed the management of humeral shaft fractures. They state the indications for operative fixation to be polytraumatic injuries, open fractures, vascular injury, ipsilateral articular fractures, floating elbow injuries, and fractures that fail nonsurgical management. Surgical techniques include external fixation, open reduction and internal fixation, minimally invasive percutaneous osteosynthesis, and antegrade or retrograde intramedullary nailing
Figure A and B shows a comminuted mid-shaft humeral fracture with intraarticular extension.
Incorrect Answers:
Answer 1,2,3,5: These associated injuries are NOT an absolute indication for surgery. An area of controversy is the occurrence of new-onset radial nerve injuries after closed manipulation. However, the current algorithm does not support early open nerve exploration and fixation.
Which of the following findings is a contraindication in retrograde nailing of a periprosthetic distal femur fracture around a total knee arthroplasty?
1) Posterior-stabilized total knee implant
2) Cruciate retaining total knee implant
3) Spiral fracture pattern
4) Distal femoral replacement
5) Knee flexion contracture of 15 degrees
A distal femoral replacement (TKA) implant will generally preclude placement of a retrograde nail due to the long stem on the femoral component.
Supracondylar femur fractures above a well-fixed TKA component are increasingly common. These fractures are often treated with a lateral locking plate, but can also be treated with a retrograde nail in certain circumstances. An important factor in determining if nailing is a viable option are knowing the TKA implant and it's design. In addition, if the TKA component is known, the maximum size of reamer head and nail can be determined preoperatively from the size of the femoral 'box'.
Schutz et al report on a prospective multicenter study of 112 patients who underwent fixation of a distal femur fracture with the LISS system. They report that 90% of fractures went on to union and they attribute all of the failures to either the high-energy nature of particular fractures or a lack of experience in applying the plate in an appropriate pattern. They also note that primary grafting of these fractures is not necessary.
Illustration A shows a periprosthetic femur fracture treated with a retrograde nail.
Incorrect Answers:
1: A posterior-stabilized implant can be treated with an intramedullary nail in many circumstances but can be technically challenging, depending on the components.
2: A cruciate retaining TKA is not a contraindication to use of a retrograde nail. 3: A spiral pattern periprosthetic supracondylar femur fracture can be treated with a femoral nail.
5: A knee flexion contracture will often provide the flexion necessary for access to the box of the femoral component. A knee extension contracture, however, can preclude access to this box for placement of a nail.
A patient falls and sustains the isolated injury seen in Figures A and B. The surgical plan includes open reduction and internal fixation with a small mini-fragment plate using a direct lateral approach. During the approach, the forearm was placed in a fully pronated position. What would be the correct position of the forearm during plate application?
1) Full pronation
2) 25 degrees pronation
3) Neutral
4) 25 degrees supination
5) Full supination
Using the lateral approach (Kocher or Kaplan), the correct placement of the arm should be in a neutral position so that the plate can be placed on the bare area of the proximal radius.
Displaced radial head fractures with less than 3 fragments can be amendable to open reduction internal fixation. The methods of fixation include buried or headless screws, if placed at the articular surface, or posterolateral plating, if placed in the bare area. The safe zone for plating is located at a 90-110 arc from the radial styloid to Lister's tubercle with the arm in neutral rotation. This position helps to avoid impingement of ulna against the plate with forearm rotation. It should be noted that during the approach, that the forearm should be fully pronated to avoid injury to the posterior interosseous nerve.
Mathew et al. reviewed the concepts of terrible triad injuries of the elbow. Radial head fractures are treated conservatively when there is an isolated minimally displaced (less than 2mm) fracture with no mechanical block to motion. Open reduction internal fixation is used for Mason II or III fractures with
A 38-year-old male is involved in a high speed motor vehicle collision. He has a Glasgow Coma Scale of 13 and receives 2 liters of fluid en route to the emergency department. Upon evaluation in the emergency department, he is found to have a bilateral femoral shaft fractures, a right ankle fracture, and a left both bone forearm fracture. He also has 2 left sided rib fracture and a grade II liver laceration. His heart rate is 130 and blood pressure is 85/50. All of the following
would be indications to practice damage control orthopaedics in this patient except:
1) Bilateral femur fractures
2) Rib fractures
3) Lactate of 5.2
4) Urine output of 20 cc/hr
5) Heart rate and blood pressure
Rib fractures without evidence of further thoracic trauma would not be an indication to practice damage control orthopaedics. This patient is underresuscitated based on his lactate level, urine output, and vital signs and definitive management should be delayed.
Damage control orthopaedics is the practice of delaying definitive management of fractures and utilizing temporary stabilization (such as an external fixator) until a patient has recovered from the initial physiologic insult of trauma.
Patients are at increased risk for perioperative complications such as ARDS and multi-system organ failure during the acute period after polytrauma. In addition to underresuscitation, other indications to practice damage control orthopaedics include: injury severity score>40 (or >20 with thoracic trauma), bilateral femoral fractures, hypothermia below 35 degrees Celsius, and pulmonary contusions.
Pape et al. (2007) studied the incidence of acute lung injuries in polytrauma patients undergoing either intramedullary nailing or external fixation and later definitive fixation of femoral shaft fractures. They found that patients undergoing immediate intramedullary nailing were nearly 6.7 times more likely to have acute lung injury
The Canadian Orthopedic Trauma Society studied the effect of reamed versus unreamed femoral nailing on incidence of ARDS for femoral shaft fractures in trauma patients using a randomized controlled study. They found no difference between the groups.
Pape et al. also examined the pathophysiological cascades that accompany soft tissue injuries of the extremities, abdomen, and pelvis and recommend a more comprehensive for evaluation of patients with these injuries.
Incorrect Answers:
Answer 1: Bilateral femur fractures are an indication to practice damage control orthopaedics and delay definitive fixation
Answers 3,4,5: All of these answers suggest that the patient is underresuscitated. Definitive fixation should be delayed
The anterior intrapelvic (modified Stoppa) approach is most appropriate for which of the following fractures?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The anterior intrapelvic (AIP) or modified Stoppa approach provides access to the quadrilateral plate, which is a common location for fracture displacement in associated both column acetabulum fractures as seen in Figure D.
Compared to the traditional ilioinguinal approach, the modified Stoppa with a lateral window can offer comparable access to the quadrilateral plate, which can allow for its use in associated both column fracture patterns.
de Peretti et al. prospectively followed 25 patients with both column fractures
treated via an iliofemoral approach. Results led the authors to not recommend the extensile approach for both column fractures due to lack of efficiency and high complication rates.
Alonso et al. compared the extensile iliofemoral and triradiate approaches, and both reported acceptable results. However, concerning were the relatively high rates of heterotopic ossification, despite prophylaxis.
Bible al. performed a cadaver study to quantify the amount of access provided by the modified Stoppa approach. This approach provides access to approximately 80% of both the inner pelvis, and the quadrilateral plate, however, comparison to the ilioinguinal approach was not performed.
Shazar et al., in a cohort comparison between the ilioguinal and Stoppa approaches, noted better visualization and potential improve fracture reduction via the Stoppa approach for both column fractures. However, this study was limited in its retrospective and relative observer bias.
Figure A depicts a posterior wall fracture dislocation with concomitant femoral neck fracture. Figure B is an iliac oblique view which depicts a posterior column fracture. Figure C exhibits a posterior column + posterior wall fracture. Figure D depicts acetabular fracture with protrusio. Figure E exhibits a posterior wall fracture.
Incorrect answers:
Answers 1,2,3, and 5: Posterior sided injuries, especially for these injuries, would probably be best approached via the Kocher-Langenback approach. Surgical dislocation with a trochanteric slide may help visualization in answer 1.
Figure A is a radiograph of a 75-year-old woman that fell onto her non-dominant shoulder from a standing height. She was treated nonoperatively for 9 months but continues to complain of pain when she elevates her arm. In patients with this type of fracture pattern, what factor has the greatest impact on fracture healing?
1) Hand dominance
2) Angulation of fracture
3) Smoking
4) Early physical therapy
5) Diet
This patient has an impacted varus proximal humerus fracture. Smoking has been shown to increase the nonunion risk up to 5.5 times with these fractures.
Impacted varus proximal humerus fractures can be managed effectively with non-operative care. The major factors that influence non-union are age and smoking. Solid bony union can be seen in 93-98% of patients at 1 year, with more than 97% of people returning to pre-injury level of function. The angulation of fracture, hand dominance and physical therapy does not seem to influence bone union or functional outcomes with this fracture pattern.
Court-Brown et al. looked at the outcomes of impacted varus fractures. They determined that the age of the patient was the major factor in overall outcome. They showed that the best results occurred in younger patients, but results deteriorate with advancing age. Physical therapy was not found to
impact outcome.
Hanson et al. showed that impacted varus fractures can be successfully managed with non-operative care. They found that overall fracture displacement had a minor impact of fracture healing and functional outcome. The predicted risk of delayed union and nonunion was 7% with patients that smoke. This was 5.5 times greater than non-smokers.
Figure A shows an AP radiograph of a varus angulated proximal humerus fracture. This radiograph shows delayed atrophic union.
Incorrect Answers:
Answers 1,2,4: These factors do not have a significant influence on bone healing.
Answer 5: Diet has shown to improve bone healing but this does not have the greatest impact.
A 26-year-old male epileptic patients presents with right shoulder pain and deformity after a grand mal seizure. After medical stabilization, he denies previous injury to his shoulder. Pre-reduction and post-reduction radiographs of the shoulder are shown in Figures A-C, respectively; physical examination reveals a normal upper extremity neurovascular examination. After shoulder immobilization, what would be the next most appropriate step in management of this patient?
1) Abduction brace for three weeks, followed by therapy
2) Right shoulder MR arthrogram
3) Open reduction and internal fixation
4) Hemiarthroplasty
5) Early range of motion
This patient has presented with a fracture dislocation of the right shoulder. After urgent closed reduction, this patient requires open reduction internal fixation of the proximal humerus, and greater tuberosity fracture fragment in particular.
Isolated greater tuberosity fractures may be associated with shoulder dislocations. Careful review of imaging is critical to identify fracture lines that may extend into the humeral neck and head. If these extensions go undetected, catastrophic propagating fractures may occur during closed reduction maneuvers. Treatment is usually with open reduction internal fixation (ORIF). Young patients with proximal humerus fractures should be treated more aggressively with ORIF as compared to elderly patients. Another example would be a severely impacted valgus proximal humeral fracture in a young patient.
Erasmo et al. examined of 82 cases of humerus fracture dislocations treated with the lateral locking plates. Overall outcomes were excellent to good based on standard scoring systems. Complications included avascular necrosis (12%), varus positioning of the head (4.8%), impingement syndrome (3.6%), secondary screw perforation (3.6%), non-union (2.4%) and infection (1.2%).
Robinson et al. looked at severely impacted valgus proximal humeral fractures treated with open reduction internal fixation in young patients. Anatomic reduction is required with lateral plating to re-establish the normal head/neck angle. Good to excellent results can be achieved with fixation methods.
Figure A shows an anterior fracture-dislocation of the right shoulder. Figure B and C show post-reduction radiographs with a congruent glenohumeral joint. Displacement of the greater tuberosity (GT) fragment is greater than 5mm.
Incorrect Answers:
Answer 1: The GT fragment is displaced more than 5-10mm which would warrant surgical reduction and stabilization of the fracture.
Answer 2: MR arthrogram may be indicated to rule out an intra-capsular soft-tissue injury. However, this would not be warranted prior to fixation of the fracture.
Answer 4: Hemiarthroplasty would be indicated in some 4-part proximal humerus fractures or elderly patients. Considering this patient's age and valgus impaction of the fracture, ORIF would be most appropriate.
Answer 5: Early range of motion would be warranted AFTER fixation of the fracture.
Pelvic packing can be performed to temporarily treat a hemodynamically unstable patient with a pelvic ring fracture. Which of the following is the preferred location of the skin incision to perform pelvic packing?
1) Right anterior superior iliac spine (ASIS) to mid-symphysis, left lateral window incision
2) Left ASIS to mid-symphysis, right lateral window incision
3) Subumbilical incision
4) ASIS to ASIS bilaterally
5) Pararectus incision
The preferred skin incision location is a subumbilical incision, 6-8cm extending upwards from the pubic symphysis towards the umbilicus; this allows access to all of the appropriate areas for pelvic packing.
Following skin incision, the rectus fascia is then divided in the midline which allows for access to both sides of the bladder for packing deep in the pelvic
brim. On each side, 3 lap pads are placed from sacroiliac joint to the retropubic space, all placed below the level of the pelvic brim.
Hak et al. review the options for emergent treatment in life threatening hemorrhage secondary to pelvic fractures. The authors offer several options for emergent treatment, which includes the use of pelvic binders, the placement of external fixators, pelvic packing and interventional angiography. Goals include reduction of pelvic volume and stopping rapid hemorrhage to save a patient's life. Pelvic packing, properly performed, is done through a subumbilical incision, as described above.
Osborn et al. retrospectively reviewed and compared emergent pelvic packing to angiography in hemorrhagic pelvic fracture clinical scenarios. The authors noted comparable results in mortality with a noted decrease in need for post-procedure transfusions in the pelvic packing group.
Cothren et al. reported their outcomes following an institutional algorithmic change from pelvic ex-fix/angiography to pelvic packing and ex-fix. Since their institutional change, the authors noted a significant decrease in transfusions, need for angiography and mortality.
Incorrect answers:
Answers 1,2: While these approaches may give access to the pelvic brim, each only give access to one side; one needs to circumferentially access and pack the pelvis.
Answer 4: An ASIS to ASIS skin incision is an unnecessary dissection with too many important structures that lie very close to the skin, including the femoral vessels.
Answer 5: A pararectus incision is an alternative approach to access the quadrilateral plate for acetabular fractures and does not play a role in pelvic packing.
A 28-year-old man is brought by ambulance to the emergency department after falling from the roof of his home four hours ago. Upon initial evaluation, he has visible deformities of his bilateral lower extremities and a positive FAST exam. Heart rate is 135, blood pressure 85/58, and urine output is 40 cc over 3 hours. According to ATLS guidelines, what percentage of his blood volume has this patient likely lost?
1/.
1) 30-40%
2) 40-50%
3) >50%
This patient has likely lost 30-40% of his blood volume and is likely in stage III hemorrhagic shock on the basis of his heart rate, blood pressure, and urine output.
Initial assessment of a trauma patient should involve evaluation of airway, breathing and circulation. An average adult has approximately 5 L of circulating blood volume. Class III and IV hemorrhagic shock, approximated by loss of greater than 30% of blood volume, typically requires resuscitation with fluids and blood products. Lactate level (normal 100 and diminished urine output
4, 5: Blood loss of greater than >40% typically leads to heart rate >140, decreased blood pressure and negligible urine output.
Which of the following fracture patterns would be most appropriately treated with open reduction and internal fixation with posteromedial and lateral plates via dual incisions?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The patient in Figure D has a bicondylar tibial plateau fracture with a posteromedial fracture fragment, which is an indication for lateral and posteromedial plating via dual incisions.
Bicondylar tibial plateau fractures are typically treated with open reduction internal fixation. Studies have shown that the posteromedial fragment is common in bicondylar tibial plateau fractures. Standard lateral implants do not gain adequate screw purchase in posteromedial bone. Posteromedial incisions using the interval between the semimembranosus and medial head of the gastrocnemius can be used to gain access to the fragment and provide exposure to place a posteromedial plate.
Barei et al. reviewed 57 OTA C-type bicondylar tibial plateau fractures, and found the presence of a posteromedial fragment in 74% of cases. They suggest
the use of alternate methods of fixation for the posteromedial fragment rather than lateral fixed-angle plates alone.
Higgins et al. reviewed 111 patients with bicondylar tibial plateaus that underwent CT scan evaluation. They found the incidence of a posteromedial fragment in 59% of the patients and on average accounted for 25% of the articular surface.
Barei et al. reviewed 83 patients treated with dual incisions for fixation of bicondylar tibial plateau fractures. They found deep infections in 8.4% of patients. Satisfactory articular reduction was found in 62% of patients, satisfactory coronal alignment in 91% of patients, satisfactory sagittal alignment in 72%, and satisfactory condylar width in 98%.
Figure A shows an AP and lateral radiograph of a split/depressed lateral tibial plateau fracture. Figure B shows an AP and lateral radiograph of a proximal third tibial shaft fracture with a proximal fibula fracture. Figure C shows an AP and lateral radiograph of a medial plateau fracture with articular depression. Figure D shows an AP and lateral radiograph of a bicondylar tibial plateau fracture. Figure E shows an AP and lateral radiograph of a tibial tubercle fracture in a tibia with open physes.
Incorrect Answers:
Answer 1: Schatzker II tibial plateau fractures can be treated with a single lateral plate.
Answer 2: Proximal third tibial shaft fractures can be treated with an intramedullary nail or percutaneous plating
Answer 3: Schatzker IV tibial plateau fractures can be treated with a single medial or posteromedial plate.
Answer 5: Tibial tubercle fractures in children can be treated with anterior to posterior screws.
Figure A shows the radiographs of a 87-year-old patient after a fall from standing. He lives in a nursing home and uses a walker to transfer from bed to chair. His past medical history includes recurrent urinary tract infections, congestive heart failure, angina and diabetes. Which of the following factors is associated with the best postoperative outcome in this patient?
1) Immediate surgical intervention
2) Postoperative epidural analgesia
3) Postoperative antibiotics
4) Pre-operative medical optimization
5) Choosing total hip arthroplasty instead of hemiarthroplasty
Geriatric patient with hip fractures tends to have a number of coexisting medical conditions that impact surgical risk. A successful pre-operative medical evaluation has the greatest impact on surgical outcomes in this patient population.
Patients with complex past medical histories are at great risk of complications with surgery. This helped to drive the formation of the ASA classification system as a way to score patients out of 5 based on their anesthetic and surgical risks. Patients with significant systemic disease (ASA III and IV) have shown to demonstrate poorer outcomes as compared to patients with less severe medical comorbidities (ASA I and II).
Egol et al. looked at factors that impact the outcomes of hip fractures in geriatric patients. They showed that cardiac and pulmonary complications were most frequent complications post-operatively. It was stated that early mobilization and pre-operative evaluations have the greatest impact on outcomes.
Parvizi et al. looked at the thirty-day mortality following hip arthroplasty for acute fracture. They reviewed a database of 7774 consecutive patients that underwent hip arthroplasty for the treatment of an acute fractures. The overall mortality was 2.4%. Risk factors were found to be cemented implants, female patients, elderly patients, and patients with cardiorespiratory comorbidities.
Roberts et al reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. Although pre-operative medial optimization was not mentioned in this review, there is strong evidence to support an interdisciplinary care program for patients with hip fractures.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Answer 1: Most studies have shown an association between operative delay of
more than 24-48 hours and a higher 1-year mortality rate. However, In patients with with more than 3 medical comorbidities, medical optimization has a greater impact on post-operative outcomes than time to surgery.
Answer 2: Post-operative epidural anaesthesia has shown to decrease postoperative delirium but does not affect 30-day mortality.
Answer 3: Postoperative antibiotics have not shown to reduce the 30-day mortality.
Answer 5: Total hip arthroplasty has shown to improved functional outcomes at 1 year compared with hemiarthroplasty. However, there has been no change in mortality.
A 36-year-old male sustains severe injuries as a result of a motor vehicle collision. After 5 days, the patient is stabilized and transferred to your facility for continued management. After obtaining appropriate imaging, including the images shown in Figures A, B and C the patient should be given which of the following mobility restrictions?
1) Touch-down weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
2) Weight bearing as tolerated on the left lower extremity, non-weightbearing on the right lower extremity
3) Non-weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
4) Touch-down weight bearing on the left lower extremity, weight bearing as tolerated on the right lower extremity
5) Weight bearing as tolerated on the left lower extremity, weight bearing as tolerated on the right lower extremity
Figures B and C shows a stable, impacted lateral compression (LC) type I injury, which can be treated with immediate mobilization without restrictions. The right lower extremity has a pilon fracture, which should be treated with non-weight bearing.
LC-I injuries are stable patterns, as they involve an impaction injury to the anterior sacrum, which has some inherent stability. In addition, the posterior sacro-iliac (SI) soft tissue structures remain intact, which provides critical stability during immediate mobilization.
The reference by Tile is a review article on the principles of management of these injuries, and he reviews how the Tile classification system is important to help determine surgical need and where the stabilization is required. For the stable LC-1 type injury, no fixation is required.
Incorrect Answers:
Answer 1: A patient cannot do touch-down weight bearing on one side and non-weightbearing on the other side simultaneously.
Answer 3: The LC-I injury pattern is stable and can undergo immediate weightbearing as tolerated.
Answer 4: The LC-I pattern is stable and would allow immediate weightbearing, and the right pilon fracture would require non-weightbearing. Answer 5: The right pilon fracture would require non-weightbearing at this time.
A 24-year-old male sustains the fracture dislocation shown in Figure A. How is this fracture pattern best classified?
1) Moore I
2) Moore II
3) Schatzker III
4) Schatzker V
5) OTA type 41B3
Figure A shows a Moore Type II fracture. Moore type II fractures consist of fractures involving the entire tibial condyle, where the fracture line begins in the opposite compartment and extends across the tibial eminence.
A number of classification systems are used to describe tibial plateau fractures. The main classification systems that are widely used include Schatzker, AO/OTA, Hohl and Moore. The Moore classification describes high energy fracture-subluxation injuries of the knee. This is thought to have clinical implications as the type of fracture pattern can indicate an associated soft-
tissue injury.
Moore retrospectively reviewed over a 1000 proximal tibia fractures to devise a classification systems based on the characteristic of five types of tibia plateau fracture patterns. He believed this system helped to better understand knee instability and concomitant soft-tissue injury. For example, Moore Type III fractures (rim avulsion) are associated with a high rate of neurovascular injury.
Figure A shows a fracture involving the entire tibial condyle. Illustration A shows a schematic diagram of the Moore classification (I - V). Illustration B shows a table that describes the Moore classification (I - V).
Incorrect Answers:
Answer 1: Moore Type I is a coronal split fracture of the medial tibia plateau which displaces distally. It does not cross over to the contralateral side of the eminence.
Answer 3: Schatzker Type III is a pure lateral plateau depression.
Answer 4: Schatzker Type V is a bicondylar fracture where the metaphysis and diaphysis remain intact.
Answer 5: OTA type 41B3 is a partial articular fracture with a split-depression of the unilateral plateau.
A 19-year-old male football player plants and twists his right lower extremity sustaining a spiral fracture of his distal third tibial shaft. Of the following images, which is most commonly associated with distal third spiral tibial shaft fractures.
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
The patient has a spiral distal tibial shaft fracture. Spiral distal tibial shaft fractures are commonly associated with intraarticular fracture extension, usually in the form of a posterior malleolus fracture.
Spiral distal third tibial shaft fractures need to be evaluated for intraarticular extension prior to operative management. As this can be missed on x-rays, a CT scan of the ankle is recommended to identify this associated injury. This is important when intramedullary fixation is used for definitive management, as nail insertion can displace a previously non displaced intraarticular fracture.
Anteroposterior screw fixation prior to nailing may be useful in these cases.
Boraiah et al. found that in 62 patients with spiral distal tibial fractures, 39% (24 patients) had a posterior malleolus fracture. They recommended CT evaluation of the ankle to prevent missed intraarticular fractures.
Hou et al. found a posterior malleolus fracture in 9.7% (28 out of 288 cases) of patients with tibial shaft fractures. They recommended CT or MRI evaluation of the ankle prior to surgery.
Figure A shows an axial CT scan of a right ankle with a posterior malleolus
fracture. Figure B shows an AP radiograph of a right ankle with a vertical medial malleolus fracture. Figure C shows a coronal CT scan of a right ankle with a Tillaux fracture. Figure D shows a sagittal CT scan of a right ankle with a comminuted talus fracture. Figure E shows a lateral radiograph of a right knee showing a knee dislocation. Illustration A shows an AP radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration B shows a lateral radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration C shows a sagittal CT of a distal third spiral/oblique tibial shaft fracture with a posterior malleolus fracture.
Incorrect Answers:
Answer 2: Vertical medial malleolar fractures are not typically associated with distal third tibial shaft fractures.
Answer 3: Juvenile Tillaux fractures occur typically in patients with open physes. They do not occur in patients with closed physes, and are not associated with tibial shaft fractures.
Answer 4: Spiral/oblique tibial shaft fractures are not associated with talus fractures.
Answer 5: Knee dislocations are considered high energy injuries, and are not associated with tibial shaft fractures.
What would be the most appropriate treatment for this patient at this time?
1) Observation only
2) Referral to physiotherapy
3) MRI spine and hip
4) Total hip arthroplasty
5) Intramedullary femoral nail
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had
been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers
Answer 1: Symptomatic lateral femoral cortical stress fractures, known as "dreaded black lines", should be treated with early stabilization to prevent subtrochanteric fracture.
Answer 2: Referral to physiotherapy would not be indicated.
Answer 3: Symptoms are related to a subtrochanteric stress fracture, which has been identified on radiograph. MRI would not be indicated.
Answer 4: This patient has mild arthritis. Treatment with a long bridging femoral stem may stabilize the fracture, However, the gold standard treatment would be intramedullary nailing.
A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2
weeks. Which of the following would be an indication for surgical management?
1) Age greater than 70 years.
2) Fracture pattern in Figure A
3) Significant medical comorbidities.
4) Fracture pattern in Figure B
5) Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:
Answers 1, 2, 3, and 5 are all factors that would favor non-operative management for a proximal humerus fracture.
A 37-year-old male arrives to the trauma slot following a high-speed motorcycle crash. His Glasgow Coma score is 14 and his only orthopaedic injury is exhibited in Figure A. His current vital signs are a BP of 90/60, HR 120, and a lactate of 2.5 mMol/L. Other findings include a grade 1 splenic laceration and bilateral pulmonary contusions seen on chest radiograph. Which of the following has been suggested as an indication to perform damage control orthopedic care?
1) HR >110
2) Bilateral pulmonary contusions seen on chest radiograph
3) SBP = 90mmHg
4) Unilateral femur fracture
5) Lactate = 2.5 mMol/L
Pulmonary contusion severe enough to be diagnosed on chest radiograph alone is an indicator that the patient may benefit from damage control orthopaedics (DCO).
Despite the patient's overall stable nature, suffering pulmonary injury severe enough to be seen on x-ray alone suggests that temporary stabilization with staged definitive fixation may avoid potential morbidity.
Pape et al. review the evolution and balance of early total care (ETC) and DCO. Summarizing the literature, the authors report several standalone indicators that would justify DCO regardless of stable status. This includes: Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with chest trauma, multiple injuries with severe pelvic/abdominal trauma/ hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs alone, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater.
Figure A exhibits a right femoral shaft fracture. Illustration A exhibits a summarized table stating the criterion used to determine the condition of a polytrauma patient. (Table from Pape et al, PMID: 19726738)
Incorrect answers:
Answer 1: Heart rate alone (even elevated severely) is not an indicator to
implement DCO.
Answer 3: A systolic BP of 90 mmHg is not an indicator to implement DCO. A SBP of 70mmHg or lower may indicate a patient in extremis (along with other parameters) indicating the benefits of DCO.
Answer 4: A unilateral femur fracture alone in a stable patient is not an indicator of DCO; a patient with bilateral femur fractures, however, may benefit from DCO.
Answer 5:A lactate of 2.5 mMol/L, while slightly elevated, does not warrant DCO. A lactate value of greater than 6 alone would indicate the need for DCO.
A 24-year-old patient presents after a fall from the balcony of a third story building in which he landed on his feet. He reports lumbar back pain and numbness in his perineum region. Radiographs of his hips and pelvis are seen in Figure A, while CT images are shown in Figures B and C. How is this fracture pattern best classified?
1) Young-Burgess APC Type II
2) Young-Burgess LC Type I
3) "U" Type Spinopelvic Dissociation
4) Denis Zone-I
5) Denis Zone-II
This patient has a Denis zone-III "U" Type Spinopelvic Dissociation of the sacrum.
The Denis classification system for sacral fractures is based on anatomical fracture zones. Zone-III fractures involve the spinal canal and have a high rate of associated neurologic injury. It is important to recognize bilateral sacral
fractures with a transverse component, as this often causes spinopelvic discontinuity and possible cauda equina. The lack of mechanical continuity between the spine and pelvis will most likely require reduction and fixation for initial stability. There may also be a need for sacral decompression with fixation mechanisms given the onset of neurologic symptoms.
Mehta et al. reviewed sacral fractures. They report that patients with a transverse sacral fracture involving more proximal sacral segments (S1, S2, or S3) tend to have a higher prevalence of bladder dysfunction than do those involving distal sacral segments (S4 or S5).
Schildhauer et al. report the best way to visualize Denis zone-III "U" type fractures is to obtain a lateral view of the sacrum or sagittal reformatted images with a CT scan. Standard pelvic radiographs often miss this injury.
Figure A shows an AP pelvis with suggestion of sacral irregularities. No fracture pattern can be indentified. Figures B and C show CT scan images showing a "U" Type fracture pattern with angulation and translational displacement of the cephalad and caudad parts of the sacrum. Illustration A shows examples of complex sacral Denis zone-III fractures.
Incorrect Answers:
Answer 1: APC Type II fractures do not classify fracture extensions into the sacral canal. The posterior SI ligaments are considered intact. There is usually disruption of sacrospinous and sacrotuberous ligaments.
Answer 2: LC Type I is an oblique or transverse ramus fracture and ipsilateral anterior sacral ala compression fracture.
Answer 4,5: Figures A-C demonstrate a "U" type fracture of the sacrum.
A 55-year-old male presents with the radiographs seen in Figures A and B after falling off his bike. Physical examination reveals an isolated, closed elbow injury. His limb is neurovascularly intact. Which complication would be most likely with surgical fixation of this injury?
1) Ulnar neuropathy
2) Posterior interosseous nerve injury
3) Early loss of fixation
4) Elbow flexion contracture
5) Avascular necrosis
This patient is presenting with a comminuted capitellar and trochlear fracture. If treated with open reduction internal fixation, the most likely post-operative complication would be elbow stiffness or contracture.
An axial compression force transmitted by the radial head to the capitellum with the elbow in a semiflexed position can result in a shear fracture of the anterior portion of the capitellum. AP, lateral, and radiocapitellar radiographs are recommended to identify these injuries. The lateral X-ray may reveal the “double arc” sign, which represents extension of the capitellum fracture into the trochlea. Extension of the fracture into the trochlea has important implications into the surgical approach to these injuries.
Ruchelsman et al. retrospectively reviewed the outcomes of sixteen patients with capitellar fractures treated with open reduction internal fixation. They found the presence of greater flexion contractures at the time of follow-up in elbows with Type-IV capitellar fractures. All fractures healed, and no elbows had instability or weakness with fixation.
Ring et al. retrospectively reviewed the outcomes of twenty one distal humerus articular fractures that were reduced and stabilized with implants buried beneath the articular surface. Ten patients required a second operation: (6) release of an elbow contracture; (2) treatment of ulnar neuropathy; (1) removal of hardware; (1) early loss of fixation.
Figures A and B show AP and lateral radiographs of the elbow with a comminuted fracture of the capitellum and trochlea. Note the “double arc” sign on the lateral view. Illustrations A and B show open reduction internal fixation of the fracture. Note fixation with multiple interfragmentary screws.
Incorrect Answers:
Answers 1,2,3,5: All of these may be complications with this surgery. These complications are not as common as elbow contracture or stiffness.
Figure A shows a radiograph of a 30-year-old male who underwent fixation of a left leg injury just over two years ago. He presents with persistent pain and drainage from the distal wound despite 4 months of oral antibiotics. He has no systemic symptoms. He has a past medical history of Grave's disease and Irritable Bowel Syndrome. What would be the best management at this stage?
1) Chronic suppressive, culture-directed, antibiotic therapy
2) Above knee amputation
3) Endocrine consultation, irrigation and debridement, removal of hardware and negative-pressure wound therapy
4) Irrigation and debridement, removal of hardware, over-reaming medullary canal, external fixation and culture-directed antibiotics
5) Irrigation and debridement, retention of hardware, acute bone grafting and culture-directed antibiotics
This is a case of fracture nonunion in the setting of chronic osteomyelitis and infected hardware. The best treatment option available would be irrigation and debridement, removal of hardware, ring external fixator and culture directed antibiotics.
The management of infected nonunion in the setting of chronic osteomyelitis is technically demanding. The aims of treatment are to eradicate the infection and obtain bone union. Non-surgical options are largely unsuccessful in patients with draining chronic osteomyeltis in the setting of infected hardware and nonunion. Surgical options involve incision and debridement of necrotic tissue followed by reconstruction of bone and possible soft tissue (to provide
healthy viable coverage). The most common techniques are ringed fixator/circular frames, staged intramedullary device with or without external fixator, free tissue transfer, or radical debridement, bone grafting, and fixation.
Motsitsi et al. reviewed the management of infected nonunion of long bones. They suggest that the Ilizarov technique is regarded as a standard treatment in infected nonunion of the tibia. When there is bone defect after debridement, the bone can be shortened or treated with bone transport.
Egol et al look at a series of patients with chronic osteomyelitis. Limb salvage should be attempted in all patients. The presence of a chronic draining sinus requires surgical debridement and culture directed antibiotics. Infected hardware should be removed. A two-stage strategy is the best and well-proven treatment option.
Figure A shows a intramedullary nail in the left tibia. There is a moderate amount of bone loss at the fracture site with mixed sclerotic bone suggestive of osteomyelitis.
Incorrect Answers:
Answer 1: Chronic suppressive therapy would be considered in a patient that is unable to undergo surgical intervention
Answer 2: Amputation is a primary option for patients unable to undergo lengthy or multiple surgical interventions.
Answer 3: After removing the hardware, the fracture non-union will need to be stabilized.
Answer 5: This patients has a chronic infection that requires radical bone debridement and local infection control. The use of acute bone grafting in a single stage procedure in the distal 1/3 tibia (poor blood supply) is less ideal, especially in the setting of infection.
A 32-year-old male sustained the injury seen in Figure A after a motor vehicle accident. Which of the following factors is most predictive of mortality with this type of injury?
1) Fracture classification
2) Number of blood transfusions in the first 24 hours
3) Gender
4) Time to operative fixation
5) Use of pelvic binders
The best predictors of mortality with pelvic ring fractures include older age and hemodynamic shock at presentation. The amount of blood transfused indicates the severity of hemodynamic instability.
Pelvic ring fractures are typically high energy, blunt injuries. The leading cause of mortality with these injuries is hemorrhage and hemodynamic instability.
The most common source of hemorrhage include venous injury (80%), which is usually caused by a shearing injury of posterior thin walled venous plexus and bleeding cancellous bone. Other sources of hemorrhage include arterial injury (10-20%) from the superior gluteal artery (posterior ring injury, anterior posterior compression [APC] pattern), internal pudendal artery (anterior ring injury, lateral compression [LC] pattern) and obturator artery.
Smith et al. found fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased Injury Severity Scores (ISS) scores. Deaths were most commonly from exsanguination (24 hours).
Starr et al. demonstrated that age and shock on presentation were most predictive of mortality after pelvic ring injury.
Figure A shows a APC III pelvic fracture. Illustration A shows a table describing the Young-Burgress classification of pelvic ring fractures.
Incorrect Answers:
Answers 1,3-5: Gender, fracture pattern, time to operative fixation or use of pelvic blinders do not correlate directly with mortality.
Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?
1) Early range of motion
2) Hinged elbow brace for 4 weeks
3) Repair lateral collateral ligament
4) Remove and upsize implant
5) Remove and downsize implant
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intra-operatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by
>or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
Answer 1: Early range of motion is supported after radial head arthroplasty. However, the next most appropriate step in this scenario would be the intraoperative assessment for radiohumeral joint overstuffing.
Answer 2: Hinged braces may be used in the post operative period. However, overstuffing the radiohumeral joint is of first priority.
Answer 3: There is no indication in this question for lateral collateral ligament repair
Answer 4: Removing the implant and upsizing the radial head would be the opposite of what is needed in this scenario.
Aside from improving the intramedullary nail starting point in Figure A, the use of blocking screws could have been used at the time of fixation to prevent this post-operative deformity. What would have been the correct orientation of these screw(s) in the proximal fragment?
1) Medial only
2) Lateral only
3) Anterior and medial
4) Posterior and medial
5) Posterior and lateral
The clinical presentation is consistent with a malunion of a proximal one-third tibia fracture with a valgus and procurvatum deformity. The correct orientation of Poller blocking screws to help prevent this malalignment would be in the posterior and lateral aspects of the metaphyseal fragment.
Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to
prevent valgus deformity. The semiextended position of the knee for nail insertion also helps to eliminate the tendency for the fracture to flex, due to the avoidance of excessive knee flexion during the reduction.
Stedtfeld et al. describes the mechanical model for blocking screws. They state that two or more blocking screws can be placed in each plane (AP and lateral) alongside the nail to create a narrow canal for the nail. This allows for multiple points of fixation and realignment of the bone as the nail is passed.
Lindvall et al looked at a series of 56 extra-articular proximal tibial fractures treated with intramedullary nailing or percutaneous locked plating. Neither nailing or plating these fractures showed a distinct advantage in the overall outcomes. Apex anterior malreduction however was the most prevalent form of malreduction in both groups.
Lang et al. looked at a series of proximal third tibia fracture treated with intramedullary nailing. They reported that posterior tibial comminution will also contribute to apex anterior angulation. They states this occurs when the fracture hinges on the intact cortex anteriorly during nail insertion.
Figure A shows a proximal one third tibia fracture treated with an intramedullary nail. There is malreduction of the fracture with valgus and procurvatum deformity.
Incorrect Answers:
Answer 1: would prevent varus malalignment Answer 2: would prevent valgus malalignment alone
Answer 3: would prevent varus and recurvatum malalignment Answer 4: would prevent varus and procurvatum malalignment
When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
1) A fracture of the radial head requiring ORIF
2) A highly comminuted radial head fracture requiring radial head arthroplasty or resection
3) An MCL injury requiring repair
4) A type I avulsion fracture of the coronoid
5) An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture.
Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:
Answers 1, 2, 3: Radial head fractures, and MCL injuries are not seen in varus/posteromedial mechanisms. They are seen in terrible triad elbow injuries which are due to valgus and posterolateral rotatory forces.
Answer 4: The coronoid fracture seen in these injuries is an anteromedial facet fracture, and not an avulsion fracture of the tip of the coronoid.
A 26-year-old female presented to the emergency department with the injury seen in Figure A after an awkward fall while intoxicated. She undergoes closed reduction and repeat radiographs are seen in Figure B. After a normal physical examination, including ranging the hip from 0-90 degrees, which of the following options would be the next most appropriate step in management?
1) Femoral skeletal traction
2) CT scan
3) Hip spica cast application
4) Observation only
5) Serial neurovascular examinations
This patient has presented with a posterior left hip dislocation. The next most appropriate step would be performing a post-reduction CT scan to assess for joint reduction and congruity, associated fractures, or loose bodies.
Hip dislocations occur most commonly in young patients with high energy trauma. They are usually classified as simple or complex, with complex dislocations being those with associated fractures of the acetabulum or proximal femur. Urgent close reduction should occur within 6 hours from the time of injury. Post reduction CT scans must be performed for all traumatic hip dislocations to look for fractures or impacted areas of the femoral head or acetabulum, as well as incongruent reductions and free intra-articular joint fragments.
Calkins et al. looked at measurements of the posterior acetabulum on CT scans (the Acetabular Fracture Index) after hip dislocations to evaluate for hip stability. Hips were found to be unstable if less than 34% of the remaining posterior acetabulum was present after dislocation. Hips with greater than 55% were stable. In between 34 and 55% were indeterminate.
Moed et al. found that posterior wall fractures involving less than 20% of the posterior wall were considered stable. Fractures involving more than 40%-50% were unstable, leaving a wide range of posterior wall fractures classified as indeterminate.
Figure A shows a left posterior hip dislocation. Figure B shows a reduced left hip with no obvious fracture. Illustration A shows an axial CT scan image of the left hip. There is no acetabular fracture identified.
Incorrect Answers:
Answer 1: Femoral skeletal traction would be considered if there was an associated acetabular fracture or loose body.
Answer 3: Hip spica casts are not used with these injuries.
Answer 4: Observation would be considered after the CT scan is performed. Answer 5: There was no mention of neurovascular injury. This patient has a normal neurovascular examination. There is no fracture or risk of hematoma formation. This would not be necessary.
A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management?
1) MRI angiography of leg
2) Four-compartment fasciotomy
3) Follow-up examination the following day
4) Continued monitoring and serial examinations
5) EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) 30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P
A 10-year-old girl suffers a displaced tibia fracture. Initial numbness over the dorsum of the the foot resolved following an anatomic closed reduction and placement in a long leg cast performed in the emergency room. The cast was placed with the the ankle dorsiflexed just above neutral to prevent equinus contracture and then the cast and padding was adequately bivalved. Overnight, the patient began experiencing recurrent numbness and paresthesias in her exposed toes and a slight increase in her pain at the fracture site. Your next best step would be:
1) Repeat closed reduction under conscious sedation
2) Selective compartment fasciotomies
3) External fixation and compartment monitoring
4) 4-compartment fasciotomies with fracture fixation done emergently
5) Modify the cast to reposition the ankle into slight plantarflexion
Circumferential casting with the ankle dorsiflexed can cause increased intracompartmental pressures in the leg. However, this patient's cast has been adequately bivalved during initial cast placement. Therefore, the next best step is cast modification to allow the ankle to assume an angle between neutral and 30 degrees of plantar flexion and further reducing the compartment pressure.
Tibia fractures are one of many common underlying etiologies for the development of compartment syndrome in the leg. Fracture reduction as well as eliminating circumferential dressings are important early preventative steps to take. Bivalving casts - including splitting the cast padding - is often indicated in fractures of long bones that are treated with initial casting. While casting patients in a plantigrade or dorsiflexed position reduces the risk of equinus contractures and holds the ankle mortise reduced, dorsiflexing the ankle has been shown to increase the intracompartmental pressures throughout the leg compartments.
Weiner et al. placed pressure monitors into the anterior and deep posterior compartments in healthy volunteers to measure the effects of casting on compartment pressures. They found that the intramuscular pressures were lowest with the ankle positioned between plantigrade and a resting plantar flexion position (0-37 degrees), and that bivalving the cast reduced the pressures 33-47%.
Illustration A shows the needle trajectories for compartment pressure monitoring in the leg. This should be performed within 5 cm of the fracture to get accurate peak pressures.
Incorrect Answers:
Answers 1, 3: The stem does not suggest that the reduction was lost, so neither repeating a closed reduction or placement of an external fixator is indicated at this time.
Answers 2, 4: While suspicion should remain elevated for the development of compartment syndrome, simple conservative measures such as cast modification are ideal first steps to avoid onset of compartment syndrome. The clinical vignette given does not portray clinical compartment syndrome requiring emergent fasciotomy. It would be reasonable to maintain a high level of suspicion given the injury, but non-invasive cast modification is a simple, safe and quick first step.
A 35-year-old male horseback rider was bucked into the air and then landed forcefully with his perineum on the saddlehorn of the saddle. At a one year follow-up, the only long term sequela of his injuries is erectile dysfunction. Which radiographic injury seen in Figures A-E is most commonly associated with this complication?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
This patient has sustained a saddle-horn injury to the pelvis. An anterior posterior compression (APC) injury is the most common pelvic injury associated with this mechanism.
Saddle-horn injury to the pelvis occurs when a horseback rider is bucked into the air and then lands forcefully with his or her perineum on the saddlehorn of the saddle. The bony injury to the pelvis usually consists of a diastasis of the pubic symphysis with/without subsequent widening of the sacroiliac joints. The
majority of patients are able to return close to their pre-injury level of employment and activity after these injuries. However, sexual dysfunction is a common complication with this injury. Sexual dysfunction can be due to urethral, vascular, neurologic, and psychogenic injuries.
Collinge et al. looked at a series of male patients with injuries to the perineum after coming into contact with the saddle or saddle horn on a horse. Eighteen of the twenty patients were found to have sexual dysfunction at the time of the latest follow-up. A multi-disciplinary approach to these patients is needed when treating pelvic injuries.
Cannada et al. surveyed 71 women of childbearing age who had a pelvic fracture. She found that half the patients reported physical genitourinary complaints with 38 percent of women noting new onset pain with intercourse. In terms of psychological impact, they showed that 45 percent of patients answered affirmatively to decreased interest in intercourse and decreased orgasm frequency after the injury.
van Nieuwenhoven et al. describe three equestrians who suffered from straddle injuries with symphysis diastasis and rupture of sacroiliac ligaments after falls or kicks from horses. They show that these presumed low-energy injuries can cause extremely severe injuries to the pelvis itself and to the adjacent organs.
Figure A shows a Burgess APC Type II pelvic fracture. Figure B shows left ASIS avulsion fracture. Figure C shows a left hip dislocation. No pelvic fracture is identified. Figure D shows a subacute superior/inferior pubic rami fracture.
Figure E shows a right femoral neck fracture.
Incorrect Answers:
Answers 2,3,4,5: Any pelvic or lower limb fracture can cause a disruption in a patients activities of daily living. This may include sexual dysfunction, for both men and women. The injury pattern that has the greatest potential for sexual dysfunction are APC type pelvic injuries.
A 31-year-old male driver was involved in a high-speed motor vehicle accident. His injuries include a left subdural hematoma (Abbreviated Injury Score [AIS]=4), left segmental femur fracture (AIS=3), ruptured spleen (AIS=4), nasal fracture (AIS=2), fractured left ribs 4 to 7 (AIS=2), and a closed pelvic ring fracture (AIS=3). What is his Injury Severity Score (ISS)?
1/. 18
1) 25
2) 33
3) 41
4) 48
This patients Injury Severity Score (ISS) is 41. In this patient, the highest AIS scores were from the head (AIS=4), abdomen (AIS=4) and pelvis (AIS=3).
Therefore, the calculation for the ISS score was 4^2 + 4^2 + 3^2 = 41.
The ISS score is calculated as the sum of the square values from the highest Abbreviated Injury Score [AIS] scores in the three most severely injured ISS body regions. ISS scores range from 1 to 75. A single score of 6 on any AIS region results in automatic score of 75. ISS scores > 15 are associated with mortality of 10%.
Poole et al. found that the AIS and ISS appropriately reflect the impact of extraskeletal injuries in patients with femur fractures, but they do not adequately reflect the increased morbidity associated with multiple lower extremity fractures.
Balogh et al. aimed to compare the scoring efficacy of the injury severity score (ISS) and the new injury severity score (NISS) in predicting post-injury outcomes. They found that multiple orthopaedic injuries, as used in the NISS system, had a significantly greater impact on reported poor post-injury outcomes. They suggest that NISS should replace the traditional ISS when grading trauma related outcomes.
Illustration A shows a table of the various ways to score injury severity in trauma patients.
Incorrect Answers:
Answers 1,2,3,5: ISS = A^2 + B^2 + C^2, where A, B, C are the AIS scores of the three most severely injured ISS body regions. The only correct answer is ISS=41.
A 60-year-old otherwise healthy female sustains the fracture in Figure A. Immediate surgical treatment would most likely prevent which of the following complications?
1) Malunion.
2) Regional osteopenia.
3) Skin necrosis.
4) Posttraumatic arthritis.
5) Refracture.
The patient has a calcaneal tuberosity fracture. The Achilles tendon is attached to the displaced fragment, which can cause soft tissue compromise and skin necrosis if not treated promptly.
Displaced calcaneal tuberosity and tongue-type calcaneus fractures have a high incidence of wound complications if not treated urgently. Recommended management includes surgical fixation often performed percutaneously. Lag screws are typically directed from the posterior superior tuberosity inferiorly and distal. In cases of skin sloughing and skin necrosis, flaps may be needed.
Gardner et al. reviewed 139 tongue-type calcaneus fractures, and found that 21% had some degree of posterior skin compromise. Additionally, there was a statistically significant increase in posterior skin compromise with delayed presentations.
Hess et al. reviewed 3 cases of calcaneal tuberosity avulsion fractures that let to skin necrosis because of a delay in treatment.
Tornetta reviewed the indications for percutenaous treatment of calcaneus fractures, and found it was successful and most useful in tongue-type calcaneus fractures.
Figure A shows a lateral radiograph of a R ankle showing a calcaneal tuberosity fracture. Illustration A shows an AP radiograph of a R ankle following percutaneous reduction and internal fixation of the calcaneus fracture with two cannulated screws. Illustration B shows a lateral radiograph of a R ankle showing interval reduction and fixation of the calcaneus fracture. Illustration C shows a clinical photograph of posterior skin compromise associated with a calcaneal tuberosity fracture.
Incorrect Answers:
Malunion, regional osteopenia, posttraumatic arthritis, and refracture risk would not be significantly altered with immediate surgical intervention as opposed to operative management within a reasonable time frame.
When elevating the joint surface in the injury pattern seen in Figure A, what material has the highest compressive strength when filling the metaphyseal void?
1) Calcium phosphate
2) Tricalcium phosphate
3) Cancellous autograft
4) Cancellous allograft
5) rhBMP-7
Figure A illustrates a depressed lateral tibial plateau. One of the key components of fixing a depressed articular segment is maintaining the reduction.
Trenholm et al reviewed an experimental study where a split depression (Schatzker II) fracture was created in a cadaveric model. The stiffness of the elevated fragment in cadavers using calcium phosphate cement versus cancellous bone graft as support showed no difference, but calcium phosphate cement was found to have greater compressive strength than cancellous bone alone.
The review article by Hak reviews the composition, advantages, and disadvantages of commerically available bone graft substitutes.
Incorrect answers:
2: Tricalcium phosphate is a bone graft substitute that is osteoconductive, but has less compressive strength.
3-4: Cancellous bone has less compressive strength than calcium phosphate. 5: rhBMP-7 is not used as a bone filling agent in this instance, as it is typically provided on a easily compressible collagen sponge.
A 42-year-old male sustains multiple abdominal injuries along with the fractures shown in Figures A and B. Which of the following factors is most useful to determine the patient's resuscitation and ability to undergo early definitive fixation of these two fractures?
1) Pulse pressure
2) Respiratory rate
3) Urine output
4) Platelet count
5) Base deficit
The base deficit, or lactate level, has been shown to best reflect the resuscitation status and survival after trauma.
Normalization of hemodynamic parameters does not accurately reflect the resuscitation status and a patient can be in compensated shock (occult tissue hypoperfusion) despite normalization of the heart rate and blood pressure. The use of temporizing measures with delayed definitive fracture treatment has been shown to decrease systemic complications in these patients with occult hypoperfusion.
Crowl et al. performed a retrospective study of 127 patients with femoral shaft fractures undergoing intramedullary nailing, assessing for occult hypoperfusion. Patients with occult hypoperfusion preoperatively had a twofold increase in postoperative complications and significant increase in postoperative infections.
Tisherman et al. present a review of hemodynamic parameters and their use in assessment of resuscitation. They report that hyperlactatemia is common among critically ill patients, and lactate levels and their trend may be reliable markers of illness severity and mortality. Therefore, measurement of blood lactate is recommended to stratify patients based on the need for fluid resuscitation and the risks of multiple organ dysfunction syndrome and death. They conclude that lactate is a reliable indicator of sepsis severity and a marker of resuscitation; however, it is an unreliable quantitative marker of tissue hypoxia/hypoperfusion.
Pallister et al. present a review of the effect of early stabilization of long bone fractures. They note that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure, both of which are caused by activation of the systemic inflammatory response. This activation results in tissue recruitment of and injury by circulating polymorphonuclear leukocytes.
Figure A is a radiograph showing a femoral shaft fracture, while Figure B shows an open tibial shaft fracture.
Incorrect Answers:
Answers 1-4: Normalization of these factors does not always predict adequate resuscitation.
Interleukin-6 levels have been shown to be a reliable measure of which of the following?
1) Osteoporosis
2) Severity of injury
3) Sarcomatous tumor burden
4) Bone turnover
5) Hyperparathyroidism
Interleukin-6 (IL-6) is a proinflammatory cytokine that is increased according to the level of injury sustained and acts to activate the host immune system. In addition, new literature exists to indicate its high sensitivity and specificity for detecting infection in total joint arthroplasty.
Overactivation of the immune system and cytokines can lead to systemic inflammatory response syndrome (SIRS), which results in end-organ damage, including small-vessel vascular damage; this would lead to parenchymal cell death from hypoxic insult.
Keel et al. report that immediate and early trauma deaths are determined by brain injuries or significant blood loss, while late mortality is caused by secondary brain injuries and host defense failure. The secondary effects are characterized by local and systemic release of pro-inflammatory cytokines, arachidonic acid metabolites, proteins of the contact phase and coagulation systems, complement factors and acute phase proteins, as well as hormonal mediators.
Pape et al. investigated the effect of surgeries as a "second-hit" phenomenon. They found that surgery on days 2-4 was associated with a greater amount of postoperative organ dysfunction than if the secondary surgery was done on days 5-8. They also found a significant association between IL-6 values above 500pg/dL at the time of surgery and development of multiple organ failure.
Sears et al. review the effect of the inflammatory response to trauma and the development of complications (death, multiple organ failure). They report that IL-6 and the HLA-DR2 molecules currently appear to have the most potential for use in predicting outcomes in trauma patients.
Illustration A is a diagram that shows some of the effects of IL-6 production.
Incorrect Answers:
1,3-5: IL-6 levels are not known to be reliably altered by these factors.
A 31-year-old male sustained a displaced proximal humerus fracture after a motor vehicle accident. Which of the following factors has the lowest association with humeral head ischemia in these injuries?
1) Four-part fracture
2) Head-splitting fracture
3) Neck fracture with a long calcar segment
4) Disrupted medial periosteal hinge
5) AO type C3 fracture
A long calcar fracture segment, also known as the posteromedial metaphyseal head extension, is a good prognostic sign against the development of osteonecrosis in displaced proximal humerus fractures.
The humeral head is directly supplied by the anterior and posterior humeral circumflex arteries. Disruption of these vessels can result in humeral head osteonecrosis. Fracture patterns with long medial metaphyseal segments (greater than 8 mm) have not shown to critically disrupt the vascular supply to the humeral head causing osteonecrosis. Other factors shown to be protective against osteonecrosis after trauma include an intact medial hinge and simple fracture patterns.
Hertel et al. examined the factors predictive of osteonecrosis of the humeral
head after fracture. These include four-part fragments, angular displacement
>45 degrees of the head, displacement of the tuberosities greater than 10 mm, glenohumeral fracture-dislocation, and head-splitting fractures.
In Hertel's second paper and follow up study they noted that the initial post-fracture humeral head ischemia does not predict development of necrosis.
Illustration A shows an example of a long and short calcar fracture segment. Illustration B shows the AO classification of proximal humerus fractures.
Incorrect Answers:
Answers 1,2,4,5: All these factors are predictive of osteonecrosis.
A 50-year-old female has been diagnosed with osteomyelitis of her left tibia. The infection is isolated to the meduallary canal of the bone, and her past medical history is significant for heavy smoking and chronic venous stasis. Based on the clinical staging of osteomyelitis, what would be her Cierney-Mader classification?
1) Stage 2A
2) Stage 1B
3) Stage 1C
4) Stage 3B
5) Stage 4C
The Cierny-Mader classification is a clinical classification based on clinical and anatomic features. This patient's Cierny-Mader classification is Stage 1B.
The Cierney-Mader classification system characterizes osteomyelitis in one of four anatomic stages. Stage 1 is confined to the medullary cavity of the bone. Stage 2 involves only cortical bone. Stage 3 is a localized infection to cortical and medullary bone. However, the bone remains stable. Stage 4 involves the entire thickness of the bone, with loss of bone stability. The Cierny-Mader system also sub-characterizes patients as A, B, or C. The [A} patients have no systemic or local immune compromising factors. The [B] patients have one or more systemic or local compromising factors. The [C] patients are severely immunocompromised and treatment will lead to greater morbidity than the infection.
Mader et al. described the treatment algorithm of osteomyelitis using the Cierny-Mader classification. Treatment involves both antibiotic and surgical debridement. For type 1 infection, thorough intramedullary reaming and unroofing is usually performed.
Illustration A shows a table for the Cierny-Mader classification. Illustration B shows a schematic illustration of the anatomical involvement of osteomyelitis using the Cierny-Mader classification.
Incorrect Answers:
Answer 1: This would be a cortical infection only in a healthy patient. Answer 3: This would be a medullary cavity infection only in a severely compromised patient.
Answer 4: This would be a localized infection to cortical and medullary bone in a patient with one or more systemic or local compromising factors.
Answer 5: This would be a diffuse infection involving the entire bone in a severely compromised patient.
A 68-year-old female sustains a fall to her dominant arm and sustains the fracture seen in Figure A. She undergoes uneventful open reduction internal fixation with a locked plate and screw construct. Which of the following radiographs (Figures B, C, D, E, or F) show the most common complication associated with this treatment modality?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
Figure B shows screw penetration of the articular surface, which is the most common complication following locked plate and screw fixation.
Inadequate fixation, typically in the humeral head, subsequently fails leading to varus deformity and screw penetration. This most commonly occurs in fixation for 3 and 4 part fractures, but can also occur following fixation for 2 part fractures.
Egol et al. retrospectively reviewed 51 patients following locked plating of 3-and 4-part proximal humerus fractures, they found 16% had screw penetration. The authors recommended ensuring appropriate number and length of the screws placed to prevent cut-out.
Brunner et al. reviewed 158 proximal humerus fractures. They found at 1 year follow-up noted 14% screw penetration rate. They recommended close followup to monitor for cut-out.
Figure A shows a 3-part proximal humerus fracture. Figure B exhibits varus cut-out and screw penetration. Figure C exhibits non-union and fixation failure. Figure D exhibits avascular necrosis and complete head collapse. Figure E (arrow) exhibits changes consistent with heterotopic ossification.
Figure F exhibits non-union and fixation failure at the level of the shaft.
Incorrect answers:
Answer choice 2/5 (figure C/F): Non-union and fixation failure can also occur, but at a relatively low rate.
Answer choice 3 (Figure D): Avascular necrosis also occurs, but at a lower rate than screw penetration.
Answer choice 4 (Figure E): Heterotopic ossification (arrow) can occur but is rare.
Figure A shows an acute, isolated and closed, left knee injury in a 40-year-old male struck by a motor vehicle. What would be the most
appropriate surgical fixation for this injury?
1) Definitive external fixation
2) Temporary external fixation then lateral percutaneous screws
3) Lateral nonlocking plate +/- bone graft substitutes
4) Medial and lateral locking plate +/- bone graft substitutes
5) Lateral percutaneous screws with assisted arthroscopy
This patient has sustained a Schatzker 2 (AO/OTA Type B) fracture of the lateral tibial plateau. The most appropriate treatment of this fracture would be fixation with a lateral nonlocking plate +/- bone graft substitute.
Displaced, widened and depressed tibia plateau fractures are an indication for operative intervention. The aim of surgery is to restore anatomic articular congruity, length, alignment and rotation of the proximal tibia. This is best achieved by (1) direct reduction of the articular surface, and (2) fixation of the interfragmentary piece with a plate and screw construct, which provides subarticular support, interfragmentary compression, and prevents shearing of the fracture. In patients with good bone quality, this is best achieved with an undercontoured lateral nonlocking plate in buttress mode.
Karunakar et al. showed that there was no significant difference between split depression tibial plateau fractures (Shatzker II) fixed with either (1) buttress plate with rafting screws versus (2) periarticular plate with built in rafting screw hole options.
Gardner et al. examined 62 consecutive Schatzker type II fractures with radiographs and MRIs preoperatively. They found that joint depression greater than 6mm and widening of greater than 5mm was associated with a lateral meniscal injury over 80% of the time.
Figure A provided a sequence of coronal CT scan images of a left knee. There is a lateral split depression tibial plateau fracture with significant joint
depression, articular impaction and condylar widening.
Incorrect Answers:
Answer 1: Definitive external fixation of tibial plateau fractures may be considered in patients who are unable to tolerate definitive surgery, severe open fractures, infections, or significant bone loss.
Answer 2: Temporary external fixation would be considered in patients with significant soft tissue injury.
Answer 4: Locking plates do not provide buttress effect when used in pure locking mode. In addition, locking plates add significant incremental cost to the procedure. Medial plating would support a bicondylar fracture.
Answer 5: Screws alone are unlikely to be adequately stable in this patient. Although not commonly employed, knee arthroscopy is considered by some surgeons to be a valuable method to assist in obtaining the best articular surface reduction during surgery.
An otherwise healthy young adult male sustains a transverse radial shaft and ulna fracture. He undergoes definitive surgical fixation with two non-locking compression plates (LCPs) as shown in Figure A. What is the principle of this fixation technique on bone healing?
1) Absolute stability with direct healing by callus formation
2) Relative stability with indirect healing by callus formation
3) Absolute stability with direct healing by internal remodeling
4) Relative stability with indirect healing by internal remodeling
5) Absolute stability with endochondral bone formation
Definitive surgical fixation for a simple transverse both bone forearm fracture would include open reduction and internal fixation with absolute stability with direct healing by internal remodelling (i.e., primary bone healing). The radius is fixed with a 7-hole 3.5mm LC-DCP plate in compression mode. The ulna was fixed with a 8-hole 3.5mm LC-DCP neutralization plate with (2) lag screws.
Restoration of the radial bow, length, and alignment in conjunction with primary bone healing would optimize the restoration of pronation/supination in the forearm. Compression plating and anatomic reduction of articular fractures are examples of absolute stability. Casting, bridge plating, external fixation, and intramedullary nailing provide relative stability, with secondary bone healing resulting.
Moed et al. reviewed 56 patients with open diaphyseal forearm fractures treated with immediate internal fixation. The complications included deep infection in 2 patients and non-union in 6. This study indicated immediate stable plate fixation was a beneficial method of treatment for open diaphyseal forearm fractures.
Jones et al. discussed current literature on treating adult diaphyseal forearm fractures with open reduction internal fixation versus intramedullary nailing, and concluded a randomized prospective study is needed. They stated current literature is inconclusive.
Figure A shows a both bone forearm fracture fixed with absolute stability. The radius is fixed with a 7-hole 3.5mm LC-DCP plate in compression mode. The ulna was fixed with a 8-hole 3.5mm LC-DCP neutralization plate with (2) lag screws.
Incorrect Answers:
Answers 1-2, 4-5: Absolute stability is a biological process of osteonal bone remodelling. This is predominantly intramembranous ossification. Enchondral bone formation occurs in non-rigid fracture healing (secondary bone healing).
A 27-year-old man sustains a tibial plateau fracture as pictured in Figure A-D. Which combination of fixation constructs and stability
would optimize his outcome?
1) Intramedullary nailing for a relative stability construct
2) Posteromedial buttress plating for an absolute stability construct
3) Locked lateral plating an absolute stability construct
4) Medial antiglide plating for a relative stability construct
5) Spanning external fixation for an absolute stability construct
Intraarticular tibial plateau fractures require absolute stability constructs to maintain anatomic joint reductions without callus formation. This condylar split fracture is ideally treated with buttress fixation at the apex of the fracture to avoid the high likelihood of shear failure with a laterally placed fixed-angle construct.
Tibial plateau fractures in young adults are high energy injuries, and the condylar split components of the fractures occur due to shear failure. The mechanism of failure - axial loading combined with a varus or valgus moment with the knee extended or flexed - dictates the orientation of the condylar split fracture line(s). There are multiple fracture classification schemes that assist with surgical decision making, particularly with placement of buttress plate fixation to resist shear failure. Articular impaction and joint depression must also be addressed.
Bai et al. performed a biomechanical study on fresh cadavers to simulate residual articular step-offs after fixation. With a >5 mm step-off, contact pressures increased over 200%.
AO guidelines of tibial plateau fracture management are discussed in depth in AO Principles of Fracture Management, and up-to-date principles can be found on the AO surgery reference. Anatomic reduction and absolute stability are important elements of all intraarticular proximal tibia fractures.
Figures A and B are injury films of a tibial plateau fracture with a large posterior split of the medial condyle. Figure C shows an axial CT cut displaying the same fracture. Illustrations A-C show how the injury was treated. Through a posterior incision, an under-contoured anti-glide plate was used to reduce the fracture at the apex. Subsequently, a pre-contoured posteromedial buttress plate was placed to maintain the reduction. The articular reduction was finalized with rafting screws outside of the plating construct to optimize the angle of subchondral support.
Incorrect Answers:
Answers 1, 4: Relative stability is inappropriate for intraarticular fractures that require anatomic reductions
Answer 3: Laterally-based locked plating for a medial condyle fracture creates large moments about the screw-plate interface, and the construct is apt to fail in shear
Answer 5: Spanning external fixation is most commonly used for temporizing tibial plateau fractures when significant soft tissue is present - in the absence of additional fixation for a hybrid construct, it would provide relative stability
Surgical fixation with absolute stability would be most appropriate for which of the following fracture patterns?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Anatomic reduction and fixation with absolute stability is appropriate for articular fractures, such as posterior malleolar ankle fractures with significant joint involvement.
Compression plating and anatomic reduction of periarticular fractures yield absolute stability. Fractures treated with absolute stability achieve primary bone healing. Posterior malleolar ankle fractures comprising greater than 25% of the joint and non-comminuted lateral malleolar ankle fractures are typically treated with internal fixation to achieve absolute stability. Casting, bridge plating, external fixation, and intramedullary nailing provide relative stability, with secondary bone healing resulting. In fractures with significant comminution and in lower extremity diaphyseal long bone fractures, relative stability is employed.
Gardner et al. surveyed members of the Orthopaedic Trauma Association (OTA) and American Orthopaedic Foot and Ankle Society (AOFAS) regarding treatment of posterior malleolus ankle fractures. They found that size influenced decision making, with 97% electing to treat those posterior malleolus fractures that comprised 50% of the joint. The most common used
approach was the posterolateral approach, which utilizes the interval between the flexor hallucis longus and peroneals.
Forsberger et al. reviewed 45 consecutive patients treated with surgical fixation of the posterior malleolus through the posterolateral approach. This approach allowed excellent exposure with few soft tissue complications.
De Vries et al. reviewed 45 patients with ankle fractures that had a posterior malleolar component. Those patients that had the posterior malleolar fragment fixed did not have statistically better functional scores than those who did not have the fragment fixed. They concluded that those patients with fragment sizes less than 25% did not require fixation and had good functional outcomes at 13 year follow-up.
Figure A shows an AP and lateral radiograph of a right comminuted distal third radial shaft fracture. Figure B shows an AP and lateral radiograph of a lateral and posterior malleolar ankle fracture in addition to a deltoid rupture. Figure C shows an AP and lateral radiograph of a comminuted middle third tibial shaft fracture. Figure D shows an AP radiograph of a minimally displaced greater trochanter fracture. Figure E shows an AP and lateral radiograph of a pediatric distal radial metaphyseal fracture. Illustration A shows an AP, mortise, and lateral radiograph of a posterior and lateral malleolus ankle fracture treated with open reduction and internal fixation.
Incorrect answers:
Answer 1: Significant comminuted radial shaft fractures are treated with bridge plating, which would achieve relative stability.
Answer 3: Diaphyseal tibial fractures are treated with intramedullary nailing, which achieves relative stability.
Answer 4: Minimally displaced greater trochanter fractures are treated nonoperatively.
Answer 5: Pediatric distal radius fractures are typically treated with closed reduction and casting, which achieves relative stability.
Figures A and B are radiographs of a 72-year-old male who presented to hospital 3 days after an unwitnessed fall. He presents with pain and the inability to mobilize since the fall. The patient lives independently and has no significant past medical history. Physical examination reveals an alert and oriented patient. This is an isolated injury with no other focal or systemic deficits. What would be the most important investigation to be obtained before taking this patient to the operating room?
1) Pelvic inlet and outlet views
2) CT head
3) Duplex ultrasound of both lower extremities
4) CT hip and pelvis
5) MRI hip and pelvis
The most appropriate investigation to order in this patient would be a duplex ultrasound of both lower extremities.
Immobilized elderly patients with a delay of more than two days from the fracture to presentation at the hospital are at a higher risk of deep-vein thrombosis (DVT). The risk can be higher in patients with factors that predispose to clot formation, such as malignancy. Patients with a delayed presentation to hospital should be investigated for DVT. The most common screening modality is duplex ultrasound of both lower extremities.
Hefley et al. looked at the effect of delayed admission to the hospital on the preoperative prevalence of DVT associated with hip fractures. They found that 6 out of 11 patients with a delay of more than two days between the fracture and admission to the hospital had evidence of thrombosis. They conclude all patients with delayed admission, after a hip fracture, should be evaluated for DVT preoperatively.
Figure A and B are AP and lateral radiographs that show a displaced left subcapital hip fracture.
Incorrect Answers:
Answer 1: There is no indication of pelvic inlet and out views. Generally speaking, pelvic inlet and outlet views assess the pelvic ring and pelvic bone stock, which are normal in this patient.
Answer 2: CT head would be indicated after an unwitnessed fall if the patient admitted to head injury, had neurological symptoms or acute focal/systemic deficits on exam. None of these are present in this patient.
Answer 4 and 5: A CT or MRI of the hip and pelvis are not indicated in a displaced fracture, but may be useful in diagnosing nondisplaced fractures.
A 67-year-old female sustains the injury shown in Figure A after a trip and fall. When discussing the outcomes of surgery with the patient, which of the following statements is true?
1) Post-surgical mortality rates are significantly lower after total hip arthroplasty compared to hemiarthroplasty
2) Internal fixation shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to arthroplasty
3) Bipolar hemiarthroplasty shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to unipolar hemiarthroplasty
4) A delay in surgery greater than 48 hours is acceptable if the patient has multiple medical comorbiditiesm which are not fully optimized
5) Dislocation rates are equivalent between total hip arthroplasty and hemiarthroplasty
Moderate evidence supports that hip fracture surgery within 48 hours of admission is associated with better outcomes. However, patients with significant medical comorbidity should be fully optimized before surgery.
Although several studies have shown a benefit to surgery within 48 hours, no definitive time frame has been elucidated. The majority of literature has shown improved outcomes in regards to pain, complications, and length of stay with early surgery. Patients with significant medical comorbidities have been shown to have the highest mortality rates.
Moran et al. aimed to determine whether a delay in surgery for hip fractures had an affect on postoperative mortality among elderly patients. In an observational study of 2660 patients, they showed that mortality following hip fracture surgery was 9% at 30-days, 19% at 90-days, and 30% at 12-months.
Patients with medical comorbidities had 2.5 times the risk of death within 30-days of surgery. In addition, individuals who had surgery delayed beyond 4 days had increased mortality at 90-days and 12-months.
Papakostidis et al. examined the timing of internal fixation of intracapsular fractures of the neck of femur on the development of late complications, particularly osteonecrosis of femoral head (ONFH) and non-union. They showed no benefit of early surgery on incidence of AVN. However, delay of internal fixation of more than 24 hours showed increased rates of non-union.
Figure A shows a displaced right femoral neck fracture. Incorrect Answers:
Answer 1: Patients treated with hemiarthroplasty or total hip arthroplasty
demonstrated no statistically significant difference in mortality.
Answer 2: Arthroplasty consistently has better outcomes compared to internal fixation for the treatment of unstable/displaced (Garden III and IV) femoral neck fractures in elderly patients.
Answer 3: Outcomes of unipolar and bipolar hemiarthroplasty for unstable femoral neck fractures are similar.
Answer 5: Dislocation rates are higher with total hip arthroplasty compared to hemiarthroplasty.
An 87-year-old female sustains the injury shown in Figure A after a fall from standing. At baseline, she ambulates with a walker in her home and lives with a 24-hour home health aide. She has a past medical history of stroke and mild dementia. Following medical optimization, what is the most appropriate treatment modality?
1) Intramedullary nail
2) Hemiarthroplasty
3) Closed reduction percutaneous pinning
4) Total hip arthroplasty
5) Sliding hip screw
At baseline, with minimal ambulatory status and dependence on a 24-hour home health aide, the best treatment choice is hemiarthroplasty.
Arthroplasty is the gold standard for displaced femoral neck fractures in the elderly. In community ambulators with relative independent lives, total hip arthroplasty (THA) is recommended. For minimal ambulator, hemiarthroplasty is recommended.
van den Bekerom et al. randomized 252 patients over 70-years-old to either THA or hemiarthroplasty for displaced femoral neck fractures. With increased blood loss, operative time and dislocation risk, they did not recommend THA unless there was good preoperative ambulatory status, and/or pre-existing osteoarthritis or rheumatoid arthritis.
Figure A exhibits a displaced femoral neck fracture
Incorrect answers:
Answers 1, 3, 5 are not the treatment standards for displaced femoral neck fractures in the elderly.
Answer 4 is incorrect because the patient is minimally ambulatory at baseline with little independence.
A 20-year-old female arrives to the trauma bay following a motor vehicle accident. She was a restrained driver and has bilateral chest tubes placed in the trauma slot. Initial laboratory values are significant for a hematocrit of 45.5 g/dL and a lactate of 7 mmol/L. Both lower extremities exhibit grossly open wounds. Radiographs are shown in Figure A and B. What is the best initial management of her orthopaedic injuries?
1) Irrigation and debridement of left femur and right tibia with bilateral external fixator placement
2) Irrigation and debridement of left femur and right tibia with left external fixator placement and right tibial intramedullary nail placement
3) Irrigation and debridement of left femur and right tibia with left femoral and right tibial intramedullary nail placement
4) Irrigation and debridement of left femur and right tibia with left femur open reduction and internal fixation and right tibial intramedullary nail placement
5) Irrigation and debridement of left femur and right tibia with bilateral long leg splint placement
Presenting as an unstable patient, damage control orthopaedics (DCO) should be performed by placing bilateral external fixators following irrigation and debridement.
Signs of clinical instability include an elevated lactate level as well as injuries to both lungs, necessitating bilateral chest tubes. Furthermore, while the patient is young and her hematocrit reflects a 'normal' number, more likely is a hypovolemic state due to bilateral open long bone injuries. Resuscitation is required and early total care (ETC) should be avoided.
Pape et al. review the early data regarding DCO and ETC. Identification of patients in extremis, borderline, unstable or stable patients is critical to determining appropriate management. Adequate resuscitation, by tracking lactate, as well as full evaluation of the multiply injured patient is crucial in determining application of DCO versus ETC. DCO is necessary as a temporizing stage to improve mortality in critically injured patients.
Renaldo and Egol revisit the evolution of trauma care where early, acute treatment evolved to ETC, and again to the development and implementation of DCO and staged fixation. Reviewing the initial post-traumatic inflammatory response, the authors review literature that supports the implementation of DCO in the unstable patient, especially the role of the 'second hit' phenomenon and the spike in inflammatory cascade that occurs between days 2-5 following injury.
Figure A is a lateral x-ray of a comminuted, displaced, open distal femur fracture. Figure B is an anteroposterior radiograph of a spiral, oblique, open tibia fracture.
Incorrect Answers:
Answers 2-4: Due to the elevated lactate levels and unstable nature of the patient, DCO should be applied via placement of external fixators. Definitive fixation at this time could worsen the patient's acute condition and subsequent
morbidity and mortality.
Answer 5: This patient, while unstable, is not in extremis, therefore temporary skeletal stabilization should be placed with external fixators.
Figure A is a radiograph of a 31-year-old male cyclist who was struck by a vehicle. Physical examination revealed a 2 cm opening in the skin over the anteromedial leg. He was treated operatively with an unreamed intramedullary nail. What outcome can be expected using this operative modality when compared with reamed intramedullary nailing?
1) Higher rates of nonunion
2) Higher rates of malunion
3) Higher rates of infection
4) Lower rates of infection
5) No difference
The best definitive surgical fixation option for an open fracture of the tibia would be either a reamed or unreamed intrameduallary nail.
Treatment of open tibia fractures require immediate antibiotics and early
irrigation and debridement. Surgical fixation options are vast, but largely based on the severity of injuries both locally or systemically. External fixation devices are mainly used for provisional fixation in polytrauma patients or definitively in proximal or distal metaphyseal fractures. Plating may be used in a staged fashion after a period of external fixation. The most common fixation method is intramedullary nailing. The use of a reamed or unreamed nail technique does not affect union rates, infection rates, or need for additional surgeries in open tibia fractures.
Bhandari et al conducted a multicenter, blinded randomized trial of 1319 adults in whom a tibial shaft fracture was treated with either reamed or unreamed intramedullary nailing. When comparing outcomes in open and closed injuries at twelve months, they found a benefit for reamed intramedullary nailing in patients with closed fractures, but found no difference between approaches in patients with open fractures.
Finkenmeier et al conducted a randomized controlled study of reamed vs. unreamed nails in open and closed tibia fractures (excluding Grades IIIB and IIIC). They found that the use of reamed insertion of IM nails for the treatment of closed tibia fractures lead to an earlier time to union without increased complications. The authors reported no differences in infection rate, compartment syndrome rate, or percent needing additional surgeries to obtain union. More secondary procedures were needed with unreamed nails in closed fractures only.
Figure A shows a mid-shaft tibia fracture. Incorrect Answers:
Answers 1, 2, 3, 4: All prospective studies show no difference in the rates of
non-union, malunion, or infection when using a reamed or unreamed nails to treat open tibia fractures.
A 27-year-old male presented to the trauma bay following a motor vehicle crash and was diagnosed with a comminuted open tibia fracture. He was subsequently treated with an irrigation and debridement, and un-reamed intramedullary nail. At 4 months followup, despite some signs of healing, the fracture is not fully united. Which of the following is true?
1) Patient should be scheduled for exchange nailing.
2) Use of an un-reamed nail increased this patients risk of infection.
3) Use of an un-reamed nail increased this patient's risk of non-union.
4) Patient should continue to be observed without intervention.
5) Use of an un-reamed nail decreased this patient's risk of infection.
Tibia fractures, open or closed, when treated with an intramedullary nail can take 6 months or longer to achieve clinical and radiographic healing, and should be observed for at least 6 months before secondary intervention is considered.
Open tibia fractures should be managed with debridement and irrigation initially. The choice of definitive fixation between reamed and unreamed nailing remains controversial. Recent randomized controlled studies have examined the outcomes of reamed and unreamed nailing for both closed and open tibia shaft fractures.
Bhandari et al. present a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. Surgeons participating in the study were mandated to delay intervention for delayed union/nonunion until 6 months after the initial procedure. The authors found that many tibia fractures in both the reamed and unreamed nailing groups progressed to union without secondary intervention with this 6 month delay.
Finkemeier et al. present a prospective randomized trial of tibia fractures treated with reamed or un-reamed intramedullary nails. For closed fractures they found a higher rate of union at 4 months in the reamed group, but no difference at 6 or 12 months. There was no difference in union rates for open fractures at any time point. They found no differences in other variables such as infection or compartment syndrome.
Incorrect answers:
Answer 1: This fracture has signs of healing at 4 months, and should continue to be observed until at least 6 months before a secondary operation is considered.
Answers 2 and 5: There is no difference in infection risk between reamed and un-reamed nails for open tibia fractures
Answer 3: There is no difference in rate of eventual union between reamed and un-reamed nails for open tibia fractures.
A 27-year-old male sustains a type I open both bone forearm fracture as seen in Figure A. During irrigation and debridement a 1 cm of cortex is removed leaving a segmental gap. Which of the following adjuvants is recommended to supplement your internal fixation?
1) Bone grafting
2) Tricalcium phosphate
3) Calcium phosphate
4) Calcium sulphate
5) BMP-3
Bone grafting in the primary fixation of fractures is typically limited to those with segmental defects. While the increased surface area of a comminuted fracture may aid in the healing potential, the segmental defect is a limiting factor to fracture healing. Calcium sulphate, tricalcium phosphate, BMP-3, and calcium phosphate are not indicated in this clinical picture. BMP-2,4,6, and 7 all have osteoinductive activity but BMP-3 does not demonstrate osteoinductive activity.
In their retrospective review of 198 fracture, Wright et. al found BG was not indicated for comminuted open fracture, and only recommend BG when there is a segmental bone defect.
Wei et. al also performed a retrospective review of 64 fractures in 49 patients and found BG was not indicated for comminuted open fracture, and only recommend BG when there is a segmental defect.
Finally, Schemitsch and Richards determined that optimal outcome post forearm fracture depends on restoration of the radial bow.
A 30-year-old female falls onto her outstretched arm and sustains the injury shown in Figures A and B. After intra-articular lidocaine injection, her elbow range of motion is 30°-95° extension/flexion, 45° supination, 65° pronation. There is no wrist tenderness and the radius pull test is symmetric to the contralateral forearm. What is the most appropriate treatment?
1) Fragment excision via the extensor carpi ulnaris / anconeus approach
2) Internal fixation with headless compression screws via the brachialis / pronator teres approach
3) Internal fixation with a periarticular plate via the extensor carpi ulnaris /
anconeus approach
4) Radial head arthroplasty via the brachialis / pronator teres approach
5) Sling and early elbow range of motion
This patient has a Mason type III radial head fracture composed of two articular fragments with a mechanical block to motion and should be treated with open reduction internal fixation (ORIF) using a lateral approach to the radial head.
Treatment of radial head fractures depends on fracture anatomy, elbow/forearm motion and ipsilateral forearm injury. Minimally displaced fractures with no mechanical block to motion (Type I; see Illustration C) are most common and are treated with a sling and early motion. Displaced fractures with one fragment (Type II) and block to motion are often managed with ORIF. Fragments less than ~30% of the articular surface may be excised, provided there is no concern for ipsilateral forearm instability. Displaced multi-fragmentary fractures (Type III) are usually managed with radial head arthroplasty, but may be treated with ORIF in young patients with less than three fragments.
Ring et al. performed a retrospective study of 56 patients who underwent radial head ORIF. Patients with more than three articular fragments had significantly poorer patient outcome scores, loss of forearm rotation and required more secondary procedures to ultimately resect the radial head. The authors concluded that ORIF is effective for fractures with less than three articular fragments and that fractures with three or more fragments are better managed with prosthetic replacement.
Ruchelsman et al. reviewed radial head and neck fractures. Choice of treatment is impacted by fragment number, size (percentage of articular disc), comminution and stability, as well as radiocapitellar alignment and block to motion. When feasible, ORIF allows restoration of anatomic congruity and initiation of early motion. Radial head arthroplasty is preferred for radial head fractures with multiple fragments or if stable fixation cannot be ensured.
Figures A and B are the AP and lateral radiographs of the left elbow showing a displaced complete articular radial head fracture with two articular fragments [Ruchelsman et al.]. Illustrations A and B are fluoroscopic images showing subsequent fixation of the fracture with a periarticular plate [Ruchelsman et al.]. Illustration C is the Mason classification of radial head fractures.
Illustration D is an intraoperative photograph showing exposure of the radial head fracture via the Kocher approach (extensor carpi ulnaris / anconeus
interval).
Incorrect Answers:
Answer 1: While the patient has no evidence of ipsilateral distal radioulnar joint or interosseous membrane injury (no wrist tenderness, normal radius pull test), fragment excision is reserved for partial articular fractures involving less than 30% of the articular surface. Complete radial head resection can lead to long-term elbow dysfunction and should be reserved for elderly, low-demand patients.
Answer 2: Using the medial approach to the elbow for an isolated radial head procedure is not appropriate. ORIF can be performed with either headless compression screws or periarticular plates. Use of headless compression screws has been associated with improved postoperative ROM compared to plates.
Answer 4: Using the medial approach to the elbow for an isolated radial head procedure is not appropriate. Radial head arthroplasty should be reserved for older patients and fractures with three or more articular fragments.
Answer 5: Nonoperative treatment is not appropriate for this patient with a displaced fracture and mechanical block to motion.
What nerve is most at risk when applying the external fixator shown in Figure A using a minimally invasive fluoroscopic technique of pin insertion?
1) Ilioinguinal nerve
2) Obturator nerve
3) First branch of the femoral nerve
4) Lateral femoral cutaneous nerve
5) Superior gluteal nerve
Pelvic external fixation with supraacetabular pins through the AIIS can be utilized to stabilize a pelvic fracture. While using this technique, care must be taken not to injure the lateral femoral cutaneous nerve (LFCN). Gardner et al describe the technique for placement of supraacetabular external fixation pins and state that pins in this location are more stable biomechanically compared to other locations in the iliac crest. Grothaus et al performed a cadaveric study to determine the anatomic detail and variation of the LFCN and the distances it traveled from various landmarks.The found the nerve to potentially be at risk as far as 7.3 cm medial to the anterior superior iliac spine along the inguinal ligament and as much as 11.3 cm distal on the sartorius muscle from the anterior superior iliac spine. Riina et al performed a cadaveric study to define the neurovascular structures at risk with the placement of anterior-posterior locking screws in the proximal femur. They found that risks to the neurovascular structures during anterior-posterior locking in the proximal femur are diminished if locking is performed above the level of the lesser trochanter.
A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?
1) Sural nerve injury
2) Tethering of the flexor hallucis longus by fracture fragments
3) Medial plantar nerve neuropathy
4) Weakness of the tibialis posterior
5) Unrecognized foot compartment syndrome
Contracture of the intrinsic flexor muscles of the foot can be the result of unrecognized foot compartment syndrome. Foot compartment syndrome is a known complication of calcaneus fractures.
Myerson reported 3/43 patients in his series below had chronic foot compartment syndrome. There are 9 compartments in the foot: (1) medial, (2) superficial, (3) lateral, (4) adductor, (5-8) four interossei, and (9) calcaneal.
The plantar fascia limits the space available for hematoma and swelling, causing damage to the intrinsic flexors of the foot (particularly the lumbricals and interossei), resulting in clawtoes.
A 25-year-old male sustains a closed elbow dislocation after falling during a soccer game. Two months later, the patient continues to complain of pain and instability. Radiographs and physical exam are concerning for posteromedial instability. Which of the following fracture patterns is most consistent with this diagnosis?
1) Coronoid tip
2) Coronoid anteromedial facet
3) Radial head
4) Olecranon
5) Capitellar impaction injury
of coronoid fractures, they indicate that identification of anteromedial facet injuries is often difficult and that treatment should be instituted promptly to limit persistent instability and subsequent arthritis.
Illustration A shows an AP radiograph of the affected elbow. An event of posteromedial instability is evidenced by the fracture through the anteromedial facet of the coronoid. Illustrations B and C show the AP and lateral radiographs of a patient who developed significant arthrosis after inadequate treatment of varus posteromedial rotatory instability.
Incorrect answers
Answers 1, 3, 5: These injuries may be seen as the sequlae of posterolateral rotatory instability.
Answer 4: Large coronoid fractures are seen in olecranon fracture-dislocations around the elbow.
A 7-year old boy presents to the emergency room following a ATV accident with complaints of left pelvic pain. In the emergency room he is alert and oriented and is hemodynamically stable. On physical exam he is unable to bear weight on his left lower extremity. There is no tenderness to palpation at the posterior pelvis. A radiograph is performed and shown in Figure A and CT examination shows the posterior ring is stable and age-appropriate. What is the most appropriate treatment for this injury pattern?
1) Nonoperative management with weight bearing as tolerated
2) Percutaneous sacroiliac screw
3) Pelvic external fixation
4) Anterior pelvic ring plating
5) Anterior and posterior pelvic ring plating
The clinical presentation is consistent for a mildly displaced parasymphyseal fracture in a pediatric patient with an open triradiate cartilage. Weight bearing as tolerated is the most appropriate treatment.
In skeletally immature pelvic ring fractures, the majority of cases can be treated nonoperatively. Open reduction and internal fixation is required for acetabular fractures with >2 mm of fracture displacement and for any intraarticular or triradiate cartilage fracture displacement >2 mm. External fixation is necessary for pelvic ring displacement of >2 cm to prevent limb-length discrepancies.
Holden et al. emphasize that children with open triradiate cartilage have
different fracture patterns than do children whose triradiate cartilage has closed. They report because of the immaturity of the pelvis, the iliac wing is weaker than the elastic pelvic ligaments, resulting in bone failure before pelvic ring disruption has a chance to occur. For this reason fractures usually involve the pubic rami and iliac wings and rarely require surgical treatment.
Spiguel et al. reviewed 2850 pediatric trauma admissions at their institution and reviewed cases with a pelvic ring fracture. They found that although pelvic fractures are an uncommon injury in pediatric trauma patients, the morbidity associated with these injuries is significant. They report while the majority of pelvic fractures in children are treated nonoperatively, more than one-half of these patients have concomitant injuries requiring operative management.
Figure A shows an inferior rami fracture in a pediatric patient with an open triradiate cartilage.
Incorrect Answers:
Answers 1,3,4,5: These treatment options are not appropriate in a stable pelvic ring fracture in a child with open triradiate cartilage.
A 75-year-old-male presents after being struck by a vehicle while crossing the street. He complains of right leg pain, and physical exam reveals no evidence of an open fracture. Initial radiographs are shown in Figures A and B, and intramedullary nailing of the fracture is planned. What is the proper blocking screw technique to prevent apex anterior and valgus deformity of the fracture?
1) Insertion of blocking screws lateral and posterior to the nail
2) Insertion of blocking screws medial and posterior to the nail
3) Insertion of blocking screws lateral and anterior to the nail
4) Insertion of blocking screws medial and anterior to the nail
5) Insertion of blocking screws medial, lateral, and posterior to the nail
Apex anterior and valgus deformity of the proximal tibia fracture can be prevented by inserting blocking screws lateral and posterior to the nail in the proximal segment.
Blocking screws may be used to prevent deformity when performing intramedullary fixation of proximal tibia fractures. Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to prevent valgus deformity. Stability screws can be placed prior to insertion of the nail to prevent deformity during nail passage, or after nail insertion to prevent postoperative deformity from developing.
Ricci et al. describe the technique and results of using blocking screws and intramedullary nails to treat patients with fractures of the proximal third of the tibial shaft. Post-operatively, all patients in their series had less than 5 degrees
of angular deformity in the planes in which blocking screws were used to control alignment. At 6 months follow-up, 10/11 patients maintained this alignment.
Figures A and B demonstrate a segmental tibial shaft fracture. Illustration A shows an intraoperative fluoroscopic image demonstrating insertion of the blocking screws intraoperatively. Illustrations B and C show post-operative radiographs demonstrating placement of the blocking screws and adequate alignment of the proximal segment.
A 36-year-old man sustains blunt chest trauma, an open right femur fracture, and a closed left tibia fracture following a high-speed MVC. Upon presentation to the emergency room, blood pressure is 80/40, HR 135, and urine output is .4 cc/kg/hr. Fluids and blood products are administered, and the patient is transferred to the ICU for further care. As an alternative to lactate and base deficit measurements, which of the following would best indicate adequate resuscitation has been achieved?
1) Systolic blood pressure > 120
2) Heart rate between 60-100
3) Urine output equals 0.4 cc/kg/hr
4) Gastric intramucosal pH of 7.4
5) Potassium between 3.5-4.5
Of the following variables, only a normal gastric mucosal pH (>7.3) is associated with restoration of tissue oxygenation.
Shock is an abnormality of the circulatory system that results in inadequate organ perfusion and tissue oxygenation. This leads to anaerobic metabolism
with the development of lactic acidosis and oxygen debt. Shock is either classified as compensated or uncompensated. Compensated shock exists when there is evidence of ongoing inadequate tissue perfusion despite the normalization of blood pressure, heart rate, and urine output. Uncompensated shock occurs when there is inadequate tissue perfusion and abnormal blood pressure, heart rate, and urine output. Thus, a patient may have normal vital signs but still be in a state of compensated shock that requires additional resuscitation.
Porter et al. review the optimal end points of resuscitation in trauma patients. They conclude that using traditional end points such as blood pressure, urine output and heart rate, may leave up to 85% of patients in "compensated" shock. They urge the use of lactate, base deficit, and gastric intramucosal pH as appropriate end points of resuscitation.
Roberts et al. discuss various aspects of damage control orthopaedics in the multiply injured trauma patient. Although they do not discuss the end points for resuscitation, they note that they presence of shock is a clinical parameter associated with adverse outcomes in the trauma patient.
Incorrect answers:
Answers 1-3: A patient may have normalized blood pressure, heart rate, and urine output but may still be in a state of compensated shock requiring further resuscitation.
Answer 5: Potassium levels do not assess adequate resuscitation
A 32-year-old man sustains the knee injury seen in Figure A after falling from a ladder. Which of the following options is the most biomechanically stable and appropriate definitive surgical treatment?
1) Spanning knee external fixation
2) Lateral plateau locking plate
3) Posteromedial locking plate
4) Lateral plateau percutaneous lag screws and posteromedial plate
5) Lateral plateau and posteromedial plating
The above clinical scenario is consistent with a bicondylar tibial plateau fracture. Bicondylar tibial plateau fractures are best definitively treated with dual incision technique using separate lateral plateau and posteromedial plates.
Yoo et al perfored a biomechanical study comparing locking and nonlocking single and dual plating constructs in maintaining posteromedial fragment reduction in a bicondylar tibial plateau fractures. They found that the posteromedial fracture fragment tolerated higher loads with a posteromedial conventional plate construct. The superiority of this dual plating construct may be caused by unreliable penetration of the posteromedial fragment by the lateral locking screws alone.
Zeng et al also performed a biomechanical study comparing the biomechanical strength of four different fixation methods for the posteromedial tibial plateau split fracture. The four following constructs: anteroposterior lag-screws, an anteromedial limited contact dynamic compression plate (LC-DCP), a lateral locking plate, or a posterior T-shaped buttress plate were studied. They found that the posterior-based buttress plating technique was the most biomechanically stable fixation method allowing the least amount of fracture subsidence for posteromedial split tibial plateau fractures.
Figure A shows an AP radiograph of a bicondylar tibial plateau. Illustration A shows a post-operative radiograph following the dual-plating technique for bicondylar tibial plateau fractures.
Incorrect answers:
Answer 1: External fixation is not the most appropriate definitive care for bicondylar tibial plateau fractures.
Answers 2-4: Not as biomechanically stable as dual plating technique for bicondylar tibial plateau fractures.
A 35-year-old male sustains a closed tibial shaft fracture after falling from 12 feet. Which of the following measurements would be concerning for an evolving compartment syndrome?
1) Intraoperative anterior compartment measurement of 29, with preoperative diastolic pressure 58
2) Preoperative anterior compartment measurement of 25, with preoperative diastolic pressure of 60
3) Intraoperative anterior compartment measurement of 25, with intraoperative diastolic pressure of 54
4) Intraoperative anterior compartment measurement of 28, with intraoperative diastolic pressure of 72
5) Preoperative anterior compartment measurement of 22, with mean arterial pressure of 70
A delta P (diastolic blood pressure minus compartment pressure measurement)of
A 44-year-old male is involved in a motorcycle collision and presents with the radiographs shown in Figure A. A CT scan is obtained which shows intra-articular extension of the fracture, and lateral locked plating with intercondylar lag screw fixation is planned. Which of the following is important intra-operatively to ensure that the
intercondylar screws are contained within the bone and are of appropriate length?
1) AP fluoroscopic imaging with the leg in 30 degrees of internal rotation
2) AP fluoroscopic imaging with the leg in 30 degrees of external rotation
3) AP fluoroscopic imaging with the knee in full extension
4) Lateral fluoroscopic imaging with the knee in 30 degrees of internal rotation
5) Lateral fluoroscopic imaging with the knee in 15 degrees of flexion
Figure A illustrates a comminuted distal femur fracture. AP fluoroscopic imaging with the leg in 30 degrees of internal rotation is important to prevent intercondylar screw prominence.
Hardware irritation is a common post-operative complication of distal femoral plate fixation. Two common sites of pain are laterally where the iliotibial band is in contact with the plate, and medially where intercondylar screws may penetrate the cortex if they are of inappropriate length. Iliotibial irritation most commonly presents with activities requiring knee flexion and extension. It is important to remember that the lateral metaphysis of the distal femur is angulated 10 degrees from the sagittal plane, and the medial metaphysis is angulated 25 degrees from the sagittal plane. Therefore, if a straight AP view is obtained, a distal screw can appear to be inside the bone even if it is too long. In order to assess the exact length of the screw, one must obtain an AP view with 30° internal rotation of the lower extremity.
Gwathmey et al discuss distal femoral fractures in their review article. They state that the goal of surgical management is to promote early knee motion while restoring the articular surface, maintaining limb length and alignment,
and preserving the soft-tissue envelope with a durable fixation that allows functional recovery during bone healing. They describe a variety of surgical exposures, techniques, and implants developed to treat these injuries, including intramedullary nailing, screw fixation, and periarticular locked plating, possibly augmented with bone fillers.
Illustration A demonstrates the sagittal plane angulation of the medial and lateral cortex of the distal femur. Illustration B shows a knee in external rotation, with the intercondylar screw appearing to be of appropriate length. Illustration C shows the knee in internal rotation, which indicates that the screw is penetrating the medial cortex.
A 68-year-old male falls onto his outstretched hand and suffers the injury shown in Figures A and B. He undergoes operative treatment of his fracture, and immediate post-op radiographs are shown in Figure C. Two weeks later he presents with significantly increased pain and deformity. He denies any new trauma, and has followed all postoperative activity restrictions. Current radiographs are shown in Figure D and a clinical photograph of the affected wrist is shown in Figure E. Which of the following is the most likely cause for failure of fixation in this patient?
1) Failure to support the lunate facet with fragment specific fixation
2) Use of a non-locking plate
3) Lack of volar tilt restoration
4) Lack of radial styloid column plating
5) Use of only three bicortical screws in the intact radial shaft proximally
The failure of this patient's fixation post-operatively is caused by failure to support the lunate-facet fragment noted on the injury radiographs.
The stability of comminuted fractures of the distal part of the radius with volar fragmentation is determined not only by the reduction of the major fragments but also by the reduction of the small volar lunate fragment. The distal volar lunate fragment is the site of origin of the strong volar radiolunate ligaments which insert onto the lunate, and so displacement of this small piece volarly will allow the lunate and the rest of the carpus to subluxate volarly. The unique anatomy of this fragment may prevent standard fixation devices for distal radial fractures from supporting the entire volar surface effectively, as a standard volar plate cannot capture this small distal piece without risking injury to the flexor tendons. Fragment specific fixation of the volar lunate facet fragment with commercially available small plates, or with a tension-band construct or augmentation with K-wires may be required to reduce and stabilize this fragment.
Harness et al. reported on a cohort of 7 patients with a volar shearing fracture of the distal radius who lost fixation of a volar lunate facet fragment with subsequent carpal displacement after open reduction and internal fixation. Five patients underwent revision surgery with adequate results. The authors concluded that with regards to lunate facet fracture fragments, it is preferable to recognize the complexity of the injury prior to the initial surgical intervention and to plan accordingly to prevent early post-operative failure.
Taylor et al. compared the biomechanical stability of a fixed-angle volar plate versus a fragment specific fixation system in the treatment of an intraarticular, dorsally comminuted distal radius fracture model. They found that both fixed-angle volar plate and fragment-specific fixation systems performed comparably in a simulated early postoperative motion protocol. Fragment-specific fixation had improved stiffness characteristics only with respect to the smaller ulnar-sided fragment.
Figures A and B show a shearing radiocarpal-fracture subluxation with small lunate-facet fracture. Figure C shows an immediate post-operative radiograph. Figure D shows subluxation of the radiocarpal joint caused by failure to support lunate-facet fragment. Figure E shows the clinical appearance of a volarly subluxated wrist.
Incorrect Answers:
Answer 2: The use of a non-locking plate in this situation did not directly lead to the failure of fixation, and applying a similar construct with locking fixation
would not have prevented volar subluxation of the lunate facet fragment. Answer 3: Volar tilt was grossly restored post-operatively.
Answer 4: Radial styloid plating would not have prevented volar subluxation of the lunate facet fragment.
Answer 5: Three bicortical screws in the intact radial shaft proximally is adequate fixation.
Which of the following is most commonly associated with both simple and complex elbow dislocations?
1) radial head fracture
2) radial neck fracture
3) loss of terminal extension
4) repeat dislocation
5) coronoid base fracture
Elbow dislocations are classified as either simple (no associated fracture) or complex (associated fracture). The goal of treatment is a stable joint that tolerates early motion. The initial range of motion is the stable arc found on postreduction examination. Studies have demonstrated a better outcome when simple elbow dislocations are treated non-surgically rather than with surgical repair. Simple elbow dislocations usually have an excellent outcome (return of functional range of motion with normal strength). A loss of terminal extension is the most common sequelae.
Ross et al. reported on 20 patients with simple closed posterior elbow dislocations who were treated with immediate active ROM under close supervision. They found a final arc of motion of -4 to 139 degrees, with final motion reached a mean of 19 days after dislocation. Only 1 patient had recurrent instability.
A 36-year-old female sustains a knee injury after falling from a ladder onto her flexed knee; she cannot do a straight leg raise after a lidocaine injection into her knee. A radiograph is shown in Figure A. Which of the following treatment options has been shown to have the best outcomes with this injury?
1) Long leg cast
2) Hinged knee brace use with functional rehabilitation protocol
3) Open treatment with internal fixation or excision with patellar tendon advancement
4) Distal patellar resection and allograft reconstruction
5) Placement of a cerclage wire from patella to proximal tibia
The clinical presentation is consistent with and inferior pole patella fracture. Open reduction and internal fixation or excision with patellar tendon advancement is the most appropriate treatment of this injury pattern.
Whenever possible, salvage of the inferior pole through open reduction internal fixation is favored over simple excision and patellar tendon advancement, as this has been shown to be associated with improved outcomes. This is not always possible, however, and pole resection can be performed if the inferior comminution precludes fixation. Inferior outcomes of the partial distal patellectomy and patellar tendon advancement are (aside from the possible resulting patella baja) probably not directly related to the patellofemoral articulation. On the undersurface, the proximal 75% of the patella is covered with articular cartilage; however, the distal 25% is not, and does not articulate with the femoral trochlea.
Kastelec et al. performed a retrospective review of ORIF v. pole resection followed over 4.6 years postoperatively. There was a significant increase (better) in patellofemoral score with ORIF; significant differences in knee pain,
tolerated activity levels, and ROM were also noted. Patella baja was frequently noted with pole resection and correlated with worse functional outcomes.
Matejcic et al. performed a retrospective review of ORIF v. pole resection followed over 5.3 years postoperatively. Results were excellent/good in 90.1% of the ORIF and only 73.1% of the pole resection patients. In addition, significant differences between the groups were noted with regard to knee pain, swelling, level activity, compression pain, range of motion, muscular atrophy, muscular strength, and final patellofemoral score (all better with ORIF).
Figure A is a lateral knee radiograph showing an inferior pole patella fracture.
Which of the following factors increase the risk of nonunion in midshaft clavicle fractures when treated nonoperatively?
1) Sling immobilization
2) Displacement and comminution
3) Age less than 40 years old
4) Immediate motion exercises
5) Male
Robinson et al have shown that lack of cortical apposition, comminution, female gender, and advancing age are the 4 factors that contribute to nonunion.
The Canadian Orthopaedic Trauma Society in a randomized, prospective study showed that for midshaft fracture in adults with 100% displacement, ORIF results in improved DASH and Constant scores (p = 0.001 and p
A 34-year-old male presents after falling off a roof at his job. He has an obvious deformity of his left lower extremity, and injury radiographs are shown in Figures A and B. He has no other injuries. Which of the following definitive treatment algorithms will most likely lead to the best outcomes in this patient?
1) Closed reduction and percutaneous screw fixation of the femoral neck, followed by reamed antegrade nailing of the femur fracture
2) Reamed antegrade nailing of the femoral shaft fracture, followed by open reduction and percutaneous screw fixation of the femoral neck fracture
3) Reamed retrograde nailing of the femoral shaft fracture, followed by closed
reduction and percutaneous screw fixation of the femoral neck
4) Open reduction and screw fixation of the femoral neck, followed by reamed retrograde nailing of the femoral shaft fracture
5) Open reduction and screw fixation of the femoral neck, followed by plating of the femoral shaft fracture
The clinical presentation is consistent with a femoral shaft fracture with an ipsilateral femoral neck fracture. Of the options presented, the most appropriate treatment is open reduction and lag screw fixation of the femoral neck fracture followed by reamed retrograde nailing of the femoral shaft fracture.
Ipsilateral femoral neck/shaft fractures are an uncommon injury estimated to occur in 2-6% of all femoral shaft fractures. It is generally agreed upon that due to the potentially devastating complications of the femoral neck fracture in young patients, the neck fracture should be treated first and the shaft fracture second. Anatomic reduction of the femoral neck fracture is paramount in obtaining successful healing, and therefore open reduction is recommended in the setting of fracture displacement. Provisional reduction of the femoral neck fracture, followed by antegrade nailing with subsequent addition of definitive fixation of the femoral neck is also acceptable.
Peljovich et al. present a review article on ipsilateral femoral neck and shaft fractures. The treatment algorithm they propose consists of first treating the femoral neck fracture, and then addressing the femoral shaft fracture with retrograde nailing. They also highlight the risk and benefits of each treatment approach.
Watson et al. reviewed 13 patients who had healing complications after undergoing surgical fixation of their ipsilateral femoral neck and shaft fractures. They found that lag screw fixation of the femoral neck fracture and reamed intramedullary nailing for shaft fracture stabilization were associated with the fewest complications. Therefore, this approach was recommended as the treatment of choice.
Figures A and B demonstrate an ipsilateral comminuted femoral shaft fracture, and a displaced femoral neck fracture. Illustrations A-C show an example of a femoral shaft fracture with an ipsilateral femoral neck fracture treated with lag screws of the femoral neck fx and retrograde nailing.
Incorrect Answers:
Answer 1: Open reduction of the femoral neck fracture with anatomic
alignment is preferred to closed reduction in this case.
Answer 2,3: The femoral neck fracture should be addressed first.
Answer 5: Nailing of the femoral shaft fracture would be preferred initially in this case to prevent disruption of the biology and fracture healing around the comminuted segments.
During surgical treatment of the most common variation of distal femoral "Hoffa" fractures, which of the following orientations for screw fixation should be used?
1) Medial to lateral screw placement across lateral femoral condyle
2) Anterior to posterior screw placement across medial femoral condyle
3) Medial to lateral screw placement across medial femoral condle
4) Anterior to posterior screw placement across lateral femoral condyle
5) Anterior to posterior screw placement across intercondylar notch
The most common variation of a Hoffa fracture is a coronal fracture of the lateral femoral condyle. The most appropriate screw placement of the above answer choices in the treatment of the most common Hoffa fracture variant would be anterior to posterior screws across the lateral condyle for fixation.
Hoffa fractures are coronally oriented fractures of the femoral condyles, with most occurring in the lateral condyle. They are commonly associated with high-energy fractures of the distal femur and can often be overlooked during the assessment and treatment of distal femur fractures. Hoffa fractures are best evaluated using CT scans.
Nork et al. studied the association of supracondylar-intercondylar distal femoral fractures and coronal plane fractures. Of 202 supracondylar-intercondylar distal femoral fractures, they found coronal plane fractures were diagnosed in 38%. A coronal fracture of the lateral femoral condyle was involved more frequently than the medial condyle. Eighty-five percent of these coronal fractures involved a single lateral femoral condyle.
Holmes et al. looked at five cases of coronal fractures of the femoral condyle. All cases received open reduction and internal fixation with lag screws through a formal parapatellar approach. They reported good results with all fractures healing within 12 weeks without complications with final range of motion at least 0 degrees to 115 degrees.
Illustration A shows sagittal and axial CT scan cuts showing a Hoffa fracture of the lateral femoral condyle. Illustration B shows multiple anterior to posterior, and posterior to anterior oriented screws for ORIF of the Hoffa fracture.
A 26-year-old right hand dominant male is involved in a motor vehicle collision and sustains the left humerus injury demonstrated in Figure A. The brachial artery is disrupted and requires urgent attention in the operating room. The patient's preoperative nerve evaluation demonstrates that the patient is unable to initiate extensor carpi radialis longus, extensor carpi radialis brevis, extensor pollicis brevis, extensor digitorum, extensor indicis proprius, and extensor pollicis longus motor activity. What is the most likely etiology for this observed neurologic examination?
1) Neurapraxia of the median nerve
2) Axonotmesis of the radial nerve
3) Neurotmesis of the ulnar nerve
4) Neurotmesis of the radial nerve
5) Axonotmesis of the ulnar nerve
The most likely cause of the radial nerve palsy in a high energy open humerus fracture is laceration or complete disruption of the radial nerve (Neurotmesis).
Neurotmesis is complete disruption of nerve and is associated witn no spontaneous recovery without intervention. Axonotmesis constitutes axon disruption, but the surrounding neural connective tissue is intact and nerve regeneration can occur(Wallerian or antegrade degeneration). Neurapraxias occur often by compression and the axon maintains continuity but local demyelination and ischemia occur.
Ring et al. present a Level 4 study of 24 patients that had radial nerve palsy associated with a humerus fracture. All 6 patients with a transected radial nerve had an open humerus fracture also. The results of primary nerve repair in this circumstance found that there was no recovery in any of the patients.
Foster et al. authored a Level 4 review of 14 patients had a radial nerve palsy and an associated open humerus fracture. 64% of the 14 patients had a radial nerve that was either lacerated or interposed between the fracture fragments. They recommend exploration of the radial nerve in the setting of a radial nerve palsy and concomitant open humerus fracture in contrast to observation of a radial nerve palsy in closed humerus fractures.
Figure A demonstrates an open left humerus fracture.
Incorrect Answers:
Answer 1,3,5: The radial nerve provides distal motor activity to the ECRL, ECRB, EPB, EIP, and EPL.
Answer 2: Axonotmesis of the radial nerve is not the most common form of injury associated with closed or open humerus fractures.
Which of the following is true regarding the center of rotation of angulation (CORA) as it refers to tibial diaphyseal angular deformity?
1) It is the point at which the proximal mechanical axis and distal mechanical axis meet
2) It is the point at which the proximal anatomical axis and proximal mechanical axis meet
3) It is always the point on the cortex at the most concave portion of the deformity
4) It is the point at which the distal anatomical axis and distal mechanical axis meet
5) It is always the point on the cortex at the most convex portion of the deformity
The center of rotation of angulation(CORA) in diaphyseal tibial deformity is defined as the intersection of the proximal mechanical(PMA) or anatomical axis(PAA), and the distal mechanical(DMA) or anatomical axis(DAA).
Angular deformity of the femur or tibia involves angulation not only of the bone but also of its axes. When a bone is divided and angulated, the mechanical and anatomic axis of the bone are also divided into proximal and distal segments.
The pairs of proximal and distal axis lines intersect to form an angle. The point at which the proximal and distal axis lines intersect is called the CORA.
The axis line of the proximal bone segment is called the PMA or PAA, and axis line of the distal segment is called the DMA or DAA. In the tibia, because the mechanical and anatomical axes are almost the same, the PMA and PAA lines overlap, as do the DMA and DAA lines.
Illustration A shows the CORA as it relates to the axes of an angulated tibia.
Incorrect Answers:
2-5:These do not describe the CORA or any other specific anatomical points as they related to long bone deformity.
At long term follow-up, a male who sustains multiple traumatic injuries compared with a premenopausal female, who sustained similar polytrauma, is most likely to have which of the following?
1) Higher quality-of-life scores than females
2) Increased rates of complex regional pain syndrome
3) Require more psychiatric counseling and pharmacologic management than females
4) Take more absentee days at work as a result of illness than females
5) Decreased incidence of lower extremity amputation
Ten or more years after severe polytrauma, premenopausal women, compared to men, demonstrate a higher incidence of posttraumatic stress disorder (PTSD) and take more sick leave time from work.
Depression following polytrauma should be screened for by treating orthopaedic surgeons. Depression commonly arises from a protracted injury and can compound the disability by increasing the perception of more physical illness.
Probst et al. present a Level 4 review of over 600 polytrauma patients. They found that quality-of-life was significantly lower in women (Short form-12 psychologic F = 48.6 +/- 10.8 vs. M = 50.8 +/- 9.4; p = 0.02), but the same rate of women (75.3%) and men (75.4%; p = 0.995) felt well rehabilitated.
Holbrook et al. report a Level 4 study of 1,048 polytrauma patients. They found that females had lower quality-of-life scores and were significantly more likely to develop early combined depression.
Incorrect Answers:
Answer 4: Females take more absentee days at work.
Answers 2, 3, 5: There is no data supporting these answer options.
A 29-year-old healthy Caucasian female presents to the emergency department with her boyfriend with a left anterior shoulder dislocation and several facial abrasions after tripping in the shower approximately three hours prior to arrival. She is 5’7’’ and weights 120 lbs (BMI 18.8). The patient notes that she has not had a menstrual period in three months and that she is training for a long-distance triathlon. Physical examination reveals no other obvious injuries. Basic serum laboratory values are unremarkable. A urine pregnancy test is positive. In addition to treating her shoulder dislocation, the orthopaedic surgeon should
1) Perform a skeletal survey to evaluate for other fractures or dislocations
2) Question the patient in private about the specific details of this injury and her sense of safety in the home
3) Refer the patient to a nutritionist given the patient’s BMI of 18.8
4) Obtain additional laboratory studies and admit the patient to the hospital for treatment of anorexia nervosa
5) Obtain advanced imaging of the shoulder to evaluate for underlying pathologic lesions
for her current injury, it is imperative for health care providers to inquire into the safety of the home environment in potential cases of intimate partner violence (IPV).
Risk factors for female victims IPV include being in the 2nd or 3rd decade of life, current pregnancy, having 1 or more prior children, and low socioeconomic status. Reporting requirements for adult abuse are not standardized amongst most states and physicians must understand the importance of identification and documentation in cases of suspected IPV.
Bhandari et al. state that musculoskeletal injuries are the second most common form of IPV (28%) after head and neck injuries (40%).
Musculoskeletal injuries can be variable, including sprains, fractures, dislocations, and foot injuries.
Della Rocca et al. conducted a survey and found orthopaedic surgeons have several misconceptions regarding victims of IPV and further, nearly half of their survey respondents reported identifying a victim of IPV while only 4% reported that they currently screen their injured female patients for IPV.
Zillmer presents a review of the issues surrounding IPV including proper identification, documentation, appropriate questioning and how to involve community services.
Illustration A shows some basic facts regarding IPV during pregnancy as reported by the CDC. Additional information can be found at the following link.
[htt](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)[p](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)[://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm](http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/index.htm)
Incorrect Answers:
Answer 1. There is no indication for a skeletal survey and it would be inappropriate to subject this pregnant patient to additional radiation.
Answer 3. There is no need to refer a patient to a nutritionist for a normal BMI Answer 4. There is no indication for admission or other laboratory studies in this otherwise healthy patient.
Answer 5. There is no need for advanced imaging in the emergency department in the case of an isolated traumatic shoulder dislocation
A 19-year-old military recruit complains of 7 weeks of right heel pain. He notes the pain is worse with jumping and long distance running. He has completed a course of plantar fascia and Achilles tendon stretching with no significant improvement in his symptoms. He denies constitutional symptoms. On examination, his body mass index is 22, he has a normal foot posture and can perform a single leg heel rise without difficulty. There is no pain with palpation of the lateral border of the foot or with external rotation stress to the midfoot. There is tenderness with medial and lateral compression of the hindfoot and there is a negative syndesmosis squeeze test. There is a negative Tinel's sign at the tibial nerve. Axial and lateral radiographs are shown in Figures A and B. What is the most appropriate next step in management?
1) Heel pad cortisone injection
2) Platelet rich plasma injection and 6 weeks of physical therapy
3) Restricted weight bearing and magnetic resonance imaging of the foot
4) Release of the first branch of the lateral plantar nerve
5) ASTYM or Graston physical therapy techniques to the achilles and plantar fascia
Restricted weight bearing and magnetic resonance imaging of the foot is indicated in this military recruit with a positive heel compression test and suspicion for calcaneal stress fracture.
Calcaneal stress fractures occur as a result of repetitive loading and are more common in females with the female athlete triad (anorexia athletica) of disordered eating, amenorrhea, and osteoporosis. On exam tenderness is obtained with medial and lateral compression of the calcaneus.
Sormaala et al. performed a Level 4 review over 8 years of the Finnish military. They found 34 calcaneal stress fractures with 19 occurring in the posterior part of the calcaneus. Only 15% of the patients had the stress fracture visualized on plain radiography. They conclude that MRI is warranted if plain radiography does not show abnormalities in a physically active patient with exercise-induced pain in the ankle or heel. A nuclear medicine bone scan is also appropriate for diagnosis but MRI may give greater detail.
Gehrmann et al. present a Level 5 review of foot stress fractures. They report that with calcaneal stress fractures the fracture lines are oriented vertically or obliquely in the tuberosity of the calcaneus.
Figures A and B show some sclerosis in the central calcaneus with no evidence of overt fracture and an enthesophyte at the Achilles tendon insertion.
Illustration A and B are T2 sagittal and coronal images demonstrating a stress fracture in the superior calcaneal tuberosity with surrounding edema.
Incorrect Answers:
Answer 1: Heel pad cortisone injections are typically avoided due to risk of fat pad atrophy and are not indicated in calcaneal stress fractures.
Answer 2: Platelet rich plasma is not indicated in calcaneal stress fractures. Answer 4: The patient presents with a negative Tinel's at the tibial nerve and presentation is not consistent with first branch of the lateral plantar nerve entrapment.
Answer 5: ASTYM and Graston physical therapies are not indicated for calcaneal stress fractures.
A 35-year old male is involved in a fall from height and present with the isolated injury shown in Figures A and B. The body of the talus is extruded medially through a large linear open wound. Along with irrigation and debridement, what is the most appropriate definitive management of this injury?
1) Reimplantation of the talar body followed by cast immobilization
2) Reduction of talar body, fracture fixation with smooth Steinman pins, and spanning fixator placement
3) Talar body allograft with internal fixation to native talar head
4) Fragment removal, antibiotic spacer placement and external fixation
5) Reduction of native talar body and ORIF of talar neck fracture
The patient is presenting with a displaced talar neck fracture with extrusion of the talar body. Reimplantation of the talar body and ORIF of the talar neck fracture is the most appropriate treatment.
Talar extrusions are rare injuries and are caused by high energy mechanisms. Complete dislocation without a concomitant fracture is extremely rare. The talus is prone to dislocation as there are no muscular attachments. These injuries need to be treated with anatomic reduction and internal fixation to prevent avascular necrosis and post-traumatic arthritis.
Smith et al. investigated the clinical results and functional outcome after reimplantation of the extruded talus. They concluded that salvage and reimplantation of the talus is a relatively safe procedure with only 2 of the 27 patients developing an infection. No association was found between outcome and associated talar fracture.
Van Opstal et al. reported on two cases of talar extrusions following high energy injuries and reviewed the associated literature. Both cases were treated with wound I&D, reduction and external fixation. After 1 year they had pain free ROM with no signs of AVN or arthritis. Review of the literature showed that anterolateral dislocations are more common than anteromedial. Total talar dislocation is thought to be the endpoint of maximum pronation or supination injuries.
Figures A and B show an extruded talar body in the setting of a Hawkins III talar neck fracture. Illustration A shows a clinical photo of an extruded talus.
Incorrect Answers:
Answer 1: Displaced talar neck fractures should not be treated in a cast, especially open fractures
Answer 2: Definitive treatment of this injury is most effectively accomplished with formal ORIF. Steinman pin fixation is not adequate, even in the presence of an external fixator.
Answer 3: There is no data supporting removal of fragment and use of allograft overuse of native talar body
Answer 4: There is no data supporting removal of the fragment. The associated
Scientific References
- support retaining the fragment.
An 18-year-old male sustains a right hip injury after being tackled on the football field. Figure A shows his radiograph upon presentation to the emergency room three hours later. On physical exam, he is noted to have a foot drop and decreased sensation globally throughout his entire lower leg. Closed reduction under conscious sedation is immediately performed, and the hip is able to be ranged through a stable arc of motion following reduction. A post-reduction radiograph is shown in Figure B. Shortly after the reduction, the patient continues to have a foot drop, but his sensation is slightly improved. Which of the following is the most appropriate next step in management?
1) Exploration of his sciatic nerve
2) EMG
3) CT scan of his right hip
4) Touch-down weight bearing of his right leg and observation of his sciatic nerve palsy
5) Skeletal traction on the distal femur to relax tension on the sciatic nerve
Following successful reduction of a traumatic hip dislocation, a CT scan must be obtained to evaluate for any entrapped osteochondral fragments.
Traumatic hip dislocations are typically the result of high-energy trauma and are frequently associated with posterior wall acetabular fractures. Initial management of a traumatic hip dislocation, with or without a fracture, is immediate closed reduction under conscious sedation. If closed reduction is unsuccessful, immediate open reduction in the operating room should be performed. Following successful reduction, a CT scan is necessary to rule-out
intra-articular osteochondral fragments, even in the absence of fracture on radiographs. The incidence of sciatic nerve palsy following a traumatic hip dislocation is roughly 10%.
Pascarella et. al. review 127 traumatic hip dislocations with and without associated fractures. 5 were anterior dislocations, 13 were central dislocations, and 109 were posterior dislocations. In 45 of the cases, an intra-articular fracture fragment was found after successful closed reduction. They stress the importance of post-reduction CT scans given the large incidence of intraarticular fragments.
Bartlett et al. present a case study of a man who sustained cardiac arrest after attempted arthroscopic removal of a loose body in the hip following a traumatic hip fracture-dislocation. They believe that arthroscopic fluid extravasated through the fracture site under pump pressure and resulted in an intraabdominal compartment syndrome that presented as cardiopulmonary arrest. They do not support arthroscopic procedures of the hip following acute or healing acetabular fractures.
Figure A shows an AP pelvic radiograph with a R hip dislocation. Figure B shows the post-reduction radiograph with a concentrically reduced hip joint and no evidence of fracture.
Incorrect Answers:
Answer 1: Acute exploration of the sciatic nerve is controversial, and shouldn't be entertained before a CT scan has been completed.
Answer 2: EMG scan may be useful if the sciatic nerve fails to recover after a period of weeks to months.
Answer 4: CT scan must be obtained, even in the absence of a fracture on radiographs. In the absence of entrapped fragments, and if a concentric reduction is obtained, the next step would be TDWB and observation of the sciatic palsy.
Answer 5: Skeletal traction is not necessary if the hip is stable after concentric reduction and there are no associated fractures.
Which of the following injuries is anticipated to have a 20% chance of mortality and 50% chance of loss of independence at one year when sustained by an 85-year-old female?
1) Intra-articular distal humerus fracture
2) Distal radius fracture
3) Femoral neck fracture
4) Trimalleolar ankle fracture-dislocation
5) Periprosthetic distal femur fracture
A femoral neck fracture has been shown to have an estimated mortality rate of 20% or more at one year after injury, and estimates regarding loss of independence are at 50%.
Most literature on the topic points out the highest mortality rate is in the first 3-6 months, with mortality rates of 14-36% at one year; mortality rates have been found to return to normal, age-matched controls after that.
Egol et al. provide a review of the factors involved in functional recovery of patients with femoral neck fractures. They report the successes of integrated care pathways and review the risk factors (institutionalization, comorbidities, etc.) that go into the outcomes of these patients. They recommend comanagement of these patients with a medical or geriatric service in order to improve patient outcomes.
Incorrect Answers:
Answer 1,2,4,5: These can be debilitating injuries, but no evidence exists to show these injuries are associated with these levels of morbidity and mortality at one year.
A 17-year-old male falls from a retaining wall onto his left arm. He sustains the injury shown in Figure A. The patient undergoes open reduction and internal fixation of the fracture. Upon discharge from the hospital the medication reconciliation includes an order for daily Vitamin C 500mg supplementation. This medication is given in an effort to decrease the incidence of which of the following?
1) Upper extremity deep vein thrombosis (DVT)
2) Acute carpal tunnel syndrome (ACTS)
3) Complex regional pain syndrome (CRPS)
4) Lower extremity deep vein thrombosis (DVT)
5) Surgical site infection (SSI)
The patient has the clinical presentation of a distal radius fracture and Vitamin C administration has been associated with a lower incidence of complex regional pain syndrome (CRPS) in this group of patients.
Vitamin C administration is associated with a lower risk of complex regional pain syndrome (CRPS), formerly known as reflex sympathetic dystrophy (RSD), after wrist fractures. Vitamin C is thought to reduce lipid peroxidation, scavenge free hydroxyl radicals, protect the capillary endothelium, and inhibit vascular permeability.
Zollinger et al. performed a prospective randomized trial that included 317 adult patients who sustained 328 distal radius fractures and were treated conservatively. They had allocated treatment groups to 200mg, 500mg, or 1500mg vitamin C dosages for 50 days. RSD/CRPS occurrence was lowest in the 1500mg group, however the 500mg dosage for 50 days was recommended at the conclusion of the study. The prevalence of CRPS was 2.4% in the vitamin C group and 10.1% in the placebo group. They found that all of the affected patients were elderly women.
Besse et al. performed a study of 392 patients that underwent foot surgery. They found that the group that received 1 gram daily of Vitamin C following foot surgery had a CRPS incidence of 1.7% compared to a control group that
did not receive Vitamin C and had a CRPS incidence of 9.6%. Figure A is a clinical photo of a distal radius fracture.
A 34-year-old female requests a second opinion following open reduction internal fixation (ORIF) of her left ankle three weeks ago. Which of the following is most appropriate step based on Figures A and B?
1) Progressive weightbearing in 3-4 weeks based on radiographs
2) Deltoid ligament repair vs reconstruction
3) Revision ORIF of fibula with lengthening
4) Revision ORIF of fibula and syndesmosis
5) Removal of syndesmotic screws in 3-6 months
The above clinical scenario shows acute postoperative fibular malrotation and tibiofibular syndesmotic malreduction. Restoration of the proper syndesmotic relationship involves regaining fibular length as well as reestablishing correct
rotation and position of the fibula relative to the tibia. In addition, removal of interposed tissue (deltoid ligament) in the medial joint space may be necessary. However, deltoid reconstruction is not routinely required.
Syndesmosis screw fixation in ankle fractures with syndesmotic disruption is indicated if there is residual or dynamic instability with stress testing of the tibiofibular joint after fixation of the fibula. Syndesmotic screws are commonly maintained in place for at least 12 weeks before removal, if necessary or desired. Controversy exists over use of 1 or 2 screws, screw size, and purchase of 3 or 4 cortices.
Gardner et al. compared radiographic measurements vs CT scans to assess reduction of the tibiofibular syndesmosis in ankle fractures. They found CT was better able to detect syndesmotic malreduction. Although they did not seek to correlate this with functional outcomes, they recommended heightened vigilance for assessing accurate syndesmosis reduction.
Zalavras et al. performed a review on ankle syndesmotic injuries. In their review, they highlight that syndesmotic injuries may occur in isolation or may be associated with ankle fractures. In the absence of fracture, physical examination findings suggestive of injury include ankle tenderness over the anterior aspect of the syndesmosis and a positive squeeze or external rotation test. They recommend stress testing for detecting syndesmotic instability with fixation of the syndesmosis when evidence of a diastasis is present.
Figures A and B show an ankle fracture treated with ORIF and syndesmotic repair, with syndesmotic and fibular malreduction.
Incorrect Answers:
Answer 1&5: Would not address the current syndesmotic malreduction which should be addressed.
Answer 2: Would not address the syndesmotic malreduction.
Answer 3: Fibular length appears appropriate on AP and lateral radiographs.
A 45-year-old patient sustains the injury shown in figure A. What radiographic finding most highly suggests a lateral meniscal injury?
1) Joint depression of 3mm
2) Ipsilateral femoral shaft fracture
3) Joint widening of 6mm
4) Ipsilateral tibial shaft fracture
5) Displaced tibial spine fracture
Figure A shows a Schatzker II tibial plateau fracture. Joint widening of 6mm is commonly asociated with a lateral meniscal injury.
Tibial plateau fractures are commonly associated with soft tissue injuries and the operative surgeon needs to be aware of these commonly associated injuries.
Gardner et al. (2005) examined 62 consecutive Schatzker type II fractures with radiographs and MRIs preoperatively. They found that joint depression greater than 6mm and widening of greater than 5mm was associated with a lateral meniscal injury over 80% of the time.
Gardner et all. (2006) that looked at MRIs for 103 consecutive patients with all types of tibial plateau fractures, only one patient had no soft tissue injuries. 94 (91%) patients had a lateral meniscal injury, 79 (77%) patients had cruciate ligament injury and 70 (68%) patients had a posterior lateral corner injury.
Figure A: shows a Schatzker type II fracture of a tibial plateau.
Incorrect Answers:
Answer 1: The above mentioned articles only found associations with lateral meniscal injuries when joint depression was at least 6mm.
Answer 2: No known association with soft tissue injuries after tibial plateau fractures.
Answer 4: No known association with soft tissue injuries after tibial plateau fractures.
Answer 5: Suggestive of an ACL injury, not an injury to the lateral meniscus.
A 37-year-old male is struck by a car while walking at night. He is hemodynamically unstable at initial evaluation in the trauma bay. Advanced Trauma Life Support protocols are started, and an initial survey is completed. A chest radiograph and a pelvis AP radiograph (Figure A) are obtained. What is the most appropriate next step?
1) The patient should be taken directly to the OR for percutaneous placement of a pelvic external fixator
2) Dedicated inlet and outlet views of the pelvis to better classify the fracture
3) Continued resuscitation and immediate CT of the chest, abdomen and plevis
4) Emergent trip to interventional radiology for pelvic embolization
5) Immediate application of pelvic binder, continued resuscitation and re-evaluation of hemodynamic status
The patient has an Anterior-Posterior Compression type 3 pelvic ring injury (APC3), and this injury places the patient at risk of life- threatening hemorrhage. The most appropriate next step in the trauma bay is to place the patient in a pelvic binder in order to minimize pelvic volume and impart stability to the injured hemipelvis to allow for clot formation.
Pelvic fractures are high energy injuries with a high association of concomitant musculoskeletal trauma and damage to multiple organ systems. It is important that any patient with a high-energy pelvic ring injury undergo a complete
work-up including a CT of the chest abdomen and pelvis to look for alternative sources of bleeding. Application of a pelvic binder should occur once a pelvic ring injury is identified as part of the ongoing resuscitation of the patient.
Karadimas et al. retrospectively reviewed 34 patients at a single center who underwent pelvic arterial embolization as part of their resuscitation. APC injuries had the highest mean transfusion rate during the initial 24 hours, and the overall mortality for pelvic fractures requiring embolization was 23.5% in this series.
Manson et al. conducted a retrospective case-controlled study, evaluating mortality factors on LC-1 fractures. They found that in LC-1 fractures, the sacral fracture pattern does not predict mortality; however, mortality rate was increased in patients with a brain injury, chest injury, or abdominal injury.
Figure A demonstrates an APC3 pelvic ring injury with widening of both the symphysis and the right SI joint. Illustration A demonstrates the same injury as seen in Figure A after application of a pelvic binder with improved alignment of the pelvic ring. Illustration B shows appropriate application of a pelvic binder in a multiply injured patient.
Incorrect Answers:
Answer 1: While this patient may need to go emergently to the OR for multiple reasons, the work-up needs to be completed. However, the patient’s pelvis should be stabilized with a pelvic binder in the interim.
Answer 2: These images should be obtained, but the pelvis should be closed with a pelvic binder first.
Answer 3: While the pelvis may not be the only location of bleeding, the patient has a known source for bleeding, and it can be quickly stabilized with a pelvic binder. After the pelvic binder is placed, continued resuscitation and investigation of other possible locations of bleeding should occur.
Answer 4: While this patient may benefit from embolization, the first step is to close down the pelvis. Closing down the pelvis may prevent the need for embolization.
A 33-year-old man sustains blunt trauma to his forearm and presents with the injury seen in Fig A and B. Definitive management of this injury involves the following:
1) Perform closed reduction of the radius, then immobilize the forearm in a long arm cast in supination.
2) Perform open reduction and internal fixation of the radius, then assess the proximal radioulnar joint for instability, and percutaneously fix the proximal radioulnar joint if instability persists.
3) Perform open reduction and internal fixation of the radius, then assess the distal radioulnar joint for instability, and reconstruct the distal radioulnar joint with a looped palmaris longus autograft if instability persists.
4) Perform closed reduction of the radius, then assess the distal radioulnar joint for instability, and perform internal fixation of the radius if instability persists.
5) Perform open reduction and internal fixation of the radius, then assess the distal radioulnar joint for instability, and percutaneously fix the distal radioulnar joint if instability persists.
Galeazzi fracture-dislocations are fractures of necessity and must be managed surgically. The first step involves surgical fixation of the radial fracture. Next, the distal radioulnar joint (DRUJ) needs to be assessed for stability by looking for gross motion of the distal ulna in forearm supination. If DRUJ instability persists, this needs to be addressed with temporary percutaneous pin fixation with one or two 1.2- or 1.6mm K-wires placed transversely proximal to the sigmoid notch. This is followed by immobilization in above-elbow plaster casts
in forearm supination for 6 weeks postop. Anatomic reduction and rigid fixation of the radius alone does not guarantee DRUJ stability.
Rettig et al. found that the anatomical location of the radial shaft fracture could be used to predict DRUJ instability. Fractures within 7.5cm of the midarticular surface of the distal radius were more likely to require K wire stabilization (55%) compared with fractures more than 7.5cm away (6%).
Korompilias et al. found fractures of the distal third were more likely to require DRUJ stabilization (54%) than fractures of the middle third (12%) and proximal third (11%).
Giannoulis et al., in a review of Galeazzi fracture-dislocations, summarized the options as follows: (1) Stable DRUJ, cast in supination for 6 weeks; (2) Unstable DRUJ, TFCC repair and DRUJ pinning with a K wire in neutral rotation;
(3) Unstable DRUJ with ulnar styloid fracture, ORIF of ulnar styloid with tension band wire or lag screw; (4) Irreducible DRUJ because of tendon interposition (ECU, EDC or EDM), open reduction and TFCC repair.
Figures A and B are AP and lateral radiographs demonstrating a Galeazzi fracture-dislocation with marked disruption of the DRUJ. The radial head is visible in both radiographs and is not dislocated.
Incorrect Answers:
Answer 1: The radius fracture requires surgical fixation. While casting in supination may reapproximate DRUJ alignment, only pinning can prevent future subluxation.
Answer 2: Dislocation of the radial head and proximal radioulnar joint instability is characteristic of Monteggia fracture-dislocations. In this injury complex, the proximal ulnar shaft is fractured and not the radius. Galeazzi fracture-dislocations must not be confused with a Monteggia fracture-dislocation.
Answer 3: Tendon graft stabilization is an option for chronic DRUJ instability. Answer 4: The radial fracture must first be reduced and fixed with a plate.
Assessment of DRUJ stability is only possible after rigid fixation of the radial fracture has been performed.
Which of the following is true when comparing Figure A to Figure B?
1) Figure B is more likely to have an associated fracture
2) Figure A is more likely to be blocked from closed reduction by the extensor digitorum brevis
3) FIgure A is more likely to be open
4) FIgure B is more likely to be blocked from closed reduction by the posterior tibial tendon
5) Figure A more likely to be stable following closed reduction
While medial subtalar dislocations (Figure B) are more common, lateral subtalar dislocations (Figure A) are more likely to be open and have associated fractures.
Subtalar dislocations are devastating injuries with high rates of subtalar arthritis. Medial dislocations are more common and are occasionally blocked from closed reduction by the extensor digitorum brevis. Lateral dislocations are more likely to be open, have an associated fracture, and are occasionally blocked from closed reduction by the posterior tibial tendon, flexor digitorum longus, or flexor hallucis longus. Despite these differences, the injuries are treated similarly with closed reduction and immobilization followed by range-of-motion exercises.
DeLee et al. review 17 cases of subtalar dislocations. They found worse longterm results with lateral subtalar dislocations secondary to associated fractures and frequency of open injuries. They recommend cast immobilization for three weeks followed by early motion.
Heppenstall et al. review 20 cases of subtalar dislocations. They maintained reduction in a short-leg cast for 6 weeks following the injury and had 14 excellent results. The most common complications were restriction of motion and radiographic evidence of degenerative changes.
Goldner et al. review the long-term results of 15 patients who sustained a type III, open, subtalar dislocation. In contrast to closed injuries, they found that open subtalar dislocations are more likely to develop osteonecrosis of the talar body requiring pantalar arthrodesis.
Figure A shows a lateral subtalar dislocation. Figure B shows a medial subtalar dislocation.
Incorrect Answers:
Answer 1: Lateral subtalar dislocations are more likely to have associated fractures.
Answer 2: Lateral subtalar dislocations are most commonly blocked from closed reduction by the posterior tibial tendon.
Answer 4: Medial subtalar dislocations are more commonly blocked from closed reduction by the extensor digitorum brevis.
Answer 5: Medial subtalar dislocations are more likely to be stable, likely secondary to a decreased rate of associated fractures.
A 33-year-old motorcyclist is involved in a motor vehicle accident and sustains a Grade III open fracture of his tibia that is treated surgically. Over the next 35 years, he undergoes multiple debridements for a persistently draining wound. Over the last year, he has noticed "tissue growing out of the wound" and a malodorous smell. A photograph of the wound and a recent radiograph are seen in Figure A. A biopsy of the mass is shown in Figures B, and C. What is the most likely pathologic process?
1) Infection
2) Squamous cell carcinoma
3) Basal cell carcinoma
4) Melanoma
5) Soft-tissue sarcoma
A Marjolin's ulcer is a malignant tumor (Figure A) that develops around chronic osteomyelitis. The increasing size and foul smell suggest malignant change.
These tumors are most commonly squamous cell carcinoma (90%). Figures B and C confirm the diagnosis of squamous cell carcinoma.
Marjolin's ulcers can arise in the setting of burns, venous and decubitus ulcers, vaccination, snake bites and hidradenitis suppurativa. They usually involve the lower extremities. While squamous-cell carcinoma is most common, a small percentage of cases are basal-cell carcinoma, melanoma and sarcoma.
Copcu et al. examined 31 Marjolin's ulcers arising at burn sites. 58% were on the extremities, and had an average time lag of 19 years. Four of 31 cases had regional lymph node spread. They also drew attention to the fact that Marjolin's ulcers are more aggressive, with higher rates of metastasis, recurrence and fatality than other types of skin cancer.
Pandey et al. reviewed the literature on Marjolin's ulcers in chronic bone infections and found that the treatment of choice was still amputation (90% of cases). The challenges faced by the surgeon considering a more conservative approach include: wide resection of cancer for cure, resection of infected bone and soft tissue, preservation of limb function, and reconstruction.
Figure A shows the appearance of a fungating soft tissue tumor, together with a radiograph of chronic osteomyelitis. Figure B (low power) shows the
transition between normal epithelium (left) and squamous cell carcinoma (right), which is infiltrating downward. Figures C is a high power image of SCC. Illustration A shows basal cell carcinoma (Answer 3) with a cleft (red arrow) separating basaloid cells (green arrow) from the stroma. Illustration B shows melanoma with asymmetric proliferation of nests of melanocytes (red arrow), descending into the dermis (Answer 4).
Incorrect Answers:
Answer 1: While there is underlying chronic osteomyelitis, the more concerning disease process is malignant transformation into squamous cell carcinoma (Marjolin's ulcer)
Answer 3: There is no evidence of basal-cell carcinoma. Answer 4: There is no evidence of melanoma.
Answer 5: There is no evidence of sarcoma.
A 36-year-old male sustains an open segmental tibia fracture associated with an overlying 8 cm soft tissue avulsion that requires
skin grafting for soft tissue coverage. No vascular injury is identified. What is the most appropriate Gustilo-Anderson classification of this injury?
1) Type I
2) Type II
3) Type IIIA
4) Type IIIB
5) Type IIIC
An 8cm open segmental tibia fracture requiring skin grafting (but not a skin flap) qualifies as a Gustilo Type IIIA.
An open segmental tibia fracture meets criteria to be a type III injury, and subclassification as a IIIA is due to the lack of a need for free or regional tissue transfer for coverage. Classification as a type IIIB would require a free or regional soft tissue transfer (flap) for coverage. Also, remember that definitive classification is done intraoperatively, after full assessment of the fracture and wound are complete.
Gustilo et al. performed a retrospective review of 673 patients and a prospective review of 352 patients with open fractures. Infection rate of the type I and II in the retrospective series was 12%, and this decreased with use of a standardized modern treatment protocol to 2.5% in the prospective cohort. Type III deep infection rate was 44% in the retrospective study and 9% in the prospective study.
Incorrect Answers:
Answer 1: Involves a wound
A 25-year-old man sustains an open forearm fracture from an auger as depicted in Figures A and B. After debridement of nonviable bone, a 10cm bone defect is left. In planning future definitive treatment of the bone void, the use of an interposed strut allograft
instead of transfer of a vascularized fibula graft would most likely result in which of the following complications?
1) Higher incidence of infection
2) Lower nonunion rate
3) Decreased forearm arc of rotation
4) Complex regional pain syndrome
5) Synostosis
The patient has an open fracture with a large amount of bone loss. A higher incidence of infection would be expected with the interposed allograft strut graft treatment option.
Segmental bone loss in a limb secondary to trauma, tumor resection, or other disease require reconstruction to produce a functional limb. Bone loss of up under 5 centimeters is amenable to bone grafting. Larger defects will require vascularized grafts transfers or allografts. Other surgical options include
distraction osteogenesis and induced membrane technique. Vascularized fibular graft transfers have been shown to have good hypertrophy to support new biomechanical stresses and low rates of infection. Strut allografts have the advantage of unlimited size and no complications associated with donor site, however, complication rates including infection, fracture, and delayed union are higher than vascularized fibular grafts.
Wood et al. retrospectively assessed the outcomes of using vascularized fibula grafts for upper extremity reconstruction. The investigators reconstructed 21 limbs (clavicles, ulnas, radiuses, and humeruses) with defects greater than 6cm and measured rate of union. They experienced a primary healing rate of 71.4%. This rate went up to 81% after 2 patients underwent a secondary procedure revising the construct and adding iliac bone graft to the nonunion site. They concluded that the use vascularized fibular bone grafts are successful for reconstruction of limbs with large bony defects.
Falder et al. investigated the physiologic response to free vascularized fibula grafts. Thirty two graft outcomes were assessed for amount of hypertrophy of the fibular graft, bony union, and rate of limb salvage. They reported that 74% primary bony union occurred at a median of 4.75 months, median hypertrophy of the grafts was 71%, and 90% of patients regained the use of their affected limb within 12 months of the procedure. The authors concluded that vascularized free fibula flaps are an "excellent" option for limb salvage in patient with large bony defects and that these grafts respond well to biomechanical stresses.
Calkins et al conducted a Level 4 study looking at segmental bone defects of the upper extremity with open injuries. The investigators performed thorough debridement and irrigation to the extremities, applied iliac corticocancellous bone grafts with fixation, and secondary wound closure for all 22 patients.
They found a 60% rate of infection and 43% rate of union with use of corticocancellous strut grafts concluding that this technique translated well to the hand, but did not have satisfactory results in the arm and forearm for large defects.
Incorrect Answers:
Answer 2: There is a higher nonunion rate
Answer 3: Strut allograft has not been shown to have inferior forearm motion Answer 4: Strut allograft has not been shown to be associated with complex regional pain syndrome
Answer 5: Strut allograft has not been shown to have a higher rate of synostosis
A 46-year-old male falls 15 feet from a ladder while working. He presents with the radiographs shown in Figures A and B. The injury is closed, and soft tissues are intact upon arrival. Which of the following treatment regimens has been shown to decrease wound complications in the definitive management of these injuries?
1) Immediate definitive fixation of the tibia, and nonoperative treatment of the fibula
2) Immediate ankle-spanning external fixation device with consideration of immediate fixation of the fibula, followed by delayed reconstruction of the tibia
3) Placement of a temporary splint, elevation, and definitive fixation 1 week from injury
4) Immediate definitive fixation of the tibia and fibula
5) Immediate placement of a spanning Ilizarov fixator with limited internal fixation of the distal tibia and fibula
Studies have shown that a staged treatment protocol consisting of immediate fixation of the fibula with placement of an ankle-spanning external fixation device followed by delayed reconstruction of the tibia results in minimal surgical wound complications.
Historically, high rates of infection have been associated with open reduction and internal fixation of pilon fractures due to attempts at immediate fixation through swollen, compromised soft tissues. When a staged procedure is performed with initial restoration of fibula length and tibial external fixation, soft tissue stabilization is possible. Once soft tissue swelling has significantly diminished, anatomic reduction and internal fixation of the tibia can then be performed semi-electively with only minimal wound problems.
Sirkin et al performed a study to determine whether open reduction and internal fixation of intra-articular pilon fractures using a staged treatment protocol (defined in the above paragraph) resulted in improved surgical wound complications. In their cohort of 29 patients with closed pilon injuries treated in this manner, all wounds healed, and none exhibited wound dehiscence or full-thickness tissue necrosis requiring secondary soft tissue coverage postoperatively.
Patterson et al evaluated the use of a two-staged technique for the treatment of 21 consecutive patients with 22 C3 pilon fractures. All patients underwent immediate fibular fixation and placement of a medial spanning external fixator. After, on average, twenty-four days, patients underwent removal of the external fixator and formal open reduction and internal fixation of the pilon fractures. There were no infections or soft tissue complications.
Figure A and Figure B demonstrate orthogonal views of a high-energy intraarticular distal tibia fracture.
Incorrect Answers:
1,3,5: These treatment regimens have not been shown in the trauma literature to be associated with decreased wound complications in the fixation of complex pilon fractures.
A 42-year-old man sustains the injury shown in Figure A after a fall from 6 feet. Physical exam after the injury reveals a flaccid ipsilateral limb. An MRI is performed that reveals nerve root avulsions from C5-T1. Which of the following is the most appropriate management of his fracture at this time?
1) Closed management with a coaptation splint
2) Closed management with a coaptation splint followed by transition to a functional brace after 7-10 days
3) External fixation of humeral shaft fracture until brachial plexus injury resolves
4) Open reduction, surgical fixation with plating
5) Closed management with a sling until brachial plexus injury resolves
A coexisting brachial plexus injury is an absolute indication for open reduction and internal fixation of humeral shaft fractures.
A majority of humeral shaft fractures may be treated non-operatively in a
functional brace. Absolute indications of operative management include open fracture with severe soft tissue injury, vascular injury requiring repair, and a coexisting brachial plexus injury. Patients with a brachial plexus injury are more likely to go on to nonunion when treated non-operatively due to lack of muscular support controlling the fracture fragments.
Sarmiento et al. review 620 patients with humeral shaft fracture treated nonoperatively in a coaptation splint followed by a functional brace. Only 16 patients developed a non-union, and any residual deformity was usually functionally and aesthetically acceptable.
Rutgers et al. present a retrospective case series of 49 patients who had humeral shaft fractures that were treated non-operatively in a functional brace. 44 of 49 patients went on to successful union. Fractures of the proximal third of the humeral shaft were most likely to go on to nonunion.
Figure A shows a midshaft humerus fracture. Incorrect Answers:
Answer 1, 2, 5: operative management is indicated with a coexisting brachial
plexus injury.
Answer 3: a coexisting brachial plexus injury is not an indication for external fixation of humeral shaft fractures.
A 65-year-old diabetic male with forefoot gangrene is evaluated for possible amputation. When discussing the amputation levels with the patient, which of the following should be noted to require the greatest increase in energy expenditure for ambulation?
1) Syme amputation
2) Unilateral transtibial amputation
3) Transfemoral amputation
4) Bilateral transtibial amputations
5) Through the knee amputation
A transfemoral level amputation requires the greatest increase in energy expenditure of the amputation levels given, and a Syme amputation the least.
Biologic joints are energy couples. When performing amputation surgery, more
proximal amputations, accompanied by the removal of more joints, decreases the ability of patients to walk and live independently. Therefore a Syme amputation would require only a small increase in energy needed for ambulation. Bilateral transtibial amputee patients have an energy expenditure that is 40% above baseline levels. According to Miller's Review text, unilateral transfemoral amputee's require a 65% increase in energy expenditure.
Pinzur et al. retrospectively studied 97 adult patients with diabetes mellitus who underwent Syme ankle disarticulation because of a neuropathic foot with an infection or gangrene, or both, during an 11 year period. They found that overall 84.5% of the patients achieved wound healing. Their data support the value of Syme ankle disarticulation in diabetic patients with infection or gangrene.
Laughlin et al. retrospectively reviewed the surgical results and functional outcome of 52 patients treated with Syme amputations for forefoot gangrene. Wound healing was correlated with the preoperative status of the posterior tibial artery and follow-up averaged 27 months. The authors found that that posterior tibial artery Doppler examination is predictive of healing in the Syme amputation performed on diabetics, and that furthermore, diabetics can attain a functional level of ambulation with a Syme amputation.
Illustration A shows a clinical photo of a standard Syme amputation with a healthy heel pad which can allow for limited weight bearing in the absence of a prosthesis.
Incorrect Answers:
1,2,4,5: All of these amputation levels have lower energy expenditure increases than a transfemoral amputation.
A 76-year-old female with underlying osteoporosis presents with severe right leg pain after stepping off a curb. Current femur
radiographs are shown in Figure A. Review of the patient's medical records reveal that she had been evaluated 3 months prior for right hip pain, and work-up at that time was negative. Radiographs of the patient's femur from that previous visit are shown in Figure B. What is the most likely cause of this patient's femur fracture?
1) Fibrous cortical defect
2) Metastatic lesion
3) Acute trauma
4) Bisphosphonate treatment
5) Osteomyelitis
The patient's injury is most consistent with a bisphosphonate induced atypical femur fracture.
Atypical subtrochanteric femoral fractures have been identified as a potential complication of long-term bisphosphonate therapy for the treatment of osteoporosis. Prodromal symptoms of thigh pain are common prior to fracture, and bony failure is usually associated with low energy mechanisms.
Puhaindran et al. performed a retrospective review of the imaging studies and case notes for patients with skeletal malignant involvement who received a minimum of twenty-four doses of intravenous bisphosphonates. Patients were classified as having an atypical subtrochanteric femoral fracture if they had a transverse subtrochanteric fracture following low-energy trauma or an impending fracture, together with radiographic findings. In the study cohort of 327 patients, four patients developed an atypical subtrochanteric femoral fracture. All four patients were female, three had breast cancer, and one had myeloma.
Feldman et al. reviewed the imaging presentations on routine radiographs, alternate imaging modalities, and associated pitfalls in nine atypical femur fractures in six patients. The author states that effects may differ with each bisphosphonate's route of administration and prolongation of activity, despite discontinuation. The review also discusses the theoretical mechanisms of bisphosphonates as a class rather than with a specific alendronate association and provides a broader basis for evaluating the recently observed clinical and radiographic complications.
Figure A shows a transverse subtrochanteric femur fracture. Figure B shows diaphyseal cortical thickening and cortical beaking at the subtrochanteric area.
Incorrect Answers:
Answer 1: The radiographic findings are not consistent with a fibrous cortical defect.
Answer 2: The radiographic findings are not consistent with the presence of a metastatic lesion.
Answer 3: Subtrochanteric fractures are typically associated with high energy
trauma, and this patients mechanism of injury is atypical.
Answer 5: There is no radiographic or clinical evidence supporting the presence of chronic osteomyelits.
Risk factors for intimate partner violence after musculoskeletal injury includes all of the following EXCEPT?
1) Shorter length of relationship
2) Younger age
3) Current pregnancy
4) Alcohol dependency
5) History of prior divorce
History of marriage ending in divorce has not been identified in the literature as a risk factor for intimate partner violence (emotional, physical, and sexual abuse).
The approximate prevalence of intimate partner violence (emotional, physical, and sexual abuse) is 32% among females within the 1 year before they are seen by an orthopaedist for the treatment of musculoskeletal injuries.
Bhandari et al. performed a level 2 cohort study of 282 females presenting to their institution for orthopaedic injuries. The prevalence of intimate partner violence (emotional, physical, and sexual abuse) within the twelve months prior to presentation was 32%.
Bhandari et al. also performed a level 4 review of 263 females referred to the Minnesota Domestic Abuse Program. Identified risk factors for physical abuse included younger age, shorter length of relationship, emotional abuse, psychological abuse, sexual abuse, drug dependency, and alcohol dependency.
Illustration A shows a table that outlines the roles and responsibilities of orthopaedic surgeons according to the Canadian Orthopaedic Association 2012 position statement.
Incorrect Answers:
Shorter length of relationship, younger age, current pregnancy, and alcohol dependency have all been indentified as risk factors for intimate partner violence.
A 30-year-old woman falls onto an outstretched arm while rollerblading. She presents to the emergency room with the elbow deformity shown in Figure A. On physical examination she is unable to range her elbow. She is distally neurovascularly intact. Her radiograph is shown in Figure B. What is the next step in management of this patient?
1) Closed reduction, hinged external fixator
2) Closed reduction, acute surgical repair of the lateral collateral ligament complex
3) Open reduction and surgical repair of the lateral collateral ligament complex
4) Closed reduction, splinting & early passive ROM
5) Closed reduction, splinting & early active ROM
The clinical presentation is consistent with a simple elbow dislocation. Initial management should include closed reduction, splinting or sling placement for comfort and early active ROM exercises.
Simple elbow dislocations should be reduced and treatment guided by the relative stability of the joint during the arc of motion. The elbow should be splinted where it is most stable. After 5-7 days the splint can be discontinued and active ROM started to apply compressive stability to the joint. A hinged brace with an appropriate extension block can facilitate motion through the stable arc.
Armstrong discusses pathomechanics and basis for treatment in simple elbow dislocations. She emphasizes delineating the arc through which the elbow is stable and using this to guide initial management. Early surgical management may be warranted when the elbow is unstable with 60 degrees or more of flexion.
Josefsson et al. studied 30 patients who had sustained simple elbow dislocations and prospectively randomized the patients into non-operative and operative study arms. Operative intervention included reattachment of avulsed ligaments/muscles from the distal humerus. They found no statistical difference in clinical outcomes between the groups regardless of the severity of the instability.
Figure A demonstrates a clinical photo of a patient having sustained an elbow dislocation. Figure B is a radiograph demonstrating a posterolateral elbow dislocation, which is named based on the direction that the ulna/radius move relative to the humerus. Illustration A is a video that reviews the pathomechanics of elbow dislocations.
Incorrect Answers
Answer 1, 2: While use of a hinged external fixator may be appropriate when instability persists after repair/reconstruction of the LCL complex, it is not the first step in the initial management of a simple elbow dislocation.
Answer 3: Open reduction may be warranted if closed reduction is unsuccessful, however an initial attempt at conservative measures should be made.
Answer 4: Closed reduction needs to be followed by splinting to give the tissues a chance to recover from the initial injury; use of ACTIVE range of motion exercises early, will help to provide dynamic compressive stability to the joint.
A 21-year-old male undergoes intramedullary nailing of the closed tibial shaft fracture shown in Figure A. At his 6-week follow-up,
he is noted to have peroneal nerve deficits that were not present preoperatively. Which of the following findings is most consistent with a diagnosis of transient peroneal nerve neurapraxia as the result of his intramedullary nailing?
1) Decreased lateral hindfoot sensation
2) Decreased Achilles reflex
3) Decreased peroneus longus strength
4) Decreased extensor hallucis longus strength
5) Decreased plantar forefoot sensation
Decreased extensor hallucis longus strength is the physical exam finding most consistent with transient peroneal nerve neurapraxia.
Transient peroneal nerve neuropraxia has been noted in up to 5% of patients undergoing closed nailing of tibial shaft fractures. This is of unknown etiology, although injury to the peroneal nerve branches can be from placement of the interlocking screws into the nail. In this syndrome, extensor hallucis longus weakness is noted and decreased sensation is seen in the 1st dorsal webspace (deep peroneal nerve distribution). These symptoms generally begin improving by 3 months and have variable rates of recovery.
Robinson et al. reported on 'dropped hallux' syndrome, with weakness of extensor hallucis longus and numbness in the first web space, without clinical involvement of extensor digitorum longus or tibialis anterior. They found this in 5% of their patients after tibial nailing of closed tibia fractures, and all recovered either partially or completely by 4 months.
Lawrence et al. performed an anatomic study that reported the deep peroneal nerve was located superficial to the anterior tibial artery between the tibialis anterior and extensor hallucis longus muscles in the distal one third of the leg. They also found that the deep peroneal nerve crossed deep to the extensor hallucis longus tendon to enter the interval between the extensor hallucis longus and extensor digitorum longus at an average distance of 12.5 mm proximal to the ankle.
Figure A shows a tibial shaft fracture with mild displacement. Incorrect Answers:
Answer 1: Lateral hindfoot sensation is generally via the sural nerve.
Answer 2: Achilles reflex is via S1 roots.
Answer 3: The peroneus longus is innervated by the superficial peroneal nerve. Answer 5: Plantar forefoot sensation is via the tibial nerve along with the medial and lateral plantar branches.
A 24-year-old male presents after being shot in the lower back. Radiographs and advanced imaging show that the bullet traversed the paraspinal musculature, entered the pelvis below the pelvic brim, did not cross the midline, and is currently lodged in the ilium. No intraarticular involvement was noted, and the bony injury is stable. No occult blood is noted on the rectal examination. The police report indicates that the bullet was fired from a low-velocity weapon. Which of the following is the most important treatment for this patient assuming he is hemodynamically stable?
1) Immediate exploratory laparotomy and bullet removal
2) Bullet removal followed by surgical stabilization of the ilium
3) Immediate surgical debridement of the bullet tract and delayed closure of the soft tissue wound
4) Empiric antibiotic therapy and observation
5) Sigmoidoscopy
Based on the clinical presentation, this patient should be treated initially with empiric antibiotic therapy and observation.
The available literature shows that transabdominal GSW with intra-articular contamination should be urgently débrided and irrigated; extra-articular transabdominal GSW with stable fracture patterns may be managed with observation and empiric antibiotics. Bullets lodged in intra-articular locations should be removed, but retained bullets in other anatomic locations do not necessarily warrant removal.
Watters et al. retrospectively collected Information regarding surgical débridement of pelvis low velocity gunshot wounds, retained foreign bodies, and/or concomitant gastrointestinal (GI) injury was analyzed for relationships of such events to infection rate in 56 patients. The authors found that there was no increased incidence of infection in the absence of aggressive surgical débridement of pelvis gunshot wounds. The study also demonstrated that retained bullets and bullet fragments did not increase the risk of infection, even after penetrating the GI tract organs.
Zura et al. completed a review article on the treatment of gunshot wounds to the hip and pelvis. The authors state that antibiotic treatment usually is indicated for patients with gunshot wounds to the pelvis, but is controversial in patients with low-energy wounds. Furthermore they state that fractures are treated based on their stability and wound care should be determined by the personality of the injury, and not solely based on the velocity of the missile.
Miller et al. completed a recent review article on transabdominal gunshot wounds to the hip and pelvis. They state that extra-articular transabdominal GSW with stable fracture patterns may be managed with observation and empiric antibiotics.
Incorrect Answers:
Answer 1: Immediate exploratory laparotomy would be indicated in the setting of persistent hemodynamic instability or positive peritoneal signs.
Answer 2: There is no evidence that bullet removal is necessary when it is in an extra-articular location. Furthermore the bony injury is stable, and does not warrant fixation.
Answer 3: Immediate surgical debridement is not necessary without intraarticular involvement or severe soft tissue injury.
Answer 5: Sigmoidoscopy would be necessary if occult blood was noted on rectal examination or if the bullet crossed the midline below the pelvic brim.
She lives in an assisted living facility, and reports no other major medical problems. The best functional outcome can be expected with which of the following definitive treatment options?
1) Open reduction internal fixation of the distal humerus fracture
2) Nonsurgical management with early passive range of motion exercises
3) Initial nonsurgical management followed by interpositional arthroplasty when the fracture has healed
4) Total elbow arthroplasty
5) Excision of the capitellar fragments and fixation of the trochlear fragments
This elderly, low demand patient is presenting with a distal and comminuted distal humerus fracture in the setting of poor bone quality. These are extremely difficult to reconstruct and rehabilitate from, and therefore in this particular case total elbow arthroplasty is the best option.
Total elbow arthroplasty has become the treatment of choice for complex, comminuted distal humerus fractures in patients older than age 70. It yields a faster recovery with more predictable functional outcomes, although limitations of lifting weight more than 10-15 pounds must be followed to avoid loosening.
Kamineni et al. retrospectively reviewed 49 acute distal humerus fractures in 48 patients who were treated with total elbow arthroplasty as the primary option. Forty-three of these fractures were followed for 2 years. At the latest follow-up examination, the average flexion arc was 24 degrees to 131 degrees
and the Mayo elbow performance score averaged 93 of a possible 100 points. This review supports a recommendation for total elbow arthroplasty for the treatment of an acute distal humerus fracture when strict inclusion criteria are observed.
Frankle et al. compared open reduction and internal fixation (ORIF) with total elbow arthroplasty (TEA) for intraarticular distal humerus fractures in women older than 65 years of age. Follow-up was a minimum of two years. Using the Mayo Elbow Performance score, the outcomes of the 12 patients treated with ORIF were as follows: 4 excellent, 4 good, 1 fair, and 3 poor. Outcomes of the 12 patients treated with TEA were as follows: 11 excellent and 1 good. There were no fair or poor outcomes in the TEA group, and no patients treated with TEA required revision surgery.
The AP and lateral elbow radiographs shown in Figures A demonstrate a severely comminuted and displaced distal humerus fracture.
Incorrect Answers:
Answer 1: Stable ORIF is nearly impossible to attain in the setting of a very distal fracture of the humerus with comminution and poor bone quality.
Answer 2: Although nonsurgical management of these injuries showed some favor in the past, range of motion and pain control are ultimately better with TEA in the appropriate patient.
Answer 3: Interpositional arthroplasty is indicated in younger patients who may not be able to comply with the strict weight lifting restrictions of a TEA. Answer 5: Fixation of the trochlear fragments would be extremely difficult in this case, and capitellar excision would likely lead to an unstable elbow joint in the setting of a compromised ulnohumeral articulation.
A 52-year-old carpenter falls off of a balcony while at work and sustains the injury shown in Figure A. The patient's BMI is 52 and he smokes 2 packs of cigarettes per day; a clinical photograph of the limb is shown in Figure B. What is the most appropriate next step in management?
1) Short leg splint placement and transition to short leg cast at 2 weeks
2) Closed reduction and spanning external fixation of the ankle
3) Open reduction and internal fixation of the fibula and tibia
4) Open reduction and internal fixation of the fibula with Blair arthrodesis of the ankle
5) Open reduction and internal fixation of the tibia and articulating external fixation of the ankle
Closed reduction with spanning external fixation of the ankle is the most appropriate next step in management with planned definitive tibia ORIF when soft tissue swelling allows. Fixation of the fibula at the time of external fixation has been well-described but is a controversial subject.
Pilon fracture treatment with a staged procedure is performed with initial restoration of length and tibial external fixation. Once soft tissue swelling has significantly diminished, anatomic reduction and internal fixation of the tibia can then be performed semi-electively with only minimal wound problems.
Sirkin et al performed a Level 4 retrospective review of open reduction and internal fixation of intra-articular pilon fractures using a staged treatment protocol. The protocol consisted of ORIF of the fibula and application of an external fixator spanning the ankle joint within twenty-four hours. Patients then underwent formal open reconstruction of the articular surface by plating when soft tissue swelling had subsided at around the 2 week mark. This protocol resulted in improved surgical wound complications. In their cohort of 29 patients with closed pilon injuries treated in this manner, all wounds healed, and none exhibited wound dehiscence or full-thickness tissue necrosis requiring
secondary soft tissue coverage postoperatively.
Illustration A shows an external fixator used for initial stabilization of a pilon fracture.
Incorrect Answers:
Answer 1: Nonoperative management is not indicated in displaced pilon fractures.
Answer 3 & 5: Immediate ORIF of the tibia plafond fracture has a higher incidence of wound complications.
Answer 4: Blair fusion of the ankle is not indicated in pilon fractures
A 23-year-old male right hand dominant minor league hockey player sustains the injury shown in Figure A and B. The patient is apprised of the risks and benefits of both conservative and surgical treatments. He chooses to undergo surgical intervention and wishes to minimize the chance of requiring a second operation. Which of the following is the most appropriate surgical procedure for this patient?
1) Distal clavicle resection
2) Transacromial wire fixation with possible coracoclavicular ligament reconstruction
3) Coracoclavicular screw fixation
4) Hook plate fixation with coracoclavicular ligament reconstruction
5) Small fragment plate fixation with possible coracoclavicular ligament reconstruction
Small fragment plate fixation with possible coracoclavicular ligament reconstruction is the most appropriate treatment for a displaced distal clavicle fracture in a patient that wishes to avoid a second procedure.
The Neer classification describes lateral third distal clavicle fractures. Type II fractures (where the proximal fragment is detached from the CC ligaments and the distal fragment remains attached to the scapula via the AC joint capsule) and Type V (where a inferior clavicular fragment remains attached to the CC ligaments) are often displaced and are believed to have a higher rate of nonunion. Treatment of distal third as well as midshaft clavicle nonunions is best treated with open reduction and internal fixation of the nonunion.
Banerjee et al performed a Level 5 review of the management of distal clavicle fractures. They recommend primary nonsurgical management of type I, type III, and nondisplaced type II distal clavicle fractures. For patients with displacement, the authors offer surgical treatment but counsel them that the current evidence suggests equivalent outcomes between surgical and nonsurgical treatment.
Oh et al. performed a Level 4 systematic review of 425 cases from 21 studies. With surgical treatment, the nonunion rate was not significantly different among the modalities (p = 0.391). The complication rate was significantly higher in cases of the hook plate (40.7%) and the K-wire plus tension band wiring (20.0%) than those of the coracoclavicular stabilization (4.8%), the intramedullary (2.4%) and the interfragmentary fixation (6.3%).
Jin et al present a Level 4 review of 17 patients that underwent CC screw fixation of their distal clavicle fracture. They routinely removed the CC screw at 8 weeks as a second procedure and noted that all but one patient had a good outcome based on the UCLA score.
Figures A and B demonstrate displaced Type V distal clavicle fractures. Illustration A and B demonstrate an example of the use of a hook plate for distal clavicle fixation. Illustration C shows an example of a CC screw fixation and Illustration D demonstrates a distal clavicle plate fixation. Illustration E depicts the Neer classification for distal clavicle fractures. Illustration F displays a distal clavicle fracture ORIF with small fragment locking plate.
Incorrect Answers:
Answer 1: Isolated distal clavicle excision may lead to instability if the fragments are attached to the CC ligaments.
Answer 2: Transacromial wire fixation has a high rate of secondary procedure for wire removal and concern for hardware breakage and migration.
Answer 3: Coracoclavicular screw fixation routinely requires a secondary procedure for removal of the screw.
Answer 4: Hook plate fixation has a high rate of secondary procedure for plate removal to prevent acromial osteolysis.
A 32-year-old male sustains the injury shown in Figures A through D as the result of a high-speed motorcycle collision. He initially undergoes spanning external fixation and returns to the office for soft tissue evaluation prior to his definitive surgery. During this visit, you discuss that the most appropriate fixation is which of the following?
1) Lateral precontoured locked plating
2) Posterior buttress plating
3) Medial antiglide plating
4) Anterolateral and posteromedial plating
5) Posterolateral neutralization plating
Posterior tibial plateau fractures are typically sustained from an axial load with the knee in flexion, leading to a large posterior shearing force on the tibial plateau from the condyles. This most commonly leads to a posterior fracture fragment, with variable involvement of the posteromedial or posterolateral joint line. The shearing nature of this fracture leads to an unstable fracture pattern.
Bhattacharyya et al reviewed 13 patients who underwent fixation of posterior tibial plateau fractures and noted a consistent fracture pattern with a primary, inferiorly displaced posteromedial shear fracture. They reported excellent clinical outcomes at a mean of 20 months, with the quality of articular reduction being one factor that correlated with functional outcome scores.
Fakler et al. was the first English-language study to publish the surgical outcomes of posterior tibial plateau fractures using the Lobenhoffer approach. In their two case study, the authors suggest that the Lobenhoffer approach is less morbid to the soft-tissues in comparison to other commonly described posterior approaches.
Figures A, B, C, and D show a tibial plateau fracture with posterior shear involvement. Illustrations A and B are postoperative images showing the same fracture pattern after posterior buttress plating.
Incorrect Answers:
Answer 1: This fracture fragment is not adequately captured with a lateral based plate; the lateral cortex is also intact, which limits the indications for this plate.
Answer 3: The primary fracture fragment is posterior and not medial. Answer 4: No fracture is seen laterally; posteromedial plating can be utilized, however.
Answer 5: No fracture fragment is seen posterolaterally.
A 40-year-old female sustains the injury seen in Figure A. What other associated soft-tissue knee injury is most commonly associated with this fracture?
1) Anterior cruciate ligament midsubstance tear
2) Horizontal cleavage lateral meniscus tear
3) Peripheral lateral meniscus tear
4) Lateral collateral ligament and popliteofibular ligament tear
5) Lateral meniscus posterior root avulsion
Figure A shows a displaced Schatzker II (lateral split-depression) tibial plateau fracture. These injuries are commonly associated with peripheral meniscal tears.
According to the referenced article by Abdel-Hamid et al, the overall incidence of associated soft tissue injuries of the knee in tibial plateau fractures is 71%. The incidence of each injury in their study was: meniscal tears (57% - usually peripheral tears), ACL (25% - more common in more severe fractures), PCL (5%), LCL (3%), MCL (3%), peroneal nerve (1%). No vascular injury was seen in their collection of 98 patients.
The posterior wall of the acetabulum is best visualized on which of the following radiographic views?
1) Inlet pelvis
2) Outlet pelvis
3) Anteroposterior pelvis
4) Obturator oblique pelvis
5) Iliac oblique pelvis
The posterior wall is best visualized on the obturator oblique pelvic view.
The obturator oblique and iliac oblique views make up the Judet views that are used to evaluate acetabular fractures, along with a standard AP pelvis radiograph. The obturator oblique pelvic view is best to view the anterior column and posterior wall in detail. The iliac oblique shows the profile of involved iliac wing, the posterior column, and the anterior wall.
Letournel reviewed his classification and treatment protocols, based on his 22 years of experience at that time. He noted that perfect anatomical reduction of the acetabulum led to the best outcomes.
Patel et al reviewed of the Letournel classification, and they found moderate to high inter- and intra-observer reliability with this classification system. The presence of articular displacement, marginal impaction, incongruity, intraarticular fragments and osteochondral injuries to the femoral head were found to have less reliability (intra- and interobserver).
Illustration A shows a right-sided obturator oblique radiograph, while Illustration B shows a right-sided iliac oblique radiograph. Illustration C shows a diagram of the obturator oblique radiograph, with the radiographic lines marked out.
Incorrect Answers:
Answers 1: Inlet pelvic imaging is best for assessing pelvic ring injuries (rotation and anterior-posterior or medial-lateral translation).
Answers 2: Outlet pelvic imaging is best for assessing pelvic ring injuries (proximal-distal translation, rotation).
Answers 3: AP pelvis is a good screening tool for pelvic and acetabular fractures.
Answers 5: Iliac oblique pelvis is best for assessing the posterior column and anterior wall of the acetabulum.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
QUESTION 30 OF 50
C omplications after wrist arthroscopy occur in what percentage of patients:
1
5%
2
10%
3
15%
4
20%
5
25%
The complication rate after routine wrist arthroscopy is between 2% and 5%.
QUESTION 31 OF 50
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should
consist of
consist of
1
proximal biceps tenodesis.
2
application of a sling for 3 weeks, followed by physical therapy.
3
anterior capsulolabral reconstruction.
4
repair of the subscapularis tendon.
5
repair of the pectoralis major tendon.
Rupture of the pectoralis major tendon most commonly occurs during bench pressing. Wolfe and associates have shown that the most inferiorly located fibers of the sternal head lengthen disproportionately during the final 30 degrees of humeral extension during the bench press. This creates a mechanical disadvantage in the final portion of the eccentric phase of the lift; with forceful flexion of the shoulder these maximally stretched fibers may rupture. In most patients, particularly in young athletes, the treatment of choice is anatomic repair of the ruptured tendon to its insertion in the proximal humerus either with suture anchors or transosseous sutures. Following surgery, most patients experience a near normal return of strength and significant improvement in the cosmetic appearance of the deformity. While more technically challenging, repair of chronic rupture is possible and is indicated in some patients.
REFERENCES: Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Schepsis AA, Grafe MW, Jones HP, Lemos MJ: Rupture of the pectoralis major muscle: Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
REFERENCES: Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Schepsis AA, Grafe MW, Jones HP, Lemos MJ: Rupture of the pectoralis major muscle: Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
QUESTION 32 OF 50
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of
1
observation.
2
dynamic splinting.
3
resection of the synostosis.
4
proximal radial excision.
5
forearm osteotomy.
The patient has a proximal synostosis; therefore, resection of the synostosis is considered the best option to regain motion. While forearm osteotomy can place the hand in a more functional position, rotation will not be restored. Proximal radial excision can provide forearm rotation; however, this procedure is reserved for patients who have a proximal radioulnar synostosis that is too extensive to allow a safe resection, involves the articular surface, and is associated with an anatomic deformity. Motion will not be restored with dynamic splinting.
REFERENCES: Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Jupiter JB, Ring D: Operative treatment of post-traumatic proximal radioulnar synostosis.
J Bone Joint Surg Am 1998;80:248-257.
REFERENCES: Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Jupiter JB, Ring D: Operative treatment of post-traumatic proximal radioulnar synostosis.
J Bone Joint Surg Am 1998;80:248-257.
QUESTION 33 OF 50
Which of the following factors is considered to be the strongest predictor of outcome following arthroscopic partial meniscectomy?
1
Patient age
2
Patient body mass index
3
Amount of meniscal resection
4
Location of the meniscal tear
5
Modified Outerbridge cartilage score
DISCUSSION: In a recent evidence-based review of the literature, the only consistent factor predicting outcome after arthroscopic partial meniscectomy was the extent of osteoarthritis as classified by the modified Outerbridge cartilage score at the time of surgery. All other factors listed (ie, location of meniscal tear, patient age, patient BMI, and amount of meniscal resection) were shown to not predict outcome following partial meniscectomy. While not provided as an
hoice, female gender was shown to be a predictor for slower recovery in the short term. The Preferred Respon # 114 is 5.
QUESTION 34 OF 50
Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a
successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?

successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?
1
Open reduction and internal fixation (ORIF) of the fracture
2
Removal of the current stem, femur ORIF, and insertion of a longer revision stem
3
Femur ORIF with cables and strut graft, leaving the current stem in situ
4
Femur ORIF combined with reimplantation of the primary component
The fracture has occurred around the stem, representing a Vancouver type B fracture, and the stem is clearly loose, making it a type B2 fracture. The appropriate treatment is removal of the loose in situ stem; ORIF of the femur using cerclage wires, cables, or a plate; and insertion of a longer revision stem such as a tapered fluted modular titanium or fully porous coated cylindrical stem to bypass the fracture. All of the other options are incorrect, because they represent inappropriate treatment options for a Vancouver type B2 fracture.
QUESTION 35 OF 50
At the first postoperative visit after mini-open carpal tunnel release, a patient reports hand weakness. Poor index finger interphalangeal joint extension and metacarpophalangeal joint flexion are present. This finding is most consistent with
1
unrecognized injury to the recurrent motor branch.
2
neuropraxia of the proper palmar digital nerve.
3
new-onset stenosing flexor tenosynovitis.
4
injury to the flexor digitorum profundus to the index finger.
Complications after carpal tunnel release are relatively uncommon. The clinical picture described above is most consistent with lumbrical muscle weakness secondary to neuropraxia of the proper palmar digital nerve to the index finger supplying motor innervation to that muscle. The recurrent motor branch of the median nerve innervates the thenar musculature and would not present as index finger weakness. A new onset of trigger finger may result from a loss of the pulley effect of the transverse carpal ligament, postoperative tendon inflammation, or previously unrecognized flexor tendon triggering. Flexor digitorum profundus to the index finger lies deep within the carpal tunnel, making its injury unlikely. If _it were injured, the result would not be weakness of interphalangeal joint extension._
QUESTION 36 OF 50
Which of the following is not a common finding in cloacal exstrophy:
1
Omphalocele
2
Spinal dysrhaphism
3
Hydrocephalus
4
Dysplasia of the sacroiliac joints
5
Dislocation of the hip(s)
Hydrocephalus is rare because most patients have lipomeningocele, not myelomeningocele.
Omphalocele is common in cloacal exstrophy.
Most patients with cloacal exstrophy have a lipomeningocele that is a form of spinal dysrhaphism. Many patients have malformations of the sacroiliac joints.
Approximately 25% of patients have dislocations of at least one hip.
Omphalocele is common in cloacal exstrophy.
Most patients with cloacal exstrophy have a lipomeningocele that is a form of spinal dysrhaphism. Many patients have malformations of the sacroiliac joints.
Approximately 25% of patients have dislocations of at least one hip.
QUESTION 37 OF 50
A 24-year-old white man presents to the emergency department. He was bitten on his fist while fighting with another man. You notice teeth marks on the dorsum of the metacarpophalangeal (MC P) joint of the right middle finger. The bite does not appear to be deep because the joint is not exposed, and you can see the extensor tendon, which seems intact. The patient has active extension at the MC P joint. The wound is red and swollen, but there is no tenderness or redness on the volar aspect of the MC P joint. The patient has some limitation in range of motion. He is afebrile. Radiographs reveal soft tissue involvement but no joint dislocation or fracture, and there is no neurovascular deficit. The most appropriate antibiotic treatment includes:
1
Imipenam and ciprofloxacin
2
C efotaxime and ciprofloxacin
3
Amoxicillin and ciprofloxacin
4
Amoxicillin and flocloxacillin
5
Bactrim and rifampin
Imipenam and ciprofloxacin provide treatment for gram-negative and gram-positive organisms.
QUESTION 38 OF 50
The most common organism implicated in an infected total hip replacement is:
1
Staphylococcus aureus
2
Streptococcus
3
Staphylococcus epidermidis
4
Escherichia coli
5
Salmonella typhi
Staphylococcus epidermidis accounts for 50% to 75% of all arthroplasty infections. This is the most common organism cultured from the skin of preoperative patients
QUESTION 39 OF 50
A 33-year-old male patient presents with a comminuted open tibia fracture after involvement in a motor vehicle crash. He has a history of smoking but is otherwise healthy. He is given antibiotics, and taken immediately for irrigation and debridement, followed by an un-reamed stainless steel intramedullary nail. Due to bone loss there is a non-circumferential cortical defect measuring 12 mm at the fracture site. All of the following factors in this patient's history and presentation increase his risk for adverse outcome EXCEPT:
1
High-energy mechanism of injury
2
Use of un-reamed nail
3
Implant material
4
Fracture gap
5
History of smoking
Of the factors listed only the use of an un-reamed intramedullary nail for an open tibia fracture has not been shown to increase the risk of adverse outcome or need for reoperation.
The treatment of open tibia fractures with intramedullary nailing can be complicated by many factors. High energy mechanism of injury, use of a stainless steel nail, residual fracture gap greater than 1 cm, and a history of smoking have all been shown to increase the risk of adverse outcome. The use of reamed and un-reamed nails for open tibia fractures have been studied, and no significant difference in outcome has been found.
Schemitsch et al. present data from a prospective randomized trial of tibia fractures treated with reamed or unreamed intrameduallry nails. They found no difference in risk of adverse outcome between reamed and un-reamed nails in open tibia fractures. They did, however, find an increased risk of adverse outcomes in high-energy mechanisms, use of stainless steel (versus titanium) rods, and a residual fracture gap of greater than 1 cm. They comment that their data did not show a significant increase in risk due to history of smoking, but cite other studies that have demonstrated such a relationship.
Bhandari et al. present data from a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. For closed fractures they found a lower rate of primary events (most commonly need for dynamization) in the reamed group. However, they found no difference in outcomes for either technique in open fractures.
Incorrect answers:
Answers 1, 3, 4, 5: Each of these factors have been shown to increase the risk of adverse outcome when treating an open tibia fracture with an intramedullary nail.
The treatment of open tibia fractures with intramedullary nailing can be complicated by many factors. High energy mechanism of injury, use of a stainless steel nail, residual fracture gap greater than 1 cm, and a history of smoking have all been shown to increase the risk of adverse outcome. The use of reamed and un-reamed nails for open tibia fractures have been studied, and no significant difference in outcome has been found.
Schemitsch et al. present data from a prospective randomized trial of tibia fractures treated with reamed or unreamed intrameduallry nails. They found no difference in risk of adverse outcome between reamed and un-reamed nails in open tibia fractures. They did, however, find an increased risk of adverse outcomes in high-energy mechanisms, use of stainless steel (versus titanium) rods, and a residual fracture gap of greater than 1 cm. They comment that their data did not show a significant increase in risk due to history of smoking, but cite other studies that have demonstrated such a relationship.
Bhandari et al. present data from a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. For closed fractures they found a lower rate of primary events (most commonly need for dynamization) in the reamed group. However, they found no difference in outcomes for either technique in open fractures.
Incorrect answers:
Answers 1, 3, 4, 5: Each of these factors have been shown to increase the risk of adverse outcome when treating an open tibia fracture with an intramedullary nail.
QUESTION 40 OF 50
of 100
Figure 46a is the lateral radiograph of a 54-year-old man who has had a painless soft-tissue mass on his right foot that has been growing slowly for about 1 year. MR sequences are shown in Figures 46b through 46e. A biopsy is performed, and a low-power hematoxylin and eosin photomicrograph is seen in Figure 46f. The most appropriate treatment for this lesion is

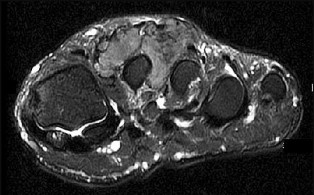
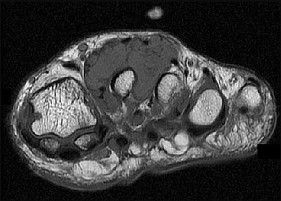
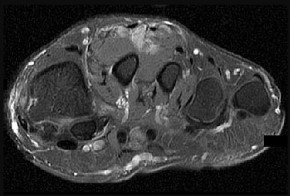
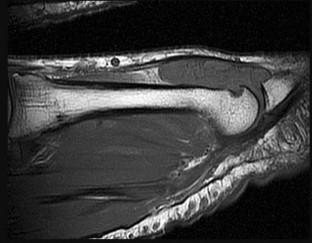
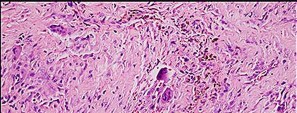
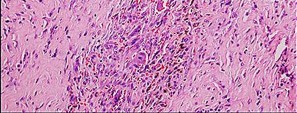
Figure 46a is the lateral radiograph of a 54-year-old man who has had a painless soft-tissue mass on his right foot that has been growing slowly for about 1 year. MR sequences are shown in Figures 46b through 46e. A biopsy is performed, and a low-power hematoxylin and eosin photomicrograph is seen in Figure 46f. The most appropriate treatment for this lesion is
1
a diet that reduces uric acid production.
2
wide local resection followed by radiotherapy.
3
marginal excision.
4
excision and radiotherapy after the mineralization matures.







This is a giant-cell tumor of the tendon sheath. A solid lesion larger than 1.5 cm in the hand or foot warrants biopsy to rule out malignancy. The 3 most common benign tumors of the foot are ganglion cysts, giant-cell tumors of tendon sheath, and hemangiomas. Radiographs are nonspecific but may reveal extrinsic erosions of bone by a giant-cell tumor of the tendon sheath. MR findings of prominent low-signal intensity (seen with T2 weighting) and “blooming” artifact from the hemosiderin (seen with gradient-echo sequences) are nearly pathognomonic of this diagnosis, as
seen here. Pathology shows hemosiderin-laden macrophages and giant cells as seen in the histology. Uric acid reduction would be indicated for gout and wide local excision for a soft-tissue sarcoma. Observation awaiting mature mineralization would apply to heterotopic ossification.
RECOMMENDED READINGS
29. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: radiologic-pathologic correlation. Radiographics. 2008 Sep-Oct;28(5):1493-
[518/. doi: 10.1148/rg.285085134. PubMed PMID: 18794322. ](http://www.ncbi.nlm.nih.gov/pubmed/18794322)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18794322)
30. [Ruggieri P, Angelini A, Jorge FD, Maraldi M, Giannini S. Review of foot tumors seen in a university tumor institute. J Foot Ankle Surg. 2014 May-Jun;53(3):282-5. doi: 10.1053/j.jfas.2014.01.015. Review. PubMed PMID: 24751209. ](http://www.ncbi.nlm.nih.gov/pubmed/24751209)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24751209)
seen here. Pathology shows hemosiderin-laden macrophages and giant cells as seen in the histology. Uric acid reduction would be indicated for gout and wide local excision for a soft-tissue sarcoma. Observation awaiting mature mineralization would apply to heterotopic ossification.
RECOMMENDED READINGS
29. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: radiologic-pathologic correlation. Radiographics. 2008 Sep-Oct;28(5):1493-
[518/. doi: 10.1148/rg.285085134. PubMed PMID: 18794322. ](http://www.ncbi.nlm.nih.gov/pubmed/18794322)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18794322)
30. [Ruggieri P, Angelini A, Jorge FD, Maraldi M, Giannini S. Review of foot tumors seen in a university tumor institute. J Foot Ankle Surg. 2014 May-Jun;53(3):282-5. doi: 10.1053/j.jfas.2014.01.015. Review. PubMed PMID: 24751209. ](http://www.ncbi.nlm.nih.gov/pubmed/24751209)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24751209)
QUESTION 41 OF 50
A child with an idiopathic clubfoot is successfully treated by the Ponseti method. The risk of recurrence of the deformity is most dependent on which of the following factors?
1
Maternal age
2
Positive family history
3
Family’s compliance with bracing
4
The child’s age at walking
5
The child’s body mass index
DISCUSSION: The recurrence rate of clubfoot deformity after successful correction by the Ponseti method has been shown to inversely correlate with reported brace compliance. Maternal age, walking age, and body mass index have not been correlated to recurrence. A positive family history increases the risk of a child being bom with a clubfoot but does not influence the recurrence rate.
REFERENCES: Dobbs MB, Rudzki JR, Purcell DB, et al: Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet. J Bone Joint Surg Am 2004;86:22-27.
Noonan KJ, Richards BS: Nonsurgical management of idiopathic clubfoot. J Am Acad Orthop Surg 2003;11:392-402.
■
**2010 Pediatric Orthopaedic Examination Answer Book • 31**
Figure 33
REFERENCES: Dobbs MB, Rudzki JR, Purcell DB, et al: Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet. J Bone Joint Surg Am 2004;86:22-27.
Noonan KJ, Richards BS: Nonsurgical management of idiopathic clubfoot. J Am Acad Orthop Surg 2003;11:392-402.
■
**2010 Pediatric Orthopaedic Examination Answer Book • 31**
Figure 33
QUESTION 42 OF 50
An obese 62-year-old man (BMI 38) who underwent a cementless total hip arthroplasty 14 months ago fell from a ladder and is now unable to bear weight on the extremity. A radiograph from his 3-month visit is shown in Figure 77a and a radiograph from the time of the injury is shown in Figure 77b. Appropriate management includes which
of the following?
of the following?
1
Nonsurgical management with the use of a cast-brace
2
Nonsurgical management with skeletal traction
3
Open treatment with a plate with or without strut allograft
4
Revision of the femoral component to a cemented femoral component that bypasses the fracture site by two cortical diameters
5
Revision of the femoral component to a cementless femoral component that bypasses the
fracture site by at least two cortical diameters
The patient has a Vancouver type B1 fracture of the femur with a well-fixed femoral component. When comparing the two radiographs, the proximal femoral component position has not changed and remodeling is seen around the component. Nonsurgical management is associated with the complications of extended recumbency. As the femoral component is well-fixed, revision of the femoral component is not necessary.
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Ricci WM, Bolhofner BR, Lofitus T, et al: Indirect reduction and plate fixation, without grafting, for
periprosthetic femoral shaft fractures about a stable intramedullary implant. J Bone Joint Surg Am 2005;87:2240-2245.
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Ricci WM, Bolhofner BR, Lofitus T, et al: Indirect reduction and plate fixation, without grafting, for
periprosthetic femoral shaft fractures about a stable intramedullary implant. J Bone Joint Surg Am 2005;87:2240-2245.
QUESTION 43 OF 50
A 4-year-old girl sustains an isolated spiral femoral fracture after falling from her tricycle. Management should consist of
1
external fixation.
2
plate fixation.
3
skeletal traction for 5 weeks.
4
immediate spica cast immobilization.
5
flexible nailing with titanium nails.
Immediate spica casting is ideal for younger children with uncomplicated femoral fractures that are the result of relatively low-energy injury. Surgical stabilization of pediatric femoral fractures is most commonly performed in children who are older than age 6 years or in children with other factors associated with their femoral fracture, such as concomitant head injury, open fracture, floating knee, severe comminution, or vascular injury.
REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.
Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365.
Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Levy J, Ward WT: Pediatric femur fractures: An overview of treatment. Orthopedics 1993;16:183-190.
REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.
Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365.
Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Levy J, Ward WT: Pediatric femur fractures: An overview of treatment. Orthopedics 1993;16:183-190.
QUESTION 44 OF 50
A 38-year-old woman underwent left knee anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft and medial meniscus repair 11 years ago. She has no complaints of instability since surgery. She presents with left knee pain, swelling and the inability to extend her knee after getting up from a kneeling position one week prior. She reports feeling a pop in her knee at the time of injury. On examination she lacks 5° of extension and has a symmetric Lachman test. Figure 1 is the radiograph of her knee. Figures 2 through 4 show the findings at the time of arthroscopy. What is the most appropriate treatment?
40
40
1
artial lateral meniscectomy
2
Revision ACL reconstruction and medial meniscus repair
3
Lateral meniscus repair
4
Partial medial meniscectomy
The arthroscopic images and the patient's history are consistent with a bucket handle tear of the medial meniscus. The ACL graft is intact and well- vascularized as shown in the arthroscopic image. The morphology of the meniscus and that the images are one of a left knee allows the determination that this is a tear of the medial and not the lateral meniscus. The image of the reduced bucket handle medial meniscus tear reveals plastic deformation and a large overlapping peripheral remnant that would make the possibility of healing after revision medial meniscus repair unlikely or suboptimal. The best treatment option for this patient is partial medial meniscectomy.
41
41
QUESTION 45 OF 50
A 58-year-old man has persistent pain and weakness of his right shoulder after undergoing primary rotator cuff repair 1 year ago. A clinical photograph is shown in Figure 11. Which of the following factors might make functional improvement problematic with revision rotator cuff surgery?
1
Patient’s age
2
Patient’s gender
3
Number of prior surgical procedures
4
Detachment of the deltoid
5
Duration of the rotator cuff tear
Functional improvement after revision rotator cuff surgery is most likely to occur in patients with an intact deltoid, good-quality rotator cuff tissue, preoperative active elevation alone to 90 degrees, and only one prior rotator cuff repair. In this patient, the compromised deltoid origin might make functional improvement less likely.
REFERENCES: Djurasovic M, Marra G, Arroyo JS, et al: Revision rotator cuff repair: Factors influencing results. J Bone Joint Surg Am 2001;83:1849-1855.
Bigliani LU, Cordasco FA, McIlveen SJ, et al: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
Neviaser RJ, Neviaser TJ: Operation for failed rotator cuff repair: Analysis of fifty cases.
J Shoulder Elbow Surg 1992;1:283-286.
REFERENCES: Djurasovic M, Marra G, Arroyo JS, et al: Revision rotator cuff repair: Factors influencing results. J Bone Joint Surg Am 2001;83:1849-1855.
Bigliani LU, Cordasco FA, McIlveen SJ, et al: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
Neviaser RJ, Neviaser TJ: Operation for failed rotator cuff repair: Analysis of fifty cases.
J Shoulder Elbow Surg 1992;1:283-286.
QUESTION 46 OF 50
Figures 1 and 2 are the radiographs of a 46-year-old man with left shoulder pain and
limited range of motion two years after a proximal humerus fracture, which was treated non-operatively. He has forward elevation to 100 degrees with pain at the terminal arc of motion. A subsequent MRI reveals no soft tissue abnormality. After a failed course of non-operative treatment, what is the most appropriate surgical treatment?
---
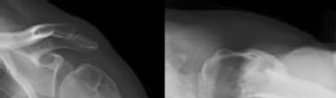
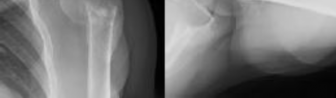
limited range of motion two years after a proximal humerus fracture, which was treated non-operatively. He has forward elevation to 100 degrees with pain at the terminal arc of motion. A subsequent MRI reveals no soft tissue abnormality. After a failed course of non-operative treatment, what is the most appropriate surgical treatment?
---
1
Arthroscopic tuberoplasty
2
Valgus-producing osteotomy
3
Humeral hemiarthroplasty
4
Reverse total shoulder arthroplasty
The patient has a varus malunion of his left proximal humerus. There are no signs of advanced glenohumeral arthrosis or osteonecrosis. After failed nonsurgical treatment, the surgery most likely to improve his symptoms is a valgus-producing osteotomy of the proximal humerus. Arthroscopic tuberoplasty addresses
massive rotator cuff tears or greater tuberosity malunions, but does not address the varus alignment of the articular surface. Humeral hemiarthroplasty can address the deformity but would sacrifice an otherwise normal humeral head in a relatively young patient. Reverse total shoulder arthroplasty would not be indicated in a patient this age with an intact rotator cuff.
massive rotator cuff tears or greater tuberosity malunions, but does not address the varus alignment of the articular surface. Humeral hemiarthroplasty can address the deformity but would sacrifice an otherwise normal humeral head in a relatively young patient. Reverse total shoulder arthroplasty would not be indicated in a patient this age with an intact rotator cuff.
QUESTION 47 OF 50
Figures 1 through 3 represent the radiographs obtained from a 37-year- old man with severe right knee pain. He has a history of prior tibial osteotomy for adolescent tibia vara but notes residual bowing of his legs. On examination, he is 5'8" tall and weighs 322 pounds. He has a waddling gait with a bilateral varus thrust and 20° varus deformity of both legs. His right knee range of motion is 0° to 120° with a fixed varus deformity. What is the best next step?
15
15
1
Total knee arthroplasty with standard components
2
Correction of tibial deformity with osteotomy and nonsurgical management of the osteoarthritis
3
Arthrodesis with a long antegrade nail
4
Total knee arthroplasty with a constrained device
This patient has severe, uncorrectable varus deformity and pain from end- stage osteoarthritis secondary to prior adolescent tibia vara. Although he is young to consider arthroplasty, this option is likely to give him the most functional limb, compared with arthrodesis with a long antegrade nail. During arthroplasty surgery, his knee will likely require extensive medial release to achieve anatomic limb alignment. Standard components in total knee arthroplasty likely would result in lateral instability, so this option is not the best answer. The best choice is total knee arthroplasty with a constrained device, which adds constraint to the knee to provide balance.
16
16
QUESTION 48 OF 50
ORTHOPEDIC MCQS 20 OB TRAUMA 1B
ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 1B
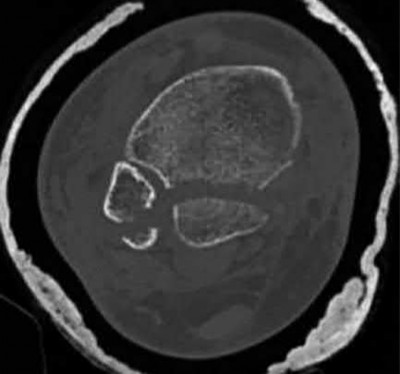
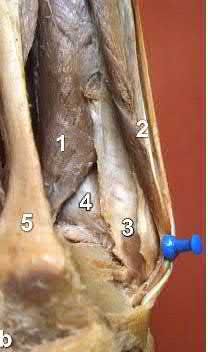







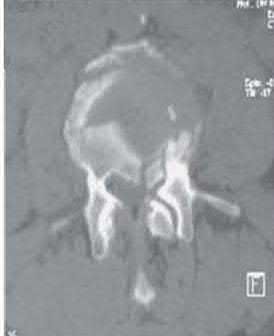

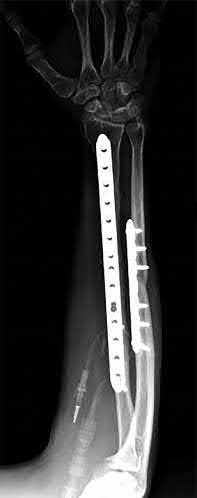

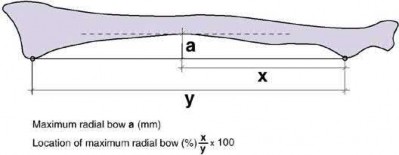



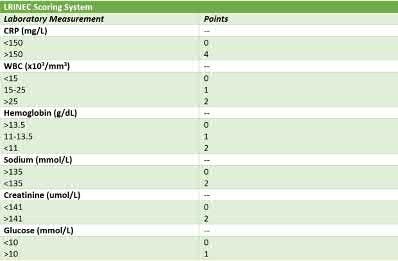


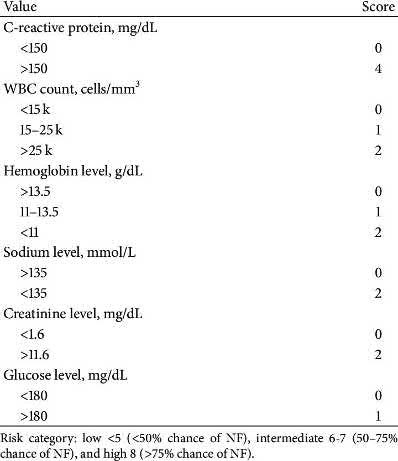

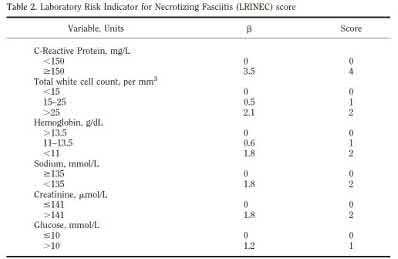






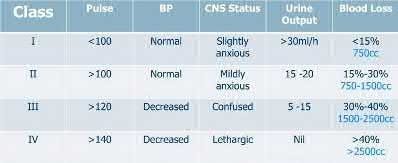
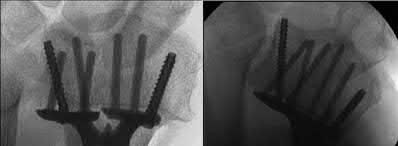


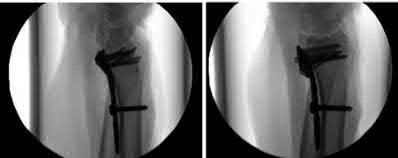



























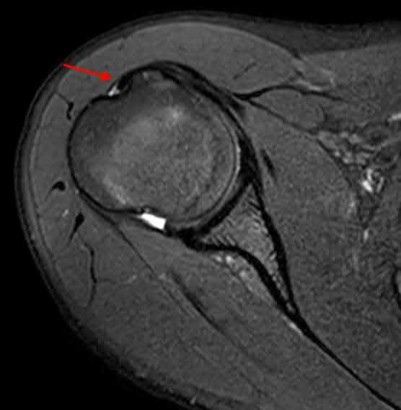







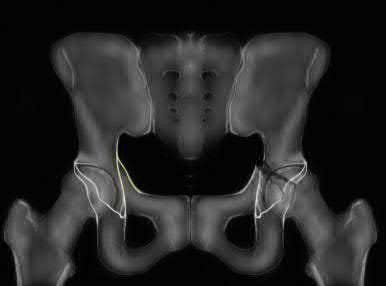



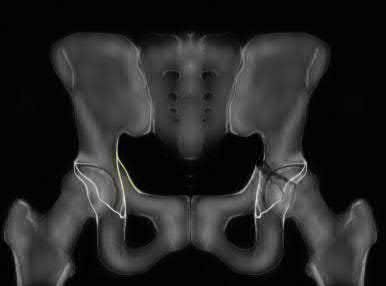
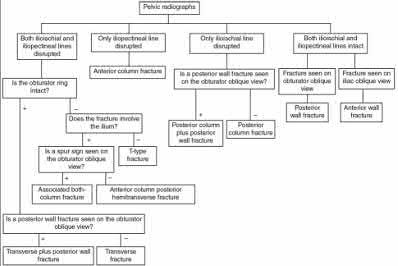
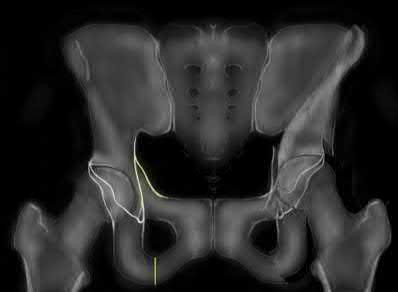

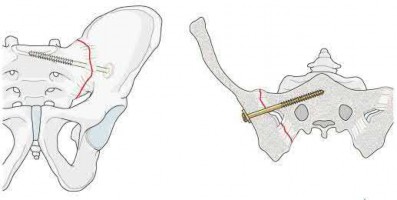

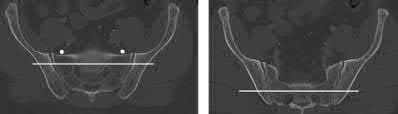
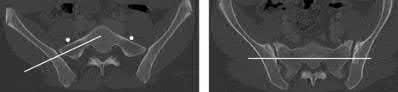






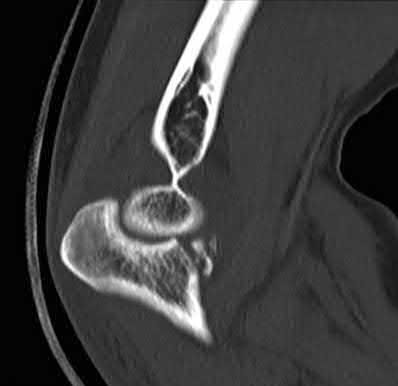



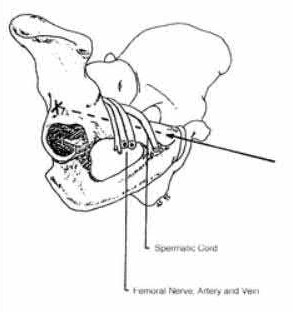
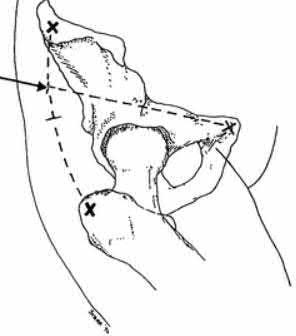
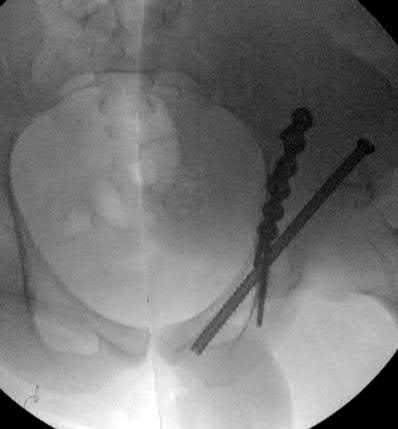
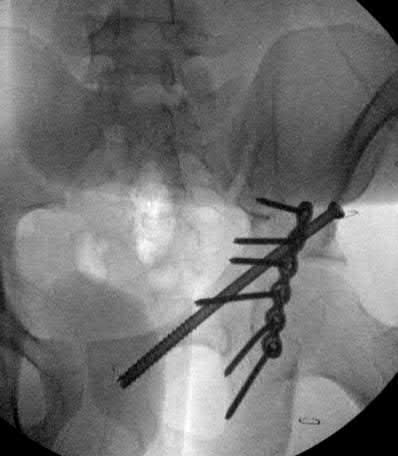




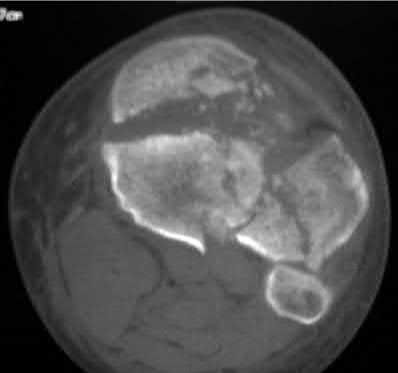
















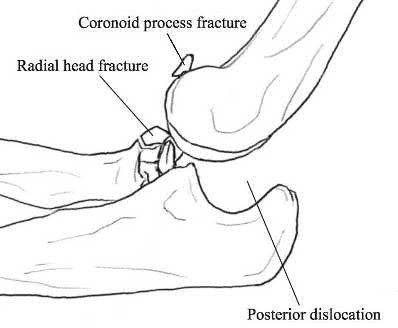

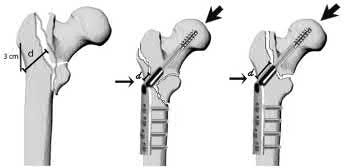


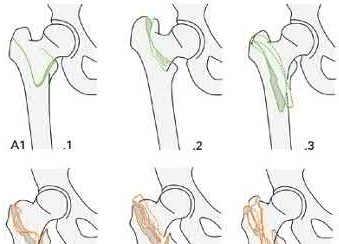
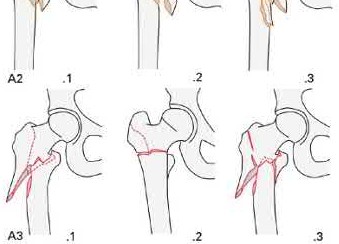

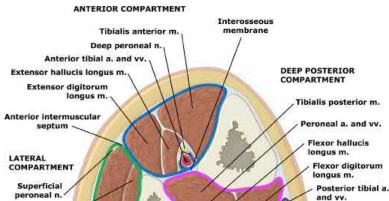
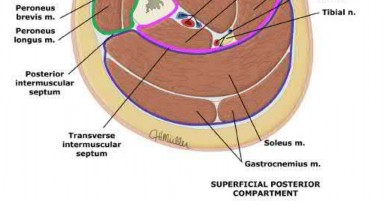

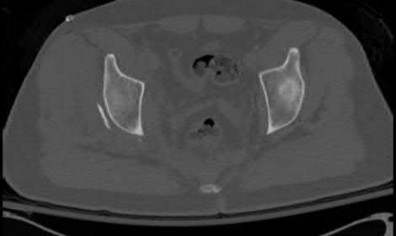
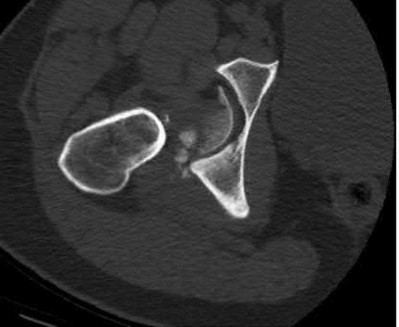


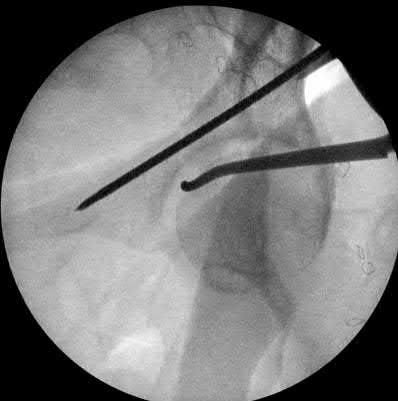
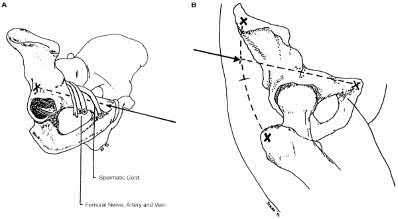
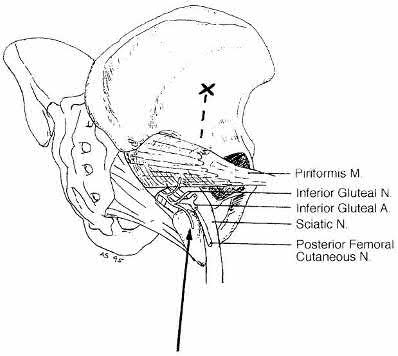


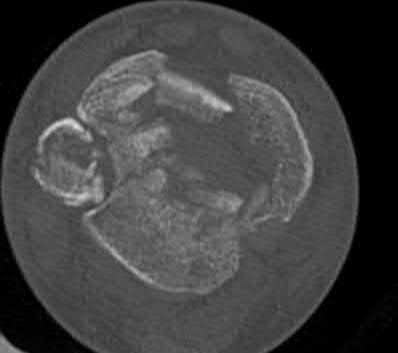






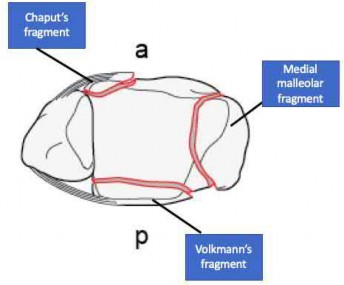


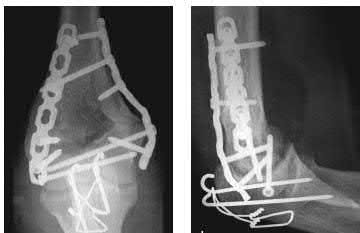
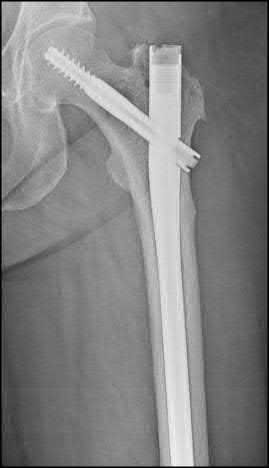

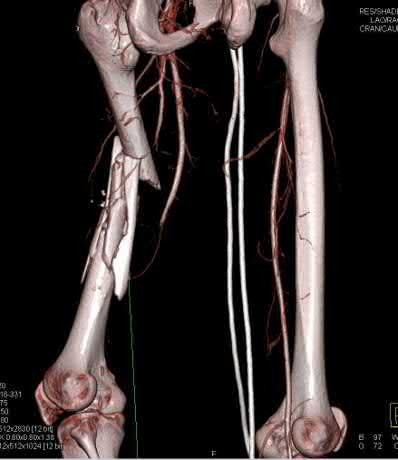





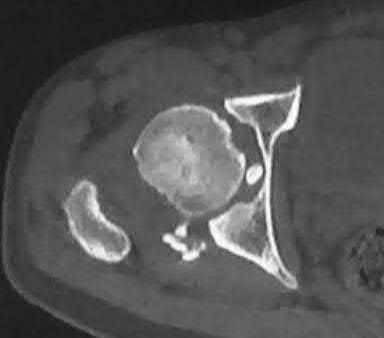
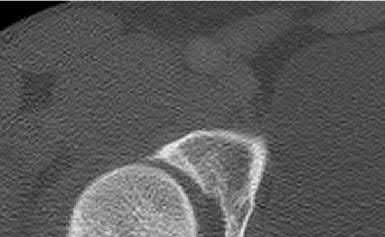
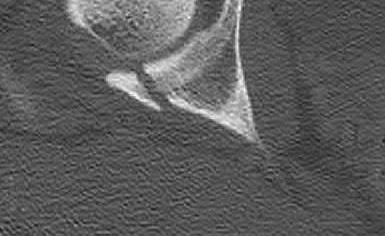
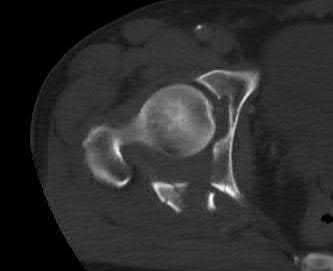



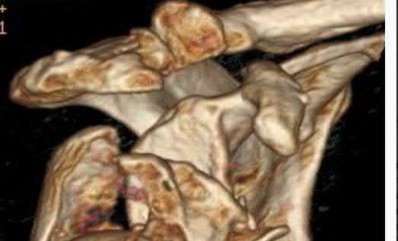

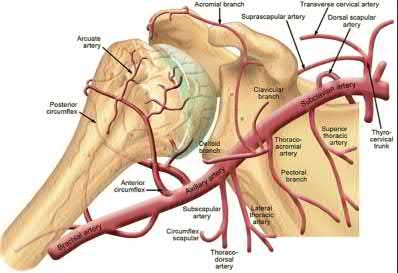

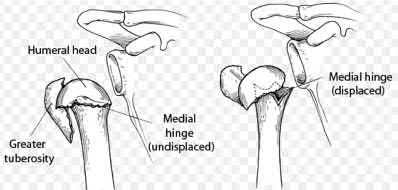


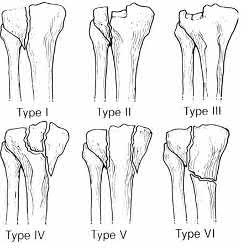








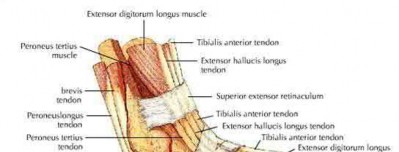
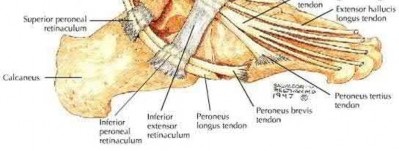
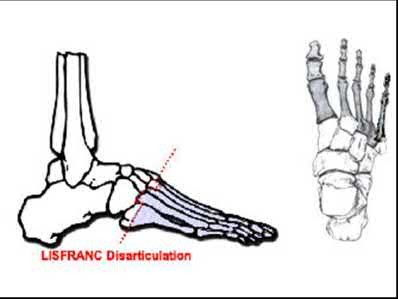

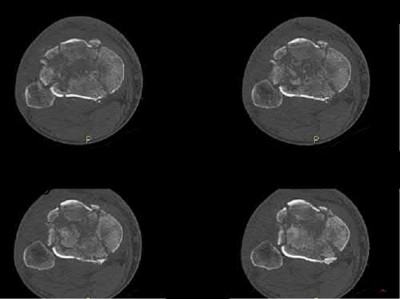



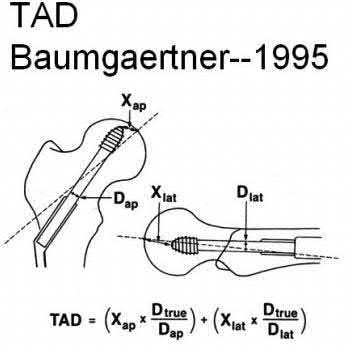






ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 1B
1
Deep peroneal nerve, sural nerve
2
Deep peroneal nerve, tibial nerve
3
Superficial and deep peroneal nerves
4
Superficial peroneal nerve, tibial nerve
5
There is no true internervous plane
The posterolateral approach is most appropriate, through which direct anatomic reduction and fixation of both the distal fibular and posterior malleolar fractures can be achieved. The interval is between the peroneal tendons, innervated by the superficial peroneal nerve, and the flexor halluces longus, innervated by the tibial nerve.
Posterior malleolar fractures most often occur in the setting of rotational ankle injuries and almost always with concomitant fracture of the lateral and/or medial malleoli. The posterior malleolus is not only an important buttress to posterior translation of the talus, but serves as the origin of the posterior inferior tibiofibular ligament (PITFL) and is therefore essential to syndesmotic stability. For this reason, most authors recommend anatomic reduction and fixation or large posterolateral fragments. The ideal surgical approach is controversial, with some advocating for indirect reduction with anterior-to-posterior screw fixation and others for direct visualization through a posterolateral approach. The posterolateral approach is advantageous in that it provides for both anatomic reduction and fixation of the posterior malleolus as well as the often associated lateral malleolar fractures through the interval between the flexor halluces longus and peroneal tendons.
Irwin et al. review the presentation and management of posterior malleolar fractures. They discuss the various surgical techniques which have been described, noting that the posterolateral approach provides the most direct visualization through which anatomic reduction and fixation can be achieved of both the posterior malleolar and distal fibular fractures. There is debate over which fracture should be fixed first, as fibular fixation can restore length and facilitate reduction of the posterior malleolus, but the fibular hardware often interferes with fluoroscopic visualization.
Forberger et al. evaluated the functional outcomes and morbidity following fixation of posterior malleolar fractures via a posterolateral approach performed in 45 consecutive patients. The authors found that the approach not only permitted excellent surgical exposure and stable fixation of the posterior malleolar fragment, but complications were minimal. Functional outcomes were furthermore excellent in the majority of patients.
Figures and Illustrations:
Figures A through C are AP, oblique, and lateral radiographic views of a right ankle demonstrating displaced fractures of the lateral and posterior malleoli. Figure D is an axial CT scan of the right ankle following closed reduction and splint application.
Illustration A is demonstrates the plane of the posterolateral approach. A cadaveric specimen is shown with a pin in the lateral malleolus retracting the peroneal tendons (2) laterally. The Achilles (5), FHL (1) and PITFL (3) are shown. The posterior malleolus (4) is visualized in the interval between the distal fibula and FHL.
Incorrect Answers:
: This is not considered an internervous plane, given that the sural nerve is strictly sensory.
Answer 2: This interval describes medially-based approaches to the foot. Answer 3: This interval describes the anterolateral approach to the ankle. Answer 5: A true internervous plane between the tibial and superficial peroneal nerves exists.
Figures A-C are the radiographs of a 26-year-old male who presents to the emergency department following a motocross accident. Two attempts at a closed reduction by the on-call orthopedic resident were unsuccessful. Figures D and E are the pre-operative axial CT-images that were obtained. The patient undergoes surgical fixation seen in Figure F. Limitations in post-operative dorsiflexion is likely influenced by which of the following?
1) Fracture extension to the posteromedial rim
2) Initial displacement of the fibula fracture
3) Posterolateral approach to address both the fibula and posterior malleolus
4) Initial talar subluxation
5) Inability to reduce the ankle
This patient sustained a Bosworth fracture-dislocation and a posterolateral approach to the ankle is used to reduce the fibula back into the incisura and stabilize both the fibula and posterior malleolus. Loss of dorsiflexion is the most common arc of motion that is limited following this fracture pattern with posterior fixation.
The rare Bosworth fracture-dislocation is a posterior dislocation of the fibula which becomes entrapped behind the tibia. As demonstrated in this vignette, these injuries are extremely difficult to close reduce secondary to the ridge of the posterolateral distal tibia. The irreducible nature of this injury is a known risk factor for the development of compartment syndrome. The CT images further demonstrate fracture extension to the posteromedial rim (“posterior pilon variant”). In this situation, the only effective method to reduce the fracture is through an open posterolateral approach with the interval between the flexor hallucis longus and the peroneal tendons. This is the same approach that is utilized for fixation of the posterolateral fragment and fibula. Loss of dorsiflexion has been demonstrated following this fracture pattern with posterior fixation. The positioning of the plates in Figure F suggests the
utilization of a posterolateral approach.
Switaj et al. retrospectively reviewed 270 patients with posterior malleolus and pilon variant fractures that were operatively treated. They reported that female gender, increasing age, and diabetes may be associated with both fractures of the posterior malleolus as well as the posterior pilon variant. They concluded that the relative frequency of the posterior malleolar fracture and posterior pilon variant in operatively treated ankle fractures was 50% and 20%, respectively.
Gardner et al. reviewed closed pronation-external rotation 4 (PER4) ankle fractures that involved the posterior malleolus without a complete tear of the posterior-inferior tibiofibular ligament (PITFL) treated with either posterior malleolus ORIF or syndesmotic stabilization. They reported that stiffness was restored to 70% after fixation of the posterior malleolus, and to 40% after syndesmosis stabilization. They concluded that syndesmotic stability may be obtained more effectively by the fixation of the posterior malleolus rather than by using a syndesmotic screw.
Berkes et al. reviewed 108 supination-external rotation 4 (SER4) fractures to examine the impact of articular surface congruity on the functional outcomes. They reported that 33% of patients had elements of articular surface incongruity on postoperative CT scanning. They found that the group with articular incongruity had significantly worse foot and ankle outcome scores (FAOS) with regards to symptoms, pain, and activities of daily living. They concluded that the presence of postoperative articular incongruity correlated with inferior early clinical outcomes.
Kalem et al. compared the results of AP screws, PA screws and posterior buttress plate use for posterior malleolar fixation of trimalleolar fractures. They report better AOFAS scores in the PA group and the plate group compared to the AP screw group. However, they concluded that utilization of a posterolateral approach was found to have a loss of ankle dorsiflexion of 5 degrees or greater for both the PA screws and plate groups; 39% and 24%, respectively.
Chen et al. addressed the term “posterior pilon” in their letter to the Editor. He reports that this term was first introduced to describe severe trimalleolar fractures with the presence of a fourth fragment located deeper than the avulsed posterior fragment. The mechanism for this injury results from the impaction of the posterior fragments secondary from axial loading, which is the main causative factor of a classic pilon fracture.
Figures A-C: The initial radiographs reveal the posterior subluxation of the talus with associated posterior subluxation of the fibula without significant coronal plane deformity. This deformity should raise the suspicion of a Bosworth fracture-dislocation, especially if closed reduction is not successful. Figures D and E: Axial CT images demonstrating Bosworth fracture-dislocation of the fibula entrapped behind the tibia. Also, note the fracture extension to the posteromedial rim in this posterior pilon variant.
Figure F: Positioning of the plate suggests a posterolateral approach to address both the fibula and posterior malleolus fractures.
Incorrect Answers:
Answer 1: Fracture extension to the posteromedial rim makes this a "posterior pilon variant," but in itself is not the reason for a decrease in postoperative dorsiflexion
Answer 2: Initial displacement of the fibula fracture may be significant with some ankle injuries. However, the amount of initial displacement has not been correlated with a loss of postoperative dorsiflexion.
Answer 4: The presence of talar subluxation is often seen with ankle injuries. While this may be a result of a large posterior malleolus fragment requiring surgery through a posterolateral approach, the subluxation itself has not been shown to limit postoperative dorsiflexion.
Answer 5: The inability to reduce the ankle may suggest a Bosworth fracture-dislocation. Though reduction helps with soft tissue swelling and chondrolysis, it has not been shown to correlate with postoperative dorsiflexion limitations.
A 69-year-old man presents with the injury depicted in Figures A and B after a fall from his attic. On initial presentation, his lower extremity strength is grade 3/5 but has full sensation in bilateral lower extremities. When his indwelling urinary catheter is pulled, his anal sphincter tightens. He remains bed-bound for the next 4 days and unfortunately develops aspiration pneumonia, requiring urgent intubation and increased positive end-expiratory pressures and a high ventilatory rate to keep him oxygenated. He remains febrile to 39°C, has a pulse rate of 130 bpm, and requires high dose pressors to keep his mean arterial pressure above 65 mmHg. Laboratory markers include WBC 18,000 with 95% PMNs, ESR 120 mm/h, and CRP 200 mg/L. Which of the following findings would most likely be observed in the type of shock this patient is currently in?
1) Decreased mixed venous oxygen saturation
2) Increased pulmonary capillary wedge pressure
3) Bradycardia
4) Loss of rectal tone
5) Decrease in systemic vascular resistance
This patient sustained an L3 burst fracture with no evidence of spinal shock on presentation, however, suffered an aspiration event causing pneumonia and is now in septic shock. Decreased systemic vascular resistance is observed during septic shock.
Septic shock has a mortality rate estimated at 25%-50%. It is a medical emergency resulting from decreased tissue perfusion and oxygen delivery as a result of severe infection and sepsis. Septic shock is associated with decreased cardiac output, decreased pulmonary capillary wedge pressure, decreased central venous pressure, and increased mixed venous oxygen saturation. It is differentiated from hypovolemic shock in that the systemic vascular resistance is decreased in septic shock, whereas it is increased in hypovolemic shock.
Although this patient has a burst fracture, it is important to distinguish this injury from neurogenic shock, which is usually a consequence of traumatic spinal cord injuries to the upper thoracic or cervical levels that results in autonomic dysregulation (loss of sympathetic tone and unopposed parasympathetic response, leading to bradycardia and decreased vascular resistance).
Schouten et al. reviewed the initial assessment and emergency treatment in
the spine-injured patient. They reported that hypotension should always be assumed to be of hemorrhagic etiology until proven otherwise, with initial treatment involving fluid resuscitation with a focus on raising systemic vascular resistance in cases of septic shock. They recommended that all aspects of emergent care, including resuscitation and choice of imaging modalities, be systematically reviewed, and practice guidelines are adopted institutionally.
Hadley et al. reviewed blood pressure management after acute spinal cord injury. They reported that hemodynamic alterations during acute spinal cord injury include hypotension, cardiac dysrhythmias, decreased peripheral vascular resistance, and reduced cardiac output. They recommended that hypotension (systolic blood pressure
A 45-year-old female barista from Portland fell off her skateboard and sustained a closed distal radius fracture. The patient undergoes
open reduction internal fixation (ORIF). Post-operatively she is given a prescription with the goal of mitigating a potential adverse outcome.
Which of the following has evidence to support its utility in this clinical situationr?
1) Alendronate 700mg once per week for 3 months
2) Vitamin C 500mg once daily for 50days
3) Alendronate 70mg once per week for 3 months
4) Vitamin C 200mg once daily for 50days
5) Vitamin C 1500mg once daily for 100days
There is some evidence to support that Vitamin C 500mg PO taken daily for 50 days may decrease the chances of developing complex region pain syndrome (CRPS) following ORIF of distal radius fractures.
CRPS is generally classified as type I, in which symptoms develop in an absence of specific nerve injury, or type II, in which there is the presence of specific identifiable nerve injury. The diagnostic criteria include pain disproportionate to the inciting event and a combination of sensory, vasomotor, sudomotor, and trophic signs. Treatment often involves a combination of physical therapy and pharmacologic treatment, nerve blocks, or chemical or surgical sympathectomy. However success is mixed, therefore prevention is paramount. Given that the etiology is thought to involve a traumatic incident that elicits an overwhelming systemic inflammatory reactions, causing disproportion pain and increased vascular permeability, it is hypothesized that the administration of Vitamin C as a free radical scavenger may protect the vascular endothelium and reduce the incidence of CRPS. Prophylactic administration after management of distal radius fractures is supported by moderate evidence as per the 2013 AAOS guidelines on the Treatment of Distal Radius Fractures.
Zollinger et al. performed a double-blinded randomized controlled trial of 427 wrist fractures, allocating patients to receive placebo or 200, 500, or 1500mg of vitamin C for 50 days. The authors found that in the vitamin C group, the incidence of CRPS was 2.4%, while it was 10.1% in the placebo group. They showed no difference in relative risk between the 500mg and 1500mg groups. The authors concluded that Vitamin C reduces the prevalence of CRPS and a daily dose of 500mg for 50 days is recommended.
Koval et al. comprehensively reviewed controversies in the management of distal radius fractures. The authors highlight the evidence supporting vitamin C use in treating disproportionate pain. However, because there is no objective
measure for the diagnosis CRPS, the evidence remains limited.
Incorrect Answers:
Answer 1: A prospectiv randomized controlled trial was conducted to evaluate healing rates in patients following administration of 70mg alendronate weekly for three months. There was no difference in clinical outcomes or healing between control and experimental groups.
Answer 3: Alendroate has not shown to be beneficial in this setting.
Answer 4: The recommended length and dose of treatment is Vitamin C 500mg for 50 days.
Answer 5: Studies have shown no difference between 500mg and 1500mg. A daily 500mg dose is recommended by the AAOS.
A 30-year-old plastic surgery resident fell from a height of 12' and sustained a right both-bone forearm fracture. The patient underwent open reduction and internal fixation with 3.5mm Limited Contact Dynamic Compression Plating. Three months after fixation the patient has no forearm tenderness and has full active range of motion of his fingers, hand, and wrist. However, pronation and supination are severely limited. This affects his ability to suture during surgery and knit, although he has returned to his other recreational activities. His most recent radiographs are shown in Figures A and B. What is the most likely cause for his lack motion?
1) Fracture nonunion
2) Posterior interosseous nerve (PIN) palsy
3) ECU interposition at the DRUJ
4) Heterotopic ossification
5) Loss of radial bow
This patient sustained a both-bone forearm fracture that was fixed with a long, straight plate which did not account for the native radial bow. This is the most likely reason for his limited pronosupination.
Open reduction with internal fixation of both-bone forearm fractures has generally demonstrated a high rate of union and excellent functional results. However, restoration of the radial bow is a critical. A lack of radial bow will limit pronosupination. To avoid this problem, the surgeon could have used a shorter plate or a plate with an anatomic radial bow, which many modern forearm plating systems now account for. The assessment and calculation for radial bow is highlighted in Illustration A. Other factors which may contribute to limited pronosupination include heterotopic ossification and scarring, though the former is not seen on radiographs.
Matthews et al. evaluated the impact of radial bow on pronosupination in a cadaveric both-bone forearm fracture model. The authors found that with a 10-degree deviation from the anatomic radial contour, there was no loss of pronosupination. However when this was increased to a 20-degree angulation, there was a significant loss of forearm pronosupination. The authors underscored the importance of restoration of radial bow in fixation of both-bone forearm fractures.
Schemitsch and Richards evaluated the outcomes in 55 adult patients following both-bone forearm fracture fixation. They reported good-excellent outcomes in 84% of cases. The authors found that bone grafting did not affect union (54/55 achieved union), but noted that restoration of the radial bow affected functional outcome and grip strength. The authors stressed the importance of restoration of radial bow.
Figure A is an AP radiograph of the forearm following ORIF of a both-bone forearm fracture with a long straight plate which fails to restore the anatomic radial bow. Figure B is a lateral radiograph of the same patient demonstrating fracture fixation with a long straight plate. Illustration A demonstrates the method for determining radial bow. A line from the sigmoid notch to the bicipital tuberosity is drawn (Y). A perpendicular line is drawn from Y to the point on the radial with maximal bow (a) (This number is usually 7%). The point of this intersection to the bicipital tuberosity is marked (x). The location of maximal bow is x/y (This number is usually 60%).
Incorrect Answers:
Answer 1: The patient is non-tender and has returned to activities. He does not have any clinical or radiographic evidence of fracture nonunion.
Answer 2: The patient has full active range of motion of his digits and wrist, which would indicate that the PIN is functional.
Answer 3: The ECU can be interposed at the DRUJ, particularly in radial shaft fractures in which the DRUJ is unstable after fracture fixation. However, this patient does not have DRUJ instability. Furthermore, there is no evidence of DRUJ diastasis on X-Ray.
Answer 4: The radiographs are negative for any evidence of heterotopic ossification, though this is another potential source of limited motion following ORIF of both-bone forearm fractures.
A 46-year-old male presents with the radiographs in Figure A following a skiing accident. You decide to treat this injury with an intramedullary nail. During insertion of your nail, it's decided that blocking screws are needed. In which position should they be placed to prevent the most common malunion?
1) A and D
2) A and C
3) B and C
4) B and D
5) A and B
Proximal third tibial shaft fractures have a propensity to be malunited in valgus and procurvatum. To prevent this, blocking screws can be used in the
concavity of the expected deformity, locations B and C.
Malunion and soft tissue compromise are two complications with a high association to proximal third tibial shaft fractures. The most common deformity seen in a malunited fracture is valgus and procurvatum due to the pull of the pes anserine and the patellar tendon, respectively. Numerous techniques exist to help prevent this deformity including the use of blocking screws, unicortical plating, and the universal distractor. If blocking screws are employed they should be placed on the concavity of the expected deformity, which in this case would be posterior in the sagittal plane and laterally in the coronal plane of the proximal fragment. Once reduction is obtained, if the blocking screws are left in place they have the added benefit of creating a stronger construct.
Kulkarni et al review the use of blocking screws for intramedullary nailing of proximal third tibial shaft fractures. They report an average time to union of
4.2 months with 5/66 cases going on to non-union, which were all successfully treated with bone grafting, and 1/66 resulting in a malunion. They conclude that blocking screws help maintain fixation and alignment of proximal third tibia fractures treated with intramedullary nails.
Stinner et al review techniques for intramedullary nailing of proximal third tibial shaft fractures. They report on several techniques including blocking screws, unicortical plating, and clamp reduction to assist the surgeon in obtaining an adequate reduction. They conclude that while implant design and surgical techniques have improved, the surgeon must still be cognizant of the valgus and apex anterior deformity and know how to neutralize these forces.
Franke et al review the indications and techniques for suprapatellar nailing of tibia fractures. They report that placing the knee in 20 degrees of flexion for suprapatellar nailing acts to neutralize the pull from the quadriceps muscle, thus decreasing the apex anterior deformity. They conclude that this technique can be used for Gustilo-Anderson Grade I-II tibial shaft fractures to help reduce the incidence of valgus and apex anterior malunions.
Figure A is the AP and lateral radiographs of a proximal third tibial shaft fracture. Blocking screws should be placed in positions B and C to help reduce the incidence of valgus and apex anterior malalignment.
Incorrect Answers:
Answers 1-2,4-5: Blocking screws should be placed in the concavity of the deformity to be prevented, thus positions B and C in this example.
Figures 1 and 2 are the radiographs of a 41-year-old diabetic male presenting with right lower extremity pain after cutting his leg it on a piece of rusty metal yesterday. Serial physical exam demonstrates rapid progression of the overlying erythema and worsening pain. In the emergency department, labs are significant for a C-reactive protein (CRP) of 180 mg/L, white blood cell (WBC) count of 19,000/mm3, glucose of 11 mmol/L, creatinine of 150 umol/L, and sodium of 120 mmol/L. He has a temperature of 102°F and a heart rate of 110 bpm. What additional laboratory value is needed to calculate this patient’s LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score?
1) ESR
2) Hemoglobin
3) Potassium
4) Bicarbonate
5) Calcium
The LRINEC score is based on the patient's serum CRP, WBC count, hemoglobin, sodium, creatinine, and glucose.
The LRINEC score is a clinical tool designed to help distinguish between necrotizing fasciitis and other soft tissue infections using these 6 key laboratory values. The most important of these is CRP, as a value >150 mg/L
contributes 4 of a possible 13 points. Illustration A demonstrates the scoring system for each laboratory value used in the calculation of the LRINEC score. A score >6 has been shown to have a PPV of 92% for having necrotizing fasciitis. The patient in this vignette already has a score of 10 without knowledge of the hemoglobin level, which is very concerning for necrotizing fasciitis. As a result, emergent surgical debridement is indicated.
Stoneback et al. reviews the presentation and management of necrotizing fasciitis. The authors note that the incidence of necrotizing fasciitis is between 500 and 1500 cases per year in the United States, and that the mortality rate averages 21.9%. They emphasize that necrotizing fasciitis may be difficult to distinguish from more common skin infections such as cellulitis or soft tissue abscess in its early stages but will often rapidly deteriorate, as illustrated in this vignette.
Wong et al. developed the LRINEC scoring system. In a retrospective review of 145 patients with necrotizing fasciitis and 309 patients with severe cellulitis or abscesses, they used their scoring system to demonstrate that a LRINEC score of 6 points or greater had a PPV of 92.0% and an NPV of 96.0%.
Tsai et al. challenged the utility of the LRINEC score in aiding in the diagnosis of Vibrio Necrotizing Fasciitis. In their retrospective review of 70 patients with Vibrio Necrotizing Fasciitis, they showed that only 11% of patients had a LRINEC score >6/. The authors concluded that the LRINEC scoring system is of more limited utility for this subset of the disease and propose that severe hypoalbuminemia, thrombocytopenia, and increased banded forms of leukocytes may have greater utility.
Figures A and B are AP and lateral radiographs of the lower leg demonstrating diffuse subcutaneous gas. This is concerning for necrotizing fasciitis.
Illustration A is a table showing the LRINEC scoring breakdown. A maximum total score of 13 could be achieved.
Incorrect Answers:
Answer 1: ESR is a non-specific measure of inflammation. While likely elevated with necrotizing fasciitis, it is not used to help calculate LRINEC score.
Answer 3: Hyperkalemia may occur with myonecrosis but potassium is not included in the LRINEC score calculation.
Answer 4: Acidosis may be seen in the setting of necrotizing fasciitis, but bicarbonate is not included in the LRINEC score calculation.
Answer 5: Calcium is not a component of the LRINEC scoring system.
A 35-year-old male presents to the emergency department following a motorcycle accident. On initial examination in the emergency department, he is found to have a left flail arm and multiple other injuries. There is a concern for a brachial plexus injury. What examination findings would support a diagnosis of a pre-ganglionic injury?
1) Abnormal histamine response
2) Flail arm
3) Intact sensory nerve action potentials (SNAPs)
4) Lateral scapular winging
5) Normal cervical paraspinal signal on EMG/NCV
Brachial plexus injuries are classified as either pre-ganglionic or post-ganglionic. A pre-ganglionic injury would be supported by intact sensory nerve action potentials (SNAPs).
Diagnosing brachial plexus injuries as either pre- or post-ganglionic is multi-faceted and begins with a thorough physical examination. Findings suggestive of a pre-ganglionic injury would include Horner Syndrome (due to disruption of the sympathetic chain), MEDIAL scapular winging resulting from rhomboid and serratus anterior paralysis, cervical paraspinal muscle weakness, absent sensation, and hemidiaphragmatic paralysis. CT myelography may demonstrate pseudomeningocele, and NCS/EMG would show intact sensory nerve action potentials (SNAPs) with denervation of the cervical paraspinal musculature. Finally, a histamine test would show a triple response, with redness, wheal, AND flare. Conversely, a post-ganglionic injury would be
supported by BOTH motor and sensory deficits of the flail arm, maintained innervation to cervical paraspinal muscles, and an abnormal histamine response test (redness and wheal with NO flare).
Limthongthang et al. reviews the common clinical findings associated with pre-and post-ganglionic injuries. The authors discuss the diagnostic algorithm, including a thorough history, physical examination, electrodiagnostic studies, and CT myelogram or MRI. They emphasize that an angiogram should additionally be considered given that 20% of brachial plexus injuries have associated major vascular injuries. The authors conclude with appropriate surgical timing and suggest potential treatments depending on injury location.
Giuffree et al. reviews management of brachial plexus injuries. The authors discuss appropriate timing of treatment based on the injury mechanism. They emphasize the priorities of functional restoration, beginning with elbow flexion, followed by a stable shoulder, and lastly intrinsic hand function. The authors present various surgical options to attain these goals and discuss their outcomes.
O'Shea et al. discusses the utilization of advanced imaging and electrodiagnostic testing for evaluation of brachial plexus injuries. The authors note the utility of CT myelogram toward identifying root avulsions. They also suggest that electrodiagnostic studies be obtained no sooner than 4 weeks following injury and subsequently at 6-week intervals to monitor progression. They note that SNAPs are the most important criteria in distinguishing between pre- and post-ganglionic injuries, and conclude that electromyographic studies are crucial in determining not only the level of injury but also donor nerves for transfers.
Incorrect Answer:
Answer 1: A normal “triple” response to intradermal injection of histamine involves erythema due to capillary dilation, wheal due to fluid extravasation from increased permeability, and flare due to arteriolar dilatation AND to axon reflex in sensory nerve. A response with a flare in an insensate area of skin suggest that the reflex arc is intact and that the lesion has to be proximal to the dorsal root ganglion. Conversely, when the lesion is post-ganglionic, the test will be “abnormal” (i.e. without the flare) as the continuity between the skin and dorsal root ganglion will have been interrupted.
Answer 2: A flail arm is characteristic of both pre- and post-ganglionic brachial plexus injuries, given that both involve absence of motor function.
Answer 4: Lateral scapular winging is not associated with a pre-ganglionic injury. Lateral winging characteristically results from trapezial pathology, which is associated with CN XI injury. Instead, MEDIAL scapular winging would be
indicative of a pre-ganglionic injury due to involvement of the dorsal scapular nerve (branching from the C5 root) and the long thoracic nerve (branching from the C5-7 roots).
Answer 5: Normal EMG/NCV results in the cervical paraspinal muscles would be indicative of a post-ganglionic injury.
A 47-year-old male diabetic has developed a calcaneal ulcer, as shown in figure A, that has been managed with wound care and a total contact cast. He presents to the emergency department with worsening erythema progressing up his leg with new draining wounds. On admission, despite antibiotics and intravenous fluids, he develops worsening pain and new bullae shown in Figure B. His laboratory studies indicate CRP >200, WBC 25k, Sodium 127, glucose 233, and hemoglobin 12. What is the best next step in the management of his condition?
1) Emergent vascular exploration
2) Upgrade level of care ICU with antibiotic escalation
3) MRI foot for osteomyelitis evaluation
4) Emergent surgical debridement including possible amputation
5) CT with contrast of lower extremity
This patient meets the clinical criteria for the diagnosis of necrotizing fascitis, therefore the next step in management is surgical debridement with possible amputation.
Necrotizing fasciitis is an aggressive infection with rapid spread along fascial planes. Initial presentation may be consistent with cellulitis; however, rapid progression along fascial planes may result in skin necrosis, muscular invasion, and subsequent myonecrosis. The rapidity of diagnosis and emergent surgical debridement is essential. Risk factors including intravenous drug abuse, alcohol abuse, and diabetes should be assessed, and if necrotizing fascitis is on the differential, the LRINEC score may be employed for diagnosis in equivocal cases. This scoring system can be found on our associated Orthobullets page.
Wong et. al. developed the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score to assist in early diagnosis of necrotizing soft tissue infections. The authors used logistic regression to identify significant predictors of necrotizing fasciitis. The score utilizes a total white cell count, hemoglobin, sodium, glucose, serum creatinine, and CRP. A LRINEC score of 6 points or higher has a positive predictive value of 92%, and below 6 points a negative predictive value of 96%. Importantly, ESR is not a component in the scoring system as it correlated poorly with risk. The patient presented already has two positive serum findings with an LRINEC score of 6.
Stoneback et al. review the diagnosis and management of necrotizing fasciitis. They note that Group A streptococcus is one of the most prevalent organisms, but infections are typically polymicrobial. Because of the need for prompt initiation of treatment, adjunctive diagnostic tests should not impede the timing of surgical exploration and debridement. Necrotizing fasciitis is a clinical diagnosis where only emergent surgical debridement and appropriate antibiotic treatment can prevent progression and death.
Tsai et al. retrospectively reviewed 70 patients with 71 episodes of Vibrio necrotizing fasciitis and sepsis. Of the 70 patients, 68 had a history of contact with seawater or raw seafood; 66 had underlying chronic diseases. They noted that severe hypoalbuminemia, severe thrombocytopenia, and increased banded forms of leukocytes are laboratory risk indicators of necrotizing fasciitis
that aid in pointing toward the initiation of early surgery and predict a higher risk of death.
Figure A is a clinical photograph of a calcaneal ulcer. Figure B shows ascending erythema and bullae consistent with a necrotizing skin infection. Illustration A demonstrates the LRINEC scoring system. The scoring system is not largely utilized as a screening tool due to its poor sensitivity in studies that attempted to validate it.
Incorrect answers:
Answer 1: There is no indication in this scenario that this patient's clinical picture is due to a vascular issue.
Answer 2: This patient will likely require ICU admission, but surgical debridement is most prudent.
Answers 3 and 5: Imaging studies can assist with the diagnosis, but advanced imaging takes valuable time and should not delay emergent surgical debridement. The incidence of gas in the subcutaneous tissues is only 13%, but its presence should trigger urgent debridement.
A 36-year-old man with HIV, chronic kidney failure, and chronic IV drug use presents with worsening fevers, chills, and purulent drainage from his leg. His infection progresses rapidly and he becomes acutely septic. He is therefore taken urgently to the OR for radical debridement of the fascia and surrounding tissues, with a plan for delayed closure. His CRP is 90 mg/dL and he is hyponatremic. Intraoperative cultures are obtained. To cover the most common organism(s) associated with this condition, what antibiotic would you initially recommend?
1) Intravenous vancomycin
2) Intravenous vancomycin and gentamicin
3) Intravenous gentamicin
4) Intravenous linezolid and meropenem
5) Intravenous micafungin
This patient with lower extremity necrotizing fasciitis underwent a radical debridement of fascia and surrounding tissues. The most common culture isolate from necrotizing fasciitis is polymicrobial, which should be the target of initial antibiotic treatment. Of the above options, intravenous Linezolid and Meropenem would be an acceptable empiric therapy as Linezolid would cover MRSA and invasive group A Streptococcus while Meropenem would cover gram-positive/negative anaerobic coverage and enteric organisms.
Necrotizing fasciitis is an aggressive infection with rapid spread along fascial planes. While the initial presentation may suggest cellulitis, rapid progression along fascial planes may result in skin necrosis and subsequent myofascial necrosis. The time from admission to debridement has been shown to be a significant predictor of outcomes. Immediate empiric antibiotics covering
polymicrobial species including aerobic, anaerobic, gram-positive and gram-negative bacteria are of equal importance.
Stoneback et al. reviewed the diagnosis and management of necrotizing fasciitis. They reported that while most necrotizing fasciitis infections are polymicrobial, group A Streptococcus remains one of the more prevalent organisms in isolation. They recommended surgical debridement as the utmost importance in necrotizing fasciitis management and emphasized appropriate antibiotic selection in treating sepsis and halting the further bacterial spread.
Wong et al. developed the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score, a novel diagnostic scoring system for distinguishing necrotizing fasciitis from other soft tissue infections based on laboratory tests routinely performed for the evaluation of severe soft tissue infections. This score allocated 1 point each to the following labs: total white cell count, hemoglobin, sodium, glucose, serum creatinine, and C-reactive protein. They reported that a cutoff value of 6 points had a positive predictive value of 92.0% and a negative predictive value of 96.0%, and concluded that the LRINEC score is a powerful score that can detect even clinically early cases of necrotizing fasciitis.
Tsai et al. investigated whether clinical indicators predict laboratory findings during the initial stages of necrotizing fasciitis and the relationship between the LRINEC score and the diagnosis of vibrio infection. They reported that a systolic blood pressure of 90mmHg or less at the time of admission predicted mortality and that patients with a LRINEC score of >6 had an 11% chance of surviving vibro-specific necrotizing fasciitis.
Figure A is a clinical image depicting necrotizing fasciitis of the lower extremity, with characteristic ischemic patches, cutaneous gangrene, dermal induration, bullae formation. Illustration A is a table from Wong's study that demonstrates the components, clinical values, and scoring system for the LRINEC score.
Scores of 6 or greater are highly concerning. They concluded that severe hypoalbuminemia, severe thrombocytopenia, and increased leukocytosis were reliable markers.
Incorrect Answers:
Answer 1: While intravenous Vancomycin would cover MRSA and aggressive streptococcus species, it would not cover gram-negative anaerobic organisms. Answer 2: This patient has chronic kidney failure, which would be worsened by 2 antibiotic agents that are known to be nephrotoxic.
Answer 3: Intravenous Mentamicin alone would not cover the gram-positive organisms.
Answer 5: Intravenous Micafungin would cover fungal organisms, but would fail to cover bacteria.
A 27-year-old male is involved in a motor vehicle collision and presents to the ER with the right lower extremity injury shown in Figures A and B. He undergoes immediate closed reduction and the post-reduction CT is shown in Figures C and D. The patient undergoes percutaneous surgical screw fixation of the injury. At 2 years followup, he presents with a supination deformity with decreased eversion of the foot at rest. Radiographs reveal no evidence of talus subchondral sclerosis or collapse. Which of the following is the most likely cause of the finding in this patient?
1) Avascular necrosis
2) Subtalar arthritis
3) Tibiotalar arthritis
4) Varus malunion
5) Planovalgus
The patient has sustained a displaced talar neck fracture with medial comminution which requires open reduction and internal fixation to restore anatomic alignment. The patient has likely sustained varus malunion which is a common deformity noted with non-anatomical reduction leading to hindfoot supination and decreased eversion.
Talar neck fractures, while uncommon, can lead to significant morbidity in the ambulatory patient. Treatment of these injuries requires prompt reduction due to the tenuous blood supply to the talus. The most common complications noted after a talar neck fracture are avascular necrosis, subtalar arthritis, tibiotalar arthritis, and varus malunion. A talus varus malunion generally occurs due to medial talar neck comminution and/or non-anatomic reduction of the injury. This deformity can lead to decreased eversion and a supination deformity causing patients to ambulate on the lateral aspect of the foot. These malunions are generally treated with a medial opening wedge osteotomy.
Fortin and Balazsy review the pathology and treatment of traumatic talus fractures. They cite that injuries to the head, neck, or body of the talus can result in permanent pain, loss of motion, and deformity. They note that failure to recognize fracture displacement (even when minimal) can lead to undertreatment and poor outcomes. They conclude that unrecognized medial talar neck comminution can lead to varus malunion and a supination deformity with a decreased range of motion of the subtalar joint.
Lindvall et al. performed a retrospective review to evaluate the long-term results (average of 74-month followup) of surgical treatment of isolated, displaced talar neck and/or body fractures with stable internal fixation in 25 patients. They noted an overall union rate of 88% regardless of surgical timing. The authors noted posttraumatic subtalar arthritis in all patients (100%) and talus osteonecrosis in 13/26 (50%) of patients. The authors concluded that a delay in surgical fixation does not appear to affect the outcome, union, or prevalence of osteonecrosis and that posttraumatic arthritis is a more common complication than osteonecrosis following operative treatment.
Figures A and B are the Lateral and AP radiographs of a displaced talar neck fracture with tibiotalar dislocation. Figures C and D are the post-reduction sagittal foot CT cuts that reveal a displaced talar neck fracture with medial
comminution.
Incorrect Answers:
Answer 1: The patient does not have any radiographic signs of avascular necrosis according to the vignette.
Answer 2: Subtalar arthritis is the most common complication following talar neck fractures but the clinical appearance of the patient's foot is due to varus malunion.
Answer 3: Tibiotalar arthritis is a common complication following talar neck fractures but the clinical appearance of the patient's foot is due to varus malunion.
Answer 5: A planovalgus foot is unlikely to occur after a talus fracture, furthermore a planovalgus foot would lead to a pronation deformity.
Figures A-C are a 32-year-old female who presents to the trauma bay after falling off a roof. Paramedics state that she was initially complaining of back pain, but she now appears irritable and lethargic. She has received 2 liters of crystalloid since arriving in the trauma bay. Her blood pressure is now 76/42. A Foley catheter is placed, and her urine output is 12 ml/hour. What additional finding would suggest hemorrhagic shock over neurogenic shock?
1) Tachycardia
2) Bradycardia
3) Decreased cardiac output
4) Vasodilation
5) Warm dry skin
This patient sustained a multi-traumatic injury and is suffering from hemorrhagic shock. The presence of tachycardia would favor the diagnosis of hemorrhagic shock over neurogenic shock.
In initial hypovolemic shock (stage I,
A 32-year-old inebriated male falls from a mechanical bull at a bar and sustains a closed displaced intra-articular distal radius fracture. He presents to your clinic and given his age and the fracture characteristics, he is taken for open reduction with volar locking plate
fixation. After completing instrumentation, radiocarpal screw penetration is best assessed on which fluoroscopic view?
1) Extended wrist tangential view
2) Flexed wrist tangential view
3) PA anatomic tilt view
4) Radial inclination view
5) Standard lateral view
While no single radiographic view can completely rule out intra-articular screw penetration, radial inclination views (most commonly a 22-degree anatomic tilt lateral view) best demonstrates screw penetration of the radiocarpal joint.
Intra-articular screw penetration is a potential complication of distal radius fracture fixation. Due to the complex native geometry, standard PA and lateral fluoroscopic views are not effective in evaluation of the joint reduction, screw length or screw position. For this reason, various supplemental views have been described to facilitate identification of articular incongruity as well as dorsal or intra-articular penetration of screws, either into the radiocarpal or distal radioulnar joint.
Tweet et al. reviewed the most commonly used imaging techniques and views for the evaluation of intra-articular screw penetration during volar plate fixation of distal radius fractures. Of nearly 700 ASSH members surveyed, 87% relied exclusively on fluoroscopy, three-quarters (74%) of which implemented tilt views or rotational fluoroscopy. Cadaveric analysis supported use of a 22-degree lateral projection and rotational fluoroscopy as adjuncts for the detection of intra-articular screw penetration. They concluded that no combination of imaging effectively allowed the detection of all intra-articular screws.
Patel et al. evaluated the utility of supplemental radiography in assessing screw placement in distal radius fracture fixation using volar locking plates. The authors found that supplementation of the standard AP and lateral views with lateral tilt views significantly increased accuracy and confidence.
Specifically, more acute angles (15 and 23-degree views) provided better visualization of ulnar screws while larger angles (30 degrees) allowed assessment of more radial-sided distal plate screws.
Illustration A is an example of an extended wrist tangential view showing clear visualization of the sigmoid notch and distal radioulnar joint (DRUJ), with intraarticular penetration of the DRUJ shown on the left and extra-articular screws
free of the DRUJ.
Illustration B is an example of a flexed wrist tangential view, or “skyline” view, demonstrating no dorsal penetration of the screws, which can be obscured on a true lateral due to Lister’s tubercle.
Illustration C shows an example of a standard PA view (left) and 11-degree anatomic tilt PA view, allowing better visualization of the articular surface. Illustration D shows a standard true lateral view (left) and 22-degree radial inclination lateral view (right), allowing better visualization of screw relationship to the radiocarpal joint.
Incorrect Answers:
Answer 1: The extended wrist tangential view, or “sigmoid notch” view, has been described as a technique by which intra-articular penetration of the sigmoid notch can be evaluated.
Answer 2: The flexed wrist tangential view, or “skyline” view, best demonstrates dorsal screw penetration.
Answer 3: The PA anatomic tilt view is an 11-degree anatomic tilt view that best demonstrates the degree of articular congruity of the joint surface.
Answer 5: The standard lateral view can demonstrate the position of a volar plate with respect to the watershed line but has limited utility in evaluating radiocarpal screw penetration due to radial inclination.
When considering operative intervention for the injury shown in Figures A and B, which of the following factors has the LEAST correlation with complication rate?
1) Skin integrity
2) Age
3) Smoking status
4) Peripheral neuropathy
5) Diabetes
In patients with an unstable ankle fracture, age has not shown to have an effect on complication rate.
An increasing number of elderly patients retain an active lifestyle with high functional demands. Cast immobilization for highly unstable ankle fractures (especially inherently unstable pronation-abduction fractures that are frequently seen in the elderly) leads to malunion or nonunion rates between 48% and 73%. Therefore, in the absence of severe comorbidities, the principal indications for surgery should not differ from those in younger patients.
Herscovici et al. evaluated 243 elderly patients with high-energy foot and ankle injuries, 73 of which had ankle fractures, who underwent surgical fixation.
They report on their preferred approach to treatment of these patients. Their article does not report on any outcome variables but states that, in their expert opinion, elderly patients should be considered for operative intervention as a young patient would.
Pagliaro et al. analyzed outcomes after surgical treatment of unstable ankle fractures in 23 patients who were at least 65 years old. They found that open reduction and internal fixation of unstable ankle fractures in geriatric patients is an effective treatment that leads to a complication rate comparable to the general population.
Figure A and B demonstrate AP and lateral radiographs of a trimalleolar ankle fracture.
Incorrect Answers:
Answer 1, 3-5: All of these factors lead to an increased risk of complications for unstable ankle fractures.
Which of the following statements is true regarding the outcomes when using a high-pressure pulse lavage irrigation system versus
simple low-pressure bulb irrigation for the treatment of the open fracture shown in Figure A?
1) It is more cost effective when including the cost of reoperation
2) There is an increased rate of associated nerve injury
3) There is an increased rate of primary wound healing problems
4) There is increased rate of infection
5) There is no difference in union rates
There is no difference in union rates when either high-pressure (pulse lavage) or low-pressure (bulb) irrigation with saline is used for open tibia fractures.
The mainstay of early treatment of open fractures includes debridement and irrigation along with IV antibiotics. Multiple trials have looked at the most efficacious and cost-effective irrigation method both in terms of the type of solution and irrigation method. With regard to the irrigation method, recent studies have shown simple bulb irrigation has the same union rate as more expensive high-pressure pulse lavage systems. With regard to the type of solution, recent studies have shown castile soap actually leads to a decreased rate of primary wound healing problems as compared using an irrigation solution with antibiotics.
Bhandari et al. in the FLOW study (Fluid Lavage of Open Wounds), a multicenter randomized trial demonstrated that the rates of reoperation were similar regardless of irrigation pressure, a finding that indicates that very low pressure is an acceptable low-cost alternative for the irrigation of open fractures.
Anglen et al. demonstrated that the use of a nonsterile liquid soap additive (castile soap) was at least as effective as the use of bacitracin with regards to the rate of postoperative infection and fracture healing, but showed a significant decrease in problems with soft-tissue healing.
Bhandari et al. as a follow up by the FLOW group in the study above analyzed 2551 patients to look for risk factors for reoperation. The rates of reoperation were similar regardless of irrigation pressure, a finding that indicates that very low pressure is an acceptable low-cost alternative for the irrigation of open fractures. The reoperation rate was higher in the castile soap group than in the saline group.
Figure A is a clinical photograph demonstrating a Type IIIB open tibia fracture. Incorrect Answers:
Answers 1: The high-pressure irrigation system is more expensive and has not
been shown to decrease reoperation rates.
Answer 2: There is not a higher risk of nerve injury with high-pressure irrigation.
Answer 3: There has been no difference in regards to wound healing problems when comparing high and low-pressure irrigation.
Answer 4: No difference in postoperative infection has been found, regardless of high or low-pressure irrigation.
A 71-year-old man presents after 9 months of functional bracing for a closed right humeral shaft fracture. Current radiographs are shown in Figure A. Infectious workup was negative. Appropriate next steps in evaluation will most likely reveal which of the following?
1) Vitamin D deficiency
2) Low testosterone
3) Iron deficiency
4) Thyroid deficiency
5) Magnesium deficiency
Metabolic/endocrinologic workup for an atrophic nonunion following appropriate treatment for a humeral shaft fracture is likely to reveal a vitamin D deficiency.
Nonunion of the humeral shaft occurs approximately 10% of the time following open or closed treatment. In the case of nonunion, there is likely a lack of mechanical and biologic factors. Biologic workup for nonunion should include ruling out infection followed by an evaluation for metabolic and endocrine abnormalities.
Brinker et al. reviewed 37 low-energy fractures that went on to nonunion. These patients were evaluated by clinical endocrinologists for evaluation of metabolic abnormalities. Thirty-one of the 37 patients (84%) had a metabolic issue, with 68% (25 of 37 patients) having a Vitamin D deficiency. They conclude any patient with a nonunion should be referred to an endocrinologist for metabolic screening and treatment.
Kuo et al. looked at the compliance of 155 patients treated for osteoporosis
shortly after sustaining a fragility fracture. They found 47% had a prior fracture with only 26% having a prior BMD and 15% on calcium and vitamin D. They concluded that osteoporotic treatment provided at the time of fracture leads to long-term compliance in 90% and 73% of osteoporotic and osteopenic patients, respectively.
Figure A shows a radiograph of the right humerus demonstrating a nonunion of a humeral shaft fracture. Illustration A shows postoperative radiograph after open reduction internal fixation with compression plating.
Incorrect Answers:
Answer 2: Low testosterone would be possible given the patient demographics but would not be included in the appropriate next steps in the evaluation of this nonunion.
Answer 3: Iron deficiency may be present but would not be the next best laboratory study in evaluating a nonunion.
Answer 4 & 5: Metabolic and endocrinologic workup is the next appropriate step; however, thyroid and magnesium deficiencies are less common than a vitamin D deficiency.
A 62-year-old woman falls off a bike and sustains the injury shown in Figure A. She presents to clinic for her 6-month follow-up appointment and reports persistent pain. Current imaging is shown in Figure B. Which of the following factors is not a risk factor to the development of this patient’s diagnosis?
1) Shortening of 3cm
2) Comminution
3) Sling immobilization as opposed to figure-of-eight brace
4) Female gender
5) Advanced age
This patient presents with a symptomatic non-union of a midshaft clavicle fracture (classic "z-type" fracture for it's shape), which is not associated with type of immobilization (sling vs. figure-of-eight brace).
Clavicle fractures treated non-operatively are at risk for complications such as non-union, poorer cosmesis, and decreased shoulder strength and endurance. The risk of non-union, in particular, ranges from 1-5% and has been shown to increase with shortening > 2cm, comminution, female gender, and advanced age. Open reduction internal fixation of clavicle fractures has also shown to have increased union rates compared to those treated non-operatively but
presents its own risks such as hardware complications and infections.
Robinson et al. performed a prospective observational cohort study to evaluate the prevalence of and risk factors for non-union of clavicle fractures treated non-operatively. They found that the risk of non-union was significantly increased by advancing age, female gender, displacement of the fracture, and the presence of comminution.
Lazarides et al. performed a retrospective study to determine the relevance of shortening and clinical outcomes for midshaft clavicle fractures treated nonoperatively. They found that final clavicular shortening of > 18mm in male patients and of > 14mm in female patients was significantly associated with an unsatisfactory result.
The Canadian Orthopaedic Trauma Society performed a multicenter prospective randomized clinical trial to compare outcomes of clavicle fractures treated non-operatively versus operatively with plate fixation. They found that operative fixation of a displaced clavicular shaft fracture results in improved functional outcome and a lower rate of malunion and nonunion compared with nonoperative treatment at one year of follow-up.
Figure A is an AP radiograph demonstrating a displaced midshaft clavicle fracture. Figure B is an AP radiograph demonstrating non-union of a midshaft clavicle fracture.
Incorrect Answers:
Answers 1, 2, 4, 5: Each of these factors is associated with an increased risk of non-union.
Which of the following statements about polytrauma and organ failure is most correct when comparing children to adults?
1) Adults have a more robust initial inflammatory response, affecting the pulmonary system first
2) Adults have a dampened immune response, affecting all organ systems simultaneously
3) Adults have a more robust initial inflammatory response, affecting all organ systems simultaneously
4) Children have a more robust initial inflammatory response, affecting all organ systems simultaneously
5) Children have a dampened immune response, affecting the pulmonary system first
Adults have been shown to have a robust initial inflammatory response that affects the pulmonary system first.
There is a difference in the systemic response to trauma between children and adults. Children initially have a dampened systemic immune response. They do, however, have a robust local inflammatory response that causes organ failure and affects all organ systems simultaneously. Adults have a robust systemic response with organ failure occurring 2-3 days after injury. The pulmonary system is usually the first organ system affected in adults.
Wood et al. performed a review of the inflammatory response to injury in children. They found that the inflammatory response to injury in children is functionally and mechanistically unique. The incidence of multi-organ failure in children is rare, but affects all organ systems simultaneously when it does occur.
Pandya et al. performed a review of the pediatric polytrauma patient. They report that the orthopaedic surgeon plays an important role in managing hemodynamic instability, vascular insult, and neurologic damage in the child with multiple injuries. They recommend that, if surgical fixation is deemed urgent in the pediatric patient, it can be performed in the early period of multi-system insult.
Incorrect Answers:
Answers 2 & 3: Adults initially have a robust, systemic inflammatory response. When organ failure does occur, the pulmonary system is usually the first affected.
Answers 4 & 5: Children initially have a dampened systemic inflammatory response. When organ failure occurs, it affects all organ systems simultaneously.
A 63-year-old patient presents with right ankle pain after a fall down four stairs. Figures A and B are the radiographs of the injury. The patient reports a history of diabetes mellitus type 2 and peripheral neuropathy with a most recent hemoglobin A1c of 9.8. The injury is
reduced and placed in a well-padded bivalved cast. The patient is then discharged with outpatient follow-up without DVT prophylaxis. Twelve weeks later, the patient presents to the clinic for the first time in the same bivalved cast. The has remained non-weight bearing and the bottom of the cast confirms this. What is the expected outcome at this point?
1) Charcot arthropathy
2) Diabetic foot ulcer
3) Deep vein thrombosis
4) Elevation of A1c
5) Fracture displacement
The patient is a diabetic with poorly controlled blood sugar and peripheral neuropathy presenting with a bimalleolar ankle fracture with a loss to follow-up for 3 months. All of the answer choices are potential complications with nonoperative treatment, but fracture displacement is the most likely to occur.
Ankle fractures in diabetic patients are associated with increased complications compared to nondiabetic counterparts. The glycation damage to cellular
components as well as the decreased blood flow with microangiopathic changes results in substantially decreased bone healing. Patients diabetic comorbidities, such as retinopathy, nephropathy, vasculopathy, and neuropathy have a higher rate of wound complications, deep infections, malunion, nonunion, and Charcot arthropathy. Due to the delayed healing, surgical treatment with supplemental fixation is recommended.
Lovy et al. performed a retrospective review of 28 diabetic ankle fractures with 20 patients being treated nonoperatively and 8 patients treated operatively initially. Nonoperative treatment was associated with a 21-fold increase in complication risk. Delayed surgery (>3 weeks from injury) for nonunion or malunion was associated with greater complications than immediate ORIF. The authors concluded that nonoperative treatment for diabetic ankle fractures was associated with unacceptably high consequences.
Wukich et al. reviewed the treatment of ankle fractures in diabetic patients. Nonoperative treatment was recommended as a viable option for nondisplaced isolated unimalleolar and stable ankle fractures. Additionally, they proposed diabetic patients without diabetic comorbidities can be surgically treated with standard internal fixation constructs as they have similar outcomes. Finally, despite surgical treatment having a higher rate of complications than nondiabetic patients, operative management is more likely to result in a functional lower extremity in displaced and unstable ankle fractures.
Chaudhary et al. performed a review of ankle fractures in diabetic patients and concluded that diabetic ankle fractures are at high risk for fracture displacement and delayed union, even with surgical treatment. The authors recommend supplemental fixation with external fixation or multiple syndesmotic screws. Postoperatively patients should undergo prolonged immobilization, 2-3 times that of nondiabetics.
Figure A demonstrates an AP radiograph of a bimalleolar ankle fracture. Figure B demonstrates a lateral radiograph of a bimalleolar ankle fracture.
Incorrect Answers:
Answer 1: Charcot arthropathy occurs in diabetic ankle fractures, especially in neuropathic patients treated nonoperatively and with delayed treatment.
However, fracture displacement is more likely to occur.
Answer 2: Diabetic foot ulcers are a potential complication, especially in neuropathic patients. However, with a well-padded cast and the patient adhering to non-weight bearing recommendations, this is not as likely as fracture displacement.
Answer 3: Deep vein thrombosis is a potential complication of fractures in the
lower extremity, but the risk is typically higher in surgically managed patients. Answer 4: Non-operative treatment of ankle fractures in diabetic patients has not been associated with increases in A1c. However, with non-weight bearing activities the patient is likely to have poorer control of blood glucose, but the incidence of this has not been characterized.
Regarding Syme amputations, which of the following is true?
1) It does not require a patent tibialis posterior artery
2) It is dependent on a stable heel pad
3) It is less energy efficient than a midfoot amputation
4) The primary complication is an equinus deformity
5) It is also known as a hindfoot amputation
Syme amputations rely on a stable heel pad.
Syme amputations, or ankle disarticulations, are the most proximal type of ankle/foot amputations but are more energy efficient than midfoot amputations. A successful Syme amputation requires a patent tibialis posterior artery and a stable heel pad. The two most common problems are skin sloughing from a compromised vascular supply and migration of the heel pad due to instability. A hypermobile heel pad can cause difficulty with prosthesis wear and damage to the soft tissues, eventually leading to failure.
Finkler et al. performed a retrospective study on the long-term outcomes of Syme amputations. They found that patients who underwent Syme's ankle disarticulation amputation appeared to fare better than similar patients with transtibial amputations. These patients required less rehabilitation and achieved improved levels of functional independence as demonstrated by patient-reported outcome measures.
Pinzur et al. performed a retrospective study on Syme ankle disarticulation in patients with diabetes. They found that patients managed with a Syme ankle disarticulation had better ambulatory function and survival compared to transtibial amputations. They concluded that the results of this retrospective review support the value of Syme ankle disarticulation in diabetic patients with infection or gangrene.
Illustration A is an example of a Syme amputation.
Incorrect Answers:
Answer 1: Syme amputations require a patent tibialis posterior artery. Answer 3: Syme amputations are more energy efficient than midfoot amputations.
Answer 4: Equinus deformites are not a complication of Syme amputations. Answer 5: Syme amputations are also known as ankle disarticulations, not hindfoot amputations.
A 65-year-old patient, who is a current smoker, presents with left hip pain after a fall from standing height and is unable to bear weight. The patient's radiograph is shown in figure A. The use of a sliding hip screw construct has been shown to have what benefit compared to multiple cannulated screws?
1) Decreased fracture shortening
2) Decreased non-union rate
3) Decreased implant failure
4) Lower reoperation rates
5) Lower rate of avascular necrosis
The patient is a current smoker presenting with a left displaced basicervical femoral neck fracture. The use of a sliding hip screw (SHS) in this fracture pattern in patients that are current smokers has been associated with decreased reoperation rates compared to multiple cannulated screws (MCS).
Femoral neck fractures are highly morbid injuries and are the most expensive fractures to treat. Treatment options include MCS fixation, SHS, hemiarthroplasty, and total hip arthroplasty. Hemiarthroplasty is preferred in the low demand and elderly population. In younger patients with higher activity levels, reduction and internal fixation with MCS or SHS provide bone-preserving treatment options. Total hip arthroplasty is preferred in patients
>65 years of age with higher activity levels.
The Fixation using Alternative Implants for the Treatment of Hip fractures
study group (FAITH) performed a multicenter randomized control trial that included 1108 patients treated with either dynamic SHS or MCS. Fixation with SHS was associated with increased rates of avascular necrosis compared to MCS, 9% vs 5%, but was not significant. Overall, there were no differences in reoperation rates or union rates between the two groups. However, subgroup analysis revealed lower reoperation rates with SHS in displaced fractures, basicervical fractures, and in current smokers.
Zielinski et al. 2013 performed a subanalysis of 76 patients from the FAITH study examining femoral neck shortening, WOMAC scores, gait analysis, and hip muscle strength in patients treated for femoral neck fractures. Increased fracture shortening was observed with increased patient weight, age, and higher Pauwel's classifications. There was no comparison between implant type and gait outcomes.
Lee et al. 2008 performed a retrospective review of femoral neck fractures in 90 patients undergoing either minimally invasive SHS, MCS, or conventional SHS. The authors found that conventional DHS was associated with significantly larger incisions, greater blood transfusion requirements, and longer hospital stays compared to minimally invasive SHS and MCS. The authors recommended minimally invasive SHS due to lower soft tissue complications.
Figure A demonstrates an AP hip radiograph with a right femoral neck fracture. Illustration A depicts an SHS implant providing internal fixation for a femoral neck fracture. Illustration B depicts MCS fixation of a femoral neck fracture.
Incorrect Answers:
Answer 1: Fracture shortening has not been found to occur at lower rates with SHS or MCS.
Answer 2: Non-union rates are not significantly different between the two fixation methods.
Answer 3: Implant failure has not occurred differently between SHS and MCS. Answer 5: Avascular necrosis in the FAITH was found to occur at a higher rate in the SHS group, but this finding was not significant.
Which of the following will most likely result with the use of a fracture table when treating the injury shown in Figures A and B?
1) Internal malrotation deformity
2) External malrotation deformity
3) Recurvatum deformity
4) Varus deformity
5) Valgus deformity
The fracture table has been shown to induce an internal malrotation deformity when it is used for treating femoral shaft fractures.
Intramedullary nailing with reaming of the bone and static locking of the nail is the treatment of choice for femoral shaft fractures in adults. The fracture table has been used with excellent results. Compared to manual traction, the fracture table provides an advantage as only one assistant is necessary.
However, it may limit access to the patient if other body areas are injured. Additionally, the fracture table has been shown to induce an internal malrotation deformity, which results from internally rotating the limb to facilitate access to the starting point and to improve visualization of the hip in the lateral plane. Rotation may also be difficult to assess clinically once the limb is positioned and draped.
Kelly et al. performed a retrospective study to determine complications associated with the use of the fracture table in pediatric femoral fractures.
They found 8 palsies related to positioning. They also found that patients who developed nerve palsies were significantly heavier. They ultimately concluded that the fracture table is safe for fixation but every effort should be made to minimize time in traction to avoid iatrogenic nerve palsy, particularly in heavier children (> 80 kg).
Stephen et al. performed a randomized study comparing the fracture table and manual traction when nailing femoral shaft fractures. They found that internal malrotation was significantly more common when the fracture table was used. Operative time was also greater for the fracture table group. There were no other differences in complications. They concluded that manual traction is an effective technique that decreases operative time and improves the quality of reduction.
Figures A and B are AP radiographs demonstrating a femoral shaft fracture. Incorrect Answers:
Answers 2, 3, 4, & 5: Internal malrotation has been shown to be a risk when
using a fracture table to treat femoral shaft fractures by intramedullary nailing.
A 35-year-old patient is involved in a motor vehicle collision and sustains multiple injuries, including an APC pelvis fracture. He is stabilized following placement of a pelvic binder and receiving blood products as part of a massive transfusion protocol. He is subsequently taken to radiology for radiographs and a chest, abdomen, and pelvis CT with 4mm cuts. What effect will these modalities have on the radiographic appearance of his pelvis fracture and what further intervention should be performed?
1) Make the injury look more severe; obtained radiographs with the binder removed
2) Make the injury look less severe; perform fluoroscopic examination under anesthesia
3) Accurate representation of injury severity; no further studies needed
4) Make the injury look less severe; repeat CT with 0.625 mm cuts
5) Make the injury look more severe; obtain Judet views of the pelvis
Application of a pelvic binder and CT scans prior to standard AP pelvis radiographs results in an underestimation of pelvic ring injury severity. Since this patient was hemodynamically unstable and required a massive transfusion,
removal of the pelvic binder is not recommended and further injury stability should be evaluated by fluoroscopic examination under anesthesia.
Pelvic ring fractures are high energy injuries that usually follow motor vehicle collisions. There is a high rate of hemodynamic instability with these injuries due to the increase in pelvic volume and abundant venous bleeding. Proper identification of injury severity in the initial evaluation is crucial to ensure appropriate definitive treatment. Ideally, if the patient is hemodynamically stable, AP pelvis radiographs without a pelvic binder have been found to be effective at identifying unstable pelvic injuries.
Fagg et al. performed a retrospective study of 97 patients presenting with pelvic ring fractures requiring operative stabilization. The authors found that 7% of patients that initially had binder-on imaging were found to have unstable fractures that were not identified on the original images. The authors suggested that pelvic CT scans with the binder on are insufficient in determining the severity of pelvic fractures.
Swartz et al. performed a retrospective study of 43 patients presenting with pelvic ring fractures that received AP pelvic radiographs, pelvic binder, pelvic CT, and fluoroscopic stress examination in sequential order. They found that pre-binder radiographs had a greater sensitivity at detecting unstable fractures than pelvic CT with a binder. The authors concluded that placement of a binder prior to imaging can underestimate the severity of the pelvic injury and in cases where a binder is placed prior to imaging a fluoroscopic examination under anesthesia can be useful in detection.
Gibson et al. performed a retrospective review of 72 patients that presented with pubic diastasis requiring internal fixation. The authors found that pelvic CT scans without a pelvic binder underestimated the diastasis by 6.6mm compared to AP pelvic radiographs. The authors recommend obtaining radiographs prior to performing a CT, as underestimation of pubic diastasis can alter definitive management decisions.
Incorrect Answers:
Answer 1: Placement of a pelvic binder prior to radiographs and early CT scans underestimate the severity of pelvic ring injuries. In this case, the patient is hemodynamically unstable and removing the binder would likely result in increased pelvic bleeding by destabilizing clots.
Answer 3: The CT scan with the binder in place will underestimate the injury severity in this patient. In order to provide proper definitive care, the severity of the injury must be determined.
Answer 4: The current study has underestimated the degree of pelvic
instability. However, decreasing the cut thickness on CT will be unlikely to better determine the degree of pelvic ring instability.
Answer 5: The current injuries are underestimated by the current image study regimen with binder placement. Judet views, especially with the binder in place, will not enhance the detectability of pelvic ring instability.
A 26-year-old male with a BMI of 37 is involved in a motor vehicle collision and requires extrication. During evaluation in the trauma bay, he becomes hemodynamically unstable and is found to have the injury shown in Figure A, as well as an associated bladder injury. Which of the following statements regarding the patient's injury is true?
1) His male gender places him at a lower risk for post-operative infection
2) His BMI places him at a higher risk for post-operative infection
3) The mechanism of his injury was likely a lateral compression force
4) The internal pudendal artery is the most likely source of arterial hemorrhage
5) Pelvic binder placement is contraindicated in this patient given his bladder injury
The patient has an APC pelvis injury. Increased BMI has been associated with a higher risk of infection after surgical intervention of pelvic and acetabular fractures.
Pelvic fractures result from high-energy mechanisms and frequently require surgical intervention. When performing open procedures in the pelvis, the risk of infection is of concern. Elevated BMI has been shown to be the most
important risk factor for infection. Other risk factors include prolonged operative time, prolonged ICU stay, increased red blood cell transfusions, leukocytosis, Morel-Lavallée lesion, and associated genitourinary and abdominal trauma. Preoperative angioembolization as a risk factor for SSI remains controversial but is thought to be associated with embolization and not with angiography itself.
Iqbal et al. performed a retrospective study on surgical site infection following fixation of acetabular fractures. They found that prolonged operation time, increased BMI, prolonged ICU stay, larger amount of packed red blood cell transfusions, and associated genitourinary and abdominal trauma were associated with surgical site infection following acetabular fracture fixation.
They concluded that measures should be undertaken to attenuate the chances of surgical site infection in this major surgery by considering the risk factors significantly associated with it.
Sagi et al. performed a retrospective study on the risk for deep postoperative wound infection after pelvic and acetabular surgery. They found that obesity, obesity plus leukocytosis, and preoperative angioembolization were strong predictors of postoperative infection.
Firoozabadi et al. performed a retrospective study to evaluate the impact of pelvic embolization on postoperative infection rate after acetabular fracture fixation. They found that, despite previous reports of high infection rates after pelvic embolization, the deep infection rate was only 4% after embolization in their cohort. They therefore state that concerns for higher rates of infection are not substantiated, and pelvic embolization should be performed when indicated.
Figure A is an AP radiograph of the pelvis demonstrating symphyseal widening and left SI joint widening.
Incorrect Answers:
Answer 1: Gender has not been found to affect the risk of post-operative infection.
Answer 3: The patient's mechanism of injury was likely an anterior-posterior compression force, not a lateral compression force.
Answer 4: The superior gluteal artery is the most likely source of arterial hemorrhage in patients with APC pelvic fractures, while the internal pudendal artery or obturator artery is the most likely source of hemorrhage in patients with LC pelvic fractures.
Answer 5: Urogenital injury is not a contraindication for pelvic binder placement.
A 70-year-old female with a history of osteoporosis complains of vague left hip pain. She does not complain of right hip pain. Her imaging is shown in Figures A & B. What is the next best step in treatment?
1) Observation and pain control
2) Bone scan
3) Intramedullary nailing of the left femur
4) Intramedullary nailing of bilateral femurs
5) Referral to an orthopaedic oncologist
This patient has bisphosphonate-related changes of her femurs. Given that the left side is the only symptomatic side, it should be prophylactically nailed.
Bisphosphonates have been implicated in causing atypical low-energy femur fractures. Radiographic clues for this impending injury include lateral cortical thickening (beaking), varus remodeling of the femur, and increased diaphyseal cortical thickness. When a fracture occurs, it usually occurs in the subtrochanteric region. The fracture patterns are usually transverse or short-oblique in orientation. There is also a lack of comminution. The ideal treatment for these injuries is an intramedullary nail, ensuring to restore native alignment and avoiding varus.
Vasikaran performed a review of low-energy femoral fractures with prolonged bisphosphonate use. He reported that long-term bisphosphonate therapy is thought to lead to profound suppression of bone turnover, increased
microdamage accumulation, and alteration of bone tissue mineral properties as well as possibly bone tissue composition by altering collagen cross-linking, all of which can in turn cause brittleness of bone and propensity to fracture with minimal trauma. He concludes that, if a patient becomes symptomatic or sustains a fracture, the cessation of bisphosphonate therapy should be considered. If a fracture has not occurred and the patient is having prodromal symptoms, prophylactic intramedullary nailing should be performed.
Balach et al. performed a review on atypical femur fractures associated with disphosphonate use. They report that following the diagnosis of a complete or impending atypical femur fracture, discontinuation of diphosphonates is recommended to help promote a more favorable fracture healing environment. They conclude that surgical treatment should allow endochondral fracture healing such as an intramedullary nail.
Figures A and B are AP radiographs of the left and right proximal femurs demonstrating lateral cortical beaking, cortical thickening, and mild varus remodeling.
Incorrect Answers:
Answer 1: Observation and pain control is not appropriate in this case as the patient has an impending fracture.
Answer 2: A bone scan is not necessary in this case as the diagnosis can be made from radiographs.
Answer 4: Intramedullary nailing of both sides is not necessary at this time as the right side is asymptomatic.
Answer 5: Referral to an orthopaedic oncologist is not necessary for treating these injuries.
A 26-year-old male recreational basketball player sustained an ankle injury 6 months prior. He continues to complain of ankle pain and instability. Current imaging is shown in Figures A & B. Imaging of the proximal fibula is unremarkable and there is little concern for syndesmotic injury. What is the next best step in treatment?
1) Open reduction and internal fixation (ORIF) with autograft
2) Fragment excision
3) Obtain stress radiographs
4) Physical therapy and management of symptoms
5) Percutaneous skeletal fixation
This patient sustained a medial malleolar fracture that went on to nonunion. The next best step in treatment would be ORIF with autograft.
Historically, nonunion rates for malleolar fractures are somewhere between 5 and 30%. Nonunion following rotationally unstable ankle fractures can have detrimental effects on patient outcomes, leading to continued debilitating pain, instability, and late posttraumatic osteoarthritis. Patients with symptomatic nonunion should have surgical treatment. Fragment excision may be possible in patients with small distal fractures. However, if the fragment is large and well-preserved, ORIF with bone graft augmentation is the treatment of choice.
Khurana et al. performed a study to evaluate the outcomes following operative treatment of nonunited rotational distal fibula and medial malleolar fractures. They identified 17 patients. All patients were treated with open reduction with plate and screw fixation or screw fixation alone. Adjunctive grafting was performed in all but 2 cases. They found that after a mean of 33.9 months all nonunions had resolved. They conclude that patients who have surgery for nonunion will have outcomes similar to patients who undergo surgery for acute ankle fractures.
Capogna and Egol wrote a guide regarding the treatment of nonunions after malleolar fractures. They report that most medial malleolar nonunions are addressed by fixation with partially threaded cancellous screws. They suggest that osteopromoting materials or bone graft should be added before reduction. They conclude that fixation with two partially-threaded screws is sufficient for reliable fracture healing.
Figure A is an AP radiograph demonstrating a medial malleolar nonunion. Figure B is a coronal CT slice demonstrating a medial malleolar nonunion. Illustrations A and B are AP and lateral radiographs, respectively, demonstrating a medial malleolar nonunion that has been stabilized with 2 cannulated screws. Bone graft augmentation was also performed. Illustrations C and D are AP and lateral radiographs, respectively, demonstrating a healed medial malleolar nonunion.
Incorrect Answers:
Answer 2: Fragment excision is not appropriate in this case as the fragment is large and well-preserved.
Answer 3: Stress radiographs are unnecessary in this case as the patient is symptomatic and the diagnosis is made with the available imaging.
Answer 4: Non-operative treatment of symptomatic malleolar nonunions is not recommended.
Answer 5: Percutaneous skeletal fixation in the presence of a nonunion is not recommended as the fracture site cannot be debrided and it will not be possible to augment with bone graft.
A 76-year-old left-handed female presents to your office after a fall with the injury seen in Figure A. When treating this fracture with hemiarthroplasty, which of the following is the most important for a successful outcome?
1) Anatomic healing of the tuberosities
2) Stem retroversion of 25 degrees
3) Surgical fixation within 24 hours
4) Anterior superior labral repair
5) Age over 75
When performing a hemiarthroplasty for a displaced four-part proximal humerus fracture, the best predictor of a successful outcome is anatomic healing of the tuberosities.
Although most proximal humerus fracture can be treated nonoperatively, especially in elderly low-demand patients, some debate remains regarding the use of a hemiarthroplasty vs. reverse total shoulder arthroplasty. When performing a hemiarthroplasty for a displaced four-part proximal humerus fracture, it is of the utmost importance to achieve a stable and anatomic reduction of the tuberosities. Studies have shown malpositioned or migrated tuberosities leads to stiffness, weakness, and persistent pain. Restoration of humeral height and version is also important for successful outcomes of hemiarthroplasty.
Rangan et al., in the PROFHER trial, studied the outcomes of patients with displaced proximal humerus fractures treated with surgical vs. nonsurgical intervention. Of note, in the surgical group, 83% of patients were treated with ORIF, 9% were treated with hemiarthroplasty, and the remainder were treated with some other fixation method. They found no difference at 2 years between the surgical and nonsurgical groups with regard to outcome scoring, complications from surgery or nonoperative care, secondary surgery, new therapy requirement, or mortality. They concluded the current increase in surgery in patients with displaced proximal humerus fractures is not supported by this data.
Boileau et al. followed 66 patients with displaced proximal humerus fractures treated with hemiarthroplasty to evaluate for clinical and radiographic parameters that could lead to worse outcomes. They found that 50% of patients had malpositioning of the greater tuberosity, which correlated with unsatisfactory results, superior migration of the prosthesis, stiffness or weakness, and persistent pain. They concluded that the primary goal of arthroplasty for proximal humerus fractures should be obtaining anatomic tuberosity healing.
Figure A shows a displaced four-part proximal humerus fracture. Incorrect Answers:
Answer 2: Although appropriate retroversion is important for optimal function,
anatomic healing of the tuberosities is felt to contribute more to successful outcomes.
Answer 3: Surgical timing has not been reported to be associated with improved outcomes in this fracture pattern.
Answer 4: Anterior superior labral repair would not be indicated and would be of little benefit in this setting.
Answer 5: Age over 75 has been shown to predict worse tuberosity healing as subsequent worse outcomes.
A 25-year-old man sustains a left leg injury during a motorcycle accident. A radiograph is provided in Figure A. The fracture is treated in a minimally invasive manner with a lateral locking plate and percutaneous screw fixation. A post-operative radiograph is provided in Figure B. Which of the following complications has been associated with this fixation construct?
1) Compartment syndrome
2) Common peroneal nerve injury
3) Superficial peroneal nerve injury
4) Deep peroneal nerve injury
5) Popliteal artery injury
Figures A and B demonstrate pre and post-operative radiographs of a comminuted proximal tibia fracture treated with a long locking plate. Compartment syndrome is a significant complication associated with this fracture. However, there is no greater risk of compartment syndrome with use of this specific construct plate. Long lateral locking plates have been shown to put the superficial peroneal nerve at risk with insertion of distal locking screws. Use of a larger incision and careful dissection down to the plate in this region may minimize the risk of damage to the nerve.
Deangelis et al performed a cadaveric study evaluating 14 extremities and the relationship between the superficial peroneal nerve to the percutaneous screws of the 13-hole proximal tibia Less Invasive Stabilization System (LISS) plate.
The average distance from the superficial peroneal nerve to the center of holes 11, 12, and 13 was 10.0 mm, 6.8 mm, and 2.7 mm, respectively. In 12 of 14 legs (86%), the superficial peroneal nerve was 5.0 mm or less from the center of hole 13.
Cole et al reviewed his experience of 77 proximal tibia fractures treated with the LISS plate. He reported a high rate of union (97%) with only 2 infections, 2 nonunions, 1 nerve palsy, and 8 patients with an angular malunion approaching 10 degrees.
A 48-year-old male returns to your office 8 months after sustaining a proximal humerus fracture that was successfully treated nonoperatively. However he is still having persistent anterior shoulder/arm pain that worsens with most activities. He has not done any physical therapy nor received a corticosteroid injection. What nerve innervates the structure identified by the red arrow in Figure A, what is its primary function, and where does it originate from?
1) Subscapular nerves, shoulder internal rotation, ventral scapula
2) Musculocutaneous nerve, elbow pronation, coracoid
3) Axillary nerve, shoulder external rotation, dorsal scapula
4) Musculocutaneous nerve, elbow supination, supraglenoid tubercle
5) Suprascapular nerve, shoulder abduction, dorsal scapula
The figure demonstrates a rupture of the long head of the biceps brachii (LHB). The biceps primarily supinates the elbow via innervation from the musculocutaneous nerve.
The long head of the biceps originates in the shoulder at the supraglenoid tubercle, traverses through the bicipital groove, forms the muscle belly of the biceps brachii with the short head from the coracoid process. This then inserts distally onto the radial tuberosity in the proximal radius. This consistent anatomy allows it to be used as an anatomical reference during repair of comminuted proximal humerus fracture patterns.
Tosounidis et al. compared the histological appearance of LHB tendons from individuals undergoing hemiarthroplasty for proximal humerus fractures to control cadaveric specimens. They noted a significant rate of degenerative lesions within the LHB in the fracture cohort. They use this as a basis for performing tenotomy/tenodesis of the LHB during fracture surgery.
Soliman et al. performed a prospective randomized trial of individuals undergoing shoulder hemiarthroplasties who either received an LHB tenodesis or it was neglected. They reported improved Constant and PRO scores for those who received a tenodesis while there was no strength difference noted. Based on this they concluded biceps tenodesis during hemiarthroplasty is indicated.
Nho et al. reviewed the pathology and management of biceps pathology. They note the LHB can be the primary isolated pathologic process but more often LHB lesions are in conjunction with other intra-articular pathology. Various methods exist do address biceps pathology, ranging from simple tenotomy to open or arthroscopic tenodesis.
Figure A is a fluid-sensitive axial MR sequence with the arrowhead pointing to the LHB within the groove.
Incorrect Answers:
Answer 1: This describes the subscapularis muscle. Answer 2: The biceps is responsible for elbow supination. Answer 3: This describes the teres minor muscle.
Answer 5: This describes the supraspinatus muscle.
A 23-year-old-male was involved in a motorcycle accident. Imaging is shown in Figure A. In order to prevent the most common deformity associated with intramedullary nailing of this injury, where should blocking screws be placed and what deformity are they trying to prevent?
1) Lateral and posterior to the nail in the proximal segment; procurvatum and valgus
2) Medial and posterior to the nail in the proximal segment; procurvatum and varus
3) Lateral and posterior to the nail in the proximal segment; recurvatum and varus
4) Medial and anterior to the nail in the proximal segment; recurvatum and valgus
5) Anterior and posterior to the nail in the proximal segment; recurvatum
When using intramedullary nails (IMNs) for treatment of proximal tibia fractures, blocking screws can be used to prevent the typical deformity of valgus and apex anterior. Traditionally, these blocking screws are placed lateral and posterior to the nail in the proximal segment.
Proximal tibia fractures have a tendency to displace into valgus and procurvatum due to deforming forces from the pes anserinus and anterior compartment (valgus) and patellar ligament (procurvatum). It is difficult to correct or prevent this mal-alignment with IMN insertion alone due to the capacious nature of the proximal tibial metaphysis compared to the canal fit of
the IMN in the diaphyseal segment. Blocking screws placed lateral and posterior to the nail have been found to prevent this translation by effectively decreasing canal space for the intramedullary device. In the proximal tibia, a good "rule of thumb" is to place the blocking screws on the concavity of the deformity in the metaphyseal segment; however blocking screws are not only used this way.
Krettek et al. performed a study to evaluate the mechanical effects of medial and lateral blocking screws in supplementing intramedullary nail fixation of high proximal and low distal tibia fractures treated with small-diameter intramedullary nails. They found that the addition of a medial blocking screw in the proximal tibia increased the deformation of the construct. They conclude that medial blocking screws can increase the primary stability of proximal metaphyseal fractures after nailing. This study exemplifies the use of blocking screws not only to help achieve alignment when treating a fracture but also maintain the alignment during fracture healing when the IMN is not canal-fitting around a fracture site.
Another study by Krettek et al. evaluated the clinical use of blocking screws as a supplement to stability after fixation with statically locked intramedullary nails in metaphyseal fractures. They prospectively studied 21 tibial fractures, 10 in the proximal third and 11 in the distal third. They found that losses of reduction were minimal when using blocking screws. They also had no complications related to the use of blocking screws. They conclude that blocking screws are a useful adjunct when nailing metaphyseal fractures of the tibia.
Figures A and B are AP and lateral radiographs of the tibia and fibula, respectively, demonstrating proximal tibia and fibula fractures. Illustrations A and B are AP and lateral images of the same injury, respectively, treated with an intramedullary nail. Note the use of blocking screws lateral and posterior to the nail.
Incorrect Answers:
Answers 2, 3, 4, & 5: Blocking screws are typically used to "block" the IMN from creating or fixing a mal-reduction. In this case, they should be placed lateral and posterior to the nail to prevent a valgus and apex anterior deformity.
Which of the following distal radius fractures is associated with volar translation of carpus relative to the radial articulation?
1) Displaced impaction fracture of the lunate fossa
2) Displaced intra-articular fracture with a fragment consisting of the volar-ulnar corner
3) Displaced radial styloid fracture
4) Displaced extra-articular fracture with apex volar
5) Displaced extra-articular fracture with apex dorsal
A displaced intra-articular fracture with a fragment containing the critical volar-ulnar corner rim of the distal radius would result in volar translation of the carpus.
Distal radius fractures are one of the most common orthopedic injuries and can result from low-energy trauma in older and osteoporotic patients or high-energy trauma in young patients. Intra-articular involvement poses treatment
challenges for these fractures as the fragments are crucial to articular stability and are difficult to achieve fixation with traditional distal radius plates.
Fractures with intra-articular comminution of the distal radius that involve either the dorsal or volar rim of the lunate fossa, which can destabilize the radiocarpal joint, can lead to volar or ulnar translation of the carpus.
Orbay et al. performed a retrospective review of patients undergoing either hook plate fixation or volar opening wedge osteotomy for volar marginal fragment distal radius fractures. For the patients treated with hook extension plates, there was a 90% success rate in the prevention of volar subluxation of the carpus. For patients that required volar open wedge osteotomy to redistribute joint loading forces in those that developed avascular necrosis of the volar marginal fragments, all patients had improved pain, function, and radiographic concentric reduction of the radiocarpal joint. They concluded that hook plate fixation provides an effective means of fixation of a volar marginal fracture of the distal radius with volar opening wedge osteotomy as an effective salvage procedure.
O'Shaughnessy et al. performed a retrospective study of hook plate fixation of distal radius fractures with volar marginal rim fragments. There were no patients in the study that lost fixation of the volar marginal fragments after treatment with hook plates with the most common complication being symptomatic hardware requiring removal of both the traditional plate and the hook plate. The authors concluded that hook plate fixation provides a highly effective means of distal radial fragment fixation that is not amenable to traditional plate fixation.
Illustration A depicts a lateral radiograph of the right wrist with a fracture of the volar-ulnar corner resulting in volar translation of the carpus. Illustration B depicts a lateral radiograph of the wrist with a ulnar hook plate buttressing an articular surface rim fracture.
Incorrect answers:
Answer 1: Impaction fractures of the lunate fossa do not result in translational instability of the carpus.
Answer 3: A radial styloid fracture can result in ulnar translation of the carpus if the fragment is large enough to involve the large radiocarpal stabilizing ligaments.
Answer 4: An extra-articular fracture of the distal radius with apex volar angulation may have dorsal comminution, but there is no added risk of volar carpal translation.
Answer 5: An extra-articular distal radius fracture with apex dorsal angulation
leads to volar tilting of the articular surface, but there is no volar translation of the carpus.
Which of the following acetabular fractures is classified as an elementary fracture pattern that involves two columns?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure B is a radiograph of a transverse acetabular fracture, which is the only elementary fracture pattern that involves two columns.
The acetabulum consists of two columns arranged in an inverted Y-shaped configuration. Fractures are divided into five elementary patterns and five associated patterns. Elementary fractures involve only one fracture plane or surface while associated fractures involve multiple fracture planes or surfaces. The transverse fracture is the only elementary pattern that involves two
columns. Six fundamental landmarks of the acetabulum must be evaluated on each AP pelvic radiograph: the lateral border of the anterior wall; the lateral border of the posterior wall; the acetabular roof, representing the weightbearing dome; the teardrop; the ilioischial line, representing the posterior column; and the iliopectineal line, representing the anterior column or pelvic brim.
Mauffrey et al. performed a review of the radiographic evaluation of acetabular fractures. They report that plain radiographs remain the initial step in the classification of acetabular fractures. The ability to accurately interpret the injury allows the surgeon to develop a thorough preoperative plan and to evaluate the quality of the reduction and fixation intraoperatively. Though CT and three-dimensional imaging is obtained in addition to radiographs, radiographs still have a vital role to play in the diagnosis and treatment of acetabular fractures.
Durkee et al. performed a study to characterize and classify the radiographic and CT appearance of common acetabular fractures. They report that for a transverse fracture, there is no involvement of the obturator ring. It causes disruption of both the iliopectineal and ilioischial lines, however. On CT, this fracture line is sagittally oriented. It is transverse relative to the plane of the acetabulum.
Figures A-E are AP radiographs of the pelvis demonstrating an associated both column (ABC) acetabular fracture, a transverse acetabular fracture, a posterior wall acetabular fracture, a T-type acetabular fracture, and a normal pelvis, respectively. Illustration A is an image demonstrating normal acetabular lines and morphology on the right and a transverse acetabular fracture on the left.
Illustration B is an algorithm to determine acetabular fracture patterns (Mauffrey et al.).
Incorrect Answers:
Answers 1, 3, 4, & 5: The transverse acetabular fracture is the only elementary pattern to involve two columns.
A 90-year-old patient presents after a fall down a flight of stairs and sustains a hip fracture, several rib fractures, a right pneumothorax, a right grade 1 open humerus fracture, and a subdural hematoma. The patient requires intubation in the trauma bay. The trauma team assesses the Injury Severity Score to 36. Which factor is associated with the highest risk of mortality at 1-year?
1) Presence of a head injury
2) The need for mechanical ventilation
3) Injury severity score greater than 25
4) Presence of a hip fracture
5) Presence of an open fracture
The patient is a nonagenarian presenting with multiple injuries after trauma. The need for mechanical ventilation is associated with the highest risk of mortality at 1-year with 78.7% risk.
Geriatric patients pose different treatment challenges in the trauma setting compared to patients under the age of 65. The treatment course is complicated by many medical comorbidities, polypharmacy, lower physiologic reserve, and increased risk of medical complications. Several factors have been described as predictors of mortality in admission including the presence of a head injury, the need for mechanical ventilation, higher Injury Severity Score (ISS), and treatment at a facility other than a trauma center. Of these factors, the need for mechanical ventilation has the highest association with mortality, especially at 1-year.
Hwabejire et al. performed a retrospective study of mortality predictors in trauma patients greater than 90 years of age. The in-hospital mortality was significantly associated with Injury Severity Score, cervical spine injury, and the need for mechanical ventilation with an overall in-hospital mortality rate being 9.5%. At 1-year, mortality rates were increased to 78.7% if the patient required mechanical ventilation at the time of admission. The authors concluded that despite the low in-hospital mortality these risk factors are strong predictors to 1-year from the injury.
Mock et al. performed a retrospective cohort study investigating the predictors of mortality in geriatric trauma patients. The found through multivariate analysis that the need for mechanical ventilation, admission lactate, and the length of mechanical ventilation were significant predictors of mortality. They stipulated that the need for mechanical ventilation is a predictor of mortality, but this finding is confounded with the withdrawal of care.
Meldon et al. performed a retrospective cohort study looking at outcomes and care settings of trauma patients over the age of 80. The authors reported a significantly higher mortality rate with treatment performed at acute care hospitals compared to level 1 and level 2 trauma centers. Additionally, mortality was associated with increased ISS and decreased Glasgow Coma Score. They concluded that treatment at a trauma verified center as a survival benefit for geriatric trauma patients.
Incorrect answers:
Answer 1: The presence of a head injury at the time of admission does increase the mortality risk at 1-year, with one study citing 51.1%.
Answer 3: An injury severity score greater than 25 has been associated with increased mortality at 1-year, but several studies have linked the need for
mechanical ventilation to greater mortality risk. One study reported 73.2% mortality at 1-year in patients with ISS greater than 25.
Answer 4: The effect of a hip fracture in geriatric trauma patient mortality has not been characterized, but 1-year mortality risk is approximately 30%.
Answer 5: The mortality risk of an open fracture in a geriatric trauma patient has been seldom studied, but some authors report risks similar to geriatric hip fractures.
What is the spur sign and on which view is it best seen?
1) Intact ilium; obturator oblique
2) Intact ilium; iliac oblique
3) Posterior wall fragment; iliac oblique
4) Posterior wall fragment; obturator oblique
5) Posterior wall fragment; oburator inlet
The spur sign represents the intact posteroinferior aspect of the ilium that is seen in an associated both column (ABC) acetabular fracture. It is best seen on the obturator oblique view.
The spur sign is the portion of nonarticular ilium above the acetabulum that becomes visible on the obturator oblique view with medial displacement of the acetabulum. Nondisplaced associated both-column fractures will not have a spur sign on the obturator oblique view. Computed tomography should be used to verify the continuity between the axial skeleton and the acetabular articular surface.
Mauffrey et al. performed a radiographic evaluation of acetabular fractures. They report that, when evaluating acetabular fractures, CT scans are useful because they allow the clinician to trace an intact strut of bone from the sacroiliac joint to the weight-bearing dome of the acetabulum. If a piece of bone is not present in continuity between the sacroiliac joint and the acetabulum, the fracture must be an associated both-column fracture. If a spur sign is not present and a continuous bony bridge between the sacroiliac joint and the acetabulum is present, the fracture is classified as an anterior column posterior hemitransverse fracture.
Kellam and Messer performed a study to assess acetabular joint congruity and postoperative reconstructions. They evaluated the use of coronal and sagittal
reconstruction of transaxial CT scans. They found in all cases of marginal impaction coronal and sagittal CT reconstruction showed that the fragments were larger than they appeared to be on the transaxial CT scan. They conclude that coronal and sagittal CT reconstruction provided more detailed evaluations of complex fractures than other studies.
Illustration A is an electronically simulated image demonstrating an associated both column acetabular fracture on the left side. Illustration B is an obturator oblique of the same image with the spur sign indicated by the arrow.
Incorrect Answers:
Answers 2, 3, 4, & 5: The spur sign is a portion of the intact ilium that is best seen on the obturator oblique view. It is indicative of an associated both column fracture.
An errant screw is placed during the procedure shown in Figure
A. What is the most likely physical exam manifestation?
1) Weakness in knee extension
2) Weakness in ankle plantarflexion
3) Weakness in great toe extension
4) Numbness over the medial aspect of the leg
5) Numbness over the posterior leg
The most likely location for an errantly placed screw is anterior. This would lead to injury in the L5 nerve root, which would manifest with weakness in great toe extension.
Indications for iliosacral screw fixation include complete sacral fractures (i.e. fractures that extend through the sacrum in its entirety, anterior to posterior), sacroiliac joint disruptions, and combinations of these posterior pelvic injuries following reduction. The safe zone for screws is the area within the sacrum where the screws remain within the bone. The L5 and S1 nerve roots course from the spinal canal in an anterior-lateral-caudal and oblique direction. The L5 nerve root is located on the anterior-cranial sacral alar surface and may be injured by an errant screw that is placed too anteriorly. The S1 nerve root is located within the oblique neural tunnel, beginning at the spinal canal and exiting through the anterior sacral foramina between the upper and second sacral segments.
Kaiser et al. performed a study to evaluate anatomic determinants of sacral dysmorphism and implications for safe screw placement. They found the prevalence of upper sacral segment dysplasia at 41%. The major determinants of sacral dysmorphism are upper sacral segment coronal and axial angulations. They developed a sacral dysmorphism score, derived with the equation: (first sacral coronal angle) + 2(first sacral axial angle). They conclude that the sacral dysmorphism score quantifies dysmorphism and can be used in preoperative planning of IS screw placement.
Miller and Routt performed a review of variations in sacral morphology and
implications for iliosacral screw fixation. They report that knowledge of the posterior pelvic anatomy, its variations, and related imaging is critical to performing reproducibly safe surgery. They report that the dysmorphic pelvis has several key characteristics. The upper portion is colinear with the iliac crests on the outlet view. Mamillary bodies (underdeveloped transverse processes) may be present as well. A residual upper sacral disk may be present along with an acute alar slope. They conclude that the surgeon must be knowledgeable about individual patient anatomy to ensure safe iliosacral screw placement.
Figure A is an illustration of a sacroiliac-style iliosacral screw. Illustration A is an inlet fluoroscopic image demonstrating the drill within the sacrum with an arrow indicating the location of the L5 nerve root. Illustration B is an axial CT of a patient with normal sacral anatomy through the first sacral and second sacral segments, respectively. Illustration C is an axial CT of a patient with dysmorphic sacral anatomy through the first sacral and second sacral segments, respectively. The L5 nerve roots are indicated by the white circles.
Incorrect Answers:
Answer 1: Weakness in knee extension would indicate injury to the L4 nerve root.
Answer 2: Weakness in ankle plantarflexion would indicate injury to the S1 nerve root.
Answer 4: Numbness to the medial leg would indicate injury to the L4 nerve root.
Answer 5: Numbness over the posterior leg would indicate injury to the S1 nerve root.
During which surgical approach to the acetabulum is the sciatic nerve placed at risk, and how should the patient be positioned to minimize the risk of injury?
1) Kocher-Langenbeck; hip extended and knee extended
2) Kocher-Langenbeck; hip extended and knee flexed
3) Kocher-Langenbeck; hip flexed and knee extended
4) Ilioinguinal; hip extended and knee extended
5) Ilioinguinal; hip extended and knee flexed
The sciatic nerve is placed at risk when performing the Kocher-Langenbeck approach to the acetabulum. Positioning the patient with the hip extended and the knee flexed minimizes the risk of injury to the sciatic nerve.
During the surgical fixation of acetabular fractures through a Kocher-Langenbeck approach, the sciatic nerve is placed at risk. It can be injured during the internal fixation of acetabular fractures, as well as during plate fixation and retractor placement. The sciatic nerve is maintained in the least
tension by keeping the hip extended and the knee flexed.
Isaak et al. published a review on sciatic nerve injuries associated with acetabular fractures. They reported that sciatic nerve injuries may occur as a result of the initial acetabular trauma (posttraumatic), as a result of iatrogenic trauma during surgery (perioperative), or as a later complication of surgery (postoperative). Iatrogenic injuries, in particular, can result from: (1) a stretch injury due to excessive retraction of the posterior gluteal muscle mass with the hip in flexion or continuous extension of the ipsilateral knee, (2) placement of retractors or reduction clamps in the lesser or greater sciatic notch, or (3) drilling or placing screws into the greater sciatic notch.
Fassler et al. performed a study on functional outcomes of sciatic nerve injuries after a displaced acetabular fracture. They found that all but one patient had a satisfactory (fair or better) functional outcome, but 11 patients had residual neurological sequelae that ranged from minor paresthesia to footdrop. They also found that the patients who had isolated mild involvement of the peroneal nerve had a favorable prognosis, but those who had a severe injury of the peroneal component, whether it was isolated or associated with an injury of the tibial component, did not recover good function.
Incorrect Answers:
Answers 1 and 3: The sciatic nerve is maintained in the least tension when the hip is extended and the knee is flexed.
Answers 4 and 5: The femoral and lateral cutaneous femoral nerves, not the sciatic nerve, are at risk of injury when performing the ilioinguinal approach to the acetabulum.
A 59-year-old patient presents with right elbow pain after a fall off a ladder. There is swelling of the elbow with a visible deformity. The patient is neurovascularly intact with decreased sensation in the ring and small fingers. The patient states that this has been present for several years. Figures A and B are radiographs of the right elbow. What is the most appropriate treatment that provides the greatest construct rigidity and appropriately addresses the patient's ulnar nerve symptoms?
1) Bicolumnar orthogonal plating with submuscular transposition
2) Bicolumnar parallel plating with all distal screws passing through a plate and in situ cubital tunnel release
3) Bicolumnar parallel plating with all distal screws passing through a plate and observation of ulnar neuropathy
4) Bicolumnar orthogonal plating with in situ cubital tunnel release
5) Interfragmentary screw fixation of the articular surface with neutralization plating and subcutaneous transposition of the ulnar nerve
The patient is presenting with a H-type distal humerus fracture with previous cubital tunnel symptoms. The biomechanically strongest treatment option would include bicolumnar parallel plating following the fixation objectives of O'Driscoll and a cubital tunnel release to address the ulnar nerve symptoms.
Distal humerus fractures are potentially complex fractures that require special fixation considerations when performing open reduction and internal fixation. The fixation objectives of O'Driscoll state that every screw should pass through a plate, each screw should be as long as possible, engaging as many articular fragments as possible, screws from each plate should interdigitate, and that compression is achieved in both columns through the supracondylar region and shaft. Studies have demonstrated that parallel plating provides the greatest construct rigidity than orthogonal plating. Bicolumnar parallel plating has been found to have significant greater biomechanical strength and rigidity compared to orthogonal plating, but clinical differences between the two plate types are minimal to absent. In the setting of chronic cubital tunnel syndrome, an in situ ulnar nerve decompression should be performed at the time of open reduction and internal fixation.
Cobb et al. performed a retrospective study of elderly patients, with a mean age of 72 years, undergoing a primary total elbow arthroplasty for distal humerus fractures. The authors reported there to be excellent outcomes in 75% of patients at 3.3 years according to the Mayo elbow performance score with the mean range of motion being 25-130 degrees and only one implant requiring revision. The authors concluded that total elbow replacement is an effective option for severely comminuted distal humerus fractures in elderly patients, but is not recommended in younger patients.
Taylor et al. performed a biomechanical cadaveric study testing for construct rigidity and strength between parallel and orthogonal distal humeral plating. They found the parallel plating had greater external and internal torsional rigidity, flexion and extension bending rigidity, and bend to failure strength. They concluded that parallel plating was a significantly stronger construct that
may be desirable in the treatment of comminuted distal humerus fractures.
Shearin et al. performed a meta-analysis comparing ulnar nerve decompression to ulnar nerve transposition during surgical treatment of distal humerus fractures. The pooled data in their analysis revealed an overall 19.3% incidence of ulnar nerve neuropathy with a 15.3% incidence with an in situ release and 23.5% incidence with ulnar nerve transposition. They concluded that transposition of the ulnar nerve did not have a protective effect against post-operative neuropathy, but there could have been a confounding effect of increased fracture severity observed in this group.
In a current concepts review in the Journal of Hand Surgery, Fajolu et al. propose that a transposition should only be performed at the conclusion of the case if the surgeon feels that the previously released nerve is in contact with the hardware or if the surgeon feels that there was excessive traction on the nerve during the case.
Figures A and B depict an AP and lateral radiograph of the elbow with a severely comminuted bicolumnar distal humerus fracture. Illustrations A and B depict the postoperative radiographs with bicolumnar plating following the fixation objectives of O'Driscoll.
Incorrect answers:
Answer 1: Parallel plating provides the greater biomechanical construct rigidity than orthogonal plating. Submuscular transposition is indicated if there is subluxation of the ulnar nerve or recurrence of cubital tunnel release.
Answer 3: Observation of chronic ulnar neuropathy is not recommended since these symptoms are likely to worsen after open reduction and internal fixation if not addressed.
Answer 4: Parallel plating provides the greater biomechanical construct rigidity than orthogonal plating.
Answer 5: Use of interfragmentary lag screws that are not passing through a plate is not part of the fixation objectives of O'Driscoll.
A 35-year-old female fell while riding a motorcycle and sustained the left elbow injury shown in Figures A and B. Figures C and D are the CT scan and 3D reconstruction of the injury. After closed reduction, the elbow is unstable with valgus stress at 40 degrees of flexion. What is the most appropriate definitive treatment?
1) Radial head ORIF and MCL repair
2) Radial head replacement and LUCL repair
3) Radial head excision, coronoid ORIF, and LUCL repair
4) Radial head replacement, coronoid ORIF, and LUCL repair
5) Radial head excision and LUCL repair
The patient has a terrible triad injury of the elbow, which will require a radial head replacement, coronoid ORIF, and lateral ulnar collateral ligament (LUCL) repair.
Terrible triad injuries are the result of a radial head fracture, a coronoid tip fracture, and a posterior elbow dislocation. The structures damaged with this injury pattern begins with the disruption of the LUCL, then the anterior capsule, and possibly the medial collateral ligament. Treatment involves ORIF of the radial head if 40% articular involvement. Repair of the LUCL to the humeral insertion is required in most cases. Coronoid fractures result from avulsion of the anterior capsule and usually involve small bone fragments.
Tejwani et al. reviewed the management of fractures of the radial head and neck. The authors recommended performing an open reduction and internal fixation when fractures of the radial head involve three or fewer pieces. Radial head excision is not recommended when there is associated elbow dislocation or ligamentous instability.
Acevedo et al. reviewed the current literature on implant designs for radial head arthroplasty (RHA). Loose-fitting prostheses settle to a level of anatomic stability over time and have low complication rates. Press-fit stems obtain intramedullary fixation through hoop stresses. However, implants with plasma-sprayed titanium stem have been associated with increased revision rates because of subsequent loosening. Bipolar prostheses consist of a press-fit stem that articulates with a polyethylene head component at the head and neck junction and is associated with increased dislocation rates, especially in the setting of a terrible triad injury. Understanding the prosthesis design of radial head implants is necessary to ensure good outcomes following terrible triad injuries.
Wyrick et al. reviewed the management of complex elbow dislocations. The literature suggests terrible triad injuries should be urgently closed reduced to avoid potential neurovascular injuries and splinted in 90 degrees flexion to confer a stable reduction until operative management. The recommended sequence of repair begins with lasso fixation of the coronoid, followed by fixation or replacement of the radial head, and then repair of the LUCL.
Figures A and B are AP and lateral radiographs of the left elbow with a terrible triad injury and comminution of the radial head. Figure C is the sagittal CT scan of the ulnohumeral joint demonstrating a coronoid fracture. Figure D is
the 3D CT reconstruction of the elbow with comminution of the radial head and a type 2 fracture of the coronoid.
Incorrect answers:
Answer 1: The patient has a comminuted fracture of the radial head that would require an RHA rather than an ORIF. MCL is less likely than a LUCL injury.
Answer 2: The patient sustained a coronoid fracture with greater than 10% involvement, which should be addressed with ORIF.
Answers 3 and 5: Radial head excision should never be performed in the setting of elbow instability.
A 35-year-old male sustains the injury shown in Figure A. He is currently not cleared for surgery due to a severe head injury. At what time point after the injury is there an increased risk of a poor outcome?
1) 48 hours
2) 5 days
3) 1 week
4) 2 weeks
5) 3 weeks
This patient has sustained an anterior column acetabular fracture. Delay of fixation for more than 3 weeks is associated with difficulty in achieving adequate reduction and poor outcomes.
Historically earlier treatment of acetabular fractures has been shown to improve clinical and functional outcomes. Delays of more than 3 weeks have been associated with difficulty obtaining an anatomic reduction and decreased overall patient outcomes. An increased delay has not been shown to increase the chances of neurological injury, infection, or heterotopic ossification.
Plaisier et al. performed a study to evaluate the effect of the timing of fixation for acetabular and pelvic ring fractures on patient outcome. They found that early fixation of acetabular fractures was associated with a decreased total length of stay. Functional outcome was improved in early fixation of acetabular fractures with a greater proportion of patients being discharged home rather than to rehabilitation or skilled care. They conclude that patients with early repair of acetabular fractures had significantly less organ dysfunction and exhibited improved functional outcome.
Madhu et al. performed a retrospective case review to determine if the time to surgery was predictive of radiological and functional outcomes of acetabular fractures. For elementary fractures, an increase in the time to surgery of one day reduced the odds of an excellent/good functional result by 15% and of an anatomical reduction by 18%. For associated fractures, the odds of obtaining an excellent/good result were reduced by 19% and an anatomical reduction by 18% per day. They conclude that the time to surgery is a significant predictor of radiological and functional outcome for both elementary and associated displaced fractures of the acetabulum.
Figure A is an AP pelvis demonstrating a displaced fracture of anterior column. Incorrect Answers:
Answers 1, 2, 3, & 4: Delay of fixation for more than 3 weeks is associated
with difficulty in achieving adequate reduction and poor outcomes.
A 43-year-old male presents to the trauma bay with the injury sustained in Figure A after a motor vehicle collision. After appropriate resuscitation, you have decided to proceed with open reduction and internal fixation via a Kocher approach and percutaneous fixation of the anterior column. The inlet view can be used to help visualize which of the following during guidewire placement?
1) Anterior-posterior position of the wire within the ramus
2) Ensure appropriate reduction of the fracture
3) Cranial-caudal position of the wire
4) Rule out joint penetration of the wire
5) Ensure the wire is within the tables of the ilium
An inlet view of the anterior pelvis can be used to help visualize the anterior-posterior position of the guide-wire in reference to the ramus during the placement of an anterior column screw.
Anterior column fixation can be performed percutaneously with a medullary screw as a less-invasive alternative to ORIF of the anterior column. Medullary implants can be inserted safely through the anterior column osseous fixation pathway from anterograde or retrograde start points (Illustrations A and B). When placed anterograde, the start point is on the gluteal pilar and the implant is then inserted and directed towards the pubic tubercle. The combined obturator oblique outlet (COOO) view helps ensure the screw does not penetrate the hip joint nor the vascular lacuna. An inlet view demonstrates the anterior-posterior limits of the osseous fixation pathway in the ramus portion of the corridor. Some authors have described a modified inlet with iliac-oblique rollback to it, however the tangential lines of the ramus are usually best seen on a pure inlet view.
Starr et al. wrote a technique on percutaneous fixation of the columns of the acetabulum. They report to safely place an anterior column screw, the C-arm should be oriented perpendicular to the superior pubic ramus. The C-arm is rotated during screw placement between an iliac inlet view and an obturator outlet view. The iliac inlet view is used to ensure that the guidewire does not penetrate the inner cortex of the superior ramus. The obturator outlet view is used to make sure the wire does not penetrate the hip joint.
Mauffrey et al. performed a review of the radiographic evaluation of acetabular fractures. They report that the acetabulum consists of two columns of bone arranged in an inverted Y-shaped configuration and attached to the ilium. They report that radiographic evaluation and classification of acetabular fractures is necessary to guide treatment decisions. They conclude that CT scans provide invaluable information in classifying these injuries.
Figure A is the AP pelvis radiograph revealing a right transverse acetabulum fracture. Illustration A demonstrates the path for retrograde placement of an anterior column screw. Illustration B demonstrates the path for anterograde placement of an anterior column screw. Illustration C and D are intra-operative fluoroscopy views revealing an inlet view and obturator outlet views, respectively.
Incorrect Answers:
Answer 2: The best view ensuring appropriate reduction is direct visualization of the fracture (open reduction).
Answer 3: The obturator outlet view is used to determine the cranial-caudal position of the wire during the placement of an anterior column screw.
Answer 4: The obturator outlet view is used to help rule out joint penetration during the placement of an anterior column screw.
Answer 5: The obturator inlet view is used to help determine if a supra-acetabular wire is within the tables of the ilium.
An 87-year-old female sustained the injury shown in Figure A. Which of the following is/are factor(s) that increase the risk of perforation of the anterior cortex during surgical treatment with a long cephalomedullary nail?
1) Radius of curvature mismatch between the bone and the implant
2) Anterior starting point on the greater trochanter
3) Posterior starting point on the greater trochanter
4) Answers 1 and 2
5) Answers 1 and 3
This patient sustained an intertrochanteric femur fracture. A mismatch of curvature between the nail and a posterior start point are both risk factors for anterior cortex perforation during surgical treatment with a long cephalomedullary nail.
When treating elderly patients with long intramedullary nails, there are certain factors that need to be accounted for. There is a mismatch between the radius of the femoral nails currently available and the femoral canal, ie, nails with a larger radius of curvature (straighter) are being inserted in a femur with a
smaller radius of curvature (less straight than the nail). As a result, the distal tip of the nail is forced into a nonanatomic anterior position during final seating of the nail distally. To avoid this complication, a lateral view of the distal femur while inserting the nail is recommended. Additionally, a posterior starting point on the greater trochanter is also a risk factor for anterior perforation of the nail.
Ostrum et al. performed a case report of 3 cases with penetration of the distal femoral anterior cortex during intramedullary nailing for subtrochanteric femur fractures. They report that the difference in the femoral anteroposterior bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration. The radius of curvature of the femur is less than the radius of curvature of the nails.
Roberts et al. performed a retrospective review to determine risk factors for impingement and penetration of the anterior cortex of the distal femur during intramedullary nailing of proximal femur fractures. The found that shorter patients and patients with an increased femoral bow were likely to have an anterior nail tip position or cortical impingement. They conclude that anterior starting points should be used to avoid this complication.
Figure A is an AP radiograph demonstrating a left intertrochanteric femur fracture.
Incorrect Answers:
Answers 1, 2, 3, 4: Risk factors for perforation of the anterior cortex while placing a long nail in an elderly patient are a mismatch in the radius of curvature and a posterior start point.
A 65-year-old man sustained the closed injury seen in Figures A and B and is being treated nonoperatively in a functional brace. At what time point after the injury does the lack of callus formation and motion at the fracture site first become concerning for nonunion?
1) 2 weeks
2) 4 weeks
3) 6 weeks
4) 12 weeks
5) 6 months
In a closed humeral shaft fracture, gross motion at the fracture site and no callus formation on radiographs at 6 weeks has a specificity of 100% and positive predictive value of 100% of going on to nonunion.
Closed midshaft humerus fractures treated with nonoperative measures such as functional bracing have been shown to go on to union in most patients.
Treatment with functional bracing relies on hydrostatic compressive forces from the surrounding soft tissues to provide adequate stability for healing. However, approximately 10% of patients go on to nonunion and require subsequent surgical stabilization. Predictors of nonunion include no callous at the fracture site and gross motion at the fracture site at 6 weeks from injury.
Papasoulis et al. reviewed the clinical studies of humeral shaft fractures treated with functional bracing. They found that this set of studies showed healing at
10.7 weeks from injury at a union rate of 94.5%. They concluded that functional bracing has many known benefits and remains a reliable treatment however certain parameters such as functional outcome, residual deformity, and loss of joint motion remain unclear and require further research.
Driesman et al. followed 84 consecutive patients with diaphyseal humeral shaft fractures treated nonoperatively. They found that mobile fracture sites at 6 weeks from injury predicted nonunion with 82% sensitivity and 99% specificity. They concluded that knowledge of fracture motion can help in determining the appropriate management in decision making in nonoperatively treated humeral shaft fractures.
Figures A and B show AP and transthoracic lateral radiographs of a mid diaphyseal spiral humeral shaft fracture, respectively.
Incorrect Answers:
Answers 1 & 2: 2 weeks and 4 weeks would be too early to reliably determine the risk of nonunion.
Answers 4 & 5: 12 weeks and 6 months have not been described as a timeframe for prediction of nonunion of humeral shaft fractures treated nonoperatively.
A patient presents with the injury shown in figures A and B. What has been associated with the technique depicted in figures C and D?
1) Longer operative times
2) Increased deep surgical infection rates
3) Unacceptably high malunion/nonunion rates
4) Slower early return to function
5) Longer hospital stays
Treatment of Shatzker V and VI tibial plateau fractures with hybrid external fixation is associated with increased malunion and nonunion rates.
Hybrid external fixation for treating tibial plateau fractures involves the use of an external fixator to achieve reduction through ligamentotaxis. Additional fracture reduction is achieved through limited open incisions with fixation augmented through percutaneous cannulated screws. Definitive treatment with this technique avoids soft tissue complications that have been associated with traditional open reduction and internal fixation with bicondylar plating.
However, studies have reported high malunion and nonunion rates due to a lack of rigid fixation.
Bertrand et al. performed a prospective cohort study of patients undergoing either open reduction and internal fixation versus hybrid external fixation for Schatzker V and VI tibial plateau fractures. Hybrid external fixation was associated with significantly shorter operative times but insignificantly increased complication rates. They concluded that there were limited statistically differences between these techniques, but further studies are required before advising hybrid external fixation for higher Schatzker tibial plateau fractures.
Gross et al. performed a retrospective study of patients treated with hybrid external fixation for Shatzker V and VI tibial plateau fractures. The authors found there was an 80% union rate, a 70% satisfactory reduction rate, and a 52% rate of malunion. The development of osteoarthritis was associated with plateau widening, articular comminution, articular step-off, and incorrect mechanical alignment. The authors concluded that hybrid external fixation is an effective means for the treatment of tibial plateau fractures that minimizes tissue dissection, with decreased blood loss, and shorter operative times, but associated with a very high malunion rate.
Hall et al. performed a multicenter randomized controlled trial comparing the treatment of Schatzker V and VI fractures with open reduction and internal fixation with hybrid external fixation. Patients with hybrid external fixation had less intraoperative blood loss, fewer unanticipated secondary procedures, slightly faster return to pre-injury activity at 6 months and 1 year, and shorter
hospital stay. They concluded that both hybrid external fixation and open reduction and internal fixation provide effective means for fracture treatment, but hybrid external fixation avoids soft tissue complications with deleterious consequences.
Figure A is an AP radiograph of the right knee with a Schatzker VI tibial plateau fracture. Figure B is an axial CT slice of the articular surface of the tibia with extensive comminution. Figures C and D are the AP and lateral radiographs of the knee with a hybrid external fixation construct for a tibial plateau fracture
Incorrect answers:
Answers 1, 2, 4, and 5: Hybrid external fixation for the treatment of bicondylar tibial plateau fractures is associated with higher malunion and nonunion rates, shorter operative times, increased superficial infection rates, faster earlier return to pre-injury activities, and shorter hospital stay.
An 89-year-old female sustained the injury shown in Figure A and underwent a hemiarthroplasty. Which of the following has been associated with increased rates of post-operative dislocation?
1) Posterior approach
2) Anterior approach
3) Anterolateral approach
4) Use of a bipolar implant
5) Use of a monopolar implant
The incidence of dislocation after hemiarthroplasty is highest when using a posterior approach.
Elderly femoral neck fractures are one of the most common fractures encountered by orthopaedists and will only become more common as the population continues to age. The displacement of the femoral head is associated with delayed union or nonunion, an increased risk of femoral head necrosis due to disrupted blood flow at the femoral neck, and failure of internal fixation devices. For this reason, displaced femoral neck fractures in older patients are often treated with hemiarthroplasty. Three approaches to hemiarthroplasty have been described: a lateral approach, a posterior approach, and an anterior approach. The posterior approach has been used more historically; however, its use has been called into question as it has been associated with increased dislocation rates.
Parker performed a trial on all patients with intracapsular femoral neck fractures being treated with hemiarthroplasty. Patients were randomized to surgery using either a lateral or posterior approach. They found that there were no statistically significant differences observed for any of the outcome measures including mortality, degree of residual pain and regain of walking ability. They concluded that both surgical approaches appear to produce comparable functional outcomes.
van der Sijp et al. performed a meta-analysis to compare the outcomes based on approaches for hemiarthroplasty in the treatment of proximal femur fractures. They found 21 studies and found that the posterior approach poses an increased risk of dislocation and reoperation compared to the lateral approach and anterior approaches. They conclude that there are no evident advantages of the posterior approach and its routine use for fracture-related hemiarthroplasty should be questioned.
Figure A is an AP pelvis radiograph demonstrating a displaced right femoral neck fracture.
Incorrect Answers:
Answers 2, 3, 4, & 5: None of these factors have been associated with an increased risk of dislocation after hemiarthroplasty for a femoral neck fracture.
A 50-year-old male sustained a humeral shaft fracture treated operatively 6 months ago. He denies medical problems but smokes 10 cigarettes per day. His current radiograph is shown in Figure A. He continues to have pain in his arm that is affecting his quality of life. On physical examination, there is motion at the fracture site. C-reactive protein and erythrocyte sedimentation rate are within normal limits. Which is the most appropriate definitive treatment for this fracture?
1) Exchange humeral nailing
2) Augmentative plating
3) Nail removal with open reduction compression plating
4) Smoking cessation and medical optimization
5) Nail removal with open reduction and compression plating with bone grafting
This patient has sustained an atrophic nonunion of a humeral shaft fracture treated with an intramedullary nail. The most appropriate definitive treatment is nail removal with open reduction and compression plating with bone grafting.
Most diaphyseal humeral fractures can be managed non-operatively with functional bracing. Operative treatment is indicated under a number of circumstances including open fractures, associated neurovascular injury, proximal and distal articular extension of the fracture, and in patients with other multiple injuries. Surgical stabilization can be accomplished with different implants and techniques. The two most common are plate and screw fixation and intramedullary nailing. Plate fixation has the advantages of potential absolute stability and sparing the rotator cuff from an incision. Intramedullary nailing has to be inserted proximally with potential damage to the rotator cuff. It, however, can be inserted with small incisions. If a nonunion develops after intramedullary nailing, nail removal and compression plating is the preferred treatment choice.
Heineman et al. performed a metanalysis on plate fixation or intramedullary nailing of humeral shaft fractures. They performed a literature search from 1967-2007 comparing nails and plates in patients with humeral shaft fractures that reported complications due to surgery. They found that the risk of a complication is lower when plating a fracture of the humeral shaft than when using an intramedullary nail.
Gerwin et al. performed an anatomical study to define the course of the radial nerve in the posterior aspect of the arm, with particular reference to its relationship to operative exposures of the posterior aspect of the humeral diaphysis. They found that the radial nerve crosses the posterior aspect of the humerus from an average of 20.7 +/- 1.2 centimeters proximal to the medial epicondyle to 14.2 +/- 0.6 centimeters proximal to the lateral epicondyle. They found the approach to permit the most visualization was the triceps reflecting approach.
Figure A is a lateral radiograph of an atrophic nonunion of a humeral shaft being stabilized with an intramedullary nail.
Incorrect Answers:
Answer 1: Exchange nailing is not a preferred treatment for humeral nonunions.
Answer 2: Augmentative plating may be used for hypertrophic nonunions that require additional stability, but not for an atrophic nonunion.
Answer 3: Bone grafting should be performed in this case to improve the biologic environment to induce fracture healing.
Answer 4: Smoking cessation and medical optimization should be performed however they are not the preferred definitive treatment.
A 45-year-old man is struck while crossing a major highway and sustains the injury depicted in Figure A. Which of the following statements comparing the techniques in Figure B and C is most accurate?
1) Technique depicted in Figure B is associated with an increased risk of septic arthritis
2) Technique depicted in Figure B is associated with increased rate of anterior knee pain
3) Technique depicted in Figure B is associated with improved postoperative fracture alignment
4) Technique depicted in Figure C is associated with an increased risk of septic arthritis
5) Technique depicted in Figure C is associated with improved postoperative fracture alignment
Compared to infrapatellar tibial nailing, suprapatellar tibial nailing is associated with improved postoperative fracture alignment.
While antegrade tibial nailing results in postoperative anterior knee pain in approximately 20% of patients, there is no significant difference in the incidence of anterior knee pain when the conventional infrapatellar approach is compared to suprapatellar approaches. In open tibial shaft fractures, no difference has been observed in the incidence of knee sepsis with either approach. However, several studies have demonstrated that intramedullary nail fixation through a suprapatellar approach is associated with a more accurate entry position and a more accurate fracture reduction when compared with an infrapatellar technique, particularly in more proximal and distal shaft
fractures, without evidence of a functional impact on the patellofemoral joint. Lastly, intraoperative radiography is generally less cumbersome with suprapatellar nailing.
Marecek et al. performed a multicenter comparison study of suprapatellar and infrapatellar approaches and the risk of knee sepsis after treatment of open tibia fractures. They reported no differences in the rates of infection, deep infection, or reoperation between suprapatellar and infrapatellar nailing groups. They concluded that the risk of knee sepsis after suprapatellar nailing of open fractures is low.
Avilucea et al. performed a retrospective cohort study comparing postoperative alignment after suprapatellar versus infrapatellar nailing for distal tibial shaft fractures. They reported a significantly increased rate of primary angular malalignment of greater than 5 degrees in the infrapatellar compared to the suprapatellar nailing cohort. They concluded that in the treatment of distal tibial fractures, suprapatellar nailing results in a significantly lower rate of malalignment compared with the infrapatellar nailing.
Jones et al. performed a study comparing the radiologic outcome and patient-reported function after suprapatellar and infrapatellar intramedullary nailing. They reported no difference in anterior knee pain, however, found a more accurate fracture reduction, both in terms of angulation and translation in the coronal plane, with the use of the suprapatellar technique. They concluded that when compared with infrapatellar nailing, the suprapatellar technique was not associated with more anterior knee pain, yet more accurate nail insertion and fracture reduction.
Figure A depicts a displaced distal third tibial shaft fracture. Figure B depicts the infrapatellar tibial nailing technique. Figure C depicts the suprapatellar tibial nailing technique.
Incorrect Answers:
Answer 1 & 4: No significant difference has been reported in the incidence of knee sepsis with either technique.
Answer 2: No significant difference has been reported in the incidence of anterior knee pain with either technique.
Answer 3: The suprapatellar technique, not the infrapatellar, is associated with more accurate alignment.
A 56-year-old woman sustains the closed injury depicted in Figures A-B. On examination, her wrist is mildly swollen and she is unable to actively oppose her thumb. She also complains of some paresthesias in her thumb and index finger. The patient undergoes closed reduction and splinting; however, her paresthesias worsen significantly in the next 12 hours. What is the likely mechanism of her paresthesias and what is the most appropriate treatment?
1) Nerve compression; open reduction internal fixation with open carpal tunnel release
2) Nerve laceration; open reduction internal fixation with primary nerve repair or grafting
3) Decreased arterial inflow; fasciotomy with open reduction internal fixation
4) Reflex sympathetic dystrophy; vitamin C
5) Nerve compression; repeat closed reduction
This patient is presenting with signs of acute carpal tunnel syndrome (CTS) in the setting of a displaced distal radial fracture. The pathogenesis of acute CTS is nerve compression, requiring urgent open carpal release with open reduction internal fixation (ORIF).
Acute CTS is a well-recognized phenomenon after distal radial fractures. Risk factors include ipsilateral upper extremity fractures, translation of the fracture fragments, and articular distal radius fractures (DRFs). Acute CTS can manifest with paresthesias in the median nerve distribution and opponens pollicis weakness. Acute CTS is an indication for urgent surgical decompression of the median nerve.
Odumala et al. performed a study to evaluate the role of carpal tunnel decompression in the prevention of median nerve dysfunction after buttress plating of DRFs. They reported that prophylactic decompression of the carpal tunnel results in twice the relative odds of developing median nerve dysfunction, which routinely self-resolved. They concluded that prophylactic median nerve decompression does not alter the course of median nerve dysfunction and may actually increase postoperative morbidity.
Medici et al. performed a case-control study to investigate whether carpal tunnel release (CTR) during fixation DRFs improves outcomes. They reported no statistically significant difference between the groups in VAS and Mayo Wrist Scores, however, an increased risk of subsequent CTR in the group who underwent ORIF with no CTR at the index procedure. They concluded that the release of the transverse carpal ligament during ORIF may reduce the incidence of postoperative median nerve dysfunction.
Niver et al. reviewed CTS after DRFs. They reported that acute CTS noted at the time of DRF warrants urgent surgical release of the carpal tunnel and fracture fixation, and that delayed CTS presenting after a distal radius fracture has healed may be managed in the standard fashion for CTR. They concluded that there is no role for prophylactic CTR at the time of distal radius fixation in a patient who is asymptomatic.
Figures A and B depict a displaced apex volar DRF and a mildly displaced ulnar styloid fracture.
Incorrect Answers:
Answer 2: Acute CTS after DRF most often commonly occurs after median nerve compression and contusion, not laceration.
Answer 3: This describes compartment syndrome, which is less likely than acute CTS given the clinical exam described.
Answer 4: Reflex sympathetic dystrophy usually occurs after the acute phase of the DRF.
Answer 5: Acute CTS after DRF requires urgent open carpal tunnel release.
Figures A and B depict the closed injury radiograph of a 79-year-old right-hand-dominant woman who fell on her left wrist. According to meta-analysis and systematic reviews, which of the following statements is most accurate regarding her injury?
1) Improved functional outcomes with open reduction internal fixation (ORIF) through FCR approach vs. closed treatment
2) No difference in radiographic outcomes after ORIF vs. closed treatment
3) No difference in functional outcomes after ORIF vs. closed treatment
4) Improved functional outcomes with closed treatment vs. ORIF
5) Improved functional outcomes with external fixation and K wire fixation vs. ORIF
This elderly patient has sustained a closed intra-articular and shortened distal radial fracture (DRF). Many studies have reported no difference in functional outcomes when patients aged 60 and over are treated in a closed manner versus operatively for unstable fractures.
The treatment of DRFs in the elderly population is controversial. A variety of nonoperative and operative treatments are available, including closed reduction and splinting/casting, K wire stabilization, external fixation, and ORIF. While conservative management of DRFs in the elderly is common,
recent systematic reviews and meta-analyses have demonstrated that despite worse radiographic outcomes after closed treatment of unstable fractures, functional outcomes were no different between patients treated closed versus surgically in patients over the age of 60 years.
Ju et al. published a systematic review and meta-analysis comparing treatment outcomes between nonsurgical and surgical treatment of unstable DRFs in the elderly. They reported no significant differences in DASH score, VAS pain score, grip strength, wrist extension, pronation, supination, and ulnar deviation between the groups. They concluded that operative and nonoperative treatments result in similar outcomes in the treatment of unstable DRFs in the elderly, with no impact on subjective function outcome and quality of life with closed treatment.
Diaz-Garcia et al. published a systematic review of the outcomes and complications after treating unstable DRFs in the elderly, comparing various treatment techniques. They reported significant differences in wrist motion, grip strength, DASH score, although these findings may not be clinically meaningful. They concluded that although the operatively treated group had improved radiographic outcomes, functional outcomes were no different when compared to the group treated in a closed manner.
Figure A depicts an unstable intra-articular and shortened DRF. Incorrect Answers:
Answers 1, 4 & 5: Systematic reviews and meta-analyses have demonstrated
no difference in functional outcomes between operative and closed treatment modalities for DRF.
Answer 2: Systematic reviews and meta-analyses have demonstrated superior radiographic outcomes after surgical treatment when compared to closed treatment.
An active 60-year-old woman falls from her attic and presents with the injury in Figure A. She undergoes successful closed reduction and sling immobilization. At follow up, she is unable to move her shoulder. New radiographs are depicted in Figures B and C. What is the next best step?
1) Continued sling immobilization
2) Closed reduction percutaneous pinning
3) Open reduction internal fixation
4) Hemiarthroplasty
5) Reverse total shoulder arthroplasty
This active patient presents with a greater tuberosity fracture dislocation. Open reduction internal fixation (ORIF) is indicated, particularly when the greater tuberosity fragment is displaced greater than 5mm.
Many proximal humerus fractures are minimally displaced and respond acceptably to nonoperative management. Isolated greater tuberosity fractures or rotator cuff injuries are associated with shoulder dislocations in the elderly population. The greater tuberosity fragment undergoes deforming forces by the supraspinatus and infraspinatus muscles. In active patients, it is well-accepted that greater tuberosity fracture displacement greater than 5mm is an indication for ORIF to restore their ability to perform overhead activities and prevent impingement.
Schumaier et al. published a review article on the treatment of proximal humerus fractures in the elderly. They highlighted that while bone density was a predictor of reduction quality, social independence was a better predictor of outcome. They concluded that although the majority of minimally displaced fractures can be treated successfully with early physical therapy, treatment for displaced fractures should consider the patient's level of independence, bone quality, and surgical risk factors. They emphasized that there was no clear evidence-based treatment of choice, and the surgeon should consider their comfort level during their decision-making.
George et al. published a review article on greater tuberosity humerus fractures. They reported that these fractures may occur in the setting of anterior shoulder dislocations or impaction injuries against the acromion or superior glenoid, with surgical fixation recommended for fractures with greater than 5 mm of displacement in the general population or greater than 3 mm of displacement in active patients involved in frequent overhead activity. They recommended close followup and supervised rehabilitation to increase successful outcomes.
Figure A depicts a greater tuberosity fracture dislocation of the left shoulder. Figures B and C depict reduction of the glenohumeral joint with residual displacement of the greater tuberosity. Illustrations A and B depict radiographs after ORIF.
Incorrect Answers:
Answer 1: While most proximal humerus fractures can be treated nonoperatively, greater tuberosity fractures displaced 5 mm or greater should be treated with ORIF.
Answer 2: ORIF allows for anatomical realignment, reducing the possibility of impingement and weakness from greater tuberosity malunion.
Answer 4 & 5: Hemiarthroplasty and reverse total shoulder arthroplasty would be indicated in some 4-part proximal humerus fractures in active elderly patients.
A 21-year-old football player is tackled as he falls onto an outstretched arm. He sustains the injury shown in Figure A. He undergoes successful operative treatment of his injury. In which order did his injury occur?
1) MCL > LCL > anterior capsule
2) MCL > anterior capsule > LCL
3) anterior capsule > MCL > LCL
4) LCL > anterior capsule > MCL
5) LCL > MCL > anterior capsule
The patient sustained a terrible triad injury of the elbow, which progresses from the LCL to the anterior capsule and then the MCL.
Terrible triad injuries of the elbow are traumatic injuries that occur after a fall on an extended arm that results in a combination of valgus, axial, and posterolateral rotatory forces. The key features of a terrible triad injury include a radial head fracture, a coronoid fracture, and an elbow dislocation. Disruption of the structures in the elbow characteristically occurs from lateral to medial, affecting the LCL first, followed by the anterior capsule and MCL. Outcomes following terrible triad injuries have historically been poor; however, more recent literature has shown that good outcomes can be achieved with surgical stabilization of the elbow followed by an early rehabilitation protocol. Some authors use temporary immobilization, but range-of-motion exercises are typically initiated by 48 hours postoperatively. Active range of motion is particularly important, as it recruits muscles that act as dynamic stabilizers of the elbow. Depending on the injury, method of fixation, and stability that is achieved, the range of motion may be limited to 30° of extension during the early postoperative period but should allow full flexion.
Giannicola et al. (2013) performed a study to determine the critical time period for recovery of functional range of motion after surgical treatment of complex elbow instability (CEI). They found that the first 6 months after surgery represent the critical rehabilitation period to obtain a functional elbow and that elbow flexion recovered at a rate slower than that of the other elbow movements. They recommend that, following CEI surgical treatment, a rehabilitation program should be started promptly and should be continued for at least 6 months because a significant improvement of ROM occurs in this period.
Giannicola et al. (2015) performed a study analyzing the predictability of outcomes of terrible triad injuries (TTI) treated according to current diagnostic and surgical protocols. They found that the current diagnostic and therapeutic protocols allow for satisfactory clinical outcomes in a majority of cases but a high number of major and minor unpredictable complications still persist. Low compliance, obesity, and extensive soft elbow tissue damage caused by high-energy trauma represented negative prognostic factors unrelated to surgery.
McKee et al. performed a review on their standard surgical protocol for the treatment of elbow dislocations with radial head and coronoid fractures. Their surgical protocol included fixation or replacement of the radial head; fixation of the coronoid fracture, if possible; repair of associated capsular and lateral ligamentous injuries; and, in selected cases, repair of the medial collateral ligament and/or adjuvant-hinged external fixation. They found that their surgical protocol restored sufficient elbow stability to allow early motion postoperatively, enhancing the functional outcome. They recommend early operative repair with a standard protocol for these injuries.
Figure A is a lateral radiograph of the elbow demonstrating a terrible triad injury with a comminuted radial head/neck fracture, displaced coronoid fracture, and posterior elbow dislocation. Illustration A is a rendered image of the radiograph shown in Figure A with the components labeled.
Incorrect Answers:
Answers 1, 2, 3, and 5: Terrible triad injuries occur from the LCL to the anterior capsule and then the MCL.
An 82-year-old female sustains the fracture shown in Figure A as the result of a ground level fall. Which of the following has been shown to be a reliable predictor of postoperative lateral wall fracture for this injury after treatment with a sliding hip screw?
1) Reverse obliquity fracture pattern
2) Lateral wall thickness
3) Previous contralateral hip fracture
4) DEXA T-score
5) Calcar comminution
Lateral wall thickness has been shown to be a predictor of postoperative lateral wall fracture. As the lateral wall thickness decreases, there is an increased chance of fracture.
Lateral wall fracture creates an unstable fracture pattern and increased screw sliding/collapse. This shortens the neck and abductors, leading to worse patient outcomes (radiographic and clinical). Recognition of a thin wall should lead toward the use of an intramedullary device or adjunct use of a trochanteric stabilizing plate with a sliding hip screw device.
Baumgaertner et al. reported that the failure of peritrochanteric fractures that have been treated with a fixed-angle sliding hip-screw device is frequently related to the position of the lag screw in the femoral head. They established the tip-apex distance as the sum of the distance from the tip of the lag screw to the apex of the femoral head on an anteroposterior radiograph and this distance on a lateral radiograph, after controlling for magnification. Upon reviewing their series, none of the 120 screws with a tip-apex distance of twenty-five millimeters or less cut out, but there was a very strong statistical relationship between an increasing tip-apex distance and the rate of cutout, regardless of all other variables related to the fracture.
Socci et al. performed a literature review of relevant papers and appropriate clinical databases and concluded that fixation of AO 31A1 fractures was best achieved with a sliding hip screw device and that all other types of intertrochanteric hip fractures be fixed with an intramedullary device.
Utrilla et al. reported no difference in outcome in stable fractures, but better mobility at one year following intramedullary fixation of unstable fractures.
Hsu et al. measured the thickness of the lateral wall of patients with AO/OTA 31-A1 and 31-A2 type intertrochanteric hip fractures. They found that the lateral wall thickness was a reliable predictor of postoperative lateral wall fracture for unstable AO Type A2 fractures and concluded that the lateral wall thickness threshold value for risk of developing a secondary lateral wall fracture was found to be 20.5 mm.
Figure A shows a standard obliquity intertrochanteric hip fracture.
Illustration A from the Hsu article demonstrates the measurement of the lateral wall thickness. The distance is measured along a 135-degree angle, between a point 3cm distal to the innominate tubercle of the greater trochanter and the fracture line (midway between the two cortical lines).
Incorrect Answers:
Answer 1: This pattern is unstable and requires treatment with an intramedullary nail as opposed to a sliding hip screw.
Answer 3: There has been no proven association with this factor. Answer 4: There has been no proven association with this factor.
Answer 5: Fracture comminution is not associated unless the lateral wall is already fractured or comminuted itself.
A 78-year-old patient presents with right hip pain and inability to bear weight after an unwitnessed fall at a nursing home. Figures A and B are the radiographs of the hip and pelvis. Which statement is true regarding the treatment of these injuries?
1) Smaller lateral wall thickness favors sliding hip screw constructs
2) Unstable fractures are best treated with sliding hip screw constructs
3) Avoiding distal locking screws in intramedullary implants protects against refracture
4) Stable fractures have no differences in outcomes between sliding hip screws and intramedullary implants
5) Implant stability has a greater impact on outcomes rather than reduction quality
Studies have shown that in stable intertrochanteric femur fractures there are no differences in outcomes between sliding hip screws and intramedullary implants.
Intertrochanteric femur fractures are one of the most common fractures in the geriatric population. Implant selection has been a great topic of research with most studies reporting minimal to no differences in outcomes between intramedullary and sliding hip screw constructs in stable fracture patterns.
Unstable fractures, however, are reportedly better treated with a distally locked intramedullary implant. The quality of fracture reduction has a greater impact on the overall outcome than implant selection.
Hsu et al. performed a retrospective study of risk factors for postoperative lateral wall fractures in patients treated with sliding hip screws for intertrochanteric femur fractures. They found that fracture classification and lateral wall thickness, which is measured from 3 cm distal from innominate tubercle and angled 135 degrees to the fracture line, were associated with postoperative lateral wall fracture. They recommended not treating intertrochanteric femur fractures with sliding hip screws if the lateral wall thickness is less than 20.5 mm.
Socci et al. reviewed the literature regarding the treatment of intertrochanteric femur fractures. Based on the literature, they recommend treatment of AO/OTA type 31A1 fractures with sliding hip screws, type 31A2 fractures with short intramedullary implants, and 31A3 fractures with long intramedullary implants. Simple basicervical fractures of the femoral neck can be treated with sliding hip constructs whereas comminuted fractures treated with intramedullary devices due to the inherent instability of the pattern. The most import aspect in fracture healing is the quality of the reduction rather than the choice of implant.
Lindvall et al. performed a retrospective study of refracture rates in patients treated with either long or short cephalomedullary nails. The authors found a 97% union rate with both implant types and refracture not associated with either long or short implants. Rather, refracture was associated with the lack of a distal locking screw. The authors recommended locking intramedullary implants to avoid refracture.
Utrilla et al. performed a randomized control trial of elderly patients treated
with compression hip screw or Trochanteric Gamma Nail for intertrochanteric femur fractures. They reported the only differences between the two implants were quicker operating time, less fluoroscopy use, and better walking with unstable fractures treated with intramedullary implants. The authors recommended either construct for stable fractures, but intramedullary implants for unstable fractures.
Figures A and B are the AP and lateral radiographs of the right hip radiographs demonstrating a simple and minimally displaced intertrochanteric femur fracture, classified as an AO/OTA 31A1 fracture. Illustration A depicts the AO/OTA classification system for proximal femur fractures.
Incorrect answers:
Answer 1: Thinner lateral wall thickness in intertrochanteric femur fractures favors the use of an intramedullary implant due to the risk of lateral wall fracture.
Answer 2: Unstable intertrochanteric femur fractures are best treated with intramedullary implants.
Answer 3: The lack of distal locking screws has been shown to increase the risk of refracture.
Answer 5: Reduction quality has been shown in several studies to have a greater impact on outcomes rather than implant selection.
A 28-year-old male that sustained a closed left femoral shaft fracture 12 months ago and underwent intramedullary nailing presents with persistent pain in the right thigh. The patient walks with an antalgic gait. He denies any fevers or chills. His surgical sites are well healed and there are no signs of drainage. Serum ESR and CRP are 12 mm/hr (reference
1) Nail removal with compression plating and open bone grafting
2) Closed reamed exchange nailing
3) Nail dynamization
4) Nail retention with plate augmentation and bone grafting
5) Electrical bone stimulator
The patient is presenting with a hypertrophic nonunion of the femur below the isthmus, which studies have shown to have a higher union rate when treated with plate augmentation. Retention of the nail allows for full weight-bearing postop.
Hypertrophic nonunion of the femur is the result of fracture site hypermobility with sufficient biology for healing. This is demonstrated with abundant callus formation without bridging trabeculae. Traditionally, this is treated with closed reamed exchange nailing which increased construct stiffness with a larger diameter nail, improved isthmic fit, and extrusion of reaming contents to the nonunion site. However, studies have demonstrated a higher union rate with open plate augmentation, bone grafting, and nail retention. This is due to the ability to correct nonunion site deformity, provide added compression at the nonunion site, and increase fracture site biology with bone graft.
Lynch et al. reviewed the literature regarding the treatment options for femoral nonunions. The literature suggests high union rates when hypertrophic nonunions are treated with exchanged reamed nailing. However, the use of augmentative plate fixation allows for further deformity correction. The proposed mechanism by which exchange reamed nailing is increased construct stiffness with a large diameter nail, usually by 1-2 mm, increased isthmic fit, and autogenous bone graft extrusion into the nonunion site.
Somford et al. performed a systematic review of the surgical treatment of femoral nonunions. Results demonstrate that exchange nailing provides a 73% union rate compared to plate augmentation of 96%. They speculated that there were increased indications for exchange nailing for oligotrophic nonunions in many of the included studies, which may have reduced the union rate. Further, plate augmentation does allow for deformity correction, which can further improve the union rate.
Figures A and B are the AP and lateral radiographs of the femur with hypertrophic nonunion as suggested with the abundant callus formation and broken distal interlock screws. Illustration A and B are the AP and lateral radiographs of the distal femur subsequent plate augmentation and fracture healing.
Incorrect Answers:
Answer 1: Compression plating and bone grafting provide deformity correction across the nonunion site and added biology, but there is loss of weight-bearing benefits with nail removal.
Answer 2: Closed reamed exchange nailing can provide healing of the nonunion by increasing the nail diameter and improving the isthmic fit, but studies have shown a lower union rate in subisthmic femoral nonunions compared to augmentation plating.
Answer 3: Nail dynamization provides the benefit of weight-bearing forces across the nonunion site to enhance the differentiation of osteoblasts and promote fracture healing. In hypertrophic nonunions, fracture site stability is the cause of nonunion rather than the lack of fracture site biology.
Answer 5: Electrical bone stimulators do not provide the added fracture stability that is required to address hypertrophic nonunion.
A 25-year-old male sustains the injury depicted in Figure A. He is splinted in the field, but on arrival to the emergency room, he complains of painful "tightness" around the leg and severe uncontrolled pain despite maximum dose narcotics. His pain is exacerbated when the toes and ankle are passively stretched in flexion and extension. What is the most appropriate next step in treatment?
1) External fixation with serial doppler examinations
2) Intramedullary nailing
3) Open reduction internal fixation using plates and screws
4) Immediate 2-compartment fasciotomies and external fixation
5) Immediate 4-compartment fasciotomies and external fixation
This patient has clinical symptoms and signs of leg compartment syndrome and should undergo immediate fasciotomies of all 4 leg compartments, followed by external fixation for fracture stabilization.
Tibial fractures are among the most common reasons for compartment syndromes of the leg. A clinical assessment is key in the diagnosis of acute compartment syndrome. If there is uncertainty, intracompartmental pressure measurement has been advocated to help confirm the diagnosis. An absolute
compartment pressure >30 mm Hg or a difference in diastolic pressure and compartment pressure (delta p)
A 24-year-old male is brought to the ED after an MVC. He is found to have a closed comminuted segmental fibula fracture after a prolonged extraction from the vehicle. Several hours after arrival, the patient reports increasing pain and is noted to have an exacerbation of his pain with passive stretching of the ankle. He has a heart rate of 103 and a blood pressure of 141/87. Compartment pressures are obtained and are 27 mmHg in the anterior compartment, 47 mmHg in the lateral compartment, 28 mmHg in the superficial posterior compartment, and 27 mmHg in the deep posterior compartment. Which of the following correctly describes the initial pathophysiology of compartment syndrome and the neurologic deficit that would likely occur in this patient if left untreated?
1) Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the first webspace
2) Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
3) Decreased arterial inflow; inability to dorsiflex his ankle
4) Decreased venous outflow; decreased sensation on the dorsum of his foot involving the first webspace
5) Decreased venous outflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Compartment syndrome initially results from a decrease in venous outflow relative to arterial inflow. This patient has elevated pressures in the lateral compartment of the leg, which is where the superficial peroneal nerve runs to supply sensation to the dorsum of the foot including the hallux and 3rd and 4th toes.
Compartment syndrome results from compromised venous outflow from the leg relative to the arterial inflow. This venous congestion leads to elevated compartment pressures that ultimately lead to compromised arterial inflow without compartment release. There are 4 compartments in the leg: anterior, lateral, superficial posterior, and deep posterior. The anterior compartment contains the deep peroneal nerve, the lateral compartment of the leg contains the superficial peroneal nerve, and the deep posterior compartment contains the tibial nerve.
McQueen et al. performed a study to determine risk factors for acute compartment syndrome. They found that young patients, especially men, were most at risk of acute compartment syndrome after injury. They recommend that, when treating such injured patients, the diagnosis should be made early, utilizing measurements of tissue pressure.
Olson et al. published a review on acute compartment syndrome in lower extremity musculoskeletal trauma. They reported that acute compartment syndrome is a potentially devastating condition in which the pressure within an osseofascial compartment rises to a level that decreases the perfusion gradient across tissue capillary beds, leading to cellular anoxia, muscle ischemia, and death. They report that recognizing compartment syndromes requires having and maintaining a high index of suspicion, performing serial examinations in patients at risk, and carefully documenting changes over time.
Illustration A is a diagram depicting the compartments of the leg and its contents.
Incorrect Answers:
Answers 1, 2, 3, and 4: Compartment syndrome initially results from a decrease in venous outflow relative to arterial inflow. The superficial peroneal nerve runs in the lateral compartment and provides sensation to the dorsum of the foot including the hallux and 3rd and 4th toes.
Which of the following amputations results in an approximate 40% increase in energy expenditure for ambulation?
1) Syme
2) Traumatic transtibial
3) Vascular transtibial
4) Traumatic transfemoral
5) Vascular transfemoral
The energy expenditure of a vascular transtibial amputation is approximately 40% greater.
The energy expenditure for ambulation increases with lower extremity amputation. Diabetics and vasculopathic patients who undergo amputation
have significantly increased energy requirements compared with nondiabetic patients undergoing amputations for trauma. The metabolic cost for a vascular transtibial amputation is 40% compared to a 25% increase in normal patients who sustain a traumatic amputation.
Huang et al. used a mobile instrument system to measure energy consumption by indirect calorimetry at rest and during ambulation in 25 unimpaired subjects, 6 unilateral below-knee (BK) amputee patients, 6 unilateral above-knee (AK) amputee patients and 4 bilateral AK amputee patients. They found that in comparison to unimpaired subjects, the mean oxygen consumption was 9% higher in unilateral BK amputee patients, 49% higher in unilateral AK amputee patients and 280% higher in bilateral AK amputee patients.
Pinzur et al. performed a study to measure cardiac function and oxygen consumption in 25 patients who underwent amputation for peripheral vascular disease (PVD), and in five similarly aged control patients without PVD. They found Normal walking speed and cadence decreased and oxygen consumption per meter walked increased with more proximal amputation. They conclude that peripheral vascular insufficiency amputees function at a level approaching their maximum functional capacity and more proximal amputation levels, the capacity to walk short or long distances is greatly impaired.
Incorrect Answers:
Answer 1: A Syme amputation increases energy expenditure by 15%.
Answer 2: A traumatic transtibial amputation increases energy expenditure by 25%.
Answer 4: A traumatic transfemoral amputation increases energy expenditure by 68%.
Answer 5: A vascular transfemoral amputation increases energy expenditure by 100%.
A 25-year-old man sustains the injury shown in Figures A-C. What is the primary advantage of using a trochanteric flip osteotomy (TFO) in treating this injury?
1) It may be performed in a minimally invasive manner
2) It involves minimal soft tissue stripping
3) It leads to higher union rates
4) It allows the surgeon to address all sites of injury through one approach
5) Answers 1 and 2
This patient has sustained a right hip fracture-dislocation with fractures of the femoral head and posterior wall. The TFO allows the surgeon to address all sites of injury through a single approach.
Femoral head fracture-dislocations are a result of high-energy trauma. Treatment ranges from closed reduction and conservative management to total hip arthroplasty. Intermediate options include open reduction and internal fixation or excision of fracture fragments. Complications of this injury include post-traumatic hip arthritis, avascular necrosis, and heterotopic ossification.
The injury is further complicated when a fracture of the acetabulum is concomitantly present. There has been no consensus treatment on this injury constellation as it presents quite rarely. The TFO is one approach that allows the surgeon to treat and stabilize both injuries concurrently. It should be noted that a surgical hip dislocation is performed in conjunction with the TFO to allow access to the femoral head.
Solberg et al. performed a retrospective study of patients sustaining Pipkin IV fracture/dislocations with a TFO. They had 12 patients over a 6 month period. They found that all patients healed radiologically and one patient developed osteonecrosis. 10 out of 12 patients had good to excellent outcomes. They concluded that using a surgical protocol with TFO rendered clinical results
comparable to previously reported outcomes in a series of isolated femoral head fractures.
Giannoudis et al. performed a systematic review to investigate data regarding femoral head fractures, particularly focusing on their management, complications and clinical results. They reported that fracture-dislocations were managed with emergent closed reduction, followed by definite treatment, aiming at an anatomic restoration of both fracture and joint incongruity. They concluded that neither the TFO nor an anterior approach seems to endanger femoral head blood supply compared to the posterior one, with the TFO possibly providing better long-term functional results and lower incidence of major complication rates.
Henle et al. reported on the result of 12 patients of femoral head fractures with associated posterior wall fractures treated with a TFO. They found good to excellent results in 10 patients. The two patients with poor outcome developed avascular necrosis of the femoral head and underwent total hip arthroplasty.
Heterotopic ossification was seen in five patients. They concluded that the TFO may lead to favorable outcomes in this injury constellation.
Figure A is an AP radiograph of the right hip demonstrating a femoral head fracture-dislocation. Figure B is an axial CT image demonstrating a posterior wall fracture. Figure C is an axial CT image demonstrating a femoral head fragment within the acetabulum. Illustration A is the Pipkin classification of femoral head fractures: Type I is below the fovea, Type II is above the fovea, Type III is associated with a femoral neck fracture, and Type IV is associated with an acetabular fracture.
Incorrect Answers:
Answers 1, 2, & 5: The TFO is not a minimally invasive approach.
Answer 3: There is no evidence that shows that this approach leads to higher union rates of this injury
A 30-year-old male is brought to your emergency department following a motor vehicle collision at high speed. He is intubated in the field for airway protection but is hemodynamically stable. Subsequent workup shows a displaced acetabular fracture, in addition to an intracranial bleed and liver laceration which do not require surgery. When placing an antegrade anterior column screw, what radiographic view should be used to avoid intra-pelvic screw penetration?
1) Iliac oblique view with hip and knee flexed
2) Iliac oblique inlet view
3) Obturator oblique view with hip and knee flexed
4) Obturator oblique outlet view
5) Obturator oblique inlet view
The iliac oblique inlet view will best show the the anterior-posterior placement of an anterior column ramus screw.
Percutaneous and limited-open acetabular fixation is becoming increasingly common as it avoids the morbidity of extensile pelvic dissection and allows early mobilization. However, it relies heavily on a mastery of radiographic landmarks and ability to interpret these images to reduce fracture fragments without direct visualization. Slight deviations of the fluoroscopy beam and/or fracture displacement will distort the radiographic image. Without a facile ability to interpret these and make appropriate adjustments, percutaneous fixation will be extremely onerous.
Starr et al. described their early techniques for percutaneous and limited-open acetabular fixation. They first implemented this for minimally displaced fracture patterns but have expanded these to a wider range of pathology. They cite the benefit of earlier mobilization in the poly-traumatized patient as great use for this technique.
Mauffrey et al. reviewed radiograph utilization during acetabular fracture care. Though CT has added tremendously to demonstrating subtleties of acetabular fractures, they state the use of AP and orthogonal iliac and obturator oblique Judet views cannot be overlooked. Interpreting these radiographs allows the surgeon to recreate 2-dimensional images into a 3-dimensional fracture pattern and better understand the character of the injury.
Illustrations A and B demonstrate the iliac oblique inlet view and obturator oblique outlet views, respectively.
Illustration C demonstrates the relationship of the critical structures at risk of injury during anterior column screw placement. Illustrations D and E show the starting point with screw trajectory, and position of the hip during posterior column screw.
Incorrect Answers:
Answers 1 and 3- These would be utilized when placing a posterior column screw.
Answer 4- This view would show the supra-acetabular corridor with help with the starting point for external fixator placement.
Answer 5- This shows the inner and outer tables of the iliac wing and confirms pins have not violated the cortex.
A 34-year-old male sustains the injury shown in Figures A and B. Which factor has been found to be elevated in the synovial fluid and contributes to post-traumatic arthritis?
1) TGF-Beta
2) RANKL
3) IL-2
4) IL-6
5) cAMP
The patient has sustained a tibial plafond or pilon fracture as depicted in Figures A and B. IL-6 is one of many inflammatory molecules that has been found to be elevated in the synovial fluid following an intra-articular ankle fracture.
Post-traumatic arthritis following intra-articular fractures is a known complication. It commonly appears 1-2 years following injury and is related to chondrocyte death at the margins. There has not been shown to be any association between prolonged non-weight bearing, poor patient compliance with weight-bearing restrictions, and hardware reactions with the development of post-traumatic arthritis. However, literature has shown that the inflammatory molecules present in the synovial fluid can have a significant effect on the development of posttraumatic arthritis. Important inflammatory factors that have been found to be elevated include IL-6, IL-8, MMP-1, MMP-2, MMP-3, MMP-9 and MMP-10.
Adams et al. looked at the synovial fluid of 21 patients with an intra-articular ankle fracture and used the un-injured ankle as a control. They found the inflammatory molecules of GM-CSF, IL-10, IL-1 beta, IL-6, IL-8, IL-10, IL-12p70, TNF-alpha, MMP-1, MMP-2, MMP-3, MMP-9, MMP-10 were all elevated. They concluded that these inflammatory molecules may play a role in posttraumatic arthritis development.
Adams et al. looked at the synovial fluid of 7 patients from his previous 21 patients that had intra-articular ankle fractures. They found that IL-6, IL-8, MMP-1, MMP-2, and MMP-3 were significantly elevated in comparison to the uninjured ankle. They concluded that the sustained elevated intra-articular inflammatory environment is a potential contributor to post-traumatic arthritis.
Figures A and B are sagittal and axial CT slices, respectively, that depict a tibial plafond or pilon fracture.
Incorrect Answers:
Answer 1: TGF-Beta has not been shown to be elevated in the synovial fluid and contribute to post-traumatic arthritis. However, TGF-Beta has been shown to be a factor in the inflammatory cycle, immune system signaling and bone signaling (inhibits osteoclasts via osteoprotegrin).
Answer 2: RANKL has not been shown to be elevated in the synovial fluid and contribute to post-traumatic arthritis. RANKL is an important part of bone signaling and metabolism.
Answer 3: IL-2 has not been shown to be elevated in the synovial fluid and contribute to post-traumatic arthritis. IL-2 has important functions within the
immune system.
Answer 5: cAMP has not been shown to be elevated in the synovial fluid and contribute to post-traumatic arthritis. cAMP is an intra-cellular signaling molecule.
A 29-year-old female presents to the trauma bay from the scene of a high-speed motor vehicle accident. She is found to have a closed intraarticular distal radius fracture with a concomitant ulnar styloid base fracture. She subsequently undergoes ORIF of the distal radius fracture with a volar locking plate. The ulnar styloid fracture is not addressed. Which of the following, if present, is least likely to affect functional outcomes?
1) Ulnar styloid nonunion
2) DRUJ instability
3) Articular step-off >3mm
4) Radial shortening
5) Workers compensation claim
Ulnar styloid non-unions do not affect the overall outcome of hand or wrist function following ORIF of distal radius fractures.
Ulnar styloid base fractures can be associated with DRUJ disruption and TFCC rupture. The DRUJ should be independently evaluated following ORIF of the distal radius. Without instability, unlar styloid fractures do not need to be addressed. If instability exists, the DRUJ should be treated as a separate entity, typically cross-pinned using k-wires. The result of ulnar styloid nonunions are inconsequential to the overall outcome of patients undergoing distal radius ORIF.
Daneshvar et al review the effects of ulnar styloid fractures on patients sustaining distal radius fractures. They report that patients with a concomitant ulnar styloid fracture had a slower recovery of wrist flexion and grip strength compared to those with an isolated distal radius fracture. They conclude, however, that even the presence of an ulnar styloid nonunion did not significantly affect outcomes.
Buijze et al review the clinical impact of united versus non-united fractures of the proximal half of the ulnar styloid following volar plate fixation of the distal radius. They report no difference in motion, strength or outcome scores
between the united and non-united groups at 6 months follow up. They conclude that nonunion of the ulnar styloid does not have an effect on the overall outcome of hand or wrist function.
Incorrect Answers:
Answer 2: Unrecognized DRUJ instability leads to decreased pronosupination and posttraumatic arthritis.
Answer 3: With 1-2mm of articular step-off 90% of young adults will develop radioulnar arthrosis
Answer 4: Radial shortening is one of the most important factors for predicting poor functional outcomes following distal radius ORIF.
Answer 5: Workers compensation claims negative impact functional outcomes following fixation of distal radius fractures.
Which of the following proximal humerus fractures has the highest likelihood of developing humeral head ischemia?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Posteromedial calcar length of the humeral head less than 8 mm and a loss of medial hinge are among the most reliable predictors of ischemia in the surgical management of humeral head fractures.
Proximal humerus fractures are classified based on the Neer classification, in which 4 parts are described: greater tuberosity, lesser tuberosity, articular surface, and the shaft. A fragment is considered a part if it is greater than 45 degrees angulated or displaced >1cm. The posterior humeral circumflex artery is the main blood supply to the humeral head. Following ORIF, humeral head ischemia may occur and is associated with the initial fracture pattern. Several factors including 10mm and angulation >45 degrees have been associated with a disruption of the vascular supply to the humeral head.
Campochiaro et al review Hertel’s criteria of calcar length and medial hinge integrity and its reliability in predicting humeral head necrosis. They reported a 3.7% incidence of ischemia across all 267 fractures evaluated. In those patients that developed AVN, 30% had all of the predictors described by Hertel, however, in the non-AVN group, only 4.7% had these same findings.
They concluded that while Hertel’s criteria are helpful, they may not be sufficient and the authors recommended 3-dimensional evaluation of any fracture involving the calcar.
Xu et al reviewed avascular necrosis in patients with proximal humerus fractures who were treated surgically. They reported on 291 patients throughout 7 studies in which there was no difference in the incidence of AVN for those treated surgically or nonoperatively. However, they concluded through subgroup analysis looking at different fixation constructs that, plate fixation specifically was associated with a higher risk of AVN than conservative management of proximal humerus fractures.
Figure A demonstrates a proximal humerus fracture with a medial calcar length of >8mm attached to the articular segment. Figure B is a proximal humerus fracture with a displaced greater tuberosity fragment. Figure C demonstrates a proximal humerus fracture with a medial calcar length of 8mm.
Incorrect Answers:
Answer 1, 2, 5: These fracture patterns do not have the prognostic characteristics described by Hertel for humeral head ischemia: articular segment calcar length 10mm or angulation >45 degrees.
Answer 4: Humeral head ischemia is very rare following pediatric proximal humerus fractures.
A 34-year-old man presents with the closed injury depicted in Figure A after a high energy twisting injury. Which of the other injuries below is most commonly associated with his known injury?
1) Nondisplaced medial malleolus vertical shear fracture
2) Nondisplaced Volkmann's fragment
3) Nondisplaced Chaput's fragment
4) Nondisplaced lateral wall talar fracture
5) Posterior inferior tibiofibular ligament disruption
This patient has sustained a distal third tibial shaft spiral fracture, which is commonly associated with nondisplaced posterior tibial plafond fractures, with the classic Volkmann's fragment.
Prior to operative management, distal third spiral tibial shaft fractures should always be evaluated for intra-articular extension. As this commonly associated injury can be missed on plain radiographs, an ankle CT is often recommended. This is especially important when intramedullary fixation is used for definitive management of the tibial shaft fracture, as nail insertion can displace a
previously nondisplaced intraarticular fracture. Anterior to posterior lag screw fixation prior to nailing may be useful in these cases.
Sobol et al. investigated the incidence of concomitant posterior malleolar fractures (PMFs) in operative distal third spiral tibial shaft fractures. They reported that spiral distal third tibial shaft fractures were identified with an ipsilateral posterior malleolus fracture in 92.3% of cases. They recommended a preoperative ankle CT in all cases with this specific fracture morphology to properly diagnose this commonly associated injury.
Hou et al. investigated the posterior malleolar fracture association with spiral tibial shaft fractures. They reported that plain radiography (both preoperative and intraoperative) resulted in rare identification of these associated injuries, which resulted in missed injuries. They concluded that a CT or MRI ankle may be a higher yield method to detect these injuries.
Figure A demonstrates a distal third spiral tibial shaft fracture. Illustration A is a schematic demonstrating the Volkmann, Chaput, and medial malleoli intraarticular fragments of the distal tibia.
Incorrect Answers:
Answer 1: Medial malleolar vertical shear fractures are not typically associated with distal third tibial shaft fractures.
Answer 3: Nondisplaced anterior tibial plafond fractures (Chaput's fragment) are not as highly associated with spiral distal third tibial shaft fractures.
Answer 4: Nondisplaced lateral wall talar fractures are not associated with spiral distal third tibial shaft fractures.
Answer 5: The PITFL is typically intact with posterior malleoli fractures.
An 18-year-old male is admitted for a diaphyseal, open, tibial shaft fracture after falling off a motorcycle. He has a past medical history of nicotine dependence and obesity. He undergoes provisional splinting by the resident on call and is noted to be "neurovascularly intact" following splint placement. Throughout the evening, however, the patient has an increasing narcotic requirement and develops pain with passive stretch of his toes. What factor listed below is most associated with his progressive symptoms overnight?
1) Age
2) Male gender
3) Body mass index >/ 30 kg/m^2
4) Open fracture
5) Nicotine use
The highest prevalence of compartment syndrome is found in patients aged 12-19 years, followed by 20-29 years.
One theory for the higher prevalence of compartment syndrome in younger patients is increased muscle mass in this cohort. If there is more muscle in a compartment, there is less room for swelling. On the flip side, elderly or deconditioned patients who have less muscle or fatty atrophy may be better able to accommodate muscle swelling. Additionally, a diaphyseal fracture location is associated with a higher risk of compartment syndrome. Again, this may be due to the fact that there is more muscle than tendon, and thus more swelling, in the proximal leg.
Shadgan et al. retrospectively reviewed 1,125 patients with diaphyseal tibia fractures to look for risk factors associated with the development of compartment syndrome. Compartment syndrome occurred in approximately 8% of patients with this injury. They concluded that younger patients were at a higher risk of developing compartment syndrome and that male gender, open fracture, and intramedullary nailing were not risk factors.
Beebe et al. set out to determine the correlation between the OTA/AO classification of tibia fractures and the development of compartment syndrome. they conducted a retrospective review of a prospectively collected database comprising 2,885 fractures. They concluded that age, sex, and the OTA/AO classification were highly predictive for the development of compartment syndrome in this cohort.
McQueen et al. similarly looked at predictors of compartment syndrome after tibial fractures in a retrospective cohort study. There were 1,388 patients in their study with ages ranging from 12-98; identical to the Shadgan study, 69% of patients were male. They concluded the strongest risk factor was age, with the highest prevalence in 12 to 19-year-olds.
Park et al. additionally analyzed 414 patients with tibia fractures in a retrospective cohort study. The main outcome measure of this study was the rate of clinically determined compartment syndromes requiring fasciotomy by anatomic region. The found that diaphyseal fractures were more frequently associated with the development of compartment syndrome than proximal (next most common site) and distal tibia fractures, specifically in younger patients.
Incorrect Answers:
Answers 2-5: Gender, body mass index, open fracture, and nicotine use are not associated with a higher risk for the development of a compartment syndrome.
Figure A is the radiograph of a 79-year-old female with elbow pain following a fall. Compared with a total elbow artrhoplasty, open reduction and internal fixation would most likely result in?
1) Greater Mayo Elbow Performance Score
2) Greater Disabilities of the Arm, Shoulder and Hand Score
3) Increased flexion-extension arc
4) Increased reoperation rate
5) Decreased complication rate
This patient sustained a comminuted distal humerus fracture. Open reduction and internal fixation (ORIF) is found to have higher repoeration rates compared with total elbow arthroplasty (TEA) in the elderly: 27% versus 12%, respectively.
Distal humerus fractures account for approximately 30% of elbow fractures. There is often a low energy mechanism of injury in the elderly patient. While ORIF and TEA may be utilized in bicolumnar distal humerus fractures in the elderly patient, recent literature has demonstrated favorable outcomes with TEA in this aged cohort. TEA is indicated in the low demand osteoporotic patients with bicolumnar distal humerus fractures that are not amendable to ORIF. Utilization of TEA has demonstrated greater functional outcome scores, greater motion, less complications, and a lower revision rate.
Mckee et al. conducted a prospective, randomized, controlled trial comparing functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with ORIF or primary semiconstrained TEA. They reports that patients who underwent TEA had significantly better motion, performance and outcome scores, lower reoperation rates compared with the ORIF group. They concluded that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF and that TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation.
Githens et al. performed a systematic review and meta-analysis to analyze outcomes and complication rates in elderly patients with intra-articular distal humerus fractures being treated with either TEA or ORIF with locking plates. They report that TEA and ORIF for the treatment of geriatric distal humerus fractures produced similar functional outcome scores and range of motion.
However, they found a non-statistical trend toward a higher rate of major complications and reoperation after ORIF. They conclude that the quality of study methodology was generally weak and ongoing research including prospective trials and cost analysis is indicated.
Figure A is the AP radiograph of a comminuted bicolumnar distal humerus
fracture. Illustration A are the radiographs of a comminuted distal humerus fracture in an elderly patient treated with a TEA. Illustration B is the postoperative radiographs of a comminuted distal humerus fracture treated with ORIF.
Incorrect Answers:
Answers 1-3,&5: TEA has demonstrated greater functional outcome scores, greater motion, less complications, and a lower revision rate compared with ORIF.
Figure A is the postoperative radiograph of an 82-year-old female who was treated with a cephalomedually nail for a left intertrochanteric hip fracture. Which of the following is the most common complication following use of this device?
1) Anterior perforation of distal femur
2) Breakage of the screw
3) Implant cutout
4) Malunion
5) Nonunion
Intertrochanteric hip fractures are most commonly treated with a cephalomedullary nail. The most common complication following utilization of a cephalomedullary nail is implant failure and cutout.
Intertrochanteric hip fractures are extra-capsular injuries that are common in the elderly osteoporotic patient. These injuries carrry a 20-30% mortality rate in the first year following fracture. Femoral cephalomedullary nails are often used to treat these injuries. Often a helical blade or screw may be used to provide fixation within the femoral neck. Overall, the most common complication following use of this device is implant failure and cutout, which occurs most commonly within 3 months following surgery. A known risk factor of this complication is an increased tip-apex distance, with a 60% failure rate reported with a distance exceeding 45mm.
Gardner et al. reviewed the use of a helical blade device to stabilize
intertrochanteric hip fractures. They reported a mean telescoping in unstable and stable fractures of 4.3 mm and 2.6 mm, respectively. They also found that blade migration within the femoral head averaged 2.2 mm overall, with no difference between stable and unstable fractures. They concluded that position changes occurred within the first 6 weeks postoperatively, with no subsequent detectable migration or telescoping.
Haidukewych et al. reviewed patients with failed internal fixation of a hip fracture. They report that salvage options are dependent on the anatomic site of the nonunion, the quality of the remaining bone and articular surface, and patient factors such as age and activity level. They conclude that in younger patients with either a femoral neck or intertrochanteric fracture nonunion with a satisfactory hip joint, treatment typically involves revision internal fixation with or without osteotomy or bone grafting. Conversely, in older patients with poor remaining proximal bone stock or a badly damaged hip joint, conversion to hip arthroplasty is recommended.
Figure A is the AP radiograph of the right hip treated with a cephalomedullary nail. Illustration A demonstrates screw cutout.
Incorrect Answers:
Answers 1,2,4,5: These are not the most common complications following use of a cephalomedullary nail
Figures A is the CT angiogram of a 22-year-old male (Patient A) who presents to the trauma bay after sustaining a low-velocity gunshot injury to the femur. Compared to Figure B, which is a different patient (Patient B) who also sustained a low velocity gunshot wound, the associated injury seen in Patient A places him at increased risk for which of the following?
1) Hip disarticulation
2) Infection
3) Malunion
4) Hardware failure
5) Neuropraxia
This patient sustained a low-velocity gunshot wound to the femur with an associated vascular injury. The presence of a vascular injury has been shown to increase the risk of infection.
A low-velocity GSW is defined as a muzzle velocity
Figure A is the radiograph of a 24-year-old male who presents to the trauma bay following a motor vehicle accident. After initial evaluation the patient begins to become hemodynamically unstable and a pelvic binder is placed. The binder should be centered over what anatomic structure?
1) Anterior superior iliac spine (ASIS)
2) Lesser trochanter
3) Greater trochanter
4) Superior aspect of the iliac crest
5) Umbilicis
Figure A demonstrates an APC 3 pelvic ring injury. In the setting of hemodynamic instability, they should be treated with a pelvic binder centered over the greater trochanters.
APC pelvic ring injuries are highly associated with intrapelvic hemorrhage, most commonly from bridging veins. The pelvis can hold a significant amount of blood; thus, the purpose of the pelvic binder is to decrease the total intrapelvic volume. It is crucial that the binder be placed in the proper position at the level of the greater trochanter. Alternatively, a sheet can be applied to the pelvis if a binder is not available.
Prasarn et al review the difference between external fixation and pelvic orthotic devices in a cadaveric study. They report that with logrolling the patient and with elevating the head of the bed the orthotic device placed at the level of the greater trochanters provided improved stability in all planes, however, this did not reach statistical significance. They conclude that there were no significant differences in the stability conferred by an external fixator and a binder for unstable pelvic ring injuries.
Beltran et al review resuscitation and the treatment of shock. They report that placement of a pelvic binder over the greater trochanters serves as an immediate maneuver capable of reducing pelvic volume and stabilizing the pelvis, ultimately aiding in clot formation. They conclude that sheets may also be used and are widely available and can be cut for vascular access to allow for emergent laparotomy.
Prasarn et al compare circumferential sheeting and the use of pelvic binders for unstable pelvic ring injuries. They report no difference in the motion of the hemipelvis during application, logroll, or elevating the head of the bed. They conclude that sheets are more readily available, cost less and are more versatile than pelvic binders.
Incorrect Answers:
Answers 1,2,4, & 5: For maximal volume reduction and stability, pelvic binders and circumferential sheets should be placed over the level of the greater trochanter.
A 54-year-old female sustains a closed comminuted, intraarticular distal radius fracture and a small ulnar styloid tip fracture. She works as a housekeeper and is otherwise healthy. You are considering external fixation (EF) with supplemental K-wire fixation of her articular surface versus volar locking plate (VLP) application. Which of the following considerations is true?
1) Regardless of method of radius fixation, ulnar styloid tip fractures should be fixed to preserve DRUJ stability
2) Placing a VLP proximal to the watershed line increases the likelihood for flexor tendon injury
3) Wound complications are higher for the VLP
4) Both methods of fixation will yield satisfactory results
5) Pillar pain is likely in both groups
Both external fixation (EF) and volar locking plate (VLP) fixation produce successful results in the treatment of distal radius fractures.
Indications for operative intervention on distal radius fractures generally include younger patients with dorsal angulation, displaced intra-articular fragments, radial shortening, intra-articular shear patterns, or die punch fractures of the lunate facet. EF can effectively reduce and stabilized distal radius fractures although the VLP has become more prevalent in recent times, as evident in the 13-fold increase in surgical fixation of distal radius fractures from 1998-2008. Despite this paradigm shift, external fixation remains an effective treatment for distal radius fractures.
Williksen et al. randomized 111 unstable distal radius fractures to VLP or EF. At 5-year follow-up, the authors found no difference in DASH scores. However, for comminuted intra-articular fractures, VLP demonstrated mildly superior supination, flexion, grip strength, Mayo wrist score, and less ulnar shortening. The authors additionally noted that among the VLP cohort, 21% required HWR for surgical complications. They concluded that both methods of fixation achieved satisfactory outcomes at 5 years.
Agee reviewed multiplanar ligamentotaxis in the reduction and stabilization of distal radius fractures. Ligamentotaxis refers to the tension applied across a fracture by the surrounding soft tissues. Dr. Agee contends that the use of an EF allows for adjustments in many planes which in turn helps restore anatomic alignment until the distal radius fracture heals.
Egol et al. randomized 120 wrist fractures that received EF for fracture stabilization into three groups for pin site care: weekly dry dressings, daily pin site care with hydrogen peroxide, and chlorhexidine discs around the pins. The fixators remained in place for 5.9 weeks and 19% had a pin tract complication. There were no differences between the three groups in terms of the prevalence of pin-site complications. However, increasing the age of the patient was correlated to pin-track complications.
Incorrect Answers:
Answer 1: Ulnar styloid tip fixation is not necessary and an ulnar styloid tip non-union does not have a significant impact on clinical outcomes.
Answer 2: Placement of the VLP DISTAL to the watershed line increases the risk for flexor tendon injury.
Answer 3: Wound complications such as pin tract infection are significantly higher in the EF cohort.
Answer 5: Pillar pain is frequent in carpal tunnel release, but is not commonly reported in distal radius fracture fixation.
An 8-year-old boy is involved in an ATV crash. Xrays were obtained in the trauma bay after being airlifted to your facility, shown in Figures A. On the day of presentation, you perform the treatment shown in the figure B. On postoperative day 1, the patient states his pain is controlled, however, you find that his calf is tense, his foot is cool and has diminished pulses compared to the contralateral extremity. What is the best next step of the options below?
1) Remove your fixation and perform repeat reduction
2) Measure leg compartment pressures
3) Request vascular consultation
4) Measure ankle-brachial index (ABI)
5) Duplex ultrasound evaluation
This patient is presenting with symptoms concerning for compartment syndrome without significant pain. The next best step in evaluation would be to perform compartment pressure measurements.
Compartment syndrome is the process where osseofascial compartment pressures rise to levels that decrease perfusion to the structures within. This is an orthopedic emergency, requiring opening the compartment via fasciotomy to relieve the pressure within. Delay in treatment can result in irreversible muscle and nerve damage. Compartment syndrome is a clinical diagnosis, and treatment should not be delayed if your index of suspicion is high. Diagnosis can be more difficult in children due to inability to verbalize symptoms.
However, compartment pressures can be measured if the clinical picture is uncertain, such as when patients sedated or otherwise have altered mental status. Typically a difference of 48 hours after injury. They conclude by emphasizing the importance of extended vigilance in pediatric patients for the development of compartment syndrome.
Figures A shows an AP radiograph of a tibial shaft fracture in a pediatric patient. Figure B shows a diagram of flexible nailing of a tibia.
Incorrect answers:
Answer 1: This would not aid in the diagnosis or treatment of compartment syndrome.
Answer 3: While vascular compromise can be a late manifestation of the compartment syndrome, the treatment is fasciotomy to re-establish blood flow. Answer 4: An ABI would likely show an abnormality, however, this would not be the appropriate study.
Answer 5: This is the appropriate workup if you were concerned about deep venous thrombosis.
A 72-year-old female presents to your office with a 12-month old painful nonunion of a 2-part (surgical neck) proximal humerus fracture which was managed non-operatively. Prior to her injury, she denied shoulder pain and had excellent range of motion. Since the injury, she has had persistent debilitating pain and dysfunction with motion above the shoulder level. X-Rays show good bone stock, no significant shoulder arthritis or avascular necrosis, and well-positioned tuberosities. Which of the following is the most optimal treatment for the patient?
1) Closed reduction and percutaneous pinning
2) Shoulder hemiarthroplasty
3) Open bone grafting
4) Open reduction and internal fixation (ORIF) with or without bone grafting
5) Reverse total shoulder arthroplasty (rTSA) with lattisimus dorsi transfer to assist with internal rotation
A 2-part proximal humerus non-union in a patient with good bone stock without evidence of arthritis or osteonecrosis can be effectively managed with
ORIF with locked plating with or without bone grafting.
Treatment of a chronic nonunion of the proximal humerus in the elderly should be treated with fixation when possible. Critical attention should be paid to correct all deformities: tuberosity positioning, articular surface realignment, soft tissue balancing, rotator cuff repair (when needed), and treatment of soft tissue contractures. Attempts at arthroplasty are generally recommended only when there is significant osteopenia or avascular necrosis, if the tuberosities have resorbed, if the rotator cuff has a pre-existing tear, or if other findings are present that would limit the success rate of fixation.
A 68-year-old woman undergoes a hemiarthroplasty for a proximal humerus fracture through a deltopectoral approach. Care
should be taken with which of the following activities in the immediate postoperative period due to concerns about lesser tuberosity fixation?
1) Passive forward flexion of the shoulder in the scapular plane
2) Passive internal rotation of the shoulder to the plane of the body
3) Active abduction of the shoulder past 45 degrees
4) Passive external rotation of the shoulder
5) Active extension of the shoulder
Due to extensive pull on the lesser tuberosity via the subscapularis, care should be taken with increased levels of passive external rotation in the immediate post-operative period.
Proximal humerus injuries resulting in head-splitting fractures, avascular necrosis, or nonunion can be treated reliably with arthroplasty. During reconstruction with arthroplasty, the tuberosities need to be anatomically fixed in order to allow for a proper range of motion post-operatively. The subscapularis tendon inserts on the lesser tuberosity and is the deforming force when placed under tension during external rotation and during active internal rotation. As such, post-operative passive external rotation and active internal rotation are both limited initially until the lesser tuberosity has healed in its anatomic location.
Frankle et al. performed a biomechanical study to determine the importance of anatomic fixation of tuberosities after hemiarthroplasty for proximal humerus fractures. The authors noted that non-anatomic tuberosity reconstruction led to significant impairment in external rotation kinematics and an 8-fold increase in torque requirements whereas anatomic reconstruction produced indistinguishable results from normal shoulder controls. The authors concluded that the rotational alignment of tuberosities during reconstruction is critical in order to allow patients to perform an adequate range of motion postoperatively.
Frankle and Mighell performed a review of the techniques of tuberosity fixation for shoulder hemiarthroplasty for the treatment of proximal humerus fractures. The authors describe that variable geometry and known anatomic relationships can facilitate tuberosity reconstruction. This requires a re-producible technique, an instrumentation system, and a prosthesis that can maximize tuberosity reconstruction.
Incorrect Answer:
Answers 1, 2, 3 and 5: Passive external rotation and active internal rotation
both places stress on the lesser tuberosity due to the insertion of the subscapularis tendon and are limited in the immediate post-operative setting following hemiarthroplasty.
A 24-year-old man was involved in a MVC and sustained the injury shown in Figure A. A closed reduction is performed and a post-reduction CT scan is obtained. Which of the following correctly pairs the CT with the most appropriate management?
1) Figure B; Protected weightbearing
2) Figure B; Examination under anesthesia (EUA) to assess hip stability
3) Figure C; Protected weightbearing
4) Figure C; Examination under anesthesia (EUA) to assess hip stability
5) Figure D; Protected weightbearing
This patient sustained a posterior hip dislocation. Of the answer choices listed, the fracture pattern seen in Figure C would be appropriately managed with EUA to assess hip stability.
Posterior wall fractures are the most common type of acetabular fracture. Management of posterior wall fractures is dictated by the extent of posterior wall involvement, with those involving >40-50% best treated with ORIF. Management of fractures involving 20-40% of the posterior wall, on the other hand, should be based on hip stability. As suggested by Tornetta, assessment of hip instability with dynamic stress views is helpful to determine which posterior wall fractures are unstable and therefore require open reduction and internal fixation. Protected weightbearing may be employed if the hip is stable; however, hip stability must be determined first.
Tornetta performed a study to assess the use of dynamic stress views in the non-operative management of acetabular fractures. He found that the use of dynamic stress views in determining the need for ORIF was effective, leading to good or excellent results in 91% of cases. He concluded that dynamic stress views can identify subtle instability in patients who would normally be considered for non-operative treatment.
Moed et al. performed a retrospective study to evaluate the role of CT in predicting hip stability in posterior wall fractures of the acetabulum. They analyzed 3 methods of calculating posterior wall fracture fragment size on CT and compared it to findings on EUA. They found that the alternative method (which measures fragment size at the level of the largest posterior wall deficit) was more accurate than the Calkins method (which measures the smallest amount of intact acetabular arc) and the Keith method (which measures fragment size at the level of the fovea). However, given the low risk of EUA and the inherent problems making CT measurements, they concluded that dynamic fluoroscopic stress testing under general anesthesia should be the preferred method for the determination of hip stability status after posterior wall fractures of the acetabulum.
Calkins et al. performed a study to assess the efficacy of CT in predicting hip stability based on measurements of the percentage of remaining posterior acetabulum. They found that all hips with 55% were stable. They concluded that a simple linear measurement of the remaining posterior acetabulum on CT can be done easily by a physician and can provide a means of predicting hip stability for individual patients.
Figure A is an AP radiograph of the right hip demonstrating a posterior hip dislocation. Figure B is an axial CT of the right hip demonstrating a posterior wall fracture with intraarticular fragments. Figure C is an axial CT of the right hip demonstrating a posterior wall fracture involving > 20% of the posterior
wall. Figure D is an axial CT of the right hip demonstrating a posterior wall fracture involving > 40% of the posterior wall.
Incorrect Answers:
Answer 1: Protected weightbearing would be inappropriate for a posterior wall fracture with intraarticular fragments.
Answer 2: EUA would be inappropriate for a posterior wall fracture with intraarticular fragments.
Answer 3: Posterior wall fractures involving 20-40% of the posterior wall may be treated with protected weightbearing; however, EUA to assess for instability is recommended prior to making the final decision to proceed with nonoperative treatment.
Answer 5: Open reduction internal fixation is indicated in unstable fractures such as posterior wall fractures involving >40-50% of the posterior wall.
A 44-year-old male fell onto his arm and presents to the emergency department with elbow pain, swelling, and inability to use the right arm. The ED staff place the patient in a posterior mold splint and call after radiographs are obtained. The current images are shown in Figures A and B. What is the next best step in management?
1) CT scan of the elbow
2) Examination of the elbow under anesthesia
3) Obtain traction views
4) Continued immobilization and outpatient follow-up in three weeks
5) Immediate ORIF of coronoid, radial head, and repair of LCL
The patient is presenting with an anteromedial facet fracture of the coronoid due to a posteromedial rotatory force. A CT of the elbow should be performed to asses the extent of articular involvement, degree of comminution, and the size of the coronoid fragment.
The coronoid process is one of the main constraints that provide ulnohumeral joint stability. The coronoid process and the radial head provide a buttress against the posterior displacement of the elbow joint. The anteromedial facet of the coronoid process, also known as the sublime tubercle, is the insertion of the anteromedial bundle of the ulnar collateral ligament, which provides valgus stability of the elbow. Fracture of the coronoid process can be either an isolated finding following elbow dislocation or part of a more complex fracture-dislocation. This patient had a fracture to the of the anteromedial portion of the coronoid, therefore the medial side of the elbow is unsupported to varus stresses. As a result, the joint line will narrow from lateral to medial secondary to the medial collapse of the joint. On a lateral, the crescent sign, which represents the depressed anteromedial facet of the coronoid, may be seen.
Steinmann reported that with an anteromedial coronoid fracture, the anteroposterior radiograph of the elbow will demonstrate progressive narrowing of the joint space from lateral to medial between the medial trochlea and the coronoid process. On a lateral radiograph, a coronoid fracture fragment may appear small and may be confused with a radial head fracture. A CT scan of the elbow is recommended in all cases of suspected coronoid fractures because such a fracture is readily seen with this imaging modality.
Doornberg and Ring reported that coronoid fractures are associated with specific patterns of traumatic elbow instability. They concluded that large coronoid fractures were associated with anterior and posterior olecranon fracture-dislocations while small transverse fractures were associated with terrible triad injuries. Finally, anteromedial facet fractures were associated with varus posteromedial rotational instability.
Ring and Doornberg wrote a surgical technique of repairing the anteromedial facet fracture. They report that fractures of the anteromedial facet of the coronoid may be treated with a plate, a screw, or sutures. They conclude that
the secure fixation of this fragment usually restores good elbow function.
Figures A and B are the AP and lateral radiographs of the right elbow with a fracture of the anteromedial facet of the coronoid.
Incorrect Answers:
Answer 2: Though an examination of the elbow would likely reveal instability, given the large fracture evident on radiographs, this would not provide further diagnostic information.
Answer 3: Traction view radiographs are helpful in comminuted distal humerus fractures. In this patient, traction views would provide little diagnostic benefit. Answer 4: Prolonged immobilization of elbow injuries typically results in permanent elbow stiffness. Surgical fixation of the fracture would be preferable to permit early rehab after a CT assessment to determine the extent of the injury.
Answer 5: This is the treatment for terrible triad injury of the elbow. The radial head does not appear to be affected in the current radiographs.
A 58-year-old male active smoker falls while working at his barn and sustains the closed injury depicted in Figures A and B. His neurovascular examination is unremarkable. The decision is made to perform open reduction internal fixation of his proximal humerus. Which of the following characteristics is MOST predictive of humeral head ischemia?
1) Medial hinge disruption
2) Calcar length of 4mm
3) Patient age
4) Lateral hinge disruption
5) Number of fracture parts
This patient has sustained a comminuted 4-part proximal humerus fracture. Of the above fracture characteristics, the most predictive of humeral head
ischemia is calcar length of 4mm.
In complex intra-articular proximal humerus fractures, perfusion of the humeral head is an important consideration when deciding on treatment. Recent evidence has demonstrated that the posterior humeral circumflex artery is likely the main blood supply to the humeral head, and fracture displacement can lead to disruption of this blood supply along with the anterior humeral circumflex artery, causing humeral head ischemia. Several studies have demonstrated that residual perfusion of the humeral head relies predominantly on the medial and posteromedial metaphyseal extension (i.e. calcar length) that might remain attached to the head, with other protective factors including the integrity of the medial hinge and basic fracture patterns .
Hertel et al. investigated predictors of fracture-induced humeral head ischemia at the time of surgery for articular proximal humerus fractures. They reported that the highest predictors of humeral head ischemia, from most accurate to least accurate, were calcar length 45 degrees, displacement of the tuberosities >10 mm, glenohumeral fracture-dislocation and head-split fractures. They concluded that the most relevant predictors of ischemia were the length of the posteromedial calcar, the integrity of the medial hinge, and the basic fracture type.
Nho et al. reviewed innovations in the management of displaced proximal humerus fractures. They reported that treatment should be dictated by careful scrutiny of vascular status, bone quality, fracture pattern, degree of comminution, as well as patient factors, such as age and activity level. They concluded that Fractures with AO type C pattern, metaphyseal extension 2 mm are associated with high probability of humeral head ischemia and likely are best treated with arthroplasty.
Figure A demonstrates a plain radiograph of a 4-part proximal humerus fracture. Figure B is a CT 3D-reconstruction of the 4-part proximal humerus fracture. Illustration A highlights the vascular anatomy of the proximal humerus. Illustration B depicts the differences in posteromedial calcar lengths in proximal humerus fractures. Illustration C highlights the difference between an intact and disrupted medial hinge.
Incorrect Answers:
Answer 1 and 4: While medial (not lateral) hinge disruption may predict humeral head ischemia, a short calcar length (i.e. 4 mm) is more predictive. Answer 3: Patient age is not as strong of a factor in predicting humeral head ischemia like calcar length.
Answer 5: The number of fracture fragment may predict humeral head ischemia, but it is not as strong and relevant of a predictor like calcar length.
You are called to evaluate a 32-year-old man with knee pain after being struck as a pedestrian. You recognize the fracture as a Schatzker IV tibial plateau fracture. Which of the following statements is most accurate?
1) A fracture-dislocation must be suspected as the femur follows the displaced lateral tibial plateau
2) This fracture may often be seen with medial meniscal and anterior cruciate
ligament injuries
3) Open reduction internal fixation with a lateral plating is the construct of choice
4) Open reduction internal fixation with bicondylar plating is the construct of choice
5) Vascular injuries are rare with this type of fracture
Of the above descriptions regarding the Schatzker IV tibial plateau fracture, the most accurate is that it may often be seen with medial meniscal and anterior cruciate ligament injuries.
While the lateral plateau is smaller and convex, the medial plateau is larger and concave, resulting in an eccentric load distribution in which the medial plateau bears ~ 60% of the knee's load. The relative osseous strength of the medial plateau, the valgus anatomic axis of the lower extremity, and the susceptibility of the leg to a medially directed force all result in the increased prevalence of to lateral-sided injuries (Schatzker I and II) in low-energy fractures. High-energy plateau injuries result in increased less predictable fracture patterns that are often comminuted and involve the medial plateau (Schatzker IV through VI) and may be associated with medial meniscus, ACL, and vascular injuries.
Bennett et al. reviewed tibial plateau fractures and associated soft tissue injuries. They reported a 56% rate of associated soft tissue injuries in their series, with the most common being medial, lateral collateral ligaments, and menisci. They observed that Schatzker IV and VI plateau fractures were associated with the highest rate of soft tissue injuries. They recommended pre-and post-fixation stress testing to diagnose collateral and cruciate ligament injuries
Berkson et al. reviewed high energy tibial plateau fractures. They reported that high-energy injuries can lead to comminuted fractures with significant osseous, soft-tissue, and neurovascular injury, whereas lower energy injuries result in unilateral depression type fractures. They emphasized that treatment be directed at safeguarding tissue vascularity and restoring joint congruity and the mechanical axis of the limb.
Illustrations A and B demonstrate a Schatzker IV tibial plateau fracture. Illustration C depicts the Schatzker classification of tibial plateau fractures. Schatzker I is a lateral split fracture, Schatzker II is a lateral split-depression fracture, Schatzker III is a lateral pure depression fracture, Schatzker IV is a medial plateau fracture, Schatzker V is a bicondylar fracture, and Schatzker VI
is a metaphyseal-diaphyseal dissociation.
Incorrect Answers:
Answer 1: A fracture-dislocation must be suspected as the femur follows the displaced medial (not lateral) tibial plateau
Answer 3 and 4: ORIF with a medial buttress plate is the definitive construct often used for Schatzker VI fractures.
Answer 5: Vascular injuries are commonly associated with Schatzker IV plateau fractures.
A 36-year-old female sustains the closed injury shown in Figure A as the result of a high-speed motorcycle collision. She undergoes immediate closed reduction and placement of a knee-spanning external fixator with plans for definitive fixation in 2 weeks. Which of the following is an expected finding in this patient as a result of the placement of a temporizing external fixator?
1) Increased rate of compartment syndrome during hospitalization
2) Increased transient leg compartment pressures during external fixator placement
3) Increased rate of ligamentous knee injury
4) Increased risk of deep hardware infection after 2nd stage surgery
5) Increased risk of malunion after 2nd stage surgery
Application of knee-spanning external fixation as a temporary measure for stabilization of high-energy proximal tibial fractures and dislocations may result in transient elevation of intracompartmental pressures of the leg.
The use of a staged protocol for the treatment of high-energy tibial plateau
fractures has been shown to decrease soft tissue complications. These high energy injuries are best treated with placement of a knee-spanning external fixator which allows ligamentotaxis to maintain overall length. The staged protocol generally consists of closed reduction and placement of a knee-spanning external fixator. Although some controversy exists, the pins are generally not placed within the site of injury or planned area of the plate, in order to minimize infectious risk. The limb is elevated, and ice can be used generously to allow for the resolution of edema. Once the swelling improves, and skin wrinkles are seen, the risk of wound healing complications and infection is decreased, and the surgeon can then proceed with surgery. During the placement of an external fixator, a transient elevation of compartment pressures is expected (DeltaP may fall below the threshold of 30 mm Hg), but this does not appear to lead to the development compartment syndrome.
Egol et al. (2008) reviewed the effect of spanning external fixation in regards to compartment syndrome in 25 patients. They found that 9/22 (41%) had a transient DeltaP
A 72-year-old female with a history of osteoporosis treated with bisphosphonates presents to the ED with bilateral thigh pain after falling backward at home. On examination, there is gross external rotation of bilateral lower extremities with shortening. There are no open skin lesions. Radiographs are shown in figures A and B. What is the total expected blood loss of these injuries?
1) 500-1000 cc
2) 1000-1500 cc
3) 1500-2000 cc
4) 2000-3000 cc
5) 3000-4000 cc
Average blood loss in closed femur fracture averages between 1000 to 1500
cc. With bilateral closed femoral shaft fractures, the expected blood loss would be between 2000 and 3000 cc.
The estimated blood loss for closed fractures of the femur and tibia are 1000-1500 and 500-1000 cc, respectively. Blood loss can double in open fractures. Similarly, bilateral closed femoral shaft fractures can have double the blood loss of a single closed femoral shaft fracture. In the presence of exsanguinating external hemorrhage, control of hemorrhage should take precedence over the ABCDE primary survey.
Lieurance et al. retrospectively reviewed 53 patients with isolated femur fractures. They found that 21 patients required transfusion of an average of
2.5 units PRBCs. The estimated blood loss was 1276cc and not affected by the fracture pattern or high/low energy pattern. They concluded that preoperative hemorrhage contributed to transfusion needs more than intraoperative blood loss.
Lee and Porter reviewed the prehospital management of lower limb fractures. They recommend a stepwise control of bleeding: direct pressure, elevation, wound packing, windlass technique (place a pen under a circumferential knot and rotate the pen until tight), indirect pressure (traction splint), tourniquet. In the presence of compressible/controllable bleeding, they recommend resuscitation to normal physiological parameters. In the presence of non-controllable bleeding, they recommend hypotensive resuscitation (SBP 80mmHg or to restore the radial pulse).
Figures A and B are the AP radiographs of the left and right atypical femur fractures with characteristic cortical thickening, transverse fracture pattern with medial beaking, and lateral stress reaction at the site of the fracture.
Incorrect Answers:
Answers 1, 2, 3, 5: Average blood loss for a closed femoral shaft fracture is 1000-1500 cc, with bilateral fractures having double the blood loss. The other answer choices do not reflect this.
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?
1) Decreased joint penetration of distal screws
2) Increased rigidity
3) Decreased need for delayed hardware removal
4) Decreased peroneal irritation
5) Improved distal fixation
Posterior antiglide plating is a technique that involves placement of a plate on the posterior aspect of the distal fibula, using the plate as a reduction tool and direct buttress against distal fracture fragment displacement.
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
A 24-year-old female sustains a surgical neck proximal humerus fracture in a motor-vehicle collision. She undergoes open reduction and internal fixation but heals in 45 degrees of varus and has significant limitation of shoulder range of motion despite 9 months of conservative treatments. What is the most appropriate treatment at this time?
1) Manipulation under anesthesia
2) Humeral head resurfacing
3) Shoulder hemiarthroplasty
4) Revision open reduction internal fixation with osteotomy
5) Reverse total shoulder arthroplasty
Malunions of the proximal humerus typically result in significant restrictions in range of motion. This young patient has sustained a proximal humeral malunion, and treatment should include a corrective osteotomy for improved outcomes, as she has failed conservative treatment.
The cited reference by Williams et al as well as the referenced article by Siegel et al explain various techniques in management of proximal humerus malunions. They state that the two primary indications for surgical management of proximal humerus malunion include 1) pain and 2) diminished function resulting from limited range of motion. Because this patient is young, you would attempt revision ORIF/osteotomy as opposed to humeral head arthroplasty.
A 6-year-old boy with progressive bilateral genu varum undergoes the surgeries shown in Figure A. On postoperative rounds later that day, the patient appears sedated after several doses of pain medication. His toes are pink with brisk capillary refill however, passive motion of his toes causes pain. Among the answer choices listed, what is the best management strategy for this child?
1) Elevate his legs and reevaluate on morning rounds
2) Adjust his pain medication to accommodate for his increasing pain
3) Administer a muscle relaxant for leg spasms
4) Cast removal and measurement of compartment pressures with a standard device
5) Examine the cast for areas of constriction and reevaluate in the morning
Intracompartmental pressure measurements should be performed when pain with passive motion of the toes is found in young patients with insufficient clinical data to establish a definitive diagnosis of compartment syndrome. The child in this clinical vignette has Blount’s disease which was treated with bilateral tibial osteotomies, a procedure commonly associated with compartment syndrome.
Pain with passive stretch is the most sensitive clinical sign of elevated compartment pressures prior to the onset of ischemia in compartment syndrome. Pain is difficult to assess in children at baseline, therefore, a high level of suspicion should exist and compartment pressure monitoring should be performed in unreliable patients.
Mubarak et al. reported on a series of 27 patients subjected to intracompartmental pressure monitoring for a clinical suspicion of acute compartment syndrome. The wick catheter technique was employed not only to aid in the diagnosis of compartment syndrome at an early stage but also to indicate the effectiveness of the decompressions when used intraoperatively during fasciotomies.
Matsen et al. reported on 24 children with compartment syndrome following injuries and surgery. The most common etiologies identified were fractures, vascular injuries, and tibial osteotomies. Compartment pressure measurements were helpful in establishing the diagnosis of compartment syndrome in young patients and in those with neurologic or vascular injuries with ambiguous clinical findings.
Figure A reveals an AP radiograph of bilateral knees status post valgus-producing tibial osteotomies and epiphysiolyses of the medial tibial physes in a 6-year-old male with Blount’s disease.
Incorrect Answers:
Answers 1 and 5 are wrong because immediate action should be taken to establish a definitive diagnosis and treat accordingly when a clinical suspicion of compartment syndrome arises.
Answers 2 and 3 are incorrect because administering medications that can cause sedation will exacerbate the patient’s present state of drowsiness, confuse the clinical picture, and make the diagnosis of compartment syndrome even more difficult to establish.
A 16-year-old male was struck by an automobile while riding his bicycle. He sustained the injuries in Figure A. Which of the following orthopedic injuries is MOST associated with this injury?
1) Brachial plexus injury
2) Ipsilateral clavicle fracture
3) Pelvic ring injury
4) Rib fracture
5) Spine fracture
Figure A demonstrates a scapula body fracture. Rib fractures are the most common orthopedic injury associated with these high-energy fractures, with a 52% incidence.
Scapula fractures are associated with high-energy trauma and have a reported mortality rate of 2-5%. Approximately 50% of high-energy scapular fractures involve the body and spine. Most scapular fractures may be treated conservatively with sling immobilization followed by early motion with no expected functional deficits. Indications for operative management of scapular fractures include glenohumeral instability with >25% of glenoid involvement or
>5mm of articular step-off, excessive medialization of the glenoid, displaced scapular neck or coracoid fractures, and open fractures.
Baldwin et al. retrospectively reviewed 9,543 scapular fractures utilizing the US National Trauma Database. They reported that the most commonly associated fractures were rib fractures (52.9%), followed by fractures of the spine (29.2%), clavicle (25.2%), and pelvis (15.3%). They concluded that lung and head injuries occurred in 47.1% and 39.1% of the cases, respectively.
Brown et al. retrospectively reviewed the association between scapular fractures (SF) and blunt thoracic aortic injury (BTAI). They found that in 35,541 blunt trauma admissions, SF and BTAI occurred in 1.1% and 0.6% of patients, respectively. They noted that most of the patients with SF had associated injuries (99%), but only four patients with SF had BTAI. The most common injuries associated with SF were rib (43%), lower extremity (36%), and upper extremity (33%) fractures. They concluded that SF is uncommon after blunt trauma, but patients with SF almost always have significant associated injuries and indicates a high amount of energy.
Figure A demonstrates a high-energy scapular body fracture which may benefit from surgical intervention
Incorrect Answers:
Answers 1-3,5: Fractures of the spine (29.2%), clavicle (25.2%), and pelvis (15.3%) are all associated with high-energy scapula fractures, but occur less commonly than rib fractures (52%)
Which of the following amputations will lead to the greatest oxygen requirement per meter walked following prosthesis fitting?
1) Above-knee-amputation (transfemoral)
2) Below-knee-amputation (transtibial)
3) Through Knee
4) Syme
5) Midfoot
The general trend is increasing energy requirement for more proximal amputations. Amputation should be performed at the lowest possible level in order to preserve the most function.
Pinzur compared 5 patients with amputations at midfoot, Syme’s, BKA, through knee, and AKA with five controls. Walking speed and cadence decreased while oxygen consumption per meter walked increased with each more proximal amputation.
The only exception is the Syme which was the most energy efficient even though it is more proximal to the midfoot amputation.
An otherwise healthy 30-year-old male sustains a left forearm injury as a result of a fall from a ladder. Initial examination in the emergency room reveals a clean 2 centimeter laceration over the volar forearm associated with the radiographs shown in Figures A and B. Treatment should consist of irrigation and debridement of the wound followed by which of the following?
1) Closed reduction and casting of left radius and ulna
2) Temporary external fixation of the left radius and ulna
3) Definitive external fixation of the left radius and ulna
4) Open reduction and internal fixation of the left radius and ulna with delayed skin closure
5) Open reduction and internal fixation of the left radius and ulna with immediate skin closure
The clinical scenario is consistent with an open fractures of the distal radial and ulnar shafts. Literature shows that definitive plating of an open forearm fracture followed by primary closure of the wound is acceptable treatment at the time of injury.
Chapman et al performed a retrospective review of 50 patients with immediate internal plate fixation of an open diaphyseal fracture of the forearm. The functional results were excellent or good in 85%.
The review by Levin is a comprehensive review of the literature on early versus delayed closure of open fractures, and covers the change in thought from previous literature, including change in technology, surgical techniques, and a more critical review of previous literature.
During a Lisfranc (tarsometatarsal) amputation of the foot, which of the following is crucial to prevent the patient from having a supinated foot during gait.
1) Releasing the posterior tibialis tendon
2) Preserving the soft-tissue envelope (peroneus brevis, tertius and plantar fascia) around the fifth metatarsal base
3) Myodesis of the anterior tibialis to the medial and middle cuneiforms
4) Lengthening of the gastrocsoleus (achilles tendon)
5) Osteotomy through 1st metatarsal
A Lisfranc amputation is through the tarsometatarsal joints, except the 2nd metatarsal, which is osteotomized to preserve the stability of the medial cuneiform. To prevent the patient from supinating the foot following this amputation, the evertors on the foot must be maintained. The principal evertors are the peroneus brevis and longus (Illustration A). Therefore, the function of the peroneus brevis must be preserved. Technically this is done preserving the soft-tissue envelope (peroneus brevis, tertius and plantar fascia) around the fifth metatarsal base.
Illustration B depicts the level of a Lisfranc amputation of the foot. Incorrect Answers:
1-The posterior tibialis is the primary supinator of the foot, and releasing it
would lead to an eversion deformity. The tibialis posterior tendon attachment to the bases of the second and third metatarsals will actually be released with this amputation, but the main attachment to the navicular preserved.
3-The anterior tibialis dorsiflexes and inverts the foot, but transferring it to the medial and middle cuneiforms would mimick its native function to dorsiflex and invert the foot.
4-A lengthened Achilles would lead to increased dorsiflexion, not supination.
5-Osteotomy of 2nd MT is crucial to preserve the medial cuneiform and midfoot stable.
A 39-year-old male is thrown from his motorcycle into a fast-food restaurant and sustains a closed pelvic ring injury. During placement of percutaneous iliosacral screws, the outlet radiograph in Figure A is obtained. What purpose does this view serve?
1) Evaluation of possible injury to L5 nerve root
2) Evaluation of anterior-posterior position of screw(s)
3) Best visualization of sagittal curvature of sacral ala
4) Best visualization of spinal canal
5) Best visualization of sacral neural foramina
Figure A shows an intraoperative outlet view, which provides the best visualization of the neural foramina (and possible screw placement into these foramina). This view provides information regarding cephalad-caudad placement of the screw, whereas the inlet view provides information regarding the anterior-posterior position of the screw. The lateral sacral view provides information regarding the sagittal curvature of the sacral ala and gives information regarding possible iatrogenic L5 nerve injury as it goes over the sacral ala.
The referenced article by Routt et al is a review article regarding the safety and techniques of percutaneous pelvic ring fixation.
A 35-year-old male sustains a closed Schatzker VI tibial plateau fracture. Two weeks following external fixation, examination reveals intact sensation, palpable pulses and no soft tissue compromise. An axial CT image is shown in Figure A. What is the optimal surgical plan?
1) Medial and lateral plate fixation through two approaches
2) Medial and lateral plate fixation through a single anterior approach
3) Lateral locking plate fixation
4) Continued external fixation until union
5) Multiplanar transarticular external fixator
The Figure shows a bicondylar tibial plateau fracture. The goals that need to be met when treating tibial plateau fractures are the following: restoration of mechanical axis alignment, restoration of condylar width, articular reduction, and restoration of knee stability. Since the soft tissue envelope is favorable, open reduction internal fixation with dual incisions and dual plates will provide the best probablity of achieving those goals.
Gosling et al did a biomechanical evaluation in cadavers comparing lateral locked plating with a combined medial and lateral plate and found no difference in resistance to vertical subsidence even with loads exceeding the average body weight. However, this was a cadaveric study with no mention and capability of analyzing articular reduction. Lateral locked plating only allows for indirect reduction of the medial plateau.
Barei et al in a retrospective review found that comminuted bicondylar tibial plateau fractures can be successfully treated with open reduction and medial and lateral plate fixation using 2 incisions, and postulate that the use of 2 incisions may contribute to a lower wound complication rate. A two incision approach allows not necessarily for a stronger construct as some studies are controversial, but for a more accurate reduction and restoration of alignment.
Which of the following is true regarding the use of the saline injection load test to diagnose traumatic knee arthrotomies?
1) Addition of methylene blue to the saline load test increases the sensitivity of the test
2) Injection of 110ml of saline will diagnose 95% of knee arthrotomies
3) Injection of 175ml of saline will diagnose 99% of knee arthrotomies
4) A superomedial injection location requires significantly less fluid than a inferoeromedial injection location
5) A history and physical exam by an orthopaedic surgeon has equivalent sensitivity to saline load test at detecting a traumatic arthrotomy
Injection of 175ml of saline will diagnose 99% of knee arthrotomies.
Clinical evaluation alone to determine if a periarticular laceration has penetrated the joint can often be incorrect. A Saline Load Test (SLT) is an effective methods to detect intraarticular penetration. New studies have shown addition of methylene blue does not improve the diagnostic value of the saline load test. The use of a CT scan can be helpful, especially in the presence of intra-articular air.
Voit et al. investigated the sensitivity of the clinical exam and a saline load test in 50 consecutive patients with periarticular lacerations suggestive of joint penetration. In 14 there was leakage of fluid on saline load test. In six of these patients, the clinician had judged there was no traumatic arthrotomy based on physical exam and clinical history. They therefore concluded performing a saline load test is important adjunct and the clinical exam alone can not be relied on to detect traumatic arthrotomies.
Nord et al. found that the volumes of saline that were needed in order to effectively diagnose 75%, 90%, 95%, and 99% of the knee arthrotomies were
110, 145, 155, and 175 mL, respectively. They also found that an inferomedial injection location required significantly less fluid than a superomedial injection location did.
Metzger et al. studied 58 patients that underwent saline load test with about 100ml of saline injected (methylene blue 29, normal saline 29). They found that the false-negative rate was 67% (methylene blue 69%, normal saline 66%). They concluded the addition of methylene blue does not improve the diagnostic value of the saline load test.
Konda et al. performed a study evaluationg the role of CT scan versus saline load test. They found that the sensitivity and specificity of the CT scan to detect traumatic arthrotomy was 100%. In a subgroup of 37 patients that received both a CT scan and the conventional saline load test, the sensitivity and specificity of the CT scan was 100% compared to 92% for the saline load test (p
A 36-year-old rancher is involved in a tractor roll-over accident and sustains the injury shown in Figure A to his dominant right arm. After undergoing rigid anatomic fixation of the fracture, the distal radio-ulnar joint (DRUJ) remains incongruent. What is the next step in management?
1) Revision plating of the fracture
2) Revision reduction and intramedullary fixation
3) Reduction of interposed extensor carpi ulnaris tendon
4) Reduction of interposed pronator quadratus tendon
5) Reduction of interposed flexor carpi ulnaris tendon
The most likely cause of persistent DRUJ incongruity after anatomic reduction and fixation of the radial shaft fracture of the answers above is interposition of the extensor carpi ulnaris (ECU) tendon. The tendon must be extricated from the joint to permit DRUJ reduction.
Gaeleazzi fracture-dislocations, such as that seen in Figure A, are typically stable once the radial shaft fracture is anatomically reduced. After fixation, the DRUJ is translated in pronation, supination, and in a neutral position to test for stability. A “clunk” during passive motion of the DRUJ is further evidence of gross instability. Gross laxity can be treated by splinting in supination or by pinning the DRUJ. However, ECU tendon interposition has been reported as a possible cause of a persistently irreducible DRUJ. Radiographic findings typically demonstrate a dorsally displaced ulnar head and a widened DRUJ. The interposed tendon must be removed from the joint, often through a separate dorsal approach to permit DRUJ reduction.
Bruckner et al. review the evaluation and management of complex dislocations of the DRUJ. The authors note that these injuries are associated with frequent irreducibility, recurrent subluxation, or soft reduction of the DRUJ secondary to interposed tissue. In their institutional series, four of the 11 cases of Galeazzi fractures were associated with complex DRUJ dislocations, most commonly due to displacement of the ECU tendon volar to the ulna, necessitating open reduction. They cautioned that unobtainable or unconvincing reductions should warrant surgical exploration.
Paley et al. reported two cases of an irreducible DRUJ after radial shaft fracture fixation. The authors describe an empty ECU tendon sulcus on the dorsum of the wrist in both cases. One case was noted and addressed intraoperatively.
However, the second case was not identified and this patient went on to endure persistent subluxation and diastasis of the DRUJ, ultimately experiencing a poor result. The authors advocate a separate dorsal exposure to reduce the ECU.
Hanel and Scheid reported a case of entrapment of the ECU in the DRUJ in a skeletal immature 12 year old boy. They noted that intraoperative radiographic analysis was significant for a widened DRUJ and dorsally displaced ulnar head. These authors too advocated a separate dorsal exposure to approach and extricate the ECU tendon.
Incorrect answers
Answer 1: The fracture is anatomically reduced but the DRUJ is incongruent because of an interposed ECU tendon. Revision fixation will not address the DRUJ incongruity.
Answer 2: The type of fixation is not the issue. Revising the fixation to another construct will not address the ECU interposition.
Answer 4: Pronator quadratus interposition has not been described in the setting of irreducible DRUJ dislocations.
Answer 5: Flexor carpi ulnaris tendon interposition has also not been described in the setting of irreducible DRUJ dislocations.
A 58-year-old right-hand-dominant computer programmer trips and falls onto his right arm. He reports right arm pain and that his elbow felt "sloppy". His initial lateral radiograph is shown in Figure A. The orthopedic junior resident counsels him that he will likely need a radial head arthroplasty, ligament repair, and possible fixation of the ulna. What factor would most significantly affect the decision to surgically address the ulna fracture?
1) Degree of radial head comminution
2) The deforming force acting on the avulsed fracture fragment
3) Size of fragment and elbow stability after radial head replacement
4) The degree of fracture displacement
5) Patient age and bone quality
The size of the fragment and degree of elbow instability following radial head fixation or replacement most often determines the intraoperative decision on coronoid fragment fixation.
The radial head is a secondary restraint to posterolateral rotatory instability (PLRI) of the elbow, while the coronoid provides an anterior and varus buttress to the ulnohumeral joint, resisting posterior dislocation. The medial ulnar collateral ligament attaches to the anteromedial facet of the coronoid, so large medial facet fractures may displace and cause varus posteromedial instability (PMRI). However, in terrible triad injuries (causing PLRI), small coronoid tip fractures are more common. These are typically left as they most often do not contribute to elbow instability. Therefore in most cases, radial head replacement and lateral ligamentous repair are sufficient to restore stability.
However larger coronoid base fractures may require fixation in order to stabilize the elbow. In these cases, the coronoid fracture may be addressed through the lateral window after radial head resection and before the trial implant is assessed. The anterior capsule can be tied down to the ulna or if the fracture is large enough, it may sometimes tolerate internal fixation.
Conversely, a buttress plate for the coronoid may be applied via a medial approach in the setting of a large coronoid base fracture as in PMRI.
Ring et al. reviewed 11 terrible triad injuries including 7 of which had the radial head surgically addressed and 4 of which had undergone radial head excision. The authors found that all four patients who underwent radial head excision dislocated after surgery. Only four patients had a satisfactory result, and all of these had fixation of the radial head, two requiring concomitant repair of the lateral ulnar collateral ligament (LUCL). The authors concluded that terrible triad injuries were unstable, prone to redislocation and that radiocapitellar contact is critical for ulnohumeral stability.
Pugh et al. reviewed 36 cases of terrible triad injuries in which all coronoid fractures were addressed, either with screw fixation or suture repair of the anterior capsule. The authors reported that the average arc of motion postoperatively was 112 degrees, Mayo score was 88, and concentric stability was restored in 34/36. There were 8 complications requiring re-operation. They concluded that coronoid fixation with radial head fixation or replacement yields a stable elbow suitable for early motion.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They found that radial head excision even in the setting of an intact LUCL lead to posterolateral laxity. Furthermore, if 30% of the coronoid tip was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement. However, if 50% of the coronoid was
excised, even with a radial head replacement dislocation occurred. They concluded that so long as the radial head is replaced, small coronoid fractures may not need to be repaired.
Figure A demonstrates a comminuted radial head fracture, a small coronoid fracture, and subluxation of the ulnohumeral joint.
Incorrect answers:
Answer 1: The degree of radial head comminution impacts the decision to replace or fix the radial head. However, this does not affect the decision to fix the coronoid.
Answer 2: Though the tip of the coronoid often remains attached to the anterior capsule which attaches slightly distal to the coronoid tip, there is no deforming force on this fracture which is instead a shear and not an avulsion injury.
Answer 4: Elbow stability, not the degree of coronoid displacement, affects the decision to address the fracture.
Answer 5: The patient's age and bone quality does not factor into elbow stability or decision making on coronoid fixation.
What is the most appropriate plating technique utilized for the medial malleolus fracture typically seen in a displaced supination-adduction ankle fracture?
1) Tension band plating
2) Antiglide plating
3) Bridge plating
4) Neutralization plating
5) Submuscular plating
A supination-adduction ankle fracture leads to a vertical fracture of the medial malleolus. Traditional fixation of the medial malleolus with oblique screws from the tip of the malleolus directed proximally will ineffectively protect against shear forces at the fracture site; these also are directed quite obliquely to the vertical fracture line, and therefore have poor biomechanical resistance to failure. An antiglide plate is used medially to prevent displacement of the fracture segment due to shear forces.
According to the referenced article by Toolan et al, placement of two horizontal (perpendicular to the fracture line) lag screws from medial to lateral are
biomechanically the most important aspect of the construct whether a plate is used or not.
A 25-year-old Norwegian amateur curler slips on the ice, falling onto an outstretched right elbow. He is taken to the local teaching hospital and radiographs demonstrate a significantly comminuted radial head fracture and coronoid base fracture. His elbow is reduced and splinted. To restore stability and allow early range of motion, which of the following will most likely need to be performed in most cases?
1) Radial head fixation or replacement
2) Radial head fixation or replacement and coronoid fixation
3) Radial head fixation or replacement, coronoid fixation, and lateral ulnar collateral ligament (LUCL) repair
4) Radial head fixation or replacement, coronoid fixation, LUCL and medial ulnar collateral ligament (MUCL) repair
5) Radial head fixation or replacement, coronoid fixation, LUCL and MUCL repair, and application of a hinged fixator
The patient has sustained a "terrible triad" injury, classically involving a radial head fracture, coronoid fracture, and elbow dislocation. These often involve LUCL injuries and a traumatic injury in the radiocapitellar joint. Stability is achieved with radial head replacement (or fixation), coronoid fixation (in cases with a large coronoid fracture), and lateral soft tissue repair.
Posterolateral rotatory instability (PLRI) following a terrible triad injury is usually caused by a fall on an extended arm that produces a valgus, axial, and rotatory force. The mechanism of injury begins laterally and moves medially.
Hence, the LUCL fails first, followed by the anterior capsule (or coronoid), and lastly the MUCL. Even following fixation, patients often lose some degree of their flexion-extension arc, may develop post-traumatic arthritis, or most commonly may have persistent instability. The radial head is a primary restraint to PLRI and must be either replaced with a prosthesis or fixed in the setting of a terrible triad injury. Replacement is typically chosen when the radial head is in more than 3 fragments. Coronoid fractures should be fixed when they involve >30-50% of the coronoid base. However, the best way to determine if coronoid fixation is necessary is with an intraoperative fluoroscopic examination.
Forthman et al. reviewed outcomes following the management of 34 elbow fracture-dislocations. In all cases, the radial head was replaced or underwent fixation. The MUCL was not repaired in any case. The authors noted only 2 cases of post-operative instability, one terrible triad, and one combined capitellum and trochlea fracture. The authors noted that both cases were related to non-compliance. The remaining 32 averaged 120 degrees of flexion-extension and 74% had good-excellent outcomes. The authors concluded that MUCL repair is not required for elbow dislocations so long as the radial head, large coronoid fractures, and LUCL are addressed.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They found that radial head excision even in the setting of an intact LCL leads to posterolateral laxity. If 30% of the coronoid was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement. However, if 50% of the coronoid was excised, even with a radial head replacement, dislocation occurred. This led the authors to conclude that long as the radial head was replaced, small coronoid fractures may not need to be repaired.
Papatheodorou et al. reviewed 14 terrible triad injuries (all of which had Regan-Morrey type 1 or 2 coronoid fractures) that underwent surgical fixation or replacement of the radial head combined with LUCL repair. The authors noted that intraoperative stability was confirmed in all cases without coronoid fixation, MCL repair, or an external fixator. The authors concluded that coronoid fixation is not required in fractures up to 50% the height of the coronoid and that MCL repair is not necessary.
Incorrect answers:
Answer 1: Large coronoid base fractures need to be fixed in PLRI to confer elbow stability.
Answer 2: The lateral collateral ligamentous complex should be repaired as this soft tissue sleeve is usually avulsed in elbow dislocations.
Answer 4: In PLRI, ligamentous repair of the medial aspect of the elbow is often unnecessary.
Answer 5: A hinged fixator (internal or external) is not typically required. This could be applied in a case where the elbow is persistently unstable at the conclusion of the case.
A 32-year-old female sustains the injury shown in Video A. The right-sided pelvic injury is best classified as which of the following?
1) Lateral compression 1
2) Lateral compression 2
3) Vertical shear
4) Anterior-posterior compression 2
5) Anterior-posterior compression 3
The injury shown in Video V reveals a right sided posterior ilium fracture, which is known as a crescent fracture. The presence of a crescent fracture is consistent with a lateral compression type 2 injury; this differentiates this from a type I injury. The ipsilateral anterior sacrum has a small impaction injury anteriorly while the contralateral SI joint has a minor amount of anterior sacral impaction indicative of a lateral compression type I injury.
The reference by Burgess et al is the primary source of the mechanism classification of pelvic ring injuries. Overall blood replacement averaged 5.9 units (lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units). Overall mortality was 8.6% (lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear,
0%; combined mechanical, 18.0%).
Incorrect answers:
1: The presence of a crescent fracture means this is at least a LC-2 injury. The left-sided fracture pattern is consistent with an LC-1 pattern.
3: A vertical shear fracture pattern would exhibit some vertical displacement and does not typically exhibit the crescent fragment.
4: The fracture pattern does not match an anterior-posterior compression pattern.
5: The fracture pattern does not match an anterior-posterior compression pattern.
A 35-year-old zookeeper fell 10 feet while preparing an exhibit for a grand reopening, landing on his left arm. The patient is then evaluated by a keen orthopedic resident in the emergency room who describes the zookeeper's injuries to his chief. He describes a comminuted radial head fracture and posterolateral ulnohumeral dislocation. The chief resident orders a CT scan which demonstrates a coronoid fracture involving 50% the height with no involvement of the anteromedial facet. During surgery, the trauma surgeon replaces the radial head and repairs the lateral collateral ligament complex. The
elbow is splinted in elbow flexion and pronation. The patient begins range of motion exercises with her occupational therapist 3 days after surgery, and her elbow dislocates. What is the most likely reason for her instability?
1) Length of immobilization
2) Position of immobilization
3) Lack of coronoid fixation with medial buttress plate
4) Lack of coronoid fixation from lateral approach
5) Lack of medial collateral ligament repair
The zookeeper sustained a "terrible triad" injury with resulting posterolateral rotatory instability (PLRI). To prevent post-operative instability, large coronoid fractures should be fixed, and this would be performed through a lateral approach given that the radial head will be replaced.
The coronoid serves as an anterior and varus buttress to the ulnohumeral joint, resisting posterior dislocation. Though the coronoid tip has no soft tissue attachments, the medial ulnar collateral ligament attaches to the anteromedial facet of the coronoid. A coronoid fracture through the anteromedial facet, such as in the setting of posteroMEDIAL rotatory instability, would require a medial buttress plate to restore varus stability. In a coronoid base fracture involving 50% of the coronoid, fixation is required even when a radial head arthroplasty is performed. This can be done with suture fixation via a bone tunnel through the ulna or with screws from dorsal to volar. Failure to fix a large coronoid base fracture would result in persistent instability, as with the patient in this vignette.
Ring et al. reviewed 11 terrible triad injuries - including 7 of which had the radial head surgically addressed and 4 of which underwent radial head excision. They noted that all four patients who underwent radial head excision dislocated after surgery. Moreover, only four patients had a satisfactory result, and all of these had fixation of the radial head, with two requiring concomitant repair of the lateral ulnar collateral ligament (LUCL). The authors concluded that terrible triad injuries are unstable, prone to redislocation and that radiocapitellar contact is critical for ulnohumeral stability.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They showed that radial head excision even with an intact LUCL resulted in persistent posterolateral laxity. If 30% of the coronoid was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement alone. If 50% of the coronoid was excised, even with
a radial head replacement, dislocation occurred. The authors concluded that so long as the radial head was replaced, small coronoid fractures may not need to be repaired, but large fractures involving 50% or more would require fixation even if the radial head and LUCL were addressed.
Moro et al. treated 25 unreconstructible radial head fractures with a metal radial head arthroplasty. The authors reported a DASH score of 17, PRWE of 17, and Mayo elbow score of 80. Poor outcomes were seen in those with psychiatric disorders or those involved in a worker's compensation claim. The authors reported that radial head arthroplasty resulted in stable elbows with mild-moderate physical impairment.
Ring, Quintero, and Jupiter reviewed 56 patients with radial head fractures who underwent surgical fixation. Of the comminuted Mason type-3 fractures that underwent ORIF, they found that 13/14 had a poor result. The authors recommend that fractures with 3 or fewer fragments are amenable to fixation while those with 4 or more articular fragments are not.
Incorrect answers:
Answer 1: Early range of motion is appropriate after adequate fixation. Answer 2: Flexion and pronation is the position that stabilizes the lateral elbow. In the setting of PLRI, this is the correct position to splint the upper extremity in following surgery, therefore the position of immobilization is not the issue in this case.
Answer 3: Large anteromedial facet fragments result in posteromedial rotatory instability. These do not typically occur in conjunction with a radial head fracture. These result in varus instability and need to be buttressed with a medial plate. In this case, a medial buttress plate is not needed.
Answer 5: In PLRI, the medial side of the elbow is not typically addressed. The more obvious cause of instability is the lack of coronoid fixation.
Which of the following injuries would require plating of the radius along with closed reduction and evaluation of the distal radioulnar joint (DRUJ)?
1) Nightstick fracture
2) Galeazzi fracture
3) Monteggia fracture
4) Rolando fracture
5) Smith fracture
A Galeazzi fracture is a fracture of the distal third of the radius with dislocation of the distal radioulnar joint. It commonly results from a fall onto an outstretched hand with the forearm in pronation.
A Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction and fixation of the radial shaft, and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. Otherwise, either open or closed reduction with pinning can be undertaken to stabilize the joint. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
Acute intervention results in improved outcomes as compared to delayed reconstruction.
Rettig et al. retrospectively analyzed 40 patients with Galeazzi fracture-dislocations that were treated with open reduction and internal fixation of the radial shaft fracture. They noted that a radial shaft fracture located within
7.5cm of the articular surface resulted in a 55% incidence of DRUJ instability, while 5.6% of those located further from the joint were unstable. They concluded that a high index of suspicion, early recognition, and acute treatment of DRUJ instability will avoid chronic problems in this complex injury.
Illustration A is an AP and lateral radiograph demonstrating a Galeazzi fracture. Incorrect Answers:
Answer 1: A nightstick fracture is an isolated ulnar shaft fracture.
Answer 3: A Monteggia fracture is a proximal ulnar fracture associated with a radial head dislocation.
Answer 4: A Rolando fracture is a comminuted intra-articular fracture through the base of the first metacarpal bone.
Answer 5: Smith fractures are fractures of the distal radius with associated volar angulation of the distal fracture fragment(s).
In trauma patients with multiple injuries, patients with scapula fractures have been shown to have an association with which of the following, as compared to patients without scapula fractures?
1) Increased length of hospital stay
2) Increased mortality rate
3) Increased rate of extremity fracture(s)
4) Increased Injury Severity Scores
5) Increased length of intensive care unit stay
According to the reference by Veysi et al, patients presenting to a trauma center with scapula fractures have an increased rate of pulmonary complications and increased Injury Severity Scores (ISS), but have no difference in mortality, length of ICU stay, or overall hospital stay. No differences were seen in abdominal or head injury rates either. A lower rate of extremity fractures was seen as compared to non-scapular fracture patients in their series.
According to the referenced study by Brown et al, rib fx (44%) are the most common associated injury with scapula fractures.
All of the following techniques can help to prevent apex-anterior angulation during intramedullary nailing of proximal one-third tibia fractures EXCEPT:
1) Posterior blocking screw
2) Posterior starting hole
3) Interlocking the nail in a semi-extended knee position
4) Anteriorly directing the nail
5) Anterior blocking screw
Sagittal malalignment is commonly seen after nailing proximal tibia fractures. The start point as well as the direction of the nail can lead to sagittal deformity. Freedman found in nailing tibia fractures that malalignment was seen in 58% of proximal third fractures, 7% of middle third fractures, and 8% of distal third fractures. Of the malaligned fractures, 83% were either segmental or comminuted.
Lang found that a medialized nail entry point and a posteriorly and laterally directed nail insertion angle contributed to malalignment. It is logical that a fracture that is reamed and then nailed in the posterior direction will lead to a gap anteriorly, and that posterior comminution will lead to anterior angulation as the fracture hinges on the intact cortex anteriorly. An anterior starting hole will tend to lead to more of a posterior nail direction.
Tornetta found that using only 15 degrees knee flexion (semi extended) eliminated the extension force of the quadriceps on the proximal fragment, which otherwise would have tended to cause anterior angulation at the fracture site; therefore interlocking in flexion leads to anterior angulation.
Krettek found that a posteriorly placed blocking screw is meant to prevent posterior placement of the nail and therefore encourages decreased anterior angulation of the fracture.
Henley found that if the fracture is high and the nail bend is within the distal fracture fragment, as the nail is inserted, the nail will drive the distal fragment posteriorly.
Which of the following factors has been shown to be the strongest predictor of screw cutout of a dynamic compression hip screw used for an intertrochanteric femur fracture?
1) Age of the patient
2) Intrinsic stability of the fracture
3) Tip-apex distance
4) Quality of reduction
5) Angle of the sideplate
Illustration A found below depicts the method to calculate Tip-apex distance (TAD). The tip-apex distance is the sum of the distances from the tip of the lag screw to the apex of the femoral head as seen on the AP and lateral radiographs.
Baumgaertner et al reported that he had no screws cut out if the tip-apex distance was less than 25mm. Tip-apex distance was the strongest predictor of cutout. Increasing age of the patient, poor reduction, use of a high angle sideplate, and unstable fracture were weaker predictors of cutout.
Kyle et al demonstrated that obtaining an anatomic reduction when using a sliding hip screw with intertrochanteric fractures leads to the best radiographic and clinical outcomes.
A 66-year-old male sustains an open crush injury to his right lower leg with significant skin loss. His history is significant for COPD, diabetes controlled with an insulin pump, and testicular cancer treated with bleomycin twenty years ago. A radiograph of the chest shows a small pneumothorax which is being observed and does not require a thoracostomy tube. Which of the following is not a contraindication to hyperbaric oxygen treatment for this patient?
1) Presence of an acute open fracture and crush injury
2) History of COPD
3) History of bleomycin treatment
4) Presence of a pneumothorax
5) Presence of an insulin pump
The presence of a crush injury to an extremity is an indication for hyperbaric oxygen (HBO) therapy. The remainder of the options listed are contraindications to hyperbaric oxygen treatment.
Hyperbaric oxygen therapy potentially can provide enhanced oxygen delivery to peripheral tissues affected by vascular disruption, cytogenic and vasogenic edema, and cellular hypoxia caused by extremity trauma. The idea behind HBO is to provide enhanced oxygen delivery to peripheral tissues affected by vascular disruption, cytogenic and vasogenic edema, and cellular hypoxia caused by extremity trauma.
Greensmith et al provide a review of HBO therapy and discuss the relative and absolute contraindications and indications for this treatment. They report in patients with crush injury or early compartment syndrome, hyperbaric oxygen therapy may reduce the penumbra of cells at risk for delayed necrosis and secondary ischemia. They report that both animal studies and prospective human clinical trials suggest the benefits of such therapy.
Buettner et al found that based on clinical evidence and cost analysis, medical institutions that treat open fractures and crush injuries are justified in incorporating HBO theray as a standard of care.
Illustration A shows an example of a hyperbaric oxygen(HBO) chamber. Incorrect Answers:
Answer 2: COPD is a contraindication to hyperbaric oxygen treatment due to
the possible presence of air trapping or bleb formation, which could place the patient at risk of pneumothorax.
Answer 3: History of bleomycin treatment is a contraindication to hyperbaric oxygen treatment because supplemental oxygen may cause life threatening pneumonitis.
Answer 4: Presence of a pneumothorax is a contraindication as hyperbaric oxygen treatment may cause a gas embolism, tension pneumothorax, or pneumomediastinum.
Answer 5: Presence of an insulin pump is a contraindication to hyperbaric oxygen treatment because malfunction or deformation of the device may occur under pressure.
A 34-year-old male falls off of a ladder and sustains the ankle injury shown in Figure. Which of the following is unique with this particular ankle fracture pattern and must be recognized by the operating surgeon to optimize outcomes?
1) Marginal impaction of the anteromedial tibial plafond
2) Syndesmosis diastasis
3) Deltoid ligament tear
4) Posterolateral osteochondral lesion of the talus
5) Fibular overlengthening
The radiograph demonstrates a Lauge-Hansen supination-adduction fracture-dislocation. There is a transverse fibula fracture and a vertical medial malleolus fracture.
McConnell and Tornetta performed a Level 4 review and found that nearly 50% of these injuries have marginal impaction of the anteromedial tibial plafond and they found that anatomic reduction of that aspect of the injury led to good to excellent outcomes.
A 42-year-old female undergoes a subtalar bone block distraction arthrodesis as sequelae of a nonoperatively treated calcaneus fracture ten years prior. This procedure improves which of the following issues?
1) Subtalar joint stiffness
2) Midfoot supination
3) Sinus tarsi impingement
4) Anterior ankle impingement
5) Hammertoe deformity
The subtalar fusion technique involves distraction of the subtalar joint, insertion of a bone block, fusion, and rigid screw fixation. The distraction allows correction of the talocalcaneal relationship.
In Carr’s series, pre- and postoperative radiographic analysis for tibiotalar impingement, lateral talocalcaneal angle, and talonavicular alignment was performed, with improvement to a normal range seen in the cases analyzed.
Bednarz did a radiographic analysis and showed an average increase of 8 mm in hindfoot height, 9 degrees in lateral talocalcaneal angle, and 11 degrees in lateral talar declination angle.
Rammelt found that compared with the unaffected side, the talocalcaneal height was corrected by 61.8%, the talus-first metatarsal axis by 46.5%, the talar declination angle by 38.5% and the talocalcaneal angle by 35.4%. Based on these three
Posterior malleolar fractures most often occur in the setting of rotational ankle injuries and almost always with concomitant fracture of the lateral and/or medial malleoli. The posterior malleolus is not only an important buttress to posterior translation of the talus, but serves as the origin of the posterior inferior tibiofibular ligament (PITFL) and is therefore essential to syndesmotic stability. For this reason, most authors recommend anatomic reduction and fixation or large posterolateral fragments. The ideal surgical approach is controversial, with some advocating for indirect reduction with anterior-to-posterior screw fixation and others for direct visualization through a posterolateral approach. The posterolateral approach is advantageous in that it provides for both anatomic reduction and fixation of the posterior malleolus as well as the often associated lateral malleolar fractures through the interval between the flexor halluces longus and peroneal tendons.
Irwin et al. review the presentation and management of posterior malleolar fractures. They discuss the various surgical techniques which have been described, noting that the posterolateral approach provides the most direct visualization through which anatomic reduction and fixation can be achieved of both the posterior malleolar and distal fibular fractures. There is debate over which fracture should be fixed first, as fibular fixation can restore length and facilitate reduction of the posterior malleolus, but the fibular hardware often interferes with fluoroscopic visualization.
Forberger et al. evaluated the functional outcomes and morbidity following fixation of posterior malleolar fractures via a posterolateral approach performed in 45 consecutive patients. The authors found that the approach not only permitted excellent surgical exposure and stable fixation of the posterior malleolar fragment, but complications were minimal. Functional outcomes were furthermore excellent in the majority of patients.
Figures and Illustrations:
Figures A through C are AP, oblique, and lateral radiographic views of a right ankle demonstrating displaced fractures of the lateral and posterior malleoli. Figure D is an axial CT scan of the right ankle following closed reduction and splint application.
Illustration A is demonstrates the plane of the posterolateral approach. A cadaveric specimen is shown with a pin in the lateral malleolus retracting the peroneal tendons (2) laterally. The Achilles (5), FHL (1) and PITFL (3) are shown. The posterior malleolus (4) is visualized in the interval between the distal fibula and FHL.
Incorrect Answers:
: This is not considered an internervous plane, given that the sural nerve is strictly sensory.
Answer 2: This interval describes medially-based approaches to the foot. Answer 3: This interval describes the anterolateral approach to the ankle. Answer 5: A true internervous plane between the tibial and superficial peroneal nerves exists.
Figures A-C are the radiographs of a 26-year-old male who presents to the emergency department following a motocross accident. Two attempts at a closed reduction by the on-call orthopedic resident were unsuccessful. Figures D and E are the pre-operative axial CT-images that were obtained. The patient undergoes surgical fixation seen in Figure F. Limitations in post-operative dorsiflexion is likely influenced by which of the following?
1) Fracture extension to the posteromedial rim
2) Initial displacement of the fibula fracture
3) Posterolateral approach to address both the fibula and posterior malleolus
4) Initial talar subluxation
5) Inability to reduce the ankle
This patient sustained a Bosworth fracture-dislocation and a posterolateral approach to the ankle is used to reduce the fibula back into the incisura and stabilize both the fibula and posterior malleolus. Loss of dorsiflexion is the most common arc of motion that is limited following this fracture pattern with posterior fixation.
The rare Bosworth fracture-dislocation is a posterior dislocation of the fibula which becomes entrapped behind the tibia. As demonstrated in this vignette, these injuries are extremely difficult to close reduce secondary to the ridge of the posterolateral distal tibia. The irreducible nature of this injury is a known risk factor for the development of compartment syndrome. The CT images further demonstrate fracture extension to the posteromedial rim (“posterior pilon variant”). In this situation, the only effective method to reduce the fracture is through an open posterolateral approach with the interval between the flexor hallucis longus and the peroneal tendons. This is the same approach that is utilized for fixation of the posterolateral fragment and fibula. Loss of dorsiflexion has been demonstrated following this fracture pattern with posterior fixation. The positioning of the plates in Figure F suggests the
utilization of a posterolateral approach.
Switaj et al. retrospectively reviewed 270 patients with posterior malleolus and pilon variant fractures that were operatively treated. They reported that female gender, increasing age, and diabetes may be associated with both fractures of the posterior malleolus as well as the posterior pilon variant. They concluded that the relative frequency of the posterior malleolar fracture and posterior pilon variant in operatively treated ankle fractures was 50% and 20%, respectively.
Gardner et al. reviewed closed pronation-external rotation 4 (PER4) ankle fractures that involved the posterior malleolus without a complete tear of the posterior-inferior tibiofibular ligament (PITFL) treated with either posterior malleolus ORIF or syndesmotic stabilization. They reported that stiffness was restored to 70% after fixation of the posterior malleolus, and to 40% after syndesmosis stabilization. They concluded that syndesmotic stability may be obtained more effectively by the fixation of the posterior malleolus rather than by using a syndesmotic screw.
Berkes et al. reviewed 108 supination-external rotation 4 (SER4) fractures to examine the impact of articular surface congruity on the functional outcomes. They reported that 33% of patients had elements of articular surface incongruity on postoperative CT scanning. They found that the group with articular incongruity had significantly worse foot and ankle outcome scores (FAOS) with regards to symptoms, pain, and activities of daily living. They concluded that the presence of postoperative articular incongruity correlated with inferior early clinical outcomes.
Kalem et al. compared the results of AP screws, PA screws and posterior buttress plate use for posterior malleolar fixation of trimalleolar fractures. They report better AOFAS scores in the PA group and the plate group compared to the AP screw group. However, they concluded that utilization of a posterolateral approach was found to have a loss of ankle dorsiflexion of 5 degrees or greater for both the PA screws and plate groups; 39% and 24%, respectively.
Chen et al. addressed the term “posterior pilon” in their letter to the Editor. He reports that this term was first introduced to describe severe trimalleolar fractures with the presence of a fourth fragment located deeper than the avulsed posterior fragment. The mechanism for this injury results from the impaction of the posterior fragments secondary from axial loading, which is the main causative factor of a classic pilon fracture.
Figures A-C: The initial radiographs reveal the posterior subluxation of the talus with associated posterior subluxation of the fibula without significant coronal plane deformity. This deformity should raise the suspicion of a Bosworth fracture-dislocation, especially if closed reduction is not successful. Figures D and E: Axial CT images demonstrating Bosworth fracture-dislocation of the fibula entrapped behind the tibia. Also, note the fracture extension to the posteromedial rim in this posterior pilon variant.
Figure F: Positioning of the plate suggests a posterolateral approach to address both the fibula and posterior malleolus fractures.
Incorrect Answers:
Answer 1: Fracture extension to the posteromedial rim makes this a "posterior pilon variant," but in itself is not the reason for a decrease in postoperative dorsiflexion
Answer 2: Initial displacement of the fibula fracture may be significant with some ankle injuries. However, the amount of initial displacement has not been correlated with a loss of postoperative dorsiflexion.
Answer 4: The presence of talar subluxation is often seen with ankle injuries. While this may be a result of a large posterior malleolus fragment requiring surgery through a posterolateral approach, the subluxation itself has not been shown to limit postoperative dorsiflexion.
Answer 5: The inability to reduce the ankle may suggest a Bosworth fracture-dislocation. Though reduction helps with soft tissue swelling and chondrolysis, it has not been shown to correlate with postoperative dorsiflexion limitations.
A 69-year-old man presents with the injury depicted in Figures A and B after a fall from his attic. On initial presentation, his lower extremity strength is grade 3/5 but has full sensation in bilateral lower extremities. When his indwelling urinary catheter is pulled, his anal sphincter tightens. He remains bed-bound for the next 4 days and unfortunately develops aspiration pneumonia, requiring urgent intubation and increased positive end-expiratory pressures and a high ventilatory rate to keep him oxygenated. He remains febrile to 39°C, has a pulse rate of 130 bpm, and requires high dose pressors to keep his mean arterial pressure above 65 mmHg. Laboratory markers include WBC 18,000 with 95% PMNs, ESR 120 mm/h, and CRP 200 mg/L. Which of the following findings would most likely be observed in the type of shock this patient is currently in?
1) Decreased mixed venous oxygen saturation
2) Increased pulmonary capillary wedge pressure
3) Bradycardia
4) Loss of rectal tone
5) Decrease in systemic vascular resistance
This patient sustained an L3 burst fracture with no evidence of spinal shock on presentation, however, suffered an aspiration event causing pneumonia and is now in septic shock. Decreased systemic vascular resistance is observed during septic shock.
Septic shock has a mortality rate estimated at 25%-50%. It is a medical emergency resulting from decreased tissue perfusion and oxygen delivery as a result of severe infection and sepsis. Septic shock is associated with decreased cardiac output, decreased pulmonary capillary wedge pressure, decreased central venous pressure, and increased mixed venous oxygen saturation. It is differentiated from hypovolemic shock in that the systemic vascular resistance is decreased in septic shock, whereas it is increased in hypovolemic shock.
Although this patient has a burst fracture, it is important to distinguish this injury from neurogenic shock, which is usually a consequence of traumatic spinal cord injuries to the upper thoracic or cervical levels that results in autonomic dysregulation (loss of sympathetic tone and unopposed parasympathetic response, leading to bradycardia and decreased vascular resistance).
Schouten et al. reviewed the initial assessment and emergency treatment in
the spine-injured patient. They reported that hypotension should always be assumed to be of hemorrhagic etiology until proven otherwise, with initial treatment involving fluid resuscitation with a focus on raising systemic vascular resistance in cases of septic shock. They recommended that all aspects of emergent care, including resuscitation and choice of imaging modalities, be systematically reviewed, and practice guidelines are adopted institutionally.
Hadley et al. reviewed blood pressure management after acute spinal cord injury. They reported that hemodynamic alterations during acute spinal cord injury include hypotension, cardiac dysrhythmias, decreased peripheral vascular resistance, and reduced cardiac output. They recommended that hypotension (systolic blood pressure
A 45-year-old female barista from Portland fell off her skateboard and sustained a closed distal radius fracture. The patient undergoes
open reduction internal fixation (ORIF). Post-operatively she is given a prescription with the goal of mitigating a potential adverse outcome.
Which of the following has evidence to support its utility in this clinical situationr?
1) Alendronate 700mg once per week for 3 months
2) Vitamin C 500mg once daily for 50days
3) Alendronate 70mg once per week for 3 months
4) Vitamin C 200mg once daily for 50days
5) Vitamin C 1500mg once daily for 100days
There is some evidence to support that Vitamin C 500mg PO taken daily for 50 days may decrease the chances of developing complex region pain syndrome (CRPS) following ORIF of distal radius fractures.
CRPS is generally classified as type I, in which symptoms develop in an absence of specific nerve injury, or type II, in which there is the presence of specific identifiable nerve injury. The diagnostic criteria include pain disproportionate to the inciting event and a combination of sensory, vasomotor, sudomotor, and trophic signs. Treatment often involves a combination of physical therapy and pharmacologic treatment, nerve blocks, or chemical or surgical sympathectomy. However success is mixed, therefore prevention is paramount. Given that the etiology is thought to involve a traumatic incident that elicits an overwhelming systemic inflammatory reactions, causing disproportion pain and increased vascular permeability, it is hypothesized that the administration of Vitamin C as a free radical scavenger may protect the vascular endothelium and reduce the incidence of CRPS. Prophylactic administration after management of distal radius fractures is supported by moderate evidence as per the 2013 AAOS guidelines on the Treatment of Distal Radius Fractures.
Zollinger et al. performed a double-blinded randomized controlled trial of 427 wrist fractures, allocating patients to receive placebo or 200, 500, or 1500mg of vitamin C for 50 days. The authors found that in the vitamin C group, the incidence of CRPS was 2.4%, while it was 10.1% in the placebo group. They showed no difference in relative risk between the 500mg and 1500mg groups. The authors concluded that Vitamin C reduces the prevalence of CRPS and a daily dose of 500mg for 50 days is recommended.
Koval et al. comprehensively reviewed controversies in the management of distal radius fractures. The authors highlight the evidence supporting vitamin C use in treating disproportionate pain. However, because there is no objective
measure for the diagnosis CRPS, the evidence remains limited.
Incorrect Answers:
Answer 1: A prospectiv randomized controlled trial was conducted to evaluate healing rates in patients following administration of 70mg alendronate weekly for three months. There was no difference in clinical outcomes or healing between control and experimental groups.
Answer 3: Alendroate has not shown to be beneficial in this setting.
Answer 4: The recommended length and dose of treatment is Vitamin C 500mg for 50 days.
Answer 5: Studies have shown no difference between 500mg and 1500mg. A daily 500mg dose is recommended by the AAOS.
A 30-year-old plastic surgery resident fell from a height of 12' and sustained a right both-bone forearm fracture. The patient underwent open reduction and internal fixation with 3.5mm Limited Contact Dynamic Compression Plating. Three months after fixation the patient has no forearm tenderness and has full active range of motion of his fingers, hand, and wrist. However, pronation and supination are severely limited. This affects his ability to suture during surgery and knit, although he has returned to his other recreational activities. His most recent radiographs are shown in Figures A and B. What is the most likely cause for his lack motion?
1) Fracture nonunion
2) Posterior interosseous nerve (PIN) palsy
3) ECU interposition at the DRUJ
4) Heterotopic ossification
5) Loss of radial bow
This patient sustained a both-bone forearm fracture that was fixed with a long, straight plate which did not account for the native radial bow. This is the most likely reason for his limited pronosupination.
Open reduction with internal fixation of both-bone forearm fractures has generally demonstrated a high rate of union and excellent functional results. However, restoration of the radial bow is a critical. A lack of radial bow will limit pronosupination. To avoid this problem, the surgeon could have used a shorter plate or a plate with an anatomic radial bow, which many modern forearm plating systems now account for. The assessment and calculation for radial bow is highlighted in Illustration A. Other factors which may contribute to limited pronosupination include heterotopic ossification and scarring, though the former is not seen on radiographs.
Matthews et al. evaluated the impact of radial bow on pronosupination in a cadaveric both-bone forearm fracture model. The authors found that with a 10-degree deviation from the anatomic radial contour, there was no loss of pronosupination. However when this was increased to a 20-degree angulation, there was a significant loss of forearm pronosupination. The authors underscored the importance of restoration of radial bow in fixation of both-bone forearm fractures.
Schemitsch and Richards evaluated the outcomes in 55 adult patients following both-bone forearm fracture fixation. They reported good-excellent outcomes in 84% of cases. The authors found that bone grafting did not affect union (54/55 achieved union), but noted that restoration of the radial bow affected functional outcome and grip strength. The authors stressed the importance of restoration of radial bow.
Figure A is an AP radiograph of the forearm following ORIF of a both-bone forearm fracture with a long straight plate which fails to restore the anatomic radial bow. Figure B is a lateral radiograph of the same patient demonstrating fracture fixation with a long straight plate. Illustration A demonstrates the method for determining radial bow. A line from the sigmoid notch to the bicipital tuberosity is drawn (Y). A perpendicular line is drawn from Y to the point on the radial with maximal bow (a) (This number is usually 7%). The point of this intersection to the bicipital tuberosity is marked (x). The location of maximal bow is x/y (This number is usually 60%).
Incorrect Answers:
Answer 1: The patient is non-tender and has returned to activities. He does not have any clinical or radiographic evidence of fracture nonunion.
Answer 2: The patient has full active range of motion of his digits and wrist, which would indicate that the PIN is functional.
Answer 3: The ECU can be interposed at the DRUJ, particularly in radial shaft fractures in which the DRUJ is unstable after fracture fixation. However, this patient does not have DRUJ instability. Furthermore, there is no evidence of DRUJ diastasis on X-Ray.
Answer 4: The radiographs are negative for any evidence of heterotopic ossification, though this is another potential source of limited motion following ORIF of both-bone forearm fractures.
A 46-year-old male presents with the radiographs in Figure A following a skiing accident. You decide to treat this injury with an intramedullary nail. During insertion of your nail, it's decided that blocking screws are needed. In which position should they be placed to prevent the most common malunion?
1) A and D
2) A and C
3) B and C
4) B and D
5) A and B
Proximal third tibial shaft fractures have a propensity to be malunited in valgus and procurvatum. To prevent this, blocking screws can be used in the
concavity of the expected deformity, locations B and C.
Malunion and soft tissue compromise are two complications with a high association to proximal third tibial shaft fractures. The most common deformity seen in a malunited fracture is valgus and procurvatum due to the pull of the pes anserine and the patellar tendon, respectively. Numerous techniques exist to help prevent this deformity including the use of blocking screws, unicortical plating, and the universal distractor. If blocking screws are employed they should be placed on the concavity of the expected deformity, which in this case would be posterior in the sagittal plane and laterally in the coronal plane of the proximal fragment. Once reduction is obtained, if the blocking screws are left in place they have the added benefit of creating a stronger construct.
Kulkarni et al review the use of blocking screws for intramedullary nailing of proximal third tibial shaft fractures. They report an average time to union of
4.2 months with 5/66 cases going on to non-union, which were all successfully treated with bone grafting, and 1/66 resulting in a malunion. They conclude that blocking screws help maintain fixation and alignment of proximal third tibia fractures treated with intramedullary nails.
Stinner et al review techniques for intramedullary nailing of proximal third tibial shaft fractures. They report on several techniques including blocking screws, unicortical plating, and clamp reduction to assist the surgeon in obtaining an adequate reduction. They conclude that while implant design and surgical techniques have improved, the surgeon must still be cognizant of the valgus and apex anterior deformity and know how to neutralize these forces.
Franke et al review the indications and techniques for suprapatellar nailing of tibia fractures. They report that placing the knee in 20 degrees of flexion for suprapatellar nailing acts to neutralize the pull from the quadriceps muscle, thus decreasing the apex anterior deformity. They conclude that this technique can be used for Gustilo-Anderson Grade I-II tibial shaft fractures to help reduce the incidence of valgus and apex anterior malunions.
Figure A is the AP and lateral radiographs of a proximal third tibial shaft fracture. Blocking screws should be placed in positions B and C to help reduce the incidence of valgus and apex anterior malalignment.
Incorrect Answers:
Answers 1-2,4-5: Blocking screws should be placed in the concavity of the deformity to be prevented, thus positions B and C in this example.
Figures 1 and 2 are the radiographs of a 41-year-old diabetic male presenting with right lower extremity pain after cutting his leg it on a piece of rusty metal yesterday. Serial physical exam demonstrates rapid progression of the overlying erythema and worsening pain. In the emergency department, labs are significant for a C-reactive protein (CRP) of 180 mg/L, white blood cell (WBC) count of 19,000/mm3, glucose of 11 mmol/L, creatinine of 150 umol/L, and sodium of 120 mmol/L. He has a temperature of 102°F and a heart rate of 110 bpm. What additional laboratory value is needed to calculate this patient’s LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score?
1) ESR
2) Hemoglobin
3) Potassium
4) Bicarbonate
5) Calcium
The LRINEC score is based on the patient's serum CRP, WBC count, hemoglobin, sodium, creatinine, and glucose.
The LRINEC score is a clinical tool designed to help distinguish between necrotizing fasciitis and other soft tissue infections using these 6 key laboratory values. The most important of these is CRP, as a value >150 mg/L
contributes 4 of a possible 13 points. Illustration A demonstrates the scoring system for each laboratory value used in the calculation of the LRINEC score. A score >6 has been shown to have a PPV of 92% for having necrotizing fasciitis. The patient in this vignette already has a score of 10 without knowledge of the hemoglobin level, which is very concerning for necrotizing fasciitis. As a result, emergent surgical debridement is indicated.
Stoneback et al. reviews the presentation and management of necrotizing fasciitis. The authors note that the incidence of necrotizing fasciitis is between 500 and 1500 cases per year in the United States, and that the mortality rate averages 21.9%. They emphasize that necrotizing fasciitis may be difficult to distinguish from more common skin infections such as cellulitis or soft tissue abscess in its early stages but will often rapidly deteriorate, as illustrated in this vignette.
Wong et al. developed the LRINEC scoring system. In a retrospective review of 145 patients with necrotizing fasciitis and 309 patients with severe cellulitis or abscesses, they used their scoring system to demonstrate that a LRINEC score of 6 points or greater had a PPV of 92.0% and an NPV of 96.0%.
Tsai et al. challenged the utility of the LRINEC score in aiding in the diagnosis of Vibrio Necrotizing Fasciitis. In their retrospective review of 70 patients with Vibrio Necrotizing Fasciitis, they showed that only 11% of patients had a LRINEC score >6/. The authors concluded that the LRINEC scoring system is of more limited utility for this subset of the disease and propose that severe hypoalbuminemia, thrombocytopenia, and increased banded forms of leukocytes may have greater utility.
Figures A and B are AP and lateral radiographs of the lower leg demonstrating diffuse subcutaneous gas. This is concerning for necrotizing fasciitis.
Illustration A is a table showing the LRINEC scoring breakdown. A maximum total score of 13 could be achieved.
Incorrect Answers:
Answer 1: ESR is a non-specific measure of inflammation. While likely elevated with necrotizing fasciitis, it is not used to help calculate LRINEC score.
Answer 3: Hyperkalemia may occur with myonecrosis but potassium is not included in the LRINEC score calculation.
Answer 4: Acidosis may be seen in the setting of necrotizing fasciitis, but bicarbonate is not included in the LRINEC score calculation.
Answer 5: Calcium is not a component of the LRINEC scoring system.
A 35-year-old male presents to the emergency department following a motorcycle accident. On initial examination in the emergency department, he is found to have a left flail arm and multiple other injuries. There is a concern for a brachial plexus injury. What examination findings would support a diagnosis of a pre-ganglionic injury?
1) Abnormal histamine response
2) Flail arm
3) Intact sensory nerve action potentials (SNAPs)
4) Lateral scapular winging
5) Normal cervical paraspinal signal on EMG/NCV
Brachial plexus injuries are classified as either pre-ganglionic or post-ganglionic. A pre-ganglionic injury would be supported by intact sensory nerve action potentials (SNAPs).
Diagnosing brachial plexus injuries as either pre- or post-ganglionic is multi-faceted and begins with a thorough physical examination. Findings suggestive of a pre-ganglionic injury would include Horner Syndrome (due to disruption of the sympathetic chain), MEDIAL scapular winging resulting from rhomboid and serratus anterior paralysis, cervical paraspinal muscle weakness, absent sensation, and hemidiaphragmatic paralysis. CT myelography may demonstrate pseudomeningocele, and NCS/EMG would show intact sensory nerve action potentials (SNAPs) with denervation of the cervical paraspinal musculature. Finally, a histamine test would show a triple response, with redness, wheal, AND flare. Conversely, a post-ganglionic injury would be
supported by BOTH motor and sensory deficits of the flail arm, maintained innervation to cervical paraspinal muscles, and an abnormal histamine response test (redness and wheal with NO flare).
Limthongthang et al. reviews the common clinical findings associated with pre-and post-ganglionic injuries. The authors discuss the diagnostic algorithm, including a thorough history, physical examination, electrodiagnostic studies, and CT myelogram or MRI. They emphasize that an angiogram should additionally be considered given that 20% of brachial plexus injuries have associated major vascular injuries. The authors conclude with appropriate surgical timing and suggest potential treatments depending on injury location.
Giuffree et al. reviews management of brachial plexus injuries. The authors discuss appropriate timing of treatment based on the injury mechanism. They emphasize the priorities of functional restoration, beginning with elbow flexion, followed by a stable shoulder, and lastly intrinsic hand function. The authors present various surgical options to attain these goals and discuss their outcomes.
O'Shea et al. discusses the utilization of advanced imaging and electrodiagnostic testing for evaluation of brachial plexus injuries. The authors note the utility of CT myelogram toward identifying root avulsions. They also suggest that electrodiagnostic studies be obtained no sooner than 4 weeks following injury and subsequently at 6-week intervals to monitor progression. They note that SNAPs are the most important criteria in distinguishing between pre- and post-ganglionic injuries, and conclude that electromyographic studies are crucial in determining not only the level of injury but also donor nerves for transfers.
Incorrect Answer:
Answer 1: A normal “triple” response to intradermal injection of histamine involves erythema due to capillary dilation, wheal due to fluid extravasation from increased permeability, and flare due to arteriolar dilatation AND to axon reflex in sensory nerve. A response with a flare in an insensate area of skin suggest that the reflex arc is intact and that the lesion has to be proximal to the dorsal root ganglion. Conversely, when the lesion is post-ganglionic, the test will be “abnormal” (i.e. without the flare) as the continuity between the skin and dorsal root ganglion will have been interrupted.
Answer 2: A flail arm is characteristic of both pre- and post-ganglionic brachial plexus injuries, given that both involve absence of motor function.
Answer 4: Lateral scapular winging is not associated with a pre-ganglionic injury. Lateral winging characteristically results from trapezial pathology, which is associated with CN XI injury. Instead, MEDIAL scapular winging would be
indicative of a pre-ganglionic injury due to involvement of the dorsal scapular nerve (branching from the C5 root) and the long thoracic nerve (branching from the C5-7 roots).
Answer 5: Normal EMG/NCV results in the cervical paraspinal muscles would be indicative of a post-ganglionic injury.
A 47-year-old male diabetic has developed a calcaneal ulcer, as shown in figure A, that has been managed with wound care and a total contact cast. He presents to the emergency department with worsening erythema progressing up his leg with new draining wounds. On admission, despite antibiotics and intravenous fluids, he develops worsening pain and new bullae shown in Figure B. His laboratory studies indicate CRP >200, WBC 25k, Sodium 127, glucose 233, and hemoglobin 12. What is the best next step in the management of his condition?
1) Emergent vascular exploration
2) Upgrade level of care ICU with antibiotic escalation
3) MRI foot for osteomyelitis evaluation
4) Emergent surgical debridement including possible amputation
5) CT with contrast of lower extremity
This patient meets the clinical criteria for the diagnosis of necrotizing fascitis, therefore the next step in management is surgical debridement with possible amputation.
Necrotizing fasciitis is an aggressive infection with rapid spread along fascial planes. Initial presentation may be consistent with cellulitis; however, rapid progression along fascial planes may result in skin necrosis, muscular invasion, and subsequent myonecrosis. The rapidity of diagnosis and emergent surgical debridement is essential. Risk factors including intravenous drug abuse, alcohol abuse, and diabetes should be assessed, and if necrotizing fascitis is on the differential, the LRINEC score may be employed for diagnosis in equivocal cases. This scoring system can be found on our associated Orthobullets page.
Wong et. al. developed the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score to assist in early diagnosis of necrotizing soft tissue infections. The authors used logistic regression to identify significant predictors of necrotizing fasciitis. The score utilizes a total white cell count, hemoglobin, sodium, glucose, serum creatinine, and CRP. A LRINEC score of 6 points or higher has a positive predictive value of 92%, and below 6 points a negative predictive value of 96%. Importantly, ESR is not a component in the scoring system as it correlated poorly with risk. The patient presented already has two positive serum findings with an LRINEC score of 6.
Stoneback et al. review the diagnosis and management of necrotizing fasciitis. They note that Group A streptococcus is one of the most prevalent organisms, but infections are typically polymicrobial. Because of the need for prompt initiation of treatment, adjunctive diagnostic tests should not impede the timing of surgical exploration and debridement. Necrotizing fasciitis is a clinical diagnosis where only emergent surgical debridement and appropriate antibiotic treatment can prevent progression and death.
Tsai et al. retrospectively reviewed 70 patients with 71 episodes of Vibrio necrotizing fasciitis and sepsis. Of the 70 patients, 68 had a history of contact with seawater or raw seafood; 66 had underlying chronic diseases. They noted that severe hypoalbuminemia, severe thrombocytopenia, and increased banded forms of leukocytes are laboratory risk indicators of necrotizing fasciitis
that aid in pointing toward the initiation of early surgery and predict a higher risk of death.
Figure A is a clinical photograph of a calcaneal ulcer. Figure B shows ascending erythema and bullae consistent with a necrotizing skin infection. Illustration A demonstrates the LRINEC scoring system. The scoring system is not largely utilized as a screening tool due to its poor sensitivity in studies that attempted to validate it.
Incorrect answers:
Answer 1: There is no indication in this scenario that this patient's clinical picture is due to a vascular issue.
Answer 2: This patient will likely require ICU admission, but surgical debridement is most prudent.
Answers 3 and 5: Imaging studies can assist with the diagnosis, but advanced imaging takes valuable time and should not delay emergent surgical debridement. The incidence of gas in the subcutaneous tissues is only 13%, but its presence should trigger urgent debridement.
A 36-year-old man with HIV, chronic kidney failure, and chronic IV drug use presents with worsening fevers, chills, and purulent drainage from his leg. His infection progresses rapidly and he becomes acutely septic. He is therefore taken urgently to the OR for radical debridement of the fascia and surrounding tissues, with a plan for delayed closure. His CRP is 90 mg/dL and he is hyponatremic. Intraoperative cultures are obtained. To cover the most common organism(s) associated with this condition, what antibiotic would you initially recommend?
1) Intravenous vancomycin
2) Intravenous vancomycin and gentamicin
3) Intravenous gentamicin
4) Intravenous linezolid and meropenem
5) Intravenous micafungin
This patient with lower extremity necrotizing fasciitis underwent a radical debridement of fascia and surrounding tissues. The most common culture isolate from necrotizing fasciitis is polymicrobial, which should be the target of initial antibiotic treatment. Of the above options, intravenous Linezolid and Meropenem would be an acceptable empiric therapy as Linezolid would cover MRSA and invasive group A Streptococcus while Meropenem would cover gram-positive/negative anaerobic coverage and enteric organisms.
Necrotizing fasciitis is an aggressive infection with rapid spread along fascial planes. While the initial presentation may suggest cellulitis, rapid progression along fascial planes may result in skin necrosis and subsequent myofascial necrosis. The time from admission to debridement has been shown to be a significant predictor of outcomes. Immediate empiric antibiotics covering
polymicrobial species including aerobic, anaerobic, gram-positive and gram-negative bacteria are of equal importance.
Stoneback et al. reviewed the diagnosis and management of necrotizing fasciitis. They reported that while most necrotizing fasciitis infections are polymicrobial, group A Streptococcus remains one of the more prevalent organisms in isolation. They recommended surgical debridement as the utmost importance in necrotizing fasciitis management and emphasized appropriate antibiotic selection in treating sepsis and halting the further bacterial spread.
Wong et al. developed the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score, a novel diagnostic scoring system for distinguishing necrotizing fasciitis from other soft tissue infections based on laboratory tests routinely performed for the evaluation of severe soft tissue infections. This score allocated 1 point each to the following labs: total white cell count, hemoglobin, sodium, glucose, serum creatinine, and C-reactive protein. They reported that a cutoff value of 6 points had a positive predictive value of 92.0% and a negative predictive value of 96.0%, and concluded that the LRINEC score is a powerful score that can detect even clinically early cases of necrotizing fasciitis.
Tsai et al. investigated whether clinical indicators predict laboratory findings during the initial stages of necrotizing fasciitis and the relationship between the LRINEC score and the diagnosis of vibrio infection. They reported that a systolic blood pressure of 90mmHg or less at the time of admission predicted mortality and that patients with a LRINEC score of >6 had an 11% chance of surviving vibro-specific necrotizing fasciitis.
Figure A is a clinical image depicting necrotizing fasciitis of the lower extremity, with characteristic ischemic patches, cutaneous gangrene, dermal induration, bullae formation. Illustration A is a table from Wong's study that demonstrates the components, clinical values, and scoring system for the LRINEC score.
Scores of 6 or greater are highly concerning. They concluded that severe hypoalbuminemia, severe thrombocytopenia, and increased leukocytosis were reliable markers.
Incorrect Answers:
Answer 1: While intravenous Vancomycin would cover MRSA and aggressive streptococcus species, it would not cover gram-negative anaerobic organisms. Answer 2: This patient has chronic kidney failure, which would be worsened by 2 antibiotic agents that are known to be nephrotoxic.
Answer 3: Intravenous Mentamicin alone would not cover the gram-positive organisms.
Answer 5: Intravenous Micafungin would cover fungal organisms, but would fail to cover bacteria.
A 27-year-old male is involved in a motor vehicle collision and presents to the ER with the right lower extremity injury shown in Figures A and B. He undergoes immediate closed reduction and the post-reduction CT is shown in Figures C and D. The patient undergoes percutaneous surgical screw fixation of the injury. At 2 years followup, he presents with a supination deformity with decreased eversion of the foot at rest. Radiographs reveal no evidence of talus subchondral sclerosis or collapse. Which of the following is the most likely cause of the finding in this patient?
1) Avascular necrosis
2) Subtalar arthritis
3) Tibiotalar arthritis
4) Varus malunion
5) Planovalgus
The patient has sustained a displaced talar neck fracture with medial comminution which requires open reduction and internal fixation to restore anatomic alignment. The patient has likely sustained varus malunion which is a common deformity noted with non-anatomical reduction leading to hindfoot supination and decreased eversion.
Talar neck fractures, while uncommon, can lead to significant morbidity in the ambulatory patient. Treatment of these injuries requires prompt reduction due to the tenuous blood supply to the talus. The most common complications noted after a talar neck fracture are avascular necrosis, subtalar arthritis, tibiotalar arthritis, and varus malunion. A talus varus malunion generally occurs due to medial talar neck comminution and/or non-anatomic reduction of the injury. This deformity can lead to decreased eversion and a supination deformity causing patients to ambulate on the lateral aspect of the foot. These malunions are generally treated with a medial opening wedge osteotomy.
Fortin and Balazsy review the pathology and treatment of traumatic talus fractures. They cite that injuries to the head, neck, or body of the talus can result in permanent pain, loss of motion, and deformity. They note that failure to recognize fracture displacement (even when minimal) can lead to undertreatment and poor outcomes. They conclude that unrecognized medial talar neck comminution can lead to varus malunion and a supination deformity with a decreased range of motion of the subtalar joint.
Lindvall et al. performed a retrospective review to evaluate the long-term results (average of 74-month followup) of surgical treatment of isolated, displaced talar neck and/or body fractures with stable internal fixation in 25 patients. They noted an overall union rate of 88% regardless of surgical timing. The authors noted posttraumatic subtalar arthritis in all patients (100%) and talus osteonecrosis in 13/26 (50%) of patients. The authors concluded that a delay in surgical fixation does not appear to affect the outcome, union, or prevalence of osteonecrosis and that posttraumatic arthritis is a more common complication than osteonecrosis following operative treatment.
Figures A and B are the Lateral and AP radiographs of a displaced talar neck fracture with tibiotalar dislocation. Figures C and D are the post-reduction sagittal foot CT cuts that reveal a displaced talar neck fracture with medial
comminution.
Incorrect Answers:
Answer 1: The patient does not have any radiographic signs of avascular necrosis according to the vignette.
Answer 2: Subtalar arthritis is the most common complication following talar neck fractures but the clinical appearance of the patient's foot is due to varus malunion.
Answer 3: Tibiotalar arthritis is a common complication following talar neck fractures but the clinical appearance of the patient's foot is due to varus malunion.
Answer 5: A planovalgus foot is unlikely to occur after a talus fracture, furthermore a planovalgus foot would lead to a pronation deformity.
Figures A-C are a 32-year-old female who presents to the trauma bay after falling off a roof. Paramedics state that she was initially complaining of back pain, but she now appears irritable and lethargic. She has received 2 liters of crystalloid since arriving in the trauma bay. Her blood pressure is now 76/42. A Foley catheter is placed, and her urine output is 12 ml/hour. What additional finding would suggest hemorrhagic shock over neurogenic shock?
1) Tachycardia
2) Bradycardia
3) Decreased cardiac output
4) Vasodilation
5) Warm dry skin
This patient sustained a multi-traumatic injury and is suffering from hemorrhagic shock. The presence of tachycardia would favor the diagnosis of hemorrhagic shock over neurogenic shock.
In initial hypovolemic shock (stage I,
A 32-year-old inebriated male falls from a mechanical bull at a bar and sustains a closed displaced intra-articular distal radius fracture. He presents to your clinic and given his age and the fracture characteristics, he is taken for open reduction with volar locking plate
fixation. After completing instrumentation, radiocarpal screw penetration is best assessed on which fluoroscopic view?
1) Extended wrist tangential view
2) Flexed wrist tangential view
3) PA anatomic tilt view
4) Radial inclination view
5) Standard lateral view
While no single radiographic view can completely rule out intra-articular screw penetration, radial inclination views (most commonly a 22-degree anatomic tilt lateral view) best demonstrates screw penetration of the radiocarpal joint.
Intra-articular screw penetration is a potential complication of distal radius fracture fixation. Due to the complex native geometry, standard PA and lateral fluoroscopic views are not effective in evaluation of the joint reduction, screw length or screw position. For this reason, various supplemental views have been described to facilitate identification of articular incongruity as well as dorsal or intra-articular penetration of screws, either into the radiocarpal or distal radioulnar joint.
Tweet et al. reviewed the most commonly used imaging techniques and views for the evaluation of intra-articular screw penetration during volar plate fixation of distal radius fractures. Of nearly 700 ASSH members surveyed, 87% relied exclusively on fluoroscopy, three-quarters (74%) of which implemented tilt views or rotational fluoroscopy. Cadaveric analysis supported use of a 22-degree lateral projection and rotational fluoroscopy as adjuncts for the detection of intra-articular screw penetration. They concluded that no combination of imaging effectively allowed the detection of all intra-articular screws.
Patel et al. evaluated the utility of supplemental radiography in assessing screw placement in distal radius fracture fixation using volar locking plates. The authors found that supplementation of the standard AP and lateral views with lateral tilt views significantly increased accuracy and confidence.
Specifically, more acute angles (15 and 23-degree views) provided better visualization of ulnar screws while larger angles (30 degrees) allowed assessment of more radial-sided distal plate screws.
Illustration A is an example of an extended wrist tangential view showing clear visualization of the sigmoid notch and distal radioulnar joint (DRUJ), with intraarticular penetration of the DRUJ shown on the left and extra-articular screws
free of the DRUJ.
Illustration B is an example of a flexed wrist tangential view, or “skyline” view, demonstrating no dorsal penetration of the screws, which can be obscured on a true lateral due to Lister’s tubercle.
Illustration C shows an example of a standard PA view (left) and 11-degree anatomic tilt PA view, allowing better visualization of the articular surface. Illustration D shows a standard true lateral view (left) and 22-degree radial inclination lateral view (right), allowing better visualization of screw relationship to the radiocarpal joint.
Incorrect Answers:
Answer 1: The extended wrist tangential view, or “sigmoid notch” view, has been described as a technique by which intra-articular penetration of the sigmoid notch can be evaluated.
Answer 2: The flexed wrist tangential view, or “skyline” view, best demonstrates dorsal screw penetration.
Answer 3: The PA anatomic tilt view is an 11-degree anatomic tilt view that best demonstrates the degree of articular congruity of the joint surface.
Answer 5: The standard lateral view can demonstrate the position of a volar plate with respect to the watershed line but has limited utility in evaluating radiocarpal screw penetration due to radial inclination.
When considering operative intervention for the injury shown in Figures A and B, which of the following factors has the LEAST correlation with complication rate?
1) Skin integrity
2) Age
3) Smoking status
4) Peripheral neuropathy
5) Diabetes
In patients with an unstable ankle fracture, age has not shown to have an effect on complication rate.
An increasing number of elderly patients retain an active lifestyle with high functional demands. Cast immobilization for highly unstable ankle fractures (especially inherently unstable pronation-abduction fractures that are frequently seen in the elderly) leads to malunion or nonunion rates between 48% and 73%. Therefore, in the absence of severe comorbidities, the principal indications for surgery should not differ from those in younger patients.
Herscovici et al. evaluated 243 elderly patients with high-energy foot and ankle injuries, 73 of which had ankle fractures, who underwent surgical fixation.
They report on their preferred approach to treatment of these patients. Their article does not report on any outcome variables but states that, in their expert opinion, elderly patients should be considered for operative intervention as a young patient would.
Pagliaro et al. analyzed outcomes after surgical treatment of unstable ankle fractures in 23 patients who were at least 65 years old. They found that open reduction and internal fixation of unstable ankle fractures in geriatric patients is an effective treatment that leads to a complication rate comparable to the general population.
Figure A and B demonstrate AP and lateral radiographs of a trimalleolar ankle fracture.
Incorrect Answers:
Answer 1, 3-5: All of these factors lead to an increased risk of complications for unstable ankle fractures.
Which of the following statements is true regarding the outcomes when using a high-pressure pulse lavage irrigation system versus
simple low-pressure bulb irrigation for the treatment of the open fracture shown in Figure A?
1) It is more cost effective when including the cost of reoperation
2) There is an increased rate of associated nerve injury
3) There is an increased rate of primary wound healing problems
4) There is increased rate of infection
5) There is no difference in union rates
There is no difference in union rates when either high-pressure (pulse lavage) or low-pressure (bulb) irrigation with saline is used for open tibia fractures.
The mainstay of early treatment of open fractures includes debridement and irrigation along with IV antibiotics. Multiple trials have looked at the most efficacious and cost-effective irrigation method both in terms of the type of solution and irrigation method. With regard to the irrigation method, recent studies have shown simple bulb irrigation has the same union rate as more expensive high-pressure pulse lavage systems. With regard to the type of solution, recent studies have shown castile soap actually leads to a decreased rate of primary wound healing problems as compared using an irrigation solution with antibiotics.
Bhandari et al. in the FLOW study (Fluid Lavage of Open Wounds), a multicenter randomized trial demonstrated that the rates of reoperation were similar regardless of irrigation pressure, a finding that indicates that very low pressure is an acceptable low-cost alternative for the irrigation of open fractures.
Anglen et al. demonstrated that the use of a nonsterile liquid soap additive (castile soap) was at least as effective as the use of bacitracin with regards to the rate of postoperative infection and fracture healing, but showed a significant decrease in problems with soft-tissue healing.
Bhandari et al. as a follow up by the FLOW group in the study above analyzed 2551 patients to look for risk factors for reoperation. The rates of reoperation were similar regardless of irrigation pressure, a finding that indicates that very low pressure is an acceptable low-cost alternative for the irrigation of open fractures. The reoperation rate was higher in the castile soap group than in the saline group.
Figure A is a clinical photograph demonstrating a Type IIIB open tibia fracture. Incorrect Answers:
Answers 1: The high-pressure irrigation system is more expensive and has not
been shown to decrease reoperation rates.
Answer 2: There is not a higher risk of nerve injury with high-pressure irrigation.
Answer 3: There has been no difference in regards to wound healing problems when comparing high and low-pressure irrigation.
Answer 4: No difference in postoperative infection has been found, regardless of high or low-pressure irrigation.
A 71-year-old man presents after 9 months of functional bracing for a closed right humeral shaft fracture. Current radiographs are shown in Figure A. Infectious workup was negative. Appropriate next steps in evaluation will most likely reveal which of the following?
1) Vitamin D deficiency
2) Low testosterone
3) Iron deficiency
4) Thyroid deficiency
5) Magnesium deficiency
Metabolic/endocrinologic workup for an atrophic nonunion following appropriate treatment for a humeral shaft fracture is likely to reveal a vitamin D deficiency.
Nonunion of the humeral shaft occurs approximately 10% of the time following open or closed treatment. In the case of nonunion, there is likely a lack of mechanical and biologic factors. Biologic workup for nonunion should include ruling out infection followed by an evaluation for metabolic and endocrine abnormalities.
Brinker et al. reviewed 37 low-energy fractures that went on to nonunion. These patients were evaluated by clinical endocrinologists for evaluation of metabolic abnormalities. Thirty-one of the 37 patients (84%) had a metabolic issue, with 68% (25 of 37 patients) having a Vitamin D deficiency. They conclude any patient with a nonunion should be referred to an endocrinologist for metabolic screening and treatment.
Kuo et al. looked at the compliance of 155 patients treated for osteoporosis
shortly after sustaining a fragility fracture. They found 47% had a prior fracture with only 26% having a prior BMD and 15% on calcium and vitamin D. They concluded that osteoporotic treatment provided at the time of fracture leads to long-term compliance in 90% and 73% of osteoporotic and osteopenic patients, respectively.
Figure A shows a radiograph of the right humerus demonstrating a nonunion of a humeral shaft fracture. Illustration A shows postoperative radiograph after open reduction internal fixation with compression plating.
Incorrect Answers:
Answer 2: Low testosterone would be possible given the patient demographics but would not be included in the appropriate next steps in the evaluation of this nonunion.
Answer 3: Iron deficiency may be present but would not be the next best laboratory study in evaluating a nonunion.
Answer 4 & 5: Metabolic and endocrinologic workup is the next appropriate step; however, thyroid and magnesium deficiencies are less common than a vitamin D deficiency.
A 62-year-old woman falls off a bike and sustains the injury shown in Figure A. She presents to clinic for her 6-month follow-up appointment and reports persistent pain. Current imaging is shown in Figure B. Which of the following factors is not a risk factor to the development of this patient’s diagnosis?
1) Shortening of 3cm
2) Comminution
3) Sling immobilization as opposed to figure-of-eight brace
4) Female gender
5) Advanced age
This patient presents with a symptomatic non-union of a midshaft clavicle fracture (classic "z-type" fracture for it's shape), which is not associated with type of immobilization (sling vs. figure-of-eight brace).
Clavicle fractures treated non-operatively are at risk for complications such as non-union, poorer cosmesis, and decreased shoulder strength and endurance. The risk of non-union, in particular, ranges from 1-5% and has been shown to increase with shortening > 2cm, comminution, female gender, and advanced age. Open reduction internal fixation of clavicle fractures has also shown to have increased union rates compared to those treated non-operatively but
presents its own risks such as hardware complications and infections.
Robinson et al. performed a prospective observational cohort study to evaluate the prevalence of and risk factors for non-union of clavicle fractures treated non-operatively. They found that the risk of non-union was significantly increased by advancing age, female gender, displacement of the fracture, and the presence of comminution.
Lazarides et al. performed a retrospective study to determine the relevance of shortening and clinical outcomes for midshaft clavicle fractures treated nonoperatively. They found that final clavicular shortening of > 18mm in male patients and of > 14mm in female patients was significantly associated with an unsatisfactory result.
The Canadian Orthopaedic Trauma Society performed a multicenter prospective randomized clinical trial to compare outcomes of clavicle fractures treated non-operatively versus operatively with plate fixation. They found that operative fixation of a displaced clavicular shaft fracture results in improved functional outcome and a lower rate of malunion and nonunion compared with nonoperative treatment at one year of follow-up.
Figure A is an AP radiograph demonstrating a displaced midshaft clavicle fracture. Figure B is an AP radiograph demonstrating non-union of a midshaft clavicle fracture.
Incorrect Answers:
Answers 1, 2, 4, 5: Each of these factors is associated with an increased risk of non-union.
Which of the following statements about polytrauma and organ failure is most correct when comparing children to adults?
1) Adults have a more robust initial inflammatory response, affecting the pulmonary system first
2) Adults have a dampened immune response, affecting all organ systems simultaneously
3) Adults have a more robust initial inflammatory response, affecting all organ systems simultaneously
4) Children have a more robust initial inflammatory response, affecting all organ systems simultaneously
5) Children have a dampened immune response, affecting the pulmonary system first
Adults have been shown to have a robust initial inflammatory response that affects the pulmonary system first.
There is a difference in the systemic response to trauma between children and adults. Children initially have a dampened systemic immune response. They do, however, have a robust local inflammatory response that causes organ failure and affects all organ systems simultaneously. Adults have a robust systemic response with organ failure occurring 2-3 days after injury. The pulmonary system is usually the first organ system affected in adults.
Wood et al. performed a review of the inflammatory response to injury in children. They found that the inflammatory response to injury in children is functionally and mechanistically unique. The incidence of multi-organ failure in children is rare, but affects all organ systems simultaneously when it does occur.
Pandya et al. performed a review of the pediatric polytrauma patient. They report that the orthopaedic surgeon plays an important role in managing hemodynamic instability, vascular insult, and neurologic damage in the child with multiple injuries. They recommend that, if surgical fixation is deemed urgent in the pediatric patient, it can be performed in the early period of multi-system insult.
Incorrect Answers:
Answers 2 & 3: Adults initially have a robust, systemic inflammatory response. When organ failure does occur, the pulmonary system is usually the first affected.
Answers 4 & 5: Children initially have a dampened systemic inflammatory response. When organ failure occurs, it affects all organ systems simultaneously.
A 63-year-old patient presents with right ankle pain after a fall down four stairs. Figures A and B are the radiographs of the injury. The patient reports a history of diabetes mellitus type 2 and peripheral neuropathy with a most recent hemoglobin A1c of 9.8. The injury is
reduced and placed in a well-padded bivalved cast. The patient is then discharged with outpatient follow-up without DVT prophylaxis. Twelve weeks later, the patient presents to the clinic for the first time in the same bivalved cast. The has remained non-weight bearing and the bottom of the cast confirms this. What is the expected outcome at this point?
1) Charcot arthropathy
2) Diabetic foot ulcer
3) Deep vein thrombosis
4) Elevation of A1c
5) Fracture displacement
The patient is a diabetic with poorly controlled blood sugar and peripheral neuropathy presenting with a bimalleolar ankle fracture with a loss to follow-up for 3 months. All of the answer choices are potential complications with nonoperative treatment, but fracture displacement is the most likely to occur.
Ankle fractures in diabetic patients are associated with increased complications compared to nondiabetic counterparts. The glycation damage to cellular
components as well as the decreased blood flow with microangiopathic changes results in substantially decreased bone healing. Patients diabetic comorbidities, such as retinopathy, nephropathy, vasculopathy, and neuropathy have a higher rate of wound complications, deep infections, malunion, nonunion, and Charcot arthropathy. Due to the delayed healing, surgical treatment with supplemental fixation is recommended.
Lovy et al. performed a retrospective review of 28 diabetic ankle fractures with 20 patients being treated nonoperatively and 8 patients treated operatively initially. Nonoperative treatment was associated with a 21-fold increase in complication risk. Delayed surgery (>3 weeks from injury) for nonunion or malunion was associated with greater complications than immediate ORIF. The authors concluded that nonoperative treatment for diabetic ankle fractures was associated with unacceptably high consequences.
Wukich et al. reviewed the treatment of ankle fractures in diabetic patients. Nonoperative treatment was recommended as a viable option for nondisplaced isolated unimalleolar and stable ankle fractures. Additionally, they proposed diabetic patients without diabetic comorbidities can be surgically treated with standard internal fixation constructs as they have similar outcomes. Finally, despite surgical treatment having a higher rate of complications than nondiabetic patients, operative management is more likely to result in a functional lower extremity in displaced and unstable ankle fractures.
Chaudhary et al. performed a review of ankle fractures in diabetic patients and concluded that diabetic ankle fractures are at high risk for fracture displacement and delayed union, even with surgical treatment. The authors recommend supplemental fixation with external fixation or multiple syndesmotic screws. Postoperatively patients should undergo prolonged immobilization, 2-3 times that of nondiabetics.
Figure A demonstrates an AP radiograph of a bimalleolar ankle fracture. Figure B demonstrates a lateral radiograph of a bimalleolar ankle fracture.
Incorrect Answers:
Answer 1: Charcot arthropathy occurs in diabetic ankle fractures, especially in neuropathic patients treated nonoperatively and with delayed treatment.
However, fracture displacement is more likely to occur.
Answer 2: Diabetic foot ulcers are a potential complication, especially in neuropathic patients. However, with a well-padded cast and the patient adhering to non-weight bearing recommendations, this is not as likely as fracture displacement.
Answer 3: Deep vein thrombosis is a potential complication of fractures in the
lower extremity, but the risk is typically higher in surgically managed patients. Answer 4: Non-operative treatment of ankle fractures in diabetic patients has not been associated with increases in A1c. However, with non-weight bearing activities the patient is likely to have poorer control of blood glucose, but the incidence of this has not been characterized.
Regarding Syme amputations, which of the following is true?
1) It does not require a patent tibialis posterior artery
2) It is dependent on a stable heel pad
3) It is less energy efficient than a midfoot amputation
4) The primary complication is an equinus deformity
5) It is also known as a hindfoot amputation
Syme amputations rely on a stable heel pad.
Syme amputations, or ankle disarticulations, are the most proximal type of ankle/foot amputations but are more energy efficient than midfoot amputations. A successful Syme amputation requires a patent tibialis posterior artery and a stable heel pad. The two most common problems are skin sloughing from a compromised vascular supply and migration of the heel pad due to instability. A hypermobile heel pad can cause difficulty with prosthesis wear and damage to the soft tissues, eventually leading to failure.
Finkler et al. performed a retrospective study on the long-term outcomes of Syme amputations. They found that patients who underwent Syme's ankle disarticulation amputation appeared to fare better than similar patients with transtibial amputations. These patients required less rehabilitation and achieved improved levels of functional independence as demonstrated by patient-reported outcome measures.
Pinzur et al. performed a retrospective study on Syme ankle disarticulation in patients with diabetes. They found that patients managed with a Syme ankle disarticulation had better ambulatory function and survival compared to transtibial amputations. They concluded that the results of this retrospective review support the value of Syme ankle disarticulation in diabetic patients with infection or gangrene.
Illustration A is an example of a Syme amputation.
Incorrect Answers:
Answer 1: Syme amputations require a patent tibialis posterior artery. Answer 3: Syme amputations are more energy efficient than midfoot amputations.
Answer 4: Equinus deformites are not a complication of Syme amputations. Answer 5: Syme amputations are also known as ankle disarticulations, not hindfoot amputations.
A 65-year-old patient, who is a current smoker, presents with left hip pain after a fall from standing height and is unable to bear weight. The patient's radiograph is shown in figure A. The use of a sliding hip screw construct has been shown to have what benefit compared to multiple cannulated screws?
1) Decreased fracture shortening
2) Decreased non-union rate
3) Decreased implant failure
4) Lower reoperation rates
5) Lower rate of avascular necrosis
The patient is a current smoker presenting with a left displaced basicervical femoral neck fracture. The use of a sliding hip screw (SHS) in this fracture pattern in patients that are current smokers has been associated with decreased reoperation rates compared to multiple cannulated screws (MCS).
Femoral neck fractures are highly morbid injuries and are the most expensive fractures to treat. Treatment options include MCS fixation, SHS, hemiarthroplasty, and total hip arthroplasty. Hemiarthroplasty is preferred in the low demand and elderly population. In younger patients with higher activity levels, reduction and internal fixation with MCS or SHS provide bone-preserving treatment options. Total hip arthroplasty is preferred in patients
>65 years of age with higher activity levels.
The Fixation using Alternative Implants for the Treatment of Hip fractures
study group (FAITH) performed a multicenter randomized control trial that included 1108 patients treated with either dynamic SHS or MCS. Fixation with SHS was associated with increased rates of avascular necrosis compared to MCS, 9% vs 5%, but was not significant. Overall, there were no differences in reoperation rates or union rates between the two groups. However, subgroup analysis revealed lower reoperation rates with SHS in displaced fractures, basicervical fractures, and in current smokers.
Zielinski et al. 2013 performed a subanalysis of 76 patients from the FAITH study examining femoral neck shortening, WOMAC scores, gait analysis, and hip muscle strength in patients treated for femoral neck fractures. Increased fracture shortening was observed with increased patient weight, age, and higher Pauwel's classifications. There was no comparison between implant type and gait outcomes.
Lee et al. 2008 performed a retrospective review of femoral neck fractures in 90 patients undergoing either minimally invasive SHS, MCS, or conventional SHS. The authors found that conventional DHS was associated with significantly larger incisions, greater blood transfusion requirements, and longer hospital stays compared to minimally invasive SHS and MCS. The authors recommended minimally invasive SHS due to lower soft tissue complications.
Figure A demonstrates an AP hip radiograph with a right femoral neck fracture. Illustration A depicts an SHS implant providing internal fixation for a femoral neck fracture. Illustration B depicts MCS fixation of a femoral neck fracture.
Incorrect Answers:
Answer 1: Fracture shortening has not been found to occur at lower rates with SHS or MCS.
Answer 2: Non-union rates are not significantly different between the two fixation methods.
Answer 3: Implant failure has not occurred differently between SHS and MCS. Answer 5: Avascular necrosis in the FAITH was found to occur at a higher rate in the SHS group, but this finding was not significant.
Which of the following will most likely result with the use of a fracture table when treating the injury shown in Figures A and B?
1) Internal malrotation deformity
2) External malrotation deformity
3) Recurvatum deformity
4) Varus deformity
5) Valgus deformity
The fracture table has been shown to induce an internal malrotation deformity when it is used for treating femoral shaft fractures.
Intramedullary nailing with reaming of the bone and static locking of the nail is the treatment of choice for femoral shaft fractures in adults. The fracture table has been used with excellent results. Compared to manual traction, the fracture table provides an advantage as only one assistant is necessary.
However, it may limit access to the patient if other body areas are injured. Additionally, the fracture table has been shown to induce an internal malrotation deformity, which results from internally rotating the limb to facilitate access to the starting point and to improve visualization of the hip in the lateral plane. Rotation may also be difficult to assess clinically once the limb is positioned and draped.
Kelly et al. performed a retrospective study to determine complications associated with the use of the fracture table in pediatric femoral fractures.
They found 8 palsies related to positioning. They also found that patients who developed nerve palsies were significantly heavier. They ultimately concluded that the fracture table is safe for fixation but every effort should be made to minimize time in traction to avoid iatrogenic nerve palsy, particularly in heavier children (> 80 kg).
Stephen et al. performed a randomized study comparing the fracture table and manual traction when nailing femoral shaft fractures. They found that internal malrotation was significantly more common when the fracture table was used. Operative time was also greater for the fracture table group. There were no other differences in complications. They concluded that manual traction is an effective technique that decreases operative time and improves the quality of reduction.
Figures A and B are AP radiographs demonstrating a femoral shaft fracture. Incorrect Answers:
Answers 2, 3, 4, & 5: Internal malrotation has been shown to be a risk when
using a fracture table to treat femoral shaft fractures by intramedullary nailing.
A 35-year-old patient is involved in a motor vehicle collision and sustains multiple injuries, including an APC pelvis fracture. He is stabilized following placement of a pelvic binder and receiving blood products as part of a massive transfusion protocol. He is subsequently taken to radiology for radiographs and a chest, abdomen, and pelvis CT with 4mm cuts. What effect will these modalities have on the radiographic appearance of his pelvis fracture and what further intervention should be performed?
1) Make the injury look more severe; obtained radiographs with the binder removed
2) Make the injury look less severe; perform fluoroscopic examination under anesthesia
3) Accurate representation of injury severity; no further studies needed
4) Make the injury look less severe; repeat CT with 0.625 mm cuts
5) Make the injury look more severe; obtain Judet views of the pelvis
Application of a pelvic binder and CT scans prior to standard AP pelvis radiographs results in an underestimation of pelvic ring injury severity. Since this patient was hemodynamically unstable and required a massive transfusion,
removal of the pelvic binder is not recommended and further injury stability should be evaluated by fluoroscopic examination under anesthesia.
Pelvic ring fractures are high energy injuries that usually follow motor vehicle collisions. There is a high rate of hemodynamic instability with these injuries due to the increase in pelvic volume and abundant venous bleeding. Proper identification of injury severity in the initial evaluation is crucial to ensure appropriate definitive treatment. Ideally, if the patient is hemodynamically stable, AP pelvis radiographs without a pelvic binder have been found to be effective at identifying unstable pelvic injuries.
Fagg et al. performed a retrospective study of 97 patients presenting with pelvic ring fractures requiring operative stabilization. The authors found that 7% of patients that initially had binder-on imaging were found to have unstable fractures that were not identified on the original images. The authors suggested that pelvic CT scans with the binder on are insufficient in determining the severity of pelvic fractures.
Swartz et al. performed a retrospective study of 43 patients presenting with pelvic ring fractures that received AP pelvic radiographs, pelvic binder, pelvic CT, and fluoroscopic stress examination in sequential order. They found that pre-binder radiographs had a greater sensitivity at detecting unstable fractures than pelvic CT with a binder. The authors concluded that placement of a binder prior to imaging can underestimate the severity of the pelvic injury and in cases where a binder is placed prior to imaging a fluoroscopic examination under anesthesia can be useful in detection.
Gibson et al. performed a retrospective review of 72 patients that presented with pubic diastasis requiring internal fixation. The authors found that pelvic CT scans without a pelvic binder underestimated the diastasis by 6.6mm compared to AP pelvic radiographs. The authors recommend obtaining radiographs prior to performing a CT, as underestimation of pubic diastasis can alter definitive management decisions.
Incorrect Answers:
Answer 1: Placement of a pelvic binder prior to radiographs and early CT scans underestimate the severity of pelvic ring injuries. In this case, the patient is hemodynamically unstable and removing the binder would likely result in increased pelvic bleeding by destabilizing clots.
Answer 3: The CT scan with the binder in place will underestimate the injury severity in this patient. In order to provide proper definitive care, the severity of the injury must be determined.
Answer 4: The current study has underestimated the degree of pelvic
instability. However, decreasing the cut thickness on CT will be unlikely to better determine the degree of pelvic ring instability.
Answer 5: The current injuries are underestimated by the current image study regimen with binder placement. Judet views, especially with the binder in place, will not enhance the detectability of pelvic ring instability.
A 26-year-old male with a BMI of 37 is involved in a motor vehicle collision and requires extrication. During evaluation in the trauma bay, he becomes hemodynamically unstable and is found to have the injury shown in Figure A, as well as an associated bladder injury. Which of the following statements regarding the patient's injury is true?
1) His male gender places him at a lower risk for post-operative infection
2) His BMI places him at a higher risk for post-operative infection
3) The mechanism of his injury was likely a lateral compression force
4) The internal pudendal artery is the most likely source of arterial hemorrhage
5) Pelvic binder placement is contraindicated in this patient given his bladder injury
The patient has an APC pelvis injury. Increased BMI has been associated with a higher risk of infection after surgical intervention of pelvic and acetabular fractures.
Pelvic fractures result from high-energy mechanisms and frequently require surgical intervention. When performing open procedures in the pelvis, the risk of infection is of concern. Elevated BMI has been shown to be the most
important risk factor for infection. Other risk factors include prolonged operative time, prolonged ICU stay, increased red blood cell transfusions, leukocytosis, Morel-Lavallée lesion, and associated genitourinary and abdominal trauma. Preoperative angioembolization as a risk factor for SSI remains controversial but is thought to be associated with embolization and not with angiography itself.
Iqbal et al. performed a retrospective study on surgical site infection following fixation of acetabular fractures. They found that prolonged operation time, increased BMI, prolonged ICU stay, larger amount of packed red blood cell transfusions, and associated genitourinary and abdominal trauma were associated with surgical site infection following acetabular fracture fixation.
They concluded that measures should be undertaken to attenuate the chances of surgical site infection in this major surgery by considering the risk factors significantly associated with it.
Sagi et al. performed a retrospective study on the risk for deep postoperative wound infection after pelvic and acetabular surgery. They found that obesity, obesity plus leukocytosis, and preoperative angioembolization were strong predictors of postoperative infection.
Firoozabadi et al. performed a retrospective study to evaluate the impact of pelvic embolization on postoperative infection rate after acetabular fracture fixation. They found that, despite previous reports of high infection rates after pelvic embolization, the deep infection rate was only 4% after embolization in their cohort. They therefore state that concerns for higher rates of infection are not substantiated, and pelvic embolization should be performed when indicated.
Figure A is an AP radiograph of the pelvis demonstrating symphyseal widening and left SI joint widening.
Incorrect Answers:
Answer 1: Gender has not been found to affect the risk of post-operative infection.
Answer 3: The patient's mechanism of injury was likely an anterior-posterior compression force, not a lateral compression force.
Answer 4: The superior gluteal artery is the most likely source of arterial hemorrhage in patients with APC pelvic fractures, while the internal pudendal artery or obturator artery is the most likely source of hemorrhage in patients with LC pelvic fractures.
Answer 5: Urogenital injury is not a contraindication for pelvic binder placement.
A 70-year-old female with a history of osteoporosis complains of vague left hip pain. She does not complain of right hip pain. Her imaging is shown in Figures A & B. What is the next best step in treatment?
1) Observation and pain control
2) Bone scan
3) Intramedullary nailing of the left femur
4) Intramedullary nailing of bilateral femurs
5) Referral to an orthopaedic oncologist
This patient has bisphosphonate-related changes of her femurs. Given that the left side is the only symptomatic side, it should be prophylactically nailed.
Bisphosphonates have been implicated in causing atypical low-energy femur fractures. Radiographic clues for this impending injury include lateral cortical thickening (beaking), varus remodeling of the femur, and increased diaphyseal cortical thickness. When a fracture occurs, it usually occurs in the subtrochanteric region. The fracture patterns are usually transverse or short-oblique in orientation. There is also a lack of comminution. The ideal treatment for these injuries is an intramedullary nail, ensuring to restore native alignment and avoiding varus.
Vasikaran performed a review of low-energy femoral fractures with prolonged bisphosphonate use. He reported that long-term bisphosphonate therapy is thought to lead to profound suppression of bone turnover, increased
microdamage accumulation, and alteration of bone tissue mineral properties as well as possibly bone tissue composition by altering collagen cross-linking, all of which can in turn cause brittleness of bone and propensity to fracture with minimal trauma. He concludes that, if a patient becomes symptomatic or sustains a fracture, the cessation of bisphosphonate therapy should be considered. If a fracture has not occurred and the patient is having prodromal symptoms, prophylactic intramedullary nailing should be performed.
Balach et al. performed a review on atypical femur fractures associated with disphosphonate use. They report that following the diagnosis of a complete or impending atypical femur fracture, discontinuation of diphosphonates is recommended to help promote a more favorable fracture healing environment. They conclude that surgical treatment should allow endochondral fracture healing such as an intramedullary nail.
Figures A and B are AP radiographs of the left and right proximal femurs demonstrating lateral cortical beaking, cortical thickening, and mild varus remodeling.
Incorrect Answers:
Answer 1: Observation and pain control is not appropriate in this case as the patient has an impending fracture.
Answer 2: A bone scan is not necessary in this case as the diagnosis can be made from radiographs.
Answer 4: Intramedullary nailing of both sides is not necessary at this time as the right side is asymptomatic.
Answer 5: Referral to an orthopaedic oncologist is not necessary for treating these injuries.
A 26-year-old male recreational basketball player sustained an ankle injury 6 months prior. He continues to complain of ankle pain and instability. Current imaging is shown in Figures A & B. Imaging of the proximal fibula is unremarkable and there is little concern for syndesmotic injury. What is the next best step in treatment?
1) Open reduction and internal fixation (ORIF) with autograft
2) Fragment excision
3) Obtain stress radiographs
4) Physical therapy and management of symptoms
5) Percutaneous skeletal fixation
This patient sustained a medial malleolar fracture that went on to nonunion. The next best step in treatment would be ORIF with autograft.
Historically, nonunion rates for malleolar fractures are somewhere between 5 and 30%. Nonunion following rotationally unstable ankle fractures can have detrimental effects on patient outcomes, leading to continued debilitating pain, instability, and late posttraumatic osteoarthritis. Patients with symptomatic nonunion should have surgical treatment. Fragment excision may be possible in patients with small distal fractures. However, if the fragment is large and well-preserved, ORIF with bone graft augmentation is the treatment of choice.
Khurana et al. performed a study to evaluate the outcomes following operative treatment of nonunited rotational distal fibula and medial malleolar fractures. They identified 17 patients. All patients were treated with open reduction with plate and screw fixation or screw fixation alone. Adjunctive grafting was performed in all but 2 cases. They found that after a mean of 33.9 months all nonunions had resolved. They conclude that patients who have surgery for nonunion will have outcomes similar to patients who undergo surgery for acute ankle fractures.
Capogna and Egol wrote a guide regarding the treatment of nonunions after malleolar fractures. They report that most medial malleolar nonunions are addressed by fixation with partially threaded cancellous screws. They suggest that osteopromoting materials or bone graft should be added before reduction. They conclude that fixation with two partially-threaded screws is sufficient for reliable fracture healing.
Figure A is an AP radiograph demonstrating a medial malleolar nonunion. Figure B is a coronal CT slice demonstrating a medial malleolar nonunion. Illustrations A and B are AP and lateral radiographs, respectively, demonstrating a medial malleolar nonunion that has been stabilized with 2 cannulated screws. Bone graft augmentation was also performed. Illustrations C and D are AP and lateral radiographs, respectively, demonstrating a healed medial malleolar nonunion.
Incorrect Answers:
Answer 2: Fragment excision is not appropriate in this case as the fragment is large and well-preserved.
Answer 3: Stress radiographs are unnecessary in this case as the patient is symptomatic and the diagnosis is made with the available imaging.
Answer 4: Non-operative treatment of symptomatic malleolar nonunions is not recommended.
Answer 5: Percutaneous skeletal fixation in the presence of a nonunion is not recommended as the fracture site cannot be debrided and it will not be possible to augment with bone graft.
A 76-year-old left-handed female presents to your office after a fall with the injury seen in Figure A. When treating this fracture with hemiarthroplasty, which of the following is the most important for a successful outcome?
1) Anatomic healing of the tuberosities
2) Stem retroversion of 25 degrees
3) Surgical fixation within 24 hours
4) Anterior superior labral repair
5) Age over 75
When performing a hemiarthroplasty for a displaced four-part proximal humerus fracture, the best predictor of a successful outcome is anatomic healing of the tuberosities.
Although most proximal humerus fracture can be treated nonoperatively, especially in elderly low-demand patients, some debate remains regarding the use of a hemiarthroplasty vs. reverse total shoulder arthroplasty. When performing a hemiarthroplasty for a displaced four-part proximal humerus fracture, it is of the utmost importance to achieve a stable and anatomic reduction of the tuberosities. Studies have shown malpositioned or migrated tuberosities leads to stiffness, weakness, and persistent pain. Restoration of humeral height and version is also important for successful outcomes of hemiarthroplasty.
Rangan et al., in the PROFHER trial, studied the outcomes of patients with displaced proximal humerus fractures treated with surgical vs. nonsurgical intervention. Of note, in the surgical group, 83% of patients were treated with ORIF, 9% were treated with hemiarthroplasty, and the remainder were treated with some other fixation method. They found no difference at 2 years between the surgical and nonsurgical groups with regard to outcome scoring, complications from surgery or nonoperative care, secondary surgery, new therapy requirement, or mortality. They concluded the current increase in surgery in patients with displaced proximal humerus fractures is not supported by this data.
Boileau et al. followed 66 patients with displaced proximal humerus fractures treated with hemiarthroplasty to evaluate for clinical and radiographic parameters that could lead to worse outcomes. They found that 50% of patients had malpositioning of the greater tuberosity, which correlated with unsatisfactory results, superior migration of the prosthesis, stiffness or weakness, and persistent pain. They concluded that the primary goal of arthroplasty for proximal humerus fractures should be obtaining anatomic tuberosity healing.
Figure A shows a displaced four-part proximal humerus fracture. Incorrect Answers:
Answer 2: Although appropriate retroversion is important for optimal function,
anatomic healing of the tuberosities is felt to contribute more to successful outcomes.
Answer 3: Surgical timing has not been reported to be associated with improved outcomes in this fracture pattern.
Answer 4: Anterior superior labral repair would not be indicated and would be of little benefit in this setting.
Answer 5: Age over 75 has been shown to predict worse tuberosity healing as subsequent worse outcomes.
A 25-year-old man sustains a left leg injury during a motorcycle accident. A radiograph is provided in Figure A. The fracture is treated in a minimally invasive manner with a lateral locking plate and percutaneous screw fixation. A post-operative radiograph is provided in Figure B. Which of the following complications has been associated with this fixation construct?
1) Compartment syndrome
2) Common peroneal nerve injury
3) Superficial peroneal nerve injury
4) Deep peroneal nerve injury
5) Popliteal artery injury
Figures A and B demonstrate pre and post-operative radiographs of a comminuted proximal tibia fracture treated with a long locking plate. Compartment syndrome is a significant complication associated with this fracture. However, there is no greater risk of compartment syndrome with use of this specific construct plate. Long lateral locking plates have been shown to put the superficial peroneal nerve at risk with insertion of distal locking screws. Use of a larger incision and careful dissection down to the plate in this region may minimize the risk of damage to the nerve.
Deangelis et al performed a cadaveric study evaluating 14 extremities and the relationship between the superficial peroneal nerve to the percutaneous screws of the 13-hole proximal tibia Less Invasive Stabilization System (LISS) plate.
The average distance from the superficial peroneal nerve to the center of holes 11, 12, and 13 was 10.0 mm, 6.8 mm, and 2.7 mm, respectively. In 12 of 14 legs (86%), the superficial peroneal nerve was 5.0 mm or less from the center of hole 13.
Cole et al reviewed his experience of 77 proximal tibia fractures treated with the LISS plate. He reported a high rate of union (97%) with only 2 infections, 2 nonunions, 1 nerve palsy, and 8 patients with an angular malunion approaching 10 degrees.
A 48-year-old male returns to your office 8 months after sustaining a proximal humerus fracture that was successfully treated nonoperatively. However he is still having persistent anterior shoulder/arm pain that worsens with most activities. He has not done any physical therapy nor received a corticosteroid injection. What nerve innervates the structure identified by the red arrow in Figure A, what is its primary function, and where does it originate from?
1) Subscapular nerves, shoulder internal rotation, ventral scapula
2) Musculocutaneous nerve, elbow pronation, coracoid
3) Axillary nerve, shoulder external rotation, dorsal scapula
4) Musculocutaneous nerve, elbow supination, supraglenoid tubercle
5) Suprascapular nerve, shoulder abduction, dorsal scapula
The figure demonstrates a rupture of the long head of the biceps brachii (LHB). The biceps primarily supinates the elbow via innervation from the musculocutaneous nerve.
The long head of the biceps originates in the shoulder at the supraglenoid tubercle, traverses through the bicipital groove, forms the muscle belly of the biceps brachii with the short head from the coracoid process. This then inserts distally onto the radial tuberosity in the proximal radius. This consistent anatomy allows it to be used as an anatomical reference during repair of comminuted proximal humerus fracture patterns.
Tosounidis et al. compared the histological appearance of LHB tendons from individuals undergoing hemiarthroplasty for proximal humerus fractures to control cadaveric specimens. They noted a significant rate of degenerative lesions within the LHB in the fracture cohort. They use this as a basis for performing tenotomy/tenodesis of the LHB during fracture surgery.
Soliman et al. performed a prospective randomized trial of individuals undergoing shoulder hemiarthroplasties who either received an LHB tenodesis or it was neglected. They reported improved Constant and PRO scores for those who received a tenodesis while there was no strength difference noted. Based on this they concluded biceps tenodesis during hemiarthroplasty is indicated.
Nho et al. reviewed the pathology and management of biceps pathology. They note the LHB can be the primary isolated pathologic process but more often LHB lesions are in conjunction with other intra-articular pathology. Various methods exist do address biceps pathology, ranging from simple tenotomy to open or arthroscopic tenodesis.
Figure A is a fluid-sensitive axial MR sequence with the arrowhead pointing to the LHB within the groove.
Incorrect Answers:
Answer 1: This describes the subscapularis muscle. Answer 2: The biceps is responsible for elbow supination. Answer 3: This describes the teres minor muscle.
Answer 5: This describes the supraspinatus muscle.
A 23-year-old-male was involved in a motorcycle accident. Imaging is shown in Figure A. In order to prevent the most common deformity associated with intramedullary nailing of this injury, where should blocking screws be placed and what deformity are they trying to prevent?
1) Lateral and posterior to the nail in the proximal segment; procurvatum and valgus
2) Medial and posterior to the nail in the proximal segment; procurvatum and varus
3) Lateral and posterior to the nail in the proximal segment; recurvatum and varus
4) Medial and anterior to the nail in the proximal segment; recurvatum and valgus
5) Anterior and posterior to the nail in the proximal segment; recurvatum
When using intramedullary nails (IMNs) for treatment of proximal tibia fractures, blocking screws can be used to prevent the typical deformity of valgus and apex anterior. Traditionally, these blocking screws are placed lateral and posterior to the nail in the proximal segment.
Proximal tibia fractures have a tendency to displace into valgus and procurvatum due to deforming forces from the pes anserinus and anterior compartment (valgus) and patellar ligament (procurvatum). It is difficult to correct or prevent this mal-alignment with IMN insertion alone due to the capacious nature of the proximal tibial metaphysis compared to the canal fit of
the IMN in the diaphyseal segment. Blocking screws placed lateral and posterior to the nail have been found to prevent this translation by effectively decreasing canal space for the intramedullary device. In the proximal tibia, a good "rule of thumb" is to place the blocking screws on the concavity of the deformity in the metaphyseal segment; however blocking screws are not only used this way.
Krettek et al. performed a study to evaluate the mechanical effects of medial and lateral blocking screws in supplementing intramedullary nail fixation of high proximal and low distal tibia fractures treated with small-diameter intramedullary nails. They found that the addition of a medial blocking screw in the proximal tibia increased the deformation of the construct. They conclude that medial blocking screws can increase the primary stability of proximal metaphyseal fractures after nailing. This study exemplifies the use of blocking screws not only to help achieve alignment when treating a fracture but also maintain the alignment during fracture healing when the IMN is not canal-fitting around a fracture site.
Another study by Krettek et al. evaluated the clinical use of blocking screws as a supplement to stability after fixation with statically locked intramedullary nails in metaphyseal fractures. They prospectively studied 21 tibial fractures, 10 in the proximal third and 11 in the distal third. They found that losses of reduction were minimal when using blocking screws. They also had no complications related to the use of blocking screws. They conclude that blocking screws are a useful adjunct when nailing metaphyseal fractures of the tibia.
Figures A and B are AP and lateral radiographs of the tibia and fibula, respectively, demonstrating proximal tibia and fibula fractures. Illustrations A and B are AP and lateral images of the same injury, respectively, treated with an intramedullary nail. Note the use of blocking screws lateral and posterior to the nail.
Incorrect Answers:
Answers 2, 3, 4, & 5: Blocking screws are typically used to "block" the IMN from creating or fixing a mal-reduction. In this case, they should be placed lateral and posterior to the nail to prevent a valgus and apex anterior deformity.
Which of the following distal radius fractures is associated with volar translation of carpus relative to the radial articulation?
1) Displaced impaction fracture of the lunate fossa
2) Displaced intra-articular fracture with a fragment consisting of the volar-ulnar corner
3) Displaced radial styloid fracture
4) Displaced extra-articular fracture with apex volar
5) Displaced extra-articular fracture with apex dorsal
A displaced intra-articular fracture with a fragment containing the critical volar-ulnar corner rim of the distal radius would result in volar translation of the carpus.
Distal radius fractures are one of the most common orthopedic injuries and can result from low-energy trauma in older and osteoporotic patients or high-energy trauma in young patients. Intra-articular involvement poses treatment
challenges for these fractures as the fragments are crucial to articular stability and are difficult to achieve fixation with traditional distal radius plates.
Fractures with intra-articular comminution of the distal radius that involve either the dorsal or volar rim of the lunate fossa, which can destabilize the radiocarpal joint, can lead to volar or ulnar translation of the carpus.
Orbay et al. performed a retrospective review of patients undergoing either hook plate fixation or volar opening wedge osteotomy for volar marginal fragment distal radius fractures. For the patients treated with hook extension plates, there was a 90% success rate in the prevention of volar subluxation of the carpus. For patients that required volar open wedge osteotomy to redistribute joint loading forces in those that developed avascular necrosis of the volar marginal fragments, all patients had improved pain, function, and radiographic concentric reduction of the radiocarpal joint. They concluded that hook plate fixation provides an effective means of fixation of a volar marginal fracture of the distal radius with volar opening wedge osteotomy as an effective salvage procedure.
O'Shaughnessy et al. performed a retrospective study of hook plate fixation of distal radius fractures with volar marginal rim fragments. There were no patients in the study that lost fixation of the volar marginal fragments after treatment with hook plates with the most common complication being symptomatic hardware requiring removal of both the traditional plate and the hook plate. The authors concluded that hook plate fixation provides a highly effective means of distal radial fragment fixation that is not amenable to traditional plate fixation.
Illustration A depicts a lateral radiograph of the right wrist with a fracture of the volar-ulnar corner resulting in volar translation of the carpus. Illustration B depicts a lateral radiograph of the wrist with a ulnar hook plate buttressing an articular surface rim fracture.
Incorrect answers:
Answer 1: Impaction fractures of the lunate fossa do not result in translational instability of the carpus.
Answer 3: A radial styloid fracture can result in ulnar translation of the carpus if the fragment is large enough to involve the large radiocarpal stabilizing ligaments.
Answer 4: An extra-articular fracture of the distal radius with apex volar angulation may have dorsal comminution, but there is no added risk of volar carpal translation.
Answer 5: An extra-articular distal radius fracture with apex dorsal angulation
leads to volar tilting of the articular surface, but there is no volar translation of the carpus.
Which of the following acetabular fractures is classified as an elementary fracture pattern that involves two columns?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure B is a radiograph of a transverse acetabular fracture, which is the only elementary fracture pattern that involves two columns.
The acetabulum consists of two columns arranged in an inverted Y-shaped configuration. Fractures are divided into five elementary patterns and five associated patterns. Elementary fractures involve only one fracture plane or surface while associated fractures involve multiple fracture planes or surfaces. The transverse fracture is the only elementary pattern that involves two
columns. Six fundamental landmarks of the acetabulum must be evaluated on each AP pelvic radiograph: the lateral border of the anterior wall; the lateral border of the posterior wall; the acetabular roof, representing the weightbearing dome; the teardrop; the ilioischial line, representing the posterior column; and the iliopectineal line, representing the anterior column or pelvic brim.
Mauffrey et al. performed a review of the radiographic evaluation of acetabular fractures. They report that plain radiographs remain the initial step in the classification of acetabular fractures. The ability to accurately interpret the injury allows the surgeon to develop a thorough preoperative plan and to evaluate the quality of the reduction and fixation intraoperatively. Though CT and three-dimensional imaging is obtained in addition to radiographs, radiographs still have a vital role to play in the diagnosis and treatment of acetabular fractures.
Durkee et al. performed a study to characterize and classify the radiographic and CT appearance of common acetabular fractures. They report that for a transverse fracture, there is no involvement of the obturator ring. It causes disruption of both the iliopectineal and ilioischial lines, however. On CT, this fracture line is sagittally oriented. It is transverse relative to the plane of the acetabulum.
Figures A-E are AP radiographs of the pelvis demonstrating an associated both column (ABC) acetabular fracture, a transverse acetabular fracture, a posterior wall acetabular fracture, a T-type acetabular fracture, and a normal pelvis, respectively. Illustration A is an image demonstrating normal acetabular lines and morphology on the right and a transverse acetabular fracture on the left.
Illustration B is an algorithm to determine acetabular fracture patterns (Mauffrey et al.).
Incorrect Answers:
Answers 1, 3, 4, & 5: The transverse acetabular fracture is the only elementary pattern to involve two columns.
A 90-year-old patient presents after a fall down a flight of stairs and sustains a hip fracture, several rib fractures, a right pneumothorax, a right grade 1 open humerus fracture, and a subdural hematoma. The patient requires intubation in the trauma bay. The trauma team assesses the Injury Severity Score to 36. Which factor is associated with the highest risk of mortality at 1-year?
1) Presence of a head injury
2) The need for mechanical ventilation
3) Injury severity score greater than 25
4) Presence of a hip fracture
5) Presence of an open fracture
The patient is a nonagenarian presenting with multiple injuries after trauma. The need for mechanical ventilation is associated with the highest risk of mortality at 1-year with 78.7% risk.
Geriatric patients pose different treatment challenges in the trauma setting compared to patients under the age of 65. The treatment course is complicated by many medical comorbidities, polypharmacy, lower physiologic reserve, and increased risk of medical complications. Several factors have been described as predictors of mortality in admission including the presence of a head injury, the need for mechanical ventilation, higher Injury Severity Score (ISS), and treatment at a facility other than a trauma center. Of these factors, the need for mechanical ventilation has the highest association with mortality, especially at 1-year.
Hwabejire et al. performed a retrospective study of mortality predictors in trauma patients greater than 90 years of age. The in-hospital mortality was significantly associated with Injury Severity Score, cervical spine injury, and the need for mechanical ventilation with an overall in-hospital mortality rate being 9.5%. At 1-year, mortality rates were increased to 78.7% if the patient required mechanical ventilation at the time of admission. The authors concluded that despite the low in-hospital mortality these risk factors are strong predictors to 1-year from the injury.
Mock et al. performed a retrospective cohort study investigating the predictors of mortality in geriatric trauma patients. The found through multivariate analysis that the need for mechanical ventilation, admission lactate, and the length of mechanical ventilation were significant predictors of mortality. They stipulated that the need for mechanical ventilation is a predictor of mortality, but this finding is confounded with the withdrawal of care.
Meldon et al. performed a retrospective cohort study looking at outcomes and care settings of trauma patients over the age of 80. The authors reported a significantly higher mortality rate with treatment performed at acute care hospitals compared to level 1 and level 2 trauma centers. Additionally, mortality was associated with increased ISS and decreased Glasgow Coma Score. They concluded that treatment at a trauma verified center as a survival benefit for geriatric trauma patients.
Incorrect answers:
Answer 1: The presence of a head injury at the time of admission does increase the mortality risk at 1-year, with one study citing 51.1%.
Answer 3: An injury severity score greater than 25 has been associated with increased mortality at 1-year, but several studies have linked the need for
mechanical ventilation to greater mortality risk. One study reported 73.2% mortality at 1-year in patients with ISS greater than 25.
Answer 4: The effect of a hip fracture in geriatric trauma patient mortality has not been characterized, but 1-year mortality risk is approximately 30%.
Answer 5: The mortality risk of an open fracture in a geriatric trauma patient has been seldom studied, but some authors report risks similar to geriatric hip fractures.
What is the spur sign and on which view is it best seen?
1) Intact ilium; obturator oblique
2) Intact ilium; iliac oblique
3) Posterior wall fragment; iliac oblique
4) Posterior wall fragment; obturator oblique
5) Posterior wall fragment; oburator inlet
The spur sign represents the intact posteroinferior aspect of the ilium that is seen in an associated both column (ABC) acetabular fracture. It is best seen on the obturator oblique view.
The spur sign is the portion of nonarticular ilium above the acetabulum that becomes visible on the obturator oblique view with medial displacement of the acetabulum. Nondisplaced associated both-column fractures will not have a spur sign on the obturator oblique view. Computed tomography should be used to verify the continuity between the axial skeleton and the acetabular articular surface.
Mauffrey et al. performed a radiographic evaluation of acetabular fractures. They report that, when evaluating acetabular fractures, CT scans are useful because they allow the clinician to trace an intact strut of bone from the sacroiliac joint to the weight-bearing dome of the acetabulum. If a piece of bone is not present in continuity between the sacroiliac joint and the acetabulum, the fracture must be an associated both-column fracture. If a spur sign is not present and a continuous bony bridge between the sacroiliac joint and the acetabulum is present, the fracture is classified as an anterior column posterior hemitransverse fracture.
Kellam and Messer performed a study to assess acetabular joint congruity and postoperative reconstructions. They evaluated the use of coronal and sagittal
reconstruction of transaxial CT scans. They found in all cases of marginal impaction coronal and sagittal CT reconstruction showed that the fragments were larger than they appeared to be on the transaxial CT scan. They conclude that coronal and sagittal CT reconstruction provided more detailed evaluations of complex fractures than other studies.
Illustration A is an electronically simulated image demonstrating an associated both column acetabular fracture on the left side. Illustration B is an obturator oblique of the same image with the spur sign indicated by the arrow.
Incorrect Answers:
Answers 2, 3, 4, & 5: The spur sign is a portion of the intact ilium that is best seen on the obturator oblique view. It is indicative of an associated both column fracture.
An errant screw is placed during the procedure shown in Figure
A. What is the most likely physical exam manifestation?
1) Weakness in knee extension
2) Weakness in ankle plantarflexion
3) Weakness in great toe extension
4) Numbness over the medial aspect of the leg
5) Numbness over the posterior leg
The most likely location for an errantly placed screw is anterior. This would lead to injury in the L5 nerve root, which would manifest with weakness in great toe extension.
Indications for iliosacral screw fixation include complete sacral fractures (i.e. fractures that extend through the sacrum in its entirety, anterior to posterior), sacroiliac joint disruptions, and combinations of these posterior pelvic injuries following reduction. The safe zone for screws is the area within the sacrum where the screws remain within the bone. The L5 and S1 nerve roots course from the spinal canal in an anterior-lateral-caudal and oblique direction. The L5 nerve root is located on the anterior-cranial sacral alar surface and may be injured by an errant screw that is placed too anteriorly. The S1 nerve root is located within the oblique neural tunnel, beginning at the spinal canal and exiting through the anterior sacral foramina between the upper and second sacral segments.
Kaiser et al. performed a study to evaluate anatomic determinants of sacral dysmorphism and implications for safe screw placement. They found the prevalence of upper sacral segment dysplasia at 41%. The major determinants of sacral dysmorphism are upper sacral segment coronal and axial angulations. They developed a sacral dysmorphism score, derived with the equation: (first sacral coronal angle) + 2(first sacral axial angle). They conclude that the sacral dysmorphism score quantifies dysmorphism and can be used in preoperative planning of IS screw placement.
Miller and Routt performed a review of variations in sacral morphology and
implications for iliosacral screw fixation. They report that knowledge of the posterior pelvic anatomy, its variations, and related imaging is critical to performing reproducibly safe surgery. They report that the dysmorphic pelvis has several key characteristics. The upper portion is colinear with the iliac crests on the outlet view. Mamillary bodies (underdeveloped transverse processes) may be present as well. A residual upper sacral disk may be present along with an acute alar slope. They conclude that the surgeon must be knowledgeable about individual patient anatomy to ensure safe iliosacral screw placement.
Figure A is an illustration of a sacroiliac-style iliosacral screw. Illustration A is an inlet fluoroscopic image demonstrating the drill within the sacrum with an arrow indicating the location of the L5 nerve root. Illustration B is an axial CT of a patient with normal sacral anatomy through the first sacral and second sacral segments, respectively. Illustration C is an axial CT of a patient with dysmorphic sacral anatomy through the first sacral and second sacral segments, respectively. The L5 nerve roots are indicated by the white circles.
Incorrect Answers:
Answer 1: Weakness in knee extension would indicate injury to the L4 nerve root.
Answer 2: Weakness in ankle plantarflexion would indicate injury to the S1 nerve root.
Answer 4: Numbness to the medial leg would indicate injury to the L4 nerve root.
Answer 5: Numbness over the posterior leg would indicate injury to the S1 nerve root.
During which surgical approach to the acetabulum is the sciatic nerve placed at risk, and how should the patient be positioned to minimize the risk of injury?
1) Kocher-Langenbeck; hip extended and knee extended
2) Kocher-Langenbeck; hip extended and knee flexed
3) Kocher-Langenbeck; hip flexed and knee extended
4) Ilioinguinal; hip extended and knee extended
5) Ilioinguinal; hip extended and knee flexed
The sciatic nerve is placed at risk when performing the Kocher-Langenbeck approach to the acetabulum. Positioning the patient with the hip extended and the knee flexed minimizes the risk of injury to the sciatic nerve.
During the surgical fixation of acetabular fractures through a Kocher-Langenbeck approach, the sciatic nerve is placed at risk. It can be injured during the internal fixation of acetabular fractures, as well as during plate fixation and retractor placement. The sciatic nerve is maintained in the least
tension by keeping the hip extended and the knee flexed.
Isaak et al. published a review on sciatic nerve injuries associated with acetabular fractures. They reported that sciatic nerve injuries may occur as a result of the initial acetabular trauma (posttraumatic), as a result of iatrogenic trauma during surgery (perioperative), or as a later complication of surgery (postoperative). Iatrogenic injuries, in particular, can result from: (1) a stretch injury due to excessive retraction of the posterior gluteal muscle mass with the hip in flexion or continuous extension of the ipsilateral knee, (2) placement of retractors or reduction clamps in the lesser or greater sciatic notch, or (3) drilling or placing screws into the greater sciatic notch.
Fassler et al. performed a study on functional outcomes of sciatic nerve injuries after a displaced acetabular fracture. They found that all but one patient had a satisfactory (fair or better) functional outcome, but 11 patients had residual neurological sequelae that ranged from minor paresthesia to footdrop. They also found that the patients who had isolated mild involvement of the peroneal nerve had a favorable prognosis, but those who had a severe injury of the peroneal component, whether it was isolated or associated with an injury of the tibial component, did not recover good function.
Incorrect Answers:
Answers 1 and 3: The sciatic nerve is maintained in the least tension when the hip is extended and the knee is flexed.
Answers 4 and 5: The femoral and lateral cutaneous femoral nerves, not the sciatic nerve, are at risk of injury when performing the ilioinguinal approach to the acetabulum.
A 59-year-old patient presents with right elbow pain after a fall off a ladder. There is swelling of the elbow with a visible deformity. The patient is neurovascularly intact with decreased sensation in the ring and small fingers. The patient states that this has been present for several years. Figures A and B are radiographs of the right elbow. What is the most appropriate treatment that provides the greatest construct rigidity and appropriately addresses the patient's ulnar nerve symptoms?
1) Bicolumnar orthogonal plating with submuscular transposition
2) Bicolumnar parallel plating with all distal screws passing through a plate and in situ cubital tunnel release
3) Bicolumnar parallel plating with all distal screws passing through a plate and observation of ulnar neuropathy
4) Bicolumnar orthogonal plating with in situ cubital tunnel release
5) Interfragmentary screw fixation of the articular surface with neutralization plating and subcutaneous transposition of the ulnar nerve
The patient is presenting with a H-type distal humerus fracture with previous cubital tunnel symptoms. The biomechanically strongest treatment option would include bicolumnar parallel plating following the fixation objectives of O'Driscoll and a cubital tunnel release to address the ulnar nerve symptoms.
Distal humerus fractures are potentially complex fractures that require special fixation considerations when performing open reduction and internal fixation. The fixation objectives of O'Driscoll state that every screw should pass through a plate, each screw should be as long as possible, engaging as many articular fragments as possible, screws from each plate should interdigitate, and that compression is achieved in both columns through the supracondylar region and shaft. Studies have demonstrated that parallel plating provides the greatest construct rigidity than orthogonal plating. Bicolumnar parallel plating has been found to have significant greater biomechanical strength and rigidity compared to orthogonal plating, but clinical differences between the two plate types are minimal to absent. In the setting of chronic cubital tunnel syndrome, an in situ ulnar nerve decompression should be performed at the time of open reduction and internal fixation.
Cobb et al. performed a retrospective study of elderly patients, with a mean age of 72 years, undergoing a primary total elbow arthroplasty for distal humerus fractures. The authors reported there to be excellent outcomes in 75% of patients at 3.3 years according to the Mayo elbow performance score with the mean range of motion being 25-130 degrees and only one implant requiring revision. The authors concluded that total elbow replacement is an effective option for severely comminuted distal humerus fractures in elderly patients, but is not recommended in younger patients.
Taylor et al. performed a biomechanical cadaveric study testing for construct rigidity and strength between parallel and orthogonal distal humeral plating. They found the parallel plating had greater external and internal torsional rigidity, flexion and extension bending rigidity, and bend to failure strength. They concluded that parallel plating was a significantly stronger construct that
may be desirable in the treatment of comminuted distal humerus fractures.
Shearin et al. performed a meta-analysis comparing ulnar nerve decompression to ulnar nerve transposition during surgical treatment of distal humerus fractures. The pooled data in their analysis revealed an overall 19.3% incidence of ulnar nerve neuropathy with a 15.3% incidence with an in situ release and 23.5% incidence with ulnar nerve transposition. They concluded that transposition of the ulnar nerve did not have a protective effect against post-operative neuropathy, but there could have been a confounding effect of increased fracture severity observed in this group.
In a current concepts review in the Journal of Hand Surgery, Fajolu et al. propose that a transposition should only be performed at the conclusion of the case if the surgeon feels that the previously released nerve is in contact with the hardware or if the surgeon feels that there was excessive traction on the nerve during the case.
Figures A and B depict an AP and lateral radiograph of the elbow with a severely comminuted bicolumnar distal humerus fracture. Illustrations A and B depict the postoperative radiographs with bicolumnar plating following the fixation objectives of O'Driscoll.
Incorrect answers:
Answer 1: Parallel plating provides the greater biomechanical construct rigidity than orthogonal plating. Submuscular transposition is indicated if there is subluxation of the ulnar nerve or recurrence of cubital tunnel release.
Answer 3: Observation of chronic ulnar neuropathy is not recommended since these symptoms are likely to worsen after open reduction and internal fixation if not addressed.
Answer 4: Parallel plating provides the greater biomechanical construct rigidity than orthogonal plating.
Answer 5: Use of interfragmentary lag screws that are not passing through a plate is not part of the fixation objectives of O'Driscoll.
A 35-year-old female fell while riding a motorcycle and sustained the left elbow injury shown in Figures A and B. Figures C and D are the CT scan and 3D reconstruction of the injury. After closed reduction, the elbow is unstable with valgus stress at 40 degrees of flexion. What is the most appropriate definitive treatment?
1) Radial head ORIF and MCL repair
2) Radial head replacement and LUCL repair
3) Radial head excision, coronoid ORIF, and LUCL repair
4) Radial head replacement, coronoid ORIF, and LUCL repair
5) Radial head excision and LUCL repair
The patient has a terrible triad injury of the elbow, which will require a radial head replacement, coronoid ORIF, and lateral ulnar collateral ligament (LUCL) repair.
Terrible triad injuries are the result of a radial head fracture, a coronoid tip fracture, and a posterior elbow dislocation. The structures damaged with this injury pattern begins with the disruption of the LUCL, then the anterior capsule, and possibly the medial collateral ligament. Treatment involves ORIF of the radial head if 40% articular involvement. Repair of the LUCL to the humeral insertion is required in most cases. Coronoid fractures result from avulsion of the anterior capsule and usually involve small bone fragments.
Tejwani et al. reviewed the management of fractures of the radial head and neck. The authors recommended performing an open reduction and internal fixation when fractures of the radial head involve three or fewer pieces. Radial head excision is not recommended when there is associated elbow dislocation or ligamentous instability.
Acevedo et al. reviewed the current literature on implant designs for radial head arthroplasty (RHA). Loose-fitting prostheses settle to a level of anatomic stability over time and have low complication rates. Press-fit stems obtain intramedullary fixation through hoop stresses. However, implants with plasma-sprayed titanium stem have been associated with increased revision rates because of subsequent loosening. Bipolar prostheses consist of a press-fit stem that articulates with a polyethylene head component at the head and neck junction and is associated with increased dislocation rates, especially in the setting of a terrible triad injury. Understanding the prosthesis design of radial head implants is necessary to ensure good outcomes following terrible triad injuries.
Wyrick et al. reviewed the management of complex elbow dislocations. The literature suggests terrible triad injuries should be urgently closed reduced to avoid potential neurovascular injuries and splinted in 90 degrees flexion to confer a stable reduction until operative management. The recommended sequence of repair begins with lasso fixation of the coronoid, followed by fixation or replacement of the radial head, and then repair of the LUCL.
Figures A and B are AP and lateral radiographs of the left elbow with a terrible triad injury and comminution of the radial head. Figure C is the sagittal CT scan of the ulnohumeral joint demonstrating a coronoid fracture. Figure D is
the 3D CT reconstruction of the elbow with comminution of the radial head and a type 2 fracture of the coronoid.
Incorrect answers:
Answer 1: The patient has a comminuted fracture of the radial head that would require an RHA rather than an ORIF. MCL is less likely than a LUCL injury.
Answer 2: The patient sustained a coronoid fracture with greater than 10% involvement, which should be addressed with ORIF.
Answers 3 and 5: Radial head excision should never be performed in the setting of elbow instability.
A 35-year-old male sustains the injury shown in Figure A. He is currently not cleared for surgery due to a severe head injury. At what time point after the injury is there an increased risk of a poor outcome?
1) 48 hours
2) 5 days
3) 1 week
4) 2 weeks
5) 3 weeks
This patient has sustained an anterior column acetabular fracture. Delay of fixation for more than 3 weeks is associated with difficulty in achieving adequate reduction and poor outcomes.
Historically earlier treatment of acetabular fractures has been shown to improve clinical and functional outcomes. Delays of more than 3 weeks have been associated with difficulty obtaining an anatomic reduction and decreased overall patient outcomes. An increased delay has not been shown to increase the chances of neurological injury, infection, or heterotopic ossification.
Plaisier et al. performed a study to evaluate the effect of the timing of fixation for acetabular and pelvic ring fractures on patient outcome. They found that early fixation of acetabular fractures was associated with a decreased total length of stay. Functional outcome was improved in early fixation of acetabular fractures with a greater proportion of patients being discharged home rather than to rehabilitation or skilled care. They conclude that patients with early repair of acetabular fractures had significantly less organ dysfunction and exhibited improved functional outcome.
Madhu et al. performed a retrospective case review to determine if the time to surgery was predictive of radiological and functional outcomes of acetabular fractures. For elementary fractures, an increase in the time to surgery of one day reduced the odds of an excellent/good functional result by 15% and of an anatomical reduction by 18%. For associated fractures, the odds of obtaining an excellent/good result were reduced by 19% and an anatomical reduction by 18% per day. They conclude that the time to surgery is a significant predictor of radiological and functional outcome for both elementary and associated displaced fractures of the acetabulum.
Figure A is an AP pelvis demonstrating a displaced fracture of anterior column. Incorrect Answers:
Answers 1, 2, 3, & 4: Delay of fixation for more than 3 weeks is associated
with difficulty in achieving adequate reduction and poor outcomes.
A 43-year-old male presents to the trauma bay with the injury sustained in Figure A after a motor vehicle collision. After appropriate resuscitation, you have decided to proceed with open reduction and internal fixation via a Kocher approach and percutaneous fixation of the anterior column. The inlet view can be used to help visualize which of the following during guidewire placement?
1) Anterior-posterior position of the wire within the ramus
2) Ensure appropriate reduction of the fracture
3) Cranial-caudal position of the wire
4) Rule out joint penetration of the wire
5) Ensure the wire is within the tables of the ilium
An inlet view of the anterior pelvis can be used to help visualize the anterior-posterior position of the guide-wire in reference to the ramus during the placement of an anterior column screw.
Anterior column fixation can be performed percutaneously with a medullary screw as a less-invasive alternative to ORIF of the anterior column. Medullary implants can be inserted safely through the anterior column osseous fixation pathway from anterograde or retrograde start points (Illustrations A and B). When placed anterograde, the start point is on the gluteal pilar and the implant is then inserted and directed towards the pubic tubercle. The combined obturator oblique outlet (COOO) view helps ensure the screw does not penetrate the hip joint nor the vascular lacuna. An inlet view demonstrates the anterior-posterior limits of the osseous fixation pathway in the ramus portion of the corridor. Some authors have described a modified inlet with iliac-oblique rollback to it, however the tangential lines of the ramus are usually best seen on a pure inlet view.
Starr et al. wrote a technique on percutaneous fixation of the columns of the acetabulum. They report to safely place an anterior column screw, the C-arm should be oriented perpendicular to the superior pubic ramus. The C-arm is rotated during screw placement between an iliac inlet view and an obturator outlet view. The iliac inlet view is used to ensure that the guidewire does not penetrate the inner cortex of the superior ramus. The obturator outlet view is used to make sure the wire does not penetrate the hip joint.
Mauffrey et al. performed a review of the radiographic evaluation of acetabular fractures. They report that the acetabulum consists of two columns of bone arranged in an inverted Y-shaped configuration and attached to the ilium. They report that radiographic evaluation and classification of acetabular fractures is necessary to guide treatment decisions. They conclude that CT scans provide invaluable information in classifying these injuries.
Figure A is the AP pelvis radiograph revealing a right transverse acetabulum fracture. Illustration A demonstrates the path for retrograde placement of an anterior column screw. Illustration B demonstrates the path for anterograde placement of an anterior column screw. Illustration C and D are intra-operative fluoroscopy views revealing an inlet view and obturator outlet views, respectively.
Incorrect Answers:
Answer 2: The best view ensuring appropriate reduction is direct visualization of the fracture (open reduction).
Answer 3: The obturator outlet view is used to determine the cranial-caudal position of the wire during the placement of an anterior column screw.
Answer 4: The obturator outlet view is used to help rule out joint penetration during the placement of an anterior column screw.
Answer 5: The obturator inlet view is used to help determine if a supra-acetabular wire is within the tables of the ilium.
An 87-year-old female sustained the injury shown in Figure A. Which of the following is/are factor(s) that increase the risk of perforation of the anterior cortex during surgical treatment with a long cephalomedullary nail?
1) Radius of curvature mismatch between the bone and the implant
2) Anterior starting point on the greater trochanter
3) Posterior starting point on the greater trochanter
4) Answers 1 and 2
5) Answers 1 and 3
This patient sustained an intertrochanteric femur fracture. A mismatch of curvature between the nail and a posterior start point are both risk factors for anterior cortex perforation during surgical treatment with a long cephalomedullary nail.
When treating elderly patients with long intramedullary nails, there are certain factors that need to be accounted for. There is a mismatch between the radius of the femoral nails currently available and the femoral canal, ie, nails with a larger radius of curvature (straighter) are being inserted in a femur with a
smaller radius of curvature (less straight than the nail). As a result, the distal tip of the nail is forced into a nonanatomic anterior position during final seating of the nail distally. To avoid this complication, a lateral view of the distal femur while inserting the nail is recommended. Additionally, a posterior starting point on the greater trochanter is also a risk factor for anterior perforation of the nail.
Ostrum et al. performed a case report of 3 cases with penetration of the distal femoral anterior cortex during intramedullary nailing for subtrochanteric femur fractures. They report that the difference in the femoral anteroposterior bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration. The radius of curvature of the femur is less than the radius of curvature of the nails.
Roberts et al. performed a retrospective review to determine risk factors for impingement and penetration of the anterior cortex of the distal femur during intramedullary nailing of proximal femur fractures. The found that shorter patients and patients with an increased femoral bow were likely to have an anterior nail tip position or cortical impingement. They conclude that anterior starting points should be used to avoid this complication.
Figure A is an AP radiograph demonstrating a left intertrochanteric femur fracture.
Incorrect Answers:
Answers 1, 2, 3, 4: Risk factors for perforation of the anterior cortex while placing a long nail in an elderly patient are a mismatch in the radius of curvature and a posterior start point.
A 65-year-old man sustained the closed injury seen in Figures A and B and is being treated nonoperatively in a functional brace. At what time point after the injury does the lack of callus formation and motion at the fracture site first become concerning for nonunion?
1) 2 weeks
2) 4 weeks
3) 6 weeks
4) 12 weeks
5) 6 months
In a closed humeral shaft fracture, gross motion at the fracture site and no callus formation on radiographs at 6 weeks has a specificity of 100% and positive predictive value of 100% of going on to nonunion.
Closed midshaft humerus fractures treated with nonoperative measures such as functional bracing have been shown to go on to union in most patients.
Treatment with functional bracing relies on hydrostatic compressive forces from the surrounding soft tissues to provide adequate stability for healing. However, approximately 10% of patients go on to nonunion and require subsequent surgical stabilization. Predictors of nonunion include no callous at the fracture site and gross motion at the fracture site at 6 weeks from injury.
Papasoulis et al. reviewed the clinical studies of humeral shaft fractures treated with functional bracing. They found that this set of studies showed healing at
10.7 weeks from injury at a union rate of 94.5%. They concluded that functional bracing has many known benefits and remains a reliable treatment however certain parameters such as functional outcome, residual deformity, and loss of joint motion remain unclear and require further research.
Driesman et al. followed 84 consecutive patients with diaphyseal humeral shaft fractures treated nonoperatively. They found that mobile fracture sites at 6 weeks from injury predicted nonunion with 82% sensitivity and 99% specificity. They concluded that knowledge of fracture motion can help in determining the appropriate management in decision making in nonoperatively treated humeral shaft fractures.
Figures A and B show AP and transthoracic lateral radiographs of a mid diaphyseal spiral humeral shaft fracture, respectively.
Incorrect Answers:
Answers 1 & 2: 2 weeks and 4 weeks would be too early to reliably determine the risk of nonunion.
Answers 4 & 5: 12 weeks and 6 months have not been described as a timeframe for prediction of nonunion of humeral shaft fractures treated nonoperatively.
A patient presents with the injury shown in figures A and B. What has been associated with the technique depicted in figures C and D?
1) Longer operative times
2) Increased deep surgical infection rates
3) Unacceptably high malunion/nonunion rates
4) Slower early return to function
5) Longer hospital stays
Treatment of Shatzker V and VI tibial plateau fractures with hybrid external fixation is associated with increased malunion and nonunion rates.
Hybrid external fixation for treating tibial plateau fractures involves the use of an external fixator to achieve reduction through ligamentotaxis. Additional fracture reduction is achieved through limited open incisions with fixation augmented through percutaneous cannulated screws. Definitive treatment with this technique avoids soft tissue complications that have been associated with traditional open reduction and internal fixation with bicondylar plating.
However, studies have reported high malunion and nonunion rates due to a lack of rigid fixation.
Bertrand et al. performed a prospective cohort study of patients undergoing either open reduction and internal fixation versus hybrid external fixation for Schatzker V and VI tibial plateau fractures. Hybrid external fixation was associated with significantly shorter operative times but insignificantly increased complication rates. They concluded that there were limited statistically differences between these techniques, but further studies are required before advising hybrid external fixation for higher Schatzker tibial plateau fractures.
Gross et al. performed a retrospective study of patients treated with hybrid external fixation for Shatzker V and VI tibial plateau fractures. The authors found there was an 80% union rate, a 70% satisfactory reduction rate, and a 52% rate of malunion. The development of osteoarthritis was associated with plateau widening, articular comminution, articular step-off, and incorrect mechanical alignment. The authors concluded that hybrid external fixation is an effective means for the treatment of tibial plateau fractures that minimizes tissue dissection, with decreased blood loss, and shorter operative times, but associated with a very high malunion rate.
Hall et al. performed a multicenter randomized controlled trial comparing the treatment of Schatzker V and VI fractures with open reduction and internal fixation with hybrid external fixation. Patients with hybrid external fixation had less intraoperative blood loss, fewer unanticipated secondary procedures, slightly faster return to pre-injury activity at 6 months and 1 year, and shorter
hospital stay. They concluded that both hybrid external fixation and open reduction and internal fixation provide effective means for fracture treatment, but hybrid external fixation avoids soft tissue complications with deleterious consequences.
Figure A is an AP radiograph of the right knee with a Schatzker VI tibial plateau fracture. Figure B is an axial CT slice of the articular surface of the tibia with extensive comminution. Figures C and D are the AP and lateral radiographs of the knee with a hybrid external fixation construct for a tibial plateau fracture
Incorrect answers:
Answers 1, 2, 4, and 5: Hybrid external fixation for the treatment of bicondylar tibial plateau fractures is associated with higher malunion and nonunion rates, shorter operative times, increased superficial infection rates, faster earlier return to pre-injury activities, and shorter hospital stay.
An 89-year-old female sustained the injury shown in Figure A and underwent a hemiarthroplasty. Which of the following has been associated with increased rates of post-operative dislocation?
1) Posterior approach
2) Anterior approach
3) Anterolateral approach
4) Use of a bipolar implant
5) Use of a monopolar implant
The incidence of dislocation after hemiarthroplasty is highest when using a posterior approach.
Elderly femoral neck fractures are one of the most common fractures encountered by orthopaedists and will only become more common as the population continues to age. The displacement of the femoral head is associated with delayed union or nonunion, an increased risk of femoral head necrosis due to disrupted blood flow at the femoral neck, and failure of internal fixation devices. For this reason, displaced femoral neck fractures in older patients are often treated with hemiarthroplasty. Three approaches to hemiarthroplasty have been described: a lateral approach, a posterior approach, and an anterior approach. The posterior approach has been used more historically; however, its use has been called into question as it has been associated with increased dislocation rates.
Parker performed a trial on all patients with intracapsular femoral neck fractures being treated with hemiarthroplasty. Patients were randomized to surgery using either a lateral or posterior approach. They found that there were no statistically significant differences observed for any of the outcome measures including mortality, degree of residual pain and regain of walking ability. They concluded that both surgical approaches appear to produce comparable functional outcomes.
van der Sijp et al. performed a meta-analysis to compare the outcomes based on approaches for hemiarthroplasty in the treatment of proximal femur fractures. They found 21 studies and found that the posterior approach poses an increased risk of dislocation and reoperation compared to the lateral approach and anterior approaches. They conclude that there are no evident advantages of the posterior approach and its routine use for fracture-related hemiarthroplasty should be questioned.
Figure A is an AP pelvis radiograph demonstrating a displaced right femoral neck fracture.
Incorrect Answers:
Answers 2, 3, 4, & 5: None of these factors have been associated with an increased risk of dislocation after hemiarthroplasty for a femoral neck fracture.
A 50-year-old male sustained a humeral shaft fracture treated operatively 6 months ago. He denies medical problems but smokes 10 cigarettes per day. His current radiograph is shown in Figure A. He continues to have pain in his arm that is affecting his quality of life. On physical examination, there is motion at the fracture site. C-reactive protein and erythrocyte sedimentation rate are within normal limits. Which is the most appropriate definitive treatment for this fracture?
1) Exchange humeral nailing
2) Augmentative plating
3) Nail removal with open reduction compression plating
4) Smoking cessation and medical optimization
5) Nail removal with open reduction and compression plating with bone grafting
This patient has sustained an atrophic nonunion of a humeral shaft fracture treated with an intramedullary nail. The most appropriate definitive treatment is nail removal with open reduction and compression plating with bone grafting.
Most diaphyseal humeral fractures can be managed non-operatively with functional bracing. Operative treatment is indicated under a number of circumstances including open fractures, associated neurovascular injury, proximal and distal articular extension of the fracture, and in patients with other multiple injuries. Surgical stabilization can be accomplished with different implants and techniques. The two most common are plate and screw fixation and intramedullary nailing. Plate fixation has the advantages of potential absolute stability and sparing the rotator cuff from an incision. Intramedullary nailing has to be inserted proximally with potential damage to the rotator cuff. It, however, can be inserted with small incisions. If a nonunion develops after intramedullary nailing, nail removal and compression plating is the preferred treatment choice.
Heineman et al. performed a metanalysis on plate fixation or intramedullary nailing of humeral shaft fractures. They performed a literature search from 1967-2007 comparing nails and plates in patients with humeral shaft fractures that reported complications due to surgery. They found that the risk of a complication is lower when plating a fracture of the humeral shaft than when using an intramedullary nail.
Gerwin et al. performed an anatomical study to define the course of the radial nerve in the posterior aspect of the arm, with particular reference to its relationship to operative exposures of the posterior aspect of the humeral diaphysis. They found that the radial nerve crosses the posterior aspect of the humerus from an average of 20.7 +/- 1.2 centimeters proximal to the medial epicondyle to 14.2 +/- 0.6 centimeters proximal to the lateral epicondyle. They found the approach to permit the most visualization was the triceps reflecting approach.
Figure A is a lateral radiograph of an atrophic nonunion of a humeral shaft being stabilized with an intramedullary nail.
Incorrect Answers:
Answer 1: Exchange nailing is not a preferred treatment for humeral nonunions.
Answer 2: Augmentative plating may be used for hypertrophic nonunions that require additional stability, but not for an atrophic nonunion.
Answer 3: Bone grafting should be performed in this case to improve the biologic environment to induce fracture healing.
Answer 4: Smoking cessation and medical optimization should be performed however they are not the preferred definitive treatment.
A 45-year-old man is struck while crossing a major highway and sustains the injury depicted in Figure A. Which of the following statements comparing the techniques in Figure B and C is most accurate?
1) Technique depicted in Figure B is associated with an increased risk of septic arthritis
2) Technique depicted in Figure B is associated with increased rate of anterior knee pain
3) Technique depicted in Figure B is associated with improved postoperative fracture alignment
4) Technique depicted in Figure C is associated with an increased risk of septic arthritis
5) Technique depicted in Figure C is associated with improved postoperative fracture alignment
Compared to infrapatellar tibial nailing, suprapatellar tibial nailing is associated with improved postoperative fracture alignment.
While antegrade tibial nailing results in postoperative anterior knee pain in approximately 20% of patients, there is no significant difference in the incidence of anterior knee pain when the conventional infrapatellar approach is compared to suprapatellar approaches. In open tibial shaft fractures, no difference has been observed in the incidence of knee sepsis with either approach. However, several studies have demonstrated that intramedullary nail fixation through a suprapatellar approach is associated with a more accurate entry position and a more accurate fracture reduction when compared with an infrapatellar technique, particularly in more proximal and distal shaft
fractures, without evidence of a functional impact on the patellofemoral joint. Lastly, intraoperative radiography is generally less cumbersome with suprapatellar nailing.
Marecek et al. performed a multicenter comparison study of suprapatellar and infrapatellar approaches and the risk of knee sepsis after treatment of open tibia fractures. They reported no differences in the rates of infection, deep infection, or reoperation between suprapatellar and infrapatellar nailing groups. They concluded that the risk of knee sepsis after suprapatellar nailing of open fractures is low.
Avilucea et al. performed a retrospective cohort study comparing postoperative alignment after suprapatellar versus infrapatellar nailing for distal tibial shaft fractures. They reported a significantly increased rate of primary angular malalignment of greater than 5 degrees in the infrapatellar compared to the suprapatellar nailing cohort. They concluded that in the treatment of distal tibial fractures, suprapatellar nailing results in a significantly lower rate of malalignment compared with the infrapatellar nailing.
Jones et al. performed a study comparing the radiologic outcome and patient-reported function after suprapatellar and infrapatellar intramedullary nailing. They reported no difference in anterior knee pain, however, found a more accurate fracture reduction, both in terms of angulation and translation in the coronal plane, with the use of the suprapatellar technique. They concluded that when compared with infrapatellar nailing, the suprapatellar technique was not associated with more anterior knee pain, yet more accurate nail insertion and fracture reduction.
Figure A depicts a displaced distal third tibial shaft fracture. Figure B depicts the infrapatellar tibial nailing technique. Figure C depicts the suprapatellar tibial nailing technique.
Incorrect Answers:
Answer 1 & 4: No significant difference has been reported in the incidence of knee sepsis with either technique.
Answer 2: No significant difference has been reported in the incidence of anterior knee pain with either technique.
Answer 3: The suprapatellar technique, not the infrapatellar, is associated with more accurate alignment.
A 56-year-old woman sustains the closed injury depicted in Figures A-B. On examination, her wrist is mildly swollen and she is unable to actively oppose her thumb. She also complains of some paresthesias in her thumb and index finger. The patient undergoes closed reduction and splinting; however, her paresthesias worsen significantly in the next 12 hours. What is the likely mechanism of her paresthesias and what is the most appropriate treatment?
1) Nerve compression; open reduction internal fixation with open carpal tunnel release
2) Nerve laceration; open reduction internal fixation with primary nerve repair or grafting
3) Decreased arterial inflow; fasciotomy with open reduction internal fixation
4) Reflex sympathetic dystrophy; vitamin C
5) Nerve compression; repeat closed reduction
This patient is presenting with signs of acute carpal tunnel syndrome (CTS) in the setting of a displaced distal radial fracture. The pathogenesis of acute CTS is nerve compression, requiring urgent open carpal release with open reduction internal fixation (ORIF).
Acute CTS is a well-recognized phenomenon after distal radial fractures. Risk factors include ipsilateral upper extremity fractures, translation of the fracture fragments, and articular distal radius fractures (DRFs). Acute CTS can manifest with paresthesias in the median nerve distribution and opponens pollicis weakness. Acute CTS is an indication for urgent surgical decompression of the median nerve.
Odumala et al. performed a study to evaluate the role of carpal tunnel decompression in the prevention of median nerve dysfunction after buttress plating of DRFs. They reported that prophylactic decompression of the carpal tunnel results in twice the relative odds of developing median nerve dysfunction, which routinely self-resolved. They concluded that prophylactic median nerve decompression does not alter the course of median nerve dysfunction and may actually increase postoperative morbidity.
Medici et al. performed a case-control study to investigate whether carpal tunnel release (CTR) during fixation DRFs improves outcomes. They reported no statistically significant difference between the groups in VAS and Mayo Wrist Scores, however, an increased risk of subsequent CTR in the group who underwent ORIF with no CTR at the index procedure. They concluded that the release of the transverse carpal ligament during ORIF may reduce the incidence of postoperative median nerve dysfunction.
Niver et al. reviewed CTS after DRFs. They reported that acute CTS noted at the time of DRF warrants urgent surgical release of the carpal tunnel and fracture fixation, and that delayed CTS presenting after a distal radius fracture has healed may be managed in the standard fashion for CTR. They concluded that there is no role for prophylactic CTR at the time of distal radius fixation in a patient who is asymptomatic.
Figures A and B depict a displaced apex volar DRF and a mildly displaced ulnar styloid fracture.
Incorrect Answers:
Answer 2: Acute CTS after DRF most often commonly occurs after median nerve compression and contusion, not laceration.
Answer 3: This describes compartment syndrome, which is less likely than acute CTS given the clinical exam described.
Answer 4: Reflex sympathetic dystrophy usually occurs after the acute phase of the DRF.
Answer 5: Acute CTS after DRF requires urgent open carpal tunnel release.
Figures A and B depict the closed injury radiograph of a 79-year-old right-hand-dominant woman who fell on her left wrist. According to meta-analysis and systematic reviews, which of the following statements is most accurate regarding her injury?
1) Improved functional outcomes with open reduction internal fixation (ORIF) through FCR approach vs. closed treatment
2) No difference in radiographic outcomes after ORIF vs. closed treatment
3) No difference in functional outcomes after ORIF vs. closed treatment
4) Improved functional outcomes with closed treatment vs. ORIF
5) Improved functional outcomes with external fixation and K wire fixation vs. ORIF
This elderly patient has sustained a closed intra-articular and shortened distal radial fracture (DRF). Many studies have reported no difference in functional outcomes when patients aged 60 and over are treated in a closed manner versus operatively for unstable fractures.
The treatment of DRFs in the elderly population is controversial. A variety of nonoperative and operative treatments are available, including closed reduction and splinting/casting, K wire stabilization, external fixation, and ORIF. While conservative management of DRFs in the elderly is common,
recent systematic reviews and meta-analyses have demonstrated that despite worse radiographic outcomes after closed treatment of unstable fractures, functional outcomes were no different between patients treated closed versus surgically in patients over the age of 60 years.
Ju et al. published a systematic review and meta-analysis comparing treatment outcomes between nonsurgical and surgical treatment of unstable DRFs in the elderly. They reported no significant differences in DASH score, VAS pain score, grip strength, wrist extension, pronation, supination, and ulnar deviation between the groups. They concluded that operative and nonoperative treatments result in similar outcomes in the treatment of unstable DRFs in the elderly, with no impact on subjective function outcome and quality of life with closed treatment.
Diaz-Garcia et al. published a systematic review of the outcomes and complications after treating unstable DRFs in the elderly, comparing various treatment techniques. They reported significant differences in wrist motion, grip strength, DASH score, although these findings may not be clinically meaningful. They concluded that although the operatively treated group had improved radiographic outcomes, functional outcomes were no different when compared to the group treated in a closed manner.
Figure A depicts an unstable intra-articular and shortened DRF. Incorrect Answers:
Answers 1, 4 & 5: Systematic reviews and meta-analyses have demonstrated
no difference in functional outcomes between operative and closed treatment modalities for DRF.
Answer 2: Systematic reviews and meta-analyses have demonstrated superior radiographic outcomes after surgical treatment when compared to closed treatment.
An active 60-year-old woman falls from her attic and presents with the injury in Figure A. She undergoes successful closed reduction and sling immobilization. At follow up, she is unable to move her shoulder. New radiographs are depicted in Figures B and C. What is the next best step?
1) Continued sling immobilization
2) Closed reduction percutaneous pinning
3) Open reduction internal fixation
4) Hemiarthroplasty
5) Reverse total shoulder arthroplasty
This active patient presents with a greater tuberosity fracture dislocation. Open reduction internal fixation (ORIF) is indicated, particularly when the greater tuberosity fragment is displaced greater than 5mm.
Many proximal humerus fractures are minimally displaced and respond acceptably to nonoperative management. Isolated greater tuberosity fractures or rotator cuff injuries are associated with shoulder dislocations in the elderly population. The greater tuberosity fragment undergoes deforming forces by the supraspinatus and infraspinatus muscles. In active patients, it is well-accepted that greater tuberosity fracture displacement greater than 5mm is an indication for ORIF to restore their ability to perform overhead activities and prevent impingement.
Schumaier et al. published a review article on the treatment of proximal humerus fractures in the elderly. They highlighted that while bone density was a predictor of reduction quality, social independence was a better predictor of outcome. They concluded that although the majority of minimally displaced fractures can be treated successfully with early physical therapy, treatment for displaced fractures should consider the patient's level of independence, bone quality, and surgical risk factors. They emphasized that there was no clear evidence-based treatment of choice, and the surgeon should consider their comfort level during their decision-making.
George et al. published a review article on greater tuberosity humerus fractures. They reported that these fractures may occur in the setting of anterior shoulder dislocations or impaction injuries against the acromion or superior glenoid, with surgical fixation recommended for fractures with greater than 5 mm of displacement in the general population or greater than 3 mm of displacement in active patients involved in frequent overhead activity. They recommended close followup and supervised rehabilitation to increase successful outcomes.
Figure A depicts a greater tuberosity fracture dislocation of the left shoulder. Figures B and C depict reduction of the glenohumeral joint with residual displacement of the greater tuberosity. Illustrations A and B depict radiographs after ORIF.
Incorrect Answers:
Answer 1: While most proximal humerus fractures can be treated nonoperatively, greater tuberosity fractures displaced 5 mm or greater should be treated with ORIF.
Answer 2: ORIF allows for anatomical realignment, reducing the possibility of impingement and weakness from greater tuberosity malunion.
Answer 4 & 5: Hemiarthroplasty and reverse total shoulder arthroplasty would be indicated in some 4-part proximal humerus fractures in active elderly patients.
A 21-year-old football player is tackled as he falls onto an outstretched arm. He sustains the injury shown in Figure A. He undergoes successful operative treatment of his injury. In which order did his injury occur?
1) MCL > LCL > anterior capsule
2) MCL > anterior capsule > LCL
3) anterior capsule > MCL > LCL
4) LCL > anterior capsule > MCL
5) LCL > MCL > anterior capsule
The patient sustained a terrible triad injury of the elbow, which progresses from the LCL to the anterior capsule and then the MCL.
Terrible triad injuries of the elbow are traumatic injuries that occur after a fall on an extended arm that results in a combination of valgus, axial, and posterolateral rotatory forces. The key features of a terrible triad injury include a radial head fracture, a coronoid fracture, and an elbow dislocation. Disruption of the structures in the elbow characteristically occurs from lateral to medial, affecting the LCL first, followed by the anterior capsule and MCL. Outcomes following terrible triad injuries have historically been poor; however, more recent literature has shown that good outcomes can be achieved with surgical stabilization of the elbow followed by an early rehabilitation protocol. Some authors use temporary immobilization, but range-of-motion exercises are typically initiated by 48 hours postoperatively. Active range of motion is particularly important, as it recruits muscles that act as dynamic stabilizers of the elbow. Depending on the injury, method of fixation, and stability that is achieved, the range of motion may be limited to 30° of extension during the early postoperative period but should allow full flexion.
Giannicola et al. (2013) performed a study to determine the critical time period for recovery of functional range of motion after surgical treatment of complex elbow instability (CEI). They found that the first 6 months after surgery represent the critical rehabilitation period to obtain a functional elbow and that elbow flexion recovered at a rate slower than that of the other elbow movements. They recommend that, following CEI surgical treatment, a rehabilitation program should be started promptly and should be continued for at least 6 months because a significant improvement of ROM occurs in this period.
Giannicola et al. (2015) performed a study analyzing the predictability of outcomes of terrible triad injuries (TTI) treated according to current diagnostic and surgical protocols. They found that the current diagnostic and therapeutic protocols allow for satisfactory clinical outcomes in a majority of cases but a high number of major and minor unpredictable complications still persist. Low compliance, obesity, and extensive soft elbow tissue damage caused by high-energy trauma represented negative prognostic factors unrelated to surgery.
McKee et al. performed a review on their standard surgical protocol for the treatment of elbow dislocations with radial head and coronoid fractures. Their surgical protocol included fixation or replacement of the radial head; fixation of the coronoid fracture, if possible; repair of associated capsular and lateral ligamentous injuries; and, in selected cases, repair of the medial collateral ligament and/or adjuvant-hinged external fixation. They found that their surgical protocol restored sufficient elbow stability to allow early motion postoperatively, enhancing the functional outcome. They recommend early operative repair with a standard protocol for these injuries.
Figure A is a lateral radiograph of the elbow demonstrating a terrible triad injury with a comminuted radial head/neck fracture, displaced coronoid fracture, and posterior elbow dislocation. Illustration A is a rendered image of the radiograph shown in Figure A with the components labeled.
Incorrect Answers:
Answers 1, 2, 3, and 5: Terrible triad injuries occur from the LCL to the anterior capsule and then the MCL.
An 82-year-old female sustains the fracture shown in Figure A as the result of a ground level fall. Which of the following has been shown to be a reliable predictor of postoperative lateral wall fracture for this injury after treatment with a sliding hip screw?
1) Reverse obliquity fracture pattern
2) Lateral wall thickness
3) Previous contralateral hip fracture
4) DEXA T-score
5) Calcar comminution
Lateral wall thickness has been shown to be a predictor of postoperative lateral wall fracture. As the lateral wall thickness decreases, there is an increased chance of fracture.
Lateral wall fracture creates an unstable fracture pattern and increased screw sliding/collapse. This shortens the neck and abductors, leading to worse patient outcomes (radiographic and clinical). Recognition of a thin wall should lead toward the use of an intramedullary device or adjunct use of a trochanteric stabilizing plate with a sliding hip screw device.
Baumgaertner et al. reported that the failure of peritrochanteric fractures that have been treated with a fixed-angle sliding hip-screw device is frequently related to the position of the lag screw in the femoral head. They established the tip-apex distance as the sum of the distance from the tip of the lag screw to the apex of the femoral head on an anteroposterior radiograph and this distance on a lateral radiograph, after controlling for magnification. Upon reviewing their series, none of the 120 screws with a tip-apex distance of twenty-five millimeters or less cut out, but there was a very strong statistical relationship between an increasing tip-apex distance and the rate of cutout, regardless of all other variables related to the fracture.
Socci et al. performed a literature review of relevant papers and appropriate clinical databases and concluded that fixation of AO 31A1 fractures was best achieved with a sliding hip screw device and that all other types of intertrochanteric hip fractures be fixed with an intramedullary device.
Utrilla et al. reported no difference in outcome in stable fractures, but better mobility at one year following intramedullary fixation of unstable fractures.
Hsu et al. measured the thickness of the lateral wall of patients with AO/OTA 31-A1 and 31-A2 type intertrochanteric hip fractures. They found that the lateral wall thickness was a reliable predictor of postoperative lateral wall fracture for unstable AO Type A2 fractures and concluded that the lateral wall thickness threshold value for risk of developing a secondary lateral wall fracture was found to be 20.5 mm.
Figure A shows a standard obliquity intertrochanteric hip fracture.
Illustration A from the Hsu article demonstrates the measurement of the lateral wall thickness. The distance is measured along a 135-degree angle, between a point 3cm distal to the innominate tubercle of the greater trochanter and the fracture line (midway between the two cortical lines).
Incorrect Answers:
Answer 1: This pattern is unstable and requires treatment with an intramedullary nail as opposed to a sliding hip screw.
Answer 3: There has been no proven association with this factor. Answer 4: There has been no proven association with this factor.
Answer 5: Fracture comminution is not associated unless the lateral wall is already fractured or comminuted itself.
A 78-year-old patient presents with right hip pain and inability to bear weight after an unwitnessed fall at a nursing home. Figures A and B are the radiographs of the hip and pelvis. Which statement is true regarding the treatment of these injuries?
1) Smaller lateral wall thickness favors sliding hip screw constructs
2) Unstable fractures are best treated with sliding hip screw constructs
3) Avoiding distal locking screws in intramedullary implants protects against refracture
4) Stable fractures have no differences in outcomes between sliding hip screws and intramedullary implants
5) Implant stability has a greater impact on outcomes rather than reduction quality
Studies have shown that in stable intertrochanteric femur fractures there are no differences in outcomes between sliding hip screws and intramedullary implants.
Intertrochanteric femur fractures are one of the most common fractures in the geriatric population. Implant selection has been a great topic of research with most studies reporting minimal to no differences in outcomes between intramedullary and sliding hip screw constructs in stable fracture patterns.
Unstable fractures, however, are reportedly better treated with a distally locked intramedullary implant. The quality of fracture reduction has a greater impact on the overall outcome than implant selection.
Hsu et al. performed a retrospective study of risk factors for postoperative lateral wall fractures in patients treated with sliding hip screws for intertrochanteric femur fractures. They found that fracture classification and lateral wall thickness, which is measured from 3 cm distal from innominate tubercle and angled 135 degrees to the fracture line, were associated with postoperative lateral wall fracture. They recommended not treating intertrochanteric femur fractures with sliding hip screws if the lateral wall thickness is less than 20.5 mm.
Socci et al. reviewed the literature regarding the treatment of intertrochanteric femur fractures. Based on the literature, they recommend treatment of AO/OTA type 31A1 fractures with sliding hip screws, type 31A2 fractures with short intramedullary implants, and 31A3 fractures with long intramedullary implants. Simple basicervical fractures of the femoral neck can be treated with sliding hip constructs whereas comminuted fractures treated with intramedullary devices due to the inherent instability of the pattern. The most import aspect in fracture healing is the quality of the reduction rather than the choice of implant.
Lindvall et al. performed a retrospective study of refracture rates in patients treated with either long or short cephalomedullary nails. The authors found a 97% union rate with both implant types and refracture not associated with either long or short implants. Rather, refracture was associated with the lack of a distal locking screw. The authors recommended locking intramedullary implants to avoid refracture.
Utrilla et al. performed a randomized control trial of elderly patients treated
with compression hip screw or Trochanteric Gamma Nail for intertrochanteric femur fractures. They reported the only differences between the two implants were quicker operating time, less fluoroscopy use, and better walking with unstable fractures treated with intramedullary implants. The authors recommended either construct for stable fractures, but intramedullary implants for unstable fractures.
Figures A and B are the AP and lateral radiographs of the right hip radiographs demonstrating a simple and minimally displaced intertrochanteric femur fracture, classified as an AO/OTA 31A1 fracture. Illustration A depicts the AO/OTA classification system for proximal femur fractures.
Incorrect answers:
Answer 1: Thinner lateral wall thickness in intertrochanteric femur fractures favors the use of an intramedullary implant due to the risk of lateral wall fracture.
Answer 2: Unstable intertrochanteric femur fractures are best treated with intramedullary implants.
Answer 3: The lack of distal locking screws has been shown to increase the risk of refracture.
Answer 5: Reduction quality has been shown in several studies to have a greater impact on outcomes rather than implant selection.
A 28-year-old male that sustained a closed left femoral shaft fracture 12 months ago and underwent intramedullary nailing presents with persistent pain in the right thigh. The patient walks with an antalgic gait. He denies any fevers or chills. His surgical sites are well healed and there are no signs of drainage. Serum ESR and CRP are 12 mm/hr (reference
1) Nail removal with compression plating and open bone grafting
2) Closed reamed exchange nailing
3) Nail dynamization
4) Nail retention with plate augmentation and bone grafting
5) Electrical bone stimulator
The patient is presenting with a hypertrophic nonunion of the femur below the isthmus, which studies have shown to have a higher union rate when treated with plate augmentation. Retention of the nail allows for full weight-bearing postop.
Hypertrophic nonunion of the femur is the result of fracture site hypermobility with sufficient biology for healing. This is demonstrated with abundant callus formation without bridging trabeculae. Traditionally, this is treated with closed reamed exchange nailing which increased construct stiffness with a larger diameter nail, improved isthmic fit, and extrusion of reaming contents to the nonunion site. However, studies have demonstrated a higher union rate with open plate augmentation, bone grafting, and nail retention. This is due to the ability to correct nonunion site deformity, provide added compression at the nonunion site, and increase fracture site biology with bone graft.
Lynch et al. reviewed the literature regarding the treatment options for femoral nonunions. The literature suggests high union rates when hypertrophic nonunions are treated with exchanged reamed nailing. However, the use of augmentative plate fixation allows for further deformity correction. The proposed mechanism by which exchange reamed nailing is increased construct stiffness with a large diameter nail, usually by 1-2 mm, increased isthmic fit, and autogenous bone graft extrusion into the nonunion site.
Somford et al. performed a systematic review of the surgical treatment of femoral nonunions. Results demonstrate that exchange nailing provides a 73% union rate compared to plate augmentation of 96%. They speculated that there were increased indications for exchange nailing for oligotrophic nonunions in many of the included studies, which may have reduced the union rate. Further, plate augmentation does allow for deformity correction, which can further improve the union rate.
Figures A and B are the AP and lateral radiographs of the femur with hypertrophic nonunion as suggested with the abundant callus formation and broken distal interlock screws. Illustration A and B are the AP and lateral radiographs of the distal femur subsequent plate augmentation and fracture healing.
Incorrect Answers:
Answer 1: Compression plating and bone grafting provide deformity correction across the nonunion site and added biology, but there is loss of weight-bearing benefits with nail removal.
Answer 2: Closed reamed exchange nailing can provide healing of the nonunion by increasing the nail diameter and improving the isthmic fit, but studies have shown a lower union rate in subisthmic femoral nonunions compared to augmentation plating.
Answer 3: Nail dynamization provides the benefit of weight-bearing forces across the nonunion site to enhance the differentiation of osteoblasts and promote fracture healing. In hypertrophic nonunions, fracture site stability is the cause of nonunion rather than the lack of fracture site biology.
Answer 5: Electrical bone stimulators do not provide the added fracture stability that is required to address hypertrophic nonunion.
A 25-year-old male sustains the injury depicted in Figure A. He is splinted in the field, but on arrival to the emergency room, he complains of painful "tightness" around the leg and severe uncontrolled pain despite maximum dose narcotics. His pain is exacerbated when the toes and ankle are passively stretched in flexion and extension. What is the most appropriate next step in treatment?
1) External fixation with serial doppler examinations
2) Intramedullary nailing
3) Open reduction internal fixation using plates and screws
4) Immediate 2-compartment fasciotomies and external fixation
5) Immediate 4-compartment fasciotomies and external fixation
This patient has clinical symptoms and signs of leg compartment syndrome and should undergo immediate fasciotomies of all 4 leg compartments, followed by external fixation for fracture stabilization.
Tibial fractures are among the most common reasons for compartment syndromes of the leg. A clinical assessment is key in the diagnosis of acute compartment syndrome. If there is uncertainty, intracompartmental pressure measurement has been advocated to help confirm the diagnosis. An absolute
compartment pressure >30 mm Hg or a difference in diastolic pressure and compartment pressure (delta p)
A 24-year-old male is brought to the ED after an MVC. He is found to have a closed comminuted segmental fibula fracture after a prolonged extraction from the vehicle. Several hours after arrival, the patient reports increasing pain and is noted to have an exacerbation of his pain with passive stretching of the ankle. He has a heart rate of 103 and a blood pressure of 141/87. Compartment pressures are obtained and are 27 mmHg in the anterior compartment, 47 mmHg in the lateral compartment, 28 mmHg in the superficial posterior compartment, and 27 mmHg in the deep posterior compartment. Which of the following correctly describes the initial pathophysiology of compartment syndrome and the neurologic deficit that would likely occur in this patient if left untreated?
1) Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the first webspace
2) Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
3) Decreased arterial inflow; inability to dorsiflex his ankle
4) Decreased venous outflow; decreased sensation on the dorsum of his foot involving the first webspace
5) Decreased venous outflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Compartment syndrome initially results from a decrease in venous outflow relative to arterial inflow. This patient has elevated pressures in the lateral compartment of the leg, which is where the superficial peroneal nerve runs to supply sensation to the dorsum of the foot including the hallux and 3rd and 4th toes.
Compartment syndrome results from compromised venous outflow from the leg relative to the arterial inflow. This venous congestion leads to elevated compartment pressures that ultimately lead to compromised arterial inflow without compartment release. There are 4 compartments in the leg: anterior, lateral, superficial posterior, and deep posterior. The anterior compartment contains the deep peroneal nerve, the lateral compartment of the leg contains the superficial peroneal nerve, and the deep posterior compartment contains the tibial nerve.
McQueen et al. performed a study to determine risk factors for acute compartment syndrome. They found that young patients, especially men, were most at risk of acute compartment syndrome after injury. They recommend that, when treating such injured patients, the diagnosis should be made early, utilizing measurements of tissue pressure.
Olson et al. published a review on acute compartment syndrome in lower extremity musculoskeletal trauma. They reported that acute compartment syndrome is a potentially devastating condition in which the pressure within an osseofascial compartment rises to a level that decreases the perfusion gradient across tissue capillary beds, leading to cellular anoxia, muscle ischemia, and death. They report that recognizing compartment syndromes requires having and maintaining a high index of suspicion, performing serial examinations in patients at risk, and carefully documenting changes over time.
Illustration A is a diagram depicting the compartments of the leg and its contents.
Incorrect Answers:
Answers 1, 2, 3, and 4: Compartment syndrome initially results from a decrease in venous outflow relative to arterial inflow. The superficial peroneal nerve runs in the lateral compartment and provides sensation to the dorsum of the foot including the hallux and 3rd and 4th toes.
Which of the following amputations results in an approximate 40% increase in energy expenditure for ambulation?
1) Syme
2) Traumatic transtibial
3) Vascular transtibial
4) Traumatic transfemoral
5) Vascular transfemoral
The energy expenditure of a vascular transtibial amputation is approximately 40% greater.
The energy expenditure for ambulation increases with lower extremity amputation. Diabetics and vasculopathic patients who undergo amputation
have significantly increased energy requirements compared with nondiabetic patients undergoing amputations for trauma. The metabolic cost for a vascular transtibial amputation is 40% compared to a 25% increase in normal patients who sustain a traumatic amputation.
Huang et al. used a mobile instrument system to measure energy consumption by indirect calorimetry at rest and during ambulation in 25 unimpaired subjects, 6 unilateral below-knee (BK) amputee patients, 6 unilateral above-knee (AK) amputee patients and 4 bilateral AK amputee patients. They found that in comparison to unimpaired subjects, the mean oxygen consumption was 9% higher in unilateral BK amputee patients, 49% higher in unilateral AK amputee patients and 280% higher in bilateral AK amputee patients.
Pinzur et al. performed a study to measure cardiac function and oxygen consumption in 25 patients who underwent amputation for peripheral vascular disease (PVD), and in five similarly aged control patients without PVD. They found Normal walking speed and cadence decreased and oxygen consumption per meter walked increased with more proximal amputation. They conclude that peripheral vascular insufficiency amputees function at a level approaching their maximum functional capacity and more proximal amputation levels, the capacity to walk short or long distances is greatly impaired.
Incorrect Answers:
Answer 1: A Syme amputation increases energy expenditure by 15%.
Answer 2: A traumatic transtibial amputation increases energy expenditure by 25%.
Answer 4: A traumatic transfemoral amputation increases energy expenditure by 68%.
Answer 5: A vascular transfemoral amputation increases energy expenditure by 100%.
A 25-year-old man sustains the injury shown in Figures A-C. What is the primary advantage of using a trochanteric flip osteotomy (TFO) in treating this injury?
1) It may be performed in a minimally invasive manner
2) It involves minimal soft tissue stripping
3) It leads to higher union rates
4) It allows the surgeon to address all sites of injury through one approach
5) Answers 1 and 2
This patient has sustained a right hip fracture-dislocation with fractures of the femoral head and posterior wall. The TFO allows the surgeon to address all sites of injury through a single approach.
Femoral head fracture-dislocations are a result of high-energy trauma. Treatment ranges from closed reduction and conservative management to total hip arthroplasty. Intermediate options include open reduction and internal fixation or excision of fracture fragments. Complications of this injury include post-traumatic hip arthritis, avascular necrosis, and heterotopic ossification.
The injury is further complicated when a fracture of the acetabulum is concomitantly present. There has been no consensus treatment on this injury constellation as it presents quite rarely. The TFO is one approach that allows the surgeon to treat and stabilize both injuries concurrently. It should be noted that a surgical hip dislocation is performed in conjunction with the TFO to allow access to the femoral head.
Solberg et al. performed a retrospective study of patients sustaining Pipkin IV fracture/dislocations with a TFO. They had 12 patients over a 6 month period. They found that all patients healed radiologically and one patient developed osteonecrosis. 10 out of 12 patients had good to excellent outcomes. They concluded that using a surgical protocol with TFO rendered clinical results
comparable to previously reported outcomes in a series of isolated femoral head fractures.
Giannoudis et al. performed a systematic review to investigate data regarding femoral head fractures, particularly focusing on their management, complications and clinical results. They reported that fracture-dislocations were managed with emergent closed reduction, followed by definite treatment, aiming at an anatomic restoration of both fracture and joint incongruity. They concluded that neither the TFO nor an anterior approach seems to endanger femoral head blood supply compared to the posterior one, with the TFO possibly providing better long-term functional results and lower incidence of major complication rates.
Henle et al. reported on the result of 12 patients of femoral head fractures with associated posterior wall fractures treated with a TFO. They found good to excellent results in 10 patients. The two patients with poor outcome developed avascular necrosis of the femoral head and underwent total hip arthroplasty.
Heterotopic ossification was seen in five patients. They concluded that the TFO may lead to favorable outcomes in this injury constellation.
Figure A is an AP radiograph of the right hip demonstrating a femoral head fracture-dislocation. Figure B is an axial CT image demonstrating a posterior wall fracture. Figure C is an axial CT image demonstrating a femoral head fragment within the acetabulum. Illustration A is the Pipkin classification of femoral head fractures: Type I is below the fovea, Type II is above the fovea, Type III is associated with a femoral neck fracture, and Type IV is associated with an acetabular fracture.
Incorrect Answers:
Answers 1, 2, & 5: The TFO is not a minimally invasive approach.
Answer 3: There is no evidence that shows that this approach leads to higher union rates of this injury
A 30-year-old male is brought to your emergency department following a motor vehicle collision at high speed. He is intubated in the field for airway protection but is hemodynamically stable. Subsequent workup shows a displaced acetabular fracture, in addition to an intracranial bleed and liver laceration which do not require surgery. When placing an antegrade anterior column screw, what radiographic view should be used to avoid intra-pelvic screw penetration?
1) Iliac oblique view with hip and knee flexed
2) Iliac oblique inlet view
3) Obturator oblique view with hip and knee flexed
4) Obturator oblique outlet view
5) Obturator oblique inlet view
The iliac oblique inlet view will best show the the anterior-posterior placement of an anterior column ramus screw.
Percutaneous and limited-open acetabular fixation is becoming increasingly common as it avoids the morbidity of extensile pelvic dissection and allows early mobilization. However, it relies heavily on a mastery of radiographic landmarks and ability to interpret these images to reduce fracture fragments without direct visualization. Slight deviations of the fluoroscopy beam and/or fracture displacement will distort the radiographic image. Without a facile ability to interpret these and make appropriate adjustments, percutaneous fixation will be extremely onerous.
Starr et al. described their early techniques for percutaneous and limited-open acetabular fixation. They first implemented this for minimally displaced fracture patterns but have expanded these to a wider range of pathology. They cite the benefit of earlier mobilization in the poly-traumatized patient as great use for this technique.
Mauffrey et al. reviewed radiograph utilization during acetabular fracture care. Though CT has added tremendously to demonstrating subtleties of acetabular fractures, they state the use of AP and orthogonal iliac and obturator oblique Judet views cannot be overlooked. Interpreting these radiographs allows the surgeon to recreate 2-dimensional images into a 3-dimensional fracture pattern and better understand the character of the injury.
Illustrations A and B demonstrate the iliac oblique inlet view and obturator oblique outlet views, respectively.
Illustration C demonstrates the relationship of the critical structures at risk of injury during anterior column screw placement. Illustrations D and E show the starting point with screw trajectory, and position of the hip during posterior column screw.
Incorrect Answers:
Answers 1 and 3- These would be utilized when placing a posterior column screw.
Answer 4- This view would show the supra-acetabular corridor with help with the starting point for external fixator placement.
Answer 5- This shows the inner and outer tables of the iliac wing and confirms pins have not violated the cortex.
A 34-year-old male sustains the injury shown in Figures A and B. Which factor has been found to be elevated in the synovial fluid and contributes to post-traumatic arthritis?
1) TGF-Beta
2) RANKL
3) IL-2
4) IL-6
5) cAMP
The patient has sustained a tibial plafond or pilon fracture as depicted in Figures A and B. IL-6 is one of many inflammatory molecules that has been found to be elevated in the synovial fluid following an intra-articular ankle fracture.
Post-traumatic arthritis following intra-articular fractures is a known complication. It commonly appears 1-2 years following injury and is related to chondrocyte death at the margins. There has not been shown to be any association between prolonged non-weight bearing, poor patient compliance with weight-bearing restrictions, and hardware reactions with the development of post-traumatic arthritis. However, literature has shown that the inflammatory molecules present in the synovial fluid can have a significant effect on the development of posttraumatic arthritis. Important inflammatory factors that have been found to be elevated include IL-6, IL-8, MMP-1, MMP-2, MMP-3, MMP-9 and MMP-10.
Adams et al. looked at the synovial fluid of 21 patients with an intra-articular ankle fracture and used the un-injured ankle as a control. They found the inflammatory molecules of GM-CSF, IL-10, IL-1 beta, IL-6, IL-8, IL-10, IL-12p70, TNF-alpha, MMP-1, MMP-2, MMP-3, MMP-9, MMP-10 were all elevated. They concluded that these inflammatory molecules may play a role in posttraumatic arthritis development.
Adams et al. looked at the synovial fluid of 7 patients from his previous 21 patients that had intra-articular ankle fractures. They found that IL-6, IL-8, MMP-1, MMP-2, and MMP-3 were significantly elevated in comparison to the uninjured ankle. They concluded that the sustained elevated intra-articular inflammatory environment is a potential contributor to post-traumatic arthritis.
Figures A and B are sagittal and axial CT slices, respectively, that depict a tibial plafond or pilon fracture.
Incorrect Answers:
Answer 1: TGF-Beta has not been shown to be elevated in the synovial fluid and contribute to post-traumatic arthritis. However, TGF-Beta has been shown to be a factor in the inflammatory cycle, immune system signaling and bone signaling (inhibits osteoclasts via osteoprotegrin).
Answer 2: RANKL has not been shown to be elevated in the synovial fluid and contribute to post-traumatic arthritis. RANKL is an important part of bone signaling and metabolism.
Answer 3: IL-2 has not been shown to be elevated in the synovial fluid and contribute to post-traumatic arthritis. IL-2 has important functions within the
immune system.
Answer 5: cAMP has not been shown to be elevated in the synovial fluid and contribute to post-traumatic arthritis. cAMP is an intra-cellular signaling molecule.
A 29-year-old female presents to the trauma bay from the scene of a high-speed motor vehicle accident. She is found to have a closed intraarticular distal radius fracture with a concomitant ulnar styloid base fracture. She subsequently undergoes ORIF of the distal radius fracture with a volar locking plate. The ulnar styloid fracture is not addressed. Which of the following, if present, is least likely to affect functional outcomes?
1) Ulnar styloid nonunion
2) DRUJ instability
3) Articular step-off >3mm
4) Radial shortening
5) Workers compensation claim
Ulnar styloid non-unions do not affect the overall outcome of hand or wrist function following ORIF of distal radius fractures.
Ulnar styloid base fractures can be associated with DRUJ disruption and TFCC rupture. The DRUJ should be independently evaluated following ORIF of the distal radius. Without instability, unlar styloid fractures do not need to be addressed. If instability exists, the DRUJ should be treated as a separate entity, typically cross-pinned using k-wires. The result of ulnar styloid nonunions are inconsequential to the overall outcome of patients undergoing distal radius ORIF.
Daneshvar et al review the effects of ulnar styloid fractures on patients sustaining distal radius fractures. They report that patients with a concomitant ulnar styloid fracture had a slower recovery of wrist flexion and grip strength compared to those with an isolated distal radius fracture. They conclude, however, that even the presence of an ulnar styloid nonunion did not significantly affect outcomes.
Buijze et al review the clinical impact of united versus non-united fractures of the proximal half of the ulnar styloid following volar plate fixation of the distal radius. They report no difference in motion, strength or outcome scores
between the united and non-united groups at 6 months follow up. They conclude that nonunion of the ulnar styloid does not have an effect on the overall outcome of hand or wrist function.
Incorrect Answers:
Answer 2: Unrecognized DRUJ instability leads to decreased pronosupination and posttraumatic arthritis.
Answer 3: With 1-2mm of articular step-off 90% of young adults will develop radioulnar arthrosis
Answer 4: Radial shortening is one of the most important factors for predicting poor functional outcomes following distal radius ORIF.
Answer 5: Workers compensation claims negative impact functional outcomes following fixation of distal radius fractures.
Which of the following proximal humerus fractures has the highest likelihood of developing humeral head ischemia?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Posteromedial calcar length of the humeral head less than 8 mm and a loss of medial hinge are among the most reliable predictors of ischemia in the surgical management of humeral head fractures.
Proximal humerus fractures are classified based on the Neer classification, in which 4 parts are described: greater tuberosity, lesser tuberosity, articular surface, and the shaft. A fragment is considered a part if it is greater than 45 degrees angulated or displaced >1cm. The posterior humeral circumflex artery is the main blood supply to the humeral head. Following ORIF, humeral head ischemia may occur and is associated with the initial fracture pattern. Several factors including 10mm and angulation >45 degrees have been associated with a disruption of the vascular supply to the humeral head.
Campochiaro et al review Hertel’s criteria of calcar length and medial hinge integrity and its reliability in predicting humeral head necrosis. They reported a 3.7% incidence of ischemia across all 267 fractures evaluated. In those patients that developed AVN, 30% had all of the predictors described by Hertel, however, in the non-AVN group, only 4.7% had these same findings.
They concluded that while Hertel’s criteria are helpful, they may not be sufficient and the authors recommended 3-dimensional evaluation of any fracture involving the calcar.
Xu et al reviewed avascular necrosis in patients with proximal humerus fractures who were treated surgically. They reported on 291 patients throughout 7 studies in which there was no difference in the incidence of AVN for those treated surgically or nonoperatively. However, they concluded through subgroup analysis looking at different fixation constructs that, plate fixation specifically was associated with a higher risk of AVN than conservative management of proximal humerus fractures.
Figure A demonstrates a proximal humerus fracture with a medial calcar length of >8mm attached to the articular segment. Figure B is a proximal humerus fracture with a displaced greater tuberosity fragment. Figure C demonstrates a proximal humerus fracture with a medial calcar length of 8mm.
Incorrect Answers:
Answer 1, 2, 5: These fracture patterns do not have the prognostic characteristics described by Hertel for humeral head ischemia: articular segment calcar length 10mm or angulation >45 degrees.
Answer 4: Humeral head ischemia is very rare following pediatric proximal humerus fractures.
A 34-year-old man presents with the closed injury depicted in Figure A after a high energy twisting injury. Which of the other injuries below is most commonly associated with his known injury?
1) Nondisplaced medial malleolus vertical shear fracture
2) Nondisplaced Volkmann's fragment
3) Nondisplaced Chaput's fragment
4) Nondisplaced lateral wall talar fracture
5) Posterior inferior tibiofibular ligament disruption
This patient has sustained a distal third tibial shaft spiral fracture, which is commonly associated with nondisplaced posterior tibial plafond fractures, with the classic Volkmann's fragment.
Prior to operative management, distal third spiral tibial shaft fractures should always be evaluated for intra-articular extension. As this commonly associated injury can be missed on plain radiographs, an ankle CT is often recommended. This is especially important when intramedullary fixation is used for definitive management of the tibial shaft fracture, as nail insertion can displace a
previously nondisplaced intraarticular fracture. Anterior to posterior lag screw fixation prior to nailing may be useful in these cases.
Sobol et al. investigated the incidence of concomitant posterior malleolar fractures (PMFs) in operative distal third spiral tibial shaft fractures. They reported that spiral distal third tibial shaft fractures were identified with an ipsilateral posterior malleolus fracture in 92.3% of cases. They recommended a preoperative ankle CT in all cases with this specific fracture morphology to properly diagnose this commonly associated injury.
Hou et al. investigated the posterior malleolar fracture association with spiral tibial shaft fractures. They reported that plain radiography (both preoperative and intraoperative) resulted in rare identification of these associated injuries, which resulted in missed injuries. They concluded that a CT or MRI ankle may be a higher yield method to detect these injuries.
Figure A demonstrates a distal third spiral tibial shaft fracture. Illustration A is a schematic demonstrating the Volkmann, Chaput, and medial malleoli intraarticular fragments of the distal tibia.
Incorrect Answers:
Answer 1: Medial malleolar vertical shear fractures are not typically associated with distal third tibial shaft fractures.
Answer 3: Nondisplaced anterior tibial plafond fractures (Chaput's fragment) are not as highly associated with spiral distal third tibial shaft fractures.
Answer 4: Nondisplaced lateral wall talar fractures are not associated with spiral distal third tibial shaft fractures.
Answer 5: The PITFL is typically intact with posterior malleoli fractures.
An 18-year-old male is admitted for a diaphyseal, open, tibial shaft fracture after falling off a motorcycle. He has a past medical history of nicotine dependence and obesity. He undergoes provisional splinting by the resident on call and is noted to be "neurovascularly intact" following splint placement. Throughout the evening, however, the patient has an increasing narcotic requirement and develops pain with passive stretch of his toes. What factor listed below is most associated with his progressive symptoms overnight?
1) Age
2) Male gender
3) Body mass index >/ 30 kg/m^2
4) Open fracture
5) Nicotine use
The highest prevalence of compartment syndrome is found in patients aged 12-19 years, followed by 20-29 years.
One theory for the higher prevalence of compartment syndrome in younger patients is increased muscle mass in this cohort. If there is more muscle in a compartment, there is less room for swelling. On the flip side, elderly or deconditioned patients who have less muscle or fatty atrophy may be better able to accommodate muscle swelling. Additionally, a diaphyseal fracture location is associated with a higher risk of compartment syndrome. Again, this may be due to the fact that there is more muscle than tendon, and thus more swelling, in the proximal leg.
Shadgan et al. retrospectively reviewed 1,125 patients with diaphyseal tibia fractures to look for risk factors associated with the development of compartment syndrome. Compartment syndrome occurred in approximately 8% of patients with this injury. They concluded that younger patients were at a higher risk of developing compartment syndrome and that male gender, open fracture, and intramedullary nailing were not risk factors.
Beebe et al. set out to determine the correlation between the OTA/AO classification of tibia fractures and the development of compartment syndrome. they conducted a retrospective review of a prospectively collected database comprising 2,885 fractures. They concluded that age, sex, and the OTA/AO classification were highly predictive for the development of compartment syndrome in this cohort.
McQueen et al. similarly looked at predictors of compartment syndrome after tibial fractures in a retrospective cohort study. There were 1,388 patients in their study with ages ranging from 12-98; identical to the Shadgan study, 69% of patients were male. They concluded the strongest risk factor was age, with the highest prevalence in 12 to 19-year-olds.
Park et al. additionally analyzed 414 patients with tibia fractures in a retrospective cohort study. The main outcome measure of this study was the rate of clinically determined compartment syndromes requiring fasciotomy by anatomic region. The found that diaphyseal fractures were more frequently associated with the development of compartment syndrome than proximal (next most common site) and distal tibia fractures, specifically in younger patients.
Incorrect Answers:
Answers 2-5: Gender, body mass index, open fracture, and nicotine use are not associated with a higher risk for the development of a compartment syndrome.
Figure A is the radiograph of a 79-year-old female with elbow pain following a fall. Compared with a total elbow artrhoplasty, open reduction and internal fixation would most likely result in?
1) Greater Mayo Elbow Performance Score
2) Greater Disabilities of the Arm, Shoulder and Hand Score
3) Increased flexion-extension arc
4) Increased reoperation rate
5) Decreased complication rate
This patient sustained a comminuted distal humerus fracture. Open reduction and internal fixation (ORIF) is found to have higher repoeration rates compared with total elbow arthroplasty (TEA) in the elderly: 27% versus 12%, respectively.
Distal humerus fractures account for approximately 30% of elbow fractures. There is often a low energy mechanism of injury in the elderly patient. While ORIF and TEA may be utilized in bicolumnar distal humerus fractures in the elderly patient, recent literature has demonstrated favorable outcomes with TEA in this aged cohort. TEA is indicated in the low demand osteoporotic patients with bicolumnar distal humerus fractures that are not amendable to ORIF. Utilization of TEA has demonstrated greater functional outcome scores, greater motion, less complications, and a lower revision rate.
Mckee et al. conducted a prospective, randomized, controlled trial comparing functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with ORIF or primary semiconstrained TEA. They reports that patients who underwent TEA had significantly better motion, performance and outcome scores, lower reoperation rates compared with the ORIF group. They concluded that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF and that TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation.
Githens et al. performed a systematic review and meta-analysis to analyze outcomes and complication rates in elderly patients with intra-articular distal humerus fractures being treated with either TEA or ORIF with locking plates. They report that TEA and ORIF for the treatment of geriatric distal humerus fractures produced similar functional outcome scores and range of motion.
However, they found a non-statistical trend toward a higher rate of major complications and reoperation after ORIF. They conclude that the quality of study methodology was generally weak and ongoing research including prospective trials and cost analysis is indicated.
Figure A is the AP radiograph of a comminuted bicolumnar distal humerus
fracture. Illustration A are the radiographs of a comminuted distal humerus fracture in an elderly patient treated with a TEA. Illustration B is the postoperative radiographs of a comminuted distal humerus fracture treated with ORIF.
Incorrect Answers:
Answers 1-3,&5: TEA has demonstrated greater functional outcome scores, greater motion, less complications, and a lower revision rate compared with ORIF.
Figure A is the postoperative radiograph of an 82-year-old female who was treated with a cephalomedually nail for a left intertrochanteric hip fracture. Which of the following is the most common complication following use of this device?
1) Anterior perforation of distal femur
2) Breakage of the screw
3) Implant cutout
4) Malunion
5) Nonunion
Intertrochanteric hip fractures are most commonly treated with a cephalomedullary nail. The most common complication following utilization of a cephalomedullary nail is implant failure and cutout.
Intertrochanteric hip fractures are extra-capsular injuries that are common in the elderly osteoporotic patient. These injuries carrry a 20-30% mortality rate in the first year following fracture. Femoral cephalomedullary nails are often used to treat these injuries. Often a helical blade or screw may be used to provide fixation within the femoral neck. Overall, the most common complication following use of this device is implant failure and cutout, which occurs most commonly within 3 months following surgery. A known risk factor of this complication is an increased tip-apex distance, with a 60% failure rate reported with a distance exceeding 45mm.
Gardner et al. reviewed the use of a helical blade device to stabilize
intertrochanteric hip fractures. They reported a mean telescoping in unstable and stable fractures of 4.3 mm and 2.6 mm, respectively. They also found that blade migration within the femoral head averaged 2.2 mm overall, with no difference between stable and unstable fractures. They concluded that position changes occurred within the first 6 weeks postoperatively, with no subsequent detectable migration or telescoping.
Haidukewych et al. reviewed patients with failed internal fixation of a hip fracture. They report that salvage options are dependent on the anatomic site of the nonunion, the quality of the remaining bone and articular surface, and patient factors such as age and activity level. They conclude that in younger patients with either a femoral neck or intertrochanteric fracture nonunion with a satisfactory hip joint, treatment typically involves revision internal fixation with or without osteotomy or bone grafting. Conversely, in older patients with poor remaining proximal bone stock or a badly damaged hip joint, conversion to hip arthroplasty is recommended.
Figure A is the AP radiograph of the right hip treated with a cephalomedullary nail. Illustration A demonstrates screw cutout.
Incorrect Answers:
Answers 1,2,4,5: These are not the most common complications following use of a cephalomedullary nail
Figures A is the CT angiogram of a 22-year-old male (Patient A) who presents to the trauma bay after sustaining a low-velocity gunshot injury to the femur. Compared to Figure B, which is a different patient (Patient B) who also sustained a low velocity gunshot wound, the associated injury seen in Patient A places him at increased risk for which of the following?
1) Hip disarticulation
2) Infection
3) Malunion
4) Hardware failure
5) Neuropraxia
This patient sustained a low-velocity gunshot wound to the femur with an associated vascular injury. The presence of a vascular injury has been shown to increase the risk of infection.
A low-velocity GSW is defined as a muzzle velocity
Figure A is the radiograph of a 24-year-old male who presents to the trauma bay following a motor vehicle accident. After initial evaluation the patient begins to become hemodynamically unstable and a pelvic binder is placed. The binder should be centered over what anatomic structure?
1) Anterior superior iliac spine (ASIS)
2) Lesser trochanter
3) Greater trochanter
4) Superior aspect of the iliac crest
5) Umbilicis
Figure A demonstrates an APC 3 pelvic ring injury. In the setting of hemodynamic instability, they should be treated with a pelvic binder centered over the greater trochanters.
APC pelvic ring injuries are highly associated with intrapelvic hemorrhage, most commonly from bridging veins. The pelvis can hold a significant amount of blood; thus, the purpose of the pelvic binder is to decrease the total intrapelvic volume. It is crucial that the binder be placed in the proper position at the level of the greater trochanter. Alternatively, a sheet can be applied to the pelvis if a binder is not available.
Prasarn et al review the difference between external fixation and pelvic orthotic devices in a cadaveric study. They report that with logrolling the patient and with elevating the head of the bed the orthotic device placed at the level of the greater trochanters provided improved stability in all planes, however, this did not reach statistical significance. They conclude that there were no significant differences in the stability conferred by an external fixator and a binder for unstable pelvic ring injuries.
Beltran et al review resuscitation and the treatment of shock. They report that placement of a pelvic binder over the greater trochanters serves as an immediate maneuver capable of reducing pelvic volume and stabilizing the pelvis, ultimately aiding in clot formation. They conclude that sheets may also be used and are widely available and can be cut for vascular access to allow for emergent laparotomy.
Prasarn et al compare circumferential sheeting and the use of pelvic binders for unstable pelvic ring injuries. They report no difference in the motion of the hemipelvis during application, logroll, or elevating the head of the bed. They conclude that sheets are more readily available, cost less and are more versatile than pelvic binders.
Incorrect Answers:
Answers 1,2,4, & 5: For maximal volume reduction and stability, pelvic binders and circumferential sheets should be placed over the level of the greater trochanter.
A 54-year-old female sustains a closed comminuted, intraarticular distal radius fracture and a small ulnar styloid tip fracture. She works as a housekeeper and is otherwise healthy. You are considering external fixation (EF) with supplemental K-wire fixation of her articular surface versus volar locking plate (VLP) application. Which of the following considerations is true?
1) Regardless of method of radius fixation, ulnar styloid tip fractures should be fixed to preserve DRUJ stability
2) Placing a VLP proximal to the watershed line increases the likelihood for flexor tendon injury
3) Wound complications are higher for the VLP
4) Both methods of fixation will yield satisfactory results
5) Pillar pain is likely in both groups
Both external fixation (EF) and volar locking plate (VLP) fixation produce successful results in the treatment of distal radius fractures.
Indications for operative intervention on distal radius fractures generally include younger patients with dorsal angulation, displaced intra-articular fragments, radial shortening, intra-articular shear patterns, or die punch fractures of the lunate facet. EF can effectively reduce and stabilized distal radius fractures although the VLP has become more prevalent in recent times, as evident in the 13-fold increase in surgical fixation of distal radius fractures from 1998-2008. Despite this paradigm shift, external fixation remains an effective treatment for distal radius fractures.
Williksen et al. randomized 111 unstable distal radius fractures to VLP or EF. At 5-year follow-up, the authors found no difference in DASH scores. However, for comminuted intra-articular fractures, VLP demonstrated mildly superior supination, flexion, grip strength, Mayo wrist score, and less ulnar shortening. The authors additionally noted that among the VLP cohort, 21% required HWR for surgical complications. They concluded that both methods of fixation achieved satisfactory outcomes at 5 years.
Agee reviewed multiplanar ligamentotaxis in the reduction and stabilization of distal radius fractures. Ligamentotaxis refers to the tension applied across a fracture by the surrounding soft tissues. Dr. Agee contends that the use of an EF allows for adjustments in many planes which in turn helps restore anatomic alignment until the distal radius fracture heals.
Egol et al. randomized 120 wrist fractures that received EF for fracture stabilization into three groups for pin site care: weekly dry dressings, daily pin site care with hydrogen peroxide, and chlorhexidine discs around the pins. The fixators remained in place for 5.9 weeks and 19% had a pin tract complication. There were no differences between the three groups in terms of the prevalence of pin-site complications. However, increasing the age of the patient was correlated to pin-track complications.
Incorrect Answers:
Answer 1: Ulnar styloid tip fixation is not necessary and an ulnar styloid tip non-union does not have a significant impact on clinical outcomes.
Answer 2: Placement of the VLP DISTAL to the watershed line increases the risk for flexor tendon injury.
Answer 3: Wound complications such as pin tract infection are significantly higher in the EF cohort.
Answer 5: Pillar pain is frequent in carpal tunnel release, but is not commonly reported in distal radius fracture fixation.
An 8-year-old boy is involved in an ATV crash. Xrays were obtained in the trauma bay after being airlifted to your facility, shown in Figures A. On the day of presentation, you perform the treatment shown in the figure B. On postoperative day 1, the patient states his pain is controlled, however, you find that his calf is tense, his foot is cool and has diminished pulses compared to the contralateral extremity. What is the best next step of the options below?
1) Remove your fixation and perform repeat reduction
2) Measure leg compartment pressures
3) Request vascular consultation
4) Measure ankle-brachial index (ABI)
5) Duplex ultrasound evaluation
This patient is presenting with symptoms concerning for compartment syndrome without significant pain. The next best step in evaluation would be to perform compartment pressure measurements.
Compartment syndrome is the process where osseofascial compartment pressures rise to levels that decrease perfusion to the structures within. This is an orthopedic emergency, requiring opening the compartment via fasciotomy to relieve the pressure within. Delay in treatment can result in irreversible muscle and nerve damage. Compartment syndrome is a clinical diagnosis, and treatment should not be delayed if your index of suspicion is high. Diagnosis can be more difficult in children due to inability to verbalize symptoms.
However, compartment pressures can be measured if the clinical picture is uncertain, such as when patients sedated or otherwise have altered mental status. Typically a difference of 48 hours after injury. They conclude by emphasizing the importance of extended vigilance in pediatric patients for the development of compartment syndrome.
Figures A shows an AP radiograph of a tibial shaft fracture in a pediatric patient. Figure B shows a diagram of flexible nailing of a tibia.
Incorrect answers:
Answer 1: This would not aid in the diagnosis or treatment of compartment syndrome.
Answer 3: While vascular compromise can be a late manifestation of the compartment syndrome, the treatment is fasciotomy to re-establish blood flow. Answer 4: An ABI would likely show an abnormality, however, this would not be the appropriate study.
Answer 5: This is the appropriate workup if you were concerned about deep venous thrombosis.
A 72-year-old female presents to your office with a 12-month old painful nonunion of a 2-part (surgical neck) proximal humerus fracture which was managed non-operatively. Prior to her injury, she denied shoulder pain and had excellent range of motion. Since the injury, she has had persistent debilitating pain and dysfunction with motion above the shoulder level. X-Rays show good bone stock, no significant shoulder arthritis or avascular necrosis, and well-positioned tuberosities. Which of the following is the most optimal treatment for the patient?
1) Closed reduction and percutaneous pinning
2) Shoulder hemiarthroplasty
3) Open bone grafting
4) Open reduction and internal fixation (ORIF) with or without bone grafting
5) Reverse total shoulder arthroplasty (rTSA) with lattisimus dorsi transfer to assist with internal rotation
A 2-part proximal humerus non-union in a patient with good bone stock without evidence of arthritis or osteonecrosis can be effectively managed with
ORIF with locked plating with or without bone grafting.
Treatment of a chronic nonunion of the proximal humerus in the elderly should be treated with fixation when possible. Critical attention should be paid to correct all deformities: tuberosity positioning, articular surface realignment, soft tissue balancing, rotator cuff repair (when needed), and treatment of soft tissue contractures. Attempts at arthroplasty are generally recommended only when there is significant osteopenia or avascular necrosis, if the tuberosities have resorbed, if the rotator cuff has a pre-existing tear, or if other findings are present that would limit the success rate of fixation.
A 68-year-old woman undergoes a hemiarthroplasty for a proximal humerus fracture through a deltopectoral approach. Care
should be taken with which of the following activities in the immediate postoperative period due to concerns about lesser tuberosity fixation?
1) Passive forward flexion of the shoulder in the scapular plane
2) Passive internal rotation of the shoulder to the plane of the body
3) Active abduction of the shoulder past 45 degrees
4) Passive external rotation of the shoulder
5) Active extension of the shoulder
Due to extensive pull on the lesser tuberosity via the subscapularis, care should be taken with increased levels of passive external rotation in the immediate post-operative period.
Proximal humerus injuries resulting in head-splitting fractures, avascular necrosis, or nonunion can be treated reliably with arthroplasty. During reconstruction with arthroplasty, the tuberosities need to be anatomically fixed in order to allow for a proper range of motion post-operatively. The subscapularis tendon inserts on the lesser tuberosity and is the deforming force when placed under tension during external rotation and during active internal rotation. As such, post-operative passive external rotation and active internal rotation are both limited initially until the lesser tuberosity has healed in its anatomic location.
Frankle et al. performed a biomechanical study to determine the importance of anatomic fixation of tuberosities after hemiarthroplasty for proximal humerus fractures. The authors noted that non-anatomic tuberosity reconstruction led to significant impairment in external rotation kinematics and an 8-fold increase in torque requirements whereas anatomic reconstruction produced indistinguishable results from normal shoulder controls. The authors concluded that the rotational alignment of tuberosities during reconstruction is critical in order to allow patients to perform an adequate range of motion postoperatively.
Frankle and Mighell performed a review of the techniques of tuberosity fixation for shoulder hemiarthroplasty for the treatment of proximal humerus fractures. The authors describe that variable geometry and known anatomic relationships can facilitate tuberosity reconstruction. This requires a re-producible technique, an instrumentation system, and a prosthesis that can maximize tuberosity reconstruction.
Incorrect Answer:
Answers 1, 2, 3 and 5: Passive external rotation and active internal rotation
both places stress on the lesser tuberosity due to the insertion of the subscapularis tendon and are limited in the immediate post-operative setting following hemiarthroplasty.
A 24-year-old man was involved in a MVC and sustained the injury shown in Figure A. A closed reduction is performed and a post-reduction CT scan is obtained. Which of the following correctly pairs the CT with the most appropriate management?
1) Figure B; Protected weightbearing
2) Figure B; Examination under anesthesia (EUA) to assess hip stability
3) Figure C; Protected weightbearing
4) Figure C; Examination under anesthesia (EUA) to assess hip stability
5) Figure D; Protected weightbearing
This patient sustained a posterior hip dislocation. Of the answer choices listed, the fracture pattern seen in Figure C would be appropriately managed with EUA to assess hip stability.
Posterior wall fractures are the most common type of acetabular fracture. Management of posterior wall fractures is dictated by the extent of posterior wall involvement, with those involving >40-50% best treated with ORIF. Management of fractures involving 20-40% of the posterior wall, on the other hand, should be based on hip stability. As suggested by Tornetta, assessment of hip instability with dynamic stress views is helpful to determine which posterior wall fractures are unstable and therefore require open reduction and internal fixation. Protected weightbearing may be employed if the hip is stable; however, hip stability must be determined first.
Tornetta performed a study to assess the use of dynamic stress views in the non-operative management of acetabular fractures. He found that the use of dynamic stress views in determining the need for ORIF was effective, leading to good or excellent results in 91% of cases. He concluded that dynamic stress views can identify subtle instability in patients who would normally be considered for non-operative treatment.
Moed et al. performed a retrospective study to evaluate the role of CT in predicting hip stability in posterior wall fractures of the acetabulum. They analyzed 3 methods of calculating posterior wall fracture fragment size on CT and compared it to findings on EUA. They found that the alternative method (which measures fragment size at the level of the largest posterior wall deficit) was more accurate than the Calkins method (which measures the smallest amount of intact acetabular arc) and the Keith method (which measures fragment size at the level of the fovea). However, given the low risk of EUA and the inherent problems making CT measurements, they concluded that dynamic fluoroscopic stress testing under general anesthesia should be the preferred method for the determination of hip stability status after posterior wall fractures of the acetabulum.
Calkins et al. performed a study to assess the efficacy of CT in predicting hip stability based on measurements of the percentage of remaining posterior acetabulum. They found that all hips with 55% were stable. They concluded that a simple linear measurement of the remaining posterior acetabulum on CT can be done easily by a physician and can provide a means of predicting hip stability for individual patients.
Figure A is an AP radiograph of the right hip demonstrating a posterior hip dislocation. Figure B is an axial CT of the right hip demonstrating a posterior wall fracture with intraarticular fragments. Figure C is an axial CT of the right hip demonstrating a posterior wall fracture involving > 20% of the posterior
wall. Figure D is an axial CT of the right hip demonstrating a posterior wall fracture involving > 40% of the posterior wall.
Incorrect Answers:
Answer 1: Protected weightbearing would be inappropriate for a posterior wall fracture with intraarticular fragments.
Answer 2: EUA would be inappropriate for a posterior wall fracture with intraarticular fragments.
Answer 3: Posterior wall fractures involving 20-40% of the posterior wall may be treated with protected weightbearing; however, EUA to assess for instability is recommended prior to making the final decision to proceed with nonoperative treatment.
Answer 5: Open reduction internal fixation is indicated in unstable fractures such as posterior wall fractures involving >40-50% of the posterior wall.
A 44-year-old male fell onto his arm and presents to the emergency department with elbow pain, swelling, and inability to use the right arm. The ED staff place the patient in a posterior mold splint and call after radiographs are obtained. The current images are shown in Figures A and B. What is the next best step in management?
1) CT scan of the elbow
2) Examination of the elbow under anesthesia
3) Obtain traction views
4) Continued immobilization and outpatient follow-up in three weeks
5) Immediate ORIF of coronoid, radial head, and repair of LCL
The patient is presenting with an anteromedial facet fracture of the coronoid due to a posteromedial rotatory force. A CT of the elbow should be performed to asses the extent of articular involvement, degree of comminution, and the size of the coronoid fragment.
The coronoid process is one of the main constraints that provide ulnohumeral joint stability. The coronoid process and the radial head provide a buttress against the posterior displacement of the elbow joint. The anteromedial facet of the coronoid process, also known as the sublime tubercle, is the insertion of the anteromedial bundle of the ulnar collateral ligament, which provides valgus stability of the elbow. Fracture of the coronoid process can be either an isolated finding following elbow dislocation or part of a more complex fracture-dislocation. This patient had a fracture to the of the anteromedial portion of the coronoid, therefore the medial side of the elbow is unsupported to varus stresses. As a result, the joint line will narrow from lateral to medial secondary to the medial collapse of the joint. On a lateral, the crescent sign, which represents the depressed anteromedial facet of the coronoid, may be seen.
Steinmann reported that with an anteromedial coronoid fracture, the anteroposterior radiograph of the elbow will demonstrate progressive narrowing of the joint space from lateral to medial between the medial trochlea and the coronoid process. On a lateral radiograph, a coronoid fracture fragment may appear small and may be confused with a radial head fracture. A CT scan of the elbow is recommended in all cases of suspected coronoid fractures because such a fracture is readily seen with this imaging modality.
Doornberg and Ring reported that coronoid fractures are associated with specific patterns of traumatic elbow instability. They concluded that large coronoid fractures were associated with anterior and posterior olecranon fracture-dislocations while small transverse fractures were associated with terrible triad injuries. Finally, anteromedial facet fractures were associated with varus posteromedial rotational instability.
Ring and Doornberg wrote a surgical technique of repairing the anteromedial facet fracture. They report that fractures of the anteromedial facet of the coronoid may be treated with a plate, a screw, or sutures. They conclude that
the secure fixation of this fragment usually restores good elbow function.
Figures A and B are the AP and lateral radiographs of the right elbow with a fracture of the anteromedial facet of the coronoid.
Incorrect Answers:
Answer 2: Though an examination of the elbow would likely reveal instability, given the large fracture evident on radiographs, this would not provide further diagnostic information.
Answer 3: Traction view radiographs are helpful in comminuted distal humerus fractures. In this patient, traction views would provide little diagnostic benefit. Answer 4: Prolonged immobilization of elbow injuries typically results in permanent elbow stiffness. Surgical fixation of the fracture would be preferable to permit early rehab after a CT assessment to determine the extent of the injury.
Answer 5: This is the treatment for terrible triad injury of the elbow. The radial head does not appear to be affected in the current radiographs.
A 58-year-old male active smoker falls while working at his barn and sustains the closed injury depicted in Figures A and B. His neurovascular examination is unremarkable. The decision is made to perform open reduction internal fixation of his proximal humerus. Which of the following characteristics is MOST predictive of humeral head ischemia?
1) Medial hinge disruption
2) Calcar length of 4mm
3) Patient age
4) Lateral hinge disruption
5) Number of fracture parts
This patient has sustained a comminuted 4-part proximal humerus fracture. Of the above fracture characteristics, the most predictive of humeral head
ischemia is calcar length of 4mm.
In complex intra-articular proximal humerus fractures, perfusion of the humeral head is an important consideration when deciding on treatment. Recent evidence has demonstrated that the posterior humeral circumflex artery is likely the main blood supply to the humeral head, and fracture displacement can lead to disruption of this blood supply along with the anterior humeral circumflex artery, causing humeral head ischemia. Several studies have demonstrated that residual perfusion of the humeral head relies predominantly on the medial and posteromedial metaphyseal extension (i.e. calcar length) that might remain attached to the head, with other protective factors including the integrity of the medial hinge and basic fracture patterns .
Hertel et al. investigated predictors of fracture-induced humeral head ischemia at the time of surgery for articular proximal humerus fractures. They reported that the highest predictors of humeral head ischemia, from most accurate to least accurate, were calcar length 45 degrees, displacement of the tuberosities >10 mm, glenohumeral fracture-dislocation and head-split fractures. They concluded that the most relevant predictors of ischemia were the length of the posteromedial calcar, the integrity of the medial hinge, and the basic fracture type.
Nho et al. reviewed innovations in the management of displaced proximal humerus fractures. They reported that treatment should be dictated by careful scrutiny of vascular status, bone quality, fracture pattern, degree of comminution, as well as patient factors, such as age and activity level. They concluded that Fractures with AO type C pattern, metaphyseal extension 2 mm are associated with high probability of humeral head ischemia and likely are best treated with arthroplasty.
Figure A demonstrates a plain radiograph of a 4-part proximal humerus fracture. Figure B is a CT 3D-reconstruction of the 4-part proximal humerus fracture. Illustration A highlights the vascular anatomy of the proximal humerus. Illustration B depicts the differences in posteromedial calcar lengths in proximal humerus fractures. Illustration C highlights the difference between an intact and disrupted medial hinge.
Incorrect Answers:
Answer 1 and 4: While medial (not lateral) hinge disruption may predict humeral head ischemia, a short calcar length (i.e. 4 mm) is more predictive. Answer 3: Patient age is not as strong of a factor in predicting humeral head ischemia like calcar length.
Answer 5: The number of fracture fragment may predict humeral head ischemia, but it is not as strong and relevant of a predictor like calcar length.
You are called to evaluate a 32-year-old man with knee pain after being struck as a pedestrian. You recognize the fracture as a Schatzker IV tibial plateau fracture. Which of the following statements is most accurate?
1) A fracture-dislocation must be suspected as the femur follows the displaced lateral tibial plateau
2) This fracture may often be seen with medial meniscal and anterior cruciate
ligament injuries
3) Open reduction internal fixation with a lateral plating is the construct of choice
4) Open reduction internal fixation with bicondylar plating is the construct of choice
5) Vascular injuries are rare with this type of fracture
Of the above descriptions regarding the Schatzker IV tibial plateau fracture, the most accurate is that it may often be seen with medial meniscal and anterior cruciate ligament injuries.
While the lateral plateau is smaller and convex, the medial plateau is larger and concave, resulting in an eccentric load distribution in which the medial plateau bears ~ 60% of the knee's load. The relative osseous strength of the medial plateau, the valgus anatomic axis of the lower extremity, and the susceptibility of the leg to a medially directed force all result in the increased prevalence of to lateral-sided injuries (Schatzker I and II) in low-energy fractures. High-energy plateau injuries result in increased less predictable fracture patterns that are often comminuted and involve the medial plateau (Schatzker IV through VI) and may be associated with medial meniscus, ACL, and vascular injuries.
Bennett et al. reviewed tibial plateau fractures and associated soft tissue injuries. They reported a 56% rate of associated soft tissue injuries in their series, with the most common being medial, lateral collateral ligaments, and menisci. They observed that Schatzker IV and VI plateau fractures were associated with the highest rate of soft tissue injuries. They recommended pre-and post-fixation stress testing to diagnose collateral and cruciate ligament injuries
Berkson et al. reviewed high energy tibial plateau fractures. They reported that high-energy injuries can lead to comminuted fractures with significant osseous, soft-tissue, and neurovascular injury, whereas lower energy injuries result in unilateral depression type fractures. They emphasized that treatment be directed at safeguarding tissue vascularity and restoring joint congruity and the mechanical axis of the limb.
Illustrations A and B demonstrate a Schatzker IV tibial plateau fracture. Illustration C depicts the Schatzker classification of tibial plateau fractures. Schatzker I is a lateral split fracture, Schatzker II is a lateral split-depression fracture, Schatzker III is a lateral pure depression fracture, Schatzker IV is a medial plateau fracture, Schatzker V is a bicondylar fracture, and Schatzker VI
is a metaphyseal-diaphyseal dissociation.
Incorrect Answers:
Answer 1: A fracture-dislocation must be suspected as the femur follows the displaced medial (not lateral) tibial plateau
Answer 3 and 4: ORIF with a medial buttress plate is the definitive construct often used for Schatzker VI fractures.
Answer 5: Vascular injuries are commonly associated with Schatzker IV plateau fractures.
A 36-year-old female sustains the closed injury shown in Figure A as the result of a high-speed motorcycle collision. She undergoes immediate closed reduction and placement of a knee-spanning external fixator with plans for definitive fixation in 2 weeks. Which of the following is an expected finding in this patient as a result of the placement of a temporizing external fixator?
1) Increased rate of compartment syndrome during hospitalization
2) Increased transient leg compartment pressures during external fixator placement
3) Increased rate of ligamentous knee injury
4) Increased risk of deep hardware infection after 2nd stage surgery
5) Increased risk of malunion after 2nd stage surgery
Application of knee-spanning external fixation as a temporary measure for stabilization of high-energy proximal tibial fractures and dislocations may result in transient elevation of intracompartmental pressures of the leg.
The use of a staged protocol for the treatment of high-energy tibial plateau
fractures has been shown to decrease soft tissue complications. These high energy injuries are best treated with placement of a knee-spanning external fixator which allows ligamentotaxis to maintain overall length. The staged protocol generally consists of closed reduction and placement of a knee-spanning external fixator. Although some controversy exists, the pins are generally not placed within the site of injury or planned area of the plate, in order to minimize infectious risk. The limb is elevated, and ice can be used generously to allow for the resolution of edema. Once the swelling improves, and skin wrinkles are seen, the risk of wound healing complications and infection is decreased, and the surgeon can then proceed with surgery. During the placement of an external fixator, a transient elevation of compartment pressures is expected (DeltaP may fall below the threshold of 30 mm Hg), but this does not appear to lead to the development compartment syndrome.
Egol et al. (2008) reviewed the effect of spanning external fixation in regards to compartment syndrome in 25 patients. They found that 9/22 (41%) had a transient DeltaP
A 72-year-old female with a history of osteoporosis treated with bisphosphonates presents to the ED with bilateral thigh pain after falling backward at home. On examination, there is gross external rotation of bilateral lower extremities with shortening. There are no open skin lesions. Radiographs are shown in figures A and B. What is the total expected blood loss of these injuries?
1) 500-1000 cc
2) 1000-1500 cc
3) 1500-2000 cc
4) 2000-3000 cc
5) 3000-4000 cc
Average blood loss in closed femur fracture averages between 1000 to 1500
cc. With bilateral closed femoral shaft fractures, the expected blood loss would be between 2000 and 3000 cc.
The estimated blood loss for closed fractures of the femur and tibia are 1000-1500 and 500-1000 cc, respectively. Blood loss can double in open fractures. Similarly, bilateral closed femoral shaft fractures can have double the blood loss of a single closed femoral shaft fracture. In the presence of exsanguinating external hemorrhage, control of hemorrhage should take precedence over the ABCDE primary survey.
Lieurance et al. retrospectively reviewed 53 patients with isolated femur fractures. They found that 21 patients required transfusion of an average of
2.5 units PRBCs. The estimated blood loss was 1276cc and not affected by the fracture pattern or high/low energy pattern. They concluded that preoperative hemorrhage contributed to transfusion needs more than intraoperative blood loss.
Lee and Porter reviewed the prehospital management of lower limb fractures. They recommend a stepwise control of bleeding: direct pressure, elevation, wound packing, windlass technique (place a pen under a circumferential knot and rotate the pen until tight), indirect pressure (traction splint), tourniquet. In the presence of compressible/controllable bleeding, they recommend resuscitation to normal physiological parameters. In the presence of non-controllable bleeding, they recommend hypotensive resuscitation (SBP 80mmHg or to restore the radial pulse).
Figures A and B are the AP radiographs of the left and right atypical femur fractures with characteristic cortical thickening, transverse fracture pattern with medial beaking, and lateral stress reaction at the site of the fracture.
Incorrect Answers:
Answers 1, 2, 3, 5: Average blood loss for a closed femoral shaft fracture is 1000-1500 cc, with bilateral fractures having double the blood loss. The other answer choices do not reflect this.
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?
1) Decreased joint penetration of distal screws
2) Increased rigidity
3) Decreased need for delayed hardware removal
4) Decreased peroneal irritation
5) Improved distal fixation
Posterior antiglide plating is a technique that involves placement of a plate on the posterior aspect of the distal fibula, using the plate as a reduction tool and direct buttress against distal fracture fragment displacement.
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
A 24-year-old female sustains a surgical neck proximal humerus fracture in a motor-vehicle collision. She undergoes open reduction and internal fixation but heals in 45 degrees of varus and has significant limitation of shoulder range of motion despite 9 months of conservative treatments. What is the most appropriate treatment at this time?
1) Manipulation under anesthesia
2) Humeral head resurfacing
3) Shoulder hemiarthroplasty
4) Revision open reduction internal fixation with osteotomy
5) Reverse total shoulder arthroplasty
Malunions of the proximal humerus typically result in significant restrictions in range of motion. This young patient has sustained a proximal humeral malunion, and treatment should include a corrective osteotomy for improved outcomes, as she has failed conservative treatment.
The cited reference by Williams et al as well as the referenced article by Siegel et al explain various techniques in management of proximal humerus malunions. They state that the two primary indications for surgical management of proximal humerus malunion include 1) pain and 2) diminished function resulting from limited range of motion. Because this patient is young, you would attempt revision ORIF/osteotomy as opposed to humeral head arthroplasty.
A 6-year-old boy with progressive bilateral genu varum undergoes the surgeries shown in Figure A. On postoperative rounds later that day, the patient appears sedated after several doses of pain medication. His toes are pink with brisk capillary refill however, passive motion of his toes causes pain. Among the answer choices listed, what is the best management strategy for this child?
1) Elevate his legs and reevaluate on morning rounds
2) Adjust his pain medication to accommodate for his increasing pain
3) Administer a muscle relaxant for leg spasms
4) Cast removal and measurement of compartment pressures with a standard device
5) Examine the cast for areas of constriction and reevaluate in the morning
Intracompartmental pressure measurements should be performed when pain with passive motion of the toes is found in young patients with insufficient clinical data to establish a definitive diagnosis of compartment syndrome. The child in this clinical vignette has Blount’s disease which was treated with bilateral tibial osteotomies, a procedure commonly associated with compartment syndrome.
Pain with passive stretch is the most sensitive clinical sign of elevated compartment pressures prior to the onset of ischemia in compartment syndrome. Pain is difficult to assess in children at baseline, therefore, a high level of suspicion should exist and compartment pressure monitoring should be performed in unreliable patients.
Mubarak et al. reported on a series of 27 patients subjected to intracompartmental pressure monitoring for a clinical suspicion of acute compartment syndrome. The wick catheter technique was employed not only to aid in the diagnosis of compartment syndrome at an early stage but also to indicate the effectiveness of the decompressions when used intraoperatively during fasciotomies.
Matsen et al. reported on 24 children with compartment syndrome following injuries and surgery. The most common etiologies identified were fractures, vascular injuries, and tibial osteotomies. Compartment pressure measurements were helpful in establishing the diagnosis of compartment syndrome in young patients and in those with neurologic or vascular injuries with ambiguous clinical findings.
Figure A reveals an AP radiograph of bilateral knees status post valgus-producing tibial osteotomies and epiphysiolyses of the medial tibial physes in a 6-year-old male with Blount’s disease.
Incorrect Answers:
Answers 1 and 5 are wrong because immediate action should be taken to establish a definitive diagnosis and treat accordingly when a clinical suspicion of compartment syndrome arises.
Answers 2 and 3 are incorrect because administering medications that can cause sedation will exacerbate the patient’s present state of drowsiness, confuse the clinical picture, and make the diagnosis of compartment syndrome even more difficult to establish.
A 16-year-old male was struck by an automobile while riding his bicycle. He sustained the injuries in Figure A. Which of the following orthopedic injuries is MOST associated with this injury?
1) Brachial plexus injury
2) Ipsilateral clavicle fracture
3) Pelvic ring injury
4) Rib fracture
5) Spine fracture
Figure A demonstrates a scapula body fracture. Rib fractures are the most common orthopedic injury associated with these high-energy fractures, with a 52% incidence.
Scapula fractures are associated with high-energy trauma and have a reported mortality rate of 2-5%. Approximately 50% of high-energy scapular fractures involve the body and spine. Most scapular fractures may be treated conservatively with sling immobilization followed by early motion with no expected functional deficits. Indications for operative management of scapular fractures include glenohumeral instability with >25% of glenoid involvement or
>5mm of articular step-off, excessive medialization of the glenoid, displaced scapular neck or coracoid fractures, and open fractures.
Baldwin et al. retrospectively reviewed 9,543 scapular fractures utilizing the US National Trauma Database. They reported that the most commonly associated fractures were rib fractures (52.9%), followed by fractures of the spine (29.2%), clavicle (25.2%), and pelvis (15.3%). They concluded that lung and head injuries occurred in 47.1% and 39.1% of the cases, respectively.
Brown et al. retrospectively reviewed the association between scapular fractures (SF) and blunt thoracic aortic injury (BTAI). They found that in 35,541 blunt trauma admissions, SF and BTAI occurred in 1.1% and 0.6% of patients, respectively. They noted that most of the patients with SF had associated injuries (99%), but only four patients with SF had BTAI. The most common injuries associated with SF were rib (43%), lower extremity (36%), and upper extremity (33%) fractures. They concluded that SF is uncommon after blunt trauma, but patients with SF almost always have significant associated injuries and indicates a high amount of energy.
Figure A demonstrates a high-energy scapular body fracture which may benefit from surgical intervention
Incorrect Answers:
Answers 1-3,5: Fractures of the spine (29.2%), clavicle (25.2%), and pelvis (15.3%) are all associated with high-energy scapula fractures, but occur less commonly than rib fractures (52%)
Which of the following amputations will lead to the greatest oxygen requirement per meter walked following prosthesis fitting?
1) Above-knee-amputation (transfemoral)
2) Below-knee-amputation (transtibial)
3) Through Knee
4) Syme
5) Midfoot
The general trend is increasing energy requirement for more proximal amputations. Amputation should be performed at the lowest possible level in order to preserve the most function.
Pinzur compared 5 patients with amputations at midfoot, Syme’s, BKA, through knee, and AKA with five controls. Walking speed and cadence decreased while oxygen consumption per meter walked increased with each more proximal amputation.
The only exception is the Syme which was the most energy efficient even though it is more proximal to the midfoot amputation.
An otherwise healthy 30-year-old male sustains a left forearm injury as a result of a fall from a ladder. Initial examination in the emergency room reveals a clean 2 centimeter laceration over the volar forearm associated with the radiographs shown in Figures A and B. Treatment should consist of irrigation and debridement of the wound followed by which of the following?
1) Closed reduction and casting of left radius and ulna
2) Temporary external fixation of the left radius and ulna
3) Definitive external fixation of the left radius and ulna
4) Open reduction and internal fixation of the left radius and ulna with delayed skin closure
5) Open reduction and internal fixation of the left radius and ulna with immediate skin closure
The clinical scenario is consistent with an open fractures of the distal radial and ulnar shafts. Literature shows that definitive plating of an open forearm fracture followed by primary closure of the wound is acceptable treatment at the time of injury.
Chapman et al performed a retrospective review of 50 patients with immediate internal plate fixation of an open diaphyseal fracture of the forearm. The functional results were excellent or good in 85%.
The review by Levin is a comprehensive review of the literature on early versus delayed closure of open fractures, and covers the change in thought from previous literature, including change in technology, surgical techniques, and a more critical review of previous literature.
During a Lisfranc (tarsometatarsal) amputation of the foot, which of the following is crucial to prevent the patient from having a supinated foot during gait.
1) Releasing the posterior tibialis tendon
2) Preserving the soft-tissue envelope (peroneus brevis, tertius and plantar fascia) around the fifth metatarsal base
3) Myodesis of the anterior tibialis to the medial and middle cuneiforms
4) Lengthening of the gastrocsoleus (achilles tendon)
5) Osteotomy through 1st metatarsal
A Lisfranc amputation is through the tarsometatarsal joints, except the 2nd metatarsal, which is osteotomized to preserve the stability of the medial cuneiform. To prevent the patient from supinating the foot following this amputation, the evertors on the foot must be maintained. The principal evertors are the peroneus brevis and longus (Illustration A). Therefore, the function of the peroneus brevis must be preserved. Technically this is done preserving the soft-tissue envelope (peroneus brevis, tertius and plantar fascia) around the fifth metatarsal base.
Illustration B depicts the level of a Lisfranc amputation of the foot. Incorrect Answers:
1-The posterior tibialis is the primary supinator of the foot, and releasing it
would lead to an eversion deformity. The tibialis posterior tendon attachment to the bases of the second and third metatarsals will actually be released with this amputation, but the main attachment to the navicular preserved.
3-The anterior tibialis dorsiflexes and inverts the foot, but transferring it to the medial and middle cuneiforms would mimick its native function to dorsiflex and invert the foot.
4-A lengthened Achilles would lead to increased dorsiflexion, not supination.
5-Osteotomy of 2nd MT is crucial to preserve the medial cuneiform and midfoot stable.
A 39-year-old male is thrown from his motorcycle into a fast-food restaurant and sustains a closed pelvic ring injury. During placement of percutaneous iliosacral screws, the outlet radiograph in Figure A is obtained. What purpose does this view serve?
1) Evaluation of possible injury to L5 nerve root
2) Evaluation of anterior-posterior position of screw(s)
3) Best visualization of sagittal curvature of sacral ala
4) Best visualization of spinal canal
5) Best visualization of sacral neural foramina
Figure A shows an intraoperative outlet view, which provides the best visualization of the neural foramina (and possible screw placement into these foramina). This view provides information regarding cephalad-caudad placement of the screw, whereas the inlet view provides information regarding the anterior-posterior position of the screw. The lateral sacral view provides information regarding the sagittal curvature of the sacral ala and gives information regarding possible iatrogenic L5 nerve injury as it goes over the sacral ala.
The referenced article by Routt et al is a review article regarding the safety and techniques of percutaneous pelvic ring fixation.
A 35-year-old male sustains a closed Schatzker VI tibial plateau fracture. Two weeks following external fixation, examination reveals intact sensation, palpable pulses and no soft tissue compromise. An axial CT image is shown in Figure A. What is the optimal surgical plan?
1) Medial and lateral plate fixation through two approaches
2) Medial and lateral plate fixation through a single anterior approach
3) Lateral locking plate fixation
4) Continued external fixation until union
5) Multiplanar transarticular external fixator
The Figure shows a bicondylar tibial plateau fracture. The goals that need to be met when treating tibial plateau fractures are the following: restoration of mechanical axis alignment, restoration of condylar width, articular reduction, and restoration of knee stability. Since the soft tissue envelope is favorable, open reduction internal fixation with dual incisions and dual plates will provide the best probablity of achieving those goals.
Gosling et al did a biomechanical evaluation in cadavers comparing lateral locked plating with a combined medial and lateral plate and found no difference in resistance to vertical subsidence even with loads exceeding the average body weight. However, this was a cadaveric study with no mention and capability of analyzing articular reduction. Lateral locked plating only allows for indirect reduction of the medial plateau.
Barei et al in a retrospective review found that comminuted bicondylar tibial plateau fractures can be successfully treated with open reduction and medial and lateral plate fixation using 2 incisions, and postulate that the use of 2 incisions may contribute to a lower wound complication rate. A two incision approach allows not necessarily for a stronger construct as some studies are controversial, but for a more accurate reduction and restoration of alignment.
Which of the following is true regarding the use of the saline injection load test to diagnose traumatic knee arthrotomies?
1) Addition of methylene blue to the saline load test increases the sensitivity of the test
2) Injection of 110ml of saline will diagnose 95% of knee arthrotomies
3) Injection of 175ml of saline will diagnose 99% of knee arthrotomies
4) A superomedial injection location requires significantly less fluid than a inferoeromedial injection location
5) A history and physical exam by an orthopaedic surgeon has equivalent sensitivity to saline load test at detecting a traumatic arthrotomy
Injection of 175ml of saline will diagnose 99% of knee arthrotomies.
Clinical evaluation alone to determine if a periarticular laceration has penetrated the joint can often be incorrect. A Saline Load Test (SLT) is an effective methods to detect intraarticular penetration. New studies have shown addition of methylene blue does not improve the diagnostic value of the saline load test. The use of a CT scan can be helpful, especially in the presence of intra-articular air.
Voit et al. investigated the sensitivity of the clinical exam and a saline load test in 50 consecutive patients with periarticular lacerations suggestive of joint penetration. In 14 there was leakage of fluid on saline load test. In six of these patients, the clinician had judged there was no traumatic arthrotomy based on physical exam and clinical history. They therefore concluded performing a saline load test is important adjunct and the clinical exam alone can not be relied on to detect traumatic arthrotomies.
Nord et al. found that the volumes of saline that were needed in order to effectively diagnose 75%, 90%, 95%, and 99% of the knee arthrotomies were
110, 145, 155, and 175 mL, respectively. They also found that an inferomedial injection location required significantly less fluid than a superomedial injection location did.
Metzger et al. studied 58 patients that underwent saline load test with about 100ml of saline injected (methylene blue 29, normal saline 29). They found that the false-negative rate was 67% (methylene blue 69%, normal saline 66%). They concluded the addition of methylene blue does not improve the diagnostic value of the saline load test.
Konda et al. performed a study evaluationg the role of CT scan versus saline load test. They found that the sensitivity and specificity of the CT scan to detect traumatic arthrotomy was 100%. In a subgroup of 37 patients that received both a CT scan and the conventional saline load test, the sensitivity and specificity of the CT scan was 100% compared to 92% for the saline load test (p
A 36-year-old rancher is involved in a tractor roll-over accident and sustains the injury shown in Figure A to his dominant right arm. After undergoing rigid anatomic fixation of the fracture, the distal radio-ulnar joint (DRUJ) remains incongruent. What is the next step in management?
1) Revision plating of the fracture
2) Revision reduction and intramedullary fixation
3) Reduction of interposed extensor carpi ulnaris tendon
4) Reduction of interposed pronator quadratus tendon
5) Reduction of interposed flexor carpi ulnaris tendon
The most likely cause of persistent DRUJ incongruity after anatomic reduction and fixation of the radial shaft fracture of the answers above is interposition of the extensor carpi ulnaris (ECU) tendon. The tendon must be extricated from the joint to permit DRUJ reduction.
Gaeleazzi fracture-dislocations, such as that seen in Figure A, are typically stable once the radial shaft fracture is anatomically reduced. After fixation, the DRUJ is translated in pronation, supination, and in a neutral position to test for stability. A “clunk” during passive motion of the DRUJ is further evidence of gross instability. Gross laxity can be treated by splinting in supination or by pinning the DRUJ. However, ECU tendon interposition has been reported as a possible cause of a persistently irreducible DRUJ. Radiographic findings typically demonstrate a dorsally displaced ulnar head and a widened DRUJ. The interposed tendon must be removed from the joint, often through a separate dorsal approach to permit DRUJ reduction.
Bruckner et al. review the evaluation and management of complex dislocations of the DRUJ. The authors note that these injuries are associated with frequent irreducibility, recurrent subluxation, or soft reduction of the DRUJ secondary to interposed tissue. In their institutional series, four of the 11 cases of Galeazzi fractures were associated with complex DRUJ dislocations, most commonly due to displacement of the ECU tendon volar to the ulna, necessitating open reduction. They cautioned that unobtainable or unconvincing reductions should warrant surgical exploration.
Paley et al. reported two cases of an irreducible DRUJ after radial shaft fracture fixation. The authors describe an empty ECU tendon sulcus on the dorsum of the wrist in both cases. One case was noted and addressed intraoperatively.
However, the second case was not identified and this patient went on to endure persistent subluxation and diastasis of the DRUJ, ultimately experiencing a poor result. The authors advocate a separate dorsal exposure to reduce the ECU.
Hanel and Scheid reported a case of entrapment of the ECU in the DRUJ in a skeletal immature 12 year old boy. They noted that intraoperative radiographic analysis was significant for a widened DRUJ and dorsally displaced ulnar head. These authors too advocated a separate dorsal exposure to approach and extricate the ECU tendon.
Incorrect answers
Answer 1: The fracture is anatomically reduced but the DRUJ is incongruent because of an interposed ECU tendon. Revision fixation will not address the DRUJ incongruity.
Answer 2: The type of fixation is not the issue. Revising the fixation to another construct will not address the ECU interposition.
Answer 4: Pronator quadratus interposition has not been described in the setting of irreducible DRUJ dislocations.
Answer 5: Flexor carpi ulnaris tendon interposition has also not been described in the setting of irreducible DRUJ dislocations.
A 58-year-old right-hand-dominant computer programmer trips and falls onto his right arm. He reports right arm pain and that his elbow felt "sloppy". His initial lateral radiograph is shown in Figure A. The orthopedic junior resident counsels him that he will likely need a radial head arthroplasty, ligament repair, and possible fixation of the ulna. What factor would most significantly affect the decision to surgically address the ulna fracture?
1) Degree of radial head comminution
2) The deforming force acting on the avulsed fracture fragment
3) Size of fragment and elbow stability after radial head replacement
4) The degree of fracture displacement
5) Patient age and bone quality
The size of the fragment and degree of elbow instability following radial head fixation or replacement most often determines the intraoperative decision on coronoid fragment fixation.
The radial head is a secondary restraint to posterolateral rotatory instability (PLRI) of the elbow, while the coronoid provides an anterior and varus buttress to the ulnohumeral joint, resisting posterior dislocation. The medial ulnar collateral ligament attaches to the anteromedial facet of the coronoid, so large medial facet fractures may displace and cause varus posteromedial instability (PMRI). However, in terrible triad injuries (causing PLRI), small coronoid tip fractures are more common. These are typically left as they most often do not contribute to elbow instability. Therefore in most cases, radial head replacement and lateral ligamentous repair are sufficient to restore stability.
However larger coronoid base fractures may require fixation in order to stabilize the elbow. In these cases, the coronoid fracture may be addressed through the lateral window after radial head resection and before the trial implant is assessed. The anterior capsule can be tied down to the ulna or if the fracture is large enough, it may sometimes tolerate internal fixation.
Conversely, a buttress plate for the coronoid may be applied via a medial approach in the setting of a large coronoid base fracture as in PMRI.
Ring et al. reviewed 11 terrible triad injuries including 7 of which had the radial head surgically addressed and 4 of which had undergone radial head excision. The authors found that all four patients who underwent radial head excision dislocated after surgery. Only four patients had a satisfactory result, and all of these had fixation of the radial head, two requiring concomitant repair of the lateral ulnar collateral ligament (LUCL). The authors concluded that terrible triad injuries were unstable, prone to redislocation and that radiocapitellar contact is critical for ulnohumeral stability.
Pugh et al. reviewed 36 cases of terrible triad injuries in which all coronoid fractures were addressed, either with screw fixation or suture repair of the anterior capsule. The authors reported that the average arc of motion postoperatively was 112 degrees, Mayo score was 88, and concentric stability was restored in 34/36. There were 8 complications requiring re-operation. They concluded that coronoid fixation with radial head fixation or replacement yields a stable elbow suitable for early motion.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They found that radial head excision even in the setting of an intact LUCL lead to posterolateral laxity. Furthermore, if 30% of the coronoid tip was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement. However, if 50% of the coronoid was
excised, even with a radial head replacement dislocation occurred. They concluded that so long as the radial head is replaced, small coronoid fractures may not need to be repaired.
Figure A demonstrates a comminuted radial head fracture, a small coronoid fracture, and subluxation of the ulnohumeral joint.
Incorrect answers:
Answer 1: The degree of radial head comminution impacts the decision to replace or fix the radial head. However, this does not affect the decision to fix the coronoid.
Answer 2: Though the tip of the coronoid often remains attached to the anterior capsule which attaches slightly distal to the coronoid tip, there is no deforming force on this fracture which is instead a shear and not an avulsion injury.
Answer 4: Elbow stability, not the degree of coronoid displacement, affects the decision to address the fracture.
Answer 5: The patient's age and bone quality does not factor into elbow stability or decision making on coronoid fixation.
What is the most appropriate plating technique utilized for the medial malleolus fracture typically seen in a displaced supination-adduction ankle fracture?
1) Tension band plating
2) Antiglide plating
3) Bridge plating
4) Neutralization plating
5) Submuscular plating
A supination-adduction ankle fracture leads to a vertical fracture of the medial malleolus. Traditional fixation of the medial malleolus with oblique screws from the tip of the malleolus directed proximally will ineffectively protect against shear forces at the fracture site; these also are directed quite obliquely to the vertical fracture line, and therefore have poor biomechanical resistance to failure. An antiglide plate is used medially to prevent displacement of the fracture segment due to shear forces.
According to the referenced article by Toolan et al, placement of two horizontal (perpendicular to the fracture line) lag screws from medial to lateral are
biomechanically the most important aspect of the construct whether a plate is used or not.
A 25-year-old Norwegian amateur curler slips on the ice, falling onto an outstretched right elbow. He is taken to the local teaching hospital and radiographs demonstrate a significantly comminuted radial head fracture and coronoid base fracture. His elbow is reduced and splinted. To restore stability and allow early range of motion, which of the following will most likely need to be performed in most cases?
1) Radial head fixation or replacement
2) Radial head fixation or replacement and coronoid fixation
3) Radial head fixation or replacement, coronoid fixation, and lateral ulnar collateral ligament (LUCL) repair
4) Radial head fixation or replacement, coronoid fixation, LUCL and medial ulnar collateral ligament (MUCL) repair
5) Radial head fixation or replacement, coronoid fixation, LUCL and MUCL repair, and application of a hinged fixator
The patient has sustained a "terrible triad" injury, classically involving a radial head fracture, coronoid fracture, and elbow dislocation. These often involve LUCL injuries and a traumatic injury in the radiocapitellar joint. Stability is achieved with radial head replacement (or fixation), coronoid fixation (in cases with a large coronoid fracture), and lateral soft tissue repair.
Posterolateral rotatory instability (PLRI) following a terrible triad injury is usually caused by a fall on an extended arm that produces a valgus, axial, and rotatory force. The mechanism of injury begins laterally and moves medially.
Hence, the LUCL fails first, followed by the anterior capsule (or coronoid), and lastly the MUCL. Even following fixation, patients often lose some degree of their flexion-extension arc, may develop post-traumatic arthritis, or most commonly may have persistent instability. The radial head is a primary restraint to PLRI and must be either replaced with a prosthesis or fixed in the setting of a terrible triad injury. Replacement is typically chosen when the radial head is in more than 3 fragments. Coronoid fractures should be fixed when they involve >30-50% of the coronoid base. However, the best way to determine if coronoid fixation is necessary is with an intraoperative fluoroscopic examination.
Forthman et al. reviewed outcomes following the management of 34 elbow fracture-dislocations. In all cases, the radial head was replaced or underwent fixation. The MUCL was not repaired in any case. The authors noted only 2 cases of post-operative instability, one terrible triad, and one combined capitellum and trochlea fracture. The authors noted that both cases were related to non-compliance. The remaining 32 averaged 120 degrees of flexion-extension and 74% had good-excellent outcomes. The authors concluded that MUCL repair is not required for elbow dislocations so long as the radial head, large coronoid fractures, and LUCL are addressed.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They found that radial head excision even in the setting of an intact LCL leads to posterolateral laxity. If 30% of the coronoid was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement. However, if 50% of the coronoid was excised, even with a radial head replacement, dislocation occurred. This led the authors to conclude that long as the radial head was replaced, small coronoid fractures may not need to be repaired.
Papatheodorou et al. reviewed 14 terrible triad injuries (all of which had Regan-Morrey type 1 or 2 coronoid fractures) that underwent surgical fixation or replacement of the radial head combined with LUCL repair. The authors noted that intraoperative stability was confirmed in all cases without coronoid fixation, MCL repair, or an external fixator. The authors concluded that coronoid fixation is not required in fractures up to 50% the height of the coronoid and that MCL repair is not necessary.
Incorrect answers:
Answer 1: Large coronoid base fractures need to be fixed in PLRI to confer elbow stability.
Answer 2: The lateral collateral ligamentous complex should be repaired as this soft tissue sleeve is usually avulsed in elbow dislocations.
Answer 4: In PLRI, ligamentous repair of the medial aspect of the elbow is often unnecessary.
Answer 5: A hinged fixator (internal or external) is not typically required. This could be applied in a case where the elbow is persistently unstable at the conclusion of the case.
A 32-year-old female sustains the injury shown in Video A. The right-sided pelvic injury is best classified as which of the following?
1) Lateral compression 1
2) Lateral compression 2
3) Vertical shear
4) Anterior-posterior compression 2
5) Anterior-posterior compression 3
The injury shown in Video V reveals a right sided posterior ilium fracture, which is known as a crescent fracture. The presence of a crescent fracture is consistent with a lateral compression type 2 injury; this differentiates this from a type I injury. The ipsilateral anterior sacrum has a small impaction injury anteriorly while the contralateral SI joint has a minor amount of anterior sacral impaction indicative of a lateral compression type I injury.
The reference by Burgess et al is the primary source of the mechanism classification of pelvic ring injuries. Overall blood replacement averaged 5.9 units (lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units). Overall mortality was 8.6% (lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear,
0%; combined mechanical, 18.0%).
Incorrect answers:
1: The presence of a crescent fracture means this is at least a LC-2 injury. The left-sided fracture pattern is consistent with an LC-1 pattern.
3: A vertical shear fracture pattern would exhibit some vertical displacement and does not typically exhibit the crescent fragment.
4: The fracture pattern does not match an anterior-posterior compression pattern.
5: The fracture pattern does not match an anterior-posterior compression pattern.
A 35-year-old zookeeper fell 10 feet while preparing an exhibit for a grand reopening, landing on his left arm. The patient is then evaluated by a keen orthopedic resident in the emergency room who describes the zookeeper's injuries to his chief. He describes a comminuted radial head fracture and posterolateral ulnohumeral dislocation. The chief resident orders a CT scan which demonstrates a coronoid fracture involving 50% the height with no involvement of the anteromedial facet. During surgery, the trauma surgeon replaces the radial head and repairs the lateral collateral ligament complex. The
elbow is splinted in elbow flexion and pronation. The patient begins range of motion exercises with her occupational therapist 3 days after surgery, and her elbow dislocates. What is the most likely reason for her instability?
1) Length of immobilization
2) Position of immobilization
3) Lack of coronoid fixation with medial buttress plate
4) Lack of coronoid fixation from lateral approach
5) Lack of medial collateral ligament repair
The zookeeper sustained a "terrible triad" injury with resulting posterolateral rotatory instability (PLRI). To prevent post-operative instability, large coronoid fractures should be fixed, and this would be performed through a lateral approach given that the radial head will be replaced.
The coronoid serves as an anterior and varus buttress to the ulnohumeral joint, resisting posterior dislocation. Though the coronoid tip has no soft tissue attachments, the medial ulnar collateral ligament attaches to the anteromedial facet of the coronoid. A coronoid fracture through the anteromedial facet, such as in the setting of posteroMEDIAL rotatory instability, would require a medial buttress plate to restore varus stability. In a coronoid base fracture involving 50% of the coronoid, fixation is required even when a radial head arthroplasty is performed. This can be done with suture fixation via a bone tunnel through the ulna or with screws from dorsal to volar. Failure to fix a large coronoid base fracture would result in persistent instability, as with the patient in this vignette.
Ring et al. reviewed 11 terrible triad injuries - including 7 of which had the radial head surgically addressed and 4 of which underwent radial head excision. They noted that all four patients who underwent radial head excision dislocated after surgery. Moreover, only four patients had a satisfactory result, and all of these had fixation of the radial head, with two requiring concomitant repair of the lateral ulnar collateral ligament (LUCL). The authors concluded that terrible triad injuries are unstable, prone to redislocation and that radiocapitellar contact is critical for ulnohumeral stability.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They showed that radial head excision even with an intact LUCL resulted in persistent posterolateral laxity. If 30% of the coronoid was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement alone. If 50% of the coronoid was excised, even with
a radial head replacement, dislocation occurred. The authors concluded that so long as the radial head was replaced, small coronoid fractures may not need to be repaired, but large fractures involving 50% or more would require fixation even if the radial head and LUCL were addressed.
Moro et al. treated 25 unreconstructible radial head fractures with a metal radial head arthroplasty. The authors reported a DASH score of 17, PRWE of 17, and Mayo elbow score of 80. Poor outcomes were seen in those with psychiatric disorders or those involved in a worker's compensation claim. The authors reported that radial head arthroplasty resulted in stable elbows with mild-moderate physical impairment.
Ring, Quintero, and Jupiter reviewed 56 patients with radial head fractures who underwent surgical fixation. Of the comminuted Mason type-3 fractures that underwent ORIF, they found that 13/14 had a poor result. The authors recommend that fractures with 3 or fewer fragments are amenable to fixation while those with 4 or more articular fragments are not.
Incorrect answers:
Answer 1: Early range of motion is appropriate after adequate fixation. Answer 2: Flexion and pronation is the position that stabilizes the lateral elbow. In the setting of PLRI, this is the correct position to splint the upper extremity in following surgery, therefore the position of immobilization is not the issue in this case.
Answer 3: Large anteromedial facet fragments result in posteromedial rotatory instability. These do not typically occur in conjunction with a radial head fracture. These result in varus instability and need to be buttressed with a medial plate. In this case, a medial buttress plate is not needed.
Answer 5: In PLRI, the medial side of the elbow is not typically addressed. The more obvious cause of instability is the lack of coronoid fixation.
Which of the following injuries would require plating of the radius along with closed reduction and evaluation of the distal radioulnar joint (DRUJ)?
1) Nightstick fracture
2) Galeazzi fracture
3) Monteggia fracture
4) Rolando fracture
5) Smith fracture
A Galeazzi fracture is a fracture of the distal third of the radius with dislocation of the distal radioulnar joint. It commonly results from a fall onto an outstretched hand with the forearm in pronation.
A Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction and fixation of the radial shaft, and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. Otherwise, either open or closed reduction with pinning can be undertaken to stabilize the joint. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
Acute intervention results in improved outcomes as compared to delayed reconstruction.
Rettig et al. retrospectively analyzed 40 patients with Galeazzi fracture-dislocations that were treated with open reduction and internal fixation of the radial shaft fracture. They noted that a radial shaft fracture located within
7.5cm of the articular surface resulted in a 55% incidence of DRUJ instability, while 5.6% of those located further from the joint were unstable. They concluded that a high index of suspicion, early recognition, and acute treatment of DRUJ instability will avoid chronic problems in this complex injury.
Illustration A is an AP and lateral radiograph demonstrating a Galeazzi fracture. Incorrect Answers:
Answer 1: A nightstick fracture is an isolated ulnar shaft fracture.
Answer 3: A Monteggia fracture is a proximal ulnar fracture associated with a radial head dislocation.
Answer 4: A Rolando fracture is a comminuted intra-articular fracture through the base of the first metacarpal bone.
Answer 5: Smith fractures are fractures of the distal radius with associated volar angulation of the distal fracture fragment(s).
In trauma patients with multiple injuries, patients with scapula fractures have been shown to have an association with which of the following, as compared to patients without scapula fractures?
1) Increased length of hospital stay
2) Increased mortality rate
3) Increased rate of extremity fracture(s)
4) Increased Injury Severity Scores
5) Increased length of intensive care unit stay
According to the reference by Veysi et al, patients presenting to a trauma center with scapula fractures have an increased rate of pulmonary complications and increased Injury Severity Scores (ISS), but have no difference in mortality, length of ICU stay, or overall hospital stay. No differences were seen in abdominal or head injury rates either. A lower rate of extremity fractures was seen as compared to non-scapular fracture patients in their series.
According to the referenced study by Brown et al, rib fx (44%) are the most common associated injury with scapula fractures.
All of the following techniques can help to prevent apex-anterior angulation during intramedullary nailing of proximal one-third tibia fractures EXCEPT:
1) Posterior blocking screw
2) Posterior starting hole
3) Interlocking the nail in a semi-extended knee position
4) Anteriorly directing the nail
5) Anterior blocking screw
Sagittal malalignment is commonly seen after nailing proximal tibia fractures. The start point as well as the direction of the nail can lead to sagittal deformity. Freedman found in nailing tibia fractures that malalignment was seen in 58% of proximal third fractures, 7% of middle third fractures, and 8% of distal third fractures. Of the malaligned fractures, 83% were either segmental or comminuted.
Lang found that a medialized nail entry point and a posteriorly and laterally directed nail insertion angle contributed to malalignment. It is logical that a fracture that is reamed and then nailed in the posterior direction will lead to a gap anteriorly, and that posterior comminution will lead to anterior angulation as the fracture hinges on the intact cortex anteriorly. An anterior starting hole will tend to lead to more of a posterior nail direction.
Tornetta found that using only 15 degrees knee flexion (semi extended) eliminated the extension force of the quadriceps on the proximal fragment, which otherwise would have tended to cause anterior angulation at the fracture site; therefore interlocking in flexion leads to anterior angulation.
Krettek found that a posteriorly placed blocking screw is meant to prevent posterior placement of the nail and therefore encourages decreased anterior angulation of the fracture.
Henley found that if the fracture is high and the nail bend is within the distal fracture fragment, as the nail is inserted, the nail will drive the distal fragment posteriorly.
Which of the following factors has been shown to be the strongest predictor of screw cutout of a dynamic compression hip screw used for an intertrochanteric femur fracture?
1) Age of the patient
2) Intrinsic stability of the fracture
3) Tip-apex distance
4) Quality of reduction
5) Angle of the sideplate
Illustration A found below depicts the method to calculate Tip-apex distance (TAD). The tip-apex distance is the sum of the distances from the tip of the lag screw to the apex of the femoral head as seen on the AP and lateral radiographs.
Baumgaertner et al reported that he had no screws cut out if the tip-apex distance was less than 25mm. Tip-apex distance was the strongest predictor of cutout. Increasing age of the patient, poor reduction, use of a high angle sideplate, and unstable fracture were weaker predictors of cutout.
Kyle et al demonstrated that obtaining an anatomic reduction when using a sliding hip screw with intertrochanteric fractures leads to the best radiographic and clinical outcomes.
A 66-year-old male sustains an open crush injury to his right lower leg with significant skin loss. His history is significant for COPD, diabetes controlled with an insulin pump, and testicular cancer treated with bleomycin twenty years ago. A radiograph of the chest shows a small pneumothorax which is being observed and does not require a thoracostomy tube. Which of the following is not a contraindication to hyperbaric oxygen treatment for this patient?
1) Presence of an acute open fracture and crush injury
2) History of COPD
3) History of bleomycin treatment
4) Presence of a pneumothorax
5) Presence of an insulin pump
The presence of a crush injury to an extremity is an indication for hyperbaric oxygen (HBO) therapy. The remainder of the options listed are contraindications to hyperbaric oxygen treatment.
Hyperbaric oxygen therapy potentially can provide enhanced oxygen delivery to peripheral tissues affected by vascular disruption, cytogenic and vasogenic edema, and cellular hypoxia caused by extremity trauma. The idea behind HBO is to provide enhanced oxygen delivery to peripheral tissues affected by vascular disruption, cytogenic and vasogenic edema, and cellular hypoxia caused by extremity trauma.
Greensmith et al provide a review of HBO therapy and discuss the relative and absolute contraindications and indications for this treatment. They report in patients with crush injury or early compartment syndrome, hyperbaric oxygen therapy may reduce the penumbra of cells at risk for delayed necrosis and secondary ischemia. They report that both animal studies and prospective human clinical trials suggest the benefits of such therapy.
Buettner et al found that based on clinical evidence and cost analysis, medical institutions that treat open fractures and crush injuries are justified in incorporating HBO theray as a standard of care.
Illustration A shows an example of a hyperbaric oxygen(HBO) chamber. Incorrect Answers:
Answer 2: COPD is a contraindication to hyperbaric oxygen treatment due to
the possible presence of air trapping or bleb formation, which could place the patient at risk of pneumothorax.
Answer 3: History of bleomycin treatment is a contraindication to hyperbaric oxygen treatment because supplemental oxygen may cause life threatening pneumonitis.
Answer 4: Presence of a pneumothorax is a contraindication as hyperbaric oxygen treatment may cause a gas embolism, tension pneumothorax, or pneumomediastinum.
Answer 5: Presence of an insulin pump is a contraindication to hyperbaric oxygen treatment because malfunction or deformation of the device may occur under pressure.
A 34-year-old male falls off of a ladder and sustains the ankle injury shown in Figure. Which of the following is unique with this particular ankle fracture pattern and must be recognized by the operating surgeon to optimize outcomes?
1) Marginal impaction of the anteromedial tibial plafond
2) Syndesmosis diastasis
3) Deltoid ligament tear
4) Posterolateral osteochondral lesion of the talus
5) Fibular overlengthening
The radiograph demonstrates a Lauge-Hansen supination-adduction fracture-dislocation. There is a transverse fibula fracture and a vertical medial malleolus fracture.
McConnell and Tornetta performed a Level 4 review and found that nearly 50% of these injuries have marginal impaction of the anteromedial tibial plafond and they found that anatomic reduction of that aspect of the injury led to good to excellent outcomes.
A 42-year-old female undergoes a subtalar bone block distraction arthrodesis as sequelae of a nonoperatively treated calcaneus fracture ten years prior. This procedure improves which of the following issues?
1) Subtalar joint stiffness
2) Midfoot supination
3) Sinus tarsi impingement
4) Anterior ankle impingement
5) Hammertoe deformity
The subtalar fusion technique involves distraction of the subtalar joint, insertion of a bone block, fusion, and rigid screw fixation. The distraction allows correction of the talocalcaneal relationship.
In Carr’s series, pre- and postoperative radiographic analysis for tibiotalar impingement, lateral talocalcaneal angle, and talonavicular alignment was performed, with improvement to a normal range seen in the cases analyzed.
Bednarz did a radiographic analysis and showed an average increase of 8 mm in hindfoot height, 9 degrees in lateral talocalcaneal angle, and 11 degrees in lateral talar declination angle.
Rammelt found that compared with the unaffected side, the talocalcaneal height was corrected by 61.8%, the talus-first metatarsal axis by 46.5%, the talar declination angle by 38.5% and the talocalcaneal angle by 35.4%. Based on these three
Scientific References
- , this procedure ultimately addresses the lost hindfoot height, subtalar arthritis (joint is fused), ankle impingement (improvement of the talus 1st MT axis), and peroneal impingement. It does not address hindfoot valgus. However, the deformity after a calcaneus fracture is usually from lateral wall blowout and hindfoot varus.
Illustration A shows a lateral radiograph of a distraction/bone block subtalar arthrodesis.
A 29-year-old male sustained a mid-shaft femur fracture in a motorcycle accident. Which of the following is associated with approximately 5% of patients sustaining this injury?
1) Heterotopic ossification
2) Ipsilateral femoral neck fracture
3) Ipsilateral posterolateral corner injury
4) Pudendal nerve injury
5) Ipsilateral superficial femoral artery injury
Ipsilateral femoral neck fractures are seen in 1-9% of femoral shaft fractures and the femoral neck must be properly imaged either preoperatively or intraoperatively in any patient with a femoral shaft fracture. Dedicated hip films, possibly including an internal rotation AP, should be obtained before entering the OR.
Daffner et al reported that in 11 of 20 cases of combined femoral shaft and neck fractures, the initial preoperative radiographs did not demonstrate the femoral neck fracture. Intraoperative fluoroscopy should also be used to evaluate for a femoral neck fracture both before (to evaluate for unrecognized fx) and after (to evaluate for iatrogenic fx) IM nailing.
Tornetta et al also describe using preoperative CT scans to evaluate for a
femoral neck fracture and found that they were able to reduce the number of missed ipsilateral femoral neck fractures.
A 51-year-old right-hand-dominant male fell onto his left arm and sustained the isolated injury shown in Figures A and B approximately 6 months prior to presentation. Examination of the wrist is notable for a stable DRUJ and no tenderness. The elbow shows no ligamentous laxity, and the patient reports isolated elbow pain during attempted pronation/supination Current radiographs reveal a malunited radial head fracture. Treatment should now consist of?
1) Radial head resection
2) Radial head replacement
3) ORIF of the malunited fracture
4) Arthroscopic debridement
5) Total elbow replacement
The injury films represent a highly comminuted radial head fracture, which when treated with ORIF, is likely to have a poor outcome especially in the delayed setting. In the absence of DRUJ and elbow instability, and no wrist tenderness, radial head resection is the best treatment option. While a radial
head prosthesis may theoretically prevent proximal radial head migration that can occur with radial head excision, this is unlikely in an isolated radial head fracture without other ligamentous injury (elbow ligaments, interosseous membrane or DRUJ).
Herbertsson et al (March, 2004) reported on 100 patients with Mason II and III radial head fractures. Nine of those initially treated nonoperatively had continued pain and underwent late radial head excision with good results.
In another report by Herbertsson et al (September, 2004) the authors report on radial head excision in both an acute and delayed setting and found fair-good results for most patients in both subgroups.
Jackson et al present a review article on radial head fractures where management and operative technique are discussed.
Finally, Antuna et al in their study conclude "Radial head resection in young patients with isolated fractures without instability yields long-term satisfactory results in >90% of cases. Osteoarthritic changes are uniformly present but typically are not associated with functional impairment".
What risk factor leads to the highest rate of postoperative loss of reduction in unstable posterior pelvic ring injuries?
1) Type of anterior fixation
2) Male sex
3) Usage of a transiliac bar
4) Vertical sacral fracture
5) Sacroiliac joint fracture-dislocation
According to the referenced article by Griffin et al, the risk of postoperative loss of reduction is greatest with a vertical sacral fracture pattern (13%, all within 3 weeks). There was no significant association between failure and anterior fixation method, iliosacral screw arrangement or length, or any demographic or injury variable.
Their conclusion: "Percutaneous iliosacral screw fixation is a useful technique in the management of vertically unstable pelvic fractures, but a vertical sacral fracture should make the surgeon more wary of fixation failure and loss of reduction."
A 22-year-old male sustains the closed injury seen in figure A. The injury is best treated with which of the following methods?
1) External fixation
2) Flexible intramedullary nailing
3) Open reduction and internal fixation with acute bone grafting
4) Open reduction and internal fixation
5) Closed reduction and functional bracing
The xray shows a comminuted, high energy both bone forearm fracture. Open reduction and internal fixation without bone grafting is the most appropriate treatment. Acute bone grafting is only indicated if a large bony void, such as segmental bone loss of the radius, is present to allow the displaced bone ends to heal together despite their diastasis.
In Moed et al's review, primary internal fixation in open forearm fractures led to nearly a 90% union rate (44/50) and good/excellent results in 85%.
Autogenous cancellous grafting was anecdotally recommended if interfragmental compression could not be obtained.
In Wright et al's review, there was no significant difference between union rates in comminuted both bone forearm fractures whether or not autograft was used (97% v. 98%). The fractures in this series were all comminuted without open injuries.
Ring et al. reported on their series of comminuted forearm fractures, assessing risks of nonunion. They reported that the largest risk of nonunion was associated with polytrauma patients, followed by open injuries. They found no improvement in union with acute grafting any of their forearm injuries in this series.
Incorrect Answers:
QUESTION 49 OF 50
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
The surgical approach for definitive reduction and stabilization of this pattern is
---
---


Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
The surgical approach for definitive reduction and stabilization of this pattern is
---
---
1
anterior midline.
2
anterolateral.
3
medial parapatellar.
4
posteromedial.
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally
stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally
stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
QUESTION 50 OF 50
of 100
A 16-year-old boy who is a competitive basketball player (Figure 43)

A 16-year-old boy who is a competitive basketball player (Figure 43)
1
Ligamentous reconstruction
2
Meniscal repair
3
Meniscectomy 39
4
Immobilization
- Meniscal repair
